
5
Reaching the Last Mile: Potential Opportunities to Improve Coordination and Communication Among Local, State, and Federal Agencies
PERSPECTIVES OF PUBLIC HEALTH DEPARTMENTS AT THE STATE AND LOCAL LEVELS
Michigan MCM Planning
Jennifer Lixey Terrill, health care and public health emergency management and policy specialist, Michigan Department of Health and Human Services, provided an overview of the state of Michigan’s emergency preparedness strategy, which comprises 83 counties and 45 local health departments divided into 8 regions with 100 emergency management programs.1 She provided a schematic of the state’s distribution strategy (see Figure 5-1).
Lixey Terrill explained that one warehouse serves as the receipt, storage, and staging (RSS) site for the state and is set to receive countermeasures, which are then shipped by ground or air to 45 local distribution nodes and to hospitals, with roughly 225 to 245 different shipment locations. Dispensing is a local function, with local health departments responsible for transporting the assets to dispensing locations (hospitals run alternate care facilities with support from emergency management and the health departments). She emphasized that local health departments have autonomy as to their dispensing operations (e.g., the use of open or closed points of dispensing [PODs]), with the state providing guidance and support.
___________________
1 Serviced by more than 190 hospitals, 435 long-term-care facilities, 800 life-support agencies, and 300 federally qualified health centers, migrant health centers, and rural health centers.

NOTE: CDC = Centers for Disease Control and Prevention; RSS = receipt, storage, and staging; SNS = Strategic National Stockpile.
SOURCE: Lixey Terrill presentation, February 5, 2016.
Lixey Terrill described some of the challenges in medical countermeasures (MCMs) distribution and dispensing faced by Michigan, including lack of resources as well as challenges with respect to its geography and climate. It can take 9 to 10 hours to ship countermeasures from state-identified warehouses to the most northwestern portions of the upper peninsula, even with favorable weather conditions.
Another set of major challenges in Michigan pertains to the feasibility and acceptability of POD operations, Lixey Terrill explained. She elaborated that feasibility issues surround establishing and staffing the dispensing sites to the extent that the necessary throughput can be achieved. Acceptability relates to the public’s willingness to bring their entire families to a government-staffed site to deal with large crowds, parking, traffic, security, and so forth: “We know that trust of government in general is going to be tough in an emergency.” Further concerns are that a predicted small percentage of people will actually come to the POD, then only a percentage of those who will actually take the medication, and a further diminishing percentage of those who will take a full 60-day course of antibiotics when they do not feel sick and do not even know that they have been exposed. Adding a three-dose vaccine with an annual booster to the regimen makes it an even harder sell to the public, according to Lixey Terrill.
Importance of Partnerships in Dealing with MCM Distribution and Dispensing Challenges
Lixey Terrill explained that partnerships have been crucial to the way that the state of Michigan deals with challenges of MCM distribution and dispensing. The Civil Air Patrol plays a critical role in addressing the state’s unique geographical challenges with respect to distribution. It is a national organization with the largest fleet of single-engine aircraft in the world, staffed by around 60,000 volunteer members nationwide and 1,400 members in the Michigan division2 whose services can be requested through the National Operations Center. The organization is emergency driven; its members are security and incident-command trained. During the H1N1 event, the Civil Air Patrol was deployed and was able to deliver six separate shipments of antivirals from Lansing (centrally located in the lower peninsula) to the upper peninsula in less than 8 hours. The Civil Air Patrol can also be mission-assigned through the Air Force, at which point it becomes a federal resource and thus paid (alleviating the need for the state to pay) and able to tap into a network of resources, including aircraft, from all over the country.
___________________
2 She noted that only 200 of those are actually pilots and the others are ground crews who could augment local operations in other contexts.
Fostering acceptability of POD operations, Lixey Terrill commented, also requires working with trusted public- and private-sector partners in the community to work within and leverage existing infrastructure and routine distribution systems, ideally supported by professionals who perform distribution and dispensing functions on a day-to-day basis. In Michigan, pharmacies and pharmacists are serving effectively in this role because they are already trusted community resources. More than 95 percent of Americans live within 5 miles of a pharmacy; everyone knows where their local pharmacies are located. She noted, however, that pharmacies can tend to be small and congestion may become an issue. Independent pharmacies do not have the huge storage capacity that large pharmacy chains have, with their own warehouses facilities and the ability to ship to local stores.
Michigan also has a vital and robust system of eight regional health care coalitions, each of which is supported by a medical director and health care coalition coordinators, which have monthly regional meetings and perform regular trainings and exercises. Partners include local public health agencies, private-sector partners, emergency management agencies, long-term-care facilities, dialysis centers, and hospitals. Many community-based organizations are involved; for example, Dearborn, Michigan, which is home to more Arab Americans than anywhere else outside the Middle East, has a group called Access, sponsored by the Henry Ford Health System. As part of the health care coalition, the organization is one of the largest closed POD partners that has unique access to that community. Muskegon, Michigan, has a mass dispensing plan that includes using all the physician offices in the county as closed PODs that works well for its jurisdiction, but is not a “one-stop shop”—they also have other open PODs in federally qualified health centers that participate in the health care coalitions. During an emergency response, the state’s Medical Coordination Center works with partners up to the state level.
Texas MCM Planning
Poole offered the state’s perspective on MCMs. The size of Texas poses a challenge in and of itself, with 254 counties divided into 8 health service regions, 45 local health departments, and 20 additional Cities Readiness Initiative jurisdictions coordinated with county emergency managers. The state of Texas has a multiple-point delivery system for MCMs (see Figure 5-2). The Centers for Disease Control and Prevention (CDC) ships to 18 RSS warehouse sites across the state (operated in partnership with 18 private vendors), at which point the state is responsible for distributing to closed PODs, open PODs, and local jurisdictions. This number of RSS sites is necessary due to the size of the state and the time sensitivity of many Strategic National Stockpile (SNS) products.
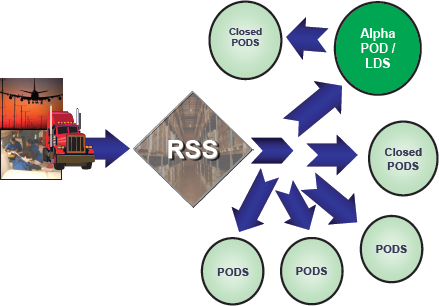
NOTE: LDS = local distribution site; POD = point of dispensing; RSS = receipt, storage, and staging.
SOURCE: Poole presentation, February 5, 2016.
Poole explained that the state’s strategy for distribution comprises around 75 percent open PODs, 20 percent closed PODs, and 5 percent mobile PODs (e.g., school buses, Meals on Wheels™). The “alpha POD” is the point at which responsibility is transferred to the local level for distribution to smaller closed PODs. However, there are direct delivery drops whereby assets are shipped directly from the RSS to each of the open PODs as well as larger closed PODs (including hospitals) in certain regions. Some of the smaller closed PODs, such as nursing homes, depend on local health departments to set up an alpha POD to facilitate distribution (usually by pick up). But Poole noted that Texas considers distribution a state responsibility, so the system tries to avoid placing too much of the responsibility for distribution on the local level to allow its primary focus to be on dispensing. Transportation is variable depending on the specific setting, but the first stage is typically making the resources available for transport at the RSS site, followed by contractors with the Department of State Health Services, and then the state operations center or emergency management (which has many contracts, but is subject to more delays).
Engagement with private partners has been one of the state’s biggest successes, according to Poole, who noted that H1N1 exposed the fact that public health cannot provide dispensing operations on its own and must depend on private partners who perform these types of operations on a daily basis: “we need to be flexible and our system needs to be able to pick and choose what will work best given whatever the scenario we are facing.” For instance, Texas has statewide closed PODs with large grocery store chains that cover 200,000 people across the state.
Poole highlighted the success of RE-PLAN, based out of the University of North Texas Center for Computational Epidemiology and Response Analysis, which is aimed at improving the balance between distribution and dispensing (resources that take on distribution take away resources from dispensing). RE-PLAN is a modeling software that can be used for dispensing operations, identifying POD locations, and helping RSS sites to increase their number of direct deliveries. The program can automatically select POD sites using heads of households, and provides visual information regarding location, transportation routing, and traffic information (see Figure 5-3).
Poole noted that one of the benefits of RE-PLAN is helping new SNS program coordinators to visualize their jurisdictions’ challenges and vulnerabilities, allowing them to optimize POD locations and incorporate public
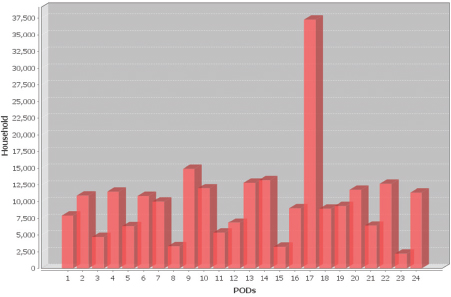
SOURCE: Poole presentation, February 5, 2016.
transport options into planning. So far, the program has been used in the Dallas-Fort Worth region, and since 2010, the number of direct delivery sites in Texas has decreased from more than 3,000 to fewer than 2,000, improving the distribution network and freeing available resources for other purposes. See Box 5-1 for a description of the differences between rural and urban MCM planning in Texas after distribution is completed at the state level.
New York City MCM Planning
David Starr is the director of the Countermeasures Response Unit, which is situated within the Office of Emergency Preparedness at the New York City Department of Health and Mental Hygiene. The unit is responsible for all mass prophylaxis and MCM planning in New York City. See Box 5-2 for a description of New York City’s 2014 mass prophylaxis exercise.
Starr explained that one of the key goals of the exercise was to test the ability to mobilize staff, truck assets, and warehouse, and then set up PODs as fast as possible. But another aim was to beat the delivery time lines set by the CDC Division for Strategic National Stockpile (DSNS), and the exercise demonstrated that those time lines could leave PODs waiting for hours to receive their medications after setup was complete: in this context CDC was in fact a rate limiter. When provided with data proving that this was the case, CDC responded appropriately, and Starr’s unit and CDC have been working together to mitigate the effects of this delay by forward-deploying assets into the unit’s warehouse in order to dispense to large numbers of the public without delays at the PODs. Starr cited this as an example of collaboration that is a model for the interaction between the local, state, and federal levels.
The postexercise participant survey had an extremely high response rate (89 percent; 763 of 860 field staff), and confirmed that 91 percent of participants were not aware of the date of the exercise. The unit has an extensive training program for POD leadership staff in the field (a full day of operations training every other year), the value of which was confirmed when 80 percent of participants stated that training helped them perform. The survey responses further confirmed ability to respond (86 percent were able to report to the POD on time) and willingness to respond (92 percent stated that they would have responded in their role if it had been an actual event).
Last-Mile Successes and Challenges Demonstrated by RAMPEx
One of the last-mile successes demonstrated by RAMPEx (Rapid Activation for Mass Prophylaxis Exercise) was the preassignment of
leadership staff to POD sites. Starr noted that a primary reason that New York City is so vulnerable to bioterrorist attack is due in large part because of its density, so they tried to use the fact that the vast majority of participating staff live in the city to their advantage. Leadership staff (in particular) are preassigned to the 165 POD sites around the city, which are distributed according to models of population density. People are assigned according to distances on the street network (as opposed to “as the bird flies” distance lines), with a significant number of the people assigned to staff POD sites very close to their homes. Although the system tries to equalize assignments, some people may have to travel farther to fulfill specific positions in certain PODs. For instance, all leadership staff are assigned to PODs in the city regardless of where they live (see Figure 5-4).
Around 47 percent of the leadership team are assigned to POD sites 1 mile or less from their homes, with around 70 percent within 2 miles or less. This type of preassignment allows leadership staff to be provided with detailed site manuals (including, for instance, floorplans specific to their assigned site), as well as a detailed POD Procedure Guide giving step-by-step directions for setting up and operating a POD.
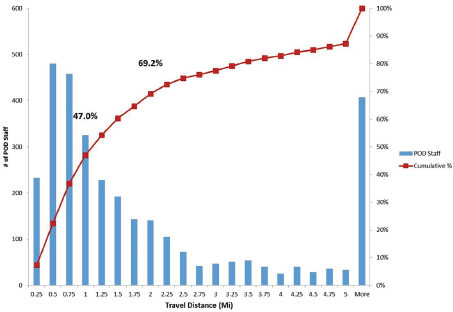
SOURCE: Starr presentation, February 5, 2016.
Around half of the general staff in the city are also assigned to PODs, with the aim of no staff having to leave their borough (except Brooklyn and Queens) or cross a bridge (see Figure 5-5).
Starr explained that this strategy resolves multiple issues because “You have a neighborhood serving a neighborhood. You have a community serving a community. Your chances of staffing your site with people who come from the neighborhoods, speak the languages, and understand the culture of that neighborhood are extremely high.”
Starr emphasized that this type of data and analysis are particularly useful when dealing with city governments, for example, having health department staff mandatorily assigned to PODs. This was difficult, even though the city incident management system mandates this as a core competency for the unit to be able to execute these operations. Assignment of staff had not become a focal issue until shelter understaffing proved a problem during Hurricanes Irene and Sandy, and the commissioner ordered health department staff to respond to that (not their core mission), but not to POD assignment, which is in fact their core mission. When pointed out, this contradiction facilitated mandatory assignment and, more recently, mandatory training of staff.
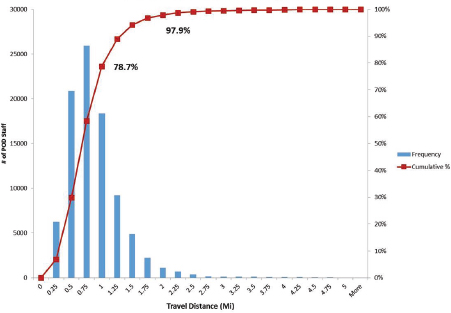
SOURCE: Starr presentation, February 5, 2016.
A challenge that Starr identified is the need for more quality leadership staff to be assigned as close to their homes as general staff are. Nominally, there are three leadership staff assigned to every position in about 32 of the 165 PODs. But there is a battle between quantity and quality, in terms of having people assigned appropriately in terms of skill levels and geography to enable easy response.
Starr highlighted a key point of contention in Executive Order 13527. Research from the Bureau of Labor indicates that there are roughly 30,000 federal workers working in New York City, though about 9,000 live in New Jersey; that still leaves 21,000 federal workers living in New York City and New York State. In several venues, New York City made the request for access to federal staff living in the local area who want to participate in the POD Responder Program and support PODs in their neighborhoods, most recently as a key element in the Federal Emergency Management Agency (FEMA) Region II federal MCM plan as well as to various federal executive boards, but to no avail, despite advocacy from DSNS. Starr characterized this as an appalling gap, and the FEMA New York City MCM plan remains in “draft” status because of the inability to fulfill the principal request in the document.
Starr outlined further last-mile successes with regard to emergency medical logistics planning on the dispensing side.3 The Countermeasures Response Unit recently finalized pre-scripted mission requests (PSMRs) that detail the various elements of the SNS request,4 which are now on file at the City Office of Emergency Management Watch Command so that when leadership chooses a Phase I response, the appropriate request on file can be pulled immediately. It defines the exact quantities of each type of antibiotic (doxycycline and ciprofloxacin) that matches the screening algorithm in the field and what public messaging guidelines should be used. The ratios of antibiotics that go to each warehouse differ depending on the scenario, because they will be serving different numbers of PODs in the second wave after the Phase 1 response is complete.
Another success factor has been the development of predefined turn-by-turn routing in the form of a routing book developed by New York City Department of Transportation staff that will be provided to the drivers and the law enforcement escort officers. It covers a multitude of potential routes (with 13-foot clearance height) in great detail, including the exact entrance to the POD. The POD site manual shows the primary receiving area and the
___________________
3 The unit is responsible for receiving supplies from SNS distribution as well as dispensing them, unlike many jurisdictions in which the state is responsible for the first part and the locality for the other.
4 These PSMRs have been reviewed by City and State Offices of Emergency Management, New York State Department of Health, FEMA, the Department of Health and Human Services (HHS), and CDC.
path into the POD and the pharmacy room. Starr noted that professional transportation vendors do a great job of routing on a day-to-day basis on routes that they know, but they could not be depended on to develop routing to match every response scenario.
Starr reported that after a 2-year process, a Memorandum of Understanding has been signed with HHS to work with the General Services Administration in New York City to dispense MCMs to federal emergency response officials. This is not a traditional federal closed POD; it is only for mission-essential federal personnel, because other employees could come to the public POD network.
Greg Burel commended New York City’s efforts and ability to demonstrate, through its RAMPEx exercise, that it is a suitable candidate for predeployment of materials, sharing that the risk-based approach has been beneficial; a new effort is being made to identify specific at-risk areas and work with them on more in-depth planning regarding dispensation of MCMs.
However, he noted that in many cases SNS materials arrive long before localities are prepared to dispense them, which is a big concern. He suggested that hard-line logistics consulting and discussions with those localities would be a way to address this.
He also noted that many of the issues at hand, particularly upstream components such as the development of MCMs, are not directly under the SNS’s control, although they do have some degree of engagement. Regarding the last mile, Burel noted that the SNS does not want to hand materials off to local jurisdictions without support or guidance, but commented: “We also recognize that we don’t have command and control from the time we turn it over to the state. Each one has to handle things differently in the way that makes sense in their particular area for their particular population and needs.”
CDC STRATEGIES FOR ENSURING READINESS AT THE LAST MILE
Christine Kosmos, director, CDC Division of State and Local Readiness (DSLR), focused on CDC strategies for ensuring preparedness at the “last mile”; specifically, she explored what CDC is doing to ensure operational readiness at the state and local levels to improve capabilities within state and local public health departments (see Box 5-3).
Public Health Emergency Preparedness Program
Kosmos explained that CDC embarked on a very deliberate process to describe the contributions of the Public Health Emergency Prepared-
ness (PHEP) Program to state and local public health, with the intent to frame the program to better understand both its original intent and ways to move forward. The process generated a set of key messages for understanding the conversation about medical countermeasure readiness. First, since 9/11, the PHEP Program has created the new domain of “public health emergency management” experts, which differs from traditional emergency management in that it views emergency management through a public health lens. The second key message is to support the public health capabilities that are necessary for state and local public health by framing those into a doctrine of 15 public health preparedness capabilities published in 2012 (see Box 5-4).
The CDC PHEP Program is also intended to ensure response readiness within the nation’s public health system for public health emergencies and disasters, with the broader aim of ensuring the health security of our nation and our communities. Together with the SNS, the program further seeks to ensure a nationwide system capable of rapidly distributing and dispensing lifesaving medications and emergency medical supplies to the public during emergency responses.
After developing the PHEP Program capabilities, Kosmos explained that CDC gauged the progress made since 9/11, which she characterized as an “eye opener” for state and local public health that helped to expose gaps in terms of emergency preparedness. For example, prior to 9/11, the
capabilities for storage, delivery, dispensation, and distribution were practically nonexistent, but reflecting on a review of capabilities in 2012, Kosmos observed “post-9/11, 2012 across the board yes, yes, yes, and yes. Yes, we have warehousing capability. Yes, we have plans. Yes, we have people. Those people are trained. They are prepared and they can do it.”
Development of the CDC Medical Countermeasures Readiness Review Process and Tool
Kosmos explained that DSLR has worked closely and productively with DSNS from the beginning in efforts to build capabilities for state and local readiness for MCM planning; today, the DSLR continues to work with the DSNS to advance the work of state and local public health. Moving forward will require the flexibility to adapt to the changes of the ever-evolving
discipline of emergency preparedness and response, so they looked to a wide range of stakeholders, including state and local experts, for input. She quoted a former SNS director as suggesting a focus on doing what they say they can do: “Can we really execute the plans that are on our shelves?”
To continue improving the process, DSLR developed a new evidence-based tool, called the Medical Countermeasure Operational Readiness Review (ORR), in consultation with subject-matter experts for evaluating operational readiness at the state and local levels. It was designed with extensive input from state and local partners in order to determine the specific capabilities to focus on, to understand the targets, and to establish where state and local public health needs to be going forward. It evaluates evidence of a jurisdiction’s operational ability to execute components of preparedness (e.g., staff, mobilization ability, associated throughputs, gathering data and meeting objectives with data, and ability to evaluate the capacity to execute), rather than merely asking jurisdictions for a plan.
Kosmos explained that the tool has now been piloted, tested, and rigorously evaluated. At the current stage in the process, staff are evaluating every state, every directly funded city,5 every U.S. territory, and selected local municipalities in each state to evaluate their levels of operational readiness. By the end of 2016, they will have evaluated more than 400 states, directly funded cities, and local jurisdictions, providing a useful snapshot of the levels of capability within state and local public health. To date, more than $300 million has been invested in MCM planning since the beginning of the project. “We have to be able to answer the question of what the level of readiness in state and local public health is; we have to be able to answer that question in a very scientific evidence-based way. . . . It has got to be a deliberative process.”
Kosmos described how the tool itself contains 90 planning and operational elements across 8 public health preparedness capabilities, with level of readiness status (1 = early, 2 = intermediate, 3 = established, and 4 = advanced) assessed within each of those 8 domains, based on criteria outlined in CDC’s preparedness capability standards. The planning section is used for analyzing the content of the plans and evaluating the completeness of those plans. A companion section focuses on evidence of their ability to execute. The PHEP Program goal is that by 2022, all 62 PHEP jurisdictions will achieve a status of “established” for planning and operational elements.
Baseline data reveal that on the planning side, many state and local partners are assessed at 3/4 (a score at which the metric is considered complete or achieved) on the planning side and 2/4 or 3/4 on the execution side. Kosmos explained that this provides very granular specific information
___________________
5 Directly funded cities include Chicago, Los Angeles, New York City, and Washington, DC.
about where we need to drill down, exposing the gaps and vulnerabilities in state and local public health in a way that facilitates the design of appropriate technical assistance strategies.
State and local partners completed an anonymous survey about the process; 89 percent of the responses were overwhelmingly supportive of how it will move the nation forward in MCM readiness. Kosmos construed this as very positive, because the process is aimed not only at improving the level of readiness in state and local public health, but also at ensuring that the program is accountable for the dollars that they have invested in state and local public health.
Petersen noted that his state has carried out more than 60 evaluations for the preparedness programs and operational activities. Though it is not a CDC requirement, Tennessee requires each jurisdiction to carry out exercises, including large-scale exercises every 5 years per grant requirement. They evaluate how often they can use their redundant communication systems, how often they can activate their emergency operations centers effectively, and so forth; those exercises are documented appropriately with after-action reports and improvement plans developed to enhance the system going forward. Multiple metrics are captured, including accuracy. Furthermore, there has been activity with the CDC ORR tool that he attributed to raising the bar and setting higher goals for state and local agencies. He commented that state and local public health departments are not funded to the degree that they can carry out preparedness functions without support (they have many responsibilities other than just dispensing and distribution), so they must work with private-sector partners, the health care community, and others to be able to have force multipliers to ensure preparedness.
MCM CHALLENGES FROM THE STATE AND LOCAL PERSPECTIVES
Poole explained some of the challenges that Texas faces. Acquiring and maintaining local and state caches is problematic due to rotation issues that drain resources. Time and space are also barriers, due to the size of the state and the amount of storage needed.
Poole noted that local SNS program staff turnover continues to be a challenge; there is a 10-35 percent turnover rate for SNS coordinators in Texas’ 45 local health jurisdictions (due to promotion or transfers out), so it can be difficult to train new coordinators and bring them up to speed as quickly as possible. New and improved training manuals and informational materials incorporating the wealth of available information from other states and agencies are being developed to address this.
Exercising with the private partners (closed PODs and RSS sites) in Texas has been a challenge, according to Poole, due to the volume of agree-
ments and number of partners that need to be coordinated, but efforts are under way to truly test the state’s SNS system. To enable a tighter delivery time frame at each RSS, Poole suggested that it would be very beneficial to have site-specific estimates regarding shipment volumes and timing for each of the eight regions, which can be used to help private vendors to be better prepared.
Gore, from Dallas, maintained that key challenges derive from the lack of clarity with regard to the time frame of the formal request process for the SNS, coupled with distribution uncertainty. From the local perspective, once a threat or trigger is identified and the request for SNS assets is activated, it is unclear what concrete steps and formal processes are required before the trucks are on the road. In terms of long-term planning, her concern is not how quickly she can set up the POD, but the subsequent delay in when the medicines will actually arrive.
Noting that all programs, regardless of size, are subject to the same program requirements, documentation, and level of response, Gore suggested that realistic versus worst-case planning should be factored into those requirements. She emphasized that the expectations and priorities of rural versus urban jurisdictions are very different: “When I was in Brown County, it was very much the understanding that we were on our own and that even if distribution was happening, it was going to the big jurisdictions first. And if I wanted the drugs, I was going to have to drive to go get them regardless of what on paper was the plan.”
Another issue for Gore is the modularization of the SNS; a push pack can cover about 500,000 people, which is sufficient for smaller jurisdictions, but in Dallas County, it will only cover first responders. Furthermore, push packs contain a range of items, and she suggested that it would be much better to be able to automatically activate vendor inventory of the specific item needed. Citing the example of the H1N1 vaccine that was not available when demand was high and they were ready to dispense, she reiterated that dispensing is not where the problem will be, it will be how fast the MCMs come out.
Starr highlighted a barrier that pertains to the process of requesting supplies from the SNS due to confusion surrounding the process. He suggested the possibility of integrating the request exercises with SNS’s ongoing annual exercises to help address this. A related issue raised by Starr is the discovery that SNS would not be able to fulfill exact requests being made, due to a decision made years ago by the Public Health Emergency Medical Countermeasures Enterprise (PHEMCE) regarding the ratio of antibiotics held in the SNS stockpile. Starr criticized this decision as being made without local-level input, despite its significant impact on local-level operations and planning. The SNS would be able to provide the overall quantity of requested antibiotics, but could not fulfill the specific ratio requested (i.e.,
85 percent doxycycline and 15 percent ciprofloxacin).6 The quantity would only be available in the ratios held in the SNS, which is 50:50. Starr contended that receiving a 50:50 ratio regardless of the request,
we are going to be encountering bottlenecks and difficulties from the very beginning, from the time it hits the warehouse when we are not prepared to receive it. We cannot build the orders that we prebuilt and that we pre-waived into our warehouse management system. And then we have to start making allocation decisions based on no guidance whatsoever. . . . This is an upstream decision that has deep and critical downstream consequences.
For instance, people will assume that they are being mistreated when different people are receiving different antibiotics (this was borne out in the 2001 anthrax response). Equitability of response is a primary concern for Starr, who noted that it cannot be alleviated with risk messaging; it must be evident in the response itself.7 Gore concurred that supply uncertainty is an issue because most jurisdictions have a doxycycline-dominated algorithm that is not compatible with the PHEMCE-mandated 50:50 ratio of doxycycline to ciprofloxacin.8
Lack of funding is an ongoing problem, as is lack of visibility on the supply chain inbound to warehouses from the SNS. This is particularly problematic when multiple requests are going to multiple warehouses for multiple jurisdictions in a congested region: what is being shipped, where the trucks are, what is on each truck, etc. Starr suggested that some kind of electronic portal with the ability to pull data could be operationalized in the field.
POTENTIAL OPPORTUNITY FOR ALTERNATIVE DISTRIBUTION AND DISPENSING MODELS
Sosin remarked that identifying unique approaches to distribution and dispensing models that leverage existing resources is important, but reminded the group that the work involved is more than just, for example, a suggestion to do user-managed inventory. Strains of the volume of material that can be held in the stockpile should be taken into account. He commented:
___________________
6 Like most jurisdictions, New York City has a doxycycline-dominant screening algorithm.
7 He cited surveys of pandemic response demonstrating that the people in the neighborhoods of lower socioeconomic levels believe that they are going to be treated last if they get treated at all.
8 A related concern is the availability of amoxicillin for people who are counterindicated for both ciprofloxacin and doxycycline. Currently, the plan is to send people to pharmacies, but the mechanism for funding that is unclear.
To the point that we need to have more options, we need to understand what our options are and the scenarios within which they work. We must consider that every unique and creative solution to distribution and stockpiling will have constraints, and we need to effectively work to assure we understand them.
Engaging the Private Sector in Distribution
Michael Loehr, chief of emergency preparedness and response, Washington State Department of Health, drew on his experiences in working with issues associated with the response to and recovery from biological disasters to suggest a set of distribution strategies that could be applied to the MCM enterprise. Not only are the issues highly complex, but their cascading effects are linked to both the hazards and the decisions made surrounding a response. This exposes the limitations of the current planning and thinking around the development of MCM distribution capability and dispensing. He cast into doubt the current ability to achieve the core objectives of a large-scale MCM response: making medications available to all who need them in any part of the jurisdiction, with sufficient speed and accuracy to minimize mortality and morbidity, and in a manner that retains the public’s trust and confidence. “The public is an unwritten responder in our plans. We assume they are going to do certain things but in reality, we don’t know.” Loehr called for three areas of focus to improve the chances of being able to achieve those objectives in the future.
The first is rethinking how the SNS distribution process works, Loehr said, from storage to dissemination to the public during an incident—to remove all inefficiencies from the system and add value by improving the safety and accuracy of products at each step in the process. The vast supply of MCMs must pass through the extraordinarily tight bottleneck of a government-run, government-designed, and single-purpose distribution process. During a large-scale, rapidly moving biological disaster, Loehr contended, a government-centric approach to distribution and dispensing was destined to fail. So the State of Washington partnered with pharmacies, which medicate 60 percent of the population on a daily basis, to use their existing capacity; all 700 pharmacies in the State of Washington have been incorporated into the statewide MCM-dispensing plan as PODs. See Box 5-5 for another example of collaboration between pharmacies and state health officials.
With state health departments still hampered by recession and reduced capacity, Loehr suggested turning to large private-sector health care systems9
___________________
9 One of these systems touches 10 percent of the entire state population, 700,000 people, between members and employees.
with large-scale capacity for distribution and dispensing. They approached the private-sector health care systems and pharmacies to build dispensing capacity; they stressed the need to learn from the problems of H1N1 and to inculcate central decision making, organization, and a coordinated approach to priorities to protect the people. Loehr said the approach would thus focus on sustaining the private sector’s critical infrastructure for dispensing as well as maintaining the public’s trust. Incorporating private-sector expertise has led to a dramatic increase in capacity over the past several years. He acknowledged that there is certainly a role for state and local governments in distribution, particularly among rural populations without pharmacy capacity in the area, but that the government’s role should be closely measured to ensure that it is only adding value.
The second area of focus Loehr highlighted is the need for “quick-strike” capabilities such that medicines are being consumed by people within hours of the decision being made to make them available. Loehr endorsed the idea of forward deployment to cities who have proven ability to rapidly open public PODs quicker than the SNS medications can arrive, but argued that the same should also be granted to jurisdictions that have any capability that is sufficient to meet the needs of a significant portion of the public. He cited two reasons for this. First, public PODs in some states and local jurisdictions do not provide sufficient capacity and are a strategy geared toward specific populations who cannot get medications in any other way; Loehr predicted that many states will recognize the need to involve the private sector in this part of dispensing.
Second, a bioevent in an urban area is not going to be restricted to the city; quick-strike capabilities must be activated across city and county boundaries. Furthermore, he argued that RSS sites are redundant for jurisdictions that rely on pharmacies and health care systems as the backbone of distribution and dispensing capabilities. Thus, Loehr suggested forward-deploying medications directly into the supply chain to improve efficiency, bypassing the RSS except for a small portion for quickly deploying to a few public PODs. A commitment to establishing quick-strike capability requires the willingness to cede control to private-sector partners when they say “just give us the drugs and get out of the way.”
The third area of focus Loehr mentioned is to invest in decision making, which represents a critical gap across the country. There are many different types of dispensing modalities, but there is limited knowledge of their relative efficiencies and whether they are complementary or conflicting.10 Loehr said planning needs to be refined despite the many unanswered questions going forward, but he suggested the development, modeling, and testing of decision tools at the national level to give leadership “decision space” with justification for various options and a better understanding of how to make controversial decisions during rare but high-consequence events. According to Loehr,
We should rethink the entire SNS distribution model from the standpoint of logistical efficiency. . . . There is a lot of talk about that last mile and for me, it’s really that last 10 feet. It’s going to be the private sector that makes a difference. It’s not government. We don’t have an effect on the
___________________
10 Loehr queried: “Should the size of incident affect which dispensing and distribution strategy we mobilize? If so, how? When should we widely distribute our medications across a wide range of modalities but when should we concentrate them on just a select few? Are some modalities applicable in only certain scenarios, like closed pods? Very controversial in certain scenarios. Are some modalities conflicting with others? Did they slow us down during certain events?”
last mile other than the decisions we make. And I think the decisions at the federal level regarding how distribution happens dramatically impacts whether we can succeed in that last mile.
Noting that pharmacies are often overwhelmed during regular operations, O’Toole questioned their ability to deliver as a POD during a biological event in which MCMs need to be delivered very quickly to very large numbers of people.
Loehr countered that there are no real-world examples demonstrating the success of either a government-managed or private-sector-managed approaches, but there are reasons for optimism about pharmacies’ capacities to deliver. The public POD strategy is a government model that relies on either government or volunteer staffing (which is limited). So many PODs would have to be set up in order to instill public confidence that the lines will be short enough to move people through in a rapid amount of time; with parking capacity as a critical limiting factor. Pharmacies are everywhere, often in large shopping centers, and they are already medicating a large proportion of the population every day. They have demonstrated expertise and skills in inventory management, distribution, and dispensation. He stressed that the key is recognizing the full available capacity by partnering with everyone, including private-sector organizations, to contribute their capacities to protect the community.
Engaging Large Employers in Dispensation of MCMs at the Local Level
Meg Nash, vice president, Consulting Services, Bio-Defense Network, emphasized the challenge of engaging large national-level employers to participate under the Public Readiness and Emergency Preparedness (PREP) Act to alleviate the burden on public health; it is difficult to get a large employer to engage and commit to participate. She explained that a primary barrier is the burden (from the employers’ perspectives) of entering into an agreement at jurisdictional level in all of their locations. If those employers are resistant to these types of jurisdiction-by-jurisdiction-level agreements, she questioned whether there is a way to quantify their participation in the distribution of MCMs under the PREP Act. For example, she suggested the possibility of providing a more generic agreement than jurisdiction-level MOUs that would still allow employers to be covered under the PREP Act for their liability.
Sherman replied that the declaration so far has covered two different scenarios: situations that involve any type of federal agreement and situations involving emergency response mass dispensing. The language was purposefully broad to cover a range of situations whereby the jurisdiction has the authority to respond in any declared emergency; there is not a specific arrangement required. The statutes can only point to conditions thought to
be helpful to people and suggest why they should be covered. For example, if a person sues a retailer who claims protection under the PREP Act, ultimately it is up to the presiding judge to make that decision. That said, Sherman sympathized with why these employers are looking for specific documentation and highlighted this as an issue to address going forward.
Burel commented that it would be difficult for a big-box retailer, for example, to successfully assist in a dispensing operation in the absence of a state- or local-level agreement: “I don’t think you would want Best Buy acting independently to try to distribute countermeasures without some agreement with you about how you were going to do that with them.” Sherman noted that any federal arrangement could be pointed to as the basis for coverage regardless of the relationship to the authority having jurisdiction to respond.
Gore elaborated that from the employers’ perspective, the primary issue does not seem to be liability, but rather the desire for a national-level paper document agreement; retailers, communications companies, banks, and corporations generally refuse to cooperate with individual jurisdiction-specific agreements. Sherman commented that this gives rise to a tension because every state and locality has its own requirements, prescriptions, authorities, and actors. Thus, it became very difficult to create a national-level agreement that is generic enough to be effective while balancing those competing needs.
Nash reiterated that a national-level agreement, whereby the employer agrees to participate and gives its locations the authority to participate, would simplify things significantly at the local level. For instance, her department has a national-level agreement with a very large grocery store chain, but they still have to negotiate MOUs individually in each jurisdiction (a huge burden for the employer).
O’Toole concluded the exchange by commenting: “I think [this] is a very important issue that is quite familiar to many people in the room in different versions and guises. It illustrates the complexity of actually administering a big federal program across all of the different public health jurisdictions in the country. It is another illustration of the brilliance and the complexity of the federal–state arrangement that is the United States of America when it comes to health authorities.”
POTENTIAL OPPORTUNITY FOR IMPROVING TRANSPARENCY AND COORDINATION AMONG LOCAL, STATE, AND FEDERAL AGENCIES
From the local perspective, Gore suggested several ways to move forward with the SNS. The first is exercising the whole SNS process from beginning to end: from identification of a bioterrorism threat that triggers
the request, to the activation and mobilization of the asset, to the distribution and then the dispensing. Gore cautioned that expanding the scope and mission of the SNS should be done with an awareness of local impact. That is, a fast response to emerging threats concerns not just the countermeasure itself, but the local capacity to identify said threat (testing and confirmation rule out or require lab capabilities, for example).
Transparency Around SNS Inventory and Planning Assumptions
Gore emphasized that better information sharing with the local level is crucial: better clarity regarding how much of each individual item is needed and in what form, and being aware of what else is in the stockpile beyond ciprofloxacin and doxycycline in pill form. Much of what she knows about other stockpile contents she learned from her own research, not directly from DSNS. Access to these kinds of information is crucial for informing local-level operations and planning. Fri similarly contended that DSNS leadership needs to make its structure more visible to people working in public health and the commercial supply chain.
Gore raised the issue of whether planning assumptions regarding delivery are standardized across the board for the products in the SNS (e.g., why a certain product is a one-off, versus coming through traditional routes of distribution). She suggested better informing local agencies about these types of assumptions would allow for more effective planning and clinical guidance, noting that the concept of operations (CONOPS) framework idea would be ideal, especially if it were tied into a mechanism among local jurisdictions as well as between the local, state, and federal levels.
Starr also called for increasing visibility into the SNS at the local level:
Smoothing that interface when it comes so that not only do we know what is in it, but they know what we want and we know what is on its way. We know when it is going to get there. We can upload. We have all the data that we need to receive it and move it on properly so it smooths that seam. I think you can reduce some of the seams, those tiers, but you cannot get rid of all of them, particularly in all scenarios.
Carlin asked whether the challenge of understanding what is in the stockpile beyond planning and preparation for anthrax (oral medications) drives planning at the local level to the exclusion of preparedness for other types of threats. Gore explained that because of the program requirements and the way they are structured, the amount of time spent focusing on MCM specifics prevents the opportunity to adequately prepare and plan for other types of non-CBRN threats (e.g., sheltering or water crisis). Even within the CBRN space, the focus is on CHEMPAK, on pills and people.
Involvement of State and Local Stakeholders in Requirement Setting (PHEMCE)
Starr maintained that it is important that decisions on requirement setting and quantities purchased take into account the ground-level operational impacts of the decisions that are made. Burhans emphasized the importance of including state and local stakeholders in the requirement-setting process for PHEMCE, because decisions on CONOPS and on the formulary have profound impacts on the last mile. Specifically, he advised that as CONOPS are developed, they should be shared with state and local health departments to make sure they understand the assumptions from PHEMCE’s side. Jaffe commented that operationally, the state and local levels are CDC’s responsibility, but in the requirement-setting process the scenarios are based on material threat assessments. The threat assessments that are used to identify which scenarios are requirement setting will soon be shared with state and local authorities in nonclassified form.
The scenarios upon which requirements are set are the same ones that can be used for exercising and planning. The PHEMCE operational capacity workgroup is also an important venue for state- and local-level engagement and involvement, Jaffe noted. Burhans suggested a formal process identified by the executive committee of PHEMCE to integrate local health department input into requirement setting for the stockpile. Furthermore, Burhans suggested the development of scenario-specific CONOPS tailored for the most likely scenarios that would require deployment of the SNS, in order to better align the federal, state, and local agencies.
Sosin commented that: “Information system problems just are inevitable, especially in public health, but they seem like low-hanging fruit. Just articulating the specific things that you need, I need this bill of lading to come electronically. We can take many of those off the table pretty quickly and we should.”
Best-Practice Sharing Among Local Entities
Petersen suggested reviving best-practice sharing among local entities in regional planning meetings to learn from other’s experiences (see Box 5-6).
Lee also called for improved integration between state and federal governments. For example, complex macro- and micro-level models at different levels of granularities could be used to analyze risk assessment and trade-off, and how it propagates upstream as well as downstream. This is important, because decision making at any level is going to influence many parts of the system. Decision makers and policy makers are facing a challenging problem with many variables and stakeholders with differing objectives. Best practice across different jurisdictions should be shared, but a mecha-
nism for doing so is needed. She suggested that communication—including horizontally among state and local agencies—also needs to be improved.
POTENTIAL OPPORTUNITY FOR IMPROVING CAPACITY TO REACH THE LAST MILE
Fri noted that starting at the dispensing level, response is primarily local and location specific. Thus, the SNS should transfer the medicines to the local and state authorities in the most efficient and effective way possible (improved electronic data interchange [EDI], standardization,11 logistics, etc.) and “get out of the way.” Petersen advocated for a “Swiss cheese” approach to fill gaps in capacity through layering at the state and local levels: incorporating private-sector partners (see Box 5-7), including pharmacies and multiple forms of PODs (closed PODs; public PODs, drive thru). Petersen construed the last mile as when someone actually consumes the MCM, noting that controlling compliance with those medications is part of a bigger issue. Innovative ways to ensure public compliance is needed
___________________
11 She noted that standards already exist in the health care industry for barcoding, EDI, recalls, reverse logistics, etc.
(e.g., he suggested transdermal patches for ease of use for both children and adults).
Inglesby reiterated that the last mile is a huge area of concern, and that no system can work in every location in the country. Working collaboratively will be important to make this complicated process work; everyone is working hard, but the transitions, handoffs, and bridges are difficult and require renewed focus and energy. He suggested that the public health enterprise and PHEMCE should work together to address logistical requirements for a variety of programs, and he suggested the benefit of comparing plans from disparate jurisdictions along common metrics.
Reevaluate Stockpiling in Local-Level MCM Caches
Petersen noted that as funding decreases, it not always sustainable for locals to continue to put funding in local caches. For years, they have had to dispose of medications when there is a national repository of the needed drugs, but it is contingent on timing, and how critical it is to get the product to where it needs to be. He noted that while there are myriad existing innovations that could be applied, not everyone has had access to innovation about how to have industry rotate products, for example.
Gore suggested that utilizing federal buying power for local responses could benefit local jurisdictions that have purchased their own caches for first responders because they could not dispense to them fast enough with SNS assets. In terms of rotation and recycling, having access to the Shelf-Life Extension Program—or even just knowing what the standards for qualifying are—would be very helpful.
Adapting to Variations in Capabilities and Standards Among State and Local Health Authorities
Shah commented that there is wide variation in capabilities at the local public health level. Starr called into question the need to resolve perceived gaps in the last mile in the same way across all municipalities: whether they need to be held to the same standard of necessary preparedness, or if basic capacity related to the risk analysis is sufficient (e.g., being able to provide prophylaxis to the entire state in 48 hours).
Gore sought clarification about what triggers that 48-hour window,12 because it means different things to different people.13 Holding people to a standard requires clearly establishing what that standard is. Lixey Terrill applied this concern to the time frame for dispensing, noting that it could take up to 12 hours for the state to receive the product, plus additional time to move it from the state to the local levels (which still have to dispense to first responders before the general public). She maintained that because state and local caches are often unaffordable, to dispense to staff and first responders and then open to the public narrows that window down to 24 hours. Carlin suggested that two options for “low-hanging fruit” with respect to specific challenges from the state and local perspectives that can be addressed by the standing committee: What does 48 hours really mean? What is in the stockpile, and how can that information be relayed to state and local jurisdictions? These answers, she predicted, would help smooth the handoff or transition and bridge the existing gap.
Improving the “Handoff” Transition
Khan suggested moving away from framing the transition of products from the federal to the state and local levels as a “handoff,” but rather a seamless transition from warehouse to POD to mouths without break-points. Poole commented that this could be improved by factors such as exercising and standardized barcoding. Petersen noted that whenever a product is placed into a distribution chain that works every day, then it will be more effective: “If we can push the product out to some of these multi-modal partners that we have, it is going to help us be more efficient and make the handoff be more integrative.” Starr commented that the capacities and skill sets that are there to rapidly adapt and be flexible to different things are built as part of a system in New York City that has been used in practice for a variety of responses.
___________________
12 Khan noted that events such as influenza outbreak do not need to be addressed within that same 48-hour window that an anthrax attack requires.
13 Is it being exposed versus the confirmation testing? Is it from when the request is made? Is it from when the drugs go out the door, or is it when the drugs get to my doorstep?
This page intentionally left blank.






























