
6
Achieving the Vision
Over the course of the workshop, several themes emerged which highlighted areas in genomic medicine that may benefit from the tools and approaches of implementation science. Genetic research has contributed a great deal to the understanding and treatment of human diseases, and the adoption of genomic medicine holds tremendous potential to improve public health (Green et al., 2015). However, evidence suggests that individuals from minority populations and disadvantaged socioeconomic backgrounds receive fewer therapeutic interventions and poorer quality medical care (AHRQ, 2015). Several workshop speakers pointed out that in order to ensure equitable access to genomic medicine, greater efforts will be required to address health inequities across low income and minority groups.1 To maximize the benefits of genomic medicine across populations, patients and study participants will need adequate knowledge about genomics that allows them to make well-informed health decisions (Hurle et al., 2013). Projects aimed at increasing genomic literacy among patients, providers, and the public would facilitate a more efficient uptake of genomics into clinical practice, said Bernice Coleman of Cedars Sinai Medical Center, Los Angeles. Finally, additional research and recommendations that address the variability in reimbursement policies for genomic applications may help to accelerate their uptake, said Robert McDonough of Aetna.
In the final session of the workshop, a panel of stakeholders individually proposed actionable next steps that could potentially improve and accelerate the translational pipeline for genomics. Box 6-1 contains suggested next steps from the individual workshop speakers.
___________________
1For more information and background reading on potential health disparities and building trust, see Appendix F.
ADDRESSING HEALTH DISPARITIES IN GENOMIC MEDICINE
Because genome-wide association study (GWAS) data often come from populations that lack diversity, the genetic applications developed from those data may be useful only for certain groups (Haga, 2010). Even when the evidence base for genetic applications represents a diverse population, there is a need to ensure that the benefits of those data are equitably distributed across the population (see Figure 6-1), said Alexandra Shields of Harvard Medical School and Massachusetts General Hospital. At each stage in genomic research and the clinical uptake of that information, there is the possibility that a health disparity can be introduced, which is why Shields reminded the audience that “genomics will only achieve its full potential to improve health when the advances it engenders become accessible to all” (Green and Guyer, 2011).
One important contribution that could be made toward addressing health disparities, Shields said, would be to research and share information on a case study that successfully applied implementation science to avoid such disparities. A case study in genomics could report on a number of implementation issues, including
- Knowledge and evidence gaps
- Provider readiness
- Patient willingness
- Coverage and financing
- Data infrastructure, including health information technology
- New or expanded roles for personnel in implementation and the associated costs
- Outcomes and emerging evidence
Some of the same issues were described as possible barriers to and facilitators of implementation by individual speakers in Chapter 5 (see Box 5-1).
To prioritize which health conditions to use as a potential case study, Shields suggested considering the prevalence, cost, mortality, and health disparities of different diseases. As an example, she noted that cancer introduces health disparities among racial groups and is highly prevalent, extremely costly, and carries high rates of mortality. Furthermore, oncology is an area that adopted genomics early and thus may offer opportunities to learn about the challenges and successes of implementation. In developing a
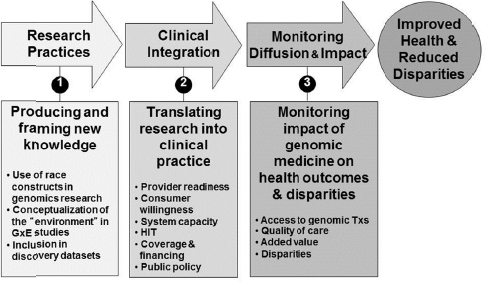
NOTE: GxE = gene–environment interaction; HIT = health information technology; Txs = therapies.
SOURCE: Alexandra Shields, National Academies of Sciences, Engineering, and Medicine workshop presentation, November 19, 2015. Figure was developed in discussions with Harvard/Massachusetts General Hospital Center on Genomics, Vulnerable Populations, and Health Disparities. For more information on the Harvard/Massachusetts General Hospital Center on Genomics, Vulnerable Populations, and Health Disparities, see http://cgvh.harvard.edu (accessed February 26, 2016).
case study, it is important to examine the evidence base carefully, Shields said. For example, for oncology genomics research, Lynch syndrome and BRCA-associated hereditary breast and ovarian cancer might have the strongest overall evidence bases, but, she asked, are there data available across all populations? Whether the somatic mutations discovered to date largely in white populations are present in minority patients at the same rate is an unanswered question that needs to be addressed, Shields said.
Provider readiness is another issue that arises when addressing health disparities in genomic medicine. Providers who care for poor and minority communities might believe that genomic medicine is too esoteric, given the health needs of the populations they serve, Shields said. In a national survey of 2,000 primary care physicians, only 5 percent said they felt very confident in their ability to interpret genetic tests, and only
4 percent felt prepared to counsel patients considering genetic testing (Shields et al., 2008).
According to that survey, physicians serving minority populations or a disproportionate number of Medicaid patients were less likely to order genetic tests for their patients than physicians who saw fewer minority patients or those with Medicaid, Shields said. In short, genomic applications are not reaching minority and low-income patients at the same rates as other populations, she said.
Different communities can have highly variable cultural beliefs and preferences which may be important to take into account when designing implementation projects. The opportunity for implementation science to affect how genomics is incorporated into practice lies at the intersection of understanding a high-priority condition and persistent health disparities, Shields said.
IMPROVING LITERACY IN GENOMICS AND IMPLEMENTATION SCIENCE2
Implementation science could potentially be useful for educating members of all population groups and recruiting them to participate in studies, said Bernice Coleman of Cedars Sinai Medical Center, Los Angeles. The need for greater literacy in genomics and implementation science among all stakeholders was a topic addressed by individual speakers including Coleman, Jane Perlmutter of the Gemini Group, Consuelo Wilkins of the Meharry-Vanderbilt Alliance and Vanderbilt University Medical Center, and David Chambers of the National Cancer Institute.
Efforts to enhance genomic literacy would benefit the public and potentially prevent future misunderstandings about genomic medicine, Perlmutter said. Early in 2015, President Obama announced the Precision Medicine Initiative (PMI), a plan aimed at improving disease treatment and prevention by accounting for individual variability in genetics and environment. While the announcement generated a great deal of public
___________________
2On March 2, 2016, the Roundtable on Health Literacy of the National Academies of Sciences, Engineering, and Medicine conducted a workshop titled Health Literacy and Precision Medicine: An Important Partnership. To read more about the workshop and the issues that surround the role of health literacy in the growing field of precision medicine, see: http://www.nationalacademies.org/hmd/Activities/PublicHealth/HealthLiteracy/2016MAR-2.aspx (accessed April 13, 2016).
enthusiasm, many came away with a misunderstanding about how long it is likely to take for most people to personally benefit from precision medicine, Perlmutter said. Although some areas, such as newborn screening and oncology, are further along than other fields in the implementation of genomics, she said, generally speaking, additional research will be needed for the PMI to reach its full potential even in these areas. It will be very important to be upfront with the public about the current benefits and limitations of genomic medicine, Perlmutter cautioned. Genomic information is different from other health care data in that some of it is not currently clinically actionable, Shields observed. However, what is not currently actionable may become important in the future. Health care systems have an obligation to ensure that patients have a complete understanding of what information is generated by a test, Shields said, so that they can make an informed decision about how to manage test results. Patients should be able to decide if they want genomic information stored in their electronic health record (EHR) and how they want to proceed with disclosure of results to themselves or family members.
Perlmutter also noted that there is often confusion about the differences between research and practice. For example, when researchers say a discovery will be in the clinic within 2 years, they often mean in phase I clinical trials, whereas a patient might interpret that as meaning that the discovery will be available from a doctor in 2 years, she said.
Involving Stakeholders Early in the Process
As demonstrated by some of the cases discussed at the workshop, involving patients and advocates from the very beginning can help strengthen genomic literacy, Perlmutter said. In certain instances, clinical study endpoints are not as important as they could be because it is not really known what patients want and need, Perlmutter said. For example, privacy, security, and family issues are major concerns for some patients, she said, and “we need to talk about these issues.” However, involving people early generates buy-in, she observed. While efforts to disseminate information to clinicians are laudable, unless there is a parallel effort to help the public understand and embrace genomics, problems will arise, Perlmutter added.
Implementation science could help set standards for educating minority or low-income patients on these issues, which would require adequate genetic counseling, Shields said. Enrollment in biobanks often occurs through an opt-out rather than an opt-in policy, which can result
in confusion for patients. Ensuring that adequate information is provided to patients before they submit samples to biobanks will help prevent distrust over the use of the samples.
Engaging Health Care System Leaders About Genomics
Implementation science has the potential to be a key facilitator in the movement of genomics into practice, and it may provide insights on both top-down and bottom-up approaches, Coleman said. The leaders at hospital health care systems need to be on board for change to occur, as was the case with the Geisinger Health System, said Geoffrey Ginsburg, the Roundtable’s co-chair and the director at the Duke Center for Applied Genomics & Precision Medicine (see Chapter 3). Health care system leadership plays a key role in changing cultures, setting frameworks, and providing incentives, feedback, and motivation. Therefore, Coleman said, it is important to increase literacy on genomics and implementation science among health care system leaders so that novel approaches can be integrated efficiently. It may be beneficial for implementation scientists and researchers to work hand in hand to design research projects that evaluate current practices, identify gaps, and benefit all populations. One key component to successfully monitoring outcomes, Coleman added, is to identify evaluation metrics in advance through collaboration with stakeholders.
COVERAGE AND REIMBURSEMENT CONSIDERATIONS
Reimbursement is necessary but not sufficient for the successful implementation of genomic approaches in medicine, Aetna’s Robert McDonough emphasized. A nascent field known as reimbursement science is aimed at standardizing the way that payers, guideline developers, and health care policy makers create reimbursement parameters, McDonough said. One of the goals of reimbursement science is to create tools and approaches for assessing the effectiveness and value of products that are covered by public and private health plans. Findings from reimbursement science could hasten the delivery of useful products and therapies to patients in need.
Genomic testing presents special challenges to reimbursement science because of the rapid evolution of new technologies, McDonough said. The Center for Medical Technology Policy and the Tapestry Net-
work and its Sustainable Predictive Oncology Therapeutics and Diagnostics (SPOT/Dx) program have developed guidance for payers and other policy makers on evaluating the validity of genomic tests. Most of the work thus far has focused on oncology; however, it is applicable to other types of genomic tests. If product developers in genomics had a clear understanding of the requirements for inclusion in coverage policies, it would be easier to predict whether their tests would receive reimbursement, McDonough said.
Genomics often focuses on rare conditions; therefore, payers are more likely to rely on guidelines, rather than an incomplete evidence base. One example of a genomic test with a very solid evidence base was cell-free fetal DNA (cffDNA) testing for aneuploidy, McDonough said (see Chapter 4). The cffDNA test received recommendations from major professional societies, leading to consistent reimbursement among payers and rapid adoption into clinical practice. In contrast, testing for maturity-onset diabetes of the young (MODY) poses more challenges, McDonough said (see Chapter 5). The criteria for whether or not to perform screening are inconsistent, and the condition is relatively rare. Consistent guidance from the leading professional organizations on when MODY testing would be appropriate would help enable consistent coverage policies, McDonough said. Payers are not just passive participants; instead, they can be important for promoting valuable tests to their constituents. Most payers now have programs in which they use their own data to identify care gaps and alert physicians and patients to those gaps, he said.
Payers are considering options such as bundled payments or risk-sharing agreements so that genetic tests are accompanied by treatment and an entire continuum of care, McDonough said. If the genetic test was included in the bundle for a condition, the payer would not have to assess individual claims for a test; however, it is not known whether that would increase or decrease the uptake of the test or how it would affect implementation.
Coverage for genomic panels has been a complicated issue. McDonough pointed out that no consensus exists as to what should be covered on any given panel. Furthermore, though the costs of testing have been going down, the cost to payers has been going up, McDonough said. Higher costs are part of the reason why payers are reluctant to allow additional components of the test to be covered, he said, and even though the additional incremental cost to the lab is negligible, that does not necessarily correspond to how the insurer is billed.
An effort to research and showcase model reimbursement policies that would apply to many of the key stakeholder groups, including payers, would help advance the field, said Brian Mittman of Kaiser Permanente Research. This would set an important precedent in this era of considerable ambiguity, uncertainty, and heterogeneity in genomic medicine policies, he said.
IMPLEMENTATION SCIENCE AND GENOMICS: THE ROAD AHEAD
A tremendous opportunity exists for integrating implementation science into genomics, Chambers said. At the end of the workshop, he summarized several of the main points of the presentations, and he highlighted possible approaches for using implementation science-based approaches to advance genomics. First, for ongoing and future discovery studies he suggested that researchers try to capture and quantify how clinicians, patients, and health systems are using the findings. Hybrid studies that examine effectiveness alongside implementation measures may be useful for reducing the amount of time it takes to integrate a research discovery in the clinic (see Chapter 2). Gaining an understanding of the demand for genomic tests and working toward enhancing that demand by increasing genomic literacy across all population subgroups is critical, Chambers said.
Secondly, within existing implementation science efforts, stakeholders can gather useful knowledge from case studies of “exceptional implementation,” instances of rapid uptake of genomic applications, as well as of failures—or “unsuccesses,” as Chambers called them. Assessing the qualities of highly nimble and adaptive implementation processes will be useful for future efforts, Chambers said. Clarifying the short- and long-term outcomes of success, along with designing a set of common report forms for patients and families, could help to streamline the process.
Finally, leveraging existing health systems and networks, such as those at the state level, may be useful during implementation, as was shown by Debra Duquette, genomics coordinator at the Michigan Department of Health and Human Services, in her explanation of the work of that department (see Chapter 5). Improving the interpretation of and communication about existing tests will enhance the trust between patients and the health care system, Chambers said. Overall, a patient-centered approach could help integrate testing and research within clinical
practice. Such an approach may require better strategies, increased transparency and disclosure, more inclusiveness, higher quality care, increased use of metrics, and even the minimization of travel inconveniences.
Overall, Chambers said, implementation science seeks to create generalizable knowledge that can be applied to a variety of challenges over a spectrum of disciplines. Even where a specific finding does not have a natural link to a different test or field, lessons can be derived that have a broader impact. “Sometimes we get lost in tests,” Chambers said, but “the reality is that there are a lot of people who we are trying to help.” We need to think of the young girl, for example, still searching for a diagnosis with her family, “who has interfaced with the health care financing system and has found that there are still tests that are not currently insured. . . . How do we navigate, how do we implement effectively, this entire cascade that would yield the best possible outcomes for her” and for all patients that are in need of finding answers?










