
5
Targeted Interventions Supporting Parents of Children with Special Needs, Parents Facing Special Adversities, and Parents Involved with Child Welfare Services
The previous chapter describes universal and widely available interventions designed to strengthen parenting and support parents of young children. This chapter turns to evidence-based and evidence-informed interventions used in a variety of settings (e.g., health care, education, the home) with some evidence of effectiveness in supporting parents and parenting knowledge, attitudes, and practices among (1) parents of children with special needs; (2) parents facing special personal and situational adversities; and (3) parents who have in some way been involved with the child welfare system, including those who have a history of or are believed to be at risk for maltreatment and foster parents. These interventions target specific populations of interest named in the committee’s statement of task (Box 1-2 in Chapter 1), such as parents of children with disabilities, parents with mental health conditions, and parents with a history of substance abuse, as well as other populations of parents the committee believes also warrant specific attention based on its review of the evidence. The chapter concludes with a summary.
In a well-known book published some years ago titled Disadvantaged Children: What Have They Compelled Us to Learn?, Julius Richmond advances the idea that much can be learned about the needs of all children by studying populations at risk (Richmond, 1970). In much the same way, the committee believes that examining the needs of specific populations of parents and children, such as those with disabilities and families dealing with mental illness or other challenges, can highlight important principles that extend beyond the needs of those particular populations.
PARENTS OF CHILDREN WITH SPECIAL NEEDS
Among the challenges facing many parents is support and care of their young children who are either born with special needs or develop such needs early in life. This section describes research-based interventions for parents of children with developmental disabilities, behavioral and mental health disorders,1 and serious or chronic medical illnesses, as well as very-low-birthweight, premature infants. Parents often seek out these programs to help them develop skills, learn problem-solving approaches, or receive support because of the challenges they face in carrying out the type of parenting they wish to provide. They recognize that their child’s characteristics may demand special skills in addition to the general knowledge, attitudes, and practices needed by parents.
Parents of Children with Developmental Disabilities
Parents, and indeed family members, of children with developmental disabilities experience challenges that differ from those experienced by parents of typically developing children (Woodman, 2014). When a child with one or more disabilities is born into a family or when parents receive the diagnosis of their child’s disability, they often experience a range of emotions (e.g., shock, grief, anger) that are somewhat similar to those experienced upon learning about the death of a loved one (Kandel and Merrick, 2003). Parents experiencing such emotional reactions require a period of time to adjust, and during that time, parenting and caregiving may be affected.
Some children with disabilities pose particular challenges because of developmental needs and behaviors that require specific parenting skills
___________________
1 It is important to note that behavioral and mental disorders in children may represent an adaptive response to adverse circumstances. In such cases, interventions need to focus on improving the child’s circumstances in addition to addressing the behavioral or mental health disorder.
or actions not required for children who are developing typically (Durand et al., 2013). In addition, parents of children with disabilities tend to experience challenges at certain points of transition during the early childhood years (e.g., hospital to home, entry to early intervention programs, movement from early intervention to preschool programs, movement from preschool to kindergarten) (Malone and Gallagher, 2008, 2009). Young children with disabilities affect families in different ways, but a common finding in the literature is that parents of children with disabilities experience more stress than parents of typically developing children (Woodman, 2014). Given the difficulties faced by parents of children with disabilities, a range of programs focus on parenting skills and engagement for these parents.
Several entities at the federal level define disability. The Eunice Kennedy Shriver National Institute on Child Health and Human Development (2012), drawing on definitions issued by the American Association on Intellectual and Developmental Disabilities (2013) and the Centers for Disease Control and Prevention (n.d.), states
Intellectual and developmental disabilities are disorders that are usually present at birth and that negatively affect the trajectory of the individual’s physical, intellectual, and/or emotional development. Many of these conditions affect multiple body parts or systems. Intellectual disability starts any time before a child turns 18 and is characterized by problems with both: intellectual functioning or intelligence, which include the ability to learn, reason, problem solve, and other skills; and adaptive behavior, which includes everyday social and life skills. The term “developmental disabilities” is a broader category of often lifelong disability that can be intellectual, physical, or both.
The U.S. Department of Education also has established numerous definitions for disabilities that qualify children and families for early intervention and special education services through the Individuals with Disabilities Education Act (IDEA) (U.S. Department of Education, 2015b). The definition of “developmental delay” is particularly relevant in the present context in that it is used most commonly in early intervention and early childhood programs, with carryover through the later grades. IDEA notes that states are required to define developmental delay, but the term usually refers to a rate of development that is slower than normative rates in one or more of the following areas: physical development, cognitive development, communication, social or emotional development, or adaptive (behavioral) development. In addition, a growing population of infants and young children are being diagnosed with autism spectrum disorder (ASD). Although IDEA defines autism as one of its eligibility categories, the ASD definition that researchers and practitioners typically use is from the Diagnostic and Statistical Manual of Mental Disorders (DSM), fifth edition (DSM-5) (American
Psychiatric Association, 2013). According to DSM-5, defining features of ASD are “persistent deficits in social communication and social interaction across multiple contexts (and) . . . restricted, repetitive patterns of behavior, interests, or activities.”
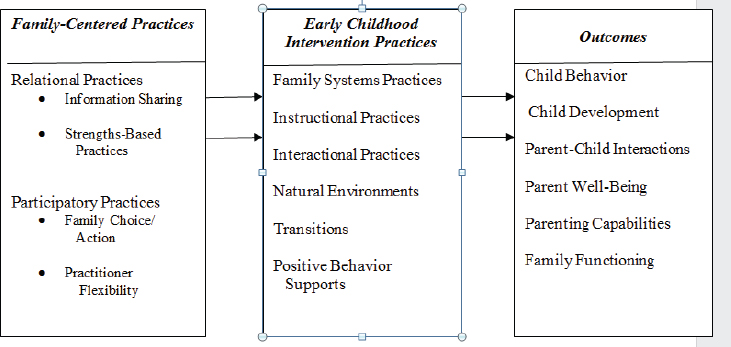
For parents of children with developmental disabilities, the committee expands on the scope of parenting to encompass family-centered care as foundational for parenting practice (Dunst and Trivette, 2010). Family-centered care is a critical concept in programs for young children with disabilities and is written into the provisions of IDEA, which outlines how services to children with disabilities should be provided (see below). The committee draws on a conceptual framework developed by Dunst and Espe-Sherwindt (2016) that explains the linkage among family-centered practices, early childhood intervention practices, and child outcomes (see Figure 5-1) to organize the literature in this section. Dunst and Espe-Sherwindt propose two primary types of family-centered practice—relational practices and participatory practices—that underlie early childhood intervention. The early childhood intervention practices then lead to child outcomes.
IDEA requires for each child and family receiving services establishment of an Individualized Family Service Plan that includes “family-directed assessment of the resources, priorities, and concerns of the family and the identification of the supports and services necessary to enhance the family’s capacity to meet the developmental needs of the infant or toddler” (U.S. Department of Education, 2015a). This provision applies to children with disabilities from birth to age 3. After age 3, children with disabilities may
SOURCE: Dunst and Espe-Sherwindt (2016).
begin special education services that public school programs are required to provide. Families are involved in the development of their child’s Individualized Education Plan.
The three clearinghouses reviewed by the committee for this study (the National Registry of Evidence-based Programs and Practices [NREPP], Blueprints, and the California Evidence-Based Clearinghouse for Child Welfare [CEBC]) do not cover the literature on programs for parents of children with developmental disabilities, although some of the programs developed for other populations that are included in these clearinghouses have been used with families of children with disabilities (e.g., the Triple P-Positive Parenting Program and Incredible Years, which are described in greater detail in the following section). When available, the committee drew on information from evaluations of those programs that is relevant to children with disabilities, but the discussion in this section also includes findings from studies accessed directly from the research literature. In all cases, the findings reviewed here are from studies that employed randomized controlled trials, high-quality quasi-experimental designs, and/or high-quality meta-analyses published in peer-reviewed journals.
Intervention Strategies
Interventions designed to support parents of children with developmental disabilities fall into four overlapping areas: family systems programs, instructional programs, interactional programs, and positive behavior support. Each is discussed in turn below.
Family systems programs Family systems programs follow a systems approach in that they most commonly focus on parents’ internal variables, such as stress, depression, or coping, based on the assumption that changes in those variables will affect the quality of parenting. Singer and colleagues (2007) conducted a meta-analysis examining the primary and secondary effects of parenting and stress management interventions for parents of children with developmental disabilities. Among the 17 studies with experimental or quasi-experimental designs that qualified for the analysis based on the quality of their research methodology, the authors identified three classes of interventions: behavioral parent training (i.e., teaching parents behavior management skills); coping skills interventions, based on principles of cognitive-behavioral therapy; and a combination of the two. They found that interventions in all three groups had significant effects on reducing psychological distress among mothers and fathers of children with developmental disabilities. In a randomized controlled trial involving 70 families of children with ASD, for example, Tonge and colleagues (2006) provided parent education and behavior management training in group and
individual sessions. They found significantly positive outcomes for parents on the General Health Questionnaire postintervention and in follow-up. Feldman and Werner (2002) provided behavior management training with follow-up over a 3- to 6-month period for parents of children with developmental delays and found significantly lower levels of depression for parents randomized into the treatment group. In their summary, Singer and colleagues (2007) note that interventions occurring over a longer period of time and having multiple components (e.g., those that address parents’ well-being as well as parenting skills) produced greater reductions in parental stress relative to those of shorter duration and a simpler design.
In a recent randomized controlled trial of 59 parents of children with autism, parents received six individual sessions in a problem-solving education program, adapted from the well-known problem-solving treatment (PST) (Feinberg et al., 2014). Each session focused on working through a problem identified by the mother using the steps of PST (goal setting, brainstorming, evaluating solutions, choosing a solution, and action planning). Study findings showed that the intervention reduced parents’ depressive symptoms, but not their stress levels.
A more recent trend has been the application of mindfulness training for parents of children with developmental disabilities, with the goal of reducing stress and potentially increasing self-efficacy. Benn and colleagues (2012) conducted randomized controlled trials to examine the effects of mindfulness-based stress reduction techniques, and found significantly positive effects on stress reduction and associated variables (e.g., personal growth). Collateral effects of these techniques are seen in caregiver competence as reported by parents (Benn et al., 2012) and in fewer behavior problems reported by teachers (Neece, 2014).
Instructional programs A large literature documents the effectiveness of programs designed to instruct parents in implementing approaches that promote the skills (e.g., developmental, language, social, play) of their children with disabilities (Girolametto et al., 1998; Green et al., 2010). Roberts and Kaiser (2011), for example, found strong positive effects on the receptive and expressive language skills of young children with intellectual disabilities in a meta-analysis of 18 studies of parent-implemented language training programs that utilized a control group. Effect sizes ranged from .35 to .81 in studies in which parent-implemented treatment was compared with nontreatment or business-as-usual comparison groups. Smaller effects were found for studies comparing parent-delivered and professional-delivered treatment. This finding suggests that children receiving the treatment from parents and speech pathologists made comparable progress, which indicates in turn that, when appropriately trained, parents can be effective facilitators of the language development of children with disabilities.
Programs that have instructed parents in promoting the reading skills of their young children with disabilities have likewise documented positive effects. Two randomized controlled studies (Crain-Thoreson and Dale, 1999; Dale et al., 1996) document the efficacy of parent-implemented dialogic (shared) reading approaches in improving the reading skills of young children with language delays. Using a version of the dialogic reading approach, parents read a book to their child, monitor the child’s understanding through questions, give the child opportunities to respond, repeat and elaborate on what the child says, refer to illustrations to enhance meaning, praise and encourage the child, and focus on making reading a fun activity. The What Works Clearinghouse (2014) has examined this literature and found that these studies meet their standards of acceptability.
Particularly for children with ASD, interventions involving parents have generated positive outcomes. Many comprehensive treatment programs have been designed for children with ASD, and almost all have a parenting component (Odom et al., 2014). These comprehensive programs comprise a set of practices that are based on an organizing conceptual framework, address a variety of developmental needs of the child, and generally occur over an extended period of time (e.g., 1-2 years or more). These elements are detailed in program manuals. Some programs begin in a clinical setting, with the clinician taking the lead, and also are implemented at home by the parent. The Early Start Denver Model (ESDM) is the best and most well-validated example of this approach. Dawson and colleagues (2010) conducted an experimental evaluation of the ESDM, finding significant effects on cognitive developmental and adaptive behavior. They also found differences in brain activation for children in the treatment and control groups (Dawson et al., 2012), and the effects of the ESDM were partially replicated with families in community settings (Rogers et al., 2012). In a quasi-experimental design study of Project ImPACT (Improving Parents as Communication Teachers) (Ingersoll and Wainer, 2013), an evidence-based program that teaches parents of children with autism how to promote their children’s social-communication skills during daily routines and activities, Stadnick and colleagues (2015) found that parents could implement the intervention with fidelity, and the program produced positive child outcomes. In a review of eight intervention programs for toddlers with ASD, Siller and colleagues (2013) document the variety of approaches used by these programs, nearly all involving families and most employing experimental designs to document efficacy (although this summative review does not include effect sizes).
Other studies have documented the positive effects of early intensive behavior therapy delivered by parents. For example, in a meta-analysis of 13 studies conducted in 2009-2011 using experimental and other design types, Strauss and colleagues (2013) found that early intensive behavioral
interventions delivered by parents were more effective than those delivered only by a therapist. In summary, it appears that involving parents is an essential element of early interventions for children with ASD and in some cases may produce stronger positive outcomes than such interventions in which parents are not directly involved.
Interactional programs Interactional programs are designed to promote positive social interactions between caregivers and young children with disabilities. They are based on research showing that some young children with disabilities have difficulty engaging in positive interactions with their parents and others (Adamson et al., 2012), and parents at times may interact with their children in ways that discourage social interaction (e.g., they may be overly directive) (Cress et al., 2008; Lussier et al., 1994). In these interventions, parents are taught how to set up play situations that encourage interaction and to respond in particularly encouraging ways. In a number of randomized studies, Mahoney and colleagues (2006) employed a responsive parenting approach that resulted in increased social interactions among children with disabilities (Karaaslan and Mahoney, 2013; Karaaslan et al., 2013). For many young children with ASD, joint attention—a specific form of parent-child interaction that is a building block for later communication development—is limited or fails to develop. Several investigators have developed interventions designed to promote joint attention among young children with ASD and their parents that have demonstrated positive effects in randomized studies (Kasari et al., 2010; Schertz et al., 2013).
Positive behavior support For parents of young children with disabilities, their child’s behavior often poses challenges, results in negative parent-child interaction, and creates great stress for the parents (Hastings, 2002). A variety of approaches have been developed to promote parenting practices related to behavior management. One such approach—positive behavior intervention and support (PBIS)—is a multicomponent program involving problem-behavior prevention strategies and increasing levels of behavioral intervention (Dunlap and Fox, 2009). In a randomized controlled study, Durand and colleagues (2013) examined the effects of PBIS on parents and their children with a developmental disability and serious challenging behavior. They found significant improvement in challenging behavior, as well as reduction in parent pessimism. Effects of the PBIS model were stronger when it was paired with a complementary program of optimism training aimed at helping parents identify and restructure their parenting-related thought patterns.
The Triple P-Positive Parenting Program (Triple P) (Sanders et al., 2008) was initially designed for school-age children with conduct disorders, and has been used with parents of young children with behavioral and men-
tal health challenges (described in the next section). An adaptation of this program—Stepping Stones—has been used with parents of young children with disabilities. Individual randomized controlled studies (Sofronoff et al., 2011) and a meta-analysis (Tellegen and Sanders, 2013) of Stepping Stones revealed strong effects on reducing challenging behavior and improving broader parenting variables (e.g., style, adjustment, parental relationship). Similarly, the Incredible Years Program was initially designed for parents of school-age children with conduct disorders (Webster-Stratton, 1984), but has been adapted for and applied with parents of young children with disabilities. In a randomized trial, McIntyre (2008) found that the Incredible Years Program reduced negative parent-child interactions and child behavioral problems.
In another study focused on parents of children with autism, investigators evaluated a pilot study of 16 families with children ages 3-6 with a diagnosis of autism and parent-reported disruptive behaviors (Bearss et al., 2013). This study evaluated the RUPP (Research Units on Pediatric Psychopharmacology) Autism Network Parent Training Program, an 11-session structured program designed to teach parents of children with autism and serious behavioral problems skills needed to reduce their children’s disruptive behavior. In a single group pre-post evaluation, parents reported a reduction in their children’s disruptive behaviors and improvements in their adaptive functioning (Bearss et al., 2013).
Research Gaps
There are significant research gaps in the area of interventions for parents of children with developmental disabilities, such as implementation of interventions in natural environments and support for child and family transitions. Although a primary feature of early intervention programs funded through IDEA—a feature required by the federal government—is that they must occur in natural settings, and although IDEA encourages the creation of a transition plan for children moving from early intervention to preschool, the committee found that little or no such experimental research has been conducted, nor do these gaps appear to inform directions for future program development and research.
Parents of Children with Behavioral Challenges and Mental Health Disorders
Behavioral and mental health challenges encompass a range of behaviors and conditions. The psychiatric, psychological, and educational professional communities use somewhat different terminologies, but they agree in identifying these behaviors and conditions as occurring in children who
present with externalizing (e.g., aggression, tantrums) or internalizing (e.g., childhood depression, social withdrawal) behavior. In addition, attention deficit hyperactivity disorder (ADHD), while overlapping to some extent with these behaviors, manifests more distinctly in high levels of physical activity, difficulty with attention, and difficulty in completing tasks (American Psychiatric Association, 2013).
Aggression and antisocial behavior in young children appear to reach a peak between the ages of 2 and 4 and then decline, only to reemerge in the adolescent years (Wahl and Metzner, 2012). Lavigne and colleagues (1996) report that during the early years (ages 2-5), the prevalence of such behavior problems in a sample of 3,860 children averages 8.3 percent, with gender differences (boys having a higher prevalence than girls). In a small proportion of children, however, studies have found that aggressive/antisocial behavior is severe and persists through early childhood (Wahl and Metzner, 2012). It is these children that are diagnosed as having oppositional defiant disorder (ODD) (American Psychiatric Association, 2013). Children with ODD may lose their temper; argue with adults; actively defy rules; and harm people, animals, and/or property.
Intervention Strategies: Parents of Children with Externalizing Behavior
A number of interventions have focused on improving the knowledge, attitudes, and practices of parents of children with externalizing behavior. For the most part, effective interventions have been designed to provide parents with skills needed to better manage their children’s behavior. These interventions have included applications of general parent management training to parents of children with challenging behavior, as well as parent training developed specifically for this population.
Triple P One of the most frequently used and internationally replicated interventions for helping parents prevent and address behavioral challenges in their children is Triple P (Sanders et al., 2008), a multilevel system of support that provides increasingly intensive interventions based on parents’ and children’s needs. The interventions range from basic information on parenting at the least intensive level to behavior management through different modalities (e.g., group, one-on-one, or self-directed learning) (see Box 5-1).
In experimental and quasi-experimental studies of the Primary Care, Standard and Group, and Enhanced Triple P levels conducted in the United States and in other countries, parents have reported less frequent use of dysfunctional parenting practices in such areas as discipline, laxness, and over-reactivity and greater parenting competence. Improvements in observed and parent-reported negative behavior in children relative to controls also have
been found (Hoath and Sanders, 2002; Sanders et al., 2000; Turner and Sanders, 2006; Zubrick et al., 2005). A systematic review and meta-analysis of the multilevel Triple P system that includes 101 studies shows significant short-term improvements in parenting practices; parenting satisfaction and self-efficacy; parental adjustment; parental relationship; and children’s social, emotional, and behavioral well-being (Sanders et al., 2014).2 Triple P has an average NREPP rating of 3 out of 4, where programs rated 4 have the strongest evidence of effectiveness (National Registry of Evidence-based Programs and Practices, 2016e). Triple P level 4 has a CEBC rating of 1 (out of 5), and the entire Triple P system has a CEBC rating of 2, where programs rated 1 have the strongest evidence of effectiveness (California Evidence-Based Clearinghouse, 2016n). The positive results from these assessments provide empirical support for Triple P and a blending of universal and targeted parenting interventions to promote child, parent, and family well-being (Sanders et al., 2014).
The Incredible Years The Incredible Years Program is a developmentally based training intervention for children ages 0-12 and their parents and teachers. Children of families in the program often have behavioral problems. Drawing on developmental theory, the program consists of parent, teacher, and child components that are designed to work jointly to promote emotional and social competence and prevent, reduce, and treat behavioral and emotional problems in young children (National Registry of Evidence-based Programs and Practices, 2016a). Incredible Years received an average NREPP rating of 3.5 out of 4 in a July 2012 review and 3.7 out of 4 in an August 2007 review. It has a CEBC rating of 1 (California Evidence-Based Clearinghouse, 2016g).
The Incredible Years Program addresses parental attitudes by helping parents increase their empathy for their children and educates parents about
___________________
2 Some concerns regarding Triple P studies that report child-based outcomes are raised in a 2012 review of 33 such studies (Wilson et al., 2012). Among the concerns are the use of wait list or no-treatment comparison groups in most of the studies reviewed and potential reporting bias attributed to author affiliation with Triple P and the fact that few of the abstracts for the studies reviewed reported negative findings. A follow-up commentary (Sanders et al., 2012) challenges the findings of this review, noting that it includes a limited subsample of Triple P studies and pools findings from interventions of various intensities and types. Further, the commentary notes that most of the studies reviewed included maintenance probes many of which showed that post-treatment improvements were maintained over various lengths of follow-up. With regard to author affiliation, the commentary states that while developers are often authors of evaluations of Triple P and other parenting programs, the claim that most Triple P evidence is authored by affiliates of the program is untrue (Sanders et al., 2012). The controversy about the proper treatment of the Wilson and Sanders reviews continues in a series of published papers, blog postings, and policy decisions in Australia, the United States, and Europe.
healthy child development, positive parent-child interaction techniques, and positive child behaviors (Marcynyszyn et al., 2011). Sessions focus on building skills to strengthen the parent-child relationship; reduce the use of harsh discipline; and support children’s social, emotional, and language development, as well as their school readiness. The parent program varies in length from 12 to 20 weekly group sessions, each of which lasts 2 to 3 hours. In the teacher program, presented in a workshop format, early childhood and elementary school teachers learn strategies for building positive
relationships with students and families, discipline techniques, and how to stimulate and support children’s academic achievement. The child arm of the program aims to improve children’s social and emotional competence through more than 60 classroom lesson plans lasting about 45 minutes each, delivered by teachers at least twice weekly over consecutive years. Incredible Years has been implemented in almost every U.S. state and is delivered in a variety of education, health, and social service settings.
A systematic review and meta-analysis of 39 randomized controlled
studies of Incredible Years found intervention effects in reducing disruptive behavior and increasing prosocial behavior in children based on parent, teacher, and observer reports (Menting et al., 2013). Perrin and colleagues (2014) conducted a randomized trial of a 10-week Incredible Years parent training program involving families in pediatric practices with toddlers with disruptive behaviors. They found greater improvements in the intervention group compared with the control group for parent-reported and observed child disruptive behavior, negative parenting, and negative child-parent interactions. In another primary care-based experimental study involving 117 parents of children with ODD, however, Lavigne and colleagues (2008) compared Incredible Years led by a nurse, led by a psychologist, or using materials only with no in-person sessions. Findings suggested that all groups showed short- and long-term improvement, but there was no intervention effect. In a randomized controlled trial (independent from the developer, Webster-Stratton), Brotman and colleagues (2003) identified low-income families with a child ages 2-5 at risk for disruptive behaviors as a result of having a sibling or other relative with ODD or conduct disorder or a criminal history. Using a fairly intensive version of Incredible Years, they found that, compared with children receiving usual care, intervention children had fewer behavioral problems, and intervention parents performed better on observed parenting practices of responsiveness and affection. These postintervention improvements, however, were not sustained at 6-month follow-up (Brotman et al., 2003).
Parent Management Training One of the earliest training programs for parents, Parent Management Training (PMT), involving parents of children with externalizing behavior, originated with Gerald Patterson and colleagues. Parents participate in therapy sessions to learn behavior management techniques they would use with their children. In an initial experimental study (Patterson et al., 1982), observations revealed significant reductions in children’s externalizing behavior relative to the control group. In a subsequent randomized study, Hughes and Wilson (1988) followed the PMT model to teach parents of children with conduct disorders to use contingency management. They also found significantly greater changes in child behavior and parent attitudes for the intervention relative to the control group.
Parent-Child Interaction Therapy Elaborating on the model used by Patterson and colleagues (1982), Eyberg and Boggs (1998) designed the parent-child interaction therapy (PCIT) approach, which not only includes a therapy-based child management component but also incorporates elements of play therapy that involve the child directly in clinic sessions. PCIT is an evidence-based intervention developed as a treatment for children ages 2-7 with emotional and behavioral disorders and their parents. Evaluations
of PCIT have involved children ages 0-12. Parents learn skills to encourage prosocial behavior and discourage negative behavior in their children, with the ultimate goal of developing nurturing and secure parent-child relationships.
The intervention has two phases. In the first phase—child-directed interaction—parents learn nondirective play skills and engage their child in a play situation with the objective of strengthening the parent-child relationship. In the second phase—parent-directed interaction—parents learn to use age-appropriate instructions and consistent messages about consequences to direct their child’s behavior, with the goal of improving the child’s compliance with parental instruction. At the beginning of the child- and parent-directed phases, parents attend a didactic session with a PCIT professional to learn interaction skills. The entire intervention is typically delivered in weekly 1-hour sessions over a 15-week period in an outpatient clinic or school setting. PCIT has been applied with families with a history of child abuse, as well as families of children who have developmental disabilities or were exposed to substances prior to their birth (National Registry of Evidence-based Programs and Practices, 2016c; Parent-Child Interaction Therapy International, 2015).
In a randomized controlled efficacy study of PCIT involving parents of children with externalizing behavior and noncompliance, Schuhmann and colleagues (1998) found that parents in the PCIT group interacted more positively with their child, were more successful in gaining their child’s compliance, experienced less stress, and reported more internal locus of control relative to parents in the control group. Other randomized studies comparing outcomes for parents participating in PCIT and those participating in standardized community-based parenting classes or waitlist controls have shown improvements resulting from the intervention in parenting skills (reflective listening, physical proximity, prosocial verbalization), parent-child interactions and child compliance with parental instruction, and child behavior. In addition, compared with controls, parents who participate in PCIT are more likely to report reductions in parenting stress and improvement in parenting locus of control (Bagner and Eyberg, 2007; Boggs et al., 2005; Chaffin et al., 2004; Nixon et al., 2003; Parent-Child Interaction Therapy International, 2015). Participants in evaluations of PCIT have been relatively diverse in terms of race and ethnicity (National Registry of Evidence-based Programs and Practices, 2016c). PCIT received an average NREPP rating of 3.4 out of 4 and a CEBC rating of 1 (California Evidence-Based Clearinghouse, 2016k; National Registry of Evidence-based Programs and Practices, 2016c).
Several randomized controlled evaluation studies have documented the efficacy of a PCIT intervention delivered in a pediatric setting to mothers of infants and toddlers. Bagner and colleagues (2010) found significant effects
on positive parenting and reductions in ineffective parenting practices (as reported by parents). Berkovits and colleagues (2010) compared a PCIT intervention that included anticipatory guidance (i.e., receiving materials ahead of time) with a standard PCIT intervention among mothers of young children expressing subclinical levels of behavior problems. They found that both groups of mothers reported positive effects on their parenting, with no difference between versions at postintervention or 6-month follow-up groups.
Other interventions for externalizing behavior Although Triple P, The Incredible Years, and PCIT have the strongest evidence of efficacy, documented through randomized controlled studies and international replications, a variety of other interventions have been designed to promote parenting (primarily behavior management) skills among parents of children with externalizing behavior. Play Nicely is a video-based training program provided to parents during well-baby visits that is focused on discipline. Randomized controlled studies have found effects on parents’ attitudes toward spanking, as measured immediately after the training (Chavis et al., 2013; Scholer et al., 2010). Early Pathways is an in-home therapy intervention for low-income children with severe externalizing behavioral and emotional problems (e.g., aggression and oppositional behavior) and their parents. In experimental evaluations of standard and culturally adapted versions of Early Pathways, Fung and Fox (2014) and Harris and colleagues (2015) found improvements in parenting (caregiver limit setting and nurturing), parent-child relationships, and child behavior and a decrease in clinical diagnoses following treatment. Results were sustained several weeks postintervention. Intervention components delivered in families’ homes over 8-10 sessions were child-led play to improve the parent-child relationship and parent skills training related to maintaining developmentally appropriate expectations of children and improving parents’ disciplinary practices (time-outs, redirection, ignoring). Early Pathways has been rated by NREPP as having strong evidence of a favorable effect.
Interventions for children with ADHD As noted, children with ADHD have characteristics and presenting issues that differ from those of children with externalizing or internalizing behaviors; thus interventions targeting ADHD address different issues from those addressed by the interventions reviewed above. Lehner-Dua (2001) compared a 10-week program of parent skills training based on the Defiant Children Program (Barkley, 1997) with a parent support group for parents of children newly diagnosed with ADHD ages 6-10. Parents in both groups reported significant improvement in parenting-related competence, while parents randomized to skills training were more likely to report reductions in children’s problem behavior.
Mikami and colleagues (2010) in a randomized controlled study provided the Parental Friendship Coaching intervention to parents to teach them strategies they could use to promote the social skills and peer relationships of their children with ADHD ages 6-10. The intervention resulted in parents’ greater provision of corrective feedback and reduced criticism, and improvement in children’s social skills based on parent but not teacher reports.
Working with fathers of children with ADHD (average age around 8), Fabiano and colleagues (2009) developed a program called COACHES (Coaching Our Acting-Out Children: Heightening Essential Skills), which included parent behavioral training and sports skill training. Although investigators found no significant intervention effects on child ADHD-related behavioral outcomes, fathers participating in the program scored higher on satisfaction measures and were significantly more likely to attend sessions (76% of intervention fathers versus 57% of controls attended ≥ 75% of sessions) and complete parent training “homework” compared with the control group of fathers who only received parent behavioral training.
Intervention Strategies: Parents of Children with Internalizing Behavior and Mental Illness
Internalizing behavior and mental illness are manifest in young children primarily as anxiety and depression. Most of the literature on interventions that involve parents has focused on externalizing behavior, given that internalizing behavior is less prevalent (McKee et al., 2008). Yet the trajectory of internalizing behavior across childhood is often persistent, serious, and linked to adult outcomes (Dekker et al., 2007). DSM-5 (American Psychiatric Association, 2013) includes diagnostic classification and criteria for both anxiety disorder and depression that extend to young children. Some internalizing conditions have been inversely associated with certain parenting practices, such as those that are overinvolved and those that display low warmth (Bayer et al., 2006). Empirically validated intervention approaches have been developed to address both anxiety disorder and depression in children.
Anxiety disorder Anxiety in some situations is normal for young children, such as when very young children are anxious around strangers or in new places. However, severe and debilitating forms of anxiety may manifest in phobias, sleep terrors, posttraumatic stress disorder (PTSD), and separation anxiety. Recent systematic, critical reviews by Anticich and colleagues (2012) and Luby (2013) have identified empirically supported interventions for anxiety disorder in young children. Cognitive-behavioral therapy, once used primarily with older children and youth and in clinical settings, has
been adapted for young children in several approaches that involve parents directly (Cohen and Mannarino, 1996; Deblinger et al., 2001; Hirshfeld-Becker et al., 2010; Kennedy et al., 2009). PCIT, described earlier as treatment for externalizing conditions, also has been adapted for anxiety in young children (Comer et al., 2012; Pincus et al., 2008). In addition, other supported treatments have employed psychoeducational approaches addressing anxiety disorders (Rapee et al., 2005) and play therapy (Santacruz et al., 2006). All of these studies used experimental designs with active control, passive control, or wait list control groups.
Childhood depression The intervention studies discussed above for anxiety have at times included children with depression. Luby and colleagues (2012) adapted the PCIT intervention specifically for parents and their young children with depression. They found significant improvements in children’s executive functioning and decreases in parents’ stress relative to randomly assigned active control group participants.
Parents of Children with Serious or Chronic Medical Illness
For parents of children with serious or chronic medical illness, the concern for their child’s welfare and the challenges related to health care provision and coverage may affect their ability to provide positive parenting. One of the most promising approaches for supporting these parents is problem-solving therapy. Bright IDEAS is a problem-solving skills training program provided by a mental health professional over eight 1-hour individual sessions (Sahler et al., 2002, 2005, 2013). It has been tested in a randomized controlled trial involving mothers of children newly diagnosed with cancer at hospitals/cancer centers in the United States and Israel (Sahler et al., 2002); in a second, larger trial involving mothers at U.S. hospitals/cancer centers, with the intervention being expanded to include Spanish-speaking participants (Sahler et al., 2005); and in a third trial using an active therapy control (Sahler et al., 2013) (the first two trials used standard psychosocial services in the hospital as the control). Significant differences between intervention and control mothers were documented for the mother’s report of her mood, depressive symptoms, and stress across multiple studies (Sahler et al., 2005, 2013).
Melnyk and colleagues developed an educational-behavioral intervention called Creating Opportunities for Parent Empowerment (COPE) for mothers of critically ill children in pediatric intensive care units. In this intervention, mothers are provided information about their child’s course of treatment and recovery, and then trained in structured interaction activities in which to engage when the child is discharged. In two randomized controlled studies (Melnyk et al., 1997, 2007), researchers found that,
compared with mothers in the control group, mothers in the COPE group provided more emotional support for their child during invasive procedures and experienced less stress, and their children showed less internalizing or externalizing behavior after discharge. Researchers also found that treatment effects were mediated by parent beliefs and (inversely) negative maternal mood state.
A number of other programs have tested cognitive-behavioral approaches as well as training in communication and social support for parents of children with illnesses ranging from cancer to diabetes to other chronic diseases. Unfortunately, most of these studies have either been underpowered or shown no significant benefits.
Parents of Very Low-Birth Weight, Premature Infants
Very low birthweight is defined as less than 1,500 grams at birth and extremely low birthweight as less than 1,000 grams. The terms are most commonly used to designate an infant as being born prematurely. Very-low-birth weight infants are admitted to neonatal intensive care units (NICUs), may reside in those units for weeks to months, and at times sustain chronic health or developmental conditions. Because these infants do not come home immediately after birth, a concern is that the normal formation of attachment and transition to parenthood (especially for first-time parents) may be disrupted (Odom and Chandler, 1990). In addition, the children may have ongoing and significant medical needs (e.g., use of respirators or heart monitors) after transitioning home to which the parents must attend.
A range of studies have focused on supporting parents of infants admitted to the NICU (Heidari et al., 2013; Obeidat et al., 2009). Some have evaluated parenting training designed to support effective early parenting skills, while others have looked at psychosocial support for parents to prevent or address posttraumatic stress or depressive symptoms. An approach that has been used for decades is called Kangaroo Mother Care (KMC). This program involves mothers and infants having consistent skin-to-skin contact during the hospitalization period and care providers supporting mothers’ appropriate interactions with their child. In a Cochrane-like quantitative review, Athanasopoulou and Fox (2014) evaluated 13 experimental and quasi-experimental studies of KMC. They found that, although the outcomes of these studies were mixed, mothers in the KMC groups experienced significantly less negative mood and more positive interactions with their infant relative to mothers in the control groups.
Schroeder and Pridham (2006) examined a guided participation approach to supporting mothers’ competencies in relating to their preterm (less than 28 weeks’ gestation) infants admitted to the NICU. Compared
with mothers receiving standard care teaching, mothers in the guided participation group developed expectations and intentions that were more attuned and adaptive to their infants’ needs and showed consistently higher relationship competencies in a randomized clinical trial. In a study of the impact of providing information about prematurity to mothers of preterm infants, Browne and Talmi (2005) provided educational materials about the infants’ behavior and development delivered either through videos and slides and written information or one-on-one teaching sessions. Mothers receiving both interventions scored higher on knowledge of preterm infants’ behavior and reported lower parenting stress at 1-month postdischarge from the NICU relative to control mothers who participated in an informal discussion about care for preterm infants (Browne and Talmi, 2005). To examine the effects of the COPE model, described previously, applied with mothers with very low-birth weight infants in the NICU, Melnyk and colleagues (2008) conducted a secondary analysis of a larger randomized controlled study. They found that mothers experiencing COPE had less anxiety and depression and higher parent-child interaction scores compared with the control group. Segre and colleagues (2013) used the Listening Visits intervention, consisting of six 45- to 60-minute individual sessions provided by a trained neonatal nurse practitioner. The sessions entailed empathic listening on the part of the nurse practitioner to understand the mother’s situation and collaborative problem solving. Improvements were detected in primary outcomes of maternal depressive and anxiety symptoms, as well as quality-of-life measures in a single group pre-post test trial (Segre et al., 2013).
Much of the research in this area has focused on low-birth weight infants in the NICU, and there is a set of well-articulated programs that can be beneficial to these parents. Given the stress created by a premature birth, the psychological trauma associated with prolonged stays in the NICU, and the possible chronic health and developmental conditions that may emerge in these infants, these programs may produce ongoing benefits. It is also important to note the long-standing finding that low-birth weight children born to families living in poverty often have poorer outcomes relative to those born to families not living in poverty (Sameroff and Chandler, 1975), even when interventions are implemented to support their early development (Brooks-Gunn et al., 1995). Parents with limited financial resources or social supports who have premature and low-birth weight children may well need more assistance than their better-off counterparts.
PARENTS FACING SPECIAL ADVERSITIES
This section reviews programs addressing the needs of parents facing special adversities related to mental illness, substance abuse disorders,
intimate partner violence, and parental developmental disabilities, as well as adolescent parents, who often face a number of challenges. It is important to emphasize that approaches for intimate partner violence differ from those applied, for example, with parents with mental illness in that concerns about the safety of the child—even removing the child from the home—must be the priority rather than providing treatment for parents and supporting them in their parental role. Certainly, concerns about the safety of the child are part of the evaluation in the latter cases, but they are not the central focus. It should also be noted that, because of the lack of definitive research on support for parents facing other adversities, such as homelessness or incarceration, the discussion does not address these adversities, even though they affect the lives of millions of children.
The fact that parents are experiencing one or more of these adversities does not necessarily mean that they need help with parenting. Many parents facing such problems are able to provide adequate parenting. However, these adversities can impair parents’ ability to provide their children with the safe, nurturing environment they wish to provide. Coping with these adversities can reduce parents’ overall coping ability and their ability to engage in the types of positive parenting behaviors identified in Chapter 2. As discussed below, it is well established that children living with parents facing these adversities are less likely to attain the desired outcomes identified in Chapter 2 relative to children whose parents are of similar socioeconomic status but do not face these adversities. Providing effective interventions for these parents to support and strengthen their parenting is therefore critical for both them and their children.
At present, the majority of parents experiencing one or more of these adversities are receiving no services for their condition. For higher-risk families most in need of effective treatment programs, engagement rates may be even lower (Ingoldsby, 2010). Although not specific to parents, one study estimates the percentage of persons who needed but did not receive substance abuse treatment to be about 90 percent (Batts et al., 2014). With respect to mental health, a national study of low-income women found that just one-quarter of those with any mental health disorder had sought treatment in the past month (Rosen et al., 2006). Again, even when individuals do receive services, the services generally focus on the presenting problem but do not address parenting issues; in fact, individuals receiving treatment for mental health or substance abuse disorders frequently are not asked whether they are parents.
Three interrelated factors are particularly common barriers to seeking and receiving support among the parent populations discussed in this section: stigma (e.g., that associated with having a mental illness or substance
use disorder),3 parents’ fear that they will be reported to child protection agencies, and distrust of service providers. Parents facing adversities may have an internalized sense of stigma about their condition that affects their sense of self-worth and competence (Borba et al., 2012; Krumm et al., 2013; Nicholson et al., 1998; Wittkowski et al., 2014). The widespread stigma associated with mental illness often increases parental and family stress and poses a barrier to seeking any parenting support, even basic health care (Blegen et al., 2010; Borba et al., 2012, Byatt et al., 2013, Dolman et al., 2013; Gray et al., 2008; Henderson et al., 2013; Krumm et al., 2013; Lacey et al., 2015; Rose and Cohen, 2010; Wittkowski et al., 2014). This appears to be particularly true for parents with severe mental illnesses. Similarly, societal stigma may increase the self-blame, remorse, and shame already felt by mothers with substance abuse disorders, pushing them further away from seeking help and contributing to the denial that is a hallmark of the disease of addiction. Substance abusing mothers cite enormous guilt and shame for “failing” as mothers as a major barrier to accessing treatment (Nicholson et al., 2006).
In addition, many adults living with mental illness, substance abuse, developmental disabilities, or intimate partner violence are cognizant that their condition negatively influences other people’s beliefs about their parenting abilities. Mothers report feeling significant vulnerability based on fear of not being perceived as a good mother. They recognize that as a result of their condition, they can be at risk for involvement of child protective services and loss of child custody, a perception that is based in fact (Berger et al., 2010; Cook and Mueser, 2014; Fletcher et al., 2013; Niccols and Sword, 2005; Park et al., 2006; Seeman, 2012). For example, using Medicaid and child welfare system data, a large study of Medicaid-eligible mothers with severe mental illness found almost three times higher odds of being involved with child welfare services and a four-fold higher risk of losing custody at some point compared with mothers without psychiatric diagnoses (Park et al., 2006). In the case of mothers with substance abuse, caseworkers may be more likely to perceive that children have experienced severe risk and harm (Berger et al., 2010). And the law in many states requires that reports of domestic violence be investigated by child welfare agencies (Blegen et al., 2010; Cook and Mueser, 2014; Dolman et al., 2013; Wittkowski et al., 2014), which makes some victims reticent to invite service providers into their homes (Brown, 2007).
___________________
3 The Substance Abuse and Mental Health Services Administration and other stakeholders are moving away from the use of the term “stigma,” as noted in the recent report Ending Discrimination Against People with Mental and Substance Use Disorders: The Evidence for Stigma Change (2016). Because the word “stigma” continues to be widely accepted in the research community, the committee chose to use this term in this report.
These factors also contribute to parents’ distrust of service providers. Ambivalent feelings about parenting support programs may come from past experiences, as well as familial or social histories or perceptions (McCurdy and Daro, 2001). Some parents report stigmatizing remarks or comments from health care or social service providers. Parents with substance use problems, for example, frequently report that they experience anger and blame from medical and other treatment professionals instead of being viewed as suffering from an illness and treated as such (Camp and Finkelstein, 1997; Nicholson et al., 2006). In the case of parents with mental illness, the distrust may be part of the general attitudes associated with paranoia or delusions (Healy et al., 2015; Stepp et al., 2012).
Although generating participation can be challenging, a wide range of programs are available that are designed to meet the needs of these populations, both by addressing the underlying problems and with respect to supporting and strengthening parenting. High-quality trials of such interventions are limited, however. Although there have been randomized controlled trials, many smaller studies, observational research, and case-control studies provide some guidance on best practices. This section reviews the available evidence on interventions designed specifically to support parents facing adversities related to mental illness, substance abuse disorders, intimate partner violence, and parental developmental disabilities, since each has unique needs that should be considered in offering services to strengthen and support parenting. As noted, many parents face two or more of these challenges, and some face nearly all of them. There has been almost no rigorous evaluation of interventions for these very complex cases, and many of these families are referred to child welfare agencies. Later in this chapter, the committee assesses parenting interventions offered through the child welfare system.
Parents with Mental Illness
Many parents struggle with mental illness at the same time they are trying to provide a safe, nurturing environment for their family. It is estimated that 43.6 million adults in the United States experience mental illness annually, and 9.8 million of them are living with serious mental illness (Center for Behavioral Health Statistics and Quality, 2015). Research indicates that one-half of all lifetime cases of diagnosable mental illness occur by age 14 and three-fourths by age 24 (Institute of Medicine and National Research Council, 2009; Kessler et al., 2005), suggesting that the onset of mental illness precedes or overlaps with the parenting years in most cases.
Determining the prevalence of mental illness specifically among parents is more challenging. Depression is the most common mental illness. A report issued by the National Research Council (NRC) and Institute
of Medicine (IOM) estimates that in a given year, as many as 15 million children may live in a household with a parent experiencing an episode of major depression (Institute of Medicine and National Research Council, 2009). Depression occurring around the time of childbearing is common, with 13 to 19 percent of women experiencing postpartum depression and many others experiencing depressive symptoms during pregnancy (O’Hara and McCabe, 2013). But many parents who experience mental illness have not been formally diagnosed, and patients with a diagnosis of mental illness often are not identified as being parents. It is particularly challenging to estimate the number of parents with severe mental illness (often defined as schizophrenia, psychosis, and bipolar disorder). The relevant research typically has assessed individuals in community settings (community service agencies, mental health clinics, child welfare agencies, prisons, or hospitals), who likely do not represent the broader population (Nicholson et al., 2006). Analysis of data from the National Co-Morbidity Survey suggests that approximately one-half of mothers (46.8%) and one-third of fathers (29.5%) have had a psychiatric disorder at some point during their lifetime (Nicholson et al., 2002). In another study, among adults identified with severe persistent mental illness, approximately two-thirds of women and three-quarters of men were also parents (Gearing et al., 2012; Nicholson et al., 2002).
Mental health disorders encompass a wide spectrum of illnesses and levels of severity, and symptoms may wax and wane over time; thus their impact on parenting and the supports these parents need can be quite variable. As with prevalence, far more is known about the impact of depression on parenting (Institute of Medicine and National Research Council, 2009) than about the impact of severe mental illness (Bee et al., 2014; Schrank et al., 2015). The 2009 IOM and NRC report describes research showing that parental depression is associated with more negative and withdrawn parenting and with worse physical health and well-being of children. But the same report describes a number of promising two-generational programs focused on prevention and emphasizes the potential for helping parents with treatment and parenting programs.
For individuals with mental illness, being a parent is not only a challenge but also often one of the most rewarding parts of their lives (Dolman et al., 2013; Lacey et al., 2015; Wittkowski et al., 2014). Many of these parents are motivated to cope with their own symptoms by focusing on meeting their children’s needs, and they value these relationships (Barrow et al., 2014; Oyserman et al., 2000; Wittkowski et al., 2014). However, mental illness also can interfere with the quality of parenting. A cross-sectional study using video observation of 251 depressed mothers with their toddlers demonstrated that those with more severe depressive symptoms engaged in fewer positive interactions and more negative interactions with
their children and also provided less developmental stimulation (Beeber et al., 2014). Children of parents with mental illness also have a higher risk of developing their own mental health issues, developmental delays, and behavioral problems (Beardslee et al., 2011; Craig, 2004; Dean et al., 2012; Friesen et al., 2009; Gearing et al., 2012; McCoy et al., 2014). Children’s development of these problems can add to the challenges parents face in childrearing and also can increase the fear and guilt they may feel about the impact of their own illness on their child.
There have been few high-quality large-scale evaluations of interventions designed for parents with mental illness and even fewer of those for parents with severe mental illness. The 2009 IOM and NRC report notes that few studies of parental depression focus on parental outcomes or issues specific to parents (Institute of Medicine and National Research Council, 2009). However, many universal interventions have the potential to prevent or mitigate mental illness before it has serious impacts on parenting, and a number of smaller studies have shown positive or promising results of such interventions. For example, the MOMS Partnership, operated by Yale University, interviewed more than 1,300 low-income urban mothers of young children to create a set of developmental and community-based mental health and workforce supports (Smith, 2014). These supports included cognitive-behavioral therapy delivered by community “mental health ambassadors,” along with phone applications to help strengthen mothers’ executive functioning skills and capacity for stress management and reduce depression. Early results based on a participant questionnaire reveal an increase in positive parenting and reduction in depression (Smith, 2014).
Interventions for Parents with Depressive Disorders
A number of programs are designed to prevent adverse child outcomes among families with known parental mental illness. For postpartum depression, limited controlled research indicates that simply treating the illness leads to gains in the quality of parenting (O’Hara and McCabe, 2013). An analysis of the Sequence Treatment Alternatives to Relieve Depression (STAR*D) trial found that treatment leading to remission of mothers’ depression was associated with improved mental health among their children in a nonexperimental study, although the mechanism of change was not assessed (Institute of Medicine and National Research Council, 2009; Weissman et al., 2006). The evidence for treating maternal depression for mothers of infants, however, is mixed. Several reviews found that while sustained interventions may improve the cognitive development of the child, additional research is needed to determine the success of these treatments over time, particularly with regard to the benefits for the child as well as the mother (Nylen et al., 2006; Pooblan et al., 2007). Forman and colleagues
(2007) found in an experimental study that relieving maternal depression alone affected only parenting stress and did not necessarily improve the mother-infant relationship or child outcomes (Forman et al., 2007).
Nonetheless, most studies have demonstrated that interventions combining mental health treatment and parenting support, or at least including a component focused on parenting, often lead to better outcomes relative to programs that focus solely on the illness. A systematic review of the impact of maternal-infant dyadic interventions on postpartum depression included 19 single group pre-post and randomized controlled studies. The author concluded that strategies focused on the dyad and maternal coaching were most effective at reducing psychiatric symptoms and demonstrated modest improvements in the mother-child relationship and maternal responsiveness (Tsivos et al., 2015). Not all such approaches are successful, however. A 2015 Cochrane review assessing the impact specifically of parent-infant psychotherapy versus control or an alternative intervention found no significant effects of the psychotherapy on maternal depression or the mother-child dyad (Barlow et al., 2015).
With the advent of primary care medical homes and the resultant integration of physical, mental, and behavioral health care, there has been growing interest in incorporating parenting interventions and support into primary care settings. This may be a particularly effective way of diagnosing and addressing parental mental health issues. Parents may be more willing to seek health care for their children than for themselves, but during pediatric visits, health care providers may identify a parent who would benefit from mental health treatment (Nicholson and Clayfield, 2004). Screening adults for depression in primary care settings with the capacity to provide accurate diagnosis, effective treatment, and follow-up is endorsed by the U.S. Preventive Services Task Force (2009). Models of stepped collaborative care entail screening for and identifying depression in primary care settings and providing straightforward care in those locations while referring patients with more severe or resistant illness to mental health specialists (Dennis, 2014).
Additional primary prevention programs for parental depression have focused on the period from conception through age 5, although most address parents with infants rather than those with toddlers (Bee et al., 2014; Craig, 2004). Selective primary prevention of depression among parents has been tested most frequently in the perinatal period, with most programs targeting high-risk groups, such as mothers with preterm infants or those at increased risk for postpartum depression (Ammerman et al., 2013; Beardslee et al., 2010; Dennis, 2014; Silverstein et al., 2011). The perinatal period appears to be an effective time to reach a broad population of parents.
Home visiting programs (discussed in detail in Chapter 4) serve parents with high rates of depression, interpersonal trauma, and PTSD, yet less than
one-half of state-based home visiting programs currently have improving parental mental health as an objective (Johnson, 2009). Early studies examining the mental health benefits of home visiting interventions for parents had mixed results, but the results of more recent studies have been positive. In recent studies, for example, home visiting that includes psychotherapy for mothers has been found to improve depression, and as depression improves, so do many measures of parenting (Ammerman et al., 2011, 2013, 2015; Paradis et al., 2013; Tandon et al., 2014). A randomized controlled trial enrolled women in home visiting programs who were identified as being at risk for perinatal depression (Tandon et al., 2014). The intervention consisted of six 2-hour group sessions focused on cognitive-behavioral therapy, with skills being reinforced during regular home visits. At 6-month follow-up, 15 percent of mothers in the intervention group versus 32 percent of the control mothers had experienced an episode of major depression (Tandon et al., 2014). In a randomized trial of the Building Healthy Children Collaborative, there was no difference in rate of referral to child protective services for mothers who received mental health services as part of home visits and women in a comparison group who did not receive such services; in both groups, almost all mothers avoided referral to child protective services (Paradis et al., 2013).
There also have been efforts to help parents with children in center-based care. In a randomized controlled trial of depressed mothers who had infants and toddlers in Early Head Start, investigators tested interpersonal therapy combined with parenting enhancement training versus just treatment for the depression (Beeber et al., 2013). Both groups had a significant improvement in depression scores, but only the group with parent training showed enhanced parent-child interaction skills. Beardslee and colleagues (2010) describe a nonrandomized, multiyear, multicomponent pilot intervention with parents, staff, and administration in an Early Head Start program serving up to 200 children a year. The intervention, Family Connections, was intended to help staff with strategies for addressing mental health problems in the families they served. The program, which was provided to all the families, not just those identified as suffering from depression, utilized widespread education of staff and parents and a parent support group. It resulted in improved parent self-reported parenting knowledge and social support and increased parent engagement with the center.
Other approaches have been tried in public health settings. A randomized study tested two different parenting interventions (Family Talk Intervention and Let’s Talk about Children) in families with a parent diagnosed with a mood disorder (Solantaus et al., 2010). Both interventions improved child mental health symptoms and behaviors. Family Talk utilizes manual-based psychoeducation prevention strategies. One study of 93 families with
at least one depressed parent and one child ages 8-15 found significant and sustained improvement in parental attitudes toward parenting and reduction in internalizing symptoms (predictive of future depression) in the children whose families were assigned to a lecture or clinician-facilitated intervention, although outcomes in terms of levels of parental depression are not described (Beardslee et al., 2003, 2011).
Interventions for Parents with Severe Mental Illness
While parents with brief or time-limited mental health problems can benefit from brief interventions, those with severe mental illness or more complex mental health disorders are likely to need ongoing support and crisis intervention services. Unfortunately, interventions to support and strengthen parenting for parents with severe mental illness have typically not been rigorously evaluated using the types of well-designed randomized controlled trials used to test other parenting interventions described in this report, and this is an identified area of need (Schrank et al., 2015). Shrank and colleagues (2015) conducted a systematic review of parenting studies involving parents who had severe mental illness (psychosis or bipolar disorder) and at least one child between the ages of 1-18. The review included a heterogeneous range of interventions, and child outcomes were evaluated. Four of six randomized controlled trials included in the review showed significant benefits from the interventions, which included intensive home visits, parenting lectures, clinician counseling, and Online Triple P; the lower-quality studies showed mixed results.
A 3-year observational study of mothers with severe mental illness with children ages 4-16 demonstrated that over time, as serious symptoms remitted, parents became more nurturing, raising the hope that treatment could lead to improved child outcomes (Kahng et al., 2008). A meta-analysis of a variety of parenting interventions found a medium to large effect size in improving short-term parent mental health but noted that these benefits may wane over time, again emphasizing the need for longer and more enduring programs (Bee et al., 2014).
One approach for parents with severe mental illness that appears to be promising is to provide parenting interventions during intensive outpatient treatment or inpatient treatment for mental health crises (Krumm et al., 2013). A few hospitals in the United States (many more in Europe and Australia) have mother-baby mental health units where the baby can stay with the mother while she is hospitalized. A systematic review of inpatient parenting programs for women with schizophrenia evaluated 29 studies of interventions in mother-baby units and found improved maternal outcomes, but the review included no randomized controlled studies, and most such studies have been descriptive, observational, and/or quasi-experimental
designs (Gearing et al., 2012; Hinden et al., 2006). A newer observational study in the United Kingdom using a video feedback intervention found that between the time of admission and discharge, mothers with schizophrenia, severe depression, and mania became more sensitive and less unresponsive, and their infants became more cooperative and less passive (Kenny et al., 2013). Notably, mothers at discharge had better outcomes on all parenting measures than both a comparison group of nonhospitalized mothers with mental illness of comparable severity and a group of mothers without mental illness in the community.
Interventions and treatment for parents with mental illness have been found to significantly reduce the risk of children developing the same mental health problems as well as behavior challenges. A meta-analysis included 1,490 children in 13 randomized controlled trials of interventions with cognitive, behavioral, or psychoeducational elements for parents with a variety of mental illnesses and substance use problems (Siegenthaler et al., 2012). The studies included in the review focused on maternal stress reduction, family interventions, home visits, or parenting skills, and reported a 40 percent reduction in the risk of new diagnoses of mental health disorders in the children as well as a significant decrease in the children’s internalizing and externalizing symptoms.
Given the enormous complexity of comorbidities and varieties of presentation in mental illness, sorting out which risks to children derive from parental mental illness and which should be attributed to other stressors is challenging. Doing so is critical, however, for identifying the best strategies for helping families and in considering interventions at both the micro and macro levels. For example, many parents living with severe mental illness will need support in learning parenting knowledge, attitudes, and practices, specifically in understanding normal child development and milestones and how to provide emotional support for their children. They, like all parents, may also benefit from training in such skills as getting children to have a consistent bedtime routine, feeding them, administering nonphysical discipline, and providing emotional support (Nicholson and Henry, 2003; Stepp et al., 2012). Mothers living with severe mental illness themselves have identified generic parenting issues for which they may need help—both in accessing essential resources and in developing critical parenting skills (Nicholson and Henry, 2003).
Tailoring of Services to Individual Needs
Mental illnesses include a wide range of conditions. One mother may have severe depression and struggle with lifelong, recurrent episodes, while another may have a single episode of mild postpartum depression. One disorder may cause symptoms that make it difficult to recognize the emo-
tions or affect of others, while another may cause a parent to display odd behaviors or make unusual comments, and still another may lead to social withdrawal (Healy et al., 2015; Stepp et al., 2012). Even a single diagnosis can manifest with different symptoms and severity at different stages of the illness, and the illness itself can lead to complications. Parents with severe or recurrent illness also may face separation from their children due to hospitalization or temporary or permanent loss of custody, which can impact parental self-efficacy as well as attachment (Gearing et al., 2012; Nicholson et al., 2006). Thus it is important for programs to tailor services to the individual needs of parents. Programs that offer service coordination are likely to be effective for parents with mental illness who face other adversities as well, such as poverty, family violence, housing instability, and substance abuse. Providers and policy makers also need to be mindful of the multiple layers of risk these co-occurring conditions pose to families, since childhood outcomes will be affected by far more than the parenting behaviors or knowledge targeted by many programs.
Parents with or Recovering from Substance Abuse Disorders
Like mental health conditions, substance use and abuse can affect parenting attitudes and practices, as well as engagement and retention in parenting programs. It has been estimated that nearly 22 million Americans have a substance use disorder (Center for Behavioral Health Statistics and Quality, 2015). Yet in 2014, only 4.1 million out of 21.6 million people ages 12 and older with illicit drug or alcohol dependence or abuse received treatment (Substance Abuse and Mental Health Services Administration, 2014b). Moreover, both research and clinical practice have seen little integration of child development and parenting with addiction prevention and treatment. Most studies on substance abuse to date have measured mainly retention in treatment and reduction in maternal substance use as the primary outcomes, with less attention to parenting and work with children (Finkelstein, 1994, 1996; Nicholson et al., 2006).
Abuse of alcohol and drugs can impact parenting in multiple ways. Prenatal exposure to substances can significantly affect infants, resulting in behaviors that are extremely challenging to parents (O’Connor and Paley, 2006; Preece and Riley, 2011; Schuetze et al., 2007). Potential neonatal effects include prematurity and low birth weight; greater reactivity to stress; increased arousal; higher irritability and restlessness; disordered sleep and feeding; tremulousness, high-pitched cry, and startled response; difficulties with sensory integration, such as abnormal responses to light, visual stimuli, and sounds; and hyperactivity (Iqbal et al., 2002; U.S. Department of Health and Human Services, 2014a). An infant who cannot regulate sleep, wakefulness, or stress is therefore often partnered with a mother who has
reduced capacity to deal with stress and to respond to infant cues (Beeghly and Tronick, 1994; Pajulo et al., 2012).
Research has recently combined the neurobiology of addiction with the neurobiology of parenting, and has examined how the disregulation of the stress-reward neural circuits in addiction may impact the capacity to parent (Rutherford et al., 2013). It is well documented that increases in stress result in increases in cravings and substance use (Sinha, 2001). More specifically, the rewarding value of drugs for a substance-dependent individual comes from ameliorating withdrawal and other stressful situations, and this value may diminish biochemically the rewarding and pleasurable aspects of parenting (Rutherford et al., 2013).
One suggested mechanism by which substance abuse impairs parenting is its impact on the neurocircuitry of the mother’s brain, particularly the oxytocin and dopamine systems (Strathearn and Mayes, 2010). Oxytocin motivates social behavior by stimulating a reward response to proximity and social interaction and has been shown to increase significantly in both mother and infant during periods of close contact and breastfeeding (Strathearn et al., 2008). Substance abuse interferes with this process. For example, cocaine specifically coopts this neuropathway by decreasing the production of oxytocin and thereby making maternal care less rewarding for a cocaine user (Elliott et al., 2001). Dopamine operates similarly: it rewards social behavior and regulates the production of stress-response chemicals. Most addictive substances affect dopamine production by providing drug-induced surges of dopamine, decreasing the body’s natural production of the chemical, and nullifying the rewarding effects of normal human behavior. The dysregulation of dopamine also impairs a mother’s ability to regulate stress, making her more susceptible to the exhaustion and frustration inherent in early parenting (Strathearn and Mayes, 2010). From a neurobiological perspective, therefore, the motivation to engage with and respond to infants may be compromised in the presence of addiction, and this diminished motivation may result in part from infant signals holding less reward value (Rutherford et al., 2013). In addition, the increased stress inherent in the parenting role may increase cravings, drug-seeking behaviors, and relapse to substance use (Rutherford et al., 2013).
The few studies that have been conducted on parenting and substance use/abuse have focused primarily on adults entering treatment, who account for a relatively small share of the broader population of parents with substance abuse disorders (Mayes and Truman, 2002). From this limited sample, studies have described a range of parenting deficits and consequences, sometimes associated with specific drugs (including alcohol), as well as the amount, frequency and duration of use.
Chronic substance abuse affects parents’ ability to regulate their own emotions, to provide safe and consistent care for their child, and to be men-
tally alert for bonding and intellectual development (Suchman et al., 2013). Parents may become preoccupied by drug cravings and drug-seeking behaviors, which in turn may lead to physical absences and multiple disruptions in parenting. Studies have found a strong association between substance abuse and emotional/physical neglect and physical abuse (Suchman et al., 2004, 2008).
Further complicating this picture is that all too frequently, the substance-dependent mother has herself been a victim of violence and abuse. High levels of trauma history and moderate to high levels of PTSD diagnosis co-occur among both men and women with substance abuse disorders (Back et al., 2003; Miller et al., 2000; Najavits et al., 1997; Read et al., 2004). Women whose childhood history includes sexual abuse are significantly more likely than women without such a history to report substance use and abuse, as well as depression, anxiety, and other mental health problems (Camp and Finkelstein, 1997).
Although prenatal substance exposure and early mother-child interactions characterized by intoxication and withdrawal have independent affects, it is the cumulative risk of chemical, psychological, and environmental disturbances related to substance abuse disorders that interferes with parenting and child development (Huxley and Foulger, 2008; Mayes and Truman, 2002). These secondary risk factors are amenable to early intervention, identification, and comprehensive treatment modalities, offering an avenue for improved outcomes for both mother and child (Barnard and McKeganey, 2004). Indeed, childrearing conditions appear to greatly outweigh substance abuse in predicting adolescent outcomes for drug-exposed children (Fisher et al., 2011b).
Parenting status is nonetheless frequently neglected in the development of treatment interventions for parents with substance abuse, and rarely are critical needs for child care or children’s services taken into account in developing services and parenting programs for these parents (Finkelstein, 1994, 1996). In addition, most adult and infant/child mental health professionals view families affected by addiction as highly challenging to treat, frequently eliciting feelings of frustration, helplessness, and lack of empathy. The result too often is that individuals suffering from addiction are excluded from community programs, as well as research and evaluation studies (Camp and Finkelstein, 1997; U.S. Department of Health and Human Services, 1999). This exclusion includes home visiting programs, which may screen out parents who use alcohol and drugs. According to the Department of Health and Human Services’ recent report on the Maternal, Infant, and Early Childhood Home Visiting (MIECHV) Program (discussed in Chapter 4), only 12 percent of enrolled families had substance use issues, and only 21 percent of grantees selected alcohol, tobacco, or other drug use as issues to monitor in their families (U.S. Department of Health and Human Services, 2014b).
Substance abuse can be successfully treated. However, while there is good reason to believe that decreased substance use should lead to improved parenting, there have been no experimental evaluations of whether successful treatment of substance abuse disorders, in and of itself, leads to better parenting. Described below are interventions for substance abuse that include a specific focus on parenting.
Residential Treatment Programs for Mothers with Their Children
The standard of care for women’s residential treatment for substance abuse disorders has shifted over the past 15-20 years from mothers being treated in single-adult programs apart from their children to women and children residing together and mothers receiving integrated addiction treatment and parenting education and services (Bromberg et al., 2010). Research suggests that mothers who reside with their children are more likely to enter, remain in, and complete treatment, as well as remain drug free for longer periods of time, relative to mothers who are separated from their children (Clark, 2001; d’Arlach et al., 2006; Grella et al., 2000; Lundgren et al., 2003; Metsch et al., 2001; Pajulo et al., 2006, 2012).
The literature describes a number of specific residential treatment programs for mothers with their children. The majority of studies report positive parent and child outcomes using pre-post evaluation designs (Allen and Larson, 1998; Conners et al., 2001; Grella et al., 2000; Jackson, 2004; Metsch et al., 2001; Moore and Finkelstein, 2001; Porowski et al., 2004; Szuster et al., 1996; Wobie et al., 1997). The Substance Abuse and Mental Health Services Administration (SAMHSA) conducted a national cross-site study of 24 of its funded residential treatment programs for pregnant and parenting women and their children. Data on 1,847 women showed positive results, including an infant mortality rate 57 percent lower than that in the general population. Seventy-five percent of 97 mothers at one site reported improved relationships with their children and learned better stress coping skills (Clark, 2001).
Family Drug Courts
In response to high rates of nonviolent drug-related arrests in the early 1990s, the United States began utilizing drug courts as an alternative to traditional sentencing procedures. These courts often mandate treatment for substance abuse disorders, frequent drug testing, and periodic court appearances for status hearings (Mitchell et al., 2012). If drug court sentences are completed successfully, the individual will have the charges against him/her dropped or, if postconviction, will receive a sentence of time served.
As of 2014, nearly 3,400 drug courts were operating in the United States (National Institute of Justice, 2016).
An expansion of the adult drug court model, family treatment drug courts (FTDCs) were created as an alternative pathway to reunification in child protective cases. Parental substance abuse is one of five recognized risk factors for involvement in the child welfare system; once child protective services are involved, children of parents with substance abuse disorders tend to stay in the system longer and spend more time out of their home of origin (Child Welfare Information Gateway, 2014). The aim of FTDCs is to combat these trends by giving parents with these disorders access to treatment, accountability, support, and a system of structured rewards and sanctions aimed at their ultimately regaining full custody of their children.
One large-scale outcome study compared 301 families served through three FTDCs with a matched control group of more than 1,200 families with substance abuse issues who received traditional child welfare services. This study found that the FTDC mothers were more likely to enter treatment, entered treatment more quickly, and were twice as likely to complete at least one treatment relative to the control group. Also, children of mothers who participated in FTDCs were more likely than children in the control group to be reunited with their mothers (Worcel et al., 2008). Another, smaller, quasi-experimental study showed that parents participating in FTDCs were significantly more likely than those not participating to enter treatment, entered treatment more quickly, received more treatment, and were more likely to complete treatment successfully. The FTDC-group children spent less time placed out of home, their involvement with child welfare services ended sooner, and they were more likely to return to parental care upon discharge (Bruns et al., 2012). Other nonexperimental research has found FTDCs to be one of the most effective ways to increase initiation and completion of treatment for substance abuse disorders among those involved in the child welfare system (Marlowe and Carey, 2012). Reviews of FTDCs have found some evidence of positive findings related to reunification, completion of treatment episodes, fewer parental criminal arrests, and significant cost savings for the child welfare system (Brook et al., 2015; Marlowe and Carey, 2012). However, the lack of rigorous, randomized, intent-to-treat studies leaves unaddressed the possibility that those women who elect to participate in FTDCs are different from those who do not.
Parenting Skills Training for Parents with or Recovering from Substance Abuse Disorders
While research has demonstrated that family and parenting skills can be improved when specific parenting programs are integrated into treatment for substance abuse (Camp and Finkelstein, 1997; Kerwin, 2005; Suchman
et al., 2008, 2010), few targeted parenting interventions have been developed for parents who have or are recovering from such disorders. A study published in 2013 sampled 125 addiction programs in the United States with respect to the extent and nature of parenting skills interventions offered. Only 43 percent of addiction programs surveyed reported offering formal classes on parenting. Of programs that did offer such classes, only 19 percent stated that they had a standardized curriculum. In general, programs did not rate parenting as a high priority relative to other issues addressed in treatment (Arria et al., 2013). Few programs have reached the threshold of a high evidence rating by NREPP and CEBC.
Strengthening Families and the Nurturing Parenting Programs (NPP) are two of the few highly rated group-based parenting programs. Strengthening Families and the NPP for Families in Substance Abuse Treatment and Recovery specifically target substance abuse and parenting. Both of these curriculums are widely used in substance abuse treatment programs nationally, often within residential, day treatment, or FTDC settings. Both emphasize reducing parents’ alcohol and drug use while helping them learn new patterns of nurturing their children to replace existing, possibly abusive patterns. Strengthening Families also has a youth prevention focus, with the goal of reducing risk factors and building resilience against children’s future alcohol and drug use. Strengthening Families and NPP have average NREPP ratings of 3.1 and 3.0, respectively, and the NPP received a CEBC rating of 3 for the version of the program for parents of 5- to 12-year-olds (however, the specific adaptation for substance abuse was not rated independently) (California Evidence-Based Clearinghouse, 2016j; National Registry of Evidence-based Programs and Practices, 2016b, 2016d).
Strengthening Families is one of the first structured group parenting programs developed within an addiction framework (reviewed by NREPP in 2007) (National Registry of Evidence-based Programs and Practices, 2016d). Developed by a university-based research team, the program has been able to gather higher-quality data relative to most other parenting programs that address parental substance abuse. A family-skills training program targeting parents of children ages 3-16, Strengthening Families consists of three courses—parenting skills for parents; life skills for children; and family life skills for the entire family, consisting of structured family activities. All three courses have a strong emphasis on communication skills, effective discipline, reinforcing positive behaviors, and planning family activities together. The goal is to reduce risk factors for behavioral and emotional problems such as substance use. Findings from evaluations of this intervention include improvements in children’s behavior, mental health, and social skills and in parental involvement, parenting supervision, and parenting efficacy. Improvements also have been found in family cohe-
sion and communication, including a decrease in family conflict, as well as reduced alcohol and drug use (Kumpfer et al., 2007).
The NPP was developed specifically for families involved with child welfare services. The emphasis is on participants learning how to nurture themselves while developing nurturing families and parenting skills. The five core domains of the intervention are age-appropriate expectations; empathy, bonding, and attachment; nonviolent nurturing discipline; self-awareness and self-worth; and empowerment, autonomy, and healthy independence. Multiple adaptations, focused on the same core domains, include the NPP for Families in Substance Abuse Treatment and Recovery, which integrates recovery from substance abuse disorders with improved parenting and nurturing relationships with children. Correlational evidence relevant to parenting practices indicates improvements in such parenting outcomes as parental empathy, reduced child abuse and neglect recidivism, decreased family conflict, and decreased support for corporal punishment (Bavolek et al., 1983, 1988; Camp and Finkelstein, 1997; Hodnett et al., 2009).
Other well-supported programs—adult-focused family behavioral therapy and behavioral couples therapy for alcoholism and drug abuse—utilize individual therapy for addressing co-occurring problems so as to improve family relationships and parenting skills. Both of these interventions are conducted primarily in outpatient mental health settings. Adult-focused family behavioral therapy, with a CEBC rating of 2 (“supported by research evidence”), focuses on adults with drug abuse, as well as other co-occurring problems such as depression, trauma, and child maltreatment (California Evidence-Based Clearinghouse, 2016b). This intervention, based in outpatient behavioral health systems, requires delivery by licensed mental health professionals. It includes a focus on improving family relationships; communication skills; and child management skills, including effective discipline. Outcomes in randomized and longitudinal studies that utilized control groups include improvements in family relationships and parental employment as well as reductions in parental substance use and depression (Azrin et al., 1994, 1996; Donohue et al., 2014). Behavioral couples therapy for alcoholism and drug abuse, rated highly by NREPP, is an intervention for couples focused on reducing alcohol and drug use and intimate partner violence and increasing treatment compliance. Although not used solely with parents, its outcomes, in addition to reduction in intimate partner violence, have been found to include improvement in children’s psychosocial functioning and decline in children’s clinical impairment in randomized controlled research (Kelley and Fals-Stewart, 2002).
Schaeffer and colleagues (2013) describe a pilot study of Multisystemic Therapy-Building Stronger Families (MST-BSF), an integrated treatment model designed to address parental substance abuse and child maltreatment among families in the child welfare system. A quasi-experimental study
of 43 mother-youth dyads (25 MST-BSF participants and 18 comparison dyads) found fewer substantiated maltreatment reports and reduced time out of the home in the MST-BSF group (Schaeffer et al., 2013). This home-based intervention is currently being studied in a large, randomized clinical trial funded by the National Institute on Drug Abuse.
A recent review of 21 outcome studies on parenting programs used in substance abuse disorder treatment included 17 different parenting interventions. Studies consisted of 9 randomized controlled trials, 3 quasi-experimental studies, and 9 studies with no comparison group. Results indicate that combining substance abuse treatment with a parenting intervention may be more effective than substance abuse treatment alone for reducing parental substance use and improving parenting. Parents appeared to benefit the most when, prior to learning specific parenting techniques, they learned general psychological coping strategies, such as developing emotional regulation. In addition, many of the parenting programs showed common obstacles to attendance, including lack of transportation, hunger, unsupervised children, and stigma (Neger and Prinz, 2015).
Helping Parents Nurture Child Security
Given the complexity of addiction and the way it impacts parenting and the parent-child relationship, a number of newer, promising interventions grounded in attachment theory and focused on the parent-child relationship have been developed and described in the literature (Pajulo and Kalland, 2013; Pajulo et al., 2006; Suchman et al., 2008). These newer interventions focus mainly on assisting parents in being more emotionally attuned to their children and in developing their own capacity for emotional regulation. They include individual and dyadic interventions, such as child-parent psychotherapy, parental reflective functioning (Fonagy et al., 2012), and mentalization-based therapy—that is, keeping the child in mind (Suchman et al., 2013). They also include parenting program adaptations for adults with substance abuse disorders that have been the subject of several small pilot studies.
Berlin and colleagues (2014) in a randomized study piloted Attachment and Behavioral Catch Up, a residential treatment program for new mothers focused on coaching parents in nurturing that follows the child’s lead and reducing frightening caregiving behaviors. Mothers who received 10 sessions of this attachment-based parenting program revealed more supportive parenting behaviors relative to controls. However, the pilot was very small, with only 11 mothers in the intervention group and 10 in the control group (Berlin et al., 2014). In a randomized pilot study testing the efficacy of the Mothers and Toddlers Program (MTP), a 12-week attachment-based parenting intervention for mothers enrolled in methadone treatment,
mothers participating in MTP demonstrated better caregiving behaviors compared with mothers enrolled in a traditional parenting education program (Suchman et al., 2010). This individual psychotherapy intervention emphasized reflective functioning and mentalization and targeted mothers of children ages 0-3. MTP, now known as Mothering from the Inside Out, is currently undergoing a 5-year randomized clinical trial targeting children 12-60 months of age (Suchman et al., 2013).
Preventing Substance Use during Pregnancy
Another promising intervention, known as the Parent-Child Assistance Program (PCAP), follows pregnant and parenting mothers with alcohol and/or drug abuse to prevent substance-exposed births. The program provides office- and home-based substance abuse treatment and case management services over several years that include attention to parenting, family planning, education and employment, and reunification with children. Evaluations of PCAP in experimental and single group pre-post studies show increased substance use disorder treatment completion rates and reductions in substance-exposed births and disrupted parenting (Grant and Ernst, 2014; Grant et al., 2005; Ryan et al., 2008). In one experimental study, 12 percent of mothers participating in PCAP had a subsequent alcohol- or drug-exposed infant within 3 years, compared with 21 percent of similar mothers in typical substance abuse disorder treatment that did not include case management (Ryan et al., 2008). Data from Washington State for the period 2007-2014 show that after 3 years in PCAP, 90 percent (of 924) of mothers had completed substance abuse treatment, and 83 percent of children whose mothers were in the program were living with their own families (Grant and Ernst, 2014).
Recently, several federal agencies have evaluated programs and systems of care that coordinate substance abuse disorder treatment with children’s physical and mental health services (including trauma-specific services), as well as child welfare. In the Children Affected by Methamphetamine (CAM) Grant Program, SAMHSA funded 12 grantees to develop integrated and coordinated approaches to care for parents with substance abuse disorders and child welfare involvement, as well as to expand and enhance services for children ages 0-17 in families participating in an FTDC. Specialized client outreach and engagement strategies, as well as strengthened care coordination, were part of the program design. Data from 1,850 families served through the end of program year 3 show that parents stayed in substance abuse treatment an average of 6 months, and 42 percent completed treatment. The percentage of adults with reduced substance use at treatment discharge ranged from approximately 33 to 63 percent, depending on the substance. Families showed statistically significant improvements in over-
all child well-being and family functioning, including safety and parental capabilities (Substance Abuse and Mental Health Services Administration, 2014a). This was not a randomized controlled demonstration.
A second program designed to enhance collaborative projects between child welfare and substance abuse treatment services—the Regional Partnership Grant Program—has been funded by the U.S. Children’s Bureau. Fifty-three grantees representing state, county, and tribal partnerships were funded initially, during 2007-2012, and a 2-year extension was awarded to eight of these grantees. A second 5-year cohort of 17 grantees is funded for 2012-2017, with a more specific focus on both trauma and child well-being, as well as participation in a national cross-state evaluation. All grantees were required to provide activities addressing child maltreatment; safety; parenting capacity; family well-being; and substance abuse treatment, including reduced substance use, care coordination, and cross-system collaboration. Grantees were not required to implement a specific intervention or program model. Interim findings from a subset of 10 grantees based on the North Carolina Family Assessment Scale showed that the percentage of overall parental capability with a rating of mild to clear strength increased from 16.6 to 49.7 percent. Parents in the grant program showed significant improvements in four of seven parental capability areas, including development/enrichment opportunities and supervision of children (U.S. Department of Health and Human Services, 2014a).
Parents Affected by Intimate Partner Violence
A major issue to be addressed in designing any approach for strengthening and supporting parenting is the impact of high levels of intimate partner violence on the quality of parenting and on outcomes for children. Intimate partner violence often affects parenting capacity and can have a direct effect on children who witness its occurrence. While most attention has focused on the impact of physical intimate partner violence, children exposed to a parent’s threatening or otherwise verbally abusing a partner also are at elevated risk for a variety of mental health and other developmental problems, especially when such behavior is frequent, intense, and poorly resolved (Geffner et al., 2014; Repetti et al., 2002). For example, a child who regularly watches or hears one parent4 threaten or scream at the other may feel fear, anxiety, and anger similar to what is experienced by a child who regularly sees one parent slap or shove the other. Infants, toddlers, and preschoolers in particular cannot distinguish between the severity of aggressive verbal threats and that of mild physical violence.
___________________
4 The term “parent” here refers to biological parents as well as to any other intimate partners who are regularly a part of the household.
While a number of national studies have found that as many as one-third of women and one-fourth of men are exposed to intimate partner violence at some point, the evidence regarding the number of exposed children is limited, and there are no data on the number of children exposed to all forms of high family conflict (Black et al., 2011; Finkelhor et al., 2009). According to the 2008 National Survey on Children’s Exposure to Violence, 6.1 percent of all children in the United States had witnessed an interparental assault in the past year, and 17.3 percent had witnessed an interparental physical assault at some point in their lifetime (Finkelhor et al., 2015).5
Like parents with mental illness or substance abuse, parents experiencing intimate partner violence often feel ashamed and guilty about what has happened to their children. These feelings, plus fear of being reported to child welfare, discourage many victims from reporting the violence and may affect parents’ willingness and capacity to engage in parenting programs, as well as other support services (Lieberman et al., 2005).
Impact
Various studies have found that, across a number of measures, 4-20 percent of individual differences in children’s functioning can be attributed to exposure to intimate partner violence (Davies and Cummings, 2006). Numerous studies have found that children living in households with intimate partner violence evidence a variety of emotional and developmental problems (Edleson, 1999; Holt et al., 2008; Wolfe et al., 2003). Witnessing intimate partner violence is a traumatic event for children and can directly impact their mental health and behaviors by undermining their sense of safety, security, and support (Lieberman et al., 2011). School-age children and adolescents exposed to intimate partner violence perform more poorly than their peers in school (Kitzmann et al., 2003; Koenen et al., 2003) and are more likely to display externalizing behaviors, conduct and oppositional defiant disorder, and aggressive interactions with peers (Cummings and Davies, 2011; Voisin and Hong, 2012). Exposure to intimate partner violence also is associated with depression and anxiety, poorer physical health, and increased risk of involvement in teen pregnancy (Anda et al., 2001), as well as juvenile delinquency (Herrera and McCloskey, 2001). Additionally, longitudinal studies have found an association between childhood exposure to intimate partner violence and adult alcohol abuse, particularly in
___________________
5 This study was based on interviews with parents and children, with assault broadly defined. It included pushing and shoving, as well as more serious forms of violence. The lifetime exposure percentage was almost three times as high as the past year exposure percentage, suggesting that many of the children who had witnessed domestic violence in the past had not recently been exposed to this particular form of violence (Finkelhor et al., 2015).
women (Repetti et al., 2002). Moreover, one analysis of school and court record data of 3rd through 5th graders and their families found that being in a class with children exposed to domestic violence was associated with significantly decreased reading and math scores and significantly increased misbehavior among other children in the classroom (Carrell and Hoekstra, 2010).
Mechanisms
Many researchers have sought to identify the mechanisms through which exposure to intimate partner violence affects children’s development. Summarizing this research, Davies and Cummings (2006, p. 88) conclude that “interspousal conflict increases child vulnerability to maladaptive trajectories through multiple mechanisms and pathways.”
Physical or verbal violence in the home can impair parental functioning, the parent-child relationship, and the co-parenting relationship and can impact children directly. For example, parents in a violent home often suffer from trauma and physical and mental problems. As a result, they may be unable to provide consistent nurturing and support or appropriate discipline for their children, which may in turn have an effect on children’s externalizing or internalizing behaviors, thereby making parenting more difficult. Parents experiencing intimate partner violence often engage in overly harsh or overly permissive parenting or have difficulty responding to children in a consistent and positive manner (Conger et al., 2011; Cowan et al., 2014; Cummings and Davies, 2011). In some situations involving intimate partner violence, children are subjected to physical punishment that constitutes legal child abuse.
Not all exposed children will experience adverse outcomes. There is evidence that parenting practices can either buffer or exacerbate the effects of intimate partner violence on children’s behavior. For example, longitudinal research has found that high maternal control and appropriate authority mitigate the effects of a partner’s violence on children’s externalizing behaviors (Tajima et al., 2011). But while a body of research has tested various theories, “the nature of the interplay between marital conflict and parenting practices is not well understood” (Davies and Cummings, 2006, p. 103).
The majority of families reporting intimate partner violence face a host of other challenges in their daily lives. Common co-occurring risk factors include drug and alcohol abuse, low parental educational attainment, and maternal depression (Riggs et al., 2000; Stover et al., 2009). The highly violent neighborhoods in which many families live may increase the likelihood of intimate partner violence (Benson et al., 2003). The complexity of understanding the mechanisms by which intimate partner violence affects both adults and children and the associated variations in family and child
dynamics poses challenges for designing interventions that can improve parenting in these families.
Interventions Designed to Address Intimate Partner Violence and Parenting
While the harmful impact of intimate partner violence on children and adults is widely recognized, no system is in place for identifying these families and providing assistance to all family members, including children. The nature of the response and services provided generally depends on how the violence comes to light, the attitudes of the parent suffering the violence, and the nature of the available local services. Most interventions focus primarily on mothers. Programs often focus solely on the intimate partner violence, without addressing parenting strategies in general or parenting behaviors that might buffer children from the risks stemming from the violence.
Intimate partner violence raises a special issue with respect to interventions designed to strengthen and support parenting in these families, in that such interventions must consider the repetitive nature of the violence in many families, which may pose an ongoing threat to the safety of one of the adults. Many researchers and clinicians believe the use of violence often is part of perpetrators’ need to exercise complete control over their partner (and often the children in the home), which is harmful to both the nonviolent partner and the children (Bancroft et al., 2011). As discussed below, this raises both policy and programmatic issues related to determining whether interventions should target just one or both partners.
Programs in connection with a parental report of violence Intimate partner violence comes to official attention most commonly when a victim, usually female, calls the police (although most female victims do not report their victimization to the police [Catalano et al., 2009]), requests protection from a court, seeks shelter, or is treated for injuries in an emergency room, or the issue of violence is raised in the context of divorce and child custody proceedings. While historically, few of these families received parenting services, recent years have seen the provision of such services, most commonly to the mother and children, and in a small number of cases to the perpetrating father. (Although more women are now being arrested for intimate partner violence, there is little information on what happens in these situations.)
Parenting services may become available when the custodial mother enters a domestic violence shelter (which occurs for only a small portion of families), and such services are offered during the stay or when the parent leaves the shelter. Some shelters now offer structured parenting programs, although there is very little evidence on the nature or effectiveness of these
programs (Sullivan, 2012). Moreover, many women bring their young children with them to shelters, and over time, shelter-based programs have been developed to meet some of the children’s basic needs (e.g., periodic visits from a public health nurse). Many shelters also offer counseling for children.
Increasing numbers of community programs outside of the shelter system work with mothers, couples, and children experiencing intimate partner violence. Mothers may enter these programs following a stay in shelter care; through a referral from police, a court, or a domestic violence support agency; or on their own initiative (few programs serve fathers who have been subject to intimate partner violence). Prosecutors in a number of cities have established specialized domestic violence units, and there are now more than 100 specialized domestic violence courts (Labriola et al., 2010).
These programs use a variety of approaches. Four programs focused on parenting are considered evidence-based as the result of randomized controlled trials: child-parent psychotherapy, parent-child interaction therapy (PCIT, discussed earlier), Kids’ Club and Moms’ Empowerment, and Project Support (Chamberlain, 2014). These programs have been found effective in reducing children’s behavioral problems, reducing mental health issues for mothers and children, and reducing mothers’ stress and improving their parenting (Chamberlain, 2014; Lieberman et al., 2005; Van Horn and Reyes, 2014).
Three interventions focused on helping children exposed to intimate partner violence also have proven effective. Trauma-focused cognitive-behavioral therapy works directly with children to reduce posttraumatic stress. Cognitive-Behavioral Intervention for Trauma in Schools, developed for children who have experienced trauma, including witnessing domestic violence, is delivered by school-based mental health clinicians—primarily to children, but there are sessions for parents. Finally, Child and Family Traumatic Stress Intervention provides brief psychoeducation and early intervention to address posttraumatic stress reactions and prevent the onset of PTSD among children and adolescents ages 7-18 who experience trauma, including intimate partner violence. Each of these programs has been shown to reduce symptoms resulting from trauma in children (Chamberlain, 2014), but not through changes in parenting.
Men also may receive counseling services for intimate partner violence, often through the criminal justice system. These programs focus largely or exclusively on trying to prevent further violence rather than on improving the couple or parent-child relationship. A few programs, such as Caring Dads, are available to batterers who have not been arrested or convicted of intimate partner violence, and these programs may also focus on family issues. A small number of studies have evaluated programs for men who commit intimate partner violence, with recidivism being the measured
outcome. Meta-analyses of experimental and quasi-experimental studies of these programs have found small to no effects on recidivism, and dropout rates are very high (Babcock et al., 2004; Feder and Wilson, 2005; Stith et al., 2012). Some evidence suggests that men are more likely to change their violent behavior when they understand the impact of the violence on their children.
Debates are ongoing in the field about the best approach to strengthening and supporting parenting following reports of intimate partner violence. Reports to the police or a court may lead to the arrest of the perpetrator and his or her removal from the home; many jurisdictions have mandatory or preferred arrest policies if a victim calls the police (Goodmark, 2012).
In recent years, many in the field have questioned the heavy reliance on arrest and prosecution in these cases (Goodmark, 2012), arguing that these actions often fail to promote the well-being of the parent experiencing violence or that of the children, although some people with extensive experience strongly advocate for separating all perpetrators of violence from the family and against working jointly with the parents (Bancroft et al., 2011). Clearly, it often is inappropriate to treat couples together, at least initially, since doing so may pose a threat to a parent or child (Babcock et al., 2004). There is some evidence from experimental and quasi-experimental research, however, that working with couples can be beneficial to the parents and children (Babcock et al., 2004). It may be that interventions at the couple level best follow after some initial individual work and assessment of the potential danger to the victim of working with the couple.
In some states, a report of intimate partner violence can lead to involvement by child welfare services. There is high overlap between intimate partner violence and physical abuse of children, which often justifies that involvement. In many jurisdictions, the fact that a child has witnessed intimate partner violence is a basis for investigation by child welfare services. The appropriateness and impact of these interventions are discussed in the section below on child welfare services.
Court-affiliated parenting education for divorcing parents As noted, family conflict, including intimate partner violence, may come to light through divorce and child custody proceedings. In most jurisdictions, public policy or case law favors continued involvement of both divorcing parents in custody of the child through various living or visitation arrangements. Yet substantial clinical evidence shows that high conflict following divorce has extremely negative impacts on children (Amato and Keith, 1991).
A small number of states have mandated that all divorcing parents participate in court-affiliated parenting education programs, with the goals of preventing future parental conflict and minimizing negative effects of the divorce on children (Sandler et al., 2015). A number of small studies have
evaluated such programs using a no-treatment control group design. Overall, these studies have found a moderate positive effect in reducing conflict and improving parenting after divorce (Pruett and Barker, 2010; Sandler et al., 2015). However, most of these programs “were conducted under controlled, experimental conditions. Several studies suggest that parenting programs are less effective when implemented as community-based services delivered at scale. . . .” (Sandler et al., 2015, p. 169).
These studies, moreover, have not examined mandatory counseling in situations involving intimate partner violence. Some experts oppose required counseling, especially joint counseling, in these cases. Joint counseling, and especially any form of joint custody, can entail continued efforts at coercive control by the violent parent, with traumatic effects on the other parent and the children. Some evidence shows that courts may ignore these potential harms and may even penalize the parent who has suffered the violence if she or he resists contact with the other parent (Meier, 2015). No studies on the impact of court decisions or procedures in custody disputes involving intimate partner violence have been conducted.
Parents seeking help in dealing with children’s problem behaviors associated with intimate partner violence As discussed earlier in this chapter, many programs, such as PCIT, Incredible Years, and Triple P, are available for parents seeking help when their child is exhibiting problem behaviors. Children’s problem behaviors often are associated with living in a family experiencing intimate partner violence (Bancroft et al., 2011; Chamberlain, 2014; Tajima et al., 2011). Child-parent psychotherapy has been used with preschoolers exposed to domestic violence and showing symptoms of PTSD and behavioral problems. In randomized controlled studies, child-parent psychotherapy has led to significant declines in these problems compared with a control group, as well as improvements in maternal behaviors (Ippen et al., 2011; Lieberman et al., 2005, 2006). PCIT, which works with families in which intimate partner violence no longer exists, has been found in a nonrandomized controlled study to be effective in helping children and reducing parental conflict as long as the violence has ceased (Timmer et al., 2010).
Couples seeking relationship counseling Many couples experiencing high levels of conflict seek family therapy. This conflict may include intimate partner violence that has not been reported to the police or led to separation (Jose and O’Leary, 2009). Many family therapists now regularly screen for intimate partner violence and try to assess whether joint therapy is safe, although practices in this regard are highly uneven (Stith et al., 2012).
Several specific approaches for addressing violence in couples therapy have been evaluated with respect to whether the treatment reduces intimate partner violence. None of these studies has examined the impact of
the treatment on parenting behaviors or on the well-being of children in the family. Behavioral couples treatment is a dyadic intervention used to treat adults with substance abuse disorders. Studies of this intervention, including several large, federally funded randomized controlled clinical trials, have found significant reductions in both alcohol use and violent behaviors among both males and females (Fals-Stewart et al., 2005, 2009). Domestic violence-focused couples treatment is aimed at eliminating all forms of violence (psychological, physical, sexual, and stalking); promoting self-responsibility; and, if the couple chooses to remain together, enhancing their relationship (Stith and McCollum, 2009; Stith et al., 2012). Finally, the Couples Abuse Prevention Program is a cognitive-behavioral treatment intended to address the risk factors for intimate partner violence in couples with a history of minor to moderate physical and/or psychological aggression when there is no threat of imminent harm (LaTaillade et al., 2006). The small number of studies that have assessed these approaches have found that they decreased future violence and risk factors for violence (LaTaillade et al., 2006; Moore, 2012). None of these studies looked at the process for such change, for whom the interventions are successful, or how they work with different cultural groups. Based on the preliminary results from these small-scale studies, the federal government funded two randomized trials of systemic interventions to prevent intimate partner violence: Couples Together Against Violence (CTAV) and Couple Care for Parents (CCP). One study showed improvements in relationship satisfaction for both men and women in CCP relative to participants in a mother-focused program, but found little effect on parenting outcomes (Petch et al., 2012).
Although therapy for couples experiencing intimate partner violence is relatively new, there is a long history of therapy for couples experiencing high levels of conflict without intimate partner violence (Gottman et al., 2010). While little of this therapy has undergone evaluation, experimental studies have found that therapies based on cognitive-behavioral principles can reduce verbal aggression and coercion and help couples develop more positive ways of interacting with each other (Shadish and Baldwin, 2005).
Home visiting Few home visiting programs have focused on reducing intimate partner violence as an outcome, although studies have found that up to 48 percent of the women receiving such services have reported incidents of domestic violence since the birth of the study child (Eckenrode et al., 2000). One randomized follow-up study found that the positive effects of home visitation were reduced when a mother was experiencing intimate partner violence, and for those experiencing high rates of intimate partner violence, the beneficial effects of home visiting in terms of preventing child abuse disappeared completely (Eckenrode et al., 2000).
A number of clinicians and advocates have proposed that all home visiting programs be redesigned to address intimate partner violence and that home visitors be trained accordingly (Futures Without Violence, 2010). Home visitors well trained in the dynamics of intimate partner violence might be able to identify situations involving intimate partner violence, link mothers to appropriate community resources, and help the mother improve her safety and the safety and stability of her children. In recent years, a small number of home visiting programs have been developing, implementing, and testing interventions designed specifically to address intimate partner violence as part of the home visitor’s activities (Chamberlain, 2014; Futures Without Violence, 2010; Sharps et al., 2013). Few of these interventions have as yet been evaluated. Results from an evaluation of the Enhanced Yakima County Nurse-Family Partnership at Children’s Village in Yakima, Washington, indicate decreased family conflict/family management problems, improved parent-child interaction, and reduced child maltreatment (Yakima Valley Farm Workers Clinic, 2013).
Many home visitors, however, are not well trained in recognizing intimate partner violence. They may have a suspicion that it is occurring based on the child’s or caregiver’s behavior. But confirming this suspicion presents significant challenges. The visitor may encounter hostility from one or both caregivers if the issue is raised. Furthermore, many professionals who work with young children have not been trained to communicate effectively with women victimized by domestic violence and thus may be uncomfortable having such conversations. There is concern that without training, a home visitor may make an inappropriate report of child abuse or neglect that results in the needless separation of a nonoffending mother and her child.
Parents with Developmental Disabilities
Although exact numbers are not available, many of the estimated 15 percent of children and adolescents with developmental disabilities (Boyle et al., 2011) go on to become parents. Whether and the extent to which such disabilities may impair parenting has been a subject of debate over many years (Reinders, 2008).
Several studies have examined the predictors of success or difficulty in parenting for individuals with intellectual disabilities. To differentiate “high-risk” and “low-risk” parents with such disabilities, McGaw and colleagues (2010) conducted a secondary analysis of data on a sample of mothers and children from the United Kingdom. They found that risk was not predicted by intellectual ability; rather, the major predictors were mothers’ reports of their own trauma in childhood, the presence and characteristics of their partner, other special needs the parent might have, and special needs of the children.
For many parents, individualized programs based on assessment of needs, level of stress in everyday life, and parenting skills appear beneficial (Aunos et al., 2008). Systematic reviews of experimental and quasi-experimental efficacy studies (Feldman, 1994; Wade et al., 2008) indicate that home-based, didactic programs can result in improved childrearing skills for parents with developmental disabilities, although the effects on family functioning and other family measures remain unexamined. A Cochrane review by Coren and colleagues (2011) found three randomized controlled studies of such programs that met their criteria for inclusion. First, in a Canadian sample of mothers with intellectual disabilities and their children, Feldman and colleagues (1992) implemented a home-based individualized intervention to teach the mothers infant and child care skills, and found significantly more competent parenting in child care routines during the day at postintervention and follow-up. Working with mothers with such disabilities in the United States, Keltner and colleagues (1995) developed and implemented the Support to Access to Rural Services intervention, which focused on building sensitivity to children’s cues; increases in maternal-child interaction, including providing children with verbal feedback, were seen at 12 months postintervention. A third program for parents with intellectual disabilities, conducted in Australia, delivered a home-based intervention focusing on child health and home safety, finding significantly more positive health outcomes for children in the experimental group (Llewellyn et al., 2003). Finally, although falling below the scientific threshold for inclusion in a Cochrane review because it employed only a single-group, pretest-posttest design, an adaptation of Triple P was provided to a group of Belgian parents with intellectual disabilities. All parents completed the program and reported significant reductions in psychological stress, maladaptive parenting, and child conduct problems (Glazemakers and Deboutte, 2013).
Adolescent Parents
While adolescent childbearing (births to a mother between the ages of 15-19) in the United States has fallen to an historic low in recent years,6 6 percent of live births were to females under age 20 in 2014 (Hamilton et al., 2015). Most adolescents who give birth are 18 or older; in 2014, about 73 percent of adolescent females who gave birth were ages 18-19, while 23 percent were 16-17 and 4 percent were 15 or under (Hamilton et al., 2015). It is estimated that 77 percent of births to 15- to 19-year-olds during 2006-2010 were unintended (Mosher et al., 2012).
Pregnant adolescents and adolescent parents may need special attention and support with respect to parenting for a number of reasons. Relative to older females, pregnant adolescents are less likely to receive adequate prenatal care and are more likely to smoke and have inadequate nutrition during pregnancy, posing risks to the development of the fetus. Adolescent parenthood also is associated with worse mental health outcomes among mothers, which may affect the parent-child relationship (Anderson and McGuinness, 2008; Boden et al., 2008; Hodgkinson et al., 2010, 2014; Siegel and Brandon, 2014). In particular, having a child during adolescence is associated with poorer mental health in mothers, including depression, suicidal ideation, anxiety disorders, and PTSD, both prenatally and postpartum (Anderson and McGuinness, 2008; Boden et al., 2008; Hodgkinson et al., 2010, 2014; Siegel and Brandon, 2014). While adolescent parenthood does not necessarily end the mother’s education or pursuit of career or other goals (Assini-Meytin and Green, 2015; Gruber, 2012), adolescent mothers compared with their nonparent peers are much more likely to drop out of high school, although many go on to complete their general education diploma (GED) (Jutte et al., 2010; Perper et al., 2010). Adolescent mothers and fathers also are more likely than those who have children at a later age to face poverty and unemployment and to depend on welfare (Asheer et al., 2014).
Many adolescent mothers (12-49%, according to one study [Meade and Ickovics, 2005]) become pregnant for a second time within 1 year of a first delivery. In 2014, 17 percent of births to 15- to 19-year-olds were to females who already had one or more children (Hamilton et al., 2015). These rapid repeat pregnancies have been linked to even poorer health, education, and economic outcomes for adolescent mothers and their children (Chen et al., 2007; Hoffman and Maynard, 2008; Manlove et al., 2000; Stevens-Simon et al., 2001). Accordingly, avoiding repeat births among adolescents is a goal of federal initiatives such as the Office of Adolescent
___________________
6 The birth rate for teenagers fell 9 percent between 2013 and 2014 among females ages 15-19. The rate has declined 42 percent since 2007 (the most recent peak) and 61 percent since 1991 (Martin et al., 2015).
Health’s Pregnancy Assistance Fund grants to states and tribes (Office of Adolescent Health, 2015).
The children of adolescent parents relative to those of older parents are more likely to be born preterm and at a low birth weight and have a greater risk of developmental challenges (Chen et al., 2007; Pinzon et al., 2012). In longitudinal research, children born to adolescent mothers on average fare worse in cognitive, academic, and behavioral domains during childhood and adolescence relative to those born to older parents. They also have worse employment outcomes and are at higher risk for mental illness and substance abuse in adulthood (Dahinten et al., 2007; Morinis et al., 2013; Pogarsky et al., 2006). The children of adolescent parents themselves are more likely than their peers with older parents to become parents during adolescence (Meade et al., 2008; Pogarsky et al., 2006; Wu et al., 2012).
For many underserved adolescents, pregnancy and parenthood represent an opportunity to enter a comprehensive system of supportive care that can address multiple needs for themselves and their children. Some researchers argue that the experience of parenthood orients many adolescent parents toward self-improvement and enhances their sense of responsibility, making this an important time for intervention (Gruber, 2012; Hotz et al., 2005; Shanok and Miller, 2007).
The core parenting knowledge, attitudes, and practices for adolescent parents are not different from those for other parents. As described above, however, adolescent parents are at increased risk for adversities that affect their parenting capacity. Strategies discussed below that are used in evidence-based and evidence-informed interventions have targeted some of these risks, focusing on preventing rapid repeat births, promoting economic self-sufficiency, and improving birth and developmental outcomes for children of adolescents. Multigenerational approaches also are discussed, as many adolescent parents reside with their own parents or other individuals who may play a role in the parenting and development of young children.
The Nurse-Family Partnership
The Nurse-Family Partnership (NFP), discussed in the previous chapter, is an evidence-based program involving prenatal and postpartum home visitation by nurses for low-income first-time mothers, many of whom are adolescent. Home visits begin as early as the mother’s first trimester and continue until the child’s second birthday. Among NFP’s many objectives are to promote the economic self-sufficiency of young mothers by supporting educational attainment and employment and delaying subsequent pregnancy. NFP also aims to improve child health and development (Middlemiss and McGuigan, 2005).
A number of experimental studies have found participation in NFP to be associated with a decrease in rapid-succession second pregnancies (Bouris et al., 2012; Conroy et al., 2013; Kitzman et al., 2000; Olds et al., 2004, 2007). In one relatively large randomized trial involving primarily adolescent mothers, those who received NFP home visits had fewer births and longer intervals between births of first and second children at 7-year followup compared with mothers who did not receive visits (Olds et al., 2007). In general, NFP has been found to have little to no effect on indicators of continued education, such as graduation from high school and highest level of education completed for parents. However, some studies have found positive short- and long-term effects on indicators of family economic self-sufficiency, such as reduced use of Temporary Assistance for Needy Families (TANF) and the Supplemental Nutrition Assistance Program (SNAP, formerly the Food Stamp program) (Administration for Children and Families, 2015). Studies of NFP that have evaluated birth outcomes generally have found no effects on gestational age or birth weight, but have found longer-term positive effects for children in the areas of school readiness, substance use, and adolescent parenthood years postintervention (Administration for Children and Families, 2005). In addition, several experimental evaluations of NFP have found positive effects on parenting related to the knowledge, attitudes, and practices identified in Chapter 2, including using appropriate discipline and creating a safe home environment.
The Adolescent Parenting Program
The Adolescent Parenting Program (APP), rated by CEBC as having a “promising” level (3) of research evidence, provides support to first-time pregnant and parenting adolescents who are enrolled in school or a GED-completion program and their children ages 0-5 (California Evidence-Based Clearinghouse, 2016a). Through intensive monthly home visiting (using either the Partners for a Healthy Baby or Parents as Teachers home visiting curriculum), goal-setting and case management services, and peer group education, APP aims to delay subsequent pregnancies and increase graduation and GED completion rates, as well as enrollment in postsecondary education or vocational training, employment, and safe and stable housing. APP also focuses on improving the developmental outcomes of the young children of adolescent parents through prenatal and postnatal support (California Evidence-Based Clearinghouse, 2014).
In a 2006 quasi-experimental study of 2,520 adolescent pregnant and parenting females, participation in APP was associated with significantly longer intervals between first and second births and increased likelihood of normal birth weight and full-term birth. The groups had similar rates of use of prenatal care (Sangalang et al., 2006). The authors point to case
management and provision of direct services as central to helping adolescent mothers postpone subsequent births and achieve favorable birth outcomes (Sangalang et al., 2006). In a more recent study, APP graduates were found to have greater enrollment in higher education, job stability, and focus on career goals relative to other adolescent parents, but the study was not experimental and involved a very small number of participants (Gruber, 2012). In another nonexperimental study, a pre- and postintervention comparison showed improvement in use of contraception and parenting knowledge postintervention among 91 adolescents participating in APP (Sangalang and Rounds, 2005). Although research on APP to date has yielded promising initial findings, further experimental research with larger study populations is needed to confirm those findings.
Other evidence-based home visiting programs that likely reach a large number of adolescent parents (e.g., Family Check-Up, Home Instruction for Parents of Preschool Youngsters [HIPPY], Durham Connects) also have shown positive child health and developmental outcomes, but fewer positive effects have been observed for parents’ economic self-sufficiency (see Table 4-1 in Chapter 4).
Computer-Assisted Motivational Interviewing
Computer-assisted motivational interviewing (CAMI) is another intervention used with adolescent mothers to reduce rapid repeat births by promoting consistent use of condoms and other forms of contraception. It has been rated by CEBC as having a promising level of evidence (California Evidence-Based Clearinghouse, 2016d). CAMI entails at least two 60-minute sessions conducted in two parts by trained counselors, who meet one on one with pregnant and parenting adolescent mothers in the home or in a community agency or outpatient clinic. In one study, adolescents randomized to CAMI plus intensive home visiting or CAMI only who participated in sessions at quarterly intervals until 2 years postpartum had nonsignificantly lower birth rates compared with participants receiving usual care. Significant effects were seen for those adolescent mothers in the CAMI-only group who received two or more sessions of CAMI (Barnet et al., 2009). In a followup study with the same participants, adolescent mothers in the CAMI plus home visiting and CAMI-only groups had significantly reduced repeat births compared with those in the usual-care group (Barnet et al., 2010).
In an older, nonequivalent control group study of a multicomponent community-based intervention (the Family Growth Center [FGC]) designed to provide adolescent mothers in high-risk neighborhoods with a range of educational and support services for the prevention of rapid repeat pregnancy and school dropout, mothers participating in FGC followed over 3 years had a significantly lower rate of repeat pregnancy and signifi-
cantly higher rate of school completion compared with nonparticipating adolescent mothers. However, the study sample was very small (Solomon and Liefeld, 1998). FGC has received a rating of promising from CEBC (California Evidence-Based Clearinghouse, 2016f).
School-Based Interventions
Provision of parenting-related interventions and child care in the school setting may serve as a means of providing multidisciplinary services to adolescents while keeping them engaged in school, but additional research on the benefits of this approach is needed (Crean et al., 2001; Pinzon et al., 2012; Sadler et al., 2003, 2007). In one study, adolescent mothers and their children receiving on-site child care while participating in a school-based program that included parenting classes and referral services were found to have better school attendance than nonparticipants, with 70 percent and 28 percent, respectively, graduating from high school (Crean et al., 2001). Some states have implemented their own programs for pregnant and parenting adolescents in schools as well as home settings, with positive impacts on education (e.g., completion of high school) and economic self-sufficiency (National Association of County and City Health Officials, 2009). However, findings from evaluations of these programs often are not published in the peer-reviewed literature.
Multigenerational Households
As noted above, many adolescent parents live with their own parents or rely on family members for support in raising young children. Multigenerational households are becoming more common in the United States, especially among racial and ethnic minorities, but a dearth of research has examined the nature and quality of parenting in these homes. Preliminary research on multigenerational households indicates that parenting and child development are influenced by interactions between parents and grandparents in the household (Barnett et al., 2012). A few well-supported parenting programs, such as NFP, take family-level functioning into account, but the committee was unable to identify any comparisons of the use and nonuse of multigenerational approaches. The FGC model described above did include an explicit focus on involving the mothers of adolescent parents in the intervention (Solomon and Liefeld, 1998).
Summary
In summary, with the exception of NFP, many of the studies reviewed are limited by small sample sizes and lack of follow-up. Taken together,
the studies reviewed provide good evidence that intensive home visiting with adolescent mothers, as provided in NFP, APP, and CAMI plus home visiting, is effective for reducing rapid repeat pregnancy and improving birth and developmental outcomes in children of adolescent parents. While other strategies (e.g., motivational interviewing provided in one version of CAMI and services designed to address families’ multiple needs as provided in the FGC model) also show promise with respect to these outcomes, those preliminary findings need to be replicated. With respect to parent self-sufficiency, intensive home visiting in NFP is associated in several studies with improvements in indicators of economic well-being but not continued education, although CAMI and school-based interventions and child care have shown positive effects on continuation of schooling among adolescent mothers. As with research on parenting in general, fathers are underrepresented in evaluations of interventions to support adolescent parents. Finally, because many adolescent parents live with their own parents and rely on other family members to assist with childrearing, the lack of research on the effectiveness of multigenerational approaches is a gap in research on interventions for adolescent parents.
FAMILIES INVOLVED WITH CHILD WELFARE SERVICES
Child welfare services play a unique role in parenting policy and programming. They represent the only universal set of services addressing parenting in every state. These services are, however, a residual system. Child welfare services become involved with families when the quality of parenting falls below what society considers a minimally adequate threshold. The purpose of the services is to investigate allegations of child maltreatment and intervene when it is established that the quality of parenting is deficient and that as a result, the safety and/or basic physical or mental health of a child has been put at substantial risk. In a large percentage of substantiated cases of maltreatment, the threat to the child’s safety requires monitoring of the parent’s care; in almost a quarter of substantiated cases, the child is removed altogether from parental care, and parents must participate in parenting interventions if they want to regain custody.
The focus of child welfare services is protecting children’s safety, although once involvement with a family is initiated, the focus extends to enhancing children’s well-being. Parents involved with child welfare services are most often formally designated by “child neglect: failure to supervise” or “child neglect: failure to provide,” which indicates they have not addressed basic safety concerns, largely as the result of omission of effective parenting. Together, these designations represent more than one-half of child maltreatment reports (Administration for Children and Families, 2005; Casanueva et al., 2012). In about a quarter of all cases, the parent
has engaged in behaviors that constitute physical abuse; a smaller and declining percentage involve sexual involvement with the child by the parent or a family member.
Even though child welfare services are recognized as a last-resort or residual response for children whose parents are not meeting their responsibility to provide a safe home environment, some contact with these services is now broadly experienced. In 2014, an investigation or other intervention by child welfare services was conducted for more than 3 million children (a rate of 42.9 per 1,000 children) (Administration for Children and Families, 2016). Approximately 702,000 of these children (a rate of 9.4 per 1,000 children) were determined to have a substantiated or indicated finding of abuse and/or neglect (Administration for Children and Families, 2016). A study in California found that 5.2 percent of all children younger than age 1 are reported for child maltreatment each year (Putnam-Hornstein et al., 2015), and 2.1 percent of children experience confirmed maltreatment by age 1 (Wildeman et al., 2014). Although national data are lacking on the reasons for these reports, they appear to be strongly associated with maternal substance abuse (Wulczyn et al., 2002).
These findings reflect yearly contacts. Taking a longitudinal perspective, one study concluded that one in eight children experience a substantiated instance of maltreatment by age 18, and nearly 6 percent do so by age 5 (Wildeman et al., 2014). For African American children, the latter figure is 1 in 5, and for Native American children, it is 1 in 7 (Wildeman et al., 2014). Within some subpopulations—for example, the children of young adult parents who were clients of child welfare services as children—interaction with child welfare services is experienced by more than one-half of children (Putnam-Hornstein et al., 2015).
The Impact of Inadequate Parenting on Children
In addition to threats to their safety, the children involved with child welfare services have high rates of behavioral and developmental problems—about twice the rates found among children in the general population (Burns et al., 2004; Casanueva et al., 2012). The largest study of children receiving child welfare services—the National Survey of Child and Adolescent Well-Being (NSCAW)—found that at the time of entry into child welfare, about one-third (37%) of children had a mental or medical condition with a high probability of resulting in developmental delays and/or of being 2 or more standard deviations below the mean in at least one developmental area or 1.5 standard deviations below the mean in two areas (Casanueva et al., 2014). Among children ages 0-2, 3-5, and 7-10, only 83 percent, 84 percent, and 78 percent, respectively, were in very good or excellent health. Among children ages 3-5, fully 15.7 percent were reported
by their parents as having behavioral problems in the clinical range on the Child Behavior Checklist (CBCL) (Achenbach, 1991a; Achenbach and Rescorla, 2001). Among children ages 6-17, a significantly higher proportion (about 26%) had a score in the clinical range for behavioral health problems (as measured by the CBCL), about three times what would be expected in the general population (Achenbach, 1991b).
The Impact of Child Welfare Services
A full evaluation of the functioning of child welfare services is beyond the scope of this report, but a number of issues related to these services have been identified in prior IOM and NRC reports (Institute of Medicine and National Research Council, 2014; National Research Council, 1993). As noted in those and many other reports, agencies providing child welfare services throughout the country face many challenges both in protecting the long-term development of children and in providing adequate services to parents.
Given the scope and impact on children of parental behaviors constituting “maltreatment,” it is essential that these parents receive high-quality parenting interventions. An effective response by child welfare services is especially needed for parents of young children. It appears clear, however, that too many families are not receiving effective services. A large proportion of children—perhaps exceeding 80 percent—remain in the home following the initial report to child welfare services (Institute of Medicine and National Research Council, 2014). A recent California using a longitudinal dataset of birth and child protective service records found that nearly 70 percent of infants who received ongoing in-home family child welfare services were re-reported during the first 5 years (Putnam-Hornstein et al., 2015). Infants whose reports were screened out were as likely to be re-reported as those who received services. This finding is consistent with decades of research showing that the future risks for “unsubstantiated cases” remain high (e.g., The Center for Community Partnerships in Child Welfare, 2006; Drake and Jonson-Reid, 1999a, 1999b).
Caregiver instability is a significant factor in the lives of children who have been maltreated and reported to child welfare services. Even though most infants who come to the attention of child welfare services do not go immediately into foster care, Casanueva and colleagues (2012) in an analysis of longitudinal data from the NSCAW found that nearly all such infants (about 86%) had one or more changes in caregivers by the end of 2 years, and approximately 40 percent had four or more placement changes between infancy and entering school.
Children of any age with child welfare services involvement have a high risk of continuing to experience developmental, cognitive, and behavioral
health problems regardless of whether they are placed in foster care or provided with ongoing services (Dolan et al., 2012). In another NSCAW analysis that followed 5,872 children under the supervision of child welfare for a 5-year period, by 3-year follow-up, the proportion of children in any type of placement setting who had developmental problems remained largely unchanged from the high levels described above (Casanueva et al., 2014).
The impact of living in poverty is a critical factor. After controlling for maltreatment type and severity, demographic traits, and a few caregiver characteristics, the NSCAW revealed that infants who had remained in foster care for the first 5 years of life were developing more slowly than children who had been returned home or adopted (Lloyd and Barth, 2011). Living in poverty in the final setting in which they were studied predicted decreased cognitive development as well as academic problems and tended to explain behavioral health. The well-being of children was powerfully influenced by ongoing exposure to poverty, regardless of the poverty level in which they lived at the time of original placement or the placement type at the end of placement.
Intervention Strategies
According to the NSCAW, in about two-thirds of cases that enter child welfare services, a recommendation for parent training is made, and nearly three-fourths of cases also involve a referral for mental health counseling or substance abuse treatment for the caregiver (Dolan et al., 2011). The form of parent training is rarely specified, and no assessment is made of whether parenting improved as a result of the training; at most, the courts learn only whether parents have attended parenting classes (Barth et al., 2005).
While parent training has always been common for families receiving child welfare services, those services have lagged behind other mental and physical health services both in the assessment of interventions and in the adoption of evidence-based practices. In the past, lack of access to research-based information about the effectiveness of parent training programs and limited comfort with selecting and implementing evidence-based interventions resulted in sluggish adoption of these practices among child welfare services (Horwitz et al., 2009). It was not until 2004 and thereafter, when resources such as the Journal of Evidence-Based Social Work and CEBC became available that information on effective practices became more widely available. As recently as 2006, a Cochrane review of parenting programs for the treatment of physical child abuse and neglect (Barlow et al., 2006) found insufficient evidence to support the use of the reviewed programs, although limited evidence showed that some programs could be effective in addressing outcomes associated with physically abusive parenting practices.
Recent years have seen much greater focus on the use of evidence-based practices among child welfare agencies, perhaps reflecting increased federal policy direction and support for the use of these practices. In some cases, agencies are adopting evidence-based programs used in helping parents not involved with the child welfare system, such as Incredible Years, sometimes adapting the program to better meet the characteristics of families that are involved with the system. Interventions also have been developed specifically for parents involved with child welfare services. Given that the implementation of evidence-based practices is relatively new in child welfare services, the literature on evidence-based strategies to support these families is emergent.
Skills Training and Family-Centered Treatment for Families with a History of Child Maltreatment or with Child Maltreatment Risk Factors
Three parent skills training programs reviewed earlier (PCIT, Incredible Years, and Triple P), often delivered in a group setting, have been found in randomized controlled studies to be suitable for implementation in the child welfare context (Linares et al., 2006, 2012, 2015) and effective for reducing child abuse recidivism and coercive and punitive discipline practices (Chaffin et al., 2004, 2011), as well as reducing parental stress associated with childrearing and increasing parental confidence. A high cost for the Incredible Years materials and a small number of approved trainers have slowed the adoption of Incredible Years by child welfare services—a problem that applies as well to other evidence-based practices (Powers et al., 2010).
A number of programs have been designed specifically for families involved with child welfare services. ABC (Attachment and Bio-Behavioral Catch-up) is an evidence-based home visiting intervention (CEBC evidence rating of 1) that utilizes videotape feedback to teach parenting skills over a 10-week period (California Evidence-Based Clearinghouse, 2016c). The program helps caregivers reinterpret children’s behavioral signals to offer more nurturance, provide a responsive and predictable environment to help children with self-regulation, follow their child’s lead, and decrease the use of behaviors that overwhelm and frighten the child. Randomized controlled research has shown that children in families who participate in the intervention are less disorganized in their attachment with their parents and display less sadness and anger compared with controls (Bernard et al., 2012). The attitudes and behaviors that change as a result of receiving ABC are, arguably, fundamental to helping parents and children reduce stress-inducing interactions and enhance parent-child closeness. There is, however, no direct evidence that child maltreatment is lowered by such approaches.
Another program, discussed in Chapter 4, SafeCare® (Lutzker and Chaffin, 2012) (CEBC rating of 2), was designed for parents whose children had been reported for neglect and who needed explicit, easily implemented strategies for improving home safety and increasing the use of needed medical or behavioral interventions (California Evidence-Based Clearinghouse, 2016l). During weekly or biweekly sessions, home visitors conduct baseline and follow-up assessments, observations, and trainings with parents and provide parents with feedback. The trainings focus on practices related to reducing the incidence of child maltreatment, enhancing home safety and supervision, and improving the parent-child relationship. SafeCare home visitors are required only to have a bachelor’s degree, and the program uses competency-based training approaches that make its replication highly dependable and scalable. SafeCare has been the focus of considerable implementation research—including studies focused on variation in supervision, American Indian populations, and culturally enhanced training methods for working with Latino professionals and parents (Beasley et al., 2014). In randomized and single group pre-post design studies, caregivers who participate in SafeCare have been found to be less likely to abuse their children. Participation also is associated with improvements in home safety (Chaffin et al., 2012; Gershater-Molko et al., 2002, 2003). In a small pilot study of SafeCare that incorporated use of flash cards to improve parents’ knowledge of developmental milestones—one of the core knowledge areas identified in Chapter 2—the intervention was found to be effective in improving parental knowledge in this area; however, the findings of this study are preliminary, and additional research is needed (Guastaferro, 2011).
Multisystemic Therapy for Child Abuse and Neglect (MST-CAN) (CEBC rating of 2) and Trauma Adapted Family Connections (TA-FC) are programs used with caregivers and/or children who have experienced trauma. Both programs work with the entire family to address concerns in the home so as to keep children safe (California Evidence-Based Clearinghouse, 2016i).
MST-CAN is an adaptation of MST for child welfare-involved families that is supported by research evidence for children ages 6-17 (Swenson and Schaeffer, 2011; Swenson et al., 2010) and founded on basic principles of care coordination. Treatment entails safety planning, cognitive-behavioral therapy for managing anger and addressing the impact of trauma, counseling for adult substance misuse, family therapy, and getting parents to take responsibility for events that brought the family to child protection. Research indicates that MST-CAN is significantly more effective than enhanced outpatient treatment in reducing parents’ psychiatric distress and behaviors associated with maltreatment, increasing parents’ social support, improving children’s mental health symptoms, and reducing children’s out-
of-home placements and changes in children’s placement. Yet no statistically significant difference was found for incidents of reabuse among participants and families receiving outpatient treatment in a randomized effectiveness trial (Swenson et al., 2010). One evaluation showed that MST was effective in addressing the dual needs of families involved with child welfare services and substance abuse (Swenson et al., 2009).
TA-FC builds on the service components of the Family Connections model, a promising program (CEBC rating of 3) designed to reduce risk factors for child maltreatment through family assessment and individual and family counseling, emergency assistance, and service planning and referral (California Evidence-Based Clearinghouse, 2016e). TA-FC integrates a focus on trauma into family assessment and counseling, such as by assisting families with identification of trauma symptoms and teaching trauma-informed parenting practices (Collins et al., 2011, 2015). TA-FC has not identified specific parenting knowledge, attitudes, and practices that may be the active ingredient in reducing the likelihood of maltreatment, but pilot noncontrolled evaluation of the program demonstrates reductions in child problem behaviors (Collins et al., 2011, 2015). Even though this is not the explicit program target, these findings suggest that reducing parental stress, recognizing and addressing a range of parental risk factors, and matching services (e.g., special education) to parents can benefit family functioning (DePanfilis et al., 2008).
Supporting Foster and Kinship Families to Improve Placement Stability
Many children involved with child welfare services are placed with relatives or nonrelative foster parents. Foster and kinship providers often need training in parenting skills that addresses the unique challenges associated with parenting children who have experienced maltreatment. Treatment Foster Care Oregon for Preschoolers (TFCO-P) (Chamberlain and Fisher, 2003; Fisher et al., 1999) is a well-supported treatment model (CEBC rating of 2) designed for children ages 3-6 (California Evidence-Based Clearinghouse, 2016m). The intervention is delivered through a treatment team approach that incorporates training and ongoing consultation with foster parents, skills training and therapeutic playgroups for children, and family therapy for birth parents, with the goal of promoting secure attachment with foster parents and successful permanent placement with birth parents or through adoption. Randomized controlled evaluations comparing TFCO-P with conventional foster care have shown that children who experience the consistent, contingent, responsive parenting that is taught in TFCO-P, along with other services, have reduced rates of problem behaviors (as reported daily by the foster parents), and the foster parents demonstrate less stress. As a result, children in TFCO-P have more stable
placements relative to those in conventional foster care (Fisher et al., 2005, 2006, 2009, 2011a).
Keeping Foster and Kin Parents Supported and Trained (KEEP) (CEBC rating of 3) is a derivative of Multidimensional Treatment Foster Care created for use with children of elementary school age who are in out-of-home care supervised by child welfare services (California Evidence-Based Clearinghouse, 2016h). The program model includes weekly group work among foster families to learn effective parenting methods and daily or weekly calls to check on problems with parenting, which are addressed using a flexible curriculum (Price et al., 2009). KEEP is being implemented with diverse populations in both urban and rural areas in a number of states. Randomized controlled research has found foster family satisfaction and improvements in child behavior and placement outcomes (e.g., chances of a child being reunited with his or her biological parents) (Chamberlain et al., 2008; Price et al., 2009), although a replication study does not show effects of the same size (Greeno et al., 2016). A program modeled after KEEP showed increased positive behavior for foster youth in Chicago (Leathers et al., 2011), and KEEP for preschoolers is under development as a plausible alternative to TFCO-P.
Knowledge, Attitudes, and Practices and Child Welfare Services
The knowledge, attitudes, and practices needed by parents who become involved with child welfare services are not different from those needed by other parents. Knowledge of child development generally is considered a necessary precursor to reducing maltreatment. Evidence indicates that maltreating parents often have unrealistic expectations for what a child is able to do and may misinterpret a young child’s actions and/or lack of capacity as intentional. Further, parents who are depressed or angry about other matters may be more likely than those who are not to view their children’s behavior as controllable and negatively intended (Leung and Slep, 2006). Yet changes in parental attitudes are not well articulated as a mediator of the effectiveness of parenting training in achieving better outcomes with respect to child maltreatment. Even when modest changes in knowledge are achieved, an impact on reducing future child maltreatment is not highly likely given the array of adverse influences on parents’ responses to their children’s perceived misbehavior. As demonstrated by studies referenced above, parenting programs based heavily on providing information are typically outperformed by those with more of a behavioral focus (e.g., ABC, SafeCare, PCIT).
Improving the executive functioning, actions, and circumstances of parents is necessary for avoiding neglect and abuse, as is developing alternatives to neglectful and abusive practices (Knerr et al., 2013; Leung and
Slep, 2006). None of the programs reviewed here focus on specific measurement of attitude change as an indicator of whether progress is being made; instead, the programs require demonstration of desired behaviors during the course of treatment. A potential limitation of current approaches for families with a history of or at high risk for child maltreatment is that, with the exception of ABC, they generally do not address how parents’ current parenting styles developed or what trauma they themselves experienced as children or parents, although ABC does systematically explore the way experience as a child affects parents’ views about parenting.
Emerging knowledge about the core components that make evidence-based practices successful can support the broader distribution of what works, earlier rather than later, to the parents who need it the most. Barth and Liggett-Creel (2014) explored the common elements of programs for parents of children ages 0-8 involved with the child welfare system by building on prior work in this area (Chorpita et al., 2005; Geeraert et al., 2004; Kaminski et al., 2008). In a review of well-supported interventions in CEBC, common elements were identifiable in training programs for parents of children ages 4-8, but far less so in programs for parents of children ages 0-3 (Barth and Liggett-Creel, 2014). CEBC includes four programs (Incredible Years, PCIT, PMT-Oregon [PMT-O], and 1-2-3 Magic) with a very similar history and operational components for the older age group. Common treatment elements include being offered in a clinic setting (two of the four are also offered in the home to allow for practicing newly acquired skills) and the use of a group format. All four models have social learning theory as their foundation. PCIT also uses attachment theory to guide its work. The use of social learning theory across the four models and the core set of parenting skills taught (i.e., attending, positive reinforcement, and use of time-out) means that certain common practice elements are likely to contribute to the success of interventions for child abuse and neglect.
SUMMARY
The following key points emerged from the committee’s review of evidence-based and evidence-informed interventions for parents of children with special needs, parents facing special adversities, and parents involved with child welfare services.
Parents of Children with Special Needs
- The efficacy research on programs designed to promote different dimensions of parenting for young children with special needs suggests that efficacious programs and resources are available to support parenting knowledge, attitudes, and practices for these
parents. The strongest evidence is for programs that (1) teach parents how to support the learning and development of their children with disabilities, (2) promote positive parent-child interactions, and (3) focus on reducing the children’s problem behaviors. Some of these programs do appear to have secondary outcomes that affect the larger family system, such as increased parental optimism, decreased parental stress, and generalized changes in parenting style.
Parents of Children with Developmental Disabilities
- Research indicates the effectiveness of family interventions designed to reduce stress among parents of children with developmental disabilities, especially when such interventions occur over a relatively long period and have multiple components (e.g., a combination of group and individual elements).
- Instructional interventions that teach parents how to facilitate the language, social, and play skills of children with developmental disabilities are effective in achieving these outcomes, indicating that with appropriate supports, parents can help their children develop these skills. For parents of children with ASD, instructional interventions focused on promoting children’s social-communication skills show positive effects on children’s cognitive development when they are based on a conceptual framework, address a variety of developmental needs, and occur over an extended period (1-2 years). Furthermore, interventions that involve parents appear to be more effective than other approaches for these children.
- Interventions that teach parents dialogic reading skills show positive impacts on the reading skills of young children with language delays.
- Interactional practice interventions that promote positive social interactions between parents and young children with disabilities by teaching parents how to arrange play in a way that encourages parent-child interaction and facilitates parental responsiveness have been found to improve responsive parenting and increase social interactions among these children.
- Parent training in support of positive behavior, such as that provided by the widely used Triple P and Incredible Years, including in a group format, is associated with improved parent-child interactions and reduced challenging behavior in children with developmental disabilities.
- Gaps in research and practice relevant to interventions for parents of children with developmental disabilities include the development and evaluation of interventions that take place in natural environ-
ments and that support parents and children during important life transitions, such as that from early intervention to preschool.
Parents of Children with Behavioral Challenges and Mental Health Disorders
- Active skills training with rehearsal for parents of children with externalizing behavior problems delivered in a series of one-on-one and/or group sessions in community-based settings (as in Triple P and Incredible Years) can lead to improved parent-child relationships, less frequent dysfunctional parenting (e.g., harsh discipline), improved parenting competence, and reduced child behavior problems. Multiple evaluations have found that therapy-based child management combined with play therapy (PCIT), delivered in weekly sessions in outpatient and clinic settings to teach parents the skills to encourage prosocial behavior in their children, improves parent-child interactions, imparts parenting skills related to gaining children’s compliance, and reduces parental stress, among other benefits. PCIT and cognitive-behavioral therapy have been found to be effective among parents of children with internalizing behavior problems such as anxiety and depression.
- Other interventions have focused directly on a particular type of externalizing or internalizing condition. More examples of these interventions exist for externalizing conditions, although efficacy studies for children with anxiety disorders also have been documented. Few interventions have been developed to help parents address childhood depression, perhaps because depression is a fairly low-prevalence disorder in children. However, the role of parents in moderating the effects of childhood depression and potential impacts on life outcomes certainly deserves more attention and activity in intervention research.
Parents of Children with Serious or Chronic Medical Illness
- Efficacious programs (e.g., COPE) are available to support families of children with critical illnesses that require hospitalization and intensive medical services. In general, much research has been conducted on support for parents within other portions of the health care sector, but such studies often are not well powered and lack adequate evaluation. Data on long-term outcomes and on fathers are lacking, and both of these areas deserve increased attention.
Parents of Very Low-Birth Weight, Premature Infants
- Research on mothers of very-low-birth weight infants shows that interventions designed to encourage and support interactions and physical contact between mothers and infants result in improved mother-infant relationships, better maternal mood, and reduced anxiety.
Parents Facing Special Adversities
- Common barriers to receipt of support for parents facing special adversities are stigma, such as that which can be associated with having a mental illness, substance abuse disorder, or other condition; concerns that because of one’s mental health, substance use, or other condition, or because of a history of maltreatment, one will be reported to child protective services; and distrust of service providers.
Parents with Mental Illness
- Recognition of individuals with mental illness as also being parents is frequently lacking among service providers.
- There have been few high-quality large-scale evaluations of interventions designed for parents with mental illness, especially those with serious mental illness.
- For parents with depressive disorders, interventions that combine mental health treatment and parenting support lead to better outcomes in terms of reducing psychiatric symptoms and increasing maternal responsiveness relative to programs focused solely on mental illness.
- Integrating parenting interventions and support into primary care may be an effective way of diagnosing and treating parents’ mental health issues. The perinatal period appears to be an opportune time to reach a broad population of parents.
- Research provides preliminary evidence that home visiting programs that include therapy for parental depression improve parental mental health and parenting. Yet many home visiting programs do not include mental health as an objective, and further research is needed to confirm these preliminary findings. Efforts within Early Head Start and public health settings also show promising effects on depression, parenting practices, and child behavior, but further research on these efforts is needed as well.
- Research on strategies for supporting parents with severe mental illness who may need ongoing and intensive support is lacking. Some evidence indicates significant benefits for the parenting skills of parents with severe mental illness and the behavior of their children from interventions involving home visits, parenting lectures, and clinician counseling. Triple P in particular has shown promise, and intensive outpatient or inpatient treatment (e.g., in mother-baby mental health units) may be effective as well. Available data on interventions and treatment for parents with severe mental illness indicate an association with significantly reduced risk that children will develop the same mental health problems.
Parents with or Recovering from Substance Use Disorders
- Mothers who are permitted to reside with their children during substance abuse treatment are more likely to enter, remain in, and complete treatment and remain drug free for longer. Evaluations of specific residential treatment programs show improved parent-child relationships as well as child outcomes.
- FTDCs that provide parents with access to substance abuse treatment along with accountability, support, and rewards and sanctions aimed at regaining child custody result in improved entry into and completion of treatment. Children of parents participating in these programs are more likely to be reunited with their parents relative to children of nonparticipants. However, these findings may be biased by the fact that women who enter FTDCs may be more motivated to change their behavior than women who do not enter these programs.
- Few targeted parenting interventions have been developed for parents who have or are recovering from a substance abuse disorder. However, available evidence indicates that combining substance abuse treatment with parenting intervention improves parenting beyond the improvement achieved with substance abuse treatment alone. Parents may benefit most when instruction in specific parenting techniques is preceded by instruction in psychological coping strategies.
- Data from evidence-based parenting programs (Strengthening Families and the Nurturing Parent Program) indicate that family skills training in residential, day treatment, and FTDC settings that emphasizes reducing parents’ alcohol and drug use while helping them learn new patterns of parenting results in reduced substance use and also is associated with improved parenting (involvement, supervision) and less family conflict and child maltreatment. In
-
addition, therapy in outpatient mental health settings designed to improve family relationships and communication and child management is associated with improvements in family relationships and other outcomes.
- Substance use can interfere with parent-child attachment. Preliminary data from pilot studies show that parent coaching sessions aimed at improving parents’ nurturing of young children provided in combination with substance abuse treatment improve attachment-related parenting behaviors.
- Findings from office- and home-based substance abuse treatment and case management programs for pregnant and parenting women focused on parenting, family planning, education, and other areas indicate that these programs are associated with reduced likelihood that a woman will give birth to a drug-exposed infant.
Parents Affected by Intimate Partner Violence
- Community programs for mothers, couples, and children experiencing intimate partner violence that target parenting and/or child outcomes have been found to be effective in reducing children’s behavior problems, mental health problems among both mothers and children, and maternal stress and improving parenting. Programs focused on reducing the effects of trauma in children have been found to be effective, but not through changes in parenting. There is little evidence that counseling services for men prevent further violence, and although more women are now being arrested for intimate partner violence, data on intimate partner violence perpetrated by women are scarce. With regard to couples involved in intimate partner violence who seek services, some research shows that PCIT with families reduces conflict between parents if the violence has ceased. Dyadic interventions designed to treat adults with substance abuse disorders (behavioral couples treatment) show reductions in alcohol use and violent behaviors among both men and women.
- Few home visiting programs have focused on intimate partner violence, but many women who receive home visiting services report incidents of domestic violence. Some home visiting programs are developing, implementing, and testing strategies for reducing intimate partner violence, but findings from evaluations of these strategies are not yet available.
- A small number of studies on programs for couples designed to prevent intimate partner violence have found that these programs can reduce future violence and violence risk factors, but these studies
have not assessed the process for change or how the intervention works with different cultural groups.
Parents with Developmental Disabilities
- Many parents with intellectual disabilities provide adequate caregiving and parenting for their young children, but for a substantial minority, programs providing support for child caregiving, health care, and home safety may be important. A moderate level of evidence suggests that these programs have positive effects. The Triple P program, which has been effective with other populations of parents, is being adapted for parents with intellectual disabilities.
Adolescent Parents
- Adolescents’ participation in intensive home visiting is associated with a reduction in rapid repeat pregnancies and improved birth and developmental outcomes in children of adolescent parents. Several studies have found that the intensive home visiting offered in NFP is associated with improvements in indicators of economic well-being. While other strategies (e.g., motivational interviewing and provision of services to address families’ multiple needs) also show promise in improving these outcomes, preliminary findings need to be replicated.
- Many adolescent parents face barriers to continuing their schooling, although many go on to complete their GED. There is some evidence that home visiting programs and school-based interventions that provide child care have positive effects on continuation of schooling among adolescent mothers, but further research in this area is needed.
- As with research on parenting in general, fathers are underrepresented in evaluations of interventions designed to support adolescent parents. Another gap in research on adolescent parents is the effectiveness of multigenerational approaches, given that many adolescent parents live with their own parents and rely on them and other family members to help with parenting.
Families Involved with Child Welfare Services
- Effective parenting programs in child welfare are rooted largely in social learning theory. They focus on encouraging the use of anticipatory guidance and timely attention to increase parents’ positive
- In families with a history of child maltreatment or at high risk for maltreatment, both skills training in home and community settings that involves observation and corrective feedback and multipronged family-system approaches that address trauma and other co-occurring challenges (e.g., substance use) can be effective for improving child behavior and the parent-child relationship, parents’ psychiatric distress, and behaviors associated with child maltreatment. In addition, successful interventions for prevention of child abuse and neglect appear to include detailed, active methods for increasing the frequency of effective parenting practices, often without much attention to how parents originally began to rely on ineffective methods.
- Training and ongoing consultation with foster and kinship families are associated with reduced rates of problematic behaviors among children in these family arrangements, indicators of attachment between caregivers and children, and greater placement stability.
behavior and, in turn, teach them to use these tools more effectively with their children. The underlying theory is that positive changes in children’s behavior will reinforce parents’ positive attitudes and beliefs about their children and about the possibility of successful parenting.
REFERENCES
Achenbach, T.M. (1991a). Manual for Child Behavior Checklist/2-3 and 1991 Profile. Burlington: University of Vermont Department of Psychiatry.
Achenbach, T.M. (1991b). Manual for Child Behavior Checklist/4-18 and 1991 Profile. Burlington: University of Vermont Department of Psychiatry.
Achenbach, T.M., and Rescorla, L.A. (2001). Manual for the ASEBA School-Age Forms & Profiles: An Integrated System of Multi-Informant Assessment. Burlington: University of Vermont, Research Center for Children, Youth, & Families.
Adamson, L.B., Bakeman, R., Deckner, D.F., and Nelson, P.B. (2012). Rating parent-child interactions: Joint engagement, communication dynamics, and shared topics in autism, Down syndrome, and typical development. Journal of Autism and Developmental Disorders, 42(12), 2622-2635.
Administration for Children and Families. (2005). National Survey of Child and Adolescent Well-Being (NSCAW): CPS Sample Component Wave 1 Data Analysis Report. Available: http://www.acf.hhs.gov/sites/default/files/opre/cps_report_revised_090105.pdf [January 2016].
Administration for Children and Families. (2016). Child Maltreatment 2014. Washington, DC: U.S. Department of Health and Human Services; Administration for Children and Families; Administration on Children, Youth and Families; Children’s Bureau.
Allen, M., and Larson, J. (1998). Healing the Whole Family: A Look at Family Care Programs. Washington, DC: Children’s Defense Fund.
Amato, P.R., and Keith, B. (1991). Parental divorce and the well-being of children: A meta-analysis. Psychological Bulletin, 110(1), 26-46.
American Association on Intellectual and Developmental Disabilities. (2013). Definition of Intellectual Disability. Available: http://aaidd.org/intellectual-disability/definition#.Vk35DHarTGg [October 2016].
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM5®) (5th ed.). Arlington, VA: American Psychiatric Association.
Ammerman, R.T., Putnam, F.W., Stevens, J., Bosse, N.R., Short, J.A., Bodley, A.L., and van Ginkel, J.B. (2011). An open trial of in-home CBT for depressed mothers in home visitation. Maternal and Child Health Journal, 15(8), 1333-1341.
Ammerman, R.T., Putnam, F.W., Altaye, M., Stevens, J., Teeters, A.R., and van Ginkel, J.B. (2013). A clinical trial of in-home CBT for depressed mothers in home visitation. Behavior Therapy, 44(3), 359-372.
Ammerman, R.T., Altaye, M., Putnam, F.W., Teeters, A.R., Zou, Y., and van Ginkel, J.B. (2015). Depression improvement and parenting in low-income mothers in home visiting. Archives of Women’s Mental Health, 18(3), 555-563.
Anda, R.F., Felitti, V.J., Chapman, D.P., Croft, J.B., Williamson, D.F., Santelli, J., Dietz, P.M., and Marks, J.S. (2001). Abused boys, battered mothers, and male involvement in teen pregnancy. Pediatrics, 107(2), E19.
Anderson, C., and McGuinness, T.M. (2008). Do teenage mothers experience childbirth as traumatic? Journal of Psychosocial Nursing and Mental Health Services, 46(4), 21-24.
Anticich, S.A.J., Barrett, P.M., Gillies, R., and Silverman, W. (2012). Recent advances in intervention for early childhood anxiety. Journal of Psychologists and Counsellors in Schools, 22(Special Issue 2), 157-172.
Arria, A.M., Mericle, A.A., Rallo, D., Moe, J., White, W.L., Winters, K.C., and O’Connor, G. (2013). Integration of parenting skills education and interventions in addiction treatment. Journal of Addiction Medicine, 7(1), 1-7.
Asheer, S., Berger, A., Meckstroth, A., Kisker, E., and Keating, B. (2014). Engaging pregnant and parenting teens: Early challenges and lessons learned from the evaluation of adolescent pregnancy prevention approaches. Journal of Adolescent Health, 54(Suppl. 3), S84-S91.
Assini-Meytin, L.C., and Green, K.M. (2015). Long-term consequences of adolescent parenthood among African-American urban youth: A propensity score matching approach. Journal of Adolescent Health, 56(5), 529-535.
Athanasopoulou, E., and Fox, J.R. (2014). Effects of kangaroo mother care on maternal mood and interaction patterns between parents and their preterm, low birth weight infants: A systematic review. Infant Mental Health Journal, 35(3), 245-262.
Aunos, M., Feldman, M., and Goupil, G. (2008). Mothering with intellectual disabilities: Relationship between social support, health and well-being, parenting and child behaviour outcomes. Journal of Applied Research in Intellectual Disabilities, 21(4), 320-330.
Azrin, N.H., McMahon, P.T., Donohue, B., Besalel, V.A., Lapinski, K.J., Kogan, E.S., Acierno, R.E., and Galloway, E. (1994). Behavior therapy for drug abuse: A controlled treatment outcome study. Behaviour Research & Therapy, 32(8), 857-866.
Azrin, N.H., Acierno, R., Kogan, E.S., Donohue, B., Besalel, V.A., and McMahon, P.T. (1996). Follow-up results of supportive versus behavioral therapy for illicit drug use. Behaviour Research & Therapy, 34(1), 41-46.
Babcock, J.C., Green, C.E., and Robie, C. (2004). Does batterers’ treatment work? A meta-analytic review of domestic violence treatment. Clinical Psychology Review, 23(8), 1023-1053.
Back, S.E., Sonne, S.C., Killeen, T., Dansky, B.S., and Brady, K.T. (2003). Comparative profiles of women with PTSD and comorbid cocaine or alcohol dependence. American Journal of Drug and Alcohol Abuse, 29(1), 169-189.
Bagner, D.M., and Eyberg, S.M. (2007). Parent-child interaction therapy for disruptive behavior in children with mental retardation: A randomized controlled trial. Journal of Clinical Child and Adolescent Psychology, 36(3), 418-429.
Bagner, D.M., Sheinkopf, S.J., Vohr, B.R., and Lester, B.M. (2010). Parenting intervention for externalizing behavior problems in children born premature: An initial examination. Journal of Developmental and Behavioral Pediatrics, 31(3), 209-216.
Bancroft, L., Silverman, J.G., and Ritchie, D. (2011). The Batterer as Parent: Addressing the Impact of Domestic Violence on Family Dynamics. Thousand Oaks, CA: Sage.
Barkley, R.A. (1997). Defiant Children: A Clinician’s Manual for Parent Training (2nd ed.). New York: Guilford Press.
Barlow, J., Johnston, I., Kendrick, D., Polnay, L., and Stewart-Brown, S. (2006). Individual and group-based parenting programmes for the treatment of physical child abuse and neglect. Cochrane Database of Systematic Reviews, 3, CD005463.
Barlow, J., Bennett, C., Midgley, N., Larkin, S.K., and Wei, Y. (2015). Parent-infant psychotherapy for improving parental and infant mental health. Cochrane Database of Systematic Reviews, 1, CD010534.
Barnard, M., and McKeganey, N. (2004). The impact of parental problem drug use on children: What is the problem and what can be done to help? Addiction, 99(5), 552-559.
Barnet, B., Liu, J., DeVoe, M., Duggan, A.K., Gold, M.A., and Pecukonis, E. (2009). Motivational intervention to reduce rapid subsequent births to adolescent mothers: A community-based randomized trial. Annals of Family Medicine, 7(5), 436-445.
Barnet, B., Rapp, T., DeVoe, M., and Mullins, C.D. (2010). Cost-effectiveness of a motivational intervention to reduce rapid repeated childbearing in high-risk adolescent mothers: A rebirth of economic and policy considerations. Archives of Pediatrics & Adolescent Medicine, 164(4), 370-376.
Barnett, M.A., Mills-Koonce, W.R., Gustafsson, H., Cox, M., and Family Life Project Key Investigators. (2012). Mother-grandmother conflict, negative parenting, and young children’s social development in multigenerational families. Family Relations, 61(5), 864-877.
Barrow, S.M., Alexander, M.J., McKinney, J., Lawinski, T., and Pratt, C. (2014). Context and opportunity: Multiple perspectives on parenting by women with a severe mental illness. Psychiatric Rehabilitation Journal, 37(3), 176-182.
Barth, R.P., and Liggett-Creel, K. (2014). Common components of parenting programs for children birth to eight years of age involved with child welfare services. Children and Youth Services Review, 40, 6-12.
Barth, R.P., Landsverk, J., Chamberlain, P., Reid, J.B., Rolls, J.A., Hurlburt, M.S., Farmer, E.M.Z., James, S., McCabe, K.M., and Kohl, P.L. (2005). Parent-training programs in child welfare services: Planning for a more evidence-based approach to serving biological parents. Research on Social Work Practice, 15(5), 353-371.
Batts, K., Pemberton, M., Bose, J., Weimer, B., Henderson, L., Penne, M., Gfroerer, J., Trunzo, D., and Strashny, A. (2014). Comparing and Evaluating Substance Use Treatment Utilization Estimates from the National Survey on Drug Use and Health and Other Data Sources. Washington, DC: Center for Behavioral Health Statistics and Quality.
Bavolek, S.J., Comstock, C.M., and McLaughlin, J. (1983). The Nurturing Program: A Validated Approach for Reducing Dysfunctional Family Interactions. Available: http://www.nurturingparenting.com/images/cmsfiles/the_nurturing_program_nimh_study.pdf [March 2016].
Bavolek, S.J., Henderson, H.L., and Schultz, B.B. (1988). Reducing Chronic Neglect in Utah. Salt Lake City: University of Utah, College of Health.
Bayer, J.K., Sanson, A.V., and Hemphill, S.A. (2006). Parent influences on early childhood internalizing difficulties. Journal of Applied Developmental Psychology, 27(6), 542-559.
Beardslee, W.R., Gladstone, T.R., Wright, E.J., and Cooper, A.B. (2003). A family-based approach to the prevention of depressive symptoms in children at risk: Evidence of parental and child change. Pediatrics, 112(2), e119-e131.
Beardslee, W.R., Ayoub, C., Avery, M.W., Watts, C.L., and O’Carroll, K.L. (2010). Family Connections: An approach for strengthening early care systems in facing depression and adversity. The American Journal of Orthopsychiatry, 80(4), 482-495.
Beardslee, W.R., Gladstone, T.R., and O’Connor, E.E. (2011). Transmission and prevention of mood disorders among children of affectively ill parents: A review. Journal of the American Academy of Child and Adolescent Psychiatry, 50(11), 1098-1109.
Bearss, K., Johnson, C., Handen, B., Smith, T., and Scahill, L. (2013). A pilot study of parent training in young children with autism spectrum disorders and disruptive behavior. Journal of Autism and Developmental Disorders, 43(4), 829-840.
Beasley, L.O., Silovsky, J.F., Owora, A., Burris, L., Hecht, D., DeMoraes-Huffine, P., Cruz, I., and Tolma, E. (2014). Mixed-methods feasibility study on the cultural adaptation of a child abuse prevention model. Child Abuse and Neglect, 38(9), 1496-1507.
Bee, P., Bower, P., Byford, S., Churchill, R., Calam, R., Stallard, P., Pryjmachuk, S., Berzins, K., Cary, M., Wan, M., and Abel, K. (2014). The clinical effectiveness, cost-effectiveness and acceptability of community-based interventions aimed at improving or maintaining quality of life in children of parents with serious mental illness: A systematic review. Health Technology Assessment, 18(8), 1-250.
Beeber, L.S., Schwartz, T.A., Holditch-Davis, D., Canuso, R., Lewis, V., and Hall, H.W. (2013). Parenting enhancement, interpersonal psychotherapy to reduce depression in low-income mothers of infants and toddlers: A randomized trial. Nursing Research, 62(2), 82-90.
Beeber, L.S., Schwartz, T.A., Martinez, M.I., Holditch-Davis, D., Bledsoe, S.E., Canuso, R., and Lewis, V.S. (2014). Depressive symptoms and compromised parenting in low-income mothers of infants and toddlers: Distal and proximal risks. Research in Nursing & Health, 37(4), 276-291.
Beeghly, M., and Tronick, E.Z. (1994). Effects of prenatal exposure to cocaine in early infancy: Toxic effects on the process of mutual regulation. Infant Mental Health Journal, 15(2), 158-175.
Benn, R., Akiva, T., Arel, S., and Roeser, R.W. (2012). Mindfulness training effects for parents and educators of children with special needs. Developmental Psychology, 48(5), 1476-1487.
Benson, M.L., Fox, G.L., DeMaris, A., and Van Wyk, J. (2003). Neighborhood disadvantage, individual economic distress and violence against women in intimate relationships. Journal of Quantitative Criminology, 19(3), 207-235.
Berger, L.M., Slack, K.S., Waldfogel, J., and Bruch, S.K. (2010). Caseworker-perceived caregiver substance abuse and child protective services outcomes. Child Maltreatment, 15(3), 199-210.
Berkovits, M.D., O’Brien, K.A., Carter, C.G., and Eyberg, S.M. (2010). Early identification and intervention for behavior problems in primary care: A comparison of two abbreviated versions of parent-child interaction therapy. Behavior Therapy, 41(3), 375-387.
Berlin, L.J., Shanahan, M., and Appleyard Carmody, K. (2014). Promoting supportive parenting in new mothers with substance-use problems: A pilot randomized trial of residential treatment plus an attachment-based parenting program. Infant Mental Health Journal, 35(1), 81-85.
Bernard, K., Dozier, M., Bick, J., Lewis-Morrarty, E., Lindhiem, O., and Carlson, E. (2012). Enhancing attachment organization among maltreated children: Results of a randomized clinical trial. Child Development, 83(2), 623-636.
Black, M.C., Basile, K.C., Breiding, M.J., Smith, S.G., Walters, M.L., Merrick, M.T., and Stevens, M. (2011). National Intimate Partner and Sexual Violence Survey: 2010 Summary Report. Atlanta, GA: Centers for Disease Control and Prevention.
Blegen, N.E., Hummelvoll, J.K., and Severinsson, E. (2010). Mothers with mental health problems: A systematic review. Nursing & Health Sciences, 12(4), 519-528.
Boden, J.M., Fergusson, D.M., and John Horwood, L. (2008). Early motherhood and subsequent life outcomes. Journal of Child Psychology and Psychiatry, 49(2), 151-160.
Boggs, S.R., Eyberg, S.M., Edwards, D.L., Rayfield, A., Jacobs, J., Bagner, D., and Hood, K.K. (2005). Outcomes of parent-child interaction therapy: A comparison of treatment completers and study dropouts one to three years later. Child & Family Behavior Therapy, 26(4), 1-22.
Borba, C.P.C., DePadilla, L., McCarty, F.A., von Esenwein, S.A., Druss, B.G., and Sterk, C.E. (2012). A qualitative study examining the perceived barriers and facilitators to medical healthcare services among women with a serious mental illness. Women’s Health Issues, 22(2), e217-e224.
Bouris, A., Guilamo-Ramos, V., Cherry, K., Dittus, P., Michael, S., and Gloppen, K. (2012). Preventing rapid repeat births among Latina adolescents: The role of parents. American Journal of Public Health, 102(10), 1842-1847.
Boyle, C.A., Boulet, S., Schieve, L.A., Cohen, R.A., Blumberg, S.J., Yeargin-Allsopp, M., Visser, S., and Kogan, M.D. (2011). Trends in the prevalence of developmental disabilities in U.S. children, 1997-2008. Pediatrics, 127(6), 1034-1042.
Bromberg, S.R., Backman, T.L., Krow, J., and Frankel, K.A. (2010). The Haven Mother’s House Modified Therapeutic Community: Meeting the gap in infant mental health services for pregnant and parenting mothers with drug addiction. Infant Mental Health Journal, 31(3), 255-276.
Brook, J., Akin, B.A., Lloyd, M.H., and Yan, Y. (2015). Family drug court, targeted parent training and family reunification: Did this enhanced service strategy make a difference? Juvenile and Family Court Journal, 66(2), 35-52.
Brooks-Gunn, J., Klebanov, P.K., and Liaw, F.-R. (1995). The learning, physical, and emotional environment of the home in the context of poverty: The Infant Health and Development Program. Children and Youth Services Review, 17(1), 251-276.
Brotman, L.M., Klein, R.G., Kamboukos, D., Brown, E.J., Coard, S.I., and Sosinsky, L.S. (2003). Preventive intervention for urban, low-income preschoolers at familial risk for conduct problems: A randomized pilot study. Journal of Clinical Child and Adolescent Psychology, 32(2), 246-257.
Brown, E. (2007). Women in the middle: The intersection of domestic violence and the child welfare system. Columbia University Journal of Student Social Work, 5(1), 21-29.
Browne, J.V., and Talmi, A. (2005). Family-based intervention to enhance infant-parent relationships in the neonatal intensive care unit. Journal of Pediatric Psychology, 30(8), 667-677.
Bruns, E.J., Pullmann, M.D., Weathers, E.S., Wirschem, M.L., and Murphy, J.K. (2012). Effects of a multidisciplinary family treatment drug court on child and family outcomes: Results of a quasi-experimental study. Child Maltreatment, 17(3), 218-230.
Burns, B.J., Phillips, S.D., Wagner, H.R., Barth, R.P., Kolko, D.J., Campbell, Y., and Landsverk, J. (2004). Mental health need and access to mental health services by youths involved with child welfare: A national survey. Journal of the American Academy of Child and Adolescent Psychiatry, 43(8), 960-970.
Byatt, N., Biebel, K., Friedman, L., Debordes-Jackson, G., Ziedonis, D., and Pbert, L. (2013). Patient’s views on depression care in obstetric settings: How do they compare to the views of perinatal health care professionals? General Hospital Psychiatry, 35(6), 598-604.
Camp, J.M., and Finkelstein, N. (1997). Parenting training for women in residential substance abuse treatment. Results of a demonstration project. Journal of Substance Abuse Treatment, 14(5), 411-422.
Carrell, S.E., and Hoekstra, M.L. (2010). Externalities in the classroom: How children exposed to domestic violence affect everyone’s kids. American Economic Journal: Applied Economics, 2(1), 211-228.
Casanueva, C., Dozier, M., Tueller, S., Jones Harden, B., Dolan, M., and Smith, K. (2012). Instability and Early Life Changes among Children in the Child Welfare System. No. 18. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Casanueva, C., Tueller, S., Smith, K., Dolan, M., and Ringeisen, H. (2014). NSCAW II Wave 3 Tables. OPRE Report No. 2013-43. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Catalano, S., Smith, E., Snyder, H., and Rand, M. (2009). Female Victims of Violence. Washington, DC: U.S. Department of Justice, Bureau of Justice Statistics.
Centers for Disease Control and Prevention. (n.d.). Facts about Intellectual Disability. Available: http://www.cdc.gov/ncbddd/actearly/pdf/parents_pdfs/IntellectualDisability.pdf [October 2016].
California Evidence-Based Clearinghouse. (2016a). Adolescent Parenting Program (APP). Available: http://www.cebc4cw.org/program/adolescent-parenting-program-app [March 2016].
California Evidence-Based Clearinghouse. (2016b). Adult-Focused Family Behavior Therapy (Adult-Focused FBT). Available: http://www.cebc4cw.org/program/adult-focused-family-behavior-therapy [March 2016].
California Evidence-Based Clearinghouse. (2016c). Attachment and Biobehavioral Catchup (ABC). Available: http://www.cebc4cw.org/program/attachment-and-biobehavioral-catch-up [March 2016].
California Evidence-Based Clearinghouse. (2016d). Computer-Assisted Motivational Intervention (CAMI). Available: http://www.cebc4cw.org/program/computer-assisted-motivational-intervention [March 2016].
California Evidence-Based Clearinghouse. (2016e). Family Connections (FC). Available: http://www.cebc4cw.org/program/family-connections [March 2016].
California Evidence-Based Clearinghouse. (2016f). The Family Growth Center (FGC). Available: http://www.cebc4cw.org/program/the-family-growth-center-fgc [March 2016].
California Evidence-Based Clearinghouse. (2016g). The Incredible Years (IY). Available: http://www.cebc4cw.org/program/the-incredible-years [March 2016].
California Evidence-Based Clearinghouse. (2016h). KEEP (Keeping Foster and Kin Parents Supported and Trained). Available: http://www.cebc4cw.org/program/keeping-foster-and-kin-parents-supported-and-trained [March 2016].
California Evidence-Based Clearinghouse. (2016i). Multisystemic Therapy for Child Abuse and Neglect (MST-CAN). Available: http://www.cebc4cw.org/program/multisystemic-therapy-for-child-abuse-and-neglect [March 2016].
California Evidence-Based Clearinghouse. (2016j). Nurturing Parenting Program for Parents and Their School-age Children 5 to 12 Years. Available: http://www.cebc4cw.org/program/nurturing-parenting-program-for-parents-and-their-school-age-children-5-to-12-years [March 2016].
California Evidence-Based Clearinghouse. (2016k). Parent-Child Interaction Therapy (PCIT). Available: http://www.cebc4cw.org/program/parent-child-interaction-therapy [March 2016].
California Evidence-Based Clearinghouse. (2016l). SafeCare®. Available: http://www.cebc4cw.org/program/safecare [March 2016].
California Evidence-Based Clearinghouse. (2016m). Treatment Foster Care Oregon for Preschoolers (TFCO-P). Available: http://www.cebc4cw.org/program/treatment-foster-care-oregon-for-preschoolers [March 2016].
California Evidence-Based Clearinghouse. (2016n). Triple P—Positive Parenting Program®System (System Triple P). Available: http://www.cebc4cw.org/program/triple-p-positive-parenting-program-system [March 2016].
Center for Behavioral Health Statistics and Quality. (2015). Behavioral Health Trends in the United States: Results from the 2014 National Survey on Drug Use and Health. HHS Publication No. SMA 15-4927, NSDUH Series H-50. Rockville, MD: Substance Abuse and Mental Health Services Administration.
The Center for Community Partnerships in Child Welfare. (2006). Families with Repeat Involvement with Child Welfare Systems: The Current Knowledge Base and Needed Next Steps. New York: The Center for Community Partnerships in Child Welfare of the Center for the Study of Social Policy.
Chaffin, M., Silovsky, J.F., Funderburk, B., Valle, L.A., Brestan, E.V., Balachova, T., Jackson, S., Lensgraf, J., and Bonner, B.L. (2004). Parent-child interaction therapy with physically abusive parents: Efficacy for reducing future abuse reports. Journal of Consulting and Clinical Psychology, 72(3), 500-510.
Chaffin, M., Funderburk, B., Bard, D., Valle, L.A., and Gurwitch, R. (2011). A combined motivation and parent-child interaction therapy package reduces child welfare recidivism in a randomized dismantling field trial. Journal of Consulting and Clinical Psychology, 79(1), 84-95.
Chaffin, M., Hecht, D., Bard, D., Silovsky, J.F., and Beasley, W.H. (2012). A statewide trial of the SafeCare home-based services model with parents in child protective services. Pediatrics, 129(3), 509-515.
Chamberlain, P., Price, J., Reid, J. B., and Landsverk, J. (2008). Cascading implementation of a foster and kinship parent intervention. Child Welfare, 87(5), 27-48.
Chamberlain, P. (2014). Comprehensive Review of Interventions for Children Exposed to Domestic Violence. San Francisco, CA: Futures Without Violence.
Chamberlain, P., and Fisher, P.A. (2003). An application of multidimensional treatment foster care for early intervention. In P. Chamberlain (Ed.), Treating Chronic Juvenile Offenders: Advances Made through the Oregon Multidimensional Treatment Foster Care Model (pp. 129-140). Washington, DC: American Psychological Association.
Chavis, A., Hudnut-Beumler, J., Webb, M.W., Neely, J.A., Bickman, L., Dietrich, M.S., and Scholer, S.J. (2013). A brief intervention affects parents’ attitudes toward using less physical punishment. Child Abuse and Neglect, 37(12), 1192-1201.
Chen, X.K., Wen, S.W., Fleming, N., Yang, Q., and Walker, M.C. (2007). Teenage pregnancy and congenital anomalies: Which system is vulnerable? Human Reproduction, 22(6), 1730-1735.
Child Welfare Information Gateway. (2014). Parental Substance Use and the Child Welfare System. Available: https://www.childwelfare.gov/pubPDFs/parentalsubabuse.pdf [January 2016].
Chorpita, B.F., Daleiden, E.L., and Weisz, J.R. (2005). Identifying and selecting the common elements of evidence based interventions: A distillation and matching model. Mental Health Services Research, 7(1), 5-20.
Clark, H.W. (2001). Residential substance abuse treatment for pregnant and postpartum women and their children: Treatment and policy implications. Child Welfare, 80(2), 179-198.
Cohen, J.A., and Mannarino, A.P. (1996). A treatment outcome study for sexually abused preschool children: Initial findings. Journal of the American Academy of Child and Adolescent Psychiatry, 35(1), 42-50.
Collins, K.S., Strieder, F.H., DePanfilis, D., Tabor, M., Freeman, P.A., Linde, L., and Greenberg, P. (2011). Trauma adapted family connections: Reducing developmental and complex trauma symptomatology to prevent child abuse and neglect. Child Welfare, 90(6), 29-47.
Collins, K.S., Freeman, P.A.C., Strieder, F.H., Reinicker, P., and Baldwin, C. (2015). A pilot study examining the reduction of trauma symptomatology in families to prevent child abuse and neglect: Trauma adapted family connections. Journal of Public Child Welfare, 9(5), 506-527.
Comer, J.S., Puliafico, A.C., Aschenbrand, S.G., McKnight, K., Robin, J.A., Goldfine, M.E., and Albano, A.M. (2012). A pilot feasibility evaluation of the CALM Program for anxiety disorders in early childhood. Journal of Anxiety Disorders, 26(1), 40-49.
Conger, R., Cui, M., and Lorenz, F. (2011). Intergenerational continuities in economic pressure and couple conflict in romantic relationships. In F. Fincham and M. Cui (Eds.), Romantic Relationships in Emerging Adulthood (pp. 101-122). New York: Cambridge University Press.
Conners, N.A., Bradley, R.H., Whiteside-Mansell, L., and Crone, C.C. (2001). A comprehensive substance abuse treatment program for women and their children: An initial evaluation. Journal of Substance Abuse Treatment, 21(2), 67-75.
Conroy, K., Engelhart, T., Arandia, P., and Forbes, P. (2013). Relationship between rapid repeat pregnancy and depression in low-income, minority teen mothers. Journal of Adolescent Health, 52(2 Suppl. 1), S109.
Cook, J.A., and Mueser, K.T. (2014). Improving services for parents with psychiatric disabilities: Three new opportunities in the field of psychiatric rehabilitation. Psychiatric Rehabilitation Journal, 37(1), 1-3.
Coren, E., Thomae, M., and Hutchfield, J. (2011). Parenting training for intellectually disabled parents: A Cochrane Systematic Review. Research on Social Work Practice, 21(4), 432-441.
Cowan, P.A., Cowan, C.P., Pruett, M.K., Pruett, K., and Gillette, P. (2014). Evaluating a couples group to enhance father involvement in low-income families using a benchmark comparison. Family Relations, 63(3), 356-370.
Craig, E.A. (2004). Parenting programs for women with mental illness who have young children: A review. Australian & New Zealand Journal of Psychiatry, 38(11-12), 923-928.
Crain-Thoreson, C., and Dale, P.S. (1999). Enhancing linguistic performance: Parents and teachers as book reading partners for children with language delays. Topics in Early Childhood Special Education, 19(1), 28-39.
Crean, H.F., Hightower, A.D., and Allan, M.J. (2001). School-based child care for children of teen parents: Evaluation of an urban program designed to keep young mothers in school. Evaluation and Program Planning, 24(3), 267-275.
Cress, C.J., Moskal, L., and Hoffmann, A. (2008). Parent directiveness in free play with young children with physical impairments. Communication Disorders Quarterly, 29(2), 99-108.
Cummings, E.M., and Davies, P.T. (2011). Marital Conflict and Children: An Emotional Security Perspective. New York: Guilford Press.
Dahinten, V.S., Shapka, J.D., and Willms, J.D. (2007). Adolescent children of adolescent mothers: The impact of family functioning on trajectories of development. Journal of Youth and Adolescence, 36(2), 195-212.
Dale, P.S., Crain-Thoreson, C., Notari-Syverson, A., and Cole, K. (1996). Parent-child book reading as an intervention technique for young children with language delays. Topics in Early Childhood Special Education, 16(2), 213-235.
d’Arlach, L., Olson, B.D., Jason, L.A., and Ferrari, J.R. (2006). Children, women, and substance abuse: A look at recovery in a communal setting. Journal of Prevention & Intervention in the Community, 31(1-2), 121-131.
Davies, P., and Cummings, E. (2006). Interparental discord, family process, and developmental psychopathology. In D. Cicchetti and D.J. Cohen (Eds.), Developmental Psychopathology (vol. 3, pp. 86-128). New York: Wiley & Sons.
Dawson, G., Rogers, S., Munson, J., Smith, M., Winter, J., Greenson, J., Donaldson, A., and Varley, J. (2010). Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics, 125(1), e17-e23.
Dawson, G., Jones, E.J., Merkle, K., Venema, K., Lowy, R., Faja, S., Kamara, D., Murias, M., Greenson, J., Winter, J., Smith, M., Rogers, S.J., and Webb, S.J. (2012). Early behavioral intervention is associated with normalized brain activity in young children with autism. Journal of the American Academy of Child and Adolescent Psychiatry, 51(11), 1150-1159.
Dean, K., Mortensen, P.B., Stevens, H., Murray, R.M., Walsh, E., and Agerbo, E. (2012). Criminal conviction among offspring with parental history of mental disorder. Psychological Medicine, 42(3), 571-581.
Deblinger, E., Stauffer, L.B., and Steer, R.A. (2001). Comparative efficacies of supportive and cognitive behavioral group therapies for young children who have been sexually abused and their nonoffending mothers. Child Maltreatment, 6(4), 332-343.
Dekker, M.C., Ferdinand, R.F., van Lang, N.D., Bongers, I.L., van der Ende, J., and Verhulst, F.C. (2007). Developmental trajectories of depressive symptoms from early childhood to late adolescence: Gender differences and adult outcome. Journal of Child Psychology and Psychiatry, 48(7), 657-666.
Dennis, C.L. (2014). Psychosocial interventions for the treatment of perinatal depression. Best Practice & Research. Clinical Obstetrics & Gynaecology, 28(1), 97-111.
DePanfilis, D., Dubowitz, H., and Kunz, J. (2008). Assessing the cost-effectiveness of family connections. Child Abuse and Neglect, 32(3), 335-351.
Dolan, M., Smith, K., Casanueva, C., and Ringeisen, H. (2011). NSCAW II Baseline Report: Caseworker Characteristics, Child Welfare Services, and Experiences of Children Placed in Out-of-Home Care. OPRE Report No. 2011-27E. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Dolan, M., Smith, K., Casanueva, C., and Ringeisen, H. (2012). NSCAW II Wave 2 Report: Child and Caregiver Need and Receipt of Child Welfare Services Post-Baseline. Washington, DC: Office of Planning, Research and Evaluation; Administration for Children and Families; U.S. Department of Health and Human Services.
Dolman, C., Jones, I., and Howard, L.M. (2013). Pre-conception to parenting: A systematic review and meta-synthesis of the qualitative literature on motherhood for women with severe mental illness. Archives of Women’s Mental Health, 16(3), 173-196.
Donohue, B., Azrin, N.H., Bradshaw, K., Van Hasselt, V.B., Cross, C.L., Urgelles, J., Romero, V., Hill, H.H., and Allen, D.N. (2014). A controlled evaluation of family behavior therapy in concurrent child neglect and drug abuse. Journal of Consulting and Clinical Psychology, 82(4), 706-720.
Drake, B., and Jonson-Reid, M. (1999a). Some thoughts on the increasing use of administrative data in child maltreatment research. Child Maltreatment, 4(4), 308-315.
Drake, B., and Jonson-Reid, M. (1999b). Substantiated and Unsubstantiated Cases: Patterns and Predictors of Recurrence. Year 2 Progress and Preliminary Findings. Paper presented at the Children’s Bureau Child Abuse and Neglect Discretionary Grants Meeting, Washington, DC.
Dunlap, G., and Fox, L. (2009). Positive behavior support and early intervention. In W. Sailor, G. Dunlap, G. Sugai, and R. Horner (Eds.), Handbook of Positive Behavior Support (pp. 49-71). New York: Springer.
Dunst, C.J., and Espe-Sherwindt, M. (2016). Family-centered practices in early intervention. In B. Reichow, B. Boyd, E. Barton, and S. Odom (Eds.), Handbook of Early Childhood Special Education. New York: Springer.
Dunst, C.J., and Trivette, C.M. (2010). Family-centered helpgiving practices, parent-professional partnerships, and parent, family and child outcomes. In S.L. Christenson and A.L. Reschley (Eds.), Handbook of School-Family Partnerships (pp. 362-379). New York: Routledge.
Durand, V.M., Hieneman, M., Clarke, S., Wang, M., and Rinaldi, M.L. (2013). Positive family intervention for severe challenging behavior I: A multisite randomized clinical trial. Journal of Positive Behavior Interventions, 15(3), 133-143.
Eckenrode, J., Ganzel, B., Henderson, C.R., Jr., Smith, E., Olds, D.L., Powers, J., Cole, R., Kitzman, H., and Sidora, K. (2000). Preventing child abuse and neglect with a program of nurse home visitation: The limiting effects of domestic violence. Journal of the American Medical Association, 284(11), 1385-1391.
Edleson, J.L. (1999). Children’s witnessing of adult domestic violence. Journal of Interpersonal Violence, 14(8), 839-870.
Elliott, J.C., Lubin, D.A., Walker, C.H., and Johns, J.M. (2001). Acute cocaine alters oxytocin levels in the medial preoptic area and amygdala in lactating rat dams: Implications for cocaine-induced changes in maternal behavior and maternal aggression. Neuropeptides, 35(2), 127-134.
Eyberg, S.M., and Boggs, S.R. (1998). Parent-child interaction therapy: A psychosocial intervention for the treatment of young conduct-disordered children. In C.E. Schaefer and J.M. Briesmeister (Eds.), Handbook of Parent Training: Parents as Co-therapists for Children’s Behavior Problems (2nd ed., pp. 61-97). New York: Wiley.
Fabiano, G.A., Chacko, A., Pelham, W.E., Jr., Robb, J., Walker, K.S., Wymbs, F., Sastry, A.L., Flammer, L., Keenan, J.K., Visweswaraiah, H., Shulman, S., Herbst, L., and Pirvics, L. (2009). A comparison of behavioral parent training programs for fathers of children with attention-deficit/hyperactivity disorder. Behavior Therapy, 40(2), 190-204.
Fals-Stewart, W., Klostermann, K., Yates, B.T., O’Farrell, T.J., and Birchler, G.R. (2005). Brief relationship therapy for alcoholism: A randomized clinical trial examining clinical efficacy and cost-effectiveness. Psychology of Addictive Behaviors, 19(4), 363-371.
Fals-Stewart, W., Klostermann, K., and Clinton-Sherrod, M. (2009). Substance abuse and intimate partner violence. In K.D. O’Leary and E.M. Woodin (Eds.), Psychological and Physical Aggression in Couples: Causes and Interventions (pp. 251-269). Washington, DC: American Psychological Association.
Feder, L., and Wilson, D. (2005). A meta-analytic review of court-mandated batterer intervention programs: Can courts affect abusers’ behavior? Journal of Experimental Criminology, 1, 239-262.
Feinberg, E., Augustyn, M., Fitzgerald, E., Sandler, J., Ferreira-Cesar Suarez, Z., Chen, N., Cabral, H., Beardslee, W., and Silverstein, M. (2014). Improving maternal mental health after a child’s diagnosis of autism spectrum disorder: Results from a randomized clinical trial. Journal of the American Medical Association Pediatrics, 168(1), 40-46.
Feldman, M.A. (1994). Parenting education for parents with intellectual disabilities: A review of outcome studies. Research in Developmental Disabilities, 15(4), 299-332.
Feldman, M.A., and Werner, S.E. (2002). Collateral effects of behavioral parent training on families of children with developmental disabilities and behavior disorders. Behavioral Interventions, 17(2), 75-83.
Feldman, M.A., Case, L., and Sparks, B. (1992). Effectiveness of a child-care training program for parents at-risk for child neglect. Canadian Journal of Behavioural Science, 24(1), 14.
Finkelhor, D., Turner, H., Ormrod, R., Hamby, S., and Kracke, K. (2009). Children’s exposure to violence: A comprehensive national survey. Juvenile Justice Bulletin (October). Available: https://www.ncjrs.gov/pdffiles1/ojjdp/227744.pdf [March 2016].
Finkelhor, S., Turner, H.., Shattuck, A., Hamby, S., and Kracke, K. (2015). Children’s exposure to violence, crime, and abuse: An update. Juvenile Justice Bulletin (September). Available: http://www.ojjdp.gov/pubs/248547.pdf [March 2016].
Finkelstein, N. (1994). Treatment issues for alcohol- and drug-dependent pregnant and parenting women. Health and Social Work, 19(1), 7-15.
Finkelstein, N. (1996). Using the relational model as a context for treating pregnant and parenting chemically dependent women. Journal of Chemical Dependency Treatment, 6(1-2), 23-44.
Fisher, P.A., Ellis, B.H., and Chamberlain, P. (1999). Early intervention foster care: A model for preventing risk in young children who have been maltreated. Children’s Services, 2(3), 159-182.
Fisher, P.A., Burraston, B., and Pears, K. (2005). The Early Intervention Foster Care Program: Permanent placement from a randomized trial. Child Maltreatment, 10(1), 61-71.
Fisher, P.A., Gunnar, M., Dozier, M., Bruce, J., and Pears, K. (2006). Effects of therapeutic interventions for foster children on behavioral problems, caregiver attachment, and stress regulatory neural systems. Annals of the New York Academy of Sciences, 1094, 215-225.
Fisher, P.A., Kim, H.K., and Pears, K.C. (2009). Effects of Multidimentional Treatment Foster Care for Preschoolers (MTFC-P) on reducing permanent failures among children with placement instability. Child and Youth Services Review, 31, 541-546.
Fisher, P.A., Stoolmiller, M., Mannering, A.M., Takahashi, A., and Chamberlain, P. (2011a). Foster placement disruptions associated with problem behavior: Mitigating a threshold effect. Journal of Consulting and Clinical Psychology, 79(4), 481-487.
Fisher, P.A., Lester, B.M., DeGarmo, D.S., LaGasse, L.L., Lin, H., Shankaran, S., Bada, H.S., Bauer, C.R., Hammond, J., Whitaker, T., and Higgins, R. (2011b). The combined effects of prenatal drug exposure and early adversity on neurobehavioral disinhibition in childhood and adolescence. Development and Psychopathology, 23(3), 777-788.
Fletcher, R.J., Maharaj, O.N., Fletcher Watson, C.H., May, C., Skeates, N., and Gruenert, S. (2013). Fathers with mental illness: Implications for clinicians and health services. The Medical Journal of Australia, 199(Suppl. 3), S34-S36.
Fonagy, P., Bateman, A.W., and Luyten, P. (2012). Introduction and overview. In A.W. Bateman and P. Fonagy (Eds.), Handbook of Mentalizing in Mental Health Practice (pp. 3-42). Washington, DC: American Psychiatric Association.
Forman, D.R., O’Hara, M.W., Stuart, S., Gorman, L.K., Larsen, K.E., and Coy, K.C. (2007). Effective treatment for postpartum depression is not sufficient to improve the developing mother-child relationship. Development and Psychopathology, 19(2), 585-602.
Friesen, B.J., Nicholson, J., Kaplan, K., and Solomon, P. (2009). Parents with a mental illness and implementation of the Adoption and Safe Families Act. In O. Golden and J. Macomber (Eds.), Intentions and Results: A Look Back at the Adoption and Safe Families Act (pp. 102-114). Washington, DC: Urban Institute, Center for the Study of Social Policy.
Fung, M.P., and Fox, R.A. (2014). The culturally-adapted early pathways program for young Latino children in poverty: A randomized controlled trial. Journal of Latina/o Psychology, 2(3), 131-145.
Futures Without Violence. (2010). Realizing the Promise of Home Visitations: Addressing Domestic Violence and Child Maltreatment. San Francisco, CA: Family Violence Prevention Fund.
Gearing, R.E., Alonzo, D., and Marinelli, C. (2012). Maternal schizophrenia: Psychosocial treatment for mothers and their children. Clinical Schizophrenia & Related Psychoses, 6(1), 27-33.
Geeraert, L., Van den Noortgate, W., Grietens, H., and Onghena, P. (2004). The effects of early prevention programs for families with young children at risk for physical child abuse and neglect: A meta-analysis. Child Maltreatment, 9(3), 277-291.
Geffner, R., Igelman, R.S., and Zellner, J. (2014). The Effects of Intimate Partner Violence on Children. New York: Routledge.
Gershater-Molko, R.M., Lutzker, J.R., and Wesch, D. (2002). Using recidivism data to evaluate Project SafeCare: Teaching bonding, safety, and health care skills to parents. Child Maltreatment, 7(3), 277-285.
Gershater-Molko, R.M., Lutzker, J.R., and Wesch, D. (2003). Project SafeCare: Improving health, safety, and parenting skills in families reported for, and at-risk for child maltreatment. Journal of Family Violence, 18(6), 377-386.
Girolametto, L., Weitzman, E., and Clements-Baartman, J. (1998). Vocabulary intervention for children with Down syndrome: Parent training using focused stimulation. Infant-Toddler Intervention: The Transdisciplinary Journal, 8(2), 109-125.
Glazemakers, I., and Deboutte, D. (2013). Modifying the “Positive Parenting Program” for parents with intellectual disabilities. Journal of Intellectual Disability Research, 57(7), 616-626.
Goodmark, L. (2012). A Troubled Marriage: Domestic Violence and the Legal System. New York and London: New York University Press.
Gottman, J., Gottman, J., and Shapiro, A. (2010). A new couples approach to interventions for the transition to parenthood. In M.S. Schulz, M.K. Pruett, P.K. Kerig, and R.D. Parke (Eds.), Strengthening Couple Relationships for Optimal Child Development: Lessons from Research and Intervention (pp. 165-179). Washington, DC: American Psychological Association.
Grant, T.M., and Ernst, C.C. (2014). Report to the Division of Behavioral Health and Recovery for Washington State PCAP Sites as of June 30, 2014. Fetal Alcohol and Drug Unit, Alcohol and Drug Abuse Institute. Seattle: University of Washington Health Sciences Administration.
Grant, T.M., Ernst, C.C., Streissguth, A., and Stark, K. (2005). Preventing alcohol and drug exposed births in Washington state: Intervention findings from three parent-child assistance program sites. The American Journal of Drug and Alcohol Abuse, 31(3), 471-490.
Gray, B., Robinson, C., and Seddon, D. (2008). Invisible children: Young carers of parents with mental health problems—The perspectives of professionals. Child and Adolescent Mental Health, 13(4), 169-172.
Green, J., Charman, T., McConachie, H., Aldred, C., Slonims, V., Howlin, P., Le Couteur, A., Leadbitter, K., Hudry, K., Byford, S., Barrett, B., Temple, K., Macdonald, W., and Pickles, A. (2010). Parent-mediated communication-focused treatment in children with autism (PACT): A randomised controlled trial. Lancet, 375(9732), 2152-2160.
Greeno, J.E., Uretsky, M.C., Lee, B.R., Moore, J.E., Barth, R.P., and Shaw, T.V. (2016). Replication of the KEEP foster and kinship parent training program in a population of youth with externalizing behavior problems. Children and Youth Services Review, 61(Issue C), 75-82.
Grella, C.E., Joshi, V., and Hser, Y.I. (2000). Program variation in treatment outcomes among women in residential drug treatment. Evaluation Review, 24(4), 364-383.
Gruber, K.J. (2012). A comparative assessment of early adult life status of graduates of the North Carolina Adolescent Parenting Program. Journal of Child and Adolescent Psychiatric Nursing, 25(2), 75-83.
Guastaferro, K.M. (2011). Teaching Young Mothers to Identify Developmental Milestones. Thesis, Georgia State University, Atlanta, GA.
Hamilton, B.E., Martin, J.A., Osterman, M.J., and Curtin, S.C. (2015). Births: Final data for 2014. National Vital Statistics Reports, 64(12).
Harris, S.E., Fox, R.A., and Love, J.R. (2015). Early pathways therapy for young children in poverty: A randomized controlled trial. Counseling Outcome Research and Evaluation, 6(1), 3-17.
Hastings, R.P. (2002). Parental stress and behaviour problems of children with developmental disability. Journal of Intellectual and Developmental Disability, 27(3), 149-160.
Healy, S., Lewin, J., Butler, S., Vaillancourt, K., and Seth-Smith, F. (2015). Affect recognition and the quality of mother-infant interaction: Understanding parenting difficulties in mothers with schizophrenia. Archives of Women’s Mental Health, 19(1), 113-124.
Heidari, H., Hasanpour, M., and Fooladi, M. (2013). The experiences of parents with infants in neonatal intensive care unit. Iranian Journal of Nursing and Midwifery Research, 18(3), 208-213.
Henderson, C., Evans-Lacko, S., and Thornicroft, G. (2013). Mental illness stigma, help seeking, and public health programs. American Journal of Public Health, 103(5), 777-780.
Herrera, V.M., and McCloskey, L.A. (2001). Gender differences in the risk for delinquency among youth exposed to family violence. Child Abuse and Neglect, 25(8), 1037-1051.
Hinden, B.R., Biebel, K., Nicholson, J., Henry, A., and Katz-Leavy, J. (2006). A survey of programs for parents with mental illness and their families: Identifying common elements to build the evidence base. Journal of Behavioral Health Services & Research, 33(1), 21-38.
Hirshfeld-Becker, D.R., Masek, B., Henin, A., Blakely, L.R., Pollock-Wurman, R.A., McQuade, J., DePetrillo, L., Briesch, J., Ollendick, T.H., Rosenbaum, J.F., and Biederman, J. (2010). Cognitive behavioral therapy for 4- to 7-year-old children with anxiety disorders: A randomized clinical trial. Journal of Consulting and Clinical Psychology, 78(4), 498-510.
Hoath, F.E., and Sanders, M.R. (2002). A feasibility study of enhanced group Triple P—Positive Parenting Program for parents of children with attention-deficit/hyperactivity disorder. Behaviour Change, 19(4), 191-206.
Hodgkinson, S.C., Colantuoni, E., Roberts, D., Berg-Cross, L., and Belcher, H.M.E. (2010). Depressive symptoms and birth outcomes among pregnant teenagers. Journal of Pediatric and Adolescent Gynecology, 23(1), 16-22.
Hodgkinson, S.C., Beers, L., Southammakosane, C., and Lewin, A. (2014). Addressing the mental health needs of pregnant and parenting adolescents. Pediatrics, 133(1), 114-122.
Hodnett, R.H., Faulk, K., Dellinger, A., and Maher, E. (2009). Evaluation of the Statewide Implementation of a Parent Education Program in Louisiana’s Child Welfare Agency: The Nurturing Parenting Program for Infants, Toddlers, and Pre-School Children. Final Evaluation Report. Available: http://nurturingparenting.com/images/cmsfiles/nurturingparentprogram_exsum_fin_lo.pdf [March 2016].
Hoffman, S.D., and Maynard, R.A. (2008). Kids Having Kids: Economic Costs & Social Consequences of Teen Pregnancy. Washington, DC: Urban Institute.
Holt, S., Buckley, H., and Whelan, S. (2008). The impact of exposure to domestic violence on children and young people: A review of the literature. Child Abuse and Neglect, 32(8), 797-810.
Horwitz, S.M., Landsverk, J., Hurlburt, M., and Aarons, G.A. (2009). Strategies to Increase Readiness to Adopt Evidence-Based Parent Training Programs in Child Welfare Agencies: Preliminary Findings. Paper presented at the Child and Adolescent Mental Health Services: Issues and Solutions Conference, September 23-24, Nashville, TN.
Hotz, V.J., McElroy, S.W., and Sanders, S.G. (2005). Teenage childbearing and its life cycle consequences: Exploiting a natural experiment. The Journal of Human Resources, 40(3), 683-715.
Hughes, R.C., and Wilson, P.H. (1988). Behavioral parent training: Contingency management versus communication skills training with or without the participation of the child. Child & Family Behavior Therapy, 10(4), 11-23.
Huxley, A., and Foulger, S. (2008). Parents who misuse substances: Implications for parenting practices and treatment seeking behaviour. Drugs and Alcohol Today, 8(3), 9-16.
Ingersoll, B., and Wainer, A. (2013). Initial efficacy of Project ImPACT: A parent-mediated social communication intervention for young children with ASD. Journal of Autism and Developmental Disorders, 43(12), 2943-2952.
Ingoldsby, E.M. (2010). Review of interventions to improve family engagement and retention in parent and child mental health programs. Journal of Child and Family Studies, 19(5), 629-645.
Institute of Medicine and National Research Council. (2009). Depression in Parents, Parenting, and Children: Opportunities to Improve Identification, Treatment, and Prevention. M.J. England and L.J. Sim (Eds.). Committee on Depression, Parenting Practices, and the Healthy Development of Children; Division of Behavioral and Social Sciences and Education. Washington, DC: The National Academies Press.
Institute of Medicine and National Research Council. (2014). New Directions in Child Abuse and Neglect Research. A. Petersen, J. Joseph, and M. Feit (Eds.). Committee on Child Maltreatment Research, Policy, and Practice for the Next Decade: Phase II; Board on Children, Youth, and Families. Washington, DC: The National Academies Press.
Ippen, C., Harris, W.W., Van Horn, P., and Lieberman, A.F. (2011). Traumatic and stressful events in early childhood: Can treatment help those at highest risk? Child Abuse and Neglect, 35(7), 504-513.
Iqbal, M.M., Sobhan, T., and Ryals, T. (2002). Effects of commonly used benzodiazepines on the fetus, the neonate, and the nursing infant. Psychiatric Services, 53(1), 39-49.
Jackson, V. (2004). Residential treatment for parents and their children: The village experience. Science and Practice Perspectives, 2(2), 44-53.
Johnson, K. (2009). State-Based Home Visiting: Strengthening Programs through State Leadership. New York: Columbia University, National Center for Children in Poverty.
Jose, A., and O’Leary, K.D. (2009). Prevalence of partner aggression in representative and clinic samples. In K.D. O’Leary and E.M. Woodin (Eds.), Psychological and Physical Aggression in Couples: Causes and Interventions (pp. 15-35). Washington, DC: American Psychological Association.
Jutte, D.P., Roos, N.P., Brownell, M.D., Briggs, G., MacWilliam, L., and Roos, L.L. (2010). The ripples of adolescent motherhood: Social, educational, and medical outcomes for children of teen and prior teen mothers. Academic Pediatrics, 10(5), 293-301.
Kahng, S.K., Oyserman, D., Bybee, D., and Mowbray, C. (2008). Mothers with serious mental illness: When symptoms decline does parenting improve? Journal of Family Psychology, 22(1), 162-166.
Kaminski, J.W., Valle, L.A., Filene, J.H., and Boyle, C.L. (2008). A meta-analytic review of components associated with parent training program effectiveness. Journal of Abnormal Child Psychology, 36(4), 567-589.
Kandel, I., and Merrick, J. (2003). The birth of a child with disability. Coping by parents and siblings. The Scientific World Journal, 3, 741-750.
Karaaslan, O., and Mahoney, G. (2013). Effectiveness of responsive teaching with children with Down syndrome. Intellectual and Developmental Disabilities, 51(6), 458-469.
Karaaslan, O., Diken, I.H., and Mahoney, G. (2013). A randomized control study of responsive teaching with young Turkish children and their mothers. Topics in Early Childhood Special Education, 33(1), 18-27.
Kasari, C., Gulsrud, A.C., Wong, C., Kwon, S., and Locke, J. (2010). Randomized controlled caregiver mediated joint engagement intervention for toddlers with autism. Journal of Autism and Developmental Disorders, 40(9), 1045-1056.
Kelley, M.L., and Fals-Stewart, W. (2002). Couples- versus individual-based therapy for alcohol and drug abuse: Effects on children’s psychosocial functioning. Journal of Consulting and Clinical Psychology, 70(2), 417-427.
Keltner, B., Finn, D., and Shearer, D. (1995). Effects of family intervention on maternal-child interaction for mothers with developmental disabilities. Family & Community Health: The Journal of Health Promotion & Maintenance, 17(4), 35-49.
Kennedy, S.J., Rapee, R.M., and Edwards, S.L. (2009). A selective intervention program for inhibited preschool-aged children of parents with an anxiety disorder: Effects on current anxiety disorders and temperament. Journal of the American Academy of Child & Adolescent Psychiatry, 48(6), 602-609.
Kenny, M., Conroy, S., Pariante, C.M., Seneviratne, G., and Pawlby, S. (2013). Mother-infant interaction in mother and baby unit patients: Before and after treatment. Journal of Psychiatric Research, 47(9), 1192-1198.
Kerwin, M.E. (2005). Collaboration between child welfare and substance-abuse fields: Combined treatment programs for mothers. Journal of Pediatric Psychology, 30(7), 581-597.
Kessler, R.C., Berglund, P., Demler, O., Jin, R., Merikangas, K.R., and Walters, E.E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593-602.
Kitzman, H., Olds, D.L., Sidora, K., Henderson, C.R., Jr., Hanks, C., Cole, R., Luckey, D.W., Bondy, J., Cole, K., and Glazner, J. (2000). Enduring effects of nurse home visitation on maternal life course: A 3-year follow-up of a randomized trial. Journal of the American Medical Association, 283(15), 1983-1989.
Kitzmann, K.M., Gaylord, N.K., Holt, A.R., and Kenny, E.D. (2003). Child witnesses to domestic violence: A meta-analytic review. Journal of Consulting and Clinical Psychology, 71(2), 339-352.
Knerr, W., Gardner, F., and Cluver, L. (2013). Improving positive parenting skills and reducing harsh and abusive parenting in low- and middle-income countries: A systematic review. Prevention Science, 14(4), 352-363.
Koenen, K.C., Moffitt, T.E., Caspi, A., Taylor, A., and Purcell, S. (2003). Domestic violence is associated with environmental suppression of IQ in young children. Development and Psychopathology, 15(2), 297-311.
Krumm, S., Becker, T., and Wiegand-Grefe, S. (2013). Mental health services for parents affected by mental illness. Current Opinion in Psychiatry, 26(4), 362-368.
Kumpfer, K., Greene, J., Bates, R., Cofrin, K., and Whiteside, H. (2007). State of New Jersey DHS Division of Addiction Services Strengthening Families Program Substance Abuse Prevention Initiative: Year Three Evaluation Report. Reporting period: July 1, 2004-June 30, 2007. Salt Lake City, UT: LutraGroup.
Labriola, M., Bradley, S., O’Sullivan, C.S., Rempel, M., and Moore, S. (2010). A National Portrait of Domestic Violence Courts. Report submitted to the National Institute of Justice. New York: Center for Court Innovation.
Lacey, M., Paolini, S., Hanlon, M.C., Melville, J., Galletly, C., and Campbell, L.E. (2015). Parents with serious mental illness: Differences in internalised and externalised mental illness stigma and gender stigma between mothers and fathers. Psychiatry Research, 225(3), 723-733.
LaTaillade, J.J., Epstein, N.B., and Werlinich, C.A. (2006). Conjoint treatment of intimate partner violence: A cognitive behavioral approach. Journal of Cognitive Psychotherapy, 20(4), 393-410.
Lavigne, J.V., Gibbons, R.D., Christoffel, K.K., Arend, R., Rosenbaum, D., Binns, H., Dawson, N., Sobel, H., and Isaacs, C. (1996). Prevalence rates and correlates of psychiatric disorders among preschool children. Journal of the American Academy of Child & Adolescent Psychiatry, 35(2), 204-214.
Lavigne, J.V., Lebailly, S.A., Gouze, K.R., Cicchetti, C., Pochyly, J., Arend, R., Jessup, B.W., and Binns, H.J. (2008). Treating oppositional defiant disorder in primary care: A comparison of three models. Journal of Pediatric Psychology, 33(5), 449-461.
Leathers, S.J., Spielfogel, J.E., McMeel, L.S., and Atkins, M.S. (2011). Use of a parent management training intervention with urban foster parents: A pilot study. Children and Youth Services Review, 33(7), 1270-1279.
Lehner-Dua, L.L. (2001). The Effectiveness of Russell A. Barkley’s Parent Training Program on Parents with School-Aged Children Who Have ADHD on Their Perceived Severity of ADHD, Stress, and Sense of Competence Ph.D. Dissertation, Hofstra University, Hempstead, NY.
Leung, D.W., and Slep, A.M. (2006). Predicting inept discipline: The role of parental depressive symptoms, anger, and attributions. Journal of Consulting and Clinical Psychology, 74(3), 524-534.
Lieberman, A.F., Van Horn, P., and Ippen, C.G. (2005). Toward evidence-based treatment: Child-parent psychotherapy with preschoolers exposed to marital violence. Journal of the American Academy of Child & Adolescent Psychiatry, 44(12), 1241-1248.
Lieberman, A.F., Ghosh Ippen, C., and Van Horn, P. (2006). Child-parent psychotherapy: 6-month follow-up of a randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry, 45(8), 913-918.
Lieberman, A.F., Chu, A., Van Horn, P., and Harris, W.W. (2011). Trauma in early childhood: Empirical evidence and clinical implications. Development and Psychopathology, 23(2), 397-410.
Linares, L.O., Montalto, D., Li, M., and Oza, V.S. (2006). A promising parenting intervention in foster care. Journal of Consulting & Clinical Psychology, 74(1), 32-41.
Linares, L.O., Li, M., and Shrout, P.E. (2012). Child training for physical aggression?: Lessons from foster care. Children and Youth Services Review, 34(12), 2416-2422.
Linares, L.O., Jimenez, J., Nesci, C., Pearson, E., Beller, S., Edwards, N., and Levin-Rector, A. (2015). Reducing sibling conflict in maltreated children placed in foster homes. Prevention Science, 16(2), 211-221.
Llewellyn, G., McConnell, D., Honey, A., Mayes, R., and Russo, D. (2003). Promoting health and home safety for children of parents with intellectual disability: A randomized controlled trial. Research in Developmental Disabilities, 24(6), 405-431.
Lloyd, E.C., and Barth, R.P. (2011). Developmental outcomes after five years for foster children returned home, remaining in care, or adopted. Children and Youth Services Review, 33(8), 1383-1391.
Luby, J.L. (2013). Treatment of anxiety and depression in the preschool period. Journal of the American Academy of Child & Adolescent Psychiatry, 52(4), 346-358.
Luby, J.L., Lenze, S., and Tillman, R. (2012). A novel early intervention for preschool depression: Findings from a pilot randomized controlled trial. Journal of Child Psychology and Psychiatry, 53(3), 313-322.
Lundgren, L.M., Schilling, R.F., Fitzgerald, T., Davis, K., and Amodeo, M. (2003). Parental status of women injection drug users and entry to methadone maintenance. Substance Use and Misuse, 38(8), 1109-1131.
Lussier, B.J., Crimmins, D.B., and Alberti, D. (1994). Effect of three adult interaction styles on infant engagement. Journal of Early Intervention, 18(1), 12-24.
Lutzker, J.R., and Chaffin, M. (2012). SafeCare®: An evidence-based constantly dynamic model to prevent child maltreatment. In H. Dubowitz (Ed.), World Perspectives on Child Abuse (10th ed., pp. 93-96). Canberra, Australia: International Society for the Prevention of Child Abuse and Neglect.
Mahoney, G., Perales, F., Wiggers, B., and Herman, B. (2006). Responsive teaching: Early intervention for children with Down syndrome and other disabilities. Down Syndrome, Research and Practice, 11(1), 18-28.
Malone, D.G., and Gallagher, P.A. (2008). Transition to preschool programs for young children with disabilities. Journal of Early Intervention, 30(4), 341-356.
Malone, D.G., and Gallagher, P.A. (2009). Transition to preschool special education: A review of the literature. Early Education and Development, 20(4), 584-602.
Manlove, J., Mariner, C., and Papillo, A.R. (2000). Subsequent fertility among teen mothers: Longitudinal analyses of recent national data. Journal of Marriage and Family, 62(2), 430-448.
Marcynyszyn, L.A., Maher, E.J., and Corwin, T.W. (2011). Getting with the (evidence-based) program: An evaluation of the Incredible Years parenting training program in child welfare. Children and Youth Services Review, 33(5), 747-757.
Marlowe, D.B., and Carey, S.M. (2012). Research Update on Family Drug Courts. Alexandria, VA: National Association of Drug Court Professionals.
Martin, J.A., Hamilton, B.E., Michelle, J., Curtin, S.C., and Matthews, T. (2015). Division of Vital Statistics births: Final data for 2013. National Vital Statistics Reports, 64(1).
Mayes, L., and Truman, S. (2002). Substance abuse and parenting. In M. Bornstein (Ed.), Handbook of Parenting (vol. 4, pp. 329-359). Mahwah, NJ: Lawrence Erlbaum Associates.
McCoy, B.M., Rickert, M.E., Class, Q.A., Larsson, H., Lichtenstein, P., and D’Onofrio, B.M. (2014). Mediators of the association between parental severe mental illness and offspring neurodevelopmental problems. Annals of Epidemiology, 24(9), 629-634.
McCurdy, K., and Daro, D. (2001). Parent involvement in family support programs: An integrated theory. Family Relations, 50(2), 113-121.
McGaw, S., Scully, T., and Pritchard, C. (2010). Predicting the unpredictable? Identifying high-risk versus low-risk parents with intellectual disabilities. Child Abuse and Neglect, 34(9), 699-710.
McIntyre, L.L. (2008). Parent training for young children with developmental disabilities: Randomized controlled trial. American Journal of Mental Retardation, 113(5), 356-368.
McKee, L., Colletti, C., Rakow, A., Jones, D.J., and Forehand, R. (2008). Parenting and child externalizing behaviors: Are the associations specific or diffuse? Aggression and Violent Behavior, 13(3), 201-215.
Meade, C.S., and Ickovics, J.R. (2005). Systematic review of sexual risk among pregnant and mothering teens in the USA: Pregnancy as an opportunity for integrated prevention of STD and repeat pregnancy. Social Science & Medicine, 60(4), 661-678.
Meade, C.S., Kershaw, T.S., and Ickovics, J.R. (2008). The intergenerational cycle of teenage motherhood: An ecological approach. Health Psychology, 27(4), 419-429.
Meier, J.S. (2015). Johnson’s differentiation theory: Is it really empirically supported? Journal of Child Custody, 12(1), 4-24.
Melnyk, B.M., Alpert-Gillis, L.J., Hensel, P.B., Cable-Beiling, R.C., and Rubenstein, J.S. (1997). Helping mothers cope with a critically ill child: A pilot test of the COPE intervention. Research in Nursing & Health, 20(1), 3-14.
Melnyk, B.M., Crean, H.F., Feinstein, N.F., Fairbanks, E., and Alpert-Gillis, L.J. (2007). Testing the theoretical framework of the COPE program for mothers of critically ill children: An integrative model of young children’s post-hospital adjustment behaviors. Journal of Pediatric Psychology, 32(4), 463-474.
Melnyk, B.M., Crean, H.F., Feinstein, N.F., and Fairbanks, E. (2008). Maternal anxiety and depression after a premature infant’s discharge from the neonatal intensive care unit: Explanatory effects of the Creating Opportunities for Parent Empowerment Program. Nursing Research, 57(6), 383-394.
Menting, A.T., Orobio de Castro, B., and Matthys, W. (2013). Effectiveness of the Incredible Years parent training to modify disruptive and prosocial child behavior: A meta-analytic review. Clinical Psychology Review, 33(8), 901-913.
Metsch, L.R., Wolfe, H.P., Fewell, R., McCoy, C.B., Elwood, W.N., Wohler-Torres, B., Petersen-Baston, P., and Haskins, H.V. (2001). Treating substance-using women and their children in public housing: Preliminary evaluation findings. Child Welfare, 80(2), 199-220.
Middlemiss, W., and McGuigan, W. (2005). Ethnicity and adolescent mothers’ benefit from participation in home-visitation services. Family Relations, 54(2), 212-224.
Mikami, A.Y., Lerner, M.D., Griggs, M.S., McGrath, A., and Calhoun, C.D. (2010). Parental influence on children with attention-deficit/hyperactivity disorder: II. Results of a pilot intervention training parents as friendship coaches for children. Journal of Abnormal Child Psychology, 38(6), 737-749.
Miller, B.A., Wilsnack, S.C., and Cunradi, C.B. (2000). Family violence and victimization: Treatment issues for women with alcohol problems. Alcoholism, Clinical and Experimental Research, 24(8), 1287-1297.
Mitchell, O., Wilson, D.B., Eggers, A., and MacKenzie, D.L. (2012). Assessing the effectiveness of drug courts on recidivism: A meta-analytic review of traditional and nontraditional drug courts. Journal of Criminal Justice, 40(1), 60-71.
Moore, B.A. (2012). Handbook of Counseling Military Couples. New York: Taylor & Francis.
Moore, J., and Finkelstein, N. (2001). Parenting services for families affected by substance abuse. Child Welfare, 80(2), 221-238.
Morinis, J., Carson, C., and Quigley, M.A. (2013). Effect of teenage motherhood on cognitive outcomes in children: A population-based cohort study. Archives of Disease in Childhood, 98(12), 959-964.
Mosher, W.D., Jones, J., and Abma, J.C. (2012). Intended and Unintended Births in the United States: 1982-2010. No. 55. Washington, DC: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics.
Najavits, L.M., Weiss, R.D., and Shaw, S.R. (1997). The link between substance abuse and posttraumatic stress disorder in women. A research review. The American Journal on Addictions, 6(4), 273-283.
National Association of County and City Health Officials. (2009). Meeting the Needs of Pregnant and Parenting Teens: Local Health Department Programs and Services. Available: http://www.dhs.state.mn.us/main/groups/agencywide/documents/pub/dhs16_148996.pdf [June 2016].
National Institute on Child Health and Human Development. (2012). What Are Intellectual and Developmental Disabilities? Available: https://www.nichd.nih.gov/health/topics/idds/conditioninfo/Pages/default.aspx [October 2016].
National Institute of Justice. (2016). Drug Courts. Available: http://www.nij.gov/topics/courts/drug-courts/pages/welcome.aspx [June 2016].
National Registry of Evidence-based Programs and Practices. (2016a). SAMHSA’s National Registry of Evidence-based Programs and Practices: Intervention Summary—Incredible Years (IY). Available: http://legacy.nreppadmin.net/ViewIntervention.aspx?id=311 [March 2016].
National Registry of Evidence-based Programs and Practices. (2016b). SAMHSA’s National Registry of Evidence-based Programs and Practices: Intervention Summary—Nurturing Parenting Programs. Available: http://legacy.nreppadmin.net/ViewIntervention.aspx?id=171 [March 2016].
National Registry of Evidence-based Programs and Practices. (2016c). SAMHSA’s National Registry of Evidence-based Programs and Practices: Intervention Summary—Parent-Child Interaction Therapy (PCIT). Available: http://legacy.nreppadmin.net/ViewIntervention.aspx?id=23 [March 2016].
National Registry of Evidence-based Programs and Practices. (2016d). SAMHSA’s National Registry of Evidence-based Programs and Practices: Intervention Summary—Strengthening Families Program. Available: http://legacy.nreppadmin.net/ViewIntervention.aspx?id=44 [March 2016].
National Registry of Evidence-based Programs and Practices. (2016e). SAMHSA’s National Registry of Evidence-based Programs and Practices: Intervention Summary—Triple P-Positive Parenting Program. Available: http://legacy.nreppadmin.net/ViewIntervention.aspx?id=1 [October 2016].
National Research Council. (1993). Understanding Child Abuse and Neglect. Panel on Research on Child Abuse and Neglect, Commission on Behavioral and Social Sciences and Education. Washington, DC: National Academy Press.
Neece, C.L. (2014). Mindfulness-based stress reduction for parents of young children with developmental delays: Implications for parental mental health and child behavior problems. Journal of Applied Research in Intellectual Disabilities, 27(2), 174-186.
Neger, E.N., and Prinz, R.J. (2015). Interventions to address parenting and parental substance abuse: Conceptual and methodological considerations. Clinical Psychology Review, 39, 71-82.
Niccols, A., and Sword, W. (2005). “New choices” for substance-using mothers and their children: Preliminary evaluation. Journal of Substance Use, 10(4), 239-251.
Nicholson, J., and Clayfield, J.C. (2004). Responding to depression in parents. Pediatric Nursing, 30(2), 136-142.
Nicholson, J., and Henry, A.D. (2003). Achieving the goal of evidence-based psychiatric rehabilitation practices for mothers with mental illnesses. Psychiatric Rehabilitation Journal, 27(2), 122-130.
Nicholson, J., Sweeney, E.M., and Geller, J.L. (1998). Mothers with mental illness: I. The competing demands of parenting and living with mental illness. Psychiatric Services, 49(5), 635-642.
Nicholson, J., Biebel, K., Katz-Leavy, J., and Williams, V. (2002). The Prevalence of Parenthood in Adults with Mental Illness: Implications for State and Federal Policymakers, Programs, and Providers. Paper 153. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Nicholson, J., Finkelstein, N., Williams, V., Thom, J., Noether, C., and DeVilbiss, M. (2006). A comparison of mothers with co-occurring disorders and histories of violence living with or separated from minor children. Journal of Behavioral Health Services & Research, 33(2), 225-243.
Nixon, R.D., Sweeney, L., Erickson, D.B., and Touyz, S.W. (2003). Parent-child interaction therapy: A comparison of standard and abbreviated treatments for oppositional defiant preschoolers. Journal of Consulting and Clinical Psychology, 71(2), 251-260.
Nylen, K.J., Moran, T.E., Franklin, C.L., and O’Hara, M.W. (2006). Maternal depression: A review of relevant treatment approaches for mothers and infants. Infant Mental Health Journal, 27(4), 327-343.
Office of Adolescent Health. (2015). OAH Vision and Strategic Priorities. Available: http://www.hhs.gov/ash/oah/about-us [January 2016].
Obeidat, H.M., Bond, E.A., and Callister, L.C. (2009). The parental experience of having an infant in the newborn intensive care unit. The Journal of Perinatal Education, 18(3), 23-29.
O’Connor, M.J., and Paley, B. (2006). The relationship of prenatal alcohol exposure and the postnatal environment to child depressive symptoms. Journal of Pediatric Psychology, 31(1), 50-64.
Odom, S.L., and Chandler, L. (1990). Transition to parenthood for parents of technology-assisted infants. Topics in Early Childhood Special Education, 9(4), 43-54.
Odom, S.L., Boyd, B.A., Hall, L.J., Hume, K.A., Volkmar, F.R., Paul, R., Rogers, S.J., and Pelphrey, K.A. (2014). Comprehensive treatment models for children and youth with autism spectrum disorders. In F.R. Volkmar, R. Paul, S.J. Rogers, and K.A. Pelphrey (Eds.), Handbook of Autism and Pervasive Developmental Disorders (4th ed., pp. 770-787). Hoboken, NJ: John Wiley & Sons.
O’Hara, M.W., and McCabe, J.E. (2013). Postpartum depression: Current status and future directions. Annual Review of Clinical Psychology, 9, 379-407.
Olds, D.L., Robinson, J., O’Brien, R., Luckey, D.W., Pettitt, L.M., Henderson, C.R., Jr., Ng, R.K., Sheff, K.L., Korfmacher, J., Hiatt, S., and Talmi, A. (2002). Home visiting by paraprofessionals and by nurses: A randomized, controlled trial. Pediatrics, 110(3), 486-496.
Olds, D.L., Robinson, J., Pettitt, L., Luckey, D.W., Holmberg, J., Ng, R.K., Isacks, K., Sheff, K., and Henderson, C.R., Jr. (2004). Effects of home visits by paraprofessionals and by nurses: Age 4 follow-up results of a randomized trial. Pediatrics, 114(6), 1560-1568.
Olds, D.L., Sadler, L., and Kitzman, H. (2007). Programs for parents of infants and toddlers: Recent evidence from randomized trials. Journal of Child Psychology and Psychiatry, 48(3/4), 355-391.
Oyserman, D., Mowbray, C.T., Meares, P.A., and Firminger, K.B. (2000). Parenting among mothers with a serious mental illness. American Journal of Orthopsychiatry, 70(3), 296-315.
Pajulo, M., and Kalland, M. (2013). Mentalizing-based intervention with mother-baby dyads. In M. Pajulo and L.M. Mayes (Eds.), Parenting and Substance Abuse (pp. 282-302). New York: Oxford University Press.
Pajulo, M., Suchman, N., Kalland, M., and Mayes, L. (2006). Enhancing the effectiveness of residential treatment for substance abusing pregnant and parenting women: Focus on maternal reflective functioning and mother-child relationship. Infant Mental Health Journal, 27(5), 448.
Pajulo, M., Pyykkonen, N., Kalland, M., Sinkkonen, J., Helenius, H., Punamaki, R.L., and Suchman, N. (2012). Substance-abusing mothers in residential treatment with their babies: Importance of pre- and postnatal maternal reflective functioning. Infant Mental Health Journal, 33(1), 70-81.
Paradis, H.A., Sandler, M., Manly, J.T., and Valentine, L. (2013). Building healthy children: Evidence-based home visitation integrated with pediatric medical homes. Pediatrics, 132(Suppl. 2), S174-S179.
Parent-Child Interaction Therapy International. (2015). About PCIT. Available: http://www.pcit.org/resources-for-pcit-therapists/about [October 2016].
Park, J.M., Solomon, P., and Mandell, D.S. (2006). Involvement in the child welfare system among mothers with serious mental illness. Psychiatric Services, 57(4), 493-497.
Patterson, G.R., Chamberlain, P., and Reid, J.B. (1982). A comparative evaluation of a parent-training program. Behavior Therapy, 13(5), 638-650.
Perper, K., Peterson, K., and Manlove, J. (2010). Diploma Attainment among Teen Mothers. Fact Sheet. Publication No. 2010-01. Washington, DC: Child Trends.
Perrin, E.C., Sheldrick, R.C., McMenamy, J.M., Henson, B.S., and Carter, A.S. (2014). Improving parenting skills for families of young children in pediatric settings: A randomized clinical trial. Journal of the American Medical Association Pediatrics, 168(1), 16-24.
Petch, J.F., Halford, W.K., Creedy, D.K., and Gamble, J. (2012). A randomized controlled trial of a couple relationship and coparenting program (couple care for parents) for high- and low-risk new parents. Journal of Consulting and Clinical Psychology, 80(4), 662-673.
Pincus, D.B., Santucci, L.C., Ehrenreich, J.T., and Eyberg, S.M. (2008). The implementation of modified Parent-Child Interaction Therapy for youth with separation anxiety disorder. Cognitive and Behavioral Practice, 15(2), 118-125.
Pinzon, J.L., Jones, V.F., Blythe, M.J., Adelman, W.P., Breuner, C.C., Levine, D.A., Marcell, A.V., Murray, P.J., O’Brien, R.F., High, P.C., Donoghue, E., Fussell, J.J., Gleason, M.M., Jaudes, P.K., Rubin, D.M., and Schulte, E.E. (2012). Care of adolescent parents and their children. Pediatrics, 130(6), e1743-e1756.
Pogarsky, G., Thornberry, T.P., and Lizotte, A.J. (2006). Developmental outcomes for children of young mothers. Journal of Marriage and Family, 68(2), 332-344.
Pooblan, A.S., Aucott, L.S., Ross, L., Smith, W.C.S., Helms, P.J., and Williams, J.H.G. (2007). Effects of treating postnatal depression on mother-infant interaction and child development. British Journal of Psychiatry, 191, 378-386.
Porowski, A.W., Burgdorf, K., and Herrell, J.M. (2004). Effectiveness and sustainability of residential substance abuse treatment programs for pregnant and parenting women. Evaluation and Program Planning, 27(2), 191-198.
Powers, J.D., Bowen, N.K., and Bowen, G.L. (2010). Evidence-based programs in school settings: Barriers and recent advances. Journal of Evidence-Based Social Work, 7(4), 313-331.
Preece, P.M., and Riley, E.P. (2011). Alcohol, Drugs and Medication in Pregnancy: The Long-Term Outcome for the Child. Clinics in Developmental Medicine No. 188. London, UK: MacKeith Press.
Price, J.M., Chamberlain, P., Landsverk, J., and Reid, J. (2009). KEEP foster-parent training intervention: Model description and effectiveness. Child & Family Social Work, 14(2), 233-242.
Prinz, R. (2014). Scaling Family-Focused Preventive Interventions: The Triple P System. Presentation at the Workshop on Strategies for Scaling Tested and Effective Family-Focused Preventive Interventions to Promote Children’s Cognitive, Affective, and Behavioral Health, April 1-2, Washington, DC.
Pruett, M.K., and Barker, R.K. (2010). Effectively intervening with divorcing parents and their children: What works and how it works. In M.S. Schulz, M.K. Pruett, P.K. Kerig, and R.D. Parke (Eds.), Strengthening Couple Relationships for Optimal Child Development: Lessons from Research and Intervention (pp. 181-196). Washington, DC: American Psychological Association.
Putnam-Hornstein, E., Simon, J.D., Eastman, A.L., and Magruder, J. (2015). Risk of re-reporting among infants who remain at home following alleged maltreatment. Child Maltreatment, 20(2), 92-103.
Rapee, R.M., Kennedy, S., Ingram, M., Edwards, S., and Sweeney, L. (2005). Prevention and early intervention of anxiety disorders in inhibited preschool children. Journal of Consulting and Clinical Psychology, 73(3), 488-497.
Read, J.P., Brown, P.J., and Kahler, C.W. (2004). Substance use and posttraumatic stress disorders: Symptom interplay and effects on outcome. Addictive Behaviors, 29(8), 1665-1672.
Reinders, H.S. (2008). Persons with disabilities as parents: What is the problem? Journal of Applied Research in Intellectual Disabilities, 21(4), 308-314.
Repetti, R.L., Taylor, S.E., and Seeman, T.E. (2002). Risky families: Family social environments and the mental and physical health of offspring. Psychological Bulletin, 128(2), 330-366.
Richmond, J.B. (1970). Disadvantaged children: What have they compelled us to learn? Yale Journal of Biology and Medicine, 43(3), 127-144.
Riggs, D.S., Caulfield, M.B., and Street, A.E. (2000). Risk for domestic violence: Factors associated with perpetration and victimization. Journal of Clinical Psychology, 56(10), 1289-1316.
Roberts, M.Y., and Kaiser, A.P. (2011). The effectiveness of parent-implemented language interventions: A meta-analysis. American Journal of Speech-Language Pathology, 20(3), 180-199.
Rogers, S.J., Estes, A., Lord, C., Vismara, L., Winter, J., Fitzpatrick, A., Guo, M., and Dawson, G. (2012). Effects of a brief Early Start Denver Model (ESDM)-based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 51(10), 1052-1065.
Rose, H.D., and Cohen, K. (2010). The experiences of young carers: A meta-synthesis of qualitative findings. Journal of Youth Studies, 13(4), 473-487.
Rosen, D., Warner, L.A., and Tolman, R.M. (2006). Comparing psychiatric service use among low-income women and women in a general household population. Social Work Research, 30(4), 223-232.
Rutherford, H., Potenza, M., and Mayes, L. (2013). Neurobiology of addiction and attachment. In N. Suchman, M. Pajulo, and L. Mayes (Eds.), Parenting and Substance Abuse: Developmental Approaches to Intervention (pp. 3-23). New York: Oxford University Press.
Ryan, J.P., Choi, S., Hong, J.S., Hernandez, P., and Larrison, C.R. (2008). Recovery coaches and substance exposed births: An experiment in child welfare. Child Abuse and Neglect, 32(11), 1072-1079.
Sadler, L.S., Swartz, M.K., and Ryan-Krause, P. (2003). Supporting adolescent mothers and their children through a high school-based child care center and parent support program. Journal of Pediatric Health Care, 17(3), 109-117.
Sadler, L.S., Swartz, M.K., Ryan-Krause, P., Seitz, V., Meadows-Oliver, M., Grey, M., and Clemmens, D.A. (2007). Promising outcomes in teen mothers enrolled in a school-based parent support program and child care center. Journal of School Health, 77(3), 121-130.
Sahler, O.J.Z., Varni, J.W., Fairclough, D.L., Butler, R.W., Noll, R.B., Dolgin, M.J., Phipps, S., Copeland, D.R., Katz, E.R., and Mulhern, R.K. (2002). Problem-solving skills training for mothers of children with newly diagnosed cancer: A randomized trial. Journal of Developmental & Behavioral Pediatrics, 23(2), 77-86.
Sahler, O.J.Z., Fairclough, D.L., Phipps, S., Mulhern, R.K., Dolgin, M.J., Noll, R.B., Katz, E.R., Varni, J.W., Copeland, D.R., and Butler, R.W. (2005). Using problem-solving skills training to reduce negative affectivity in mothers of children with newly diagnosed cancer: Report of a multisite randomized trial. Journal of Consulting and Clinical Psychology, 73(2), 272-283.
Sahler, O.J., Dolgin, M.J., Phipps, S., Fairclough, D.L., Askins, M.A., Katz, E.R., Noll, R.B., and Butler, R.W. (2013). Specificity of problem-solving skills training in mothers of children newly diagnosed with cancer: Results of a multisite randomized clinical trial. Journal of Clinical Oncology, 31(10), 1329-1335.
Sameroff, A.J., and Chandler, M.J. (1975). Reproductive risk and the continuum of caretaking casualty. In F.D. Horowitz, M. Hetherington, S. Scarr-Salapatek, and G. Siegel (Eds.), Review of Child Development Research (vol. 4, pp. 187-244). Chicago, IL: University of Chicago Press.
Sanders, M.R., and Prinz, R.J. (2005). The Triple P system: A multi-level, evidence-based, population approach to the prevention and treatment of behavioral and emotional problems in children. The Register Report, 31, 42-46.
Sanders, M.R., Markie-Dadds, C., Tully, L.A., and Bor, W. (2000). The Triple P-Positive Parenting Program: A comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. Journal of Consulting and Clinical Psychology, 68(4), 624.
Sanders, M., Calam, R., Durand, M., Liversidge, T., and Carmont, S.A. (2008). Does self-directed and web-based support for parents enhance the effects of viewing a reality television series based on the Triple P-Positive Parenting Programme? Journal of Child Psychology and Psychiatry, 49(9), 924-932.
Sanders, M. R., Pickering, J. A, Kirby, J. N., Turner, K. M., Morawska, A., Mazzucchelli, T., Ralph, A., and Sofronoff, K. (2012). A commentary on evidence-based parenting programs: Redressing misconceptions of the empirical support for Triple P. BMC Medicine, 10, 145.
Sanders, M.R., Kirby, J.N., Tellegen, C.L., and Day, J.J. (2014). The Triple P-Positive Parenting Program: A systematic review and meta-analysis of a multi-level system of parenting support. Clinical Psychology Review, 34(4), 337-357.
Sandler, I., Ingram, A., Wolchik, S., Tein, J.-Y., and Winslow, E. (2015). Long-term effects of parenting-focused preventive interventions to promote resilience of children and adolescents. Child Development Perspectives, 9(3), 164-171.
Sangalang, B.B., and Rounds, K. (2005). Differences in health behaviors and parenting knowledge between pregnant adolescents and parenting adolescents. Social Work in Health Care, 42(2), 1-22.
Sangalang, B.B., Barth, R.P., and Painter, J.S. (2006). First-birth outcomes and timing of second births: A statewide case management program for adolescent mothers. Health and Social Work, 31(1), 54-63.
Santacruz, I., Méndez, F.J., and Sánchez-Meca, J. (2006). Play therapy applied by parents for children with darkness phobia: Comparison of two programmes. Child & Family Behavior Therapy, 28(1), 19-35.
Schaeffer, C.M., Swenson, C.C., Tuerk, E.H., and Henggeler, S.W. (2013). Comprehensive treatment for co-occurring child maltreatment and parental substance abuse: Outcomes from a 24-month pilot study of the MST-Building Stronger Families Program. Child Abuse and Neglect, 37(8), 596-607.
Schertz, H.H., Odom, S.L., Baggett, K.M., and Sideris, J.H. (2013). Effects of joint attention mediated learning for toddlers with autism spectrum disorders: An initial randomized controlled study. Early Childhood Research Quarterly, 28(2), 249-258.
Scholer, S.J., Hudnut-Beumler, J., and Dietrich, M.S. (2010). A brief primary care intervention helps parents develop plans to discipline. Pediatrics, 125(2), e242-e249.
Schrank, B., Moran, K., Borghi, C., and Priebe, S. (2015). How to support patients with severe mental illness in their parenting role with children aged over 1 year? A systematic review of interventions. Social Psychiatry and Psychiatric Epidemiology, 50(12), 1765-1783.
Schroeder, M., and Pridham, K. (2006). Development of relationship competencies through guided participation for mothers of preterm infants. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 35(3), 358-368.
Schuetze, P., Eiden, R.D., and Coles, C.D. (2007). Prenatal cocaine and other substance exposure: Effects on infant autonomic regulation at 7 months of age. Developmental Psychobiology, 49(3), 276-289.
Schuhmann, E.M., Foote, R.C., Eyberg, S.M., Boggs, S.R., and Algina, J. (1998). Efficacy of parent-child interaction therapy: Interim report of a randomized trial with short-term maintenance. Journal of Clinical Child Psychology, 27(1), 34-45.
Seeman, M.V. (2012). Antipsychotic-induced somnolence in mothers with schizophrenia. The Psychiatric Quarterly, 83(1), 83-89.
Segre, L.S., Siewert, R.C., Brock, R.L., and O’Hara, M.W. (2013). Emotional distress in mothers of preterm hospitalized infants: A feasibility trial of nurse-delivered treatment. Journal of Perinatology, 33(12), 924-928.
Shadish, W.R., and Baldwin, S.A. (2005). Effects of behavioral marital therapy: A meta-analysis of randomized controlled trials. Journal of Consulting and Clinical Psychology, 73(1), 6-14.
Shanok, A.F., and Miller, L. (2007). Stepping up to motherhood among inner-city teens. Psychology of Women Quarterly, 31(3), 252-261.
Sharps, P., Alhusen, J.L., Bullock, L., Bhandari, S., Ghazarian, S., Udo, I.E., and Campbell, J. (2013). Engaging and retaining abused women in perinatal home visitation programs. Pediatrics, 132(Suppl. 2), S134-S139.
Siegel, R.S., and Brandon, A.R. (2014). Adolescents, pregnancy, and mental health. Journal of Pediatric and Adolescent Gynecology, 27(3), 138-150.
Siegenthaler, E., Munder, T., and Egger, M. (2012). Effect of preventive interventions in mentally ill parents on the mental health of the offspring: Systematic review and meta-analysis. Journal of the American Academy of Child & Adolescent Psychiatry, 51(1), 8-17.
Siller, M., Morgan, L., Turner-Brown, L., Baggett, K.M., Baranek, G.T., Brian, J., Bryson, S.E., Carter, A.S., Crais, E.R., Estes, A., Kasari, C., Landa, R.J., Lord, C., Messinger, D.S., Mundy, P., Odom, S.L., Reznick, J.S., Roberts, W., Rogers, S.J., Schertz, H.H., Smith, I.M., Stone, W.L., Watson, L.R., Wetherby, A.M., Yoder, P.J., and Zwaigenbaum, L. (2013). Designing studies to evaluate parent-mediated interventions for toddlers with autism spectrum disorder. Journal of Early Intervention, 35(4), 355-377.
Silverstein, M., Feinberg, E., Cabral, H., Sauder, S., Egbert, L., Schainker, E., Kamholz, K., Hegel, M., and Beardslee, W. (2011). Problem-solving education to prevent depression among low-income mothers of preterm infants: A randomized controlled pilot trial. Archives of Women’s Mental Health, 14(4), 317-324.
Singer, G.H., Ethridge, B.L., and Aldana, S.I. (2007). Primary and secondary effects of parenting and stress management interventions for parents of children with developmental disabilities: A meta-analysis. Mental Retardation and Developmental Disabilities Research Reviews, 13(4), 357-369.
Sinha, R. (2001). How does stress increase risk of drug abuse and relapse? Psychopharmacology, 158(4), 343-359.
Smith, M.V. (2014). The New Haven Moms Partnership: Combatting Depression, Reducing Stress and Building Foundational Skills for Success. Available: http://www.buildingbetterprograms.org/wp-content/uploads/2014/03/New-Haven-MOMSPartnership-Slides.pdf [February 2016].
Sofronoff, K., Jahnel, D., and Sanders, M. (2011). Stepping Stones Triple P seminars for parents of a child with a disability: A randomized controlled trial. Research in Developmental Disabilities, 32(6), 2253-2262.
Solantaus, T., Paavonen, E.J., Toikka, S., and Punamäki, R.-L. (2010). Preventive interventions in families with parental depression: Children’s psychosocial symptoms and prosocial behaviour. European Child & Adolescent Psychiatry, 19(12), 883-892.
Solomon, R., and Liefeld, C.P. (1998). Effectiveness of a family support center approach to adolescent mothers: Repeat pregnancy and school drop-out rates. Family Relations, 47(2), 139-144.
Stadnick, N.A., Stahmer, A., and Brookman-Frazee, L. (2015). Preliminary effectiveness of Project ImPACT: A parent-mediated intervention for children with autism spectrum disorder delivered in a community program. Journal of Autism and Developmental Disorders, 45(7), 2092-2104.
Stepp, S.D., Whalen, D.J., Pilkonis, P.A., Hipwell, A.E., and Levine, M.D. (2012). Children of mothers with borderline personality disorder: Identifying parenting behaviors as potential targets for intervention. Personality Disorders: Theory, Research, and Treatment, 3(1), 76-91.
Stevens-Simon, C., Kelly, L., and Kulick, R. (2001). A village would be nice but . . . : It takes a long-acting contraceptive to prevent repeat adolescent pregnancies. American Journal of Preventive Medicine, 21(1), 60-65.
Stith, S.M., and McCollum, E.E. (2009). Couples treatment for psychological and physical aggression. In K.D. O’Leary and E.M. Woodin (Eds.), Psychological and Physical Aggression in Couples: Causes and Interventions (pp. 233-250). Washington, DC: American Psychological Association.
Stith, S.M., McCollum, E.E., Amanor-Boadu, Y., and Smith, D. (2012). Systemic perspectives on intimate partner violence treatment. Journal of Marital and Family Therapy, 38(1), 220-240.
Stover, C.S., Meadows, A.L., and Kaufman, J. (2009). Interventions for intimate partner violence: Review and implications for evidence-based practice. Professional Psychology: Research and Practice, 40(3), 223-233.
Strathearn, L., and Mayes, L.C. (2010). Cocaine addiction in mothers: Potential effects on maternal care and infant development. Annals of the New York Academy of Sciences, 1187, 172-183.
Strathearn, L., Li, J., Fonagy, P., and Montague, P.R. (2008). What’s in a smile? Maternal brain responses to infant facial cues. Pediatrics, 122(1), 40-51.
Strauss, K., Mancini, F., and Fava, L. (2013). Parent inclusion in early intensive behavior interventions for young children with ASD: A synthesis of meta-analyses from 2009 to 2011. Research in Developmental Disabilities, 34(9), 2967-2985.
Substance Abuse and Mental Health Services Administration. (2014a). Grants to Expand Services to Children Affected by Methamphetamine in Families Participating in Family Drug Court. Available: https://ncsacw.samhsa.gov/files/CAM_Brief_2014-Final.pdf [January 2016].
Substance Abuse and Mental Health Services Administration. (2014b). Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings. NSDUH Series H-48, HHS Publication No. (SMA) 14-4863. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Suchman, N., Mayes, L., Conti, J., Slade, A., and Rounsaville, B. (2004). Rethinking parenting interventions for drug-dependent mothers: From behavior management to fostering emotional bonds. Journal of Substance Abuse Treatment, 27(3), 179-185.
Suchman, N., DeCoste, C., Castiglioni, N., Legow, N., and Mayes, L. (2008). The Mothers and Toddlers Program: Preliminary findings from an attachment-based parenting intervention for substance-abusing mothers. Psychoanalytic Psychology, 25(3), 499-517.
Suchman, N.E., DeCoste, C., Castiglioni, N., McMahon, T.J., Rounsaville, B., and Mayes, L. (2010). The Mothers and Toddlers Program, an attachment-based parenting intervention for substance using women: Post-treatment results from a randomized clinical pilot. Attachment & Human Development, 12(5), 483-504.
Suchman, N., DeCoste, C., Ordway, M.R., and Bers, S. (2013). Mothering from the inside out: A mentalization-based individual therapy for mothers with substance use disorders. In N.E. Suchman, M. Pajula, and L.M. Mayes (Eds.), Parenting and Substance Abuse: Developmental Approaches to Intervention (pp. 407-433). New York: Oxford University Press.
Sullivan, C.M. (2012). Domestic Violence Shelter Services: A Review of the Empirical Evidence, Harrisburg, PA: National Resource Center on Domestic Violence. Available: http://www.dvevidenceproject.org/wp-content/themes/DVEProject/files/research/DVShelterResearchSummary10-2012.pdf [January 2016].
Swenson, C.C., and Schaeffer, C.M. (2011). Multisystemic therapy for child abuse and neglect. In A. Rubin and D. Springer (Eds.), Programs and Interventions for Maltreated Children and Families at Risk (pp. 31-42). Hoboken, NJ: Wiley.
Swenson, C.C., Schaeffer, C.M., Tuerk, E.H., Henggeler, S.W., Tuten, M., Panzarella, P., Laue, C., Remmele, L., Foley, T., Cannata, E., and Guillorn, A. (2009). Adapting multisystemic therapy for co-occurring child maltreatment and parental substance abuse: The building stronger families project. Emotional and Behavioral Disorders in Youth, 1, 3-8.
Swenson, C.C., Schaeffer, C.M., Henggeler, S.W., Faldowski, R., and Mayhew, A.M. (2010). Multisystemic therapy for child abuse and neglect: A randomized effectiveness trial. Journal of Family Psychology, 24(4), 497-507.
Szuster, R.R., Rich, L.L., Chung, A., and Bisconer, S.W. (1996). Treatment retention in women’s residential chemical dependency treatment: The effect of admission with children. Substance Use and Misuse, 31(8), 1001-1013.
Tajima, E.A., Herrenkohl, T.I., Moylan, C.A., and Derr, A.S. (2011). Moderating the effects of childhood exposure to intimate partner violence: The roles of parenting characteristics and adolescent peer support. Journal of Research on Adolescence, 21(2), 376-394.
Tandon, S.D., Leis, J.A., Mendelson, T., Perry, D.F., and Kemp, K. (2014). Six-month outcomes from a randomized controlled trial to prevent perinatal depression in low-income home visiting clients. Maternal and Child Health Journal, 18(4), 873-881.
Tellegen, C.L., and Sanders, M.R. (2013). Stepping Stones Triple P-Positive Parenting Program for children with disability: A systematic review and meta-analysis. Research in Developmental Disabilities, 34(5), 1556-1571.
Timmer, S.G., Ware, L.M., Urquiza, A.J., and Zebell, N.M. (2010). The effectiveness of parent-child interaction therapy for victims of interparental violence. Violence and Victims, 25(4), 486-503.
Tonge, B., Brereton, A., Kiomall, M., Mackinnon, A., King, N., and Rinehart, N. (2006). Effects on parental mental health of an education and skills training program for parents of young children with autism: A randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 45(5), 561-569.
Tsivos, Z.-L., Calam, R., Sanders, M.R., and Wittkowski, A. (2015). Interventions for postnatal depression assessing the mother-infant relationship and child developmental outcomes: A systematic review. International Journal of Women’s Health, 7, 429-447.
Turner, K.M., and Sanders, M.R. (2006). Help when it’s needed first: A controlled evaluation of brief, preventive behavioral family intervention in a primary care setting. Behavior Therapy, 37(2), 131-142.
U.S. Department of Education. (2015a). Building the Legacy: IDEA 2004: Sec. 636 Individualized Family Service Plan. Available: http://idea.ed.gov/explore/view/p/%2Croot%2Cstatute%2CI%2CC%2C636%2C [October 2016].
U.S. Department of Education. (2015b). Building the Legacy: IDEA 2014: Sec. 632 Definitions. Available: http://idea.ed.gov/explore/view/p/%2Croot%2Cstatute%2CI%2CC%2C632%2C [October 2016].
U.S. Department of Health and Human Services. (1999). Blending Perspectives and Building Common Ground. A Report to Congress on Substance Abuse and Child Protection. Washington, DC: U.S. Government Printing Office.
U.S. Department of Health and Human Services. (2014a). Targeted Grants to Increase the Well-Being of, and to Improve the Permanency Outcomes for, Children Affected by Methamphetamine or Other Substance Abuse: Third Annual Report to Congress. Washington, DC: U.S. Department of Health and Human Services; Administration for Children and Families; Administration on Children, Youth and Families; Children’s Bureau.
U.S. Department of Health and Human Services. (2014b). The Maternal, Infant, and Early Childhood Home Visiting (MIECHV) Program: Snapshot Reports of Benchmark Measures Selected by Grantees. ORE Report No. 2014-26. Available: http://mchb.hrsa.gov/programs/homevisiting/ta/resources/snapshotbenchmarkmeasures.pdf [October 2016].
U.S. Preventive Services Task Force. (2009). Screening for depression in adults: U.S. Preventive Services Task Force recommendation statement. Annals of Internal Medicine, 151(11), 784-792.
Van Horn, P., and Reyes, V. (2014). Child-parent psychotherapy with infants and very young children. In S. Timmer and A. Urquiza (Eds.), Evidence-Based Approaches for the Treatment of Maltreated Children (pp. 61-77). New York: Springer.
Voisin, D., and Hong, J. (2012). A conceptual formulation examining the relationship between witnessing domestic violence and bullying behaviors and victimization among youth. Educational Psychology Review, 24(4), 479-498.
Wade, C., Llewellyn, G., and Matthews, J. (2008). Review of parent training interventions for parents with intellectual disability. Journal of Applied Research in Intellectual Disabilities, 21(4), 351-366.
Wahl, K., and Metzner, C. (2012). Parental influences on the prevalence and development of child aggressiveness. Journal of Child and Family Studies, 21(2), 344-355.
Webster-Stratton, C. (1984). Randomized trial of two parent-training programs for families with conduct-disordered children. Journal of Consulting and Clinical Psychology, 52(4), 666-678.
Weissman, M.M., Pilowsky, D.J., Wickramaratne, P.J., Talati, A., Wisniewski, S.R., Fava, M., Hughes, C.W., Garber, J., Malloy, E., King, C.A., Cerda, G., Sood, A.B., Alpert, J.E., Trivedi, M.H., and Rush, A.J. (2006). Remissions in maternal depression and child psychopathology: A STAR*D-child report. Journal of the American Medical Association, 295(12), 1389-1398.
What Works Clearinghouse. (2014). What Works Clearinghouse: Procedures and Standards Handbook Version 3.0. Washington, DC: U.S. Department of Education, Institute of Education Sciences.
Wildeman, C., Emanuel, N., Leventhal, J.M., Putnam-Hornstein, E., Waldfogel, J., and Lee, H. (2014). The prevalence of confirmed maltreatment among U.S. children, 2004 to 2011. Journal of the American Medical Association Pediatrics, 168(8), 706-713.
Wilson, P., Rush, R., Hussey, S., Puckering, C., Sim, F., Allely, C.S., Doku, P., McConnachie, A., and Gillberg, C. (2012). How evidence-based is an “evidence-based parenting program”? A prisma systematic review and meta-analysis of Triple P. BMC Medicine, 10, 130.
Wittkowski, A., McGrath, L., and Peters, S. (2014). Exploring psychosis and bipolar disorder in women: A critical review of the qualitative literature. BMC Psychiatry, 14(1), 1-14.
Wobie, K., Eyler, F.D., Conlon, M., Clarke, L., and Behnke, M. (1997). Women and children in residential treatment: Outcomes for mothers and their infants. Journal of Drug Issues, 27(3), 585-606.
Wolfe, D.A., Crooks, C.V., Lee, V., McIntyre-Smith, A., and Jaffe, P.G. (2003). The effects of children’s exposure to domestic violence: A meta-analysis and critique. Clinical Child and Family Psychology Review, 6(3), 171-187.
Woodman, A.C. (2014). Trajectories of stress among parents of children with disabilities: A dyadic analysis. Family Relations, 63(1), 39-54.
Worcel, S.D., Furrer, C.J., Green, B.L., Burrus, S.W.M., and Finigan, M.W. (2008). Effects of family treatment drug courts on substance abuse and child welfare outcomes. Child Abuse Review, 17(6), 427-443.
Wu, J., DiCicco-Bloom, B., Greenberg, S., and Sahulhameed, F. (2012). Breaking the cycle of adolescent pregnancy: Can mothers influence their daughters’ contraceptive behavior? Contraception, 86(2), 186.
Wulczyn, F., Hislop, K.B., and Harden, B.J. (2002). The placement of infants in foster care. Infant Mental Health Journal, 23(5), 454-475.
Yakima Valley Farm Workers Clinic. (2013). Yakima Valley Farm Workers Clinic Enhanced Yakima County Nurse-Family Partnership (EYCNFP) Program at Children’s Village: Final Report. Grant No. 90CA1756. Available: https://library.childwelfare.gov/cwig/ws/library/docs/gateway/Blob/89704.pdf;jsessionid=77C9A30DCC63FDD5597CA41BE0329685?w=NATIVE%28%27TITLE+ph+is+%27%27Final+Report%3A+Yakima+Valley+Farm+Workers+Clinic%27%27%2C%27%27Enhanced+Yakima+County+NurseFamily+Partnership+%28EYCNFP%29+Program+at+Children%27%27%27%27s+Village%27%27%27%29&upp=0&order=native%28%27year%2FDescend%27%29&rpp=25&r=1&m=1 [January 2016].
Zubrick, S., Ward, K., Silburn, S., Lawrence, D., Williams, A., Blair, E., Robertson, D., and Sanders, M. (2005). Prevention of child behavior problems through universal implementation of a group behavioral family intervention. Prevention Science, 6(4), 287-304.
































































































