
6
Epidemiologic Studies: Background on Multiply Referenced Populations
This chapter presents study-design information on populations of Vietnam veterans, occupational cohorts, and environmentally exposed groups that have been reported on repeatedly, often for many health outcomes, as well as case-control studies that have generated multiple publications relevant to the Veterans and Agent Orange1 (VAO) series. One-time reports on given study populations that addressed only single health outcomes are not discussed in this chapter.
In drawing its conclusions, the committee synthesized the evidence from studies that have gathered data and published results over an extended period of time, taking into account the interdependence among related studies. In particular, if new results are based on updating or adding subjects to previously studied populations or concern a subset of original study populations, then this synthesis considers the redundancy among studies while recognizing that separately reported information can impart new relevance to other data on a study population. The design information provided in this chapter links repeated studies and clarifies their interdependence.
This chapter also provides design information on studies involving multiple health outcomes in order to avoid repetition in the health-outcomes chapters (Chapters 7–13). Some of the populations have been studied previously and reviewed in previous VAO publications (thus, these populations are multiply referenced both over time and among health outcomes), and others have not been
________________
1Despite loose usage of “Agent Orange” by many people, in numerous publications, and even in the title of this series, this committee uses “herbicides” to refer to the full range of herbicide exposures experienced in Vietnam, while “Agent Orange” is reserved for a specific one of the mixtures sprayed in Vietnam.
addressed in other VAO publications. The procedures used to identify relevant literature on health effects in human populations in conjunction with exposure to the chemicals of interest (COIs) are provided in Chapter 2. The details of the exposure assessments conducted within individual studies are presented in this chapter, whereas generic issues of exposure assessment are discussed in Chapter 3 along with the special challenges involved in characterizing and reconstructing the herbicide exposures of Vietnam veterans.
In Update 2010, the committee undertook a major change in the formatting of the tables of cumulative results on the health outcomes that was aimed at making relationships among publications more evident for its own deliberations and for the reader. The prior practice had been to insert findings from new publications in the results tables at the beginning of the sections on veteran, occupational, and environmental studies and so to create bands of studies reviewed in individual updates. Since Update 2010, however, the reported findings on a given condition from a particular study population described in any of the VAO reports are gathered and presented in reverse chronologic order in order to provide the full history of the study of each endpoint in each group studied. The current update has attempted to shift the focus further to the total picture presented by a study population by clustering related findings and shifting the citations that were the source of particular results to the far right of the results tables. For instance, all incidence findings on the Seveso cohort over the successive follow-up periods are grouped first, and they are followed by all the analogous mortality findings, even when that means separating various sorts of results from the same publication.
Within the three general types of exposure that cohorts or cross-sectional study populations may have experienced, the order of the study populations (Vietnam veterans, occupationally exposed workers, and environmentally exposed people) roughly reflects the degree of importance attributed to the information generated. Because of substantial differences in the nature and intensity of their exposures, the occupational-study populations have been partitioned into those involved in the production of herbicides and other industrial products contaminated with 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) and those involved in occupational use of the herbicides of interest. In Update 2012 this entailed splitting the findings on cohorts of sprayers from those on cohorts of production workers in the large International Agency for Research on Cancer (IARC) cohort of phenoxy herbicide workers.
The studies of subgroups are presented after those on an overarching cohort. For example, when first reported (Saracci et al., 1991), the original IARC Cohort of Phenoxy Herbicide Workers was composed of 20 cohorts in 10 countries that had been studied separately. When the mortality in those workers was followed up (Kogevinas et al., 1997), they were augmented with 16 additional cohorts—4 German study populations and 12 groups of workers studied separately in US manufacturing facilities—which together make up the independently studied National Institute for Occupational Safety and Health (NIOSH) cohort. To simplify
the location of underlying information on study populations, the discussion of the study populations in this chapter follows the order in which the findings on each population are presented in the results tables for each health outcome.
The initial review section below on Vietnam veterans covers studies conducted in the United States by the Air Force, the Centers for Disease Control and Prevention (CDC), the Department of Veterans Affairs (VA), the American Legion, and individual states; it also covers studies of Australian, New Zealand, and South Korean Vietnam veterans. The section “Occupational Studies” covers studies of workers other than Vietnam veterans exposed occupationally to the COIs and dioxin-like compounds, including production workers, agriculture and forestry workers (including herbicide and pesticide applicators), and paper and pulp workers. The section “Environmental Studies” covers studies of populations exposed to the COIs and dioxin-like compounds from nonoccupational sources, including the general population, such as the National Health and Nutrition Examination Survey cohort, and people who had unusually high exposures because of industrial sources in their residential neighborhoods, such as the residents of Seveso, Italy; southern Vietnam; suburban Taichung, Taiwan; Chapaevsk, Russia; and Times Beach, Missouri. This chapter ends with a section that addresses the publications that are based on repeatedly mentioned case-control study populations; the case-control studies that assessed Vietnam-veteran status, however, are included in the section on veteran studies, and nested case-control studies are presented in conjunction with the cohorts from which they were derived.
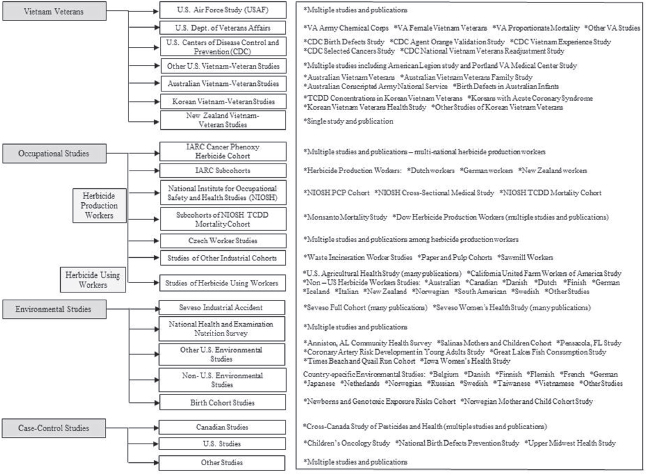
Because of the breadth of literature reviewed in this chapter, Figure 6-1 provides the reader with a comprehensive overview of the individual study populations reviewed.
VIETNAM-VETERAN STUDIES
Studies of Vietnam veterans who might have been exposed to herbicides, including Agent Orange, have been conducted in the United States at the national and state levels and in Australia, South Korea, and New Zealand. Exposures have been defined in various ways, and health outcomes have been evaluated with reference to various comparison or control groups. This section is organized primarily by research sponsor because it is more conducive to a methodologic presentation of the studies. The specificity of exposure spans a wide range from the individual exposures of Ranch Hand and Army Chemical Corps (ACC) personnel, as reflected in serum TCDD measurements, to the use of service in Vietnam as a surrogate for TCDD exposure in some studies.
Several comparison groups have been used for veteran cohort studies: Vietnam veterans who were stationed in areas where herbicide-spraying missions were unlikely to have taken place; Vietnam-era veterans who were in the military at the time of the conflict but did not serve in Vietnam; veterans who served in
other wars or conflicts, such as the Korean War and World War II; and various state and national populations.
In all studies of Vietnam veterans, whether or not the study participants were American, the study participants are the target population of the committee’s charge, and they are assumed to have had a higher probability of exposure to the COIs than people who did not serve in Vietnam, whether or not their individual exposures are characterized beyond the mere fact that they were deployed to Vietnam.
The publication period considered in the present update included the examination of a range of health outcomes among Vietnam veterans with service history from the United States, as well as countries outside the United States. This included a long-term mortality analysis conducted among US female Vietnam veterans (Kang et al., 2014), a 20-year mortality and cancer incidence study among New Zealand Vietnam veterans (McBride et al., 2013), and six publications from an exceptionally large cohort of approximately 120,000 Korean veterans (Yi, 2013; Yi and Ohrr, 2014; Yi et al., 2013a,b, 2014a,b). For the Korean Vietnam veteran studies, multiple methods of exposure ascertainment were used, including self-report perceived exposure to herbicides and an objective geography-based exposure opportunity model. Similarly, multiple methods of health outcome ascertainment were used, including veteran self-report and a review of data from the Korean Cancer Incidence Database, the Korea National Health Insurance system, and death records from the National Statistical Office. The committee carefully considered the strengths and limitations of the different methods of exposure and health outcome ascertainment in synthesizing the evidence from the large Korean Veteran study. In addition, a series of four publications was reviewed looking at Australian Vietnam veterans (ADVA, 2014a,b,c,d), but the focus of these publications was on the family members of Australian veterans, and many health outcomes of these family members are not central to the charge of the committee (e.g., mental health and social functioning). Thus, minimal consideration was given to the new evidence from these publications.
US Air Force Health Study
Reports and findings from the US Air Force Health Study (AFHS) have provided important information that was incorporated into the previous VAO reports and continue to play an important role in the committee’s assessment of the overall evidence for the current report. The data-gathering phase of this study is complete, but VAO committees have remained interested in having the opportunity to review additional publications that provide longitudinal analysis of the vast amount of information assembled and to make use of the collection of preserved biologic samples. As yet, such comprehensive summarizations of findings from the AFHS have not materialized, but the current committee is glad to note that the samples are being used in research even though the questions investigated do not necessarily address health outcomes in these Vietnam-era veterans themselves (IOM, 2015).
Major defoliation activities in Vietnam were conducted by Air Force personnel as part of Operation Ranch Hand (ORH). Veterans who took part in the defoliation activities became the first subpopulation of Vietnam veterans to receive special attention with regard to herbicides exposure and have become known as the Ranch Hand cohort within the AFHS. To determine whether exposure to herbicides, including Agent Orange, had adverse health effects, the Air Force made a commitment to Congress and the White House in 1979 to conduct an epidemiologic study of Ranch Hand personnel (AFHS, 1982). The results of biologic-marker studies of Ranch Hand personnel have been consistent with their being exposed, as a group, to TCDD. When the Ranch Hand cohort was classified by military occupation, a general increase in serum TCDD was detected in people whose jobs involved more frequent handling of herbicides (AFHS, 1991b). This provides a strong rationale for close examination of this study cohort.
The exposure index initially proposed in the AFHS relied on military records of spraying of TCDD-containing herbicides (Agent Orange, Agent Purple, Agent Pink, and Agent Green) as reported in the Herbicide Reporting System (HERBS) tapes for the period starting in July 1965 and on military procurement records and dissemination information for the period before July 1965. In 1991 the exposure index was compared with the results of the Ranch Hand serum-TCDD sampling conducted on personnel years after their service in Vietnam. The exposure index and the TCDD body burden correlated weakly.
Michalek et al. (1995) developed several indexes of herbicide exposure of members of the Ranch Hand cohort and tried to relate them to the measurements of serum TCDD from 1987 to 1992. Self-administered questionnaires completed by veterans of ORH were used to develop three indexes of herbicide or TCDD exposure: The number of days of skin exposure, the percentage of skin area exposed, and the product of the number of days of skin exposure, the percentage of skin exposed, and a factor for the concentration of TCDD in the herbicide. A fourth index, which used no information gathered from individual study participants, was calculated by multiplying the volume of herbicide sprayed during a person’s tour of duty by the concentration of TCDD in herbicides sprayed in that period and then dividing the product by the number of crew members in each job specialty at the time.
Each of the four indexes tested was significantly related to serum TCDD although the models explained only 19 to 27 percent of the variability in serum TCDD concentrations. Days of skin exposure had the highest correlation. Military job classification (for example, Ranch Hand combat troops, Ranch Hand administrators, Ranch Hand flight engineers, and Ranch Hand ground crew), which is separate from the four indexes, explained 60 percent of the variability in serum TCDD. When the questionnaire-derived indexes were applied within each job classification, days of skin exposure added statistical significance, but not substantially, to the variability explained by job alone.
As depicted in Figure 6-2, a retrospective matched-cohort study design was used to examine morbidity and mortality; follow-up was scheduled to continue until 2002. Records from the National Personnel Records Center and the US Air Force Human Resources Laboratory were searched and cross-referenced to identify all Ranch Hand personnel (AFHS, 1982; Michalek et al., 1990). A total of 1,269 participants were originally identified (AFHS, 1983). A control population of 24,971 C-130 crew members and support personnel assigned to duty in Southeast Asia (SEA) but not occupationally exposed to herbicides (AFHS, 1983) was selected from the same data sources. Control participants were individually matched for age, type of job (based on Air Force specialty code), and race (white or not white) to control for possible differences in the development of chronic disease that may relate to age, race, or educational and socioeconomic status. To control for the many potential confounders related to the physical and psycho-physiologic effects of combat stress and the SEA environment, Ranch Hands were matched to control participants who performed similar combat or combat-related jobs (AFHS, 1982). Rank also was used as a surrogate of exposure. Alcohol use and smoking were included in the analysis when they were known risk factors for the outcome of interest.
Ten matches formed a control set for each exposed participant. For the mortality study, the intent was to follow each exposed participant and a random sample of half each participant’s control set for 20 years in a 1:5 matched design. The morbidity component of follow-up consisted of a 1:1 matched design; the first control was randomized to the mortality-ascertainment component of the study. If a control was noncompliant, then another control from the matched “pool” was selected; controls who died were not replaced.
The baseline physical examination occurred in 1982, and examinations took place in 1985, 1987, 1992, 1997, and 2002. Morbidity was ascertained through questionnaires and physical examination, which emphasized dermatologic, neurobehavioral, hepatic, immunologic, reproductive, and neoplastic conditions. Some 1,208 Ranch Hands and 1,668 comparison participants were eligible for the baseline examination. Initial questionnaire response rates were 97 percent for the exposed cohort and 93 percent for the nonexposed; baseline physical-examination responses were 87 percent and 76 percent, respectively (Wolfe et al., 1990). Deaths were identified and reviewed by using US Air Force Military Personnel Center records, the VA Beneficiary Identification Record Locator Subsystem (BIRLS), and the Internal Revenue Service database of active Social Security numbers. Death certificates were obtained from the appropriate health departments (Michalek et al., 1990).
Ranch Hands were divided into three categories on the basis of their potential exposure:
- Low potential. Pilots, copilots, and navigators. Exposure was primarily through preflight checks and spraying missions.
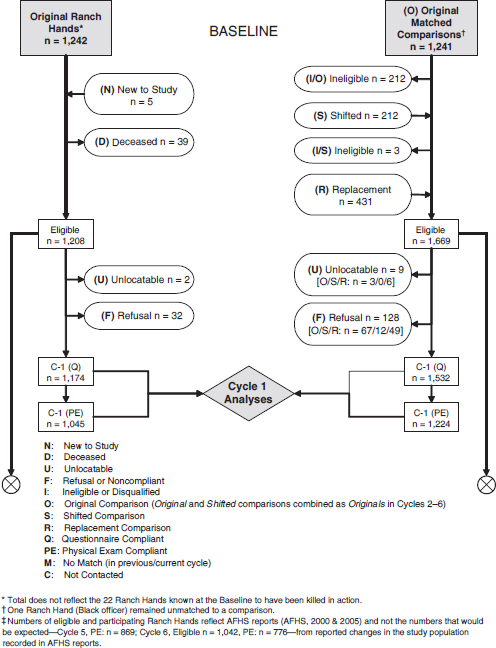
NOTE: Flowchart numbers reflect what was known to Air Force Health Study (AFHS) investigators at any given cycle according to AFHS reports and do not reflect corrections made to earlier cycles due to the identification of misclassified subjects in later cycles. Identical study population counts vary on occasion within and across cycle reports. Thus,
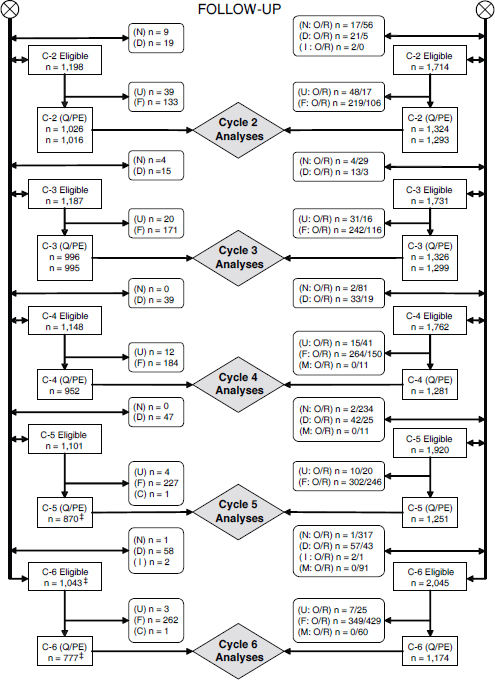
SOURCES: AFHS, 1984a, 1987, 1990, 1995, 2000, 2005c.
- Moderate potential. Crew chiefs, aircraft mechanics, and support personnel. Exposure could occur by contact during de-drumming and aircraft loading operations, onsite repair of aircraft, and repair of spray equipment.
- High potential. Spray-console operators and flight engineers. Exposure could occur during operation of spray equipment and through contact with herbicides in the aircraft.
Ostensibly, the AFHS was designed to answer exactly the question that the VAO project is asking, but the nature of the “exposed” (Ranch Hand veterans) and “comparison” (SEA veterans) groups and the evolving practices of VAO committees in endeavoring to fulfill the intention of their congressional mandate make interpretation less straightforward.
Results have been published for baseline morbidity (AFHS, 1984a), baseline mortality (AFHS, 1983), and for reproductive outcomes (AFHS, 1992; Michalek et al., 1998a; Wolfe et al., 1995). Mortality updates have been published for 1984–1986, 1989, and 1991 (AFHS, 1984b, 1985, 1986, 1989, 1991b). An interim technical report updated cause-specific mortality in Ranch Hands through 1993 (AFHS, 1996). Michalek et al. (1998b) and Ketchum and Michalek (2005) reported on 15-year and 20-year follow-up of post-service mortality, respectively, in veterans of ORH, updating an earlier cause-specific mortality study by Michalek et al. (1990). Comparisons presented in the voluminous reports on the follow-up examinations of 1984, 1987, 1992, 1997, and 2002 cited as AFHS (1987, 1990, 1995, 2000, 2005) have been deemed not useful for the purposes of the VAO reviews because of the prevalence or cross-sectional nature of the data on only those in the cohort who were still alive and participated in a particular examination.
Blood samples for determination of serum TCDD concentrations were drawn at the periodic examinations conducted in 1982 from 36 Ranch Hands (Pirkle et al., 1989), in 1987 from 866 Ranch Hands (AFHS, 1991a), in 1992 from 455 Ranch Hands (AFHS, 1995), and in 1997 from 443 Ranch Hands (AFHS, 2000). For veterans whose TCDD was not measured in 1987 but was measured later, the later measurement was extrapolated to 1987 by using a first-order kinetics model with a constant half-life of 7.6 years. Analyses of the serum TCDD readings were included in the report on the 1987 follow-up examination (AFHS, 1991a), and other Ranch Hand publications have addressed the relationship between serum TCDD and reproductive hormones (Henriksen et al., 1996); diabetes mellitus, glucose, and insulin (Henriksen et al., 1997); skin disorders (Burton et al., 1998); infant death (Michalek et al., 1998a); sex ratios (Michalek et al., 1998c); skin cancers (Ketchum et al., 1999); insulin, fasting glucose, and sex-hormone-binding globulin (Michalek et al., 1999a); immunologic responses (Michalek et al., 1999b); diabetes mellitus (Longnecker and Michalek, 2000; Steenland et al., 2001); cognitive function (Barrett et al., 2001); hepatic abnormalities (Michalek
et al., 2001b); peripheral neuropathy (Michalek et al., 2001c); hematologic results (Michalek et al., 2001a); psychologic functioning (Barrett et al., 2003); correlations between diabetes and TCDD elimination (Michalek et al., 2003); thyroid function (Pavuk et al., 2003); cancer incidence (Akhtar et al., 2004; Pavuk et al., 2005); insulin sensitivity (Kern et al., 2004); prostate cancer (Pavuk et al., 2006); serum testosterone and risk of benign prostate hyperplasia (Gupta et al., 2006a); and diabetes and cancer incidence (Michalek and Pavuk, 2008). All of the VAO updates, Veterans and Agent Orange: Herbicide/Dioxin Exposure and Type 2 Diabetes (IOM, 2000), and Veterans and Agent Orange: Length of Presumptive Period for Association Between Exposure and Respiratory Cancer (IOM, 2004) discussed the reports and papers that address the cohort in more detail.
The tendency of the AFHS researchers to use differing cutpoints and population definitions for analogous analyses suggests that they used a posteriori selection in a fashion that influenced the results. For example, Michalek and Pavuk (2008) allude to the commonly held assumption that Agent Orange was more heavily contaminated earlier in the war as the motivation for making various temporal partitions in their analyses, but the choices were not consistent. For cancers, service in 1968 or before was considered to fall in the critical exposure period, whereas days of spraying were counted through 1967 and the variable for “days of spraying” was assigned the value “low” or “high” by partitioning the resulting distribution at 30 days. For diabetes, however, service in 1969 or before was regarded as being in the critical exposure period, and the variable “days of spraying” was split into “low” and “high” at 90 days or more, with no specification of the period over which the counting was done.
The AFHS is perceived by many to be the central piece of research for decision making by the VAO committees, but it also has important limitations that all VAO committees have had to consider. A prior Institute of Medicine (IOM) report, Disposition of the Air Force Health Study (IOM, 2006b), which was undertaken by another IOM committee as the AFHS was approaching the end of its data-gathering phase, effectively described the limitations of the AFHS and was quoted in extensive detail in Updates 2006 and 2008. In summary, VAO committees have recognized the following features as the primary strengths and limitations of the AFHS:
- The AFHS is one of the most pertinent studies for the VAO reviews, with a study population that was directly exposed to the COIs in the Vietnam War theater.
- It can be argued that the AFHS population is not representative of the entire population of Vietnam veterans, so its findings might not be generalizable to all Vietnam veterans.
- The AFHS might be underpowered for detecting small effects, especially rare outcomes, because of its relatively small sample. Therefore, its
- findings are vulnerable to false negatives (failure to detect an important association). This also raises questions about the stability of positive findings; this is somewhat less of a problem if they are repeated over examination cycles, although the results of the examination cycles themselves are not fully independent repetitions.
- For AFHS analyses that used non-AFHS Vietnam veterans as the comparison group, the comparison group might also have been exposed to the COIs although the exposure was likely to be substantially higher in the AFHS group than in the comparison group. Therefore, the comparison is not an ideal exposed-versus-unexposed comparison but rather a high-exposure-versus-low-exposure comparison. The exposure in the comparison group might also make the study findings vulnerable to false negatives if the exposure differential between the AFHS group and the comparison group was not large enough to allow an association between exposure and outcome to be detected. However, that problem does not affect the validity of positive findings.
Only one new report from the AFHS (Pavuk et al., 2014) was identified in the current literature review. In this report, serum concentrations of dioxin-like compounds (i.e., polychlorinated dibenzo-p-dioxins [PCDDs], polychlorinated dibenzofurans [PCDFs], polychlorinated biphenyls [PCBs]) in addition to TCDD were analyzed from samples collected in 2002 from 777 ORH subjects and 1,173 in the comparison group. In addition, the results were compared with serum samples from 436 age- and gender-matched adults from the National Health and Nutrition Examination Survey (NHANES). The main findings showed that median serum TCDD levels were more than two times higher in the ORH veterans compared to both the Air Force control veterans and the NHANES comparison group. However, the absolute values of serum TCDD levels, as well as the group differences in median serum TCDD levels, were substantially lower than results from prior serum samples collected in 1987. For the other dioxin-like compounds, the concentrations in 2002 were similar in all three groups. These data demonstrate the unique TCDD signature experienced from herbicide exposure in Vietnam and indicate that, over time, the elimination rate is higher than the ongoing intake rate from background exposure to TCDD in both groups of Air Force veterans.
US Department of Veterans Affairs
VA Army Chemical Corps Cohort
The study of members of the US ACC was conducted by VA, whose other research efforts on Vietnam veterans are discussed together below. The ACC study is discussed immediately after the discussion of the AFHS because of the
importance that VAO committees have attributed to it. Like the Ranch Hand personnel, members of the ACC were involved directly in handling and distributing herbicides in Vietnam. Because the ACC personnel were expected to have been highly exposed to herbicides, VAO committees recommended studying this important group of Vietnam veterans (IOM, 1994) and later encouraged the publication of the study’s findings (IOM, 2004). The availability of serum TCDD concentrations in a subset of this cohort of Vietnam veterans has made its findings particularly useful in appraising possible associations with various health outcomes.
ACC troops performed chemical operations on the ground and by helicopter and were thereby involved in the direct handling and distribution of herbicides in Vietnam. The ACC population was belatedly identified for the study of health effects related to herbicide exposure (Thomas and Kang, 1990). In an extension, Dalager and Kang (1997) compared mortality among veterans of the ACC specialties, including Vietnam veterans and non-Vietnam veterans. The results of an initial feasibility study were reported by Kang et al. (2001). The researchers recruited 565 veterans: 284 Vietnam veterans and 281 non-Vietnam veterans as controls. Blood samples were collected in 1996 from 50 Vietnam veterans and 50 control veterans, and 95 of the samples met CDC standards of quality assurance and quality. A comparison of the entire Vietnam cohort with the entire non-Vietnam cohort showed that the geometric mean TCDD concentrations did not differ significantly (p = 0.6). Of the 50 Vietnam veterans sampled, an analysis of the questionnaire responses indicated that those who reported spraying herbicides had higher TCDD concentrations than did those who reported no spraying activities. The authors concluded that Agent Orange exposure was a likely contributor to TCDD concentrations in Vietnam veterans who had a history of spraying herbicides.
Kang et al. (2006) reported the findings of the main study. A health survey of 1,499 Vietnam veterans and 1,428 non-Vietnam veterans was administered by telephone. Exposure to herbicides was assessed by analyzing serum specimens from a sample of 897 veterans for dioxin. Veterans who reported spraying herbicides had significantly higher TCDD serum concentrations than did Vietnam veterans and other veterans who did not report herbicide spraying. The final analysis compared Vietnam-veteran sprayers with Vietnam-veteran nonsprayers in the entire study population.
Having determined the vital status of the ACC personnel through 2005, Cypel and Kang (2010) presented results on mortality from the following causes: cancers (oral and pharyngeal, digestive, respiratory, prostate, testicular, skin, brain, and lymphopoietic [leukemia]), diabetes, circulatory (hypertension and cerebrovascular), respiratory conditions (pneumonia, influenza, and chronic obstructive pulmonary disease), and cirrhosis of the liver. The study compared 2,872 ACC personnel who served in Vietnam with 2,737 ACC personnel who did not serve in
Vietnam, using survival analysis that controlled for race, age at entry into follow-up, rank, and duration of military service. It also compared 662 ACC personnel who served in Vietnam and reported spraying herbicides with 811 who did not serve in Vietnam and did not report spraying, controlling for additional covariates obtained in the telephone survey—body mass index (BMI) and smoking status. Mortality in both cohorts was also compared with the expected mortality in US males. Concerns were raised that the findings in Cypel and Kang (2010) regarding respiratory diseases were not adjusted for smoking status, which was probably an important confounding factor for respiratory diseases, in the analyses based on the entire ACC cohort that compared those who served in Vietnam with those who did not. (The subcohort analyses that compared sprayers with nonsprayers were adjusted for smoking status.)
The primary strengths and limitations of the ACC studies are similar to those of the AFHS. No new ACC studies were reported during the current review period.
VA Female US Vietnam-Veteran Cohort
Although estimates vary, 5,000 to 7,000 US women are believed to have served in Vietnam after volunteering for military service (Thomas et al., 1991). The vast majority of them served as combat nurses—mostly in the Army Nurse Corps—but some also served with the Women’s Army Corps and the Air Force, Navy, and Marine Corps (Spoonster-Schwartz, 1987; Thomas et al., 1991).
In 1986, Public Law (PL) 99-972 was enacted. It required that an epidemiologic study be conducted to examine the long-term adverse health effects on female Vietnam veterans caused by their exposure to traumatic experiences, exposure to such herbicides as Agent Orange or other chemicals or medications, or any similar experience or exposure during such service. The first study that VA conducted to assess mortality in female Vietnam veterans was by Thomas et al. (1991). No comprehensive record of female personnel who served in Vietnam in 1964–1972 existed, so the researchers gathered military service data from each branch of the armed forces to conduct the mortality study through December 31, 1987. Female Army and Navy personnel were identified from morning reports and muster rolls of hospitals and administrative support units where women were likely to have served. Military personnel were identified as female by their names, leaving open the possibility that some women may have been inadvertently excluded from the analysis. Women who served in the Air Force and Marine Corps were identified through military records. The combined roster of all female personnel from the military branches was considered by the researchers to be generally complete. A comparison group consisted of female veterans who were identified through the same process as the female Vietnam veterans but had not served in Vietnam during their military service. Demographic information and information on overseas tours of duty, unit assignments, jobs, and principal duties
were abstracted from military records. Mortality information was obtained from VA’s BIRLS, the Social Security Administration, the Internal Revenue Service, the National Death Index (NDI), and military personnel records. When women whose service in the military fell outside the period of interest, whose records were lacking data, or who served in SEA but not in Vietnam were excluded, the analysis included 132 deaths among 4,582 female Vietnam veterans and 232 deaths among 5,324 comparison veterans who served in the military from July 4, 1965, to March 28, 1973. Cause-specific mortality was derived for Vietnam veterans and comparison veterans and compared with mortality in US women with adjustments for race, age, and calendar period. Dalager et al. (1995a) updated mortality in the original cohort until December 31, 1991, using the same study protocol as Thomas et al. (1991). After updating the mortality figures and adjusting the existing cohort on the basis of new information about the study groups based on the inclusion criteria, 4,586 Vietnam veterans and 5,325 comparison veterans were included in the final analyses (Dalager et al., 1995a).
VA also published studies of pregnancy outcomes and gynecologic cancers—namely, neoplasms of the cervix, uterus, and ovary—in US female Vietnam veterans (Kang et al., 2000a,b). Army veterans were identified from a list obtained by the US Army and Joint Services Environmental Support Group; computerized lists were also provided by the Air Force, Navy, and Marine Corps. Military-service data were abstracted from personnel records. Of 5,230 eligible veterans, 4,390 whose permanent tour of duty included service in Vietnam were alive on January 1, 1992. From a pool of 6,657 potential control participants whose military units did not serve in Vietnam, 4,390 veterans who were alive on January 1, 1992, were randomly selected as controls. After exclusion of 250 veterans and 250 nonveterans who participated in a pilot study, an attempt was made to locate the remaining 4,140 veterans in each group. Various location strategies were used, and fewer than 5 percent (370) were not located; another 339 were deceased. A full telephone interview was conducted on 6,430; 775 refused (13 percent of Vietnam veterans and 17 percent of non-Vietnam veterans), and another 366 completed only a short written questionnaire. A questionnaire was administered on demographic background, general health, lifestyle, menstrual history, pregnancy history, pregnancy outcomes, and military experience, including nursing occupation and combat exposure. Information on pregnancy risks and complications—including smoking, infections, medications, exposure to X-rays, occupational history, and exposure to anesthetic gases, ethylene oxide, herbicides, and pesticides—was collected for each pregnancy. In Kang et al. (2000a), the first pregnancy after the beginning of Vietnam service was designated as the index pregnancy of each woman. For the comparison group, the first pregnancy after July 4, 1965, was used as the index pregnancy of each woman. Odds ratios (ORs) were calculated for the reproductive history and pregnancy outcomes. The study analyzed data on 3,392 Vietnam and 3,038 non-Vietnam veterans and on 1,665 Vietnam and 1,912 non-Vietnam veteran index pregnancies. In Kang et al.
(2000b), a self-reported history of gynecologic cancers (defined by the authors as cancers of the breast, ovary, uterus, and cervix) was collected. The authors attempted to “retrieve hospital records on all reported cancers as far back as 30 years.” Of records successfully found, 99 percent of the breast cancers and 90 percent of all cancers were confirmed. The authors did not provide data on validation of the three sites other than the breast, but they stated that Vietnam status was not associated with verification of outcome.
After the publications by Kang et al. (2000a,b), Congress passed PL 106-419, which provides compensation for children of female Vietnam veterans who are born with birth defects unrelated to an existing familial disorder, to a birth-related injury, or to a fetal or neonatal infirmity with a well-established cause. Eighteen birth defects are covered by the legislation, including cleft lip or palate, congenital heart disease, hypospadias, neural-tube defects, and Williams syndrome. A complete list of covered birth defects can be found in Section 3.815 of the legislation.
Cypel and Kang (2008) conducted a mortality study of female Vietnam veterans and compared their mortality with that in a control group of women who were in military service but did not participate in the Vietnam War. Non-Vietnam veterans were selected randomly from among female veterans who never served in Vietnam and were matched to the Vietnam veterans according to rank and military occupation.
Since Update 2012, Kang and colleagues (2014) have updated total and cause-specific mortality analyses of female US Vietnam-era veterans through December 31, 2010. Vital status was obtained from multiple sources including the VA BIRLS Death File, the Social Security Administration Death Master File, and the National Center for Health Statistics National Death Index (NDI). For deaths that occurred before 1992, the cause of death was ascertained from official death certificates. For deaths occurring on or after January 1, 1992, cause of death information was obtained from NDI Plus, which provides cause of death codes by the International Classification of Diseases (ICD) system. Underlying causes of death were formally assigned by a qualified nosologist.
This retrospective cohort study consisted of three study groups of female Veterans who served during the Vietnam era when combat operations occurred (July 4, 1965, through March 28, 1973). This included 4,734 female veterans who served in Vietnam, 2,062 female veterans who served near Vietnam, and a non-deployed US cohort of 5,313 female veterans. Mortality comparisons were made with the non-deployed US cohort as well as with the US general population (women) adjusted for age, race, and calendar year. Of the total sample of 12,109 female veterans, 2,743 (23 percent) were deceased by the study end date of December 31, 2010. Importantly, the cause of death information was available for 96.2 percent of the total cohort.
Cause-specific mortality results are presented in the individual chapters addressing specific disease outcomes. However, to summarize, the adjusted total
mortality rate was statistically lower in the female Vietnam veterans group than in the US cohort of female veterans as well as in the US general population. Similar results were reported for heart disease mortality, with the Vietnam veterans group having a lower rate, whereas rates of cancer mortality were approximately equal between the female Vietnam veterans group and both the US cohort of female veterans and the US general population. However, among nurses only (approximately two-thirds of the study cohort), higher adjusted mortality rates for pancreatic and brain and other nervous system cancers were reported for the female Vietnam veterans group. Whereas all reports from the female US Vietnam-veterans cohort provide direct information on the health and mortality status of female military personnel who served in Vietnam, results must be taken in the context of limitations. Specifically, female veterans likely experienced low herbicide exposure because they were not involved in applying herbicides or engaged in direct combat, and had in-country tours of duty that were generally 1 year in length and at fixed locations that were away from known defoliated areas. In summary, this analysis does not provide evidence in support of female Vietnam veterans being at higher risk of total and cause-specific mortality compared with non-Vietnam female veterans and the US general population. The suggestion of higher rates of mortality from pancreatic and brain and other nervous system cancers among nurse Vietnam veterans should be cautiously interpreted given the study’s limitations and the large number of causes of mortality examined.
VA Proportionate-Mortality Cohort
Among the earliest reports on Vietnam veterans was a proportionate-mortality study by Breslin et al. (1988). The participants were men who had served as ground troops in the US Army or Marine Corps at any time from July 4, 1965, through March 1, 1973. A list of 186,000 Vietnam-era veterans who served in the Army or Marine Corps and were reported deceased as of July 1, 1982, was assembled from VA’s BIRLS; of these, 75,617 names were randomly selected from the list for inclusion in the study. The information extracted from the selected military records included the places, dates, and branch of military service; date of birth; sex; race; military occupation specialty codes; education level; type of discharge; and confirmation of service in Vietnam. Additional information was extracted on veterans who served in SEA, including the first and last dates of service in SEA, the military unit, and the country where the veteran served. For the final sample of 52,253 Army and Marine Corps veterans, the cause of death was ascertained from death certificates or Department of Defense Report of Casualty forms for 51,421 men, including 24,235 who served in Vietnam and 26,685 men who did not serve in SEA; 501 deaths were excluded from the final analyses because service in SEA was in a country other than Vietnam or the location of military service was unknown. Each veteran’s cause of death was coded by a nosologist who used the 8th revision of the International Classification of Diseases.
On the basis of the proportionate-mortality study (Breslin et al., 1988), Burt et al. (1987) conducted a nested case-control study of non-Hodgkin lymphomas (NHLs) with controls selected from among the cardiovascular-disease deaths. In a follow-up of the Breslin et al. study, Bullman et al. (1990) compared cause-specific proportionate mortality in 6,668 Army I Corps Vietnam veterans—veterans who served in the northernmost part of South Vietnam in a combat zone designated as Military Region I by the US military—with that in 27,917 Army Vietnam-era veterans who had not served in Vietnam. The subjects studied by Bullman et al. included the study population identified by Breslin et al. and an additional 9,555 Army Vietnam-era veterans whose deaths were identified after the BIRLS mortality data were extended through December 31, 1984. Similarly, Watanabe et al. (1991) updated the Vietnam-veteran mortality experience reported by Breslin et al. (1988) by extending the follow-up from January 1, 1982, to December 31, 1984. An additional 11,325 deceased Army and Marine Vietnam-era veterans were identified from the period and included in the study. The study population for Watanabe et al. consisted of 62,068 military veterans, of whom 29,646 served in Vietnam and 32,422 never served in SEA. Proportionate-mortality ratios were calculated for three referent groups: branch-specific (Army and Marine Corps) non-Vietnam veterans, all non-Vietnam veterans combined, and the US male population. A third follow-up proportionate-mortality study (Watanabe and Kang, 1996) used the veterans from Breslin et al. (1988) and Watanabe et al. (1991) and included an additional 9,040 randomly selected Vietnam-era veterans who died from July 1, 1984, through June 30, 1988. The final study included 70,630 veterans—33,833 who had served in Vietnam and 36,797 who never served in SEA—and the analyses were performed with the same referent groups described previously (Watanabe et al., 1991).
Other VA Studies
VA also conducted studies that focused on specific health outcomes, using data from VA’s Agent Orange Registry (AO Registry), a computer database containing health information on Vietnam veterans who voluntarily undergo examinations in a VA hospital. The AO Registry was set up in 1978 to monitor those health complaints or problems of Vietnam veterans that could be related to herbicide exposure during their military service in Vietnam. The examinations consist of an exposure history, a medical history, laboratory tests, and an examination of the body systems most commonly affected by toxic chemicals. As of September 30, 2012, the AO Registry contained information on 573,088 initial examinations (an increase of 119,019 since 2008) and 65,758 follow-up evaluations, for a total of 638,846 examinations (VA, 2012). Updated statistics on the AO Registry were not reported in the next issue of VA’s Agent Orange Newsletter (VA, 2015).
Using early data from the AO Registry, Bullman et al. (1991) examined the risk of posttraumatic stress disorder (PTSD) in a case-control study of veterans
who had received medical examinations from January 1983 through December 1987. The final analyses included 374 PTSD cases and 373 controls whose military records were used to verify Vietnam service, Military Occupational Specialty Codes (MOSCs), primary duties, military branch, dates of Vietnam service, medals, awards, and disciplinary actions for each veteran. Of note, as described in Chapter 2, PTSD and other mental health conditions were not formally evaluated by more recent VAO committees. Similarly, Bullman et al. (1994) studied the risk of testicular cancer by using the AO Registry health records of veterans who received medical examinations from March 1982 through January 1991. The final analyses in that study included 97 testicular-cancer cases and 311 controls. A surrogate metric for herbicide exposure was developed by using the branch of service, combat MOSCs, geographic area of service in Vietnam, location of military units in relation to herbicide-spraying missions, and the length of time between spray missions and military operations in sprayed areas.
Watanabe and Kang (1995) compared postservice mortality in Vietnam veterans in the Marine Corps with that in Vietnam-era marines who did not serve in Vietnam. All of the study participants were on active duty during 1967–1969 and were followed from their discharge date or from the date of the US military withdrawal from Vietnam until their date of death or December 31, 1991, whichever came first. The final study population included 10,716 Vietnam and 9,346 non-Vietnam veteran marines.
Kang et al. (1991) conducted a case-control study that compared dioxin and dibenzofuran concentrations in the adipose tissue of 36 Vietnam veterans with those in 79 non-Vietnam veterans and a sample of US men born in 1936–1954. All tissue samples were archived specimens from the US Environmental Protection Agency National Human Adipose Tissue Survey and had been collected by hospitals and medical examiners from men who died from external causes or surgical procedures. Military service—branch of service, MOSC, and geographic service location in Vietnam, if applicable—was researched and verified with military records. Controls were matched by birth year and sample collection year (± 2 years), and the final analyses were adjusted by age and BMI.
Dalager et al. (1991) examined NHL in male Vietnam veterans in a hospital-based case-control study. Study participants were identified via inpatient discharge records from VA medical centers for the fiscal years 1969–1985. The cases were veterans identified as having a malignant lymphoma and a birth date from 1937 through 1954. The controls were veterans identified from VA medical-center discharge records and were matched by hospital, discharge date, and birth date. The locations and dates of each veteran’s military service were verified by using military records. A surrogate herbicide exposure opportunity was also developed for each Vietnam veteran according to the veteran’s branch of service, combat experience, and the geographic location of the military unit assignment. The final analysis included 201 cases and 358 controls. Another study by Dalager et al. (1995b) examined the association between Hodgkin lymphoma (HL) and
Vietnam service. It used the same method as the 1991 Dalager et al. study; the analysis included 283 HL cases and 404 controls.
VA has evaluated specific health outcomes, including case-control studies of soft-tissue sarcomas (STSs) (Kang et al., 1986, 1987), testicular cancer (Bullman et al., 1994), and lung cancer (Mahan et al., 1997). It also has conducted a study of self-reported physical health (Eisen et al., 1991) and PTSD (Goldberg et al., 1990) in monozygotic twins who served during the Vietnam era.
VA has examined other outcomes in Vietnam veterans: PTSD (Bullman et al., 1991; True et al., 1988), suicide and motor-vehicle crashes (Bullman and Kang, 1996; Farberow et al., 1990), and tobacco use (McKinney et al., 1997). The studies have been included for completeness, but the outcomes that they address are outside the purview of this committee. VAO and Update 1998 discuss them in detail; most did not deal with exposure to herbicides specifically, and the exposure to “combat” was evaluated as the risk factor of interest.
US Centers for Disease Control and Prevention Studies
Surveys of US Vietnam veterans who were not part of the Ranch Hand or ACC groups indicated that 25 to 55 percent believed that they were exposed to herbicides (CDC, 1989b; Erickson et al., 1984a,b; Stellman and Stellman, 1986). Several attempts have been made to estimate the exposures of Vietnam veterans who were not part of the Ranch Hand or ACC groups. CDC has undertaken a series of studies to examine various health outcomes in Vietnam veterans as directed by Congress in the Veterans Health Programs Extension and Improvement Act of 1979 (PL 96-151) and the Veterans’ Health Care, Training, and Small Business Loan Act of 1981 (PL 97-72).
CDC Birth-Defects Study
The first of these CDC studies was a case-control interview study of birth defects in the offspring of men who served in Vietnam (Erickson et al., 1984a,b). In 1983 the US government asked CDC to conduct a study of possible long-term health effects in Vietnam veterans exposed to herbicides. The CDC Agent Orange study (CDC, 1985) attempted to classify veterans’ service-related exposures to herbicides. This involved determining the proximity of troops to herbicide spraying by using military records to track troop movement and using the HERBS tapes to locate herbicide-spraying patterns. The CDC birth-defects study developed an exposure-opportunity index to score herbicide exposure (Erickson et al., 1984a,b).
CDC Agent Orange Validation Study
In 1987, CDC conducted the CDC Agent Orange Validation Study (AOVS) to test the validity of the various indirect methods used to estimate the exposure
of ground troops to herbicides in Vietnam. The study measured serum TCDD in a nonrandom sample of Vietnam veterans and in Vietnam-era veterans who did not serve in Vietnam (CDC, 1988a). Vietnam veterans were selected for the study on the basis of the number of herbicide hits that they were thought to have experienced, given the number of days on which their company was within 2 km and 6 days of a recorded herbicide-spraying event. Blood samples were obtained from 66 percent of 646 Vietnam veterans and from 49 percent of the eligible comparison group of 97 veterans. More than 94 percent of those whose serum was obtained had served in one of five battalions.
The median serum TCDD in Vietnam veterans in 1987 was 4 parts per trillion (ppt) (range, under 1 to 45 ppt). Only two veterans had concentrations above 20 ppt. The “low” exposure group consisted of 298 Vietnam veterans, the “medium” exposure group 157 veterans, and the “high” exposure group 191 veterans. The distribution of TCDD measurements was nearly identical with that in the control group of 97 non-Vietnam veterans. The CDC validation study concluded that study participants could not be distinguished from controls on the basis of serum TCDD. In addition, neither record-derived estimates of exposure nor self-reported exposure to herbicides could predict Vietnam veterans with currently high serum TCDD (CDC, 1988b, 1989b). The report concluded that it was unlikely that military records alone could be used to identify a large number of veterans who might have been heavily exposed to TCDD in Vietnam.
CDC Vietnam Experience Study
Using exposure estimates from the AOVS, CDC conducted the CDC Vietnam Experience Study (VES), a historical cohort study of the health experience of Vietnam veterans (CDC, 1989a). The study was divided into three parts: physical health, reproductive outcomes and child health, and psychosocial characteristics (CDC, 1987, 1988a,c,d, 1989a). Using VES data, CDC examined postservice mortality (through 1983) in a cohort of 9,324 US Army veterans who served in Vietnam and in 8,989 Vietnam-era Army veterans who served in Germany, Korea, or the United States (Boyle et al., 1987; CDC, 1987). Another study (O’Brien et al., 1991) combined the mortality and interview data to identify all veterans who had NHL. To evaluate whether self-reported assessment of exposure to herbicides influences the reporting of adverse health outcomes, CDC designed a study of VES participants (Decoufle et al., 1992). In a follow-up of CDC’s VES cohort, Boehmer et al. (2004) reported findings on mortality from 1965 through 2000.
The serum TCDD measurements in Vietnam veterans also suggested that the exposure to TCDD in Vietnam was substantially lower, on average, than that of persons exposed as a result of the industrial explosion in Seveso or that of the heavily exposed occupational workers who have been the focus of many of the studies evaluated by the present committee. The assessment of average
exposure does not preclude subgroups of Vietnam veterans from having had heavy exposures.
CDC Selected Cancers Study
CDC undertook the CDC Selected Cancers Study (CDC, 1990a) to investigate the effects of military service in Vietnam and of exposure to herbicides on the health of American veterans, specifically the risk of developing NHL (CDC, 1990b), STS and other sarcomas (CDC, 1990c), HL (CDC, 1990d), and nasal, nasopharyngeal, and primary liver cancers (CDC, 1990d).
CDC National Vietnam Veterans Readjustment and Longitudinal Studies
The CDC National Vietnam Veterans Readjustment Study investigated primarily psychological outcomes. It is now being updated to become the National Vietnam Veterans Longitudinal Study (NVVLS). The literature search for Update 2014 identified an additional peer-reviewed article based on data gathered during the original study (Currier and Holland, 2012), which addressed psychologic outcomes in association with combat trauma and bereavement. To date (9 months after the cut-off date for this update), the only publications arising from the new NVVLS effort have been a press release (Abt Associates, 2014) associated with a conference presentation, a non-peer-reviewed article prepared by the VA contractors for the newsletter of the Vietnam Veterans of America (Schlenger and Corry, 2015), and an article addressing the protocols and methods used in NVVLS (Schlenger et al., 2015).
Other US Vietnam-Veteran Studies
Ansbaugh et al. (2013) conducted a historical cohort analysis of 2,720 veterans who were referred to the Portland Veterans Affairs Medical Center and underwent an initial prostate biopsy. Prior exposure to herbicides was crudely classified as “yes” or “no” within the electronic medical record system in a variable called “AO exposure” and yielded an overall prevalence of 7.5 percent. In a multiple logistic regression analysis, herbicide exposure (compared to no exposure) was associated with an estimated 1.52 higher odds of prostate cancer (all subtypes), including OR estimates of 1.24 for low-grade prostate cancer, 1.75 for high-grade prostate cancer, and 2.10 for the detection of prostate cancer with Gleason scores of 8 or higher. The reliability of the medical record variable classified as “yes” or “no” is unknown in this cohort and is considered to be a methodological concern by the committee.
Clemens et al. (2014) reviewed the clinical characteristics of 100 consecutive male patients with Fitzpatrick skin types I though IV who enrolled in the AO Registry at the Veterans Affairs Hospital of Washington, DC, between August 2009
and January 2010. Because by design all participants were selected on the basis of presumably having been exposed to herbicides and having been diagnosed with non-melanotic invasive skin cancers, the committee deemed this analysis of no value with respect to examining the relationships between the COIs.
Qureshi et al. (2013) reanalyzed cases of veterans diagnosed with Barrett’s esophagus and veteran controls who have been previously assembled at the VA Medical Center in Houston, Texas, for the role of occupational pesticide exposure as a risk factor. The committee deemed this study to be of no value to its charge because it neither distinguished the types of pesticides examined nor considered the subjects’ deployment status or exposure to military herbicides as potential risk factors.
In a published abstract by Srinivas et al. (2012), demographic, clinical, and pathology data were compared between Vietnam-era and non-Vietnam-era veterans with NHL. Beyond the inadequately detailed information presented and its lack of peer review, the committee deemed this study of no value to its charge because it was unrelated to the development of NHL in relation to service in Vietnam.
American Legion Study
The American Legion, a voluntary service organization for veterans, conducted a cohort study of the health and well-being of Vietnam veterans who were members. Studies examined physical health and reproductive outcomes, social–behavioral consequences, and PTSD in veterans who had served in SEA and elsewhere (Snow et al., 1988; Stellman JM et al., 1988; Stellman SD et al., 1988b). No additional studies have been published on the cohort.
State Studies
Several states have conducted studies of Vietnam veterans, most of which have not been published in the scientific literature. VAO and Update 1996 reviewed studies of veterans of Hawaii (Rellahan, 1985), Iowa (Wendt, 1985), Maine (Deprez et al., 1991), Massachusetts (Clapp, 1997; Clapp et al., 1991; Kogan and Clapp, 1985, 1988; Levy, 1988), Michigan (Visintainer et al., 1995), New Jersey (Fiedler and Gochfeld, 1992; Kahn et al., 1988, 1992a,b,c), New Mexico (Pollei et al., 1986), New York (Greenwald et al., 1984; Lawrence et al., 1985), Pennsylvania (Goun and Kuller, 1986), Texas (Newell, 1984), West Virginia (Holmes et al., 1986), and Wisconsin (Anderson et al., 1986a,b). Chamie et al. (2008) examined the association between herbicide exposure and prostate cancer in all Vietnam-era veterans using the VA health system in northern California; the reliability of this study of about 13,000 men is limited by its reliance on self-reported exposure status and by the exclusion of prostate cases diagnosed
before 1998, when computerized records became available. No additional state studies have been published.
Additional studies have examined health outcomes that included spontaneous abortion (Aschengrau and Monson, 1989) and adverse outcomes late in pregnancy in spouses of Vietnam veterans (Aschengrau and Monson, 1990). After a published study indicated a potential association between testicular cancer in dogs and their service in Vietnam (Hayes et al., 1990), Tarone et al. (1991) conducted a case-control study of testicular cancer in male veterans. VAO summarized those studies, and no additional studies have been published on these study populations.
Australian Vietnam-Veteran Studies
Over many years the Australian government has commissioned studies to follow health outcomes in two sets of Australian veterans who served in Vietnam.
Australian Vietnam Veterans
The Australian Vietnam-veterans study population corresponds to the cohort defined by the “Nominal Roll of Vietnam Veterans,” which lists Australians who served on land or in Vietnamese waters from May 23, 1962, to July 1, 1973, including military and some nonmilitary personnel of both sexes. People who served in any branch of service in the defense forces and citizen military forces (such as diplomatic, medical, and entertainment personnel) were considered. The comprehensive studies, however, are limited to male members of the military, and most of the analyses focus on men in the defense forces—the Army (41,084), the Navy (13,538), and the Air Force (4,570). An investigation looked into the possibility of an association between Vietnam service and cancer incidence (ADVA, 2005a) by comparing diagnoses from 1982 to 2000 among male Vietnam veterans with those in the general population of Australia. The results in this report supersede those in the report of the Australian Department of Veterans’ Affairs (CDVA 1998a). Morbidity in all female Vietnam veterans had been studied in an earlier report (CDVA, 1998b). Additional case-control studies of the incidence of adrenal gland cancers, leukemias, and NHL were conducted in this population (AIHW, 1999, 2000, 2001).
A related report (ADVA, 2005b) considered the causes of death of men in all branches of service through 2001. The numbers of deaths were 4,045 in the Army, 1,435 in the Navy, and 686 in the Air Force. The mortality experience of military personnel serving in Vietnam was compared with that of the general population of Australia and reported by branch of service. The findings of this study supersede those in the report on mortality from 1980 to 1994 (CDVA, 1997a). There had been several earlier studies of mortality among Australian Vietnam veterans
(CIH, 1984a,b,c; Crane et al., 1997a,b; Evatt, 1985; Fett et al., 1987a,b; Forcier et al., 1987).
Australian Vietnam Veterans Family Study (VVFS)
Since Update 2012, the Australian Department of Veterans’ Affairs has published four large volumes that summarize the results of studies conducted among family members of Vietnam-era veterans (ADVA, 2014a,b,c,d). The first volume (2014a) provided an overview of the entire effort, which consisted of several studies of the veterans’ family members. The second (ADVA, 2012b) assessed the health of the family members with more emphasis placed on the details of psychological and social wellbeing, rather than adverse impacts on physical health. The third (ADVA, 2014c) investigated mortality among members of the veterans’ families, while the final volume (ADVA, 2014d) discussed qualitative information gathered in the course of the entire study. Although responses were collected on spouses and partners of the veterans, the analyses focused upon outcomes reported by the children of the veterans. The wide range of outcomes examined for the family members themselves included mental health outcomes, pregnancy and birth defect outcomes, physical health, social functioning, and mortality. The purpose of this study was to better understand the long-term impacts of service on the health and welfare of the families of Australian Vietnam veterans.
From the roster of Australian Vietnam veterans, more than 10,000 Australians who had served in the Vietnam War were randomly selected and contacted, along with their family members, for potential participation in the study. The Vietnam veterans who were identified and ultimately selected included 3,940 who were randomly selected and 2,569 who self-selected into the study based on media publications announcing that the study would be conducted.
The primary comparison group consisted of family members of non-deployed Vietnam-era personnel, meaning family members of Australian veterans who served from 1962 through 1975, but were not deployed to Vietnam. This included the identification and selection of 3,967 randomly selected veterans and 418 who self-selected in the study. Thus, there were far more Australian Vietnam veterans than Australian Vietnam-era veterans who self-selected into the study, and the percentage of the Vietnam veterans who self-selected was much higher than the percentage of Vietnam-era veterans who self-selected. In total, the family members of Vietnam veterans included 2,199 sons and daughters, of which 1,385 were investigated for pregnancy and birth defect–related outcomes.
The VAO series has considered comparisons of deployed and non-deployed groups to cover potential exposure to all the COIs, and thus the most relevant measures for their task (in the absence of specific exposure information). Such constrasts, however, also cover all aspects of the deployment experience, and in this set of Australian studies there was considerably more concern about psychological effects on the veterans (especially PTSD) and their secondary impact on
the veterans’ family members, which would not be expected to be an effect of herbicide exposure.
The VVFS has conducted some analyses among all study participants, as well as some analyses stratified by type of enrollment (random versus self-selected). The committee fully recognized potential reporting biases that may have emanated from the self-selected cohort, and thus it placed considerably more weight on results derived for the randomly selected cohort, as did the researchers themselves.
Australian Conscripted Army National Service
The Australian Conscripted Army National Service study population is a subset of the veterans considered in the overall Australian Vietnam Veterans study group. The 19,240 conscripted male Army veterans deployed to Vietnam (“National Service” veterans) were compared with 24,729 non-deployed counterparts (“National Service non-veterans”). This comparison between contemporaries who had been sufficiently healthy to enter the service provided a means of adjusting for a possible “healthy-warrior” effect. The results on death and cancers in the Australian conscripted Army National Service veterans (ADVA, 2005c) supersede those of earlier internal comparisons of deployed and non-deployed Vietnam War–era National Service veterans (CIH, 1984a; Crane et al., 1997b; Fett et al., 1987a,b). Those government-sponsored studies of Australian Vietnam veterans did not characterize the veterans’ exposure to the herbicides sprayed in Vietnam beyond the fact that they had served on land or in Vietnamese waters from May 23, 1962, through July 1, 1973. It is the convention of VAO committees to regard Vietnam veterans in general as being more likely to have received higher exposures to the COIs than the general public, but it would have been informative to validate that assumption by gathering biomarkers of exposure, such as serum measurements, in a sample of Australian Vietnam veterans.
Update 2000 had moved the occurrence of acute myeloid leukemia in offspring of Vietnam veterans into the limited or suggestive category of association primarily on the basis of findings reported by the Australian Institute of Health and Welfare (AIHW, 2000) but rescinded in a revised report (AIHW, 2001). The reversal of the conclusion on this matter by the committee for Update 2000 is discussed in Veterans and Agent Orange: Herbicide/Dioxin Exposure and Acute Myelogenous Leukemia in the Children of Vietnam Veterans (IOM, 2002).
Sample of 1,000 Australian Vietnam Veterans
O’Toole et al. (1996a,b,c) studied a broad spectrum of health issues in a random sample of 1,000 Australian Vietnam veterans (both regular enlisted and conscripted Army National Service members) selected from Australia’s comprehensive roster of 57,643 service members deployed to Vietnam. In wave 1,
conducted in 1990–1993, 641 members of the sample were located and interviewed. In wave 2, conducted in 2005–2006, O’Toole et al. (2009) obtained responses from 450 (51.4 percent of those not known to have died); 391 responded to both waves. The Australian Bureau of Statistics’ National Health Survey was administered in both waves with the collection of additional data on combat experience, PTSD, and general psychiatric status. The veterans’ self-reported health status was compared with that of the general male Australian population gathered during the government’s administration of the same survey in 1989–1990 and 2004–2005; it is not clear that this instrument was administered to the two groups under comparable conditions. The low response rates make the findings vulnerable to nonresponse bias and the use of self-report measures of health conditions might be of low validity and subject to recall bias. The committee for Update 2010 was skeptical about the reliability of the nearly uniform findings of statistically increased prevalence of nearly 50 health conditions. O’Toole et al. (2010) reported on the mortality in the sample through 2004 as related to previously gathered information on psychosocial factors that are not within the scope of VAO reviews. It is of interest, however, that they found that 11.7 percent of the veterans in the sample had died by the end of 2004.
Case-Control Study of Birth Defects in Australian Infants
The Australian government sponsored a case-control study of 8,517 infants with congenital anomalies born in 1966–1979 at 34 hospitals in New South Wales, Victoria, and in the Australian Capital Territory matched by period of birth, mother’s age, hospital, and means of hospital payment to live-born infants without diagnosed birth defects (Donovan et al., 1983, 1984; Evatt, 1985). The fathers of both groups were identified and their names compared to the roster of men who had served in the Australian Army in 1962–1972; additional means of verification were used to determine whether the child’s father was in the Army during this interval (329 cases and 338 controls) and also whether he was deployed to Vietnam (127 cases and 123 controls). After adjustments were made for maternal age, infant sex, multiple births, and father’s place of birth, conditional logistic regression was used to compare the Vietnam veterans (National Service or regular Army) to other era veterans and to all other fathers for all birth anomalies and for seven diagnostic groups.
Korean Vietnam-Veteran Studies
Study of TCDD Concentrations in Korean Vietnam Veterans
Military personnel of the Republic of Korea served in Vietnam from 1964 through 1973. Kim et al. (2001) attempted to use serum dioxin concentrations to validate an index for estimating group exposure. The study involved 720 veterans
who served in Vietnam and 25 veterans who did not. The exposure index was based on herbicide-spraying patterns in military regions in which Korean personnel served, time–location data on the military units stationed in Vietnam, and an exposure score derived from self-reported activities during service. A total of 13 pooled samples were submitted to CDC for serum dioxin analyses. One analytic sample was prepared from the pooled blood of the 25 veterans who did not serve in Vietnam. The remaining 12 samples were intended to correspond to 12 exposure categories; each was created by pooling blood samples from 60 veterans. The 12 exposure categories ultimately were reduced to four exposure groups, each representing a quartile of 180 Vietnam veterans but characterized by only three serum TCDD measurements.
The paper by Kim et al. (2001) reported highly significant Pearson correlation coefficients and results of multiple logistic-regression analysis. The statistical analyses apparently were based on the assignment of the pooled serum dioxin value to each person in the exposure group and thereby inflated the true sample size. The multiple regression analysis evaluated such variables as age, BMI, and consumption of tobacco or alcohol. In a later report on the same exposure groups and serum dioxin data, the authors corrected their analysis (Kim JS et al., 2003). A correlation was observed between serum dioxin concentrations and ordinal exposure categories, but the correlation was not statistically significant. The authors attributed the lack of statistical significance to the small sample size, and they noted that the data exhibited a distinct monotonic upward trend; the average serum dioxin concentrations were 0.3, 0.6, 0.62, 0.78, and 0.87 picograms per gram (pg/g) (lipid-adjusted) for, respectively, exposure categories 0 through 4. The decision to pool blood samples from a large number of persons in each exposure set (Kim et al., 2001) greatly reduced the power of the validation study. Instead of 180 samples in each of the final exposure categories, the pooled analysis produced only three samples in each category. The lipid-adjusted serum TCDD concentrations in the 12 pooled samples from Vietnam veterans ranged from 0.25 to 1.2 pg/g, whereas the single sample from the non-Vietnam veterans contained 0.3 pg/g. The narrow range of results makes the biologic relevance of any differences questionable.
Thus, it appears that there was not a clear separation between Korean Vietnam veterans and non-Vietnam veterans. Furthermore, the range of mean values in the four Vietnam-veteran exposure categories was narrow, and all concentrations were relatively low (less than 1 pg/g). The relatively low serum dioxin concentrations observed in the 1990s in those people are the residual of substantially higher initial concentrations, as has been seen in other Vietnam-veteran groups. However, the concentrations reported in the Korean-veterans study are significantly lower than those reported in American Vietnam veterans in the 1988 CDC AOVS, which was nonetheless unable to distinguish Vietnam veterans from non-Vietnam veterans on the basis of serum dioxin (CDC, 1988b). The Korean authors were able to construct plausible exposure categories based on military
records and self-reporting, but they were unable to validate the categories with serum dioxin measurements.
Study of Role of Vietnam Service in Recovery of
Koreans with Acute Coronary Syndrome
JB Kim et al. (2012) reported on the association between exposure to TCDD and recovery outcomes (hypertension, hyperlipidemia, and the rate and severity of major adverse coronary events) in men who presented with acute coronary syndrome (obstruction of coronary arteries and chest pain) from 2004 through 2009 at Gwangju Veterans Hospital. The age range was limited to 50–70 years to reflect the current age of Korean veterans of the Vietnam War. There were 251 patients: 121 were Vietnam veterans (assumed to have been exposed to TCDD), and 130 were not. Medical records were reviewed to determine a variety of cardiovascular recovery outcomes. T-tests, chi-square tests, and logistic regression were used to determine whether measures of recovery differed between the acute coronary patients who had served in Vietnam and those who did not. The study findings are not informative about associations between TCDD and acute coronary syndrome itself, as the researchers allege.
Korean (Vietnam) Veterans Health Study
The committee identified six publications from an exceptionally large epidemiological study of more than 180,000 Korean Vietnam veterans that have appeared since Update 2012. This study cohort, denoted herein as the “Korean study,” is much larger in scope than all of the other published epidemiological studies conducted among Vietnam veterans. The Korean study provides results for a very large set of health outcomes, including rare conditions, as well as information on both non-fatal outcomes and cause-specific mortality. Consequently, the synthesis of results from the Korean study by the committee members had the potential to substantially influence (i.e., update) conclusions drawn from previous updates.
The research methodology employed in the Korean study was very carefully evaluated by the committee. This was done so that across all health outcomes, committee members would weigh the results from the Korean study in a consistent manner and appropriately take into account the respective strengths and limitations from this large body of data.
For the Assessment of the Potential Exposure to Herbicides For the assessment (referred to imprecisely in the Yi articles as Agent Orange), multiple methods were employed by the Korean study investigators. Responses to six questions on a postal survey were used to derive a four-tiered categorization of self-perceived herbicide exposure (Yi et al., 2013a). The initial four-tier scale
(high, moderate, low, and none) was further compressed into simply “high” or “low” for many analyses (see Table 3-2 in Chapter 3 for the quantitative distributions). An objective index of potential herbicide exposure was calculated for each veteran based on the proximity of their military unit to herbicide-sprayed areas. The model, developed by Stellman et al. (2003b), included herbicide exposure opportunity scores, which accounted for location histories of military units and calendar dates in which spraying occurred. The Korean study investigators classified these quantitative exposure data using two-group and four-group categorizations, the details of which are presented in Tables 3-3 and 3-4 in Chapter 3.
For the Assessment of the Health Outcomes of Interest There were multiple methods used. First, veterans were asked to indicate (self-report) all current and physician-diagnosed diseases. The diseases were classified into seven groups of diseases; cancers, circulatory diseases, respiratory diseases, digestive diseases, neuromuscular diseases, endocrine diseases, and other diseases. Within the major disease groups, self-reporting was further provided for 17 cancers (including stomach cancer, liver cancer, and lung cancer), 13 circulatory diseases (including hypertension, myocardial infarction, and angina), five respiratory diseases (including chronic bronchitis and emphysema), six digestive diseases (including central nervous system disorders and peripheral neuropathy), three endocrine diseases (including diabetes and hypothyroidism), and four other diseases (including renal failure and skin disease).
Second, incidence data of individual types of cancer experienced by Korean Vietnam veterans were obtained from the Korean Cancer Incidence Database (1992–2003) and classified by use of ICD, tenth revision (ICD-10).
Third, prevalent cases of individual disease conditions were identified by extraction of claims data from the Korea National Health Insurance system during the period January 1, 2000, to September 30, 2005, along with medical care covered directly by the Korean government through the Veterans Health Service during the same period. Health outcomes examined included the prevalence of endocrine diseases (E00–E90), neurologic diseases (G00–G99), circulatory diseases (I00–I99), respiratory diseases (J00–J99), and digestive diseases (K00–K93).
Fourth, deaths of Korean Vietnam veterans and the underlying causes of their deaths were ascertained by use of the 1992–2005 death records of the National Statistical Office. Causes of death were classified according to the ICD-10. This included all-causes of death, 15 chapter diseases, 23 specific cancers, and 36 specific causes of death other than cancer.
Using these multiple methods for exposure classification and health outcome ascertainment, associations between metrics of herbicide exposure potential and health outcomes were derived. First, in some analyses, the health experiences of Korean Vietnam veterans, given their exposure status, was compared to the health status of age-matched adults in the Korean general population. This method is known as an
“external” control group. Second, some analyses were performed among Korean Vietnam veterans with the lowest herbicide exposure classification serving as the comparison group. This method is known as an “internal” control group.
The above variations in exposure assessment, health outcome ascertainment, and source of comparator (reference) group have significant implications for the appropriate interpretation of results from the Korean study. In considering these variations, the committee noted the following methodological principles and empirical observations:
- Whereas self-reported exposure may be reliable and valid in some research circumstances, it is generally considered less reliable and valid than objectively obtained estimates of exposure (Zajacova and Dowd, 2011). The potential for recall bias is of particular concern and the likelihood of it occurring increases with the length of time from potential exposure to the incidence of disease.
- For ascertaining health outcome data, objective sources (e.g., a cancer registry or health claims system) are generally preferred over self-report outcome data, assuming that the objective source of outcome data is largely comprehensive.
- For mortality analyses, the estimation of relative risk (and the corresponding confidence interval) may be more prone to bias when an external control group is used (e.g., general population) than when an internal control group is used (Monson, 1990). This may be due to the “healthy soldier” effect. That is, service members upon entry into military service are generally healthy, whereas the general population will always include some individuals of poor health. This healthy soldier effect can also apply to the risk of development of non-fatal outcomes, such as individual types of cancer.
- The concern over the healthy soldier effect is not present when an internal control group is used instead of the general population (external control group). Similarly, the examination of cancer incidence will not suffer from a potential healthy soldier effect when an internal control group is used so long as the veteran groups are similar or adjusted for potential confounding variables, such as military rank.
- Relative risk estimates that are only slightly above (e.g., 1.1) or below (e.g., 0.9) the null value of 1.0 may achieve statistical significance, yet be more liable to reflect bias (e.g., selection, confounding) and be of less clinical significance than relative risk estimates of larger magnitude.
Conclusions When reviewing results within and across publications from the Korean study, given its considerable variability in methods of exposure assessment, outcome ascertainment, and selection of control group, the committee members adhered to the following guidelines:
- Very limited overall weight was afforded to self-reported exposure data and self-reported health-outcomes data compared to objective measurements of the chemicals and health outcomes of interest.
- More weight was given to the relative risk estimates of mortality and cancers derived from the use of an internal control group than from the use of the general population in order to minimize concern about a healthy soldier effect.
- Less weight was afforded to statistically significant associations close to the null value (e.g., ranging from 0.9 to 1.1) than to those further from the null in order to account for differences of questionable clinical significance arising from this large study’s statistical power and to allow for modest selection bias and confounding.
Brief reviews of individual publications on the Korean Veteran study are presented below.
In Yi (2013), a total of 185,265 Korean men, who had served in Vietnam from 1964 to 1973 and who were alive in 1992, were followed for cancer incidence from 1992 to 2003 and for mortality through 2005. Cancer diagnoses were ascertained via linkage with the Korean National Cancer Incidence Database, whereas cancer deaths were identified using the National Statistical Office records during the follow-up of this cohort. Age-adjusted incidence and standardized incidence ratios (SIRs) were calculated using the Korean male population during 1992 to 2003 as the reference population (Yi, 2013). The overall cancer incidence in Vietnam veterans was not higher than in the general male population, although there were exceptions across the very long list of types of cancer examined. Specifically, Vietnam veterans and military rank subcohorts experienced a higher incidence of several cancers, including prostate cancer, T-cell lymphoma, lung cancer, bladder cancer, kidney cancer, and colon cancer, than the general population. This study did not examine cancer incidence and cancer mortality in terms of herbicide exposure during military service in Vietnam.
In Yi et al. (2013a), the associations between perceived self-report herbicide exposure and a wide range of self-reported diseases were reported for 114,562 Korean Vietnam veterans. For an estimation of potential herbicide exposure, a six-item perceived exposure index was used to query Korean veterans as to how they might have been exposed to herbicides in Vietnam. Veterans were categorized as having either “low” or “high” perceived exposure, and similarly, classified using four categories of perceived exposure defined as “none,” “low,” “moderate,” or “high.” In addition, herbicide exposure was objectively estimated for individual veterans based on the proximity of their military units to herbicide sprayed-areas by use of the exposure opportunity model developed by Stellman et al. (2003b). Using this method, veterans were again classified using two-group and four-group exposure categorizations. All disease outcomes were based on self-report and classified into seven groups of diseases: cancers, circulatory
diseases, respiratory diseases, digestive diseases, neuromuscular diseases, endocrine diseases, and other diseases. Subtypes of disease were reported for each disease condition. The committee’s concern about the reliability of self-reported exposure and health data are illustrated by the fact that the use of such data in Yi et al. (2013a) uniformly yielded highly significant statistical associations across an exhaustive spectrum of disease conditions, while the use of the objective (Stellman) method of exposure classification and documented reports of adverse health outcome in the later publication on this population produced more variable results. The observation of inconsistencies when theoretically more reliable measures of health and exposure were analyzed reinforced the committee’s concern about the findings based on self-report in the Korean study.
Yi et al. (2013b) examined the serum levels of TCDD in 102 of these Korean Vietnam veterans with several purposes:
- to assess their use as a potential objective tool for herbicide exposure;
- to determine their correlation to self-reported exposure (six item questionnaire); and
- to evaluate how they related to age, BMI, and smoking.
Serum sample were collected in 2002 along with information from a health examination. For the objective assessment of herbicide exposure, Exposure Opportunity Indices (EOIs) were derived from a model (Stellman et al., 2003b) based on the proximity of the veterans’ military units to areas of herbicide spraying. From this model, veterans were classified as low versus high exposure or in four categories consisting of none, low, moderate, or high exposure. The serum TCDD concentrations among the Korean Vietnam veterans were lower than those reported in other studies of Korean and US Vietnam veterans, and such concentrations were not associated with herbicide exposure indices or with age, BMI, or smoking. The net value of this study is the observation that the assessment of serum levels of TCDD among veterans long after service in Vietnam (e.g., 40 years or more) may be of very limited value as a metric for herbicide exposure unless individuals were exposed to very high levels during military service.
In Yi and Ohrr (2014), the incidence of cancer was examined among 180,251 Korean Vietnam veterans from 1992 through 2003. As opposed to classifying exposure by self-report, this analysis used the EOIs from the Stellman model. The incidence of cancer was determined through a review of records from the Korea National Cancer Incidence Database (NCIDB). Overall, the veterans classified with “high” exposure had a small yet statistically significant higher risk of cancer than the veterans classified with “low” exposure (adjusted hazard ratio [HR] = 1.08, 95% confidence interval [CI] 1.03–1.13). Compared to low exposure, high herbicide exposure appeared to be most related to an elevated risk of cancers of the mouth, salivary glands, stomach, and small intestine. The objective
classification of both herbicide exposure and cancer incidence is considered a strength of this study versus other publications from this cohort with analyses based on self-report data.
Yi et al. (2014a) looked for associations between herbicide exposure and the prevalences of a wide range of disease conditions. Herbicide exposure was objectively estimated by the use of the opportunity exposure index developed by Stellman et al. (2003b). The prevalence of disease outcomes, specifically, those pertaining to the endocrine, nervous, circulatory, respiratory, and digestive systems, was determined through a review of claims data from the Health Insurance Review and Assessment Service of Korea from January 1, 2000, to September 30, 2005. Overall, and compared to “low” exposure,” “high” herbicide exposure was associated with a significantly higher prevalence of hypothyroidism, autoimmune thyroiditis, other endocrine gland disorders including pituitary gland disorders, amyloidosis, and Alzheimer disease. The objective classification of both herbicide exposure and disease prevalence is considered a strength of this study versus other reports from the Korean study that were based on self-report data.
Finally, Yi et al. (2014b) analyzed cause-specific mortality in 180,639 Korean Veteran veterans in terms of the objective exposure metrix. The EOIs were used as the basis for two characterizations of herbicide exposure: As “low” versus “high” and per unit increased based on a log-transformed scale. The incidence of mortality and cause of death were ascertained by the use of death records from the National Statistical Office for the period 1992–2005. The long-term risk of mortality was elevated slightly—yet was statistically significant—for veterans with high herbicide exposure (HR = 1.10, 95% CI 1.07–1.14). The hazard ratio for high exposure was also slightly elevated for cancer mortality (HR = 1.13, 95% CI 1.07–1.19), with the highest cause-specific cancer mortality estimates being observed for thyroid cancer (HR = 11.31, 95% CI 1.33–96.55), chronic myeloid leukemia (HR = 7.91, 95% CI 1.67–37.52), small intestine cancer (HR = 2.88, 95% CI 1.00–8.82), and bladder cancer (HR = 2.04, 95% CI 1.17–3.55). The objective classification of both herbicide exposure and cause-specific mortality is considered a strength of this study versus other analyses of this cohort based on self-report data.
Other Studies of Korean Vietnam Veterans
Epidemiologic studies have also looked at immunotoxicologic outcomes (Kim HA et al., 2003) and skin and general disease patterns (Mo et al., 2002) in Korean Vietnam veterans who were exposed to herbicides during the Vietnam War.
New Zealand Vietnam-Veteran Studies
McBride et al. (2013) followed 2,783 male veterans from New Zealand who served in Vietnam between 1964 and 1972. Their status with respect to cancer incidence and mortality were determined from 1988 through 2008. This cohort comprised 84 percent of all 3,322 Vietnam veterans from New Zealand who had survived service in Vietnam. Standardized incidence and mortality ratios (SIRs and SMRs, respectively) were generated by comparing the observed incident cases and deaths in this cohort with the corresponding expected numbers of new cases and deaths rates from the general male population of New Zealand. For all-cause mortality, the Vietnam veterans had significantly lower mortality than the New Zealand general population (SMR = 0.85, 95% CI 0.77–0.94). On the other hand cancer mortality and incidence overall were similar between Vietnam veterans and the New Zealand general population, and heart disease mortality was non-significantly lower in Vietnam veterans (SMR = 0.84, 95% CI 0.69–1.02). In contrast, New Zealand Vietnam veterans appeared to be at higher risk of cancers of the head and neck (SMR = 2.20, 95% CI 1.09–3.93) and oral cavity, pharynx, and larynx as well as of incident chronic lymphoid leukemia than the New Zealand general population. Although the follow-up of this cohort was long (20 years), the study did not have information on cancer incidence and mortality in the time period immediately after the service (i.e., between 1972 and 1988). It also lacked an internal comparison group and information on potential confounding factors including smoking, drinking habits, and human papilloma virus status were not available, which limits the interpretation of the data, particularly regarding incident cancers.
OCCUPATIONAL STUDIES
Several occupational groups in the United States and elsewhere have been exposed to the COIs. Exposure characterization in studies of these groups varies widely in the metric used, the extent of detail, confounding by other exposures, and whether individual, surrogate, or group (ecologic) measures are used. Some studies use job titles as broad surrogates of exposure; others rely on disease-registry data.
The committee reviewed many epidemiologic studies of occupationally exposed groups for evidence of an association between exposure to TCDD or to the herbicides used in Vietnam—primarily the phenoxy herbicides 2,4-dichloro-phenoxyacetic acid (2,4-D) and 2,4,5-trichlorophenoxyacetic acid (2,4,5-T)—and health risks. TCDD is an unwanted byproduct of 2,4,5-T production but not of 2,4-D production. Other contaminants, including other dioxins (such as 1,3,6,8-tetrachlorodibenzo-p-dioxin) have been reported at low concentrations in 2,4-D, but those identified do not have the toxicity of TCDD (ATSDR, 1998; Huston, 1972; Norström et al., 1979). In reviewing the studies, the committee
considered two types of exposure separately: exposure to 2,4-D or 2,4,5-T and exposure to TCDD from 2,4,5-T or other sources. That separation is necessary because some health effects could be associated with an exposure to 2,4-D or 2,4,5-T in the absence of substantial TCDD exposure. After recognition of the problem of dioxin contamination in phenoxy herbicides, production conditions were modified to minimize contamination, but the use of the products most subject to containing specifically TCDD (2,4,5-T and Silvex) was banned. As a result, the study participants exposed to phenoxy herbicides only after the late 1970s would not be assumed to have been at risk for exposure to TCDD.
The distinction is particularly important for workers in agriculture and forestry, including farmers and herbicide appliers, whose exposure is primarily the result of mixing, loading, and applying herbicides. In addition to those occupational groups, the committee considered studies of occupational exposure to dioxins, focusing on workers in chemical plants that produced phenoxy herbicides or chlorophenols, which tend to be contaminated with PCDDs. Waste-incineration workers were also included in the occupation category because they can come into contact with dioxin-like compounds while handling byproducts of incineration. Other occupationally exposed groups included were pulp-and-paper workers exposed to dioxins through bleaching processes that use chlorinated compounds and sawmill workers exposed to chlorinated dioxins, which can be contaminants of the chlorophenates used as wood preservatives.
Studies of Herbicide Production Workers
International Agency for Research on Cancer Phenoxy Herbicide Cohort
A multisite study by IARC involved 18,390 production workers and phenoxy herbicide sprayers working in 10 countries (Saracci et al., 1991). The full cohort was established by using the International Register of Workers Exposed to Phenoxy Herbicides and Their Contaminants. Twenty cohorts were combined for the analysis: one each in Australia, Austria, Canada, Finland, and Sweden; two each in Denmark, Italy, the Netherlands, and New Zealand; and seven in the United Kingdom. There were 12,492 production workers and 5,898 sprayers in the full cohort.
Questionnaires were constructed for workers who were manufacturing chlorophenoxy herbicides or chlorinated phenols and for herbicide sprayers and were completed with the assistance of industrial hygienists. Information from production records and job histories was examined when available. Workers were classified as exposed, probably exposed, with unknown exposure, or nonexposed. The exposed-workers group (13,482) consisted of all those known to have sprayed chlorophenoxy herbicides and all who had worked in particular aspects of chemical production. Two subcohorts (totaling 416) had no job titles available but worked in chemical-production facilities that were likely to produce TCDD
exposure, so they were deemed probably exposed. Workers with no exposure information (541) were classified as of unknown exposure. Nonexposed workers (3,951) were those who had never been employed in parts of factories that produced chlorophenoxy herbicides or chlorinated phenols and had never sprayed chlorophenoxy herbicides. Two nested case-control studies were undertaken with the IARC cohort to evaluate the relationship between STSs and lymphomas (Kogevinas et al., 1992, 1995). Kogevinas et al. (1993) presented the information available on the subcohort of 701 women who were occupationally exposed to chlorophenoxy herbicides, chlorophenols, and dioxins included in 11 of the cohorts in seven of the countries; nine deaths and 29 incident cancer cases were reported (too few to tabulate results).
An expanded and updated analysis of the IARC cohort with an emphasis on cancer mortality was published in 1997 (Kogevinas et al., 1997). The researchers added herbicide production workers in 12 plants in the United States (the NIOSH cohort) and four plants in Germany. The 21,863 male and female workers exposed to phenoxy herbicides or chlorophenols were classified in three categories of exposure to TCDD or higher-chlorinated dioxins: those exposed (13,831), those not exposed (7,553), and those with unknown exposure (479). Several exposure metrics were constructed for the cohort—years since first exposure, duration of exposure (in years), year of first exposure, and job title—but detailed methods were not provided. The overall results were for mortality in 1939–1992, but for some of the subcohorts follow-up had begun as late as 1975, and at the time of publication, mortality in some had been tracked only through 1983. For non-neoplastic causes of death, Vena et al. (1998) repeated the grouped statistics for all phenoxy-herbicide workers in the updated IARC cohort (as previously presented in Kogevinas et al., 1997) and provided results partitioned according to whether the workers had the potential for exposure to TCDD and more highly chlorinated dioxin contaminants.
No new studies of the IARC cohort have been published since Update 1998.
International Agency for Research on Cancer Subcohorts
In addition to the NIOSH cohort and its component subcohorts (discussed below), several of the subcohorts that make up the IARC cohort have generated independent reports that have been evaluated separately by VAO committees to garner additional insights, such as the results associated with TCDD concentrations measured in various subjects: Austrian production workers (Jäger et al., 1998; Neuberger et al., 1998, 1999), British production workers (Coggon et al., 1986, 1991), Danish production workers (Lynge, 1985, 1993), Dutch production workers (Boers et al., 2010, 2012; Bueno de Mesquita et al., 1993; Hooiveld et al., 1998), German production workers (Becher et al., 1996; Flesch-Janys, 1997; Flesch-Janys et al., 1995; Manz et al., 1991), and New Zealand production workers (McBride et al. 2009a,b; Smith et al., 1981, 1982; ’t Mannetje et al.,
2005). Several of the component cohorts have not been the subject of any separate publications: Australian herbicide sprayers, Canadian herbicide sprayers, Finnish production workers, two cohorts of Italian production workers, and Swedish production workers. The international production-worker cohorts are discussed below in alphabetical order, followed by the NIOSH cohort and its subcohorts. The section on studies of herbicide-using workers, which follows the discussion of all the production-worker studies, includes consideration of the separate reports on the New Zealand herbicide sprayers.
Boehringer–Ingelheim Cohort in Hamburg As first reported by Manz et al. (1991), workers in the Boehringer–Ingelheim plant in Hamburg had high potential for TCDD exposure because of the production of trichlorophenol (TCP) and 2,4,5-T from 1951 to 1954 and from 1957 to 1984. The hiatus was motivated by a chloracne outbreak, and production recommenced when a process that resulted in less TCDD contamination became available. The cohort consisted of 1,184 men and 399 women who had been employed for at least 3 months from 1952 through 1984. Vital status of all but 46 workers (2.9 percent) through 1989 was established; 313 deaths were observed in the men and 54 in the women. Detailed results were reported only for the men. Mortality from all causes did not differ from what would be predicted by rates for West Germany (SMR = 1.00, 95% CI 0.89–1.12); compared with what was probably a more appropriate occupational cohort of Boehringer gas workers, however, mortality from all causes (only through 1985 because of the limitations of available information) was significantly higher (SMR = 1.34, 95% CI 1.18–1.51). The risk of death from all cancers was marginally higher than the West German rates (SMR = 1.24, 95% CI 1.00–1.52) and more definitively so compared with the gas workers (SMR = 1.39, 95% CI 1.10–1.75).
Flesch-Janys et al. (1995) updated the cohort’s vital status through 1992 and added a quantitative exposure assessment based on blood or adipose-tissue measurements of PCDDs and PCDFs. The authors estimated the maximum PCDD and PCDF exposures for 190 workers with a first-order kinetics model, half-lives with an elimination study of 48 workers in the cohort, and background concentrations in the German population. They then regressed the estimated maximum PCDD and PCDF exposures of the workers against the length of time that they worked in each production department in the plant. The working-time weights were then used with work histories of the remainder of the cohort to estimate the PCDD and PCDF exposure of each person at the end of his or her exposure. Those values were used to estimate TCDD doses in the population. (At this the stage of updating, the Hamburg cohort was discussed with three other German cohorts by Becher et al., 1996, and became a subcohort of the IARC phenoxyherbicide cohort as updated by Kogevinas et al., 1997.)
Manuwald et al. (2012) updated the mortality experience of 1,191 men and 398 women in the Hamburg cohort. Subjects entered the cohort on the date of
their first employment in the plant, and vital status was sought through 2007; the loss to follow-up was only 3.2 percent. SMRs calculated relative to the population of Hamburg showed that death from all causes was slightly higher in men (698 deaths, SMR = 1.14, 95% CI 1.06–1.23); the increase in mortality was significant in the entire cohort (SMR = 1.08, 95% CI 1.01–1.16), but not in women (180 deaths, SMR = 0.91, 95% CI 0.78–1.05). Similarly, mortality from all malignant neoplasms was slightly higher in men (226 cancer deaths, SMR = 1.14, 95% CI 1.06–1.23), and the increase in mortality was significant in the entire cohort (SMR = 1.33, 95% CI 1.18–1.49) but not in women (65 cancer deaths, SMR = 0.91, 95% CI 0.78–1.05). The individual cumulative exposure was estimated from work history on the basis of company records, and the intensity of TCDD exposure in workplaces was based on previous analyses of serum and fat-tissue dioxin concentrations. Cochran–Armitage trend tests on quartiles of cumulative exposure were conducted for deaths from all causes, all malignancies, breast cancer, cancers of digestive organs, respiratory cancers, and circulatory diseases.
BASF Ludwigshafen Plant Workers Involved in Accident Cleanup (This group was not in the IARC cohort.) An accident on November 17, 1953, during the manufacture of TCP in a BASF plant in Germany, resulted in the extreme exposure of some workers to TCDD. VAO, Update 1996, Update 1998, and Update 2000 summarized studies of those workers, including a mortality study of persons initially exposed or later involved in cleanup (Thiess et al., 1982), an update and expansion of that study (Zober et al., 1990), and a morbidity follow-up (Zober et al., 1994). In addition, Ott and Zober (1996a) and Zober et al. (1997) examined cancer incidence and mortality in workers exposed to TCDD after the accident or during reactor cleanup, maintenance, or demolition. No new studies have been published on these workers since Update 2000.
Dutch Production Workers The two Dutch subcohorts of the IARC cohort consist of 2,106 male workers employed in two manufacturing factories producing and formulating chlorophenoxy herbicides: 2,4,5-T in factory A from 1955 through 1985 and 2-methyl-4-chlorophenoxyacetic acid (MCPA), 2-(2-methyl-4-chlorophenoxy)propionic acid (Mecoprop, MCPP), and 2,4-D in factory B from 1965 through 1986. Accordingly, members of both subcohorts had potential exposure to phenoxy herbicides, but only those in factory A would have been exposed to TCDD. Contamination with the TCDD congener of dioxin in Factory A was exacerabated in 1963 by an explosion due to an uncontrolled reaction in an autoclave where 2,4,5-T was synthesized from 2,4,5-TCP that released dioxins with an exceptionally high concentration of TCDD. In factory B, the main products were 2,4-D and MCPP, which suggests that it is unlikely that there was significant exposure to TCDD. The study populations were defined as all workers who worked in factory A during 1955–1985 or factory B during 1965–1986. Bueno de Mesquita et al. (1993) reported on their mortality experience through 1985.
Hooiveld et al. (1998) updated the mortality experience (1955–1991) of the production workers in these two Dutch chemical factories. On the basis of an assumption of first-order TCDD elimination with an estimated half-life of 7.1 years, the measured TCDD concentrations were extrapolated to the time of maximum TCDD exposure of a group of 47 workers. A regression model was then used to estimate, for each cohort member, the effect on estimated maximum TCDD exposure attributable to exposure as a result of the accident, the duration of employment in the main production department, and the time of first exposure (before or after 1970).
Boers et al. (2010) conducted a third follow-up of cause-specific mortality (cancer and non-cancer) through 2006 for the 2,106 male workers employed in factories A and B, accumulating 65,087 person-years, with 567 deaths observed. The sample loss was minimal (< 1 percent lost to follow-up, < 5 percent emigrated). Death certificates obtained by linkage to Statistics Netherlands were used to ascertain the cause-specific mortality, including various cancers, endocrine or blood diseases, nervous system, ischemic heart disease, other heart disease, cerebrovascular diseases, respiratory diseases, digestive diseases, and genitourinary diseases. Exposure to chlorophenoxy herbicides was determined on the basis of the type of work experience (such as production versus office) and the involvement in the accident of 1963 in factory A (factory A: 539 exposed, 482 non-exposed; factory B: 411 exposed, 626 non-exposed). TCDD measures taken in 1993 support that exposure classification: The highest mean TCDD concentrations were found in workers involved in the 1963 accident (1,841.8 ppt) and those who worked in main production (608.2 ppt), whereas concentrations in non-exposed workers were much lower (7.6 ppt). Cox proportional-hazards models with attained age as the time scale were used to assess the hazard ratios for exposed versus nonexposed workers. The exposure to phenoxy herbicides and dioxins was expected to be different between factory A and factory B, and the factories were therefore analyzed separately. Further nested case-control studies were conducted for the factory A cohort by using all cancer cases (112) and three controls per case matched on age and employment period; the analysis used conditional logistic regression.
Boers et al. (2012) conducted more detailed dose–response analyses of the updated mortality data on the cohorts reported in Boers et al. (2010). From May 2007 to September 2008, blood was drawn for the determination of plasma TCDD concentrations in a systematically selected subsample of 187 workers (101 in factory A, 86 in factory B). Serum concentrations measured in the workers in factory B (geometric mean = 0.4 ppt) confirmed they had not experienced TCDD exposures above background. The combination of linear regression on the log-transformed serum results and the workers’ work-history details was used to derive a model to predict current TCDD concentrations in the entire cohort. A first-order, one-compartment kenetic model with the half-life of TCDD estimated to be 7.1 years was used to estimate each person’s concentration when he left
employment in factory A or B (presumably the time of maximum cumulative exposure). There were considerable individual differences from the previously assigned exposure groups, but overall the exposures predicted by the empirical model had a high rank correlation (Spearman’s r = 0.79) with the exposure statuses used in previous analyses. A Cox proportional-hazards model was used to assess exposure–outcome relationships on the basis of the predicted exposures as a time-varying covariate. To allow for latency, a 1-year lag was used for noncancer endpoints and a 10-year lag for cancer outcomes. The log-linear TCDD model was applied to the workers in factory A only and to the entire cohort, including workers from factory B, who had been exposed only to phenoxy herbicides as confirmed by the serum samples from the 86 factory B subjects who had only background concentrations of TCDD.
Saberi Hosnijeh et al. (2011) examined the association between TCDD exposure and outcomes, including humoral immunity (serum immunoglobulin and complement factor concentrations) and atopic diseases (self-reported asthma, hay fever, eczema, and allergy) in a subsample of 153 workers, including 45 who had TCDD exposure in factory A, matched individually with a non-exposed comparison group consisting of 39 in factory A and 69 in factory B. TCDD exposure was characterized by using exposure status (exposed versus non-exposed), current serum concentration, and serum concentration at the time of the last exposure as derived by Boers et al. (2012). Logarithmic transformation was used for both TCDD and immune-marker concentrations. Statistical analyses were conducted with t tests, chi-square tests, and linear regression. Similarly, Saberi Hosnijeh et al. (2012a) examined the association between TCDD exposure and serum concentrations of 16 cytokines, 10 chemokines, and 6 growth factors from the blood plasma samples taken in 2007 and 2008 from workers in factory A only (47 with high exposure, 38 with low exposure).
Since Update 2012, Saberi Hosnijeh et al. (2012b, 2013a,b) have published three additional studies based on the serum samples drawn from the Dutch cohort in 2007–2008. These studies examined immunological and metabolic parameters that may relate etiologically to some adverse health outcomes, including cancers and heart disease. In Saberi Hosnijeh et al. (2012b), changes in cell counts and lymphocyte subsets were compared between the 47 workers with high-TCDD-exposure and the 38 with low-TCDD-exposure from Factory A. Saberi Hosnijeh et al. (2013a) addressed plasma levels of CD27, CD30, and interleukin 1 receptor antagonist (IL1RA) from this same set of workers; these proteins regulate immune function and have been found to be involved in lymphopoeitic neoplasms. Similarly, in Saberi Hosnijeh et al. (2013b), serum metabolites measured in this set of serum samples by ultra-high pressure liquid chromatography and mass spectrometry were the focus of similar analyses.
Rather than being the type of health outcomes that VAO committees assess for association with herbicide exposure, the measures considered in these studies of the Dutch production workers provide information on biologic plausibility for
health outcomes involving immune response and B-cell neoplasms. Interpretation of results is complicated for these analyses of endpoints measured nearly four decades after TCDD exposure on the basis of the current TCDD level and the maximum TCDD level based on back-extrapolation. The analyses also did not take into account potential intervening exposures.
German Production Workers Becher et al. (1996) conducted an analysis of the four German cohorts added to the IARC cohort as of 1997: the Boehringer–Ingelheim cohort (also reported on in more detail by Manz et al., 1991, and later researchers), a cohort in the BASF Ludwigshafen plant that did not include those involved in a 1953 accident, and cohorts in a Bayer plant in Uerdingen and a Bayer plant in Dormagen. Preliminary information on the four cohorts had been published earlier (Becher et al., 1992). All the plants were involved in production of phenoxy herbicides or chlorophenols. Additional information is available only on the Boehringer–Ingelheim cohort, and the workers involved in the 1953 accident have been studied separately.
New Zealand Production Workers
The mortality status of the New Zealand cohort that was incorporated into the original IARC cohort was followed through 2000 by ’t Mannetje et al. (2005). The New Plymouth plant produced phenoxy herbicides from the late 1950s through the mid-1980s. This plant also produced picloram, one of the COIs about which very little information is available. Complete employment records for 1969–1984 were available, so the study included anyone who had worked at least 1 month in that period—a cohort of 713 men and 100 women (the 1984 cohort).
Burns et al. (2010), Collins et al. (2009a), and McBride et al. (2009a,b), examined the New Zealand production-worker subcohort of the IARC cohort, which consisted of employees who worked at the Dow AgroSciences (formerly Ivon Watkins-Dow) plant in New Plymouth that manufactured diverse agrochemical products, including phenoxy herbicides. McBride et al. (2009a) conducted expanded analyses and updated previous analyses of cause-specific mortality (from both cancers and other conditions). The cohort was increased to 1,599 participants (referred to hereafter as the 1988 cohort), including a substantial number of people who had minimal opportunity for exposure, by extending the employment period for eligibility to November 1, 1988, and removing the requirement that employment lasted at least 1 month. McBride et al. (2009b) further expanded the cohort to 1,754 participants (the 2003 cohort) by further extending eligibility to anyone who worked at the site at any time until October 1, 2003. Both enlarged cohorts were followed through 2004. The New Zealand Health Information Service Mortality Collection was used to identify deaths (247 in both cohorts; there seem to have been no deaths in the increment of 155 worker who were in the 2003 cohort but not in the 1988 cohort). Exposure status was classified according to
work experience. A subsample of the 1988 cohort participated in a serum-dioxin analysis (346, 70 percent exposed).
Collins et al. (2009a) described the group’s serum TCDD concentrations overall, and Burns et al. (2010) performed analyses to determine what factors might predict serum TCDD: Age, BMI, and employment history were found to be significant determinants. In particular, the exposed group had significantly (p = 0.03) higher concentrations (9.9 ppt) than the non-exposed group (4.8 ppt); the number of years since termination was associated significantly (p = 0.002) with lower TCDD; and the serum TCDD was also associated significantly (p < 0.0001) with predicted cumulative TCDD exposure on the basis of area-under-the-curve in a pharmacokinetic model of the accumulation and elimination of dioxins. Both studies reported SMRs that were derived by using the Occupational Cohort Mortality Analysis Program with the New Zealand population as the reference population and adjusted for age, sex, and calendar age. For the 1988 cohort, SMRs were stratified by exposure status (ever exposed and never exposed) and by predicted cumulative exposure categories. For the 2003 cohort, SMRs were reported for the entire cohort and stratified by employment duration (less than 3 months and at least 3 months) and by latency (15 years and less than 15 years of latency). For the 1988 cohort, proportional-hazards survival analysis was also used to test the association between mortality and predicted cumulative exposure categories.
The New Zealand studies have several important limitations. The sample loss was substantial: 13 percent were lost to follow-up in both cohorts, and 8 percent of the 1988 cohort and 9 percent of the 2003 cohort emigrated. If sample loss was nonrandom, then the study findings might be vulnerable to sample selection bias. In addition, the inclusion in the 2003 cohort of the employees hired as recently as 2003 is questionable. It appears that no deaths were observed in the increment between the 1988 cohort and the 2003 cohort (those hired since 1988), presumably because these participants are relatively young. The inclusion of the incremental participants might dilute the power of the study to detect the effects of TCDD exposure on health outcomes that require a long latent period; participants who have not yet “matured” through the latent period might be contributing noise rather than signal to the analyses. The committee, therefore, did not give substantial weight to the dose–response findings of McBride et al. (2009b). The serum concentrations of dioxins and furans observed in a subset of the workers in the Dow phenoxy-herbicide plant in New Zealand have been used in estimating individual exposure (Aylward et al., 2010; Collins et al., 2009a).
National Institute for Occupational Safety and Health Studies
NIOSH PCP Cohort Ruder and Yiin (2011) reported findings on mortality in 2,122 pentachlorophenol (PCP) production workers in four plants—Midland,
Michigan; Sauget, Illinois; Tacoma, Washington; and Wichita, Kansas—in the NIOSH dioxin registry. For analytic purposes, the cohort was partitioned into a subcohort of 1,402 workers (PCP-only group) who were employed only in the production of PCP, which has dioxin and furan contaminants that do not include the most toxic 2,3,7,8-TCDD congener, and a subcohort of 720 (PCP-plus-TCDD group) who also worked in TCP production and therefore had exposure to TCDD). The cohort was followed through December 31, 2005. Exposure was specified both as exposure status (exposed versus not exposed, for cohort members versus reference population) and as cumulative duration of exposure stratified into four quartiles. Statistical analyses were based on SMRs with the US population as the reference, and standardized rate ratios were used to compare workers in cumulative duration categories.
NIOSH Cross-Sectional Medical Study Before the first publication of mortality results in the main cohort, the NIOSH Cross-Sectional Medical Study gathered comprehensive medical histories, conducted medical examinations, and measured the pulmonary function of workers employed in chemical manufacturing at plants in Newark, New Jersey (1951–1969) and Verona, Missouri (1968–1972). The control participants were recruited from surrounding neighborhoods (Sweeney et al., 1989, 1993). The New Jersey plant manufactured 2,4,5-TCP and 2,4,5-T; the Missouri plant manufactured 2,4,5-TCP, 2,4,5-T, and hexachlorophene. Specific health outcomes were evaluated in the members of this subcohort, including porphyria cutanea tarda (Calvert et al., 1994), effects on pulmonary function (Calvert et al., 1991), effects on hepatic and gastrointestinal function (Calvert et al., 1992), mood (Alderfer et al., 1992), effects on the peripheral nervous system (Sweeney et al., 1993), and effects on reproductive hormones (Egeland et al., 1994). Sweeney et al. (1996, 1997/1998) reviewed and updated noncancer outcomes, including the effects on hepatic function, gastrointestinal disorders, chloracne, diabetes, and serum glucose, hormone, and lipid concentrations. The data gathered from the two plants were also examined for cardiovascular effects (Calvert et al., 1998); diabetes mellitus, thyroid function, and endocrine function (Calvert et al., 1999); immune characteristics (Halperin et al., 1998); and cancer incidence (Kayajanian, 2002). Halperin et al. (1995) investigated the relationship between serum TCDD concentrations and cytochrome P450 induction in 400 of the original 586 subjects in the cohort. Lawson et al. (2004) studied three birth outcomes—birth weight, preterm delivery, and birth defects—in the offspring of the cohort members by comparing serum TCDD concentrations with those in a reference population. TCDD exposures at conception were estimated by using physiologically based pharmacokinetic modeling (Dankovic et al., 1995; Thomaseth and Salvan, 1998).
NIOSH TCDD Mortality Cohort Since 1978, NIOSH has compiled an extensive set of data on chemical production workers potentially contaminated with TCDD in 1942–1984. More than 5,000 workers who were involved in production or maintenance in any of 12 companies were identified from personnel and payroll records; 172 additional workers identified previously by their employers as being exposed to TCDD were also included in the study cohort (Suskind and Hertzberg, 1984). The employees’ possible exposure resulted from working with substances of which TCDD was a contaminant: 2,4,5-TCP, 2-(2,4,5-trichloro-phenoxy) propionic acid (Silvex, 2,4,5-TP), 2-(2,4,5-trichlorophenoxy) ethyl 2,2-dichloropropionate (Erbon), O,O-dimethyl O-(2,4,5-trichlorophenyl) phosphorothioate (Ronnel®), and hexachlorophene. The 12 plants involved were large manufacturing sites of major chemical companies, so many of the participants were potentially exposed to many other compounds, some of which could be toxic and carcinogenic. The NIOSH cohort was added to the IARC cohort as of the 1997 publication by Kogevinas et al.
Exposure status was determined initially through a review of process operating conditions, employee duties, and analytic records of TCDD in industrial-hygiene samples, process streams, products, and waste (Fingerhut et al., 1991). Occupational exposure to TCDD-contaminated processes was confirmed by measuring serum TCDD in 253 cohort members. The duration of exposure, defined as the number of years worked in processes contaminated with TCDD, was used as the primary exposure metric in the study. The use of duration of exposure as a surrogate for cumulative exposure was based on a correlation (Pearson correlation efficient, 0.72) between log-transformed serum TCDD and the number of years worked in TCDD-contaminated processes. The duration of exposure of individual workers was calculated from work records, and exposure-duration categories were created: Less than 1 year, 1 to less than 5 years, 5 to less than 15 years, and 15 years and longer. In some cases, information on the duration of exposure was not available, so a separate metric, duration of employment, was defined as the total time that each worker was employed at the study plant. Fingerhut et al. (1991) used the exposure measures in assessing mortality through 1987.
A follow-up study (Steenland et al., 1999) examined the association between TCDD exposure and cause of death through 1993; it examined specific health outcomes, including cancers (all and site-specific), respiratory disease, cardiovascular disease (CVD), and diabetes. The researchers used a more refined exposure assessment than did previous analyses; it excluded workers whose records were inadequate to determine duration of exposure, and this reduced the number of study participants to a subcohort of 3,538 workers (69 percent of the overall cohort). The exposure assessment for the subcohort was based on a job–exposure matrix (JEM) that assigned each remaining worker a quantitative exposure score for each year of work (Piacitelli and Marlow, 1997).
No new studies on the entire NIOSH cohort were published during the current review period.
Subcohorts of the NIOSH TCDD Mortality Cohort
Monsanto The NIOSH study cohort (Fingerhut et al., 1991) included employees of the Monsanto facility in Nitro, West Virginia, which produced 2,4,5-T in 1948–1969. Zack and Suskind (1980) examined the mortality experience of the 121 men who had chloracne associated with an unintentional release that occurred on March 8, 1949. Other studies considered mortality and other health outcomes in additional workers involved in numerous aspects of 2,4,5-T production at the Monsanto plant (Collins et al., 1993; Moses et al., 1984; Suskind and Hertzberg, 1984; Zack and Gaffey, 1983). The Monsanto studies were discussed in more detail in VAO. No additional studies on those participants alone have been published; they have since been followed as part of the NIOSH and IARC cohorts.
Dow 2,4-D Production Workers CJ Burns et al. (2011) have reported on cancer incidence in 2,4-D production workers in the Dow Midland plant. The exposed cohort consisted of 1,316 men who worked in 2,4-D operations from 1945 through 1994 and who were alive on January 1, 1985, when the Michigan statewide cancer registry was initiated. Exposure was considered both as a category (exposed [cohort members] versus non-exposed [reference population]) and as a cumulative variable estimated as (job-specific exposure estimate) × (duration on the job) summed over all jobs held since 1945. Workers were stratified into three categories according to their estimated cumulative exposure. The cohort was followed in 1985–2007. Cancer incidence was ascertained from the Michigan statewide cancer registry and data linked to Arizona and Ohio, states where cohort members might reside. Three nested cohorts were used for statistical analyses in order to address potential problems with data that were missing because of migration outside the three states with data linkage. Cohort 1 consisted of the entire exposed cohort (1,316 who had 25,267 person-years of follow-up). Cohort 2 required Michigan residency; follow-up was terminated when a person was known to not be a Michigan resident, either because company records showed a permanent non-Michigan address or a death certificate showed a state other than Michigan as the state of residency (1,256 who had 23,354 person-years). Cohort 3 had a more stringent residency requirement; follow-up was terminated when a person was no longer known to be a Michigan resident (1,108 who had 18.897 person-years). For Cohort 2, people of unknown residency status were assumed to remain Michigan residents and were included in the follow-up; for Cohort 3, such people were assumed to be nonresident and were excluded. Standardized incidence ratios were derived for all three cohorts with Michigan white males as the reference population; Fisher’s exact confidence interval was used to characterize
the uncertainty. For Cohort, 2 additional analyses were conducted by using the National Cancer Institute (NCI) Surveillance, Epidemiology, and End Results (SEER) registry population and a regional population as the reference populations and by stratifying the cohort according to cumulative duration and cumulative exposure categories.
There are concerns that the study findings might be biased, for several reasons. First, the study cohort might be healthier than the general population being used as the reference population. Second, the lack of a latent period in the study design might lead to an attenuation effect on the risk estimates; this is similar to the Villeneuve and Steenland (2010) criticism of the Dow–Midland mortality study reported in Collins et al. (2009b). Third, Cohort 2, which was the researchers’ focus in the study, might be vulnerable to an attenuation effect because of the uncertainty in residency status. For the present VAO review, the results on Cohort 3 are considered the least subject to bias and hence the most reliable, although this smallest group is subject to the most variability; consistency in results among the three cohorts is considered confirmatory.
All Dow TCP-Exposed Workers TCP was produced in Dow’s facility in Midland, Michigan, from 1942 to 1979, and 2,4,5-T was produced there from 1948 to 1982. The cohort of TCP workers who were potentially exposed specifically to TCDD is one of the eight cohorts in the NIOSH cohort of dioxin-exposed US workers that were entered into the IARC phenoxy herbicides cohort.
Collins et al. (2009b) updated the vital status through 2003 of 1,615 people who worked with TCP or 2,4,5-T from 1942 through 1982; 58,743 person-years were accumulated, and 662 deaths were observed. SMRs for cause-specific mortality in the cohort—with and without the overlap of 196 people with the PCP cohort in Collins et al. (2009c)—were calculated by using the US population as the reference population and using the Occupational Mortality Analysis Program.
Dow PCP Production Workers This set of people were engaged in the manufacture of PCP from 1937 to 1980 in the same plant where the TCP cohort worked. Unlike TCP, PCP did not contain TCDD, but it did contain other highly chlorinated dioxin congeners, and 20 percent of the PCP workers had suffered from chloracne. Those who had no TCDD exposure are not in the IARC or NIOSH cohorts. This group is one of four cohorts included in NIOSH’s PCP cohort (Fingerhut et al., 1984; Ruder and Yiin, 2011).
Dow has tracked a cohort of its manufacturing workers who were exposed to PCP (Ramlow et al., 1996). The exposure assessment evaluated the available industrial-hygiene and process data, including recollections from employees about processes and jobs, information about changes in processes and engineering controls, measurements from surface wipes, and exposure monitoring data from area sampling and personal breathing zones. Jobs in the “flaking/prilling/
packaging area” were determined to have a higher potential exposure because of dermal exposure to airborne PCP; the industrial-hygiene data suggested a difference of about a factor of 3 between the areas of highest and lowest potential exposure. An estimated exposure-intensity score of 1–3 (from lowest to highest potential exposure intensity) was assigned to each job. Information concerning the use of personal protective equipment was deemed to be unreliable. For each participant, cumulative PCP and TCDD exposure indexes were calculated by multiplying the duration of each exposed job by its estimated exposure intensity and then summing across all exposed jobs.
Collins et al. (2009c) conducted a mortality study of the Dow PCP production workers with the accrual of years at risk starting at the beginning of 1940. The cohort was followed for up to 64 years. Although the date of closure of the follow-up was not provided explicitly, it appears that the cohort was followed through 2003, as were the TCP workers (Collins et al., 2009b). The cohort consisted of 773 PCP workers; 27,035 person-years were accumulated, and 370 deaths were observed. SMRs for the PCP cohort (with and without the overlap of 196 people in the TCP cohort) were given for cause-specific mortality with the US population as the referent population. Proportional-hazards survival analysis was also used to assess the association between mortality and predicted cumulative exposure as total toxic equivalent (TEQ) to TCDD.
Dow TCDD-Exposed Production Workers Dow conducted a study of 204 workers engaged in the production of 2,4,5-T (Ott et al., 1980) and another study of 61 TCP manufacturing workers who had chloracne (Cook et al., 1980). Industrial hygienists developed a JEM that ranked employee exposures as low, moderate, or high on the basis of available air-monitoring data and professional judgment. The matrix was merged with employee work histories to assign an estimate of exposure to each job. A cumulative dose was then developed for each of the 878 employees by multiplying the representative 8-hour time-weighted average (TWA) exposure value for each job by the number of years in the job and then adding the products for all jobs. A 2,4-D TWA of 0.05 mg/m3 was used for low, 0.5 mg/m3 for moderate, and 5 mg/m3 for high exposure. The exposure estimates do not appear to have taken into account the role of dermal exposure in the facilities. It is not clear to what extent the use of air measurements alone can provide accurate classification of workers into low-, moderate-, and high-exposure groups. Biologic monitoring of 2,4-D apparently was not included in the study.
Bond et al. (1983) investigated potential exposure to TCDD and morbidity in the sets of workers reported on by Cook et al. (1980) and Ott et al. (1980). Potential TCDD exposure and reproductive outcomes were studied in the offspring of 930 men who worked with chlorophenol from 1939 through 1975 (Townsend et al., 1982). Dow employees who had a diagnosis of chloracne or who were classified as having chloracne on the basis of a clinical description were followed
prospectively for mortality (Bond et al., 1987). There was a succession of mortality studies of workers involved in 2,4-D production in several of the plants (Bloemen et al., 1993; Bond et al., 1988; Burns et al., 2001), which also were conducted with the same exposure-assessment procedures.
Dow assembled a large cohort at the Midland, Michigan, plant (Bond et al., 1989a; Cook et al., 1986, 1987). The exposure to TCDD in the cohort was characterized on the basis of chloracne diagnosis (Bond et al., 1989b). Within the cohort, a subcohort study of women (Ott et al., 1987) and a case-control study of STS (Sobel et al., 1987) were conducted. The Dow cohorts have been followed as part of the NIOSH and IARC cohorts since 1991 and 1997, respectively.
Bodner et al. (2003) published a 10-year follow-up of the work of Cook et al. (1986), comparing the mortality experience of 2,187 male Dow workers who were potentially heavily exposed to dioxin before 1983 with that of the NIOSH and IARC cohorts. Dow researchers have published a study of serum dioxin concentrations measured in 2002 in former chlorophenol workers (Collins et al., 2006). Most of the workers in the study were included in the NIOSH and IARC cohorts. The authors used their data to estimate worker exposure at the time of exposure termination by using several pharmacokinetic models. They concluded that their findings were consistent with those of other studies that reported high serum dioxin concentrations in chlorophenol workers after occupational exposure.
Since Update 2012, Aylward et al. (2013) examined the elimination rates of dioxin congeners in former chlorophenol workers from Midland, Michigan. This study examined blood samples from 56 former chlorophenol workers in 2004–2005, and then re-sampled in 2010. The purpose of this analysis was to estimate half-life reductions for TCDD TEQs, which, in aggregate, were 9.3 years for the dioxin congeners analyzed. This analysis is informative with respect to estimating elimination rates over time for the COIs as the Vietnam-veteran cohort continues to age.
Czech Worker Studies
Several studies of Czech workers have been reviewed by VAO committees. The original committee reviewed a 10-year follow-up study of 55 men in Czechoslovakia who were exposed to TCDD during the production of 2,4,5-T (Pazderova-Vejlupková et al., 1981). The exposure occurred because of excessive temperature and pressure in the production process over an extended period (1965–1968) rather than as a consequence of a major release at a single time. More than 80 workers were affected, but the researchers provided little information about those who were not included in the study. Researchers observed several disorders in the workers, including chloracne, metabolic disturbances, abnormal results of glucose-tolerance tests, evidence of a mild hepatic lesion, nervous system focal damage, and psychologic disorders. In a 30-year follow-up, Pelclová et al. (2001, 2002) examined biochemical, neuropsychologic, neurologic,
and lipid-metabolism abnormalities in the surviving Czech cohort. Previous VAO committees concluded that there were a number of methodologic problems: selection bias; a lack of control for confounding by educational achievement, tobacco use, or alcohol use; the use of self-reported symptoms; and the lack of an objective measure of exposure. In 2004 Pelclová and colleagues (2007) compared the vascular function of 15 exposed workers with that of 14 healthy male health care workers who had no history of occupational exposure to TCDD. Urban et al. (2007) evaluated the same set of workers, looking at overall health effects. Further details on those studies were given in Update 2006 and Update 2008.
Pelclová et al. (2009) reported on an update on the exposed cohort that was based on the examination and testing of 11 participants in a follow-up visit in 2008. The testing included an internal and a neurologic examination; an eye fundus examination; tests for TCDD in plasma, thyroid-stimulating hormone, and testosterone and serum lipids; ultrasonography of the carotid artery; a nerve-conduction study; electroencephalography; visual-evoked potential; a Lanthony test of acquired visual impairment; single-photon emission computed tomography of the brain; a neuropsychologic examination (eight consented); and carbohydrate-deficient transferrin, an index of long-term alcohol consumption. The mean TCDD concentration remained high (274 pg/g of blood lipids), with a wide dispersion (53–756 pg/g) among the 11 participants. The prevalences of health conditions were compared with those in the general male population of comparable age. Paired t tests and F tests were used to test for changes in the assessments obtained repeatedly during follow-up visits; Spearman’s rank correlation coefficient was used to test the association between health outcomes (such as color-vision impairment) and risk factors (such as concentrations of TCDD and carbohydrate-deficient transferring). This study has important limitations. With a low retention rate (11 participants of the original cohort of 80), the study findings are vulnerable to nonresponse bias. No description of the sample loss was given, even regarding the loss of four participants from the 2004 follow-up reported in Pelclová et al. (2007). The comparison with the prevalence in the male population of comparable age is important in the interpretation of the study findings, but no description of the comparison group is given beyond citations of its (presumed) sources. Pelclová et al. (2011) have reported on further comparisons of markers of oxidative or nitrosative stress and inflammation in plasma, urine, and exhaled breath condensate of the 11 exposed workers studied previously in Pelclová et al. (2009) compared with 16 health care workers (7 men, 9 women). This study has limitations similar to those in Pelclová et al. (2009). In particular, the mixed-sex comparison group might not be appropriate for the all-male cohort of exposed people.
Jeanneret et al. (2014) described the use of a metabolomic strategy to determine metabolic patterns related to dioxin effects in humans, including the discovery of predictive subsets of biologically meaningful and clinically relevant
compounds. This was based on blood samples taken from 11 of these Czech workers in 2011. The analysis also incorporated results of samples drawn from Victor Yushchenko, who was poisoned in September 2004. While academically of interest with respect to a better future understanding of the molecular events related to dioxin toxicity, this work was not specifically informative to the charge of the committee.
Studies of Other Industrial Cohorts
Chinese Automobile Foundry Workers
Wang and colleagues (2013) followed a cohort of 3,529 workers who worked at least 1 year between January 1, 1980, and December 31, 1985, in an automobile foundry factory located in Hubei province in China to determine the concentrations and characteristics of PCDD/Fs (including 2,3,7,8-TCDD) found in the workers and to evaluate the chemicals’ association with mortality from all causes, all cancers, and lung, liver, and stomach cancers individually. The follow-up period was from January 1, 1980, through December 31, 2005, and for all deceased subjects during this period the cause of death was collected through medical records from local or regional hospitals. When compared to the general population, all-cause mortality was similar, yet cancer mortality overall and mortality for several specific types of cancer was higher in the automobile factory workers.
Other Chemical Plants
Several studies have reviewed the health outcomes in UK chemical workers exposed to TCDD as a result of an industrial accident in 1968 (Jennings et al., 1988; May, 1982, 1983), 2,4-D production workers in the former Soviet Union (Bashirov, 1969), 2,4-D and 2,4,5-T production workers in the United States (Poland et al., 1971), white men employed at a US chemical plant that manufactured flavors and fragrances (Thomas, 1987), and US chemical workers engaged in the production of PCP, lower-chlorinated phenols, and esters of chlorophenoxy acids (Hryhorczuk et al., 1998). The long-term immunologic effects of TCDD were examined in 11 industrial workers involved in production and maintenance operations in a German chemical factory that produced 2,4,5-T (Tonn et al., 1996), and immunologic effects were studied in a cohort of workers formerly employed at a German pesticide-producing plant (Jung et al., 1998). VAO, Update 1998, and Update 2000 detailed those studies. Garaj-Vrhovac and Zeljezić (2002) conducted a study of workers occupationally exposed to a complex mixture of pesticides (atrazine, alachlor, cyanazine, 2,4-D, and malathion) during their production.
Waste-Incineration Worker Studies
A study in Japan examined the association between serum-dioxin concentrations (TEQ values for PCDDs, PCDFs, and coplanar polychlorinated biphenyls) and oxidative DNA-damage markers in municipal waste–incineration workers (Yoshida et al., 2006).
A Korean study evaluated immunologic and reproductive toxicity (DNA damage and sperm quality) in 31 waste-incineration workers and 84 control participants (Oh et al., 2005). Rather than measuring serum dioxin, both studies inferred the dioxin exposure of individual workers on the basis of dioxin concentrations in air and estimated the exposures to polycyclic aromatic hydrocarbons by analyzing two urinary metabolites, 1-hydroxypyrene and 2-naphthol.
No studies of waste-incineration workers relevant to the COIs have been published since Update 2006.
Paper-and-Pulp Cohorts
Workers in the paper-and-pulp industry can be exposed to TCDD and other dioxins that can be generated by the bleaching process during the production and treatment of paper and paper products. VAO described mortality studies of pulp and paper–mill workers potentially exposed to TCDD in five mills in Washington, Oregon, and California (Robinson et al., 1986) and in a New Hampshire mill (Henneberger et al., 1989); studies of vested members of the United Paperworkers International Union (Solet et al., 1989); and studies of cancer incidence in male paperworkers in Finland (Jappinen and Pukkala, 1991). Rix et al. (1998) studied cancer incidence through 1993 in 11,130 male and 3,232 female workers employed at three Danish paper mills at any time from 1943 through 1990.
IARC Paper-and-Pulp Cohort Update 2006 reviewed a collaborative study of cancer mortality (McLean et al., 2006) led by IARC that was composed of cohorts in 11 countries and had follow-up through 1990 to 1996 (depending on the country). The pooled data included several cohorts that had been evaluated individually in VAO and its updates before 2006. For departments in each company, industrial-hygiene experts estimated exposure to 27 agents over time. The 60,468 pulp and paper–industry workers employed from 1920 through 1996 were assigned to the “nonvolatile organochlorines” (potential contamination with TCDD assumed) group (58,162) and the “volatile organochlorines” group (60,468). The entire cohort was portioned into apparently overlapping groups for “volatile” and “nonvolatile” organochlorines on the basis of detailed job–exposure matrices developed for each of the 27 chemicals at the department level in each mill for time periods between 1920 and 1996, and these populations were then subdivided for analyses into sets that “ever” or “never” had exposure to the chemicals on the
basis of job titles. Only the results for those in the main category with potential exposure to the nonvolatile agents are relevant to the VAO task.
Sawmill Workers Sawmills use PCP (which has some contamination with dioxins but not the TCDD congener) as a fungicide, so the exposures experienced are more like “herbicide-use” than those encountered in herbicide production or in pulp-and-paper processes. Workers in sawmills might have been exposed to pentachlorophenates, which are contaminated with higher-chlorinated PCDDs (Cl6–Cl8), or to tetrachlorophenates, which are less contaminated with higher-chlorinated PCDDs. Wood is dipped into those chemical preservatives and then cut and planed in the mills. Most exposure is dermal, but some exposure can occur by inhalation (Hertzman et al., 1997; Teschke et al., 1994).
McLean et al. (2009) studied serum dioxin concentrations in 94 former sawmill workers in New Zealand who were classified as exposed (71) or non-exposed (23) according to their work history. In addition, the serum dioxin test results on 23 former sawmill workers in Sawmill Workers Against Poisons (SWAP) were provided for the study. A semi-quantitative estimate of exposure intensity was also developed by using a PCP exposure algorithm that incorporated the participants’ job titles and specific work tasks: Mixing of PCP solutions, cleaning sludge, and spraying. Serum concentrations of PCDDs and PCDFs were analyzed; the total TEQ was calculated by using the World Health Organization (WHO) toxic equivalence factors (TEFs) (van den Berg et al., 2006). The mean concentrations in exposed workers were higher than those in the non-exposed: 1,2,3,6,7,8-hexachlorodibenzodioxin, 1,2,3,4,6,7,8-heptachlorodibenzodioxin, and octachlorodibenzodioxin concentrations were two to three times higher and the WHO TEQs about 40 percent higher (13.67 pg/g versus 9.56 pg/g). The congener profiles in serum were consistent with those in PCP solutions, and dioxin concentrations increased with both the employment duration and estimated exposure intensity. The averages in the SWAP members were two to three times those in the exposed study participants (37.74 pg/g).
Studies of Herbicide-Using Workers
Various methods have been used to estimate the occupational exposure of agricultural workers to herbicides or TCDD. The simplest method derives data from death certificates, cancer registries, or hospital records (Burmeister, 1981), in which information on “usual occupation” is used to construe likely exposure to the COIs. Although such information is relatively easy to obtain, it does not provide information on the duration or the intensity of the exposure, and it cannot be used to determine whether a worker was exposed to a specific agent. In some studies of agricultural workers, an examination of the differences between occupational practices has allowed the identification of subsets of workers who were likely to have had higher exposures (Hansen et al., 1992; Musicco et al.,
1988; Ronco et al., 1992; Vineis et al., 1986; Wiklund, 1983; Wiklund and Holm, 1986; Wiklund et al., 1988a). In other studies, the county of residence was used as a surrogate for exposure, and agricultural censuses of farm production and chemical use were relied on for characterizing the exposures in individual counties (Blair and White, 1985; Cantor, 1982; Gordon and Shy, 1981), exposure was estimated on the basis of the number of years of employment in a specific occupation as a surrogate for exposure duration, or information on herbicide use at each farm was used as a surrogate of its operator’s exposure (Morrison et al., 1992; Wigle et al., 1990). Still others used self-reported information on exposure that recounted direct handling of a herbicide, whether it was applied by a tractor or a hand-held sprayer, and what types of protective equipment or safety precautions were used (Hoar et al., 1986; Zahm et al., 1990). A set of studies validated the self-reported information with written records, signed statements, or telephone interviews with co-workers or former employers (Carmelli et al., 1981; Woods and Polissar, 1989).
Forestry and other outdoor workers, such as highway-maintenance workers, are also likely to have been exposed to herbicides and other chemicals. The exposure of those groups has been classified by using approaches similar to those noted above for agricultural workers—for example, using the number of years employed, job category, and occupational title.
The original VAO committee and the update committees up to the committee for Update 2006 were satisfied with exposure characterizations as nonspecific as “usual occupation” on a death certificate or “current occupation” from a census. With the passage of time, however, exposure assessments in epidemiology studies have been increasingly exact in both specificity and amount, and this has led the members of the more recent updates to establish stricter criteria for accepting exposure as sufficiently specific for results to be added to the evidentiary database. The current committee now seeks results expressed in terms of the five chemicals of interest for this project or their analogues, and it regards classification based only on job title as inadequate; restriction by the investigators to “herbicide” exposure is considered specific enough only to provide supporting evidence. According to the policy established by the Agent Orange Act of 1991, studies of Vietnam veterans are presumed to involve relevant exposure, as are studies of workers at a particular plant during a period when it is known to have been producing phenoxy herbicides or other chemicals recognized as having been contaminated with TCDD.
American Herbicide-User Studies
Agricultural Health Study
The US Agricultural Health Study (AHS) is a prospective investigation of cohorts of private pesticide applicators (farmers), their spouses, and commercial
pesticide applicators in Iowa and North Carolina, with a total of 89,658 participants, including 57,311 applicators (82 percent of those seeking licensing) and 32,347 spouses (75 percent of all spouses). The applicators are predominantly but not exclusively male, and the spouses are predominantly but not exclusively female. The AHS is sponsored by the NCI, the Environmental Protection Agency, and the National Institute of Environmental Health Sciences. Enrollment in the study was offered to applicants for applicator certification in Iowa and North Carolina. The project’s website (www.aghealth.org) provides many details about the study, including a specification of which pesticides were the subject of information gathered from the enrollment forms and mailed questionnaires (Alavanja et al., 1994).
In phase I (1993–1997), the enrollment form for both commercial (8.6 percent) and private (largely farmers) applicators asked for details on the use of 22 pesticides (10 herbicides, including 2,4-D; 9 insecticides; 2 fungicides; and 1 fumigant) and yes–no responses as to whether 28 other pesticides (8 herbicides, including 2,4,5-T and Silvex, 2,4,5-TP; 13 insecticides; 4 fungicides; and 3 fumigants) had ever been used.
A subset of 24,034 applicators also completed and mailed back a take-home questionnaire. The questionnaire asked for details about use of the 28 pesticides with yes–no information on the enrollment form and for yes–no responses as to whether 108 other pesticides (34 herbicides, including organic arsenic, which would cover cacodylic acid; 36 insecticides; 29 fungicides; and 9 fumigants) had ever been “frequently” used. Dosemeci et al. (2002) published an algorithm designed to characterize the personal exposures of that population. Weighting factors for the key exposure variables were developed from the literature on pesticide exposure. This quantitative approach has the potential to improve the accuracy of exposure classification for the cohort but has not yet been used in published epidemiologic studies.
The 42 percent response rate for the take-home questionnaire was rather low. Although no pronounced differences in demographics, medical histories, or farming practices were found between those who completed the questionnaire and those who did not (Tarone et al., 1997), selection bias might compromise the validity of studies based on the questionnaire because of differences that might not have been captured in the enrollment form.
Phase II was a 5-year follow-up conducted in 1999–2003. Computer-assisted telephone interviews (CATIs) were completed by 60,138 participants. The interviews specified “pesticides” in general to include herbicides. They asked about specific pesticides on individual crops; for several crops, only if atrazine or 2,4-D was specified was a participant asked whether it had been used alone or as part of the manufacturer’s mixture. A full pesticide list was not posted on the website with the follow-up questionnaire. In addition, dietary histories were completed by 35,164 respondents, and buccal-cell samples were gathered from 34,810 participants. The rate of response to the phase II survey—67 percent overall and 63
percent of the original cohort of 55,748 male applicators—was modest and leaves some room for selection bias to compromise the validity of studies based on the survey. In phase III (2005–2010), responses to an updated CATI were provided by 43,426 participants.
Numerous reports on the AHS cohort have been considered in earlier updates. All have developed pesticide-exposure estimates or exposure categories from self-administered questionnaires. Using various subsets of the study population, they have addressed a variety of health outcomes: doctor visits resulting from pesticide exposure (Alavanja et al., 1998), chemical predictors of wheeze (Hoppin et al., 2002), prostate cancer incidence (Alavanja et al., 2003, 2005), lung cancer incidence (Alavanja et al., 2004), reproductive effects (Farr et al., 2004, 2006), cancer risk in the 21,375 children of pesticide appliers born in 1975 or later (Flower et al., 2004), mortality (Blair et al., 2005a), morbidity (Alavanja et al., 2005; Blair et al., 2005b), rheumatoid arthritis (De Roos et al., 2005a), breast-cancer incidence (Engel et al., 2005), neurotoxicity of chronic exposure to modest amounts of pesticides (Kamel et al., 2005), and prevalence of wheeze (Hoppin et al., 2006a). Three additional publications have discussed pesticide-use patterns in the population (Hoppin, 2005; Hoppin et al., 2006b; Kirrane et al., 2004; Samanic et al., 2005). The AHS questionnaire collected detailed information regarding herbicide use; 2,4-D was the most commonly reported herbicide. Kamel et al. (2007a) evaluated questionnaire responses from more than 18,000 AHS participants, who listed a variety of neurologic symptoms, including memory and concentration problems. Another study by Kamel et al. (2007b) evaluated Parkinson disease (PD) in participants in the AHS. WJ Lee et al. (2007) analyzed incident colorectal cancers diagnosed in AHS participants in 1993–2005. Associations with self-reported exposures to 50 pesticides (including 2,4-D, 2,4,5-T, and 2,4,5-TP) were studied. Samanic et al. (2006) reported on the incidence of all cancers combined and selected individual cancers in male pesticide applicators in the AHS particularly with respect to reported exposures to the benzoic acid herbicide dicamba (3,6-dichloro-2-methoxybenzoic acid), which has been used in combination with other herbicides, such as 2,4-D. Montgomery et al. (2008) discussed the relationship between self-reported incidence of diabetes and pesticide and herbicide exposure in 31,787 licensed pesticide applicators and their spouses. Saldana et al. (2007) reported on the cross-sectional relationship between pesticide and herbicide exposure and a history of gestational diabetes in the wives of licensed applicators. Of 11,273 women asked about their pregnancies closest to enrollment, 506 (4.5 percent) reported gestational diabetes. Hoppin et al. (2006c) evaluated participants who experienced wheeze, Hoppin et al. (2007b) evaluated farmer’s lung (hypersensitivity pneumonitis), Hoppin et al. (2007a) and Valcin et al. (2007) evaluated chronic bronchitis, and Hoppin et al. (2008) evaluated atopic and nonatopic asthma in women.
Andreotti et al. (2009) conducted a case-control analysis of pancreatic cancer in participants who completed the enrollment form (93 incident cases in 64
applicators and 29 spouses and 82,503 cancer-free controls). The ever-use of 24 chemicals and the intensity-weighted lifetime days—(lifetime exposure days) × (exposure intensity score)—of 13 chemicals were assessed. Risk estimates were calculated by using unconditional logistic regression for various exposures and controlling for age, smoking, and diabetes.
Hoppin et al. (2009) reported on pesticide use and 127 cases of allergic and 314 cases of nonallergic adult-onset asthma in 19,704 male private applicators in the AHS who were at least 20 years old and who completed both the enrollment form and the take-home questionnaire with full information on smoking, asthma history, age, BMI, and high pesticide-exposure events. The researchers excluded 487 female applicators with 19 cases of asthma because of the small sample. Logistic regression was used to evaluate the association between farming exposures and adult-onset asthma, allowing for separate associations with allergic and nonallergic asthma and adjusting for age, state (Iowa or North Carolina), smoking status (current, past, or never), and BMI. For each of 48 pesticides, the exposure status was specified as ever-use versus never-use. Further analyses of response to exposure were conducted with a three-level specification for exposure—never used, median use or less, and greater than median use—according to the distribution for intensity-adjusted days of use for the specific pesticide. As noted previously, the findings from this study might be vulnerable to selection bias because of the low response rate (42 percent) for the take-home survey.
Mills et al. (2009) reported on the association between lifetime use of 49 pesticides and the incidence of and mortality from myocardial infarction (MI) in the AHS cohort: 476 deaths among the 54,069 male participants who completed the enrollment form and 839 nonfatal events among the 32,024 male participants who completed the phase II telephone interview. Deaths from MI, as either a primary or contributing cause, were recorded from state and national death records starting at enrollment and going through December 31, 2006. The incidence of nonfatal MI was determined on the basis of a positive response on the 5-year follow-up questionnaire to the question “Has a doctor or other health professional ever told you that you had a heart attack (or myocardial infarction)?” First MIs that occurred after enrollment were counted as incident MIs. Separate analyses for mortality and incidence were conducted by using Cox regression and adjusting for state (Iowa or North Carolina), age, and smoking status (whether or not the participant had smoked 100 cigarettes in his or her lifetime). The incidence analysis also adjusted for BMI. The analyses were conducted for each pesticide specified as ever used and as lifetime days of exposure. As noted previously, the validity of the findings for the incidence analysis might be compromised because of the modest rate of response to the phase II survey—63 percent according to the committee’s calculation (35,088 respondents of 55,748 in the original cohort), reported as 70 percent in Mills et al. (2009). In particular, for incidence analyses reported in Mills et al. (2009), this survey is vulnerable to selection bias because of left truncation, that is, missing participants who died before the survey.
Goldner et al. (2010) examined the association between organochlorine exposure and thyroid disease in 19,529 female spouses in the AHS. The analysis was limited to female spouses of private applicators who completed both the take-home survey in phase I (pesticide use) and the follow-up interview in phase II (thyroid disease) and for whom there were complete data on all covariates. Thyroid-disease status (none in 14,486, hyperthyroidism in 369, hypothyroidism in 1,114, and other in 560) was ascertained from a self-reported history of physician diagnoses obtained during the phase II interviews. Logistic regression was used to estimate the association between the use of herbicides (including 2,4-D and 2,4,5-T) and insecticides and thyroid-disease status (with no disease as the reference group) with adjustments for education, age, smoking (never, past, or current), BMI, and hormone-replacement therapy (ever or never). As noted previously, the findings from this study might be vulnerable to selection bias because of the low overall rate of response to the combination of the take-home survey and the follow-up interview.
Dennis et al. (2010) reported on 150 cases of cutaneous melanoma diagnosed after enrollment in the AHS of pesticide applicators who completed both the enrollment form and the take-home questionnaire during phase I, excluding 24,704 who had a cancer diagnosis before enrollment. Cases were identified through linkage to cancer registries, state death registries, and the NDI with a cutoff date of December 31, 2005. Dichotomous measures (ever or never used) were used for arsenic pesticides (lead arsenate and inorganic and organic arsenic). Categorical measures (no, low, or high) based on intensity-weighted lifetime days of exposure were used for other chemicals, including 2,4-D, 2,4,5-T, and 2,4,5-TP. Unconditional logistic regression was used to estimate the association between melanoma and exposure with adjustments for age, sex, and other variables “as indicated” (apparently selection through an unspecified variable selection procedure), including sun exposure, tendency to burn, red hair, and BMI.
Thomas et al. (2010) reported on a monitoring study of 2,4-D and chlorpyrifos exposures in a sample of AHS participants. For 69 2,4-D applicators, the geometric mean values were 7.8 and 25 mg/L in pre-application and postapplication urine, respectively (p < 0.05 for the difference), and 0.37 mg/m3 in personal air. The estimated amounts of dermal absorption through the hands (hand loading) and through total skin surface (body loading) were 0.39 mg and 2.9 mg of 2,4-D, respectively; the readings for individual applicators were correlated across these media. Glove use and the mode of application were found to be associated with the degree of exposure.
Slager et al. (2009) reported on current rhinitis in commercial pesticide applicators in the AHS (excluding private applicators, such as farmers). Of the 4,916 commercial pesticide applicators in the full AHS cohort, the 2,245 who provided information on all the variates in the analysis model constituted the sample for this investigation. Current rhinitis was ascertained with the following question in the take-home questionnaire: “During the past 12 months have you had a stuffy,
itchy, or runny nose?” Exposure to individual pesticides was specified both as a dichotomous measure (ever versus never in the preceding year) and as a categorical measure (days per year). Logistic regression was used to estimate the association between exposure and current rhinitis, with adjustments for age, education, and having grown up on a farm. As noted previously, the findings from this study might be vulnerable to selection bias because of the low rate of response to the take-home survey (46 percent by commercial applicators, slightly higher by the entire AHS cohort).
Crawford et al. (2008) reported on hearing loss in white male licensed pesticide applicators in the AHS, under the hypothesis that some pesticides are neurotoxic and could potentially affect hearing. The study sample consisted of participants who completed the enrollment form and the take-home questionnaire during phase I and the follow-up telephone interview during phase II. Hearing loss was ascertained with the following question in the phase II interview: “Do you have trouble with your hearing in one or both ears (this is without a hearing aid)?” Potential cases of hearing loss attributable to a congenital condition or to infection or injury (determined by responses to survey questions) were excluded. The analysis also excluded participants who reported never using pesticides and excluded nonwhite and female respondents. Of the 16,246 participants who completed all three surveys, 14,229 were retained in the final analysis sample. Logistic regression was used to estimate the associations between exposure and hearing loss with adjustments for state, age, and exposures to noise, solvents, and metals. The overall low rate of response (less than 30 percent) to the combination of the three surveys raises concerns about the validity of the study findings. The authors argued that there were too few nonwhites and females (1.5 percent of eligible participants) for analysis. Although it might be reasonable to consider those participants to be too few to be analyzed as subgroups, it is unclear why they needed to be excluded from the main analysis. (Limited analysis for nonwhites is mentioned in the discussion.)
Although health outcome results in the whole cohort or entire subgroups are not fully relevant for the COIs and might be regarded as of marginal interest to more recent VAO committees, Blair et al. (2005b) reported that 2,4-D is the pesticide most frequently used by the Iowa famers and is often used by the rest of the applicators. Consequently, the results on the relative rates of individual conditions seem comparable in exposure specificity with findings in production cohorts in which not all of the workers included were necessarily exposed to the COIs and may have had additional toxic exposures. Therefore, the findings on mortality from enrollment through 2000 (Blair et al., 2005a) and on cancer incidence through 2002 (Alavanja et al., 2005) have been retained in the results tables for health outcomes were added. Accordingly, mortality findings through 2007 on various causes of death (Waggoner et al., 2011) and comparisons with state populations for cancer incidence updated through 2006 (Koutros et al., 2010a) to the health-outcomes results tables. Conventional SMRs and SIRs were
calculated with adjustment for age, calendar year, race, sex, and state. In an effort to compensate for the pronounced healthy worker effect evident in the AHS cohorts, both Waggoner et al. (2011) and Koutros et al. (2010a) also calculated, in addition to conventional SMRs and SIRs, “relative” counterparts of these statistics—rSMR and rSIR, respectively. To obtain the relative rates, the standardized ratio for incidence or mortality was divided by the standardized ratio for all causes excluding it. Because even the usual SMRs and SIRs from these non-pesticide specific findings on the entire cohort are minimally informative, the committee opted not to consider the relative versions.
Waggoner et al. (2011) reported 4,880 deaths in the applicators (private and commercial) and 1,539 in the spouses, significantly fewer than expected for both (SMR = 0.54, 95% CI 0.52–0.55; and SMR = 0.52, 95% CI 0.50–0.5). Similarly, the deaths from all types of cancer were significantly lower than the state rates in both applicators (SIR = 0.61, 95% CI 0.58–0.864) and spouses (SIR = 0.65, 95% CI 0.60–0.70). Koutros et al. (2010a) found 4,316 cancer cases in the private applicators, 219 in the commercial applicators, and 1,896 in the spouses. Findings on the commercial applicators were set aside, and the cancer incidence rates in both the private applicators (SIR = 0.85, 95% CI 0.83–0.88) and the spouses (SIR = 8.2, 95% CI 0.79–0.86) were again significantly lower than expected.
Several recent AHS publications (Andreotti et al., 2012; Barry et al., 2011, 2012; Koutros et al., 2010b, 2011) reported on a nested case-control substudy that examined the relationship of pesticide exposure (including herbicides of interest, such as 2,4-D and 2,4,5-T) and of genetic markers with the risk of prostate cancer. All men eligible for inclusion in the study were white applicators who had not had any cancers other than non-melanoma skin cancers before enrollment in the AHS and who had provided a buccal-cell sample. Two controls matched on age to each case had to have been alive at the time of the case’s diagnosis. The final study sample consisted of 776 prostate-cancer cases diagnosed in 1993–2004 and 1,444 controls. Although the primary focus of this substudy was the interaction between pesticide exposure and genetic markers (how pesticide exposure modified the association between genetic markers and prostate cancer), some useful information about the association between exposure to particular pesticides and prostate cancer can still be gleaned as a byproduct of the interaction analyses. Intensity-weighted lifetime exposure days are used in Andreotti et al. (2012) and Barry et al. (2011, 2012). Genotyping for an array of 26,512 single-nucleotide polymorphisms (SNPs) in 1,291 candidate genes was performed at the NCI’s Core Genotype Facility. Unconditional logistic regression was used to estimate ORs and 95 percent CIs for the associations between prostate cancer and the main effect for pesticide exposure, the main effect for genetic markers, and the interaction between pesticide exposure and genetic markers, adjusted for age and state. Only Koutros et al. (2011), who reported the findings for this substudy on 1,913 SNPs in 149 candidate genes known to play a role in the metabolism of xenobiotic substrates, also adjusted for a family history of prostate cancer and
provided main effects for exposure to individual pesticides and the incidence of prostate cancer. Koutros et al. (2010b) reported the findings on 211 SNPs in the 8q24 region known to be associated with prostate cancer. Andreotti et al. (2012) reported the findings on 220 SNPs in 59 genes involved in lipid metabolism. Barry et al. (2011) reported the findings on 394 SNPs in 31 base-excision repair genes involved in repairing oxidative DNA damage that are hypothesized to be possibly important for populations exposed to pesticides or other putative oxidative stress-inducing agents. Barry et al. (2012) reported findings on 324 SNPs in 27 nucleotide excision repair (NER) genes thought to be important in repairing damage induced by putative prostate carcinogens. The false discovery rate (Benjamini and Hochberg, 1995) method is used to account for multiple comparisons involving a large number of pesticides and genetic markers.
Tanner et al. (2011) conducted a case-control study of PD in AHS participants. Suspect cases (170) were identified from self-reports and state mortality files and confirmed (115; 110 with pesticide data included in study) by a neurologist during home visits. Potential controls (644) were sampled randomly from the AHS cohort and frequency-matched about 3:1 to cases by age, sex, and state. Controls were confirmed (383; 358 with pesticide data included in study) by a neurologist or a neurologist-trained technician during home visits. CATIs were used to obtain detailed information on use, since the age of 14 years, of 31 selected pesticides expected to be possibly associated with PD (oxidative stressors and mitochondrial inhibitors) as well as key covariate information, including smoking and family history of PD. Participant characteristics were compared between cases and controls by using Fisher’s exact test or Pearson’s chi-square test for categorical variables and Wilcoxon’s rank-sum test for continuous variables. Logistic regression was used for pesticides reported by at least 10 participants, controlling for potential confounding factors, including age, sex, state, and cigarette-smoking (ever or never).
Several recent AHS studies examined a variety of exposure issues. Blair et al. (2011) examined the effect of exposure misclassification, which is likely to occur when self-reported exposure assessment is used, on the relative risks estimated in the AHS and showed substantial attenuation toward the null. Similar results are likely for other studies that use self-reported exposure status. Coble et al. (2011) reported on an updated version of an estimation algorithm for pesticide exposure intensity, developed previously in Dosemeci et al. (2002) for the AHS, to incorporate new data obtained in two exposure-monitoring studies to modify the weighting factors used in the algorithm. Payne et al. (2012) conducted a Cox proportional-hazards regression to assess the risk posed by high pesticide exposure in the AHS cohort.
Since Update 2012, a large series of papers has been published from the AHS cohort. These are described briefly below, prioritizing first the health outcomes of most interest in light of evidence considered thus far by VAO committees. This includes an examination of the relationships between occupational pesticide
exposure (i.e., among pesticide applicators and their spouses) and risk of stroke, diabetes, Parkinson’s-related diseases, and hypothyroidism. More details on these individual health outcomes are provided in the individual chapters concerning health outcomes of interest to the committee.
Rinsky et al. (2013) examined the relationship between self-reported pesticide use provided by the male private and commercial pesticide applicators and stroke as an underlying or contributing cause of death based on ICD-9 and ICD-10 criteria. The composite set of 50 commonly used pesticides included 2,4-D, but the set of 22 pesticides for which individual analyses of lifetime frequency and duration of use did not include 2,4-D. Although additional information about stroke and the COIs would be of considerable interest, the relevance of this publication to the VAO task is minimal.
Starling et al. (2014) conducted an analysis of 13,637 farmers’ wives without a history of diabetes who reported ever personally mixing or applying any pesticides before enrollment in the AHS. At enrollment, the women were asked to report the number of years and average number of days per year that they personally mixed or applied any pesticides or herbicides. The herbicides 2,4,5-T and 2,4,5-TP were combined into a single variable because of their similar chemical structures and similar use patterns in the cohort and because both contained dioxin at some points in time. A total of 45 pesticides were examined for possible association with incident diabetes among study women over a 10-year follow-up period. With respect to the COIs, picloram, cacodylic acid, and TCDD were not examined. Analyses were adjusted for the state of residence and body mass index at enrollment. During the follow-up period, 5 percent of women reported development of diabetes. Whereas exposure assessment is based on self-report, two strengths of this analysis are that the ascertainment of exposure history included a specific examination of 2,4,5-T and 2,4,5-TP combined and that the incident development of diabetes (by self-report) was prospectively ascertained.
Kamel at el. (2014) examined the association between dietary fat intake, pesticide use, and Parkinson disease. A nested case-control design (within the AHS) was used whereby self-reported levels of dietary fat intake, specifically consumption of monounsaturated, polyunsaturated, and saturated fats, and pesticide use were compared between 89 confirmed cases of PD versus 336 control subjects frequency-matched by age, gender, and state and who did not develop PD. Dietary fat intake was assessed using the Diet History Questionnaire version I, a self-administered 144-item food frequency questionnaire developed by the NCI. Analyses were adjusted for age, gender, state, smoking, and total energy. The applicability of the analysis in addressing the committee’s charge is severely limited because the study evaluated the pesticides paraquat and rotenone and pesticides similar to the Vietnam veteran COIs and also because it focused on interaction with dietary fat intake, which is not germane to the experience of Vietnam veterans.
Goldner et al. (2013) examined the association between use of 50 specific pesticides and self-reported hypothyroidism, hyperthyroidism, and “other” thyroid disease among 22,246 male pesticide applicators. The approach was very similar to earlier analyses done on females spouses (Goldner et al., 2010). The relationship between exposure and response was assessed on the basis of intensity-weighted cumulative days of use. Specifically, the exposure distribution for each pesticide was split at the median value of intensity-adjusted cumulative days of use among users to create a three-level variable categorized as no exposure (zero days of use), low exposure (median or less), or high exposure. Comparisons of the history of thyroid disease between the three groups in relation to pesticide use were adjusted for age, education, and BMI at enrollment. During follow-up, 2 percent of pesticide applicators reported a history of hypothyroidism, 1 percent reported a history of hyperthyroidism, and 1 percent reported a history of other thyroid disease. A strength of this analysis is that separate risk estimates were calculated for self-reported use of 2,4-D and 2,4,5-T, chemicals of direct interest to Vietnam veterans, and for the chemically related herbicides 2,4,5-TCP and dicamba. A significant limitation of this analysis is that the assessment of thyroid disease was based on a lifetime history of disease because thyroid disease was not reported at baseline and information on age of diagnosis was incomplete at follow-up. Thus, this analysis is based on the untested and unconfirmed assumptions that essentially all reports of thyroid disease at follow-up assessments were incident cases, and that the prevalence of thyroid disease at study entry did not differ between the pesticide exposure groups.
In addition to the recently published studies from the AHS that relate specifically to health outcomes of interest among Vietnam veterans, Hou et al. (2013) examined the relationship between self-reported lifetime pesticide-use days and intensity-weighted lifetime pesticide use (log-transformed) and relative telomere length among 1,234 cancer-free white male pesticide applicators in the AHS. For purposes of the analysis, pesticide exposure was classified into four categories consisting of none, low, medium, and high. The rationale for the investigation of telomere length is based on human epidemiologic investigations that suggest that telomere length in surrogate tissues (blood or buccal cells) may be associated with some cancers. The 48 pesticides examined were grouped into seven classes of pesticides, with one group of interest consisting of 2,4-D. A strength of this analysis is that the outcome measure, relative telomere length, is biologically based and not based on self-report. On the other hand, the direct relevance of relative telomere length to the specific outcomes of interest to Vietnam veterans is unknown, particularly because studies are inconsistent as to the extent to which telomere length reliably predicts an elevated risk of cancer development of various types. The fact that self-reported exposure to 2,4-D as a class of pesticides was included in the analysis is considered a strength of this study.
Karami et al. (2013) evaluated interactions between 41 pesticides and 152 SNPs involved in nine vitamin-D pathway genes among 776 prostate cancer cases
diagnosed between 1993 and 2004 and 1,444 male controls in a nested case-control study of Caucasian pesticide applicators within the AHS. The method of estimating pesticide exposure matched that of Hou et al. (2013) (described above) and included self-reported lifetime pesticide-use days and intensity-weighted lifetime pesticide use (log-transformed). These quantities were then grouped into three categories consisting of none, low (median level or below), and high (above the median level). The identification of nine vitamin D–associated candidate genes was done with standard genotyping methods. In supplementary analyses, main effects of 2,4-D and 2,4,5-T were examined in relation to their association with prostate cancer. Whereas the purpose of this study was to investigate pesticide and gene interactions with respect to risk of prostate cancer, strengths of this study are that main effects of some of the COIs to the Vietnam-veteran population were examined and that the occurrence of prostate cancer was based on clinical diagnoses.
In an earlier, similar analysis of the risk of prostate cancer, Barry et al. (2012) evaluated interactions between pesticide exposure among white pesticide applicators and 324 SNPs tagging 27 nucleotide excision repair genes among 776 prostate cancer cases and 1,444 male controls using a nested case-control design in the AHS. As with Karami et al. (2013), prostate cancer cases were diagnosed between the years 1993 and 2004 and after enrollment in the AHS. For exposure assessment, lifetime days and intensity-weighted lifetime days of application for each pesticide were categorized into a three-level ordinal-valued variable consisting of none, low, and high with the low and high categories distinguished by the median value among exposed controls. Whereas 2,4-D was one of the many different pesticides assessed, it was only analyzed as an interaction with the DDB1 gene and not as a main effect. Thus, this study was deemed of very limited value to evaluating the relationship between 2,4-D and the risk of prostate cancer.
Alavanja and Bonner (2012) conducted a lengthy review of the epidemiological literature linking pesticides (including 2,4-D) to cancers in occupational studies worldwide, with a particular focus on those articles published after the release of IARC Monograph 53 (1991): Occupational Exposures in Insecticide Applications and Some Pesticides. Given the time span, and the fact that this paper was a review article and not a new data-based analysis, it was deemed of very little value by the committee other than the authors’ conclusions on the potential relationships between occupational pesticide exposure and different types of cancer. Moreover, a very similar published review article on the same subject by Alavanja et al. (2013a) was deemed of tangential value to the committee charge, as was a corresponding letter by Gray et al. (2013) to the Alavanja et al. (2013a) review, as well as the subsequent reply to Gray et al. (2013) by Alavanja et al. (2013b).
Finally, by use of the AHS, Heltshe et al. (2012) presented methodological work on the ability to use multiple imputation to assign pesticide use values for nonresponders (missing data) in the AHS follow-up questionnaire. Although
academically of interest, the paper did not provide any meaningful evidence to evaluate with respect to the charge of the committee.
California United Farm Workers of America Study
Mills and Yang (2005) and Mills et al. (2005) analyzed lymphohematopoietic cancers and breast cancer, respectively, in nested case-control studies of Hispanic workers drawn from a cohort of 139,000 Californians who were members of the United Farm Workers of America (UFW). Estimates of exposure to specific pesticides, including 2,4-D, were developed through a linkage of the union’s job histories with the California Pesticide Use Reporting Database of the state’s Department of Pesticide Regulation, which has records of all agricultural applications of pesticides in the state since 1970. Vital status and cancer incidence were ascertained through a probabilistic record linkage to the California Cancer Registry for the period 1988–2001. Mills and Yang (2007) conducted a nested case-control gastric cancer study embedded in the UFW cohort and identified cases of gastric cancer newly diagnosed in 1988–2003.
No reports relevant to the COIs have been published on the California UFW population since Update 2008.
Other US Studies of Agricultural Workers
Studies of proportionate mortality were conducted among Iowa farmers (Burmeister, 1981) and male and female farmers in 23 states (Blair et al., 1993). Mandel et al. (2005) reported the results of urinary biomonitoring of farm families in Minnesota and South Carolina as a part of CropLife America’s Farm Family Exposure Study. Curwin et al. (2005) measured 2,4-D concentrations in urine and hand-wipe samples to characterize exposures of farmers and non-farmers in Iowa.
Studies in Other Countries
Australian Herbicide-User Studies
Fritschi et al. (2005) used CATIs and occupational histories reviewed by an industrial hygienist to estimate exposures to phenoxy herbicides in an Australian study.
Canadian Herbicide-User Studies
The Ontario Farm Family Health Study (OFFHS) has produced several reports on exposure to phenoxyacetic acid herbicides, including 2,4-D. A study of male pesticide exposure and pregnancy outcome (Savitz et al., 1997) developed
an exposure metric based on self-reports of mixing or application of crop herbicides, crop insecticides, and fungicides; livestock chemicals; yard herbicides; and building pesticides. Study participants were asked whether they participated in those activities during each month, and their exposure classifications were based on activities in 3-month periods. Exposure classification was refined with answers to questions about the use of protective equipment and the specificity of pesticide use.
A related study included analysis of 2,4-D residues in semen as a biologic marker of exposure (Arbuckle et al., 1999a). The study began with 773 potential participants, but only 215 eventually consented to participation. Of the 215, 97 provided semen and urine samples for 2,4-D analysis.
The OFFHS also examined the pregnancy outcomes of stillbirth, gestational age, and birth weight (Savitz et al., 1997) and the effects of exposure to pesticides, including 2,4-D, on time to pregnancy (Curtis et al., 1999) and on the risk of spontaneous abortion (Arbuckle et al., 1999b, 2001). About 2,000 farm couples participated in the study. Exposure information was pooled from interviews with husbands and wives to construct a history of monthly agricultural and residential pesticide use. Exposure classification was based on a yes–no response for each month. Data on such variables as acreage sprayed and the use of protective equipment were collected but were not available in all cases. Other studies have used herbicide biomonitoring in a subset of the population to evaluate the validity of self-reported predictors of exposure (Arbuckle et al., 2002). Assuming that the presence of 2,4-D in urine was an accurate measure of exposure and that the results of the questionnaire indicating 2,4-D use were more likely to be subject to exposure-classification error (that is, assuming that the questionnaire results were less accurate than the results of urinalysis), the questionnaire’s prediction of exposure, compared with the urinary 2,4-D concentrations, had a sensitivity of 57 percent and a specificity of 86 percent. In multivariate models, pesticide formulation, protective clothing and gear, application equipment, handling practice, and personal-hygiene practice were valuable as predictors of urinary herbicide concentrations in the first 24 hours after application was initiated.
Urinary concentrations of 2,4-D and MCPA were measured in samples from farm applicators (Arbuckle et al., 2005) and from women who lived on Ontario farms (Arbuckle and Ritter, 2005). Potential indirect sources of farm families’ herbicide exposure were evaluated through wipe sampling of surfaces and samples of drinking water (Arbuckle et al., 2006). Weselak et al. (2008) examined occupational exposures and birth defects in the offspring of OFFHS participants. Spouses completed questionnaires that requested the history of pesticide use on the farm. Pregnancies resulting in birth defects were reported by the female study participants. All birth defects were combined for study analyses, and exposure was examined by pesticide class, family, and active ingredient for two 3-month periods—before and after conception.
No reports on the OFFHS relevant to the COIs have been published since Update 2008.
The Canadian Farm Operator Study assembled a cohort of 156,242 male farmers from 1971 Canadian census data on the provinces of Manitoba, Saskatchewan, and Alberta and linked to the national mortality database to identify deaths occurring during the period June 1971–December 1987. The cohort was also matched to the Central Farm Registers for 1966, 1976, 1981, and 1986 to gather information on reported exposures and farm practices. Information on the amount of acreage on each farm sprayed in 1970 with herbicides (without product specificity) was used as surrogate for its operator’s exposure in determining the risk of specific causes of death: NHL (Morrison et al., 1994; Wigle et al., 1990), prostate cancer (Morrison et al., 1993), brain cancer (Morrison et al., 1992), multiple myeloma (Semenciw et al., 1993), and leukemia (Semenciw et al., 1994). In the one-third sample that completed the census long form, the people most likely to have been exposed (no employees or custom expenses reported) could be identified. The age at which years at risk began to accumulate for each person varied for the various causes of death assessed, which resulted in different numbers of eligible subjects. No reports on relevant health outcomes have been published on participants in this study population since Update 1996.
Other Canadian Studies of Agricultural and Forestry Workers Faustini et al. (1996) evaluated the immune, neurobehavioral, and lung function of residents in an agricultural area of Saskatchewan, Canada, and focused on immunologic changes in 10 farmers who mixed and applied commercial formulations that contained chlorophenoxy herbicides. Studies have been conducted in forestry workers who were potentially exposed to the types of herbicides used in Vietnam. A cohort mortality study examined men employed by a Canadian public utility (Green, 1987, 1991). Senthilselvan et al. (1992) investigated asthma’s relationship to pesticide use with self-reported data gathered in a cross-sectional survey completed by 1,939 of the 2,375 male farmers approached in Saskatchewan. Mortality and reproductive effects have been studied in British Columbia sawmill workers potentially exposed to chlorophenate wood preservatives used as fungicides (Dimich-Ward et al., 1996; Heacock et al., 1998; Hertzman et al., 1997); PCP, which would be a frequently used fungicide, is expected to have dioxin and furan contamination, but the 2,3,7,8-TCDD congener is unlikely to have been present.
Danish Herbicide-User Studies
Records of the Danish Union of General Workers for 10 trade unions of gardeners were used to identify 3,156 male members on May 1, 1975; 859 women were also identified. The workers were known to be highly exposed to pesticides.
Most of the women worked in greenhouses, where herbicides are not routinely used; for the men, however, exposure was mainly to herbicides, which included the phenoxy herbicides 2,4-D, 2,4,5-T, and MCPA. Matching of union records to the Danish Central Population Registry permitted the establishment of the vital status of the entire cohort through 1984 for a determination of person-years at risk; this provided for a latent period of 10–15 years by starting accumulation when people reached the age of 30 years. Using the Danish Cancer Registry, Hansen et al. (1992) determined the cancer incidence in this cohort of Danish gardeners from 1975 to 1984 and compared it with the general Danish population and adjusted for age, sex, and calendar period.
Hansen et al. (2007) used analogous methods to extend the follow-up period for the men through 2001. The updated information was analyzed by using year of birth as a surrogate for intensity of exposure, with high exposure assumed for those born before 1915, low exposure for those born in 1934 or later, and intermediate exposure for those born in between.
Drawing from the same cohort of Danish gardeners and further stipulating that people must have been alive and living in Denmark at the beginning of 1977, Kenborg et al. (2012) established a cohort of 3,124 men who were monitored in the Danish Hospital Register for hospitalization for PD as a primary diagnosis from 1977 through 2008 and compared the results with the observed incidence of PD in all Danish men by calendar period and age group. Revisiting the Danish Cancer Registry, they also investigated the incidence of lung, larynx, and bladder cancers, which are recognized as smoking-related. The incidence of those cancers was compared by age and calendar period with the incidence in the general male Danish population, and the rates were used as a proxy for smoking frequency in the cohort. The birth cohorts defined by Hansen et al. (2007) were used again to stratify degree of exposure.
Ronco et al. (1992) studied mortality in Danish farmers. The utility of the findings was limited by their being largely unanalyzed products of linking the country’s cancer registry with census records to garner information on recent occupation.
Dutch Herbicide-User Studies
A Dutch study of forestry workers exposed to 2,4,5-T investigated the prevalence of acne and hepatic dysfunction (van Houdt et al., 1983). No reports on forestry workers have been published since 2000.
Mortality from cancers and other causes in Dutch male herbicide applicators has been studied by Swaen et al. (1992, 2004).
Finnish Herbicide-User Studies
Asp et al. (1994) conducted a follow-up through 1989 on mortality and cancer morbidity in Finnish men who had applied 2,4-D and 2,4,5-T for at least 2 weeks in 1955–1971. This group of 1,971 was assembled in 1972 from records of
the four Finnish employers primarily responsible for brush removal and assessed for mortality through 1980 (Riihimaki et al., 1982) and for cancer morbidity (Riihimaki et al., 1983) through 1978.
German Herbicide-User Studies
Barthel (1981) studied cancer incidence overall mortality from 1970 through 1978 in 1,658 male agricultural plant-protection workers in the former German Democratic Republic who spent a portion of at least 5 years in 1948–1972 applying pesticides. Unlike most of the many pesticides thought to have contributed to the exposure of these workers, the phenoxy herbicides were available for use throughout this period. It was not known, however, which individuals used the COIs, so exposure characterization was not as specific as current VAO committees require for results to be considered fully relevant. Among the cancers, only lung cancer had a large enough number of cases to permit an analysis by the amount and time period of pesticide use.
Iceland Herbicide-User Studies
Using the national cancer and death registries, Zhong and Rafnsson (1996) determined cancer incidence from entry into a pesticide-using occupation through 1993 for 2,449 men and women in Iceland. A ranked listing of the amount of specific pesticides sold for agricultural use in Iceland between 1976 and 1993 was led by 2,4-D, but the listing did not specify which of these pesticides individual subjects had been exposed to, so the results of this study do not constitute fully relevant evidence according to the criteria of recent VAO committees.
Italian Herbicide-User Studies
Ronco et al. (1992) also studied the incidence of specific types of cancer in Italian farmers. The utility of the findings was limited by their being the largely unanalyzed products of linking the country’s cancer registry with census records to garner information on recent occupation.
Cancer mortality in a cohort of rice growers in the Novara Province of northern Italy was investigated by Gambini et al. (1997).
A cohort of male farmers in Italy’s southern Piedmont region who were licensed to use agricultural pesticides in 1970–1974 was established. The use of phenoxy herbicides in the area was reported to be twice the national average. Corrao et al. (1989) evaluated cancer incidence in 25,945 on the basis of new diagnoses from hospital admissions in 1976–1983. In a continuation of that study, Torchio et al. (1994) reported on mortality through 1986 in the 23,401 who were residents of the Piedmont area at the time of registration; the cause of death was abstracted from death certificates. The cohort was partitioned into people who
lived near arable land, those who lived near woodlands, and those who lived near mixed-use land; separate results were reported for the first two groups. No reports on this cohort have been published since 1994.
New Zealand Herbicide-User Studies
A study evaluated cancer incidence in a group of New Zealand forestry workers (Reif et al., 1989). No reports on forestry workers have been published since 2000. ’t Mannetje et al. (2005) evaluated a study population that included herbicide production workers and was a subcohort of the IARC cohort.
Norwegian Herbicide-User Studies
Kristensen et al. (1997) tested whether cancers or birth defects were increased in the offspring of Norwegian farmers who worked on farms with pesticide use documented by agricultural censuses.
South American Herbicide-User Studies
Lerda and Rizzi (1991) studied the incidence of sperm abnormalities in Argentinean farmers. The utility of the findings was limited by their being the largely unanalyzed products of linking each country’s cancer registry with census records to garner information on recent occupation.
Swedish Herbicide-User Studies
The Swedish Cancer-Environment Register (CER) linked the cancer cases entered in the Swedish Cancer Registry with the records of people who responded to the 1960 and 1970 national censuses, which had obtained data on current occupation. The resulting database has been used in studies that evaluated cancer mortality and farm work (Wiklund, 1983); STS and malignant lymphoma in agricultural and forestry workers (Wiklund and Holm, 1986; Wiklund et al., 1988a); and the risk of NHL, HL, and multiple myeloma in relation to occupational activities (Eriksson et al., 1992). No new studies using the Swedish CER that are relevant to the COIs have been published since the original VAO report.
Cancer mortality in Swedish railroad workers has been studied (Axelson and Sundell, 1974; Axelson et al., 1980). Another study examined mortality and cancer incidence in a cohort of Swedish lumberjacks (Thörn et al., 2000). Cancers in Swedish pesticide and herbicide applicators has been studied repeatedly (Dich and Wiklund, 1998; Wiklund et al., 1987, 1988b, 1989a,b).
Other Studies of Workers Using Herbicides
Other studies of the agricultural use of pesticides have not provided specific information on exposure to 2,4-D, TCDD, or other compounds relevant to Vietnam veterans’ exposure (Bell et al., 2001a,b; Chiu et al., 2004; Duell et al., 2001; Garry et al., 2003; Gorell et al., 2004; Hanke et al., 2003; van Wijngaarden et al., 2003).
A series of papers from a workshop focused on methods of assessing pesticide exposure in farmworker populations (Arcury et al., 2006; Barr et al., 2006a,b; Hoppin et al., 2006b; Quandt et al., 2006). They provide a helpful review of current methodologic issues in exposure science for those populations but do not address the COIs directly.
ENVIRONMENTAL STUDIES
Industrial accidents have led to the evaluation of long-term health effects in non-worker populations that live near areas with fairly high environmental concentrations of the COIs. Effects on residents around normally performing industrial operations, such as waste incinerators, and even on people exposed only to “background” concentrations have also been studied. We note that the systematic follow-up studies that have been conducted on the Seveso population and the numerous analyses of the large database generated by the continuing US NHANES contributed prominently to the evidence base considered by VAO committees.
People’s environmental exposures to dioxin-like chemicals and their non–dioxin-like counterparts are to mixtures of components that tend to correlate, so it is not surprising that specific chemicals measured in a person’s serum also tend to correlate; this collinearity means that it is difficult for epidemiologic studies to attribute any observed association to a particular chemical configuration (Longnecker and Michalek, 2000). Analyses in terms of TEQs circumvent that problem, to some extent.
Environmental studies are presented below alphabetically by country.
Belgian Environmental Studies
From the Flemish Environment and Health Study (2002–2006), Delvaux et al. (2014) evaluated relationships between prenatal exposure to endocrine disrupting chemicals (EDCs, including dioxins) and anthropometric measures of height, weight, waist circumference, and skin folds at 7–9 years of age. The sample included 114 Flemish children with analyses adjusted for maternal BMI, age of the mother, smoking of mother during pregnancy, parental education level, and lipid content, and age and gender of the child. The strengths of this study include the objective measurement of dioxin TEQs from cord/blood samples at birth and the anthropometric measures of child development. Its limitations include only
its potential relevance to female Vietnam veterans with pregnancy subsequent to military service and the evaluation of anthropometric outcome measures among children with unknown long-term clinical significance.
Danish Environmental Studies
Halldorsson et al. (2009) studied the association between consumption of fatty fish, as a source of environmental exposure to dioxins and dioxin-like chemicals, and birth weight and development in 100 healthy pregnant women 25–35 years old selected from the Danish National Birth Cohort, which includes 101,046 women (Olsen et al., 2001). The 9,815 eligible women were stratified according to the frequency of fatty-fish intake (low, zero meals per month; medium, one to three; and high, more than three); 34, 33, and 33 were randomly sampled in three strata, respectively. Four standardized CATIs (at gestation weeks 12 and 30 and at 6 and 18 months postpartum) were used to collect information on parental lifestyle and health. Participants received a food-frequency questionnaire in week 25 of gestation, and two maternal blood samples were collected during routine visits to a general practitioner. The blood samples were analyzed for CALUX-TEQs in pg/g of lipid. Birth outcomes (weight, length, and head circumference) based on measures performed by the midwives who attended the births were extracted from the Danish National Birth Registry. Developmental milestones (such as sitting without support and crawling) were obtained from the telephone interviews conducted when the children were 5.7–7.0 months old. A total-development scale was derived by summing the indicators of 13 milestones. Linear mixed models (with the multiple plasma samples specified as an individual-level random effect) were used to estimate the association between CALUX-TEQ and birth weight with adjustments for gestational age, infant sex, and maternal smoking. Logistic regression was used for the association between CALUX-TEQ (dichotomized into high and low relative to the sample median) and infant development milestones, with adjustments for gestational age, duration of breastfeeding, infant age at interview, and maternal fish intake. Spearman rank correlation was used for the association between CALUX-TEQ and the total-development scale.
Wohlfahrt-Veje et al. (2014) examined the relationships between polychlorinated dibenzo-p-dioxins, furans, and biphenyls (PCDDs/PCDFs and PCBs), quantified as TEQs in breast milk samples, and measures of early childhood growth and serum insulin-like growth factor (IGF) levels. The sample consisted of 418 Danish children (born 1997–2001) followed longitudinally for measures of height, weight, BMI, and skinfold percentage at 0, 3, 18, and 36 months of age. Measures of IGF were obtained at 3 months. Separate estimates were provided for TCDD. The strengths of this study include an objective measurement of COIs to Vietnam veterans and anthropometric measures of infant development. Limitations include only its potential relevance to female Vietnam veterans with
pregnancy subsequent to military service and the evaluation of anthropometric outcome measures among infants with unknown long-term clinical significance.
Dutch Environmental Studies
Since Update 2012, de Jong et al. (2014) investigated relationships between pesticide and other occupational exposures and airwave obstruction in the Lifelines Cohort Study. The LifeLines cohort study is a multidisciplinary prospective population-based cohort study examining health and health-related behaviors of persons living in the northern region of The Netherlands. For the present analysis, the sample included 11,851 subjects who completed a baseline questionnaire and received a medical examination that included prebronchodilator spirometry to measure airway obstruction and respiratory function. Presumed exposure to pesticides (subcategories of herbicides and insecticides) was based on job title and description of current or last job held, with exposure classification made by use of the International Standard Classification of Occupations and subsequent assignment of “non-exposed,” “low,” and “high” exposure. Multiple linear and logistic regression models were fit with adjustment for sex, age, height, weight, current/ex-smoking, and pack-years at enrollment. Analyses were also stratified by gender and smoking status. A significant limitation of this analysis is that pesticide exposure history was based on job classification and not objective measurements, and that individual dioxin-like pesticides relevant to Vietnam veterans were not examined.
In an unrelated analysis, ten Tusscher et al. (2014) reported on relationships between prenatal and lactational dioxin exposure and a range of neurodevelopmental parameters. This included longitudinal assessment of behavior and intelligence among 41 children at ages 7–12 years, measures of behavior in adolescence at ages 14–18 among 33 children of the original group, and neurophysiological measurements done at ages 7–12 years. Assessment of neurophysiological development was based on use of magnetoencephalography (MEG) and electroencephalography (EEG). Assessment of intelligence was based on use of the Dutch version of the Wechsler Intelligence Scale for Children (WISC-R) and behavioral questionnaires, and assessment of behavior was based on the Dutch version of the Child Behavior Checklist for ages 4–18 years (CBCL 4–18) and the Teacher Report Form (TRF). In addition, current levels of dioxins and dioxin-like PCBs were measured again in adolescence at ages 14–18. Strengths of this study include objective measurement of perinatal dioxin exposure and neurophysiological development. Limitations include a particularly poor overall description of study results and direct relevance only to childbearing Vietnam veterans.
Finnish Environmental Studies
Turunen et al. (2008) studied mortality in 6,410 fishermen and their 4,260 wives in Finland in comparison with national mortality figures (standardized by sex, age, and period), assuming that the difference in mortality reflected the high consumption of contaminated fish by fishermen and their wives. A small subsample (88 fishermen and 94 wives) participated in a substudy of fish consumption and life habit and provided blood samples that were analyzed for nutrients and environmental contaminants, including dioxins and PCBs. The substudy found higher fish consumption and higher serum dioxins and PCBs in fishermen and their wives than in the general population studied in the 2000 health survey. However, the validity of the findings of the mortality study is limited by various types of confounding factors, including the possible health benefits of fish consumption by fishermen and their wives and a possible healthy-worker effect in the cases of fishermen.
Turunen et al. (2012) derived total TEQs for 17 PCDD/F and 37 PCB congeners in blood samples from 123 men and 132 women from this population of fishermen and their wives. They also measured 11 risk factors for CVD, four indicators of carotid artery plaque, and C-reactive protein (CRP), a single marker of inflammation. These variables were analyzed with respect to tertiles of overall TEQs, after adjustments for age, smoking, physical activity, dietary factors, alcohol consumption, and medications. They found that fish consumption was associated with lowered CVD risk markers, whereas consumption of high levels of dioxin-like compounds appeared to mitigate this benefit.
French Environmental Studies
Viel et al. (2000) reported on an investigation of apparent clusters of cases of STS and NHL in the vicinity of a municipal solid-waste incinerator (MSWI) in Doubs, France. The presumptive source of TCDD in the region is an MSWI in the Besançon electoral ward in western Doubs. Dioxin emissions from the incinerator were measured in international TEQ units at 16.3 ng/m3, far in excess of the European Union (EU) standard of 0.1 ng/m3. TCDD concentrations in cow’s milk that were measured on three farms near the incinerator were well below the EU guideline of 6 ng/kg of fat, but the concentrations were highest on the farm closest to the incinerator. Floret et al. (2003) examined the same population and investigated rates of NHL in Besançon, France. Cases were identified from a cancer registry of people who had a diagnosis of NHL in 1980–1995. Viel et al. (2008a) examined the same population and reported a case-control study conducted in 434 women who had breast cancer compared with 2,170 community controls selected according to the proximity of their residence to emissions from the waste incinerator.
Viel et al. (2008b) expanded the previous work and studied the association between NHL and dioxin exposure from MSWIs in four French administrative departments (Isère, Bas-Rhin, Haut-Rhin, and Tarn), which were covered by a population-based cancer registry. (The study did not include the area of previous studies, Doubs, which is a separate administrative department.) The study was conducted with geostatistical analysis at the level of block groups, and it compared exposures and outcomes in the 2,270 block groups in the area. The block groups had an average area of 9.45 km2. The cases considered for this study were in people 15 years old and older who had received a diagnosis of NHL during the period 1990–1999 and who were living in the study area at the time of their diagnosis. Anonymous data were extracted from cancer registries on the date of birth, sex, date of diagnosis, address at the time of diagnosis, and cancer category. The block group for each case was geocoded by using the residential address.
A second-generation Gaussian atmospheric-dispersion model (ADMS 3) was used to derive “immission” estimates (defined by the researchers as “the amount of pollutant reaching a particular location as a result of—and in contrast to—the emission coming out the chimney”) for dioxins, metals, and dusts in the area near each of 13 MSWIs operating in the study area. That involved a receptor grid of 200 m that was based on emission estimates for the MSWI, plant characteristics (chimney height and diameter, emission temperature, particle size, and density), topography indicators (roughness and relief), local meteorologic conditions, and so on. For each of the 2,270 block groups, the median of all immission estimates for receptors in the block group was used as the immission for the block group. For block groups under the plumes of multiple MSWIs, the sum of the immission estimates was used. A cumulative ground-level dioxin concentration estimate was derived for each block group by using the immission estimates transformed to account for the number of years that the plant had operated and the degradation rate in the soil. Poisson regression was applied at the block-group level to assess the association between the observed number of NHL cases in each block group and the dioxin concentration (with a square-root transformation) estimated for the block group and adjusted for population density, urbanization, socioeconomic level, airborne traffic pollution, and industrial pollution.
Since Update 2010, Viel et al. (2011) have reported a new case-control study of NHL in a study area consisting of three electoral wards (170,000 people) that contained the Besançon MSWI. Cases (53 eligible, 34 participated) were identified from the local university hospital. Controls (34) were matched 1:1, randomly selected from blood donors living in the area matched on sex, age (± 5 years), and date of blood draw (± 1 year); five refusals were replaced. A wide spectrum of organochlorines (OCs) was measured in a fasting blood sample drawn from each participant. Exact logistic-regression models were used to assess the association between NHL and exposure measures.
Cordier et al. (2004, 2010) studied the risk of birth defects attributable to environmental dioxins released from MSWIs in the Rhône-Alpes region (Lyon
and surrounding areas) in southern France. The studies partially overlapped the areas studied by Viel et al. (2008b). All three studies included the administrative department of Isère.
Cordier et al. (2004) conducted a geostatistical analysis at the level of communities (official municipalities), studying 2,872 communities, each with fewer than 50,000 residents. Birth defects during the study period, 1988–1997, were identified from a population-based birth-defects registry (the French Central-East Registry). Seventy MSWIs operated in the study region for at least a year during the study period. Immission scores were derived using a Gaussian plume model (POLAIR) for dioxin concentrations in kilometer grids within 10 km of the plants and using plant emission estimates, chimney heights, and local meteorologic data. For each community, the immission score at the geographic point with the highest population density was used as the contemporaneous exposure index for the community. (That is a bit different from the usual practice of using the population centroid for the community.) In addition, a cumulative exposure index was derived by multiplying the contemporaneous exposure index by the number of years that the plant was in operation. A total of 194 communities were classified as exposed, and the remaining 2,678 communities were classified as non-exposed. In the exposed communities, only births after the start of the MSWI were considered in the analysis. Poisson regression was used to derive the relative risk of congenital malformations, with adjustments for the year of birth, maternal age, department of birth, population density, average family income, and (when available) local road traffic.
Cordier et al. (2010) examined the same population with a case-control study in 2001–2003, comparing 304 infants who had urinary tract birth defects with a random sample of 226 population controls that were frequency-matched for infant sex and year and district of birth. Of the 353 cases identified in the birth-defects registry, 304 were located, and 187 were interviewed. The modest response rate (53 percent of all cases, although the authors claimed a higher response rate of 62 percent, excluding 49 cases not located) may compromise the validity of the study findings. The controls were recruited through CATIs that attempted to reach 3,000 telephone numbers in the region presumed to belong to families with children; this resulted in 226 control participants after 1,989 ineligible candidates were excluded. Exposure estimates for dioxins, furans, and metals in areas near each MSWI (in 100-m grids) were derived by using Gaussian modeling software (ADMS 3) that took into account emissions, plant characteristics (chimney height and diameter, emission temperature and speed, and distribution between gaseous and particulate phases), and local meteorologic conditions. Participants were classified as exposed or non-exposed; those exposed were further classified into above or below the median. Multiple logistic regression was used to estimate the association between dioxin exposure and urinary tract birth defects with adjustments for stratification variables (child’s sex and year and district of birth). Potential confounders were selected by using backward
selection, including community characteristics (population density, deprivation score, and industrial dioxin sources beside MSWIs), maternal age, parental geographic origin, educational level, employment status during pregnancy, treatment for chronic disease during the first trimester, folic acid supplementation, history of urinary tract birth defects in first-degree relatives, parity, obesity, tobacco and alcohol use during pregnancy, and environmental tobacco-smoke exposure.
Seveso, Italy
A large industrial accident that resulted in environmental exposure to TCDD was caused by an uncontrolled reaction during TCP production in Seveso, Italy, on July 10, 1976. The degree of TCDD contamination in the soil has been used extensively as a means of imputing exposures of members of the population. Three areas were defined on the basis of soil sampling: Zone A (556 people), the most heavily contaminated, from which all residents were permanently evacuated within 20 days; Zone B (3,920), an area of lower contamination that all children and women in the first trimester of pregnancy were urged to avoid during daytime; and Zone R (26,227), a region with some contamination in which the consumption of local crops was prohibited (Bertazzi et al., 1989a,b). The sample sizes differ among follow-up studies, presumably because of migration; the sample sizes given above were reported in Bertazzi et al. (1989b).
Cohort of Entire Exposed Population
Data on serum TCDD concentrations in Zone A residents have been presented by Mocarelli et al. (1990, 1991) and by CDC (1988e). In the 10 who had severe chloracne, TCDD concentrations were 828–56,000 ppt of lipid weight. In 10 without chloracne, TCDD concentrations were 1,770–10,400 ppt. TCDD was undetectable in all control participants but one. The highest of the concentrations exceeded any that had been estimated at the time for TCDD-exposed workers on the basis of backward extrapolation and a half-life of 7 years. Data on nearby soil concentrations, the number of days that a person stayed in Zone A, and whether local food was consumed were considered in evaluating TCDD. That none of those data correlated with serum TCDD suggested strongly that the important exposure was from fallout on the day of the accident. The presence and degree of chloracne correlated with TCDD. Adults seemed much less likely than children to develop chloracne after acute exposure, but surveillance bias could have affected that finding. Recent updates (Bertazzi et al., 1998, 2001) have not changed the exposure-assessment approach.
A number of studies of the Seveso population have used lipid-adjusted serum TCDD concentrations as the primary exposure metric (Baccarelli et al., 2002; Eskenazi et al., 2002a,b, 2003a, 2004; Landi et al., 2003). Fattore et al. (2003) measured the current air concentrations of PCDDs in Zones A and B and
compared them with measurements in a control area near Milan. The authors concluded that a release from PCDD-contaminated soil did not add appreciably to air concentrations in the Seveso study area. Finally, Weiss et al. (2003) collected breast milk from 12 mothers in Seveso to compare TCDD concentrations with those in a control population near Milan. The investigators reported that the TCDD concentrations in human milk from mothers in Seveso were twice as high as those in controls. The authors concluded that breastfed children in the Seveso area were likely to have higher body burdens of TCDD than children in other areas.
Several cohort studies have been conducted on the basis of the exposure categories. Seveso residents have had long-term follow-up of their health outcomes, especially cancers. Bertazzi and colleagues conducted 10-year mortality follow-up studies of adults and children who were 1–19 years old at the time of the accident (Bertazzi et al., 1989a,b, 1992), 15-year follow-up studies (Bertazzi et al., 1997, 1998), and a 20-year follow-up study (Bertazzi et al., 2001). Pesatori et al. (1998) also conducted a 15-year follow-up study to update non-cancer mortality. Consonni et al. (2008) reported on the 25-year follow-up (through 2001) vital status of residents (“present”) in the Seveso area and reference territory at the time of the Seveso accident and of immigrants and newborns (“non-present”) in the 10 years thereafter. Cause-specific mortality was determined for each zone, compared with that in the comparison cohort, and adjusted for presence at the accident, sex, age, and time since the Seveso accident.
In addition to a 2-year prospective controlled study of workers potentially exposed to TCDD during the cleanup of the most highly contaminated areas after the accident (Assennato et al., 1989a), studies have examined specific health effects associated with TCDD exposure in Seveso residents—chloracne, birth defects, and spontaneous abortion—as well as crude birth and death rates (Bisanti et al., 1980); the distribution of chloracne in Seveso children (Caramaschi et al., 1981); chemicals in the blood and urine of children who had chloracne (Mocarelli et al., 1986); chloracne and peripheral nervous system conditions (Barbieri et al., 1988); dermatologic and laboratory tests in a group of the children who had chloracne and in a group of controls (Assennato et al., 1989b); health status and TCDD concentrations in chloracne cases and non-cases recruited previously by Landi et al. (1997, 1998) and followed by Baccarelli et al. (2005a); hepatic enzyme–associated conditions (Ideo et al., 1982, 1985); abnormal pregnancy outcomes (Mastroiacovo et al., 1988); cytogenetic abnormalities in maternal and fetal tissues (Tenchini et al., 1983); neurologic disorders (Boeri et al., 1978; Filippini et al., 1981); cancers (Bertazzi et al., 1993; Pesatori et al., 1992, 1993); the sex ratio of offspring who were born in Zone A (Mocarelli et al., 1996); immunologic effects (Baccarelli et al., 2002); aryl hydrocarbon receptor (AHR)-dependent pathway and toxic effects of TCDD in humans (Baccarelli et al., 2004); effects of TCDD-mediated alterations in the AHR-dependent pathway in people who lived in Zones A and B (Landi et al., 2003); and NHL-related (14;18) translocation
prevalence and frequency in dioxin-exposed healthy people in Seveso (Baccarelli et al., 2006). Baccarelli et al. (2005b) reviewed statistical strategies for handling nondetectable readings or readings near the detection limit in dioxin-measurement datasets. They recommended that a distribution-based multiple-imputation method be used to analyze environmental data when substantial proportions of observations have nondetectable readings.
Baccarelli et al. (2008) reported on crude sex ratios, birth weight, and neonatal thyroid function for all births in 1994–2005 to women who were less than 18 years old at the time of the Seveso accident. Mocarelli et al. (2008) investigated TCDD’s effects on reproductive hormones and sperm quality in a comparison of 135 young men exposed to TCDD by the 1976 Seveso accident with 184 age-matched healthy men who lived outside the contamination zones. Both groups were divided into three categories that reflected their ages at the time of the Seveso accident: infancy to prepuberty (1–9 years), puberty (10–17 years), and adulthood (18–26 years).
Pesatori et al. (2008) investigated the incidence of pituitary tumors in the Seveso population (804 in Zone A, 5,941 in Zone B, and 38,624 in Zone R) compared with the reference population in the surrounding, noncontaminated area (232,745). The hospital discharge-registration system of the Lombardy Region (where the study area is) was used to identify incident cases of pituitary adenoma from 1976 through 1996. All relevant medical records were reviewed to confirm the diagnosis for each case. Risk ratios and 95 percent CIs were estimated by using Poisson regression and adjusting for age, sex, and calendar period and an assumed 10-year latent period for dioxin effects. Pesatori et al. (2009) reported on cancer incidence in a 20-year follow-up of the Seveso cohort covering the period 1977–1996. The study included all participants 0–74 years old who lived in the study area (723 in Zone A, 4,821 in Zone B, 31,643 in Zone R, and 181,574 in the reference zone) at the time of the accident. Participants who moved outside the study area were traced with a success rate of greater than 99 percent (Consonni et al., 2008). Emigration was homogeneous among zones and ranged from 4.7 percent to 6.7 percent. The difference in exposure among zones was corroborated by soil TCDD measurements, serum concentrations of TCDD, and TEQs. In the absence of a regionwide cancer registry, incident cancer cases were ascertained from the 120-hospital network of the Lombardy region, where the study area is located. Original medical records were examined to identify true cases, to retrieve diagnoses as accurately as possible, and to determine the dates of occurrence. The study covered malignant tumors at any site and benign tumors of liver, bladder, and central nervous system first diagnosed after the date of the accident. For cohort members who were not hospitalized or who emigrated outside Lombardy, cancer cases were identified solely from death certificates, so nonfatal incident cases were missed. Risk ratios and 95 percent CIs for Zones A, B, and R versus the reference zone were derived by using Poisson regression and adjusting for sex, age, and period.
Mocarelli et al. (2011) have reported on the sperm quality and hormone concentrations of sons born from March 1977 to January 1984 to women exposed to dioxin in Seveso (78 invited, 39 participated) compared with men of similar age and socioeconomic status whose mothers did not live in the dioxin-contaminated areas and who were recruited from healthy volunteer permanent blood donors (123 invited, 58 participated). The exposed group was exposed both in utero (39) and perinatally through breastfeeding (21). Mothers’ serum TCDD concentrations were measured by using serum samples collected in 1976–1977 and kept frozen since and extrapolated to the time of conception. The outcome measures included sperm concentration, total count, progressive motility, and total motility count based on semen samples and follicle-stimulating hormone concentration based on fasting blood sample. A general linear model was used to analyze sperm and hormone data—including exposure group, lactation class, and group × lactation interaction—adjusted for age, days in abstinence, smoking, chemical exposures, BMI, alcohol use, education level, and employment status. Scale transformations were taken on the outcome measures to achieve an approximate normal distribution and homoscedasticity. Although the study was carefully designed and implemented, the low response rate raises concerns about possible selection bias.
Seveso Women’s Health Study
The Seveso Women’s Health Study (SWHS) was undertaken to evaluate the association between individual serum TCDD concentrations and reproductive effects in women who resided in Seveso at the time of the 1976 accident. From a pool of 1,271 eligible women who were between infancy and 40 years old at the time of the accident, who had resided in Zone A or B, and for whom adequate serum remained from the samples collected shortly after the explosion, 981 were enrolled in the study group in 1996–1998. The fairly adequate 80 percent participation rate resulted from 17 women being lost to follow-up, 21 having died, 12 being seriously ill, and almost 250 refusing. All the women were interviewed by a nurse blinded to their exposure status, and a subset received gynecologic examinations. Medical records of those who reported ever having received a diagnosis of cancer were obtained and subjected to blind review by a pathologist. The stored samples were used for new TCDD analyses with improved analytic techniques that had become available in recent years.
As an initial step in the SWHS, Eskenazi et al. (2001) tested the validity of exposure classification by zone. Investigators measured serum TCDD in samples collected in 1976–1980 from 601 residents (97 in Zone A and 504 in Zone B). A questionnaire that the women completed in 1996–1998 included age, chloracne history, animal mortality in the vicinity, consumption of homegrown food, and the woman’s location at the time of the explosion. Participants did not know their TCDD concentrations at the time of the interview, but most knew their zones of residence. Interviewers and TCDD analysts were blinded to the participants’
zones of residence. The zone of residence explained 24 percent of the variability in serum TCDD. Adding the questionnaire data improved the regression model to the point that it explained 42 percent of the variability. Those findings demonstrate a significant association between zone of residence and serum TCDD, but much of the variability in TCDD concentration is still unexplained by the models. Warner et al. (2005) compared a chemical-activated luciferase-gene expression bioassay with a high-resolution isotope-dilution gas-chromatography mass-spectrometry assay to measure PCDDs, PCDFs, and PCBs in the serum of 78 women who resided near Seveso in order to determine average total dioxin-like chemical TEQs; similar results were obtained with the two methods.
The women enrolled in the SWHS were assessed for cancer incidence during the 20 years after the accident (Warner et al., 2002). A pathologist blinded to the women’s exposure status reviewed medical records of the 21 women who reported in their initial interview (conducted between March 1996 and July 1998) ever having received a diagnosis of cancer; 15 of these diagnoses were for breast cancer, so the analysis was limited to all cancers and to this cancer type. The remaining six cancers consisted of three cases of thyroid cancer, a melanoma, a kidney cancer, and an unspecified tumor. For each woman, the earliest post-accident blood samples with at least 0.5 mL remaining were analyzed for TCDD. The resulting readings were back-extrapolated to the time of the 1976 explosion, assuming a 9-year half-life, as derived from data obtained on Vietnam veterans in the AFHS (Pirkle et al., 1989). A Cox estimation of hazard ratios (HRs) was conducted by using those values and the women’s ages at diagnosis or when they were interviewed for the controls, and a test for trend was conducted over four exposure categories with partitions at 10, 20, and 44 TCDD ppt; the results for both tests were marginally significant for breast cancer (p = 0.05 and p = 0.07, respectively) and slightly weaker for all cancers. A broad spectrum of possible confounders was assessed, but they had to be tested individually in the model. The small number of cases observed was a consequence of the cohort’s being relatively small (981) and young at the time of interview (72 percent less than 50 years old).
Warner et al. (2011) added more than 10 years of observation on cancer incidence in the women in the SWHS, updating the borderline significant results for breast cancer published earlier (Warner et al., 2002) to cover the period from the 1976 explosion through 2009. Of the 981 women participating in the earlier study, 833 were located, alive, and willing to participate. They were reinterviewed, provided clinical measurements, and allowed access to medical records for confirmation; a subset was given bone-density tests. The average age was now 50.8 years. In the update, an additional 45 cancers had been diagnosed, for a total of 66 cases, of which 33 were breast cancers. Thyroid cancer was the next most prevalent with 7 cases, and the 15 other types of cancer observed had at most 3 cases. After adjusting for age at the time of the accident and for marital status, the risk of any cancers in association with lipid-adjusted, log-transformed
serum TCDD concentrations at the time of the accident was distinctly elevated (HR = 1.86. 95% CI 1.29–2.52). It was a small cohort, so the analyses that could be conducted were curtailed, but the availability of serum TCDD concentrations measured from blood samples gathered fairly soon after the single-substance accident (which minimizes uncertainty about what exposure had been experienced and reduces the need for back-extrapolation) contributes substantially to the value of the results.
A series of studies have examined the associations between serum TCDD and a variety of endpoints related to female reproductive functioning: menstrual cycle (Eskenazi et al., 2002a), endometriosis (Eskenazi et al., 2002b), pregnancy outcome (Eskenazi et al., 2003a), age at exposure to the accident (Eskenazi et al., 2004), age at menarche and age at menopause (Eskenazi et al., 2005), and age at menarche in women who were premenarcheal at the time of the explosion (Warner et al., 2004). Eskenazi et al. (2007) and Warner et al. (2007) examined the incidence of fibroids and ovarian function, respectively, in SWHS participants. Eskenazi et al. (2007) excluded women who had received a diagnosis of fibroids before 1976, leaving a total of 956 women for analysis. Fibroids were ascertained in 634 women by self-report, medical records, and ultrasonography. Analyses were adjusted for confounding by parity, family history of fibroids, age at menarche, current BMI, smoking, alcohol consumption, and education. Warner et al. (2007) studied menstrual function in SWHS participants who were 20–40 years old and not taking oral contraceptives; the evaluations included ultrasonography (96 women), serum hormone concentrations (87 women), and the occurrence of ovulation (203 women).
Eskenazi et al. (2010) examined the relationship between serum TCDD around the time of the accident and time to pregnancy (TTP) in 472 SWHS participants who had attempted pregnancy since the accident. In addition to other eligibility criteria for SWHS, participants were eligible for the study only if they were no more than 40 years old at the time of the accident. Nine women were excluded because of fertility-related problems, leaving 463 eligible women in the analysis sample. The main analysis was restricted to the 278 women who delivered live births that were not the results of contraceptive failure. Alternative analyses included various subsamples excluded in the main analysis. TTP for the first post-accident pregnancy was determined from responses in interviews conducted in 1996–1998 to the question “How many months did it take to become pregnant? In other words, for how many months had you been having sexual intercourse without doing anything to prevent pregnancy?” Women whose TTP was 12 months or more were classified as infertile. Initial serum TCDD concentrations at the time of the accident were measured in stored samples from 444 participants (431 collected in 1976–1977 and 13 collected in 1978–1981). For 19 participants with insufficient stored samples, new samples were collected in 1996 or 1997. For the 27 women with detectable post-1977 TCDD measurements, TCDD was back-extrapolated to 1976 using the Filser model (Kreuzer
et al., 1997). Initial serum TCDD concentrations were extrapolated to the time when each woman initiated her attempt to become pregnant; Kreuzer et al. (1997) used a toxicokinetic model for women 16 years old or younger at the time of the accident, and Pirkle et al. (1989) used a first-order kinetic model that assumed a 9-year half-life. The association between serum TCDD and TTP was assessed by using a Cox proportional-hazards model to estimate the fecundability ORs and 95 percent CIs. The association between serum TCDD and infertility was assessed by using multiple logistic regression. Both models were adjusted for maternal age, maternal smoking in the year before conception, parity, menstrual-cycle irregularity, oral-contraceptive use in the year before attempt, paternal age near the time of conception, and history of reproductive and endocrine conditions, including pelvic infection and thyroid or urogenital problems. A variety of sensitivity analyses were conducted to investigate the consistency of the study findings and to check for possible bias. Initial serum TCDD and extrapolated serum TCDD were specified as continuous variables on the logarithmic scale and as categorical variables. Since Update 2012, four additional publications from the SWHS were identified for review by the committee. Warner et al. (2013) reported on a total of 980 women with serum TCDD levels collected shortly after the 1976 Seveso chemical accident and with respect to future development of diabetes and the metabolic syndrome approximately 30 years after the accident. Analyses of serum TCDD levels were stratified by age at the time of the explosion (≤ 12 years versus > 12 years). A strength of this study is the prospective examination of serum TCDD levels in relation to the future development of diabetes. However, the analyses stratified by females ≤ 12 years of age are not relevant for inference with veterans who served in Vietnam.
Chevrier et al. (2014) examined TCDD concentrations collected from women in the Seveso cohort in 1976 (n = 981) and 1996 (n = 260) in relation to levels of total thyroxine, free thyroxine, free triiodothyronine, and thyroid-stimulating hormone, as measured in 1996 (n = 909) and 2008 (n = 724). Analyses were stratified by menarcheal status at the time of the Seveso explosion. A strength of this study is the biological measurement of TCDD levels at two different time points. Limitations include the fact that thyroid hormone levels (and disruption), in and of themselves, are not primary health outcomes of interest among Vietnam veterans. In addition, analyses stratified by females who were premenarche at the time of the explosion are not relevant for inference with veterans who served in Vietnam.
Eskenazi et al. (2014) examined the relationship between TCDD concentrations measured in 1996 and the bone mineral density of the spine and hip measured in 2008 by use of dual-energy X-ray absorptiometry (DXA) bone scan. Because this analysis was limited to women who were less than 20 years of age at the time of the Seveso explosion, and because bone mineral density is not a primary health outcome of interest among Vietnam veterans, this study was deemed of no practical value by the committee.
Wesselink et al. (2014) examined the risk of adverse pregnancy outcomes in relation to TCDD concentrations (1996) in the SWHS among 1,211 post–chemical explosion pregnancies through the 2008–2009 follow-up assessment. Birth outcomes examined included gestational age, pre-term delivery, and birth weight. Of note, only 35 percent of women in the analysis were age 21 or older at the time of explosion, thereby limiting inference of this work to female veterans who served in Vietnam.
Japanese Environmental Studies
From 2002 to 2006, Uemura et al. (2008a,b) assembled a stratified sample of 1,374 Japanese subjects 15–73 years old (627 men and 747 women) who represented urban, farming, and fishing areas of the entire country. The participants completed questionnaires on occupational, medical, smoking, and residential histories and height and weight. They also provided blood samples that were analyzed with isotope-dilution high-resolution gas chromatography–mass spectrometry for PCDDs, PCDFs, and dioxin-like PCBs. Uemura et al. (2008a) investigated the relationship of those chemicals with the prevalence of diabetes, defined as self-reported physician-diagnosed diabetes or the occurrence of plasma HbA1c greater than 6.1 percent as a predictor of fasting plasma glucose above 126 mg/dL. Uemura et al. (2008b) presented summary statistics on the serum concentrations of the individual chemicals in the blood of the study participants and on their distributions with respect to various demographic characteristics; the researchers also provided the results of log-transformed correlation analyses of all PCDDs and PCDFs combined, of all dioxin-like PCBs, and of total TEQ with total cholesterol, high-density lipoprotein, and triglycerides.
Uemura et al. (2009) conducted further studies of the same cohort and examined the association of body burdens of dioxins and related chemicals with the prevalence of metabolic syndrome, assessed by using a modification of the National Cholesterol Education Program Adult Treatment Panel III definition (NCEP, 2002) to accommodate the differences between Asian and Caucasian populations (Ko et al., 2005; Tan et al., 2004). In particular, participants were classified as having metabolic syndrome if they satisfied three or more of the following five criteria: BMI of at least 25 kg/m2 (rather than abdominal waist circumference), serum triglycerides of at least 150 mg/dL, serum high-density lipoprotein (HDL) under 40 mg/dL in men or under 50 mg/dL in women, systolic blood pressure of at least 130 mm Hg or diastolic blood pressure of at least 85 mm Hg or self-reported history of physician-diagnosed hypertension, and HbA1c of at least 5.6 percent (rather than fasting serum glucose) or a self-reported history of physician-diagnosed diabetes. Logistic regression was used to assess the associations between exposures (TEQs for PCDDs, PCDFs, and dioxin-like PCBs and total TEQs) and the prevalence of metabolic syndrome, both adjusted and not adjusted for age, sex, smoking and drinking habits, regional block, residential
area, and survey year. The analysis was conducted with and without prevalent diabetes cases. Further analyses were conducted for the adjusted associations of the TEQs with the five components of metabolic syndrome and the adjusted associations of the concentrations of the 16 selected congeners of which more than 75 percent of the subjects had detectable concentrations with the prevalence of metabolic syndrome.
From 2002 to 2010, Nakamoto et al. (2013) gathered fasting blood samples from a cross-sectional sample of 1,063 men and 1,201 women (aged 15–76 years), who were living in 125 areas of 45 prefectures throughout Japan and who were not occupationally exposed to dioxins (including TCDD). The full WHO 2005 set of dioxin-like PCDDs, PCDFs, and PCBs were measured in the samples and assessed in relation to a range of self-reported history of diseases including allergic diseases, hypertension, diabetes, hyperlipidemia, gout, thyroid disease, kidney disease, gastric ulcer, and gynecological disease. Multiple logistic regression models were fit to estimate the odds of reporting individual diseases by quartiles (pg/g lipid) for PCDDs/PCDFs, for PCBs, and for all dioxin-like chemicals measured. Models were adjusted for age, sex, smoking habit, drinking habit, regional block, survey year, and BMI. Strengths of this study include the relatively large sample and objective measurements of dioxins, which is directly relevant to military service in Vietnam. Limitations include the cross-sectional design, which precludes establishment of the temporal relationship between dioxin exposure and development of the diseases investigated and the fact that information on disease history was based on self-report and thus latent and undiagnosed patients may have been missed.
Yusho Disease Group
Tsukimori et al. (2012a) reported on the association between a mother’s dioxin exposure and her children’s birthweight among Japanese women affected by Yosho disease after an accidental exposure to rice oil contaminated with PCBs, PCDFs, and PCDDs in western Japan in 1968 that affected more than 1,900 people. Of 737 affected women officially registered with the Study Group for Yusho, 206 reported having given birth after the Yusho incident. Of them, 101 (with 190 eligible births) had their dioxin concentrations measured and participated in the mother–child study. Maternal serum concentrations of contaminants were assessed, converted into TEQs, and extrapolated to the time of delivery. Multiple linear-regression models were used to examine the association between birth weight and maternal serum contaminant concentrations, log-transformed to account for their log-normal distributions. The models adjusted for potential confounders for birth weight, including maternal age, parity, maternal smoking during pregnancy, gestation age at delivery, infant sex, duration of breast feeding, number of births, and frequency of seafood consumption.
In a follow-up analysis by Tsukimori et al. (2013), blood samples were obtained from 64 Yusho mothers who had 117 children, which included 10 with fetal Yusho disease (FYD) and 107 without FYD. Based on earlier analyses, FYD among the Yusho Disease Group was phenotypically defined as having children with low birth weight, hyperpigmentation of the gums and nails, conjunctivitis, dysplastic nails, wide fontanels, metastatic scalp calcification, diffuse dark skin pigmentation (“black baby”), and natal teeth at birth. After birth, exposed descendants also showed developmental delay, deficits on formal developmental testing, and abnormalities on behavioral assessment (Rogan et al., 1988). Maternal blood samples collected at delivery were analyzed for the presence of 7 PCDDs, 10 PCDFs, and 4 coplanar PCBs, including TCDD and by calculation of TEQs. Random effects logistic regression models were fit to estimate the odds of elevated maternal blood TEQ concentrations in relation to “black-baby” delivery versus non “black-baby” delivery. Analyses were adjusted for age at delivery, gestational age at birth, birth weight, descendant sex, and consumption of fish (times per week). This study is limited by the fact that dioxin concentrations were not measured in maternal blood at the time of delivery because the Yusho incident had taken place more than 40 years prior. In addition, the analyses are directly relevant only to childbearing Vietnam veterans.
Norwegian Environmental Studies
Stølevik et al. (2011) reported on the relationship between prenatal exposure to PCBs and increased risk of wheeze, eczema, and infections in newborns in the birth subcohort of the Norwegian Mother and Child Cohort Study. Maternal exposure to PCBs was determined from a validated food-frequency questionnaire that covered the first 4 months of pregnancy and that was adapted to include rarely eaten foods that are known to have high concentrations of PCBs and dioxins. Pregnant women were invited to enter the study in 2007–2008. The outcomes were determined through a questionnaire sent to the mothers at 1 year. Confounders in the statistical analyses were taken from the questionnaires filled out by the mothers during pregnancy and at 6 months after birth. They included previous breastfeeding, parity, history of atopy, age, smoking, education, BMI, child’s sex, and others. Logistic regression with backward selection was used to fit multivariate models. There is concern about selection bias because of the low participation rate (38.5 percent).
Russian Environmental Studies
Chapaevsk
Several studies in the Samara region of Russia have identified the Middle Volga Chemical Plant (also known as SZVH or Khimprom) in Chapaevsk,
about 950 km southeast of Moscow, as a major source of TCDD pollution (Revazova et al., 2001; Revich et al., 2001). From 1967 to 1987 the plant produced γ-hexachlorocyclohexane (lindane) and its derivatives, and many of the workers experienced chloracne. Since then, it has produced various chlorinated products. Dioxins were detected in the small number of air, soil, drinking-water, and cow’s-milk samples gathered in the region, but no description of how these media were sampled was given. When Revich et al. (2001) compared the samples with measurements from four other Russian cities that had industrial facilities, the TCDD concentrations observed in Chapaevsk exceeded all reported maximums. Revich et al. (2001) presented rudimentary comparisons of cancer incidence and mortality and reproductive outcomes with regional and national rates; residence in the city of Chapaevsk was used as a surrogate for exposure, and no attempt was made to create exposure categories based on factors that might have influenced the degree of TCDD exposure. The analyses of chromosomal aberrations and other cytologic indicators of genetic damage partitioned the women studied into three groups on the basis of worker status or distance of residence from the factory (Revazova et al., 2001).
Chapaevsk Children’s Study Later research efforts on Chapaevsk residents have focused on quantifying the serum concentrations of dioxins and TEQs associated with furans and PCBs. Akhmedkhanov et al. (2002) reported on a convenience sample of 24 volunteers. A cohort of 499 peripubertal boys (8–9 years old in 2003–2005) and their mothers has been established as the Russian Children’s Study for assessing the effect of in utero and childhood exposure on development. The information generated by this study will be relevant to VAO reports only in conjunction with effects in offspring after maternal exposure to the extent that the consequences of gestational and childhood exposure can be distinguished. To date, however, the published findings have not involved health outcomes but have been limited to detailed characterizations of serum concentrations in the boys (Burns et al., 2009) and their mothers (Humblet et al., 2010).
Swedish Environmental Studies
Prospective Study of the Vasculature in Uppsala Seniors
The Prospective Study of the Vasculature in Uppsala Seniors (PIVUS) study recruited participants, within 2 months after their 70th birthdays, randomly from the registry of residents of the community of Uppsala, Sweden, from April 2001 to June 2004. The primary aim was to investigate CVD in an elderly population with an adjustment for sex. Of the 2,025 subjects who were invited to participate, 1,016 were included, for a participation rate of about 50 percent; 50 percent of the participants were female. All participants answered a questionnaire about
their medical history, medications, diet, and smoking habits. The burden of POP including several dioxin-like PCBs, was assessed from blood serum or plasma.
Salihovic et al. (2012a) reported on circulating concentrations of POPs in 992 participants with valid measurements. They found significant sex differences in the concentrations of 17 of 21 POPs; women had higher concentrations of 5 of them. An appropriate adjustment for multiple comparisons (via Holm’s method) was applied. Salihovic et al. (2012b) investigated a new method for extracting POPs from human blood in the PIVUS study and found it to be robust.
DH Lee et al. (2011b) reported on the association between POPs and type 2 diabetes in the subjects of the PIVUS study. Of the 1,016 evaluated at baseline, 81 percent returned 5 years later at age 75. The cross-sectional study (baseline) included 989 of these participants, and 725 were in the prospective analysis. The additional value of POPs on top of the standard risk factors was evaluated with the C-statistic and the net reclassification index and the improved discrimination index. The cross-sectional analyses could not account for any measure of duration of exposure. The results are limited by the small number of incident diabetes cases (36), the multiple testing, and the correlation of POPs (and the ensuing difficulty of interpretating the association with diabetes).
Rönn et al. (2011) reported on the association of POPs with fat mass in the PIVUS study. Multiple imputation was used to handle missing dietary assessments. A strength of the study was its use of DXA screening to measure fat. There was considerable multiple testing without adjustment. The findings are limited by the cross-sectional design and the limited age of the participants inasmuch as age could affect the findings in several ways; the published paper could report on only one subset of findings for this age group.
Lee et al. (2012a) reported on the associations of POPs with abdominal obesity in the PIVUS study. Abdominal obesity was treated as a binary variable. The authors note concerns with residual confounding due to diet and physical activity. Furthermore, greater food consumption may lead to obesity and increased concentrations of chemicals. There could be alterations in the pharmacodynamics of POPs because of health disorders, which themselves may influence obesity.
Lee et al. (2012b) reported on the associations of POPS with stroke in the PIVUS study. Only hospital-treated strokes were considered. Ischemic and hemorrhagic strokes were not distinguished. There were 35 incident strokes during the 5 years of follow-up. Sex might be an important effect modifier, but the sample was too small to assess this. The POPs in this study may not be causally related to stroke, but rather may be associated with other, causal POPs. The study was not able to use time of stroke in a survival analysis, which would have been a more powerful analysis.
Lind et al. (2012) reported on the association of POPs with carotid atherosclerosis in the PIVUS study. Ordinal logistic regression was used to model the ordinal outcome of number of involved arteries. A Bonferroni adjustment for multiple testing was applied.
Eight publications from the PIVUS cohort that have appeared since Update 2012 were identified for review and evaluation. None of these studies examined relationships between POPs and “primary” health outcomes of interest to the VAO committee, but rather they examined “surrogate” health outcomes, including CVD measures and risk factors (left ventricular systolic and diastolic dysfunction, left ventricular hypertrophy, carotid atherosclerosis, weight change, inflammatory markers, complement system, and oxidative stress). These studies augment previous publications from PIVUS that examined a range of indicators related to CVD and cardiovascular health. As with previous analyses from the PIVUS cohort, results are limited by the fact that participants were recruited in the 2-month period after their 70th birthday. This potentially imparts a survival bias, meaning that persons from the catchment area with very high levels of POPs may have been disproportionately excluded from the study sample. In addition, results are limited by the relative non-specificity of the POPs examined, although, the battery of congeners included octachlorodibenzo-p-dioxin (OCDD), which is relevant to Vietnam veterans.
Sjoberg et al. (2013a) analyzed circulating levels of POPs in relation to impairments in left ventricular systolic and diastolic function. The left ventricular ejection fraction, E/A-ratio, and isovolumic relaxation time were determined by echocardiography, and 21 POPs were analyzed in serum samples measured by high-resolution chromatography coupled to high-resolution mass spectrometry in 998 subjects from the PIVUS cohort. Results were adjusted for sex, hypertension, diabetes, smoking, hypertrophy, and BMI, and subjects with myocardial infarction or atrial fibrillation were excluded from the analysis. In addition to the limitations described above for the PIVUS cohort, this analysis is limited by its cross-sectional design.
Using a study design that was essentially identical to that in Sjoberg et al. (2013a), Sjoberg et al. (2013b) analyzed circulating levels of POPs in relation to geometric measures of the left ventricle carried out with echocardiography, including the left ventricular mass index, relative wall thickness, and groups of left ventricular hypertrophy. This analysis included 1,016 elderly adults from PIVUS with statistical adjustments for sex, blood pressure, antihypertensive treatment, diabetes, and BMI.
Lind et al. (2012) examined the relationships between circulating levels of POPs and carotid artery plaques and carotid intima-media thickness. This analysis was based on 1,016 elderly adults from PIVUS with statistical adjustment for sex, waist circumference, BMI, fasting blood glucose, systolic and diastolic blood pressure, high-density lipoprotein and low-density lipoprotein (LDL) cholesterol, serum triglycerides, smoking, antihypertensive treatment, and statin use. Estimates included TEQs for two classes of dioxin-like congeners; thus the study is of relevance to Vietnam veterans, taking into account the limitations of PIVUS described above.
In a second paper by Lind et al. (2013), a retrospective classification of the magnitude of weight change between the ages of 20 and 70 (n = 1,016) was examined relative to 16 PCBs congeners and three OC pesticides. A series of linear-regression models were fit to evaluate the relationship between the change in body weight and POP levels, with the full models adjusted for sex, BMI at 20 years of age, serum cholesterol, triglycerides, education, exercise habits, and smoking. The limitations of this analysis include the fact that body weight and height at age 20 were self-reported and potentially imprecise in terms of accuracy and that there was no assessment of dietary intake measured throughout life.
In a third PIVUS paper, circulating levels of PCBs in 1,016 participants were examined in relation to genetic variation in the genes coding for P450 enzymes (Lind et al., 2014). Whereas P450 proteins catalyze reactions involved in drug metabolism and the synthesis of cholesterol, steroids, and other lipids, the direct clinical relevance of this analysis with respect to herbicide exposure and adverse health effects among Vietnam veterans is limited.
Kumar and colleagues published three papers in 2014 that examined relationships between POPs and measures of inflammatory markers, the complement system, and oxidative stress in participants enrolled in PIVUS. In the first paper (Kumar et al., 2014a), TEQ values were calculated using seven mono- and non-ortho-substituted dioxin-like PCBs and OCDD and examined in relationship to eight inflammatory markers, including C-reactive protein (n = 996). The primary analytical method used was multiple linear regression with statistical adjustment for sex, kidney function, smoking, BMI, waist circumference, blood glucose, systolic blood pressure, high-density lipoprotein, low-density lipoprotein, triglycerides, exercise habits, and education.
The second paper by Kumar et al. (2014b) used essentially identical methods as the 2014a paper. The researchers analyzed levels of 16 PCBs and 3 OC pesticides for their association with the levels of protein complement 3 (C3), 3a (C3a), and 4 (C4) and the C3a/C3 ratio (n = 992). The analysis included TEQ values with results derived from multiple linear regression. Whereas the complement system is part of innate immune system that helps to clear pathogens from the body, the direct clinical relevance of this analysis with respect to herbicide exposure and adverse health effects among Vietnam veterans is limited.
In the third paper by Kumar et al. (2014c), which again used very similar methods, 16 PCBs and 5 OC pesticides, including values derived from TEQs, were examined in relation to plasma oxidative stress markers. The full battery of oxidative stress markers included homocysteine, reduced and oxidized glutathione, the glutathione ratio, total glutathione, oxidized LDL, oxidized LDL antibodies, conjugated dienes, baseline conjugated dienes of LDL, and total anti-oxidative capacity. As with the similar papers by Kumar et al. (2014a,b), the direct clinical relevance of these analyses with respect to military service in Vietnam is limited.
Taiwanese Environmental Studies
Taiwan Residents Around Closed PCP Factory
Chang et al. (2010) reported on the relationship between exposure to PCDDs and PCDFs and hypertension in metabolic syndrome in 1,490 non-diabetic Taiwanese who lived near a highly dioxin-contaminated area. This was a cross-sectional study (2005–2007) that accrued subjects from a health center near a deserted PCP factory. The sample consisted of about 80 percent of the invited residents of the community. Univariate analyses of the relationships among several components of metabolic syndrome were conducted, as was a principal component factor analysis, in order to identify a set of uncorrelated factors from among the components of metabolic syndrome. Multiple regression models were fitted for each component. In addition, an analysis of the association between each congener and the prevalence of metabolic syndrome was conducted. The authors list the following limitations of the study: Unknown age at first exposure to PCDDs and PCDFs and an unknown duration of exposure; a cross-sectional design that evaluated the current association; an adjustment for obesity as one element of metabolic syndrome, rather than BMI; and some arbitrary choices inherent in factor analysis. In summary, the large size of this study is a strength, but the unknown age and duration of exposure are clear weaknesses.
Chang et al. (2011a) reported on the same cross-sectional study, restricted to 1,449 non-diabetic residents (the slight decrease in sample size from the 2010 study is due to slightly different starting population sizes and to a difference of 19 diabetic people between the studies). The study aimed to investigate the joint effects of exposure to dioxins and mercury on pancreatic endocrine function. People who lived near the deserted factory were exposed to both PCDDs and PCDFs and also to mercury from eating contaminated seafood from the reservoir near the factory. In their multiple-regression models, the authors did not include PCDDs and PCDFs along with mercury simultaneously but rather included each singly. They reported the correlation of PCDDs and PCDFs with mercury to be 0.14 (p < 0.001), which is low, so it is not apparent why they did not fit models that included both simultaneously and perhaps even with an interaction term to assess the magnitude of the contribution of each contaminant. They did, however, fit a model that included all combinations of tertiles of exposure to each. Again, a major limitation of this study is the absence of information on the onset and duration of exposure. Furthermore, the authors note that the homeostasis model for insulin-resistance assessment is not the gold standard and that repeated testing may be needed for assessment in older people. The study did not address co-contamination with mercury.
Chang et al. (2011b) reported on the same cross-sectional study with enrollment extended to December 2009 and restricted to 914 residents who did not have CVD and who were 30–45 years old. The study aimed to investigate the
association between PCDD and PCDF exposure and continuous measures of CVD within 10 years as measured by the Framingham risk score, a formula for combining established risk factors into a single number. Mercury concentrations were not adjusted for in the models, although seafood consumption was. One limitation is the use of the Framingham score; other factors are associated with risk but were not included in the score (such as socioeconomic position, genetics, and imaging biomarkers). As in all the publications on this cohort, this one is limited by the lack of information about the onset and duration of exposure.
Chang et al. (2012) reported on the same cross-sectional study during 2006–2009 with enrollment restricted to 1,167 residents who had fasted before blood sampling and who were more than 50 years old. The study aimed to investigate the biochemical profiles of those exposed to PCDDs and PCDFs. Na-PCP, a widely used pesticide, had been used in the production process at the abandoned factory. After the factory shut down, a large quantity was improperly stored and later released into the environment. Some of the retired workers moved away from the area and were not exposed by eating seafood, whereas others remained and were exposed, alongside other local residents. Thus, there were three exposure groups of retired Na-PCP workers: those who still lived locally (23), those who lived locally but did not knowingly eat polluted fish (37), and those who moved away (96). Three control groups did not include any Na-PCP workers: Local residents who had eaten polluted fish (345), local residents who had not eaten polluted fish (666), and “background participants” in Taiwan’s general population (645). The first two of the control groups made up the 1,167 in the study population. Limitations of the study include the unknown PCDD and PCDF concentrations in retired workers who moved away and knowledge about when the exposure ceased. There may be important unmeasured confounders related to which workers moved away and which ones did not.
US Environmental Studies
Anniston, Alabama, Community Health Survey
In 2003 the Agency for Toxic Substances and Disease Registry (ATSDR) funded a study of the health effects of environmental exposures on the residents of Anniston, Alabama. Anniston housed a plant that produced PCBs from 1929 to 1971; it had been owned and operated by Monsanto since 1935. Residents of Anniston were known to have high concentrations of PCBs although these have not been found to be associated with employment in the plant or with the consumption of local fish and produce. PCBs spread in Anniston via air, soil, and water movement. Before the ATSDR study, there had been minimal research into the health effects of PCBs on Anniston residents. Residents were recruited into the study through a stratified random sampling of housing units across the city, weighted by proximity to the plant and by race. Of the 1,110 who agreed
to be interviewed, 772 had blood drawn for biochemical and PCB analyses and had blood pressure measured. Of the 758 subjects who provided sufficient data to be retained in the study, 364 were taking antihypertensive medications and 394 were not.
Two methods were considered for PCB analysis: Wet-weight values and lipid-standardized values. The latter are thought to be more prone to bias, but both were considered. The two approaches make comparisons between the studies difficult. Another issue was the problem of PCB values that were below the level of detection (LOD). These variables amounted to left-censored covariates in a regression model. They were dealt with by a crude imputation of the LOD divided by the square root of 2 (Goncharov et al., 2010; Silverstone et al., 2012) or by 2 (Goncharov et al., 2011). This is highly biased, and alternative methods (such as multiple imputation) would have been preferable. It may also be a problem that the studies took different approaches.
Goncharov et al. (2010) studied the association between all PCBs and blood pressure. After adjusting for age there was a significant association between PCB concentrations and the risk of hypertension. When people on antihypertensive medications were included in the models, the associations between PCB concentrations and risk of hypertension were diluted; this could be due to an effect of the medications on PCB metabolism.
Goncharov et al. (2011) extended the 2010 report by considering the effect of PCBs on the entire range of continuous blood pressure and by investigating five PCB groups and 33 individual PCB cogeners. Only the 394 people who were not on antihypertensive medications were included in this study. The study found that serum PCB concentration is associated with blood pressure even in the normotensive range. Furthermore, the relationship is found to be strongest for ortho-substituted PCB congeners that have two or more chlorines and with some that have some dioxin-like activity. The overall concentrations of PCB’s are higher in the Anniston population than in the US population overall.
Silverstone et al. (2012) examined the association between PCB exposure and diabetes in the Anniston study. Diabetes was present in 27 percent of 774 participants; 75 percent of the 27 were taking glycemic control medications. People who had pre-diabetes were identified and were excluded from some regression analyses because they were intermediate between the diabetic and normoglycemic groups. There was a non-monotonic increase in the prevalence of diabetes with high PCB congener concentrations, but some of the groups (for example, by age) were small. Women had a consistently higher likelihood of diabetes in each subset of PCBs (except the estrogenic subset). The findings suggest a low-dose PCB effect inasmuch as the ORs increased in the second quintile of PCB exposure and remained high. Advantages of this study are its adjustment for family history of diabetes and exclusion of people who had prediabetes. Lipid metabolism in people who have diabetes may affect the metabolism of PCBs.
Coronary Artery Risk Development in Young Adults Study
DH Lee et al. (2010) reported on the association between low-dose POPs and type 2 diabetes in the Coronary Artery Risk Development in Young Adults (CARDIA) cohort. Serum samples were collected at year 2 (1987–1988) and were later used to measure POPs. This was a nested case-control study in which subjects were required to be free of diabetes at years 0 and 2. From 1988 to 2006, 116 received a diagnosis of diabetes; 90 were randomly selected as cases. Controls were randomly selected from those who had not received a diagnosis of diabetes. Cases and controls were frequency-matched on BMI strata. The authors analyzed summary measures of POPs. The second summary measure selected POPs on the basis of their effect in the current study; this invalidates standard inference. The authors asserted that summary measures are useful because appropriate controls are those with globally low concentrations of POPs. Other limitations are the single measure of POPs and the age of the samples at analysis (18 years). The authors stated that the study was underpowered and that extensive statistical testing was performed.
DH Lee et al. (2011a) further investigated the 90 controls selected for the nested case-control study reported in DH Lee et al. (2010). This investigation is concerned with associations between exposure to POPs and obesity, dyslipidemia, and insulin resistance in people who are free of diabetes. The multiple comparisons are of concern, as is the small sample size.
Great Lakes Fish Consumption Study
The Great Lakes Fish Consumption Study was initiated in early 1992. Bloom et al. (2006) measured serum dioxin in New York sport fishermen as part of a study of thyroid function. A methodologic study by Petreas et al. (2004) found generally high correlations between concentrations of dioxins and related chemicals in breast and abdominal fat in the same woman; this suggested that they could be used interchangeably in epidemiologic studies. The same study, however, also found that adjusting concentrations according to lipid content rather than the weight of the fat samples is important because of the presence of non-lipid components in the samples.
In 2001–2005, 1,788 of the 4,200 people who had participated in the original study were contacted and asked for updated information on health, reproductive history, and fish consumption. Blood samples gathered from 515 of them were analyzed for the serum concentrations of various POPs, including a number of PCBs. Turyk et al. (2009) investigated whether the serum results were related to self-reported diabetes. Lambertino et al. (2011) studied the self-reported occurrences of uterine leiomyomas (benign fibroid tumors) in 580 women using the serum results from the 197 women who had provided blood samples. The exposure measure for the category “dioxin-like PCBs” consisted of the summed
concentrations of only the mono-ortho PCBs 118 and 167. Because the results were based solely on mono-ortho PCBs, which typically contribute only a small percentage to total TEQs, the findings of these publications cannot be considered conclusive.
Iowa Women’s Health Study
Jones et al. (2014) analyzed data from a cohort of 37,099 Iowa women aged 55–69 years who reported their residence location (farm, rural [not a farm], population of their town) at enrollment in 1986. Incident lymphohematopoietic cancers were identified in the period 1986–2009 by linkage with the Iowa Cancer Registry. A geographic information system was used to geocode addresses and to calculate the total acreage of pasture and row crops within 750 m of homes using the 1992 National Land Cover Database. The purpose of this analysis was to estimate the cancer risk in relation to both residence location and crop acreage. This analysis was deemed to be of no value to the committee because exposure assessment was based on attributes of residence related to farming and not on specific pesticides with dioxin-like properties.
National Health and Nutrition Examination Survey
In the early 1960s, the CDC National Center for Health Statistics began the NHANES program as a means of monitoring and assessing the health and nutritional status of people of all ages living in the United States. In 1999, the survey became a continuous program that has a changing focus on a variety of health and nutrition measurements in order to meet emerging needs. A rich variety of data—demographic and socioeconomic data; dietary information; medical, dental, and physiologic assessments; and the serum concentrations of POPs, including specific congeners of dioxins, furans, and PCBs—are collected through in-person interviews, health examinations, and blood samples obtained from a nationally representative sample of adults and children in the noninstitutionalized US population. Information obtained from NHANES data is used to determine prevalences of diseases, to assess nutritional status, and to establish national standards of height, weight, and blood pressure. Researchers also conduct analyses of the NHANES data for epidemiologic studies and health-science research on serum concentrations of various compounds in association with various health outcomes.
Starting with the preparation of Update 2008, VAO committees began seeing a stream of publications addressing possible association of some pesticides and various individual and grouped dioxin-like chemicals with the occurrence of a variety of health outcomes as assessed by the surveys for particular temporal spans. NHANES data from 1999 to 2002 were used to evaluate relationships of the COIs with CVD (Ha et al., 2007); diabetes, the metabolic
syndrome, insulin resistance, and arthritis (Lee DH et al., 2006, 2007a,b,c); and thyroid-hormone concentrations (Turyk et al., 2007). Everett et al. (2008a) address hypertension over this time period and provided additional information for the years 2003–2004 in a subsequent commentary (Everett et al., 2008b)
Lee et al. (2008) examined the associations between serum concentrations of POPs and the prevalence of peripheral neuropathy and poor glycemic control (A1C ≥ 7.0 percent) in NHANES 1999–2002 participants who were at least 40 years old and had diabetes or impaired fasting glucose. Peripheral neuropathy was ascertained on the basis of one or more insensate sites on the foot. Diabetes was ascertained on the basis of high plasma glucose (≥ 126 mg/dL fasting or ≥ 200 mg/dL nonfasting) or on the basis of whether a person is taking insulin or an oral anti-diabetes agent. Although 49 POPs were measured, analysis was restricted to 25, of which at least 60 percent of the study participants had detectable concentrations: three PCDDs, four PCDFs, five dioxin-like PCBs, seven non–dioxin-like PCBs, and six OC pesticides. Logistic regression was used to determine the OR between each outcome (peripheral neuropathy or poor glycemic control) and each exposure to POP subclass with adjustment for age, sex, race or ethnicity, poverty, duration of diabetes, hypertension (yes or no), BMI, cigarette smoking (never, former, or current), cotinine concentration, alcohol consumption, leisure-time physical activity (vigorous, moderate, or none), and A1C (neuropathy only). For each POP subclass, a cumulative measure was derived by summing the rank scores among individual chemicals that belonged to the subclass; the cumulative measure was then categorized into tertiles. Additional analyses were conducted for individual compounds by using the correlation coefficient between the rank score for each chemical and each outcome with adjustment for the same covariates listed above.
Ha et al. (2009) examined the association between serum concentrations of POPs and the prevalence of newly diagnosed hypertension in NHANES 1999–2002 adult participants 40 years old or older. After the exclusion of 444 patients known to be hypertensive irrespective of antihypertensive medication, 165 diabetic patients, and 49 subjects whose blood-pressure values were missing, the final sample size was 524. Participants were considered to have hypertension if their systolic blood pressure was 140 mmHg or higher or if their diastolic blood pressure was 90 mmHg or higher. The analysis was restricted to 21 POPs of which at least 60 percent of study participants had detectable concentrations: Three PCDDs, three PCDFs, five dioxin-like PCBs, six non–dioxin-like PCBs, and four OC pesticides. The discrepancy from Lee et al. (2008) in the number of POPs detected is probably due to the difference in the samples used. For each POP, participants whose serum concentrations were below the limit of detection were regarded as the reference group; participants who had detectable concentrations were categorized into quartiles. A cumulative measure for each POP subclass was derived by summing the category numbers (0 for nondetectable, 1 for
detectable below the first quartile, and so on up to 4 for above the third quartile) of individual chemicals belonging to the subclass. The summary values were again categorized into quartiles. Logistic regression was used to derive adjusted ORs, which were stratified by sex and adjusted for age, race or ethnicity, poverty-income ratio, BMI, cigarette smoking (never, former, or current), cotinine, alcohol consumption, and leisure-time physical activity (vigorous, moderate, or none).
Cho et al. (2011) reported on the associations between bone mineral density (BMD) and exposures to POPs, including OC pesticides, assessed from serum samples from NHANES participants in 1999–2004 (2,769 for OC pesticide analyses and 2,565 for POP analyses). The study also examined whether the POP levels modified the association between BMD and fat mass or lean mass. All analyses were stratified by sex and age group (cutoff 50 years). General linear models were used to derive means that were adjusted for age, race or ethnicity, poverty-income ratio, fat mass, lean mass, height, smoking, physical activity, and postmenopausal hormone intake.
Elobeid et al. (2010) examined the association between POPs and obesity—BMI and waist circumference (WC)—in NHANES 1999–2002 participants (2,464 for BMI analysis and 2,448 for WC). Regression models were used to assess the association between the obesity measures and POPs, adjusted for sex, ethnicity, age, and age squared. An additional model for WC also adjusts for BMI.
Jones et al. (2011) examined the association between urinary arsenic and hypertension and blood pressure in NHANES 2003–2008 participants (4,167). Logistic-regression and linear-regression models were used for hypertension and blood pressure, respectively, adjusted for age, sex, race or ethnicity, urinary creatinine, education, BMI, and serum cotinine; models for blood pressure also adjusted for antihypertensive medication. All analyses accounted for the complex sample design of NHANES.
Since Update 2012, there have been several more publications based on NHANES data concerning the COIs and various health outcomes. Specifically, Lin et al. (2012) examined samples for measurement of dioxin-like chemicals from the 1999–2004 NHANES in relation to total and cause-specific (cardiovascular, cancer) mortality based on the ICD-10 system, and follow-up through 2006. The analysis was restricted to non-Hispanic whites, non-Hispanic blacks, and Mexican-American participants aged 40 years or older who provided samples for the measurement of dioxin-like chemicals. The analysis included a sample of 1,176 males and 1,185 females. The estimation of potential toxicity from exposure to dioxin-like chemicals, including PCDDs, PCDFs, and PCBs, was based on TEQs. Analyses were adjusted for age, gender, BMI, race or ethnicity, cigarette smoking, and alcohol consumption. The strengths of this study include its biological measurement of exposure to dioxin-like chemicals and the prospective assessment of mortality, which is generally believed to be reliable and accurate within NHANES.
Lee et al. (2013) evaluated associations between OC pesticides (n = 1,299) as well as PCDDs, PCDFs, and PCBs (n = 1,299) and the risk of hyperuricemia in subjects 20 years of age and older in the 2003–2004 NHANES. TEFs were calculated for dioxins and dioxin-like compounds. Hyperuricemia was defined as a blood uric acid concentration greater than 7.0 mg/dL in men and 6.0 mg/dL in women. Analyses were performed among all subjects and separately among subjects without the presence of the metabolic syndrome. The analyses were adjusted for age, race, ethnicity, and poverty income ratio. A strength of this study is the use of biological measurement of TEFs for dioxins and dioxin-like compounds. Limitations include the cross-sectional design, which does not permit the assessment of temporal effects, and the fact that hyperuricemia is a measure of disturbed metabolism, but not one of the primary health outcomes of interest specified by the committee with respect to service in Vietnam.
Everett and Thompson (2014) examined the relationship between dioxins (including TCDD) and dl-PCBs and the prevalence of diabetic nephropathy using blood samples and self-report data collected from the 1999–2004 NHANES (n = 2,588). TEQs were calculated for six different dioxins and eight dl-PCBs and analyses were stratified by subjects with and without nephropathy. Analyses were adjusted for a range of covariates including age, gender, race, ethnicity, education, poverty income ratio, fruit and vegetable consumption, physical activity, and family history of diabetes. The strengths of this study include the use of biological measurement of TEFs, including for TCDD, and the objective assessment of nephropathy by the use of urinary albumin-to-creatinine ratio. Limitations include the cross-sectional study design, and most notably, the fact that the analyses did not include a comparison group of subjects without diabetes. Thus, the analysis can only be suggestive of whether or not dioxins and dioxin-like compounds may be associated with nephropathy in the presence of diabetes, but not the development of diabetes.
Peters et al. (2014) added NHANES data for 2005–2008 to the sets for 1999–2002 and 2003–2004 previously analyzed by Everett et al. (2008a,b) for association of blood pressure with blood concentrations of dioxin-like PCBs 126 and 169 and mono-ortho PCBs 118 and 156. Using this expanded data set, they developed a model to predict blood PCB concentrations using generally available variables (age, sex, ethnicity, and blood lipid levels) as a step toward producing a structural equations model involving lead and cadmium blood levels, in addition to PCB blood concentrations for the prediction blood pressure. The PCBs metric used for this modeling effort was the total blood concentration by weight of PCBs 66, 101, 118, 128, and 187. Because this measure of PCB exposure includes only a single mono-ortho dioxin-like PCB in combination with PBC having no dioxin-like activity, this work does not augment the results previously published by Everett et al. (2008a,b) for VAO purposes.
The study population for the Priority Toxicant Reference Range Study was a subgroup of participants aged 20–59 years in NHANES III (1988–1994) established
to characterize levels of 44 environmental toxicants (including 2,4-D and its metabolite 2,4-dichlorophenol [2,4-DCP]) in urine and blood, which can be regarded as indicators of internal dose. Unlike overall NHANES samples established by rigorous statistical sampling procedures to be representative samples of the US population, this study sample is regarded as a convenient sample, because its 1,338 members had voluntarily provided an additional 20 ml of blood and had responded to an extra questionnaire during their regular NHANES medical examination.
Schreinemachers (2010) examined the association in healthy adults between exposure to 2,4-D, as indicated by its presence in urine, and biomarkers that are linked to the pathogenesis of acute myocardial infarction and type 2 diabetes, namely, serum HDL, triglycerides, total cholesterol minus HDL, insulin, C-peptide, plasma glucose, and thyroid-stimulating hormone. A sample of 727 people remained in the study after exclusion of 375 individuals without results for measurement of urinary 2,4-D and 236 more on the basis of health criteria: A history of congestive heart failure, heart attack, diabetes, thyroid disease, lupus, or cancer; a white blood cell count over 12 × 109 per liter CRP over 10 mg/dL; or glycosylated hemoglobin (HbA1c) over 8 percent. Urinary 2,4-D was detectable in 102 (14 percent), with concentrations of 1–28 mg/dL. The outcome variables were compared between participants with and without detectable urinary 2,4-D by using Wilcoxon’s rank-sum test. Further analysis was conducted with linear regression, and the outcome variables were transformed to a logarithmic scale. The linear-regression models included the following explanatory variables: 2,4-D (binary), HDL (continuous, log-transformed, and included in all models except when HDL itself was the dependent variable), urinary creatinine (continuous and log-transformed), sex, age, BMI, race or ethnicity, and smoking (none, past, and active). Alcohol consumption, education, household income, and hours of fasting before a blood sample was drawn were also checked for their effects on the regression coefficient for urinary 2,4-D. The analyses were conducted on the final study sample of 727 and on two subsamples that were expected to be more susceptible: Participants who had HbA1c above the median (5.1 percent) of the total sample and participants who had thyroxine at or below the median (8.5 μg/dL) of the total sample.
Krieg (2013) performed a limited assessment of cognition in 700 adults. Twelve pesticide metabolites were measured in the urine, including two chemicals found in the urine after 2,4-D exposure: Unmetabolized 2,4-D and 2,4-DCP (Sauerhoff et al., 1977). The analysis investigated association of their concentrations with the results of three neurobehavioral tests (simple reaction time, symbol-digit substitution, and serial digit learning).
Pensacola, Florida
Karouna-Renier et al. (2007) examined health effects related to dioxins and furans in soil at a Superfund site in Pensacola, Florida, that was contaminated by
operations at a wood-treating company that operated from 1942 to 1982. In 2001 the study collected health and exposure histories and measured serum concentrations of 17 PCDD and PCDF congeners in 47 potentially exposed people who were selected nonsystematically from among former workers, their families, and residents. Logistic regression was used to predict the prevalence of health outcomes from TEQs with adjustments for age, race, sex, BMI, tobacco and alcohol use, and worker status.
Times Beach and Quail Run Cohorts
Several reports have provided information on environmental exposure to TCDD in the Times Beach area of Missouri (Andrews et al., 1989; Patterson et al., 1986), one of the incidents that heightened concerns about the health effects of dioxin. In 1971, TCDD-contaminated sludge from a hexachlorophene-production facility was mixed with waste oil and sprayed in various areas for dust control. Soil contamination in some samples exceeded 100 ppb. Among the Missouri sites with the highest soil TCDD concentrations was the Quail Run mobile-home park. Residents were considered exposed if they had lived in the park for at least 6 months during the time when contamination occurred (Hoffman et al., 1986).
Of 51 exposed participants, 87 percent had adipose-tissue TCDD concentrations below 200 ppt; however, the TCDD concentrations in 7 of the 51 were 250–750 ppt. In 128 non-exposed control participants, adipose-tissue TCDD ranged from undetectable to 20 ppt (median, 6 ppt). On the basis of a 7-year half-life, it is calculated that two study participants would have had adipose-tissue TCDD near 3,000 ppt at the time of their last exposure (Andrews et al., 1989).
Several studies evaluated health effects potentially attributable to exposure (Evans et al., 1988; Hoffman et al., 1986; Stehr et al., 1986; Stehr-Green et al., 1987; Stockbauer et al., 1988; Webb et al., 1987). Those studies were reviewed in VAO; no further work on the cohorts has been published.
Vietnamese Environmental Studies
Various epidemiologic studies have been conducted in the Vietnamese population exposed to the spraying that occurred during the Vietnam War. In a review paper, Constable and Hatch (1985) summarized the unpublished results of studies conducted by researchers in Vietnam. They also examined nine reports that focused primarily on reproductive outcomes (Can et al., 1983a,b; Huong and Phuong, 1983; Khoa, 1983; Lang et al., 1983a,b; Nguyen, 1983; Phuong and Huong, 1983; Trung and Chien, 1983). Vietnamese researchers later published the results of four additional studies: two on reproductive abnormalities (Phuong et al., 1989a,b), one on mortality (Dai et al., 1990), and one on hepatocellular carcinoma (Cordier et al., 1993). Ngo et al. (2006) published a meta-analysis that
addressed an association between exposure to herbicides in Vietnam and birth defects and covered some reports reviewed previously by Constable and Hatch (1985), some new Vietnam studies, and studies on US and Australian veterans who served in Vietnam.
The committee has been interested in assessments of contaminant concentrations in Vietnam attributable to the storage, distribution, and spraying of herbicides by the US military during the Vietnam War, but no studies have as yet explored associations between the measured concentrations and health outcomes.
Dioxins and PCBs were among the OC chemicals measured by Schecter et al. (2003) in food samples gathered in 2002 around Bien Hoa City, Vietnam, about 32 km north of Ho Chi Minh City (formerly Saigon). Bien Hoa City is known as a dioxin “hot spot,” with a substantial leak of more than 5,000 gal of Agent Orange at the nearby Bien Hoa airbase about 30 years before the study. Marked increases in TCDD concentrations and TEQs were found in ducks, chickens, and fish, but not in pork or beef. The study concluded that food appeared to be responsible for the increase in TCDD in residents of Bien Hoa City even though the original Agent Orange contamination occurred 30 to 40 years before sampling.
Hansen et al. (2009) studied maternal serum concentrations of OC chemicals (including dioxin-like PCBs 118, 126, 156, and 169) at the time of delivery in women from two communities in southern Vietnam: Nha Trang, a coastal city about 450 km northeast of Ho Chi Minh City, and Dien Khanh, a rural district about 10 km inland from Nha Trang. Of 246 women who delivered infants in May–July 2005, 94 in Nha Trang and 95 in Dien Khanh met the study’s residence requirements, agreed to participate, and provided blood specimens. Mean concentrations of the ordinarily prevalent non–dioxin-like PCB 153 were 0.15 μg/L in Nha Trang and 0.10 μg/L in Dien Khanh; other PCB congeners were low in both communities. Age and parity were the most important predictors of plasma concentrations of all chemicals, whereas the community of residence was also predictive for PCB 153. Correlations with the health status of mothers or children were not reported.
Nhu et al. (2009) examined the correlations among dioxin concentrations in soil, sediment, and breast milk in an area in Vietnam that had been sprayed with herbicide during the war, Cam Chinh commune in Quang Tri province, and a control site that was not sprayed, Cam Phuc commune in Ha Tinh province. Soil and sediment samples were taken randomly throughout Cam Chinh commune and analyzed for PCDDs and PCDFs. The spatial distribution of PCDDs and PCDFs was estimated by using log-normal kriging (Saito and Goovaerts, 2000). Breast-milk samples were taken from lactating mothers 20–40 years old who lived in two communes (86 in Cam Chinh commune and 71 in Cam Phuc commune) in September 2002–July 2003. The participants were also interviewed to collect information on personal habits, such as smoking, alcohol drinking, contraceptive-drug use, history of pesticide contact, disease history,
number of pregnancies, age at each pregnancy, and reason for pregnancy failure, if applicable. The mean dioxin concentrations in soil and breast milk in the sprayed area were significantly higher than those in the unsprayed area. There were no significant correlations between the estimated dioxin concentrations in soil obtained with the kriging method and those in breast milk. Again, no results were presented with respect to the health status of mothers or infants.
Since Update 2012, three relevant environmental papers from Vietnam residents were identified for review. Tai et al. (2013) studied 216 mother–infant pairs living near the Da Nang airbase, a dioxin-contaminated area in Vietnam, and relationships between the dioxin levels in breast milk and infant neurodevelopment parameters at 4 months of age. Breast-milk samples were collected from each nursing mother 1 month after giving birth in order to quantify the levels of 17 different 2,3,7,8-substituted PCDD and PCDF congeners. TEQs were calculated, including for TCDD. A neurodevelopment assessment at 4 months was based on the Bayley Scales of Infant and Toddler Development. Generalized linear models were used to compare neurodevelopment parameters across four groups of dioxin exposure: Low, mild, moderate, and high. Whereas the results of this analysis are limited by inference to childbearing female Vietnam veterans, the strengths of this study include objective measurement of dioxin contamination in a known contaminated area and use of the well-validated Bayley Scales of Infant and Toddler Development.
Sun et al. (2013) compared prostate-specific antigen (PSA) levels (2009–2011) in a cross-sectional study in men over the age of 50 years between those residing in the Phu Cat district (a presumed contamination hot spot, n = 101) and those residing in the Kim Bang district (presumed non-sprayed, n = 97). Analyses were adjusted for age and included stratification by occupation, including farmers and other non-farm occupations. Results of this study are limited by its cross-sectional design and, in particular, the relatively crude measurement of exposure assessment many years after the time when herbicide spraying would have occurred.
In a second paper by Sun et al. (2014) with similar methodology to Sun et al. (2013), serum dioxin and steroid hormone levels were compared between 48 men in the presumed hotspot area (Phu Cat district) and 36 men in the non-sprayed area (Kim Bang district). Five dioxin congeners expressed as TEQs were calculated along with nine serum steroid hormones, including testosterone, cortisol, estradiol, and others. Multiple linear-regression analyses were conducted with statistical adjustment for age, BMI, employment status, and tobacco use. The limitations of this analysis include the cross-sectional design with exposure assessment occurring many years after presumed herbicide exposure.
Other Environmental Studies
A number of additional outcomes of environmental exposure to the COIs were studied: NHL in Yorkshire, England (Cartwright et al., 1988); adverse health effects after an electric-transformer fire in Binghamton, New York (Fitzgerald et al., 1989); lymphomas and STSs in Italy (Vineis et al., 1991); cancers in Finland (Lampi et al., 1992); early-onset PD in Oregon and Washington (Butterfield et al., 1993); neuropsychologic effects in Germany (Peper et al., 1993); mortality and cancer incidence in two cohorts of Swedish fishermen whose primary exposure route was assumed to be diet (Svensson et al., 1995a); the immunologic effects of prenatal and postnatal exposure to PCB or TCDD in Dutch infants from birth to the age of 18 months (Weisglas-Kuperus et al., 1995); the effects of inhalation exposure to TCDD and related chemicals in wood preservatives on cell-mediated immunity in German daycare center employees (Wolf and Karmaus, 1995); skin cancers in Alberta, Canada (Gallagher et al., 1996); immunologic effects in hobby fishermen in the Frierfjord in southeastern Norway (Lovik et al., 1996); HL, NHL, multiple myeloma, and acute myeloid leukemia in various regions of Italy (Masala et al., 1996); NHL, HL, and chronic lymphocytic leukemia in a rural Michigan community (Waterhouse et al., 1996); cancer mortality in four northern wheat-producing US states (Schreinemachers, 2000); mortality and incinerator dioxin emissions in municipalities in Japan (Fukuda et al., 2003); the prevalence of hypertension in Taiwanese who lived near MSWIs (Chen HL et al., 2006); and adverse pregnancy outcomes in Japan on the basis of maternal residence at the time of birth (Tango et al., 2004).
Combustion records in the Zeeburg area of Amsterdam in the Netherlands were used as a surrogate for exposure to dioxins in a study of orofacial clefts (ten Tusscher et al., 2000). The location downwind or upwind of an incineration source was used to define exposed and reference groups for the study. A study of STS in the general population was conducted around the city of Mantua in northern Italy (Costani et al., 2000). Several industrial facilities are in Mantua, and residential proximity to them was presumed to result in increased TCDD exposure, but TCDD was not measured in the environment or in human tissues.
A study of dioxin exposure pathways in Belgium focused on the long-time residents of an area in the vicinity of two MSWIs (Fierens et al., 2003a). Residents near a rural incinerator had significantly higher serum dioxin concentrations than a control group (38 versus 24 TEQ pg/g of lipid). The concentrations in people who lived near the incinerators increased proportionally with intake of local-animal fat. A second study (Fierens et al., 2003b) measured the dioxin body burden in 257 people who had been environmentally exposed in order to determine whether dioxin and PCB exposures were associated with type 2 diabetes and endometriosis. No difference in body burden was found between women who had endometriosis and women in a control group, but the risk of type 2 diabetes was significantly higher in those who had higher body burdens of dioxin-like
chemicals and of PCBs. Another study of the correlation between dioxin-like chemicals in Italian and Belgian women and the risk of endometriosis used measurements of TCDD and other dioxins in blood (De Felip et al., 2004). There was no difference in the body burden between women who had endometriosis and a control group, but the serum dioxin concentrations were substantially higher in the Belgian controls than in a similar group in Italy (45 versus 18 TEQ pg/g of lipid, respectively).
Birth Cohorts
Center for the Health Assessment of Mothers and Children of Salinas Cohort Castorina et al. (2010) compared the metabolites of current-use pesticides and other precursor compounds in 538 women in the Center for the Health Assessment of Mothers and Children of Salinas (CHAMACOS) cohort with those in 342 pregnant women in NHANES 1999–2002. CHAMACOS (Eskenazi et al., 2003b) is a longitudinal birth-cohort study investigating the effect of in utero and postnatal environmental exposures on the health of children who live in the Salinas Valley of Monterey County, California. The study enrolled 601 pregnant women from September 1999 to November 2000 in six prenatal clinics in the largely agricultural Salinas area. Women were eligible if they were no more than 20 weeks into gestation, were at least 18 years old, were qualified to receive poverty-based government health insurance, and planned to continue receiving prenatal care in a participating clinic. Personal interviews were conducted during which information on the demographics, household characteristics, health, and occupations of CHAMACOS participants was collected. Two interviews were conducted shortly after enrollment (mean, 13 weeks of gestation; standard deviation (SD), 5.2 weeks) and later in the second trimester (mean, 26 weeks of gestation; SD, 2.6 weeks) by bilingual (English and Spanish), bicultural study staff. At each prenatal interview, spot urine samples were collected from the CHAMACOS participants and analyzed for metabolites, including organophosphorus, OC chemicals, pyrethroid pesticides, herbicides, and ethylene bisdithiocarbamate fungicides. Adequate urine samples with valid creatinine concentrations were collected from 538 (90 percent) of the 601 participants at the first sampling point and 481 (80 percent) at the second. In addition, pesticide-use data were extracted from the California pesticide use reporting data set and geocoded into square-mile units. NHANES reported concentrations of current-use pesticide metabolites measured in spot urine collected from representative samples of the US population stratified by age, sex, and racial or ethnic group (Barr et al., 2005; CDC, 2004a). The NHANES comparison group consisted of 342 pregnant women 15–50 years old, a subset of the 3,048 US residents 6–59 years old who had metabolite concentrations measured in urine samples during NHANES testing in 1999 and 2002. The public-release versions of the NHANES data sets, including demographic information and metabolite data, were used for the analyses. No sample weights
were applied to the NHANES data. Descriptive analyses were conducted on the CHAMACOS and NHANES cohorts. Metabolite concentrations were compared between the two cohorts with a Wilcoxon rank-sum test and quantile regression at the 95th percentile adjusted for demographic variables, including age, current smoking (yes or no), ethnicity, and socioeconomic status. An analysis of variance was used to compare differences in detection frequency.
Duisburg Birth Cohort Study
Winneke et al. (2014) examined the relationship between early developmental exposure to dioxins and PCBs and behavioral sexual dimorphism, meaning the expression of feminine versus masculine traits. This analysis was based on the Duisburg birth cohort study and included 232 women who had no serious complications or illnesses during pregnancy or parturition and who gave birth to a child who was born at term (weeks 38–42 of pregnancy). TEQ measures were obtained from maternal blood samples taken during weeks 28–43 of gestation and from maternal milk collected from nursing mothers during the first 3 weeks after parturition. Blood samples were analyzed for PCDD/Fs and PCBs in relation to sexually dimorphic behavior, as reported by parents through completion of the Pre-School Activities Inventory. This analysis provides insight into potential endocrine-disrupting effects of prenatal environmental exposure to dioxins and PCBs in the children of female Vietnam veterans, but the relevance of behavioral sexual dimorphism as a “health” outcome of interest is unclear.
Newborns and Genotoxic Exposure Risks (NewGeneris) Cohort
The Newborns and Genotoxic Exposure Risks (NewGeneris) project (Papadopoulou et al., 2014; Vafeiadi et al., 2014) is a prospective, population-based effort that combines information on 1,151 mother–child dyads from existing European birth cohorts:
- RHEA mother–child cohort of pregnancies gathered in Heraklion, Crete, Greece, from February 2007 to February 2008.
- INMA [Infancia y Medio Ambiente (Environment and Childhood)] mother–child cohort of singleton pregnancies from Sabadell and Barcelona, Spain, from May 2007 to March 2010.
- Norwegian Mother and Child (MoBa) cohort of full-term singleton pregnancies in Oslo and Akershus, Norway, from 2007 to 2008 (only 2 years of Norwegian effort beginning in 2002).
- Danish mother–child cohort of singleton pregnancies gathered in Copenhagen, Denmark, from December 2006 to December 2007 and from September to December 2009.
- BiB (Born in Bradford) mother–child cohort of elective Caesarian sections in Bradford, United Kingdom, from January 2008–May 2009.
For many of these dyads, information about maternal diet during pregnancy and measurements of dioxin-like chemicals in maternal serum, cord blood, and breast milk were available. Standardized food frequency questionnaires were used to estimate the amount of particular food items consumed, which were in turn combined with local estimates of item-specific dioxin, furan, and PCB concentrations to derive TEQs associated with the maternal diet. Although considerable effort has been taken to validate this approach to estimating dietary intake, for the purposes of assessing association with birth outcomes, direct measurement in the biological fluids would be a more accurate characterization of the infants’ actual exposure and thus would be considered a preferable metric. Since Update 2012, several new papers have been identified that examined relationships between dioxins and dioxin-like compounds and birth outcomes in the NewGeneris cohort or its component subcohorts.
Anogenital distance, long used as a marker of androgen function in toxicology studies, has now been adopted in epidemiology studies as a means to assess the effects of exposures that may affect hormonally related outcomes. Papadopoulou et al. (2013b) addressed anogenital distance in 231 newborns in the Greek and Spanish subcohorts and in 476 Greek children at 1–2 years of age in light of their mothers’ diets during pregnancy. To estimate gestational exposure to OC contaminants, a fat-in-diet score between 0 and 11 was derived based on the mother’s self-reported frequency of consuming red meat, processed meat, fatty fish, other seafood, eggs, and high-fat dairy products. As might be expected considering the lipophilicity of these dioxin-like chemicals, the fat-in-diet scores were found to be correlated with dioxin-like activity as measured by CALUX in blood samples from 121 of the mothers. The mothers’ fat-in-diet scores were regressed against anogenital distance separately by infant sex and whether the mother consumed seafood, with adjustment for the infant’s birth weight and for maternal ethnicity, age, and smoking. Here again, however, direct use of the results from maternal blood samples as done by Vafeiadi et al. (2013), would be regarded as a more meaningful approach to assessing association.
Vafeiadi et al. (2013) used dioxin-like activity measured by CALUX assays in maternal blood samples collected at the time of delivery and anogenital distance. Included in the analyses were 237 newborns (119 boys and 118 girls) and 462 children aged 1–31 months (239 boys and 223 girls) each with anogenital distance measured in three ways. Regression analyses in terms of 10 pg CALUX-TEQ/g lipid with adjustment for an infant’s birth weight and gestational age at birth or child’s weight and age at time of examination, plus maternal ethnicity and education, were conducted separately by gender and age group
Papadopoulou et al. (2014) considered the entire NewGeneris cohort when investigating the relationship between a potentially dioxin-rich dietary pattern during pregnancy and gestational age and birth weight in 604 births. The fat-in-diet
scores were shown to be correlated with CALUX measurements in blood samples drawn from the mothers at delivery and divided into tertiles. The high and middle groups were compared to the lowest tertile for maternal education, energy intake, age, pre-pregnancy BMI, parity, smoking, and country of cohort, plus infant’s gestational age and gender. This study is limited by its reliance on a self-report food-frequency questionnaire rather than on actual plasma dioxin levels, an entirely different exposure history (dietary intake) compared to the spraying of herbicides, and its relevance only to childbearing female Vietnam veterans.
Vafeiadi et al. (2014) assessed CALUX measures of dioxin-like activity in maternal and cord blood plasma samples collected at delivery in relation to birth weight, gestational age, and head circumference. Birth information and at least one CALUX result were available from 967 singleton births in the entire NewGeneris cohort. Analyses were conducted separately for cord plasma and maternal plasma and also by country. Multiple linear-regression models were fit with adjustments for a range of covariates, including country, gestational age, maternal pre-pregnancy BMI, type of delivery, and sex of the child. Moreover, effect modification was examined among subgroups of interest, including sex of the child, maternal smoking status, and pre-pregnancy BMI. Strengths of this analysis include the large, diverse sample of childbearing women and objective measures of dioxin-like activity and birth outcomes. The results are limited by their direct relevance only to childbearing female Vietnam veterans and the unknown long-term clinical significance of the birth outcomes examined.
Norwegian Mother and Child Cohort Study
In a very large analysis from the entire Norwegian Mother and Child Cohort Study (MoBa) as assembled from 2002–2008, Papadopoulou et al. (2013a) investigated birth weight, length, and head circumference in relation to the estimated intake of dioxin-like chemicals from the maternal diet. After limiting analysis to babies with gestational ages of 29–42 weeks and excluding mothers whose energy intake (< −4,500 or > 20,000 kilojoules) or weight gain during pregnancy (< −30 or > −50 kg) were deemed implausible, a total of 50,651 singleton pregnancies remained. Regression analyses were conducted separately by infant gender and seafood intake during pregnancy with adjustment for maternal age, energy intake, maternal education, pre-pregnancy BMI, parity, weight gain and smoking during pregnancy, and gestational age and sex of the child. The limitations of this study include its reliance on self-report food-frequency intake to estimate dioxin exposure and its direct relevance only to childbearing female Vietnam veterans.
Taiwanese Mother-and-Child Studies
A prospective study of healthy Taiwanese mothers and their children recruited during the mothers’ pregnancy was conducted as a way to study the
associations between exposures to PCDDs, PCDFs, and PCBs and health outcomes (Chao et al., 2004, 2007; Su et al., 2010, 2012; Wang et al., 2004, 2005). The study enrolled pregnant women who had no clinical complications, were 25–35 years old, and delivered in the period December 1, 2000, to November 30, 2001 in a medical center in suburban Taichung in central Taiwan, the location of a solid-waste incinerator. Participants completed a questionnaire concerning maternal age, occupation, disease history, cigarette smoking, alcohol consumption, dietary habits, and baby’s stature. Biologic samples (including placenta, umbilical cord blood, mother’s venous blood, and breast milk) were collected for analysis of PCDDs, PCDFs, and PCBs. A total of 610 women were enrolled (80 percent of those invited). The placenta was collected from and the questionnaire completed by 430 participants. Of those, 250 provided sufficient venous blood for the chemical analyses. Of the 250, 175 provided adequate breast-milk samples. Wang et al. (2004) reported on PCDDs, PCDFs, and PCBs in the biologic samples and correlations among specimens. Chao et al. (2004) reported on PCDDs, PCDFs, and PCBs in breast milk and the cumulative dose derived for infants exclusively breastfed versus those formula-fed.
Wang et al. (2005) examined the association between in utero exposure to PCDDs, PCDFs, and PCBs and the thyroid and growth hormones in the newborns. The hormone concentrations were compared between infants with high- versus low-dioxin/PCB TEQ (above versus below the median) and between females (62) and males (57) by using a two-sample t test or the Mann-Whitney U test (when the distribution deviated significantly from the normal distribution assumed for the t test). Spearman’s correlation was used to evaluate the association between the hormone concentrations and the PCDD, PCDF, and PCB concentrations. Further analyses were carried out with stepwise multivariate regression analysis to adjust for age and other covariates selected through the stepwise selection procedure. Wang et al. (2006) examined the association between PCDDs, PCDFs, and PCBs measured in the placenta samples and estrogens and metabolites measured in mothers’ blood samples by using Pearson correlations, linear and quadratic regressions, and multivariate regression analyses.
Su et al. (2010) reported on the 2-year and 5-year follow-ups of the mother–child pairs of Wang et al. (2005). Children’s anthropomorphic measures were obtained, including height, weight, BMI, head circumference, chest girth, bone age, and the ratio between bone age and chronologic age. Thyroid, sex-hormone, and growth-factor concentrations were measured in venous blood samples obtained from those children whose mothers’ serum PCDD and PCDF TEQs were available. The anthropomorphic measures and the thyroid, sex-hormone, and growth-factor concentrations were compared by sex (29 and 14 males at years 2 and 5, respectively, and 41 and 27 females at years 2 and 5, respectively) and pooled across sexes; those who had high versus low in utero PCDD and PCDF concentrations (≥ 15 versus < 15 pg-TEQ/g of lipid) were compared with a two-sample t test or (when not normally distributed) a Wilcoxon rank-sum test.
Further analyses were conducted with multiple regression and stepwise selection for detecting factors that might affect growth or hormone concentrations. Su et al. (2012) reported on the 8-year follow-up of the same cohort in a subset of 23 boys and 33 girls, substantially more than the numbers examined in the 5-year follow-up. In addition to anthropomorphic measures used in previous waves, reproductive development (breast, genital, and armpit stages) were assessed.
CASE-CONTROL STUDIES
Cross-Canada Study of Pesticides and Health (Rare Tumors Study)
After a pilot study done for the Canadian government, McDuffie et al. (2001) initiated a full population-based case-control study of men in six Canadian provinces that addressed several fairly uncommon malignancies—HL, NHL, multiple myeloma (MM), and STS—and the relationship between their occurrence and exposure to pesticides (both occupationally and domestically). A target number of cases of each cancer type was preset for each province; cases newly diagnosed starting on September 1, 1991, were gathered from the provincial cancer registries or hospital records in Quebec until the end of 1994 or until the target number was reached. Physician consent was obtained, diagnoses were confirmed with pathology reports and preserved tissues, and consent forms and questionnaires were sent to the cases. The controls were men at least 19 years old identified in the health-insurance records of Alberta, Saskatchewan, Manitoba, and Quebec; telephone listings for Ontario; and voter lists in British Columbia. The controls were selected randomly in order to obtain a stratified age distribution matching that of the cases. The controls, too, were sent consent forms and questionnaires. People who died were dropped from the study, as were people who had Kaposi sarcoma or were HIV positive. All 1,506 controls who responded were used in comparisons for each of four cancer groups: 316 HL cases, 517 NHL cases, 342 MM cases, and 357 STS cases.
The postal questionnaire gathered standard demographic information, personal and family medical histories, employment history, smoking behavior, and basic data on pesticide exposure. The pilot study tested the reliability of self-reported pesticide use by comparison with purchase records. Any subject who reported at least 10 hours of pesticide exposure per year was asked to complete a telephone questionnaire on the details of pesticide exposure; in addition, 15 percent of the remaining subjects were randomly selected to answer the telephone survey. A conditional logistic regression stratified on age and province and adjusted for all covariates found to be associated with the outcome at the 0.05 level of significance was used to estimate ORs for specific active ingredients, including dicamba and the phenoxy herbicides 2,4-D, Mecoprop, MCPA, and diclofopmethyl. Dose–response relationships were investigated for the cumulative categories of time spent in mixing or applying particular products.
A series of publications have addressed the relationship between each of the cancers and various risk factors. Those pertaining to herbicides overall or to the particular ones of interest are as follows:
- HL—Karunanayake et al., 2012; Pahwa et al., 2003
- NHL—Hohenadel et al., 2011; McDuffie et al., 2001
- MM—P Pahwa et al., 2003, 2012b
- STS—Pahwa et al., 2003, 2011
A number of other publications arising from that data set have addressed topics somewhat more tangential to the interests of the VAO reports. For instance, McDuffie et al. (2005) and Pahwa et al. (2006) considered the possible interaction of exposure to insect repellents, particularly N,N-diethyl-m-toluamide (DEET) and phenoxy herbicides, in the genesis of the malignancies in question. McDuffie et al. (2009) examined family histories of cancers in first-degree relatives of the study participants (1,528 cases and 1,506 controls) to assess the interaction between family history and pesticide exposure. Hohenadel et al. (2011) investigated how various combinations of pesticide exposures influenced the occurrence of NHL. Ghosh et al. (2011) investigated the association of occupational exposures other than to pesticides with the occurrence of MM.
Since Update 2012, Pahwa M et al. (2012) analyzed data from the Cross-Canada Study of Pesticides and Health (CCSPH) population-based case-control study to examine the interactions between pesticide exposures and measures of immune suppression (asthma, allergies, hay fever) and risk of NHL. The analysis included 513 incident pathologically confirmed NHL cases diagnosed between the years 1991 and 1994 and 1,506 randomly selected controls identified from provincial health insurance records. Lifetime occupational history and pesticide use and other exposures were based on self-report, as was the diagnosis of various immunologic conditions. Multiple logistic regression models were fit with statistical adjustment for age, province of residence, respondent type (self or proxy), and diesel oil exposure. In addition, analyses were stratified by self-report of asthma, allergies, or hay fever versus non-reporting of such conditions. The limitations of this analysis include the self-report measurement of immunologic conditions and the nonspecific and crude self-report classification of pesticide use, which did not characterize exposure use by duration, intensity, or frequency. In addition, the focus of this analysis on the interaction between immunological conditions and pesticide use in relation to risk of NHL is not directly relevant to assessment of the effects of Agent Orange alone among Vietnam veterans.
In a second, similar examination of risk of HL in men from the CCSPH, Navaranjan et al. (2013) classified pesticide use into the categories of 0, 1, 2–4, and 5 pesticides and grouped by class, including herbicides, insecticides, and fungicides. The analysis included 316 HL cases and 1,506 control subjects. Multiple logistic regression models were fit with statistical adjustments for age and
province of residence. In addition, analyses were stratified by subjects younger than age 40 versus age 40 and older. The assessment of the effect of pesticide exposure also included estimates for work-related exposure and home-related exposure. As with Pahwa M et al. (2012), this study is limited by the relatively nonspecific and crude self-report classification of pesticide use. This significantly limits direct inference to the effects of herbicide exposure during military service in Vietnam.
Children’s Oncology Group Study (United States)
In two related case-control studies, Chen Z et al. reported on exposure to pesticides (including herbicides) and the risk of childhood germ-cell tumors. One study focused on parental occupational exposures (Chen Z et al., 2005) and the other on parental exposures to residential pesticides and chemicals (Chen Z et al., 2006), but they are based on the same overall case-control study.
No reports from the Children’s Oncology Group have been published since Update 2008.
National Birth Defects Prevention Study
The National Birth Defects Prevention Study (NBDPS) is a population-based case-control study conducted cooperatively by CDC and eight monitoring centers throughout the United States using a standardized study methodology (Yoon et al., 2001). Starting in October 1, 1997, the individual centers began monitoring births in their respective areas for the occurrence of more than 30 types of birth defect (excluding cases attributable to single-gene conditions or chromosomal abnormalities) for comparison with randomly selected sets of live-born babies without malformations. Information about demographics and possible exposures is abstracted from an extensive telephone interview that the mothers complete within 24 months of delivery, which raises concerns about recall bias addressed by the researchers. On the basis of the work histories, job classifications are assigned by an industrial hygienist and processed using a JEM and expert opinion used to derive occupational exposures. Bucchal samples are gathered for DNA testing from the infant and its parents.
Rocheleau et al. (2011a) reported on the association between maternal occupational pesticide exposure and the risk of hypospadias in the NBDPS. This was a case-control study with 647 cases of hypospadias and 1,496 controls with estimated delivery dates of October 1997–December 2002 identified by the surveillance centers in Arkansas, California, Georgia, Iowa, Massachusetts, New Jersey, New York, and Texas. Mothers were interviewed about their job status, which was then formally coded. Typical pesticide ratings were assigned to the job codes. The duration and confidence in the exposure were used to refine them. A complete case analysis was conducted, with some sensitivity analysis around
missingness (creation of a missing category). Most exposure was to insecticides only or to all three types of pesticide (insecticides, herbicides, and fungicides). The analysis did not include fetuses that died with hypospadias. Multiple comparisons are a concern. There was generally a low level of occupational pesticide exposure in the study population. Other exposures of the population could cause the outcome in question.
Using data from the NBDPS, Kielb et al. (2014) analyzed the occurrence of isolated craniosynostosis, gastroschisis, diaphragmatic hernia, or transverse limb deficiencies among employed women with due dates from October 1, 1997, to December 31, 2002. Cases included 871 live-born, stillborn, or electively terminated fetuses, which were compared to 2,857 live-born control infants. The odds of these musculoskeletal malformations were examined in relation to periconceptional maternal occupational exposure to insecticides, herbicides, or fungicides (classified as yes/no) for each job held during 1 month pre-conception through 3 months post-conception. Multiple logistic regression models were fit with adjustments for age, race, ethnicity, education, smoking, singleton versus multiple birth, BMI, folic acid use during pregnancy, and gravidity. The limitations of this analysis include the nonspecificity of pesticides with respect to the herbicides sprayed in Vietnam, the crude assessment of exposure history (yes/no) by self-reported occupational history, and its potential direct relevance only to childbearing female Vietnam veterans.
Several papers from the California Center of the NBDPS have been published since Update 2012. It has monitored deliveries in the San Joaquin Valley for 1997 to 2006 and has invested considerable effort toward developing time-specific estimates of exposure to individual pesticides by women residing in the area at the time of delivery.
Carmichael et al. (2014) evaluated 569 congenital heart defect cases (8 different types) and 785 non-malformed controls born during 1997–2006. Maternal pesticide exposure was crudely classified as “any” versus “no exposure” based on the commercial application of pesticides within a 500-meter radius of the mother’s address during a 3-month periconception window. The determination of the proximity-based pesticide application exposure was based on data obtained from the California Pesticide Use Reporting (PUR) record system concerning agricultural pesticide applications occurring during the periconception intervals corresponding observation period for births. Multiple logistic regression models were fit with statistical adjustments for maternal race/ethnicity, education, age, intake of folic acid–containing supplements, alcohol, and smoking during the month before and the first 2 months of pregnancy. Exposure to individual pesticides was examined, including the dimethylamine salt of 2,4-D. Analogous investigations were conducted on neural tube defects and orofacial clefts (Yang et al., 2014) and on gastroschisis (Shaw et al., 2014). The strengths of these studies include that it was population based and that it used medically confirmed occurrences of congential heart defects and an objective geocoded source of pesticide
exposure classification. Their limitations include a crude binary classification of pesticide exposure (yes/no) rather than dose–response estimation and the very large number of statistical comparisons made without correction for potential false-positive findings.
Upper Midwest Health Study
The Upper Midwest Health Study (UMHS) was initiated by NIOSH as a population-based case-control study of cancer risk in a nonmetropolitan Mid-western US population. Several reports from the study were reviewed in previous updates. Chiu et al. (2004) and Lee et al. (2004a) conducted pooled (combined) analyses of two earlier case-control studies of NHL carried out by the UMHS in Iowa and Minnesota (Cantor et al., 1992) and Nebraska (Zahm et al., 1990). Chiu et al. (2004) examined the association of NHL with agricultural pesticide use and familial cancers, and Lee WJ et al. (2004a, 2006) looked at NHL in asthmatic people who reported pesticide exposure. Data from Nebraska (Chiu et al., 2006, based on Zahm et al., 1990, 1993), were used to identify whether there was a higher risk of subtypes of NHL. Specifically, tissue samples were analyzed according to the presence of a specific chromosomal translocation (t[14;18] [q32;q21]); only 172 of 385 cases were included.
Two studies focused on pesticide use and the risk of adenocarcinomas of the stomach and esophagus (Lee et al., 2004b) and the risk of gliomas (Lee et al., 2005). The participants were white Nebraska residents over 21 years old who were identified from the Nebraska Cancer Registry and matched to controls drawn from an earlier study by Zahm et al. (1990).
The researchers evaluated farm pesticide exposure in men (Ruder et al., 2004) and women (Carreon et al., 2005) in Iowa, Michigan, Minnesota, and Wisconsin in relation to gliomas as part of the UMHS. Ruder et al. (2006) reported a follow-up of Ruder et al. (2004) that evaluated gliomas in UMHS participants. The new analyses provided no evidence of greater use of pesticides in cases than in controls, and there was no breakdown by specific agents.
Ruder et al. (2009) reported another follow-up, which had similar findings and no breakdown by specific agents.
Since Update 2010, Yiin et al. (2012) has reported findings from new analyses of the UMHS sample that incorporated more detailed exposure information that was not used in previous analyses, including years of use and estimated cumulative exposures to categories of pesticides, including phenoxy herbicides, and the use of specific agents, including 2,4-D and dicamba.
Other Case-Control Studies
Numerous case-control studies have been reviewed in previous updates. In 1977, case-series reports in Sweden (Hardell, 1977, 1979) of a potential
connection between exposure to phenoxyacetic acids and STS prompted several case-control investigations (Eriksson et al., 1979, 1981, 1990; Hardell, 1981; Hardell and Eriksson, 1988; Hardell and Sandström, 1979; Wingren et al., 1990). After the initial STS reports (Hardell, 1977, 1979), case-control studies of other cancer outcomes were conducted in Sweden: HL and NHL (Hardell and Bengtsson, 1983; Hardell et al., 1980, 1981; Persson et al., 1989, 1993), NHL (Hardell and Eriksson, 1999; Olsson and Brandt, 1988), nasal and nasopharyngeal carcinomas (Hardell et al., 1982), gastric cancer (Ekström et al., 1999), and primary or unspecified liver cancer (Hardell et al., 1984). To address criticism regarding potential observer bias in some of the case-control series, Hardell (1981) conducted another case-control study of colon cancer. Hardell et al. (1994) also examined the relationship between occupational exposure to phenoxyacetic acids and chlorophenols and various characteristics related to NHL—including histopathologic measures, stage, and anatomic location—on the basis of the NHL cases in a previous study (Hardell et al., 1981).
Prompted by the Swedish studies (Hardell, 1977, 1979), Smith et al. (1983, 1984) and Smith and Pearce (1986) conducted a set of case-control studies to evaluate the association between phenoxy herbicide and chlorophenol exposure and STS incidence and mortality in New Zealand. An expanded case series was collected, and additional case-control studies of exposure to phenoxy herbicides or chlorophenols and the risks of malignant lymphoma, NHL, and MM were conducted (Pearce et al., 1985, 1986a,b, 1987).
Geographic patterns of increased leukemia mortality in white men in the central part of the United States prompted a study of leukemia mortality in Nebraska farmers (Blair and Thomas, 1979). Additional case-control studies of leukemia were later conducted in Nebraska (Blair and White, 1985), in Iowa (Burmeister et al., 1982) on the basis of the cohort study of Burmeister (1981), and in Iowa and Minnesota (Brown et al., 1990). Another study investigated leukemia in association with NHL and 2,4-D in eastern Nebraska (Zahm et al., 1990).
Case-control studies have been conducted in various US populations looking for associations of herbicides with other cancers, including NHL (Cantor, 1982; Cantor et al., 1992; Hartge et al., 2005; Tatham et al., 1997; Zahm et al., 1993); MM (Boffetta et al., 1989; Brown et al., 1993; Morris et al., 1986); gastric cancer, prostate cancer, NHL, and multiple myeloma (Burmeister et al., 1983); STS, HL, and NHL (Hoar et al., 1986); NHL and HL (Dubrow et al., 1988); and STS and NHL (Woods and Polissar, 1989; Woods et al., 1987). In a subset of participants in the Hartge et al. (2005) study, De Roos et al. (2005b) studied associations between the overall TEQs of PCBs, furans, and dioxins but not TCDD alone.
Other case-control studies conducted outside the United States have addressed various cancers: STS and other cancers in the 15 regional cancer registries that constitute the National Cancer Register in England in connection with the COIs (Balarajan and Acheson, 1984); ovarian cancer in the Piedmont region of Italy (Donna et al., 1984); STS in rice weeders in northern Italy (Vineis et al.,
1986); mortality from esophageal cancer, pancreatic cancer, cutaneous melanoma, renal cancers, and brain cancer in three English counties (Magnani et al., 1987); brain gliomas in two hospitals in Milan, Italy (Musicco et al., 1988); lymphoid cancer in Milan, Italy (LaVecchia et al., 1989); primary lung cancer in pesticide users in Saskatchewan (McDuffie et al., 1990); STS and malignant lymphomas in the Victorian Cancer Registry of Australia (Smith and Christophers, 1992); oral-cancer risk in occupationally exposed workers in Sweden (Schildt et al., 1999); and renal-cell carcinoma in the Denmark Cancer Registry (Mellemgaard et al., 1994). Nanni et al. (1996) conducted a population-based case-control study, based on the work of Amadori et al. (1995), of occupational and chemical risk factors for lymphocytic leukemia and NHL in northeastern Italy.
Noncancer health outcomes have also been investigated in case-control studies: Spontaneous abortion (Carmelli et al., 1981); congenital malformations (García et al., 1998); immunosuppression and later decreased host resistance to infection in AIDS patients who had Kaposi sarcoma (Hardell et al., 1987); mortality in the US Department of Agriculture extension agents (Alavanja et al., 1988) and conservationists (Alavanja et al., 1989); PD associated with occupational risk factors (Semchuk et al., 1993); birth defects in the offspring of agriculture workers (Nurminen et al., 1994); mortality from neurodegenerative diseases associated with occupational risk factors (Schulte et al., 1996); PD associated with various rural factors, including exposure to herbicides and wood preservatives (Seidler et al., 1996); spina bifida in offspring associated with paternal occupation (Blatter et al., 1997); PD associated with occupational and environmental risk factors (Liou et al., 1997); and mortality from neurodegenerative diseases, including Alzheimer disease and presenile dementia, PD, and motor neuron disease associated with occupational factors (Park et al., 2005). Those studies have been discussed in detail in previous updates.
Orsi et al. (2009) studied the association between occupational exposures to pesticides and lymphoid neoplasms by using a hospital-based case-control study in the main hospitals of six French cities (Brest, Caen, Nantes, Lille, Toulouse, and Bordeaux) from September 2000 to December 2004. Cases were eligible if they were male, were 20 to 75 years old, were residing in the hospital’s catchment area (the administrative department where the hospital is or a neighboring department), lacked a history of immunosuppression or of taking immunosuppressant drugs, and had recently received a diagnosis of any lymphoid neoplasm except acute lymphoid leukemia. The diagnoses were classified using WHO’s International Classification of Diseases for Oncology, third edition, codes and was confirmed cytologically or histologically by a panel of pathologists and hematologists. Among the 513 eligible incident cases, 491 (96 percent) participated: 87 with HL, 244 with NHL, 56 with MMs, and 104 with lymphoproliferative syndrome (LPS). The controls were male patients from the same hospitals who had no prior history of lymphoid neoplasm (LN), were residing in the hospital’s catchment area, and were not admitted to the hospital
for conditions directly related to occupation, smoking, or alcohol abuse. The controls were individually matched with the cases by hospital and age (± 3 years). Among the 501 eligible controls, 456 (91 percent) participated. Participants were given a self-administered questionnaire, had a face-to-face interview, and had a re-interview by an occupational hygienist and an agronomist when needed to collect socioeconomic and lifestyle information, personal and family medical history, residential and occupational histories, and detailed information on occupational and nonoccupational exposure to herbicides and pesticides. Dichotomous exposure measures (ever or never exposed) were constructed for each category (insecticides, fungicides, and herbicides) and for each chemical family (such as OC chemicals and phenoxy herbicides). Unconditional logistic regression was used to estimate the ORs and CIs for each outcome (all LN, NHL, HL, LPS, and MM) and chemical exposure with adjustments for age, hospital, and socioeconomic category (white-collar or blue-collar). Logistic regression was used for NHL subtypes (diffuse large B-cell lymphoma, follicular lymphoma, and other NHL) and LPS (chronic lymphocytic leukemia and hairy-cell leukemia).
Spinelli et al. (2007) conducted a population-based case-control study of histologically confirmed NHL in men and women 20 to 79 years old who lived in the greater metropolitan areas of Vancouver and Victoria, British Columbia, from 2000 through 2004. Population controls, frequency-matched to cases by 5-year age groups and area, were identified from the client registry of the provincial health care system. A random subset of controls was included in the analyses. The analyses were based on concentrations of OC and related chemicals in serum obtained from controls at the time of interview and from cases before chemotherapy. NHL patients who lost weight rapidly were excluded. Ng et al. (2010) examined SNPs in the AHR gene that were genotyped for the same study cohorts (422 NHL cases and 459 controls) to measure the association between individual SNPs, haplotypes, and the risk of NHL. Gene–environment interaction analyses were conducted for OC chemicals and AHR SNPs by using logistic regression.
Hartge et al. (2005) conducted a case-control study that used four NCI SEER registries (Detroit, Iowa, Los Angeles County, and Seattle) to look for associations between herbicides and NHL. In a subset of participants in the Hartge et al. study, De Roos et al. (2005b) studied associations between NHL and the overall TEQs of PCBs, furans, and dioxins but not TCDD alone. Colt et al. (2009) studied whether the relationship between OC exposure and NHL was modified by immune-gene variation in the SEER study participants (1,172 cases and 513 controls). The study genotyped 61 polymorphisms in 36 immune genes and examined three exposures measured in plasma and dust: to PCB 180, to OC pesticides (TEQ), and to α-chlordane. Unconditional logistic regresson was used to estimate the exposure–outcome association with stratification by genotype and adjustments for sex, age, race, education, and study region.
Firestone et al. (2005) reported on a population-based case-control study of incident PD cases in Washington state (250 cases and 388 controls). PD cases were identified in 1992–2002 at the Group Health Cooperative (GHC, a large managed-care organization) or the University of Washington. Control participants were sampled randomly from GHC enrollees who had no history of PD or other progressive neurologic disorder and were frequency-matched to cases by age, sex, GHC clinic location, and year of GHC enrollment. Participants were interviewed to obtain information on demographics, medical and occupational history, occupational and home-based pesticide use, drinking-water source, residential history, and smoking history. Both occupational exposures and residential exposures were reported. No specific COIs were reported beyond the broad category “herbicide.” Unconditional logistic regression was used to estimate the association between PD and exposure with adjustments for age, sex, and smoking.
Firestone et al. (2010) provided an expanded update (404 cases and 526 controls) that extended the same recruitment protocol through 2006. The participation rates were good among eligible cases (70 percent) and modest among eligible controls (60 percent); this left some room for selection bias due to nonresponse. Only occupational exposures were reported. Exposures to specific chemicals were reported, including 2,4-D (9 exposed cases and 12 exposed controls).
This page intentionally left blank.






















































































































