
Each year, cardiac arrest strikes more than half a million people and contributes to avoidable death and disability across the United States; it affects seemingly healthy individuals of all ages, races, and genders, often without warning. Defined as a severe malfunction or cessation of the electrical and mechanical activity of the heart, cardiac arrest results in almost instantaneous loss of consciousness and collapse. Following a cardiac arrest, each minute without treatment decreases the likelihood of survival with good neurologic and functional outcomes. Thus, the consequences of delayed action can have profound and, in many cases, avoidable ramifications for individuals, families, and communities.
Conservative estimates identify cardiac arrest as the third leading cause of death in the United States, following cancer and heart disease (see Taniguchi et al., 2012). In 2013, approximately 395,000 people suffered a cardiac arrest in community settings (Daya et al., 2015).1 In hospital settings, annual cardiac arrests incidence is approximately 200,000 (Merchant et al., 2011).2 Of these, approximately 12,500 children experience cardiac arrest each year (Atkins et al., 2009; Morrison et al., 2013).
________________
1The 2013 out-of-hospital cardiac arrest (OHCA) incidence statistic (395,000) includes patient of all ages and cardiac arrests events with both cardiac and non-cardiac (e.g., trauma, drowning, poisoning, and other related causes) etiologies. This figure is an approximation based on analysis of data from the Resuscitation Outcomes Consortium-Epistry, the limitations of which are described in Chapter 2. The calculation of incidence is available in the committee’s commissioned paper (Daya et al., 2015).
2The reported statistics for in-hospital cardiac arrest (IHCA) are based a 2011 analysis, using the most recent available data (years 2003 through 2007) from the Get with the Guidelines-Resuscitation Registry (Chan, 2015). The study used three separate approaches to calculate the estimated ranges of annual in-hospital cardiac arrest (IHCA) events in the United States.
Overall, cardiac arrest survival rates remain low (Daya et al., 2015; Go et al., 2013), and the cost of care and the number of productive years lost because of cardiac arrest death and disability are large relative to other conditions, such as individual cancers (Stecker et al., 2014).
Cardiac arrest survival rates vary widely between communities and hospitals (Carr et al., 2009; Chatalas and Plorde, 2014; Merchant et al., 2014; Nichol et al., 2008) and are a reflection of complex system, environmental, and social challenges. Although some communities and hospitals have improved cardiac arrest outcomes (Blom et al., 2014; Chan et al., 2014; Wong et al., 2014), pronounced variations in outcomes persist, disproportionally affecting individuals who already have greater risks for poor health status. Notable disparities may be affected by individual demographics (e.g., race, age, gender, health status), location of arrest, initial cardiac arrest rhythm, rates of bystander cardiopulmonary resuscitation (CPR) and automated external defibrillator (AED) use, and characteristics of emergency medical services (EMS) and health care systems (e.g., response time, treatment availability, training, and care quality).
Effective treatments for specific types of cardiac arrest are widely available and could reduce deaths and disability if they were more efficiently implemented. Decreasing the time between cardiac arrest onset and the first chest compressions is critical. High-performing communities provide examples of public health infrastructures and organized system responses that facilitate timely treatments and effective transitions of care (see Chatalas and Plorde, 2014). Within systems of care, continuous quality improvement initiatives based on existing guidelines have led to more proactive and responsive care models that fit local needs and resources, contributing to higher quality care and better outcomes. Bystander-administered CPR is associated with increased survival rates and better neurologic outcomes following cardiac arrest (Bobrow et al., 2010; Kitamura et al., 2012; McNally et al., 2011; Sasson et al., 2010). Public education campaigns encourage discussions about the importance of being prepared to respond to a cardiac arrest, and advances in basic, clinical, and translational research could lead to new discoveries in cardiac arrest etiology and pathophysiology, facilitating innovative technologies, new research models, and the widespread adoption of new therapies.
However, even if all communities and hospitals maximized performance based on current knowledge and practice, better treatments and processes still are needed to improve cardiac arrest outcomes in the next decade. Fundamentally, cardiac arrest treatment is a community issue;
local resources and personnel must provide appropriate, high-quality care to save the life of a community member. But local decisions should be informed by data, analysis, and shared experience, evolving in response to emerging research and innovative therapies to improve cardiac arrest outcomes. To facilitate informed decision making and collaboration within the resuscitation field, specific barriers must be overcome.
From a social perspective, the resuscitation field has a public identity crisis, which has stymied attempts to communicate the public health threat of cardiac arrest for more than 30 years. The public often equates cardiac arrest with a heart attack, but cardiac arrests outside of hospitals (unlike heart attacks) rarely have early warning signs and require immediate intervention to avoid death and disability. Bystanders can provide basic life support treatments, by activating the EMS system, administering CPR, and applying defibrillation with an AED. Some European countries mandate first aid training, resulting in as many as 95 percent (Norway) and 80 percent (Germany) of the public trained in CPR and AED use (IFRC, 2009). However, less than 3 percent of the U.S. population receives CPR training annually (Anderson et al., 2014), rendering many bystanders unprepared to respond to cardiac arrest.
Within the resuscitation field, cardiac arrest is often characterized by location of the event (i.e., out-of-hospital cardiac arrest [OHCA] versus in-hospital cardiac arrest [IHCA]), which may be a natural reflection of the traditionally separate roles of EMS and hospital systems. However, this characterization tends to fragment the research community, limit advocacy coordination, and complicate efforts to best utilize finite resources. For example, the study and delivery of care for OHCA and IHCA are often viewed as independent and sometimes competing areas rather than complementary activities within the same system of response. Although the general risk factors and contexts for each type of cardiac arrest may differ, health outcomes depend on coordination across the systems and the alignment of quality improvement activities. Similarly, tensions related to prioritization and funding exist between the need to effectively implement interventions associated with improved outcomes and the need for basic, clinical, and translational research to generate new treatments and care paradigms.
The resuscitation field currently lacks comprehensive data and reliable measurement tools related to incidence and effective treatments, leading to broad ranging estimates and unknowns. Moreover, dedicated funding and infrastructure for resuscitation research is substantially lacking compared to diseases that account for fewer annual deaths in the
United States. For example, stroke kills approximately 130,000 people each year (CDC, 2015). However, in 2014 stroke research received seven times more support from the National Institutes of Health (NIH) than cardiac arrest research, which included studies related to cardiac arrest, sudden cardiac death, or resuscitation sciences (Lathrop, 2014; NIH, 2015). This lack of data and resources creates challenges for promoting general public and professional awareness about cardiac arrest and the need for immediate response and treatment. It also stifles the potential of resuscitation research to advance the field and improve patient outcomes.
The resuscitation field is well positioned to capitalize on an existing and substantial knowledge base and to improve health outcomes from cardiac arrest over the next decade. However, it must first overcome internal and external challenges in a cohesive and coordinated manner to maximize high-functioning survival rates for almost 600,000 individuals annually.3
SCOPE OF WORK
In 2013, the American College of Cardiology, the American Heart Association, the American Red Cross, the Centers for Disease Control and Prevention, NIH, and the U.S. Department of Veterans Affairs asked the Institute of Medicine (IOM) to conduct a consensus study on the factors affecting resuscitation research and outcomes in the United States. The IOM committee was charged with evaluating the public health dimensions of cardiac arrest treatment, with a focus on the following five areas: CPR and the use of AEDs, EMS and hospital systems of resuscitation care, national cardiac arrest statistics, resuscitation research, and future therapies and strategies for improving health outcomes from cardiac arrest within the next decade. The committee’s charge did not include examining the role or impact of prevention. Additionally, because of the quality and availability of evidence about cardiac arrest, the committee focused its analysis on treatments up through hospital discharge and outcomes through 90-days post discharge.
To respond to its charge, the IOM convened a 19-member committee with a broad range of expertise. The committee held five meetings and two public workshops throughout its term in order to solicit input from a variety of stakeholders. In addition to input received through public
________________
3This statistic is an approximation based on annual case counts of OHCA and IHCA.
workshops, the committee examined the available scientific literature and commissioned analyses of recent data on OHCA and IHCA.
A UNIFYING FRAMEWORK FOR CARDIAC ARREST
Since 1991, the chain of survival (see Figure S-1) has been the dominant operational model in the resuscitation field. The model focuses on early activation of basic and advanced life support responses for individuals with cardiac arrest, beginning in the prehospital phase and following through to post-arrest care. The likelihood of a positive outcome decreases if any link is delayed or improperly implemented. This model has been influential in strengthening the delivery of care within discrete systems, leading to increased survival rates for some pioneering communities. Strategies and interventions aimed at enhancing the recognition of cardiac arrest and increasing the timeliness and quality of care have been applied to further reinforce the chain. Although the chain of survival is useful to guide operational decisions within individual systems, a different framework is needed to identify overarching goals for the broader resuscitation field.
Promoting advances in cardiac arrest health outcomes will require coordination, cooperation, and consultation across many disciplines and actors. Fluid and formal transitions between sites of care help identify and target factors influencing patient care. To facilitate productive discussion between federal, state, local, and community representatives, a comprehensive systems-level framework is needed to guide the development of cohesive short- and long-term strategies that are necessary to reduce the public burden of cardiac arrest. Figure S-2 illustrates a systems-level framework that can be used to identify relationships between actors and organize actions between actors that affect cardiac arrest treatment and outcomes. One goal—to increase the likelihood of survival with good neurologic and functional outcomes for any person who suffers a cardiac arrest (i.e., improved patient outcomes)—provides the roof. Together, the foundation and pillars are part of an integral, comprehensive, system-level response that is necessary to revitalize the resuscitation field and improve population health and patient outcomes from cardiac arrest in the short and long term.

FIGURE S-1 Cardiac arrest chain of survival.
NOTE: ACLS = advanced cardiac life support; CPR = cardiopulmonary resuscitation..
SOURCE: Resuscitation Academy, n.d., p. 14.
Effective cardiac arrest response requires the actions of five groups (represented by the five columns in Figure S-2), who directly and indirectly affect patient outcomes. The public includes bystanders, who are at the forefront of the response and have the opportunity to report the event and initiate the response. The public also includes individuals who experience a cardiac arrest, friends and families, and individuals in industry, the workplace, schools, care facilities, and community organizations. EMS systems include 911 call takers, dispatchers, first responders, emergency medical technicians (EMTs), and paramedics, who respond to cardiac arrests and transport patients to local hospitals and emergency medical facilities after initiating resuscitation treatment. Similarly, individuals within EMS systems have the opportunity to instruct bystanders on how to administer CPR through dispatcher-assisted CPR.4 Hospitals and broader health care systems (which may include rehabilitation services) respond to cardiac arrests, provide essential post-arrest care for patients, and facilitate critical care transitions between EMS systems and various departments within the hospitals. Basic, clinical, and translational
________________
4Dispatcher-assisted CPR (also referred to as dispatcher-assisted bystander CPR, just-in-time instruction, and telecommunicator CPR) is a term that includes the identification of cardiac arrest and the provision of CPR instructions to a 911 caller prior to the arrival of EMS providers at the scene of a cardiac arrest (see Chapter 4). Because dispatchers and 911 call takers may not be the same person, especially in large 911 centers, “telecommunicator” is used as an umbrella term to refer to any individual who works in a 911 center and has responsibility for receiving calls and/or sending help. However, to remain consistent with recent Utstein core measures and with terminology generally used in emergency medicine and by the public, this report uses the term “dispatcher-assisted CPR” to mean CPR instruction provided over a phone to a rescuer by a trained individual.
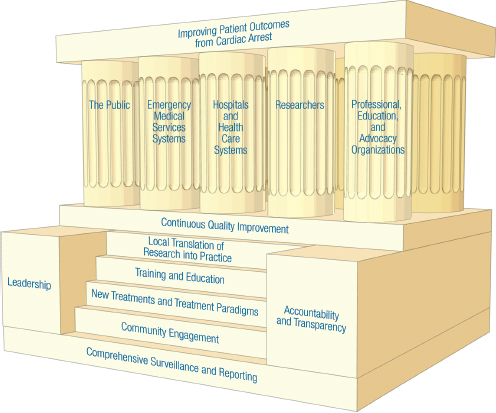
FIGURE S-2 A unifying framework for improving patient outcomes from cardiac arrest.
NOTES: This figure is based on an illustration from the Institute of Medicine’s Crisis Standards of Care series, which proposed a framework for catastrophic disaster response to assist in crisis standards of care planning (IOM, 2013, p. 18). Although the purpose and specific elements are different, the committee found the general approach useful to frame the principles, actions, and actors relevant to an overarching system of response to cardiac arrest.
researchers generate hypotheses and new insights about the mechanisms and pathophysiology of cardiac arrest identifying novel pathways for rapid delivery of innovative treatments and treatment models. Finally, professional, training, and advocacy organizations can provide opportunities to educate and train various actors across the system, promoting valuable interdisciplinary dialogue, better informed policies, and a culture of action through increased accountability. Improved patient outcomes are more likely when these actors collaborate and coordinate their activities to strengthen the field and kindle progress.
The foundation comprises six steps, each representing fundamental key actions, including (1) comprehensive surveillance and reporting, (2) community engagement, (3) new treatments and treatment paradigms, (4) training and education, (5) local translation of research into practice, and (6) continuous quality improvement. Leadership, along with transparency and accountability, serve as the cornerstones that establish the position and direction of the entire structure.
Comprehensive Surveillance and Reporting
Given the large health burden of cardiac arrest, a national responsibility exists to facilitate dialogue about cardiac arrest that is informed by comprehensive data collection and timely reporting and dissemination of information. Reliable and accurate data are needed to empower states, local health departments, EMS systems, health care systems, and researchers to develop metrics, identify benchmarks, revise education and training materials, and implement best practices. Furthermore, increasing public awareness about disparities in care and opportunities to improve outcomes can lead to greater public engagement in education and training, larger advocacy networks, and stronger community leadership efforts related to cardiac arrest.
Community Engagement
The urgent nature of cardiac arrest and the risks of mortality and disability without immediate response imply a societal obligation of bystanders to be prepared and willing to deliver basic life support before the arrival of professional emergency responders. Communities can foster a culture of action by promoting awareness of cardiac arrest symptoms, early activation of emergency medical systems, easy access to CPR and AED training, and active engagement in response to cardiac arrest. Communities can also cultivate community engagement through public advocacy, local awareness events and campaigns, and leadership opportunities that create a platform for dialogue within the community.
New Treatments and Treatment Paradigms
Strategic investment in research will increase the understanding of disease processes that can expand the availability of new therapies and drive beneficial changes in the resuscitation field. Traditional treatments
for cardiac arrest do not fully account for the complex pathophysiology of cardiac arrests. For example, although an effective treatment for some cardiac arrest rhythms (e.g., pulseless ventricular tachycardia and ventricular fibrillation), defibrillation is not effective for all cardiac arrest rhythms (e.g., those with pulseless electrical activity and asystole) nor does it address the effects of global ischemia. Treatment strategies for cardiac arrest need to evolve further based on new information generated from basic and clinical research.
Training and Education
Successful resuscitation following cardiac arrest requires a series of synchronized, exacting responses, often involving complex transitions between different actors, including bystanders, trained first responders, EMS personnel, and health care providers. Given the need for reliable competency and consistent care quality to improve health outcomes across sites of care, all actors must be educated about the burden of cardiac arrest and trained (and retrained) to provide rapid and effective treatment for cardiac arrest.
Local Translation of Research into Practice
Efficient translation of resuscitation science and research into care delivery practices is essential to optimize patient outcomes from cardiac arrest. National guidelines should be viewed as baseline standards from which regional and local practice and care delivery protocols may evolve based on emerging evidence (e.g., continuous monitoring of local data, published literature), local challenges (e.g., disparities in outcomes, low bystander response rates), state regulation and governance structure of EMS and health care systems, and available resources (e.g., trained EMS or health care personnel, funding).
Continuous Quality Improvement Programs
Widespread adoption of continuous quality improvement programs throughout the field of resuscitation would encourage data collection across all sites of care, enable comparisons within and between EMS and health care systems, and lead to the identification of best practices to improve population health and patient outcomes following cardiac arrest. Public policies encouraging such programs for other systems of care (e.g., learning health
care systems) should serve as models for the field of resuscitation, which includes a broader range of individuals responding to cardiac arrest.
Leadership
Cardiac arrest outcomes are affected by leadership across a wide range of settings, including federal agencies, state and local government (including health departments), EMS systems, health care organizations, and community clinics and advocates. Communities that have demonstrated higher cardiac arrest survival rates and favorable neurologic outcomes typically have strong civic and health care system leaders, who establish accountability for these outcomes to their communities through increased public awareness efforts, widespread training in CPR and AED use, and sustained investment in outcome measurement, data reporting, and self-assessment. With appropriate leadership, effective treatments and strategies can be implemented in other communities to save thousands of more lives across the country each year.
Accountability and Transparency
Enhanced accountability and transparency can increase operational effectiveness and efficiency by building trust among stakeholders, engaging individuals and organizations in continuous quality activities, and fostering innovation. Currently, the resuscitation field lacks appropriate transparency and accountability for cardiac arrest incidence and outcomes. As more comprehensive data become available, new opportunities will emerge to increase public awareness, enhance training across different sectors, and modify local system treatment protocols and service delivery models related to cardiac arrest. These opportunities will require explicit responsibility to collect and disseminate data to the public in order to establish accountability for system performance through various social and policy mechanisms.
ESTABLISH ROBUST DATA COLLECTION AND DISSEMINATION
Currently, national surveillance data on the incidence and factors associated with cardiac arrest do not exist. Databases that do exist are voluntary, limiting their scope and generalizability. Moreover, issues
related to data harmonization, standardized metrics and measures, common data infrastructures, and varying degrees of oversight across databases contribute to a lack of interoperability and hinder evidence-based decision making related to research support and intervention adoption and evaluation. As a result, significant gaps in knowledge persist related to the epidemiology, pathophysiology, and treatment of cardiac arrest. With critical funding for some of the larger cardiac arrest registries ending (see Chapter 2),5 it becomes increasingly important to coordinate existing surveillance activities and broaden the scope of surveillance nationally. A lead organization is necessary to promote data collection, establish sustainability and continuity, and streamline data dissemination that will drive the collective public health efforts to save lives.
Recommendation 1. Establish a National Cardiac Arrest Registry
The Centers for Disease Control and Prevention (CDC)—in collaboration with state and local health departments—should expand and coordinate cardiac arrest data collection through a publicly reported and available national cardiac arrest registry, including both out-of-hospital cardiac arrest (OHCA) and in-hospital cardiac arrest (IHCA) data, to help increase federal and state accountability for current system performance and promote actions to improve cardiac arrest outcomes.
Specifically, CDC should
- establish a cardiac arrest surveillance system for the nation that includes IHCA and OHCA data in pediatric and adult populations;
- make data publicly available through appropriate mechanisms to enable comparisons across data sets in order to increase public awareness about cardiac arrest incidence and treatments, improve accountability for emergency medical services system and health care system performance, and target interventions that will reduce disparities and improve patient outcomes;
- identify and adopt standardized definitions, criteria, and metrics (such as age, gender, race and ethnicity, socioeconomic status, and primary language) for cardiac arrest identification, treatment, and outcome assessment; and
________________
5Personal communication, J. Brown, NIH, May 22, 2015.
- promote and coordinate the development and implementation of unique diagnostic codes for OHCA and IHCA in International Classification of Diseases (ICD) coding models through its North American Collaborating Center, working with the Centers for Medicare & Medicaid Services and the World Health Organization.
Specifically, state, territorial, and local health departments should
- mandate tracking and reporting of all cardiac arrest events; and
- publicly report the incidence and outcomes of IHCA and OHCA within and across various areas within states and territories, taking appropriate steps to protect patient privacy and confidentiality.
Establishing standard definitions and data elements across local, state, national, and international stakeholders would enhance data harmonization and interoperability. These enhancements would allow for more reliable and accurate data aggregation, enable benchmarking and continuous quality improvement initiatives, and reduce unnecessary confusion in an already complex field of study.
EDUCATE AND TRAIN THE PUBLIC
Although evidence indicates that bystander CPR and AED use can significantly improve survival and outcomes from cardiac arrest, rates of bystander training in CPR and AED use remain less than 3 percent annually in the United States (Anderson et al., 2014). The public’s current inability to recognize cardiac arrest, initiate CPR, and apply AEDs presents a call for action. An informed, coordinated, and effective campaign to promote public education and training opportunities and reduce barriers to the provision of bystander CPR and defibrillation would provide immense value to the overall health of the nation.
Recommendation 2. Foster a Culture of Action Through Public Awareness and Training
State and local departments of health and education, and leading organizations in cardiac arrest response and treatment, should partner with training organizations, professional organizations, public advocacy groups, community and neighborhood organizations and service providers, and local employers to promote public awareness of the signs, symptoms, and treatment of cardiac arrest. These efforts require public cardiopulmonary resuscitation (CPR) and automated external defibrillators (AED) training across the lifespan, creating a culture of action that prepares and motivates bystanders to respond immediately upon witnessing a cardiac arrest. Specifically,
- State and local education departments should partner with training organizations and public advocacy groups to promote and facilitate CPR and AED training as a graduation requirement for middle and high school students;
- Employers (e.g., federal agencies, private business owners, and schools) should be encouraged to maintain easy-to-locate and clearly marked AEDs, provide CPR and AED training to their employees, and specifically include cardiac arrest in formal emergency response plans; and
- Local health departments should engage with community and neighborhood organizations and service providers to expand the types and locations of available CPR and AED training to populations over age 65 and caregivers for this population.
IMPROVE DELIVERY OF HIGH-QUALITY RESUSCITATION AND POST-ARREST CARE
Although it is possible to conduct broad assessments of the quality of care provided by EMS or hospital systems that are based on overall survival rates and positive neurologic and functional outcomes, it is more difficult to distinguish which specific care elements, or combination of elements, directly influence patient outcomes. Despite these challenges, a number of EMS and hospital actions related to cardiac arrest care have been associated with higher survival rates in some communities, offering
promising strategies that could be more widely adopted in order to reduce the public health burden of cardiac arrest. Standardized training and performance evaluation measures for care processes and protocols would promote a more rapid and uniform adoption and assessment of cardiac-arrest quality of care on a national scale.
Recommendation 3. Enhance the Capabilities and Performance of Emergency Medical Services (EMS) Systems
As the informal agency for EMS, the National Highway Traffic Safety Administration should coordinate with other federal agencies and representatives from private industry, states, professional organizations, first responders, EMS systems, and nonprofit organizations to promote uniformly high-quality emergency medical systems by
- convening interested stakeholders to develop standardized dispatcher-assisted cardiopulmonary resuscitation (CPR) protocols and national educational standards for use by all public safety answering points; and
- establishing a standardized definition and training curriculum for high-performance CPR to be used in basic emergency medical technician training and certification.
Recommendation 4. Set National Accreditation Standards Related to Cardiac Arrest for Hospitals and Health Care Systems
The Joint Commission—in collaboration with the American Red Cross, the American Heart Association, hospital systems, hospitals, professional organizations, and patient advocacy groups—should develop and implement an accreditation standard for health care facilities specific to cardiac arrest care for adult and pediatric populations.
Recommendation 5. Adopt Continuous Quality Improvement Programs
Emergency Medical Services (EMS) systems, health care systems, and hospitals should adopt formal, continuous quality improvement programs for cardiac arrest response that
- assign responsibility, authority, and accountability within each organization or agency for specific cardiac arrest measures;
- implement core technical and nontechnical training, simulation, and debriefing protocols to ensure that EMS and hospital personnel can respond competently to both adult and pediatric cardiac arrests; and
- actively collaborate and share data to facilitate national, state, and local benchmarking for quality improvement.
INCREASE THE IMPACT OF CARDIAC ARREST RESEARCH AND THERAPIES
Resuscitation science should be a major force in advancing patient outcomes. New research findings and emerging discoveries related to pharmaceuticals, devices, and biosensors provide compelling promise for boosting survival and positive outcomes and for reshaping approaches to the cardiac arrest treatments and care delivery models. However, federal agency support for resuscitation research is less than diseases and conditions with similar incidence. Large knowledge gaps about the etiology, epidemiology, pathophysiology, and even the effectiveness of current therapies for cardiac arrest persist. Future research must include a focus on basic, clinical, and translational science that leads to newer therapies. These, in turn, require clinical studies to develop sound evidence for, and the wide adoption of, best practices and interventions, as well as the evaluation of existing and new therapy effectiveness.
Recommendation 6. Accelerate Research on Pathophysiology, New Therapies, and Translation of Science for Cardiac Arrest
In order to identify new, effective treatments for cardiac arrest, the National Institutes of Health (NIH), the American Heart Association, and the U.S. Department of Veterans Affairs should lead a collaborative effort with other federal agencies and private industry to build the nation’s research infrastructure that will support and accelerate innovative research on the causal mechanisms of onset, pathophysiology, treatment, and outcomes of cardiac arrest. These actions should
- strengthen laboratory, clinical, and translational resuscitation research support to levels commensurate with the public health burden of cardiac arrest for adult and pediatric populations across federal agencies, including NIH institutes; and
- establish a balanced and comprehensive portfolio of grants across the full spectrum of science translation to encourage the development and application of novel and efficient research strategies and innovative trial designs in preclinical, clinical (e.g., exploratory and hypothesis-generating studies), and population-based resuscitation research.
Recommendation 7. Accelerate Research on the Evaluation and Adoption of Cardiac Arrest Therapies
The National Institutes of Health should lead a collaborative effort with the U.S. Department of Veterans Affairs, the Agency for Healthcare Research and Quality, and the Patient-Centered Outcomes Research Institute to prioritize health services research related to the identification, evaluation, and adoption of best practices; the use of innovative technologies (e.g., mobile and social media strategies to increase bystander cardiopulmonary resuscitation or automated external defibrillator use); and the development of new implementation strategies for cardiac arrest treatments.
STRENGTHEN STAKEHOLDER COLLABORATION
Numerous organizations and institutions have supported valuable activities to advance the science and implementation of resuscitation. These efforts have led to critical progress within the field over the years. These efforts, however, have not established a united advocacy presence to heighten the visibility of cardiac arrest as a treatable public health threat that warrants the attention and support of policy makers and the public. To develop shared strategies, identify and support new leaders and advocates, and maximize the impact of limited resources within a field, formal and sustained collaboration is essential.
Recommendation 8. Create a National Cardiac Arrest Collaborative
The American Heart Association and the American Red Cross—with the U.S. Department of Health and Human Services and other federal agencies, national and international resuscitation councils, professional organizations, private industry, and patient advocates—should establish a National Cardiac Arrest Collaborative to unify the cardiac arrest field, identify common
goals, and build momentum within the field to ultimately improve survival from cardiac arrest with good neurologic and functional outcomes. The Collaborative should
- provide a platform for information exchange about key successes and failures in different systems and settings and for stakeholder communication about new research findings and initiatives;
- convene working groups on short- and long-term national research priorities for cardiac resuscitation and post-arrest care, which focus on critical knowledge gaps (such as the impact of care transitions; the organization, composition, and training of resuscitation teams; optimal timing of initial neurological evaluation; and appropriate withdrawal-of-care protocols);
- develop action strategies related to health policy, research funding and translation, continuous quality improvement, and public awareness and training;
- produce and update toolkits for different stakeholders (e.g., emergency medical services [EMS] systems, hospitals, local health departments, and local health care providers) in order to facilitate effective system and individual responses to cardiac arrest;
- hold an annual collaborative meeting in conjunction with a regularly scheduled health professional conference to discuss short- and long-term goals and progress; and
- encourage public–private partnerships to support activities that focus on reducing the time to defibrillation for cardiac arrest, including the development of technologies to facilitate automated external defibrillator registries for use by the public, EMS systems, and other stakeholders.
REFERENCES
Anderson, M. L., M. Cox, S. M. Al-Khatib, G. Nichol, K. L. Thomas, P. S. Chan, P. Saha-Chaudhuri, E. L. Fosbol, B. Eigel, B. Clendenen, and E. D. Peterson. 2014. Cardiopulmonary resuscitation training rates in the United States. JAMA Internal Medicine 174(2):194-201.
Atkins, D. L., S. Everson-Stewart, G. K. Sears, M. Daya, M. H. Osmond, C. R. Warden, and R. A. Berg, for the Resuscitation Outcomes Consortium Investigators. 2009. Epidemiology and outcomes from out-of-hospital cardiac arrest in children: The Resuscitation Outcomes Consortium Epistry-Cardiac Arrest. Circulation 119(11):1484-1491.
Blom, M. T., S. G. Beesems, P. C. M. Homma, J. A. Zijlstra, M. Hulleman, D. van Hoeijen, A. Bardai, J. G. P. Tijssen, H. Tan, and R. W. Koster. 2014. Improved survival after out-of hospital cardiac arrest and use of automated external defibrillators. Circulation 130:1868-1875.
Bobrow, B. J., D. W. Spaite, R. A. Berg, U. Stolz, A. B. Sanders, K. B. Kern, T. F. Vadeboncoeur, L. L. Clark, J. V. Gallagher, J. S. Stapczynski, F. LoVecchio, T. J. Mullins, W. O. Humble, and G. A. Ewy. 2010. Chest compression-only CPR by lay rescuers and survival from out-of-hospital cardiac arrest. Journal of the American Medical Association 304(13):1447-1454.
Carr, B. G., J. M. Kahn, R. M. Merchant, A. A. Kramer, and R. W. Neumar. 2009. Inter-hospital variability in post-cardiac arrest mortality. Resuscitation 80(1):30-34.
CDC (Centers for Disease Control and Prevention). 2015. Stroke facts. http://www.cdc.gov/stroke/facts.htm (accessed June 8, 2015).
Chan, P. S. 2015. Public health burden of in-hospital cardiac arrest. Paper commissioned by the Committee on the Treatment of Cardiac Arrest: Current Status and Future Directions. http://www.iom.edu/~/media/Files/Report%20Files/2015/GWTG.pdf (accessed June 30, 2015).
Chan, P. S., B. McNally, F. Tang, and A. L. Kellermann. 2014. Recent trends in survival from out-of-hospital cardiac arrest in the United States. Circulation 130(21):1876-1882.
Chatalas, H., and M. Plorde, eds. 2014. Division of Emergency Medical Services 2014 Annual Report to the King County Council. Seattle, WA: Emergency Medical Services Division of the Public Health Department—Seattle and King County. http://www.kingcounty.gov/healthservices/health/%7e/media/health/publichealth/documents/ems/2014AnnualReport.ashx (accessed June 8, 2015).
Daya, M., R. Schmicker, S. May, and L. Morrison. 2015. Current burden of cardiac arrest in the United States: Report from the Resuscitation Outcomes Consortium. Paper commissioned by the Committee on the Treatment of Cardiac Arrest: Current Status and Future Directions. http://www.iom.edu/~/media/Files/Report%20Files/2015/ROC.pdf (accessed June 30, 2015).
Go, A. S., V. L. Roger, E. J. Benjamin, J. D. Berry, W. B. Borden, D. M. Bravata, S. Dai, E. S. Ford, C. S. Fox, S. Franco, H. J. Fullerton, C. Gillespie, S. M. Hailpern, J. A. Heit, V. J. Howard, M. D. Huffman, B. M. Kissela, S. J. Kittner, D. T. Lackland, J. H. Lichtman, L. D. Lisabeth, D. Magid, G. M. Marcus, A. Marelli, D. B. Matchar, D.K. McGuire, E. R. Mohler, C. S. Moy, M. E. Mussolino, G. Nichol, N. P. Paynter, P. J. Schreiner, P.D.
Sorlie, J. Stein, T. N. Turan, S. S. Virani, N. D. Wong, D. Woo, M. B. Turner; on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. 2013. Heart disease and stroke statistics—2013 update: A report from the American Heart Association. Circulation 127(1):e6-e245.
IFRC (International Federation for Red Cross and Red Crescent Societies). 2009. First aid for a safer future: Focus on Europe. https://www.ifrc.org/PageFiles/53459/First%20aid%20for%20a%20safer%20future%20Focus%20on%20Europe%20%20Advocacy%20report%202009.pdf?epslanguage=en (accessed June 8, 2015).
IOM (Institute of Medicine). 2013. Crisis standards of care: A toolkit for indicators and triggers. Washington, DC: The National Academies Press.
Kitamura, T., T. Iwami, T. Kawamura, M. Nitta, H. Nagao, H. Nonogi, N. Yonemoto, and T. Kimura; for the Japanese Circulation Society Resuscitation Science Study Group. 2012. Nationwide improvements in survival from out-of-hospital cardiac arrest in Japan. Circulation 126(24):2834-2843.
Lathrop, D. 2014. Charge to the consensus study committee treatment of cardiac arrest: Current status and future directions. Presentation at the first meeting of the Committee on Treatment of Cardiac Arrest: Current Status and Future Directions, Washington, DC. https://www.iom.edu/~/media/Files/Activity%20Files/PublicHealth/TreatmentofCardiacArrest/2014MAR-12/IOM%20-%20Lathrop.pdf (accessed June 8, 2015).
McNally, B., R. Robb, M. Mehta, K. Vellano, A. L. Valderrama, P. W. Yoon, C. Sasson, A. Crouch, A. B. Perez, R. Merritt, and A. Kellermann. 2011. Out-of-hospital cardiac arrest surveillance—Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005—December 31, 2010. Morbidity and Mortality Weekly Review 60(8):1-19.
Merchant, R. M., L. Yang, L. B. Becker, R. A. Berg, V. Nadkarni, G. Nichol, B. G. Carr, N. Mitra, S. M. Bradley, B. S. Abella, and P. W. Groeneveld; for the American Heart Association Get With The Guidelines-Resuscitation Investigators. 2011. Incidence of treated cardiac arrest in hospitalized patients in the United States. Critical Care Medicine 39(11):2401-2406.
Merchant, R. M., R. A. Berg, L. Yang, L. B. Becker, P. W. Groeneveld, and P. S. Chan; for the American Heart Association’s Get With The Guidelines-Resuscitation Investigators. 2014. Hospital variation in survival after in-hospital cardiac arrest. Journal of the American Heart Association 3(1):1-7.
Morrison, L. J., R. W. Neumar, J. L. Zimmerman, M. S. Link, L. K. Newby, P. W. McMullan, Jr., T. V. Hoek, C. C. Halverson, L. Doering, M. A. Peberdy, and D. P. Edelson, for the American Heart Association Emergency Cardiovascular Care Committee, the Council of Cardiopulmonary, Critical Care, Perioperative and Resuscitation; the Council on Cardiovascular and Stroke Nursing; the Council on Clinical Cardiology; and the Council on Peripheral Vascular Disease. 2013. Strategies for improving survival after in-hospital cardiac arrest in the United States: 2013 consensus
recommendations: A consensus statement from the American Heart Association. Circulation 127(14):1538-1563.
Nichol, G., E. Thomas, C. W. Callaway, J. Hedges, J. L. Powell, T. P. Aufderheide, T. Rea, R. Lowe, T. Brown, J. Dreyer, D. Davis, A. Idris, and I. Stiell; for the Resuscitation Outcomes Consortium Investigators. 2008. Regional variation in out-of-hospital cardiac arrest incidence and outcome. Journal of the American Medical Association 300(12):1423-1431.
NIH (National Institutes of Health). 2015. Estimates of funding for various research condition, and disease categories (RCDC). http://report.nih.gov/categorical_spending.aspx (accessed June 8, 2015).
Resuscitation Academy. n.d. 10 steps for improving survival from sudden cardiac arrest. http://www.resuscitationacademy.com/downloads/ebook/TenStepsforImprovingSurvivalFromSuddenCardiacArrest-RA-eBook-PDFFinal-v1_2.pdf (accessed June 8, 2015).
Sasson, C., M. A. Rogers, J. Dahl, and A. L. Kellermann. 2010. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and metaanalysis. Circulation: Cardiovascular Quality and Outcomes 3(1):63-81.
Stecker, E. C., K. Reinier, E. Marijon, K. Nayayanan, C. Teodorescu, A. Uy-Evanado, K. Gunson, J. Jui, and S. S. Chugh. 2014. Public health burden of sudden cardiac death in the United States. Circulation: Arrhythmia and Electrophysiology 7(2):212-217.
Taniguchi, D., A. Baernstein, G. Nichol. 2012. Cardiac arrest: A public health perspective. Emergency Medicine Clinics of North America 30(1):1-12.
Wong, M. K., L. J. Morrison, F. Qiu, P. C. Austin, S. Cheskes, P. Dorian, D. C. Scales, J. V. Tu, P. R. Verbeek, H. C. Wijeysundera, and D. T. Ko. 2014. Trends in short- and long-term survival among out-of-hospital cardiac arrest patients alive at hospital arrival. Circulation 130(21):1883-1890.




















