
2
The Case for Investing in Pandemic Preparedness
The global community has massively underestimated the risks that pandemics present to human life and livelihoods, at least in terms of policy outcomes. The resources devoted to preventing and responding to such threats seem wholly inadequate to the scale of the risk. While it is impossible to produce precise estimates for the probability and potential impact of pandemics, it is not difficult to demonstrate a compelling case for greater investment. There are very few risks facing humankind that threaten loss of life on the scale of pandemics.
A pandemic could kill as many people as a devastating war, yet the resources committed to pandemic prevention and response are a fraction of the resources we commit to security. There are also very few risks that have greater potential for catastrophic economic impact—potentially on the scale of a global financial crisis—but the measures we are taking to avoid another financial crisis are of an entirely different magnitude.1
The costs of significantly upgrading the world’s defenses against pandemics, while substantial, are not out of reach. The recent Ebola outbreak revealed many gaps and shortcomings in preparedness and the ability to respond effectively at both the national and global levels. These flaws in our defenses cost thousands of lives and meant that the ultimate cost of preventing Ebola from becoming a pandemic was much higher than it may otherwise have been. Ebola also demonstrated that being better prepared has huge benefits. For example, Nigeria contained the virus successfully, despite being a densely populated nation with many health and social challenges.
The Commission believes that commitment of an incremental $4.5 billion2 per year would make the world much safer. This figure includes expenditures for strengthening national public health systems; funding research and development; and financing global coordination and contingency efforts, all of which are explored in greater detail in subsequent chapters. While it may be beneficial to spend more, investing at least this much would address the most urgent weaknesses in global health security. In addition to shoring up our defenses against pandemics, this investment would also yield enormous benefits in protecting the world against other health risks, such as antimicrobial resistance (AMR) and bioterrorism.
How does $4.5 billion per year stack up against the potential risks? The 1918 influenza pandemic killed approximately 50 million people (CDC, 2014) and arguably as high as 100 million in 1918–1920 (Johnson and Mueller, 2002). As a driver of incremental mortality in the last century, few other events even compare: total deaths from World War II are estimated to be between 35 and 60 million,3 and HIV/AIDS has killed nearly 40 million people since the start of the epidemic (UNAIDS, 2014). Moreover, despite enormous advances in medicine and scientific understanding, and the containment of recent pandemic threats such as severe actue respiratory syndrome (SARS), H1N1 influenza, and, eventually, Ebola, we should not be complacent about future risks. The consensus among leading epidemiologists and public health experts is the threat from infectious diseases is growing. Emerging infectious disease events are increasing significantly over time (Jones, 2008), and, with an
___________________
1 This section draws on “Modeling the Economic Threat of Pandemics” by Anas El Turabi and Philip Saynisch (see Appendix C).
2 All monetary figures in U.S. dollars.
3 Encyclopaedia Britannica, 15th ed., s.vv. “World Wars.”
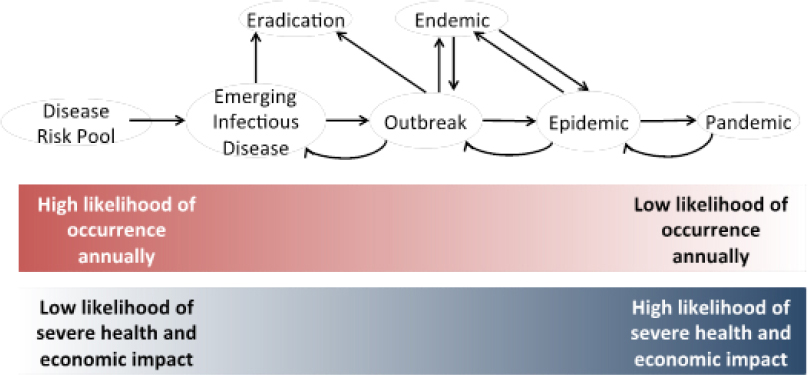
SOURCE: Figure created for the GHRF Commission by El Turabi and Saynisch, Harvard University.
ever-increasing global population, greater consumption of meat, and continuing increases in mobility and connectivity, the conditions for infectious disease emergence and contagion are more dangerous than ever. $4.5 billion annually equates to just 65 cents per person; with such a modest investment, we could better protect everyone in the world from such risks.
From an economic perspective, the argument is equally compelling. The World Bank has estimated the economic impact of a severe pandemic (that is, one on the scale of the influenza pandemic of 1918–1919) at nearly 5 percent of global gross domestic product (GDP), or roughly $3 trillion (Jonas, 2014). Some might see this as an exaggeration, but it could also be an underestimate. Aggregate cumulative GDP losses for Guinea, Liberia, and Sierra Leone in 2014 and 2015 are estimated to amount to more than 10 percent (UNDG, 2015; World Bank, 2014). This huge cost is the result of an epidemic that, for all its horror, infected only about 0.25 percent of the population of Liberia, roughly 0.25 percent of the population of Sierra Leone, and less than 0.05 percent of the population of Guinea (WHO, 2016), with approximately 11,300 total deaths (CDC, 2016). The Commission’s own scenario modeling, based on the World Bank parameters, suggests that during the 21st century global pandemics could cost in excess of $6 trillion, with an expected loss of more than $60 billion per year (see Appendix C).4
Indeed, the economic impact of infectious diseases appears to be increasing as greater human and economic connectedness—whether through transnational supply chains, increased travel, or ubiquitous access to communication technologies and media—fuel contagion, both of the virus itself and of fear. Most of the economic impact of pandemics stems not from mortality but from behavioral change, as people seek to avoid infection (Burns et al., 2008). This behavioral change is driven by fear, which in turn is driven by a potent mix of awareness and ignorance. As Poincaré noted with respect to the plague, “the plague was nothing; fear of the plague was much more formidable” (Poincaré, 1905). The experience of SARS is instructive: viewed from the perspective of overall mortality, SARS infected “only” 8,000 people and killed less than 800 (WHO, 2003). Yet the economic cost of SARS has been estimated at more than $40 billion (Lee and McKibbin, 2004). At the peak of SARS, Hong Kong saw an 80 percent reduction in air traffic (Lee and McKibbin, 2004) and a 50 percent reduction in retail sales (Siu and Wong, 2004).
One reason that pandemics are so hard to predict, and their costs so hard to estimate, is that they are not discrete events, but represent the extreme end of a spectrum of infectious disease risks (see Figure 2-1). New infectious diseases emerge annually. Outbreaks, both of new infectious
___________________
4 The expected loss refers to the amount that the global economy will lose each year of the century, on average. It is calculated by multiplying the probability of a loss occurring in any year by the size of the loss.
diseases and of known pathogens, occur many times every year. A small proportion of such outbreaks evolves into epidemics; others are contained, eradicated, or become endemic. An even smaller proportion of epidemics turns into pandemics. Therefore, pandemic risk should not be seen in isolation, but rather as part of a spectrum of escalating disease events, with both costs and potential for mitigation across the entire spectrum.
Viewed from this perspective, the task for policy makers is not just to reduce the likelihood and cost of pandemics as extreme right-tail events, but to reduce the economic and human costs across the whole spectrum of infectious disease threats. We should not become fixated on the probability of a “once-in-a-100-years” pandemic of the 1918–1919 influenza pandemic of severity. Much less virulent pandemics can still cause significant loss of life and economic impact. The influenza pandemics of 1958 and 1968, while far less deadly than the one in 1918–1919, are estimated to have cost 3.1 percent and 0.7 percent of global GDP, respectively (McKibbin and Sidorenko, 2006). Potential pandemics, that is outbreaks or epidemics that could become pandemics if not effectively contained, can also have enormous impact. Ebola, an epidemic that looked as if might have the potential to become a pandemic, has killed more than 11,000 people (CDC, 2016) and cost more than $2 billion (World Bank, 2014). While there is a high degree of uncertainty, the Commission’s own modeling suggests that we are more likely than not to see at least one pandemic over the next 100 years, and there is at least a 20 percent chance of seeing four or more (see Appendix C).
Framed in this way, the investment case for pandemic preparedness and response rests not just on the probability and costs attached to a severe pandemic, but also on the likely costs to human lives and livelihoods across the spectrum of infectious disease threats. The apparent acceleration in the emergence of new infectious diseases underscores the need for a “One Health” approach, which recognizes the connection of human health to animal and plant health. Further outbreaks of new, dormant, or even well-known diseases are a certainty. More epidemics with the potential to become pandemics should be anticipated.
Among the known threats are multiple strains of influenza, coronaviruses, and vector-borne diseases—headlined by malaria but also including other endemic conditions that are still spreading because of climate change among other reasons. There is also always the possibility of re-emerging or completely new zoonotic viruses, or of different kinds of infectious threats, such as fungal infections, particularly in the context of growing AMR. Such potential pandemics are perhaps more frequent than is recognized; in the past 15 years, we have faced at least five: SARS, H5N1, H1N1, Ebola, and Middle East respiratory syndrome (MERS).
So, even if we downplay the likelihood of a catastrophic pandemic—and this would certainly be a mistake—there is a powerful case for investing more to minimize the frequency and mitigate the impact of potential pandemics. We appear to have been successful in preventing Ebola from becoming a pandemic, but at far greater cost in terms of lives and dollars than would have been necessary had we been better prepared.
Given the degree of uncertainty in this arena, it also makes sense to think about the relative costs of error—of investing too much or investing too little. If we overinvest, we will have upgraded primary health care and public health systems more than merited by the pandemic threat alone and spent more on vaccine and diagnostic research than strictly necessary. Yet it is hard to see this as wasted money. The core capabilities of primary care and public health systems are crucial to achieving many other health objectives. For example, reinforcing disease surveillance and response capabilities will have benefits for the management and treatment of endemic diseases, such as tuberculosis and malaria, which themselves cause significant loss of life and economic harm. Tuberculosis affects 8.5 million globally each year, reducing labor productivity by about 30 percent and reducing global GDP by about $12 billion per year (Fonkwo, 2008). Malaria affects approximately 150 million people each year (Global Burden of Disease Study 2013 Collaborators, 2015), and is estimated to reduce GDP for sub-Saharan African countries by some 10 percent (Sachs and Malaney, 2002). Such investments in the foundations of national health systems would also play a role in mitigating the threats to health security from noncommunicable diseases (Heymann et al., 2015). On the other hand, if we invest too little, we open the door to potential disaster.
The investment case for reinforcing global capabilities, rather than simply each country’s own preparedness, does not depend on altruism, although such a moral argument clearly exists. To make themselves safer, rich countries must help the poorer parts of the world, because
global health security is truly a public good. Zoonotic transfers and outbreaks in even the poorest parts of the world can have global impact, as both HIV/AIDS and Ebola demonstrate.
It is instructive to take pandemics out of the medical context and think about the threat as a national security issue. For any one country, a pandemic is a threat that could kill hundreds and thousands every few years—and might potentially kill millions. Yet in most countries it attracts a small fraction of the resources devoted to national defense. Global military spending amounts to more than $2 trillion (CIA, 2015); many countries participate in highly structured and well-resourced international alliances, such as the North Atlantic Treaty Organization (NATO); and most countries regularly conduct exercises to test preparedness and response. As Bill Gates has pointed out, the contrast with the small amount of resources devoted to protecting humankind from potential pandemics is striking (Gates, 2015).
It is equally illuminating to consider pandemics as an economic risk. Despite the compelling evidence of the disruption caused by potential pandemics, their threat to economic stability typically receives very little attention from economic policy makers at either the national or international levels, and even fewer resources. Since the global financial crisis of 2008, policy makers have forced banks to dramatically increase their capital levels as a protection against future crisis, the cost of which is ultimately borne by society as a whole, through lower returns on equity or higher costs of credit. Consider the new total loss absorbing capacity (TLAC) rule, which applies only to the 27 largest banks in the world. The direct costs of this rule are estimated at $17 billion, and the resulting higher credit spreads are expected to cost approximately $20 billion in reduced GDP growth. This single component of the investment in preventing a future financial crisis dwarfs our Commission’s proposed spending on pandemic risk (BIS, 2015).
Our point is not to argue that we spend too much or too little on other threats to security or economic stability, but rather to highlight out how relatively little we invest to protect the world from the threat of infectious diseases. One truth that holds across many different types of potentially catastrophic risks, including pandemics, is that prevention is far more cost-effective than response, and that the most effective response is a well-prepared response. In other words, spending money now will save money and lives later.
Recommendations:
The G7, G20, and United Nations (UN), under the leadership of the UN Secretary General, should reinforce and sustain international focus and actions to protect human lives and livelihoods from the threat of infectious diseases by:
Recommendation A.1: Committing to implementing the framework set out in the report The Neglected Dimension of Global Security: A Framework to Counter Infectious Disease Crises and embodied in Recommendations B.1–D.3.
Recommendation A.2: Committing and mobilizing the incremental financial resources required to implement the framework, as set out in the report The Neglected Dimension of Global Security: A Framework to Counter Infectious Disease Crises, which amount to about $4.5 billion per year.
Recommendation A.3: Monitoring progress of implementation by commissioning an independent assessment in 2017 and every 3 years thereafter.
REFERENCES
BIS (Bank for International Settlements). 2015. Assessing the economic costs and benefits of TLAC implementation. Basel, Switzerland: BIS.
Burns, A., D. van der Mensbrugghe, and H. Timmer. 2008. Evaluating the economic consequences of avian influenza. Washington, DC: World Bank.
CDC (Centers for Disease Control and Prevention). 2014. Reconstruction of the 1918 Influenza Pandemic Virus. http://www.cdc.gov/flu/about/qa/1918flupandemic.htm (accessed November 15, 2015).
CDC. 2016. 2014 Ebola outbreak in West Africa—case counts. http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/casecounts.html (accessed February 1, 2016).
CIA (Central Intelligence Agency). 2015. The world factbook. https://www.cia.gov/library/publications/the-world-factbook/geos/xx.html (accessed November 30, 2015).
Fonkwo, P. N. 2008. Pricing infectious disease: The economic and health implications of infectious diseases. EMBO Reports 9(Suppl 1):S13-S17.
Gates, B. 2015. The next epidemic—lessons from Ebola. New England Journal of Medicine 372(15):1381-1384.
Global Burden of Disease Study 2013 Collaborators. 2015. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 386(9995):743-800.
Heymann, D. L., L. Chen, K. Takemi, D. P. Fidler, J. W. Tappero, M. J. Thomas, T. A. Kenyon, T. R. Frieden, D. Yach, S. Nishtar, A. Kalache, P. L. Olliaro, P. Horby, E. Torreele, L. O. Gostin, M. Ndomondo-Sigonda, D. Carpenter, S. Rushton, L. Lillywhite, B. Devkota, K. Koser, R. Yates, R. S. Dhillon, and R. P. Rannan-Eliya. 2015. Global health security: the wider lessons from the West African Ebola virus disease epidemic. Lancet 385(9980):1884-1901.
Johnson, N. P. A. S., and J. Mueller. 2002. Updating the accounts: Global mortality of the 1918–1920 “Spanish” influenza pandemic. Bulletin of the History of Medicine 76:105-115.
Jonas, O. 2014. Pandemic risk. Washington, DC: World Bank.
Jones, K. E., N. G. Patel, M. A. Levy, A. Storeygard, D. Balk, J. L. Gittleman, and P. Daszak. 2008. Global trends in emerging infectious diseases. Nature 451(7181):990-993.
Lee, J. W., and W. J. McKibbin. 2004. Estimating the global economic costs of SARS. Washington, DC: The National Academies Press. Pp. 92-109.
McKibbin, W. J., and A. A. Sidorenko. 2006. Global macroeconomic consequences of pandemic influenza. Sydney, Australia: Lowy Institute for International Policy, The Australian National University.
Poincaré, H. 1905. La valeur de la science. Paris: Flammarion.
Sachs, J., and P. Malaney. 2002. The economic and social burden of malaria. Nature 415(6872):680-685.
Siu, A., and R. Y. C. Wong. 2004. Economic impact of SARS: The case of Hong Kong. Asian Economic Papers. Cambridge, MA: MIT Press.
UNAIDS (Joint United Nations Programme on HIV/AIDS). 2014. Fact sheet 2014—global statistics. http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/documents/factsheet/2014/20140716_FactSheet_en.pdf (accessed February 1, 2016).
UNDG (United Nations Development Group)–Western and Central Africa. 2015. Socio-economic impact of Ebola virus disease in West African countries. Addis Ababa, Ethiopia: UNDG.
World Bank, 2014. The economic impact of the 2014 Ebola epidemic: Short and medium term estimates for West Africa. Washington, DC: World Bank.
WHO (World Health Organization). 2003. Summary of probable SARS cases with onset of illness from 1 November 2002 to 31 July 2003. http://www.who.int/csr/sars/country/table2003_09_23/en (accessed February 1, 2016).
WHO. 2016. Ebola Situation Report—20 January 2016. http://apps.who.int/ebola/current-situation/ebola-situation-report-20january-2016 (accessed February 1, 2016).
This page intentionally left blank.






