
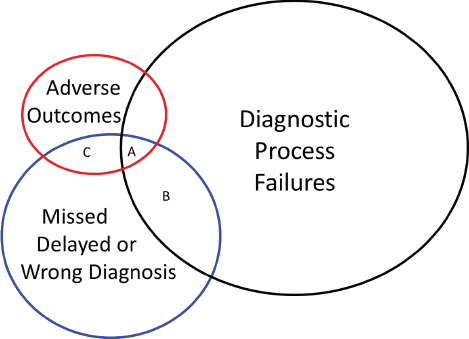
FIGURE C-1 Venn diagram illustrating relationships between errors in the diagnostic process; missed, delayed, or wrong diagnoses; and adverse patient outcomes. Group A represents adverse outcomes resulting from error-related misdiagnosis (pathology specimens erroneously mixed up [diagnostic process error], resulting in wrong patient being given diagnosis of cancer [misdiagnosis] who then undergoes surgery with adverse outcome [adverse event]). Group B represents delayed diagnoses or misdiagnoses due to process error (positive urine culture overlooked, thus a urinary tract infection is not diagnosed but patient has no symptoms or adverse consequences). Group C represents adverse events due to misdiagnoses but no identifiable process error (death from acute myocardial infarction but no chest pain or other symptoms that were missed).
SOURCES: Adapted from Schiff et al., 2005, and Schiff and Leape, 2012.
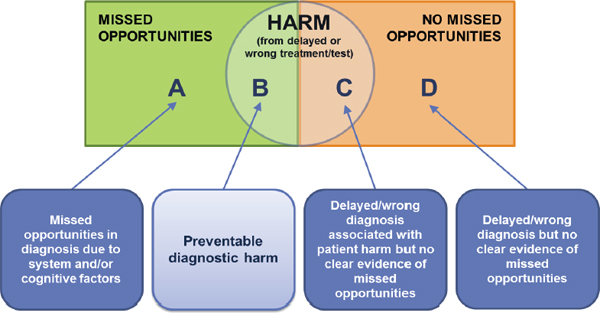
FIGURE C-2 Singh’s diagnostic error framework, which employs the term “missed opportunity” to imply “that something different could have been done to make the correct diagnosis earlier.”
SOURCE: Singh, 2014. © Joint Commission Resources: Joint Commission Journal on Quality and Patient Safety. Oakbrook Terrace, IL: Joint Commission on Accreditation of Healthcare Organizations (2014), 40(3), (100). Figure. Reprinted with permission.
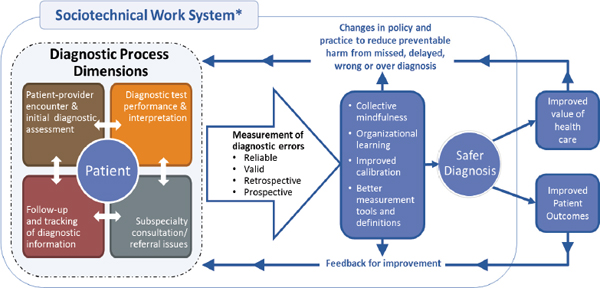
FIGURE C-3 Singh and Sittig’s diagnostic error framework, which illustrates the sociotechnical system in which diagnosis occurs and opportunities to measure and learn from diagnostic errors to improve diagnosis and patient and system outcomes.
NOTE: * Includes eight technological and non-technological dimensions.
SOURCE: Reproduced from BMJ Quality and Safety, H. Singh and D. F. Sittig, 24(2), 103–110, 2015 with permission from BMJ Publishing Group Limited.
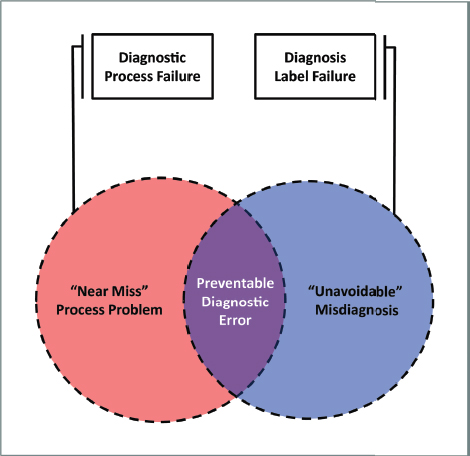
FIGURE C-4 Newman-Toker’s diagnostic error framework, which defines preventable diagnostic error as the overlap between diagnostic process failures and diagnostic label failures.
SOURCE: Reprinted, with permission, from David Newman-Toker, A unified conceptual model for diagnostic errors: Underdiagnosis, overdiagnosis, and misdiagnosis; in Diagnosis 1(1), 2014, pp. 43–48.
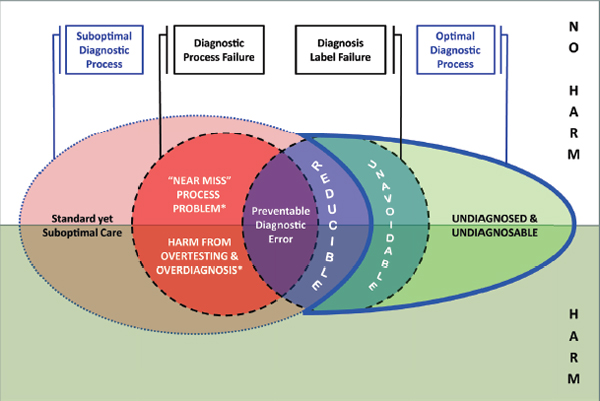
FIGURE C-5 Newman-Toker’s diagnostic error framework, including suboptimal diagnostic process and optimal diagnostic process, as well as reducible and unavoidable diagnostic error.
NOTE: * “Near misses” and harm from overtesting and overdiagnosis also result from suboptimal diagnostic processes.
SOURCE: Reprinted, with permission, from David Newman-Toker, A unified conceptual model for diagnostic errors: Underdiagnosis, overdiagnosis, and misdiagnosis; in Diagnosis 1(1), 2014, pp. 43–48.
REFERENCES
Newman-Toker, D. E. 2014. A unified conceptual model for diagnostic errors: Underdiagnosis, overdiagnosis, and misdiagnosis. Diagnosis 1(1):43–48.
Schiff, G. D., and L. L. Leape. 2012. Commentary: How can we make diagnosis safer? Academic Medicine 87(2):135–138.
Schiff, G. D., S. Kim, R. Abrams, K. Cosby, B. Lambert, A. S. Elstein, S. Hasler, N. Krosnjar, R. Odwazny, M. F. Wisniewski, and R. A. McNutt. 2005. Diagnosing diagnosis errors: Lessons from a multi-institutional collaborative project. In K. Henriksen, J. B. Battles, E. S. Marks, and D. I. Lewin (eds.), Advances in Patient Safety: From Research to Implementation (Volume 2: Concepts and Methodology). AHRQ Publication No. 05-0021-2. Rockville, MD: Agency for Healthcare Research and Quality. www.ncbi.nlm.nih.gov/books/NBK20492/pdf/Bookshelf_NBK20492.pdf (accessed Novembe 7, 2015).
Singh, H. 2014. Editorial: Helping health care organizations to define diagnostic errors as missed opportunities in diagnosis. Joint Commission Journal on Quality and Patient Safety 40(3):99–101.
Singh, H., and D. F. Sittig. 2015. Advancing the science of measurement of diagnostic errors in healthcare: The Safer Dx framework. BMJ Quality and Safety 24(2):103–110.








