
4
Emergency Medical Services Response to Cardiac Arrest
Overall outcomes from out-of-hospital cardiac arrest (OHCA), both in terms of survival and neurologic and functional ability, are poor: only 11 percent of patients treated by emergency medical services (EMS) personnel survive to discharge (Daya et al., 2015; Vellano et al., 2015). Although a few EMS systems have demonstrated the ability to significantly increase survival rates (Nichol et al., 2008; Sasson et al., 2010b), a fivefold difference in survival-to-discharge rates exists among communities in the United States (Nichol et al., 2008). This presents important challenges and opportunities to improve EMS system performance across the country.
As described in Chapter 1, the chain of survival includes five interconnected links: (1) immediate recognition of cardiac arrest and activation of the emergency response system, (2) early cardiopulmonary resuscitation (CPR), (3) rapid defibrillation, (4) effective advanced cardiac life support (ACLS), and (5) integrated post-resuscitative care (M. D. Berg et al., 2010; R. A. Berg et al., 2010). This conceptual model illustrates the sequence of events that can optimize care and outcomes for the approximately 395,000 individuals who experience an OHCA in the United States each year (Daya et al., 2015). Together, the first three steps comprise the fundamental actions within basic life support (BLS) strategies for cardiac arrest (R. A. Berg et al., 2010), including early recognition of a cardiac arrest by bystanders1 and 911 call takers, as well as the delivery of initial treatments (i.e., CPR and defibrillation) by bystanders
________________
1See Chapter 3 for a discussion of barriers and opportunities to improve bystander early access of the EMS system, as well as bystander education and training programs.
or trained first responders prior to the arrive of EMS providers (i.e., emergency medical technicians [EMTs] and paramedics).
Although the ability of an EMS system to respond effectively to cardiac arrest within a community depends to some extent on basic infrastructure and the training of EMS personnel, there are specific character-characteristics and capabilities of EMS systems that are correlated with higher cardiac arrest survival rates. This chapter focuses on the EMS system’s response to cardiac arrest and covers the EMS role across all of the links in the chain-of-survival model. Because the overall structure, organization of services, and capabilities of EMS systems affect cardiac arrest care, the chapter begins with an overview of the EMS system, including discussion of the relevant personnel and oversight at the federal, state, and local levels. The second section covers elements of the EMS response itself, including the facilitation of bystander CPR and early defibrillation strategies. The final section of the chapter focuses on opportunities to improve the timeliness and quality of cardiac arrest care, which can lead to improved patient outcomes in communities across the United States.
OVERVIEW OF EMS
For purposes of this report, the committee defines an EMS system as a system that provides emergency medical care in response to serious illness or injury, such as a cardiac arrest, in the prehospital setting. An EMS system comprises a wide range of responders who provide critical services, such as response to 911 emergency calls, dispatch of medical personnel, triage, treatment, and rapid transport of patients by ground or air ambulances to appropriate care facilities (IOM, 2007). Emergency medical response and care involves different types of people and agencies, including those in the public health, public safety, and health care sectors (see Table 4-1). As such, multiple regulatory and administrative bodies at local, state, and federal levels regulate different aspects of emergency medical care, leading to different resource and funding streams available for implementation and evaluation activities.
The myriad responsibilities of an EMS system make it challenging to assess its general performance, or to measure the impact of individual EMS system protocols and characteristics on overall system performance or particular health outcomes, such as cardiac arrest survival and

FIGURE 4-1 Contributing sectors of the emergency medical services system.
SOURCE: IOM, 2007, p. 40.
neurologic or functional outcomes. Nonetheless, some experts have argued that OHCA survival rates are a reliable and valid measure of an EMS system’s overall effectiveness and may be the most appropriate measure for comparing performance among EMS systems (AHA, 2000; El Sayed, 2011). This is because the complex and emergent nature of cardiac resuscitation requires not only highly competent EMS personnel, but also integration and formal transitions among components of the larger EMS system and between EMS and the hospital systems with which it interacts.
EMS Personnel Involved in Cardiac Arrest Response
Within an EMS system, a number of trained professionals act in concert when responding to a cardiac arrest (see Box 4-1). For example, 911 call takers or emergency medical dispatchers2 may help identify a cardiac arrest and dispatch the appropriate EMS providers. EMTs and paramedics
________________
2For simplicity, this report uses the term “dispatcher” to generally indicate personnel responsible for 911 call taking and EMS provider dispatch (see Box 4-1). This is consistent with recent Utstein core measures and with terminology generally used in emergency medicine and by the public, although “telecommunicator” is becoming more widely used.
may assess the scene to confirm whether the patient is in cardiac arrest and initiate resuscitation. They also transport the patient to the most appropriate definitive care facility—usually the closest hospital that is best equipped to care for a cardiac arrest patient. When providing patient care, both EMTs and advanced-level providers operate under a combination of physician-approved standing orders (i.e., offline medical direction), as well as real-time medical control. The state medical director oversees the entire EMS system and evaluates performance within each link in the chain of survival, while local medical directors support EMS agencies at the local, city, or county level. The responsibilities of medical directors at any level typically include, but are not limited, to establishing medical protocols for dispatchers, EMTs and paramedics; providing medical supervision online and offline; promoting evidence-based practices; supervising ongoing medical quality improvement; supervising training and continuing education; establishing controlled substance policies; and providing medical discipline (ACEP, 2012a).
EMS staffing models for cardiac arrest response often vary, in part, because of differences in the availability and proximity of the nearest providers, resources, and call volume. In suburban and urban communities, a combination of basic EMTs (EMT-Bs) and paramedics typically provide EMS care, while rural areas often provide EMS care with EMT-B-level providers exclusively. In some communities, a single responding unit may arrive with one EMT and one paramedic who must conduct the entire resuscitation without additional medical support. In many urban communities, a tiered response system is used that consists of two or more units; the first unit dispatched to the scene is staffed with basic EMTs trained in CPR and AED use, and the second unit is staffed with one or more paramedics trained and equipped to perform advanced life support. This tiered-model has advantages in that more basic-level providers are available to provide defibrillation and to perform chest compressions, allowing providers to rotate out frequently in order to avoid fatigue and diminishing CPR quality. Other communities staff all responding units with at least one paramedic, and sometimes more. Many fire-based EMS systems employ a combination of fire department vehicles (e.g., fire engine trucks) staffed by firefighters with EMT-B training, and one or more ambulances staffed
BOX 4-1
Emergency Medical Services Personnel
Emergency medical dispatchers (also known as 911 dispatchers, 911 operators, or telecommunicators) is a general term for professionals who receive 911 calls, gather vital information concerning medical emergencies, rapidly dispatch the appropriate level of EMS providers to the scene, and render assistance via a telephone in the form of CPR and automated external defibrillator (AED) instructions to 911 callers on the scene. In small 911 centers, one individual may answer calls and dispatch EMS providers. In larger centers, the roles of answering calls and dispatching are separated. “Telecommunicator” is an umbrella term used for any individual who works in a 911 center and has responsibility for receiving calls and/or sending help.
Emergency medical technicians are emergency health care providers who are trained to respond quickly to emergency situations regarding medical situations, traumatic injuries, and accident scenes. There are several different levels of providers and variations in the exact scope of practice between different EMS systems.
- Basic EMTs (EMT-Bs) are trained to provide basic, noninvasive prehospital care (although some states may allow them to perform selected invasive procedures). These personnel provide the initial aspects of care, including CPR, bag valve mask ventilation, and defibrillation at the scene of a medical emergency and during transport to the hospital.
- Advanced EMTs (EMT-As) are mid-level providers between the EMT-Bs and paramedics. They can provide interventions beyond basic life support including techniques for supporting circulation and ensuring an open airway, sufficient oxygen, and adequate ventilation. EMT-As are also authorized to start intravenous lines and administer a basic collection of medications. Their training builds on an EMT foundation and includes additional didactic and clinical elements that differ from state to state.
- Paramedics (EMT-Ps) are trained to provide advanced life support. They receive 1,000 to 2,500 hours of training depending on state requirements and paramedic school. EMT-Ps may provide CPR; defibrillation; intravenous, intraosseous, and central line placement; endotracheal intubation; laryngeal mask airway; and medication administration. The specific medications they are permitted to administer vary widely, based on local standards of care, legal restrictions, and physician or medical director preferences.
Advanced-level providers include flight medics and flight nurses. Flight nurses are registered nurses who have advanced critical care training and expertise. They provide prehospital emergency care to all types of patients during aeromedical evacuation aboard various types of medically equipped aircraft. Flight nurses are often paired with flight medics to serve as emergency and critical transport teams.
EMS medical directors have a multidimensional job of providing specialized medical oversight, as well as assisting in the development of EMS systems. The medical director is most commonly a board-certified emergency medicine physician who has particular interest and experience in prehospital care. The medical director acts as a liaison between public and private EMS agencies; hospitals; local, regional, state, and national EMS systems; national professional organizations; and other community stakeholders. The medical director assists in the development, implementation, and measurement protocols, and also ensures training and proficiency of EMS personnel.
by EMTs and paramedics. In these tiered systems, the fire department vehicles are deployed first, followed by ambulances that will transport the patient. The staffing model employed by any EMS system should promote the ability to rapidly provide high-quality CPR and defibrillation for each and every resuscitation attempt, whether the patient is an adult, adolescent, or child. Although uncommon, the special difficulties associated with pediatric resuscitation merit attention, and are discussed later in this chapter. Precisely how differences in staffing models affect performance, or how successful models developed for one community can be adapted to the needs of another, remains unclear and is a focus of ongoing research.
EMS System Oversight
Today’s EMS systems are better equipped to respond to disasters and complex medical needs—such as cardiac arrest—than in decades past. However, the field as a whole continues to exhibit signs of fragmentation, an absence of systemwide coordination and planning, and a lack of federal, state, and local accountability. To better ensure collaboration and to minimize the negative effects of disconnected institutional authorities on cardiac arrest care, it is important to understand the roles that the federal government, states, and local communities play in the oversight and evaluation of EMS system performance and how they may better work together to improve cardiac resuscitation.
Role of the Federal Government
Federal EMS oversight does not belong to a single agency or department. Instead, numerous federal agencies play assorted roles in supporting the implementation and evaluation of local, regional, and state EMS systems (IOM, 2007). Box 4-2 includes examples of federal entities and their role in overseeing EMS systems and cardiac arrest care.
Lack of integration among the federal government programs that support and regulate EMS systems contributes to unnecessary redundancies, regulatory gaps, confusion, and wasted resources. The U.S. Department of Transportation’s National Highway Traffic Safety Administration (NHTSA) has taken the informal lead for EMS oversight through its Office of EMS, which is responsible for reducing “death and disability by providing leadership and coordination to the EMS community in assessing, planning, developing, and promoting comprehensive, evidence-based emergency medical services and 911 systems” (NHTSA, 2015a). Both NHTSA and the U.S. Department of Homeland Security (DHS) develop best practices or performance standards for EMS (see Box 4-2). In 2009, NHTSA developed a set of 35 consensus-based performance standards for EMS systems, including several that are relevant to treatment of cardiac arrest (NHTSA, 2009a). NHTSA has also collaborated on research exploring the development, implementation, and evaluation of guidelines for EMS (Wright, 2014). As a direct result of this work, guidelines specific to multiple treatments and conditions were published in 2014 (Gausche-Hill et al., 2014; Shah et al., 2014; Thomas et al., 2014). Meanwhile, DHS has helped produce literature on funding sources for EMS and on the role of state EMS medical directors (DHS, 2012). The Field EMS Bill—which Congress introduced to designate NHTSA as the lead federal agency for EMS—further confused the issue (Doyle, 2011; NAEMSP, 2011). Almost simultaneously, the International Association of EMS Chiefs and the National EMS Labor Alliance produced a white paper arguing that the jurisdiction over EMS provided to DHS by the 2002 Homeland Security Act made it the most appropriate lead agency for EMS (IAEMSC, 2011). Greater clarity in terms of federal government oversight and clear scope of authority would be useful.
BOX 4-2
Examples of Federal Responsibilities and Activities Related to EMS Oversight and Cardiac Arrest Care
The U.S. Department of Transportation (DOT), through NHTSA’s Office of EMS, partners with public and private organizations to advance a national vision for EMS, facilitate EMS workforce data collection and analysis, and promote system performance evaluation through guideline development and benchmarking metrics, including public safety answering point (PSAP) contact to defibrillation and electrocardiogram intervals (NHTSA, 2009a). NHTSA’s EMS-related activities include identification of national data elements, development of data collection protocols, maintenance of the National EMS Information System (described in Chapter 2), and development of national EMS education standards and performance standards (NHTSA, 2015a).
- The Centers for Disease Control and Prevention’s (CDC’s) Division of Heart Disease and Stroke Prevention provides public health leadership to improve cardiovascular health, reduce the burden, and eliminate disparities associated with heart disease and cardiac arrest. CDC’s North American Collaborating Center promotes and coordinates the development of medical diagnostic and procedure codes, including those related to cardiac arrest. CDC collaborated on the development of Cardiac Arrest Registry to Enhance Survival (CARES), produces disaster preparedness plans for EMS, and funds EMS-related projects through the National Institute for Occupational Health and Safety.
- The Centers for Medicare & Medicaid Services (CMS) provides reimbursement for identified EMS system transportation costs, including ambulance services, for more than 120 million beneficiaries under the Medicare and Medicaid programs (CMS, 2013, 2015a,b).
- The National Institutes of Health (NIH) funds emergency and trauma-related research through several different NIH Institutes, including the National Heart, Lung, and Blood Institute, which is the lead institute for the study of cardiac arrest.
The U.S. Department of Homeland Security (DHS) “provides the coordinated, comprehensive federal response in the event of a terrorist attack, natural disaster, or other large-scale emergency while working with federal, state, local, and private-sector partners to ensure a swift and effective recovery effort” (NHTSA, 2015c). Within the DHS office
of Health Affairs, the Workforce Health and Medical Support Division identifies first-responder best practices; provides guidance and support for the implementation of those practices; responds to gaps in first-responder disaster planning, resources, and education; and develops cross-DHS EMS protocols, credentialing, and quality assurance standards (DHS, 2013).
The U.S. Department of Defense (DOD) provides criteria, guidance, and instructions to inform EMS delivery through active duty and civilian EMS personnel, who respond to emergencies on military installations and in local communities worldwide as a result of mutual aid agreements with host nations (NHTSA, 2015c).
The Federal Communications Commission (FCC), through its Public Safety and Homeland Security Bureau (PSHSB), works to ensure that first responders, including EMS personnel, have access to reliable, interoperable equipment during emergencies (NHTSA, 2015c). “The PSHSB provides information on federal resources available to EMS personnel, assists in the development of emergency communications plans, and enrolls first-responder organizations in priority services, including the telecommunications service priority, wireless priority service, and government entity telecommunications service” (NHTSA, 2015c).
The Federal Interagency Committee on EMS (FICEMS) ensures coordination among federal agencies involved with state, local, tribal, and regional EMS and 911 systems. NHTSA, in cooperation with the Health Resources and Services Administration and the Assistant Secretary of Health Affairs at DHS, provide administrative support to FICEMS, which employs a technical working group consisting of interagency staff-level employees who meet monthly to provide support to several ongoing EMS projects (NHTSA, 2015c).
The National EMS Advisory Council (NEMSAC) is a national council of EMS representatives and consumers that provides advice and recommendations to NHTSA about EMS. NEMSAC does not have program management or regulatory development responsibilities (NHTSA, 2015c).
A lack of clear administrative oversight also perpetuates divisions among public safety, public health, and health care professionals, who must work as a cohesive unit to respond effectively to cardiac arrest. Clear designation of a lead federal agency “with primary programmatic responsibility for the full continuum of emergency medical services and care for adults and children” would contribute to a “coordinated, regionalized, and accountable emergency and trauma care system” (IOM, 2007, p. 107). This would provide the governance and infrastructure necessary to streamline EMS guideline and performance measure processes and to
coordinate evaluations that could enhance EMS system performance overall and improve care delivery for cardiac arrest specifically.
In addition to the lack of formal federal oversight, the degree to which federal agencies have explicit authority to regulate and coordinate components of EMS systems directly affects the extent to which EMS-related cardiac arrest care can be monitored, evaluated, and standardized. For example, NHTSA is involved in EMS guidelines, benchmarking, and statewide evaluation of EMS systems in order to identify critical performance and information gaps (NHTSA, 2015a). This includes development of national EMS education standards, which define the minimal entry-level competencies for first responders, EMTs, advanced EMTs, and paramedics (NHTSA, 2009b). Separately, NHTSA has produced management, instructor, and trainee guides for emergency medical dispatch programs (NHTSA, 1996a).
Although 48 states voluntarily follow NHTSA’s national standard curriculum for EMS Basic and Paramedic (FICEMS, 2012, p. 243),3,4 accreditation and certification standards for emergency medical dispatchers are currently developed and managed by the private sector, including organizations such as the Association of Public-Safety Communications Officials International (APCO, 2015), the International Academies of Emergency Dispatch (IAED, 2015), and PowerPhone (PowerPhone, 2015). The curricula available through these organizations are not identical and may not adhere consistently to the NHTSA guidelines for training emergency medical dispatchers. Data on how these emergency medical dispatch protocol reference systems (EMDPRSs) are used by EMS is limited: NHTSA’s EMS performance measures only assess the type of EMDPRS an EMS system employs, and whether the use of lights and sirens and the dispatch of EMTs as compared to paramedics is predicated on that EMDPRS (NHTSA, 2009a, pp. 5-7). This lack of standardization has significant implications for implementing and
________________
3The 2011 National EMS Assessment was commissioned to better understand what data about EMS systems is available at state, regional, and local levels (FICEMS, 2012). This assessment used data from the National EMS Information System Technical Assistance Center and the NASEMSO 2011 EMS Industry Snapshot. The results are limited by which states responded to assessment questions and the accuracy of the data submitted. For each statistic presented, the corresponding assessment question is provided.
4The National Association of State EMS Officials (NASEMSO) 2011 EMS Industry Snapshot was delivered to the director of each state’s EMS regulatory office. The data above is based on responses to the question: “Which of the following EMS credentialed levels in your state are based on the current federal DOT curriculum?” Subsequent references to this survey will list the related query.
assessing specific EMS dispatch protocols that have been associated with improved cardiac arrest outcomes, as discussed later in this chapter.
Role of State Governments
State EMS agencies play multiple roles in overseeing and coordinating local and regional EMS activities. In most states, state law governs the scope, authority, and operation of EMS agencies, leading to considerable variability in the size, organizational structure, and funding of EMS agencies from state to state. In the case of funding, 911 services are usually paid for by grants, modest surcharges on telephone bills, or through state and local taxes (NENA, 2015; NHTSA, 2013). Funding levels may fluctuate, and available funding may not be sufficient to develop next-generation 911 capabilities (NHTSA, 2013). Funding for EMS and ambulance services comes from a similarly diverse set of mechanisms (CMS, 2015c; FEMA, 2012).
All states have a state EMS office, and the vast majority of these offices are located within a state department or government entity (FICEMS, 2012, p. 128).5 EMS office responsibilities typically include data collection, professional credentialing, EMS training standards, training programs for EMS professionals, credentialing for EMS training programs, and stroke system management. Forty-six states report having developed EMS data collection systems, 39 require data collection by law, and another 8 plan to begin requiring data collection in the next few years (FICEMS, 2012, pp. 288, 290).6 However, less than half of the states that have legal requirements for data collection actually enforce collection for all EMS response incidents, and only 40 percent of responding state EMS offices report quality assurance and/or improvement activities as a frequent function (FICEMS, 2012, pp. 141, 292).7
State EMS offices are usually managed by state medical directors, a role that has been recognized by several professional organizations (Na-
________________
5NASEMSO Survey Question: “Where is the State EMS Office organizationally positioned within the State?”
6NASEMSO Survey Question: “Does your State maintain a State EMS data system?” and “Is the submission of EMS data to the State required?” At the time of the survey, although Louisiana did not have a state EMS data system, it did intend to begin requiring EMS data collection within a few years.
7NASEMSO Survey Question: “What percentage of the efforts of the State EMS Office are directed toward each of the following?” and “(If yes to the previous question) Based on the following EMS Agency types, what percentage of each is actively submitting data into the State EMS data system?”
tional Association of EMS Physicians [NAEMSP], American College of Emergency Physicians [ACEP], and NASEMSO) as playing an integral role in the safety and quality of prehospital medical care (ACEP, 2012a,b). Thirty-seven states report having an EMS medical director (FICEMS, 2012, p. 191); of those, 18 serve only in an advisory capacity, rather than having a more comprehensive role defined by state law (NHTSA, 2012, p. 192).8 Furthermore, only one state EMS system reported that the medical director’s roles and responsibilities included a cardiac arrest system of care, although data were not available for 14 states (FICEMS, 2012, p. 199).9
Local and Regional Responsibilities
EMS systems are largely local-level operations, with many counties and local municipalities playing instrumental roles, such as determining the EMS system structure; developing training programs on triage, treatment, and transport protocols; and implementing EMS interventions, based on local needs and available resources. There are an estimated 21,283 EMS agencies in the United States with approximately 86 percent of these responding to 911 events (FICEMS, 2012, p. 21).10 Local prehospital services can be managed by fire departments, hospitals, independent government agencies (e.g., public health agency), nonprofit corporations, commercial for-profit companies, or volunteer-supported EMS programs. Most states reported multiple organizational structures for local EMS systems, with fire department, non-fire government, hospital, and private, nonhospital EMS systems being most common (FICEMS, 2012, p. 31).11 This diversity suggests that training of EMS personnel needs to be adapted to the particular types of providers and organizational structures in a given system.
________________
8NASEMSO Survey Question: “Do you have a State EMS Medical Director?” and “Please select the appropriate response regarding the authority of the State EMS Medical Director within your State.”
9NASEMSO Survey Question: “What are the roles and responsibilities of the State EMS Medical Director?”
10Not all EMS systems respond to 911 calls. Out of 20,877 EMS systems in 49 states, 14 percent provided specialty care transport by ground or air, nonemergent convalescent medical transport, or medical emergency dispatch services (FICEMS, 2012, p. 13). NASEMSO Survey question: “For each of the listed EMS Agency Types, how many EMS Agencies are currently licensed in your State?”
11NASEMSO Survey Question: “For each of the listed EMS Agency organizational types, how many EMS Agencies are currently licensed in your State?”
State EMS offices commonly certify and credential local EMS providers based on completion of predetermined coursework that develops cognitive and practical skillsets. These training programs are administered at the local and regional levels and may use a variety of models that utilize the resources of community colleges, fire departments, private companies, and hospitals. Although the National Registry of EMTs accredits training centers, only 21 states require this accreditation (FICEMS, 2012, p. 236).12 Consequently, there is wide variability in the rigor of local EMS training programs. EMS providers must also complete a certain number of continuing education credits covering various aspects of EMS care (e.g., trauma, pediatrics, and cardiac) in order to recertify, which usually occurs on a biennial basis. As with the initial certification, continuing education is commonly provided and managed by individual EMS systems with varying degrees of stringency. This overall lack of consistency in training and educational standards may result in variability in EMS provider competency and skill proficiency. For example, studies have determined that national accreditation and lead instructor qualifications are associated with student success on paramedic credentialing examinations that test for competency in practical and cognitive skills (Dickison et al., 2006; Fernandez et al., 2008). Other studies have found that certificate-based paramedic programs produce students who are less confident in their ability to perform nonpatient care tasks than do programs that lead to an associate of applied science degree (Brown and Fowler, 1999). Finally, practicing EMTs with more accurate knowledge of CPR guidelines also adhere more closely to those performance standards (Brown et al., 2006). In short, less rigorously trained personnel perform less well on assessments, are less confident of their abilities, and are less competent rescuers. However, the relationship between education and performance remains incompletely understood. For example, one study found no significant relationship between the cognitive competency of EMTs, and the volume of calls they responded to each week or the continuing education they possessed (Studnek et al., 2009a). Further research about the relationship between the training and performance of EMS providers is needed.
At the local level, the size and population density of the areas served by EMS agencies vary greatly, as do the resources available to local EMS agencies to treat those populations. Local EMS agencies may be responsible for towns and municipalities, or entire counties. In terms of
________________
12NASEMSO Survey Question: “Are your EMS educational institutions required to be accredited by an independent agency?”
resources, not all areas have access to enhanced 911 services (NHTSA, 2015b), and the number of local medical directors varies considerably among states (FICEMS, 2012, p. 217).13 Differences in the regions and populations affect EMS performance. As compared to systems in urban centers, rural EMS systems are often responsible for larger and less densely populated areas, resulting in longer transport distances and response times that negatively affect patient outcomes (Yasunaga et al., 2011). Yet, areas with urban sprawl, where traffic hazards and delays are common, are also associated with longer response times (Trowbridge et al., 2009). In urban centers, EMS response times can also be delayed when patients arrest in the upper floors of high-rise buildings (Morrison et al., 2005). EMS performance is also affected by the demographics of the neighborhoods to which they respond. For example, residents of high-income neighborhoods may have faster EMS response times than those living in lower-income neighborhoods (Govindarajan and Schull, 2003). The relationship between other demographic factors, such as race and ethnicity, and the quality of EMS treatment and patient outcomes, is discussed in the following section.
THE EMS RESPONSE TO CARDIAC ARREST
The chain of survival—early access, early CPR, early defibrillation, early ACLS, and early post-resuscitative care—is an operational framework that can be used to assess the EMS response to OHCA. Actions specific to each link in the chain must be considered when identifying possible delays and opportunities to improve the quality of EMS treatments for cardiac arrest patients (see Figure 4-2). After a bystander recognizes an emergency (which may or may not be a cardiac arrest) and calls 911,14 the 911 dispatcher works with the bystander to confirm the nature
________________
13NASEMSO Survey Question: “How many local EMS Medical Directors are functioning within your State?”
14Communities have unequal access to 911 services. Rural areas often have fewer PSAPs and 911 call takers. Next Generation 911 (NG911), which allows PSAPs to receive and transfer call data from multiple sources (e.g., Voice over Internet Protocol, cell, text), is not universally available: more than half of states have NG911 systems that are entirely nonoperational, while only 21 percent of states have fully operational NG911 systems (NHTSA, 2015b, p. 3).
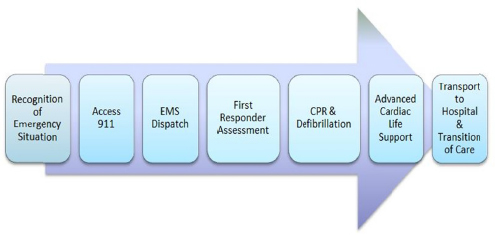
FIGURE 4-2 Actions within the overarching EMS system response to cardiac arrest.
of the emergency and may initiate the dispatch process, which alerts first responders to the type and location of the emergency. In some systems, the 911 dispatcher may instruct the bystander to perform CPR and apply defibrillation. CPR and defibrillation may be provided by a bystander, a first responder, or subsequently by EMS personnel. In the United States, ACLS in the field is typically provided by paramedics and is used to stabilize patients after return of spontaneous circulation (ROSC) during transport to a medical facility (NHTSA, 2007; NREMT, 2015). Although many post-arrest care treatments are traditionally delivered in the hospital setting, EMS personnel may also provide some elements of postarrest care before or during transport to a hospital (Pinchalk, 2010).
EMS Activation and Dispatch
EMS activation and dispatch are similar, but not identical processes. The structure for receiving and processing 911 calls is not standardized throughout the United States. Emergency 911 dispatch centers use a variety of models and are operated by an assortment of agencies, including public safety, police, and fire departments. Box 4-3 provides additional detail about the 911 dispatch system in the United States. A common model is for 911 centers managed by law enforcement to transfer calls unrelated to law enforcement to a fire department or ambulance service for purposes of dispatching EMS.
For almost any location within the United States, personnel in one of more than 7,000 primary and secondary PSAPs are available to receive
911 calls, identify the type of emergency, determine the required EMS response, and activate local EMS (FCC, 2015b).15 PSAPs are defined geographically within states, but where a specific call is routed may depend on how busy the applicable PSAPS are (i.e., load balancing), the operational status, the time of day, or the day of the week (GSA, 2014).
Operationally, PSAPs can be administered through any public safety organization, including fire, emergency management, EMS, or law enforcement, as well as tribal, hospital, or private organizations. While many PSAPs have emergency medical dispatchers who are trained to provide necessary medical instructions during a 911 call (e.g., dispatcher-assisted CPR), PSAPs not administered by EMS are often unable to provide such instruction due to a lack of training or restrictions on the scope of practice of call takers (NENA/APCO, 2011). Approximately 30 percent of all PSAPs do not have emergency medical dispatch capabilities; for these PSAPs, medically-related calls must be transferred before medical instruction can be provided (FICEMS, 2012, p. 407).16 This variation suggests the need for national, standardized training and policies to ensure that all PSAP personnel are sufficiently trained to recognize and instruct callers about cardiac arrest regardless of the PSAP location and that the policies governing the PSAPs support the provision of these instructions. As discussed later in the chapter, emergency medical dispatchers can help callers correctly identify cardiac arrest and perform CPR prior to the arrival of EMS services, contributing to increased survival rates.
EMS response intervals are strongly associated with cardiac arrest survival rates, with longer response intervals linked to worse outcomes (Stiell et al., 1999). Studies indicate that the likelihood of survival with favorable neurologic outcome following a cardiac arrest increases the sooner that treatment begins, and the effect of any BLS treatment is minimal if a patient has not achieved ROSC within 10 minutes of collapse (Weisfeldt and Becker, 2002). See Chapter 6 for research into novel therapies that may extend the window of effective treatment. Given the numerous variables and actors between recognition of an emergency and
________________
15 “A primary PSAP is defined as a PSAP to which 911 calls are routed directly from the 911 Control Office, such as, a selective router or 911 tandem. A secondary PSAP is defined as a PSAP to which 911 calls are transferred from a primary PSAP” (FCC, 2015b).
16NASEMSO Survey Question: “How many of the PSAPs provide Emergency Medical Dispatch in your State?”
BOX 4-3
911 Dispatch System in the United States
The Wireless Communications and Public Safety Act of 1999 (also known as the 911 Act) aimed to enhance public safety by facilitating the deployment of a seamless national communications infrastructure for emergency services and designating 911 as the universal emergency number in the United States. Since then, the Federal Communications Commission (FCC) has taken steps to increase public safety by facilitating and organizing the development of an integrated national emergency communications system.
Approximately 70 percent of 911 calls are placed from cell phones, and that percentage is growing (NHTSA, 2015a, p. 2). More than 60 percent of states report that 75 percent and 70 percent of their geographic service areas are covered by enhanced 911 services and enhanced wireless 911 services, respectively. These enhanced services allow PSAPs to locate callers using a landline or cell phone (FICEMS, 2012, pp. 397, 403).a Thirty-one states report that PSAPs can determine the location of at least 90 percent of landline and wireless 911 callers (NHTSA, 2015b, p. 98).b EMS dispatch centers are increasingly able to capture automatic crash notification (e.g., OnStar) data, receive text message requests for assistance, receive cell phone photographs, and use social networking for monitoring purposes (FICEMS, 2012, p. 400).c
Some PSAPs also have the technological capabilities to determine the precise status of all rescue units available in a particular service area using a computer-aided dispatch (CAD) system. The CAD system allows a dispatcher to contact responding units via two-way radio or text message and can also be used to match EMS calls with the closest, and most appropriate, public safety resource. These technological capabilities are powerful assets for EMS systems in relationship to cardiac arrest. They can quickly and accurately identify the precise location of a cardiac arrest patient, allowing specially trained and equipped EMS providers to arrive within a few minutes of the 911 call.
_______________
aNASEMSO Survey Question: “What percentage of your States Geographic Area is covered by wireless 911 (with location for cellular phones) from at least one carrier?” and “Based on the following 911 coverage types, what percentage of your States Geographic Area is covered by each?”
bThe location of these callers can be determined within 125 meters, 67 percent of the time (NHTSA, 2015b, p. 98).
cNASEMSO Survey Question: “Which of the following describes the 911 access within your State?”
defibrillation or provision of CPR, there are many points at which delays might occur. For example, delays could occur if a call center was not able to track the location of a cell phone and could not immediately dispatch EMS personnel to the scene. Delays may also occur in collecting information from bystanders, routing calls between PSAPs and dispatchers, assessing a patient’s medical condition, locating available nearby EMS responders, or in transitions between individuals performing BLS or ACLS and the transfer of care to hospital staff.
Although some studies have found no significant differences in EMS response times for minority patients (Becker et al., 1993; Cowie et al., 1993; David and Harrington, 2010; Sayegh et al., 1999), race and ethnicity have been associated with delays in activation of the emergency response system. Among minorities, many barriers to the immediate activation of 911 have been identified. For example, some minority groups are more likely to have negative feelings about EMS services (Finnegan et al., 2000), to believe that EMS responds slowly to emergencies taking place in neighborhoods stigmatized by a history of violence, or to feel confronted and discouraged by EMS dispatchers’ questions (Skolarus et al., 2013). Among Latinos, the fear of legal action (e.g., deportation due to undocumented immigrant status) also contributes to delays in activation of emergency response systems (Sasson et al., 2014; Watts et al., 2011). Minority populations who have experience with less competent and timely prehospital care, may be deterred from calling 911 by these experiences (Watts et al., 2011). Limited proficiency in English also represents a barrier to EMS activation. Language barriers delay initiation of dispatcher-assisted CPR (Bradley et al., 2011) and are a source of frustration and anxiety for callers who are not fluent in English (Sasson et al.,2014; Watts et al., 2011). Among Cambodians, a lack of proficiency in English often causes witnesses of a cardiac arrest to call family members or friends rather than 911 (Meischke et al., 2014). Key barriers to rapid activation of the emergency response system by members of minority groups are listed in Box 4-4.
Delayed activation of the emergency response system may account for the higher rates of nonshockable arrhythmias observed among black and Hispanic patients of cardiac arrest, as compared to Caucasians (Becker et al., 1993; Moon et al., 2014). One study of 4,653 cardiac arrests in New York found that race was also associated with respectively higher and lower rates of OHCA incidence and survival to hospital discharge (see Table 4-1) (Galea et al., 2007). The primary causes for these observed disparities remain undetermined: factors such as initial cardiac rhythm, patient demographics, and event-related characteristics account
for less than half of the difference in survival rates, and EMS response times were not a significant contributor (Galea et al., 2007). Further research is needed about whether and how race or ethnicity relates to EMS performance, and how EMS can improve the lower rates of survival from cardiac arrest among minority populations (David and Harrington, 2010; Galea et al., 2007). For example, more information is needed about targeted communication between EMS and the minority communities, and the implementation of strategies for improving survival from cardiac arrest among groups with limited English proficiency, such as increasing the prevalence of multilingual dispatchers.
BOX 4-4
Barriers to Early EMS Activation in Minority and Immigrant Communities
- Resigned attitudes about delays in EMS response in stigmatized neighborhoods
- Distrust of law enforcement, especially among immigrants who may fear deportation
- Language barriers that delay dispatcher-assisted CPR and are a source of frustration and anxiety for non-English speakers
TABLE 4-1 Racial Disparities in Cardiac Arrest Incidence and Survival
| Initial Rhythm and Survival | ||||
| White | Black | Hispanic | ||
| Age-adjusted OHCA incidence | 5.8 of 10,000 | 10.1 of 10,000 | 6.5 of 10,000 | |
| VF/pVT (%) | 16.7 | 12.0 | 15.1 | |
| Asystole (%) | 62.8 | 68.1 | 66.4 | |
| Survival to discharge (%) | 3.4 | 1.4 | 1.9 | |
NOTE: OHCA = out-of-hospital cardiac arrest; pVT = pulseless ventricular tachycardia; VF = ventricular fibrillation.
SOURCE: Galea et al., 2007.
Response intervals include the time required to receive and process the initial 911 call, notify closest EMS responders, and for responders to arrive on scene with a defibrillator. These intervals vary considerably among EMS systems because of differences in geography, traffic, population density, and distribution of EMS units. Survival decreases by approximately 7 to 10 percent for every minute after witnessed cardiac arrest that passes without administration of CPR (Larsen et al., 1993). In the majority of OHCA cases where bystander CPR is not provided, cardiac arrest survival is extremely low. As discussed in Chapter 3, bystander CPR is especially important in areas where response times are often delayed.
The negative effects of transport distance and population density on EMS response times and patient outcomes can be mitigated by the use of computer-aided dispatching and coordination among ambulance crews. For example, a study of the Singapore EMS system found that by moving ambulances to locations where, and staffing them at times when, OHCAs were more likely to occur, response times decreased significantly from a monthly median of 10.1 minutes to 7.1 minutes (Ong et al., 2010). Importantly, this improvement was achieved without the addition of new ambulances, personnel, or total working hours (Ong et al., 2010). Similar efforts to decrease response times by predicting cardiac events and efficiently deploying ambulances have been successful in the United States and elsewhere (Gonzalez et al., 2009; Jermyn, 2000; Peleg and Pliskin, 2004). Response times may also be reduced by expanding access to the emergency response system. The Next Generation 911 (NG911) program seeks to enable 911 callers anywhere in the United States to connect to PSAPs via wireless and Voice over Internet Protocol (VoIP) communication devices, to locate these callers, and to allow 911 dispatchers to freely exchange call data among PSAPs (DOT, 2015). Given the increasing prevalence of smartphones in the United States, the ability to text 911 in an emergency holds promise for expanding access to 911. In 2014, the FCC adopted an order requiring all wireless carriers to develop the capability to send text messages to 911 and to deliver emergency texts to PSAPs upon request (FCC, 2015c). As a result, PSAPs began to prepare to receive emergency text messages from wireless providers; as of March 2015, more than 200 PSAPs were capable of doing so (FCC, 2015a). However, much progress remains to be made, because only 21 percent of NG911 systems are fully operational, and more than half have zero functionality (NHTSA, 2015b, p. 3).
Treatment by First Responders and EMS Personnel
First responders and EMS personnel are the vanguard of a formal EMS system; as such, they are responsible for early administration of high-quality BLS and ACLS treatments, and the initial post-arrest care of the cardiac arrest patient. Although much research has been devoted to improving prehospital care for cardiac arrest patients, many unknowns remain. As a major driver of improvements in survival from OHCA, ongoing research to develop treatment protocols and novel medical technologies is needed.
CPR and Defibrillation in the Field
BLS underpins all successful cardiac resuscitation and includes CPR and defibrillation. Unlike bystander CPR (discussed in Chapter 3), CPR provided by first responders and EMS personnel includes both compressions and ventilations. The purpose of ventilation during CPR is to ensure sufficient oxygenation and adequate removal of carbon dioxide (CO2), while minimizing interruptions in chest compressions and not hyperventilating—two common problems that have prompted considerable research. Delivering high-quality chest compressions, minimizing interruptions, and following a protocol for minimizing hyperventilation while preparing for and delivering defibrillation is a challenging skill that requires considerable multi-provider integration, coordination, communication, training, and rehearsal.
Although optimal ventilation parameters during CPR (e.g., delivery method, rate, volume per breath, and oxygen concentration) remain undetermined (Meaney et al., 2013a), two things seem certain: oxygen delivery during CPR is essential, and hyperventilation is common and adversely affects survival (Aufderheide and Lurie, 2004; Aufderheide et al., 2004). Excessive oxygenation causes acute lung injury, and is a risk factor for aspiration. Paradoxically, hyperventilation actually decreases oxygenation of the vital organs, by lowering coronary perfusion pressure and raising intrathoracic pressure (Aufderheide and Lurie, 2004; McInnes et al., 2011; O’Neill and Deakin, 2007). The prevalence of hyperventilation during CPR is a consequence of many factors including a lack of awareness of the dangers of hyperventilation, inexperience and incompetence on the part of rescuers, and the stress and excitement of responding to a cardiac arrest (Aufderheide and Lurie, 2004; Aufderheide et al., 2004).
Research indicates that interrupting chest compressions to provide ventilation may adversely impact outcomes (Berg et al., 2001; Kern et al., 2002). In response to these findings, some EMS systems have developed protocols for minimally interrupted cardiac resuscitation, which has been associated with significant improvements in survival as compared to traditional CPR (Bobrow et al., 2008; Ewy, 2005; Ewy and Sanders, 2013; Kellum et al., 2008). In order to minimize interruptions in chest compressions, these protocols delay definitive airway management with intubation, the placement of which can cause prolonged interruptions in compressions. In one observational study, intubation-related interruptions in chest compressions averaged 109.5 seconds, with one-quarter of patients not receiving chest compressions for more than 3 minutes (Wang et al., 2009).
CPR for pediatric patients can be even more challenging for a number of reasons. First, OHCA is less common in children than in adults (Daya et al., 2015; Vellano et al., 2015), so EMS providers may be less experienced at resuscitating children. Second, CPR protocols are slightly different for pediatric populations: chest compressions are shallower and compression-to-ventilation ratio is lower when two rescuers are present (Kitamura et al., 2010). Third, the smaller size of pediatric patients can exacerbate the harm associated with hyperventilation and other instances of rescuer error or imprecision (Davis et al., 2004; Gausche et al., 2000). Finally, children require specialized resuscitation equipment (e.g., smaller bag-valve masks, airways, and defibrillator pads) that may not always be available and with which rescuers may be less familiar. These obstacles compound the challenges associated with inexperienced providers and may contribute to the lower OHCA survival rates for this population (Daya et al., 2015; Vellano et al., 2015). Further research is necessary to determine the best way to minimize rescuer error for pediatric populations. Key issues regarding treatment of pediatric cardiac arrest patients are discussed in Box 4-5.
BOX 4-5
Key Pediatric Issues
- The quality of CPR provided by EMS personnel for pediatric OHCA patients can be improved (Sutton et al., 2015).
- High-quality CPR leads to improved arterial blood pressure and outcomes among children with in-hospital cardiac arrest (Sutton et al., 2013a,b).
- Dispatcher-assisted CPR is also effective at improving outcomes in pediatric patients (Akahane et al., 2012; Goto et al., 2014; Rodriguez et al., 2014). Dispatchers may need specialized training in order to provide high-quality dispatcher-assisted CPR for pediatric patients.
- Ventricular fibrillation occurs less commonly in children, but increases with age (M. D. Berg et al., 2010). Early defibrillation improves outcomes.
- Out-of-hospital clinical trials have been infrequent because of the large multi-center trials needed to achieve adequate power. The Pediatric Emergency Care Applied Research Network administered by the Emergency Services for Children has been the most successful.a
_________________
aFor more information, see http://www.pecarn.org.
Various types of defibrillators are used by emergency personnel. EMT-Bs typically use AEDs, which automatically diagnose treatable rhythms and deliver shocks (NHLBI, 2011). EMT-As may use devices that include both a manual mode that allows rescuers to interpret the heart rhythm and decide whether a shock is needed and an automated mode, which operates much like an AED where the device decides based on preset electrocardiographic parameters whether a shock is needed and the rescuer simply pushes a button as indicated (FDA, 2013; IDHS, 2015). Both types of devices deliver the same electrical shock. However, the manual mode has the advantage of allowing for more rapid interpretation of the heart rhythm by a skilled provider as opposed to waiting for the machine’s diagnosis. In trials comparing the effectiveness of AEDs and manual defibrillators, AEDs were associated with longer interruptions in CPR and, consequently, with poorer outcomes (Berg et al., 2003; Kramer-Johansen et al., 2007). However, the addition of real-time audiovisual feedback to AEDs has been shown to improve CPR along a number of parameters (Fischer et al., 2011a). Paramedics (EMT-Ps) use manual defibrillators, which are capable of performing defibrillation and
also of monitoring several physiological parameters such as heart rhythm, blood pressure, pulse oximetry, and end-tidal CO2. Pulse oximetry and end-tidal CO2, available in paramedic manual defibrillators, are particularly useful in guiding post-resuscitative care and assessing the patients’ response to resuscitative efforts.
Although both CPR and defibrillation are critical components of resuscitation, one of the most important aspects of resuscitation is the interplay between CPR and defibrillation. Currently, most defibrillators require a pause in CPR while analyzing the patient’s cardiac rhythm or providing shocks. Growing clinical evidence suggests that these perishock pauses are detrimental to survival (Cheskes et al., 2011b; Edelson et al., 2006; Sell et al., 2010). One study found that optimal pre- and post-shock pauses were less than 3 seconds and 6 seconds, respectively—much shorter than the average perishock pause interval (Sell et al., 2010). Another study found that, as compared to pre- and perishock pauses greater than 20 seconds and 40 seconds, respectively, those less than 10 seconds and 20 seconds, respectively, were associated with significantly higher rates of survival to hospital discharge (Cheskes et al., 2011). An American Heart Association (AHA)-recommended technique for minimizing the perishock pause is to provide compressions during the period between rhythm analysis and shock while the AED is charging, or to charge the AED prior to rhythm analysis and while compressions are ongoing. Studies have found that this technique significantly reduces perishock pause intervals and is not associated with an increase in inappropriate shocks (R. A. Berg et al., 2010; Cheskes et al., 2014, 2015).
Advances in defibrillator technology hold the promise of reducing or eliminating perishock pauses. First, the software that assesses cardiac rhythms will become more powerful, allowing AEDs to more quickly determine whether a shock is appropriate. Second, similar software advances may allow rescuers to deliver chest compression without affecting the defibrillator’s ability to assess the patient’s cardiac rhythm. Third, new technological capabilities may allow rescuers to continue chest compressions, eliminating the preshock pause. Defibrillators and other patient monitoring devices that provide real-time performance feedback can improve the quality of CPR or allow rescuers to adapt their interventions to meet physiological targets, such as a specific patient blood pressure. Adapting current wireless technologies for use in these devices will someday enable the automated transmittal of a patient’s physiological data to the admitting emergency room, thereby allowing
hospital staff to better prepare for the particular needs of a given cardiac arrest patient.
It is important to note that recommendations for treatment of cardiac arrest change with advances in medical science and technology. For example, the development of the AED allowed bystanders to defibrillate patients rather than to wait for EMS personnel to provide shocks. Available resources also affect how quickly, and by whom, lifesaving treatments are provided. Some communities provide dispatcher-assisted CPR and public access defibrillation programs, while others do not. These differences can impact survival rates. Although the evolution of treatment recommendations can complicate the training and evaluation of EMS personnel, as well as the monitoring and assessment of performance, they can also lead to improvements in patient outcomes. See Chapter 6 for a discussion of these and other facets of learning systems of response.
Advanced Cardiac Life Support
ACLS is the fourth link in the chain of survival and includes advanced airway management, drug therapies, intravenous and intraosseous access, physiological monitoring, and hemodynamic support. The scientific literature is unclear as to whether these therapies result in improved survival from OHCA. One meta-analysis found that survival was higher for OHCA patients who received ACLS compared to those who received BLS care only (Bakalos et al., 2011). Other studies have found that provision of ACLS treatment was associated with significantly higher rates of ROSC, survival to hospital admision, and survival to discharge (Ma et al., 2007; Woodall et al., 2007). Conversely, a recent Medicare database review found higher survival rates among OHCA patients treated by BLS-only EMS units than among those treated by ACLS units, an analysis of Canadian EMS systems found no improvement in survival from OHCA after ACLS capability was added to BLS units with defibrillation, and a study of 189 pediatric OHCA patients found no survival benefit associated with ACLS over BLS care (Pitetti et al., 2002; Sanghavi et al., 2015; Stiell et al., 2004).
Research also suggests that specific ACLS treatments may reduce OHCA survival rates. For example, the advanced airway management techniques used in ACLS (e.g., endotracheal intubation) have been associated with interrupted chest compressions, hyperventilation, and misplacement of the tube in the esophagus—all of which have been
associated with detrimental outcomes in both adult and pediatric populations (Aufderheide and Lurie, 2004; Aufderheide et al., 2004; Morrison et al., 2010a). Similar concerns have been expressed about the efficacy of drug therapies used to treat cardiac arrest. Consider epinephrine, which increases both cerebral and coronary blood flow and pressure during CPR, and is the most commonly used medication during resuscitation (Michael et al., 1984; Morrison et al., 2010a). As will be discussed in Chapter 5, recent studies suggest that administration of epinephrine after cardiac arrest may confer no therapeutic benefit, and may even negatively affect long-term outcomes in some cases (Callaway, 2013). Other studies indicate that the time of administration is critical to the drug’s efficacy (Donnino et al., 2014; Hayashi et al., 2012; Jacobs et al., 2011).
Conflicting evidence regarding ACLS effectiveness may be caused by clinically relevant variations in the characteristics of, and interactions among, patient, condition, provider, and EMS system. Cardiac arrest is a syndrome and the final outcome of many disease processes, yet many studies do not account for the effect of etiology or patient medical history on survival or the variability in EMS system capabilities and provider competencies. Additional research is needed to determine whether specific drug therapies are beneficial, harmful, or merely ineffectual, and how dosage, timing, and route of administration affect their impact on OHCA survival. Targeting a particular subset of patients that may benefit from a discrete treatment could be informative. Chapter 6 discusses such alternative approaches to resuscitation research and how they might replace standard algorithms with individualized treatment protocols.
EMS Post-Resuscitative Care
Once ROSC is achieved, the risks of post–cardiac arrest syndrome rise. Post–cardiac arrest syndrome is a distinctive, multifaceted combination of pathophysiological processes that include the possibility of post–cardiac arrest brain injury, myocardial dysfunction, and ischemia and reperfusion injuries that result from prolonged oxygen deprivation and restoration of blood circulation. A more thorough discussion of postresuscitation phase of care is included in Chapter 5. Understanding pathophysiological processes can yield treatments, some of which can be administered by EMS providers prior to arrival at a hospital, to help improve OHCA outcomes.
Some notable therapies and factors are believed to improve survival. For example, percutaneous coronary intervention, antiarrhythmic medication, hemodynamic support, and appropriate ventilation can all increase the likelihood of positive outcomes following ROSC. Although research indicates that targeted temperature management (TTM) in a hospital setting has a beneficial effect on patient outcomes, and is recommended by the AHA for comatose patients with ROSC, no association between improved survival and the TTM use in the prehospital setting has been demonstrated (Debaty et al., 2014; Kim et al., 2014). Another important factor for EMS systems and providers is consideration of transport options to a facility where these therapies are readily available.
Two aspects of post–cardiac arrest syndrome that may require EMS monitoring and intervention during transport are fever and hemodynamic instabilities. Following cardiac arrest, fever is exceptionally harmful to the brain, which has been deprived of oxygen and nutrients throughout CPR. Health care providers can use TTM to prevent and rapidly treat elevated temperature (Nolan et al., 2003; Peberdy et al., 2010; Soar and Nolan, 2007). However, the evidence on specific protocols remain a subject of debate (Peberdy et al., 2010). Hemodynamic instability commonly occurs after OHCA and manifests as dysrhythmias, hypotension (i.e., low blood pressure), and low cardiac index. Transport intervals can vary considerably (Propp and Rosenberg, 1991; Schull et al., 2003; Spaite et al., 2009), but were determined by one meta-analysis to range from 10.77 to 17.28 minutes, depending on whether the arrest occurred in an urban or a rural setting (Carr et al., 2006). Therefore, the majority of OHCA patients only require limited hemodynamic support during transit. However, prolonged transport intervals, particularly in rural settings, may require EMS providers to be competent in managing hypotension (low blood pressure) as well as rearrest.
Termination of Resuscitation
Even prolonged and expertly performed resuscitation at the scene will not always revive an OHCA patient. In these circumstances, EMS systems and personnel must decide whether to transport the patient to the hospital while continuing resuscitation efforts, or to terminate resuscitation. Multiple studies have found that survival is rare among OHCA patients who are transported to the hospital after failing to respond to BLS and ACLS treatment in the field; patients that do survive often suffer moderate to severe neurological deficits (Kellermann et al., 1993;
Morrison et al., 2007). The documented decrease in CPR quality that occurs during patient transport almost certainly contributes to this low survival rate (Chung et al., 2010; Olasveengen et al., 2008). In fact, some experts question whether EMS systems should transport any cardiac arrest patients without ROSC, arguing that the most effective treatments for cardiac arrest—CPR and defibrillation—can be performed equally well or better in the field as compared to the hospital, and that interruptions in these treatments that occur as a result of transportation do more harm than relocating to the hospital does good (Adams and Benger, 2014).
The risks of transport extend beyond the patient to EMS personnel and the public. Rapid transport is itself associated with motor vehicle crashes and vehicle-pedestrian collisions, while performing CPR during high-speed transport poses additional risks for EMS personnel, who can sustain serious injuries in these circumstances (Maguire et al., 2002; Slattery and Silver, 2009). The multiple risks and minimal benefits of transporting OHCA patients who have not responded to resuscitation have led national organizations such as the AHA and NAEMSP to develop termination of resuscitation (TOR) protocols for adult OHCA patients (Millin et al., 2011; Morrison et al., 2010b). A recent policy statement by ACEP, NAEMSP, the American College of Surgeons, and the American Academy of Pediatrics proposed TOR protocols for traumatic pediatric OHCA, but protocols for terminating resuscitation of nontraumatic pediatric OHCA patients are not available (American College of Surgeons et al., 2014). These protocols can be highly accurate at predicting survival: one study found that TOR rules for use by BLS and ACLS providers had positive predictive values of 0.998 and 1.000, respectively (Sasson et al., 2008). Thus, there is clear practical and scientific support for TOR protocols.
Despite the accuracy of these protocols at predicting patient survival, research indicates that adherence can be less than 50 percent (O’Brien et al., 2008). This non-use of TOR protocols can be the result of a combination of factors, including legal mandates that restrict use of TOR protocols to a small subset of OHCA patients, cultural values that prohibit or discourage termination of resuscitation, EMS leaders without the authority to set or enforce such protocols, and poor communication between medical directors and EMS personnel (Sasson et al., 2009, 2010a). Nevertheless, accurate and comprehensive termination of resuscitation protocols for treating OHCA have the potential to improve the quality of BLS and ACLS care and reduce risks to the patient, EMS personnel, and the pub-
lic. These protocols are grounded in ethical principles, and have the support of major professional and scientific organizations. EMS systems should review and adopt nationally endorsed TOR protocols to the greatest extent possible.
Transport and Transitions of Care
For transportation of the cardiac arrest patient to the hospital to be successful, many factors must be addressed. Transportation must be rapid, while remaining safe and limiting interruptions in treatment. It must deliver the patient to an appropriate hospital, by comparing the needs of the patient with the capabilities of the receiving facility and staff. Patient data and care must be efficiently and accurately transferred from EMS to hospital personnel. Meeting these challenges will require further research and the concerted efforts of the larger EMS community.
Transport of Cardiac Arrest Patients
EMS systems in the United States treat and transport approximately 25 million patients per year, the vast majority of whom are not cardiac arrest patients (NAEMSP, 2011). Given the multifaceted nature of postarrest care, EMS providers need ready access to predetermined protocols and transport plans that are designed to integrate EMS providers into multidisciplinary hospital teams in order to optimize post-resuscitation care. For example, a large proportion of cardiac arrests in adult patients are triggered by an acute coronary artery blockage. Using an electrocardiogram, paramedics could detect this coronary condition as an ST segment elevation myocardial infarction. In these circumstances, it would be advantageous for the patient to be transported to a hospital equipped to perform immediate coronary angiography and stenting, if indicated. Predetermined policies and protocols, along with hospital prenotification that the patient is in transit, can streamline hospital-administered postarrest care. Furthermore, the EMS system has a responsibility to transport cardiac arrest patients who achieve ROSC but remain comatose to the best, and most appropriate, health care facility regionally available for subsequent treatment. The AHA’s 2010 guidelines recommend that, if available, post-arrest patients who are unconscious or unresponsive after cardiac arrest should be directed to a medical center that has a comprehensive care plan that includes not only acute cardiovascular interven-
tions and TTM, but also advanced neurological monitoring and care (Peberdy et al., 2010).
Regionalization of cardiac arrest care, which involves transporting patients to facilities that provide the guideline recommended treatments listed above, has been suggested as another opportunity for ensuring the best possible outcomes following a cardiac arrest. The overarching concept of regionalization is to transport eligible patients to designated centers of excellence (see Chapter 5) that offer the appropriate level of care as soon as possible (Lurie et al., 2005; Mechem et al., 2010). In the case of emergency surgical care, research indicates that regionalization of care can contribute to improved patient access to specialty care (Roche-Nagle et al., 2013). Furthermore, evidence has shown that regionalization of care can improve outcomes and reduce overall health care costs for high-risk patients (Bardach et al., 2004; Chang and Klitzner, 2002). For cardiac arrest patients, research suggests that minimizing transport intervals is not closely associated with improved outcomes (Nichol and Soar, 2010), while the value of guideline-recommended post-arrest treatments, which are not everywhere available, has been demonstrated in studies (Arrich et al., 2012; Reynolds et al., 2009; Sunde et al., 2007). More importantly, EMS systems experimenting with regionalization of care for cardiac arrest patients have seen improvements in survival with good neurological status in association with these programs (Bosson et al., 2014; Spaite et al., 2014). These findings suggest that regionalizing care for patients with cardiac arrest warrants further consideration, testing, and evaluation.
Another emerging practice that is technically feasible and associated with survival in some case reports is the transport of OHCA patients with refractory ventricular fibrillation directly into the cardiac catheterization laboratory, while providing continuous, mechanically aided CPR. This practice can improve the chance of achieving ROSC and survival rates in some patients (Bangalore and Hochman, 2010; Dumas et al., 2010; Frohlich et al., 2013; Kern, 2012). One study of this practice achieved rates of survival to discharge as high as 66 percent (Fothergill et al., 2014). Research also suggests that cardiac catheterization performed shortly after hospital admission may improve outcomes among resuscitated OHCA patients. For example, a retrospective cohort study of resuscitated OHCA patients found that patients who received cardiac catheterization within 6 hours of hospital admission were significantly more likely to survive to discharge than patients who received catheterization more than 6 hours after admission or not at all (Strote et al., 2012),
while literature review found that survival with good neurological status among OHCA patients who received acute cardiac catheterization was 58 percent overall, as compared to 35.8 percent among controls (Camuglia et al., 2014). Though limited, this evidence supports further investigation of cardiac catheterization immediately upon hospital admission as a potentially beneficial intervention for some OHCA patients.
Transitions of Care
EMS providers face an exceptionally challenging situation each time they transfer the cardiac arrest care of a patient to the hospital care team or the next health care provider. Within a short period of time, EMS providers must hand off the ongoing treatment of the patient, complete patient care documentation, and prepare their vehicles and themselves for future emergencies. In general, care transitions are associated with increased rates of medical errors (Horwitz et al., 2009; The Joint Commission, 2012, 2013). In the context of cardiac arrest, EMS providers may not be familiar with the hospital settings or personnel, which may affect communication and continuous quality of care. Efforts to improve direct communication between providers, the standardization of some transition components, appropriate feedback, and transparency may help overcome challenges associated with these types of transitions (ACEP, 2012c; Meisel et al., 2015). Available and developing technologies may also improve necessary information exchange (Meisel et al., 2015).
To effectively and safely transfer the care of a cardiac arrest patient from EMS to another health care provider, a formal written or printed report of the EMS care should be provided at the time of the transfer. However, a recent survey found that only 23 of 48 states that provided data have a requirement to “leave a formal copy of the EMS patient care report with the patient’s receiving healthcare provider at the time of transfer” (FICEMS, 2012, p. 284).17 The Joint Commission is currently exploring key elements of care transition models in order “to define methods for achieving improvement in the effectiveness of the transitions of patients between health care organizations, which provide for the continuation of safe, quality care for patients in all settings” (The Joint Commission, 2012, p. 2). These investigations have highlighted the importance of emphasizing collaboration and standardized transition
________________
17NASEMSO survey question: “Does your State have a regulatory requirement for EMS Agencies to provide a formal copy of the EMS patient care report to the receiving hospital or healthcare facility at the time care is transferred (before EMS leaves the facility)?”
protocols, and minimizing lapses in accountability and communication (The Joint Commission, 2012, 2013). Although EMS personnel are expected to communicate basic facts about the cardiac arrest patient during the transition to the receiving care facility and health care providers, a lack of formal documentation can lead to information gaps, which may affect patient care.
If documentation is completed and transferred with the patient, the EMS systems must be able to track that patient to hospital discharge in order to evaluate the relationship between specific care components and cardiac arrest survival or neurologic outcomes. According to a recent survey, of 49 states for which data were available, 36 states require local EMS agencies to collect patient data based on the National Emergency Medical Systems Information System (NEMSIS) data set, and 44 states maintain a data repository based on the NEMSIS standard, which includes data elements on patient disposition in the emergency room and hospital (FICEMS, 2012, pp. 286, 288; NEMSIS, 2015).18 This same survey found that only 4 of 48 states were able to report the number of EMS-treated cardiac arrest patients that survived to emergency department admission, just 1 state could report the number of OHCA patients that survived to hospital admission, and 2 states were able to report the number of patients who survived to hospital discharge (FICEMS, 2012, pp. 451, 453, 454).19 However, questions about the accuracy of NHTSA’s survey exist. The CARES registry, which allows EMS systems to collect OHCA patient data through hospital discharge, reports participation by 400 EMS agencies in 29 states (CDC, 2015). Consolidating surveillance activities into one national database could eliminate confusion about database accuracy and could generate data that are standardized, more accessible, and of higher quality.
________________
18NASEMSO Survey Questions: “Does your State by law or regulation require local EMS Agencies to collect data based on the NEMSIS standard dataset?” and “Does your State maintain a State EMS data system?”
19NASEMSO Survey Questions: “Do you know how many out of hospital cardiac arrest patients treated by EMS in your State survived to Emergency Department admission?,” “Do you know how many out of hospital cardiac arrest patients treated by EMS in your State survived to Hospital admission?,” and “Do you know how many out of hospital cardiac arrest patients treated by EMS in your State survived to Hospital discharge?”
OPPORTUNITIES FOR IMPROVING THE RESPONSE
While the efficiency and efficacy of an EMS system is important for all emergencies, activating the chain of survival is especially critical for cardiac arrest patients, for whom any delay or error throughout the resuscitation process could have fatal consequences. Efforts to improve cardiac arrest outcomes need to focus on iniatives that will optimize both the timeliness and performace of care provided by EMS systems across the United States.
Dispatcher-Assisted CPR
Bystander CPR and AED use are often the crucial bridge between collapse and arrival of trained responders. As the initial communication point between the public and the EMS system, trained 911 dispatchers have the potential to guide the preliminary and most critical phases of the cardiac arrest response. Dispatcher-assisted CPR involves the identification of cardiac arrest and the provision of CPR instructions to the 911 caller prior to the arrival of EMS providers at the scene of the cardiac arrest and represents an important area of opportunity for improving outcomes.
Organized and ongoing efforts to improve the early recognition of OHCA during a 911 call and engage individuals to perform bystander CPR are associated with statistically significant improvements in both bystander CPR and patient survival (Lewis et al., 2013; Rea et al., 2001; Tanaka et al., 2012). Specifically, clinical studies have shown a strong association between dispatcher-assisted CPR and increased bystander CPR rates and improved CPR quality and cardiac arrest survival rates (Eisenberg et al., 1985; Kellermann et al., 1989; Lewis et al., 2013; Rea et al., 2001; Song et al., 2014; Vaillancourt et al., 2007). In one study conducted in Korea, bystander CPR rates more than doubled after the implementation of a systemwide dispatcher-assisted CPR program (Song et al., 2014). Tanaka and colleagues (2012) also found that bystander CPR rates increased from 41 to 56 percent when a dispatcher-assisted CPR program was implemented in conjunction with a continuous quality improvement (CQI) program (Tanaka et al., 2012). When dispatcher-assisted CPR protocols, training, and a CQI program were implemented in three large regional 911 centers in Arizona as part of a statewide initiative, these interventions were associated with an increased likelihood of survival (Bobrow, 2014). In King County, Washington, which has one
of the highest rates of bystander CPR in the nation, dispatcher-assisted CPR has been credited for approximately half of all bystander CPR performed in the system (Lewis et al., 2013). Importantly, dispatcher-assisted CPR is also effective at improving outcomes in pediatric patients (Akahane et al., 2012; Goto et al., 2014; Rodriguez et al., 2014) as long as dispatchers are aware of the different CPR protocols for children and adults. Moreover, dispatcher-assisted CPR has been found to be cost-effective, because it requires only training costs and no additional capital investments (Dameff et al., 2014; Lewis et al., 2013).
As noted previously, dispatcher-assisted CPR is not provided by all EMS systems, and the programs that do exist are not equivalent to one another (Lerner et al., 2012). Among centers that provide dispatcher-assisted CPR instructions, dispatchers are able to recognize a cardiac arrest and facilitate the initiation of bystander CPR at different time intervals, with reports ranging from 40 seconds to 1 minute and 15 seconds for recognition of the cardiac arrest followed by 2 minutes and 56 seconds to 5 minutes and 30 seconds for the time to first chest compression (Heward et al., 2004; Lewis et al., 2013; Van Vleet and Hubble, 2012).
Training and Certification
Although Web-based training modules for dispatcher-assisted CPR are available, no nationally endorsed dispatcher-assisted CPR curriculum currently exists. Training should acquaint dispatchers with scientific findings that relate to cardiac arrest outcomes and dispatcher-assisted CPR—the nature and frequency of cardiac arrest, the importance of dispatcher-assisted CPR, and the role that dispatchers can play in improving cardiac arrest survival. Training could include didactic and simulation modules that focus on the three phases of dispatcher-assisted CPR: (1) identifying a cardiac arrest (i.e., asking if the patient is unconscious and breathing abnormally), (2) initiating CPR instructions, and (3) providing continuous coaching to keep callers focused and calm until trained first responders can take over. Identification of patients in need of CPR can be hindered by the abnormal breathing sometimes present in cardiac arrest, which bystanders can confuse with normal respiration. Protocols designed to distinguish between these types of respiration can significantly improve identification of cardiac arrest patients and increase rates of bystander CPR (Roppolo et al., 2009). Dispatchers should also be well versed in how AEDs function and be able to assist a bystander in the use of an AED, in case one is available during a 911 call.
As mentioned above, NHTSA has developed a national standard curriculum for emergency medical dispatchers, in response to the need expressed by states and municipalities for a set of “uniform program standards” that mitigate “inconsistencies in program development and implementation” (NHTSA, 1996a). Despite this recognized need for standardization, adherence to NHTSA’s curriculum is strictly voluntary (NHTSA, 1996b, p. vi). Consequently, private organizations sometimes base their dispatcher training programs off NHTSA’s curriculum, but do not follow it in a consistent or rigorous manner. Efforts made on the part of organizations that currently manage dispatcher training (e.g., APCO, International Academies of Emergency Dispatch, and PowerPhone) to collaborate on the development of a single, national-level training program could aid researchers in their efforts to improve dispatcher-assisted CPR by determining the training-related factors that limit or promote its effectiveness.
Evaluation
As in many other health care interventions, iterative evaluation and quality improvement are correlated with improved adherence to guidelines and outcomes in dispatcher-assisted CPR (Chassin and Galvin, 1998; Tanaka et al., 2012). Numerous strategies exist to evaluate the quality of dispatcher-assisted CPR. For example, auditing 911 recordings to assess dispatcher performance could provide data for CQI efforts (Clegg et al., 2014; Dameff et al., 2014; Lewis et al., 2013). Auditing can also be woven into a 911 center’s basic operation plan, whereby 911 CPR calls can be automatically flagged within a computer-aided dispatch system and then reviewed for key performance and quality indicators at a later time. Although the committee does not endorse any particular set of dispatcher-assisted CPR performance metrics or guidelines, there are categories of performance metrics that should be considered by any organization developing a training curriculum for dispatcher-assisted CPR including those listed in Box 4-6.
Training and Participation in High-Performance CPR and Other Quality Improvements
High-quality CPR is associated with improved survival in numerous studies (Bobrow et al., 2013; Cheskes et al., 2011b; Christenson et al., 2009;
BOX 4-6
Examples of Dispatcher-Assisted CPR Performance Metrics
- Percentage of cardiac arrests recognized when dispatchers have a chance to assess patient consciousness and breathing
- Time from call receipt to recognition of cardiac arrest
- Percentage of cases that receive chest compressions when dispatchers have a chance to assess patient status and CPR is not already in progress
- Time from call receipt to first chest compression
Stiell et al., 2012). Yet, observational data from actual OHCA resuscitation attempts reveal that the quality of EMS-provided CPR or both adult and pediatric cardiac arrest patients is frequently suboptimal (Cheskes et al., 2011b; Christenson et al., 2009; Lammers et al., 2014; Wik et al., 2005). Similar findings have also been documented across EMS systems (Kovacs et al., 2015; Sutton et al., 2015; Vadeboncoeur et al., 2014; Wik et al., 2005). The inconsistencies in the CPR quality may, in part, explain the wide-ranging variability in survival among and within communities (Aufderheide and Lurie, 2004; Aufderheide et al., 2005; Meaney et al., 2013; Nichol et al., 2008, 2010; Valenzuela et al., 2005; Wik et al., 2005). For many reasons, EMS providers (and other health care professionals) struggle to consistently deliver high-quality CPR. One factor is the relative lack of experience that EMS providers may have in field resuscitation. Depending on the EMS call volume and acuity, some EMS providers may not provide CPR frequently enough to maintain the necessary psychomotor skills. This holds especially true for pediatric resuscitations, which are less common than adult resuscitations (Atkins et al., 2009). Current guidelines require CPR recertification every 2 years, during which time rescuers often lose resuscitation skill proficiency, especially for pediatric resuscitation skills (Assar et al., 1998; Berden et al., 1993; Su et al., 2000). The lack of team practice for EMS providers may also contribute to lower CPR quality in high-stress and uncontrolled environments.
High-quality CPR is CPR that meets performance standards along a number of fundamental measures identified as clinically relevant in national and international guidelines. High-performance CPR emphasizes the importance of team-related factors (e.g., communication, collaboration, teamwork, and leadership) in attaining high-quality CPR, as well as other aspects of performance that affect patient outcomes. Although the
scientific literature is inconsistent in its use of these terms, the committee believes this distinction is useful for highlighting the different skillsets requisite to the performance of effective CPR. Optimally, these two concepts will be employed in tandem by any resuscitation team.
Standards for high-quality CPR are available (Meaney et al., 2013a) and include details regarding chest compression fraction (i.e., the proportion of time in which CPR is being performed during cardiac resuscitation), compression rates, length of time between compressions, chest wall recoil, and ventilation parameters—each of which has been independently associated with improved survival rates and outcomes (Aufderheide and Lurie, 2004; Aufderheide et al., 2005; Edelson et al., 2006; Fried et al., 2011; Idris et al., 2012; McInnes et al., 2011; O’Neill and Deakin, 2007; Stiell et al., 2012; Yannopoulos et al., 2005; Yu et al., 2002; Zuercher et al., 2010). Box 4-7 describes key findings specific to high-performance parameters and associated patient outcomes. The AHA recommends monitoring these parameters in order to ensure high-quality CPR (Meaney et al., 2013). Although these are discrete parameters, adjusting one may affect another in actual practice. For example, studies suggest that increasing chest compression rate can lead to decreased chest compression depth and decreased chest wall recoil (Nolan et al., 2012).
Implementation of high-quality CPR can help improve the quality of CPR delivered by EMS personnel, leading to improved cardiac arrest patient outcomes (Bobrow et al., 2013; Idris et al., 2012; Meaney et al., 2013; Monsieurs et al., 2012; Stiell et al., 2012; Travers et al., 2010). However, as described in Chapter 6, like with many aspects of health care, there is a large chasm between national guidelines and actual practice. Evidence indicates that, when measured with electronic devices, chest compressions infrequently meet the guidelines for high-performance CPR. In many cases, compressions are not continued for long enough periods of time during resuscitation attempts, and compressions that are administered are often measured as being too slow, too fast, or too shallow and having exceedingly long pauses around defibrillation attempts. Combined with ventilations that are too fast, all of these common errors can contribute to the poor cardiac arrest outcomes that are found in most communities (Aufderheide et al., 2005; Ko et al., 2005; Kramer-Johansen et al., 2006; Valenzuela et al., 2005).
BOX 4-7
Examples of Research Findings Relevant to Aspects of High-Performance CPR
Chest Compression Fraction: Results from a clinical study of OHCA resuscitations showed that lower chest compression fractions are associated with a decreased rate of ROSC and survival to hospital discharge (Christenson et al., 2009).
Compression Depth: In a study of 593 adult OHCA patients, Vadeboncoeur and colleagues (2014) found that the adjusted likelihood of survival increased by 29 percent and the likelihood of favorable functional outcomes increased by 30 percent for every 5 millimeters increase in compression depth (Vadeboncoeur et al., 2014).
Compression Rate: In a study of more than 3,000 adult OHCA patients, compression rate was found to be significantly associated with ROSC, but not survival to discharge. This study found that ROSC peaked at approximately 125 compressions per minute (Idris et al., 2012).
Compression Release Velocity: A study of more than 700 OHCAs showed that the chest compression release velocity—a measure of how fast the chest wall was released—was independently associated with improved survival (Bobrow et al., 2014).
Perishock Pause in Compressions: A study of 815 adult OHCA patients found that perishock pauses longer than 40 seconds in duration were associated with decreased odds of survival as compared to pauses less than 20 seconds in duration (Cheskes et al., 2011).
Ventilation Rate and Volume: Studies suggest that hyperventilation during CPR is common and can have an adverse effect on outcomes. In one study using animal models, six of seven animals who received 12 breaths per minute (BPM) survived, while only one of seven animals receiving 30 BPM survived (Aufderheide and Lurie, 2004). Another study found that hyperventilation occurred in each of 72 pediatric mock codes and that the mean ventilation rate of 40.8 breaths per minute was significantly higher than the AHA-recommended ventilation rate of 8-20 BPM (Niebauer et al., 2011).
One of the EMS system-level factors that can influence resuscitation quality and effectiveness is the number, training, and experience level of EMS providers who respond to a cardiac arrest. However, the manner in which these factors interact to affect performance and outcomes is not
well understood. Some studies found no increase in CPR quality or patient survival among larger or more highly trained ambulance crews (Eschmann et al., 2010; Martin-Gill et al., 2010), while other studies suggest a benefit. For example, one study of more than 16,000 OHCAs found that, as compared to events for which five or six EMS personnel were present, events with seven or eight individuals on scene were associated with higher rates of survival to discharge (Warren et al., 2015). Another study found that OHCA patients treated by EMTs with 4 or more years of experience, or by paramedics with 1 or more years of experience, were more than twice as likely to survive to hospital discharge as were patients treated by less-experienced EMS personnel (Soo et al., 1999). Additional training also seems to affect outcomes in unexpected ways. One study found that crews with two paramedics were more error prone in simulations of cardiac arrests than crews comprising one paramedic and one EMT (Bayley et al., 2008). Another study found that intermediate, but not long-term outcomes, were improved by paramedic-administered ACLS treatments (Ma et al., 2007). Similarly, ACLS treatments did not improve outcomes among pediatric patients with OHCA (Pitetti et al., 2002). At the same time, CPR is a physically demanding psychomotor skill that requires focus and coordination to achieve high quality. Several well-trained EMS providers may be preferred in order to effectively deliver high-performance CPR, rapid defibrillation, and other EMS interventions for cardiac arrest. Without sufficient numbers of care providers, a person performing chest compressions may quickly fatigue, cease to deliver the optimal depth and rate of compressions, and begin leaning on the chest—all of which are associated with worse patient survival rates (Meaney et al., 2013). In some communities as many as eight EMS providers are dispatched to cardiac arrest calls in an effort to ensure the best possible care for each patient (Warren et al., 2015). Taken together, these studies suggest that both competency and composition of ambulance crews are important.
Technology and Treatments to Advance EMS Care
Advances in technology and treatments also hold promise for improving CPR quality and OHCA outcomes. Mechanical CPR devices may be a means of providing consistent, high-quality CPR when on-scene and prehospital transport conditions render manual CPR difficult, although concrete evidence supporting widespread adoption of such devices is lacking (Brooks et al., 2014). For example, one study found that
during helicopter transport of OHCA patients, mechanical devices provided higher-quality CPR than did rescuers performing manual CPR (Gassler et al., 2015). Other studies have found that mechanical devices can improve CPR quality by decreasing the pauses in chest compressions and improving the depth and rate of chest compressions (Esibov et al., 2015; Tranberg et al., 2015). However, other studies have found no improvement in survival among patients treated with mechanical CPR devices as compared to trained rescuers (Perkins et al., 2015; Rubertsson et al., 2014). If a rescuer is unfamiliar with a mechanical CPR device, then improper use or delay can result, but this can be remedied through quality improvement activities (Levy et al., 2015).
Other technologies and treatments that may one day be employed by EMS systems to improve OHCA survival rates include thoracic impedance devices, active compression-decompression CPR, extracorporeal CPR, and post-arrest conditioning therapies. Thoracic impedance devices and active compression-decompression CPR were found in recent trials to significantly improve survival with good neurological status when used in concert (Aufderheide et al., 2011; Biondi-Zoccai et al., 2014; Fischer et al., 2014; Frascone et al., 2013; Wang et al., 2015), although a recent meta-analyses found no significant effect on ROSC or survival to hospital discharge among OHCA patients. Extracorporeal cardiopulmonary resuscitation may improve circulation to the brain and, thereby, improve outcomes from cardiac arrest. One study found that extracorporeal cardiopulmonary resuscitation used in conjunction with other experimental therapies significantly improved survival with favorable neurologic status (Sakamoto et al., 2014). Another trial found that OHCA patients treated with extracorporeal cardiopulmonary resuscitation had survival-to-discharge rates similar to IHCA patients receiving the same treatment (Wang et al., 2014). Finally, some post-arrest conditioning strategies have demonstrated the potential to improve cardiac arrest outcomes in animal models. For example, the use of a stutter-CPR protocol, alone or as part of a bundle of experimental treatments, improved neurologic and cardiac function after prolonged cardiac arrest in porcine models (Bartos et al., 2015; Segal et al., 2012). This raises questions about assumed limits on treatment futility, as described in Chapter 6.
The quality of cardiac arrest resuscitation can also be improved through training focused on cognitive knowledge acquisition, psychomotor skill proficiency, realistic scenarios, and team building. Debriefing after resuscitation can also improve CPR quality and team performance (Dine et al., 2008; Edelson et al., 2008; Sutton et al., 2012). As discussed
in Chapter 5, teamwork and leadership skills in hospital settings are associated with improved resuscitation performance in both simulation studies as well as real clinical performance (Hunziker et al., 2011; Jankouskas et al., 2011). These findings, along with the growing evidence base, suggest that teamwork and leadership training should be a component of standardized EMS resuscitation courses and training programs (R. A. Berg et al., 2010). High-fidelity, hands-on simulation is another critical aspect of training that promotes functioning as a unit when responding to cardiac arrest in the field.
Basic CPR skills diminish rapidly following CPR training (Assar et al., 1998; Berden et al., 1993; Su et al., 2000). ACLS knowledge and skills may begin to deteriorate in less than 6 weeks after training (Bhanji et al., 2010; Smith et al., 2008; Young and King, 2000). BLS skills also deteriorate, but not as rapidly (Smith et al., 2008). As such, the conventional training paradigm, which includes formal training every 2 years, may be insufficient for some providers without additional opportunities to maintain CPR skills through practice between these official training intervals (Bhanji et al., 2010; Smith et al., 2008). Evolving education and training trends are moving toward a more competency-based approach to resuscitation education with continuous maintenance, as opposed to the traditional time-set certification standards (Bhanji et al., 2010). A potential best practice may include frequent but brief, realistic team practices conducted in conjunction with debriefs from an expert objective observer. Efforts are needed to establish a standardized training curriculum for high-performance CPR, and this curriculum needs to be included as part of basic EMT training and certification. These standards need to be developed in tandem with ongoing research into novel training methods and optimal resuscitation protocols.
Another potential strategy for maintaining and developing resuscitation skillsets is the development of training centers of excellence for EMS personnel. By providing first responders, EMTs, and paramedics with access to sophisticated educational tools and exercises not commonly available outside major medical centers (e.g., high-fidelity manikins and simulation-based training), these centers could improve CPR quality and other aspects of emergency medical care provided by EMS agencies. These centers could also introduce EMS personnel to emerging technologies and therapies, potentially speeding the translation of novel treatments to the patient. Additionally, training centers designed to optimize the resuscitation skillsets of EMS personnel could form mutually informative relationships with NHTSA-recommended Centers of Excel-
lence for EMS Research (NHTSA, 2015d). Although EMS training centers and institutes exist, they vary considerably in their educational resources and offerings and rarely or infrequently offer programming beyond EMT or paramedic certification and continuing education courses.
Institute Systematic Continuous Quality Improvement
Systematic CQI initiatives have been used to elevate outcomes across numerous health care settings and diseases and health conditions. CQI principles can also be transferred and applied equally to cardiac arrest resuscitation and care (Jollis et al., 2012; Nestler et al., 2009; Santana and Stelfox, 2012). At the micro level, CQI information can be used to help EMS personnel maintain and sustain performance standards, such as those discussed for dispatcher-assisted CPR and high-performance CPR. At the macro level, local and state EMS systems need to examine and disseminate overall system performance data to identify areas for improvement and adopt new processes, training, and care protocols.
The AHA has issued a consensus statement on CPR quality recommending that every EMS system “should have an ongoing CPR QI program that provides feedback to the director, managers, and providers” (Meaney et al., 2013, p. 9). Furthermore, the AHA recommended that EMS systems develop CQI programs that monitor and assess CPR performance on a system and individual provider basis. These data could be reviewed on a regular basis to identify deficiencies and improvements, review select cases, and implement improvement plans. This type of continuous and iterative cycle of assessment and improvement efforts can lead to better care and outcomes (Edelson et al., 2008; Fischer et al., 2011b). Without such a continuous process, EMS providers cannot adequately measure and correct performance in order to improve survival.
The AHA recommends that CPR quality be monitored for all resuscitation attempts both inside and outside the hospital setting (Meaney et al., 2013). Monitoring prehospital CPR quality is feasible and effective through numerous techniques, such as electronic measurement devices, metronomes, or written checklists. Despite these guideline recommendations, which are endorsed by ACEP, many EMS systems do not consistently monitor CPR quality. As a result, wide variation persists in CPR quality. EMS systems that have implemented strategies to improve the quality of EMT-provided CPR have documented substantial improvements in both CPR quality and survival rates (Bobrow et al., 2013; Rea et al., 2006).
Guidelines also recommend that EMS providers monitor the patient’s physiological response to CPR. Specifically, direct and indirect measures of cardiac output (e.g., arterial diastolic pressure, end-tidal CO2) can be assessed to determine the effectiveness of CPR and can allow rescuers to alter their performance and adapt protocols to meet physiological targets associated with successful resuscitation (Meaney et al., 2013). Coronary perfusion pressure is another important measure of cardiac output and has been associated with ROSC and survival. Although the invasive procedure required to measure coronary perfusion pressure is not traditionally performed in the prehospital setting, recent studies suggest that it can be feasibly adapted for field use (Manning, 2013; Wildner et al., 2011). The 2011 NHTSA survey found that 21 out of 49 states reported having a performance improvement plan or guidelines in place that were mandatory for local EMS systems, but only 17 states reported having the capacity to actually monitor local EMS system response time data (FICEMS, 2012, pp. 309, 418).20 By providing EMS agencies and systems with the capacity to collect, store, and analyze performance and outcome data, cardiac arrest registries can help correct this discrepancy between the intent and ability of EMS systems to implement CQI programs, and potentially improve EMS performance and patient outcomes.
A Culture of Excellence Through Leadership and Accountability
Culture is “the norms, attitudes, and beliefs held among a group of people” (Kabcenell and Luther, 2012, p. 68). Cultural change begins with a “constancy of purpose,” wherein engaged members of an organization develop and communicate a clear vision for their performance while engaging a wide range of relevant stakeholders, which then leads to action and change (Kabcenell and Luther, 2012). Leaders can promote changes and improvements by establishing infrastructures and policies that support training, facilitate engagement, encourage the development and use of information systems, create mechanisms to ensure accountability, and recognize performance that meets defined standards or benchmarks. For example, specific EMS systems have been able to shift attitudes and promote changes in culture through a range of initiatives that have also
________________
20NASEMSO Survey Question: “Does your State have a performance improvement plan or guideline which is required to be implemented within each EMS Agency?” and “Does your State monitor EMS Response times at the local EMS Agency level?”
been used to reduce deaths and disability from cardiac arrest. In some ways, these cultural shifts have been built on the belief that the system should do everything possible to save every cardiac arrest patient within the jurisdiction of the system. In these systems, attitude changes have also been supported by implementing recognition programs for performance and outstanding work by individual providers within the system. Furthermore, the providers within these systems are given opportunities to meet cardiac arrest survivors in person, which can personalize resuscitation efforts.
A culture of excellence requires continuous and coordinated leadership across all levels. Because of the diffuse oversight structure for EMS systems, requisite leadership stems from federal agencies, elected representatives, state health departments and medical directors, voluntary professional organizations, and local EMS systems. Leaders across these levels must recognize and support the interdependence between and within the links of the chain of survival—the basis for the team approach to cardiac resuscitation. EMS leadership needs to actively engage all levels of personnel and providers in order to jointly develop and continuously refine protocols and to share data in a multidirectional fashion for purposes of CQI. Figure 4-3 develops the concept of a “chain of survival” first depicted in the executive summary by recognizing the role that leadership, accountability, and a culture of excellence play in promoting the high-quality performance of EMS systems.
State medical directors play a crucial role in contributing to high-functioning EMS systems—a prerequisite for quality care and patient safety (NASEMSO, 2010) However, lack of standardization in experience, training, and assigned responsibilities for state medical directors contributes to large variation in leadership across states. In response, NASEMSO produced a joint statement with ACEP and NAEMSP recommending a minimum set of responsibilities that include the implementation of CQI programs in EMS systems and training requirements for state medical directors. To help enact these recommendations, many federal funding sources include medical direction among their allowable expenditures (Cunningham et al., 2010). Similarly, FICEMS has recommended that state-level EMS systems should be required to have state EMS medical directors as a condition for receiving grants from the federal government (Cunningham et al., 2010). State medical directors
FIGURE 4-3 The enhanced chain of survival.
NOTE: ACLS = advanced cardiac life support; CPR = cardiopulmonary resuscitation.
SOURCE: Resuscitation Academy, 2014.
are key to implementing evidence-based EMS programs, such as high-performance CPR and dispatcher-assisted CPR, and in establishing accountability for local EMS performance and health outcomes, including cardiac arrest survival and outcomes.
Local medical directors have an enormous impact on the culture and performance of individual EMS agencies. In addition to providing on-scene medical direction, they are responsible for setting practice protocols, training and assessing personnel, educating the public, and integrating EMS with other health services (Alonso-Serra et al., 1998). Although medical director responsibility varies among EMS agencies, greater involvement on the part of the medical director has been found to enhance EMS readiness: agencies with response policies in place for handling cardiac arrests and other acute cardiovascular events are more likely to have paid, full-time medical directors who interact frequently with EMS personnel (Greer et al., 2013). Despite this connection, one study reported that less than half of EMT-Bs had interacted with their medical director in the past 6 months and that personnel in rural EMS agencies were significantly less likely to have recently interacted with a medical director than their counterparts in urban agencies (Studnek et al., 2009b). In fact, rural EMS agencies have more difficulty recruiting medical directors, and the directors they do hire are less likely to be trained in emergency medicine or to provide educational support to EMS personnel (Slifkin et al., 2009). In acknowledgment of these and other findings, ACEP, National Association of EMTs, and NAEMSP have all stated that
physician medical direction must be available at the local level (ACEP, 2012b; Alonso-Serra et al., 1998; NAEMT, 2010).
The potentially fatal and time-critical nature of cardiac arrest makes team coordination and communication simultaneously more important and more difficult to achieve (Norris and Lockey, 2012). Within teams of EMS providers, the team leader must be capable of supporting effective communication across the team members, as well as coordinating individual efforts through the organization and assignment of tasks and roles. However, in a multinational study of EMTs and paramedics, a general need for leadership training was expressed (Leggio, 2014). A highly competent resuscitation team may require only limited coordination and observations from a team leader, whereas a newly organized or less experienced team may require more intensive and specific direction. Through coordination and guidance, appropriate resuscitation team leadership can limit unnecessary interruptions in chest compressions. In these circumstances, team leaders can help minimize the number of people involved in secondary activities (e.g., trouble-shooting devices, analyzing cardiac rhythms, and securing the patient to a gurney) and ensure that the majority of the team remains directly involved in hands-on patient care (Tschan et al., 2011). Because resuscitations are dynamic events in which the status and needs of the patient fluctuate, leaders and team members must be adaptable (Hunziker et al., 2011). Strong leaders also listen to and support team members, develop the skills of their personnel through feedback and debriefing, and encourage all members of the team to question leadership decisions (Norris and Lockey, 2012). In recognition of the need for more effective and substantial leadership training in existing BLS and ACLS courses, the AHA, the International Liaison Committee on Resuscitation, and the European Resuscitation Council have all recommended that these curricula incorporate training modules targeted to fostering leadership competencies in students.21 Currently, content on team dynamics (e.g., communication and roles) is included in AHA training materials for ACLS—but not BLS—providers.
________________
21In recognition of the roles that teamwork and leadership play in the performance of resuscitation teams, the AHA recommends the incorporation of training in these nontechnical skills into ACLS coursework (Bhanji et al., 2010). ERC recommends an increased emphasis on nontechnical skills, including leadership, teamwork, task management, and structured communication. Training in these skills should be included in the coursework for advanced-level training (Nolan et al., 2010). ILCOR recommends the inclusion of specific training in teamwork and leadership skills within advanced life support courses (Mancini et al., 2010).
CONCLUSION
In general, national EMS system oversight contributes to fragmentation, an absence of systemwide coordination and planning, and suboptimal federal, state, and local leadership and accountability related to cardiac arrest. Yet, the success of a handful of communities at improving patient outcomes through high-quality EMS care shows that these barriers can be overcome. Doing so will require EMS organizations and leaders that are accountable, motivated to excel, and dedicated to improving survival from cardiac arrest. Immediate opportunities exist to markedly enhance OHCA outcomes by improving the delivery and measurement of effective prehospital cardiac arrest treatments. Dispatcher-assisted CPR is an effective means for promoting bystander CPR and AED use, which are associated with better outcomes. Educating and training EMS providers to effectively use high-performance CPR can help improve the quality of CPR and increase the likelihood of survival with good neurologic outcomes. Systematic CQI programs are used in other health-related settings to improve patient health and quality of care, and the principles can be applied equally to EMS system response to arrest. CQI programs can be implemented today, without substantial investments in infrastructure or advances in medical treatments and technology.
REFERENCES
ACEP (American College of Emergency Physicians). 2012a. Medical direction of emergency medical services. http://www.acep.org/Clinical—Practice-Management/Medical-Direction-of-Emergency-Medical-Services (accessed June 24, 2015).
ACEP. 2012b. Medical direction of emergency medical services PREP. http://www.acep.org/Clinical—Practice-Management/Medical-Direction-of-Emergency-Medical-Services-PREP (accessed June 24, 2015).
ACEP. 2012c. Transitions of care task force report. http://www.acep.org/workarea/DownloadAsset.aspx?id=89371 (accessed June 24, 2015).
Adams, B. D., and J. Benger. 2014. Should we take patients to hospital in cardiac arrest? British Medical Journal 349:g5659.
AHA (American Heart Association). 2000. Part 12: From science to survival: Strengthening the chain of survival in every community. Circulation 102(Suppl 1):I-358–I-370.
Akahane, M., T. Ogawa, S. Tanabe, S. Koike, H. Horiguchi, H. Yasunaga, and T. Imamura. 2012. Impact of telephone dispatcher assistance on the
outcomes of pediatric out-of-hospital cardiac arrest. Critical Care Medicine 40(5):1410-1416.
Alonso-Serra, H., D. Blanton, and R. E. O’Connor. 1998. Physician medical direction in EMS. Prehospital Emergency Care 2(2):153-157.
American College of Surgeons, ACEP, National Association of EMS Physicians, and American Academy of Pediatrics. 2014. Withholding or termination of resuscitation in pediatric out-of-hospital traumatic cardiopulmonary arrest. Pediatrics 133(4):e1104-e1116.
Arrich, J., M. Holzer, C. Havel, M. Mullner, and H. Herkner. 2012. Hypothermia for neuroprotection in adults after cardiopulmonary resuscitation. Cochrane Database System Review 9:CD004128.
Assar, D., D. Chamberlain, M. Colquhoun, P. Donnelly, A. J. Handley, S. Leaves, K. B. Kern, and S. Mayor. 1998. A rationale for staged teaching of basic life support. Resuscitation 39(3):137-143.
Association of Public-Safety Communications Officials International. 2015. APCO project 33 training program certification https://www.apcointl.org/training-and-certification/project-33-training-program-certification.html (accessed March 27, 2015).
Atkins, D. L., S. Everson-Stewart, G. K. Sears, M. Daya, M. H. Osmond, C. R. Warden, R. A. Berg, and Resuscitation Outcomes Consortium. 2009. Epidemiology and outcomes from out-of-hospital cardiac arrest in children: The Resuscitation Outcomes Consortium Epistry-Cardiac Arrest. Circulation 119(11):1484-1491.
Aufderheide, T. P., and K. G. Lurie. 2004. Death by hyperventilation: A common and life-threatening problem during cardiopulmonary resuscitation. Critical Care Medicine 32(9 Suppl):S345-S351.
Aufderheide, T. P., G. Sigurdsson, R. G. Pirrallo, D. Yannopoulos, S. McKnite, C. von Briesen, C. W. Sparks, C. J. Conrad, T. A. Provo, and K. G. Lurie. 2004. Hyperventilation-induced hypotension during cardiopulmonary resuscitation. Circulation 109(16):1960-1965.
Aufderheide, T. P., R. G. Pirrallo, D. Yannopoulos, J. P. Klein, C. von Briesen, C. W. Sparks, K. A. Deja, C. J. Conrad, D. J. Kitscha, T. A. Provo, and K. G. Lurie. 2005. Incomplete chest wall decompression: A clinical evaluation of CPR performance by EMS personnel and assessment of alternative manual chest compression-decompression techniques. Resuscitation 64(3):353-362.
Aufderheide, T. P., G. Nichol, T. D. Rea, S. P. Brown, B. G. Leroux, P. E. Pepe, P. J. Kudenchuk, J. Christenson, M. R. Daya, P. Dorian, C. W. Callaway, A. H. Idris, D. Andrusiek, S. W. Stephens, D. Hostler, D. P. Davis, J. V. Dunford, R. G. Pirrallo, I. G. Stiell, C. M. Clement, A. Craig, L. Van Ottingham, T. A. Schmidt, H. E. Wang, M. L. Weisfeldt, J. P. Ornato, and G. Sopko. 2011. A trial of an impedance threshold device in out-of-hospital cardiac arrest. New England Journal of Medicine 365(9):798-806.
Bakalos, G., M. Mamali, C. Komninos, E. Koukou, A. Tsantilas, S. Tzima, and T. Rosenberg. 2011. Advanced life support versus basic life support in the pre-hospital setting: A meta-analysis. Resuscitation 82(9):1130-1137.
Bangalore, S., and J. S. Hochman. 2010. A routine invasive surgery for out-of-hospital cardiac arrest survivors: Are we there yet? Circulation: Cardiovascular Interventions 3(3):197-199.
Bardach, N. S., S. J. Olson, J. S. Elkins, W. S. Smith, M. T. Lawton, and S. C. Johnston. 2004. Regionalization of treatment for subarachnoid hemorrhage a cost-utility analysis. Circulation 109(18):2207-2212.
Bartos, J. A., T. R. Matsuura, M. Sarraf, S. T. Youngquist, S. H. McKnite, J. N. Rees, D. T. Sloper, F. S. Bates, N. Segal, G. Debaty, K. G. Lurie, R. W. Neumar, J. M. Metzger, M. L. Riess, and D. Yannopoulos. 2015. Bundled postconditioning therapies improve hemodynamics and neurologic recovery after 17 min of untreated cardiac arrest. Resuscitation 87:7-13.
Bayley, R., M. Weinger, S. Meador, and C. Slovis. 2008. Impact of ambulance crew configuration on simulated cardiac arrest resuscitation. Prehospital Emergency Care 12(1):62-68.
Becker, L. B., B. H. Han, P. M. Meyer, F. A. Wright, K. V. Rhodes, D. W. Smith, and J. Barrett. 1993. Racial differences in the incidence of cardiac arrest and subsequent survival. The CPR Chicago Project. New England Journal of Medicine 329(9):600-606.
Berden, H. J., F. F. Willems, J. M. Hendrick, N. H. Pijls, and J. T. Knape. 1993. How frequently should basic cardiopulmonary resuscitation training be repeated to maintain adequate skills? British Medical Journal 306(6892):1576-1577.
Berg, M. D., S. M. Schexnayder, L. Chameides, M. Terry, A. Donoghue, R. W. Hickey, R. A. Berg, R. M. Sutton, and M. F. Hazinski. 2010. Part 13: Pediatric basic life support: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 122(18 Suppl 3):S862-S875.
Berg, R. A., A. B. Sanders, K. B. Kern, R. W. Hilwig, J. W. Heidenreich, M. E. Porter, and G. A. Ewy. 2001. Adverse hemodynamic effects of interrupting chest compressions for rescue breathing during cardiopulmonary resuscitation for ventricular fibrillation cardiac arrest. Circulation 104(20): 2465-2470.
Berg, R. A., R. W. Hilwig, K. B. Kern, A. B. Sanders, L. C. Xavier, and G. A. Ewy. 2003. Automated external defibrillation versus manual defibrillation for prolonged ventricular fibrillation: Lethal delays of chest compressions before and after countershocks. Annals of Emergency Medicine 42(4):458-467.
Berg, R. A., R. Hemphill, B. S. Abella, T. P. Aufderheide, D. M. Cave, M. F. Hazinski, E. B. Lerner, T. D. Rea, M. R. Sayre, and R. A. Swor. 2010. Part 5: Adult basic life support: 2010 American Heart Association guidelines for
cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 122(18 Suppl 3):S685-S705.
Bhanji, F., M. E. Mancini, E. Sinz, D. L. Rodgers, M. A. McNeil, T. A. Hoadley, R. A. Meeks, M. F. Hamilton, P. A. Meaney, E. A. Hunt, V. M. Nadkarni, and M. F. Hazinski. 2010. Part 16: Education, implementation, and teams: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 122(18 Suppl 3):S920-S933.
Biondi-Zoccai, G., A. Abbate, G. Landoni, A. Zangrillo, J. L. Vincent, F. D’Ascenzo, and G. Frati. 2014. An updated systematic review and metaanalysis on impedance threshold devices in patients undergoing cardiopulmonary resuscitation. Heart Lung Vessel 6(2):105-113.
Bobrow, B. 2014. Statewide implementation of a standardized pre-arrival telephone CPR program is associated with increased bystander CPR and survival from out-of-hospital cardiac arrest. Paper read at American Heart Association, Resuscitation Science Symposium, Scientific Sessions, at Chicago, Illinois.
Bobrow, B. J., L. L. Clark, G. A. Ewy, V. Chikani, A. B. Sanders, R. A. Berg, P. B. Richman, and K. B. Kern. 2008. Minimally interrupted cardiac resuscitation by emergency medical services for out-of-hospital cardiac arrest. Journal of the American Medical Association 299(10):1158-1165.
Bobrow, B. J., T. F. Vadeboncoeur, U. Stolz, A. E. Silver, J. M. Tobin, S. A. Crawford, T. K. Mason, J. Schirmer, G. A. Smith, and D. W. Spaite. 2013. The influence of scenario-based training and real-time audiovisual feedback on out-of-hospital cardiopulmonary resuscitation quality and survival from out-of-hospital cardiac arrest. Annals of Emergency Medicine 62(1):47-56.
Bobrow, B., A. Silver, U. Stolz, T. Irisawa, M. K. Aramooz, R. A. Murphy, A. Kovacs, D. Spaite. 2014. Chest compression release velocity is independently associated with survival from out-of-hospital cardiac arrest. Resuscitation 85(1):S1-S2.
Bosson, N., A. H. Kaji, J. T. Niemann, M. Eckstein, P. Rashi, R. Tadeo, D. Gorospe, G. Sung, W. J. French, D. Shavelle, J. L. Thomas, and W. Koenig. 2014. Survival and neurologic outcome after out-of-hospital cardiac arrest: Results one year after regionalization of post-cardiac arrest care in a large metropolitan area. Prehospital Emergency Care 18(2):217-223.
Bradley, S. M., C. E. Fahrenbruch, H. Meischke, J. Allen, M. Bloomingdale, and T. D. Rea. 2011. Bystander CPR in out-of-hospital cardiac arrest: The role of limited English proficiency. Resuscitation 82(6):680-684.
Brooks, S. C., N. Hassan, B. L. Bigham, and L. J. Morrison. 2014. Mechanical versus manual chest compressions for cardiac arrest. Cochrane Database System Review 2:CD007260.
Brown, L. H., and N. H. Fowler. 1999. An evaluation of EMS educational programs in North Carolina. North Carolina community college system
emergency medical science curriculum improvement project advisory and steering committees. Prehospital Emergency Care 3(2):157-162.
Brown, T. B., J. A. Dias, D. Saini, R. C. Shah, S. S. Cofield, T. E. Terndrup, R. A. Kaslow, and J. W. Waterbor. 2006. Relationship between knowledge of cardiopulmonary resuscitation guidelines and performance. Resuscitation 69(2):253-261.
Callaway, C. W. 2013. Epinephrine for cardiac arrest. Current Opinion in Cardiology 28(1):36-42.
Camuglia, A. C., V. K. Randhawa, S. Lavi, and D. L. Walters. 2014. Cardiac catheterization is associated with superior outcomes for survivors of out of hospital cardiac arrest: Review and meta-analysis. Resuscitation 85(11):1533-1540.
Carr, B. G., J. M. Caplan, J. P. Pryor, and C. C. Branas. 2006. A meta-analysis of prehospital care times for trauma. Prehospital Emergency Care 10(2):198-206.
CDC (Centers for Disease Control and Prevention). 2015. The Cardiac Arrest Registry to Enhance Survival (CARES). https://mycares.net (accessed June 15, 2015).
Chang, R. K., and T. S. Klitzner. 2002. Can regionalization decrease the number of deaths for children who undergo cardiac surgery? A theoretical analysis. Pediatrics 109(2):173-181.
Chassin, M. R., and R. W. Galvin. 1998. The urgent need to improve health care quality. Institute of Medicine national roundtable on health care quality. Journal of the American Medical Association 280(11):1000-1005.
Cheskes, S., R. H. Schmicker, J. Christenson, D. D. Salcido, T. Rea, J. Powell, D. P. Edelson, R. Sell, S. May, J. J. Menegazzi, L. Van Ottingham, M. Olsufka, S. Pennington, J. Simonini, R. A. Berg, I. Stiell, A. Idris, B. Bigham, and L. Morrison, and Resuscitation Outcomes Consortium. 2011. Perishock pause: An independent predictor of survival from out-of-hospital shockable cardiac arrest. Circulation 124(1):58-66.
Cheskes, S., M. R. Common, P. A. Byers, C. Zhan, and L. J. Morrison. 2014. Compressions during defibrillator charging shortens shock pause duration and improves chest compression fraction during shockable out of hospital cardiac arrest. Resuscitation 85(8):1007-1011.
Cheskes, S., M. Hillier, A. Byers, P. R. Verbeek, I. R. Drennan, C. Zhan, and L. J. Morrison. 2015. The association between manual mode defibrillation, pre-shock pause duration and appropriate shock delivery when employed by basic life support paramedics during out-of-hospital cardiac arrest. Resuscitation 90:61-66.
Christenson, J., D. Andrusiek, S. Everson-Stewart, P. Kudenchuk, D. Hostler, J. Powell, C. W. Callaway, D. Bishop, C. Vaillancourt, D. Davis, T. P. Aufderheide, A. Idris, J. A. Stouffer, I. Stiell, and R. Berg. 2009. Chest compression fraction determines survival in patients with out-of-hospital ventricular fibrillation. Circulation 120(13):1241-1247.
Chung, T. N., S. W. Kim, Y. S. Cho, S. P. Chung, I. Park, and S. H. Kim. 2010. Effect of vehicle speed on the quality of closed-chest compression during ambulance transport. Resuscitation 81(7):841-847.
Clegg, G. R., R. M. Lyon, S. James, H. P. Branigan, E. G. Bard, and G. J. Egan. 2014. Dispatch-assisted CPR: Where are the hold-ups during calls to emergency dispatchers? A preliminary analysis of caller–dispatcher interactions during out-of-hospital cardiac arrest using a novel call transcription technique. Resuscitation 85(1):49-52.
CMS (Centers for Medicare & Medicaid Services). 2013. Medicare enrollment—national trends 1966-2013: Medicare aged and disabled enrollees by type of coverage. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-andReports/MedicareEnrpts/Downloads/SMI2013.pdf (accessed July 31, 2015).
CMS. 2015a. Medicaid & CHIP: January 2015 monthly applications, eligibility determinations and enrollment report. http://www.medicaid.gov/medicaid-chip-program-information/program-information/downloads/medicaid-and-chip-january-2015-application-eligibility-and-enrollment-data.pdf (accessed July 31, 2015).
CMS. 2015b. Medicare coverage of ambulance services. Washington, DC: CMS. https://www.medicare.gov/Pubs/pdf/11021.pdf (accessed June 15, 2015).
CMS. 2015c. Your Medicare coverage: Is my test, item, or service covered? http://www.medicare.gov/coverage/ambulance-services.html (accessed March 31, 2015).
Cowie, M. R., C. E. Fahrenbruch, L. A. Cobb, and A. P. Hallstrom. 1993. Out-of-hospital cardiac arrest: Racial differences in outcome in Seattle. American Journal of Public Health 83(7):955-959.
Cunningham, C. A., K. Wesley, T. D. Peterson, R. Alcorta, D. F. Kupas, J. A. Nelson, P. Taillac, and J. Upchurch. 2010. The role of state medical direction in the comprehensive emergency medical services system: A resource document. Prehospital Emergency Care 14(3):404-411.
Dameff, C., T. Vadeboncoeur, J. Tully, M. Panczyk, A. Dunham, R. Murphy, U. Stolz, V. Chikani, D. Spaite, and B. Bobrow. 2014. A standardized template for measuring and reporting telephone pre-arrival cardiopulmonary resuscitation instructions. Resuscitation 85(7):869-873.
David, G., and S. E. Harrington. 2010. Population density and racial differences in the performance of emergency medical services. Journal of Health Economics 29(4):603-615.
Davis, D. P., J. V. Dunford, J. C. Poste, M. Ochs, T. Holbrook, D. Fortlage, M. J. Size, F. Kennedy, and D. B. Hoyt. 2004. The impact of hypoxia and hyperventilation on outcome after paramedic rapid sequence intubation of severely head-injured patients. Journal of Trauma 57(1):1-8; discussion 8-10.
Daya, M., R. Schmicker, S. May, and L. Morrison. 2015. Current burden of cardiac arrest in the United States: Report from the Resuscitation Outcomes Consortium. Paper commissioned by the Committee on the Treatment of Cardiac Arrest: Current Status and Future Directions. http://www.iom.edu/~/media/Files/Report%20Files/2015/ROC.pdf (accessed June 30, 2015).
Debaty, G., M. Maignan, D. Savary, F. X. Koch, S. Ruckly, M. Durand, J. Picard, C. Escallier, R. Chouquer, C. Santre, C. Minet, D. Guergour, L. Hammer, H. Bouvaist, L. Belle, C. Adrie, J. F. Payen, F. Carpentier, P. Y. Gueugniaud, V. Danel, and J. F. Timsit. 2014. Impact of intra-arrest therapeutic hypothermia in outcomes of prehospital cardiac arrest: a randomized controlled trial. Intensive Care Medicine 40(12):1832-1842.
DHS (Department of Homeland Security). 2012. Recognizing EMS week. http://www.dhs.gov/blog/2012/05/23/recognizing-ems-week (accessed July 31, 2015).
DHS. 2013. Workforce health and medical support division. http://www.dhs.gov/workforce-health-and-medical-support-division (accessed March 27, 2015).
Dickison, P., D. Hostler, T. E. Platt, and H. E. Wang. 2006. Program accreditation effect on paramedic credentialing examination success rate. Prehospital Emergency Care 10(2):224-228.
Dine, C. J., R. E. Gersh, M. Leary, B. J. Riegel, L. M. Bellini, and B. S. Abella. 2008. Improving cardiopulmonary resuscitation quality and resuscitation training by combining audiovisual feedback and debriefing. Critical Care Medicine 36(10):2817-2822.
Donnino, M. W., J. D. Salciccioli, M. D. Howell, M. N. Cocchi, B. Giberson, K. Berg, S. Gautam, and C. Callaway. 2014. Time to administration of epinephrine and outcome after in-hospital cardiac arrest with non-shockable rhythms: Retrospective analysis of large in-hospital data registry. BMJ 348:g3028.
DOT (Department of Transportation). 2015. Success stories: Next Generation 911. http://www.its.dot.gov/ng911/index.htm (accessed March 31, 2015).
Doyle, J. 2011. White paper addresses creation of a lead federal agency for EMS. Journal of Emergency Medical Services. http://www.jems.com/articles/2011/02/white-paper-addresses-creation.html (accessed July 31, 2015).
Dumas, F., A. Cariou, S. Manzo-Silberman, D. Grimaldi, B. Vivien, J. Rosencher, and J. Empana.. 2010. Immediate percutaneous coronary intervention is associated with better survival after out-of-hospital cardiac arrest insights from the PROCAT (Parisian Region Out of Hospital Cardiac ArresT) registry. Circulation: Cardiovascular Interventions 3(3):200-207.
Edelson, D. P., B. S. Abella, J. Kramer-Johansen, L. Wik, H. Myklebust, A. M. Barry, R. M. Merchant, T. L. Hoek, P. A. Steen, and L. B. Becker. 2006.
Effects of compression depth and pre-shock pauses predict defibrillation failure during cardiac arrest. Resuscitation 71(2):137-145.
Edelson, D. P., B. Litzinger, V. Arora, D. Walsh, S. Kim, D. S. Lauderdale, T. L. Vanden Hoek, L. B. Becker, and B. S. Abella. 2008. Improving in-hospital cardiac arrest process and outcomes with performance debriefing. Archives of Internal Medicine 168(10):1063-1069.
Eisenberg, M. S., A. P. Hallstrom, W. B. Carter, R. O. Cummins, L. Bergner, and J. Pierce. 1985. Emergency CPR instruction via telephone. American Journal of Public Health 75(1):47-50.
El Sayed, M. J. 2011. Measuring quality in emergency medical services: A review of clinical performance indicators. Emergency Medicine International 161630.
Eschmann, N. M., R. G. Pirrallo, T. P. Aufderheide, and E. B. Lerner. 2010. The association between emergency medical services staffing patterns and out-of-hospital cardiac arrest survival. Prehospital Emergency Care 14(1):71-77.
Esibov, A., I. Banville, F. W. Chapman, R. Boomars, M. Box, and S. Rubertsson. 2015. Mechanical chest compressions improved aspects of CPR in the LINC trial. Resuscitation 91:116-121.
Ewy, G. A. 2005. Cardiocerebral resuscitation: The new cardiopulmonary resuscitation. Circulation 111(16):2134-2142.
Ewy, G. A., and A. B. Sanders. 2013. Alternative approach to improving survival of patients with out-of-hospital primary cardiac arrest. Journal of the American College of Cardiology 61(2):113-118.
FCC (Federal Communications Commission). 2015a. Areas where text-to-911 is available. http://transition.fcc.gov/pshs/911/Text911PSAP/Text_911_Master_PSAP_Registry.xlsx (accessed March 31, 2015).
FCC. 2015b. 9-1-1 master PSAP registry. http://www.fcc.gov/encyclopedia/9-11-master-psap-registry (accessed March 27, 2015).
FCC. 2015c. What you need to know about text-to-911. http://www.fcc.gov/textto-911 (accessed March 31, 2015).
FDA (U.S. Food and Drug Administration). 2013. What is an external defibrillator? http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/CardiovascularDevices/ExternalDefibrillators/ucm232088.htm (accessed March 31, 2015).
FEMA (Federal Emergency Management Agency). 2012. Funding alternatives for emergency medical and fire services. https://www.usfa.fema.gov/downloads/pdf/publications/fa_331.pdf (accessed July 31, 2015).
Fernandez, A. R., J. R. Studnek, and G. S. Margolis. 2008. Estimating the probability of passing the national paramedic certification examination. Academic Emergency Medicine 15(3):258-264.
FICEMS (Federal Interagency Committee on Emergency Medical Services). 2012. 2011 national EMS assessment (DOT HS 811 723). Washington, DC: NHTSA. http://www.ems.gov (accessed June 15, 2015).
Finnegan, J. R., Jr., H. Meischke, J. G. Zapka, L. Leviton, A. Meshack, R. Benjamin-Garner, B. Estabrook, N. J. Hall, S. Schaeffer, C. Smith, E. R. Weitzman, J. Raczynski, and E. Stone. 2000. Patient delay in seeking care for heart attack symptoms: Findings from focus groups conducted in five U.S. regions. Preventive Medicine 31(3):205-213.
Fischer, H., J. Gruber, S. Neuhold, S. Frantal, E. Hochbrugger, H. Herkner, H. Schochl, B. Steinlechner, and R. Greif. 2011a. Effects and limitations of an AED with audiovisual feedback for cardiopulmonary resuscitation: A randomized manikin study. Resuscitation 82(7):902-907.
Fischer, H., S. Neuhold, E. Hochbrugger, B. Steinlechner, H. Koinig, L. Milosevic, C. Havel, S. Frantal, and R. Greif. 2011b. Quality of resuscitation: Flight attendants in an airplane simulator use a new mechanical resuscitation device—a randomized simulation study. Resuscitation 82(4):459-463.
Fischer, M., M. Breil, M. Ihli, M. Messelken, S. Rauch, and J. C. Schewe. 2014. Mechanical resuscitation assist devices. Anaesthesist 63(3):186-197.
Fothergill, R. T., L. R. Watson, G. K. Virdi, F. P. Moore, and M. Whitbread. 2014. Survival of resuscitated cardiac arrest patients with ST-elevation myocardial infarction (STEMI) conveyed directly to a heart attack centre by ambulance clinicians. Resuscitation 85(1):96-98.
Frascone, R. J., M. A. Wayne, R. A. Swor, B. D. Mahoney, R. M. Domeier, M. L. Olinger, D. E. Tupper, C. M. Setum, N. Burkhart, L. Klann, J. G. Salzman, S. S. Wewerka, D. Yannopoulos, K. G. Lurie, B. J. O’Neil, R. G. Holcomb, and T. P. Aufderheide. 2013. Treatment of non-traumatic out-of-hospital cardiac arrest with active compression decompression cardiopulmonary resuscitation plus an impedance threshold device. Resuscitation 84(9):1214-1222.
Fried, D. A., M. Leary, D. A. Smith, R. M. Sutton, D. Niles, D. L. Herzberg, L. B. Becker, and B. S. Abella. 2011. The prevalence of chest compression leaning during in-hospital cardiopulmonary resuscitation. Resuscitation 82(8):1019-1024.
Frõhlich, G. M., R. M. Lyon, C. Sasson, T. Crake, M. Whitbread, A. Indermuehle, A. Timmis, and P. Meier. 2013. Out-of-hospital cardiac arrest–optimal management. Current Cardiology Reviews 9(4):316.
Galea, S., S. Blaney, A. Nandi, R. Silverman, D. Vlahov, G. Foltin, M. Kusick, M. Tunik, and N. Richmond. 2007. Explaining racial disparities in incidence of and survival from out-of-hospital cardiac arrest. American Journal of Epidemiology 166(5):534-543.
Gassler, H., S. Kummerle, M. M. Ventzke, L. Lampl, and M. Helm. 2015. Mechanical chest compression: An alternative in helicopter emergency medical services? Internal Emergency Medicine.
Gausche, M., R. J. Lewis, S. J. Stratton, B. E. Haynes, C. S. Gunter, S. M. Goodrich, P. D. Poore, M. D. McCollough, D. P. Henderson, F. D. Pratt, and J. S. Seidel. 2000. Effect of out-of-hospital pediatric endotracheal
intubation on survival and neurological outcome: a controlled clinical trial. Journal of the American Medical Association 283(6):783-790.
Gausche-Hill, M., K. M. Brown, Z. J. Oliver, C. Sasson, P. S. Dayan, N. M. Eschmann, T. S. Weik, B. J. Lawner, R. Sahni, Y. Falck-Ytter, J. L. Wright, K. Todd, and E. S. Lang. 2014. An evidence-based guideline for prehospital analgesia in trauma. Prehospital Emergency Care 18(Suppl 1):25-34.
Gonzalez, R. P., G. R. Cummings, M. S. Mulekar, S. M. Harlan, and C. B. Rodning. 2009. Improving rural emergency medical service response time with global positioning system navigation. Journal of Trauma 67(5):899-902.
Goto, Y., T. Maeda, and Y. Goto. 2014. Impact of dispatcher-assisted bystander cardiopulmonary resuscitation on neurological outcomes in children with out-of-hospital cardiac arrests: a prospective, nationwide, population-based cohort study. Journal of the American Heart Association 3(3):e000499.
Govindarajan, A., and M. Schull. 2003. Effect of socioeconomic status on out-of-hospital transport delays of patients with chest pain. Annals of Emergency Medicine 41(4):481-490.
Greer, S., I. Williams, A. L. Valderrama, P. Bolton, D. G. Patterson, and Z. Zhang. 2013. EMS medical direction and prehospital practices for acute cardiovascular events. Prehospital Emergency Care 17(1):38-45.
GSA (General Services Administration). 2014. 911 Public safety answering point (PSAP) area boundary (polygon). https://catalog.data.gov/dataset/911public-safety-answering-point-psap-area-boundary-polygon (accessed March 31, 2015).
Hayashi, Y., T. Iwami, T. Kitamura, T. Nishiuchi, K. Kajino, T. Sakai, C. Nishiyama, M. Nitta, A. Hiraide, and T. Kai. 2012. Impact of early intravenous epinephrine administration on outcomes following out-of-hospital cardiac arrest. Circulation 76(7):1639-1645.
Heward, A., R. T. Donohoe, and M. Whitbread. 2004. Retrospective study into the delivery of telephone cardiopulmonary resuscitation to “999” callers. Emergency Medicine Journal 21(2):233-234.
Horwitz, L. I., T. Meredith, J. D. Schuur, N. R. Shah, R. G. Kulkarni, and G. Y. Jenq. 2009. Dropping the baton: A qualitative analysis of failures during the transition from emergency department to inpatient care. Annals of Emergency Medicine 53(6):701-710.
Hunziker, S., A. C. Johansson, F. Tschan, N. K. Semmer, L. Rock, M. D. Howell, and S. Marsch. 2011. Teamwork and leadership in cardiopulmonary resuscitation. Journal of the American College of Cardiology 57(24):2381-2388.
IAED (International Academies of Emergency Dispatch). 2015. IAED online accreditation. https://accreditation.emergencydispatch.org (accessed March 27, 2015).
IAEMSC (International Association of EMS Chiefs). 2011. Consolidated federal leadership for emergency medical services. http://iaemsc.org/
images/documents/ConsolidatedFederalLeadershipforEMS02-14-2011.pdf (accessed June 15, 2015).
IDHS (Indiana Department of Homeland Security). 2015. Advanced EMT Practical Skills Examination. http://www.in.gov/dhs/files/AEMT_practical_skills_form.pdf (accessed July 31, 2015).
Idris, A. H., D. Guffey, T. P. Aufderheide, S. Brown, L. J. Morrison, P. Nichols, J. Powell, M. Daya, B. L. Bigham, D. L. Atkins, R. Berg, D. Davis, I. Stiell, G. Sopko, and G. Nichol. 2012. Relationship between chest compression rates and outcomes from cardiac arrest. Circulation 125(24):3004-3012.
IOM (Institute of Medicine). 2007. Emergency medical services at the crossroads. http://site.ebrary.com/id/10176194 (accessed July 31, 2015).
Jacobs, I. G., J. C. Finn, G. A. Jelinek, H. F. Oxer, and P. L. Thompson. 2011. Effect of adrenaline on survival in out-of-hospital cardiac arrest: A randomised double-blind placebo-controlled trial. Resuscitation 82(9):1138-1143.
Jankouskas, T. S., K. Kopenhaver Haidet, J. E. Hupcey, A. Kolanowski, and W. B. Murray. 2011. Targeted crisis resource management training improves performance among randomized nursing and medical students. Simulation in Healthcare 6(6):316-326.
Jermyn, B. D. 2000. Reduction of the call-response interval with ambulance base paging. Prehospital Emergency Care 4(4):318-321.
The Joint Commission. 2012. Hot topics in healthcare: Transitions of care: The need for a more effective approach to continuing patient care. http://www.jointcommission.org/assets/1/18/Hot_Topics_Transitions_of_Care.pdf (accessed July 31, 2015).
The Joint Commission. 2013. Hot topics in healthcare: Transitions of care: The need for collaboration across entire care continuum. http://www.jointcommission.org/assets/1/6/TOC_Hot_Topics.pdf (accesed July 31, 2015).
Jollis, J. G., C. B. Granger, T. D. Henry, E. M. Antman, P. B. Berger, P. H. Moyer, F. D. Pratt, I. C. Rokos, A. R. Acuna, M. L. Roettig, and A. K. Jacobs. 2012. Systems of care for ST-segment-elevation myocardial infarction: A report from the American Heart Association’s mission: Lifeline. Circulation: Cardiovascular Quality Outcomes 5(4):423-428.
Kabcenell, A., and K. Luther. 2012. Creating a culture of excellence. It’s not as difficult as you might think. Healthcare Executive 27(4):68, 70-71.
Kellermann, A. L., B. B. Hackman, and G. Somes. 1989. Dispatcher-assisted cardiopulmonary resuscitation. Validation of efficacy. Circulation 80(5):1231-1239.
Kellermann, A. L., B. B. Hackman, and G. Somes. 1993. Predicting the outcome of unsuccessful prehospital advanced cardiac life support. Journal of the American Medical Association 270(12):1433-1436.
Kellum, M. J., K. W. Kennedy, R. Barney, F. A. Keilhauer, M. Bellino, M. Zuercher, and G. A. Ewy. 2008. Cardiocerebral resuscitation improves neurologically
intact survival of patients with out-of-hospital cardiac arrest. Annals of Emergency Medicine 52(3):244-252.
Kern, K. B. 2012. Optimal treatment of patients surviving out-of-hospital cardiac arrest. JACC: Cardiovascular Interventions 5(6):597-605.
Kern, K. B., R. W. Hilwig, R. A. Berg, A. B. Sanders, and G. A. Ewy. 2002. Importance of continuous chest compressions during cardiopulmonary resuscitation: Improved outcome during a simulated single lay-rescuer scenario. Circulation 105(5):645-649.
Kim, F., G. Nichol, C. Maynard, A. Hallstrom, P. J. Kudenchuk, T. Rea, M. K. Copass, D. Carlbom, S. Deem, W. T. Longstreth, Jr., M. Olsufka, and L. A. Cobb. 2014. Effect of prehospital induction of mild hypothermia on survival and neurological status among adults with cardiac arrest: A randomized clinical trial. Journal of the American Medical Association 311(1):45-52.
Kitamura, T., T. Iwami, T. Kawamura, K. Nagao, H. Tanaka, V. M. Nadkarni, R. A. Berg, and A. Hiraide. 2010. Conventional and chest-compression-only cardiopulmonary resuscitation by bystanders for children who have out-of-hospital cardiac arrests: A prospective, nationwide, population-based cohort study. Lancet 375(9723):1347-1354.
Ko, P. C., W. J. Chen, C. H. Lin, M. H. Ma, and F. Y. Lin. 2005. Evaluating the quality of prehospital cardiopulmonary resuscitation by reviewing automated external defibrillator records and survival for out-of-hospital witnessed arrests. Resuscitation 64(2):163-169.
Kovacs, A., T. Vadeboncoeur, U. Stolz, D. Spaite, T. Irisawa, A. Silver, and B. Bobrow. 2015. Chest compression release velocity: Association with survival and favorable neurologic outcome after out-of-hospital cardiac arrest. Resuscitation 92:107-114.
Kramer-Johansen, J., H. Myklebust, L. Wik, B. Fellows, L. Svensson, H. Sorebo, and P. A. Steen. 2006. Quality of out-of-hospital cardiopulmonary resuscitation with real time automated feedback: A prospective interventional study. Resuscitation 71(3):283-292.
Kramer-Johansen, J., D. P. Edelson, B. S. Abella, L. B. Becker, L. Wik, and P. A. Steen. 2007. Pauses in chest compression and inappropriate shocks: A comparison of manual and semi-automatic defibrillation attempts. Resuscitation 73(2):212-220.
Lammers, R. L., M. Willoughby-Byrwa, and W. D. Fales. 2014. Errors and error-producing conditions during a simulated, prehospital, pediatric cardiopulmonary arrest. Simulation in Healthcare 9(3):174-183.
Larsen, M., M. Eisenberg, R. Cummins, and A. Hallstrom. 1993. Predicting survival from out-of-hospital cardiac arrest: A graphic model. Annals of Emergency Medicine 22(11):1652-1658.
Leggio, W. J. 2014. The state of leadership education in emergency medical services: a multi-national qualitative study. Prehospital Disaster Medicine 29(5):478-483.
Lerner, E. B., T. D. Rea, B. J. Bobrow, J. E. Acker, 3rd, R. A. Berg, S. C. Brooks, D. C. Cone, M. Gay, L. M. Gent, G. Mears, V. M. Nadkarni, R. E. O’Connor, J. Potts, M. R. Sayre, R. A. Swor, and A. H. Travers. 2012. Emergency medical service dispatch cardiopulmonary resuscitation prearrival instructions to improve survival from out-of-hospital cardiac arrest: A scientific statement from the American Heart Association. Circulation 125(4):648-655.
Levy, M., D. Yost, R. G. Walker, E. Scheunemann, and S. R. Mendive. 2015. A quality improvement initiative to optimize use of a mechanical chest compression device within a high-performance CPR approach to out-of-hospital cardiac arrest resuscitation. Resuscitation 92:32-37.
Lewis, M., B. A. Stubbs, and M. S. Eisenberg. 2013. Dispatcher-assisted cardiopulmonary resuscitation: Time to identify cardiac arrest and deliver chest compression instructions. Circulation 128(14):1522-1530.
Lurie, K. G., A. Idris, and J. B. Holcomb. 2005. Level 1 cardiac arrest centers: Learning from the trauma surgeons. Academic Emergency Medicine 12(1):79-80.
Ma, M. H., W. C. Chiang, P. C. Ko, J. C. Huang, C. H. Lin, H. C. Wang, W. T. Chang, C. H. Hwang, Y. C. Wang, G. H. Hsiung, B. C. Lee, S. C. Chen, W. J. Chen, and F. Y. Lin. 2007. Outcomes from out-of-hospital cardiac arrest in metropolitan Taipei: Does an advanced life support service make a difference? Resuscitation 74(3):461-469.
Maguire, B. J., K. L. Hunting, G. S. Smith, and N. R. Levick. 2002. Occupational fatalities in emergency medical services: A hidden crisis. Annals of Emergency Medicine 40(6):625-632.
Mancini, M. E., J. Soar, F. Bhanji, J. E. Billi, J. Dennett, J. Finn, M. H. Ma, G. D. Perkins, D. L. Rodgers, M. F. Hazinski, I. Jacobs, and P. T. Morley. 2010. Part 12: Education, implementation, and teams: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation 122(16 Suppl 2):S539-S581.
Manning, J. E. 2013. Feasibility of blind aortic catheter placement in the prehospital environment to guide resuscitation in cardiac arrest. Journal of Trauma and Acute Care Surgery 75(2 Suppl 2):S173-S177.
Martin-Gill, C., F. X. Guyette, and J. C. Rittenberger. 2010. Effect of crew size on objective measures of resuscitation for out-of-hospital cardiac arrest. Prehospital Emergency Care 14(2):229-234.
McInnes, A. D., R. M. Sutton, A. Orioles, A. Nishisaki, D. Niles, B. S. Abella, M. R. Maltese, R. A. Berg, and V. Nadkarni. 2011. The first quantitative report of ventilation rate during in-hospital resuscitation of older children and adolescents. Resuscitation 82(8):1025-1029.
Meaney, P. A., B. J. Bobrow, M. E. Mancini, J. Christenson, A. R. de Caen, F. Bhanji, B. S. Abella, M. E. Kleinman, D. P. Edelson, R. A. Berg, T. P. Aufderheide, V. Menon, and M. Leary. 2013. Cardiopulmonary resuscitation quality:
[corrected] improving cardiac resuscitation outcomes both inside and outside the hospital: A consensus statement from the American Heart Association. Circulation 128(4):417-435.
Mechem, C. C., J. M. Goodloe, N. J. Richmond, B. J. Kaufman, and P. E. Pepe. 2010. Resuscitation center designation: Recommendations for emergency medical services practices. Prehospital Emergency Care 14(1):51-61.
Meischke, H., B. Ike, I. Painter, D. Chavez, M. P. Yip, S. M. Bradley, and S. P. Tu. 2014. Delivering 9-1-1 CPR instructions to limited English proficient callers: a simulation experiment. Journal of Immigrant and Minority Health.
Meisel, Z. F., J. A. Shea, N. J. Peacock, E. T. Dickinson, B. Paciotti, R. Bhatia, E. Buharin, and C. C. Cannuscio. 2015. Optimizing the patient handoff between emergency medical services and the emergency department. Annals of Emergency Medicine 65(3):310-317.
Michael, J. R., A. D. Guerci, R. C. Koehler, A. Y. Shi, J. Tsitlik, N. Chandra, E. Niedermeyer, M. C. Rogers, R. J. Traystman, and M. L. Weisfeldt. 1984. Mechanisms by which epinephrine augments cerebral and myocardial perfusion during cardiopulmonary resuscitation in dogs. Circulation 69(4):822-835.
Millin, M. G., S. R. Khandker, and A. Malki. 2011. Termination of resuscitation of nontraumatic cardiopulmonary arrest: Resource document for the National Association of EMS Physicians position statement. Prehospital Emergency Care 15(4):547-554.
Monsieurs, K. G., M. De Regge, K. Vansteelandt, J. De Smet, E. Annaert, S. Lemoyne, A. F. Kalmar, and P. A. Calle. 2012. Excessive chest compression rate is associated with insufficient compression depth in prehospital cardiac arrest. Resuscitation 83(11):1319-1323.
Moon, S., B. J. Bobrow, T. F. Vadeboncoeur, W. Kortuem, A. Kisakye, C. Sasson, U. Stolz, and D. W. Spaite. 2014. Disparities in bystander CPR provision and survival from out-of-hospital cardiac arrest according to neighborhood ethnicity. The American Journal of Emergency Medicine 32(9):1041-1045.
Morrison, L. J., M. P. Angelini, M. J. Vermeulen, and B. Schwartz. 2005. Measuring the EMS patient access time interval and the impact of responding to high-rise buildings. Prehospital Emergency Care 9(1):14-18.
Morrison, L. J., P. R. Verbeek, M. J. Vermeulen, A. Kiss, K. S. Allan, L. Nesbitt, and I. Stiell. 2007. Derivation and evaluation of a termination of resuscitation clinical prediction rule for advanced life support providers. Resuscitation 74(2):266-275.
Morrison, L. J., C. D. Deakin, P. T. Morley, C. W. Callaway, R. E. Kerber, S. L. Kronick, E. J. Lavonas, M. S. Link, R. W. Neumar, C. W. Otto, M. Parr, M. Shuster, K. Sunde, M. A. Peberdy, W. Tang, T. L. Hoek, B. W. Bottiger, S. Drajer, S. H. Lim, and J. P. Nolan. 2010a. Part 8: Advanced life support: 2010 international consensus on cardiopulmonary resuscitation and
emergency cardiovascular care science with treatment recommendations. Circulation 122(16 Suppl 2):S345-S421.
Morrison, L. J., G. Kierzek, D. S. Diekema, M. R. Sayre, S. M. Silvers, A. H. Idris, and M. E. Mancini. 2010b. Part 3: Ethics: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 122(18 Suppl 3):S665-S675.
NAEMSP (National Association of Emergency Medical Services Physicians). 2011. The Field EMS Quality, Innovation and Cost-Effectiveness Improvement Act, H.R. 3144. http://www.naemsp.org/Documents/fieldems-bill-whitepaper2011.pdf (accessed July 31, 2015).
NAEMT (National Association of Emergency Medical Technicians). 2010. NAEMT position statement: Medical direction of emergency medical services. https://www.naemt.org/docs/default-source/advocacy-documents/positions/3-30-10_Medical_Direction_in_EMS.pdf?sfvrsn=0 (accessed July 31, 2015).
NASEMSO (National Association of State Emergency Medical Services Officials). 2010. Role of the state EMS director: A joint statement by the American College of Emergency Physicians (ACEP), the National Association of EMS Physicians (NAEMSP), and the National Association of State EMS Officials (NASEMSO). Annals of Emergency Medicine 55(4):396-397.
NEMSIS (National Emergency Medical Services Information System). 2015. State recommended dataset. http://nemsis.org/reportingTools/reports/documents/FinalStateRecommendedDataset6-9-09.xlsx (accessed July 31, 2015).
NENA (National Emergency Number Association). 2015. 9-1-1 surcharge—user fees by state. https://www.nena.org/?page=911RateByState (accessed March 31, 2015).
NENA/APCO (National Emergency Number Association/Association of Public-Safety Communications Officials). 2011. Best practices model for third party emergency medical dispatch services and PSAPs. Alexandria, VA: NENA. https://c.ymcdn.com/sites/www.nena.org/resource/collection/ABEAA8F5-82F4-4531-AE4A-0AC5B2774E72/NENA-APCO_56-509v1_Third_Party_EMD_Best_Practices.pdf (accessed June 22, 2015).
Nestler, D. M., A. Noheria, L. H. Haro, L. G. Stead, W. W. Decker, L. N. Scanlan-Hanson, R. J. Lennon, C. C. Lim, D. R. Holmes, Jr., C. S. Rihal, M. R. Bell, and H. H. Ting. 2009. Sustaining improvement in door-to-balloon time over 4 years: The Mayo Clinic ST-elevation myocardial infarction protocol. Circulation: Cardiovascular Quality and Outcomes 2(5):508-513.
NHLBI (National Heart, Lung, and Blood Institute). 2011. What is an automated external defibrillator? http://www.nhlbi.nih.gov/health/healthtopics/topics/aed (accessed March 31, 2015).
NHTSA (National Highway Traffic Safety Administration). 1996a. 1996 EMD program implementation and administration: NSC. http://www.nhtsa.gov/
people/injury/ems/Reorder%20files%20for%20CDRom1.htm (accessed March 31, 2015).
NHTSA. 1996b. EMD program implementation and administration manager’s guide. http://www.nhtsa.gov/people/injury/ems/EMDMngrsGuide/EMDManagersGuide1stpart.pdf (accessed July 31, 2015).
NHTSA. 2007. National EMS scope of practice model. Washington, DC: NHTSA. http://www.ems.gov/education/EMSScope.pdf (accessed March 31, 2015).
NHTSA. 2009a. Emergency medical services performance measures: Recommended attributes and indicators for system and service performance. Washington, DC: NHTSA. http://www.ems.gov/pdf/811211.pdf (accessed June 15, 2015).
NHTSA. 2009b. National emergency medical services education standards. http://www.ems.gov/pdf/811077a.pdf (accessed June 15, 2015).
NHTSA. 2013. Current state of 911 funding and oversight. http://www.911.gov/pdf/Current-State-911-Funding.pdf (accessed June 15, 2015).
NHTSA. 2015a. About NHTSA EMS: Our mission. http://www.ems.gov/mission.htm (accessed March 27, 2015).
NHTSA. 2015b. 2014 national 911 progress report. Washington, DC: NHTSA. http://www.911.gov/pdf/National-911-Program-2014-ProfileDatabaseProgressReport-031315.pdf (accessed June 15, 2015).
NHTSA. 2015c. Federal partners. http://www.ems.gov/partners-FederalAgencies.htm (accessed March 27, 2015).
NHTSA. 2015d. National research agenda. http://www.nhtsa.gov/people/injury/ems/Archive/EMS03-ResearchAgenda/overcome.htm (accessed June 2, 2015).
Nichol, G., and J. Soar. 2010. Regional cardiac resuscitation systems of care. Current Opinion in Critical Care 16(3):223-230.
Nichol, G., E. Thomas, C. W. Callaway, J. Hedges, J. L. Powell, T. P. Aufderheide, T. Rea, R. Lowe, T. Brown, J. Dreyer, D. Davis, A. Idris, and I. Stiell. 2008. Regional variation in out-of-hospital cardiac arrest incidence and outcome. Journal of the American Medical Association 300(12):1423-1431.
Nichol, G., T. P. Aufderheide, B. Eigel, R. W. Neumar, K. G. Lurie, V. J. Bufalino, C. W. Callaway, V. Menon, R. R. Bass, B. S. Abella, M. Sayre, C. M. Dougherty, E. M. Racht, M. E. Kleinman, R. E. O’Connor, J. P. Reilly, E. W. Ossmann, and E. Peterson. 2010. Regional systems of care for out-of-hospital cardiac arrest: A policy statement from the American Heart Association. Circulation 121(5):709-729.
Niebauer, J. M., M. L. White, J. L. Zinkan, A. Q. Youngblood, and N. M. Tofil. 2011. Hyperventilation in pediatric resuscitation: Performance in simulated pediatric medical emergencies. Pediatrics 128(5):e1195-e1200.
Nolan, J. P., P. T. Morley, T. L. Hoek, and R. W. Hickey. 2003. Therapeutic hypothermia after cardiac arrest. An advisory statement by the Advanced
Life Support Task Force of the International Liaison Committee on Resuscitation. Resuscitation 57(3):231-235.
Nolan, J. P., J. Soar, D. A. Zideman, D. Biarent, L. L. Bossaert, C. Deakin, R. W. Koster, J. Wyllie, and B. Bottiger. 2010. European Resuscitation Council guidelines for resuscitation 2010 section 1. Executive summary. Resuscitation 81(10):1219-1276.
Nolan, J. P., G. D. Perkins, and J. Soar. 2012. Chest compression rate: Where is the sweet spot? Circulation 125(24):2968-2970.
Norris, E. M., and A. S. Lockey. 2012. Human factors in resuscitation teaching. Resuscitation 83(4):423-427.
NREMT (National Registry of Emergency Medical Technicians). 2015. Paramedic (NRP). https://www.nremt.org/nremt/about/reg_para_history.asp (accessed March 31, 2015).
O’Brien, E., D. Hendricks, and D. C. Cone. 2008. Field termination of resuscitation: Analysis of a newly implemented protocol. Prehospital Emergency Care 12(1):57-61.
Olasveengen, T. M., L. Wik, and P. A. Steen. 2008. Quality of cardiopulmonary resuscitation before and during transport in out-of-hospital cardiac arrest. Resuscitation 76(2):185-190.
O’Neill, J. F., and C. D. Deakin. 2007. Do we hyperventilate cardiac arrest patients? Resuscitation 73(1):82-85.
Ong, M. E., T. F. Chiam, F. S. Ng, P. Sultana, S. H. Lim, B. S. Leong, V. Y. Ong, E. C. Ching Tan, L. P. Tham, S. Yap, and V. Anantharaman. 2010. Reducing ambulance response times using geospatial-time analysis of ambulance deployment. Academic Emergency Medicine 17(9):951-957.
Peberdy, M. A., C. W. Callaway, R. W. Neumar, R. G. Geocadin, J. L. Zimmerman, M. Donnino, A. Gabrielli, S. M. Silvers, A. L. Zaritsky, R. Merchant, T. L. Vanden Hoek, and S. L. Kronick. 2010. Part 9: Post-cardiac arrest care: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 122(18 Suppl 3):S768-S786.
Peleg, K., and J. S. Pliskin. 2004. A geographic information system simulation model of EMS: Reducing ambulance response time. American Journal of Emergency Medicine 22(3):164-170.
Perkins, G. D., R. Lall, T. Quinn, C. D. Deakin, M. W. Cooke, J. Horton, S. E. Lamb, A. M. Slowther, M. Woollard, A. Carson, M. Smyth, R. Whitfield, A. Williams, H. Pocock, J. J. Black, J. Wright, K. Han, and S. Gates. 2015. Mechanical versus manual chest compression for out-of-hospital cardiac arrest (paramedic): A pragmatic, cluster randomised controlled trial. Lancet 385(9972):947-955.
Pinchalk, M. E. 2010. Managing post cardiac arrest syndrome in the prehospital setting. Journal of Emergency Medical Services. http://www.jems.com/article/patient-care/managing-post-cardiac-arrest-s (accessed March 27, 2015).
Pitetti, R., J. Z. Glustein, and M. S. Bhende. 2002. Prehospital care and outcome of pediatric out-of-hospital cardiac arrest. Prehospital Emergency Care 6(3):283-290.
PowerPhone. 2015. Emergency medical dispatch. http://www.powerphone.com/dispatchu/emergency-medical-dispatch (accessed June 15, 2015).
Propp, D. A., and C. A. Rosenberg. 1991. A comparison of prehospital estimated time of arrival and actual time of arrival to an emergency department. American Journal of Emergency Medicine 9(4):301-303.
Rea, T. D., M. S. Eisenberg, L. L. Culley, and L. Becker. 2001. Dispatcher-assisted cardiopulmonary resuscitation and survival in cardiac arrest. Circulation 104(21):2513-2516.
Rea, T. D., M. Helbock, S. Perry, M. Garcia, D. Cloyd, L. Becker, and M. Eisenberg. 2006. Increasing use of cardiopulmonary resuscitation during out-of-hospital ventricular fibrillation arrest: Survival implications of guideline changes. Circulation 114(25):2760-2765.
Resuscitation Academy. 2014. 10 Steps for Improving Survival from Cardiac Arrest. http://www.resuscitationacademy.com/downloads/ebook/TenStepsforImprovingSurvivalFromSuddenCardiacArrest-RA-eBook-PDFFinal-v1_2.pdf (accessed July 31, 2015).
Reynolds, J. C., C. W. Callaway, S. R. El Khoudary, C. G. Moore, R. J. Alvarez, and J. C. Rittenberger. 2009. Coronary angiography predicts improved outcome following cardiac arrest: Propensity-adjusted analysis. Journal of Intensive Care Medicine 24(3):179-186.
Roche-Nagle, G., K. Bachynski, A. B. Nathens, D. Angoulvant, and B. B. Rubin. 2013. Regionalization of services improves access to emergency vascular surgical care. Vascular 21(2):69-74.
Rodriguez, S. A., R. M. Sutton, M. D. Berg, A. Nishisaki, M. Maltese, P. A. Meaney, D. E. Niles, J. Leffelman, R. A. Berg, and V. M. Nadkarni. 2014. Simplified dispatcher instructions improve bystander chest compression quality during simulated pediatric resuscitation. Resuscitation 85(1):119-123.
Roppolo, L. P., A. Westfall, P. E. Pepe, L. L. Nobel, J. Cowan, J. J. Kay, and A. H. Idris. 2009. Dispatcher assessments for agonal breathing improve detection of cardiac arrest. Resuscitation 80(7):769-772.
Rubertsson, S., E. Lindgren, D. Smekal, O. Ostlund, J. Silfverstolpe, R. A. Lichtveld, R. Boomars, B. Ahlstedt, G. Skoog, R. Kastberg, D. Halliwell, M. Box, J. Herlitz, and R. Karlsten. 2014. Mechanical chest compressions and simultaneous defibrillation vs conventional cardiopulmonary resuscitation in out-of-hospital cardiac arrest: The LINC randomized trial. Journal of the American Medical Association 311(1):53-61.
Sakamoto, T., N. Morimura, K. Nagao, Y. Asai, H. Yokota, S. Nara, M. Hase, Y. Tahara, and T. Atsumi. 2014. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults
with out-of-hospital cardiac arrest: A prospective observational study. Resuscitation 85(6):762-768.
Sanghavi, P., A. B. Jena, J. P. Newhouse, and A. M. Zaslavsky. 2015. Outcomes after out-of-hospital cardiac arrest treated by basic vs advanced life support. Journal of the American Medical Association: Internal Medicine 175(2):196-204.
Santana, M. J., and H. T. Stelfox. 2012. Quality indicators used by trauma centers for performance measurement. Journal of Trauma Acute Care Surgery 72(5):1298-1302; discussion 1303.
Sasson, C., A. J. Hegg, M. Macy, A. Park, A. Kellermann, and B. McNally. 2008. Prehospital termination of resuscitation in cases of refractory out-of-hospital cardiac arrest. Journal of the American Medical Association 300(12):1432-1438.
Sasson, C., J. Forman, D. Krass, M. Macy, A. L. Kellermann, and B. F. McNally. 2009. A qualitative study to identify barriers to local implementation of prehospital termination of resuscitation protocols. Circulation: Cardiovascular Quality and Outcomes 2(4):361-368.
Sasson, C., J. Forman, D. Krass, M. Macy, A. J. Hegg, B. F. McNally, and A. L. Kellermann. 2010a. A qualitative study to understand barriers to implementation of national guidelines for prehospital termination of unsuccessful resuscitation efforts. Prehospital Emergency Care 14(2):250-258.
Sasson, C., M. A. Rogers, J. Dahl, and A. L. Kellermann. 2010b. Predictors of survival from out-of-hospital cardiac arrest: A systematic review and metaanalysis. Circulation: Cardiovascular Quality and Outcomes 3(1):63-81.
Sasson, C., J. S. Haukoos, L. Ben-Youssef, L. Ramirez, S. Bull, B. Eigel, D. J. Magid, and R. Padilla. 2014. Barriers to calling 911 and learning and performing cardiopulmonary resuscitation for residents of primarily Latino, high-risk neighborhoods in Denver, Colorado. Annals of Emergency Medicine 65(5):545-552.
Sayegh, A. J., R. Swor, K. H. Chu, R. Jackson, J. Gitlin, R. M. Domeier, E. Basse, D. Smith, and W. Fales. 1999. Does race or socioeconomic status predict adverse outcome after out of hospital cardiac arrest: A multi-center study. Resuscitation 40(3):141-146.
Schull, M. J., L. J. Morrison, M. Vermeulen, and D. A. Redelmeier. 2003. Emergency department overcrowding and ambulance transport delays for patients with chest pain. Canadian Medical Association Journal 168(3):277-283.
Segal, N., T. Matsuura, E. Caldwell, M. Sarraf, S. McKnite, M. Zviman, T. P. Aufderheide, H. R. Halperin, K. G. Lurie, and D. Yannopoulos. 2012. Ischemic postconditioning at the initiation of cardiopulmonary resuscitation facilitates functional cardiac and cerebral recovery after prolonged untreated ventricular fibrillation. Resuscitation 83(11):1397-1403.
Sell, R. E., R. Sarno, B. Lawrence, E. M. Castillo, R. Fisher, C. Brainard, J. V. Dunford, and D. P. Davis. 2010. Minimizing pre- and post-defibrillation
pauses increases the likelihood of return of spontaneous circulation (ROSC). Resuscitation 81(7):822-825.
Shah, M. I., C. G. Macias, P. S. Dayan, T. S. Weik, K. M. Brown, S. M. Fuchs, M. E. Fallat, J. L. Wright, and E. S. Lang. 2014. An evidence-based guideline for pediatric prehospital seizure management using grade methodology. Prehospital Emergency Care 18(Suppl 1):15-24.
Skolarus, L. E., J. B. Murphy, M. A. Zimmerman, S. Bailey, S. Fowlkes, D. L. Brown, L. D. Lisabeth, E. Greenberg, and L. B. Morgenstern. 2013. Individual and community determinants of calling 911 for stroke among African Americans in an urban community. Circulation: Cardiovascular Quality and Outcomes 6(3):278-283.
Slattery, D. E., and A. Silver. 2009. The hazards of providing care in emergency vehicles: an opportunity for reform. Prehospital Emergency Care 13(3):388-397.
Slifkin, R. T., V. A. Freeman, and P. D. Patterson. 2009. Designated medical directors for emergency medical services: Recruitment and roles. The Journal of Rural Health 25(4):392-398.
Smith, K. K., D. Gilcreast, and K. Pierce. 2008. Evaluation of staff’s retention of ACLS and BLS skills. Resuscitation 78(1):59-65.
Soar, J., and J. P. Nolan. 2007. Mild hypothermia for post cardiac arrest syndrome. BMJ 335(7618):459-460.
Song, K. J., S. D. Shin, C. B. Park, J. Y. Kim, K. Kim do, C. H. Kim, S. Y. Ha, M. Eng Hock Ong, B. J. Bobrow, and B. McNally. 2014. Dispatcher-assisted bystander cardiopulmonary resuscitation in a metropolitan city: A before-after population-based study. Resuscitation 85(1):34-41.
Soo, L. H., D. Gray, T. Young, A. Skene, and J. R. Hampton. 1999. Influence of ambulance crew’s length of experience on the outcome of out-of-hospital cardiac arrest. European Heart Journal 20(7):535-540.
Spaite, D. W., I. G. Stiell, B. J. Bobrow, M. de Boer, J. Maloney, K. Denninghoff, T. F. Vadeboncoeur, J. Dreyer, and G. A. Wells. 2009. Effect of transport interval on out-of-hospital cardiac arrest survival in the opals study: Implications for triaging patients to specialized cardiac arrest centers. Annals of Emergency Medicine 54(2):248-255.
Spaite, D. W., B. J. Bobrow, U. Stolz, R. A. Berg, A. B. Sanders, K. B. Kern, V. Chikani, W. Humble, T. Mullins, J. S. Stapczynski, and G. A. Ewy. 2014. Statewide regionalization of postarrest care for out-of-hospital cardiac arrest: Association with survival and neurologic outcome. Annals of Emergency Medicine 64(5):496-506.
Stiell, I. G., G. A. Wells, B. J. Field, D. W. Spaite, V. J. De Maio, R. Ward, D. P. Munkley, M. B. Lyver, L. G. Luinstra, T. Campeau, J. Maloney, and E. Dagnone. 1999. Improved out-of-hospital cardiac arrest survival through the inexpensive optimization of an existing defibrillation program: OPALS Study Phase II. Ontario prehospital advanced life support. Journal of the American Medical Association 281(13):1175-1181.
Stiell, I. G., G. A. Wells, B. Field, D. W. Spaite, L. P. Nesbitt, V. J. De Maio, G. Nichol, D. Cousineau, J. Blackburn, D. Munkley, L. Luinstra-Toohey, T. Campeau, E. Dagnone, and M. Lyver. 2004. Advanced cardiac life support in out-of-hospital cardiac arrest. New England Journal of Medicine 351(7):647-656.
Stiell, I. G., S. P. Brown, J. Christenson, S. Cheskes, G. Nichol, J. Powell, B. Bigham, L. J. Morrison, J. Larsen, E. Hess, C. Vaillancourt, D. P. Davis, C. W. Callaway, and Resuscitation Outcomes Consortium. 2012. What is the role of chest compression depth during out-of-hospital cardiac arrest resuscitation? Critical Care Medicine 40(4):1192-1198.
Strote, J. A., C. Maynard, M. Olsufka, G. Nichol, M. K. Copass, L. A. Cobb, and F. Kim. 2012. Comparison of role of early (less than six hours) to later (more than six hours) or no cardiac catheterization after resuscitation from out-of-hospital cardiac arrest. American Journal of Cardiology 109(4):451-454.
Studnek, J. R., A. R. Fernandez, and G. S. Margolis. 2009a. Assessing continued cognitive competence among rural emergency medical technicians. Prehospital Emergency Care 13(3):357-363.
Studnek, J. R., A. R. Fernandez, G. S. Margolis, and R. E. O’Connor. 2009b. Physician medical oversight in emergency medical services: Where are we? Prehospital Emergency Care 13(1):53-58.
Su, E., T. A. Schmidt, N. C. Mann, and A. D. Zechnich. 2000. A randomized controlled trial to assess decay in acquired knowledge among paramedics completing a pediatric resuscitation course. Academic Emergency Medicine 7(7):779-786.
Sunde, K., M. Pytte, D. Jacobsen, A. Mangschau, L. P. Jensen, C. Smedsrud, T. Draegni, and P. A. Steen. 2007. Implementation of a standardised treatment protocol for post resuscitation care after out-of-hospital cardiac arrest. Resuscitation 73(1):29-39.
Sutton, R. M., V. Nadkarni, and B. S. Abella. 2012. “Putting it all together” to improve resuscitation quality. Emergency medicine clinics of North America 30(1):105-122.
Sutton, R. M., R. A. Berg, and V. Nadkarni. 2013a. CPR technique for infants and children. Current Pediatric Reviews 9(2):100-108.
Sutton, R. M., B. French, A. Nishisaki, D. E. Niles, M. R. Maltese, L. Boyle, M. Stavland, J. Eilevstjonn, K. B. Arbogast, R. A. Berg, and V. M. Nadkarni. 2013b. American Heart Association cardiopulmonary resuscitation quality targets are associated with improved arterial blood pressure during pediatric cardiac arrest. Resuscitation 84(2):168-172.
Sutton, R. M., E. Case, S. P. Brown, D. L. Atkins, V. M. Nadkarni, J. Kaltman, C. Callaway, A. Idris, G. Nichol, J. Hutchison, I. R. Drennan, M. Austin, M. Daya, S. Cheskes, J. Nuttall, H. Herren, J. Christenson, D. Andrusiek, C. Vaillancourt, J. J. Menegazzi, T. D. Rea, and R. A. Berg. 2015. A quantitative analysis of out-of-hospital pediatric and adolescent
resuscitation quality—a report from the ROC Epistry-Cardiac Arrest. Resuscitation 93:150-157.
Tanaka, Y., J. Taniguchi, Y. Wato, Y. Yoshida, and H. Inaba. 2012. The continuous quality improvement project for telephone-assisted instruction of cardiopulmonary resuscitation increased the incidence of bystander CPR and improved the outcomes of out-of-hospital cardiac arrests. Resuscitation 83(10):1235-1241.
Thomas, S. H., K. M. Brown, Z. J. Oliver, D. W. Spaite, B. J. Lawner, R. Sahni, T. S. Weik, Y. Falck-Ytter, J. L. Wright, and E. S. Lang. 2014. An evidence-based guideline for the air medical transportation of prehospital trauma patients. Prehospital Emergency Care 18(Suppl 1):35-44.
Tranberg, T., J. F. Lassen, A. K. Kaltoft, T. M. Hansen, C. Stengaard, L. Knudsen, S. Trautner, and C. J. Terkelsen. 2015. Quality of cardiopulmonary resuscitation in out-of-hospital cardiac arrest before and after introduction of a mechanical chest compression device, LUCAS-2; a prospective, observational study. Scandinavian Journal of Trauma, Resuscitation & Emergency Medicine 23(1):37.
Travers, A. H., T. D. Rea, B. J. Bobrow, D. P. Edelson, R. A. Berg, M. R. Sayre, M. D. Berg, L. Chameides, R. E. O’Connor, and R. A. Swor. 2010. Part 4: CPR overview: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 122(18 Suppl 3):S676-S684.
Trowbridge, M. J., M. J. Gurka, and R. E. O’Connor. 2009. Urban sprawl and delayed ambulance arrival in the U.S. American Journal of Preventive Medicine 37(5):428-432.
Tschan, F., M. Vetterli, N. K. Semmer, S. Hunziker, and S. C. Marsch. 2011. Activities during interruptions in cardiopulmonary resuscitation: A simulator study. Resuscitation 82(11):1419-1423.
Vadeboncoeur, T., U. Stolz, A. Panchal, A. Silver, M. Venuti, J. Tobin, G. Smith, M. Nunez, M. Karamooz, D. Spaite, and B. Bobrow. 2014. Chest compression depth and survival in out-of-hospital cardiac arrest. Resuscitation 85(2):182-188.
Vaillancourt, C., A. Verma, J. Trickett, D. Crete, T. Beaudoin, L. Nesbitt, G. A. Wells, and I. G. Stiell. 2007. Evaluating the effectiveness of dispatch-assisted cardiopulmonary resuscitation instructions. Academic Emergency Medicine 14(10):877-883.
Valenzuela, T. D., K. B. Kern, L. L. Clark, R. A. Berg, M. D. Berg, D. D. Berg, R. W. Hilwig, C. W. Otto, D. Newburn, and G. A. Ewy. 2005. Interruptions of chest compressions during emergency medical systems resuscitation. Circulation 112(9):1259-1265.
Van Vleet, L. M., and M. W. Hubble. 2012. Time to first compression using medical priority dispatch system compression-first dispatcher-assisted cardiopulmonary resuscitation protocols. Prehospital Emergency Care 16(2):242-250.
Vellano, K., A. Crouch, M. Rajdev, and B. McNally. 2015. Cardiac Arrest Registry to Enhance Survival (CARES) report on the public health burden of out-of-hospital cardiac arrest. Paper commissioned by the Committee on the Treatment of Cardiac Arrest: Current Status and Future Directions. http://www.iom.edu/~/media/Files/Report%20Files/2015/CARES.pdf (accessed June 30, 2015).
Wang, C. H., N. K. Chou, L. B. Becker, J. W. Lin, H. Y. Yu, N. H. Chi, S. C. Hunag, W. J. Ko, S. S. Wang, L. J. Tseng, M. H. Lin, I. H. Wu, M. H. Ma, and Y. S. Chen. 2014. Improved outcome of extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest—a comparison with that for extracorporeal rescue for in-hospital cardiac arrest. Resuscitation 85(9):1219-1224.
Wang, C. H., M. S. Tsai, W. T. Chang, C. H. Huang, M. H. Ma, W. J. Chen, C. C. Fang, S. C. Chen, and C. C. Lee. 2015. Active compression-decompression resuscitation and impedance threshold device for out-of-hospital cardiac arrest: A systematic review and metaanalysis of randomized controlled trials. Critical Care Medicine 43(4):889-896.
Wang, H. E., S. J. Simeone, M. D. Weaver, and C. W. Callaway. 2009. Interruptions in cardiopulmonary resuscitation from paramedic endotracheal intubation. Annals of Emergency Medicine 54(5):645-652.
Warren, S. A., D. K. Prince, E. Huszti, T. D. Rea, A. L. Fitzpatrick, D. L. Andrusiek, S. Darling, L. J. Morrison, G. M. Vilke, G. Nichol, for the ROC Investigatorsl. 2015. Volume versus outcome: More emergency medical services personnel on-scene and increased survival after out-of-hospital cardiac arrest. Resuscitation S0300-9572(15):00086-6.
Watts, J., J. D. Cowden, A. P. Cupertino, M. D. Dowd, and C. Kennedy. 2011. 911 (nueve once): Spanish-speaking parents’ perspectives on prehospital emergency care for children. Journal of Immigrant and Minority Health 13(3):526-532.
Weisfeldt, M. L., and L. B. Becker. 2002. Resuscitation after cardiac arrest: A 3-phase time-sensitive model. Journal of the American Medical Association 288(23):3035-3038.
Wik, L., J. Kramer-Johansen, H. Myklebust, H. Sorebo, L. Svensson, B. Fellows, and P. A. Steen. 2005. Quality of cardiopulmonary resuscitation during out-of-hospital cardiac arrest. Journal of the American Medical Association 293(3):299-304.
Wildner, G., N. Pauker, S. Archan, G. Gemes, M. Rigaud, M. Pocivalnik, and G. Prause. 2011. Arterial line in prehospital emergency settings—a feasibility study in four physician-staffed emergency medical systems. Resuscitation 82(9):1198-1201.
Woodall, J., M. McCarthy, T. Johnston, V. Tippett, and R. Bonham. 2007. Impact of advanced cardiac life support-skilled paramedics on survival from out-of-hospital cardiac arrest in a statewide emergency medical service. Emergency Medicine Journal 24(2):134-138.
Wright, J. L. 2014. Evidence-based guidelines for prehospital practice: a process whose time has come. Prehospital Emergency Care 18(Suppl 1):1-2.
Yannopoulos, D., S. McKnite, T. P. Aufderheide, G. Sigurdsson, R. G. Pirrallo, D. Benditt, and K. G. Lurie. 2005. Effects of incomplete chest wall decompression during cardiopulmonary resuscitation on coronary and cerebral perfusion pressures in a porcine model of cardiac arrest. Resuscitation 64(3):363-372.
Yasunaga, H., H. Miyata, H. Horiguchi, S. Tanabe, M. Akahane, T. Ogawa, S. Koike, and T. Imamura. 2011. Population density, call-response interval, and survival of out-of-hospital cardiac arrest. International Journal of Health Geographics 10:26.
Young, R., and L. King. 2000. An evaluation of knowledge and skill retention following an in-house advanced life support course. Nursing in Critical Care 5(1):7-14.
Yu, T., M. H. Weil, W. Tang, S. Sun, K. Klouche, H. Povoas, and J. Bisera. 2002. Adverse outcomes of interrupted precordial compression during automated defibrillation. Circulation 106(3):368-372.
Zuercher, M., R. W. Hilwig, J. Ranger-Moore, J. Nysaether, V. M. Nadkarni, M. D. Berg, K. B. Kern, R. Sutton, and R. A. Berg. 2010. Leaning during chest compressions impairs cardiac output and left ventricular myocardial blood flow in piglet cardiac arrest. Critical Care Medicine 38(4):1141-1146.






































































