
2 Overview of Contemporary Civilian and Military Trauma Systems
As discussed in Chapter 1, lessons learned from United States involvement in armed conflicts have played an important role in advancing the care of injured patients in the civilian sector. One defining lesson that contributed to the development of today’s regionalized civilian trauma systems is that surviving traumatic injury depends on reaching definitive care—a hospital capable of providing optimal care—as soon as possible. This principle is captured in the commonly used phrase “right patient to the right place at the right time” (ACS, 2014; Eastman et al., 2013). In 1966, the National Research Council laid the foundation for translating this principle to the civilian center, calling for the development of regionalized trauma systems to support the timely identification and triage of patients to a level of care commensurate with the extent and severity of their injuries (NRC, 1966). Over the past 50 years, significant progress has been made to this end, with a regionalized systems-based approach to trauma care being implemented in most states around the nation. More recently, the U.S. Department of Defense (DoD) adopted the principles of a trauma system for application in the military, developing the Joint Trauma System (JTS) over the course of the wars in Afghanistan and Iraq (ACS, 2014; Bailey et al., 2012a). Despite these laudable achievements, however, the full potential of a national trauma system featuring seamless sharing of data, best practices, and lessons learned within and across the military and state-based civilian systems has not yet been realized.
This chapter provides an overview of civilian and military trauma systems in the United States, focusing on structure, process, and variability in patient outcomes. As the structure, organization of services, and capabilities
of trauma systems affect the delivery of care, the chapter begins with an overview of essential elements of a trauma care system and the inclusive approach that has emerged in the civilian sector as an optimal model for trauma system development. The chapter then describes the variability in the essential elements of a trauma care system that characterizes civilian systems across the nation, which has resulted in concomitant variability in patient outcomes. Subsequently, the chapter focuses on the development of the contemporary military trauma system and highlights the organizational structure and processes (e.g., the chain of command) that impact the delivery of trauma care on the battlefield. Lastly, this chapter describes how the military and civilian systems currently interface for bidirectional translation of trauma care advances and lessons learned.
ESSENTIAL ELEMENTS OF A HIGH-PERFORMING TRAUMA CARE SYSTEM
The overall purpose of a trauma system is to address the needs of all injured patients “wherever they are injured and wherever they receive care” (ACS, 2014, p. 1). In many ways, the organization and delivery of trauma care in the United States serve as a paradigm for health care in the 21st century adopted by the Institute of Medicine’s (IOM's) Committee on the Quality of Health Care in America, which concluded that above all else, “a framework for a new health system should be based on systems that can organize themselves to achieve a shared purpose by adhering to a few well-thought-out general rules, adapting to local circumstances, and then examining their own performance” (IOM, 2001, p. 34). In keeping with the vision set forth by that committee, the aims of trauma systems are to provide care that is safe, effective, timely, patient-centered, efficient, equitable, and sustainable over time (ACS, 2014; IOM, 2001).
Every civilian regional trauma system is unique—a reflection of stakeholders’ tailoring the system to meet local needs based on regional population, economic, and geographic characteristics. Furthermore, each system is a dynamic entity, evolving in response to lessons learned, critical review, and changes in the population. As a result, trauma care delivery in the civilian sector occurs in the context of a “system of systems.”
Although every regional trauma system is unique, certain essential elements should be in place in any civilian or military trauma system to optimize efficiency and effectiveness. These elements, described in the sections below, are
- system leadership and statutory authority, with adequate funding to maintain an enduring system infrastructure;
- a trauma system plan developed and maintained by a multidisciplinary group of stakeholders and based on the needs of the population served by the system;
- creation, verification, and assurance of a sustainable trauma care workforce across the continuum of care;
- coordinated injury prevention efforts;
- prehospital care that includes effective communication systems and timely triage, transport of the injured to the appropriate level of hospital facility, and point of injury and en route care;
- regional categorization of hospital capabilities and designation/verification of trauma centers, with established criteria for interhospital transfers to ensure that patients receive the appropriate level of care;
- seamless transfer of patients to rehabilitation services, with attention paid to both their physical and psychosocial needs;
- system-wide trauma registries and information systems to support continuous quality improvement activities;
- research to develop the evidence needed to establish treatment guidelines for optimal care and outcomes (at both the individual patient and system levels); and
- integration with disaster preparedness programs.
While not exhaustive, these elements describe the fundamental features of a regionalized approach to the delivery of trauma care. In Model Trauma System Planning and Evaluation (HRSA, 2006), the Health Resources and Services Administration (HRSA) provides further detail on these elements and has served as a guide to modern trauma system development across the states. Critical to the effective integration of the various elements is a trauma system plan that is rooted in a public health approach to injury control, incorporating the core functions of assessment, policy development, and assurance (ACS, 2014; Bailey et al., 2012a; HRSA, 2006). The public health approach ensures that a regional trauma system is not merely a cluster of emergency services, but a comprehensive, organized structure for care of all injured patients within a defined geographic region. It emphasizes a three-pronged approach to improving health by
- identifying the problem, based on data (assessment);
- developing and implementing an intervention (policy development); and
- evaluating the outcome of the intervention (assurance) (HRSA, 2006).
The public health approach allows for the systematic collection of trauma-related data; the use of these data to develop comprehensive policies; and verification that services and facilities are adhering to triage, transport, and clinical care guidelines (ACS, 2014). Using data, policy, and evaluation, a trauma system can provide optimal care along the continuum from initial injury to transfer to rehabilitation. Most important, the public health approach emphasizes a population-based approach that ensures that the needs of a defined population are met in a manner that is effective, efficient, and patient-centered. As discussed later in this chapter, this means that prehospital and hospital resources must be configured in such a way that the most severely injured patients have timely access to a limited number of specialty referral centers with sufficient patient volumes to maintain quality, while the majority of less severe injuries are adequately cared for in a larger number of lower-level facilities.
System Leadership and Statutory Authority
If a trauma system is to be successful, a lead agency must have the legal and doctrinal authority necessary to ensure a high level of care for the injured. Following from the public health approach to injury control, this lead agency must be able to (1) continually assess trauma system structure, function, and outcomes; (2) create policy and guidelines responsive to such analyses; and (3) through a verification process, ensure the system’s optimal functioning. “Statutory authority and administrative rules support trauma system leaders and maintain trauma system infrastructure, planning, oversight, and future development,” throughout the continuum of care (ACS, 2008, p. 5). Further, the lead agency ensures the integrity of the trauma system and supports integration, collaboration, and coordination with other engaged entities. This approach ensures that all system components meet or exceed predescribed standards of care and adhere to evidence-based clinical practice guidelines. Absent statutory authority or rules, there would be nothing to prevent a hospital—any hospital—from calling itself a trauma center, nor would there be any means of ensuring that an ambulance can bypass a closer hospital in favor of direct transport to a center with all the resources needed to provide a patient with immediate and effective trauma care (Eastman et al., 2013).
For the most part, authority and accountability for trauma capabilities in the civilian system are regionalized, and, as discussed later in this chapter, vary from location to location (Hoyt, 2015b). States establish the authority and oversight for trauma system development, promulgating statutes and regulations for trauma center and trauma system participation and integration. State leadership also defines funding streams for system development and processes for trauma center designation/verification (HRSA,
2006). Each state has a lead agency. While these agencies most commonly reside within health departments, some operate on a stand-alone basis. The lead agency is responsible for integrating the trauma system with a range of other health care and community-based groups, including emergency management, social service agencies, public health, law enforcement, and disaster preparedness, among others (Eastman et al., 2013). Testimony provided to the committee emphasized the extent to which leadership and advocates at the state and local levels (e.g., local responders, local government, hospital corporations, medical directors) are critical to the optimal functioning of a trauma system (Patrick, 2015). Many states have adopted the concept of a regional trauma council to oversee the development of their trauma system infrastructure.
Box 2-1 highlights one state where a strong lead agency and enabling state legislation have been critical to achieving coordination, regionalization, and accountability. Underscored in this case study is the important role played by the public in advocating for and supporting the system. Continuously engaging the public through membership on key committees can make a difference in the system’s long-term sustainability.
In addition to state authorities, a range of federal stakeholders provide further trauma system leadership. However, no single federal entity is accountable for trauma capabilities and coordination across state boundaries in the United States, despite previous recommendations that a lead agency for emergency and trauma care be established (IOM, 2007a,b,c). Rather, multiple agencies share responsibility for ensuring that gaps in access to quality trauma care are addressed and best practices are developed and promulgated within the broader context of the civilian health care delivery system (see Box 2-2).
Professional societies, which exist for the full spectrum of the trauma care workforce, are another important source of trauma system leadership. These societies engage in a range of activities, including trauma system consultation and verification (e.g., the American College of Surgeons), education and training (e.g., National Association of Emergency Medical Technicians, Society of Trauma Nurses), and advocacy (e.g., American Trauma Society, Trauma Center Association of America).1
Trauma System Plan
The trauma system, as defined in statute, is best outlined in a trauma system plan that is developed in accordance with the needs of the popula-
__________________
1 The societies named here are offered as examples and are not intended as a comprehensive list. Space does not permit listing the many specialists, disciplines, and societies of health professionals focused on ensuring quality trauma care.
tion, an inventory of services and their geographic distribution, and any gaps identified in the planning process. The plan should be developed and maintained by a multidisciplinary group of stakeholders that includes, among others, trauma surgeons, emergency physicians, nurses, trauma program managers, prehospital personnel, rehabilitation providers, information system personnel, hospital administrators, and prevention experts.
Also critical to the development and maintenance of a trauma system plan is involvement of the general public, as well as trauma patients and their families who can speak firsthand about perceived gaps in the delivery of care. The plan should clearly outline how the needs of special populations are addressed. Typically, these populations include patients with specific types of injuries (e.g., burns, spinal cord injury), pediatric patients, and populations with unique barriers to access (rural, individuals with disabilities). Finally, the plan should undergo ongoing and regular assessment and be updated to meet the changing environment of the system.
Creation, Verification, and Assurance of a Sustainable Trauma Care Workforce
Critical to the success and sustainability of any trauma system is a workforce that is adequately trained and credentialed, and whose expertise is maintained. Leadership and policy need to ensure that members of the interdisciplinary workforce (nurses, EMS providers, emergency and EMS physicians, surgeons, advanced practice providers, other medical specialists, administrators, and information specialists) are trained, educated, and resourced to provide optimal care. Moreover, results from ongoing research and advances in care need to feed into continuous improvement of training curricula and skill set competencies. Periodic evaluation and adjustment of the size and scope of practice of the workforce need to be part of the system-level performance improvement and verification process.
Coordinated Injury Prevention Efforts
Approximately half of all trauma deaths occur at the scene of the injury or during transport to a hospital (Demetriades et al., 2005). As the majority of these deaths can be avoided only by preventing the injury from occurring (i.e., through primary prevention), an effective trauma system has an injury prevention strategy as one of its key components, with local epidemiologic data being used to target prevention initiatives. The Haddon matrix,2 represents a commonly used conceptual framework for injury prevention and control efforts that can help inform such initiatives by identifying primary prevention strategies that reduce the risk of an injury-producing event (e.g., speed limits and laws that limit driving under the influence), secondary
__________________
2 The Haddon matrix was developed by William Haddon, the first director of the National Highway Traffic Safety Administration, and is configured as a grid where rows represent the injury phases (before, during, and after) and columns represent influencing factors (e.g., human factors, injury agents or vehicles, and environmental conditions). Interventions can be listed within each cell of the grid, thus generating a diverse mix of primary, secondary, and tertiary prevention strategies (Haddon, 1970, 1980).
interventions that minimize the severity of an injury once an event takes place (e.g., restraint use, vehicle design), and tertiary prevention strategies that mitigate the health impact when injuries do occur (e.g., prompt access to emergency medical services) (Haddon, 1970, 1980).
The lead agency and providers within the system need to engage the public, community-based groups, prevention experts, and business entities to enact well-defined and evidence-based prevention programs that are responsive to local needs. Trauma survivors and families who have lost a loved one as a result of trauma can play a particularly effective role in helping to identify and advocate for injury prevention programs and policies. Their involvement also can enable them to make a contribution that can be an important component of their recovery. Interaction with public service agencies, such as the state department of health, is essential to successful implementation of prevention programs, and collaborations with multiple agencies, hospitals, and professional associations can broaden the impact of prevention initiatives. It is well accepted that a multipronged approach to injury prevention is necessary, one that emphasizes the three Es:
- Education (about the risks of injury and safe behavior)
- Engineering, ergonomics, and product design (to modify the built environment)
- Enforcement (of safety legislation and regulations) (Baker, 1973)
Where relevant and/or necessary, however, legislative efforts may yield the greatest impact on injury prevention, as has been demonstrated for laws related to seat belts, driving under the influence, and bicycle helmets (Anderson et al., 2009; Mock et al., 2004; Thompson et al., 1999). It is important to emphasize that, to be effective, prevention initiatives must have equal priority with other aspects of the trauma system and thus require dedicated human and physical resources.
Prehospital and En Route Care
Trauma centers are at the core of any trauma system, but have limited value in the absence of a strategy for ensuring timely access to the appropriate level of care. Emergency medical services (EMS), including access to these services through enhanced communications and 911 call systems, provide the critical link between an injury event and definitive care. However, in the initial moments after injury, bystanders and first responders (e.g., law enforcement) can occupy a crucial role, initiating lifesaving care before EMS personnel arrive (discussed further in Box 7-8).
The focus of the EMS response is on stabilizing the injured patients and transporting them to the appropriate level of care for further intervention
(Eastman et al., 2013). Although the provision of EMS is inherently local (Patrick, 2015), local systems are configured differently across the United States. Nationwide, there are an estimated 21,283 credentialed EMS agencies (FICEMS, 2011), comprising a mixture of private, public, and volunteer systems that often operate independently and sometimes at odds with each other. There is no one-size-fits-all configuration for EMS. Therefore, a fully integrated system at the regional level will have mechanisms in place to hold local EMS providers accountable for compliance with standardized (preferably evidence-based) protocols and active participation in system-wide quality improvement activities (Kupas et al., 2015).
Prehospital care providers also play an important role in ensuring that communication systems are utilized to limit death and disability either at the single patient level or at the population level in the case of mass casualty incidents. Ongoing communication between prehospital care providers and receiving facilities is essential to ensure seamless handoff of patients to a prepared hospital-based trauma team. The EMS communication to the trauma center initiates a trauma team activation. This trauma team includes the emergency physician, nurses, trauma surgeons, a surgical specialist, radiology, interventional radiology, respiratory therapy, the laboratory, the blood bank, the operating suite, critical care, and specialty care areas. Psychologists, child life specialists, social workers, and chaplains also are needed to support families and provide psychological first aid. Ideally, real-time information on available resources within the system helps with triage and transport decisions. An effective communication system also connects the EMS system with other public safety providers, including police, fire, emergency management, and public health personnel. These linkages are particularly important in coordinating the medical response system with the incident command system in the case of disasters or mass casualty incidents.
Definitive Care Facilities
At the heart of the trauma system is a network of hospitals or trauma centers that are equipped and staffed to provide definitive care for injuries across the spectrum of severity. As discussed in greater depth in the following sections, these facilities submit data to registries, participate in performance improvement activities, and have agreements with other centers in place to address interfacility transfer, educational support, and outreach (ACS, 2014; Bailey et al., 2012a). High-quality, patient-centered care should be the standard in all trauma centers. While this is not yet the reality in most centers, efforts increasingly are being made to embrace a more collaborative care approach.
Across the United States, hospitals are recognized as trauma centers by two means: designation and verification. Trauma center designation occurs
at the state or local level. In this process, which may vary from location to location, a state or local municipality identifies criteria to categorize trauma centers (ATS, 2016). Trauma center verification on the other hand is a voluntary, evaluative process offered by the American College of Surgeons (ACS) in which the ACS verifies the presence of specific resources outlined in Resources for Optimal Care of the Injured Patient (ACS, 2014). While some states designate five levels of hospital trauma centers, ACS only verifies Level I, II, and III trauma centers (ACS, 2014). The different levels of a trauma center indicate differences in resource availability, which translate to different roles and responsibilities (see Table 2-1). Level I and Level II centers provide the highest, most sophisticated level of care for the most severely injured. Level I centers, which are often university-based teaching hospitals, provide care for every aspect of injury and have responsibility for leading trauma education, research, and system planning. Level II centers offer many of the same clinical services as Level I centers, but may not provide the same level of comprehensive care or care for the most complex injuries. Level III, IV, and V centers serve patients in communities that lack immediate access to Level I or II centers, and provide emergency assessment, resuscitation, and stabilization before possible transfer to a higher-level trauma center (ACS, 2014; Eastman et al., 2013). The readiness of these lower-level centers to resuscitate and initiate treatment for major injuries and then expedite patient transfer to a higher level of care is a fundamental characteristic of a regional trauma system, one that plays a particularly critical role in rural areas of the United States where transport times to high-level facilities are long. Well-defined transfer guidelines are an essential element of the trauma system plan. The use of telemedicine within the context of an integrated system of care also can enhance the capabilities of Level III, IV, and V centers.
The number and distribution of trauma centers within a region should be based on need and known geographic barriers to access (ACS, 2015b). Guidelines for establishing the appropriate number, level, and location of trauma centers should be included in the trauma plan, and the lead agency should have the authority to designate trauma centers according to the plan. The guidelines should be based on a locally driven consensus process that engages all the appropriate stakeholders and above all else, focuses primarily on the needs of the injured (ACS, 2015b). Operationalizing a needs-based allocation of trauma centers has been difficult, however, as a result of long-standing traditions, local politics, and the changing landscape of health care delivery and payment policies. In the 1990s, many hospitals closed their trauma centers or reduced the level of care they were able to provide (e.g., from a Level II to a Level III facility) because of financial pressures (Shen et al., 2009). As some of these pressures have dissipated, trauma center designation has become more desirable, which has led to a possible
TABLE 2-1 Description of Trauma Center Levels
| Trauma Center Level | Characteristics |
|---|---|
| Level I |
|
| Level II |
|
| Level III |
|
| Level IV |
|
| Level V |
|
SOURCE: Adapted from Eastman et al., 2013.
oversupply of trauma centers in some areas of the country (Eastman et al., 2013). The committee’s discussions with several experts suggested that developing strategies for ensuring the appropriate number and configuration of trauma centers based on population needs may be one of the most important challenges facing trauma systems in the next 5 years. Addressing this challenge will require developing evidence-based methods for determin-
ing the appropriate number and location of trauma centers within a region and ensuring that statutes are in place that give the lead agency the authority to designate trauma centers according to these methods. ACS is leading efforts to develop a needs-based assessment tool that can be used by those regions struggling with this issue.3
Transfer to Rehabilitation
Since most patients who sustain severe injuries will survive, it is critical to ensure that they have every opportunity to return home and integrate back into everyday life. The process of rehabilitation should start in the acute care facility and should address both physical and psychosocial needs of patients and their families (psychosocial considerations and the transition to rehabilitation are discussed further in Chapter 6). It is important to note that care provided in the acute phase is directly linked to the rehabilitation required later on. For example, the level and type of limb amputation can affect the fitting of a prosthesis (Krajbich et al., 2016; Robb, 2015), and effective pain management during acute care has been associated with reduced psychological sequaelae (Bryant et al., 2009; Holbrook et al., 2010). Equally important is early and ongoing screening for psychosocial distress and referral to the appropriate services to avoid the development of diagnosable conditions of posttraumatic stress and depression and their impact on long-term disability. When a patient screens positive for a mood disorder, referral to a mental health specialist is important. Timely transfer to post-acute rehabilitation services (both inpatient and outpatient) can further limit the degree of permanent impairment and allow the patient to return to the highest possible level of function. Despite the importance of rehabilitation, however, its integration with other phases of care is perhaps the weakest link in the trauma care continuum (Eastman et al., 2013). Thus, it is important for each trauma system to conduct a rehabilitation needs assessment to determine the number, type, and quality of such services required and available in the geographic region. Rehabilitation specialists should play a leadership role to ensure that rehabilitation issues are integrated into the overall trauma system plan.
Trauma Management Information Systems and Quality Improvement Activities
Data on the processes and outcomes of care within a system are critical to ensuring that the system evolves and improves over time. Trauma
__________________
3 A preliminary draft of this tool was released in September 2015 and is available at https://www.facs.org/quality-programs/trauma/tscp/nbats#nbatstool (accessed May 17, 2016).
registries have been a standard part of civilian trauma system development, research, and quality improvement activities for decades. The trauma performance improvement process and the trauma registry are the hallmark functions of the trauma center, second only to patient care. These functions entail monitoring compliance with evidence-based practice, care delivered, and system performance to ensure that opportunities for improvement are quickly identified and addressed, optimizing patient outcomes. Performance measures vary based on geographic location, size, environmental conditions, population, and economic investments. Targeted performance measures evaluate system performance such as time from call to EMS on scene, scene response times by ground and air medical services, trauma transfers within the region, and trauma patients transferred more than twice.
Trauma registries exist at the hospital, regional, state, and national levels, with data flowing along this continuum from the local to the national level, although some regions rely on the state trauma registry to provide data for performance improvement and system advancement. Information such as injury patterns, geographic locations of injury, and frequency of injuries identified by a state trauma registry can help target resources for regional and statewide injury prevention programs and special populations, identifying, for example, the need for pediatric trauma centers or burn centers.
The National Trauma Data Bank (NTDB) is the largest aggregation of U.S. trauma registry data, containing more than 6 million patient records (ACS, 2015a). Submission to the NTDB is a required structural element of ACS’s trauma center verification process,4 but all trauma centers, including those that are state-designated, are eligible to submit data to the NTDB. The NTDB also is a critical part of the ACS Trauma Quality Improvement Program (TQIP), used increasingly by ACS-verified and state-designated trauma centers to compare their outcomes against national mortality benchmarks in support of quality improvement efforts (Nathens et al., 2012).5,6 States can create state TQIP collaborative programs that benchmark outcomes and performance relative to other state TQIP collaboratives. Doing so allows the state to define high performance and highlights opportunities for improvement. NTDB data also have been used at the national level to examine variations in processes of care across levels of trauma care and the impact of these variations on outcomes (Shafi et al., 2009a). One important limitation of NTDB data is that they do not include information
__________________
4 ACS verifies Level I, II, and III trauma centers.
5 Starting in January 2017, all Level I, II, and III trauma centers seeking ACS verification or reverification must participate in TQIP.
6 Personal communication, M. Neal, American College of Surgeons, to E. Cornett, the National Academies of Sciences, Engineering, and Medicine, regarding the National Trauma Data Bank and Trauma Quality Improvement Program, April 12, 2016.
from facilities other than trauma centers and therefore cannot be used for assessing important system-level outcomes such as access to trauma center care (Olson and Bowman, 2012).
More recently, prehospital data have been aggregated into the National EMS Database, which is a component of the National Highway Traffic Safety Administration’s (NHTSA’s) National EMS Information System (NEMSIS) (Dawson, 2006). Submission of data to NEMSIS is voluntary, however, and there is as yet no program equivalent to TQIP by which EMS agencies can benchmark their institutional performance, although, as discussed further in Chapter 7, some states, including North Carolina, have established their own EMS performance improvement systems (Mears et al., 2010). Linking state-level EMS data with the state trauma registry can assist in performance reviews, such as determining time from 911 calls to arrival at appropriate trauma centers, transfer times, and tracking of patients who are transferred more than once or are transferred out of the region or state because of limited resources.
Research
Research is the empirical feedback loop that validates and sustains continuous improvement in trauma care. Research findings help define best practices and thereby alter the course of system development. To be most effective, research data in all their forms must be made available to investigators and other stakeholders, allowing for the introspection necessary for the system to evolve to meet the needs of the population being served.
Research activity is a required capability of high-level trauma centers. As noted, most Level I trauma centers reside within academic medical centers, encouraging and facilitating the development of a structured research program (ACS, 2014). In addition, researchers need to increase efforts to understand the perspectives of patients and their families and consider those perspectives in defining gaps in the knowledge base, incorporating in their research outcome measures that are meaningful to patients and their families, and identifying ethically acceptable approaches to research in the acute phases of injury.
Integration with Disaster Preparedness Programs
The trauma system is an essential resource for state, regional, and local responses to mass casualty incidents and needs to be tightly integrated into disaster and crisis response plans. This need highlights the value of integrating the trauma system with public health and emergency management systems. Working relationships and cooperation between the trauma system and these agencies enable a more rapid and organized response in the event of a
disaster. Hurricanes Katrina and Rita in 2005 and the fertilizer explosion in West, Texas, in 2013 are examples of such coordination with trauma systems at the regional and state levels, respectively (Epley et al., 2006; Walker, 2013).
It also is important for the trauma system and its centers to conduct periodic resource assessments to evaluate their surge capacity for responding to mass casualty incidents (Gomez et al., 2011; Klima et al., 2012). These resource assessments should be complemented by simulated incident or tabletop drills requiring a multiagency system-wide response. Such drills provide an opportunity to test the emergency preparedness and mass casualty response plans for the trauma system and to train the teams that will respond should such an event occur. These simulated scenarios are likely to identify gaps (e.g., in preparation, triage, and team interactions) that could threaten the integrity of a response (King et al., 2006; Rivara et al., 2006). For example, not all EMS agencies or emergency rooms are equipped with the supplies (e.g., tourniquets) necessary to respond to public health disasters or massive trauma (King et al., 2015). Performance improvement and after-action review of disaster responses help identify additional opportunities for stakeholder integration, education, and system improvement, as well as lessons learned to share with other trauma systems (Campion et al., 2016).
THE IMPORTANCE OF INCLUSIVE CIVILIAN TRAUMA SYSTEMS
Early trauma system development efforts of NHTSA were focused on state regulations, EMS education, communication systems, medical direction, and trauma center development (Mullins, 1999). The Trauma Systems Development Act of 1990 was designed to provide planning support for such system development. Preparation of the original Model Trauma Care System Plan of 1992, revised in 2006, was a product of this planning and was led by HRSA. However, limited funding to support the process impeded further development and implementation of this plan in most states.
Early efforts in trauma system development in the United States focused on establishing exclusive networks of highly specialized trauma centers, primarily in urban environments, for treatment of the most severely injured patients. Less attention was paid to integrating into the system other acute care facilities that could care adequately for the majority of less severe injuries. While this approach worked well for those injured in close proximity to a trauma center, it failed to address the broader public health challenge of how to provide optimal care to any injured patient, regardless of location (ACS, 2014). In the latter part of the 1990s, a more inclusive and population-based approach to trauma system development was embraced, in which all acute health care facilities with a round-the-clock emergency department play a role in the system by undergoing verification of their
capabilities, providing care at a level allowed by their resources, and transferring patients to a higher level of care when necessary.
An inclusive and integrated approach to regional trauma systems is designed to provide care across the full spectrum of injury severity within a defined geographic region and ensure that every injured person is triaged to a level of care commensurate with his or her injury (IOM, 2007c). To this end, the committed efforts of all medical facilities in the region are required. The goal of such a system is to serve the population by matching the needs of the injured to the appropriate levels of care, ensuring that the most severely injured are treated in a limited number of specialty centers with sufficient patient volume to maintain quality while minimizing duplication of expensive resources across the system.
The American College of Surgeons Committee on Trauma has played a key role in catalyzing the development of inclusive trauma systems, developing a series of documents—Resources for Optimal Care of the Injured Patient—that set forth the characteristics and resources that represent the minimal expectations for verification of hospitals as trauma centers at varying levels of care (ACS, 2014). ACS also offers a trauma system consultation program that provides regions and states with a multidisciplinary analysis of their system, with the goal of system improvement that is tailored to local needs (ACS, 2014).
When fully operational, inclusive systems ensure a continuum of care, from public access to services through 911 call centers to effective communication systems, out-of-hospital EMS, timely triage and transport to definitive acute care facilities, and transfer to rehabilitation services as appropriate (see Figure 2-1). The trauma care continuum thus represents a chain of survival, with communication and coordinated efforts across all providers and levels of care being essential to maximize outcomes for injured patients. Breaks in the continuum “almost certainly contribute to excess morbidity and mortality” (Bailey et al., 2012a, p. 34).
Substantial evidence now supports the benefits of such an inclusive, regionalized approach to the delivery of trauma care. Studies have shown that treating the most severely injured in a designated Level I or Level II trauma center is associated with a significant survival benefit, is cost-effective, and leads to improved quality of life among survivors (Bailey et al., 2012b; MacKenzie et al., 2006, 2010; Mann et al., 1999; Nathens et al., 2000). MacKenzie and colleagues (2006) found that the risk of dying for a patient with moderate to severe injury was significantly lower for patients treated at a trauma center as compared to those treated at a non-trauma center facility. Likewise, Haas and colleagues (2010) found that severely injured patients who were first transferred to a facility other than a trauma center were nearly 25 percent more likely to die than those who were transferred to a trauma center immediately after injury. Similarly, Sampalis and col-

leagues (1997) found that immediate transport to a Level I trauma center reduced morbidity and mortality for severely injured patients. A greater degree of integration and involvement of all acute care facilities also benefits patients, being associated with a significantly lower injury-related mortality (Utter et al., 2006).
REGIONAL VARIABILITY IN TRAUMA SYSTEMS ACROSS THE UNITED STATES
The development of a national system of regional trauma systems is an ongoing effort, shepherded by leaders at the federal, state, regional, and local levels. Some states and local jurisdictions have achieved great success with the coordinated implementation of the critical trauma system components described in this chapter, observing concomitant improvements in mortality rates and serving as exemplars for others (one model statewide system is described in Box 2-3). Despite the demonstrated benefit of inclusive, regionalized trauma systems, however, variability in implementation of the essential elements of a trauma system remains across the nation (Eastman et al., 2013; Utter et al., 2006). This failure to conform to best practices in trauma system design and trauma care has resulted in variable patient outcomes such that following a traumatic injury, where one lives may determine whether one lives.
This variability in system design and performance is at odds with the American public’s expectations for high-functioning trauma systems. According to a 2004 Harris Interactive poll, the vast majority of Americans recognize the value of trauma systems: 90 percent believe it is extremely or very important for their state to have a trauma system, and the majority view having a trauma center nearby as equally or more important than having a fire department (83 percent), police department (83 percent), or library (89 percent) (Champion et al., 2006). And despite evidence that outcomes for injured patients vary across the country (discussed in the sections below), two-thirds of Americans are extremely or very confident that they would receive the best medical care should they sustain a serious or life-threatening injury (Champion et al., 2006). It is evident, therefore, that the public’s expectations are not being met and, more alarming, that the public is relatively unaware of the disparities in trauma system development and quality nationwide.
Variability in Trauma System Access
Nearly 2,000 trauma centers exist nationwide; 2013 estimates from the American Trauma Society suggest there are 213 Level I, 313 Level II, 470 Level III, and 916 Level IV or V centers (Eastman et al., 2013). However, these centers are not distributed evenly across the country (see Figure 2-2). Although several factors influence geographic variability in trauma mortality, the association between the lack of access to an appropriate level of trauma care and higher mortality rates among trauma patients is compelling (Eastman, 2010) (see Figure 2-3). Studies have shown that 69.2 percent and 84.1 percent of Americans have access to a
Level I or Level II trauma center, respectively, within 1 hour by land or by air, but the availability of trauma center care at any level is still severely limited in some areas of the country (Branas et al., 2005). Most dramatic is the disparity between rural and urban/suburban regions; only 24 percent of rural residents have access to a Level I or Level II trauma center within 1 hour, compared with 86 percent and 95 percent of suburban and urban residents, respectively. In other areas, however, the number of Level I and II trauma centers alone far exceeds the number needed to concentrate the patient volumes that have been shown to correlate with improved quality and outcome (Branas et al., 2005; Eastman et al., 2013). In such areas, each center has a lower patient volume, which may reduce
the quality of care. Thus there is an argument to be made for limiting the number of Level I or II centers within a region (Eastman et al., 2013; Haas et al., 2009; Nathens and Maier, 2001).
Variability in Adoption of Best Trauma Care Practices
Even when patients have timely access to trauma centers, these centers must be properly utilized to make an impact. Guidelines and recommendations for best practices in field triage and in trauma care exist, but compliance with these guidelines varies widely. The American College of Surgeons and the U.S. Centers for Disease Control and Prevention (CDC) have devel-
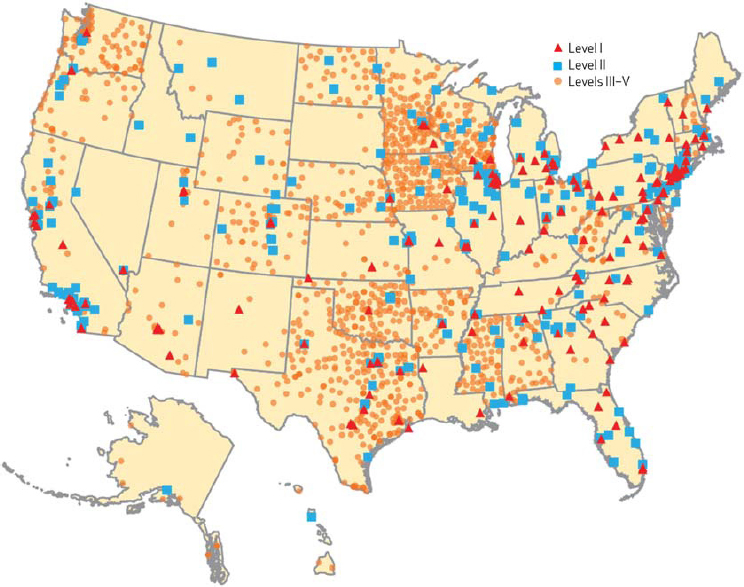
NOTE: Because of limited resolution when trauma centers are depicted on a national scale, the presence of multiple trauma centers within a single city may not be apparent in this figure.
SOURCE: Copyrighted and published by Project HOPE/Health Affairs as Eastman et al., Sustaining a coordinated, regional approach to trauma and emergency care is critical to patient health care needs. Health Aff (Millwood). 2013; 32(12):2091-2098. The published article is archived and available online at www.healthaffairs.org.
oped and promulgated evidence-based criteria for field trauma triage (ACS, 2014; CDC, 2012; Sasser et al., 2009). These criteria represent an attempt to balance both under- and overtriage, so that patients are taken to an appropriate trauma center, while higher-level trauma centers are not overwhelmed with minimally injured patients (Barnett et al., 2013; Newgard et al., 2013). The use of these criteria has been shown to be cost-effective (Faul et al., 2012), but inappropriate triage of patients remains a problem. In some regions, one-third of severely injured patients are not transferred to a Level I or II center (Nathens et al., 2004), with elderly patients at the greatest risk of being undertriaged (Gage et al., 2012; Nakamura et al., 2012). State EMS protocols vary in their incorporation of these triage criteria: as of 2011, 16 states indicated that they had fully or partially implemented the CDC’s 2006 guidelines (CDC, 2012).
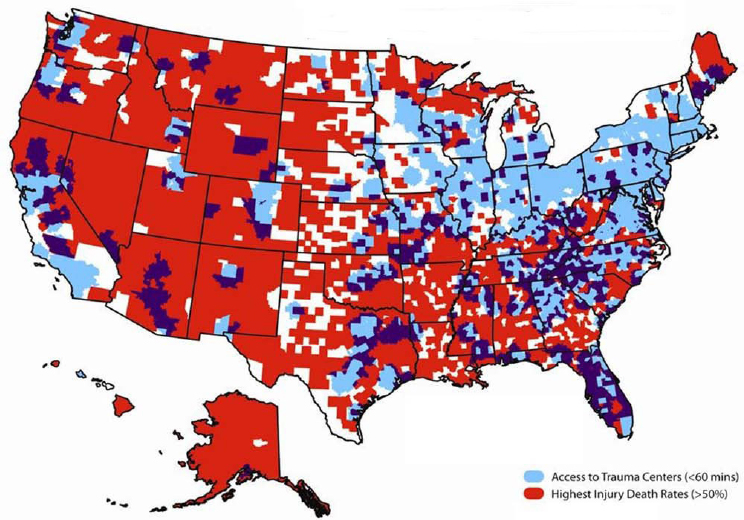
SOURCE: Map provided by Charles Branas, Ph.D., Professor of Epidemiology, University of Pennsylvania, 2016.
Once a patient has been transferred to the appropriate trauma center, his or her care may vary depending on the center. As with triage, evidence-based best practice guidelines for trauma care exist and have been shown to improve outcomes, yet compliance with these guidelines is variable (Sobrino et al., 2013). A study of 55 trauma centers found that only 1 was compliant with all 32 practice protocols, while half were compliant with 14 of the 32. Patient outcomes likewise vary at different trauma centers, and Shafi and colleagues (2014) suggest that this inconsistency may be due to the level of compliance with commonly recommended clinical practices. The five trauma centers they studied varied dramatically in the level of compliance, from a low of 12 percent to a high of 94 percent.
Interhospital variation in risk-adjusted outcomes among trauma patients indicates that the quality of care provided across trauma centers varies as well (Shafi et al., 2009b, 2010) (see Figure 2-4). While trauma centers with the highest patient volumes have been shown to have better patient outcomes, including lower mortality, fewer days on ventilator, and less severe organ failure (Minei et al., 2014), better patient outcomes
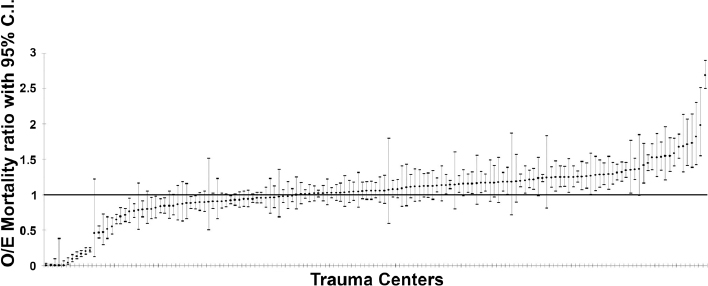
NOTES: Ratios compare observed mortality rate in a trauma center with the expected mortality rate based on the center’s patient mix, i.e., a rate that is risk adjusted for such factors as age, injury severity, and comorbidities. The figure shows three distinct groups of trauma centers: high-performing (O/E mortality ratio < 1), moderate-performing (O/E mortality ratio = 1), and low-performing (O/E mortality ratio > 1). All trauma centers with confidence intervals that cross 1 perform at the same level (moderate). C.I. = confidence interval; O/E = observed-to-expected.
SOURCE: Reprinted, with permission, from Shafi et al., 2010, Health care reform at trauma centers—mortality, complications, and length of stay. The Journal of Trauma and Acute Care Surgery 69(6):1367-1371.
also are associated with higher levels of compliance with recommended clinical practices. Shafi and colleagues (2014) found that at Level I trauma centers, every 10 percent increase in compliance with recommended practices resulted in a 14 percent reduction in in-hospital mortality. When an individual patient received all of the recommended care, he or she was 58 percent less likely to die than a patient who did not.
Variability in Emergency Medical Services Systems
Like access to and care provided at trauma centers in the United States, the organization and outcomes of the estimated 21,283 EMS systems nationwide vary significantly (FICEMS, 2011). EMS systems range from individual ambulance services that operate by “home rule”7 to coordinated regional or county-based systems. The latter comprise multiple individual ambulance services working together to achieve cohesive systems of dispatch, preparedness for mass casualties, uniform medical protocols and quality oversight, and integration with the hospitals and health care
__________________
7 “Home rule is a delegation of power from the state to its sub-units of governments (including counties, municipalities, towns or townships or villages). That power is limited to specific fields, and subject to constant judicial interpretation, but home rule creates local autonomy and limits the degree of state interference in local affairs” (National League of Cities, 2013).
systems within the region. Additionally, the ambulance services that make up EMS systems vary from fire agency based, to municipal “third service” agencies (separate from the municipal police and fire agencies), to private agencies (FICEMS, 2011). These various types of EMS systems are staffed by volunteer or paid EMS providers that are trained and equipped to offer varying levels of medical care.
The challenges inherent in such variability and the importance of unifying the many EMS stakeholders have long been recognized. In 1996, NHTSA assembled these stakeholders to craft a unifying vision for EMS. The resulting document, the EMS Agenda for the Future, has led to advances in training, education standards, and scope of practice, among others (NHTSA, 1996). Although levels of providers and scopes of practice continue to vary from state to state, NHTSA has published a national EMS scope of practice model that offers standard definitions for levels of training and interventions performed by different levels of EMS providers (NHTSA, 2007). This national scope of practice model encompasses (1) emergency medical responders (EMRs), who have minimum training to provide the most basic care as a first response to life-threatening medical emergencies; (2) emergency medical technicians (EMTs), the basic level of ambulance provider, who provide comprehensive basic life support care and expertise in extrication, patient lifting and handling, and transportation; (3) advanced EMTs (AEMTs), who are able to administer several medications and advanced life support care; and (4) paramedics, who provide a broad spectrum of advanced life support care including administration of advanced prehospital procedures and multiple medications. Although these national scopes of practice represent an attempt to standardize these levels of providers, the scope of practice for each level can differ significantly among the states (IOM, 2007b).
Beyond these variations in the types of EMS systems and the providers that staff them, wide variation exists in the acceptance of best practices and the outcomes of patients with various medical conditions. EMS providers generally follow medical protocols that may be local (applying only to a single agency), countywide, regional, or statewide (Kupas et al., 2015) (see Figure 2-5). Although there are few evidence-based guidelines that pertain to EMS, they are growing in number, and the National Association of State EMS Officials recently completed a project that produced model clinical guidelines for EMS care (NASEMSO, 2014). Data that can be used to associate outcomes of trauma patients with prehospital care provided by different types of EMS agencies or providers are scant. However, research has shown significant differences in survival—as great as twofold—among severe trauma patients treated by EMS in various communities across North America (Minei et al., 2010; Newgard et al., 2008).
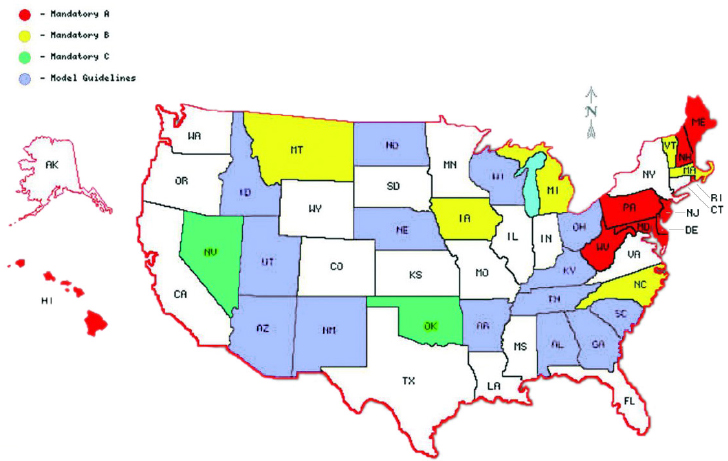
NOTES: States colored red, yellow, or green have mandatory statewide protocols (yellow and green indicate the existence of a state process by which EMS can petition to alter those protocols or develop their own). States colored blue have model protocols that local or regional EMS can choose to use. In states that are white, no statewide protocols or model guidelines exist.
SOURCE: Kupas et al., 2015, reprinted by permission of Taylor & Francis Ltd.
OVERVIEW OF THE MILITARY’S TRAUMA CARE SYSTEM
Just as the sophisticated civilian trauma systems in the United States emerged from the successes and lessons of military trauma care during the wars in Korea and Vietnam, the military has contemporized, expanded, and improved upon principles of civilian trauma system design that evolved over more than 25 years in the period between the end of the Vietnam War and the wars in Afghanistan and Iraq. This section describes the development and features of the military’s contemporary system for trauma care delivery—the Joint Trauma System (JTS)—and its relation to the broader Military Health System (MHS). Also described below is the distribution of responsibility for trauma care in the military, and the variability in trauma systems across the military.
The Development of the Military’s Joint Trauma System
At the start of the U.S. engagement in Afghanistan in 2001, there was no joint plan or system for delivering trauma care in theater. Service-specific
(i.e., Army, Navy, Air Force) medical personnel and other assets were embedded in deploying military forces, consistent with the organization of trauma care employed in previous conflicts (DHB, 2015). Following U.S. entry into combat operations in Afghanistan and Iraq, a group of military clinicians identified the need for a more systematic approach to trauma care in U.S. Central Command8 (CENTCOM) for soldiers wounded on the battlefield (Bailey et al., 2012a). This inclusive system—the Joint Theater Trauma System—was implemented in 2004 and modeled after the successful regionalized trauma systems in the civilian sector. Its stated vision was “to ensure that every soldier, marine, sailor, or airman injured on the battlefield has the optimal chance for survival and maximal potential for functional recovery” (Eastridge et al., 2006).
The critical elements and capabilities of military and civilian trauma systems are largely the same. While varying slightly in the application of these trauma system principles, both share the goal of meeting the needs of patients wherever they are injured and wherever they receive care. As in the civilian sector, the military’s inclusive trauma system is designed to integrate care across the continuum, beginning at the point of the injury, and to minimize the time to definitive care.
There are, however, some basic operational and environmental differences between military and civilian trauma care that impact the way that care is delivered. In the context of military trauma, for example, it is frequently necessary for a patient to receive care at multiple facilities after being wounded, with “life- and limb-preserving care” being provided far forward on the battlefield and at military treatment facilities (MTFs) (Bailey et al., 2012a, p. 34). Thus the military must ensure the capability to deliver trauma care interventions separated in space and time that in the civilian world often would take place within a single trauma center. Further, compared with civilian practice, the military must manage a high volume of severe multisystem injuries in an environment in which resources (supplies such as diagnostic and surgical equipment, as well as staff) are limited, and transport times are unpredictable. The military also is frequently overwhelmed by multiple or mass casualties, and point-of-injury care and evacuation may be impeded by an active firefight or other dangerous circumstances (Lenhart et al., 2012), a situation not as commonly encountered in the civilian sector. Finally, the military’s trauma system in theater must continuously and rapidly adapt to an evolving combat environment. For
__________________
8 There are nine unified (joint) combatant commands (CoCOMs) in the U.S. military, covering both regional (e.g., Central Command, Pacific Command) and functional (e.g., Special Operations Command) areas. Located between the European and Pacific CoCOMs, Central Command (CENTCOM) covers the “central” area of the globe, including Afghanistan and Iraq.
SOURCE: Adapted from Bailey et al., 2012a.
example, security situations can change rapidly in a given area and logistical support evolves as the theater matures. In contrast, civilian trauma care systems are more stable and predictable.
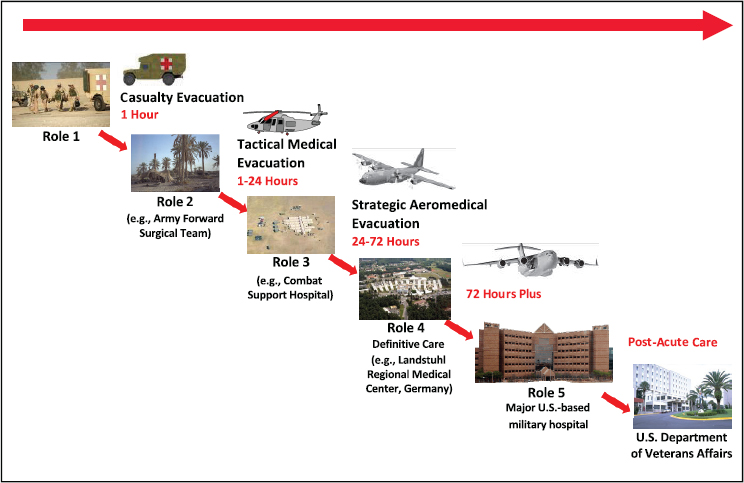
The military organizes its trauma care continuum and MTFs into five levels or “roles” of care9 (see Figure 2-6). Each role corresponds to the level of care provided. Role 1 first responders (self, buddy, or medic) in the prehospital setting assess the injury, provide emergency care (e.g., apply tourniquets for hemorrhage control), and arrange for evacuation to a higher-level facility. Role 2 provides limited hospital capability for forward resuscitative care (emergency resuscitation, damage control surgery, blood transfusion) through small treatment facilities and mobile forward surgical teams consisting of surgeons, anesthetists, nurses, and technicians. Role 3 facilities are large, semipermanent facilities (combat support hospitals) that provide surgery, intensive care, postoperative care, and specialty care. Patients requiring longer-term care are evacuated to Role 4 or 5 definitive care facilities. Transport between these echelons may include a medical team and management of the patient, although some evacuations emphasize speed over medical care (Lenhart et al., 2012). Depending on the nature of
__________________
9 While the American College of Surgeons uses Level I as the highest level of definitive care in the civilian sector, the military uses Role 5 as its highest level of care.
the injury and the distance to a higher-level medical facility, casualties may be transported directly from the point of injury to a Role 3 MTF.
In 2005, the Joint Theater Trauma Registry was established—modeled after the NTDB and now called the Department of Defense Trauma Registry (DoDTR)—to systematically collect information on injuries, including demographic, mechanistic, physiologic, diagnostic, therapeutic, and outcome data (Eastridge et al., 2009; Pruitt and Rasmussen, 2014). While prehospital data were integrated into the DoDTR in 2013, documentation of prehospital trauma care has and continues to be suboptimal (Haut et al., 2016). The analysis of data maintained in the DoDTR allows for near-real-time improvement in trauma care delivery and patient outcomes across the trauma care continuum. Additionally, the DoDTR has served as a key source of data for retrospective research and facilitated programmed, requirements-driven research performed by the military’s Combat Casualty Care Research Program. As discussed in more detail in Chapter 4, the development and maturation of the military’s registry-driven performance improvement processes and medical research program have played a key role in decreasing mortality and morbidity over the course of the wars in Afghanistan and Iraq (Pruitt and Rasmussen, 2014).
In 2010, the JTS10 became a formal program of record under the U.S. Army Institute for Surgical Research (Bailey et al., 2012a), where it provides for ongoing development and maintenance of the military trauma system’s support infrastructure, including the DoDTR and performance improvement processes (see Figure 2-7). Although the JTS serves as the military’s de facto lead agency for trauma, recognized as a DoD Center of Excellence in 2013, the military has not formalized this role (Robb, 2015). A lack of doctrinal authority limits its capacity to function as a lead agency for the military trauma system. For example, the JTS does not have the authority to set policy or ensure that standards are met through a verification process (Rotondo et al., 2011).
As shown in Figure 2-7, the JTS interfaces with two programs that both represent critical elements of a model trauma system as described earlier in this chapter—prevention and research. The DoD’s Joint Trauma Analysis and Prevention of Injuries in Combat (JTAPIC) program has the responsibility to collect, integrate, analyze, and store operations, intelligence, materiel, and medical data to inform solutions that prevent or mitigate injury in the deployed setting (i.e., primary and secondary prevention strategies) (JTAPIC, 2016). For example, data gathered about injury patterns during the conflicts in Afghanistan and Iraq have informed the design and field-
__________________
10 Whereas the functional domain of the Joint Theater Trauma System is limited to the U.S. CENTCOM theater of operations, the JTS supports a military trauma system capability across all combatant commands (Rotondo et al., 2011).
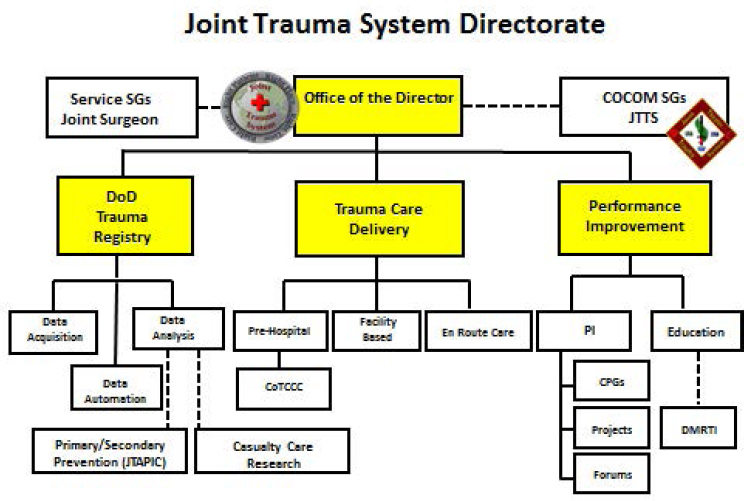
NOTE: CoCOM = combatant command; CPG = clinical practice guideline; CoTCCC = Committee on Tactical Combat Casualty Care; DoD = U.S. Department of Defense; JTTS = Joint Theater Trauma System; PI = performance improvement; SG = surgeon general.
SOURCE: Adapted from Bailey et al., 2012a.
ing of body armor and other personal protective equipment (DCBI Task Force, 2011; Eastridge et al., 2006). Similar observations regarding the increase in multiple fragment injuries resulting from the use of improvised explosive devices by insurgents (GAO, 2009) led to “up armoring” of military vehicles to reduce penetration and occupant injury (Zoroya, 2013). Protective equipment, along with the emphasis on predeployment training (discussed further in Chapter 5), have likely contributed to the significantly lower case fatality rate associated with the recent wars in Afghanistan and Iraq as compared to the Vietnam War (Eastridge et al., 2006) (see Figure 1-3). Given the value of DoDTR to support the epidemiological analysis of injury patterns and the identification of prevention strategies (e.g., uniform redesign, seat-belt education initiatives), continued coordination between the JTS and JTAPIC is essential. The JTS is also closely linked to the DoD’s combat casualty care research program, informing research priorities based on registry-driven performance improvement data and, on the
back end, integrating research-generated knowledge into evolving clinical practice guidelines (this interface is discussed in more detail in Chapter 4).
Distribution of Responsibility for Trauma Care in the Military
Mirroring the distribution of leadership across numerous local, state, and federal agencies in the civilian sector, responsibility for the delivery of military trauma care is spread across multiple entities and actors within the DoD (see Figure 2-8).11 As in the civilian sector, there is no single point of accountability for the military’s medical readiness mission.
Within the MHS, the Assistant Secretary of Defense for Health Affairs (ASD(HA)) serves as principal advisor for health issues for DoD and is responsible for policy development and oversight of all MHS programs and activities. As the Defense Health Program appropriation holder, the ASD(HA) is responsible for administering the MHS budget, which includes management of the resources that fund the service medical departments (DoD, 2014). While the ASD(HA) directs policy, the health missions of the MHS are administered through each service’s surgeon general, along the organizational lines of the Army, Navy, and Air Force. In addition, execution of policy within the MHS is facilitated by a joint combat support agency12—the Defense Health Agency (DHA) (DoD, 2014; Schwab, 2015).
Established in 2013, the DHA is charged with developing strategies to contain costs, improve efficiency, and encourage collaboration and opportunities for joint operations among the three services. As a combat support agency, the DHA’s mission is to enable the Army, Navy, and Air Force medical departments to “provide a medically ready force and ready medical force” to all combatant commands during peacetime and wartime (DHA, 2014, p. 3). To provide advice on tactical management of the MHS, the DHA works collaboratively with the service surgeons general13 and members of Joint Staff.14
The DHA consists of a number of directorates. Under its Education and Training Directorate, the DHA leads standardized education and training across the MHS and coordinates professional development and sustainment
__________________
11 The roles and responsibilities of these entities and actors are discussed in greater detail in Box 7-5.
12 Combat support agencies provide department-level and tactical support to the joint operating forces of the U.S. military during combat and other military operations (DoD Directive 3000.06). Other examples of DoD combat support agencies include the Defense Logistics Agency and the Defense Intelligence Agency.
13 The director of the DHA, a lieutenant general, holds the same rank (3-star general) as the service surgeons general.
14 The Joint Staff assists the chairman of the Joint Chiefs of Staff, who is the principal military adviser to the President, the Secretary of Defense, and the National Security Council.
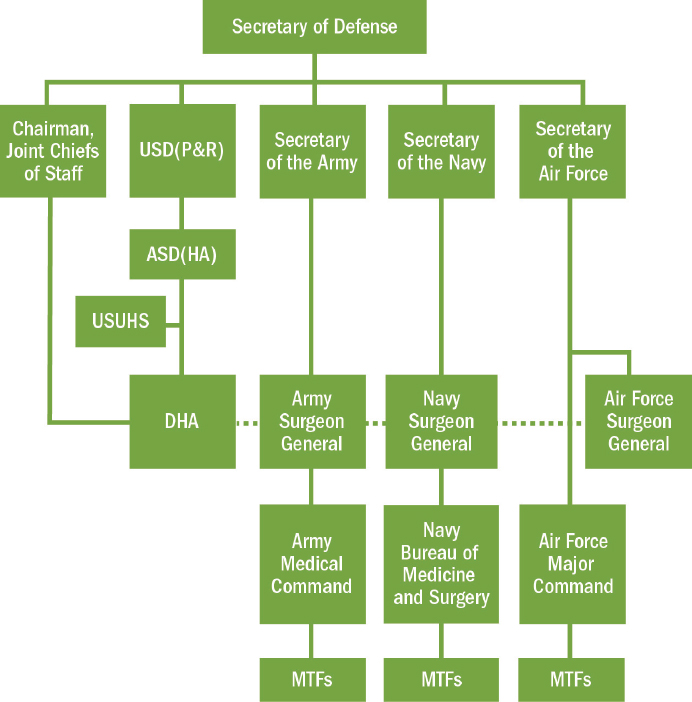
NOTE: ASD(HA) = Assistant Secretary of Defense for Health Affairs; DHA = Defense Health Agency; MTF = military treatment facility; USD(P&R) = Under Secretary of Defense for Personnel and Readiness; USUHS = Uniformed Services University of the Health Sciences.
SOURCES: Adapted from DHA, 2014; DoD, 2014.
programs. The DHA’s Research, Development, and Acquisition Directorate coordinates medical research taking place across the services and the MHS, prioritizing important research and minimizing redundant work. Within its Healthcare Operations Readiness Division, the DHA has centralized management over service-support functions, including theater information systems, logistics, and facilities. In this capacity, the DHA aims to ensure force health protection and implements deployment-related health policy (DHA, 2014; DoD, 2014).
At this time, however, the DHA remains in an immature state of transi-
tion to full operational capacity. The DHA’s roles and responsibilities, particularly in relation to those of the military departments, are still evolving.
Two distinct branches of the military chain of command affect the delivery of combat casualty care on the battlefield. The first encompasses the unified combatant commands (e.g., CENTCOM). Each unified combatant command has its own commander who reports directly to the Secretary of Defense. Combatant commanders are responsible for the operational direction of the forces assigned to the combatant command and the performance of any assigned missions. As a result, it is line—i.e., nonmedical leadership that maintains control over the budget, personnel, and equipment assigned by the military departments to support combat casualty care in theater.
The second chain of command runs from the Secretary of Defense to the Secretaries of the military departments. Through their respective service chiefs, the Secretaries of the Army, Navy, and Air Force exercise control, authority, and direction over those personnel not specifically assigned to combatant commanders or the National Capital Region.15 Each individual service medical command is responsible for and has control over its military treatment facilities (DoD, 2014). This complex hierarchical structure creates challenges to ensuring the consistent application of best trauma care practices and achieving standardization across DoD. Differences among the services in approaches to readiness and medical care capabilities in theater (particularly at Role 2 and Role 3 facilities) have been noted (DHB, 2015). The resultant deficits in interoperability impede system cohesion.
Although the DHA has been designated a combat support agency for health and medical operations, the complex overlapping and conflicting authorities among the combatant commands, the Joint Staff, the Secretary of Defense, and the military departments make it extremely difficult to establish reliable joint combat casualty care processes and systems; set and allocate funding for readiness, research, and staffing priorities; and establish a single point of accountability for delivering quality medical services across all combatant commands.
Variability in Trauma Systems Across the Military
As mentioned previously, the Joint Theater Trauma System is limited to the CENTCOM theater of operations. In contrast, the JTS is designed “to support a continuous deployable global trauma systems capability” for the entire military, ready to facilitate and guide the implementation of a theater trauma system in each combatant command (DHB, 2015). At
__________________
15 The DHA exercises control over military treatment facilities and personnel not specifically assigned to combatant commanders within the National Capital Region.
this time, however, the JTS operates largely in CENTCOM alone. The JTS is working with Pacific Command to assist that combatant command in proactively establishing its own theater trauma system (DHA, 2014; Gross, 2015). While the JTS has reached out to other combatant commands, it has received limited response (Gross, 2015). Although the JTS is a formal DoD entity with a global mission, it was established as a noncommand and tenant organization of the U.S. Army Institute of Surgical Research, which is a subordinate organization under the U.S. Army Medical Research and Materiel Command. It lacks the organizational and leadership authority to effect doctrinal change in regional combatant commands.
CENTCOM itself displays great variability in the extent to which line leaders and their units have committed to the principles of an inclusive trauma system and adhered to the best practices (e.g., clinical practice guidelines) emerging out of the JTS. This variability is reflected in patient outcomes. As discussed in Chapter 1, the 75th Ranger Regiment—characterized by complete line ownership of medical care—achieved dramatically better outcomes compared with the greater military population (Kotwal et al., 2011).
HOW MILITARY AND CIVILIAN SYSTEMS INTERFACE FOR BIDIRECTIONAL TRANSLATION
As evidenced in the preceding sections, the delivery of trauma care in the military and civilian sectors forms a diverse landscape. Partnership across the military and civilian systems can facilitate the transfer of lessons learned and encourage the continued advancement of trauma care in both sectors. While interface between the military and civilian sectors is hardly a new phenomenon, a number of collaborative platforms have recently been developed to encourage the bidirectional translation of best practices.
Training Pipeline and Practice at Military Trauma Centers
The vast majority of military surgeons, nurses, and medics receive their medical training in the civilian sector. Following graduation, the surgeons undertake residencies in the military or continue their postgraduate training in the civilian sector. For those who complete their medical education and training in the civilian sector, interface with the military is limited. Those who complete their education in the military sector are similarly isolated from the civilian world.
After residency or fellowship training, military surgeons are assigned either to an MTF or to a civilian trauma center with an embedded military cadre that oversees predeployment training. These service-specific trauma
training centers, discussed in more detail in Chapter 5, have provided valuable opportunities for bidirectional sharing of knowledge, as well as the generation of new knowledge through joint military–civilian research initiatives. In addition to surgeons, other military medical specialists assigned to civilian trauma training sites include anesthesiologists, emergency physicians, nurse anesthetists, nurses, and technicians, offering opportunities for cross-sector learning at all provider levels (Cannon, 2016).
Currently, three MTFs are verified as trauma centers by the American College of Surgeons: San Antonio Military Medical Center (SAMMC) (Level I), Walter Reed National Medical Center (Level II), and Landstuhl Regional Medical Center (Level III) (Cannon, 2016). Verification gives the physicians, nurses, and medics assigned to these facilities numerous opportunities to engage with civilian trauma leaders. Experienced civilians frequently maintain the trauma infrastructures of these MTFs, an interface that imparts to military physicians the knowledge and administrative skills necessary to provide organizational leadership for trauma care in combat zones. SAMMC also hosts civilian trauma experts as visiting professors, and SAMMC physicians are invited to attend events with visiting professors at the University of Texas Health Sciences Center at San Antonio (see Box 2-4). These interactions enable military personnel to learn about advances in civilian trauma care and expose the visiting professors to lessons learned in military trauma care (Cannon, 2016). Most military physicians, nurses, and allied health providers, however, provide beneficiary care at non-trauma center MTFs, where they have few opportunities to exchange ideas and lessons learned with civilian trauma professionals and little opportunity to put their lessons learned into practice. During the wars in Afghanistan and Iraq, military personnel deployed to Landstuhl Regional Medical Center or facilities in those two countries had the opportunity to interact with visiting civilian surgeons through the Senior Visiting Surgeon Program. Between 2005 and 2012, 192 civilian surgeons participated in this program. Participants reported that they gave lectures, conducted research, established mentorship relationships with military surgeons, and were exposed to military practices that were relevant to their civilian trauma care (Blackbourne et al., 2012; Moore et al., 2007).
In the combat context, physicians, nurses, and medics deployed through the Reserves and National Guard are an important force in encouraging bidirectional translation of best practices and lessons learned. These individuals are immersed in the civilian sector, bringing that expertise to their deployed team. Following deployment, they return to the civilian sector, where they can apply lessons learned during their military experience (Cannon, 2016).
Societies and National Meetings
Professional societies have provided support for military medical providers throughout the recent conflicts. Civilian societies, such as the American Academy of Orthopaedic Surgeons, American Association for the Surgery of Trauma, American College of Surgeons, Orthopaedic Trauma Association, and Society of Vascular Surgeons facilitate the exchange of information and collaboration between military and civilian surgeons (Cancio et al., 2015), and they give military surgeons a platform for peer review of their research, as well as an opportunity to lead and participate in academic medical activities. Nursing (e.g., Society of Trauma Nurses) and prehospital care societies (e.g., National Association of Emergency Medical Technicians) serve similar roles for those disciplines.
National meetings provide another venue for exchange and collaboration between military and civilian providers. Participation at such meetings can accelerate the translation of advances from one sector to another. For example, Cancio and colleagues (2015) found that the migration of the concept of “damage control resuscitation” from its origins in the military to civilian publications was due in part to presentations at meetings and publications in journals, suggesting successful translation of lessons learned in the military to the broader civilian context. Military personnel have participated in civilian meetings throughout the recent conflicts, with a peak in participation during 2005 to 2007 (Cancio et al., 2015). Civilian participation in military societies is less common, although civilian attendance at the Military Health Service Research Symposium has increased in recent years.
Beginning in 2006, the American Academy of Orthopaedic Surgeons, together with the Orthopaedic Trauma Association, the Society of Military Orthopaedic Surgeons, and the Orthopaedic Research Society, has sponsored an annual 2-day symposium that brings the military and civilian orthopaedic trauma communities together to share best practices and define research priorities for the future. Publications resulting from each symposium have helped define current knowledge gaps regarding management of major limb trauma for Congress, DoD, the National Institutes of Health, and industry (AAOS, 2016). The first symposium defined the current state of practice, focusing on challenges related to combat casualty care (Bosse et al., 2012). Subsequent topics included challenges in definitive reconstruction, barriers to return of function and to duty, maintaining force readiness during an era of military transition, and disaster preparedness (Andersen et al., 2015).
Unfortunately, a 2012 DoD policy change (due to sequestration) limits the number of military personnel participating in civilian meetings and the frequency of that participation despite the clear benefits to both sectors. As a cost-cutting measure, the Office of the Secretary and Deputy Secretary of Defense must now approve all conference attendance by military personnel (Carter, 2012). This change has resulted not only in fewer military personnel attending meetings, but also far fewer military papers being presented (Cancio et al., 2015).
Military–Civilian Leadership-Level Partnerships
Given the variety of stakeholders engaged in the delivery of trauma care, the transfer of best practices and lessons learned between the military and civilian systems depends on an integrated and collaborative systems approach. Recognizing this fact, military and civilian leaders in trauma care have developed two collaborative platforms—the Federal Interagency Committee on Emergency Medical Services (FICEMS) and the Military Health System American College of Surgeons (MHS/ACS) Strategic Partnership.
FICEMS
The delivery of EMS across the nation involves the work of and interaction between numerous federal agencies. To complement these activities, FICEMS was established in 2005 to institutionalize these relationships and ensure coordination among the federal agencies involved with emergency medical services. FICEMS’s membership includes DHS, DoD, DOT, the Federal Communications Commission, HHS, and a State EMS Director appointed by the Secretary of Transportation (Dawson, 2015).
Building on a number of successes, FICEMS is gradually focusing its efforts on greater specificity and accountability through a formal strategic planning process. Included within FICEMS’s Strategic Plan are objectives related to applying lessons from military and civilian incidents to the EMS community and transitioning military EMS providers to civilian practice (Dawson, 2015; FICEMS, 2013). In uniting the efforts of the military and civilian sectors and making the translation of lessons learned a priority, FICEMS serves as a meaningful platform for working toward improved care in the prehospital setting throughout the United States.
MHS/ACS Strategic Partnership
The concept behind this partnership, launched in December 2014, emerged from the shared recognition by DoD and the American College of Surgeons of the need for a synergistic and collaborative relationship between the military and civilian sectors to ensure that the next generation of surgeons would be adequately prepared to deliver optimal trauma care to patients (Hoyt, 2015a,c). Through this partnership, the civilian sector, represented by the American College of Surgeons, can partner with DoD in four areas:
- creation of a quality, learning collaborative
- education and readiness
- formal assessment of the JTS
- consideration of how to create an infrastructure for clinical trials using clinical registries and trauma hospital networks (Hoyt, 2015b)
Box 2-5 lists specific agreements outlined in the partnership charter.
CONCLUSION
When the critical elements of a trauma system are in place and integrated across the continuum of care, optimal care can be delivered. The experiences
of the 75th Ranger Regiment and the Pennsylvania and Maryland trauma systems attest to the value of such integration. As highlighted in this chapter, however, there is room for improvement in both the military and civilian trauma systems. The implementation of inclusive systems and patient outcomes vary dramatically across both sectors. Similarly, the interface between the military and civilian systems is neither structured nor systematic, limiting the exchange of best practices and lessons learned between the two systems.
Outcomes would be improved in both settings if learning processes were in place to encourage continuous bidirectional translation and diffusion of best practices. To this end, it is important to evaluate how well the trauma systems of both sectors function as learning systems. Chapter 3 outlines a framework for such an evaluation, and Chapters 4 through 7 analyze the strengths and gaps of the military and civilian trauma care systems according to this framework.
REFERENCES
AAOS (American Academy of Orthopaedic Surgeons). 2016. Extremity war injuries. http://www.aaos.org/research/advocacy/ewi/?ssopc=1 (accessed February 17, 2016).
ACS (American College of Surgeons). 2008. Regional trauma systems: Optimal elements, integration, and assessment, American College of Surgeons Committee on Trauma: Systems consultation guide. Chicago, IL: ACS.
ACS. 2014. Resources for optimal care of the injured patient. Chicago, IL: ACS.
ACS. 2015a. National Trauma Data Bank 2015: Annual report. Chicago, IL: ACS.
ACS. 2015b. Statement on trauma center designation based upon system need. http://bulletin.facs.org/2015/01/statement-on-trauma-center-designation-based-upon-system-need (accessed December 10, 2015).
Andersen, C. R., A. H. Schmidt, C. B. Fitzgerald, L. S. Tintle, M. M. Helgeson, L. R. Lehman, C. J. Davila, B. K. Potter, M. T. Burns, M. F. Swiontkowski, and C. J. Ficke. 2015. Extremity war injuries IX: Reducing disability within the military. Journal of the American Academy of Orthopaedic Surgeons 23(8):e13-e26.
Anderson, P., D. Chisholm, and D. C. Fuhr. 2009. Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcohol. The Lancet 373(9682):2234-2246.
ATS (American Trauma Society). 2016. Trauma center levels explained. http://www.amtrauma.org/?page=traumalevels (accessed April 18, 2016).
Bailey, J., M. A. Spott, G. P. Costanzo, J. R. Dunne, W. Dorlac, and B. J. Eastridge. 2012a. Joint Trauma System: Development, conceptual framework, and optimal elements. San Antonio, TX: Fort Sam Houston, U.S. Department of Defense, U.S. Army Institute for Surgical Research.
Bailey, J., S. Trexler, A. Murdock, and D. Hoyt. 2012b. Verification and regionalization of trauma systems: The impact of these efforts on trauma care in the United States. Surgical Clinics of North America 92(4):1009-1024, ix-x.
Bailey, J. A., J. J. Morrison, and T. E. Rasmussen. 2013. Military trauma system in Afghanistan: Lessons for civil systems? Current Opinion in Critical Care 19(6):569-577.
Baker, S. P. 1973. Injury control. In Preventive medicine and public health, 10th ed., edited by P. Sartwell. New York: Appleton-Century-Crofts. Pp. 987-1006.
Barnett, A. S., N. E. Wang, R. Sahni, R. Y. Hsia, J. S. Haukoos, E. D. Barton, J. F. Holmes, and C. D. Newgard. 2013. Variation in prehospital use and uptake of the national field triage decision scheme. Prehospital Emergency Care 17(2):135-148.
Blackbourne, L. H., D. G. Baer, B. J. Eastridge, F. K. Butler, J. C. Wenke, R. G. Hale, R. S. Kotwal, L. R. Brosch, V. S. Bebarta, M. M. Knudson, J. R. Ficke, D. Jenkins, and J. B. Holcomb. 2012. Military medical revolution: Military trauma system. Journal of the American Academy of Orthopaedic Surgeons 73(6 Suppl. 5):S388-S394.
Bosse, M. J., J. R. Ficke, and R. C. Andersen. 2012. Extremity war injuries: Current management and research priorities. Journal of the American Academy of Orthopaedic Surgeons 20(Suppl. 1):viii-x.
Branas, C. C., E. J. MacKenzie, J. C. Williams, C. W. Schwab, H. M. Teter, M. C. Flanigan, A. J. Blatt, and C. S. ReVelle. 2005. Access to trauma centers in the United States. Journal of the American Medical Association 293(21):2626-2633.
Bryant, R. A., M. Creamer, M. O’Donnell, D. Silove, and A. C. McFarlane. 2009. A study of the protective function of acute morphine administration on subsequent posttraumatic stress disorder. Biological Psychiatry 65(5):438-440.
Campion, E. M., C. Juillard, M. M. Knudson, R. Dicker, M. J. Cohen, R. Mackersie, A. R. Campbell, and R. A. Callcut. 2016. Reconsidering the resources needed for multiple casualty events: Lessons learned from the crash of Asiana Airlines flight 214. JAMA Surgery 151(6):512-517.
Cancio, L. C., T. E. Rasmussen, J. W. Cannon, and M. A. Dubick. 2015. The vital civilian–military link in combat casualty care research: Impact of attendance at scientific conferences. Journal of Trauma and Acute Care Surgery 79(4 Suppl. 2):S221-S226.
Cannon, J. W. 2016. Military–civilian exchange of knowledge and practices in trauma care. Paper commissioned by the Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector. nationalacademies.org/TraumaCare.
Carr, B. G. 2015. Leadership and accountability: The Emergency Care Coordination Center. Paper presented to the Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector, Meeting Two, July 23-24, Washington, DC.
Carter, A. B. 2012. Implementation of conference oversight requirements and delegation of conference approval authority. Memorandum. Washington, DC: U.S. Department of Defense.
CDC (U.S. Centers for Disease Control and Prevention). 2012. Guidelines for field triage of injured patients: Recommendations of the National Expert Panel on Field Triage, 2011. Morbidity and Mortality Weekly Report 61(1):1-20.
Champion, H. R., M. S. Mabee, and J. W. Meredith. 2006. The state of US trauma systems: Public perceptions versus reality—implications for US response to terrorism and mass casualty events. Journal of the American College of Surgeons 203(6):951-961.
Dawson, D. E. 2006. National Emergency Medical Services Information System (NEMSIS). Prehospital Emergency Care 10(3):314-316.
Dawson, D. E. 2015. Charge to the Institute of Medicine Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector. Paper presented to the Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector, Meeting One, May 18-19, Washington, DC.
DCBI (Dismounted Complex Blast Injury) Task Force. 2011. Dismounted complex blast injury. San Antonio, TX: Fort Sam Houston, Office of the Surgeon General.
Demetriades, D., B. Kimbrell, A. Salim, G. Velmahos, P. Rhee, C. Preston, G. Gruzinski, and L. Chan. 2005. Trauma deaths in a mature urban trauma system: Is “trimodal” distribution a valid concept? Journal of the American College of Surgeons 201(3):343-348.
DHA (Defense Health Agency). 2014. The Defense Health Agency: Reflections on our first year and future. Washington, DC: DHA.
DHB (Defense Health Board). 2015. Combat trauma lessons learned from military operations of 2001-2013. Falls Church, VA: DHB.
DHS (U.S. Department of Homeland Security). 2015. First responder guidance for improving survivability in improvised explosive device and/or active shooter incidents. Washington, DC: DHS.
DoD (U.S. Department of Defense). 2014. Military health system review: Final report to the Secretary of Defense. Washington, DC: DoD.
Eastman, A. B. 2010. Wherever the dart lands: Toward the ideal trauma system. Journal of the American College of Surgeons 211(2):153-168.
Eastman, A. B., E. J. MacKenzie, and A. B. Nathens. 2013. Sustaining a coordinated, regional approach to trauma and emergency care is critical to patient health care needs. Health Affairs 32(12):2091-2098.
Eastridge, B. J., D. Jenkins, S. Flaherty, H. Schiller, and J. B. Holcomb. 2006. Trauma system development in a theater of war: Experiences from Operation Iraqi Freedom and Operation Enduring Freedom. Journal of Trauma 61(6):1366-1372.
Eastridge, B. J., G. Costanzo, D. Jenkins, M. A. Spott, C. Wade, D. Greydanus, S. Flaherty, J. Rappold, J. Dunne, J. B. Holcomb, and L. H. Blackbourne. 2009. Impact of joint theater trauma system initiatives on battlefield injury outcomes. American Journal of Surgery 198(6):852-857.
Epley, E. E., R. M. Stewart, P. Love, D. Jenkins, G. M. Siegworth, T. W. Baskin, S. Flaherty, and R. Cocke. 2006. A regional medical operations center improves disaster response and inter-hospital trauma transfers. American Journal of Surgery 192(6):853-859.
Faul, M., M. M. Wald, E. E. Sullivent, S. M. Sasser, V. Kapil, E. B. Lerner, and R. C. Hunt. 2012. Large cost savings realized from the 2006 field triage guideline: Reduction in overtriage in U.S. trauma centers. Prehospital Emergency Care 16(2):222-229.
FICEMS (Federal Interagency Committee on Emergency Medical Services). 2011. National EMS assessment. Washington, DC: FICEMS.
FICEMS. 2013. Five-year strategic plan. Washington, DC: FICEMS.
Gage, A. M., N. Traven, F. P. Rivara, G. J. Jurkovich, and S. Arbabi. 2012. Compliance with Centers for Disease Control and Prevention field triage guidelines in an established trauma system. Journal of the American College of Surgeons 215(1):148-154.
GAO (U.S. Government Accountability Office). 2009. Warfighter support: Actions needed to improve visibility and coordination of DOD’s counter-improvised explosive device efforts. Washington, DC: GAO.
Gerhardt, R. T., A. P. Cap, R. Cestero, M. A. Dubick, J. Heiner, A. R. Koller, J. Lairet, A. R. McClinton, C. Manifold, R. Stewart, V. A. Convertino, and L. H. Blackbourne. 2013. The remote trauma outcomes research network: Rationale and methodology for the study of prolonged out-of-hospital transport intervals on trauma patient outcome. Journal of Trauma and Acute Care Surgery 75(2 Suppl. 2):S137-S141.
Glance, L. G., T. M. Osler, D. B. Mukamel, and A. W. Dick. 2012. Outcomes of adult trauma patients admitted to trauma centers in Pennsylvania, 2000-2009. Archives of Surgery 147(8):732-737.
Gomez, D., B. Haas, N. Ahmed, H. Tien, and A. Nathens. 2011. Disaster preparedness of Canadian trauma centres: The perspective of medical directors of trauma. Canadian Journal of Surgery 54(1):9-15.
Gross, K. 2015. Joint Trauma System. Paper presented to the Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector, Meeting One, May 18-19, Washington, DC.
Haas, B., G. J. Jurkovich, J. Wang, F. P. Rivara, E. J. MacKenzie, and A. B. Nathens. 2009. Survival advantage in trauma centers: Expeditious intervention or experience? Journal of the American College of Surgeons 208(1):28-36.
Haas, B., D. Gomez, B. Zagorski, T. A. Stukel, G. D. Rubenfeld, and A. B. Nathens. 2010. Survival of the fittest: The hidden cost of undertriage of major trauma. Journal of the American College of Surgeons 211(6):804-811.
Haddon, W. 1970. On the escape of tigers: An ecologic note. American Journal of Public Health 60(12):2229-2234.
Haddon, W. 1980. Options for the prevention of motor vehicle crash injury. Israeli Journal of Medical Sciences 16(1):45-68.
Haut, E. R., N. C. Mann, and R. S. Kotwal. 2016. Military Trauma Care’s Learning Health System: The importance of data-driven decision making. Paper commissioned by the Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector. nationalacademies.org/TraumaCare.
HHS (U.S. Department of Health and Human Services). 2009. Notices: Emergency Care Coordination Center. Federal Register 74(81, April 29):19561. https://www.gpo.gov/fdsys/pkg/FR-2009-04-29/html/E9-9719.htm (accessed February 17, 2016).
HHS. 2014. About the Emergency Care Coordination Center. http://www.phe.gov/eccc/about/Pages/default.aspx (accessed October 27, 2015).
Holbrook, T. L., M. R. Galarneau, J. L. Dye, K. Quinn, and A. L. Dougherty. 2010. Morphine use after combat injury in Iraq and post-traumatic stress disorder. New England Journal of Medicine 362(2):110-117.
Holcomb, J. B., D. J. del Junco, E. E. Fox, C. E. Wade, M. J. Cohen, M. A. Schreiber, L. H. Alarcon, Y. Bai, K. J. Brasel, and E. M. Bulger. 2013. The PRospective, Observational, Multicenter, Major Trauma Transfusion (PROMMTT) study: Comparative effectiveness of a time-varying treatment with competing risks. JAMA Surgery 148(2):127-136.
Hoyt, D. B. 2015a. American College of Surgeons’ perspective on charge to the committee. Paper presented to the Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector, Meeting One, May 18-19, Washington, DC.
Hoyt, D. B. 2015b. Leadership and accountability. Paper presented to the Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector, Meeting Two, July 23-24, Washington, DC.
Hoyt, D. B. 2015c. Looking forward—February 2015. Bulletin of the American College of Surgeons. http://bulletin.facs.org/2015/02/looking-forward-february-2015 (accessed October 28, 2015).
HRSA (Health Resources and Service Administration). 2006. Model trauma system planning and evaluation. Washington, DC: HHS.
IOM (Institute of Medicine). 2001. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
IOM. 2007a. Emergency care for children: Growing pains. Washington, DC: The National Academies Press.
IOM. 2007b. Emergency medical services: At the crossroads. Washington, DC: The National Academies Press.
IOM. 2007c. Hospital-based emergency care: At the breaking point. Washington, DC: The National Academies Press.
JTAPIC (Joint Trauma Analysis and Prevention of Injury in Combat). 2016. About JTAPIC. http://jtapic.amedd.army.mil/about.php (accessed May 2, 2016).
King, D. R., M. B. Patel, A. J. Feinstein, S. A. Earle, R. F. Topp, and K. G. Proctor. 2006. Simulation training for a mass casualty incident: Two-year experience at the Army Trauma Training Center. Journal of Trauma 61(4):943-948.
King, D. R., A. Larentzakis, and E. P. Ramly. 2015. Tourniquet use at the Boston Marathon bombing: Lost in translation. Journal of Trauma and Acute Care Surgery 78(3):594-599.
Klima, D. A., S. H. Seiler, J. B. Peterson, A. B. Christmas, J. M. Green, G. Fleming, M. H. Thomason, and R. F. Sing. 2012. Full-scale regional exercises: Closing the gaps in disaster preparedness. Journal of Trauma and Acute Care Surgery 73(3):592-597.
Knuth, T. E. 1996. The peacetime trauma experience of U.S. Army surgeons: Another call for collaborative training in civilian trauma centers. Military Medicine 161(3):137-142.
Kotwal, R. S., H. R. Montgomery, B. M. Kotwal, H. R. Champion, F. K. Butler Jr., R. L. Mabry, J. S. Cain, L. H. Blackbourne, K. K. Mechler, and J. B. Holcomb. 2011. Eliminating preventable death on the battlefield. Archives of Surgery 146(12):1350-1358.
Krajbich, I., M. Pinzer, B. Potter, and P. Stevens (Eds.). 2016. Atlas of amputations and limb deficiencies (4th ed.). Chicago, IL: American Academy of Orthopaedic Surgeons.
Kupas, D. F., E. Schenk, J. M. Sholl, and R. Kamin. 2015. Characteristics of statewide protocols for emergency medical services in the United States. Prehospital Emergency Care 19(2):292-301.
Lenhart, M. K., E. Savitsky, and B. Eastridge. 2012. Combat casualty care: Lessons learned from OEF and OIF. Falls Church, VA: Office of the Surgeon General, U.S. Department of the Army.
MacKenzie, E. J., F. P. Rivara, G. J. Jurkovich, A. B. Nathens, K. P. Frey, B. L. Egleston, D. S. Salkever, and D. O. Scharfstein. 2006. A national evaluation of the effect of trauma-center care on mortality. New England Journal of Medicine 354(4):366-378.
MacKenzie, E. J., S. Weir, F. P. Rivara, G. J. Jurkovich, A. B. Nathens, W. Wang, D. O. Scharfstein, and D. S. Salkever. 2010. The value of trauma center care. Journal of Trauma 69(1):1-10.
Mann, N. C., R. J. Mullins, E. J. MacKenzie, G. J. Jurkovich, and C. N. Mock. 1999. Systematic review of published evidence regarding trauma system effectiveness. Journal of Trauma 47(Suppl. 3):S25-S33.
Mears, G. D., D. Pratt, S. W. Glickman, J. H. Brice, L. T. Glickman, J. G. Cabanas, and C. B. Cairns. 2010. The North Carolina EMS data system: A comprehensive integrated emergency medical services quality improvement program. Prehospital Emergency Care 14(1):85-94.
MIEMSS (Maryland Institute for Emergency Medical Services Systems). 2016. State EMS Board and Statewide Emergency Medical Services Advisory Council. http://www.miemss.org/home/policy (accessed February 17, 2016).
Minei, J. P., R. H. Schmicker, J. D. Kerby, I. G. Stiell, M. A. Schreiber, E. Bulger, S. Tisherman, D. B. Hoyt, G. Nichol, and Resuscitation Outcome Consortium Investigators. 2010. Severe traumatic injury: Regional variation in incidence and outcome. Annals of Surgery 252(1):149-157.
Minei, J. P., T. C. Fabian, D. M. Guffey, C. D. Newgard, E. M. Bulger, K. J. Brasel, J. L. Sperry, and R. D. MacDonald. 2014. Increased trauma center volume is associated with improved survival after severe injury: Results of a Resuscitation Outcomes Consortium study. Annals of Surgery 260(3):456-464.
Mock, C., R. Quansah, R. Krishnan, C. Arreola-Risa, and F. Rivara. 2004. Strengthening the prevention and care of injuries worldwide. The Lancet 363(9427):2172-2179.
Moore, E. E., M. M. Knudson, C. W. Schwab, D. D. Trunkey, J. A. Johannigman, and J. B. Holcomb. 2007. Military–civilian collaboration in trauma care and the Senior Visiting Surgeon Program. New England Journal of Medicine 357(26):2723-2727.
Mullins, R. J. 1999. A historical perspective of trauma system development in the United States. Journal of Trauma 47(Suppl. 3):S8-S14.
Nakamura, Y., M. Daya, E. M. Bulger, M. Schreiber, R. Mackersie, R. Y. Hsia, N. C. Mann, J. F. Holmes, K. Staudenmayer, Z. Sturges, M. Liao, J. Haukoos, N. Kuppermann, E. D. Barton, C. D. Newgard, and WESTRN Investigators. 2012. Evaluating age in the field triage of injured persons. Annals of Emergency Medicine 60(3):335-345.
NASEMSO (National Association of State EMS Officials). 2014. National model EMS clinical guidelines. Falls Church, VA: NASEMSO.
Nathens, A. B., and R. V. Maier. 2001. The relationship between trauma center volume and outcome. Advances in Surgery 35:61-75.
Nathens, A. B., G. J. Jurkovich, P. Cummings, F. P. Rivara, and R. V. Maier. 2000. The effect of organized systems of trauma care on motor vehicle crash mortality. Journal of the American Medical Association 283(15):1990-1994.
Nathens, A. B., G. J. Jurkovich, E. J. MacKenzie, and F. P. Rivara. 2004. A resource-based assessment of trauma care in the United States. Journal of Trauma 56(1):173-178.
Nathens, A. B., H. G. Cryer, and J. Fildes. 2012. The American College of Surgeons Trauma Quality Improvement Program. Surgical Clinics of North America 92(2):441-454.
National League of Cities. 2013. Local government authority. http://www.nlc.org/buildskills-and-networks/resources/cities-101/city-powers/local-government-authority (accessed May 17, 2016).
Newgard, C. D., G. K. Sears, T. D. Rea, D. P. Davis, R. G. Pirrallo, C. W. Callaway, D. L. Atkins, I. G. Stiell, J. Christenson, J. P. Minei, C. R. Williams, and L. J. Morrison. 2008. The Resuscitation Outcomes Consortium Epistry-Trauma: Design, development, and implementation of a North American epidemiologic prehospital trauma registry. Resuscitation 78(2):170-178.
Newgard, C. D., K. Staudenmayer, R. Y. Hsia, N. C. Mann, E. M. Bulger, J. F. Holmes, R. Fleischman, K. Gorman, J. Haukoos, and K. J. McConnell. 2013. The cost of overtriage: More than one-third of low-risk injured patients were taken to major trauma centers. Health Affairs (Millwood) 32(9):1591-1599.
NHTSA (National Highway Traffic Safety Administration). 1996. EMS agenda for the future. Washington, DC: NHTSA.
NHTSA. 2000. Education agenda for the future: A systems approach. Washington, DC: NHTSA.
NHTSA. 2004. Trauma system agenda for the future. Washington, DC: NHTSA.
NHTSA. 2007. National EMS scope of practice model. Washington, DC: NHTSA.
NHTSA. 2011. The emergency medical services workforce agenda for the future. Washington, DC: NHTSA.
NRC (National Research Council). 1966. Accidental death and disability: The neglected disease of modern society. Washington, DC: National Academy Press.
Olson, L. M., and S. M. Bowman. 2012. EMS and trauma systems. In Injury research: Theories, methods, and approaches, edited by S. Baker and G. Li. New York: Springer. Pp. 569-581.
Patrick, P. 2015. Leadership and accountability. Paper presented to the Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector, Meeting Two, July 23-24, Washington, DC.
Pruitt, B. A., Jr., and T. E. Rasmussen. 2014. Vietnam (1972) to Afghanistan (2014): The state of military trauma care and research, past to present. Journal of Trauma and Acute Care Surgery 77(3 Suppl. 2):S57-S65.
PTSF (Pennsylvania Trauma Systems Foundation). 2016a. About us. http://www.ptsf.org/index.php/about-us (accessed February 25, 2016).
PTSF. 2016b. Expectations. http://www.ptsf.org/index.php/our-trauma-centers/center-standards (accessed February 25, 2016).
Rivara, F. P., A. B. Nathens, G. J. Jurkovich, and R. V. Maier. 2006. Do trauma centers have the capacity to respond to disasters? Journal of Trauma 61(4):949-953.
Robb, D. 2015. The why. Paper presented to the Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector, Meeting Two, July 23-24, Washington, DC.
Ross, M. C. 2010. Military nursing competencies. Nursing Clinics of North America 45(2):169-177.
Rotondo, M., T. Scalea, A. Rizzo, K. Martin, and J. Bailey. 2011. The United States military Joint Trauma System assessment: A report commissioned by the U.S. Central Command Surgeon, sponsored by Air Force Central Command, a strategic document to provide a platform for tactical development. Washington, DC: DoD.
Sampalis, J. S., R. Denis, P. Frechette, R. Brown, D. Fleiszer, and D. Mulder. 1997. Direct transport to tertiary trauma centers versus transfer from lower level facilities: Impact on mortality and morbidity among patients with major trauma. Journal of Trauma 43(2):288-295.
Sasser, S. M., R. C. Hunt, E. E. Sullivent, M. M. Wald, J. Mitchko, G. J. Jurkovich, M. C. Henry, J. P. Salomone, S. C. Wang, and R. L. Galli. 2009. Guidelines for field triage of injured patients. Recommendations of the National Expert Panel on Field Triage. Morbidity and Mortality Weekly Report Recommendations and Reports 58(RR-1):1-35.
Schwab, C. W. 2015. Winds of war: Enhancing civilian and military partnerships to assure readiness: White paper. Journal of the American College of Surgeons 221(2):235-254.
Shafi, S., A. B. Nathens, H. G. Cryer, M. R. Hemmila, M. D. Pasquale, D. E. Clark, M. Neal, S. Goble, J. W. Meredith, and J. J. Fildes. 2009a. The Trauma Quality Improvement Program of the American College of Surgeons Committee on Trauma. Journal of the American College of Surgeons 209(4):521-530.
Shafi, S., R. M. Stewart, A. B. Nathens, R. S. Friese, H. Frankel, and L. M. Gentilello. 2009b. Significant variations in mortality occur at similarly designated trauma centers. Archives of Surgery 144(1):64-68.
Shafi, S., S. Barnes, D. Nicewander, D. Ballard, A. B. Nathens, A. M. Ingraham, M. Hemmila, S. Goble, M. Neal, M. Pasquale, J. J. Fildes, and L. M. Gentilello. 2010. Health care reform at trauma centers—mortality, complications, and length of stay. Journal of Trauma 69(6):1367-1371.
Shafi, S., S. A. Barnes, N. Rayan, R. Kudyakov, M. Foreman, H. G. Cryer, H. B. Alam, W. Hoff, and J. Holcomb. 2014. Compliance with recommended care at trauma centers: Association with patient outcomes. Journal of the American College of Surgeons 219(2):189-198.
Shen, Y. C., R. Y. Hsia, and K. Kuzma. 2009. Understanding the risk factors of trauma center closures: Do financial pressure and community characteristics matter? Medical Care 47(9):968-978.
Sobrino, J., S. A. Barnes, N. Dahr, R. Kudyakov, C. Berryman, A. B. Nathens, M. R. Hemmila, M. Neal, and S. Shafi. 2013. Frequency of adoption of practice management guidelines at trauma centers. Proceedings (Baylor University Medical Center) 26(3):256-261.
Thompson, D. C., F. P. Rivara, and R. Thompson. 1999. Helmets for preventing head and facial injuries in bicyclists. Cochrane Database of Systematic Reviews 4(2):CD001855.
TraumaNet. 2013. Welcome to the Maryland Trauma Center Network. http://www.marylandtraumanet.com (accessed May 16, 2016).
Utter, G. H., R. V. Maier, F. P. Rivara, C. N. Mock, G. J. Jurkovich, and A. B. Nathens. 2006. Inclusive trauma systems: Do they improve triage or outcomes of the severely injured? Journal of Trauma 60(3):529-535.
Walker, P. M. 2013. Regional trauma plan worked, Waco hospital officials say. McClatchy DC, April 18. http://www.mcclatchydc.com/news/nation-world/national/article24748219.html (accessed May 16, 2016).
Zoroya, G. 2013. How the IED changed the U.S. military. USA Today, December 19. http://www.usatoday.com/story/news/nation/2013/12/18/ied-10-years-blast-woundsamputations/3803017 (accessed May 2, 2016).














































