
Summary
Avoidable vision impairment occurs too frequently in the United States and is the logical result of a series of outdated assumptions, missed opportunities, and manifold shortfalls in public health policy and health care delivery. Eyesight affects how human beings perceive and interpret the world and is used for everyday communication, social activities, educational and professional pursuits, the care of others, and the maintenance of personal health, independence, and mobility. Vision loss in adults is associated with increased risk of falls and injuries, social isolation, depression, and other psychological problems and can amplify the adverse effects of other chronic illnesses, increasing the risk for all-cause and injury-related mortality (Christ et al., 2014; Crews et al., 2016; Lam et al., 2008; Lee et al., 2003; Lord, 2006; McKean-Cowdin et al., 2007). Similarly, undiagnosed or uncorrected refractive errors and other visual disorders in children can lead to developmental, academic, and social challenges, and in some cases permanent vision loss, which has lifelong implications (Birch, 2013; Davidson and Quinn, 2011). Moreover, the economic and social costs of vision impairment and eye disease to patients, the health care system, and society are considerable (Koberlein et al., 2013; Wittenborn et al., 2013). Yet, as a chronic condition, vision impairment remains notably absent from many public health agendas and community programs. Rather, vision is often regarded as a given—until it is not.
The vast majority of individuals in the United States who reach average life expectancy are at risk for some form of vision loss and impairment during their lifetimes, given current knowledge about effective prevention strategies, injury rates, barriers to accessing appropriate health care, and the
aging process itself. Vision loss can affect any one at any time. It is the process by which physiological changes or damage to the structure of the eye or visual information processing structures in the brain occurs, resulting in compromised subclinical or clinical function of the eye or visual processing system.1 Vision loss may occur suddenly and completely, for example from injury, or may subtly evolve over time, with permanent structural damage leading to progressive changes in eye function until more pronounced deficits become noticeable. Vision impairment, defined in this report as a measure of the functional limitation of the eye or visual system that results from vision loss, remains an unmet and important public health threat and is largely attributable to a few conditions or diseases in the United States.
No reliable data exist on the number of people affected by all causes of vision impairment in the United States. One model, based on a review of 12 major epidemiological studies applied to the 2010 U.S. Census population, estimates that approximately 90 million of the 142 million adults over the age of 40 in the United States experienced vision problems attributable to vision impairment, blindness, refractive error (i.e., myopia and hyperopia), age-related macular degeneration (AMD),2 cataracts, diabetic retinopathy, and glaucoma (Prevent Blindness, 2012).3 Presbyopia, an age-related condition that affects the ability to focus clearly on near objects, affects almost everyone entering the middle-age years (Petrash, 2013). Other measures of eye and vision health have different but significant implications for broad population health strategies to reduce the burden of vision impairment. For example, uncorrectable vision impairment (i.e., the amount of vision impairment that remains after appropriate treatment or intervention) can range from mild to severe and affects an estimated 6.4 million people, including adults and children, in the United States.4Uncorrected vision impairment (i.e., the proportion of overall vision impairment that could be improved through currently available treatments) affects millions more people in the United States, with estimates for uncorrected refractive error alone ranging from 8.2 million (Varma et al., 2016) to 11.0 million (CDC,
___________________
1 The committee adopted these definitions of vision loss and vision impairment to help facilitate discussion of eye and vision health in the context of population health. Justifications for these definitions are discussed in Chapter 1.
2 The estimate for AMD includes individuals ages 50 and older.
3 This statistic was corrected following release of the prepublication copy of the report.
4 This figure was determined by combining the estimates of 4.24 million U.S. adults ages 40 and older (Varma et al., 2016) and 2.155 million U.S. children, adolescents, and young adults through age 39 (Wittenborn and Rein, 2013). Both studies define uncorrectable vision impairment and blindness separately and as a measure of visual acuity.
2015c) to 15.9 million (Wittenborn and Rein, 2016).5 As the baby boomer generation ages, older adults will account for an ever larger proportion of the total population, and the prevalence of age-related eye diseases and conditions is projected to increase accordingly (Varma et al., 2016; Wittenborn and Rein, 2016). Actions to evaluate, monitor, and protect eye and vision health should begin early in life, but the systems and policies to encourage these behaviors in a fair and equitable manner are lacking.
The prevalence and impact of vision loss, as well as the severity of vision impairment, varies across geographic areas by etiology, age, race and ethnicity, and gender, putting certain populations at higher risk for specific types of vision loss (Congdon et al., 2004; Kirtland et al., 2015; Qiu et al., 2014; Zhang et al., 2012). The probability of vision impairment increases with age among all populations, particularly among people older than 60 years (Varma et al., 2016). Increased risk for poor eye health is also associated with social, economic, cultural, health, and environmental conditions, which further contribute to overall health disparities (Ulldemolins et al., 2012; Zambelli-Weiner et al., 2012; Zhang et al., 2012). Identifying populations at high risk for certain types of vision loss can help target limited resources, tailor effective interventions, and promote policies that better achieve eye and vision health and improve population health equity.
Some of the most notable successes in preventing vision loss have been anchored in population health strategies (CDC, 2015b; Kumaresan, 2005; Rao, 2015). Preventing vision-threatening injury, infection, and underlying chronic disease could have substantial effects on protecting or maintaining eye and vision health before treatment is needed. Promoting optimal conditions for eye and vision health can also alleviate many other social ills, including poverty, other health inequities, increasing health care costs, and avoidable mortality and morbidity (Christ et al., 2014; Kirtland et al., 2015; Lee et al., 2003; Rahi et al., 2009; Rein, 2013). Short- and long-term population health strategies should address broad determinants of health, including policies that influence individual behaviors, healthy environments and social conditions, and their potential impact on eye and vision health. Some strategies may be simpler and accomplished more quickly, such as
___________________
5 The committee commissioned an analysis, which was not available in the current literature, to establish the preventable burden of vision impairment in the United States from five conditions (diabetic retinopathy, glaucoma, refractive error, cataracts, and AMD). Estimates are based on a variety of sources (including population surveys and compilations of population-based studies) and reflect the best available public data. The committee presents only the results related to cataracts and uncorrected refractive error in this report because the analyses are most robust for these conditions. Chapter 3 provides a more in-depth description of the study’s assumptions and limitations, which are also documented in the commissioned paper itself (Wittenborn and Rein, 2016). This citation was added post release.
implementing policies that encourage using protective eyewear in hazardous work environments and during some recreational activities (CDC, 2013, 2015d; NEI/NIH, 2016). Other strategies will require more concerted and coordinated efforts to support social and built environments that promote eye-healthy behaviors or improved access to health care.
Early diagnosis and appropriate access to high-quality treatment could improve the trajectory of modifiable, correctable, and uncorrectable vision impairment by either slowing the progression of specific diseases or conditions, correcting the vision impairment itself, or improving the functionality, independence, and quality of life of populations with uncorrectable vision impairment. For example, estimates suggest that vision impairment caused by uncorrected refractive error and cataracts—both largely treatable—accounts for a substantial portion of undiagnosed vision impairment every year in the United States (CDC, 2015c; Wittenborn and Rein, 2016). Many public and private health insurance coverage policies, including Medicare, exclude eye examinations for initially asymptomatic or low-risk patients, corrective lenses, and visual assistive devices. Thus, in many cases, people must purchase additional vision insurance or shoulder costs out of pocket. Moreover, interventions exist to improve or maintain the functioning of people with vision impairment, but information about, and access to, these services is often limited (Overbury and Wittich, 2012; Pollard et al., 2003). These factors contribute to inequities that already affect populations with lower socioeconomic status and poor health (DeVoe et al., 2007; Levin et al., 2013).
Coordinated efforts are needed to expand public health capacities and to encourage policies and programmatic emphases that recognize improved eye and vision health as an important population health outcome and as a strategy to achieve better health equity. This will require federal and state support, coupled with public–private partnerships, to enhance local health department capabilities and energize other local institutions and organizations, families, and individuals to respond to community needs and goals (CDC, 2007).
This report proposes a population health action framework to guide action and coordination among various—and sometimes competing—stakeholders in pursuit of improved eye and vision health and health equity in the United States. This report also introduces a model for action that highlights different levels of prevention activities across a range of stakeholders and provides specific examples of how population health strategies can be translated into cohesive areas for action at federal, state, and local levels. Initial public- and private-sector investment has helped identify some of the chief information gaps and has led to a more nuanced understanding of the connection between eye and vision health and other measures of overall health, but more is needed. Implementing a coherent and comprehensive
response to address vision loss will be challenging. Establishing conditions and policies that promote population eye and vision health and that minimize preventable and correctable vision impairment is an essential, timely, and achievable objective—one that is necessary to improve the overall quality of life, functioning, and productivity of individuals.
STATEMENT OF TASK AND REPORT OVERVIEW
In 2014, the Health and Medicine Division of the National Academies of Sciences, Engineering, and Medicine convened a multidisciplinary committee to “examine the core principles and public health strategies to reduce visual impairment and promote eye health in the United States,” including short- and long-term strategies to prioritize eye and vision health through collaborative actions across a variety of topics, settings, community stakeholders, and levels of government. The committee reviewed the relevant literature and held five meetings, including two public workshops and one public session to obtain input from an array of experts and stakeholders. To further inform its deliberations, the committee also commissioned a paper on the costs and preventable burden of vision impairment for select eye conditions.
A POPULATION HEALTH APPROACH TO IMPROVE EYE AND VISION HEALTH
A population health approach involves multiple actors who work separately and cooperatively to “[focus] on interrelated conditions and factors that influence the health of populations over the life course, identif[y] systematic variations in their patterns of occurrence, and appl[y] the resulting knowledge to develop and implement policies and actions to improve the health and well-being of those populations” (Kindig and Stoddart, 2003, p. 380). The health of individuals and populations is affected by multiple determinants, including (1) individual traits; (2) behaviors; (3) social, family, and community networks; (4) living and working conditions; and (5) broad social, economic, cultural, health, and environmental conditions and policies, which are each part of larger social and physical environments (IOM, 2003a). Health care services are an important component of the “living and working conditions” that affect health. The vast majority of health determinants exists outside the clinical care delivery system (Braveman and Gottlieb, 2014; McGinnis et al., 2002), which provides a wide range of opportunities and environments in which to influence eye and vision health. As this report documents, eye and vision health is also affected by factors within each health determinant category. Figure S-1 provides an example of how multiple determinants of health could be used to target various factors
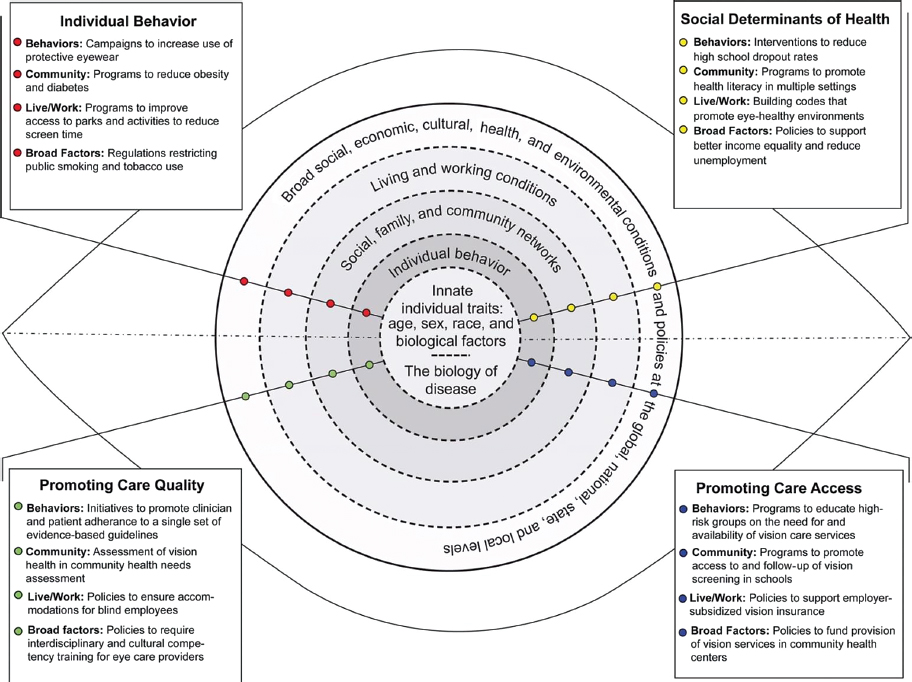
SOURCE: Adapted from IOM, 2003a, p. 52.
within each health determinant category as part of a broad population health approach to improve eye and vision health. These targets, which are included in four separate boxes, include both risk and protective factors for vision loss. The inclusion of these targets should not be interpreted as a prioritization of relevant research topics or as a conclusion that individual targets are each supported by the same strength of evidence.
The three functions of a population health approach are assessment (i.e., monitoring communities to identify and characterize public health needs and priorities); policy development (i.e., the use of scientific evidence to guide the design and implementation of programs and policies to address public health issues); and assurance (i.e., policy development and enforcement, ensuring that health and public health systems have the resources to implement programs, and evaluating the health impacts of interventions) (CDC, 2007; IOM, 1988). In the context of eye and vision health and the committee’s charge, these actions include short- and long-term strategies to address overarching determinants of health (primordial prevention) as well as efforts to support, educate, and promote healthy eye and vision behaviors (primary prevention); facilitate pre-symptomatic identification of eye diseases and treatments (secondary prevention); and preserve and enhance the health and functioning of individuals with vision impairment (tertiary prevention). Anchoring eye and vision health promotion in terms of the stages of prevention will allow the nation to reevaluate eye and vision health improvement more broadly as not only a valued outcome in and of itself, but also a potential public health tool to promote health equity among populations.
TRANSLATING A CONCEPTUAL FRAMEWORK INTO ACTION: RECOMMENDATIONS
The long-term goal of a population health approach for eye and vision health should be to transform vision impairment from a common to a rare condition, reducing associated health inequities. Given the genetic and biological components of many eye diseases and conditions, the occurrence of eye injuries, and the aging process itself, populations will never be without vision impairment. Nevertheless, this long-term goal establishes a new platform from which to identify important players, define influential behaviors, and allocate resources in a manner that will preserve and protect the eye and vision health of different populations.
Achieving the twin goals of improving eye and vision health and increasing health equity will require actions that reinforce each other. Figure S-2 identifies five core action areas that provide focus for the committee’s recommendations and support the ultimate outcome—improved population eye and vision health and health equity. These actions should

be population-centered, collaborative, culturally competent, community-tailored, evidence-based, integrated, standardized, and adequately resourced. Many of the following nine recommendations are broadly framed but are critical to establish conditions that will support a sustainable population health initiative that will effectuate a long-term reduction in vision impairment and its ramifications. These recommendations provide the foundational support for other, more specific actions by stakeholder groups, as described throughout this report.
Facilitate Public Awareness Through Timely Access to Accurate and Locally Relevant Information
According to a recent online poll, 88 percent of the 2,044 respondents surveyed identified good vision as vital to maintaining overall health, and 47 percent rated losing their vision compared to loss of limb, memory, hearing, or speech as “potentially having the greatest effect on their day-to-day life” (Scott et al., 2016, p. E3). Despite the public’s perception of the importance of good vision, millions of people continue to grapple with undiagnosed or untreated vision impairment (CDC, 2015c; Varma et al., 2016; Wittenborn and Rein, 2016). Moreover, eye and vision health remain relatively absent from national health priority lists, including efforts to stem the impact of chronic diseases. A number of factors, including the segregation of eye care from the rest of medicine, fragmentation within the eye care community, and a lack of coordination within or across federal entities, contribute to the absence of focused and sustained programmatic investment that would translate into widespread action.
A Call to Action “is a science-based document to stimulate action nationwide to solve a major public health problem” (U.S. Surgeon General, n.d.). The U.S. Department of Health and Human Services (HHS), most often through the Office of the Surgeon General, uses calls to action to draw attention to important public health issues, such as promoting walkable communities and oral health, preventing skin cancer and suicide, improving the health and wellness of persons with disabilities, and reducing underage drinking (Surgeon General, n.d.). These documents, along with other reports, are often used to establish a baseline from which to measure improvement (e.g., Anstev et al., 2011; Mertz and Mouradian, 2009; U.S. Surgeon General, 2014). Vision loss and impairment qualify as public health problems in that they (1) affect a large number of people; (2) impose large morbidity, quality-of-life, and cost burdens; (3) are increasing in severity and are predicted to continue increasing; (4) are perceived by the public to be a threat; and (5) are feasibly addressed by community or public health-level interventions (CDC, 2009). Similarly, the NEI, the U.S. Preventive Services Task Force, and the World Health Organization have identified vision impairment in various populations as national or global public health problems (HHS, 2015; NEI/NIH, 2004; WHO, 2015).
Moreover, like other chronic diseases, most causes of vision impairment require ongoing management over the lifespan of an individual to maintain the activities of daily living. A call to action is needed to stimulate nationwide discussion of eye and vision health as an essential health outcome and launch measured and directed actions that will reduce the burden of vision impairment in the United States.
Recommendation 1
The Secretary of the U.S. Department of Health and Human Services should issue a call to action to motivate nationwide action toward achieving a reduction in the burden of vision impairment across the lifespan of people in the United States. Specifically, this call to action should establish goals to:
- Eliminate correctable and avoidable vision impairment by 2030,
- Delay the onset and progression of unavoidable chronic eye diseases and conditions,
- Minimize the impact of chronic vision impairment, and
- Achieve eye and vision health equity by improving care in underserved populations.
Enhancing public knowledge about a health threat is a fundamental first step in informing discussions that promote behavior change across multiple determinants of health and aligning health policies with general public health interests. Unfortunately, lack of awareness of vision and eye health issues remains a major public health concern, especially in the context of linking patients to care and attempting to make population-level changes in behavior and health practice (Bailey et al., 2006; Zhang et al., 2012). Individuals are often unaware of what the most common risks to vision are, how the physiological progression of many eye diseases occurs, early signs of vision loss, and what steps can be taken to reduce the risk of vision-threatening eye disease, conditions, and events and the impact of subsequent vision loss (Alexander et al., 2008; Chou et al., 2014; Lam and Leat, 2015; NEI/LCIF, 2008; Varano et al., 2015). Combined with the asymptomatic nature of many eye diseases and conditions, this lack of awareness can have significant ramifications on overall health.
Although rarely adequate by themselves, public awareness campaigns can be an effective tool for improving knowledge about key messages related to health within populations (Bray et al., 2015; Oto et al., 2011) and are one essential part of an effective population health strategy. Achieving the goals outlined in recommendation 1 will require having reliable, consistent, evidence-based information that is available and accessible by a variety of stakeholders to increase overall knowledge and encourage policies,
practices, and behaviors that promote good eye and vision health, support appropriate care to correct or slow progression of a vision-threatening disease or condition, or improve function when vision impairment is uncorrectable. This approach must target various audiences and consider a wide range of factors affecting eye and vision health in communities, including individual-directed strategies, mass media campaigns, and environmental and policy changes across multiple settings within defined geographic areas (e.g., city, state, province, or country).
Recommendation 2
The Secretary of the U.S. Department of Health and Human Services, in collaboration with other federal agencies and departments, nonprofit and for-profit organizations, professional organizations, employers, state and local public health agencies, and the media, should launch a coordinated public awareness campaign to promote policies and practices that encourage eye and vision health across the lifespan, reduce vision impairment, and promote health equity. This campaign should target various stakeholders, including the general population, care providers and caretakers, public health practitioners, policy makers, employers, and community and patient liaisons and representatives.
Generate Evidence to Guide Policy Decisions and Evidence-Based Actions
Vision impairment and blindness are appropriate targets for surveillance because they adversely affect a large portion of the population, affect populations unequally, can be improved by treatment and preventive efforts, and will become an increasing burden as the population ages (Saaddine et al., 2003). A comprehensive, nationally representative surveillance system for eye and vision health is needed to better understand the epidemiological patterns, risk factors, comorbidities, and costs associated with vision loss. Such data will allow health care professionals and public health decision makers to better characterize the nature and extent of the public health burden; risk factors and at-risk populations; disparities in access, care, and outcomes; and successful interventions (West and Lee, 2012).
Recommendation 3
The Centers for Disease Control and Prevention (CDC) should develop a coordinated surveillance system for eye and vision health in the United States. To advise and assist with the design of the system, the CDC should convene a task force comprising government, nonprofit and for-profit organizations, professional organizations, academic researchers, and the health care and public health sectors. The design of this system should include, but not be limited to:
- Developing and standardizing definitions for population-based studies, particularly definitions of clinical vision loss and functional vision impairment;
- Identifying and validating surveillance and quality-of-care measures to characterize vision-related outcomes, resources, and capacities within different communities and populations;
- Integrating eye-health outcomes, objective clinical measures, and risk/protective factors into existing clinical-health and population-health data collection forms and systems (e.g., chronic disease questionnaires, community health assessments, electronic health records, national and state health surveys, Medicare’s health risk assessment, and databases); and
- Analyzing, interpreting, and disseminating information to the public in a timely and transparent manner.
Understanding the factors that affect the risk of vision impairment for different populations, the barriers to accessing care, interventions to prevent visual impairment and maintain eye function, and ways to improve the quality of care is fundamental to designing and identifying opportunities that minimize vision loss now and that will result in new knowledge and strategies to further reduce the long-term impact of vision impairment. HHS supports a number of federal programs and institutes that focus on vision loss and fund various activities to combat the effects of poor eye and vision health on at-risk populations (CDC, 2015a). Despite these activities, eye and vision health is insufficiently represented as a programmatic focus in federal government programs overall, and existing research programs lack coordination within and across federal agencies and institutes. Establishing a unified research agenda with larger financial and programmatic support to develop and advance knowledge about eye and vision health can maximize efficiencies and build on the strengths of established programs across a broad portfolio of topics and programs, which must include more than basic and clinical research.
Recommendation 4
The U.S. Department of Health and Human Services should create an interagency workgroup, including a wide range of public, private, and community stakeholders, to develop a common research agenda and coordinated eye and vision health research and demonstration grant programs that target the leading causes, consequences, and unmet needs of vision impairment. This research agenda should include, but not be limited to:
- Population-based epidemiologic and clinical research on the major causes and risks and protective factors for vision impairment, with a special emphasis on longitudinal studies of the major causes of vision impairment;
- Health services research, focused on patient-centered care processes, comparative-effectiveness and economic evaluation of clinical interventions, and innovative models of care delivery to improve access to appropriate diagnostics, follow-up treatment, and rehabilitation services, particularly among high-risk populations;
- Population health services research to reduce eye and vision health disparities, focusing on effective interventions that promote eye healthy environments and conditions, especially for underserved populations; and
- Research and development on emerging preventive, diagnostic, therapeutic, and treatment strategies and technologies, including efforts to improve the design and sensitivity of different screening protocols.
Expand Access to Appropriate Clinical Care
Professional guidelines are an important tool for advancing policies and practices that promote high-quality care for everyone. They are often used to educate the public and public health and health care professionals and serve as foundational elements of value-driven payment policies and as baselines from which to measure quality improvement and enhanced accountability for care processes and patient health outcomes. No single
set of clinical practice guidelines or measures in eye and vision care exists. Although eye and vision guidelines are consistent for the most part, there are some important differences. Differences may reflect the absence of robust data and political tensions within the field of eye and vision health. Available guidelines may provide inconsistent recommendations concerning essential measures, such as the frequency with which different age groups and at-risk populations should receive comprehensive eye exams6 (e.g., AAO, 2015; AOA, 2015). Health insurance coverage for basic examinations, preventive services and treatments (including corrective lenses), and rehabilitation (including assistive devices) should reflect these guidelines. Particular attention needs to be paid to assuring that essential services and treatments are affordable, particularly for the most vulnerable populations.
Recommendation 5
The U.S. Department of Health and Human Services should convene one or more panels—comprising members of professional organizations, researchers, public health practitioners, patients, and other stakeholders—to develop a single set of evidence-based clinical and rehabilitation practice guidelines and measures that can be used by eye care professionals, other care providers, and public health professionals to prevent, screen for, detect, monitor, diagnose, and treat eye and vision problems. These guidelines and supporting evidence should be used to drive payment policies, including coverage determinations for corrective lenses and visual assistive devices following a diagnosed medical condition (e.g., refractive error).
To cultivate professional relationships and collaboration that advances eye and vision health across medicine and beyond clinical care, it is important to establish a set of common expertise that can align overarching objectives and action among health professionals. The CDC has noted the need to elevate ophthalmic education in medical curricula (CDC, 2007; Shah et al., 2014). With a greater focus on population health in clinical care (Berwick et al., 2008), new skills will be needed to ensure that health care professionals understand the types of patient experiences and data that are relevant to population health activities, including the moral imperative to reduce inequities in both health and health care. Moreover, public health practitioners should be familiar with eye and vision health, its risk factors, and the relationship between vision loss and other chronic health conditions. Translating this knowledge into meaningful patient interactions will
___________________
6 The committee defines a comprehensive eye examination as a dilated eye examination that may include a series of other tests, in addition to the dilation of the pupil.
require cultivating trust among different patient populations, providers, and public health practitioners.
Recommendation 6
To enable the health care and public health workforce to meet the eye care needs of a changing population and to coordinate responses to vision-related health threats, professional education programs should proactively recruit and educate a diverse workforce and incorporate prevention and detection of visual impairments, population health, and team care coordination as part of core competencies in applicable medical and professional education and training curricula. Individual curricula should emphasize proficiency in culturally competent care for all populations.
Enhance Public Health Capacities to Support Vision-Related Activities
Integrating public health and local health care systems is an important strategy for improving community health (CDC, 2007). A well-functioning medical care system can expand delivery of appropriate eye and vision care services, allowing public health agencies to focus on preventive policies and action and assurance. Such preventive actions include linking people to needed care, assessing care quality, and promoting community support and policy and environmental conditions that maximize health (IOM, 2003b). Public health agencies and departments can also extend the reach of health care services through vision-specific programs. There has been insufficient partnering to coordinate existing and emerging programs, policies, and quality improvement activities that either directly or indirectly influence eye and vision health.
Recommendation 7
State and local public health departments should partner with health care systems to align public health and clinical practice objectives, programs, and strategies about eye and vision health to:
- Enhance community health needs assessments, surveys, health impact assessments, and quality improvement metrics;
- Identify and eliminate barriers within health care and public health systems to eye care, especially comprehensive eye exams, appropriate screenings and follow-up services, and items and services intended to improve the functioning of individuals with vision impairment;
- Include public health and clinical expertise related to eye and vision health on oversight committees, advisory boards, expert panels, and staff, as appropriate;
- Encourage physicians and health professionals to ask and engage in discussions about eye and vision health as part of patients’ regular office visits; and
- Incorporate eye health and chronic vision impairment into existing quality improvement, injury and infection control, and behavioral change programs related to comorbid chronic conditions, community health, and the elimination of health disparities.
Local public health departments are designed to promote health across a wide range of policies, activities, programs, and efforts to improve accountability. In the face of declining public investment, current state and local public health agencies and departments struggle to meet state mandates and requirements (Jacobson et al., 2015). Public health strategies to promote eye and vision health are rarely supported as a categorical focus or even as part of chronic disease programs in state and local health departments due to limitations in resources and other shifting priorities. Moreover, flexibility in how state and local governments use federal grant funds varies (CBO, 2013). In the absence of federal directives and programs to advance eye and vision health, state and local public health departments are hard pressed to incorporate reduction of vision impairment as a categorical programmatic focus.
Recommendation 8
To build state and local public health capacity, the Centers for Disease Control and Prevention should prioritize and expand its vision grant program, in partnership with state-based chronic disease programs and other clinical and nonclinical stakeholders, to:
- Design, implement, and evaluate programs for the primary prevention of conditions leading to visual impairment, including policies to reduce eye injuries;
- Develop and evaluate policies and systems that facilitate access to, and utilization of, patient-centered vision care and rehabilitation services, including integration and coordination among care providers; and
- Develop and evaluate initiatives to improve environments and socioeconomic conditions that underpin good eye and vision health and reduce eye injuries in communities.
Promote Community Actions That Encourage Eye- and Vision-Healthy Environments
Eye and vision health is a community issue—the needs, adequacy of resources, and priorities will vary based on population characteristics, cultures, and values. The impact that vision loss has on function and quality of life varies according to numerous factors, including the built environment, social support, access to health care and rehabilitation services, attitude, preferences, and socioeconomic factors. How these factors affect the occurrence, severity, and impact of vision loss differs for individuals and communities. It is important that community stakeholders (businesses, advocacy organizations, neighborhood groups, local health and public health departments, religious organizations, professional organizations, school boards and faculty, parent support groups, health care providers, eye care providers, etc.) be actively consulted and engaged in options to translate and implement national goals into workable community action plans to reduce the burden of vision loss and the functioning of populations with vision impairment across different community settings.
Recommendation 9
Communities should work with state and local health departments to translate a broad national agenda to promote eye and vision health into well-defined actions. These actions should encourage policies and conditions that improve eye and vision health and foster environments to minimize the
impact of vision impairment, considering the community’s needs, resources, and cultural identity. These actions should:
- Improve eye and vision health awareness among different social groups within communities;
- Engage community organizations and groups to promote eye and vision health awareness in daily activities;
- Establish and enforce laws and policies intended to promote eye safety and the functioning of people with vision impairment;
- Identify the need for, and community-level barriers to, vision-related services and resources in their communities; and
- Adopt policies and create community networks that support the design of built environments and the establishment of social environments that promote eye and vision health and independent functioning.
REFERENCES
AAO (American Academy of Ophthalmology). 2015. Policy statement: Frequency of ocular examinations. San Francisco, CA: AAO.
Alexander, Jr., R. L., N. A. Miller, M. F. Cotch, and R. Janiszewski. 2008. Factors that influence the receipt of eye care. American Journal of Health Behavior 32(5):547.
Anstev, E. H., C. A. MacGowan, and J.A. Allen. 2011. Five-year progress update on the Surgeon General’s call to action to support breastfeeding. Journal of Women’s Health 25(8):768–776.
AOA (American Optometric Association). 2015. Comprehensive eye and vision examination. http://www.aoa.org/patients-and-public/caring-for-your-vision/comprehensive-eye-andvision-examination?sso=y (accessed March 29, 2016).
Bailey, R. N., R. W. Indian, X. Zhang, L. S. Geiss, M. R. Duenas, and J. B. Saaddine. Visual impairment and eye care among older adults–five states, 2005. 2006. Morbidity Mortality Weekly Report 55(49):1321–1325.
Berwick, D. M., T. W. Nolan, and J. Whittington. 2008. The triple aim: Care, health, and cost. Health Affairs 27(8):759–769.
Birch, E. E. 2013. Amblyopia and binocular vision. Progress in Retinal and Eye Research 33:67–84.
Braveman, P., and L. Gottlieb. 2014. The social determinants of health: It’s time to consider the causes of the causes. Public Health Reports 129(Suppl 2):9–31.
Bray, J. E., L. Straney, B. Barger, and J. Finn. 2015. Effect of public awareness campaigns on calls to ambulance across Australia. Stroke 46(5):1377–1380.
CBO (Congressional Budget Office). 2013. Federal grants to state and local governments. Washington, DC: CBO.
CDC (Centers for Disease Control and Prevention). 2007. Improving the nation’s vision health: A coordinated public health approach. Atlanta, GA: CDC.
———. 2009. Why is vision loss a public health problem? http://www.cdc.gov/visionhealth/basic_information/vision_loss.htm (accessed October 7, 2015).
———. 2013. Eye safety. http://www.cdc.gov/niosh/topics/eye (accessed March 30, 2016).
———. 2015a. About us. http://www.cdc.gov/visionhealth/about/index.htm (accessed March 30, 2016).
———. 2015b. Conjunctivitis (pink eye) in newborns. http://www.cdc.gov/conjunctivitis/newborns.html (accessed March 30, 2016).
———. 2015c. National data. http://www.cdc.gov/visionhealth/data/national.htm (accessed March 30, 2016).
———. 2015d. The work-related injury statistics query system. http://wwwn.cdc.gov/wisards/workrisqs (accessed April 4, 2016).
Chou, C. F., C. E. Sherrod, X. Zhang, L. E. Barker, K. M. Bullard, J. E. Crews, and J. B. Saaddine. 2014. Barriers to eye care among people aged 40 years and older with diagnosed diabetes, 2006–2010. Diabetes Care 37(1):180–188.
Christ, S. L., D. Zheng, B. K. Swenor, B.L. Lam, S. K. West, S. L. Tannenbaum, B. E. Munoz, and D. J. Lee. 2014. Longitudinal relationships among visual acutiy, daily functional status, and mortality: The Salisbury Eye Evaluation Study. Journal of Ophthalmology. 132(12):1400–1406.
Congdon, N., B. O’Colmain, C. C. Klaver, R. Klein, B. Munoz, D. S. Friedman, J. Kempen, H. R. Taylor, and P. Mitchell. 2004. Causes and prevalence of visual impairment among adults in the United States. Archives of Ophthalmology 122(4):477–485.
Crews, J. E., C.-F. Chiu-Fung Chou, J. A. Stevens, and J. B. Saadine. 2016. Falls among persons aged > 65 years with and without severe vision impairment—United States, 2014. Morbidity and Mortality Weekly Report 65(17):433–437.
Davidson, S., and G. E. Quinn. 2011. The impact of pediatric vision disorders in adulthood. Pediatrics 127(2):334–339.
DeVoe, J. E., A. Baez, H. Angier, L. Krois, C. Edlund, and P. A. Carney. 2007. Insurance + access ≠ health care: Typology of barriers to health care access for low-income families. Annals of Family Medicine 5(6):511–518.
HHS (U.S. Department of Health and Human Services). 2015. Healthy people 2020 topics and objectives: Vision. http://www.healthypeople.gov/2020/topics-objectives/topic/vision (accessed October 7, 2015).
IOM (Institute of Medicine). 1988. The future of public health. Washington, DC: National Academy Press.
———. 2003a. The future of the public’s health in the 21st century. Washington, DC: The National Academies Press.
———. 2003b. Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, DC: The National Academies Press.
Jacobson, P. D., J. Wasserman, H. W. Wu, and J. R. Lauer. 2015. Assessing entrepreneurship in governmental public health. American Journal of Public Health 105(S2):S318–S322.
Kindig, D., and G. Stoddart. 2003. What is population health? American Journal of Public Health 93(3):380–383.
Kirtland, K. A., J. B. Saaddine, L. S. Geiss, Thompson, T. J., Cotch, M. F., and Lee, P. P. 2015. Geographic disparity of severe vision loss—United States, 2009–2013. Morbidity and Mortality Weekly Report 64(19):513–517.
Koberlein, J., K. Beifus, C. Schaffert, and R. P. Finger. 2013. The economic burden of visual impairment and blindness: A systematic review. British Medical Journal Open 3: 1–14.
Kumaresan, J. 2005. Can blinding trachoma be eliminated by 20/20? Eye 19(10):1067–1073.
Lam, B. L., S. L. Christ, D. J. Lee, D. D. Zheng, and K. L. Arheart. 2008. Reported visual impairment and risk of suicide: The 1986–1996 National Health Interview Surveys. Archives of Ophthalmology 126(7):975–980.
Lam, N., and S. J. Leat. 2015. Reprint of: Barriers to accessing low-vision care: The patient’s perspective. Canadian Journal of Ophthalmology/Journal Canadien d’Ophtalmologie 50:S34–S39.
Lee, D. J., O. Gomez-Marin, B. L. Lam, and D. D. Zheng. 2003. Visual impairment and unintentional injury mortality: The National Health Interview Survey 1986–1994. American Journal of Ophthalmology 136(6):1152–1154.
Levin, A. V., L. T. Pizzi, M. Snitzer, and K. M. Prioli. 2013. Barriers to follow up care in children with vision diseases: Development of a conceptual framework and parent/caregiver survey through the children’s eye care adherence project. Value in Health 16(3):A38.
Lord, S. R. 2006. Visual risk factors for falls in older people. Age and Ageing 35(Suppl 2): ii42–ii45.
McGinnis, J. M., P. Williams-Russo, and J. R. Knickman. 2002. The case for more active policy attention to health promotion. Health Affairs 21(2):78–93.
McKean-Cowdin, R., R. Varma, J. Wu, R. D. Hays, S. P. Azen, for the Los Angeles Latino Eye Study Group. 2007. Severity of vision field loss and health-related quality of life. American Journal of Ophthalmology 143(6):1013–1023.
Mertz, E., and W. Mouradian. 2009. Addressing children’s oral health in the new millennium: Trends in the dental workforce. Academic Pediatrics 9(6):433.
NEI/LCIF (National Eye Institute/Lions Club International Foundation). 2008. 2005 survey of public knowledge, attitudes, and practices related to eye health and disease. https://nei.nih.gov/kap (accessed October 7, 2015).
NEI/NIH (National Eye Institute/National Institutes of Health). 2004. Vision statement and mission—National plan for eye and vision research [NEI strategic planning]. https://neinih.gov/strategicplanning/np_vision (accessed February 4, 2016).
———. 2016. About sports eye injury and protective eyewear. https://nei.nih.gov/sports (accessed February 12, 2016).
Oto, M. A., O. Ergene, L. Tokgozoglu, Z. Ongen, O. Kozan, M. Sahin, M. K. Erol, T. Tezel, and M. Ozkan. 2011. Impact of a mass media campaign to increase public awareness of hypertension. Turk Kardiyoloji Dernegi Ars 39(5):355–364.
Overbury, O., and W. Wittich. 2012. Barriers to low vision rehabilitation: The Montreal Barriers Study. 2011. Investigative Ophthalmology & Visual Science 52(12):8933–8938.
Petrash, J. M. 2013. Aging and age-related diseases of the ocular lens and vitreous body. Investigative Ophthalmology & Visual Science 54(14):ORSF54–ORSF59.
Pollard, T. L., J. A. Simpson, E. L. Lamoureux, and J. E. Keefe. 2003. Barriers to accessing low vision sevices. Ophthalmic and Phsyiological Optics 23(4):321–327.
Prevent Blindness. 2012. Vision problems in the U.S. http://www.visionproblemsus.org (accessed June 5, 2016).
Qiu, M., S. Y. Wang, K. Singh, and S. C. Lin. 2014. Racial disparities in uncorrected and undercorrected refractive error in the United States. Investigative Ophthalmology & Visual Science 55(10):6996–7005.
Rahi, J. S., P. M. Cumberland, and C. S. Peckham. 2009. Visual function in working-age adults: Early life influences and associations with health and social outcomes. Ophthalmology 116(10):1866–1871.
Rao, G. 2015. The Barrie Jones Lecture—Eye care for the neglected population: Challenges and solutions. Eye 29(1):30–45.
Rein, D. B. 2013. Vision problems are a leading source of modifiable health expenditures. Investigative Ophthalmology & Visual Science 54(14):ORSF18–ORSF22.
Saaddine, J. B., K. Venkat Narayan, and F. Vinicor. 2003. Vision loss: A public health problem? Ophthalmology 110(2):253–254.
Scott, A. W., N. M. Bressler, S. Ffolkes, J. S. Wittenborn, J. Jorkavsky. 2016. Public attitudes about eye and vision health. JAMA Ophthalmology 134(10):1111–1118.
Shah, M., D. Knoch, and E. Waxman. 2014. The state of ophthalmology medical student education in the United States and Canada, 2012 through 2013. Ophthalmology 121(6):1160–1163.
Ulldemolins, A. R., V. C. Lansingh, L. Guisasola Valencia, M. J. Carter, K. A. Eckert. 2012. Social inequalities in blindness and visual impairment: A review of social determinants. Indian Journal of Ophthalmology 60(5):368–375.
U.S. Surgeon General. 2014. The health consequences of smoking—50 years of progress: A report of the Surgeon General, 2014. Rockville, MD: U.S. Department of Health and Human Services.
———. n.d. Surgeon General’s Calls to Action. http://www.surgeongeneral.gov/library/calls (accessed August 23, 2016).
Varano, M., N. Eter, S. Winyard, K. U. Wittrup-Jensen, R. Navarro, and J. Heraghty. 2015. Current barriers to treatment for wet age-related macular degeneration (WAMD): Findings from the WAMD patient and caregiver survey. Journal of Clinical Ophthalmology 9:2243–2250.
Varma, R., T. S. Vajaranant, B. Burkemper, S. Wu, M. Torres, C. Hsu, F. Choudhury, R. McKean-Cowdin. 2016. Visual impairment and blindness in adults in the United States: Demographic and geographic variations from 2015 to 2050. JAMA Ophthalmology. May 19 [Epub ahead of print].
West, S. K., and P. Lee. 2012. Vision surveillance in the United States: Has the time come? American Journal of Ophthalmology 154(6):S1–S2, e2.
WHO (World Health Organization). 2015. Blindness: Vision 2020—the global initiative for the elimination of avoidable blindness. http://www.who.int/mediacentre/factsheets/fs213/en (accessed October 7, 2015).
Wittenborn, J., and D. Rein. 2013. Cost of vision problems: The economic burden of vision loss and eye disorders in the United States. New York: Prevent Blindness America.
———. 2016. The potential costs and benefits of treatment for undiagnosed eye disorders. Paper prepared for the Committee on Public Health Approaches to Reduce Vision Impairment and Promote Eye Health. http://www.nationalacademies.org/hmd/~/media/Files/Report%20Files/2016/UndiagnosedEyeDisordersCommissionedPaper.pdf (accessed September 15, 2016).
Wittenborn, J. S., X. Zhang, C. W. Feagan, W. L. Crouse, S. Shrestha, A. R. Kemper, T. J. Hoerger, and J. B. Saaddine. 2013. The economic burden of vision loss and eye disorders among the United States population younger than 40 years. Ophthalmology 120(9):1728–1735.
Zambelli-Weiner, A., J. E. Crews, D. S. Friedman. 2012. Disparities in adult vision health in the United States. American Journal of Ophthalmology 154(Suppl):S23–S30, e1.
Zhang, X., M. F. Cotch, A. Ryskulova, S. A. Primo, P. Nair, C.-F. Chou, L. S. Geiss, L. Barker, A. F. Elliott, J. E. Crews, and J. B. Saaddine. 2012. Vision health disparities in the United States by race/ethnicity, education, and economic status: Findings from two nationally representative surveys. American Journal of Ophthalmology 154(6 Suppl):S53–S62, e51.






















