
1
The Relative Health Disadvantage
of U.S. Women
A growing literature—the result of several major investigations—is documented in a compelling manner the relative and growing health disadvantage of U.S. women in comparison with women in other countries. In particular, U.S. Health in International Perspective: Shorter Lives, Poorer Health (National Research Council and Institute of Medicine, 2013) found that, across many measures, the health of women in the United States was significantly worse than the health of women in many other high-income countries. That report and subsequent discussions have spurred in interest deeper analysis of those differences, elaborating their causes, and detailing their effects.
In her introductory remarks, workshop chair Nancy Adler (Departments of Psychiatry and Pediatrics, University of California, San Francisco) noted that the 2013 report is an example of how careful and authoritative reports not only have an immediate impact but also have ripple effects. This workshop, she said, is one of the ripple effects of that report.
In examining the causes and consequences of women’s health disparities, Adler stated that it is important to understand that these span multiple levels. Some involve the health care system, including patients and providers. Others involve risk behaviors, unhealthy diets, low levels of physical activity, and alcohol and tobacco use. Still others factors are further removed from people’s daily lives, such as socioeconomic status, insurance status, and inequities in income, housing, safety, education, and
job opportunities. And all of these intersect with issues of race, ethnicity, and geographic location.
Janine Clayton (Office of Research on Women’s Health, National Institutes of Health) outlined the rationale and objectives for the workshop. The Office of Research on Women’s Health is the architect of the institute-wide initiative at the National Institutes of Health (NIH) to require scientists to take gender into account in preclinical research studies involving animals and cells. The office also leads NIH’s efforts to advance women in science careers. Clayton emphasized the need to focus on the factors that are leading to the relative health disadvantage of U.S. women and to work on remedies to support the health of women in this country.
She pointed out that 2015 was the 25th birthday of the Office of Research on Women’s Health. Over that time, there have been major gains from research that has shown that lives can be saved and important health questions can be answered through clinical trials. Investments in medical research have yielded significant advances: examples include developing effective means to prevent mother-to-child transmission of HIV and a vaccine that prevents cervical cancer.
At the same time, she noted, the environment for women’s health has also changed over the last 25 years. For example, increased use of automobiles can lead to health risks from lack of physical activity. There has also been an increase in access to and consumption of unhealthy food. Other changes in the past 2 to 3 decades include such changes in women’s lives as the significant increase in the number of women who are heads of households and responsible for all aspects of a household and family. Many women now are also having children later in life, which poses interesting issues for both biology and sociology. The growing stress faced by women and the effect of stress on health and illness are issues that need a more comprehensive examination, as do issues of mental health and mental illness, which have become more increasingly common and thus more prominent issues for U.S. women. Chronic pain differentially affects women, which has had collateral damage in the surge of opioid abuse, Clayton noted.
During these 25 years, the U.S. maternal mortality rate has been a growing problem as the United States has experienced the highest infant mortality rate of all high-income countries. The United States also rates poorly on most other birth outcomes, such as low birth weight and the fact that American children are less likely to live to the age of 5 than children in other high-income countries.
Clayton stressed that it is important to take a multifaceted approach to these complex topics. Work needs to focus on access to medical care and bias in medical care delivery; factors that influence differences in morbid-
ity and mortality, such as socioeconomic status, education, employment and geography; and health risk behaviors.
The goal of this workshop, then, is to develop a list of key items for attention and postulate a research agenda to systematically approach the main issues. It would be useful, as well, to identify alliances to tackle those issues collaboratively. Finally, Clayton said, it will be important to specify and then to collect data as work is done so progress can be measured.
THE REPORT ON U.S. HEALTH IN INTERNATIONAL PERSPECTIVE
Steven H. Woolf (Virginia Commonwealth University), who served as the chair of the panel that authored U.S. Health in International Perspective: Shorter Lives Poorer Health, summarized the findings of that report. His presentation focused on findings with regard to international comparisons of women’s health, and he labelled the findings as “disturbing.” He offered his conclusion that there is a major public health crisis that affects more than half of the U.S. population, which needs attention.
The panel compared the health of Americans with people in 16 other high-income countries.1 The goal of the panel was to follow up on the work of a prior panel that had focused on people aged 50 and older (National Research Council, 2011), as well as to look across all age groups at how the health of people in the United States compares with people in other countries, focusing both on mortality and morbidity and quality of life. This task required examining all of the health statistics that were available for comparison purposes.
The report is divided into three parts: the first part documents the health disadvantage; the second part looks at the reasons for this health disadvantage; and the third provides the panel’s recommendations. Due to time constraints of this workshop, Woolf said, he will focus on the health findings, and more specifically, on the findings that pertain to women’s health.
Mortality in the United States can be classified as falling into three big categories: noncommunicable diseases, communicable diseases, and injuries. Noncommunicable diseases include chronic diseases, such as heart disease, cancer, and diabetes. For communicable diseases, the United States ranks next to last of the countries compared: see Figure 1-1.
______________
1The comparison countries were Australia, Austria, Canada, Denmark, Finland, France, Germany, Italy, Japan, The Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, and the United Kingdom.
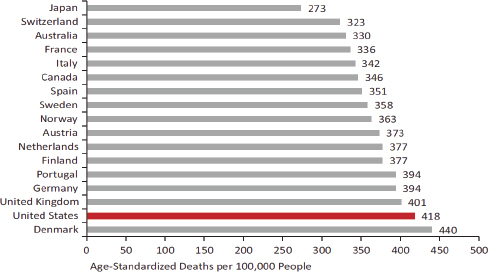
FIGURE 1-1 Mortality from noncommunicable diseases in 17 peer countries, 2008.
SOURCE: National Research Council and Institute of Medicine (2013, Fig. 1-1).
For communicable or infectious diseases, the United States ranks fourth highest in mortality among the comparison countries, and it ranks second highest for mortality from injuries.
The panel took the analysis a step further and probed the very diverse nature of those conditions, Woolf said. Some are traditional chronic diseases, some of them are injuries, some of them are psychosocial problems and some of them are related to maternal and child health. The disadvantage spans a very diverse spectrum of conditions.
The classic indicator that is used for international comparisons is life expectancy: U.S. life expectancy ranks second to the bottom for females. But life expectancy is influenced by mortality at different periods of the life course, so the panel tried to identify the stage of life at which U.S. women incur the disadvantage. Figure 1-2 shows the pattern in life expectancy at birth for females beginning in 1980: the dark dots represent the United States, and the light dots are the comparison countries. As can be seen in the figure, at the beginning of the 1980s U.S. women were was in the middle of the pack, but 25 years later they had fallen to the bottom.
Woolf pointed out that this pattern has been going on for decades and that the trend seems to be worsening. The pattern is true for every age group, from birth to age 75. After age 75, however, U.S. women no longer rank at the bottom. Some analysts have suggested that women who make
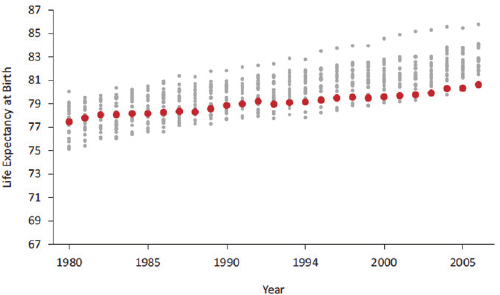
FIGURE 1-2 Life expectancy at birth for females in 21 high-income countries, 1980-2006.
SOURCE: National Research Council (2011, Fig. 1-4).
it to 75 are in good shape in the United States, but all through the life-course stages leading up to that age they are at a health disadvantage.
The life expectancy disadvantage is a pervasive problem across all age groups. The probability of a U.S. woman surviving to age 50 is lower than that of a woman in any of the comparison countries.
Woolf reported that the panel he chaired and its predecessor were both intrigued by the fact of higher U.S. female mortality and sought to identify potential explanations. One hypothesis concerns smoking rates and trends. The epidemiologic data on smoking rates and smoking-related deaths suggest that because smoking is a behavior that creates tobacco-related illness decades after the onset of the behavior, the peak in tobacco-related illness comes many years after the peak in smoking behavior.
This hypothesis is supported by the data. The peak in male smoking in the United States in the post-World War II period preceded the peak for female smoking. The U.S. women’s peak in trachea-related illness started to climb after the smoking peak, providing evidence of the after effect of the delayed increase in smoking rates. However, based on further assessment of international trends, the panel concluded that although smoking may have made some contribution to the health disadvantage, it does not fully explain it.
This analysis, Woolf explained, was a reason for the panel to take a comprehensive look at health access, health quality, and health behaviors, as well as socioeconomic conditions (poverty rates, patterns in income inequality, and educational status) and the physical and social environment (how U.S. cities are organized, the environment, air pollution, social capital, residential segregation, and social instability). A difficult but necessary domain for the panel was to assess the role of public policies in the observed outcomes, including spending, cultural values, how society make decisions about how lives are structured, education, types of jobs and employment.
Woolf next summarized some corroborating findings from other studies that continue to point to a health disadvantage for U.S. women. For example, there appears to be a geographical component. A series of studies by Kindig and colleagues have compared mortality rates at the county level for the United States for the 1990s and the current period (see, e.g., Kindig and Cheng, 2013). Importantly, in 42 percent of U.S. counties, mortality rates for women have increased since the 1990s. The conclusion is that there is more than a generic phenomenon in terms of the United States in comparison with other countries: spatial epidemiology also plays a role.
The role of education is also important. The work of David Cutler and colleagues (2011) included analysis of different datasets in order to focus on race, gender, and education trends in life expectancy. This work identified the special phenomenon that white women with low levels of education experience dramatically lower life expectancy than better educated white women. The same phenomenon was identified by Olshansky and colleagues (2012).
Recent work at the Urban Institute makes a contribution by identifying different potential factors that may explain these phenomena. Figures 1-3 and 1-4 compare reasons for causes of death rates for white and nonwhite non-Hispanic women for 1999 and 2011. The arrows indicate the direction of the causation over time.
The general trend is a decrease in mortality over the period, but with some factors having increased effects and others having decreased effects. Some interesting factors have emerged, most notably, accidental poisoning, which is mostly drug poisoning. It has increased remarkably for both males and females (Richardson et al., 2015): see Figure 1-5.
Drug poisoning deaths are now competing with motor vehicle crashes as the leading cause of unintentional injury deaths in the United States. It is important to distinguish this trend from intentional drug poisoning—
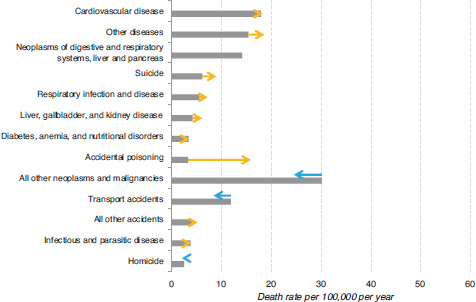
FIGURE 1-3 Trends in death rates for non-Hispanic white women aged 12-54, 1999 and 2011.
NOTE: See text for discussion.
SOURCE: Astone et al. (2015, p. 3).
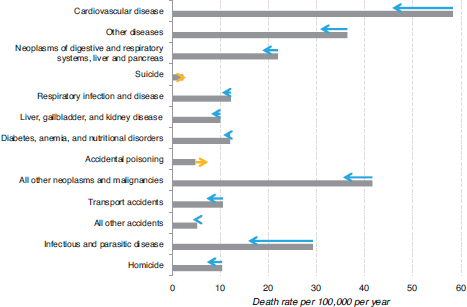
FIGURE 1-4 Trends in death rates for nonwhite, non-Hispanic women aged 15-54, 1999 and 2011.
NOTE: See text for discussion.
SOURCE: Astone et al. (2015, p. 5).
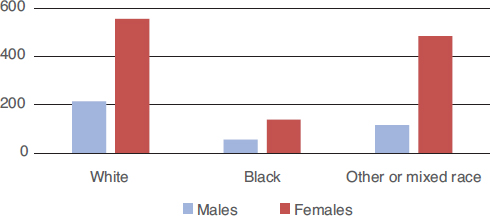
FIGURE 1-5 Percentage increase in poisonings between 1994 and 2010.
SOURCE: Data from Richardson et al. (2015, Table 1, p. 1682).
people committing suicide by taking a drug overdose, which has not increased much. Rather, it is unintentional deaths from drug ingestion (much of which is thought to be due to pharmacologic opioid prescriptions) that has climbed dramatically. As can be seen in Figure 1-5, women are far more affected by the growth of drug poisonings than men.
Woolf then turned to the big picture, using the World Health Organization’s conceptual model for the determinants of health to classify the interrelationships of the determinants and outcomes: see Figure 1-6.
Woolf suggested that the figure illustrates that it is useful to think about the inequity the health of U.S. women in terms of the environments in which women live and their life-course experience across the various domains that affect health. It also illustrates that there is a tremendous need for research, some of it the most basic of research, to try to understand the gaps revealed in descriptive epidemiology.
Woolf also stressed that public investment is an important factor in health outcomes. He referred to the work of Bradley and colleagues (2011) about how much that a society invests in social services and other programs outside of health care may be very important to health outcomes. Figure 1-7 shows all the countries of the world ranked in terms of the ratio of how much they spend on social services and health services and their gross domestic product. There is a cluster of industrialized countries in one section of the figure, with the United States clearly outside that cluster. That is, although the United States spends relatively more on health services than the other countries, it spends relatively far less on social services and, overall, it has worse health outcomes. The countries that spend relatively more on social services (above the OECD average) have longer life expectancies than the United States and better health outcomes.
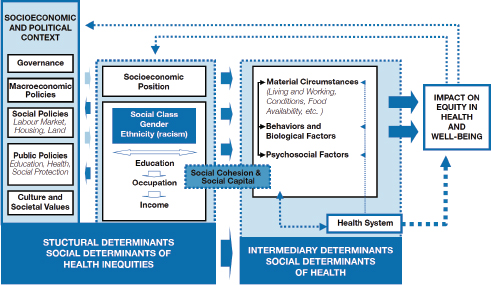
FIGURE 1-6 World Health Organization conceptual determinants model.
SOURCE: Solar, O., and Irwin, A. (2010). A Conceptual Framework for Action on the Social Determinants of Health. Social Determinants of Health Discussion Paper 2. Geneva, Switzerland: World Health Organization. Reprinted with permission, Figure A, p. 6 (final form of the CSDH conceptual framework).
Woolf pointed out that the public health implications of the problem of the disadvantage of U.S. women also extend to their children. He expressed a concern that the causes of the adverse health disadvantage for U.S. women might have implications for the next generation, who are being raised by those women. For this reason, he summarized, coming to an understanding of the cause of the growing health disadvantage for white women in the United States in comparison with their peers in other high-income countries will be important for understanding the factors that likely affect women of all races and ethnicities in the country.
Following up on this point, a workshop participant wondered if the mortality trends for white women have been evident for black women and Hispanic women over the past 25 or more years. Woolf responded that the available data do not permit the conclusion that there is a lagged effect so that the problems of white women will in the future be shown to be affecting other racial and ethnic groups. It could also be that the current trends are a sentinel effect: what is being seen in white women now is going to be coming next to other women. There is a need, he said, for
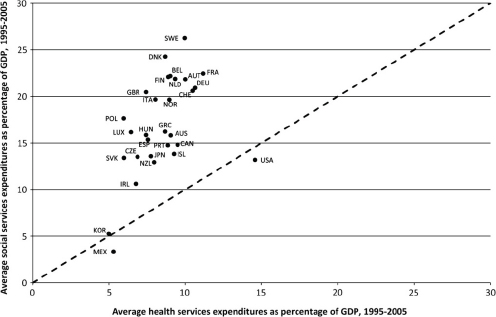
FIGURE 1-7 Countries ranked in terms of the ratio between how much they spend on social services and health services and gross domestic product (GDP), 1995-2005.
SOURCE: Bradley, E.H., Elkins, B.R., Herrin, J., and Elbel, B. (2011). Health and social services expenditures: Associations with health outcomes. BMJ Quality & Safety, 20(10), 826-831. Reprinted with permission from BMJ Publishing Group Ltd.
the funding of some simple descriptive epidemiologic studies to try to analyze in appropriate detail what conditions are responsible for what is now being observed and the time trends as to how those causes of death have evolved over time. He postulated that this would not be expensive research—just basic “shoe leather” epidemiology—to figure out the causes and answer some of the basic questions.
Another participant asked about the role of cigarette smoking, which was mentioned, relative to such other factors as physical activity or dietary factors that may contribute to the obesity epidemic that is important in terms of health outcomes and mortality. Woolf responded that it is important to think about all five domains—health systems, health behaviors, socioeconomic conditions, physical and social environment, and public policies and social values. Health behaviors, including physical activity, need to be considered, as well as the complex interactions between the domains. This kind of analysis would require postulating the interactions and then “unpacking” the interrelationships through traditional epidemiologic methods, such as multivariate regressions. He underscored the importance of considering that health behaviors are shaped by the envi-
ronment and by socioeconomic conditions and that they need to be understood holistically in the context of all of the factors.
Returning to the international comparisons, a participant asked whether it would be possible to identify countries in which women’s health outcomes are relatively better and then identify the characteristics of the countries where women are doing relatively better in comparison with U.S. men. Woolf replied that the study panel did not do that level of analysis. However, the report did look across the five domains—including the fifth domain of the nature of the macrostructural environment in those other countries—and to the extent possible with the available data, listed their public policies, social services, investments in supporting families and early childhood development, and other social services. Generally, the panel concluded that the countries that are doing better than the United States in health outcomes—for both women and men—generally have far more robust social service and related programs and policies than those in the United States. For example, mandated maternal leave is standard in in all the other countries but is not mandated or widely available in the United States. Though these comparisons yield clues, the lack of available cross-national data for making comparisons limits the ability to identify causal factors.
This page intentionally left blank.












