
4
Get Ready for Equity1
Natalie S. Burke, the president and chief executive officer of CommonHealth Action, discussed her organization’s work with clients to create institutional readiness for equity. CommonHealth Action aligns people, strategies, and resources to generate solutions to health and policy challenges, Burke said.2 CommonHealth Action approaches its work from the perspective of the social determinants of health and looks at health as a production of society. The staff of CommonHealth Action work with clients across sectors and disciplines in different communities, so they ensure that they approach projects in a language that is relevant and meaningful to the people they work with. The framework that CommonHealth Action has developed to most effectively do its work is called equity, diversity, and inclusion (EDI). EDI is used with the goal of helping others achieve equity competencies (see Box 4-1).
DEVELOP AN EQUITY LENS
A significant component of the work of CommonHealth Action is helping clients develop an equity lens (see Figure 4-1). Shifting to an
_______________
1 This chapter is the rapporteur’s synopsis of the presentation made by Natalie S. Burke, the president and chief executive officer of CommonHealth Action, and the statements have not been endorsed or verified by the National Academies of Sciences, Engineering, and Medicine.
2 See http://www.commonhealthaction.org (accessed June 21, 2016).
BOX 4-1
Equity Competencies Presented by Natalie Burke
Common language: Individuals are aware of and understand universally accepted words, phrases, and concepts. They are able to exchange knowledge and information based on shared meaning in ways that are easily understood to support collaboration and communication among colleagues, partners, and stakeholders.
Historical context: Knowledge, awareness, and understanding of U.S. history and the evolving policy environment that created past and current legal and social constructs for the privilege and oppression of certain populations. The module highlights the impact of those evolving policies on current social conditions (e.g., the impact of redlining on the inability to accumulate wealth from generation to generation and its relationship to health inequities in infant mortality).
Privilege and oppression: Knowledge, awareness, and understanding of the effect of privilege and oppression at a personal, community, and systemic level.
Equity lens: Understanding the social, political, and environmental contexts of a program, policy, or practice in order to evaluate and assess the unfair benefits and burdens within a society or population.
Policy: Knowledge and understanding of policy making, analysis, and implementation with a focus on equity impact.
Commitment to ongoing learning: Expansion of knowledge, skills, and understanding through engagement in a culture of inquiry and continuous learning.
equity lens is what CommonHealth Action calls a “perspective transformation,” which is, to paraphrase Mezirow:
the process of becoming critically aware of how and why our assumptions have come to constrain the way we perceive, understand, and feel about our world; changing these structures of habitual expectation to make possible a more inclusive and integrating perspective; and, finally, making choices or otherwise acting upon these new understandings. (Mezirow, 1978)
This perspective transformation, similar to Fullilove’s city in mind (see Chapter 3), is aided in part by giving people a vocabulary to understand and articulate a vision of equity.
People default to equality, Burke said, when they are first introduced to the concept of equity. Burke and her team use analogies in order to explain the differences between equity and equality. One example of a
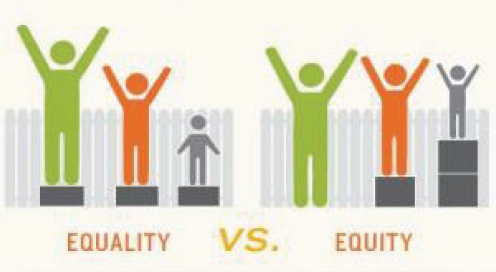
FIGURE 4-1 Equity lens: The lens through which people view conditions, circumstances, and processes to understand who experiences the benefits and burdens of a given program, policy, or practice (CommonHealth Action).
SOURCE: Burke presentation, February 6, 2016.
strategy that they use is to talk about runners competing in a 100-yard dash. It is a straight track. Everybody lines up shoulder to shoulder, so the start is even. It is equal, and there is no reason that one would want it to be any other way. But in the 400, there is a staggered start. The outside lane is longer; the inside lane is shorter. If runners line up shoulder to shoulder, there is an unfair advantage to the person in the inside lane. It does not matter how hard they trained or how hard they worked, it may not even matter how fast they run because the difference is so great that the runners in the outer lane can never catch up. This example, in addition to others, is used by CommonHealth Action to try to get people to understand what equity is. It is a real world example that tends to resonate with people, Burke said. Equality is equal treatment that may or may not result in equitable outcomes. Equity provides all people with fair opportunities to achieve their full potential, Burke said.
Privilege and Oppression
Burke emphasized the importance of considering how to frame equity when speaking to different audiences. One way to do this is to ask people to think of escalators. People who are privileged are on the up escalator for a lifetime. They do not necessarily have to take a step; they just have
to get on the escalator and it carries them to the top. But people who are oppressed are trying to go up a down escalator. If they pause even for a moment they end up back at the bottom. If they miss a step they end up back at the bottom. They have to work harder and faster. They have to be stronger.
The concepts of privilege and oppression can also be challenging for different audiences. Talking about privilege and oppression, Burke said, is a way to get people to relate to how others are experiencing differential power relationships in the society, as opposed to the term racism, which tends to make people feel like they are being judged. Burke explained that giving people terms like privilege can help them to understand the importance of membership in a group that has something of value that is denied to others simply because of the groups to which they belong rather than because of anything they have done or failed to do. She added that dominant group members may be unaware of their privilege or take it for granted. Defining oppression can also be helpful in training clients. Burke defined oppression as “the systematic targeting or marginalization of one group by a more powerful group for the social, economic, and political benefit of the more powerful group.” Burke added that since privilege and oppression occur within the context of power, it is helpful to have a definition of power, such as “access to resources and to decision makers as well as the ability to influence others and to define reality for one’s self and potentially for others.”
By looking at issues of privilege and oppression and discussing the many ways that they operate in society, along with their associated intersectionality, people can begin to understand the challenges that other people face. Sexism and racism are systems of oppression that often manifest within institutions through processes and policies that exclude and marginalize women and people of color. These systems often interact simultaneously; therefore, an intersectional analysis of how racism, sexism, and other “isms” work together to affect health is needed. Race, class, and gender inequities undergird many of the social determinants of health. Understanding the root causes of health inequities and how to change them, Burke said, is critically important.
EQUITY, DIVERSITY, AND INCLUSION
CommonHealth Action training programs teach equity competencies through a process that involves equity, diversity, and inclusion. Burke explained that CommonHealth Action defines diversity as a collective mixture of differences and similarities that includes individual and organizational characteristics, values, beliefs, experiences, backgrounds, and behaviors. It encompasses personal and professional histories that frame
how people see the world, collaborate with colleagues and stakeholders, and serve communities. Inclusion, she said, is diversity in action. Inclusion is an active, intentional, and ongoing engagement with diversity, including intentional policies and practices that promote the full participation and sense of belonging of every employee, customer, or client. There can be diversity and inclusion without equity, but equity cannot be achieved without diversity and inclusion, hence CommonHealth Action’s combination of equity, diversity, and inclusion as EDI.
Readiness and Awareness
CommonHealth Action connects EDI to the existing work and efforts of the organizations with which it is engaging. In some places EDI is approached through a value proposition and in others through a moral argument. Whether CommonHealth Action enters a community, a company, or an organization, issues of readiness, politics, and power have to be considered. Organizations have to be ready to assume a certain amount of risk, Burke said—the risk to be introspective. They have to assess who they are and prepare themselves by devoting a significant amount of support and resources. In order to fully institutionalize EDI into practice, an organization must possess a readiness and awareness of where it is at the start of training as well as make a long-term commitment to continue managing and measuring progress on the path to mastery.
Whenever CommonHealth Action goes to a place to do EDI work, it first does research on the historical context and works to understand the demographics and the shifts in the politics. The reason for this, Burke said, is that there is a potential to do harm. A group or organization cannot start this conversation if the work has not been done in advance to prepare for what emerges in an organization or a community. CommonHealth Action does research to understand as much as possible before getting started with the training process, while knowing that it is not possible to account for every situation that will come up. It does this extensive preparation in order to avoid leaving an organization or community in a worse condition than it was before the process of change started.
Burke shared an example of a training CommonHealth Action conducted in Azle, Texas. The place was nearly 100 percent white at that time, and Burke and the other trainers kept asking themselves how they would have a conversation about equity, diversity, and inclusion in a population and a community that was so homogenous. During the training, there was a woman who was rolling her eyes and using other expressive body language. Burke eventually asked her why she was behaving that way. The woman replied that she had been called a racist by a trainer during an antiracism training because of comments that
she made during a conversation about welfare. This woman went on to tell Burke that she had never met anyone other than white people who were on welfare. The only children that got into trouble that she knew were white children. The only people who had been incarcerated that she knew were white people. The only people who used drugs in their community were white people. Her frame of reference and her context were informed by being born, educated, and living her entire life in Azle.
What this story told Burke was not only that being called a racist was a very painful experience for this woman, but also that the people who had conducted the antiracist training with members of this community did not do their homework. They had their own implicit biases, even though they were the trainers—they were the people who were supposed to be coming to help folks to have this conversation in a way that was healthy and safe, and they did not do that.
Institutionalizing EDI
One of the sectors that CommonHealth Action has worked with is business. Business leaders know that diversity saves them money, makes them more money, makes them more competitive, and increases their value, Burke said. Citing data from a McKinsey analysis on “diversity’s dividend” in the report Why Diversity Matters, she noted that
- Companies in the top quartile for racial and ethnic diversity are 35 percent more likely to have financial returns above their respective national industry medians.
- Companies in the top quartile for gender diversity are 15 percent more likely to have financial returns above their respective national industry medians.3
Burke described how CommonHealth Action advised a Fortune 150 company on global health and well-being. This company has an incredible reputation with regard to diversity, but it recognized that it was time to do more. Burke suggested that the Affordable Care Act is encouraging employers to begin to look at health as more than worksite wellness programs and to recognize that they need to invest in the 16 hours per day that their employees are spending outside of the office in their com-
_______________
3 These data are based on an examination of 366 public companies in the United States, the United Kingdom, Latin America, and Canada. The data also suggested that in the United States “there is a linear relationship between racial and ethnic diversity and better financial performance: for every 10 percent increase in racial and ethnic diversity on the senior-executive team, earnings before interest and taxes (EBIT) rise 0.8 percent” (Hunt et al., 2016).
TABLE 4-1 EDI = Healthy Business
|
Current |
Future |
|---|---|
| Provide health care benefits: FOCUS = physical health | Provide on-site wellness centers: FOCUS = determinants of health and well-being |
|
Support workplace diversity and inclusion |
Use influence to advocate for equitable public policies |
|
Employee rewards = compensation + benefits |
Employee rewards = compensation + benefits + health |
|
Offer healthy worksite food |
Support healthy community food environment |
SOURCE: Burke presentation, February 6, 2016.
munities. Businesses are starting to look at health more broadly, as can be seen in the future column of Table 4-1, by focusing on factors that go beyond the worksite, such as promoting the conditions that improve overall health and well-being, supporting equitable public policies and a healthier food environment, and understanding that health is a form of compensation. For example, if employees are being encouraged to eat healthier, in order to do that throughout the day, they will need access to healthier foods within their community (IOM, 2015, 2016). Companies are starting to use their location in healthy communities as a recruitment tool, Burke said: come to work here and be healthier than if you do not.
Institutionalizing EDI work is a critical component of seeing any sustainable change in this society, in organizations, and even with regard to population health, Burke said. Institutionalizing EDI is not just about transforming the perspectives of individuals or organizations; it has to become a part of policy, program, and practice (see, for example, Chapter 6). And policy is only as good as the way that it is implemented. There are things that organizations and entities can do around employee orientation and recruitment to create an environment for equity, diversity, and inclusion. Every workplace and every community that is more equitable will result in more equitable health outcomes, she said.
This page intentionally left blank.








