
4
Universal/Preventive and Widely Used Interventions
This chapter reviews the evidence on interventions for strengthening parenting capacity and supporting parents of young children, from the prenatal period through age 8. The focus is on universal and widely used interventions that touch large numbers of families and that are primarily preventive, such as those delivered in health care settings; those delivered in connection with child care, early education, and K-3 schooling; and public education approaches. 1 These interventions and approaches generally emphasize providing parents with knowledge and guidance about children’s development and successful parenting practices; many also connect parents to a variety of needed support services. Following this review, the chapter turns to a discussion of the use of information and communication technologies to support parenting. The chapter then examines the research evaluating the impact on parenting of income, nutrition, health care, and housing support programs and parental and family leave policies described in Chapter 3. The chapter concludes with a summary.
UNIVERSAL/PREVENTIVE INTERVENTIONS
Parents seek knowledge about how to raise their children from many sources, including both formal programs and information they obtain on
___________________
1 A useful framework for thinking about interventions is described in the National Research Council and Institute of Medicine (2009) report Preventing Mental, Emotional, and Behavioral Disorders among Young People. In the prevention area, this framework specifies mental health promotion; universal interventions defined as those that are valuable for all children; and selective interventions, which are targeted at populations at high risk.
their own. Numerous books, magazine articles, and Websites provide information about parenting. Whereas earlier generations may have relied on books such as Benjamin Spock’s Baby and Child Care (e.g., Spock, 1957, 1968, 1976) and later generations on guidance from T. Berry Brazelton and Harvey Karp (Brazelton, 1992; Karp, 2002; Karp and Spencer, 2004), parents today are seeking information from a more diverse array of print, online, and human resources. Some of the information that is available is not grounded in evidence.
Parents seek information and guidance in particular about actions they can take that apply to the developmental stage of their child (e.g., infancy, toddlerhood, early childhood, early school age). They naturally look to their extended family (e.g., their own parents, siblings), the community (including others who are raising their own children), faith-based institutions, and community organizations for guidance and support. All of these sources contribute to parents’ knowledge, attitudes, and practices with respect to raising their children. In the best cases, parents have access to and knowledge of multiple resources and are able to draw on them as needed.
There are also a variety of formal sources of parenting information, guidance, and support. These sources include primary care practitioners who provide guidance on early learning, well-child care and guidance, and other health care for children. In some communities, this role also is filled by visiting nurses and others in both lay and professional disciplines with experience in parenting. Other formal programs discussed in this chapter include center-based child care and comprehensive early care and education (ECE) programs (e.g., Head Start and Early Head Start). These programs, sometimes referred to as universal interventions, reflect the shared needs of children and families for health care, educational preparation, and general support.
Well-Child Care2
Well-child care refers to preventive care visits for children that include not only basic health care, vaccination, and developmental assessment but also anticipatory guidance (counseling and education on a broad variety of topics aimed at supporting parents) and identification of family concerns that can serve as a barrier to good parenting. Conducted by pediatricians, family physicians, and other primary care providers, well-child care is a
___________________
2 Portions of this section are based on a paper commissioned for this study, authored by Tumaini R. Coker, assistant professor of pediatrics at the David Geffen School of Medicine and Mattel Children’s Hospital, and associate director of health services research at the Children’s Discovery and Innovation Institute, University of California, Los Angeles. The paper can be requested from the study public access file at https://www8.nationalacademies.org/cp/ManageRequest.aspx?key=49669 [October 2016].
mainstay of families’ interaction with the health care system. In 2013, 92 percent of children under the age of 6 and covered by health insurance had had a well-child visit in the past year (Child Trends Databank, 2014). In the 0-8-year age range, the American Academy of Pediatrics (AAP) recommends a regular schedule of multiple well-child visits during the first 2 years and annual visits thereafter and specifies that each visit should include a physical exam, anticipatory guidance, and developmental/behavioral assessment (American Academy of Pediatrics and Bright Futures, 2016). Several other organizations, including the U.S. Preventive Services Task Force and the American Academy of Family Physicians have developed similar well-child care recommendations (American Academy of Family Physicians, 2005; U.S. Preventive Services Task Force, 2015). Visits may be conducted either individually or in a group format.
Anticipatory guidance is intended to help parents prepare for and deal with issues and concerns—such as anticipated developmental steps and situational crises—they may encounter as their child grows. Guidelines for anticipatory guidance encompass a broad variety of topics pertinent to supporting evidence-based parenting knowledge and practices, ranging from promoting children’s health and safety (e.g., guidance on helmet use, gun safety, treatment and counseling on overweight and obesity, guidance for parents on tobacco cessation), to appropriate discipline techniques, to managing difficult child behavior (e.g., sibling rivalry, tantrums) (American Academy of Pediatrics, 2000, 2002; Green and Palfrey, 2002). Multiple randomized controlled studies have examined tools for enhancing anticipatory guidance, such as telephone advice lines, supplemental parent education via DVD, Websites, and waiting-room kiosks (Bergman et al., 2009; Christakis et al., 2006; Kempe et al., 1999; Paradis et al., 2011; Sanghavi, 2005). Most of these supplemental interventions have failed to show substantial benefits, but efforts to improve safe sleep by means of video education modules and nurse education for parents have shown promising results in uncontrolled trials (Canter et al., 2015; Goodstein et al., 2015). (See also the section on information and communication technologies later in this chapter.)
Unfortunately, many families do not receive all of the parenting support and guidance that is recommended in well-child care guidelines. A shortage of provider time to cover the full range of topics may be one of the most important factors in the observed variation in the quality of well-child care. Longer well-child visits have been associated with more anticipatory guidance, more psychosocial risk assessment, and better ratings of family-centeredness of care in survey research with parents (Halfon et al., 2011). Yet the AAP has estimated that it would take a clinician 90 minutes to complete just one visit if all of its guidelines were followed (American Academy of Pediatrics, 2004). Given the time limitations for well-child visits (often constrained to 15-30 minutes), there have been efforts to expand the scope
of visits by partnering families with nonphysician providers who can offer education, guidance, and counseling services to augment the care provided during formal visits, either within or outside of those visits (Farber, 2009; Zuckerman et al., 2004). However, the qualified personnel needed to provide those services are lacking.
In general, although well-child visits, including anticipatory guidance, likely support parenting and the achievement of evidence-based parenting knowledge, attitudes, and practices (e.g., vaccination), and several interventions have been designed to enhance the effectiveness of well-child care, evaluation of these interventions is limited. In addition, there is a lack of objective measures with which to evaluate effects of these interventions on parenting behavior or to identify the optimal mode of delivery of well-child care (O’Connell et al., 2015).
Some models of care and enhanced anticipatory guidance have proven successful, particularly by extending the resources provided during the initial visit through regular contact and support. Healthy Steps for Young Children is a model of care and enhanced anticipatory guidance in which a pediatric health care provider and a child specialist with training in child development (e.g., nurse, social worker) partner to provide well-child care. The specialist spends extra time with the family after the physician visit, offering home visits and connecting the family with telephone help lines, parent support groups, and community resources (Zuckerman et al., 2004). Most of the evaluations of Healthy Steps have focused on parenting outcomes rather than child outcomes (Piotrowski et al., 2009). A systematic review of experimental and quasi-experimental studies (Piotrowski et al., 2009) found that this model provided parents with effective developmental screening and anticipatory guidance (Caughy et al., 2003, 2004; Huebner et al., 2004; Johnston et al., 2006; Kinzer et al., 2004; McLearn et al., 2004; Minkovitz et al., 2003; Niederman et al., 2007). For example, parents reported improved parenting practices with respect to discipline, safety, and promotion of early reading (Minkovitz et al., 2003a). Other positive outcomes from Healthy Steps include parents reporting greater knowledge of infant development, better recognition of appropriate discipline, improved compliance with immunization and well-child visit schedules, and increased satisfaction with pediatric care (Johnston et al., 2006; Minkovitz et al., 2003).
Another program, the Parent-focused Redesign for Encounters, Newborns to Toddlers (PARENT) intervention (Coker et al., 2016), employs a team-based approach to care in which a parent coach provides the bulk of services at well-child visits and addresses specific needs faced by families in low-income communities. An initial randomized evaluation of this model among 251 parents found positive effects on parents’ receipt of anticipatory guidance and health information, psychosocial assessment, and other
services. Parents participating in the intervention had significantly reduced emergency department use (22% of control parents versus 10% of intervention parents reported two or more emergency department visits in the past 12 months) (Coker et al., 2016).
Finally, a well-known program designed to support early literacy, Reach Out and Read, provides caregivers of young children with free, age-appropriate books and anticipatory guidance on the importance of child literacy at each well-child care visit to promote caregiver-child reading. As noted in a recent review, the existing evidence on this program is limited by nonrandom designs, data collected by self-report, and high participant dropout rates (Yeager Pelatti et al., 2014). That said, a recent cross-sectional survey of eight Reach Out and Read sites found that caregivers provided with at least four books read to their children more often than those who received fewer books (Rikin et al., 2015). Other observational studies of the program also have found that it is associated with improvement in the home literacy environment for children, particularly for parents who might otherwise face obstacles in this regard, with parents participating in the program being more likely to report having books in the home and reading aloud to and looking at books with their children (Needlman et al., 2005; Zuckerman, 2009). However, there have been no studies of the reading scores of children whose caregivers participate in Reach Out and Read.
Patient-Centered Medical Homes and Shared Decision Making
The patient-centered medical home is a relatively new model of care in which primary care providers serve as the medical home for patients, offering team-based and coordinated care to increase the receipt of preventive services and reduce the need for specialty or emergency room care. Early findings from a review of randomized controlled trials and longitudinal studies suggest that interventions based on this model have a small positive impact on patient experiences with health care and a small to moderate effect on the delivery of primary care services (Jackson et al., 2013). Family-centered care recognizes a partnership among patients, families, and health care professionals and encourages shared decision making (Scholle et al., 2010), which can improve patients’ knowledge about treatment options and risk perceptions and help them take a more active role in decisions about their care (Stacey et al., 2014). In meta-analyses of studies using various designs, shared decision-making interventions designed to engage pediatric patients, parents, or both in medical decisions significantly reduced decisional conflict and improved parents’ knowledge of their children’s health conditions and how to manage them (Wyatt et al., 2015).
Universal Health Interventions for Parents for Specific Parenting Behaviors
Many interventions for parents that occur within health care settings support parents in engaging in empirically grounded parenting practices outlined in Chapter 2 that promote the physical health of their children. Examples of these practices include receiving preconception and prenatal care, breastfeeding, complying with recommended immunization schedules, limiting children’s screen time, helping children avoid overweight and obesity, reducing children’s exposure to environmental tobacco smoke, and educating caregivers on normal infant crying to reduce shaken baby syndrome/abusive head trauma.
Preconception and Prenatal Interventions
Self-identification as a parent often begins long before the birth of a baby. Pregnancy and the postpartum period serve as the transition period for becoming a parent as both mothers and fathers anticipate changes in their roles, prepare for the upcoming birth, and recall important aspects of their own childhoods (Leon, 2009). Parental attachment starts to develop during pregnancy, facilitated by fetal movement as well as biological and hormonal changes in the mother. Feeling the baby move or seeing the fetus on ultrasound has been shown to significantly increase feelings of attachment, and there are even surveys for measuring maternal-fetal attachment during pregnancy (Pisoni et al., 2014).
As a universal parenting intervention, family planning helps optimize the timing of pregnancy and defer conception for individuals who do not desire children or do not feel ready to have a child under their current circumstances. More than one-half of pregnancies in the United States are unintended. These pregnancies can have serious negative consequences for parents as well as for children, including complications with pregnancy and delivery; exposure to illicit substances in utero; low birth weight; and higher risk of infant death, abuse, and developmental delays (Finer and Zolna, 2014; Institute of Medicine, 1995; Sawhill and Venator, 2015). Family planning can include efforts both to delay the onset of sexual activity among young people and to increase access to and use of birth control among those who are sexually active but do not currently desire pregnancy (Finer and Zolna, 2014). Family planning can be particularly valuable for populations at high risk for unintended pregnancy, including adolescents, individuals who abuse substances, and parents with severe mental illness (Institute of Medicine, 1995; Seeman, 2010; Strunk, 2008). A randomized intervention in North Carolina enrolled adolescent mothers with their first child in the Adolescent Parenting Program, which offers case management and peer
group meetings aimed at keeping adolescents in school and preventing a rapid second pregnancy (Sangalang et al., 2006). Compared with usual care, the program did not reduce time to second birth among participants as a whole, but the time to next birth was significantly longer for 12- to 16-year-olds participating in the program. (The Adolescent Parenting Program is discussed further in Chapter 5.) In a longitudinal study, adolescent mothers offered subdermal contraceptive implants immediately postpartum had significant reductions in rapid repeat pregnancy compared with controls, as most had retained the implant 1 year after delivery (Tocce et al., 2012).
Preconception and prenatal health visits are universal strategies for optimizing maternal health and well-being prior to and during pregnancy and promoting healthy child development. As discussed in Chapter 1, exposures in the in utero environment can affect the developing fetus in ways that shape health across the life span (Institute of Medicine and National Research Council, 2009; Tsankova et al., 2007; van Ijzendoorn et al., 2011). Prior to conception, people can initiate many health behaviors with strong evidence for improving child birth and developmental outcomes. These behaviors include folic acid supplementation to reduce neural tube defects (De-Regil et al., 2010); weight loss for obese mothers to prevent stillbirth and infant death (Aune et al., 2014); and cessation of tobacco use (discussed further below) to reduce the risk for pregnancy complications, low birth weight, and preterm delivery. Preconception and prenatal services also are important for identifying and providing intervention for women with such conditions as psychosocial stress (e.g., depression, anxiety, job strain), which during pregnancy is associated with preterm birth and low birth weight (Gold and Marcus, 2008; Loomans et al., 2013), and mental illness, which can increase the risk of fetal death and behavioral and mental health problems in children (Lancaster et al., 2010; O’Donnell et al., 2014).
After conception, universal parenting programs promote healthy pregnancy and delivery, often through education and counseling to increase parents’ knowledge of child development and use of effective parenting practices. For example, California tested a Kit for New Parents available through prenatal care providers, delivery hospitals, home visits, and other means that provides new and expecting parents with free pregnancy and early childhood information. The kit led to a significant increase in parent knowledge at 2-month follow-up (based on an assessment of sleep safety, infant feeding and nutrition, early learning, accessing child care, low-cost medical care for babies, and smoking cessation) compared with controls in a quasi-experimental study (Neuhauser et al., 2007). Also, nearly half of mothers who received the kit reported improved parenting practices, with significant differences seen between participants and controls at 14-month follow-up in frequency of reading to their children, steps taken to childproof their homes, taking children for routine medical visits, and use of
safer bottle-feeding practices. These gains were particularly strong for Spanish-speaking mothers, suggesting that videos and written materials may be useful for such interventions as they can be easily translated into other languages (Neuhauser et al., 2007).
Childbirth classes for expecting parents are widely available. Some medical and community centers also offer classes in newborn care, first aid, breastfeeding, and infant sleep. However, such classes have not been studied for their effects on promoting evidence-based knowledge, attitudes, and practices.
The use of group visits for prenatal care has attracted strong interest because of the potential for peer support. While group care appears to result in high participant satisfaction, however, a recent Cochrane review found only four eligible studies of group prenatal care and noted no differences in either maternal or infant birth or health outcomes (Catling et al., 2015). Centering Pregnancy is a proprietary model for group prenatal care (Mittal, 2011) that has been given a “strong” evidence rating by the Agency for Healthcare Research and Quality (2015). Groups of 8 to 10 women meet with a health care provider to discuss nutrition, stress management, breastfeeding, and other issues. One large randomized controlled trial examined the impact of this model on key outcomes, including adequacy of prenatal care and rates of preterm birth. Analysis of data from individuals who enrolled and participated (N = 993) showed that those in the intervention received better prenatal care, had fewer preterm births, were more likely to initiate breastfeeding, and had better prenatal knowledge relative to those receiving usual care (Ickovics et al., 2007). Sites using the model have reported an enhanced capacity to serve nonpregnant patients, as the group sessions free up resources previously used to provide individual visits (Agency for Healthcare Research and Quality, 2015).
All of these programs address knowledge, attitudes, and practices focused on improving children’s physical and mental health at birth and beyond. However, some researchers have asserted that the sources of disparities in birth outcomes (e.g., the increased risk for preterm birth and infant mortality among African American women relative to other women) are isolated not only to the 9 months of pregnancy but also arise from parents’ own developmental trajectories (Lu and Halfon, 2003). This view implies that support for parents may need to start with support for positive environments, health behaviors, and opportunities focused on reducing risks for women long before they actually conceive. As discussed further in Chapter 5, some evidence indicates that school-based clinics that provide prenatal care for teenagers in the school setting increase the uptake of health care and also encourage adolescents to stay in school. These programs have been shown to reduce absenteeism and dropout rates, help in identifying potential developmental delays among children born to teenagers, improve
birth weights, and encourage the use of contraception in correlational and qualitative research (Griswold et al., 2013; Strunk, 2008).
Breastfeeding
A systematic review of 10 randomized controlled studies of primary care-based educational interventions designed to improve breastfeeding practices among low-income women found that such interventions are effective in encouraging mothers to initiate breastfeeding as well as to continue breastfeeding 3 months postpartum. Successful programs often involved ongoing brief follow-up sessions with health care providers (Ibanez et al., 2012). In another review of randomized controlled studies conducted primarily in the United States and other Western nations, breastfeeding interventions using lactation consultants and counselors who provide antenatal education and postnatal support were found to be associated with increased initiation of breastfeeding and increased exclusive breastfeeding rates (Patel and Patel, 2015).
A lack of research exists on how to support breastfeeding effectively among adolescent mothers in the United States, whose breastfeeding rates are disproportionately low (Sipsma et al., 2013; Wambach et al., 2011). In one randomized study (N = 289), predelivery and postnatal education and counseling from lactation consultants who were registered nurses and peer counselors significantly increased breastfeeding duration, but not initiation or exclusive breastfeeding, in adolescent mothers (Wambach et al., 2011).
Complying with Recommended Immunization Schedules
Health care providers and educational interventions delivered in health care settings play an important role in parents’ immunization practices (Dunn et al., 1998; Hofstetter et al., 2015; Mergler et al., 2013; Vannice et al., 2011; Wallace et al., 2014; Yaqub et al., 2014). Such simple tools as patient reminders and health care providers talking to parents about vaccination are associated with higher rates of child immunization (Hofstetter et al., 2015; Szilagyi et al., 2000). Experimental studies indicate that moderately intensive interventions also are effective. In a cluster randomized trial, parents recruited from primary health care centers who received an information leaflet on the measles, mumps, rubella vaccine and/or participated in a parent meeting addressing immunization experienced a decrease in decisional conflict regarding child immunization after receiving the intervention. Those who participated in the parent meeting were significantly more likely to have a fully vaccinated child than those who only received the information leaflet (Jackson et al., 2011). In another randomized trial, Dunn and colleagues (1998) found that videotape was more effective than
written material in increasing parents’ knowledge about immunization, but actual uptake of the practice was not measured. Little evidence exists on how to reduce parental refusal of vaccination (Sadaf et al., 2013).
Limiting Screen Time
Newer health interventions have focused on helping parents limit young children’s screen time, such as the time they spend watching television and using computers and hand-held devices, including playing video games. As discussed in Chapter 2, limiting young children’s screen time can reduce sedentary behavior associated with increased risk for future overweight (see also the discussion of overweight and obesity below) (Gable et al., 2007; Lumeng et al., 2006). In randomized controlled trials, family-based interventions designed to reduce screen time that include a parental component of medium to high intensity have been the most effective, and these programs appear to be most beneficial for preschool-age children (Marsh et al., 2014). Brief primary care interventions also may be effective. In an experimental study involving English- and Spanish-speaking parents, parents who watched a short video or received a handout on reducing children’s exposure to television violence, compared with parents who received standard primary care, were more likely to report reductions in their children’s media viewing habits and exposure to media violence 2 weeks postintervention. Parents who watched the brief video were slightly less likely to report a change in media viewing habits and slightly more likely to report a reduction in exposure to media violence relative to parents who received the handout (Aragon et al., 2013).
Helping Children Avoid Overweight and Obesity
The rapid increase in the percentage of children who are considered overweight or obese in the United States (currently about 30%) has led to efforts to address the issue through multiple settings, including primary care (Taveras et al., 2011). Obesity in childhood often persists into adulthood and is related to a myriad of adverse health outcomes, including diabetes, hyperlipidemia, and hypertension, among others. Most health care settings with interventions related to child obesity focus on children who are already overweight or obese rather than on primary prevention. One systematic review found that only 8 of 31 randomized controlled trials in primary care demonstrated significant benefits with respect to child weight (Seburg et al., 2015). The review also noted that all of the interventions with positive outcomes—particularly those focused on young children—included a parent-targeted component. Newer research examining the role of motivational interviewing for parents of overweight children in primary
care shows promising outcomes although this work is still in early development (Resnicow et al., 2015).
Reducing Environmental Tobacco Exposure
One of the most extensively evaluated interventions is cessation of tobacco for parents who smoke. In the United States, about 9 percent of women overall self-report smoking during pregnancy, and rates are much higher in some communities (Child Trends Databank, 2015). Tobacco use during pregnancy is associated with prematurity, growth restriction, and infant death. While the U.S. Preventive Services Task Force does not specifically target parents, it has issued Grade A recommendations that clinicians ask all adults and all pregnant women about tobacco use and provide counseling for smokers (U.S. Preventive Services Task Force, 2009). Many tobacco cessation programs for parents also involve identifying smokers at well-child exams, in the hospital during delivery, and during postpartum care, although some of the longitudinal interventions take place in the home setting or via telephone. While several programs targeted to parents of young children focus on outpatient settings (Winickoff et al., 2003), there has been growing interest in hospital interventions targeting caregivers who smoke for cases in which children are hospitalized for tobacco-sensitive illnesses, such as asthma, other respiratory diseases, or infection (Chan et al., 2005; Ralston and Roohi, 2008).
A systematic review identified 13 experimental and quasi-experimental studies on interventions designed to assist families of young children with smoking reduction and cessation (Brown et al., 2015). Ten of these studies were focused on reducing child exposure to environmental tobacco smoke, and most of them found positive outcomes, such as use of household restrictions on smoking or less smoking. Approaches that focused on smoking cessation and relapse prevention among parents were less successful. However, the heterogeneity among the interventions reviewed prevented the authors from drawing firm conclusions about essential components associated with success (Brown et al., 2015). In a separate meta-analysis of randomized controlled trials and controlled clinical trials of interventions aimed at preventing children’s exposure to tobacco smoke delivered primarily in the context of health care (including such components as provision of educational materials, counseling, and telephone check-ins), a small but statistically significant benefit was noted based on parent self-report. Studies in which child biomarkers were collected showed lower exposure to tobacco smoke for those whose parents participated in the interventions, but these findings were not significant (Rosen et al., 2014). Finally, a novel approach to promoting cessation of tobacco use among parents through primary care is a pilot program that includes electronic health record prompts for
exposure to tobacco smoke at well-child visits, as well as decision support, education, and a referral to the state quit hotline (Sharifi et al., 2014).
Educating Caregivers on Normal Infant Crying
Typically delivered by health care professionals, the Period of PURPLE Crying Program aims to educate caregivers about normal infant crying given where the infant is in his or her development and thereby prevent shaken baby syndrome/abusive head trauma. Caregivers learn that there is a unique developmental phase beginning at age 2 weeks through age 3-4 months during which infants may cry for hours despite efforts to soothe them, that shaking a baby can be fatal, and that alternatives (such as walking away) can be used instead (Barr, 2012; Reese et al., 2014). Even though this program is currently classified as promising by the California Evidence-Based Clearinghouse for Child Welfare, the concern about crying as a precursor to abuse (especially abusive head trauma) is supported by evidence showing that teaching parents about typical crying and how to respond effectively is beneficial. In one study, the program’s approach was associated with a significant reduction in cases of infants ages 0-5 months who were brought to the emergency department primarily because of crying (with no other underlying medical condition) by 29.5 percent relative to before the program was implemented (Barr et al., 2015). The Period of PURPLE Crying Program has been or is in the process of being implemented in a number of health care facilities throughout the United States (National Center on Shaken Baby Syndrome, 2013).
Public Education Approaches
As noted in Chapter 3, public education has increased general awareness of some positive parenting knowledge, attitudes, and practices among parents and families. Some public education initiatives use media to disseminate information relevant to promoting parenting knowledge, attitudes, and practices to a broad audience. An example is the universal component of the Triple P-Positive Parenting Program, referred to as Triple P level 1. (The full Triple P system is described in Chapter 5.) Triple P level 1 uses a coordinated media and communication strategy targeting all parents and other members of the community to destigmatize parents’ seeking and participating in parenting support programs, counter parent-blaming messages in the media, and connect parents with supportive resources and programs. Messages are delivered using newsletters, brochures, posters, radio and televisions spots, and other media (Shapiro et al., 2015; Triple P-Positive Parenting Program, 2016a). A number of controlled evaluations have found that parents who participate in Triple P show improved quality
of parenting compared with controls (Hoath and Sanders, 2002; Sanders et al., 2000; Turner and Sanders, 2006; Zubrick et al., 2005). To the committee’s knowledge, however, no studies have evaluated the specific effects of Triple P level 1 in changing parenting-related knowledge, attitudes, or practices at the individual or community level.
Other media efforts focused on parenting are organization driven. ZERO TO THREE, for example, is a nonprofit organization founded by experts in child development, health, and mental health that disseminates evidence-based parenting information nationwide. Based on the premise that children’s earliest years are a period of substantial growth during which experiences can have lasting impacts, ZERO TO THREE has created a variety of resources to educate parents about how to nurture children during this important developmental stage. Tools include tip sheets, brochures, podcasts, and videos on a range of parenting-related topics, such as what parents should expect from their children given their age and steps parents can take at each developmental stage to help their children acquire various skills (e.g., language, communication, thinking, self-control); how to promote young children’s social-emotional development and school readiness; and how to address challenging behaviors (ZERO TO THREE, 2015).
The Centers for Disease Control and Prevention also has developed a number of parenting resources, including information on developmental milestones and parenting tips in such areas as creating structure and rules for children, using consequences, giving directions, and using time-out. Videos and other tools are designed to help parents practice these skills (Centers for Disease Control and Prevention, 2016).
Several public health education campaigns in clinics and hospitals have proven successful. An example, reviewed in Chapter 3, is the Safe to Sleep campaign (previously known as Back to Sleep), which was thought to have played a significant role in reducing the incidence of sudden infant death syndrome (SIDS) over the past two decades (U.S. Department of Health and Human Services, 2015b). Much of the Safe to Sleep information is provided in hospital settings prior to postpartum discharge and in outpatient clinics. Similarly, use of media for wide dissemination of information about helmet safety, coupled with distribution of free and reduced-price helmets, in the National Safe Kids campaign is believed to have increased knowledge among parents about the importance of children wearing helmets during bicycling and other wheeled sports and increased children’s helmet use (Morris et al., 1994; Rouzier and Alto, 1995). Other examples with documented success range from tobacco control, to seat belt use, to reduced use of illicit drugs (Hornik, 2002).
The literature on successful public health campaigns identifies characteristics conducive to success (Randolph and Viswanath, 2004). These include maximizing exposure to targeted messages among the audience; using social
marketing tools to create the appropriate messages for distribution, drawing on “message effect” theories (Storey et al., 2008); and creating associated structural conditions, such as a supportive environment or opportunities to support the audience in making the recommended changes. The reach of the communication effort, as well as the campaign’s intensity (e.g., how often individuals are exposed to the message), duration, and messaging approach and whether it is used in combination with other elements, also may influence the extent of its impact (Boles et al., 2014; Friend and Levy, 2002).
Likewise, certain factors can reduce the success of public health campaigns. This is the case, for example, when individuals become confused or they develop distrust as a result of competing messages advocating behaviors inconsistent with or contradictory to those being promoted by a campaign (Carpenter et al., 2015; Nagler, 2014). Another characteristic of the contemporary information environment that presents a significant challenge to public health campaigns is the generation of a large body of information and data on a range of topics and the dissemination of such information on increasingly proliferating information delivery platforms (Viswanath et al., 2012). Also posing a challenge are differences among social groups in the generation, manipulation, and distribution of information at the group level and differences in access to and ability to take advantage of information at the individual level, a phenomenon characterized as communication inequalities (Viswanath, 2006).
Despite these challenges, public health campaigns can be an effective tool for reaching a large and heterogeneous population at a much lower cost than many other forms of interventions. And information and communication technologies make it possible to customize and tailor information to the needs of the parents based on their background and social circumstances. The use of information and communication technologies is discussed further later in this chapter.
Instruction in Parenting for Adolescents in the General Population
Part of the committee’s task was to describe “key periods of intervention that are more effective in supporting parenting capacity—beginning in high school or even earlier” (see Box 1-2 in Chapter 1). The committee interpreted this part of its task as including individuals of high school age and younger in the general population who are not pregnant or parents. (See Chapter 5 for a discussion of interventions for adolescent parents.) However, scarce scientific evidence supports the premise that informing individuals about the challenges of parenting during high school or earlier will help lower pregnancy rates or improve future parenting among those who do become parents. Evaluations of infant simulation programs, including the well-known “Baby Think it Over” (BTIO: now marketed by
Realityworks as “RealCare Baby”), have not yet demonstrated a direct relationship between participating in such programs and reduced pregnancy rates or improved parenting.
Some evidence from longitudinal research does point to a prospective association between perceived benefits of childbearing and subsequent pregnancy among young women wishing to avoid pregnancy (Rocca et al., 2013). Additional longitudinal data show that positive attitudes toward an adolescent birth may be predictive of a subsequent birth (Rosengard et al., 2004). The converse also may be true—that adverse attitudes toward adolescent parenting may be predictive of delayed childbearing, although this has not been shown.
Some, but not unequivocal, evidence indicates that participating in BTIO resulted in changes in adolescents’ perceptions with regard to the costs and rewards of adolescent parenting. For example, Somers (2013) used an experimental design and a 1-year follow-up with middle schoolers from low-income families in an urban district to test BTIO. The program instilled a more realistic perception of their lack of readiness among the BTIO groups; however, none of the other expected outcomes—changes in sexual behavior, contraceptive use, personal intentions to avoid teenage pregnancy, sexual attitudes, and actual pregnancy rates—was seen. Some of these effects could be due to the relatively low rate of sexual activity even after 1 year.
Roberts and McCowan (2004) implemented a randomized controlled trial of an intervention combining the New York State parenting curriculum (which focused on reflection-based parenting skills with specific child care competencies) and exposure to BTIO, with the control group experiencing only the BTIO curriculum. Their findings, based on a sample of high school students in a rural community, show that the infant simulator is an effective tool for teaching child care skills in that the students more often expressed their belief that parenting is a skill that takes time and patience to learn, that teenagers cannot afford to raise a baby, that raising a child and continuing one’s education is difficult, and that teenagers should abstain from sexual behaviors.
Herrman and colleagues (2011) concluded that 79 teens in a single-group study using a pre- and post-test design showed no changes in perceptions following six weekly BTIO classes and a weekend infant simulator experience. The committee agrees with their conclusion that “until such a time as a multiple site, large sample, randomized study with control groups using a valid instrument to measure outcomes is conducted, the use of infant stimulators will remain controversial” (Herrman et al., 2011, p. 327). It is possible that the use of infant simulators as part of a more comprehensive pregnancy prevention program providing accurate information about both abstinence and contraception could change attitudes about becoming
pregnant and encourage a reduction in unprotected sexual intercourse. Many effective pregnancy prevention programs do include exercises aimed at getting adolescents to consider the untoward impact on their lives if they become parents. Programs such as BTIO could reinforce this message, although this is not a known effect of the program. However, the committee found no direct evidence as to whether teaching youth in the general population about parenting has an impact on their future behavior as parents.
Couple Relationship Education
Over the past two decades, concerns about the state of family life in the United States have led to the creation of many general programs designed to strengthen couple relationships, prevent the emergence of conflict and violence, and increase fathers’ positive involvement with their children. Generally characterized as couple relationship education (Cowan et al., 2010; Panter-Brick et al., 2014), these programs have focused primarily on improving couples’ communication, although a very few, using clinically trained staff, also focus on parenting. Couple relationship education programs initially were targeted to middle-class couples early in their marriage and not already in marital or relationship distress. More recently, there have been efforts to provide services for couples that are at risk by virtue of low income but not otherwise identified as experiencing serious relationship difficulties.
Two relatively large-scale couple relationship education initiatives have been funded and evaluated by the federal government. Building Strong Families (Wood et al., 2014), which included three different couple relationship intervention approaches, was conducted across eight U.S. sites, with 5,102 low-income, unmarried couples being randomly assigned to intervention and control conditions. The couples were not identified as having specific relationship difficulties. The Supporting Healthy Marriage Program (Hsueh et al., 2012) was a randomized controlled trial involving 6,298 low-income married couples, expecting or with a child, at eight sites assigned randomly either to one of four couples-group programs plus a family support worker or to a no-treatment control condition. The results for Building Strong Families appear to be limited, although there is some evidence for a possible impact on conflict in low-income families. Self-report and observational measures suggest that the Supporting Healthy Marriage Program changed the way participants viewed their marriage, as well as the extent to which they were able to implement the skills taught by the program curricula (Cowan and Cowan, 2014).
A number of smaller programs have shown evidence of success (Cowan and Cowan, 2014; Faircloth et al., 2011; Feinberg et al., 2010; Pinquart and Teubert, 2010). One of these programs (Supporting Father Involvement) works with parents about to have a child. A consistent body of
research finds that marital satisfaction often decreases following the birth of a child, and marital conflict emerges or worsens. This program provides a 16-week group course to either the couple or just the father. Randomized controlled research involving several hundred families found reductions in parenting stress; stability in couples’ relationship satisfaction; and stability or reductions in children’s hyperactivity, social withdrawal, and psychological symptoms compared with families in a control group (Cowan and Cowan, 2000). Reduction in parents’ violent problem solving was linked to reductions in children’s aggression. In another randomized controlled trial involving parents of children entering kindergarten, positive effects were found on both mothers’ and fathers’ marital satisfaction and the children’s adaptation (hyperactivity and aggression), according to their teachers (Cowan et al., 2011).
WIDELY USED INTERVENTIONS
Beyond the health care system, the most widely used approaches to strengthening and supporting parenting are home visiting programs; programs focused on helping parents provide cognitive stimulation in the home through educational activities involving reading, language, and math; efforts at providing parenting education in the context of classroom-based ECE programs; and efforts to increase parent engagement in school settings and school-related activities (prekindergarten through grade 3). These are usually voluntary programs aimed at enhancing parenting knowledge, skills, and practices; improving the parent-child relationship and the quality of parent-child interactions; improving children’s school readiness and well-being; and preventing poor outcomes for children. The programs vary in their core features (e.g., requirements for staff training, number of sessions, cost to implement), target populations, and the amount of evidence of effectiveness available to guide policy and program decision making. Because these programs may cost several thousand dollars per participant per year, they often are targeted to those families considered to be in greatest need of additional support. Some programs, such as Head Start, require that families meet income requirements (e.g., a certain poverty level), and others, such as the home visiting program Durham Connects, are limited to individuals living within a specific geographic area. In addition, as described in Chapter 3, the actual numbers of families enrolled in these programs represent only a fraction of those who are eligible for them.
Home Visiting Programs
Prenatal, infant, and early childhood home visiting is a relationship-based mode of service delivery in which a professional or paraprofessional
home visitor provides services in the family home using a prescribed home visiting model or curriculum. Home visiting programs have specific goals and range from truly universal programs for new parents in the community in which it is offered to targeted programs that select families based on important descriptive characteristics (e.g., first-time pregnant woman early in her pregnancy) or key risk factors. Across models, the home visitor’s aims generally include supporting parents in their parenting role, facilitating positive parent-child interactions and relationships, reducing risks of harm, and promoting good parenting practices. Because the intervention is provided where families’ daily lives take place, a potential benefit of home visiting is the ability to tailor services to meet families’ specific needs (Johnson, 2009). Visits usually last 60 to 90 minutes and occur regularly over the course of 6 months to 2 years, with some long-term models serving families prenatally through age 5. These relatively intensive services usually are targeted to families with children at the highest risk for poor outcomes and those who are unlikely to enter kindergarten with the preacademic skills needed to make the most of formal schooling. Home visiting services generally are voluntary, although in some cases they may be court mandated (for example, in cases of child abuse and neglect). Although many home visiting programs target pregnant women and mothers, some include fathers in visits, and others provide separate visits for mothers and fathers (Sandstrom et al., 2015).
The roots of home visiting in the United States trace back to nurse and teacher home visiting in 19th-century England (Wasik and Bryant, 2001). The more than 250 home visiting programs implemented and studied at the state and local levels in the United States during the late 20th and early 21st centuries reflected those public health and education roots as well as an emphasis on prevention of child maltreatment (Boller et al., 2010; Paulsell et al., 2010). Programs focused on pregnant women and newborns often were run by public health departments and child welfare agencies, and those focused on ECE or on special education services often were run by a human service or education agency (Boller et al., 2010; Daro, 2006).
In fiscal year 2015, the federal home visiting program served about 145,500 parents and children in all 50 states, the District of Columbia, and 5 territories (Health Resources and Services Administration, 2016). There are also a number of state-based home visiting programs. In 2009, the most recent year for which the committee could find data, 40 states reported that they had state-based home visiting programs. Most states supported one or two models (Johnson, 2009), with 5 states reporting that they supported three or more, for a total of 70 state-based home visiting programs across the 40 states (Johnson, 2009). Over the past 20 years, the development of national home visiting programs with national offices and a support infra-
structure for implementation has grown (Daro, 2011; Daro and Benedetti, 2014). States, counties, and municipalities around the country have implemented different models, some that are branded and have some evidence of effectiveness and some that are home grown and have not been evaluated (Johnson, 2009).
Home Visiting Logic Model: Changing Parenting Knowledge, Attitudes, and Practices to Improve Child Outcomes
As depicted by the prenatal and early childhood home visiting logic model in Figure 4-1, some of the problems home visiting is designed to address include poor birth outcomes (low birth weight), child maltreatment, and lack of school readiness. Historically, funding agencies and communities that developed home visiting programs or selected from existing programs chose models that best suited the needs of the families they served and the particular outcomes they were trying to improve. Regardless of the specific mode, the underlying assumption of these programs is that the home is a comfortable, convenient setting for expectant parents and parents of young children to receive supports and services. As described below, a growing body of research points to the importance of high-quality implementation (such as collaboration among local public and private partners, program developers, and funders and oversight of service provision [training, quality assurance]) in achieving impacts on targeted knowledge, attitudes, and practices and child outcomes. Assuming an implementation system that brings families into services and provides high-quality visits as intended, targeted short-term outcomes include decreased parenting stress, depression, and isolation and improved parenting knowledge, attitudes, and practices.
As depicted in Figure 4-1, home visiting programs aim to support several evidence-based parenting knowledge, attitudes, and practices identified in Chapter 2. Visits are designed to improve parents’ knowledge of children’s development and how adults can support children’s exploration and learning. Some programs attempt to enhance parents’ attitudes about their own efficacy in the parenting role, given that parents who do not believe they can be effective in supporting their child’s development and learning may be unable to overcome that mind-set and engage fully in the home visits. Home visiting’s primary pathway to the targeted long-term child outcomes is through improvements in the parent-child emotional relationship and the quality of parent-child interactions (e.g., how sensitive and responsive parents are when interacting with their young children). Other specific aims of programs may include increasing parents’ use of positive guidance and decreasing their use of harsh punishment. Some programs target household and vehicular safety.
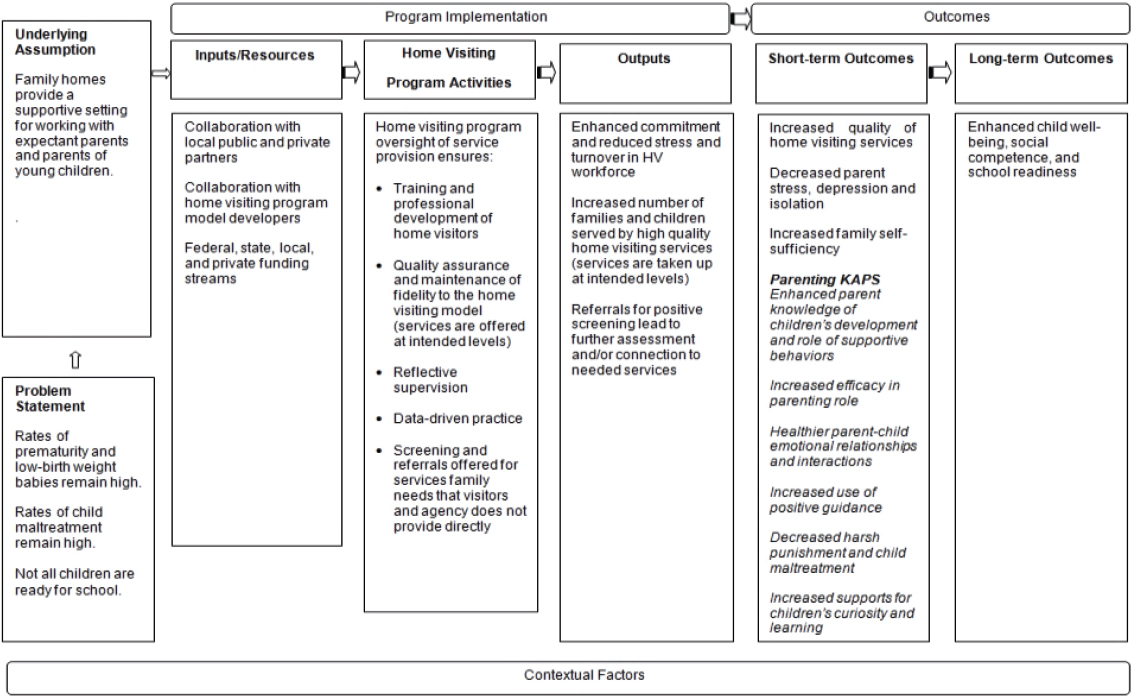
NOTE: HIV = home visiting; KAPs = knowledge, attitudes, and practices.
Throughout this section, three home visiting models are profiled to illustrate how model activities are linked to outcomes and to highlight examples of the evidence for their impacts on parenting knowledge, attitudes, and practices and child outcomes. Box 4-1 describes the Nurse-Family Partnership (NFP)®, a model rooted in a public health approach for which multiple longitudinal impact studies have been conducted. Box 4-2 describes Parents as Teachers (PAT)®, a model with roots in ECE for which a number of studies exist. Finally, Durham Connects, described in Box 4-3, is one of the newer models, focused on universal strategies for ensuring that families receive the services they need, for which two studies were included in the U.S. Department of Health and Human Services’ (HHS) 2014 Home Visiting Evidence of Effectiveness (HomVee) review.3
Home Visiting and Evidence-Based Policy Making
The Maternal, Infant, and Early Childhood Home Visiting (MIECHV) Program, funded under the Patient Protection and Affordable Care Act (ACA) of 2010, changed the national home visiting landscape considerably by providing $1.5 billion in funding to states, territories, and tribal entities to serve very high-risk families. A distinctive feature of the legislation is its emphasis on research evidence as the basis for the home visiting models states could select (75% of funds had to be allocated to models with evidence of effectiveness [see below], and the other 25% could be used to fund models that were promising if they met certain criteria and states agreed to conduct a rigorous study). In addition, the legislation identified the specific outcome areas that had to be impacted by the selected programs and the performance measures on which the states would have to report each year, which included positive parenting practices and three child outcome areas—child health, child development and school readiness, and reductions in child maltreatment.4 A national evaluation is also under way to assess MIECHV implementation and impacts (Michalopoulos et al., 2013).
Based on a systematic review of the evidence and the application of strict criteria for what counted as evidence (adapted in part from the U.S. Department of Education’s What Works Clearinghouse), the HomVEE project team identified seven national models that met the HHS evidence
___________________
3 See http://homvee.acf.hhs.gov/ [August 2016].
4 It is important to note that requirements for territories and tribal entities were different from those for the states given the available research evidence—no existing home visiting models were originally found that had evidence of effectiveness for tribal populations. Thus, HHS allowed grantees to choose from existing models but required them to conduct an evaluation.
criteria5 and to which 75 percent or more of funds had to be allocated (Paulsell et al., 2010): Early Head Start-Home Visiting (EHS-HV), Family Check-Up® for Children, Healthy Families America (HFA)®, Healthy Steps, Home Instruction for Parents of Preschool Youngsters (HIPPY)®, NFP®, and PAT®. In a second HomVEE review, published in 2012, six more models that met the evidence criteria were identified: Child FIRST, Early Intervention Program for Adolescent Mothers (EIP), Early Start (New Zealand), Oklahoma’s Community-Based Family Resource and Support (CBFRS) Program, Play and Learning Strategies-Infant (PALS Infant), and SafeCare® Augmented (Avellar et al., 2012). In 2014, 40 models were re-
___________________
5 In order to meet HHS’ criteria for an evidence-based home visiting program, models must have at least one high- or moderate-quality impact study with favorable, statistically significant impacts for two or more outcomes, or at least two high- or moderate-quality impact studies of the model using nonoverlapping participant samples with one or more favorable, statistically significant impacts in the same domain. In either case, impacts must be found for either the full sample or, if found for subgroups only, be replicated in the same domain in at least two studies using nonoverlapping participant samples. For models meeting these criteria based on randomized trials only, significant impacts must be sustained for at least 1 year after participants were enrolled and must be reported in a peer-reviewed journal. Single-case studies may be considered if at least five studies on the intervention meet the What Works Clearinghouses’ pilot design standards, are conducted by three research teams without overlapping authorship, and the combined number of cases is at least 20 (U.S. Department of Health and Human Services, 2016).
viewed, and 4 more met the HHS criteria (Avellar et al., 2014): Durham Connects/Family Connects, Family Spirit®, Maternal Early Childhood Sustained Home-Visiting (MECSH) Program, and Minding the Baby®. Two additional models were included in a September 2015 update: the Health Access Nurturing Development Services (HANDS) Program and Healthy Beginnings (Avellar et al., 2015).
Table 4-1 shows the number of favorable primary positive parent and child outcomes compared with the total number of outcomes reviewed for all of the models reviewed in 2010, 2012, 2014, and 2015.6 The table also notes where unfavorable or ambiguous outcomes were found.
A Note on Program and Evaluation Logic
It is important to note that the logic of home visiting programs and their evaluations may not always align. As depicted in the generic home visiting logic model in Figure 4-1, for example, parenting knowledge, attitudes, and practices are among the hypothesized short-term outcomes en route to the longer-term outcome of child well-being. As seen in Table 4-1, positive parenting practices were not measured in the evaluations of some programs; however, this does not necessarily mean that parenting was not part of the program logic model. For example, the program description for Child FIRST states that parenting enhancements are expected as a result of the program, but parenting practices were not measured in the study that provided evidence of the program’s effectiveness based on impacts on child outcomes (Lowell et al., 2011).
Home Visiting Program Impacts
In addition to findings from the HomVEE review, this section draws on findings from a paper commissioned by the committee on evidence for investing in parenting programs at scale, which includes six programs that were not included in the HomVEE review. These programs have rigorous designs that differ from MIECHV in either program delivery approach or outcomes.7
___________________
6 Primary outcomes refer to those that were measured through direct observation or assessment, administrative data, or self-report using a standardized instrument. Table 4-1 does not include impacts on “secondary outcomes”—those self-reported by means other than a standardized instrument.
7 The papers commissioned by the committee are in the study public access file and can be requested at https://www8.nationalacademies.org/cp/ManageRequest.aspx?key=49669 [October 2016].
| Outcome | |||||
|---|---|---|---|---|---|
| Positive Parenting Practices | Family Economic Self-Sufficiency | Child Health | Child Development and School Readiness | Reductions in Child Maltreatment | |
| Child FIRST | Not measured | Not measured | Not measured | 5/16 | 1/3 |
| Durham Connects/Family Connects | Not measured | Not measured | 6/9 | Not measured | Not measured |
| Early Head Start-Home Visiting | 3/28 | Not measured | Not measured | 2/36 | Not measured |
| Early Intervention Program for Adolescent Mothers | 0/9 | Not measured | 8/18 | Not measured | Not measured |
| Early Start (New Zealand) | 3/3 | Not measured | 2/4 | 2/6 | 1/2 |
| Family Check-Up for Children | 2/2 | Not measured | Not measured | 3/14 | Not measured |
| Family Spirit | 0/5 | Not measured | Not measured | 10/40 | Not measured |
| Health Access Nurturing Development Services | Not measured | 2/3e | 6/9 | Not measured | 1/1 |
| Healthy Beginnings | Not measured | Not measured | 1/3 | Not measured | Not measured |
| Healthy Families America | 2/50 | Not measured | 0/9 | 9/43 | 1/34 |
| Healthy Steps f | 0/1 | Not measured | 2/2 | 0/2 | Not measured |
| Home Instruction for Parents of Preschool Youngsters | 1/10 | Not measured | Not measured | 3/20 | Not measured |
| Maternal Early Childhood Sustained Home-Visiting Program | 1/6 | Not measured | 0/3 | Not measured | Not measured |
| Outcome | |||||
|---|---|---|---|---|---|
| Positive Parenting Practices | Family Economic Self-Sufficiency | Child Health | Child Development and School Readiness | Reductions in Child Maltreatment | |
| Minding the Baby | 0/2 | Not measured | 1/2 | Not measured | 0/1 |
| Nurse-Family Partnership | 4/22 | 4/21a | 4/30 | 5/59 | 7/25 |
| Oklahoma’s Community-Based Family Resource and Support Program | 2/7 | Not measured | Not measured | Not measured | Not measured |
| Parents as Teachers | 3/50b | 1/1 | 0/1 | 7/66c | 1/3 |
| Play and Learning Strategies-Infant | 11/24d | Not measured | Not measured | 1/16 | Not measured |
| SafeCare Augmented | Not measured | Not measured | Not measured | Not measured | 1/6 |
NOTE: The table shows the number of favorable outcomes relative to the total number of outcomes. Footnotes indicate when the total number of outcomes includes an unfavorable or ambiguous outcome(s). In accordance with www.homvee.acf.hhs.gov/models.aspx, descriptions of the outcomes are as follows: (1) Favorable: a statistically significant impact on an outcome measure in a direction that is beneficial for children and parents. An impact could be statistically positive or negative, and is determined “favorable” based on the end result. (2) No effect: findings for a program model that are not statistically significant. (3) Unfavorable or ambiguous: a statistically significant impact on an outcome measure in a direction that may indicate potential harm to children and/or parents. An impact could statistically be positive or negative, and is determined “unfavorable or ambiguous” based on the end result. While some outcomes are clearly unfavorable, for other outcomes it is not as clear which direction is desirable. (4) Not measured: current research (meeting HomVEE standards for a high or moderate rating) includes no measures in this domain.
aOne of the three outcomes were unfavorable or ambiguous.
bThis report focuses on Healthy Steps as implemented in the 1996 evaluation. HHS has determined that home visiting is not the primary service delivery strategy and the model does not meet current requirements for MIECHV program implementation
cOne of the 21 outcomes were unfavorable or ambiguous.
dFour of the 50 outcomes were unfavorable or ambiguous.
eOne of the 66 outcomes were unfavorable or ambiguous.
fOne of the 24 outcomes were unfavorable or ambiguous.
SOURCES: Adapted from www.homvee.acf.hhs.gov/models.aspx; Avellar et al. (2012, 2014, 2015); Paulsell et al. (2010).
Positive parenting practices PALS Infant and NFP had the highest number of favorable impacts on parenting practices (Table 4-1). Across two studies, the HomVEE evidence review found 11 favorable impacts of PALS Infant on parenting behaviors such as contingent responsiveness and maintaining child foci, although it also found a negative impact on redirecting child foci (Landry et al., 2006, 2008). The HomVEE review identified favorable impacts of NFP on a number of parenting beliefs and practices, including cognitive stimulation in the home, reductions in dangerous exposures in the home, beliefs, worry, mother-infant interaction, and sensitive interaction across a number of studies (Kitzman et al., 1997; Olds et al., 1986, 1994). Among other models with impacts on parenting practices, the specific parenting outcomes affected within and across models vary, even for those programs that share a similar theoretical grounding or logic model.
In addition, as can be seen in Table 4-1 for several programs, the number of outcomes for which no impacts were found is high, exceeding the number of outcomes for which significant impacts were found; moreover, impacts may have been found at one point of measurement but not another. For example, EHS-HV participants were no more likely than controls to report reading to their children every day at the end of the program. Two years after the program ended, however, participants were significantly more likely than controls to say that they read to their children daily (Jones Harden et al., 2012). Getting Ready, an add-on to EHS-HV that provides parents with additional training in effective engagement in routine activities that support child behavior and learning, showed changes in parent warmth, encouragement of autonomy, and supports for children’s skills and appropriate guidance, but no changes in the quality of behavior supporting children’s learning (Knoche et al., 2012). The effect of Getting Ready on child outcomes was not assessed.
Overall, while many individual evaluations of home visiting programs have shown impacts on parenting practices tied to positive developmental outcomes, the average impacts of home visiting on parenting practices are not large. Nor is there a strong pattern of effects on parenting practices across evaluation studies and home visiting models.
Family economic self-sufficiency Relatively few home visiting programs target or measure effects of home visits on family economic self-sufficiency. The HomVEE review identified several studies in which participation in NFP was associated with reduced rates of subsequent childbearing (Kitzman et al., 1997; Olds et al., 2002, 2004) and lowered use of some forms of public assistance (Olds et al., 2010). In two impact studies, participation in HANDS was associated with significant increases in maternal receipt of WIC (Williams et al., 2014a, 2014b). Other models had positive effects on aspects of parents’ self-sufficiency, such as reductions in rates of
subsequent childbearing in Minding the Baby (Sadler et al., 2013). Taking into account secondary outcomes (i.e., those self-reported by means other than a standardized instrument), Early Head Start and EIP showed improvements in parents’ receipt of education and training (Jones Harden et al., 2012; Koniak-Griffin et al., 2000; U.S. Department of Health and Human Services et al., 2001, 2002).
Child health Several programs, including EIP, Durham Connects (Box 4-3), HANDS, and NFP have had favorable impacts on child health, with some consistent findings across studies. Effects for measures of infant health, such as fewer hospitalizations and emergency room visits, were found for both EIP and Durham Connects (Dodge et al., 2013; Koniak-Griffin et al., 2002, 2003). Participation in HANDS was associated with reductions in preterm births and low birth weight across studies (Williams et al., 2014a, 2014b, 2014c). Two programs included not in the HomVEE review but in the commissioned paper—Rest Routine and the MOM Program—showed impacts on child health. Rest Routine, which focuses on reducing infant irritability or colic, a hypothesized precursor to child maltreatment, was found to reduce the number of hours of child crying and some aspects of parenting stress (Keefe et al., 2006a, 2006b). The MOM Program provides up to 11 home visits to encourage care for the health and development of the baby and use of well-child care and early intervention services if needed (Schwarz et al., 2012). The program had an impact on use of early intervention services, but no differences were seen in rates of developmental delays or cognitive outcomes. Parenting knowledge, attitudes, and practices were not assessed.
Child development and school readiness Family Spirit, HFA, PAT, Child FIRST, and NFP showed the greatest number of favorable impacts on child development and school readiness in the HomVEE review, although there were many null effects for each of these programs. Three programs showed clear evidence of effectiveness: Child FIRST (effects on externalizing problems and language problems [Lowell et al., 2011]); HFA (effects on some behavioral and academic outcomes in at least in two of the three trials in which child outcomes were measured [Caldera et al., 2007; Kirkland and Mitchell-Herzfeld, 2012]); and NFP (but only based on longer-term followup [Eckenrode et al., 2010; Kitzman et al., 2010; Olds et al., 2004]). In the commissioned paper, the University of California at Los Angeles Family Development Project is identified as improving child behavior but not cognitive skills (Heinicke et al., 2001). Minding the Baby (Sadler et al., 2013) also demonstrated evidence of efficacy but only for the child’s security of attachment, which may or may not translate to long-term benefits (other
behavioral and academic skills were not measured in the study of that program).
Effects were less clear for the EHS-HV model (U.S. Department of Health and Human Services et al., 2002), with effects being found only on parent-reported child behavioral measures and only at a later follow-up point (and no effects on cognitive skills being found at any time point). Both trials of Family Spirit showed mixed findings across parent-reported behavioral outcomes, including significant reductions in externalizing problems but not in many other similar behaviors (Barlow et al., 2013; Walkup et al., 2009); academic skills were not measured here. Effects of Healthy Steps on children were not evaluated during the intervention, and no effects were found 2 years after the intervention (Minkovitz et al., 2001, 2007).
Reductions in child maltreatment Of the programs reviewed by HomVEE, NFP showed the greatest number of favorable impacts on child maltreatment. The program had effects on hospitalizations for accidents and injuries and involvement in child protective services (CPS) in some sites and follow-ups, but not consistently across sites and studies (Administration for Children and Families, 2015b). There is also evidence of effects of Child FIRST on reductions in CPS involvement and general child maltreatment (Lowell et al., 2011). The review found improvements in measures of child maltreatment for other programs as well (e.g., HANDS and PAT).
Home Visiting Collaborative for Improvement and Innovation Network
Mary Catherine Arbour, Harvard Medical School and Brigham and Women’s Hospital, was invited to present before the committee at one of its open sessions on lessons learned in continuous quality improvement from the Home Visiting Collaborative for Improvement and Innovation Network (HV CoIIN). The HV CoIIN is operated by the Education Development Center, Inc., with funding from the Health Resources and Services Administration (HRSA). Dr. Arbour is the Improvement Advisor for this national initiative that supports the work of a set of MIECHV state grantees. HV CoIIN aims to achieve improvement in outcomes in four areas targeted by home visiting programs: breastfeeding, maternal depression, family engagement, and child development.
HV CoIIN uses the Institute for Healthcare Improvement’s Breakthrough Series Collaborative Model (Institute for Healthcare Improvement, 2003), which combines the Model for Improvement and a structured, time-limited collaborative learning model. This model is designed to close the gap between what is known from science about what works and what is happening on the ground to achieve results and facilitate the implementation of improved programs (Arbour, 2015). The collaborative’s first step is
to select a topic that has a good evidence base but is not always applied in practice. Faculty are recruited to develop a framework and set of changes expected to improve service quality and outcomes, and teams are then formed to participate in the collaborative (including leadership, front-line workers, and end-users). These teams test changes and adapt them to specific contexts, collect data on a number of indicators over time to demonstrate improvement, and share experiences to facilitate learning (Arbour, 2015). HV CoIIN is using this approach to build a culture of inquiry and improvement and enhance the implementation of improvements across a number of the home visiting models included in the MIECHV Program and across the participating states.
HV CoIIN is the first national initiative to apply continuous quality improvement (CQI) methods to evidence-based home visiting programs to improve critical outcomes for vulnerable families with young children ages 0-5. Participating home visiting teams receive training and coaching in the basic quality improvement skills of rapid-cycle hypothesis testing and data use based on the Model for Improvement. The model uses three questions to guide teams to set short-term specific aims: (1) “What are we trying to accomplish?” asks them to define aims specific to their context; (2) “What ideas do we have that can result in improvement?” asks them to use their own ideas to make home visiting work in their specific setting; and (3) “How will we know that a change is an improvement?” asks them to collect and use data to determine how well those ideas work to advance their aims. Drawing on the manufacturing and business sector, teams then subject their ideas to small, rapid-cycle testing using Plan, Do, Study, Act (PDSA).
In addition to applying the Model for Improvement in their local work, the CQI teams apply the Breakthrough Series Collaborative Model by participating in three “Learning Sessions” that bring together local teams, expert faculty, and stakeholders (including model developers and state leaders). Between Learning Sessions, CQI teams test changes in their local settings and gather data to measure the effect of those changes during 4- to 6-month-long “Action Periods.” At the first Learning Session, expert faculty presented a vision for home visiting quality and specific changes proposed by HV CoIIN, and CQI teams learned about the Model for Improvement and PDSA cycles. At the second and third Learning Sessions, teams learned from one another as they reported on successes, barriers, and lessons learned in formal presentations, workshops, and informal dialogue and exchange.
Participants in HV CoIIN commit to pursuing shared aims and to reporting a set of shared measures. Every month, data are displayed on run charts and shared transparently across the collaborative and with state
and local representatives to facilitate shared learning and rapid diffusion of good ideas.
The mission of HV CoIIN is to achieve breakthrough improvements in selected process and outcome measures, including benchmark areas legislatively mandated for the federal MIECHV Program, while reducing or maintaining program costs. Its mission also includes developing the means to diffuse the learning and improvements resulting from its efforts more widely within participating organizations and to other MIECHV grantees and home visiting agencies. During its first phase (May 2014-August 2015), the collaborative enrolled 12 states and tribes and 33 home visiting agencies using five evidence-based home visiting models serving 3,500 families. HV CoIIN integrates CQI methodologies into existing evidence-based home visiting programs with the goal of disseminating practices known to work, innovating, achieving results more rapidly, building leaders in quality improvement and sustainability in home visiting, and demonstrating the effectiveness of home visiting in large-scale implementation.
Initial data indicate that the learning and improvements resulting from the HV CoIIN efforts have enabled agencies and staff to change their practices so as to affect behaviors in ways that are associated with quality improvements that support outcomes targeted by the collaborative (Arbour, 2015). The collaborative’s approach shows promise as a way to work with staff in programs that target parenting knowledge, attitudes, and practices, and has been used in a variety of other health and related fields, including efforts focused on reducing infant mortality (McPherson et al., 2015; Selk et al., 2015).
Programs Promoting Parent Educational Activities in the Early Home Learning Environment
As discussed in Chapter 2, in recent years there has been increased attention to parent behaviors that are associated with children’s cognitive development as well as social-emotional skills. Designing interventions that generate large impacts on parent practices in promoting children’s cognitive skills has proved difficult. Two large meta-analyses of randomized controlled trials have included evaluations of parent skills training in relation to children’s cognitive outcomes. One found that parent training in promoting children’s cognitive, academic, and social skills was associated with smaller effects relative to parent training programs that did not include those components (Kaminski et al., 2008). The other found that interventions for new and expecting at-risk parents that focus on the promotion of children’s cognitive development (e.g., teaching parents how to use stimulating materials) generate small to very small effects on various noncognitive childhood outcomes, including parent-child relations (Pinquart and Teubert, 2010).
There is, however, some experimental research suggesting that interventions designed to promote parents’ provision of stimulating learning experiences do support children’s cognitive development, primarily on measures of language and literacy. Intensive parent training in the home or a community setting provided by coaches who visit parents frequently (as often as weekly) have been shown to increase responsive and developmentally stimulating parenting and, in turn, children’s early achievement and positive social behavior. Evidence-based models of this approach include Play and Learning Strategies (PALS) (Landry et al., 2006, 2008, 2012); My Baby and Me (which used the PALS curriculum for responsive parenting plus additional training on such topics as developmental milestones, health and safety, and literacy) (Guttentag et al., 2014); Let’s Play in Tandem (Ford et al., 2009); the Head Start Research-based Developmentally Informed Parent (REDI-P) Program (Bierman et al., 2015); and the Getting Ready for School Program (Noble et al., 2012).
In PALS and My Baby and Me, parents of infants are coached during 90-minute in-home sessions on contingent responsiveness, joint engagement, interactive communication, and emotional support for their children. Multiple randomized trials of these programs have indicated increased contingent responsiveness, verbal stimulation, and warmth from socially disadvantaged mothers and, in turn, later improvements in children’s receptive and/or expressive language skills and complexity of play, as well as more prosocial play with their mothers and fewer behavior problems (Guttentag et al., 2014; Landry et al., 2006, 2008, 2012). It is worth noting, however, that while My Baby and Me produced gains for mothers and children when administered from 4 to 30 months of age, PALS administered during the toddler years produced more positive outcomes for children than it did during infancy alone or across both infancy and toddlerhood. Let’s Play in Tandem (Ford et al., 2009) and REDI-P have (Bierman et al., 2015) demonstrated effectiveness in randomized controlled trials with respect to parent engagement during the preschool years, at ages 3 and 4-5, respectively. For Let’s Play in Tandem, weekly home visits for 1 year were used to train parents in how to engage children in activities designed to promote vocabulary, emergent literacy, and numeracy skills, as well as self-regulation. Although changes in parenting behaviors were not examined following treatment, significant child-level effects included improved vocabulary, literacy, numeracy, and general academic skills, as well as inhibitory control and social-behavioral skills. For REDI-P, parent training during home visits was focused primarily on developing parenting skills directed at children’s social-emotional, self-regulatory, and literacy outcomes, including how to better engage in literacy-based play and learning activities that support children’s learning skills and motivation. The intervention improved the richness of parent-child conversations and interactive reading activities.
When the children entered kindergarten, significant differences between treatment and control groups included better self-directed learning, literacy skills, and academic performance for those whose parents had received the trainings (Bierman et al., 2015).
Although generally less intensive than the other in-home and workshop trainings discussed above, several dialogic reading interventions (Arnold et al., 1994; Lonigan and Whitehurst, 1998; Whitehurst et al., 1988, 1994) have been designed to increase parents’ engagement with their children during storybook reading by training them to ask open-ended questions, respond to and encourage children’s comments and interests, and teach children vocabulary. Experimental evaluations of these interventions have shown them to be effective for improving literacy or language outcomes (e.g., expressive language skills), although these effects appear to be limited to immediately after the end of the intervention and may be most pronounced when complemented by similar interventions within child care/preschool. Similarly, programs designed to tutor parents in reading effectively with their children have demonstrated short-term but not long-term improvements in children’s literacy (Mehran and White, 1988). Notably, in these dialogic reading interventions, there is some evidence that video-based instruction and modeling that is complemented by discussion with parents is effective for training parents to better engage in their children’s early learning (Arnold et al., 1994; Whitehurst et al., 1988).
There are several other programs with some evidence of impact. In one randomized controlled study, interactions between high-risk parents and their children over developmentally stimulating, age-appropriate learning material (e.g., a book or a toy) followed by review and discussion between parents and child development specialists, were found to improve children’s cognitive and language skills at 21 months compared with a control group, and also reduced parental stress (Mendelsohn et al., 2005). In another experimental study, children of mothers who watched a series of short films on talking to children, using praise, using bath time to learn, and looking at books and puzzles, among other topics, followed by discussion with community health workers to encourage mothers to practice the activities with their children, showed significant benefits on measures of cognitive development predictive of academic achievement compared with controls (Chang et al., 2015).
Language interventions for parents of children with developmental disabilities and delays also have shown an impact. An 18-study meta-analysis found that language interventions implemented by parents had a significant and positive effect on the development of receptive and expressive language skills in children ages 18-60 months with and without intellectual disabilities (Roberts and Kaiser, 2011). In another randomized controlled study, Parent-Child Interaction Therapy, which targets child behavior problems
through mother’s use of child-directed play, improved language production among children ages 20 to 70 months with and at risk of developmental delays compared with a control group (Garcia et al., 2015).
In the Getting Ready for School intervention (Noble et al., 2012), 2-hour weekly workshops with parents over a 15-week period were used to complement existing Head Start teacher-parent workshops for families of children in randomly selected intervention classrooms. The complementary workshops, led by a trained facilitator, focused on teaching parents how to engage with their children at home in activities focused on literacy (e.g., helping their children learn the letters in their names), language (e.g., learning how to ask questions of their children), and math (e.g., helping their children recognize and extend patterns). Although parenting behaviors were not measured, compared with children in comparison classrooms, children of parents in the intervention evidenced improved language and literacy as well as applied problem and math concept scores.
There is also some evidence that aligning home learning contexts for literacy with early elementary school literacy learning is valuable, at least for increasing the frequency of literacy activities in the home of socially disadvantaged children. The Family Literacy Program (Morrow and Young, 1997), for example, encouraged parents to create home centers for parent-child literacy activities that paralleled 1st- to 3rd-grade classroom centers, while also encouraging reading daily, sharing stories, and writing journals together. Parents were guided through monthly group meetings and one-on-one mentorship. In an experimental study, according to parents and children, in-home literacy activities increased in the intervention group relative to controls, and teacher-rated literacy ability and interest improved, although no improvements were evident on a standardized reading assessment.
There is also evidence that transmedia interventions—focused on media content delivered across multiple platforms (e.g., videos, online games, and apps)—can be used to promote parent engagement in the home. From 2010 to 2015, the U.S. Department of Education supported the Ready to Learn initiative, a series of descriptive and experimental studies on parent-caregiver outcomes in supporting children’s cognitive (literacy and math) engagement and social-emotional skills. A randomized controlled evaluation study, Supporting Parent-Child Experiences with PEG+CAT Early Math Concepts, conducted by SRI International, addressed the question of how time spent viewing and playing with PBS KIDS educational, noncommercial media at home, in family settings, can foster positive outcomes for children and parents/caregivers (Moorthy et al., 2014). Using videos, online games, and tablet-based apps that allowed caregivers and children to engage with PEG+CAT characters, parents and caregivers in the treatment group reported a higher frequency of joint parent-child use of technology,
more joint gameplay, and more conversation connecting digital media and daily life than did nontreatment parents and caregivers. In addition, the study report indicates that children participating in the intervention exhibited statistically significant improvements in the mathematics skill areas of ordinal numbers, spatial relationships, and 3-D shapes compared with children in the nontreatment group. Important study limitations, however, included reliance on parent self-reports, selection bias, and inadequate assessments targeted by the study experience.
Finally, it is worth noting recent findings indicating that information about the importance of engaging in children’s learning may not be enough to achieve meaningful behavioral changes among parents. In a randomized field experiment of the Parent and Children Together Program (Mayer et al., 2015)—a 6-week intervention with English- and Spanish-speaking parents of children enrolled in Head Start programs—three behavioral tools were employed (text reminders, goal setting, and social rewards), and parents were provided with information about the importance of reading to children. Findings indicated large increases in usage of a reading app after the 6-week intervention with increases due to the behavioral tools rather than the increased information.
Parenting Education Delivered in the Context of Classroom-Based Early Care and Education Programs
ECE programs provide full- or part-time classroom-based services (center or family child care) for children from birth to age 5. They often include parenting education and other services for families (sometimes starting prenatally) designed to improve the overall circumstances of families and promote parenting knowledge, attitudes, and practices that support children’s cognitive and social-emotional development and success in school (Brooks-Gunn et al., 2000; Chase-Lansdale and Brooks-Gunn, 2014; Fantuzzo et al., 2013; Seitz, 1990). ECE programming that involves parents can be structured in several different ways, including (1) comprehensive two-generation programs with components that include multipronged, intensive classroom-based services for children, parenting education, and parent self-sufficiency support (as in Head Start, Early Head Start, and Educare); (2) primarily classroom-based services for children with some parenting education services; and (3) primarily classroom-based services for children with some parent self-sufficiency services.
The logic behind ECE programming that involves parents is the potential for additive effects for the child and family. Children’s positive experiences in care can have a direct effect on their outcomes, and if parenting education or parent self-sufficiency outcomes also are achieved, additional benefits may accrue. However, coupling ECE programs with parenting com-
ponents does entail costs, and with a fixed budget it is difficult to maintain high-quality efforts on both components. Indeed, a meta-analysis showed significant effects of preschool education on children’s cognitive and social development but found that provision of additional services tended to be associated with smaller gains (Camilli et al., 2010). Thus, it is important to identify two-generation models likely to generate benefits that justify their added expense and administrative complications.
This section summarizes findings from studies evaluating how ECE programs support parenting and healthy child development. The committee was unable to identify clearinghouses or reviews of classroom-based ECE programs that included parenting supports and thus drew on rigorous studies published in the peer-reviewed literature. Note that the discussion in this section excludes approaches used in the early intervention/special education system.
Head Start and Early Head Start
Head Start and Early Head Start are rigorously evaluated two-generation programs. (A brief description of both programs and numbers of families served can be found in Chapter 3.) In addition to education services directed at children, Head Start and Early Head Start programs are required to provide parents with activities that may include (1) parenting education, including at least two home visits per year whereby teachers give parents information about their children’s current classroom activities; (2) group parenting support classes on topics of interest to parents; and (3) opportunities to volunteer in the child’s classroom (Administration for Children and Families, 2016). Parent policy councils and center committees also provide opportunities for parents to participate in program leadership. Services are intended to be responsive to the needs and cultural and linguistic heritage of families in the communities served (Administration for Children and Families, 2016).
Parental engagement and service take-up, which have become a focus of attention because of the cost of nonparticipation and the potential impact of nonengagement on school readiness outcomes, are far from 100 percent (Administration for Children and Families, 2015d).8 Recent data show that just 41 percent of parents whose children were enrolled in Head Start attended parenting classes, although this percentage was 14 percent higher than that for control group parents. Attendance at goal-setting classes also was significantly higher for Head Start than for non-Head Start parents,
___________________
8 In June 2015, a Notice of Proposed Rulemaking on Head Start Program Performance Standards was issued, focused on the development of new targets for program participation (Administration for Children and Families, 2015d).
but take-up rates for nutrition, income, housing, utilities, education and job training assistance programs did not differ significantly between parents who won and lost lotteries for their children to enter the Head Start Program to which they had applied. Parents’ participation in the programs offered by Early Head Start was higher than was the case for Head Start parents, and almost always significantly higher for Early Head Start parents than for their control group counterparts (based on full-sample estimates) (Auger, 2015).
Head Start impacts on knowledge, attitudes, and practices and child outcomes Puma and colleagues (2012) provide a random-assignment evaluation of parenting impacts in the National Head Start Impact Study. Parenting-related measures included disciplinary practices, educational supports, parenting styles, parent participation in and communication with the school, and parent and child time together. Two cohorts of children (those entering Head Start for the first time at ages 3 and 4) were analyzed separately.
Looking first at impacts at the end of the Head Start year, in no case did any of the parenting measures differ significantly for the two cohorts of children. Practices for which significant impacts were found for only one cohort included an unexpected negative impact on the amount of time parents reported reading to their children (for the 3-year-old cohort) and beneficial impacts on spanking, reading, and cultural enrichment for the 4-year-old cohort. None of the beneficial impacts found at the end of the Head Start year persisted across the kindergarten, 1st-, and 3rd-grade follow-ups, and in no case did safety practices differ significantly between the Head Start and control groups. For the 4-year-old cohort, only 1 of 28 parenting impacts emerged as statistically significant (time spent with child in 3rd grade). For the 3-year-old cohort, there was some indication that parenting styles were more authoritative (characterized by high warmth and control) and less authoritarian for the Head Start group, although these patterns were seen in less than one-half of the tests conducted. Overall, despite the program’s stated goals of improving parenting, the Head Start evaluation found virtually no consistent evidence that this goal was achieved.
With respect to child outcomes, both cohorts showed statistically significant impacts on children’s language and literacy development while they were in Head Start, although these effects dissipated when children reached elementary school. By the end of 3rd grade, the only favorable impact was on reading, and this was only for the 4-year-old cohort. Results in the social-emotional domain differed by both cohort and source of information. In the 3-year-old cohort, early favorable impacts on social-emotional measures (problem behaviors, social skills) were sustained through 3rd grade based on parent-reported measures, but data reported by teachers suggested
no impacts on social-emotional outcomes in either the kindergarten or 1st-grade year. No social-emotional impacts were observed in the 4-year-old cohort through kindergarten, while favorable impacts were reported by parents and unfavorable impacts by teachers at the end of the 1st and 3rd grades. There was strong evidence of improved receipt of dental care at the end of the Head Start year in both cohorts (Puma et al., 2012).
One of the challenges of programs that include both direct and indirect pathways to child outcomes is the inability to assess the extent to which observed impacts are the result of any one component of the intervention. It is impossible to know in this case whether the parenting impacts noted (scattered as they were) had any role in the observed impacts on child outcomes. Nonexperimental analyses could provide exploratory answers to these types of questions.
Early Head Start center-based impacts on knowledge, attitudes, and practices and child outcomes Evidence of the impact of Early Head Start on parenting comes from the Early Head Start Research and Evaluation Project, a large-scale randomized evaluation following 3,001 children and families in 17 community sites. Sites delivered services primarily through home visits (discussed in the previous section), center-based services, or a mixed program approach whereby families received home visiting and/or center-based services (Love et al., 2005; U.S. Department of Health and Human Services et al., 2002).
A random-assignment evaluation of Early Head Start in four center-based programs found one positive impact of the program on the quality of parent-child play when the children were age 3 and one negative impact on parent knowledge of how to use a car seat correctly (U.S. Department of Health and Human Services et al., 2002). Mothers in the Early Head Start group reported lower levels of severe depression and were more likely than controls to be employed or in an education or training program. Overall, none of the other many parenting, parent well-being, home, and self-sufficiency outcomes studied was affected by Early Head Start among the families in the center-based sites. With regard to child outcomes at age 3, children in the Early Head Start group were less likely to show negativity toward their parent during a parent-child play task. There were no other impacts on child outcomes for the Early Head Start center-based group.
In sites using the mixed approach (center-based and/or home visiting services), families would in some cases receive home visiting services when they started in the program and then transition to center-based services when their children were older and the mother went to work. At age 3 and beyond, analysis indicated that among the three service delivery approaches, sites employing the mixed approach tended to have the greatest concentration of impacts with respect to both parenting and child outcomes
(U.S. Department of Health and Human Services et al., 2002). These findings may have implications for the need for increased flexibility in programming that allows families to shift from one mode of service delivery to another as their needs change.
Smaller-Scale Classroom-based ECE Interventions
Other classroom-based ECE programs that include parenting supports also have some evidence of effectiveness and provide insights into ways to reach parents. Effective interventions target improving parents’ engagement in preschool/elementary school, as well as parents’ roles as collaborators with teachers in decision making about children’s academic experiences. In some cases, these targets are complemented by attempts to improve alignment between home and classroom learning contexts.
The Companion Curriculum, for example, uses Head Start teachers to encourage parents’ participation in the classroom and provide workshops and activity spaces in the classroom that are focused on training parents to engage in parent-child learning activities. Although the program did not demonstrate benefits for parents’ involvement in the classroom or general engagement in home learning activities, it led to increased frequency of parent-child reading and improved children’s vocabulary in a quasi-experimental study (Mendez, 2010).
The Kids in Transition to School (KITS) Program is a short-term, targeted, evidence-based intervention aimed at increasing early literacy, social skills, and self-regulatory skills among children who are at high risk for school difficulties. This program provides a 24-session readiness group for children that promotes social-emotional skills and early literacy as well as a 12-session parent workshop focused on promoting parent involvement in early literacy and the use of positive parenting practices. In a pilot efficacy trial with 39 families, Pears and colleagues found that children in families who received the KITS intervention demonstrated early literacy and social skill improvements as compared with their peers who did not receive the intervention (Pears et al., 2014). In randomized controlled studies, foster children who received the intervention exhibited improvements in social competence, self-regulation skills, and early literacy skills (Pears et al., 2007, 2012, 2013).
Two-Generation Approaches
One class of early intervention programs uses a two-generation approach with an explicit focus on human capital skill building. As described by Chase-Lansdale and Brooks-Gunn (2014, p. 14), these programs “intentionally link
education, job training, and career-building services for low-income parents simultaneously with early education for their young children.”
Early versions of these kinds of two-generation programs focused on adolescent mothers, providing them with a host of education- and job-related services. Developed during a time when the nation was focusing on welfare reform and had not begun to appreciate the potential of high-quality early childhood education programs with respect to skill building for children, these programs typically viewed child care services as a means of supporting the self-sufficiency efforts of mothers rather than promoting the school readiness of their children.
Four prominent programs conducted during the 1980s and 1990s (Project Redirection, the New Chance Demonstration, Ohio’s Learning and Earning Program, and the Teen Parent Demonstration) offered adolescent mothers a wide range of services, including, in some cases, parenting classes, job training, and mandatory schooling (Granger and Cytron, 1999; Polit, 1989). Project Redirection was the earliest. It offered education and training programs for low-income adolescent mothers combined with intensive support services that included individual counseling, training in parenting and employability skills, and referrals to community services. Its evaluation, which was not based on random assignment, showed virtually no differences in parents’ education or training but some promising improvements in the quality of their children’s home environments and early literacy and behavior (Polit, 1989).
Evaluations of the other three programs were based on random assignment and showed a less positive set of impacts (Granger and Cyrton, 1999). In terms of parenting knowledge, attitudes, and practices, the New Chance Demonstration provided parenting education designed to promote positive parenting practices and better mother-child relationships and to reduce the stresses associated with parenthood. The Teen Parent Demonstration also included parenting workshops. The effects of these programs on mothers were not very promising, with virtually no impacts being seen on educational advances (New Chance increased GED holding, possibly at the expense of high school diplomas) or on mothers’ earning, employment, or welfare participation. Maternal mental health was assessed in evaluations of New Chance and the Teen Parent Demonstration, but in neither case did the program improve scores on the mental health measures employed. Moreover, mothers in the New Chance Demonstration experimental group reported significantly more parenting stress relative to their control counterparts.
Consistent with the view of child care as merely a support for the mother’s employment and education activities, none of these three programs affected any of the assessed dimensions of children’s school readi-
ness. In fact, New Chance mothers reported higher rates of child behavioral problems relative to their control group counterparts.
Another example of a rigorously evaluated comprehensive two-generation program was the Comprehensive Child Development Program (CCDP). Developed in the 1990s, this program was an ambitious attempt to provide low-income families with a range of social services designed to support infants’ and children’s cognitive, social-emotional, and physical development, as well as to enhance parents’ ability to support their children’s development and achieve economic and social self-sufficiency (St. Pierre et al., 1997). Services were intended to extend from birth through kindergarten or 1st grade but, in contrast to Head Start and some Early Head Start programs, were not built on a high-quality classroom-based program for children. The comprehensive nature of CCDP services is reflected in the program’s cost, which amounted to $15,768 per family per year, or about $47,000 per family over the entire course of the program (St. Pierre et al., 1997). (In 2014 dollars, this amounts to approximately $23,250 per family per year, or nearly $70,000 per family over the entire course of the program.)9
CCDP service delivery relied heavily on case managers and appeared to be implemented effectively (St. Pierre et al., 1997). For children, the program supported and in fact increased parents’ use of center-based child care, although evaluators did not systematically assess the quality of this care. Most sites offered biweekly home visits by a case manager or early childhood specialist between birth and age 3 in which training was provided to parents on infant and child development and, in some cases, modeling of ways to interact with children. Results of CCDP’s random-assignment evaluation 5 years after the program began showed no statistically significant impacts on parenting skills or self-sufficiency among participating mothers or on the cognitive or social-emotional development of participating children (St. Pierre et al., 1997). Nor did consistent impacts emerge for any demographic subgroups or among the families that participated in the program for most of the service period. Evaluators speculated that the lack of impacts may have been the result of some combination of the dilution of service quality caused by the overly ambitious scope of program services and, for children, the program’s reliance on indirect effects through parents rather than direct effects that might have come from high-quality classroom-based early education services.
In contrast to CCDP, the Child-Parent Center (CPC) Program in Chicago is a center-based early intervention program that offers comprehensive educational and family support services designed to increase academic success among low-income children ages 3-9 residing in disadvantaged Chicago neighborhoods (University of Minnesota, 2013). CPC employs a number of components directed at children and parents to meet the program objec-
___________________
9 Calculated based on the Consumer Price Index (Crawford et al., 2016).
tives, such as structured and diverse language-based instructional activities; low child-to-teacher ratios; a multifaceted program for parents that takes place under the supervision of a parent-resource teacher (e.g., volunteering in the classroom, attending school events, enrolling in educational courses); outreach activities (resource mobilization, home visitation); ongoing staff development; health and nutrition services; and supports to help children from 1st to 3rd grade transition to elementary school (Reynolds, 2000). Longitudinal analyses of CPC show participation to be associated with children’s improved future performance in school, such as reading and math achievement, especially for those who remain in the program for several years (Reynolds, 1997; Reynolds and Temple, 1998; Reynolds et al., 2004). Parents’ involvement in school was found to be a mediator of the program’s effects, suggesting that the program components targeting parents played a role in its success (Reynolds et al., 2004).
New in two-generation programming are so-called “Two Generation 2.0” human capital programs (Chase-Lansdale and Brooks-Gunn, 2014), which assign a key role to high-quality ECE. Examples of such programs for which evaluations are planned or under way include the CareerAdvance® Community Action Project of Tulsa, Oklahoma; the Annie E. Casey Foundation Atlanta Partnership; and the Housing Opportunity and Services Together project (see Chase-Lansdale and Brooks-Gunn, 2014, for others). In effect, these programs view ECE as an important and independent source of human capital training for children rather than merely a means of providing child care in order to promote the careers of mothers. ECE is coupled with postsecondary workforce skill development for parents, with training taking place in community colleges, job training programs, or workplaces. The theory of change behind these models is focused on the education benefits to children of high-quality ECE programs and higher parental levels of education and labor force motivation. Parenting knowledge, attitudes, and practices may be improved, but the improvement comes indirectly through higher parental job skills and education and reduced household stress rather than explicit programming directed at parenting skills.
Within programs designed to enhance school readiness, a subset of programs target children’s cognitive skills (language, literacy, and math) and focus as well on children’s social-emotional development, given the reciprocal nature of these skills. For example, Educare, based in 12 Educare schools and on Head Start’s parent involvement objectives, focuses on receptive language, vocabulary, and early reading, and children’s social-emotional skills. To date, implementation studies have shown promise for the program in addressing the quality gap of service delivery and parent engagement. A randomized controlled trial currently under way is comparing children at age 3 who are cared for at home or in other settings with
children who are served in Educare on cognitive, language, executive function and social-emotional measures, and examining whether performance on these measures differs for dual language learners. No strong evidence on program impacts is available, however, so it is impossible to determine whether this new generation of programs will change parenting knowledge, attitudes, and practices or improve child well-being.
A brief summary of two ECE programs developed in the latter half of the 20th century, in which children assigned to comparison groups faced different and often worse conditions than they do today, is provided in Box 4-4.
Parent Engagement in School Settings and School-Related Activities, Prekindergarten through Grade 3
Beyond stimulation of and support for learning activities in the home, parents engage in their children’s early learning and education through an array of practices aimed collectively at promoting educational success and well-being. These practices may include participation in school functions (e.g., classroom volunteering), communication with school personnel (e.g., parent-teacher conferences), supervision and assistance with school-related home activities (e.g., help with homework), and education-related communication and connections with other families and community members (e.g., parent social networks).
Although the terminology used to describe parenting behaviors relative to children’s learning and education varies in the empirical literature (e.g., parent engagement, parent involvement, family-school partnerships), most researchers emphasize the ways in which such engagement requires connections between parent and child and relationships across home, school, and community contexts. The parent engagement literature generally treats schools and communities as parents’ partners and collaborators because parents’ power to act on behalf of their children’s educational interests is determined, in large part, by the extent to which schools and communities make parents aware of opportunities, give them access to resources, and enable them to take advantage of these opportunities and resources (Dearing et al., 2015; Henderson and Mapp, 2002). In the parent-engagement intervention literature, programs generally take one of two approaches: (1) focusing primarily on improving parents’ level and quality of engagement in the home environment with regard to learning stimulation and behavior regulation, or (2) focusing on connecting parents with their children’s schools to promote academic achievement and/or positive behaviors.
Theory on parent engagement is built largely on ecological systems frameworks, particularly those focused on how aligning child, family, school, and community assets can help promote positive development in
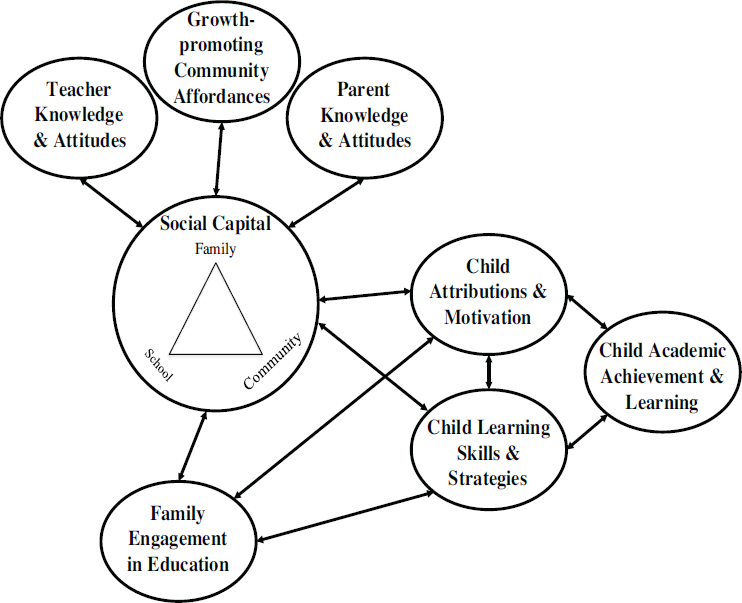
SOURCE: Dearing et al. (2015).
contexts characterized by multipronged social and economic disadvantage (García Coll et al., 1996; Huston and Bentley, 2009). More specifically, theory on parents’ engagement in children’s early education has hypothesized benefits for achievement and school success through three primary mechanisms (see Figure 4-2).
First, collaboration among families, schools, and communities can help build the capacity to stimulate and support children’s learning. This linkage holds if (and only if) the information channels and norm reinforcement provided by the social network members emphasize knowledge, attitudes, and practices that are beneficial for children’s achievement (e.g., teachers sharing with parents knowledge about best practice for promoting learning, and parents sharing with teachers nuanced information about their children as learners).
Second, it is expected that when parents are involved in their children’s schooling with developmentally appropriate levels of autonomy and
emotional support, they communicate positive beliefs about the children’s learning potential. In turn, the children are likely to have positive feelings toward learning and themselves as learners, identify positively with their parents’ achievement values, and meet learning challenges with effort and feelings of self-efficacy (Pomerantz et al., 2007).
Third, parents play a direct role in building children’s learning strategies and skills, including approaches to problem solving, study skills, domain-specific and domain-general knowledge, and meta-cognitive skills. For a review, see Dearing and Tang (2010).
As noted in a recent review of parent engagement programs, policies, and practices (Sheridan et al., 2016), practice recommendations for interventions targeting parent engagement in early childhood education tend to emphasize the value of cultivating positive parenting through connections between home and school. Also emphasized is the importance of ensuring that these partnerships can be “culturally sensitive (responsive to values, priorities, and interaction styles of families), developmentally responsive (appropriate to children’s needs across the developmental spectrum), intentional (focused on specific objectives), strengths-based (building on family and child competencies and interests), and collaborative (structured around mutual—parent and teacher—goals).” In turn, interventions proving successful in randomized experimental evaluations share such characteristics as a strong emphasis on (1) frequent communication and sharing of information between parents and early childhood teachers, (2) collaborative goal setting in which parents and teachers work in partnership to develop an educational plan for their children, and (3) improvements in parenting skills and parenting efficacy (Sheridan et al., 2016).
Evidence-Based Programs for Promoting Parent Engagement in Young Children’s Schooling
Much of the research on parents and children’s schooling has focused on the association between parent involvement and children’s academic outcomes. Studies have found that specific parent involvement behaviors, such as participation in school activities and direct communication with teachers, are linked to higher academic achievement in both reading and mathematics (El Nokali et al., 2010; Fan and Chen, 2001; Fantuzzo et al., 2004, 2013). Furthermore, parent involvement in the home, such as monitoring assigned homework and participating in learning activities, as well as having conversations with their children about school, is linked to higher reading and writing scores and report card grades. With some exceptions, the research on the effects of fathers’ similar involvement has been sparse.
Many attempts have been made to improve parent engagement through interventions in the home and through home-school connections. The focus
here is on interventions with socially disadvantaged children and families targeting home-school connections between prekindergarten and 3rd grade for which evidence of efficacy has been derived from randomized experimental evaluations.
A family mathematics curriculum intervention (Starkey and Klein, 2000) used an approach similar to that of the Family Literacy Program for improving parent engagement in children’s math learning. Specifically, Head Start teachers trained parents in the use of math learning activities and games designed to promote developmentally sequenced learning of number concepts, arithmetic operations, logical reasoning, geometric concepts, and patterns. One notable feature of this program was that Head Start teachers were matched ethnically with parents. Families also were given learning activities to use at home. Although parenting behaviors were not observed in the home, this 4-month (eight classes) intervention resulted in improved math performance among children in the treatment group compared with the control condition.
In the Parent Corps Program, parent groups—cofacilitated by preschool teachers and mental health professionals with expertise in behavior management—are used to help parents establish structure and routines for children, to teach positive parenting practices (e.g., use of positive reinforcement and consistent consequences), and to provide opportunities for facilitator-observed parent-child interactions. Parent Corps evaluators note that a critical component of the intervention model is the “numerous opportunities to directly increase parent–teacher communication. Parents heard from teachers about their use of effective behavior management practices at school and in turn shared ideas based on how their child responded to the practices at home. Teachers heard parents’ perspectives about daily struggles and the challenges of implementing these practices at home” (Brotman et al., 2011, p. 263). More effective parenting practices in the treatment compared with the control groups were evident, including parent reports of using more effective disciplinary practices, higher scores on tests of knowledge of effective behavior management strategies, and higher-quality parenting in researcher-observed parent-child interactions (Brotman et al., 2011). The intervention also resulted in reduced behavior problems among children.
Getting Ready is an evidence-supported intervention targeting parents’ decision-making role at school (Sheridan et al., 2010). This program uses structured interactions between early childhood teachers and parents during home visits, parent-teacher conferences, and monthly family socialization activities that are designed to engage parents actively in learning and behavior goal setting and decision making. Together, teachers and parents identify learning opportunities at home and school and plan how educators and parents can complement each other’s efforts to promote learning and
track children’s growth. Priorities include affirming parents’ competence, increasing their access to information on child development, and reinforcing positive parenting practices. Treatment effects have, in fact, been evident for parental warmth and sensitivity, learning support, and autonomy support (Knoche et al., 2012). In one study involving children of mothers with depression, children in the Getting Ready intervention experienced a significantly greater decline in some problem behaviors (e.g., difficulty standing still, tendency to run around) relative to children in the control group. However, no differences were observed for other learning-related behaviors (Sheridan et al., 2014). In addition, the Getting Ready intervention has been found to improve children’s language and literacy (Sheridan et al., 2011), with some evidence that its effects on achievement are largest for children at greatest risk for underachievement (e.g., those whose parents have less than a high school education and those who did not speak English prior to treatment [Sheridan et al., 2011]).
Applying a similar collaborative model focused exclusively on child behavior, the Parent-Child Action Teams intervention uses a parent liaison to create and guide partnerships among parents, teachers, and other school professionals focused on assessing and monitoring children’s learning progress. In addition to parent-reported improvements in empowerment, intervention children were found to have significant reductions in externalizing and internalizing behavior problems compared with control children.
USE OF INFORMATION AND COMMUNICATION TECHNOLOGIES TO SUPPORT PARENTING
Information and communication technologies can contribute to parenting in two ways: (1) socialization with respect to what parenting is and means through the media, especially entertainment media, and (2) development and maintenance of parenting skills through interventions that use these technologies. New information and communication technologies provide numerous opportunities to deliver interventions with the potential to improve parenting. Digital delivery of parenting interventions has been explored as a way to overcome barriers to participation and to increase the reach, sustainability, and impact of interventions. In theory, at least, parents who can access a training program from a computer or mobile device when and where it is convenient for them to do so may face fewer logistical and financial barriers (e.g., child care, transportation) to participation. The new technologies also make it possible to tailor services to special parent populations.
Established and emerging communication technologies are now common in American households and are reframing the context of modern parenting. The majority of U.S. households have a computer and Internet
access, making digital modes of intervention a promising strategy for improving program reach. In 2013, approximately 84 percent of households reported having a computer (with 78.5% having a desktop or laptop computer and 63.6% having a handheld computer), and approximately 74 percent of households reported Internet use (File and Ryan, 2014). According to data from the Pew Internet and American Life Project’s Networked Families Survey, married parents with minor children living at home relative to other household configurations have the highest rates of Internet and cell phone usage, computer ownership, and broadband adoption (Kennedy et al., 2008). Nontraditional family arrangements, such as single-parent and unmarried multiadult households, also tend to be heavy users of these technologies, particularly with respect to text messaging and use of social media (Kennedy et al., 2008). Contrary to concerns that these technologies could divide families and impede their meaningful interaction, results of nationally representative surveys from the Pew Research Center reveal that technology—particularly mobile phones and the Internet—is enabling new forms of family connectedness (Kennedy et al., 2008). In fact, the majority of parents believe technology allows their families to be as close, or closer, than their families were when they grew up (Kennedy et al., 2008). Parents use the Internet to help research, organize, and improve various aspects of their lives. As far back as 2002, one study found that 73 percent of online parents used the Internet to learn new things, and 52 percent said their use of the Internet improved the way they connected with their family members (Allen and Rainie, 2002).
While the penetration of new information and communication technologies is widespread, significant inequalities in access to the technologies persist (Viswanath et al., 2012). For example, young adults, members of minority groups, and individuals with low educational attainment and low household income are more likely to say that their phone is their main source of Internet access. In contrast to Internet access, African Americans and whites are equally likely to own a cell phone of some kind and also have similar rates of smartphone ownership (File and Ryan, 2014; Zickuhr and Smith, 2012). Nonetheless, data suggest that low-income and minority groups are more likely to experience disruptions in service due to lack of payment of bills, relocation, or a change in phone number (Smith, 2015). Furthermore, although the Internet may be widely used (Smith, 2014), disparities in access by income, education, race/ethnicity, and other factors need to be considered in the implementation of programs for the diverse population of primary caregivers of young children (see Table 4-2). In 2013, for example, just 62 percent of households earning less than $25,000 had a computer, and only 48 percent had some form of Internet access, whereas among households earning $150,000 or more, 98 percent had a computer, and 95 percent had Internet access. Blacks and Hispanics (of any race),
TABLE 4-2 Computer and Internet Use among U.S. Households, 2013
| Household Characteristic | Total Households (in thousands) | Percentage of Households with a Computer | Percentage of Households with an Internet Subscription |
|---|---|---|---|
| Race and Hispanic Origin of Householder | |||
| White alone, non-Hispanic | 80,699 | 85.4 | 77.4 |
| Black alone, non-Hispanic | 13,816 | 75.8 | 61.3 |
| Asian alone, non-Hispanic | 4,941 | 92.5 | 86.6 |
| Hispanic (of any race) | 14,209 | 79.7 | 66.7 |
| Limited English-Speaking Household | |||
| Yes | 111,084 | 84.7 | 75.5 |
| No | 5,207 | 63.9 | 51.4 |
| Metropolitan Status | |||
| Metropolitan area | 98,607 | 85.1 | 76.1 |
| Nonmetropolitan area | 17,684 | 76.5 | 64.8 |
| Household Income | |||
| Less than $25,000 | 27,605 | 62.4 | 48.4 |
| $25,000-$49,999 | 27,805 | 81.1 | 69.0 |
| $50,000-$99,999 | 34,644 | 92.6 | 84.9 |
| $100,000-$149,999 | 14,750 | 97.1 | 92.7 |
| $150,000+ | 11,487 | 98.1 | 94.9 |
| Educational Attainment of Householder | |||
| Less than high school | 12,855 | 56.0 | 43.8 |
| High school graduate | 28,277 | 73.9 | 62.9 |
| Some college/associate’s degree | 34,218 | 89.0 | 79.2 |
| Bachelor’s degree or higher | 36,349 | 95.5 | 90.1 |
SOURCE: Adapted from File and Ryan (2014).
those with a high school education or less, those living in nonmetropolitan areas, and those living in households in which limited English is spoken also were much less likely to have computer and Internet access in 2013 (File and Ryan, 2014).
Another challenge is that, compared with previous generations, parents today are exposed to a much greater amount of information via a variety of channels, including entertainment media such as television and digital platforms such as the World Wide Web and DVDs. Much of the available information is untested and sometimes contradictory, and the sheer amount of information and the fact that it may be contradictory may confuse parents and families.
As discussed in Chapter 6, despite the effectiveness of a number of various face-to-face parenting interventions, there are a number of barriers to parents’ participation and retention in these programs. According to Breitenstein and colleagues (2014), studies of involvement in face-to-face interventions for parents of children in preschool through grade school show that only 10 to 34 percent of parents enroll (Baker et al., 2011; Garvey et al., 2006; Heinrichs et al., 2005; Thornton and Calam, 2011). Among those who do participate, average attendance rates range from 35 to 50 percent of sessions (Breitenstein et al., 2012; Coatsworth et al., 2006; Scott et al., 2010). Creating online-based content may be one strategy for increasing participation in interventions by providing a more convenient way to receive the information. In addition, digital delivery of parenting interventions may reduce challenges associated with uneven implementation that often occur with face-to-face interventions, including those provided across multiple sites, where adherence to protocols may vary (Breitenstein et al., 2014, 2015). Digital modes of delivery also may decrease demands on providers’ time and reduce costs and other resources associated with providing the intervention in person. This can be an important advantage for some communities, as the costs of hiring, training, and maintaining professionals for evidence-based programs can be prohibitive for isolated and poorly resourced agencies
(Baggett et al., 2010), while rural communities may have limited numbers of professionals available to provide evidence-based programs.
The body of research on the use of technology and media to improve parenting knowledge and skills and provide social support for parents is relatively small but growing. This research has included evaluations of parenting programs, several of which are discussed in Chapter 5, that have been adapted from a face-to-face to an online format (e.g., Triple P Online, the Incredible Years), as well as programs developed at the outset for delivery in a digital format.
A recent systematic review included 11 experimental and quasi-experimental studies of seven parent training interventions utilizing digital delivery methods (electronic text, audio, video, or interactive components delivered via the Internet, DVD, or CD-ROM) for administering a portion of or the entire program (Breitenstein et al., 2014). Eight of these interventions supplemented text and other instructional content with videos of parent-child interactions (an effective teaching strategy in face-to-face interventions that is easily translated to digital formats). In the four programs for which parent and child behavioral outcomes were reported—InfantNet, Internet-Parent Management Training, Parenting Wisely, and Triple P Online—medium to large effect sizes were observed in the areas of infant and parent positive behaviors, child behavioral problems (e.g., conduct, hyperactivity), parental disciplinary practices, parental self-efficacy and satisfaction, and postpartum depression. When reported, participants’ satisfaction with the interventions was high, ranging from 87 to 95 percent (Breitenstein et al., 2014). Although these findings suggest that the programs had a positive effect, it is difficult to draw firm conclusions given the small number of studies. Furthermore, in 6 of the 11 studies, 75 percent or more of the sample was white; only one intervention had a sample with a more diverse distribution among racial groups (Scholer et al., 2010, 2012), possibly limiting the generalizability of the findings. Future studies including parents from diverse racial/ethnic and socioeconomic backgrounds are needed. The studies reviewed also relied primarily on parents’ self-reports rather than electronic tracking methods to assess completion of the intervention, and parents may misreport their completion rates. In the 2 studies that did use electronic tracking, the intervention doses were 92 percent (Baggett et al., 2010) and 67 percent (Sanders et al., 2012)—as high as or higher than those reported by parents in the other studies. Finally, as none of the interventions reviewed had been formatted for mobile devices, the review showed a need for further experimental research on parenting interventions formatted for such devices.
Other studies have examined the feasibility of adapting evidence-based training in parenting skills to information and communication technologies. A recent evaluation of the adaptation of the face-to-face Chicago Parent
Program (CPP), designed for low-income, diverse families, to an Android tablet application showed that it is feasible to accomplish such adaptation and maintain the core components of the original program when key stakeholders (parents, program developers, and designers) are engaged (Breitenstein and Gross, 2013; Breitenstein et al., 2015). The adapted program, eCPP, includes interactive activities, video examples and explanations of parenting strategies, reflection questions, evaluation of parent knowledge with feedback, and practice assignments.
Taylor and colleagues (2008) evaluated the feasibility of adapting the Incredible Years Program to a technology-based format. The study collaborators combined a computer and Web-based intervention that presented a large portion of the original Incredible Years content through technology (including video vignettes, sound files, and pictures) with support from a coach delivered through phone calls, electronic messages, and home visits. Ninety Head Start families with high levels of child behavior issues joined the study, which was implemented as part of a randomized controlled trial. Participation rates were comparable to those in the group-based Incredible Years Program, and among a subset of participants (45 families) 30 reported achieving at least one of their self-determined goals. Although further study is needed to demonstrate the effectiveness of the approach, this study showed the feasibility of using technology for adaptation and dissemination of evidence-based parenting interventions (Taylor et al., 2008).
Triple P Online is a Web version of the Triple P-Positive Parenting Program for parents of children ages 2 to 12 with behavioral problems that can be completed by parents at their own pace over a 16-week period. Triple P Online consists of eight interactive modules, each of which takes 30 to 60 minutes, on such topics as encouraging child behaviors that parents like, managing misbehavior and disobedience, and raising confident and capable children. Each of the eight modules includes video demonstrations of positive parenting skills and activities to help parents utilize these skills. After completing an initial module, parents gain access to such resources as worksheets, podcasts, and text message summaries (Triple P-Positive Parenting Program, 2016b). A focus group and survey study involving African American and Hispanic parents residing in economically depressed areas in Los Angeles County showed the feasibility of using social media in Triple P Online to reach high-risk, high-poverty families (Love et al., 2013). In a subsequent relatively small randomized study comparing two self-help versions of Triple P—Triple P Online and a self-help workbook—no differences in short-term intervention effects were observed for dysfunctional parenting and disruptive child behavior; both versions were associated with significant declines in levels of disruptive child behavior, dysfunctional parenting styles, risk of child maltreatment, and interparental conflict on
both mother and father report measures. Results were largely sustained at 6-month follow-up (Sanders et al., 2014).
SafeCare®, designed specifically to prevent and reduce the recurrence of child maltreatment among families of children ages 0-5, has used technology-based hybrid approaches for the delivery of skills training during home visits. Cellular phone technology is incorporated into the Parent-Child Interaction (PCI) module of SafeCare, from which parents learn skills to increase positive interactions with their children. In a randomized controlled trial involving 371 mother-child dyads, mothers who received cellular phone-enhanced training from home visitors (i.e., tailored cell phone text messages about skill usage delivered twice a day and weekly phone calls to discuss the text message content and other issues raised by mothers) used significantly more positive parenting skills relative to waitlist controls. Perhaps as a result of increased contact with the home visitors due to use of the technology, these mothers showed more positive parenting strategies, reduced depression, and increased child-adaptive behaviors 6 months postintervention relative to parents who received traditional training, as well as waitlist controls. They also showed greater retention in services (Bigelow, 2014; Carta et al., 2013). In a small feasibility study involving three families, use of iPhone™ video in the SafeCare home safety module showed promise as a way to identify and reduce child safety hazards. Parents used the phone between home visits to capture video of rooms in their home. They then sent these videos to the home visitor, who evaluated them for hazards and provided feedback to parents. The safety module of SafeCare is typically completed in six in-home sessions lasting between 90 and 120 minutes. As a result of the use of this technology, face-to-face time for the home visits was progressively reduced and replaced by the video data collection (Jabaley et al., 2011).
Behavioral parent training (BPT) is designed to promote changes in attitudes and practices related to harsh discipline among parents of young children with attention deficit hyperactivity disorder who display conduct problems and antisocial behaviors (Chacko et al., 2009; Cowart-Osborne et al., 2014; Kaminski et al., 2008; van den Hoofdakker et al., 2007; Webster-Stratton et al., 2011). This training has been found to be effective for preventing child maltreatment and reducing child maltreatment recidivism (Barth, 2009; Cowart-Osborne et al., 2014; Kaminski et al., 2008; Whitaker et al., 2005). In-person, group-based BPT typically takes place over several weeks and involves instruction, modeling, and practice of positive parenting behaviors; supportive group discussions; and home practice assignments. Studies provide preliminary evidence that incorporating media, such as an Internet program, videotapes supplemented by telephone or in-person coaching, and multimedia CD-ROMs into BPT is effective for improving parenting skills (Cefai et al., 2010; Irvine et al., 2014; Webster-
Stratton and Reid, 2010). For example, in a recent randomized trial of an Internet BPT program (Parenting Toolkit) using a scenario-based video hybrid instructional design conducted at urban community centers, test scores of parents of youth ages 11-14 who viewed the toolkit and completed a 1-month follow-up (N = 90) indicated that they would be less likely than controls (N = 140) to overreact and respond harshly during disciplinary interactions with their children and more likely to follow through with promised consequences. These parents also reported a reduction in their children’s problem behaviors and greater gains in their own self-efficacy and intention to engage in positive parenting practices (Irvine et al., 2014).
Another emerging area of research is parents’ use of technology and media as a source of social support. In a recent survey of parents by the Pew Research Institute, nearly three-quarters of respondents reported receiving social support from others on social media (Duggan et al., 2015). Forty-two percent of parents using social media (more mothers than fathers) reported that they had received social or emotional support specifically for a parenting issue on social media in the past month. Eight percent and 16 percent of parents, respectively, said they received social or emotional support for a parenting issue “frequently” or “sometimes” over the past month (Duggan et al., 2015).
The use of social media (e.g., Facebook, Twitter) among mothers with young children to share information about their children is an emerging trend. One correlational study of new mothers (N = 157) evaluated whether blogging and social networking is associated with improvement in maternal well-being by providing social support (McDaniel et al., 2012). Maternal well-being was assessed by means of psychological and emotional measures, such as marital functioning, parenting stress, and depression. The study demonstrated an association between the frequency of blogging and feelings of connection to extended family and friends, perceived social support, and maternal well-being, showing that blogging may be a powerful tool for developing a new mother’s sense of increased connection to the outside world and eventually improving her well-being (McDaniel et al., 2012).
In a quasi-experimental study involving 1,300 mothers of infants, intervention participants were provided with online interactive resources that offered information and social support. These resources included an information database, an online peer discussion forum, and an online answering service staffed by nurses and midwives, covering such topics as how to respond to infants’ cues and needs. The study found that the intervention had no effect on mothers’ perceptions of parenting satisfaction and depressive symptoms. Yet relative to mothers in the control group, mothers in the intervention experienced higher infant centrality at 6 weeks (Salonen et al., 2014).
Differences in preferred channels of information may depend on the
type of parenting information sought. In primary care settings, especially in pediatrician offices, parents’ preferred channel of delivery for patient educational materials may vary based on the type of message and the complexity of the information. A review of 114 studies of patient education in primary care settings using primarily randomized controlled designs looks at parents’ preference for delivery formats for information on such topics as positive parenting practices, children’s behavioral self-management, and skills for improving the well-being of both children and families (Glascoe et al., 1998). The authors report that media, including advertising campaigns and office posters, helped extend parents’ interests to new areas, while parents preferred verbal communication for brief and concrete messages. Modeling and role playing were particularly beneficial for addressing problematic parenting or child behavior. However, there may be challenges to delivering long, complex verbal messages to parents in primary care settings; limitations of memory and understanding of content may make the information difficult to absorb, particularly in stressful situations such as discussing problematic child behaviors or other family concerns. The authors suggest that written form may be more beneficial for communicating complex medical information.
Web-based strategies have also been tested among foster, adoptive, and kinship parents, who may need to deal with particularly difficult behavioral issues (Pacifici et al., 2006). In a pre- and post-test study, Pacifici and colleagues (2006) investigated the effectiveness of two interactive Web-based courses on lying and sexualized behavior in children developed for foster, adoptive, and kinship parents. Findings demonstrated significant improvement in parental knowledge for both courses and a significant increase in competency-based parenting perceptions for the course on lying. This Web-based program also led to new connections and interactions among users, and overall user satisfaction was high (Pacifici et al., 2006).
In summary, while early research on the use of information and communication technologies to support parenting has had promising results, much more remains to be done. Future research needs to include study populations that are more culturally and socioeconomically diverse and incorporate electronic tracking to monitor usage. In addition, more work is needed to develop formatting for mobile devices to extend the availability of interventions to those without access to a computer (Breitenstein et al., 2014). While some research supports the use of the Internet and other technologies for the delivery of parent training, interventions that utilize in-person support group formats (e.g., Triple P, the Incredible Years) have shown significant effects on parenting practices, some of which can be measured years later. It is not yet clear whether self-administered, technology-based interventions can replicate the effects of these interventions (Irvine et al., 2014). One attractive feature of technology-based interventions is
providing parents with the ability to learn at their own pace, although there is a risk that parents will move too quickly without taking the time to practice new skills or too slowly so they lose momentum and interest (Breitenstein et al., 2014). If programs are to remain relevant and engage a broad population, however, they would need to adapt to Americans’ growing reliance on technology for information relevant to parenting. This may be especially true for younger, including adolescent, parents, who are accustomed to communication through technologies that have been available to them their entire lives (Cowart-Osborne et al., 2014). As is the case for all parenting interventions, if technology-based parenting support interventions are to have a positive effect on parenting practices, their developers need to apply theories of behavior change (e.g., the theory of reasoned action and the theory of planned behavior) that can inform influential mechanisms through which such interventions can impact parenting knowledge, attitudes, and practices. In addition, ecological approaches that intervene at multiple levels are called for as multilevel interventions may have more lasting effects on behavior change.
Finally, a gap in the research on information and communication technologies is work on how entertainment media socialize young parents on norms of parenting. While formal avenues of classes and structured curricula are important for developing and reinforcing certain norms about parenting, entertainment media are also likely to have a significant influence. This is an area ripe for additional work.
SUPPORTING PARENTING: INCOME, NUTRITION ASSISTANCE, HEALTH CARE, AND HOUSING PROGRAMS
As described in Chapter 3, a number of programs and policies at the federal level are designed to provide resources for families. Some provide direct cash assistance, others help ensure the health of children, and some provide services and parenting education in conjunction with the material assistance. This section focuses on research evaluating the impact of these programs, both directly on children and parents and with respect to facilitating better parenting.
The Earned Income Tax Credit and Child Tax Credit
As discussed in Chapter 3, the Earned Income Tax Credit (EITC), which offsets the amount owed in taxes for low-income working families, is one of the largest poverty alleviation programs for the nonelderly in the United States (Center on Budget and Policy Priorities, 2016). The credit is paid by the federal government, as well as by 26 states and the District of Columbia, which set their own EITCs as a percentage of the federal credit
(Center on Budget and Policy Priorities, 2016). Federal benefits were as high as $6,269 for families with three or more qualifying children in 2016 (Internal Revenue Service, 2016). Single mothers are the group most likely to be eligible for the EITC. Noncustodial parents who qualify as childless workers may claim the EITC, although payments under this category are much smaller than those to custodial parents (Marr and Huang, 2015; Marr et al., 2015). The Child Tax Credit, up to $1,000 per child, offsets the costs of raising children for low- to moderate-income working families (Center on Budget and Policy Priorities, 2016). The credit is paid by the federal government and a few states that have their own programs.
A growing literature, none of it relying on random assignment, has demonstrated associations between the generosity of EITC payments and maternal work, stress, and health-related outcomes and behaviors; parenting practices discussed in Chapter 2, such as receipt of prenatal care and breastfeeding; and child well-being.
Consistent evidence suggests that tax credits improve employment-related outcomes for most recipients. Analyses of the EITC expansions that took place in the 1990s show that they contributed to significant increases in work and wage growth among single mothers and female heads of households compared with women who were otherwise similar but did not receive the EITC (Blank, 1997; Herbst, 2010; Hotz and Scholz, 2003). According to Meyer and Rosenbaum (2001), more than one-half of the large increase in employment among single mothers that occurred during the late 20th century can be attributed to the EITC expansions that took place between 1984 and 1996.
Benefits such as the EITC that are designed to encourage parents to work are not unambiguously beneficial for children and their parents, however, especially when they are provided to single low-income, parents who are particularly likely to hold jobs that are stressful and require them to work long hours or unusual shifts (Heinrich, 2014). While the income that working parents earn may benefit themselves and their children in some ways, the stress they bring home from work may undermine their parenting practices and the atmosphere in the home (Duncan et al., 2001; Heinrich, 2014). Working parents who lack access to or cannot afford quality child care may place their young children in lower-quality care or leave them unsupervised or with older child siblings. If policies such as the EITC aimed at increasing employment rates among parents are to be beneficial, these kinds of problems need to be prevented (Heinrich, 2014).
A considerable body of research has explored how the EITC may influence adult recipients’ health and health-related behaviors although a 2013 review of many of these studies found that they carry a high risk of bias from confounding and insufficient control of underlying time trends (Pega et al., 2013). One of the stronger studies links expansions of the EITC to
data from the Behavioral Risk Factor Surveillance System and the National Health and Nutrition Examination Survey (Evans and Garthwaite, 2010). In particular, between 1993 and 1996, the generosity of the EITC increased sharply, especially for mothers with two or more children. If income matters for maternal stress and health, the authors argue, greater improvement should be seen for children and mothers in two-child low-income families than in single-child low-income families. Indeed, the study found that, compared with mothers with one child, low-income mothers with two or more children experienced larger reductions in risky biomarkers and self-reported better mental health.
Additional studies have shown that the generosity of EITC payments is associated with improvement in several health-related outcomes/behaviors, including food security, smoking cessation, and efforts to lose weight. The EITC also may improve working mothers’ access to health insurance (Averett and Yang, 2012; Cebi and Woodbury, 2009). At the same time, however, the generosity of EITC payments has been found to be associated with detrimental effects on metabolic factors among women (Rehkopf et al., 2014) and morbidity indictors such as weight gain (Schmeiser, 2009).
As for child outcomes, studies have found that EITC expansions in the early 1990s contributed to improved academic achievement in the form of higher test scores (especially in math) and higher high school/GED completion rates (Chetty et al., 2011; Dahl and Lochner, 2012; Maxfield, 2013). The Maxfield (2013) study also found effects of higher EITC payments on college enrollment by age 19 or 20. An analysis of reading and math test scores among 2.5 million children in grades 3 to 8 in an urban school district and corresponding tax record data for their families, spanning the school years 1988-1989 through 2008-2009, found that additional income from the EITC resulted in significant increases in students’ test scores; a $1,000 increase in the tax credit raised students’ test scores by 6 percent of a standard deviation (Chetty et al., 2011). Students with higher test scores were more likely to attend college, have higher-paying jobs, and live in better neighborhoods as adults and less likely to have a child during adolescence. These findings led the authors to conclude that a substantial portion of the cost of tax credits may be offset by earnings gained in the longer term.
In addition, available evidence suggests an association between parents’ receipt of the EITC and improved birth and perinatal outcomes. An analysis by Arno and colleagues (2009) found that each 10 percent increase in EITC penetration (within or across states) was associated with a 23.2 per 100,000 reduction in infant mortality (P = .013). However, it is unclear how differences among states in poverty and unemployment rates, as well as in welfare programs other than the EITC, may have influenced these findings (Arno et al., 2009). Some research has found the size of EITC payments to
be associated with improvements in such indicators of perinatal health as mothers’ utilization of prenatal and postnatal care, mothers’ use of tobacco and alcohol during pregnancy, term birth, and birth weight (Baker, 2008; Rehkopf et al., 2014).
Because the Child Tax Credit is newer than the EITC, it has not been studied as extensively. The two credits share several features, however, so the benefits for families may be similar as well. Like the EITC, the Child Tax Credit alleviates poverty for working families by supplementing wages and incentivizing work (Marr et al., 2015). In terms of child outcomes, income support from the Child Tax Credit is associated with better academic achievement for elementary and middle-school students (Chetty et al., 2011; Dahl and Lochner, 2012; Duncan et al., 2011).
Temporary Assistance for Needy Families (TANF)
TANF is an income support program created to help families achieve self-sufficiency. The program provides block grants to states to be used for an assortment of services, such as income support, child care, education, job training, and transportation assistance, with services and eligibility varying by state (Center on Budget and Policy Priorities, 2015b). Additionally, states are required to include work requirements for participants, and assistance is reduced or stopped if an individual does not work. In general, TANF recipients are less educated and poorer with more mental and physical health problems relative to low-income nonrecipients, and those with larger families are impacted more than those with small families (Hildebrandt and Stevens, 2009; Muenning et al., 2015)
When TANF was created, the economy was strong, and during the first year of the program, 73 percent of funds went to cash assistance (Hahn et al., 2012). Over time, cash assistance has decreased, and states have used the block grants for other purposes. Today, they spend approximately 25 percent of TANF funds on basic assistance; 25 percent on child care and connecting families to work; and about one-third on other types of services, such as child welfare, emergency assistance, early education, teen pregnancy prevention, and two-parent family formation and marriage support (Schott et al., 2015).
Since TANF was initiated, few evaluations of the program have been conducted, and only a few studies have used national or recent data (Acs and Loprest, 2007; Bloom et al., 2011; Hildebrandt and Stevens, 2009). States are not required to report whom they serve with TANF funds or what outcomes are achieved. This lack of accountability and transparency means that little is known about TANF’s effectiveness. It has been found in analyses of studies that included randomized controlled trials that TANF has saved money for both individuals and government (Muennig et al.,
2015) and overall has increased employment and earnings among participants (Ziliak, 2015). However, there is currently no evidence that giving states broad flexibility in use of the funds has improved outcomes for poor families (Schott et al., 2015).
Health
It has been found that women with relatively smaller families who are able to work have better health and longevity outcomes under TANF, while those with disabilities or family obligations that prevent them from working are better off under Aid to Families with Dependent Children (AFDC), and in fact many of these women have enrolled in the Supplemental Security Income Program instead of TANF (Muenning et al., 2015). Over the average TANF recipient’s working life, AFDC would cost about $28,000 more than TANF, but it would increase life by an additional .44 year (Muenning et al., 2015).
Work Participation
TANF’s work incentives allow participants to work and receive assistance. The work participation rate is the primary measure of state performance for TANF. Hence, states can have an incentive not to help those who may be difficult to employ since they often need extra assistance to find work and stay employed (Hahn et al., 2012). Little evidence indicates that TANF helps participants obtain better jobs than they could have found on their own, and the jobs they find through TANF often do not help them move on to better jobs thereafter (Lower-Basch, 2013). There has been some evaluation of models aimed at helping those who are difficult to employ. It has been found that state approaches to providing such service vary. Random assignment studies have found some positive effects from employment- and treatment-focused strategies. PRIDE in Philadelphia, for example, increased employment, with impacts that lasted several years. At the end of the program, however, most participants did not have jobs, and 80 percent still were receiving cash assistance; 2 years later, only 23 percent of participants had a job (Bloom et al., 2011). Overall, employment-focused interventions have had weak longer-term employment effects, while treatment-focused interventions have increased service use but do not have strong evidence for increasing employment (Bloom et al., 2011).
Education and Future Earnings
Encouraging TANF recipients’ participation in and completion of additional education can help improve their families’ economic position. Many
states provide some basic education classes, vocational training, and postsecondary education, which may be supplemented by other supports, such as child care and tuition assistance. However, states also encourage TANF recipients to work at the same time.
Studies evaluating TANF’s education initiatives have found mixed results (Hamilton and Scrivener, 2012). Using random assignment research designs, one evaluation found an increase in enrollment in education and training, especially among single parents (Hamilton and Scrivener, 2012). Even when enrollment has increased, however, the challenge has been increasing the percentage of participants who complete the education or training. Studies suggest that the following are beneficial: financial incentives to encourage attendance, academic progress, acquisition of marketable skills, community college exposure, job search aids, and student support assistance (Hamilton and Scrivener, 2012). TANF recipients also often face challenges to pursuing postsecondary education, particularly since many recipients do not have a GED or high school diploma (Hamilton and Scrivener, 2012).
Some argue that expanding TANF’s educational support may make the program less effective at helping recipients become employed (Greenberg et al., 2009). In an analysis of results from 28 cost-benefit studies that used random assignment evaluation, programs for GED completion and basic education that recipients are required to take did not appear to increase income (Greenberg et al., 2009). Unpaid work experience programs that are mandatory after a period of unsuccessful job searching have shown limited benefits (Greenberg et al., 2009).
Nutrition Assistance Programs
Many households today are food insecure. In 2014, an estimated 14 percent of households were food insecure at some point during the past year (Coleman-Jensen et al., 2015); the proportion was 19.2 percent among households with children under age 18. Nutrition assistance programs reach millions of low-income families in the United States each year. Major programs are the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), the Supplemental Nutrition Assistance Program (SNAP), and the National School Breakfast and National School Lunch Programs.
Special Supplemental Nutrition Program for Women, Infants, and Children (WIC)
WIC helps parents obtain knowledge and adopt practices that promote their own and their young children’s health by providing nutrition educa-
tion and vouchers for the purchase of healthy foods, breastfeeding support, and health and social service referrals. The program reaches millions of low-income pregnant, postpartum, and breastfeeding women and their children under age 5 each year (U.S. Department of Agriculture, 2016d).
WIC nutrition education is provided in a manner that is easy for participants to understand and that acknowledges the real-world interactions among nutritional needs, living circumstances, and cultural preferences. Mothers meet with WIC staff either individually or in groups to learn about the role of nutrition and physical activity in health, as well as to discuss nutrition-related practices (e.g., how to read nutrition labels and prepare healthy meals) (Carlson and Neuberger, 2015). Traditionally, nutrition education has taken place in person at WIC offices, but online education is available in many jurisdictions. Parents may use WIC vouchers to purchase infant formula and baby food as well as fruits and vegetables, whole grains, and other healthy foods. For breastfeeding mothers, counseling and educational materials, as well as peer support, are provided. To promote breastfeeding, breastfeeding mothers are eligible for WIC benefits for a longer period relative to nonbreastfeeding mothers, and those who breastfeed exclusively have a broader selection of foods from which to choose for voucher purchases. Referral services may include child immunizations and health and dental care, as well as counseling for women who smoke and abuse alcohol (Carlson and Neuberger, 2015).
Since WIC was initiated about 40 years ago, abundant research has shown evidence of its effectiveness. WIC participation during pregnancy is consistently associated with longer gestations and higher birth weights, with effects tending to be greatest among children born to disadvantaged mothers. Other outcomes include improved child nutrition (e.g., increased vitamin and mineral intake, reduced consumption of fat and added sugars), better infant feeding practices, and greater receipt of preventive and curative care (Carlson and Neuberger, 2015; Fox et al., 2004). Evidence also indicates that updates to WIC-approved foods in 2007 to bring them more in line with the latest nutrition science, made in response to recommendations in the Institute of Medicine (2006) report WIC Food Packages: Time for a Change enhanced the impact of WIC on the purchase and consumption of healthy foods among families participating in the program (Carlson and Neuberger, 2015). These changes included, among others, adding whole grain and soy products; reducing milk, cheese, and juice allowances; and giving states and other jurisdictions more flexibility to accommodate food preferences of cultural groups.
Despite efforts to promote breastfeeding, mothers participating in WIC have been found to be less likely to breastfeed than those not participating. It is unclear whether this differential is related to the availability of formula through WIC or other factors. Also in response to the 2006 Institute of
Medicine report, the U.S. Department of Agriculture took steps to encourage breastfeeding among mothers participating in WIC, such as no longer routinely providing them with formula for the first month after birth and providing a limited amount of formula in subsequent months to mothers of partially breastfeeding infants. Whether these changes have had an impact on breastfeeding rates among WIC participants is thus far unknown (Carlson and Neuberger, 2015).
Research on the nonhealth benefits of WIC is limited. One recent study that analyzed data from two nationally representative longitudinal surveys showed that children whose mothers participated in WIC while pregnant performed better than those of mothers not participating on measures of cognitive skills at age 2. This finding persisted into children’s early school years based on reading assessment (Jackson, 2015).
An evaluation of the Early Developmental Screening and Intervention (EDSI) initiative among WIC participants in California illustrates how WIC can support parents’ interactions with health care professionals. The initiative used a health education class to teach parents about child development and how to talk to their child’s health care professional(s) about the child’s development. Before the class, 42 percent of parents reported by survey that they had concerns about their child’s development, learning, or behavior, and only 26 percent of them had been asked about these concerns at their child’s last health care visit (Early Developmental Screening and Intervention Initiative, 2011). The evaluation found that the parent education class was associated with increases in parents’ preparation before health care meetings, with about one-third of these parents reporting that they used material they had learned in class. However, there was no change in parents’ actions during their child’s health care visits or their attitudes while talking to their child’s health care professional based on the survey findings (Early Developmental Screening and Intervention Initiative, 2011). Another evaluation found that 30 to 40 percent of parents participating in a Parent Activation/Developmental Surveillance pilot reported discussing their concerns about their child’s development with a developmental specialist (Early Developmental Screening and Intervention Initiative, 2011).
SNAP and National School Breakfast and National School Lunch Programs
SNAP is the largest nutrition assistance program in the United States, reaching an average of 22.5 million households each month in 2015 (U.S. Department of Agriculture, 2016c). Many households receiving SNAP (76% in 2014) include a child or an elderly or disabled individual (Gray and Kochhar, 2015). By providing assistance for the purchase of food, SNAP reduces poverty among disadvantaged populations, especially for
two-parent families (Center on Budget and Policy Priorities, 2015a; Tiehen et al., 2013). A number of studies have found that SNAP reduces food insecurity, while findings on improvements in diet quality have been mixed (Andreyeva et al., 2015; Gregory et al., 2013; Hartline-Grafton, 2013). In analyses of longitudinal data, SNAP participation has been found to decrease the probability of being food insecure by approximately 30 percent and the likelihood of being very food insecure by 20 percent (Ratcliffe et al., 2011) in both urban and rural areas (Mabli, 2014). Other longitudinal analyses found that SNAP participation increased preschool children’s intake of iron, zinc, niacin, thiamin, and vitamin A (Rose et al., 1998), while another showed that young children participating in SNAP and/or WIC had lower rates of nutritional deficit relative to nonparticipants (Lee and Mackey-Bilever, 2007). However, other evidence shows that while SNAP alleviates food insecurity, participants appear to be no more likely than income-eligible nonparticipants to be meeting dietary guidelines. In a systematic review of peer-reviewed studies, diet quality among children and adults was similar for SNAP and low-income nonparticipants and of lower quality than for higher-income individuals (Andreyeva et al., 2015).
The National School Breakfast and National School Lunch Programs provide nutritionally balanced, low-cost or free breakfasts and lunches to millions of children in public and nonprofit private schools and residential child care institutions each day (U.S. Department of Agriculture, 2016a, 2016b). The evidence on the effects of these and other school-based nutrition programs on child nutrition outcomes is limited (Gundersen et al., 2012). Using National Health and Nutrition Examination Survey data for 2001-2004, Gundersen and colleagues (2012) estimate that the National School Lunch Program reduced the rate of poor health among children by at least 29 percent, the rate of obesity by at least 17 percent, and food insecurity by at least 3.8 percent.
Health Care
As reviewed in Chapter 2 and above, various elements of the health care system have the potential to affect parents positively in promoting the health of their children. Health care providers have multiple contacts with parents through the care of both children and the parents themselves.
Since the passage of the ACA in 2010, the number of adults without health insurance is estimated to have fallen by 16.4 million (U.S. Department of Health and Human Services, 2015a). This increase in insurance coverage has expanded access to a number of services for families, such as maternity care and pediatric services, preventive services, and screening and treatment for mental health disorders.
Relative to insured children, uninsured children are more likely to have
problems with access to health care and unmet health care needs. They are less likely to receive preventive care (well-child care, immunizations, basic dental care) and almost 27 percent less likely to have had a routine checkup in the past year (Alker and Kenney, 2014; White House, 2015). Medicaid and the Children’s Health Insurance Program (CHIP) play an important role in child coverage, currently providing coverage to more than one in three children (Burwell, 2016). Evidence indicates that health insurance has improved access to care for children, and utilization of primary and preventive care appears to increase after CHIP enrollment (American Academy of Pediatrics, 2014; McMorrow et al., 2014). Evaluations within and across states generally have found that enrollees report improvements in having a usual source of care, in visiting physicians or dentists, and in having fewer unmet health needs after enrollment (American Academy of Pediatrics, 2014; Damiano et al., 2003; Fox et al., 2003; Selden and Hudson, 2006; Szilagyi et al., 2004). Moreover, pre-post survey research with parents suggests that racial/ethnic disparities in health care access and utilization detected before enrollment are eliminated or greatly reduced after enrollment (American Academy of Pediatrics, 2014; Shone et al., 2005). In a cross-sectional analysis of data from the Health Reform Monitoring Survey, compared with parents with employer-sponsored insurance, parents whose children were covered under Medicaid or CHIP reported less difficulty paying children’s medical bills (9.7% versus 19%) and paying less out of pocket on health care (McMorrow et al., 2014).
McMorrow and colleagues (2014) found that 40 percent of children with Medicaid or CHIP had a parent who obtained information on all recommended anticipatory guidance topics during well-child visits (how to keep a child from getting injured, how much or what kind of food a child should eat and how much exercise a child should get, how smoking indoors is bad for a child’s health, how a child should behave and get along with parents and others), versus 26 percent of those with insurance through their parent’s employer (McMorrow et al. 2014). However, some research has found that children with public coverage have more difficulty accessing specialist care, family-centered care, and after-hours care (Bethell et al., 2011; Kenney and Coyer, 2012; McMorrow et al., 2014).
Housing Programs
Housing-related expenses (shelter, utilities, furniture) account for families’ largest share of expenditures on children across income groups, representing 30-33 percent of total expenditures on a child in two-child, husband-wife families in 2013 (Lino, 2014). Balancing housing-related expenses with expenses for other necessities, such as nutritious foods and quality child care, can be especially difficult for low-income families.
The Housing Choice Voucher Program (HCVP) (often referred to as Section 8) helps more than 5 million people in low-income families access affordable rental housing that meets health and safety standards (Center on Budget and Policy Priorities, 2015c). Studies show potential benefits of participation in HCVP, including improved nutrition due to greater food security, increased household stability after the first year, and reductions in measures of concentrated poverty and the incidence of homelessness (Carlson et al., 2012; Lindberg et al., 2010; Wood et al., 2008). A study of 8,731 families in six locations where housing vouchers were randomly assigned to eligible participants found that over a period of about 5 years the vouchers reduced the incidence of homelessness and living with relatives: 45 percent of nonrecipients versus 9 percent of recipients spent time without a place of their own in the 4th year of the study) (Wood et al., 2008). In a review of published research on neighborhood-level housing interventions, Lindberg and colleagues (2010) found that voucher holders were less likely than nonvoucher holders to experience malnutrition due to food insecurity, poverty, and overcrowding.
Another scientifically supported housing initiative—housing rehabilitation loan and grant programs—provides financial assistance to enable low-income homeowners to repair, improve, modernize, or remove health and safety hazards from their dwellings (U.S. Department of Housing and
Urban Development, 2015). Low-interest loans and grants are offered to homeowners at the federal and state levels through local lenders based on income level and rural versus urban residence. Evidence from systematic reviews and randomized controlled research suggests that housing improvements, especially those aimed at increasing household warmth, may positively impact physical and mental health and respiratory outcomes, as well as absences from school for children and from work for adults (Gibson et al., 2011; Howden-Chapman et al., 2007; Thomson et al., 2013).
PARENTAL AND FAMILY LEAVE POLICIES
The United States is the only advanced industrialized nation that does not mandate paid maternity leave and one of only a few industrialized countries that do not require paid leave for children’s health needs by national law. Of the 189 countries included in Heymann and McNeill’s (2013) examination of the World Policy Analysis Centre Adult Labour Database, nearly all offer paid leave for new mothers, although less than one-half provide paid leave to new fathers. Moreover, 48 countries have policies that provide paid leave to parents when their child is ill. Just over half of high-income countries and one-quarter of middle-income countries have policies supporting paid leave for parents for children’s health needs (Heymann and Earle, 2010; World Adult Labour, 2015). Current state and federal leave policies regarding parental and family medical leave in the United States do not cover all parents and employers; among those who are covered, the relevant policies do not cover all their needs (Schuster et al., 2011). This section characterizes the needs of new parents and the health care needs of children; existing employer, federal, and state support for families with children; and the impact of such programs and legislation on children and families.
Needs of New Parents and Young Children’s Health Care Needs
Newborns and infants require substantial, focused, and responsive care. Parents of newborns need time to bond with their child and adjust to the demands of caring for an infant while also overseeing their child’s healthy development. In addition, mothers need time to rest and recover from pregnancy and childbirth. Mothers who are breastfeeding also need to be available for the needs of their newborns.
All children, even those who are healthy, have preventive and acute health care needs (Schuster et al., 2011). In addition, about 20 percent of children ages 0-17 in the United States are considered children with special health care needs, defined as children “who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and
who also require health and related services of a type or amount beyond that required by children generally” (Child and Adolescent Health Measurment Initiative, 2012; McPherson et al., 1998, p. 138). This category may include children with such conditions as ADHD, asthma, autism, cancer, cerebral palsy, cystic fibrosis, depression, and diabetes (Newacheck and Taylor, 1998).
Children’s health care needs can be roughly divided into three categories: preventive care, intermittent acute care, and ongoing chronic care. All children are expected to receive a substantial amount of routine preventive care, including immunizations, most of which require multiple doses at multiple visits; developmental surveillance, which detects delays in speech and language development, gross and fine motor skills, and behavioral, social, and emotional growth; screening for early or hidden illness; anticipatory guidance; and dental care. At present, the American Academy of Pediatrics and Bright Futures jointly recommend a minimum of seven visits in a child’s first year and seven more in the following 3 years, followed by annual visits through age 21 (American Academy of Pediatrics, 2008).
Nearly all children will experience one or more episodes of illness serious enough to require a visit to the emergency room, hospitalization, or care at home. Three in four children under age 18 have at least one office visit in a given year, with most averaging about four visits per year, exceeding the recommended preventive visit schedule (Schuster et al., 2011). According to a 2008 study on pediatric injuries across 14 states, one-third of emergency department visits were for pediatric injuries (Owens et al., 2008). In 2014, 23 percent of children under age 6 had visited an emergency department one or more times in the past year (National Center for Health Statistics, 2015). In addition to these acute health care issues, children experience minor illnesses that may prevent them from attending day care or school, which requires the presence of an adult in the home. Nearly two-thirds of elementary school-age children miss some school each year because of illness or injury, and nearly 11 percent of these children miss more than 1 week (Bloom et al., 2013).
Children with special health care needs generally require ongoing care that may involve frequent monitoring, interventions for preventing and managing illness complications, and acute care for severe episodes of illness (see also Chapter 5). At home, parents of children with serious or complex illnesses may be required to provide treatment and care (e.g., respiratory treatments, feeding tube care, intravenous nutrition, physical and occupational therapy, developmental interventions) in addition to cleaning and maintaining devices, ordering supplies, obtaining technical support for machines, and training other caregivers (Schuster et al., 2011). Children with serious and complex illnesses account for a vastly
disproportionate number of hospital days, health care encounters, and school absences.
Because children are unable to care for themselves, their parents are expected to provide an array of health care services that are integral to the current health care system for children, including, but not limited to, providing care at home, scheduling and attending outpatient visits, and supervision during emergency ward visits and hospitalizations (Schuster et al., 2011). Parents are expected to be present whether the care is preventive, acute, or chronic. Health care providers and public health officials recommend that children experiencing acute illnesses stay home from school in addition to visiting a clinician as needed. Otherwise, their illnesses can worsen or spread to others, health care costs can increase, and small problems can become serious threats (Schuster and Chung, 2014).
Types of Support for Employed Parents
Many employed parents who must take time away from work to care for a newborn or a sick child lose wages for hours not worked. Many even risk losing their job. Employees in the United States rely on various types of support to meet the health needs of their children, including a combination of employer benefits (if offered) and federal, state, and local leave laws and programs.
Employers—Parental Leave
Policies on offering parents of newborns time off to care for their child vary by employer; some employers provide the option of taking time off from work, while others do not. Moreover, the absence of a federal-level paid parental leave policy in the United States leaves many workers in a situation of combining a number of employee-provided benefits that may include sick leave, holiday and vacation leave, disability insurance, and paid or unpaid family leave in order to take time away from work to care for a newborn.
Employers—Family Medical Leave
The patchwork of formal and informal support provided by employers to parents includes sick days; flexible paid time off that combines vacation, sick time, and family leave; telecommuting; and programs that allow employees to donate or share unused paid leave. Parents who rely on sick days to care for their children without explicit employer approval may place themselves at risk for termination. Some supervisors may informally allow parents to leave work for hours or days to care for their child (Schuster et
al., 2011). Some employers offer employee assistance or work-life programs that can help families use employee benefits and access public and private resources more effectively. According to data from the 2010 National Paid Sick Days study, more than 60 percent of all workers reported that their employer provided them with paid sick leave, which could include a combination of sick leave, vacation, and other reasons. Less than one-half reported that they received paid sick leave that they could use for sick family members (Schuster et al., 2011; Smith and Kim, 2010).
Federal and State Programs and Legislation
The Pregnancy Discrimination Act of 1978 requires that employers provide leave to women with medical conditions that are linked to pregnancy and childbirth, just as they would to any other employee with a medical condition or temporary disability, such as a heart attack or broken leg. Although the act does not require employers to provide paid leave, they must provide the same leave (paid or unpaid) or disability benefits for conditions related to pregnancy that they provide for other disabilities (U.S. Equal Employment Opportunity Commission, 2016).
Five states offer Temporary Disability Insurance (TDI) programs, which typically provide up to one-half of an employee’s wage for up to 52 weeks of temporary disability; this includes disability or conditions related to pregnancy (Lovell and Rahmanou, 2000). These programs are funded through employee contributions or a combination of employer and employee contributions. Women with newborn children often take 6-10 weeks of temporary disability leave for pregnancy, and those requiring longer leave may take up to the maximum allowable by their state’s law. As this program is intended to provide wages for leave related to disabilities or medical conditions associated with pregnancy and childbirth, fathers and adopted parents are not eligible for TDI (Hartmann et al., 2013).
With respect to family medical leave, while the federal government does not mandate paid leave, it does guarantee unpaid leave to some workers. Under the Family and Medical Leave Act of 1993 (FMLA), employees may be eligible for up to 12 weeks a year of unpaid leave with job protection for the following circumstances: serious health condition; birth of a child or to care for the employee’s newly born, adopted, or foster child; or to care for an immediate family member (spouse, child, or parent) with a serious health condition. Eligibility is limited to employees who work for employers with 50 or more employees and have worked for at least 1,250 hours for the same employer in the past 12 months. Approximately one-half of employees meet these eligibility requirements, and many are unable to take unpaid leave (Han and Waldfogel, 2003; Schuster et al., 2011). Cantor and colleagues estimated that more than three-quarters of the 3.5 million
employees in need of leave in 2000 did not take it in order to avoid loss of wages. The majority of these employees would have taken leave had they received partial or additional pay (Cantor et al., 2001; Han and Waldfogel, 2003; Schuster et al., 2011).
The proposed Healthy Families Act (H.R. 932, S. 497) would require certain employers to allow employees to earn paid sick leave that could be used to meet their own medical needs or care for a child or other family member. The proposed Family and Medical Leave Insurance Act (FAMILY Act, H.R. 3712, S. 1810) would guarantee up to 12 weeks of paid family leave, which parents could use to provide care for serious health conditions faced by themselves or family members or to meet care needs associated with the birth or adoption of a child.
At the state level, California, New Jersey, and Rhode Island have established Paid Family Leave Insurance programs that provide wage replacement to employees who take leave to care for a new child or an ill family member; employees fund the leave through payroll deductions to state-wide pools. California’s program covers most part- and full-time employees at about 55 percent of their salary, limited to $1,129 weekly in 2016 (California Employment Development Department, 2016), although prior research indicates that many parents were not aware of the benefits (Schuster et al., 2008). Some states and municipalities have laws that entitle employees with access to sick leave to use their leave to care for a newborn or an ill family member. Further, Connecticut, New York City, San Francisco, and Washington, D.C., among others, require employers to offer paid sick leave to their employees. At present, more than 24 other states and municipalities are working on legislation related to paid sick leave (National Partnership for Women and Families, 2015).
Despite these developments, approximately one-half of employees in the United States are not eligible to receive paid sick leave that they are allowed to use to care for family members (Smith and Kim, 2010). Parents without sick leave risk being penalized or losing their job when they must stay home from work to care for a newborn or a sick child.
Disparities in Access
Rates of access to paid leave among employed parents tends to vary with income, and are lower among lower-income relative to higher-income families (Clemans-Cope et al., 2008; Heymann et al., 2006; Phillips, 2004). Among women employed during pregnancy, rates of access to paid leave were found to be higher for women who are married, ages 25 and over, and college graduates (Laughlin, 2011).
Impact of Family Leave on Children and Families
Parental Leave
Research suggests that access to parental leave is associated with increases in breastfeeding rates and duration, reduced risk of infant mortality, and increased likelihood of infants receiving well-baby care and vaccinations. For instance, cohort and case-control studies have shown that women who take maternity leave are more likely to breastfeed, and longer leaves are associated with an increase in both the likelihood and duration of breastfeeding; by contrast, early return to work is associated with an increased probability of early cessation of breastfeeding (Chuang et al., 2010; Guendelman et al., 2009; Hawkins et al., 2007; Staehelin et al., 2007; Visness and Kennedy, 1997). Mothers who took paid leave through California’s Paid Family Leave Program were found to breastfeed twice as long as those who did not take leave based on a cross-sectional survey and interviews (Appelbaum and Milkman, 2011). Moreover, children whose mothers take leave from work after childbirth are more likely to receive well-baby checkups and receive all of their recommended vaccinations (Berger et al., 2005; Daku et al., 2012). Analyses of international data have found that paid leave is associated with lower mortality rates for infants and young children, whereas this association is not seen for leave that is neither paid nor job protected (Heymann, 2011; Ruhm, 1998; Tanaka, 2005).
Access to parental leave can benefit maternal health as well. Longitudinal survey data show that women who take longer maternity leaves (more than 12 weeks) tend to experience fewer depressive symptoms and a reduction in severe depression. Additionally, paid leave is associated with improvement in overall mental health (Chatterji and Markowitz, 2012).
Paid leave also is associated with improved labor force attachment among women. Research suggests that women who have access to parental leave tend to utilize that leave period and stay home longer than those without access to such leave, but they are also more likely to return to work after that period of leave (Baum and Ruhm, 2013; Berger and Waldfogel, 2004; Houser and Vartanian, 2012; Rossin-Slater et al., 2013). While women with access to leave were less likely to return to work within the first 12 weeks of giving birth, analysis of data from a longitudinal survey has found that they were 69 percent more likely to return after 12 weeks than new mothers without leave (Berger and Waldfogel, 2004). Offering paid leave is associated with increases in the amount of leave that women take, with higher uptake among women who have less education, are unmarried, or are black or Hispanic, which was found to largely reduce the pre-existing disparities in the amount of leave taken (Berger and
Waldfogel, 2004). Multiple studies have also found that availability of paid leave is associated with increases in the number of hours that a woman works after returning to work, which corresponds to a small increase in wage income (Baum and Ruhm, 2013; Berger and Waldfogel, 2004; Rossin-Slater et al., 2013).
Access to paid paternity leave appears to increase the use of leave among fathers in the early weeks after childbirth and is associated with greater paternal engagement in caregiving in cross-sectional research (Milkman and Appelbaum, 2013). In a correlational analysis of data from Australia, Denmark, the United Kingdom, and the United States to examine the effects of leave policies, fathers who took paternity leave of at least 2 weeks were more likely to engage in activities with the infant during the first several months of the child’s life relative to fathers who did not take leave (Huerta et al., 2013).
Family Medical Leave
There are many benefits for children and parents when parents have the ability to take leave that allows them to access recommended preventive care for their children and to properly care for their children when they are ill. Preventive care is crucial to child health and development. For instance, immunizations protect recipients and the public against serious and potentially debilitating diseases. Short- and long-term health benefits, as well as improved educational and economic outcomes, have been linked to the early detection and treatment of diseases (Levy, 2010; Whitlock et al., 2005; Wilcken and Wiley, 2008).
Parents who have access to paid leave can keep an ill child home from daycare or school, which minimizes the chances that their illness will spread to others and maximizes the chances that they will receive timely medical care, if needed, so their illness does not worsen. A 2010 survey found that employees who are eligible for paid sick leave are less likely than employees without this benefit to report sending an ill child to school (Smith and Kim, 2010).
When children are hospitalized, whether for acute or chronic conditions, extended parental presence is crucial in many respects. For instance parents may be required to wait with their child for long periods for an opportunity to speak with the child’s health care provider(s) about the child’s current clinical status, the anticipated course of illness, and treatment plans going forward. Parents are also valuable sources of information for clinicians, particularly when multiple clinicians are engaged in the child’s diagnosis and treatment. In this setting, parents are expected to act as an additional, and sometimes essential, line of supervision and safety for their children. Additionally, parents are able to provide care and comfort
to their hospitalized child, who may be frightened and dependent on their presence to minimize anxiety. Indeed, family presence during health care procedures has been shown to decrease anxiety for the child as well as for the parents. The immediate presence of parents before and after surgery has been linked in randomized controlled and quality improvement monitoring research to faster recovery and earlier discharge (Fina et al., 1997; Kain et al., 2007; Shelton and Stepanek, 1994).
For a child to be discharged from the hospital, parents must be present to receive training and to demonstrate their understanding of care for their child upon discharge from the hospital. Moreover, without adequate time and resources for meeting the responsibilities for home care, there may be an increase in emergency room visits, hospital readmissions, and health care costs. Giving parents additional responsibilities without providing them with more time and resources for meeting those responsibilities may lead to increases in return visits to the emergency department, hospital readmissions, morbidity, mortality, and health care costs (Schuster and Chung, 2014).
Research has shown that parents, particularly parents of chronically ill children, experience an unmet need for family medical leave (Chung et al., 2007). Many parents of children with special health care needs who have been able to take leave to care for their child believe it had positive effects on the child’s physical and emotional health. However, being away from work may cause financial strain as well as job instability (Schuster et al., 2009).
SUMMARY
An overarching finding of this chapter is that several of the interventions discussed have shown a mix of positive and null findings in evaluation studies. In addition, the variability in the body of literature available for various approaches (e.g., some having been tested in one or two randomized controlled trials, and others having been tested in multiple evaluations that utilized different designs) makes it challenging to draw conclusions about the relative effectiveness of the various approaches. The following points emerged from the committee’s review of evidence-based and evidence-informed strategies for strengthening parenting capacity in the areas of universal/preventive and widely used interventions; information and communication technologies; income, nutrition assistance, health care, and housing programs; and parental and family leave policies.
Universal/Preventive Interventions
- Well-child visits reach the majority of children in the United States and support parents in meeting goals for their children’s health (e.g., receipt of vaccinations), but few evaluations of well-child care as a parenting intervention have been conducted. Some evidence suggests that enhanced anticipatory guidance, such as that provided in Healthy Steps, is associated with improved parental knowledge of child development and improved parenting practices with respect to vaccination, as well as discipline, safety practices, and reading.
- Preconception and prenatal care optimize maternal health and well-being prior to and during pregnancy. Most women in the United States receive prenatal care, making it an important opportunity for intervention. Although further research is needed, there is some evidence that providing pregnant women with information on pregnancy and early childhood as part of prenatal care increases parental knowledge of parenting practices that promote positive child development and knowledge of how to access such services as child care and medical care. Evidence also suggests that group prenatal care is associated with improved birth outcomes, initiation of breastfeeding, and parental knowledge.
- Primary care-based educational interventions have been found to be associated with improvements in parents’ breastfeeding and vaccination practices and with reductions in children’s screen time, their exposure to environmental tobacco smoke, and infants being brought to the emergency room because of crying. Health care interventions with a parenting component versus those without a parenting component have been found to be more effective in reducing children’s screen time and child overweight and obesity.
- Few studies have explored the effect of public education efforts on parenting knowledge or practices. However, mass public education campaigns targeting safe sleep and child helmet use have been followed by improvements in parental safety practices in these areas. Likewise, evidence in other areas of public health (smoking cessation, obesity prevention) indicates that broad public education efforts can increase awareness of the benefits of health-related behaviors.
- No existing studies show that teaching parenting-related skills to youth of high school age or younger in the general population (who are not pregnant or parents), as in infant simulator programs, supports later parenting capacity or use of evidence-based parenting practices. Since many adolescent parents face obstacles to continuing their education, however, potentially impacting their future em-
ployment and income, adolescent pregnancy prevention programs may strengthen future parental self-sufficiency and parenting.
Widely Used Interventions
- Many individual evaluations of home visiting programs show positive effects on parenting, such as gaining knowledge of child development, practicing contingent responsiveness, creating a safe home environment, and reading to children, among others. However, no strong pattern of effects has emerged across studies (even within the same model). For several models, moreover, the list of outcomes showing no effect is longer than the list showing impacts. Benefits for child development and school readiness and for child maltreatment have been observed for some models. Little assessment has been done in the area of family economic self-sufficiency, although some models show improvements in measures of education and training, use of public assistance, and reductions in rapid repeat pregnancies.
- In the area of two-generation ECE interventions, national longitudinal data on the impact of Head Start provide little evidence that the program’s parent components have a positive impact on the use of evidence-based parenting practices. Data on child outcomes are mixed, depending on the time of measurement and whether the data are reported by parents or teachers. It is unclear whether the observed changes in child outcomes are related to changes in parenting or to other Head Start program components. Data on Early Head Start indicate that sites using both center-based and home visiting services tended to have more positive impacts on parenting and child outcomes, perhaps indicating a need for flexibility in programming.
- Evidence from smaller-scale classroom-based and home visiting studies indicates that programs aimed at improving parents’ engagement in their children’s schooling and parents’ decision making about their children’s academic experiences, as well as aligning home and classroom learning, are associated with improvements in child reading and language skills and other outcomes.
- Multiple studies have found that intensive (as often as weekly) parent training in the home aimed at promoting parent engagement in the early home learning environment improves parenting practices, such as contingent responsiveness, verbal stimulation, and warmth, among socially disadvantaged mothers of infants and preschool-age children. Such interventions also have been found to improve child language skills and behavior problems. Less inten-
sive interventions that coach parents in dialogic reading have been found to improve child literacy and language outcomes at least in the short term.
Information and Communication Technologies
- Information and communication technologies represent an opportunity to improve the reach of evidence-based parenting information and interventions. Preliminary research shows that integration of the Internet and other technologies into parenting interventions can be effective, but it remains to be seen whether the effects of such approaches are equal to those observed for face-to-face interventions. Further studies are needed that include study populations that are more culturally and socioeconomically diverse than those included to date in studies of the use of these technologies to support parenting, that incorporate electronic tracking to monitor usage, that use formatting for mobile devices, and that examine how entertainment media socialize parents into norms of parenting.
Income, Nutrition Assistance, Health Care, and Housing Programs
- A number of federal income, nutrition assistance, health care, and housing programs support families by providing financial assistance and reducing other stressors that can interfere with parenting, as well as by supporting parents in meeting the nutritional, safety, and health care needs of their children.
- In the area of income support, nonrandomized studies show that the generosity of EITC payments is associated with increases in maternal work, improvements in maternal health-related outcomes and behaviors (including food security and receipt of prenatal and postnatal care), and better child academic and birth outcomes, as well as reductions in maternal stress. Children whose parents receive the Child Tax Credit also have been found to have better academic outcomes. Evidence currently is mixed concerning the effectiveness of TANF in improving health, employment, and education outcomes among adults.
- With regard to nutrition assistance programs, WIC participation is associated with improved birth outcomes, especially among the most disadvantaged mothers, as well as improved child and parent nutrition, infant feeding practices, and receipt of medical care. Mothers participating in WIC have been found to be less likely than nonparticipants to breastfeed. Preliminary evidence shows that children whose mothers participated in WIC while they were
- The passage of the ACA has expanded access to health care coverage to millions more Americans, including children. This expanded coverage has increased families’ access to maternity care and pediatric services, preventive services, and screening and treatment for mental health disorders. Children with health care coverage (e.g., Medicaid, CHIP) are more likely than those without coverage to receive recommended services such as well-child care and immunizations.
- Housing assistance programs help millions of parents find affordable and safe housing for themselves and their young children, resulting in improved food security and reduced poverty and homelessness.
pregnant have improved cognitive outcomes, but further research is needed to confirm this association. Similarly, adults and children who participate in SNAP have improved food security and dietary intake and reduced poverty. Findings on the effects of SNAP on dietary quality have been mixed, with some research showing no difference in this regard between SNAP participants and eligible nonparticipants. Sparse data are available on how the National School Breakfast and National School Lunch Programs impact children’s nutritional status.
Parental and Family Leave Policies
- Parental leave is associated with positive maternal and child health outcomes. Women who take maternity leave are more likely to breastfeed than those who do not take such leave, and longer leaves are associated with greater likelihood and duration of breastfeeding. In addition, children whose mothers take leave are more likely to receive well-child visits and vaccinations. Other benefits of parental leave based on correlational research include fewer depressive symptoms for women, improved labor force attachment, and increases in fathers’ use of leave in the early weeks after childbirth, as well as greater paternal engagement and caregiving. Family medical leave allows parents to better care for their children when they are sick and ensure that they receive appropriate preventive care.
REFERENCES
Acs, G., and Loprest, P. (2007). TANF Caseload Composition and Leavers Synthesis Report: Final Report. Washington, DC: Urban Institute.
Administration for Children and Families. (2015a). Home Visiting Evidence of Effectiveness: Durham Connects/Family Connects. Available: http://homvee.acf.hhs.gov/Model/1/Durham-Connects-Family-Connects/59/1 [February 2016].
Administration for Children and Families. (2015b). Home Visiting Evidence of Effectiveness: Nurse Family Partnership. Available: http://homvee.acf.hhs.gov/Model/1/Nurse-FamilyPartnership--NFP--In-Brief/14 [June 2016].
Administration for Children and Families. (2015c). Home Visiting Evidence of Effectiveness: Parents as Teachers. Available: http://homvee.acf.hhs.gov/Model/1/Parents-as-Teachers-PAT--sup---sup-/16/1 [June 2016].
Administration for Children and Families. (2015d). Notice of Proposed Rule Making on Head Start Program Performance Standards. Washington, DC: Head Start.
Administration of Children and Families. (2016). Office of Head Start. Available: http://www.acf.hhs.gov/programs/ohs [February 2016].
Agency for Healthcare Research and Quality. (2015). Group Visits Focused on Prenatal Care and Parenting Improve Birth Outcomes and Provider Efficiency. Available: https://innovations.ahrq.gov/profiles/group-visits-focused-prenatal-care-and-parenting-improvebirth-outcomes-and-provider [October 2016].
Alker, J., and Kenney, G. (2014). A First Look at How the Affordable Care Act Is Affecting Coverage Among Parents and Children. Available: http://healthaffairs.org/blog/2014/09/09/a-first-look-at-how-the-affordable-care-act-is-affecting-coverageamong-parents-and-children [March 2016].
Allen, K., and Rainie, L. (2002). Parents Online. Available: http://www.pewinternet.org/2002/11/17/parents-online [February 2016].
American Academy of Family Physicians. (2005). Policy Recommendations for Periodic Health Examinations. Available: http://www.aafp.org/exam.xml [February 2016].
American Academy of Pediatrics. (2000). Recommendations for preventive pediatric health care. Pediatrics, 105, 645-646.
American Academy of Pediatrics. (2002). Guidelines for Health Supervision III. Elk Grove Village, IL: American Academy of Pediatrics.
American Academy of Pediatrics. (2004). Using Time as the Key Factor for Evaluation and Management Visits. Elk Grove Village, IL: American Academy of Pediatrics.
American Academy of Pediatrics. (2008). Recommendations for Preventive Pediatric Health Care. Elk Grove Village, IL: American Academy of Pediatrics.
American Academy of Pediatrics. (2014). Children’s Health Insurance Program (CHIP): Accomplishments, challenges, and policy recommendations. Pediatrics, 133(3), e784-e793.
American Academy of Pediatrics and Bright Futures. (2016). Recommendations for Preventive Pediatric Health Care. Elk Grove Village, IL: American Academy of Pediatrics.
Andreyeva, T., Tripp, A.S., and Schwartz, M.B. (2015). Dietary quality of Americans by Supplemental Nutrition Assistance Program participation status. American Journal of Preventive Medicine, 49(4), 594-604.
Appelbaum, E., and Milkman, R. (2011). Leaves That Pay: Employer and Worker Experiences with Paid Family Leave in California. Available: https://cepr.net/documents/publications/paid-family-leave-1-2011.pdf [February 2016].
Aragon, N.J., Hudnut-Beumler, J., White Webb, M., Chavis, A., Dietrich, M.S., Bickman, L., and Scholer, S.J. (2013). The effect of primary care interventions on children’s media viewing habits and exposure to violence. Academic Pediatrics, 13(6), 531-539.
Arbour, M. (2015). Lessons on Home Visiting Program Implementation from the Collaborative for Improvement and Innovation Network (HV CoIIN): Promoting Wide-Scale Adoption of Evidence-Based Strategies with Continuous Quality Improvement Methodologies. Paper presented at the Committee on Supporting the Parents of Young Children Open Session, June 29, Irvine, CA.
Arno, P.S., Sohler, N., Viola, D., and Schechter, C. (2009). Bringing health and social policy together: The case of the earned income tax credit. Journal of Public Health Policy, 30(2), 198-207.
Arnold, D.H., Lonigan, C.J., Whitehurst, G.J., and Epstein, J.N. (1994). Accelerating language development through picture book reading: Replication and extension to a videotape training format. Journal of Educational Psychology, 86(2), 235-243.
Auger, A. (2015). Child Care and Community Services: Characteristics of Service Use and Effects on Parenting and the Home Environment. Ph.D. dissertation, University of California Irvine School of Education.
Aune, D., Saugstad, O.D., Henriksen, T., and Tonstad, S. (2014). Maternal body mass index and the risk of fetal death, stillbirth, and infant death: A systematic review and meta-analysis. Journal of the American Medical Association, 311(15), 1536-1546.
Avellar, S., Paulsell, D., Sama-Miller, E., and Del Grosso, P. (2012). Home Visiting Evidence of Effectiveness Review: Executive Summary. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Avellar, S., Paulsell, D., Sama-Miller, E., Del Grosso, P., Akers, L., and Kleinman, R. (2014). Home Visiting Evidence of Effectiveness Review: Executive Summary. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Avellar, S., Paulsell, D., Sama-Miller, E., Del Grosso, P., Akers, L., and Kleinman, R. (2015). Home Visiting Evidence of Effectiveness Review: Executive Summary. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Averett, S.L., and Yang, W. (2012). The Effects of EITC Payment Expansion on Maternal Smoking. Available: http://ftp.iza.org/dp6680.pdf [April 2016].
Baggett, K.M., Davis, B., Feil, E.G., Sheeber, L.L., Landry, S.H., Carta, J.J., and Leve, C. (2010). Technologies for expanding the reach of evidence-based interventions: Preliminary results for promoting social-emotional development in early childhood. Topics in Early Childhood Special Education, 29(4), 226-238.
Baker, K. (2008). Do Cash Transfer Programs Improve Infant Health?: Evidence from the 1993 Expansion of the Earned Income Tax Credit. Working Paper. Notre Dame, IN: University of Notre Dame.
Baker, C.N., Arnold, D.H., and Meagher, S. (2011). Enrollment and attendance in a parent training prevention program for conduct problems. Prevention Science, 12(2), 126-138.
Barlow, A., Mullany, B., Neault, N., Compton, S., Carter, A., Hastings, R., Billy, T., Coho-Mescal, V., Lorenzo, S., and Walkup, J.T. (2013). Effect of a paraprofessional homevisiting intervention on American Indian teen mothers’ and infants’ behavioral risks: A randomized controlled trial. American Journal of Psychiatry, 170(1), 83-93.
Barnett, W.S., and Masse, L.N. (2007). Comparative benefit-cost analysis of the Abecedarian program and its policy implications. Economics of Education Review, 26(1), 113-125.
Barr, R.G. (2012). Preventing abusive head trauma resulting from a failure of normal interaction between infants and their caregivers. Proceedings of the National Academy of Sciences, 109(Suppl. 2), 17294-17301.
Barr, R.G., Rajabali, F., Aragon, M., Colbourne, M., and Brant, R. (2015). Education about crying in normal infants is associated with a reduction in pediatric emergency room visits for crying complaints. Journal of Developmental & Behavioral Pediatrics, 36(4), 252-257.
Barth, R.P. (2009). Preventing child abuse and neglect with parent training: Evidence and opportunities. The Future of Children, 19(2), 95-118.
Baum, C.L., and Ruhm, C.J. (2013). The Effects of Paid Family Leave in California on Labor Market Outcomes. Working Paper No. 19741. Cambridge, MA: National Bureau of Economic Research.
Berger, L.M., and Waldfogel, J. (2004). Maternity leave and the employment of new mothers in the United States. Journal of Population Economics, 17(2), 331-349.
Berger, L.M., Hill, J., and Waldfogel, J. (2005). Maternity leave, early maternal employment and child health and development in the U.S. The Economic Journal, 115(501), F29-F47.
Bergman, D.A., Beck, A., and Rahm, A.K. (2009). The use of Internet-based technology to tailor well-child care encounters. Pediatrics, 124(1), 37-43.
Bethell, C.D., Kogan, M.D., Strickland, B.B., Schor, E.L., Robertson, J., and Newacheck, P.W. (2011). A national and state profile of leading health problems and health care quality for U.S. children: Key insurance disparities and across-state variations. Academic Pediatrics, 11(Suppl. 3), S22-S33.
Bierman, K.L., Welsh, J.A., Heinrichs, B.S., Nix, R.L., and Mathis, E.T. (2015). Helping Head Start parents promote their children’s kindergarten adjustment: The research-based developmentally informed parent program. Child Development, 86(6), 1877-1891.
Bigelow, K. (2014). Cellular-Phone Enhanced Home Visitation Parenting Intervention: A Randomized Trial. Paper presented at the Society for Prevention Research 22nd Annual Meeting, May 27-30, 2013, Washington, DC.
Blank, R.M. (1997). It Takes a Nation: A New Agenda for Fighting Poverty. New York: Russell Sage Foundation and Princeton, NJ: Princeton University Press.
Bloom, B., Cohen, R.A., and Freeman, G. (2013). Summary health statistics for U.S. children: National Health Interview Survey, 2012. Vital Health Statistics, 10(258).
Bloom, D., Loprest, P.J., and Zedlewski, S.R. (2011). TANF Recipients with Barriers to Employment. Washington, DC: Urban Institute.
Boles, M., Adams, A., Gredler, A., and Manhas, S. (2014). Ability of a mass media campaign to influence knowledge, attitudes, and behaviors about sugary drinks and obesity. Preventive Medicine, 67(Suppl. 1), S40-S45.
Boller, K., Strong, D.A., and Daro, D. (2010). Home visiting: Looking back and moving forward. ZERO TO THREE Journal, 30(6), 4-9.
Brazelton, T.B. (1992). Touchpoints: Your Child’s Emotional and Behavioral Development. Reading, MA: Addison-Wesley.
Breitenstein, S.M., and Gross, D. (2013). Web-based delivery of a preventive parent training intervention: A feasibility study. Journal of Child and Adolescent Psychiatric Nursing, 26(2), 149-157.
Breitenstein, S.M., Gross, D., Fogg, L., Ridge, A., Garvey, C., Julion, W., and Tucker, S. (2012). The Chicago parent program: Comparing 1-year outcomes for African American and Latino parents of young children. Research in Nursing & Health, 35(5), 475-489.
Breitenstein, S.M., Gross, D., and Christophersen, R. (2014). Digital delivery methods of parenting training interventions: A systematic review. Worldviews on Evidence-Based Nursing, 11(3), 168-176.
Breitenstein, S.M., Shane, J., Julion, W., and Gross, D. (2015). Developing the eCPP: Adapting an evidence-based parent training program for digital delivery in primary care settings. Worldviews on Evidence-Based Nursing, 12(1), 31-40.
Brooks-Gunn, J., Berlin, L.J., and Fuligni, A.S. (2000). Early childhood intervention programs: What about the family? In J.P. Shonkoff and S.J. Meisels (Eds.), Handbook of Early Childhood Intervention (2nd ed., pp. 549-588). New York: Cambridge University Press.
Brotman, L.M., Calzada, E., Huang, K.Y., Kingston, S., Dawson-McClure, S., Kamboukos, D., Rosenfelt, A., Schwab, A., and Petkova, E. (2011). Promoting effective parenting practices and preventing child behavior problems in school among ethnically diverse families from underserved, urban communities. Child Development, 82(1), 258-276.
Brown, N., Luckett, T., Davidson, P., and Di Giacomo, M. (2015). Interventions to reduce harm from smoking with families in infancy and early childhood: A systematic review. International Journal of Environmental Research and Public Health, 12(3), 3091-3119.
Burchinal, M.R., Campbell, F.A., Bryant, D.M., Wasik, B.H., and Ramey, C.T. (1997). Early intervention and mediating processes in cognitive performance of children of low-income African American families. Child Development, 68(5), 935-954.
Burwell, S.M. (2016). The Department of Health and Human Services 2015 Annual Report on the Quality of Care for Children in Medicaid and CHIP. Available: https://www.medicaid.gov/medicaid-chip-program-information/by-topics/quality-of-care/downloads/2015-childsec-rept.pdf [April 2016].
Caldera, D., Burrell, L., Rodriguez, K., Shea Crowne, S., Rohde, C., and Duggan, A. (2007). Impact of a statewide home visiting program on parenting and on child health and development. Child Abuse and Neglect, 31(8), 829-852.
California Employment Development Department. (2016). Disability Insurance (DI) and Paid Family Leave (PFL) Benefit Amounts. Available: http://www.edd.ca.gov/disability/State_Disability_Insurance_(SDI)_Benefit_Amounts.htm [April 2016].
Camilli, G., Vargas, S., Ryan, S., and Barnett, W.S. (2010). Meta-analysis of the effects of early education interventions on cognitive and social development. Teachers College Record, 112(3), 579-620.
Campbell, F.A., and Ramey, C.T. (1994). Effects of early intervention on intellectual and academic achievement: A follow-up study of children from low-income families. Child Development, 65(2), 684-698.
Canter, J., Rao, V., Patrick, P.A., Alpan, G., and Altman, R.L. (2015). The impact of a hospital-based educational video on maternal perceptions and planned practices of infant safe sleep. Journal for Specialists in Pediatric Nursing, 20(3), 187-192.
Cantor, D., Waldfogel, J., Kerwin, J., Wright, M.M., Levin, K., Rauch, J., Hagerty, T., and Kudela, M.S. (2001). Balancing the Needs of Families and Employers. The Family and Medical Leave Surveys, 2000 Update: A Report. Washington, DC: U.S. Department of Labor.
Carlson, S., and Neuberger, Z. (2015). WIC Works: Addressing the Nutrition and Health Needs of Low-Income Families for 40 Years. Available: http://www.cbpp.org/research/food-assistance/wic-works-addressing-the-nutrition-and-health-needs-of-low-incomefamilies [October 2016].
Carlson, D., Haveman, R., Kaplan, T., and Wolfe, B. (2012). Long-term effects of public low-income housing vouchers on neighborhood quality and household composition. Journal of Housing Economics, 21(2), 101-120.
Carpenter, D. M., Geryk, L.L., Chen, A.T., Nagler, R.H., Dieckmann, N.F., and Han, P.K. (2015). Conflicting health information: A critical research need. Health Expectations [E-pub ahead of print].
Carta, J.J., Lefever, J.B., Bigelow, K., Borkowski, J., and Warren, S.F. (2013). Randomized trial of a cellular phone-enhanced home visitation parenting intervention. Pediatrics, 132(Suppl. 2), S167-S173.
Catling, C.J., Medley, N., Foureur, M., Ryan, C., Leap, N., Teate, A., and Homer, C.S. (2015). Group versus conventional antenatal care for women. Cochrane Database of Systematic Reviews, 2.
Caughy, M.O., Miller, T.L., Genevro, J.L., Huang, K.-Y., and Nautiyal, C. (2003). The effects of healthy steps on discipline strategies of parents of young children. Journal of Applied Developmental Psychology, 24(5), 517-534.
Caughy, M.O., Huang, K.-Y., Miller, T., and Genevro, J.L. (2004). The effects of the healthy steps for young children program: Results from observations of parenting and child development. Early Childhood Research Quarterly, 19(4), 611-630.
Cebi, M., and Woodbury, S.A. (2009). Health Insurance Tax Credits and Health Insurance Coverage of Low-Earning Single Mothers. Available: http://www.upjohninstitute.org/publications/wp/09-158.pdf [April 2016].
Cefai, J., Smith, D., and Pushak, R.E. (2010). Parenting wisely: Parent training via CD-ROM with an Australian sample. Child and Family Behavior Therapy, 32(1), 17-33.
Center on Budget and Policy Priorities. (2015a). Chart Book: SNAP Helps Struggling Families Put Food on the Table. Washington, DC: Center on Budget and Policy Priorities.
Center on Budget and Policy Priorities. (2015b). Policy Basics: An Introduction to TANF. Washington, DC: Center on Budget and Policy Priorities.
Center on Budget and Policy Priorities. (2015c). Policy Basics: The Housing Choice Voucher Program. Washington, DC: Center on Budget and Policy Priorities.
Center on Budget and Policy Priorities. (2016). Chart Book: The Earned Income Tax Credit and Child Tax Credit. Washington, DC: Center on Budget and Policy Priorities.
Centers for Disease Control and Prevention. (2016). Essentials for Parenting Toddlers and Preschoolers. Available: http://www.cdc.gov/ncbddd/childdevelopment/index.html [October 2016].
Chacko, A., Wymbs, B.T., Wymbs, F.A., Pelham, W.E., Swanger-Gagne, M.S., Girio, E., Pirvics, L., Herbst, L., Guzzo, J., Phillips, C., and O’Connor, B. (2009). Enhancing traditional behavioral parent training for single mothers of children with ADHD. Journal of Clinical Child & Adolescent Psychology, 38(2), 206-218.
Chan, S.S.C., Lam, T.H., Salili, F., Leung, G.M., Wong, D.C.N., Botelho, R.J., Lo, S.L., and Lau, Y.L. (2005). A randomized controlled trial of an individualized motivational intervention on smoking cessation for parents of sick children: A pilot study. Applied Nursing Research, 18(3), 178-181.
Chang, S.M., Grantham-McGregor, S.M., Powell, C.A., Vera-Hernández, M., Lopez-Boo, F., Baker-Henningham, H., and Walker, S.P. (2015). Integrating a parenting intervention with routine primary health care: A cluster randomized trial. Pediatrics, 136(2), 272-280.
Chase-Lansdale, P.L., and Brooks-Gunn, J. (2014). Two-generation programs in the twenty-first century. The Future of Children, 24(1), 13-39.
Chatterji, P., and Markowitz, S. (2012). Family leave after childbirth and the mental health of new mothers. The Journal of Mental Health Policy and Economics, 15(2), 61-76.
Chetty, R., Friedman, J.N., and Rockoff, J. (2011). New evidence on the long-term impacts of tax credits. Proceedings. Annual Conference on Taxation and Minutes of the Annual Meeting of the National Tax Association, 104,116-124.
Child and Adolescent Health Measurement Initiative. (2012). Who Are Children with Special Health Care Needs (CSHCN). Data Resource Center, supported by Cooperative Agreement 1-U59-MC06980-01 from the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA), Maternal and Child Health Bureau (MCHB). Available: http://www.childhealthdata.org [August 2016].
Child Trends Databank. (2014). Child Trends Databank: Well-Child Visits. Bethesda, MD: Child Trends.
Child Trends Databank. (2015). Mothers Who Smoke while Pregnant: Indicators on Children and Youth. Bethesda, MD: Child Trends.
Christakis, D.A., Zimmerman, F.J., Rivara, F.P., and Ebel, B. (2006). Improving pediatric prevention via the Internet: A randomized, controlled trial. Pediatrics, 118(3), 1157-1166.
Chuang, C.-H., Chang, P.-J., Chen, Y.-C., Hsieh, W.-S., Hurng, B.-S., Lin, S.-J., and Chen, P.C. (2010). Maternal return to work and breastfeeding: A population-based cohort study. International Journal of Nursing Studies, 47(4), 461-474.
Chung, P.J., Garfield, C.F., Elliott, M.N., Carey, C., Eriksson, C., and Schuster, M.A. (2007). Need for and use of family leave among parents of children with special health care needs. Pediatrics, 119(5), 1047-1055.
Clemans-Cope, L., Perry, C.D., Kenney, G.M., Pelletier, J.E., and Pantell, M.S. (2008). Access to and use of paid sick leave among low-income families with children. Pediatrics, 122(2), 480-486.
Coatsworth, J.D., Duncan, L.G., Pantin, H., and Szapocznik, J. (2006). Retaining ethnic minority parents in a preventive intervention: The quality of group process. Journal of Primary Prevention, 27(4), 367-389.
Coker, T.R., Chacon, S., Elliott, M.N., Bruno, Y., Chavis, T., Biely, C., Bethell, C.D., Contreras, S., Mimila, N.A., Mercado, J., and Chung, P.J. (2016). A parent coach model for well-child care among low-income children: A randomized controlled trial. Pediatrics, 137(3), 1-10.
Coleman-Jensen, A., Gregory, C., and Rabbitt, M. (2015). Food Security Status of U.S. Households in 2014. Available: http://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/key-statistics-graphics.aspx#children [June 2016].
Cowan, C.P., Cowan, P.A., and Barry, J. (2011). Couples’ groups for parents of preschoolers: Ten-year outcomes of a randomized trial. Journal of the Division of Family Psychology of the American Psychological Association (Division 43), 25(2), 240-250.
Cowan, C.P., and Cowan, P.A. (2000). When Partners Become Parents: The Big Life Change for Couples. Mahwah, NJ: Lawrence Erlbaum Associates.
Cowan, P.A., and Cowan, C.P. (2014). Controversies in couple relationship education (CRE): Overlooked evidence and implications for research and policy. Psychology, Public Policy, and Law, 20(4), 361-383.
Cowan, P.A., Cowan, C.P., and Knox, V. (2010). Marriage and fatherhood programs. The Future of Children, 20(2), 205-230.
Cowart-Osborne, M., Jackson, M., Chege, E., Baker, E., Whitaker, D., and Self-Brown, S. (2014). Technology-based innovations in child maltreatment prevention programs: Examples from SafeCare®. Social Sciences, 3(3), 427-440.
Crawford, M., Church, J., and Akin, B. (2016). CPI Detailed Report: Data for March 2016. Available: http://www.bls.gov/cpi/cpid1603.pdf [May 2016].
Dahl, G.B., and Lochner, L. (2012). The impact of family income on child achievement: Evidence from the Earned Income Tax Credit. The American Economic Review, 102(5), 1927-1956.
Daku, M., Raub, A., and Heymann, J. (2012). Maternal leave policies and vaccination coverage: A global analysis. Social Science and Medicine, 74(2), 120-124.
Damiano, P.C., Willard, J.C., Momany, E.T., and Chowdhury, J. (2003). The impact of the Iowa S-SCHIP Program on access, health status, and the family environment. Ambulatory Pediatrics, 3(5), 263-269.
Daro, D. (2006). Home Visitation: Assessing Progress, Managing Expectations. Chicago, IL: Chapin Hall Center for Children.
Daro, D. (2011). Home visitation. In E. Zigler, W. Gilliam, and S. Barnett (Eds.), The Pre-K Debates: Current Controversies and Issues (pp. 169-173). Baltimore, MD: Paul H. Brookes.
Daro, D., and Benedetti, G. (2014). Sustaining Progress in Preventing Child Maltreatment: A Transformative Challenge. Chicago, IL: Chapin Hall, University of Chicago.
Dearing, E., and Tang, S. (2010). The home learning environment and achievement during childhood. In S.L. Christenson and A.L. Reschly (Eds.), Handbook of School-Family Partnerships (pp. 131-157). New York: Routledge.
Dearing, E., Sibly, E., and Nguyen, H.N. (2015). Achievement mediators of family engagement in children’s education: A family-school-community systems model. In S.M. Sheridan and E. Moorman Kim (Eds.), Processes and Pathways of Family-School Partnerships across Development (vol. 2, pp. 17-39). Basel, Switzerland: Springer International.
De-Regil, L.M., Fernández-Gaxiola, A.C., Dowswell, T., and Peña-Rosas, J.P. (2010). Effects and safety of periconceptional folate supplementation for preventing birth defects. Cochrane Database of Systematic Reviews, 10.
Dodge, K.A., Goodman, W.B., Murphy, R.A., O’Donnell, K., and Sato, J. (2013). Randomized controlled trial of universal postnatal nurse home visiting: Impact on emergency care. Pediatrics, 132(Suppl. 2), S140-S146.
Duggan, M., Lenhart, A., Lampe, C., and Ellison, N.B. (2015). Seeking Parenting Advice on Social Media. Available: http://www.pewinternet.org/2015/07/16/seeking-parenting-advice-on-social-media [October 2016].
Duncan, G.J., and Magnuson, K. (2013). The long reach of early childhood poverty. In W.-J. Yeung and M.T. Yap (Eds.), Economic Stress, Human Capital, and Families in Asia (pp. 57-70). Dordrecht, Netherlands: Springer.
Duncan, G.J., Dunifon, R.E., Doran, M.B.W., and Yeung, W.J. (2001). How different are welfare and working families? And do these differences matter for children’s achievement? In G.J. Duncan and P.L. Chase-Lansdale (Eds.), For Better and for Worse: Welfare Reform and the Well-Being of Children and Families (pp. 103-131). New York: Russell Sage Foundation.
Duncan, G.J., Morris, P.A., and Rodrigues, C. (2011). Does money really matter? Estimating impacts of family income on young children’s achievement with data from random-assignment experiments. Developmental Psychology, 47(5), 1263-1279.
Dunn, R.A., Shenouda, P.E., Martin, D.R., and Schultz, A.J. (1998). Videotape increases parent knowledge about poliovirus vaccines and choices of polio vaccination schedules. Pediatrics, 102(2), e26.
Early Developmental Screening and Intervention Initiative. (2011). Roles for Women, Infants and Children (WIC) Program in Promoting Quality Developmental Care for Young Children: A Report on Lessons Learned and Options. Available: http://www.first5la.org/files/RolesforWICPrograminPromotingQuality.pdf [February 2016].
Eckenrode, J., Campa, M., Luckey, D.W., Henderson, C.R., Jr., Cole, R., Kitzman, H., Anson, E., Sidora-Arcoleo, K., Powers, J., and Olds, D. (2010). Long-term effects of prenatal and infancy nurse home visitation on the life course of youths: 19-year follow-up of a randomized trial. Archives of Pediatrics & Adolescent Medicine, 164(1), 9-15.
El Nokali, N.E., Bachman, H.J., and Votruba-Drzal, E. (2010). Parent involvement and children’s academic and social development in elementary school. Child Development, 81(3), 988-1005.
Evans, W.N., and Garthwaite, C.L. (2010). Giving Mom a Break: The Impact of Higher EITC Payments on Maternal Health. NBER Working Paper No. 16296. Cambridge, MA: National Bureau of Economic Research.
Faircloth, W.B., Schermerhorn, A.C., Mitchell, P.M., Cummings, J.S., and Cummings, E.M. (2011). Testing the long-term efficacy of a prevention program for improving marital conflict in community families. Journal of Applied Developmental Psychology, 32(4), 189-197.
Fan, X., and Chen, M. (2001). Parental involvement and students’ academic achievement: A meta-analysis. Educational Psychology Review, 13(1), 1-22.
Fantuzzo, J., McWayne, C., Perry, M.A., and Childs, S. (2004). Multiple dimensions of family involvement and their relations to behavioral and learning competencies for urban, low-income children. School Psychology Review, 33(4), 467-480.
Fantuzzo, J., Gadsden, V., Li, F., Sproul, F., McDermott, P., Hightower, D., and Minney, A. (2013). Multiple dimensions of family engagement in early childhood education: Evidence for a short form of the family involvement questionnaire. Early Childhood Research Quarterly, 28(4), 734-742.
Farber, M.L. (2009). Parent mentoring and child anticipatory guidance with Latino and African American families. Health & Social Work, 34(3), 179-189.
Feinberg, M.E., Jones, D.E., Kan, M.L., and Goslin, M.C. (2010). Effects of family foundations on parents and children: 3.5 years after baseline. Journal of the Division of Family Psychology of the American Psychological Association (Division 43), 24(5), 532-542.
File, T., and Ryan, C. (2014). Computer and Internet Use in the United States: 2013. Available: http://www.census.gov/history/pdf/2013computeruse.pdf [October 2016].
Fina, D.K., Lopas, L.J., Stagnone, J.H., and Santucci, P.R. (1997). Parent participation in the postanesthesia care unit: Fourteen years of progress at one hospital. Journal of PeriAnesthesia Nursing, 12(3), 152-162.
Finer, L.B., and Zolna, M.R. (2014). Shifts in intended and unintended pregnancies in the United States, 2001-2008. American Journal of Public Health, 104(Suppl. 1), S43-S48.
Ford, R.M., McDougall, S.J., and Evans, D. (2009). Parent-delivered compensatory education for children at risk of educational failure: Improving the academic and self-regulatory skills of a sure start preschool sample. British Journal of Psychology, 100(4), 773-797.
Fox, M.H., Moore, J., Davis, R., and Heintzelman, R. (2003). Changes in reported health status and unmet need for children enrolling in the Kansas Children’s Health Insurance Program. American Journal of Public Health, 93(4), 579-582.
Fox, M.K., Hamilton, W., and Lin, B.-H. (2004). Effects of Food Assistance and Nutrition Programs on Nutrition and Health. Food Assistance and Nutrition Research Report Number 19-3. Washington, DC: Economic Research Service, U.S. Department of Agriculture.
Friend, K., and Levy, D.T. (2002). Reductions in smoking prevalence and cigarette consumption associated with mass-media campaigns. Health Education Research, 17(1), 85-98.
Gable, S., Chang, Y., and Krull, J.L. (2007). Television watching and frequency of family meals are predictive of overweight onset and persistence in a national sample of school-aged children. Journal of the American Dietetic Association, 107(1), 53-61.
Garcia, D., Bagner, D.M., Pruden, S.M., and Nichols-Lopez, K. (2015). Language production in children with and at risk for delay: Mediating role of parenting skills. Journal of Clinical Child & Adolescent Psychology, 44(5), 814-825.
García Coll, C., Lamberty, G., Jenkins, R., McAdoo, H.P., Crnic, K., Wasik, B.H., and Garcia, H.V. (1996). An integrative model for the study of developmental competencies in minority children. Child Development, 67(5), 1891-1914.
Garvey, C., Julion, W., Fogg, L., Kratovil, A., and Gross, D. (2006). Measuring participation in a prevention trial with parents of young children. Research in Nursing & Health, 29(3), 212-222.
Gibson, M., Petticrew, M., Bambra, C., Sowden, A.J., Wright, K.E., and Whitehead, M. (2011). Housing and health inequalities: A synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health & Place, 17(1), 175-184.
Glascoe, F.P., Oberklaid, F., Dworkin, P.H., and Trimm, F. (1998). Brief approaches to educating patients and parents in primary care. Pediatrics, 101(6), E10.
Gold, K.J., and Marcus, S.M. (2008). Effect of maternal mental illness on pregnancy outcomes. Expert Review of Obstetrics & Gynecology, 3(3), 391-401.
Goodstein, M.H., Bell, T., and Krugman, S.D. (2015). Improving infant sleep safety through a comprehensive hospital-based program. Clinical Pediatrics, 54(3), 212-221.
Granger, R.C., and Cytron, R. (1999). Teenage parent programs a synthesis of the long-term effects of the new chance demonstration, Ohio’s learning, earning, and parenting program, and the teenage parent demonstration. Evaluation Review, 23(2), 107-145.
Gray, K.F., and Kochhar, S. (2015). Characteristics of Supplemental Nutrition Assistance Program Households: Fiscal Year 2014. Report No. SNAP-15-CHAR. Alexandria, VA: U.S. Department of Agriculture.
Green, M., and Palfrey, J. (2002). Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. Arlington, VA: National Center for Education in Maternal and Child Health, Georgetown University.
Greenberg, D., Deitch, V., and Hamilton, G., and Manpower Demonstration Research. (2009). Welfare-to-Work Program Benefits and Costs: A Synthesis of Research. New York: Manpower Demonstration Research Corporation.
Gregory, C., Ver Ploeg, M., Andrews, M., and Coleman-Jensen, A. (2013). Supplemental Nutrition Assistance Program (SNAP) Participation Leads to Modest Changes in Diet Quality. Economic Research Report No. 147. Washington, DC: Economic Research Service, U.S. Department of Agriculture.
Griswold, C.H., Nasso, J.T., Swider, S., Ellison, B.R., Griswold, D.L., and Brooks, M. (2013). The prenatal care at school program. The Journal of School Nursing: The Official Publication of the National Association of School Nurses, 29(3), 196-203.
Guendelman, S., Kosa, J.L., Pearl, M., Graham, S., Goodman, J., and Kharrazi, M. (2009). Juggling work and breastfeeding: Effects of maternity leave and occupational characteristics. Pediatrics, 123(1), 38-46.
Gundersen, C., Kreider, B., and Pepper, J. (2012). The impact of the National School Lunch Program on child health: A nonparametric bounds analysis. Journal of Econometrics, 166(1), 79-91.
Guttentag, C.L., Landry, S.H., Williams, J.M., Baggett, K.M., Noria, C.W., Borkowski, J.G., Swank, P.R., Farris, J.R., Crawford, A., and Lanzi, R.G. (2014). “My Baby & Me”: Effects of an early, comprehensive parenting intervention on at-risk mothers and their children. Developmental Psychology, 50(5), 1482-1496.
Hahn, H., Kassabian, D., and Zedlewski, S. (2012). TANF Work Requirements and State Strategies to Fulfill Them. Washington, DC: Urban Institute.
Halfon, N., Stevens, G.D., Larson, K., and Olson, L.M. (2011). Duration of a well-child visit: Association with content, family-centeredness, and satisfaction. Pediatrics, 128(4), 657-664.
Hamilton, G., and Scrivener, S. (2012). Increasing Employment Stability and Earnings for Low-Wage Workers: Lessons from the Employment Retention and Advancement (ERA) Project. Report 2012-19. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Han, W.-J., and Waldfogel, J. (2003). Parental leave: The impact of recent legislation on parents leave taking. Demography, 40(1), 191-200.
Hartline-Grafton, H. (2013). SNAP and Public Health: The Role of the Supplemental Nutrition Assistance Program in Improving the Health and Well-Being of Americans. Washington, DC: Food Research & Action Center.
Hartmann, H., Reichlin, L., Milli, J., Gault, B., and Hegewisch, A. (2013). Paid Parental Leave in the United States. Washington, DC: U.S. Department of Labor.
Hawkins, S.S., Griffiths, L.J., Dezateux, C., Law, C., and Millennium Cohort Study Child Health Group. (2007). The impact of maternal employment on breast-feeding duration in the UK millennium cohort study. Public Health Nutrition, 10(9), 891-896.
Health Resources and Services Administration. (2016). The Maternal, Infant, and Early Childhood Home Visiting Program: Partnering with Parents to Help Children Succeed. Washington, DC: U.S. Department of Health and Human Services,.
Heinicke, C.M., Fineman, N.R., Ponce, V.A., and Guthrie, D. (2001). Relation-based intervention with at-risk mothers: Outcome in the second year of life. Infant Mental Health Journal, 22(4), 431-462.
Heinrich, C.J. (2014). Parents’ employment and children’s well-being. The Future of Children, 24(1), 121-146.
Heinrichs, N., Bertram, H., Kuschel, A., and Hahlweg, K. (2005). Parent recruitment and retention in a universal prevention program for child behavior and emotional problems: Barriers to research and program participation. Prevention Science, 6(4), 275-286.
Henderson, A.T., and Mapp, K.L. (2002). A New Wave of Evidence: The Impact of School, Family, and Community Connections on Student Achievement. Annual Synthesis 2002. Austin, TX: National Center for Family and Community Connections with Schools.
Herbst, C.M. (2010). The labor supply effects of child care costs and wages in the presence of subsidies and the Earned Income Tax Credit. Review of Economics of the Household, 8(2), 199-230.
Herrman, J.W., Waterhouse, J.K., and Chiquoine, J. (2011). Evaluation of an infant simulator intervention for teen pregnancy prevention. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 40(3), 322-328.
Heymann, J. (2011). Creating and using new data sources to analyze the relationship between social policy and global health: The case of maternal leave. Public Health Reports, 126(Suppl. 3), 127-134.
Heymann, J., and Earle, A. (2010). Raising the Global Floor Dismantling the Myth That We Can’t Afford Good Working Conditions for Everyone. Stanford, CA: Stanford Politics and Policy.
Heymann, J., and McNeill, K. (2013). Children’s Chances: How Countries Can Move from Surviving to Thriving. Cambridge, MA: Harvard University Press.
Heymann, J., Penrose, K., and Earle, A. (2006). Meeting children’s needs: How does the United States measure up? Merrill-Palmer Quarterly, 52(2), 189-215.
Hildebrandt, E., and Stevens, P. (2009). Impoverished women with children and no welfare benefits: The urgency of researching failures of the Temporary Assistance for Needy Families Program. American Journal of Public Health, 99(5), 793-801.
Hoath, F.E., and Sanders, M.R. (2002). A feasibility study of Enhanced Group Triple P-Positive Parenting Program for parents of children with attention-deficit/hyperactivity disorder. Behaviour Change, 19(4), 191-206.
Hofstetter, A.M., Barrett, A., and Stockwell, M.S. (2015). Factors impacting influenza vaccination of urban low-income Latino children under nine years requiring two doses in the 2010-2011 season. Journal of Community Health: The Publication for Health Promotion and Disease Prevention, 40(2), 227-234.
Hornik, R.C. (Ed). (2002). Public Health Communication: Evidence for Behavior Change. New York: Lawrence Erlbaum Associates.
Hotz, V.J., and Scholtz, J.K. (2003). The Earned Income Tax Credit. In R.A. Moffitt (Ed.), Means-tested Transfer Programs in the United States (pp. 141-197). Chicago, IL: University of Chicago Press.
Houser, L., and Vartanian, T.P. (2012). Pay Matters: The Positive Economic Impacts of Paid Family Leave for Families, Businesses, and the Public. Available: http://go.nationalpartnership.org/site/DocServer/Pay_Matters_-_Positive_Economic_Impacts_of_Paid_Family_L.pdf?docID=9681 [March 2016].
Howden-Chapman, P., Matheson, A., Crane, J., Viggers, H., Cunningham, M., Blakely, T., Cunningham, C., Woodward, A., Saville-Smith, K., O’Dea, D., Kennedy, M., Baker, M., Waipara, N., Chapman, R., and Davie, G. (2007). Effect of insulating existing houses on health inequality: Cluster randomised study in the community. British Medical Journal, 334(7591), 460.
Hsueh, J., Principe Alderson, D., Lundquist, E., Michalopoulos, C., Gubits, D., Fein, D., and Knox, V. (2012). The Supporting Healthy Marriage Evaluation: Early Impacts on Low-Income Families. Report 11. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Huebner, C.E., Barlow, W.E., Tyll, L.T., Johnston, B.D., and Thompson, R.S. (2004). Expanding developmental and behavioral services for newborns in primary care: Program design, delivery, and evaluation framework. American Journal of Preventive Medicine, 26(4), 344-355.
Huerta, M.D.C., Adema, W., Baxter, J., Han, W.-J., and Lausten, M. (2013). Fathers’ Leave, Fathers’ Involvement and Child Development: Are They Related? Evidence from Four OECD Countries. OECD Social, Employment and Migration Working Paper No. 140. Paris, France: OECD.
Huston, A.C., and Bentley, A.C. (2009). Human development in societal context. Annual Review of Psychology, 61, 411-437.
Ibanez, G., de Reynal de Saint Michel, C., Denantes, M., Saurel-Cubizolles, M.-J., Ringa, V., and Magnier, A.-M. (2012). Systematic review and meta-analysis of randomized controlled trials evaluating primary care-based interventions to promote breastfeeding in low-income women. Family Practice, 29(3), 245-254.
Ickovics, J.R., Kershaw, T.S., Westdahl, C., Magriples, U., Massey, Z., Reynolds, H., and Rising, S.S. (2007). Group prenatal care and perinatal outcomes: A randomized controlled trial. Obstetrical & Gynecological Survey, 62(12), 766.
Institute of Medicine. (1995). The Best Intentions: Unintended Pregnancy and the Well-Being of Children and Families. S.S. Brown and L. Eisenberg (Eds.). Committee on Unintended Pregnancy. Washington, DC: National Academy Press.
Institute of Medicine. (2006). WIC Food Packages: Time for a Change. Committee to Review the WIC Food Packages, Food and Nutrition Board. Washington, DC: The National Academies Press.
Institute of Medicine and National Research Council. (2009). Weight Gain During Pregnancy: Reexamining the Guidelines. K.M. Rasmussen and A.L. Yaktine (Eds.). Committee to Reexamine IOM Pregnancy Weight Guidelines; Food and Nutrition Board; Board on Children, Youth, and Families. Washington, DC: The National Academies Press.
Institute for Healthcare Improvement. (2003). The Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improvement. IHI Innovation Series white paper. Boston, MA: Institute for Healthcare Improvement.
Internal Revenue Service. (2016). 2016 EITC Income Limits, Maximum Credit Amounts and Tax Law Updates. Available: https://www.irs.gov/credits-deductions/individuals/earnedincome-tax-credit/eitc-income-limits-maximum-credit-amounts-next-year [June 2016].
Irvine, A.B., Gelatt, V.A., Hammond, M., Seeley, J.R., and Irvine, A.B. (2014). A randomized study of Internet parent training accessed from community technology centers. Prevention Science, 16(4), 597-608.
Jabaley, J., Lutzker, J., Whitaker, D., and Self-Brown, S. (2011). Using iPhones™ to enhance and reduce face-to-face home safety sessions within SafeCare®: An evidence-based child maltreatment prevention program. Journal of Family Violence, 26(5), 377-385.
Jackson, C., Cheater, F.M., Harrison, W., Peacock, R., Bekker, H., West, R., and Leese, B. (2011). Randomised cluster trial to support informed parental decision-making for the MMR vaccine. BMC Public Health, 11(1), 1-11.
Jackson, G.L., Powers, B.J., Chatterjee, R., Bettger, J.P., Kemper, A.R., Hasselblad, V., Dolor, R.J., Irvine, R.J., Heidenfelder, B.L., Kendrick, A.S., Gray, R., and Williams, J.W. (2013). Improving patient care. The patient-centered medical home. A systematic review. Annals of Internal Medicine, 158(3), 169-178.
Jackson, M.I. (2015). Early childhood WIC participation, cognitive development and academic achievement. Social Science & Medicine, 126, 145-153.
Johnson, K. (2009). State-Based Home Visiting: Strengthening Programs through State Leadership. New York: National Center for Children in Poverty.
Johnston, B.D., Huebner, C.E., Anderson, M.L., Tyll, L.T., and Thompson, R.S. (2006). Healthy steps in an integrated delivery system: Child and parent outcomes at 30 months. Archives of Pediatrics & Adolescent Medicine, 160(8), 793-800.
Jones Harden, B., Chazan-Cohen, R., Raikes, H., and Vogel, C. (2012). Early Head Start home visitation: The role of implementation in bolstering program benefits. Journal of Community Psychology, 40(4), 438-455.
Kain, Z.N., Caldwell-Andrews, A.A., Mayes, L.C., Weinberg, M.E., Wang, S.M., MacLaren, J.E., and Blount, R.L. (2007). Family-centered preparation for surgery improves perioperative outcomes in children: A randomized controlled trial. Anesthesiology, 106(1), 65-74.
Kaminski, J.W., Valle, L.A., Filene, J.H., and Boyle, C.L. (2008). A meta-analytic review of components associated with parent training program effectiveness. Journal of Abnormal Child Psychology, 36(4), 567-589.
Karp, H. (2002). The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Baby Sleep Longer. New York: Bantam Books.
Karp, H., and Spencer, P. (2004). The Happiest Toddler on the Block: The New Way to Stop the Daily Battle of Wills and Raise a Secure and Well-Behaved One- to Four-Year-Old. New York: Bantam Books.
Keefe, M.R., Lobo, M.L., Froese-Fretz, A., Kotzer, A.M., Barbosa, G.A., and Dudley, W.N. (2006a). Effectiveness of an intervention for colic. Clinical Pediatrics, 45(2), 123-133.
Keefe, M.R., Kajrlsen, K.A., Lobo, M.L., Kotzer, A.M., and Dudley, W.N. (2006b). Reducing parenting stress in families with irritable infants. Nursing Research, 55(3), 198-205.
Kempe, A., Dempsey, C., and Poole, S.R. (1999). Introduction of a recorded health information line into a pediatric practice. Archives of Pediatrics & Adolescent Medicine, 153(6), 604-610.
Kennedy, T.L.M., Smith, A., Wells, A.T., and Wellman, B. (2008). Networked Families. Available: http://www.pewinternet.org/2008/10/19/networked-families [February 2016].
Kenney, G.M., and Coyer, C. (2012). National Findings on Access to Health Care and Service Use for Children Enrolled in Medicaid or CHIP. Washington, DC: Urban Institute.
Kinzer, S.L., Dungy, C.I., and Link, E.A. (2004). Healthy Steps: Resident’s perceptions. Clinical Pediatrics, 43(8), 743-748.
Kirkland, K., and Mitchell-Herzfeld, S. (2012). Evaluating the Effectiveness of Home Visiting Services in Promoting Children’s Adjustment in School: Final Report to the Pew Center on the States. Renssalaer, NY: New York State Office of Children and Family Services, Bureau of Evaluation and Research.
Kitzman, H., Olds, D.L., Henderson, C.R., Jr., Hanks, C., Cole, R., Tatelbaum, R., McConnochie, K.M., Sidora, K., Luckey, D.W., Shaver, D., Engelhardt, K., James, D., and Barnard, K. (1997). Effect of prenatal and infancy home visitation by nurses on pregnancy outcomes, childhood injuries, and repeated childbearing. A randomized controlled trial. Journal of the American Medical Association, 278(8), 644-652.
Kitzman, H.J., Cole, R.E., Anson, E.A., Olds, D.L., Knudtson, M.D., Holmberg, J.R., Hanks, C.A., Arcoleo, K.J., Luckey, D.W., and Henderson, Jr., C.R. (2010). Enduring effects of prenatal and infancy home visiting by nurses on children: Follow-up of a randomized trial among children at age 12 years. Archives of Pediatrics & Adolescent Medicine, 164(5), 412-418.
Knoche, L.L., Edwards, C.P., Sheridan, S.M., Kupzyk, K.A., Marvin, C.A., Cline, K.D., and Clarke, B.L. (2012). Getting ready: Results of a randomized trial of a relationship-focused intervention on the parent-infant relationship in rural Early Head Start. Infant Mental Health Journal, 33(5), 439-458.
Koniak-Griffin, D., Anderson, N.L.R., Verzemnieks, I., and Brecht, M.-L. (2000). A public health nursing early intervention program for adolescent mothers: Outcomes from pregnancy through 6 weeks postpartum. Nursing Research Nursing Research, 49(3), 130-138.
Koniak-Griffin, D., Anderson, N.L., Brecht, M.-L., Verzemnieks, I., Lesser, J., and Kim, S. (2002). Public health nursing care for adolescent mothers: Impact on infant health and selected maternal outcomes at 1 year postbirth. Journal of Adolescent Health, 30(1), 44-54.
Koniak-Griffin, D., Verzemnieks, I.L., Anderson, N.L., Brecht, M.-L., Lesser, J., Kim, S., and Turner-Pluta, C. (2003). Nurse visitation for adolescent mothers: Two-year infant health and maternal outcomes. Nursing Research, 52(2), 127-136.
Lancaster, C.A., Gold, K.J., Flynn, H.A., Yoo, H., Marcus, S.M., and Davis, M.M. (2010). Risk factors for depressive symptoms during pregnancy: A systematic review. American Journal of Obstetrics and Gynecology, 202(1), 5-14.
Landry, S.H., Smith, K.E., and Swank, P.R. (2006). Responsive parenting: Establishing early foundations for social, communication, and independent problem-solving skills. Developmental Psychology, 42(4), 627-642.
Landry, S.H., Smith, K.E., Swank, P.R., and Guttentag, C. (2008). A responsive parenting intervention: The optimal timing across early childhood for impacting maternal behaviors and child outcomes. Developmental Psychology, 44(5), 1335-1353.
Landry, S.H., Smith, K.E., Swank, P.R., Zucker, T., Crawford, A.D., and Solari, E.F. (2012). The effects of a responsive parenting intervention on parent-child interactions during shared book reading. Developmental Psychology, 48(4), 969-986.
Laughlin, L.L. (2011). Maternity Leave and Employment Patterns of First-Time Mothers: 1961-2008. Washington, DC: U.S. Department of Commerce, Economics and Statistics Administration, U.S. Census Bureau.
Lee, B.J., and Mackey-Bilaver, L.M. (2007). Effects of WIC and Food Stamp participation on child outcomes. Children and Youth Services Review, 19(4), 501-517.
Leon, I.G. (2009). Psychology of Reproduction: Pregnancy, Parenthood, and Parental Ties. Available: http://www.glowm.com/section_view/heading/Psychology%20of%20Reproduction:%20Pregnancy,%20Parenthood,%20and%20Parental%20Ties/item/418 [April 2016].
Levy, P.A. (2010). An overview of newborn screening. Journal of Developmental and Behavioral Pediatrics, 31(7), 622-631.
Lindberg, R.A., Shenassa, E.D., Acevedo-Garcia, D., Popkin, S.J., Villaveces, A., and Morley, R.L. (2010). Housing interventions at the neighborhood level and health: A review of the evidence. Journal of Public Health Management and Practice, 16(5), S44-S52.
Lino, M. (2014). Expenditures on Children by Families, 2013. Washington, DC: U.S. Department of Agriculture, Center for Nutrition Policy and Promotion.
Lonigan, C.J., and Whitehurst, G.J. (1998). Relative efficacy of parent and teacher involvement in a shared-reading intervention for preschool children from low-income backgrounds. Early Childhood Research Quarterly, 13(2), 263-290.
Loomans, E.M., van Dijk, A.E., Vrijkotte, T.G., van Eijsden, M., Stronks, K., Gemke, R.J., and van den Bergh, B.R. (2013). Psychosocial stress during pregnancy is related to adverse birth outcomes: Results from a large multi-ethnic community-based birth cohort. European Journal of Public Health, 23(3), 485-491.
Love, J.M., Kisker, E.E., Ross, C., Raikes, H., Constantine, J., Boller, K., Brooks-Gunn, J., Chazan-Cohen, R., Tarullo, L.B., Brady-Smith, C., Fuligni, A.S. Schocet, P.Z., Paulsell, D., and Vogel, C. (2005). The effectiveness of Early Head Start for 3-year-old children and their parents: Lessons for policy and programs. Developmental Psychology, 41(6) 885-901.
Love, S.M., Sanders, M.R., Metzler, C.W., Prinz, R.J., and Kast, E.Z. (2013). Enhancing accessibility and engagement in evidence-based parenting programs to reduce maltreatment: Conversations with vulnerable parents. Journal of Public Child Welfare, 7(1), 20-38.
Lovell, V., and Rahmanou, H. (2000). Paid Family and Medical Leave: Essential Support for Working Women and Men: Fact Sheet #A124. Washington, DC: Institute for Women’s Policy Research.
Lowell, D.I., Carter, A.S., Godoy, L., Paulicin, B., and Briggs-Gowan, M.J. (2011). A randomized controlled trial of child first: A comprehensive home-based intervention translating research into early childhood practice. Child Development, 82(1), 193-208.
Lower-Basch, E. (2013). TANF Policy Brief: Goals for TANF Reauthorization. Washington, DC: Center for Law and Social Policy.
Lu, M.C., and Halfon, N. (2003). Racial and ethnic disparities in birth outcomes: A life-course perspective. Maternal and Child Health Journal, 7(1), 13-30.
Lumeng, J.C., Rahnama, S., Appugliese, D., Kaciroti, N., and Bradley, R.H. (2006). Television exposure and overweight risk in preschoolers. Archives of Pediatrics & Adolescent Medicine, 160(4), 417-422.
Mabli, J. (2014). SNAP Participation and Urban and Rural Food Security. Washington, DC: Mathematica Policy Research.
Marr, C., and Huang, C. (2015). Strengthening the EITC for Childless Workers Would Promote Work and Reduce Poverty. Washington, DC: Center on Budget and Policy Priorities.
Marr, C., Huang, C., Sherman, A., and DeBot, B. (2015). EITC and Child Tax Credit Promote Work, Reduce Poverty, and Support Children’s Development, Research Finds. Washington, DC: Center on Budget and Policy Priorities.
Marsh, S., Foley, L.S., Wilks, D.C., and Maddison, R. (2014). Family-based interventions for reducing sedentary time in youth: A systematic review of randomized controlled trials. Obesity Reviews, 15(2), 117-133.
Maxfield, M. (2013). Panel Paper: The Effects of the Earned Income Tax Credit on Child Achievement and Long-Term Educational Attainment. Paper presented at the Annual Fall Research Conference, November 7-9, Washington, D.C.
Mayer, S.E., Kalil, A., Oreopoulos, P., and Gallegos, S. (2015). Using Behavioral Insights to Increase Parental Engagement: The Parents and Children Together (PACT) Intervention. Working Paper No. 21602. Cambridge, MA: National Bureau of Economic Research.
McDaniel, B.T., Coyne, S.M., and Holmes, E.K. (2012). New mothers and media use: Associations between blogging, social networking, and maternal well-being. Maternal and Child Health Journal, 16(7), 1509-1517.
McLearn, K.T., Strobino, D.M., Hughart, N., Minkovitz, C.S., Scharfstein, D., Marks, E., and Guyer, B. (2004). Developmental services in primary care for low-income children: Clinicians perceptions of the Healthy Steps for Young Children Program. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 81(2), 206-221.
McMorrow, S., Kenney, G.M., Anderson, N., Clemans-Cope, L., Dubay, L., Long, S.K., and Wissoker, D. (2014). Trade-offs between public and private coverage for low-income children have implications for future policy debates. Health Affairs, 33(8), 1367-1374.
McPherson, M., Arango, P., Fox, H., Lauver, C., McManus, M., Newacheck, P.W., Perrin, J.M., Shonkoff, J.P., and Strickland, B. (1998). A new definition of children with special health care needs. Pediatrics, 102(1), 137-140.
McPherson, M.E., Gloor, P.A., and Smith, L.A. (2015). Using collaborative improvement and innovation networks to tackle complex population health problems. JAMA Pediatrics, 169(8), 709-710.
Mehran, M., and White, K.R. (1988). Parent tutoring as a supplement to compensatory education for first-grade children. Remedial and Special Education, 9(3), 35-41.
Mendelsohn, A.L., Dreyer, B.P., Flynn, V., Tomopoulos, S., Rovira, I., Tineo, W., Pebenito, C., Torres, C., Torres, H., and Nixon, A.F. (2005). Use of videotaped interactions during pediatric well-child care to promote child development: A randomized, controlled trial. Journal of Developmental and Behavioral Pediatrics, 26(1), 34-41.
Mendez, J.L. (2010). How can parents get involved in preschool? Barriers and engagement in education by ethnic minority parents of children attending Head Start. Cultural Diversity and Ethnic Minority Psychology, 16(1), 26-36.
Mergler, M.J., Omer, S.B., Pan, W.K., Navar-Boggan, A.M., Orenstein, W., Marcuse, E.K., Taylor, J., DeHart, M.P., Carter, T.C., Damico, A., Halsey, N., and Salmon, D.A. (2013). Association of vaccine-related attitudes and beliefs between parents and health care providers. Vaccine, 31(41), 4591-4595.
Meyer, B.D., and Rosenbaum, D.T. (2001). Welfare, the earned income tax credit, and the labor supply of single mothers. The Quarterly Journal of Economics, 116(3), 1063-1114.
Michalopoulos, C., Duggan, A., Knox, V., Filene, J.H., Lee, H., Snell, E.E., Crowne, S., Lundquist, E., Corso, P.S., and Ingels, J.B. (2013). Revised Design for the Mother and Infant Home Visiting Program Evaluation. OPRE Report No. 2013-18. Washington, DC: Office of Planning Research and Evaluation.
Milkman, R., and Appelbaum, E. (2013). Unfinished Business: Paid Family Leave in California and the Future of U.S. Work-Family Policy. Ithaca, NY: Cornell University Press.
Minkovitz, C.S., Strobino, D., Hughart, N., Scharfstein, D., Guyer, B., and Healthy Steps Evaluation Team. (2001). Early effects of the Healthy Steps for Young Children Program. Archives of Pediatrics & Adolescent Medicine, 155(4), 470-479.
Minkovitz, C.S., Hughart, N., Strobino, D., Scharfstein, D., Grason, H., Hou, W., Miller, T., Bishai, D., Augustyn, M., McLearn, K.T., and Guyer, B. (2003). A practice-based intervention to enhance quality of care in the first 3 years of life: The Healthy Steps for Young Children Program. Journal of the American Medical Association, 290(23), 3081-3091.
Minkovitz, C.S., Strobino, D., Mistry, K.B., Scharfstein, D.O., Grason, H., Hou, W., Ialongo, N., and Guyer, B. (2007). Healthy Steps for Young Children: Sustained results at 5.5 years. Pediatrics, 120(3), e658-e668.
Mittal, P. (2011). Centering parenting: Pilot implementation of a group model for teaching family medicine residents well-child care. The Permanente Journal, 15(4), 40-41.
Moorthy, S., Llorente, C., Hupert, N., and Pasnik, S. (2014). PEG + CAT Content Study. A Report to the CPB-PBS Ready to Learn Initiative. New York, NY and Menlo Park, CA: Education Development Center and SRI International.
Morris, B.A.P., Trimble, N.E., and Fendley, S.J. (1994). Increasing bicycle helmet use in the community: Measuring response to a wide-scale, 2-year effort. Canadian Family Physician, 40(6), 1126.
Morrow, L.M., and Young, J. (1997). A family literacy program connecting school and home: Effects on attitude, motivation, and literacy achievement. Journal of Educational Psychology, 89(4), 736-742.
Muennig, P., Caleyachetty, R., Rosen, Z., and Korotzer, A. (2015). More money, fewer lives: The cost effectiveness of welfare reform in the United States. American Journal of Public Health, 105(2), 324-328.
Nagler, R.H. (2014). Adverse outcomes associated with media exposure to contradictory nutrition messages. Journal of Health Communication, 19(1), 24-40
National Center for Health Statistics. (2015). Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities. Hyattsville, MD: National Center for Health Statistics.
National Center on Shaken Baby Syndrome. (2013). Guidebook for Program Implementation and Management 2013. Available: http://www.dontshake.org/lms/files/lmspdf/PURPLEProgramGuidebook.pdf [March 2016].
The National Partnership for Women and Families. (2015). State and Local Action on Paid Sick Days. Available: http://www.nationalpartnership.org/research-library/campaigns/psd/state-and-local-action-paid-sick-days.pdf [February 2016].
National Research Council and Institute of Medicine. (2009). Preventing Mental, Emotional, and Behavioral Disorders among Young People. M.E. O’Connell, T. Boat, and K.E. Warner (Eds.). Committee on the Prevention of Mental Disorders and Substance Abuse Among Children, Youth and Young Adults: Research Advances and Promising Interventions; Board on Children, Youth and Families. Division of Behavioral and Social Sciences and Education. Washington, DC: The National Academies Press.
Needlman, R., Toker, K.H., Dreyer, B.P., Klass, P., and Mendelsohn, A.L. (2005). Effectiveness of a primary care intervention to support reading aloud: A multicenter evaluation. Ambulatory Pediatrics, 5(4), 209-215.
Neuhauser, L., Constantine, W.L., Constantine, N.A., Sokal-Gutierrez, K., Obarski, S.K., Clayton, L., Desai, M., Sumner, G., and Syme, S.L. (2007). Promoting prenatal and early childhood health: Evaluation of a statewide materials-based intervention for parents. American Journal of Public Health, 97(10), 1813-1819.
Newacheck, P.W., and Taylor, W.R. (1998). Childhood chronic illness: Prevalence, severity, and impact. American Journal of Public Health, 82(3), 364-371.
Niederman, L.G., Schwartz, A., Connell, K.J., and Silverman, K. (2007). Healthy Steps for Young Children Program in pediatric residency training: Impact on primary care outcomes. Pediatrics, 120(3), 596-603.
Noble, K.G., Duch, H., Darvique, M.E., Grundleger, A., Rodriguez, C., and Landers, C. (2012). “Getting Ready for School”: A preliminary evaluation of a parent-focused school-readiness program. Child Development Research, 2012, Art. ID 259598. doi:10.1155/2012/259598. Available: http://www.columbia.edu/cu/needlab/Publications/Noble%20et%20al.,%202012%20Hindawi.pdf [August 2016].
O’Connell, L.K., Davis, M.M., and Bauer, N.S. (2015). Assessing parenting behaviors to improve child outcomes. Pediatrics, 135(2), e286-e288.
O’Donnell, K.J., Glover, V., Barker, E.D., and O’Connor, T.G. (2014). The persisting effect of maternal mood in pregnancy on childhood psychopathology. Development and Psychopathology, 26(2), 393-403.
Olds, D.L., Henderson, C.R., Jr., Chamberlin, R., and Tatelbaum, R. (1986). Preventing child abuse and neglect: A randomized trial of nurse home visitation. Pediatrics, 78(1), 65-78.
Olds, D.L., Henderson, C.R., Jr., and Kitzman, H. (1994). Does prenatal and infancy nurse home visitation have enduring effects on qualities of parental caregiving and child health at 25 to 50 months of life? Pediatrics, 93(1), 89-98.
Olds, D.L., Eckenrode, J., Henderson, C.R., Jr., Kitzman, H., Powers, J., Cole, R., Sidora, K., Morris, P., Pettitt, L.M., and Luckey, D. (1997). Long-term effects of home visitation on maternal life course and child abuse and neglect. Fifteen-year follow-up of a randomized trial. Journal of the American Medical Association, 278(8), 637-643.
Olds, D.L., Robinson, J., O’Brien, R., Luckey, D.W., Pettitt, L.M., Henderson, C.R., Jr., Ng, R.K., Sheff, K.L., Korfmacher, J., Hiatt, S., and Talmi, A. (2002). Home visiting by paraprofessionals and by nurses: A randomized, controlled trial. Pediatrics, 110(3), 486-496.
Olds, D.L., Kitzman, H., Cole, R., Robinson, J., Sidora, K., Luckey, D.W., Henderson, C.R., Jr., Hanks, C., Bondy, J., and Holmberg, J. (2004). Effects of nurse home-visiting on maternal life course and child development: Age 6 follow-up results of a randomized trial. Pediatrics, 114(6), 1550-1559.
Olds, D.L., Kitzman, H.J., Cole, R.E., Hanks, C.A., Arcoleo, K.J., Anson, E.A., Luckey, D.W., Knudtson, M.D., Henderson, C.R., Jr., Bondy, J., and Stevenson, A.J. (2010). Enduring effects of prenatal and infancy home visiting by nurses on maternal life course and government spending: Follow-up of a randomized trial among children at age 12 years. Archives of Pediatrics & Adolescent Medicine, 164(5), 419-424.
Owens, P.L., Zodet, M.W., Berdahl, T., Dougherty, D., McCormick, M.C., and Simpson, L.A. (2008). Annual report on health care for children and youth in the United States: Focus on injury-related emergency department utilization and expenditures. Ambulatory Pediatrics: The Official Journal of the Ambulatory Pediatric Association, 8(4), 219-240.
Pacifici, C., Delaney, R., White, L., Nelson, C., and Cummings, K. (2006). Web-based training for foster, adoptive, and kinship parents. Children and Youth Services Review, 28(11), 1329-1343.
Panter-Brick, C., Burgess, A., Eggerman, M., McAllister, F., Pruett, K., and Leckman, J.F. (2014). Practitioner review: Engaging fathers—Recommendations for a game change in parenting interventions based on a systematic review of the global evidence. Journal of Child Psychology and Psychiatry, 55(11), 1187-1212.
Paradis, H.A., Conn, K.M., Gewirtz, J.R., and Halterman, J.S. (2011). Innovative delivery of newborn anticipatory guidance: A randomized, controlled trial incorporating media-based learning into primary care. Academic Pediatrics, 11(1), 27-33.
Patel, S., and Patel, S. (2015). The effectiveness of lactation consultants and lactation counselors on breastfeeding outcomes. Journal of Human Lactation. Available: http://jhl.sagepub.com/content/early/2015/12/03/0890334415618668.full.pdf+html [August 2016].
Paulsell, D., Avellar, S., Sama Martin, E., and Del Grosso, P. (2010). Home Visiting Evidence of Effectiveness Review: Executive Summary. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Pears, K.C., Fisher, P.A., and Bronz, K.D. (2007). An intervention to promote social emotional school readiness in foster children: Preliminary outcomes from a pilot study. School Psychology Review, 36(4), 665.
Pears, K.C., Kim, H.K., and Fisher, P.A. (2012). Effects of a school readiness intervention for children in foster care on oppositional and aggressive behaviors in kindergarten. Children and Youth Services Review, 34(12), 2361-2366.
Pears, K.C., Fisher, P.A., Kim, H.K., Bruce, J., Healey, C.V., and Yoerger, K. (2013). Immediate effects of a school readiness intervention for children in foster care. Early Education & Development, 24(6), 771-791.
Pears, K.C., Healey, C.V., Fisher, P.A., Braun, D., Gill, C., Conte, H.M., Newman, J., and Ticer, S. (2014). Immediate effects of a program to promote school readiness in low-income children: Results of a pilot study. Education & Treatment of Children, 37(3), 431-460.
Pega, F., Carter, K., Blakely, T., and Lucas, P.J. (2013). In-work tax credits for families and their impact on health status in adults. Cochrane Database of Systematic Reviews, 8.
Phillips, K.R. (2004). Getting Time Off: Access to Leave among Working Parents. Washington, DC: Urban Institute.
Pinquart, M., and Teubert, D. (2010). Effects of parenting education with expectant and new parents: A meta-analysis. Journal of Family Psychology, 24(3), 316-327.
Piotrowski, C.C., Talavera, G.A., and Mayer, J.A. (2009). Healthy Steps: A systematic review of a preventive practice-based model of pediatric care. Journal of Developmental and Behavioral Pediatrics, 30(1), 91-103.
Pisoni, C., Garofoli, F., Tzialla, C., Orcesi, S., Spinillo, A., Politi, P., Balottin, U., Manzoni, P., and Stronati, M. (2014). Risk and protective factors in maternal-fetal attachment development. Early Human Development, 90(Suppl. 2), S45-S46.
Polit, D.F. (1989). Effects of a comprehensive program for teenage parents: Five years after project redirection. Family Planning Perspectives, 21(4), 164-187.
Pomerantz, E.M., Moorman, E.A., and Litwack, S.D. (2007). The how, whom, and why of parents’ involvement in children’s academic lives: More is not always better. Review of Educational Research, 77(3), 373-410.
Puma, M., Bell, S., Cook, R., Heid, C., Broene, P., Jenkins, F., Mashburn, A., and Downer, J. (2012). Third Grade Follow-up to the Head Start Impact Study: Final Report. Report 2012-45. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Ralston, S., and Roohi, M. (2008). A randomized, controlled trial of smoking cessation counseling provided during child hospitalization for respiratory illness. Pediatric Pulmonology, 43(6), 561-566.
Randolph, W., and Viswanath, K. (2004). Lessons from mass media public health campaigns: Marketing health in a crowded media world. Annual Review of Public Health, 25, 419-437.
Ratcliffe, C., McKernan, S.M., and Zhang, S. (2011). How much does the Supplemental Nutrition Assistance Program reduce food insecurity? American Journal of Agricultural Economics, 93(4), 1082-1098.
Reese, L.S., Heiden, E.O., Kim, K.Q., and Yang, J. (2014). Evaluation of Period of PURPLE Crying, an abusive head trauma prevention program. Journal of Obstetric, Gynecologic & Neonatal Nursing, 43(6), 752-761.
Rehkopf, D.H., Strully, K.W., and Dow, W.H. (2014). The short-term impacts of Earned Income Tax Credit disbursement on health. International Journal of Epidemiology, 43(6), 1884-1894.
Resnicow, K., McMaster, F., Bocian, A., Harris, D., Zhou, Y., Snetselaar, L., Schwartz, R., Myers, E., Gotlieb, J., Foster, J., Hollinger, D., Smith, K., Woolford, S., Mueller, D., and Wasserman, R.C. (2015). Motivational interviewing and dietary counseling for obesity in primary care: An RCT. Pediatrics, 135(4), 649-657.
Reynolds, A.J. (1997). The Chicago Child-Parent Centers: A Longitudinal Study of Extended Early Childhood Intervention. Madison: Institute for Research on Poverty, University of Wisconsin–Madison.
Reynolds, A.J. (2000). Success in Early Intervention: The Chicago Child Parent Centers. Lincoln: University of Nebraska Press.
Reynolds, A.J., and Temple, J.A. (1998). Extended early childhood intervention and school achievement: Age thirteen findings from the Chicago Longitudinal Study. Child Development, 69(1), 231-246.
Reynolds, A.J., Ou, S.-R., and Topitzes, J.W. (2004). Paths of effects of early childhood intervention on educational attainment and delinquency: A confirmatory analysis of the Chicago child-parent centers. Child Development, 75(5), 1299-1328.
Rikin, S., Glatt, K., Simpson, P., Cao, Y., Anene-Maidoh, O., and Willis, E. (2015). Factors associated with increased reading frequency in children exposed to Reach Out and Read. Academic Pediatrics, 15(6), 651-657.
Roberts, S.W., and McCowan, R.J. (2004). The effectiveness of infant simulators. Adolescence, 39(155), 475.
Roberts, M.Y., and Kaiser, A.P. (2011). The effectiveness of parent-implemented language interventions: A meta-analysis. American Journal of Speech-Language Pathology, 20(3), 180-199.
Rocca, C.H., Harper, C.C., and Raine-Bennett, T.R. (2013). Young women’s perceptions of the benefits of childbearing: Associations with contraceptive use and pregnancy. Perspectives on Sexual and Reproductive Health, 45(1), 23-32.
Rose, D., Habicht, J.P., and Devaney, B. (1998). Household participation in the food stamp and WIC programs increases the nutrient intakes of preschool children. Journal of Nutrition, 128(3), 548-555.
Rosen, L.J., Myers, V., Hovell, M., Zucker, D., and Ben Noach, M. (2014). Meta-analysis of parental protection of children from tobacco smoke exposure. Pediatrics, 133(4), 698-714.
Rosengard, C., Phipps, M.G., Adler, N.E., and Ellen, J.M. (2004). Adolescent pregnancy intentions and pregnancy outcomes: A longitudinal examination. Journal of Adolescent Health, 35(6), 453-461.
Rossin-Slater, M., Ruhm, C.J., and Waldfogel, J. (2013). The effects of California’s Paid Family Leave Program on mothers’ leave-taking and subsequent labor market outcomes. Journal of Policy Analysis and Management, 32(2), 224-245.
Rouzier, P., and Alto, W.A. (1995). Evolution of a successful community bicycle helmet campaign. Journal of the American Board of Family Practice, 8(4), 283-287.
Ruhm, C.J. (1998). Parental Leave and Child Health. Cambridge, MA: National Bureau of Economic Research.
Sadaf, A., Richards, J.L., Glanz, J., Salmon, D.A., and Omer, S.B. (2013). A systematic review of interventions for reducing parental vaccine refusal and vaccine hesitancy. Vaccine, 31(40), 4293-4304.
Sadler, L.S., Slade, A., Close, N., Webb, D.L., Simpson, T., Fennie, K., and Mayes, L.C. (2013). Minding the Baby: Enhancing reflectiveness to improve early health and relationship outcomes in an interdisciplinary home-visiting program. Infant Mental Health Journal, 34(5), 391-405.
Salonen, A.H., Pridham, K.F., Brown, R.L., and Kaunonen, M. (2014). Impact of an Internet-based intervention on Finnish mothers’ perceptions of parenting satisfaction, infant centrality and depressive symptoms during the postpartum year. Midwifery, 30(1), 112-122.
Sanders, M.R., Montgomery, D.T., and Brechman-Toussaint, M.L. (2000). The mass media and the prevention of child behavior problems: The evaluation of a television series to promote positive outcomes for parents and their children. Journal of Child Psychology and Psychiatry, 41(7), 939-948.
Sanders, M.R., Baker, S., and Turner, K.M.T. (2012). A randomized controlled trial evaluating the efficacy of Triple P Online with parents of children with early-onset conduct problems. Behaviour Research and Therapy, 50(11), 675-684.
Sanders, M.R., Dittman, C.K., Farruggia, S.P., and Keown, L.J. (2014). A comparison of online versus workbook delivery of a self-help positive parenting program. The Journal of Primary Prevention, 35(3), 125-133.
Sandstrom, H., Gearing, M., Peters, E., Heller, C., Healy, O., and Pratt, E. (2015). Approaches to Father Engagement and Fathers’ Experiences in Home Visiting Programs. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Sangalang, B.B., Barth, R.P., and Painter, J.S. (2006). First-birth outcomes and timing of second births: A statewide case management program for adolescent mothers. Health & Social Work, 31(1), 54-63.
Sanghavi, D.M. (2005). Taking well-child care into the 21st century: A novel, effective method for improving parent knowledge using computerized tutorials. Archives of Pediatrics & Adolescent Medicine, 159(5), 482-485.
Sawhill, I., and Venator, J. (2015). Improving Children’s Life Chances through Better Family Planning. Washington, DC: Center on Children and Families at Brookings.
Schmeiser, M.D. (2009). Expanding wallets and waistlines: The impact of family income on the BMI of women and men eligible for the Earned Income Tax Credit. Health Economics, 18(11), 1277-1294.
Scholer, S.J., Hudnut-Beumler, J., and Dietrich, M.S. (2010). A brief primary care intervention helps parents develop plans to discipline. Pediatrics, 125(2), e242-e249.
Scholer, S.J., Hudnut-Beumler, J., and Dietrich, M.S. (2012). Why parents value a brief required primary care intervention that teaches discipline strategies. Clinical Pediatrics, 51(6), 538-545.
Scholle, S.H., Torda, P., Peikes, D., Han, E., and Genevro, J. (2010). Engaging Patients and Families in the Medical Home. Rockville, MD: Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services.
Schott, L., Pavetti, L., and Floyd, I. (2015). How States Use Federal and State Funds under the TANF Block Grant. Washington, DC: Center on Budget and Policy Priorities.
Schuster, M.A., and Chung, P.J. (2014). Time off to care for a sick child: Why family-leave policies matter. New England Journal of Medicine, 371(6), 493-495.
Schuster, M.A., Chung, P.J., Elliott, M.N., Garfield, C.F., Vestal, K.D., and Klein, D.J. (2008). Awareness and use of California’s paid family leave insurance among parents of chronically ill children. Journal of the American Medical Association, 300(9), 1047-1055.
Schuster, M.A., Chung, P., Elliot, M., Garfield, C., Vestal, K., and Klein, D. (2009). Perceived effects of leave from work and the role of paid leave among parents of children with special health care needs. American Public Health Association, 99(4), 698-705.
Schuster, M.A., Chung, P.J., and Vestal, K.D. (2011). Children with health issues. The Future of Children, 21(2), 91-116.
Schwarz, D.F., O’Sullivan, A.L., Guinn, J., Mautone, J.A., Carlson, E.C., Zhao, H., Zhang, X., Esposito, T.L., Askew, M., and Radcliffe, J. (2012). Promoting early intervention referral through a randomized controlled home-visiting program. Journal of Early Intervention, 34(1), 20-39.
Scott, S., O’Connor, T.G., Futh, A., Matias, C., Price, J., and Doolan, M. (2010). Impact of a parenting program in a high-risk, multi-ethnic community: The PALS trial. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 51(12), 1331-1341.
Seburg, E.M., Olson-Bullis, B.A., Bredeson, D.M., Hayes, M.G., and Sherwood, N.E. (2015). A review of primary care-based childhood obesity prevention and treatment interventions. Current Obesity Reports, 4(2), 157-173.
Seeman, M.V. (2010). Parenting issues in mothers with schizophrenia. Current Women’s Health Reviews, 6(1), 51-57.
Seitz, V. (1990). Intervention programs for impoverished children: A comparison of educational and family support models. Annals of Child Development, 7, 73-103.
Selden, T.M., and Hudson, J.L. (2006). Access to care and utilization among children: Estimating the effects of public and private coverage. Medical Care, 44(5), 119-126.
Selk, S., Finnerty, P., Fitzgerald, E., Levesque, Z., and Taylor, J. (2015). Collaborative improvement and innovation network: Increasing capacity of data systems to help save babies’ lives. BMJ Quality & Safety, 24(11), 738-739.
Shapiro, C.J., Prinz, R.J., and Sanders, M.R. (2015). Sustaining use of an evidence-based parenting intervention: Practitioner perspectives. Journal of Child and Family Studies, 24(6), 1615-1624.
Sharifi, M., Adams, W.G., Winickoff, J.P., Guo, J., Reid, M., and Boynton-Jarrett, R. (2014). Enhancing the electronic health record to increase counseling and quit-line referral for parents who smoke. Academic Pediatrics, 14(5), 478-484.
Shelton, T.L., and Stepanek, J.S. (1994). Family-Centered Care for Children Needing Specialized Health and Developmental Services. Bethesda, MD: Association for the Care of Children’s Health.
Sheridan, S.M., Knoche, L.L., Edwards, C.P., Bovaird, J.A., and Kupzyk, K.A. (2010). Parent engagement and school readiness: Effects of the getting ready intervention on preschool children’s social-emotional competencies. Early Education and Development, 21(1), 125-156.
Sheridan, S.M., Knoche, L.L., Kupzyk, K.A., Edwards, C.P., and Marvin, C.A. (2011). A randomized trial examining the effects of parent engagement on early language and literacy: The Getting Ready Intervention. Journal of School Psychology, 49(3), 361-383.
Sheridan, S.M., Knoche, L.L., Edwards, C.P., Kupzyk, K.A., Clarke, B.L., and Kim, E.M. (2014). Efficacy of the Getting Ready Intervention and the role of parental depression. Early Education and Development, 25(5), 746-769.
Sheridan, S.M., Holmes, S.R., Smith, T.E., and Moen, A.L. (2016). Complexities in field-based partnership research: Exemplars, challenges, and an agenda for the field. In M.S. Sheridan and E. Moorman Kim (Eds.), Family-School Partnerships in Context (pp. 1-23). Cham, Switzerland: Springer International.
Shone, L.P., Dick, A.W., Klein, J.D., Zwanziger, J., and Szilagyi, P.G. (2005). Reduction in racial and ethnic disparities after enrollment in the state Children’s Health Insurance Program. Pediatrics, 115(6), e697-e705.
Sipsma, H.L., Magriples, U., Divney, A., Gordon, D., Gabzdyl, E., and Kershaw, T. (2013). Breastfeeding behavior among adolescents: Initiation, duration, and exclusivity. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 53(3), 394-400.
Smith, A. (2014). African Americans and Technology Use—A Demographic Portrait. Washington, DC: Pew Research Center.
Smith, A. (2015). U.S. Smartphone Use in 2015. Available: http://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015 [February 2016].
Smith, T.W., and Kim, J. (2010). Paid Sick Days: Attitudes and Experiences. Chicago, IL: NORC, University of Chicago.
Somers, C.L. (2013). Effects of infant simulators on urban, minority, middle school students. Health Promotion Practice, 15(1), 35-43.
Spock, B. (1957). Dr. Benjamin Spock’s Baby and Child Care (1st ed.).New York: Pocket Books.
Spock, B. (1968). Baby and Child Care (2nd ed.). New York: Meredith Press.
Spock, B. (1976). Baby and Child Care (3rd ed.). New York: Pocket Books.
St. Pierre, R.G., Layzer, J.I., Goodson, B.D., and Bernstein, L.S. (1997). National Impact Evaluation of the Comprehensive Child Development Program: Final Report. Cambridge, MA: Abt Associates.
Stacey, D., Légaré, F., Col, N.F., Bennett, C.L., Barry, M.J., Eden, K.B., Holmes-Rovner, M., Llewellyn-Thomas, H., Lyddiatt, A., Thomson, R., Trevena, L., and Wu, J.H. (2014). Decision aids for people facing health treatment or screening decisions. Cochrane Database of Systematic Reviews, 1.
Staehelin, K., Bertea, P.C., and Stutz, E.Z. (2007). Length of maternity leave and health of mother and child—A review. International Journal of Public Health, 52(4), 202-209.
Starkey, P., and Klein, A. (2000). Fostering parental support for children’s mathematical development: An intervention with Head Start families. Early Education and Development, 11, 659-680.
Storey, J.D., Saffitz, G.B., and Rimon, J.G. (2008). Social marketing. In K. Glanz, B. Rimer, and K. Viswanath (Eds.), Health Behavior and Health Education: Theory, Research, and Practice (4th ed., pp. 435-464). San Francisco, CA: Jossey-Bass.
Strunk, J.A. (2008). The effect of school-based health clinics on teenage pregnancy and parenting outcomes: An integrated literature review. The Journal of School Nursing: The Official Publication of the National Association of School Nurses, 24(1), 13-20.
Szilagyi, P.G., Bordley, C., Vann, J.C., Chelminski, A., Kraus, R.M., Margolis, P.A., and Rodewald, L.E. (2000). Effect of patient reminder/recall interventions on immunization rates: A review. Journal of the American Medical Association, 284(14), 1820-1827.
Szilagyi, P.G., Dick, A.W., Klein, J.D., Shone, L.P., Zwanziger, J., and McInerny, T. (2004). Improved access and quality of care after enrollment in the New York State Children’s Health Insurance Program (SCHIP). Pediatrics, 113(5), e395-e404.
Tanaka, S. (2005). Parental leave and child health across OECD countries. The Economic Journal, 115(501), F7-F28.
Taveras, E.M., Gortmaker, S.L., Hohman, K.H., Horan, C.M., Kleinman, K.P., Mitchell, K., Price, S., Prosser, L.A., Rifas-Shiman, S.L., and Gillman, M.W. (2011). Randomized controlled trial to improve primary care to prevent and manage childhood obesity: The High Five for Kids Study. Archives of Pediatrics & Adolescent Medicine, 165(8), 714-722.
Taylor, T.K., Webster-Stratton, C., Feil, E.G., Broadbent, B., Widdop, C.S., and Severson, H.H. (2008). Computer-based intervention with coaching: An example using the Incredible Years Program. Cognitive Behaviour Therapy, 37(4), 233-246.
Thomson, H., Thomas, S., Sellstrom, E., and Petticrew, M. (2013). Housing improvements for health and associated socio-economic outcomes. Cochrane Database of Systematic Reviews, 2013, 2(CD008657). doi: 10.1002/14651858.CD008657.pub2.
Thornton, S., and Calam, R. (2011). Predicting intention to attend and actual attendance at a universal parent-training programme: A comparison of social cognition models. Clinical Child Psychology and Psychiatry, 16(3), 365-383.
Tiehen, L., Jolliffe, D., and Smeeding, T. (2013). The Effect of SNAP on Poverty. Discussion Paper No. 1415-13. Madison, WI: Institute for Research on Poverty.
Tocce, K.M., Sheeder, J.L., and Teal, S.B. (2012). Rapid repeat pregnancy in adolescents: Do immediate postpartum contraceptive implants make a difference? American Journal of Obstetrics and Gynecology, 206(6), 1-7.
Triple P-Positive Parenting Program. (2016a). Communications. Available: http://www.triplep.net/glo-en/the-triple-p-system-at-work/training-and-delivery/communications [April 2016].
Triple P-Positive Parenting Program. (2016b). Triple P-Positive Parenting Program. Available: http://www.triplep.net/glo-en/home [February 2016].
Tsankova, N., Renthal, W., Kumar, A., and Nestler, E.J. (2007). Epigenetic regulation in psychiatric disorders. Nature Reviews. Neuroscience, 8(5), 355-367.
Turner, K.M.T., and Sanders, M.R. (2006). Help when it’s needed first: A controlled evaluation of brief, preventive behavioral family intervention in a primary care setting. Behavior Therapy, 37(2), 131-142.
U.S. Department of Agriculture. (2016a). National School Lunch Program. Available: http://www.fns.usda.gov/nslp/national-school-lunch-program-nslp [April 2016].
U.S. Department of Agriculture. (2016b). School Breakfast Program. Available: http://www.fns.usda.gov/sbp/school-breakfast-program-sbp [April 2016].
U.S. Department of Agriculture. (2016c). Supplemental Nutrition Assistance Program: FY13 through FY16 National View Summary. Available: http://www.fns.usda.gov/sites/default/files/pd/34SNAPmonthly.pdf [June 2016].
U.S. Department of Agriculture. (2016d). WIC Program Participation and Costs. Available: http://www.fns.usda.gov/sites/default/files/pd/wisummary.pdf [May 2016].
U.S. Department of Health and Human Services. (2015a). Health Insurance Coverage and the Affordable Care Act. Available: https://aspe.hhs.gov/sites/default/files/pdf/139211/ib_uninsured_change.pdf [February 2016].
U.S. Department of Health and Human Services. (2015b). Sudden Unexpected Infant Death and Sudden Infant Death Syndrome: Data and Statistics. Available: http://www.cdc.gov/sids/data.htm [February 2016].
U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Commissioner’s Office of Planning, Research and Evaluation, and Head Start Bureau. (2001). Building Their Futures: How Early Head Start Programs Are Enhancing the Lives of Infants and Toddlers in Low-Income Families. Available: http://www.acf.hhs.gov/sites/default/files/opre/bldg_vol1.pdf [March 2016].
U.S. Department of Health and Human Services, Administration for Children and Families, Office of Planning, Research and Evaluation, and Administration on Children, Youth and Families. (2002). Making a Difference in the Lives of Infants and Toddlers and Their Families the Impacts of Early Head Start. Available: http://www.acf.hhs.gov/sites/default/files/opre/impacts_vol1.pdf [March 2016].
U.S. Department of Housing and Urban Development. (2015). Home Improvements. 2015, Available: http://portal.hud.gov/hudportal/HUD?src=/topics/home_improvements [March 2016].
U.S. Equal Employment Opportunity Commission. (2016). Pregnancy Discrimination. Available: https://www.eeoc.gov/eeoc/publications/fs-preg.cfm [May 2016].
U.S. Preventive Services Task Force. (2009). Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women: U.S. Preventive Services Task Force reaffirmation recommendation statement. Annals of Internal Medicine, 150(8), 551-555.
U.S. Preventive Services Task Force. (2015). Published Recommendations. Available: http://www.uspreventiveservicestaskforce.org/BrowseRec/Index [February 2016].
University of Minnesota. (2013). Chicago Longitudinal Study. Available: http://www.cehd.umn.edu/icd/research/cls/Component.html [February 2016].
van den Hoofdakker, B.J., van der Veen-Mulders, L., Sytema, S., Emmelkamp, P.M., Minderaa, R.B., and Nauta, M.H. (2007). Effectiveness of behavioral parent training for children with ADHD in routine clinical practice: A randomized controlled study. Journal of the American Academy of Child & Adolescent Psychiatry, 46(10), 1263-1271.
van Ijzendoorn, M.H., Bakermans-Kranenburg, M.J., and Ebstein, R.P. (2011). Methylation matters in child development: Toward developmental behavioral epigenetics. Child Development Perspectives, 5(4), 305-310.
Vannice, K.S., Salmon, D.A., Shui, I., Omer, S.B., Kissner, J., Edwards, K.M., Sparks, R., Dekker, C.L., Klein, N.P., and Gust, D.A. (2011). Attitudes and beliefs of parents concerned about vaccines: Impact of timing of immunization information. Pediatrics, 127(Suppl. 1), S120-S126.
Visness, C.M., and Kennedy, K.I. (1997). Maternal employment and breast-feeding: Findings from the 1988 National Maternal and Infant Health Survey. American Journal of Public Health, 87(6), 945-950.
Viswanath, K. (2006). Public communications and its role in reducing and eliminating health disparities. In Institute of Medicine, Examining the Health Disparities Research Plan of the National Institutes of Health: Unfinished Business (pp. 215-253). Committee on the Review and Assessment of NIH’s Strategic Research Plan and Budget to Reduce and Ultimately Eliminate Health Disparities. G.E. Thomson, F. Mitchell, and M.B. Williams (Eds.). Board of Health Sciences Policy. Washington, DC: The National Academies Press.
Viswanath, K., Nagler, R.H., Bigman-Galimore, C.A., McCauley, M.P., Jung, M., and Ramanadhan, S. (2012). The communications revolution and health inequalities in the 21st century: Implications for cancer control. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology, 21(10), 1701-1708.
Walkup, J.T., Barlow, A., Mullany, B.C., Pan, W., Goklish, N., Hasting, R., Cowboy, B., Fields, P., Baker, E.V., Speakman, K., Ginsburg, G., and Reid, R. (2009). Randomized controlled trial of a paraprofessional-delivered in-home intervention for young reservation-based American Indian mothers. Journal of the American Academy of Child and Adolescent Psychiatry, 48(6), 591-601.
Wallace, A.S., Mantel, C., Mayers, G., Mansoor, O., Gindler, J.S., and Hyde, T.B. (2014). Experiences with provider and parental attitudes and practices regarding the administration of multiple injections during infant vaccination visits: Lessons for vaccine introduction. Vaccine, 32(41), 5301-5310.
Wambach, K.A., Aaronson, L., Breedlove, G., Domian, E.W., Rojjanasrirat, W., and Yeh, H.W. (2011). A randomized controlled trial of breastfeeding support and education for adolescent mothers. Western Journal of Nursing Research, 33(4), 486-505.
Wasik, B.H., and Bryant, D.M. (2001). Home Visiting: Procedures for Helping Families (2nd ed.). Thousands Oak, CA: Sage.
Webster-Stratton, C., and Reid, M.J. (2010). The Incredible Years parents, teachers, and children training series: A multifaceted treatment approach for young children with conduct disorders. In J.R. Weisz and A.E. Kazdin (Eds.), Evidence-Based Psychotherapies for Children and Adolescents (2nd ed., pp. 194-210). New York: Guilford Press.
Webster-Stratton, C.H., Reid, M.J., and Beauchaine, T. (2011). Combining parent and child training for young children with ADHD. Journal of Clinical Child and Adolescent Psychology, 40(2), 191-203.
Weikart, D.P., and Lambie, D. (1970). Early enrichment in infants. In V.H. Denenberg (Ed.), Education of the Infant and the Young Child (pp. 83-107). New York: Academic Press.
Whitaker, D.J., Lutzker, J.R., and Shelley, G.A. (2005). Child maltreatment prevention priorities at the Centers for Disease Control and Prevention. Child Maltreatment, 10(3), 245-259.
White House. (2015). The Affordable Care Act Gives Parents Greater Control Over Their Children’s Health Care. Available: https://www.whitehouse.gov/files/documents/health_reform_for_children.pdf [March 2016].
Whitehurst, G.J., Falco, F.L., Lonigan, C.J., Fischel, J.E., DeBaryshe, B.D., Valdez-Menchaca, M.C., and Caulfield, M. (1988). Accelerating language development through picture book reading. Developmental Psychology, 24(4), 552-559.
Whitehurst, G.J., Arnold, D.S., Epstein, J.N., Angell, A.L., Smith, M., and Fischel, J.E. (1994). A picture book reading intervention in day care and home for children from low-income families. Developmental Psychology, 30(5), 679-689.
Whitlock, E.P., Williams, S.B., Gold, R., Smith, P.R., and Shipman, S.A. (2005). Screening and interventions for childhood overweight: A summary of evidence for the U.S. Preventive Services Task Force. Pediatrics, 116(1), e125-e144.
Wilcken, B., and Wiley, V. (2008). Newborn screening. Pathology, 40(2), 104-115.
Williams, C.M., Asaolu, I., English, B., Jewell, T., Smith, K., and Robl, J. (2014a). Child Health Improvement by Hands Home Visiting Program. Lexington: University of Kentucky Department of Obstetrics and Gynecology.
Williams, C.M., Asaolu, I., English, B., Jewell, T., Smith, K., and Robl, J. (2014b). Maternal and Child Health Improvement by Hands Home Visiting Program in the Bluegrass Area Development District. Lexington: University of Kentucky Department of Obstetrics and Gynecology.
Williams, C.M., Asaolu, I., English, B., Jewell, T., Smith, K., and Robl, J. (2014c). Maternal and Child Health Improvement by Hands Home Visiting Program in the KIPDA Area Development District, Kentucky. Lexington: University of Kentucky Department of Obstetrics and Gynecology.
Winickoff, J.P., Buckley, V.J., Palfrey, J.S., Perrin, J.M., and Rigotti, N.A. (2003). Intervention with parental smokers in an outpatient pediatric clinic using counseling and nicotine replacement. Pediatrics, 112(5), 1127-1133.
Wood, M., Turnham, J., and Mills, G. (2008). Housing affordability and family well-being: Results from the housing voucher evaluation. Housing Policy Debate, 19(2), 367-412.
Wood, R.G., Moore, Q., Clarkwest, A., and Killewald, A. (2014). The long-term effects of building strong families: A program for unmarried parents. Journal of Marriage and Family, 76(2), 446-463.
World Adult Labour, (2015). Raising the Global Floor: Adult Labour Leave for Children’s Health Needs. Montreal: McGill Institute for Health and Social Policy.
Wyatt, K.D., List, B., Brinkman, W.B., Prutsky Lopez, G., Asi, N., Erwin, P., Wang, Z., Domecq Garces, J.P., Montori, V.M., and LeBlanc, A. (2015). Shared decision making in pediatrics: A systematic review and meta-analysis. Academic Pediatrics, 15(6), 573-583.
Yaqub, O., Castle-Clarke, S., Sevdalis, N., and Chataway, J. (2014). Attitudes to vaccination: A critical review. Social Science & Medicine, 112, 1-11.
Yeager Pelatti, C., Pentimonti, J.M., and Justice, L.M. (2014). Methodological review of the quality of Reach Out and Read: Does it “work”? Clinical Pediatrics, 53(4), 343-350.
ZERO TO THREE. (2015). Behavior and Development. Available: http://www.zerotothree.org/child-development [February 2016].
Zickuhr, K., and Smith, A. (2012). Digital Differences. Available: http://www.pewinternet.org/2012/04/13/digital-differences [February 2016].
Ziliak, J.P. (2015). Temporary Assistance for Needy Families. Working Paper No. 21038. Cambridge, MA: National Bureau of Economic Research.
Zubrick, S., Ward, K., Silburn, S., Lawrence, D., Williams, A., Blair, E., Robertson, D., and Sanders, M. (2005). Prevention of child behavior problems through universal implementation of a group behavioral family intervention. Prevention Science, 6(4), 287-304.
Zuckerman, B. (2009). Promoting early literacy in pediatric practice: Twenty years of Reach Out and Read. Pediatrics, 124(6), 1660-1665.
Zuckerman, B., Parker, S., Kaplan-Sanoff, M., Augustyn, M., and Barth, M.C. (2004). Healthy Steps: A case study of innovation in pediatric practice. Pediatrics, 114(3), 820-826.








































































































