
Although recent years have seen many promising advances in cancer research, there remain surprising gaps in the fundamental knowledge about and understanding of ovarian cancer. Researchers now know that ovarian cancer cannot be categorized as a single disease; several distinct subtypes exist with different origins, risk factors, genetic mutations, biological behaviors, and prognoses. However, researchers do not have definitive knowledge of how and where these various ovarian cancers arise. Such unanswered questions impede progress in the prevention, early detection, treatment, and management of ovarian cancers. In particular, the failure to improve ovarian cancer morbidity and mortality during the past several decades is likely due to several factors, including
- A lack of research focusing on specific disease subtypes;
- An incomplete understanding of genetic and nongenetic risk factors;
- An inability to develop and validate effective screening and early detection tools;
- Inconsistency in the delivery of the standard of care;
- Limited precision medicine approaches tailored to the disease subtypes and tumor characteristics; and
- Limited attention paid to research on survivorship issues, including supportive care with long-term management of active disease.
The symptoms of ovarian cancers can be nonspecific, so they are often not seen as indicating a serious illness by women or their health care providers until the symptoms worsen, at which point the cancer is often
widespread and difficult to cure. Late diagnosis is a major factor contributing to the high mortality rate. Indeed, roughly two-thirds of women with ovarian cancer are diagnosed with an advanced-stage cancer (or a cancer that has not been thoroughly staged), which is associated with less than 30 percent overall 5-year survival. Furthermore, although many ovarian cancers initially respond to treatment, the vast majority recur. Recurrent ovarian cancers may respond to further treatment, but virtually all of them will ultimately become resistant to current drug therapies. Overall, little attention has been paid to managing the acute and long-term physical and psychosocial effects of ovarian cancer diagnosis and treatment or understanding when to transition to appropriate end-of-life care.
This report gives a broad overview of the state of the science in ovarian cancer research, highlights major knowledge gaps, and provides recommendations to help reduce the incidence of and morbidity and mortality from ovarian cancers by focusing on promising research themes that could advance risk prediction, prevention, early detection, comprehensive care (e.g., treatment and supportive care), and cure.
STUDY CONTEXT, CHARGE, AND APPROACH
Although ovarian cancer is relatively uncommon, it is one of the deadliest cancers. Each year in the United States, more than 21,000 women are diagnosed with ovarian cancer, and more than 14,000 women die from the disease. Ovarian cancer is the fifth leading cause of cancer deaths among American women, and the 5-year survival rate is just under 46 percent. By contrast, the 5-year survival rate is nearly 90 percent for breast cancer, more than 80 percent for endometrial cancer, and nearly 70 percent for cervical cancer. Indeed, although the estimated number of new cases of ovarian cancer among American women each year is only one-tenth the number of new cases of breast cancer, the death-to-incidence ratio for ovarian cancer is more than three times higher than that for breast cancer (see Figure S-1).
Ovarian cancer has been called a “silent killer” because no distinctive symptoms had been associated with the early stages of the disease. However, recent research shows that most women with ovarian cancer report symptoms such as bloating, pelvic or abdominal pain, and urinary symptoms, and many women recall having had these symptoms for an extended period of time before diagnosis. In 2006, the U.S. Congress passed the Gynecologic Cancer Education and Awareness Act of 2005 (known as Johanna’s Law) to launch a campaign to “increase the awareness and knowledge of health care providers and women with respect to gynecologic cancers.”
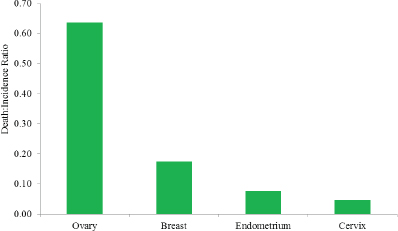
FIGURE S-1 The ratio between the death and incidence rates for ovarian, breast, endometrial, and cervical cancers per 100,000 women in the United States, 2008–2012.
Study Charge
In the fall of 2014, with support from the Centers for Disease Control and Prevention (CDC), the Institute of Medicine (IOM) formed the Committee on the State of the Science in Ovarian Cancer Research to examine and summarize the state of the science in ovarian cancer research, to identify key gaps in the evidence base and challenges to addressing those gaps, to consider opportunities for advancing ovarian cancer research, and to examine ways to disseminate new information to all stakeholders.
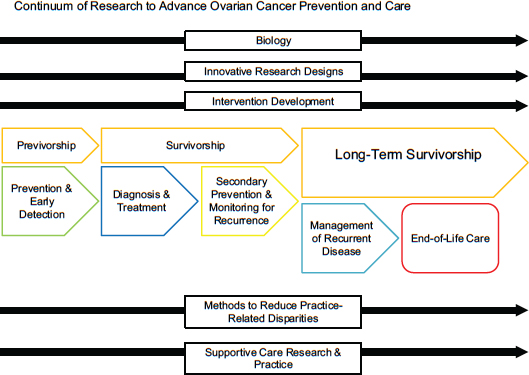
To guide its deliberative process, the committee developed a conceptual model to identify research gaps across the continuum of ovarian cancer care and also in critical areas of cross-cutting research (see Figure S-2).
Defining Ovarian Cancer
“Ovarian cancer” is a generic term often used for any primary malignant ovarian tumor, but it is a misnomer in the sense that ovarian cancer is not just one disease. Rather, it refers to a constellation of distinct types of cancer involving the ovary. Ovarian cancers with epithelial differentiation (carcinomas) represent the majority of malignant tumors and are responsible for most ovarian cancer–related deaths. This classification is complicated by recent evidence suggesting that many ovarian carcinomas do not arise in the ovary per se. Instead they may, in fact, arise in other tissues (e.g.,
the fallopian tubes) and then metastasize to the ovary, or arise from cells that are not considered intrinsic to the ovary (see Figure S-3).
Ovarian carcinomas themselves also represent a heterogeneous collection of different tumor types (see Figure S-4). Ovarian carcinomas account for more than 85 percent of ovarian cancers, and more than 70 percent of ovarian carcinomas are high-grade serous carcinomas (HGSCs). Consequently, this report focuses on ovarian carcinomas, with a particular emphasis on HGSCs, recognizing that other less common types of ovarian malignancies exist and are responsible for a smaller fraction of deaths.
RECOMMENDATIONS
The committee focused on identifying the research gaps that, if addressed, could have the greatest impact on reducing ovarian cancer morbidity or mortality. A wide variety of stakeholders are integral to ovarian cancer research, including the U.S. Congress, federal agencies (e.g., CDC, U.S. Department of Defense, U.S. Food and Drug Administration, National Institutes of Health), private foundations, industry, academic institutions, professional societies, and advocacy groups. Most of these stakeholders are engaged in research across the care continuum, and many are both funders and performers of research. The committee therefore concluded that directing research toward the gaps identified in the recommendations is the responsibility of all stakeholders in their individual and collaborative efforts to fund, perform, or advocate for ovarian cancer research.
The committee identified four overarching concepts that should be applied to each recommendation in this report:
- As the most common and lethal subtype, the study of HGSC needs to be given priority;
- Even so, more subtype-specific research is also needed to further define the differences among the various subtypes;
- Given the relative rarity and heterogeneity of ovarian cancers, collaborative research (including the pooling and sharing of data and biospecimen resources, such as through consortia) is essential; and
- The dissemination of new knowledge and the implementation of evidence-based interventions and practices are the final steps in the knowledge translation process.
These recommendations are intertwined and so need to be considered simultaneously, not sequentially. Their sequence should not be considered as indicating priority of importance or an order of implementation.
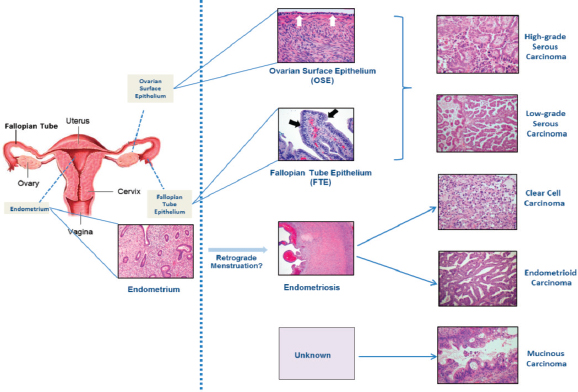
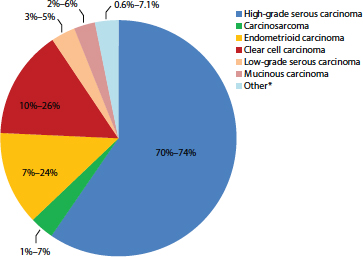
FIGURE S-4 Percentage of cases by major ovarian carcinoma subtype.
NOTE: Other* refers to mixed or transitional carcinomas where it is not possible to categorize to a single subtype.
SOURCE: Gilks et al., 2008; Seidman et al., 2003, 2004.
The Biology of Ovarian Cancer
Recent evidence suggests that many ovarian carcinomas do not arise in the ovary. Furthermore, researchers do not have a complete understanding for each subtype of how the disease progresses or the effects of the microenvironment. Without better model systems that replicate the manifestations of the human disease, the answers to many key questions will remain elusive. This research gap is further complicated by the significant degree of heterogeneity of ovarian carcinomas, including within and between subtypes. However, clinicians and researchers tend to combine them in many types of research. In spite of recent advances, the incomplete understanding of the basic biology of each subtype, including origin and pathogenesis, is an impediment to advances in prevention, screening and early detection, diagnosis, treatment, and supportive care.
RECOMMENDATION 1: Researchers and funding organizations should design and prioritize preclinical, clinical, and population-based research agendas that take into account the different ovarian cancer subtypes. A top priority should be elucidating the cellular origins and pathogenesis of each subtype. Particular attention should be paid to:
- Tumor characteristics such as microenvironment, intratumoral heterogeneity, and progression pathways;
- The development of experimental model systems that reflect ovarian cancer heterogeneity; and
- Incorporation of the multi-subtype paradigm into prevention, screening, diagnosis, and treatment research.
While it will be critical to apply this multi-subtype approach to research on ovarian cancer, an incomplete understanding of the biology of these cancers has prevented the emergence of uniform standards for describing the characteristics of the subtypes. Tumor classification, nomenclature, and grading systems have changed over time as new insights have emerged, and evidence suggests that there is substantial variability in current surgical and pathological practices for the reporting of ovarian cancers. The implementation of a single, uniformly implemented nomenclature and classification scheme (with standardized diagnostic criteria) is essential and will serve as the necessary foundation for all future research in ovarian cancer.
RECOMMENDATION 2: Pathology organizations, oncology professional groups, and ovarian cancer researchers should reach consensus on diagnostic criteria, nomenclature, and classification schemes that reflect the morphological and molecular heterogeneity of ovarian cancers, and they should promote the universal adoption of a standardized taxonomy.
Achieving this consensus will be complex. Multiple stakeholders will need to be engaged in an iterative process in which the schemes can change. Stakeholders can employ a variety of options for moving toward consensus, including the creation of ongoing working groups by subtype, as has been done in other diseases.
The committee again emphasizes that these recommendations about biology research and taxonomy need to be considered simultaneously. That is, a common taxonomy is needed based on the best currently available research, and research designs going forward will need to be based on this common taxonomy, but the taxonomy will also need to evolve as more is learned about the biology of the subtypes. For example, an improved understanding of molecular characterizations (see Recommendation 8) may, in fact, be more informative for classification than shared appearance. Simultaneously, an enhanced understanding of the characterizations of the subtypes will inform the development of targeted therapeutics (see Recommendation 9), and the drive for targeted therapeutics will, in turn, require more basic research on the biology of the ovarian cancer subtypes.
Risk Assessment, Screening, and Early Detection
Better methods for identifying high-risk women could facilitate the prevention or early detection of ovarian cancers. A family history of ovarian cancer, specific germline (inherited) genetic mutations, and certain hereditary cancer syndromes have strong associations with risk for ovarian cancer. The BRCA1 and BRCA2 genes are the most recognizable ovarian cancer risk-related genes, followed by the mismatch repair genes associated with Lynch syndrome. Several other risk-related genes have been identified but are less well studied. Although family history is linked to an increased risk for all ovarian cancer subtypes, it is most strongly linked with risk for HGSC, where up to 25 percent of women have a germline mutation. Multiple groups recommend that all women diagnosed with an invasive ovarian cancer receive genetic testing and counseling, for a variety of reasons, including to determine the appropriate therapies, to assess other health risks, and to estimate the risk for family members. Genetic counseling and testing are also recommended for the first-degree relatives of women with a hereditary cancer syndrome or germline mutation (i.e., cascade testing). For the first-degree relatives of women with ovarian cancer who have not had genetic testing, genetic counseling would be appropriate for assessing risk and the need for testing. Women without ovarian cancer who carry germline mutations associated with greatly increased risk for developing ovarian cancer (sometimes referred to as “previvors”) may benefit from enhanced screening, risk-reducing procedures, or chemoprevention. However, referrals for genetic counseling and testing are hindered by various patient-, provider-, and system-level barriers, such as a patient’s lack of awareness of her family history, the limited time that providers generally have to collect a family history, and complex and inconsistent referral criteria. Furthermore, more research is needed to determine the significance of known mutations and to discover new significant mutations for all subtypes.
RECOMMENDATION 3: Researchers, public health practitioners, and clinicians should develop and implement innovative strategies to increase genetic counseling and testing, as well as cascade testing for known germline genetic predispositions in appropriate populations (e.g., untested ovarian cancer survivors and relatives of individuals who tested positive). Furthermore, researchers, clinicians, and commercial laboratories should determine the analytic performance and clinical utility of testing for other germline mutations beyond BRCA1 and BRCA2 and the mismatch repair genes associated with Lynch syndrome.
Risk cannot be fully assessed by relying on family history alone. Up to one-half of women with high-risk germline mutations do not have an ap-
parent family history of breast or ovarian cancer, and family history may not identify risk for women with few female relatives or for women who do not know the family health history of one or both parents. Furthermore, as the majority of women with ovarian cancer do not appear to have a known high-risk germline mutation or a significant family history, it is critical to consider other potential risk factors. While several nongenetic factors are associated with either an increased or a decreased risk for developing ovarian cancer, the patterns of association are inconsistent, and the strongest factors to date are those associated with the less common and less lethal subtypes.
RECOMMENDATION 4: Researchers and funding organizations should identify and evaluate the underlying mechanisms of both new and established risk factors for ovarian cancers in order to develop and validate a dynamic risk assessment tool accounting for the various ovarian cancer subtypes. Furthermore, a spectrum of risk factors should be considered, including genetics, hormonal and other biological markers, behavioral and social factors, and environmental exposures.
Collaborations between clinicians and population and basic scientists will help identify potential new risk factors and also provide an opportunity to better understand how specific exposures influence disease development. Current research does not provide insight as into which risk factors need to be prioritized for future research. In light of the heterogeneity of the cell of origin, an emphasis on factors that influence early carcinogenesis may have the largest impact on identifying women at high risk.
Women known to be at high risk may benefit from nonsurgical and surgical preventive measures, but the risk–benefit ratios of these measures need to be better defined for different subtypes and at-risk populations. For example, the use of prescription medications (e.g., oral contraceptives) and risk-reducing surgeries (e.g., bilateral salpingo-oophorectomy and salpingectomy) need to be weighed against potential complications and long-term side effects (e.g., stroke risk, risk for other cancers, surgical complications, and overall mortality). As new prevention strategies are developed, researchers will need to amass an evidence base for their efficacy as well as their potential long-term harm.
RECOMMENDATION 5: Clinicians, researchers, and funding organizations should focus on quantifying the risk–benefit balance of nonsurgical and surgical prevention strategies for specific subtypes and at-risk populations.
Current approaches for early detection include assaying for biomarkers, often in combination with imaging technologies. While the use of these strategies in large screening trials has resulted in more ovarian cancers being detected at earlier stages, to date they have not had a substantial impact on overall mortality. Given the marked heterogeneity of ovarian cancers and the incomplete understanding of early disease development for each subtype, it is highly unlikely that a single biomarker or imaging modality will be sufficient to aid in the early detection of all the subtypes. While research on refining current methods may be fruitful, distinct multimodal approaches will likely be needed to detect each of the various subtypes at their earliest stages.
RECOMMENDATION 6: Researchers and funding organizations should focus on the development and assessment of early detection strategies that extend beyond current imaging modalities and biomarkers and that reflect the pathobiology of each ovarian cancer subtype.
Going forward, screening trials may be more informative if conducted in populations with elevated ovarian cancer risk. Research on the impact of earlier detection on quality of life will also be important.
Diagnosis and Treatment
Compared to the situation over the past few decades, newly diagnosed ovarian cancers are now being more accurately and consistently staged, and a wider variety of treatment options exist. Most women with newly diagnosed ovarian cancer undergo primary debulking surgery (PDS) to remove as much of the grossly visible tumor as possible (cytoreduction), as well as to make it possible to determine a specific diagnosis (e.g., subtype, staging). Survival is markedly better for women who have complete (or optimal) tumor resection, yet great variability exists in the extent of tumor resection. For women in whom an optimal resection is not thought to be feasible, or who are unable to undergo PDS due to comorbidities, neoadjuvant chemotherapy (NACT) can reduce tumor size and facilitate subsequent resection. After surgery, women typically receive multiple cycles of chemotherapy. While the majority of women respond well to initial treatment, most will experience a recurrence of the disease, resulting in a cycle of repeated surgeries and additional rounds of chemotherapy.
Standard of Care
Several organizations have developed national clinical practice guidelines for the assessment and treatment of women with both newly diag-
nosed and recurrent ovarian cancers. While women who receive care in accordance with these guidelines have considerably better clinical outcomes (e.g., improved survival and fewer surgical complications), less than one-half of women with ovarian cancer receive such care. For example, while the intraperitoneal (IP) route for the delivery of chemotherapy offers notable advantages over intravenous (IV) and oral routes, the adoption of IP chemotherapy protocols is not widespread. However, this is due in part to concerns regarding the efficacy and potential adverse effects of IP administration, and the better side-effects profile associated with newer IV regimens. In addition to the variation in adherence to standards of care for surgery and chemotherapy, the guidelines for cancer genetics referrals are not routinely or widely implemented (see Recommendation 3). Testing for germline mutations among women newly diagnosed with ovarian cancer is important because the presence of certain mutations informs therapy decisions.
Being treated by a gynecologic oncologist and having treatment in a high-volume hospital or cancer center are the two most significant predictors of whether a woman with ovarian cancer will receive the standard of care, and both are associated with better outcomes, but access to such care can be a challenge. Significant predictors of nonadherence to the standard of care include the patient being of advanced age at diagnosis, the presence of treatment-limiting comorbidities, being of a nonwhite race, and having a lower socioeconomic status. Like most other cancers, ovarian cancer primarily affects older adults, but little is known about the care of older women with ovarian cancer. For example, older women with comorbidities may be precluded from receiving the standard of care, which, in turn, may lead to worse outcomes. Also, historical trends show differences in outcomes by race, but the reasons for this are unknown. Finally, more research is needed on how quality metrics (including measures of outcomes) can help drive continuous quality improvement in ovarian cancer care. The current patterns of care reveal inconsistencies in therapeutic approaches and disparities in care delivery, which may contribute to poorer outcomes.
RECOMMENDATION 7: To reduce disparities in health care delivery and outcomes, clinicians and researchers should investigate methods to ensure the consistent implementation of current standards of care (e.g., access to specialist care, surgical management, chemotherapy regimen and route of administration, and universal germline genetic testing for newly diagnosed women) that are linked to quality metrics.
However, no one model of care will serve all patients in all settings. For example, women in rural settings may not have access to a gynecologic oncologist or a high-volume cancer center. Therefore, it will be necessary
to explore innovative models of care that can help deliver the standard of care, such as the use of telemedicine for consultation and the use of patient navigation systems to support self-management. The committee recognizes that, as is the case in other areas of health care, issues such as payment, policy, and education and training of the health care workforce affect the delivery of the standard of care, and so these issues will also need further examination as new models are developed.
Predicting Response
While adherence to standards of care leads to improved outcomes, little is known about why some women respond better to specific surgical and chemotherapeutic therapies, or about how age affects treatment. For example, the question of which women should receive initial PDS or NACT remains unresolved. It may be that women with certain subtypes respond better to different therapies or that women who respond particularly well to a given treatment may share characteristics that extend beyond their tumor subtype.
Current classification systems also do not, for the most part, help to tailor treatment regimens. Recurrent ovarian cancers have traditionally been categorized as platinum sensitive if recurrence is diagnosed more than 6 months from prior therapy or platinum resistant if recurrence is diagnosed less than 6 months from prior therapy, but this classification does not reflect the mechanisms of recurrent disease. Several assays have been developed (or are in development) to determine the likelihood of primary and recurrent tumors’ ability to respond to various chemotherapeutic agents, but at this time none of them have been validated.
RECOMMENDATION 8: Clinicians and researchers should focus on improving current treatment strategies, including
- The development and validation of comprehensive clinical, histopathologic, and molecular characterizations that better inform precision medicine approaches for women with newly diagnosed and recurrent disease;
- Advancement in the understanding of the mechanisms of recurrent and drug-resistant (e.g., platinum-resistant) disease and the development of a more informative classification system;
- The identification of predictors of response to therapy and near-term indicators of efficacy; and
- The determination of the optimal type and timing of surgery in women newly diagnosed with ovarian cancer and of the efficacy of subsequent cytoreduction procedures for women with recurrent disease.
Several modalities can be used to match individual patients to specific procedures and treatments. The analysis of biomarkers, the determination of the molecular features of tumors, minimally invasive assessments (e.g., laparoscopy), and the use of imaging all provide insights. Similarly, a variety of approaches can be used to predict therapeutic efficacy, including scoring systems, genetic panel testing, and molecular profiling. The knowledge gained through these precision medicine approaches will also help to inform the development of new and better treatments.
Developing Better Treatments
While clinicians need better ways to select the most appropriate among existing treatments for individual patients, they also need more treatment options, and the development of better treatments depends in large part on the clinical trials system. The 2010 IOM report A National Cancer Clinical Trials System for the 21st Century outlined principles to improve the clinical trials system in general, including
- Improve collaboration among stakeholders, including the use of consortia;
- Define an effective mechanism for combining products in clinical trials;
- Develop and evaluate novel trial designs;
- Increase the accrual volume, diversity, and speed of clinical trials; and
- Educate patients about the availability, payment coverage, and value of clinical trials.
These principles are particularly relevant for ovarian cancer research, given the relative rarity of the disease combined with the diversity of subtypes. Comparative effectiveness studies, combination therapies, and multimodality strategies will all be important. This committee endorses these principles and suggests that they be applied to all recommendations related to clinical trials for ovarian cancer research.
Clinicians currently have few options for drug therapy, and the long-term efficacy of these agents is limited by a high rate of drug resistance. A better understanding of the diversity of ovarian cancers will offer the potential for targeted treatments. Innovative early phase clinical trial designs that incorporate biomarkers predictive of efficacy are needed to help identify which subtypes are likely to be responsive to specific new therapies. However, selecting clinically meaningful endpoints for trials in ovarian cancer can be challenging. For example, it may be difficult to determine the impact of a single agent on overall survival because women have typi-
cally had multiple previous therapies. Patient preferences also need to be considered in assessing the effectiveness of new therapies (e.g., the tolerable levels of side effects, given the expected outcomes). Furthermore, little research exists on nonpharmacologic therapies and interventions (e.g., diet, exercise, stress reduction) that might affect response to treatment. Overall, the current standard of care lacks precision medicine approaches to therapy.
RECOMMENDATION 9: Researchers should develop more effective pharmacologic and nonpharmacologic therapies and combinations of therapies that take into account the unique biology and clinical course of ovarian cancer. These approaches should include
- Developing immunologic and molecularly driven treatment approaches specific to the different ovarian cancer subtypes;
- Identifying markers of therapeutic resistance and exceptional response; and
- Using interdisciplinary teams to design and conduct statistically efficient and information-rich clinical studies.
The development of new approaches, however, will depend on developing a better understanding of the basic biology of the ovarian cancer subtypes (see Recommendation 1). As the committee did not find evidence for the superiority of any single treatment, it concluded that a variety of approaches need to be evaluated, including new combinations of existing drugs, new drug formulations, targeted biologics, protein inhibitors, TP53-directed therapies, anti-angiogenics, immunotherapies, and nonpharmacologic interventions. All of these approaches have merit because their effectiveness may vary within and among subtypes.
Supportive Care Along the Survivorship Trajectory
Most research on ovarian cancers focuses on the treatment of the disease rather than on how to improve the management of the acute and long-term physical and psychosocial effects of diagnosis and treatment across the trajectory of survivorship. Although research on therapies that may provide life-saving benefit is crucial, complementary research on how to best support women living with ovarian cancer and improve their quality of life is also important for them and their families. Women with ovarian cancer require early and ongoing supportive care to ensure that aggressive, life-extending treatments are enhanced by multidisciplinary supportive care to maximize quality of life.
The 2013 IOM report Delivering High-Quality Cancer Care stated, “A high-quality cancer care delivery system depends on clinical research that gathers evidence of the benefits and harms of various treatment options
so that patients, in consultation with their clinicians, can make treatment decisions that are consistent with their needs, values, and preferences.” However, for women with ovarian cancer, shared decision making and the management of the physical and psychosocial effects of diagnosis and treatment may be neglected in the effort to urgently address the disease, which is typically at an advanced stage at diagnosis. Also, a lack of professional expertise or resources may hinder joint decision making.
Current research provides little insight as to which women are most likely to suffer physical and psychosocial effects due to their diagnosis and treatment, or the best approaches for managing these effects. Furthermore, there may be differences in the needs of and best approaches for women of different demographic groups (e.g., older women versus younger women and women of different racial and ethnic groups). These research gaps may be addressed by more effective assessment of patient-reported symptoms and outcomes during treatment, especially on the outcomes that are most important to women (e.g., improved quality of life versus overall survival). Approaches to enhancing self-management, including leveraging mobile health technologies, need to be explored. Finally, as many women with ovarian cancer continue active treatment until the end of their lives, researchers need to help better define when disease-focused treatments are unlikely to be effective and the focus needs to shift to end-of-life care.
A majority of women with ovarian cancer require long-term active disease management, necessitating more effective approaches for supportive care and self-management.
RECOMMENDATION 10: Researchers and funding organizations should study the supportive care needs of patients with ovarian cancer throughout the disease trajectory, including
- Identifying the array of factors that put women at high risk for poor physical and psychosocial outcomes;
- Identifying and overcoming barriers to the systematic assessment of the physical and psychosocial effects of disease and treatment;
- Developing and implementing more effective supportive care and self-management interventions; and
- Defining the parameters that indicate when patients and their families would benefit from transitioning to end-of-life care.
Many of the supportive care needs of women with ovarian cancer are similar to those of women with other cancers. The committee endorses the following principles from previous IOM reports:
- Develop clinical tools and strategies to ensure that all cancer patients receive the standard of psychosocial care, including
-
- Approaches for improving patient–provider communication and providing decision support,
- Screening instruments to identify psychosocial problems,
- Needs assessment instruments for psychosocial care planning, and
- Illness and wellness management interventions.
- Provide patients and their families with understandable information on cancer prognosis, treatment benefits and harms, palliative care, psychosocial support, and estimates of costs.
- Develop a common set of data elements that capture patient-reported outcomes, relevant patient characteristics, and health behaviors.
- Provide fact-based information to encourage advance care planning.
- Provide end-of-life care consistent with individual needs, values, and preferences.
Dissemination and Implementation
Amassing evidence on risk factors, treatments, and preventive strategies is not sufficient to ensure that this knowledge will be acquired and used by all stakeholders. A number of factors influence the movement of science into regular and effective use, including the complexity of health care systems, the capacity of practitioners and providers to absorb new knowledge, and the diversity of stakeholders. While the knowledge base on ovarian cancers has advanced, not all stakeholder groups are receiving important messages. This may contribute to the current variability seen in the delivery of the standard of care which, in turn, affects patient outcomes.
RECOMMENDATION 11: Stakeholders in ovarian cancer research, clinical care, and advocacy should coordinate the efforts to develop and implement efficient, effective, and reliable methods for the rapid dissemination and implementation of evidence-based information and practices to patients, families, health care providers, advocates, and other relevant parties. These efforts should include
- Researching impediments to adopting current evidence-based practices;
- Using multiple existing dissemination modalities (e.g., continuing education, advocacy efforts) to distribute messages strongly supported by the evidence base; and
- Evaluating newer pathways of dissemination and implementation (e.g., social media, telemedicine with specialists).
CONCLUSION
While progress has been made in understanding ovarian cancers over the past few decades, much remains to be learned, especially about the origins and mechanisms of development—fundamental knowledge that could change paradigms for prevention, screening and early detection, and treatment. Improved communication is also needed to recognize ovarian cancer as a constellation of many types of cancer involving the ovary. A focus on distinct areas of research within and across the continuum of ovarian cancer care will help improve the lives of all women at risk for or diagnosed with an ovarian cancer.


















