
C
Environmental Scan
Submitted to:
Health and Medicine Division and Transportation Research Board
By: Heidi Guenin, A.I.C.P., M.P.H.
This environmental scan was supported by the Federal Transit Administration (FTA) and commissioned by the Health and Medicine Division (HMD) and the Transportation Research Board (TRB), program divisions of the National Academies of Sciences, Engineering, and Medicine. Heidi Guenin conducted the interviews and wrote this report. Special thanks to Ross Peterson, Principal of GridWorks, for providing input and feedback on this report.
The views in this environmental scan do not reflect the views of FTA, HMD, or TRB. For more information, contact Heidi Guenin at (503) 841-7936 or heidi@groxie.com.
PURPOSE
This environmental scan was conducted to support the Health and Medicine Division and the Transportation Research Board workshop: Exploring Data and Metrics of Value at the Intersection of Health Care and Transportation.1
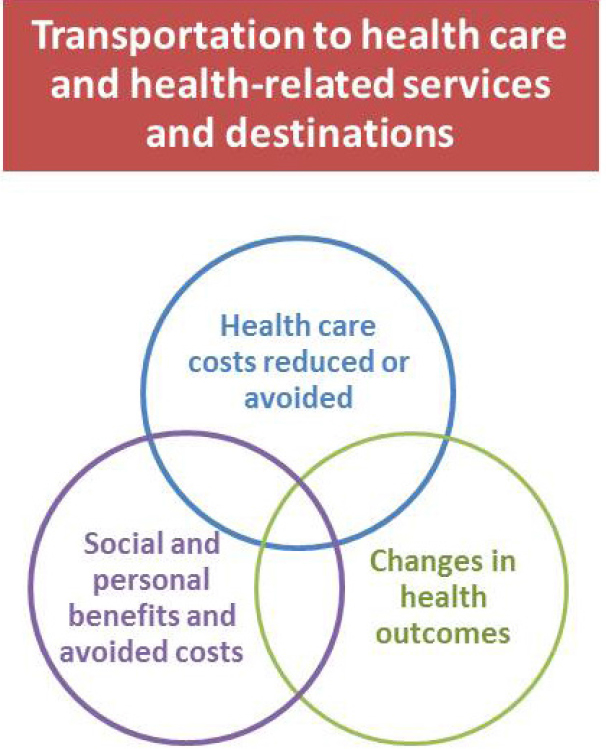
Transportation impacts health outcomes directly, especially through physical activity, safety, and air quality (see Figure C-1). Transportation also impacts access to health care directly, and through access to care, transportation also affects health care costs and health outcomes indirectly. The purpose of this scan is to examine if and how transportation and health care partners explore the return on investment of providing transportation to health care or health-related destinations. More than 70 individuals were interviewed about health care and transportation partnerships, relevant data, and the value proposition of providing transportation to health care and health-related destinations.
BACKGROUND
Transportation is well understood to be a significant factor in health care access. There are many ways that individuals access health care and other health supportive services, including walking, bicycling, riding fixed-route transit (e.g., bus or subway), using a taxi cab or shared ride service, or calling an ambulance. While some individuals have financial, physical, and cultural access to these transportation options and more, others have few to no transportation options to help them access health care. As a direct result they may delay or miss preventive or primary care appointments, not make it for follow-up care, or may be unable to fill prescriptions or access other health supports.
Individuals enrolled in Medicaid can obtain transportation (nonemergency medical transportation, or NEMT) to their Medicaid-covered appointments as part of their benefit, while individuals who are not insured, insured through Medicare, or who have private insurance are responsible for their own ride. The Americans with Disabilities Act (ADA) requires transit agencies to provide paratransit for individuals who are not able to use the fixed-route bus (guidelines for eligibility are set at the federal level and made more specific by individual agencies). Paratransit service must be available during the same hours as fixed-route service and available to pick individuals up and drop them off up to three-quarters of a mile off of the fixed route. Veterans have access to transportation to U.S. Department of Veterans Affairs (VA) health care facilities; more than 100 of the 153 VA
___________________
1 The workshop is part of a project sponsored by the Federal Transit Administration.
health care centers around the country have a mobility manager on staff to help veterans access transportation. Through the Veterans Transportation Service (VTS), veterans can access a ride to the VA from a central meeting point. Enrolled members of a federally recognized tribe have access to health care through Indian Health Services (IHS). The structure of IHS-funded clinics varies, and many provide transportation services to members in need who are not eligible for Medicaid or VTS.
Even with transportation benefits, Medicaid patients and paratransit riders experience many of the same barriers as non-NEMT and non-paratransit patients. Medicaid transportation does not include trips to the pharmacy or grocery store, for example, and some patients may not
have transportation options that match with their health care needs and schedule. Individuals needing paratransit service may need to access a destination outside of three-quarters of a mile from the fixed route or may need assistance getting out of their home or getting settled into their health care facility (transit providers can decide if they provided curb-to-curb or door-to-door service but generally do not cross the threshold of the door). If a veteran needs assistance in getting to the VTS meeting point, or, for example undergoes an outpatient surgery that prevents driving back home from the meeting point, then VTS will not meet his or her needs. Enrolled members of a federally recognized tribe may technically be able to access health care at an IHS-funded clinic, but their transportation options could range from assistance from a Community Health Representative (who may be unable to transport them when they need it), to tribal or other transit service, to Medicaid or VTS, to nothing at all. Because NEMT is a Medicaid benefit that is regulated by the Centers for Medicaid & Medicare Services (CMS), the ADA paratransit is regulated by FTA, the Veterans Transportation Program is managed by the VA, and tribal transportation funding is set aside and regulated through the federal transportation bill each service must adhere to different rules and regulations, and each service generates trip data.
While many patients travel to health care outside of NEMT, paratransit, veterans’ services, and tribal services, these four services are of particular interest when examining the return on investment of transportation access to health care. These four services are provided to some of the most medically vulnerable individuals, for whom access to transportation to health care can often mean the difference between managing an illness and developing multiple chronic conditions or ending up in the emergency room, between living independently and moving to assisted living, or worse.
Past studies have attached a financial cost to transportation barriers to health care, based primarily on missed appointments and on emergency department use and hospitalizations resulting from lack of primary and preventive care.2,3 These costs to the health care system and to patient health are predicted to increase as the U.S. population ages and as our chronic disease burden grows. Health care providers increasingly recognize that transportation is a significant barrier for many patients. Accordingly, we would expect an investment in transportation access to health care to result in benefits for the health care system and for patients. Because trans-
___________________
2 Wallace, R., Hughes-Cromwick, P., Mull, H. 2006. Cost-Effectiveness of Access to Nonemergency Medical Transportation: Comparison of Transportation and Health Care Costs and Benefits, Transportation Research Record:(1956). Pp. 86-93.
3 Cronin, J., Hagerich, J., Horton, J., and Hotaling, J. 2008. Florida Transportation Disadvantaged Programs: Return on Investment Study. Tallahassee: Florida State University College of Business.
portation and health care each manage a different transportation-related program, though, the financial benefits of one program investing in transportation may accrue to another program.
Transportation and health care providers operate under a different set of rules and regulations and have a different vocabulary to define their work and clients. These different vocabularies affect, too, what it means to examine the return on investment of providing transportation services to health and health-related destinations. How transportation and health care professionals define each concept—what is meant by health outcomes, health care savings, transportation, and return on investment—will have an impact on how data are collected and analyzed. Many interviewees discussed how to define return on investment relative to their specific program aims, citing health care savings, improvements in health outcomes for patients, and other societal and personal benefits that may be realized over a long term and/or otherwise difficult to measure or monetize. Many of the interviewees contacted for this report are engaged in some way with NEMT services. While the original contact list did not include a disproportionate number of NEMT-related contacts, interviewees often suggested additional contacts involved in NEMT. One reason may be the perception that NEMT programs:
- require specific data collection and reporting;
- are required to implement least-cost solutions; and
- have recognized gaps that may affect the cost of health care;
- making NEMT programs a likely starting point for many health care and transportation partnerships.
Health
The World Health Organization (WHO), in 1946, defined health as a “state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.”4 This definition is widely accepted and has been in place for 70 years.
Moving from a definition of health focused on an individual to the health of populations, in 1988, the Institute of Medicine described public health as “what we as a society do collectively to assure the conditions in which people can be healthy.”5
As our understanding of the factors that influence health grows, medical health and public health professionals are recognizing their shared
___________________
4 See http://www.who.int/about/definition/en/print.html (accessed September 27, 2016).
5 See http://www.nap.edu/catalog/1091/the-future-of-public-health (accessed September 27, 2016).
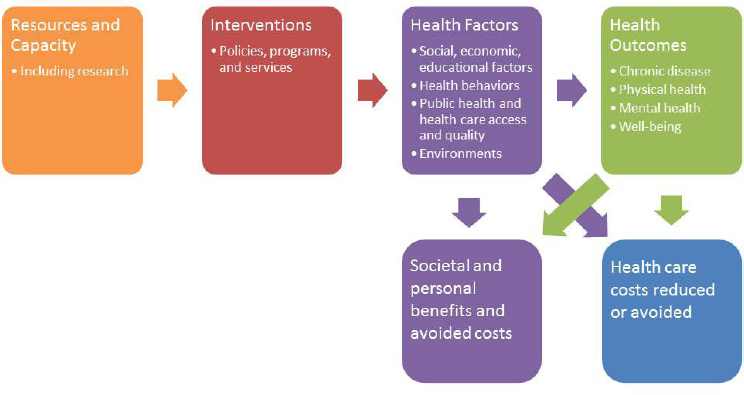
roles in improving patient outcomes. Public health logic models attempt to capture the relationship among resources, programs and policies, health factors, and health outcomes (see Figure C-2 for a logic model for transportation access to health care). Resources and understanding help drive interventions, in turn changing health conditions that impact health outcomes. Improvements in health outcomes and improvements in some health conditions may result in reductions in health care costs. In addition, both health conditions and health outcomes may result in societal and personal benefits and avoided costs that may never be directly reflected in health care costs.
For this environmental scan, the interventions we focused on are transportation policies, programs, and services to improve access to health care and health-related goods and services. Outside of the context of this environmental scan, interventions could include anything that may result in improved health factors—from violence prevention and immunization programs to building more sidewalks or increasing affordable housing supply. This wide range of possible interventions reflects the wide range of health factors that determine individual (along with population) well-being.
You may notice in Figure C-3 that another important health factor—genetics and biology—is not included in this model. Because the model (and this scan) focuses on the impacts of policies and programs, genetics and biology is not included. Also notice that clinical care is shown as being
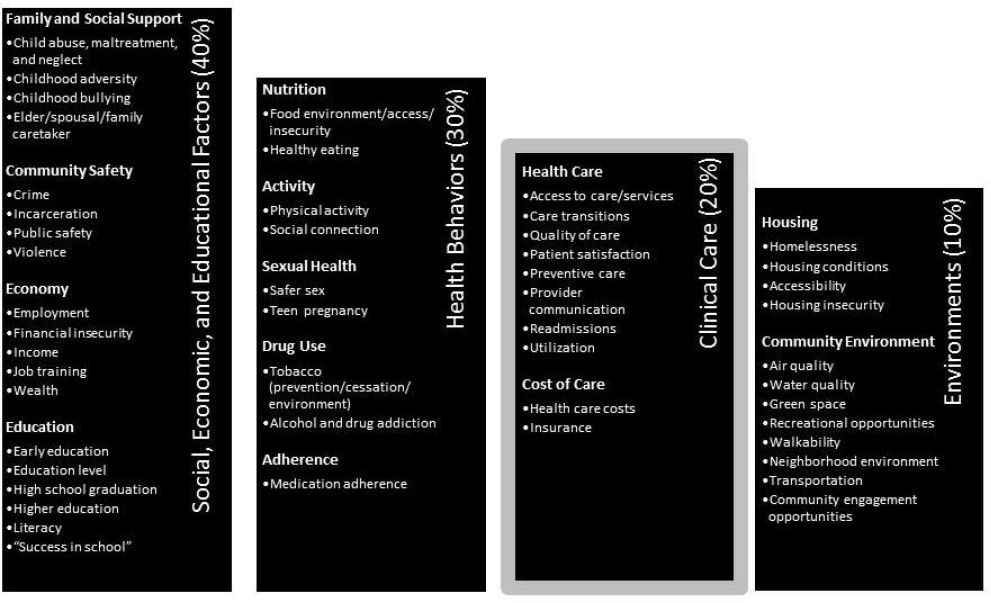
responsible for about 20 percent of the impact that policies and programs have on health outcomes. While this factor includes “cost of care,” with respect to individual health outcomes, “cost of care” here means cost to the patient. However, in considering cost savings to health care providers or insurers, factors included under “clinical care” are relevant. Figure C-3 is not comprehensive; instead, it is focused on factors most relevant to transportation and health care partnerships.
This environmental scan did not include transportation programs solely designed for social and recreational purposes, though a growing body of research indicates that these trips are important for maintaining health and some interviewees, especially those working in rural areas, mentioned isolation as an important health factor. Consider again the WHO definition of health provided earlier: “state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.” A recent report from Martha McClintock and colleagues for the Proceedings of the National Academy of Sciences of the United States of America indicates, “there has been little rigorous scientific attempt to use [the WHO definition]
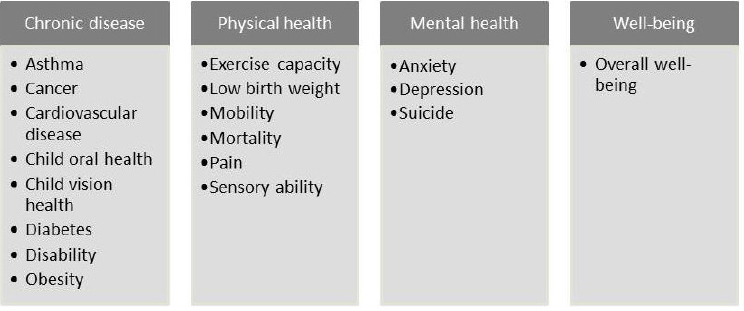
to measure and assess population health. Instead, the dominant model of health is a disease-centered Medical Model, which actively ignores many relevant domains.”6 Using medical, psychological, and health data from the National Social Life, Health, and Aging Project, McClintock and colleagues found that “specific medical diagnoses (cancer and hypertension) and health behaviors (smoking) are far less important than mental health (loneliness), sensory function (hearing), mobility, and bone fractures in defining vulnerable health classes” for older adults. Figure C-4 shows some the main health outcomes impacted by transportation access to health care. This list reflects outcomes discussed by interviewees as well as outcomes suggested by McClintock’s work and a national health improvement initiative.7
Health care and transportation partnerships explored through this environmental scan do not directly measure the results of transportation investments in terms of improved health outcomes. Instead, measurements are often focused on utilization of primary care, emergency room utilization, hospitalization, transportation trips provided, and other data directly related to the provision of transportation and care. Although health care providers may have data on patient health outcomes, interviewees noted the difficulty of understanding the impact of transportation on access to care and the resulting impact of care on health outcomes. Interviewees expressed
___________________
6 See http://www.pnas.org/content/early/2016/05/10/1514968113.full.pdf (accessed September 27, 2016).
7 Adapted from 100 Million Healthier Lives Measurement System: Progress to Date (http://www.100mlives.org/wp-content/uploads/2016/04/IHI_100MHL_Metrics_SpringGathering_ONLINE.pdf [accessed September 27, 2016]) and McClintock et al., Empirical redefinition of comprehensive health and well-being in the older adults of the United States (http://www.pnas.org/content/113/22/E3071.full.pdf [accessed September 27, 2016]).
a desire to better understand the connections among transportation access, care access, and health outcomes experienced by clients.
Transportation
Transportation encompasses a broad range of infrastructure, services, policies, and programs—from walking on city sidewalks with curb cuts that accommodate mobility devices to trains, airplanes, trucks, and barges that carry freight across the land, air, and sea. For the purposes of this scan, we focused on transportation providers, services, or programs that either primarily transport people to health care or for which access to health care or health-related goods and services is an important component. To more easily consider available data sources and possible partnerships with health care, it may be helpful to categorize transportation on a continuum of modes of transportation and the various entities that plan, design, operate, and maintain these various modes. Figure C-5 below presents a collection of entities involved in various elements of the transportation continuum. Each of these is also supported by a network of roads, sidewalks, and paths that are developed and maintained by a combination of entities ranging from state and local governments to private developers.8
Transportation programs included in this scan focused most often on Medicaid clients accessing Medicaid-covered health services. Other populations often discussed included dialysis patients, veterans, people experiencing multiple chronic conditions, pregnant women, children, individuals accessing drug treatment programs, older adults, and people living in rural areas. Several interviewees discussed the importance of transportation in alleviating social isolation and noted how difficult it can be for many clients to have access to transportation to get out into their community outside of medical trips.
Return on Investment
Return on investment (ROI) is a kind of cost–benefit analysis traditionally measuring financial returns (or gains) compared to resources invested. For example, ROI has been used to determine the effectiveness of research and development or marketing efforts for businesses. More recently ROI has been adapted to examine social and environmental impacts through Social Return on Investment. For the purposes of this scan, we began by thinking of investments in terms of (funding for) transportation access to
___________________
8 Revised from FLPPS Transportation Committee Executive Summary, personal communication. (Committee information can be found at: https://flpps.org/Workstreams/Transportation, accessed October 25, 2016.)
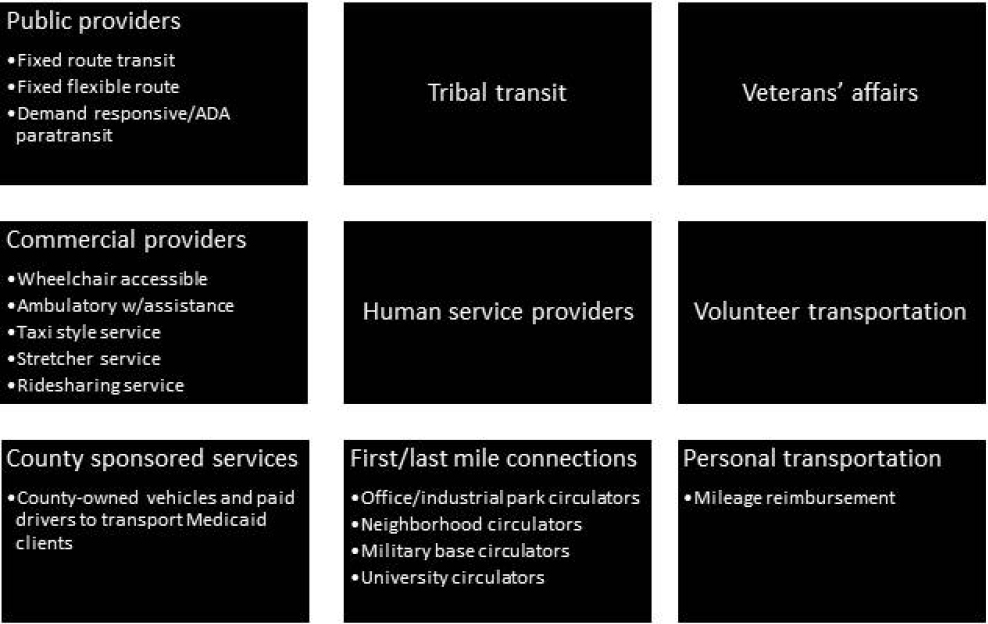
NOTE: ADA = Americans with Disabilities Act.
health care and returns in terms of health care savings or avoided health care costs. We were also interested in efforts to track changes in health outcomes related to transportation investments.
One of the first steps in determining ROI in any context is understanding the outputs and how those outputs translate into returns. For example, transportation providers typically report on:
- fare revenue
- passenger trips
- project revenue miles
- deadhead miles9
- total project miles
- vehicle service hours
- volunteers
- vehicles
- incidents
- injuries
- fatalities
___________________
9 The miles a vehicle travels when out of revenue service.
These outputs are helpful to transportation in measuring a journey, but alone they are not sufficient to understand the full impact of transportation, or what happens after the journey.
For this scan, we were interested in learning about partnerships to connect these outputs to returns through reductions in health care costs. Unfortunately, several challenges emerged through the interviews:
- such data are not readily available from all transportation providers;
- existing data are insufficient to account for important context, such as the population density of the area served; and
- even if a health care partner can attribute health care savings to a trip provided (for example, by using an estimate for missed appointments), it can be challenging to allocate the right proportion of the relevant transportation metric to that trip.
Similar challenges exist on the health care side of the equation. Interviewees most often mentioned staff capacity and technology as the primary barriers to solving the first two challenges. To address the third challenge, one strategy often used in ROI analysis in other sectors is cost allocation, which would allow transportation providers to better understand the cost of providing each individual trip. While nearly every interviewee recognized some benefit to understanding the monetary benefits to health or health care of investing in transportation access, few programs were able to measure this directly. Even without this information, though, several transportation and health care partnerships are moving forward with a shared understanding that monetary benefits will emerge.
INTERVIEW BACKGROUND
Nearly 70 individuals were interviewed for this environmental scan. The interviewee selection is not representative of all of the relevant expertise on this topic. Interviewees represent a diversity of organizations and roles within those organizations—from federal agencies to local providers and community-based organizations, from individuals who distribute funding to those who managed programs and work with individual patients or clients. For a list of individuals interviewed, please see p. 160. Throughout the scan, direct quotes from interviewees will be used as examples of the major themes. In order to protect privacy and to encourage honest and candid information sharing, quotes will not be attributed to a specific individual. Instead, quotes will be followed by the sector in which the individual works:
- brokerage
- consulting/technical assistance
- consumer/consumer advocacy
- foundation/funding
- health services
- human services
- research/academia
- transportation services
- tribal transport/health care
- veterans’ services
Interviewees were asked about health and transportation partnerships that they knew of or worked within; business models that supported those partnerships; and the data collected, analyzed, and shared through those partnerships. Interviews were conducted primarily by phone and lasted 15–60 minutes. Interviewees were asked to suggest other potential interviewees as well.
Overall, among interviewees there was an appetite for better understanding the data and evaluation measures being used or under consideration in other areas—whether those areas are disciplines, geographic areas, or specific programs. There was an accompanying sense of trepidation about the limitations of examining the costs and benefits of transportation investments in relation to health care.
Interviewees expressed gratitude to FTA for funding this workshop and the other related efforts examining the intersections between transportation and health care, and several suggested areas where FTA and other federal agencies could support local efforts to coordinate and improve service provision.
SUMMARY OF THEMES
Across sectors and other variables like geography and client demographics, interviewees shared many of the same challenges and potential solutions. Overall, the most significant challenges interviewees face in creating health and transportation partnerships and measuring return on investment fall into seven categories (not listed in order of importance):
- Defining return on investment
- Funding and basic infrastructure
- Missing information and data
- Technology
- Geography
- NEMT destination and service gaps
- Cross-sector collaboration
Within each of these themes, sub-themes emerged, which are highlighted in each theme’s section.
Solutions and opportunities emphasized by interviewees fell into eight categories (also not in order of importance):
- Grants
- Shared learning
- Start small and go slow
- Let patients tell the story
- Take the care to the patients
- Customer experience
- Sharing resources, increasing revenue
- Sharing data, analyzing solutions
Fewer sub-themes emerged during discussions about solutions and opportunities.
INTERVIEW THEMES: CHALLENGES
Defining Return on Investment
Interviewees, identified below only by their sector, discussed the concept of return on investment from many perspectives, citing challenges and opportunities for how to explore this topic in the future. Major concerns included
Value or Return on Investment Outside of Health Care Costs
Interviewees agreed across the board that investments in transportation are critically important to supporting access to health care, but they did not all agree that improving transportation access to health care would necessarily result in reduced health care costs.
“We want to comment on the assumption about reducing the health care cost. Our position has always been that these are areas that are significantly underserved. . . . You’re introducing more patients, more frequent patients—could lead to more than just screenings and regular doctor appointment. It could lead to specialty visits.” –Transportation services
“This whole notion that we’re going to reduce the transportation costs if we work more collaboratively—I don’t agree with that. We’re very efficient.” –Transportation services
Interviewees suggested that between existing patients accessing more care and new patients beginning to access care, health care costs may increase, at least in the short term (see time scale comments below) and maybe for the long term as well.
“This is like a sieve—you create a little space and there’s lots more need. No matter what we’re doing, the more access we provide, the higher the cost will be, because we’re not providing for all of those needs now.” –Transportation services
“You’re getting people access to surgeries and other care they couldn’t get before. So the trade-off is that, for us, we see hospitalizations go up, because we are getting people access to care. But they need that care.” –Health services
Some interviewees suggested that measuring benefits in monetary terms obscures the real measure of success—improved access to care and patient well-being—and may not reflect desirable outcomes achieved.
“If your investment is in health outcomes and not profit, then why are we even talking about this? [Patient’s] life improved, quality of life improved. So why are we talking about it as only monetary? Investing in patients is good in and of itself.” –Transportation services
“We’re not trying to keep people from health care, so that’s not really the cost we want to look at. Are we adjusting medication or treating someone after a stroke? Is it making a difference for you, individual person who received a ride? Transportation providers—are you giving more rides because the system is more efficient? Health care providers—are you noticing fewer no-shows?” –Human services
“We do show that they got care they wouldn’t have otherwise gotten. We worry about the people who never get connected—at homeless shelters, etc. They’re not even showing up in the health care system yet at all, and maybe we can keep them out of the ER?” –Health services
The Time Scale Over Which We Measure
Many interviewees suggested that, while health care costs may be reduced as a result of better transportation access to care, these benefits might not accrue in the short term or even the medium term. Interviewees
suggested several ways that high care costs could be reduced with increased transportation access to primary care, from preventing emergency room visits to increasing the time a person can stay in his or her own home.
“Even though we’re always concerned about the trip costs, at the same time, we’re trying not let lack of transportation become a barrier to successful treatment. Often [patients] will come in in a very vulnerable state. It takes a while before they have success with their behavior changes . . . and we can start getting them to drive again or figure out other transportation. Sometimes that takes time, and it’s worth the higher cost investment to get them to that point.” –Brokerage
“It’s like everything in life—you have to put in up front to get a return on the back. What we do costs more up front. Up front that first year or two out of the facility costs more than being in, but after that, the costs fall off greatly once a person is established at home. We talk all of the time about how much cheaper it is for an individual with a disability to live in the community than in a facility, but it costs more to actually get them there.” –Health services
“One of the things that we really believe, is that what we do supports people living in place, decreases isolation, so they’re less likely to go to an assisted living facility.” –Transportation services
Return on Investment for Whom
Interviewees described many benefits of improved transportation access to health care and health-related destinations that will not necessarily be reflected in health care costs. This topic generated some of the richest feedback from interviewees, providing ideas for future study.
For the Patient
“Our program encourages states to look at inclusion post-discharge. Rather than just moving somebody, and then you’re on your own. . . . We encourage our grantees to tell us how they’re going to encourage people to get involved—something to get them out of the house and be part of the new community” –Health services
“Indirect route and the long wait times were concerns [for patients], because they have to dialyse for so much of their life already, having to add an hour or two increases the time that they’re all about dialyses and not about their life. . . . ‘I need to go home, take a nap, so when my kids get home I can make dinner and be part of their lives.’ Doesn’t have a cost that can be quantified with money.” –Transportation services
For Caregivers and Family
“[There was a] gentleman who needed to go to bariatric treatments three times a week. His wife had a disability, and he took care of her. If he hadn’t gotten reliable transportation, his wife would have had to go into assisted living. Who knows what would have happen to his wife if he hadn’t been able to get that transportation.” –Human services
“[Could we quantify] family costs, such as costs saved because family members who are caregivers can return to work and/or engage in family activities because their role as caregiver diminishes as their loved one gets well?” –Human services
“Caregivers often quite frequently die before the people they’re caring for; so the ripples [of giving them a break from transportation] are spreading throughout the community and is ultimately just a win for everybody.” –Transportation services
For the Community
“It would be great to quantify: economic contribution of individuals because they can get to work; increases on workforce participation for those individuals who coordinate transportation service or provide the rides directly; decrease in lost productivity costs for employers—reduction in need to hire temporary employees; increased production or service; decreased health insurance costs; community costs—costs on community integration, participation in religious and civic organizations. People who are healthy can spend money in the community, participate in community recreation and entertainment events, they can vote, they can attend events (that might have entry fees), etc. Could these costs be captured?” –Human services
“[Patients using ambulance for nonemergency transportation] may put other people at risk, too. If they’re bringing people to nonemergent medical appointments, that keeps them from being able to provide emergency care.” –Research/academia
“If we have patients who are abusing drugs, they’re going to have myriad health conditions. Their children are going to have health issues, domestic violence issues, going to be in jail all of the time—it leads to societal issues as well as health issues” –Health services
Funding and Basic Infrastructure
Interviewees consistently talked about the need for more funding to effectively meet the needs of clients and patients. In response to having too few resources, interviewees emphasized two major themes—going slow and
starting small—that will be addressed in the “Solutions and Opportunities” section. In addition to the nearly unanimous call for more funding generally, individuals working with tribal transit and tribal health care highlighted the need for basic infrastructure on tribal lands.
“When [other provider] is talking about the sheer danger of being on the roads, it’s very real. The only road into their community is a 36 mile dirt road. To have a school bus driving on that road is scary. Anyone who needs higher medical care than their clinic can provide [to get there] is scary. Getting food in—18 wheelers on that road—is scary.” –Tribal transport/health care
“Sometimes [water] trucks crash, or there’s a flash flood and folks can’t get through. EMS services—sometimes the ambulance can’t even make it over their roads.” –Tribal transport/health care
“With respect to transportation for Indian country, to be quite honest, it’s not just access to the automobile that would get them there, it’s about the roads and whether they’re passable—whether they can even get there, and if they’d want to risk getting on those roads.” –Tribal transport/health care
Missing Information and Data
Another significant theme across interviewees was related to whether and how relevant questions about access were being asked at all levels of service. Several interviewees working in health care and transportation partnership noted that their work was catalyzed or informed by community needs assessments.10 Sometimes these needs assessments included questions about transportation, and other times participants brought it up on their own. Others noted that health care providers may not have information about a patient’s transportation barriers or if an appointment was missed due to transportation. For tribal transportation, data concerns were primarily focused on crash and other safety data and on GIS data.
Asking the Right Questions
“Sometimes the patient makes us aware of transportation issue, but other times they won’t voice that need if they’re not asked.” –Health services
___________________
10 Such assessments are an Internal Revenue Service requirement for not-for-profit hospitals and health systems, and are also required of public health agencies by the state or for the purpose of obtaining public health accreditation (see, for example, https://www.nlm.nih.gov/hsrinfo/community_benefit.html and http://www.phaboard.org/accreditation-overview/getting-started [accessed September 27, 2016]).
“What we found when we asked initially, a lot of them didn’t even know why people weren’t showing up for their appointments.” –Human services
“We’ve learned many things such as the anxiety that people have, of using public transportation, for behavioral health” –Transportation services
“We already had a one-call center. What we didn’t have was the mechanism to identify the at-risk patients to address re-hospitalizations.” –Health services
“Regional hospital did the community health assessment but didn’t ask about transportation. People would hand write in the margin—access, language barriers.” –Transportation services
“You call to make a doctor’s appointment. The very first question is ‘What insurance do you have?’ We want the second to be ‘What kind of transportation do you have?’” –Consumer/consumer advocacy
“If you use a lot of transportation (not counting dialysis), what are people actually doing when they’re using a large amount of transportation? Does that mean anything or not?” –Transportation services
“Ask outreach programs what they think their needs are. Our sense is that with health center data there’s a bias, based on patients that are already walking into the health center doors. For folks not accessing the health care system, the only folks who might have a sense of those barriers are outreach workers. They directly interact or observe some of the groups that don’t go to the health centers.” –Consulting/technical assistance
Some interviewees noted that it is insufficient to just ask whether or not a patient has transportation; the accessibility of that transportation in terms of culture and timing might have an impact on health care accessibility as well.
“How well are health centers asking that question? They’re not always realizing what options are out there. Need the partners to ask the question in a culturally competent way, in a way that really collects information that we’re looking for over time.” –Health services
“The need for same day service is huge—now they can go to the doctor if the doctor will accept them.” –Transportation services
“We are a city of bridges and tunnels and rivers. It’s no big deal to cross two bridges and go through a tunnel, but for some people it is [a big deal]. You need to get a handle on the culture of a place as well.” –Consumer/consumer advocacy
“Moms who are at risk of going pre-term, they have to get a progesterone shot to help them get along as far as possible. They can only get it from a compounding pharmacy—only three of them in the region, most in the suburbs. It’s a weekly shot. You’re only going to pay to get to the doctor; it’s important, but the shot is just as important in getting her to full term. If [her] level of comfort to get on the bus (if she can afford it) to go up to this working class pharmacy to get this shot—it’s just not going to happen. Gets into race and affordability. . . .” – Transportation services
Impacts of the Patient Protection and Affordable Care Act
One challenge to measuring return on investment that many interviewees noted is the impact of health care transformation. With an increase in the number of people with private insurance and eligible (in many states) for Medicaid, costs are likely to go up in the short term, making it difficult to evaluate a return on investment. New patients may require education about their benefit and other service to help them fully access care, and these costs may impact a provider’s ability to evaluate a return on investment as well.
“[Measuring is] further complicated by the ACA and whether or not the state expanded its Medicaid program. There may be an increase in cost—is that a function of delivery of transportation or simply more individuals eligible. What if medical services aren’t available [nearby], and transportation costs increase for that reason?” –Research/academia
“Ramping up for health care coverage, but for the groups most in need, having coverage was not the same as having access; [there’s] distrust and fear in the system (based on immigration, race) and transportation barriers.” –Consulting/technical assistance
“With the ACA and the expansion, we have this population that came on to a plan. A lot have never had insurance and need education about benefits, how to utilize insurance.” –Health services
Same-Sector Information Gaps
Interviewees discussed data-sharing challenges not just between transportation and health care but within each sector as well.
“Information on the transportation side of trips—some of that data is out there, we don’t necessarily have access to it. On the medical side, we can see outcomes of people. What’s missing is how to connect a person’s health to their transportation, so that when transport is identified as a barrier or
need, the health care center can make sure they’re providing the right kind of transportation to that care.”
“There’s a Medicaid broker who helped try to arrange transport. [Patient] had a behavioral appointment that Medicaid would cover. Their doctor said [patient] can take public transit. Their counselor said [patient] needs taxi service because of anxiety. The broker sides with the physician (or the cheaper form of transportation). Sure enough, [patient] doesn’t get to their appointment.” –Health services
“Trying to figure out how much money it costs for a pre-term birth, that info is not public. Negotiated rates with the insurance companies—[health care providers] won’t give that; but also, that’s not necessarily the costs. We’re only including the hospital stay [in our return on investment evaluation], but you get billed by hospital, doctor, everyone who worked on you. [We] couldn’t keep track of everything—we’d have to ask each of the individuals. So we need to have a relationship with the insurance companies to get them to tell us what’s being saved.” –Foundation/funding
HIPAA
The two biggest challenges interviewees mentioned around data was related to the Health Insurance Portability and Accountability Act (HIPAA). Many interviewees have decided to forgo working through processes related to HIPAA and instead use data related to trips or other non-health proxy data.
“The thing about HIPAA—in small towns, everybody knows who you are if you dig into it enough. [Maybe it should be] us feeding the hospital the transit data and them doing the analysis without talking about the people—just a higher-level aggregate.” –Consulting/technical assistance
“If they had told us, ‘Here are our top ten ER utilizers, go out and serve them. . .,’ but none of our partners would share anything meaningful with us because of HIPAA.” –Transportation services
Data on Tribal Lands
Interviewees working in tribal transportation and health care discussed the challenges of funding and operating transportation infrastructure and services without basic data that other sectors often take for granted—crash statistics and GIS in particular.
“When the state divvies up dollars, a lot of times they will exclude tribes, not intentionally, for a couple of reasons: they really don’t think about it,
and tribes aren’t sharing their crash data or don’t even have crash data. So even when the tribes do ask for money to improve the roads, the state doesn’t see the data to justify why they need the money to improve the roads.” –Tribal transport/health care
Technology
Technology was cited as a barrier to partnership and a tool to improve partnership and data sharing. In particular, interviewees noted the need for data standards and flexible and open software to support for partnerships. Even if an agency is up-to-date technologically, clients may not be able to access the technology due to a lack of awareness or because of their own technological limitations.
Need for Standardized Data and Open Technology
“Modern data standards, well-documented code—allows us to plug and play different solutions as needed. Everything changes so fast, and we need to be ready to meet those needs as they come. Doesn’t necessarily mean it has to be open source, but it does have to be developed in a way that is flexible enough to tap into new technology and data sources.” –Consulting/technical assistance
“A lot of it goes back to the transit program having the correct technology to dispatch their drivers on time and to the right location.” –Tribal transport/health care
“One of the biggest struggles working with the public transit providers and using fixed-route service is a lot of them don’t have OS data or GTFS files. [There’s] no one-stop shop nationwide so I can appropriately identify the trips and geocode them. Having access to OS GTFS data could make all of the difference in the world in regard to NEMT using the fixed route services. We would be open as a brokerage to exploring the option of helping these agencies create this data.” –Brokerage
“You get all of these little proprietary systems. How do you collect data when they don’t connect with each other? The FTA or some federal agency [could take] the lead and make open source platforms, standards.” –Transportation services
Client-Side Technology Barriers
“[We’re doing] one year of planning to make sure our technology will serve the needs of the individuals in the center for independent living—-
individuals who are unable to see or hear; will it work with the reader devices, etc.” –Brokerage
Tracking Trips
The difficulty of tracking transit trips emerged as a concern primarily related to NEMT but also in general for considering return on investment. The potential of electronic fare to enhance trip tracking was discussed by several interviewees.
“Public transit agencies (don’t know if they’re carrying a veteran or a NEMT trip).” –Research/academia
“One thing we found, especially in the public transit system, it can be difficult to track who is riding and what kinds of needs they have. If you don’t have a card that identifies who the riders are, then the systems are not able to identify with great accuracy. They can probably make decent estimates of what riders fall into what categories, but if you’re looking at a short period of time at increasing ridership, that can be challenging.” –Consulting/technical assistance
Geography
Challenges related to density of population and different kinds of service boundaries were a common theme among interviewees.
Rural Challenges
Interviewees noted that transportation and health care needs and appropriate measures of success are different for rural areas, compared to urban and suburban areas. Interviewees also noted that much of the transportation need in rural areas is related to health care.
“Transportation for us is really a problem in rural areas. When people want to transition back to their home on a farm, the state has to give us a 24 hour back-up plan. So states are slow to move people back to rural areas; [they do] not want them to move from a facility back into seclusion.” –Health services
“There are very different issues in the rural and non-rural areas. The metrics around transportation needs some component to take those into account. How are you using resources efficiently if there are only seven people per square mile? That’s something we’re finding. We have the numbers for each site; when we look at number of rides, distance of trips—the more rural the site, the less efficient the transportation is. Unless that is
pointed out to leadership, they just think that the program isn’t functioning well.” –Veterans services
“They had to start with criteria that said less than seven people per square mile. What about the rural parts of neighboring counties, say three people per square mile, but the county average brings it up? We’ve driving right by people who should have access.” –Veterans services
Jurisdictional and Service Boundaries
While barriers in each state differ, interviewees across the board experienced challenges crossing service or political borders. Interviewees expressed frustration at not always knowing who was imposing the boundaries and what could be done to better integrate neighboring systems.
“All of the sudden you have this brokerage in [Town A] trying to get someone to [Town B] and back. How do you even out the cost? Basically [you] need to have agreement between each of the transportation providers.” –Consulting/technical assistance
“You have to be certified by each of the providers, pay whatever rate each charges. That’s a huge barrier as far as independence. You can only go as far as my service goes—beyond that you have to work with another provider.” –Health services
“We had to get federal motor carrier authority to be able to take folks to the clinic in [other state]. We were the first transit agency to go through that process. No one really knew how to do it, and [we] had to get transferred so many times, because they don’t know their own rules. It took us a year.” –Transportation services
“That whole issue of not being able to cross lines or borders without those agreements—I understand that intellectually. But is there something they can do to make that easier? It’s ridiculous. I can get my patient to the border, but then I have 2 miles to go, and I have to get someone from another county. Is it a statutory requirement? A funding requirement? If you’re going to have regional health care, there’s got to be some way to make this a little easier to do.” –Health services
“Health care did not have the capacity to take people to regional care. We need to cross 1, 2, or 3 municipal boundaries, and the original model was designed for local rides on a recurring basis.” –Human services
NEMT Destination and Service Gaps
These issues were raised generally and in relation to Medicaid, Medicare, and VA transportation. Interviewees described several health-supportive destinations that they considered to be key factors in improving health outcomes, including pharmacies, group homes, support groups, grocery stores, assessment appointments, and benefit qualification meetings. Some interviewees also discussed difficulties arising from children and caretakers not being able to ride along with patients.
“The big one that we always hear is pharmacy; there are tricks to get your prescriptions on your way home from the doctor.” –Health services
“Even groceries—some [patients] can get them delivered, but many do not have this option. You’re at a severe disadvantage to maintaining yourself at home if you can’t even get food.” –Research/academia
“You have to have a face-to-face with a physician to say you need home services—well that requires transportation to get there in the first place!” –Research/academia
“Transportation is an issue, too, at the point of preparing to transition. We have to get people to Social Security offices, get them to go and view places they can live. If they’re not part of the paratransit system or any number of [other barriers]—if they can’t easily get to and from where they need to go to make the transition process happen, it makes things more difficult.” –Health services
“We started a rides to grocery program. We had mom and pop stores closing and nowhere to buy groceries. Rides to groceries was designed to provide options and hope for people. Little were we aware of the linkage between fresh fruits and veggies and health care. We have many partners in that program.” –Transportation services
“A lot of nonprofits have rules about not going to group homes, but a lot of group homes don’t have vehicles.” –Brokerage
“Even one of our local assisted living programs doesn’t have an ADA vehicle. They won’t buy one—we’ve tried to sell them one.” –Transportation services
“A lot of these patients wouldn’t have had any appointment for behavioral health [without our program] because Medicaid doesn’t cover the initial assessment.” –Human services
“The thing I hear the most is we have free Medicaid transportation, but I can’t bring my kid. I can’t get a babysitter for them.” –Foundation/funding
Cross-Sector Collaboration
Cross-Sector Knowledge
Interviewees described hurdles to collaboration, including confusion around language, funding sources, how different programs operate, how to connect with the right individuals in other sectors, and what programs might be appropriate to partner with. These same concerns were echoed during the Improving Healthcare Outcomes: The Mobility Management Connection symposium during the 2016 Community Transportation Association of America (CTAA) expo in Portland, Oregon. The following quotes are from interviewees, not CTAA participants.
“It would be ideal if CMS and FTA could get together and put together a common language or corresponding language.” –Brokerage
“If the state DOTs could have sort of ‘go-to people’ lists available for the transit agencies that are out there in their respective states. Even within the agencies that should know their own rules, there’s a lot of misinformation out there.” –Transportation services
Different Motivations and Measures of Success
Several interviewees suggested that diverging missions or measures of success create significant barriers to effective partnerships between health care and transportation.
“We find that both public transit and Medicaid NEMT have a similar goal—they want to provide individuals, especially those without other options, access to health care. And there’s an expectation that it will improve outcomes. Beyond that, they don’t have many additional goals or objectives in common, and in fact they sometimes diverge.” –Research/academia
“Health care operators are always going for the least cost, trying to drive down the cost as much as they can—including transportation. Or, there are some saying ‘what if we provide all these access and support services so people can be healthier? Will that reduce our costs?’ CMS is driving both of these models at the same time.” –Consulting/technical assistance
“The two professions come at this from a very different perspective. The public transit arena would like to think that through coordination and shared trips that they’re capable of providing the lowest cost, most effec-
tive transportation. But from Medicaid, the transit agency is not always lowest cost. So you see the evolution being more and more brokered through a private broker and capitated payments, so there’s not a link to the trip provided and the payment made. And the private broker is looking to make the trip at the lowest cost, maintaining their contract, and making a profit margin. Public transit agencies with fleet replacement, advanced vehicles, technology, etc.—not necessarily seen as valuable to the Medicaid transport folks. Public transit seeks to recover its operating costs, but the Medicaid brokerage is really just looking for the cheapest; [there is] not consistency about those objectives and how to measure them.” –Research/academia
“There’s a contradiction in the NEMT language. It encourages demand response trips as a last response. They encourage people to use public transportation to the maximum extent possible, but if that happens, there’s no way to track that trip. Maybe you provide a fare ticket or a fare card; short of a smart card, you can’t track it. But that’s the lowest cost for everybody. NEMT—they encourage it, it’s in the language, but there’s no effort to require that or to document, to evaluate an individual or their trip and then send them that way. You’d think brokers would encourage that since it lowers their cost, but they can’t track the encounters, so that’s counter to their mandate to track data.” –Research/academia
“The people that are most interested are the payers—the insurance and the managed care folks; not really the health care providers.” –Transportation services
“Until transportation becomes an incentive measure, then we wouldn’t have a real frequent process of looking at that. We do look at people who are the most fragile who go to the ER a lot or access care a lot. We do reach out to them to see what their needs are—that’s one thing [readmission] that is an incentive measure, and transportation is part of that.” –Health services
“Transit people have [an] assumption that more access and more rides are better. People paying for health care (mainly Medicaid, since they pay for transportation) embrace attitudes of insurance company—‘the less we have to pay, the better, so more transportation is the opposite of better.’” –Transportation services
One issue that interviewees mentioned repeatedly was that a strong emphasis on fraud prevention on the health care side might be hindering more effective partnerships between health care and transportation providers. The challenge seems to be ensuring proper use of funds and services while maximizing benefits to patients.
“Medicaid funds have to be used for a beneficiary who needs to get to an approved medical trip and no other purpose. They can’t be on a bus with a veteran or someone else. It creates a perverse incentive for some successful programs to not chat with researchers about what is actually working and successful if it fits into a grey area. If you’re trying to do something innovative that just works for your patients, not trying to break federal grant rules, you may want to avoid having to ask forgiveness. They may not even know they’re in violation.” –Research/academia
“In the VA, folks are very concrete. They’re worried that the veterans are just saying they needed [the transportation program] because they like the service.” –Veterans services
“Public transit is looking to provide any users transportation for any trip purpose in the most cost-effective manner possible. NEMT is looking to get Medicaid eligible people to Medicaid eligible appoints for the cheapest cost. [Medicaid is] really looking to prevent fraud and abuse—including using transportation for any other trip purpose, even shopping. Doing so, even as trip-chaining, would be considered fraud or abuse.” –Research/academia
Coordination
Interviewees noted that coordination improves as it is mandated, and several commented on the importance of coordination at the federal level.
“Coordination mandates need to be happening on both sides. Right now, that mandate is on the DOT side from the FAST Act, but it needs to be mandated for other folks spending money on transportation and flow down to the states and regional coordination. Medicaid sends the money to the states, and the states have great latitude to spend this money. They have no ultimate obligation back to adhere to coordination or the intent to work with local public transit agencies to work effectively with resources.” –Research/academia
“When brokerages were just getting established [health services] came out very strongly that brokerages were creating a siloed system—they already had a state coordinating council. [Recently] they said that brokers are helping facilitate, but it’s due to some of the state requirements for coordination.” –Research/academia
“Over 80 programs provide funding for transportation disadvantaged populations, around 40 or so federal programs that provide [NEMT] funding. [Where is] data on the programs, on the number of people they provide services to, which grantees, how much funding is being used.” –Research/academia
“This is going to sound way out there. It just seems to me we have so many rural veterans in this country, it would be nice if CMS could partner with the VA to leverage some of those transportation resources. They drive right by and even go through the same community.” –Research/academia
“My experience with Medicaid is that it’s one of the areas where it was hard for people to understand. [The Medicaid NEMT provider] can transport people to VA medical centers, and it’s a covered service from the perspective of transportation. From the visit side, there’s not encounter data—it’s not available. That does create some issues if you’re audited. But you’re helping a veteran get to the care that’s more appropriate and allowable. It creates a little discomfort.” –Health services
“[We’re] like 5-year-olds playing soccer—everyone storms around the soccer ball and are all trying to do the same thing, not aware of what other people are doing and when to pass the ball.” –Health services
Change Takes Time
“We’re learning we have to really start small. The willingness, for people to change and organizations to change—it’s really hard to do. The idea that we’d make suggestions and wave carrots and people would change isn’t really happening.” –Health services
“When you’re bringing worlds and disciplines and sectors together, it’s not the easiest natural place for people to go. Give adequate time and space to understand each other’s language, build trust; it takes time, intentionality, real management whether at the highest level or within community. Be mindful of the longevity of the effort, what it takes in terms of the active management could be easy to overlook if you’re just looking at it as part of the data and programmatic end.” –Foundation/funding
“It always takes more time to develop the connections than you can ever plan for. If you don’t take time to do that, you’re basically putting together a program. A program can never address a complicated social issue. Five years later, everybody’s going to look back and say, well that didn’t really work. You have to develop a lot of trust to be able to work together; it’s not for the faint of heart. We’ve certainly seen some people drop off who have no tolerance for that type of work. We would have just continued to meet and admire the problem from year to year and not changing it.” –Human services
“We’ve been working with [software company] for about 3 years to purchase our product for our call center, making significant customizations. After we began working with [Coordinated Care Organization], they required us to have a business associate agreement with any of our
contractors, especially if sharing data. It took us 18 months, but we finally got a signed business associate agreement with [software company].” –Brokerage
“I got all of the groups to come and meet and talk. ‘We’re in competition with each other for funding—your passengers aren’t going to ride in my vehicles.’ It’s changed so much since then, but it’s taken a lot, and some people are still not willing to look at new ideas.” –Brokerage
INTERVIEW THEMES: SOLUTIONS AND OPPORTUNITIES
Grants
Several interviewees viewed the Rides to Wellness and other grant opportunities as catalytic in the creation or progression of partnerships between transportation and health care.
“This opportunity came, a real reason to work with the transportation folks. We didn’t have them on our coalition. [Rides to Wellness] is what created that impetus.” –Foundation/funding
“These [projects] emerged from the conversations we had even prior to applying for the grant. After applying for the grant, were able to form partnership more coherently.” –Brokerage
Shared Learning
Interviewees relayed a need for more and better systems for sharing learning relevant to this topic. Several mentioned having met peers at conferences or learned about other projects through grantee meetings. Many interviewees suggested areas where it would be beneficial specifically to have more guidance from the federal agencies, including related to funding streams and associated rules and the Stark Law.
“[There is a] need for more knowledge management in this area—we have a tendency to have great ideas, implement them, someone comes in and tries to make it more ‘efficient’ and then basically blows it up.” –Consulting/technical assistance
“It’s now easy for us to look at these things, but prior to doing this work we wouldn’t have thought about it. And that’s how we can contribute—help folks to start seeing—‘Oh, my peer did that.’ Otherwise we get really dismissive. If people see organizations like theirs tackling these challenges—that’s the importance of the peer-to-peer learning groups.” –Consulting/technical assistance
“Brokerage [is] operating under ‘you have to be 18 to get your own approval to get transportation for health care, to get approved for health care.’ The law says as young as 12 you can receive health care without guardian permission.” –Health services
“[Health services] really hold their hat on this [Stark] law that prevents them from paying for transportation. We believe that’s just an interpretation.” –Transportation services
“They can ask for things in their states plan in the way they execute their Medicaid program, likely to be approved in an individual level. Just because someone doesn’t think the funds can be used that way, sometimes they can. How it plays out on the local level is completely locally driven.” –Research/academia
Start Small and Go Slow
By far the most commonly discussed theme across all interviewees was the amount of time that transportation and health partnerships and programs take to build. Interviewees suggested several different reasons for and benefits of going slow. Because the need for transportation to support health is so great, some programs suffer from trying to grow to quickly or setting out to solve too many issues at once. Several interviewees noted how difficult it can be for individuals and communities if a transportation program disappears or is scaled back.
“The goal is 1 year of planning to make sure our technology will serve the needs.” –Brokerage
“It was meant to be a small thing, and it grew too much. It turned into something bigger than we expected.” –Transportation services
“[We’re] definitely trying to control the growth, because we’re still learning and there’s a lot we don’t know. The bigger we get too soon, the capacity becomes an issue.” –Human services
“We are focused on a part of our state that by all indicators really needs help. It has been the beneficiary of a lot of programs saying ‘We’re coming in with the answer to your problems.’ [There was] not a lot of buy-in from the local folks. [Our] core element at this point is planning—not ready to run out and develop a service, say ‘Here is the answer.’ Lots of outreach is needed in this initial buy-in to avoid push back and avoid low utilization.” –Transportation services
“Without success, we won’t get the other folks to the table to support us. That’s why we are narrowly focused.” –Transportation services
“We had to keep scaling down this program, because the demand was so much greater than the money we had.” –Transportation services
“Those [Rides to Wellness] projects that focused on information and outreach actually seemed like they had a good first step to the future work they might be doing. Those that were trying to come up with new models of service coordination or service provision—some are going to work out, but it’s more aggressive and had more risks along the way. To try to change how to provide what we’re providing, this stuff takes time. A lot of times people are surprised by that.” –Transportation services
“For last 2 years, [we’ve been] laying foundation for starting the partnership with the transit agencies and reaching out to bring awareness to the benefits of partnering with the NEMT brokerages—for us, them, the members they serve.” –Brokerage
“We have always had an historic partnership with the [program]. It’s been the paratransit service’s largest customer for the last 25 years. I was in a meeting when we were faced with this issue. The design challenge email came through the next day, so we started working on it.” –Transportation services
“One thing that’s come out of this to me that’s been worth all of the time we put into it—we have built the greatest partnerships in this community to understand health care and how we can all work together.” –Transportation services
“We have access to our leaders; you can just pick up the phone. Maybe if you had asked me about that 5–6 years ago prior to [project], I might not have said that. Since we’ve gone through such a strong exercise of building the [project], it keeps the partnership going.” –Transportation services
“Make sure you know everything else that is going on in your community. You may be duplicating efforts, you may be so overwhelmed with demand that your great idea becomes more of a headache than anything else, and you’re still turning people away left and right. Know who you’re going to serve, who you could not service through the program. If you want to develop an effective program serving the population you want to serve—reach out to them and ask them what they need, what they’d like to see, what are the problems they’ve encountered, how can you ensure whatever gets built, provided, funded in the community addresses those needs.” –Consulting/technical assistance
Most interviewees expressed a need for more resources, but many also discussed the need to work with available resources—from funding to community assets—in the short term, while future financial funding is unknown or unstable. This theme is closely related to the next theme, because many interviewees viewed working with current assets as the most sustainable way to begin new partnerships or programs.
“What we see so often is that things develop quickly without a sustainability plan. How can we be sustainable as funding comes and goes, while we make something that’s reliable and a utility for people? Our users rely on us—we can’t just go away next year. Innovation is the hot thing, but what can we do to support, grow, and amplify the things that already exist.” –Consulting/technical assistance
“If someone would just give us a lot more money we could do this or that. But that’s not coming soon, so what are we prepared with right now with what we can provide? How can we do that most collaboratively with what we have right now? How can we best get the results we need with what we’ve got?” –Transportation services
“Some partnerships formed, a lot [are] in the beginning stages. We talk about fixed-route services first. That was the first piece, work with transit agencies all across the county, identify members who can use fixed route services and are within .75 miles of a stop.” –Brokerage
Let Patients Tell the Story
Several interviewees emphasized the importance of listening to patients’ stories and working with patients to help develop programs and resources. Some interviewees had been able to previously develop video or Photovoice11 projects and found them to be very valuable for both the patients to share their perspective and for the organizations to make progress in funding or otherwise supporting partnerships and programs.
“We talk internally about how important it is to talk about this from the perspective of the patients. The solutions are about people.” –Consulting/technical assistance
“If you’re talking to 20 providers, you should talk to 20 consumers.” –Consumer/consumer advocacy
___________________
11 A definition of the Photovoice process is available at http://ctb.ku.edu/en/table-ofcontents/assessment/assessing-community-needs-and-resources/photovoice/main (accessed on September 27, 2016).
“What needs to drive what we collect and track and use to make decisions is the relevance to the individual—to their needs and if those needs are being met. The person being served is at the center of how we’re collecting this data and how we’re using this data. Quantitative data isn’t enough—we need to know how their quality of life is being impacted.” –Transportation services
“We [dialysis patients] make a huge impact [talking to decision makers]. It’s not just a story for them—I’m real. It’s not ‘There’s 270,000 of us [dialysis patients].’ I try to put a face to it—we’re real.” –Consumer/consumer advocacy
Take the Care to the Patients
A few interviewees mentioned existing or planned mobile units to respond to transportation barriers. These existing and planned units have foci ranging from children’s health and adult primary care to behavioral health crises and hospital discharge follow-up. One interviewee recommended creating a mobile pharmacy.
“The plan once we get it up and running is to have a list of people who have been discharged from our hospital during the week, and [mobile unit] would go out within 2–3 days to visit them and make sure things are going well. They’re able to intervene within a limited scope to prevent readmission, funded through the cascade health alliance.” –Health services
“In the aftermath of CHIP passage, the period of time after the money had been given out, [there was a] lag in uptake in certain states. We put two mobile units in the deep South, heard from a lot of concerned folks—that while they were excited about the prospects of having kids enrolled, a lot of them were experiencing long-standing transportation barriers and rendered their newly gained insurance coverage not as useful as it should have been.” –Foundation/funding
Customer Experience
Customer service was a common theme among interviewees, with several noting the value of the extra training that public transit staff complete. In all regions, but especially in more rural areas, interviewees noted the benefit to clients of having regular drivers, volunteer or paid, with whom the patient develops a relationship.
“Working with insurance companies, drivers have HIPAA training—extends from the health insurance companies but is a different model. Cli-
ent base is vulnerable in some way, so the drivers need to be altruistically motivated, customer service based.” –Brokerage
“One plan originally didn’t offer public transit, and now it’s the highest utilized option. Members have been happy, complaints have gone down, and they’re saving money.” –Brokerage
“The small public transit in rural areas are people-focused and community-focused. From a brokerage perspective, it’s good to have people on the ground providing services for you.” –Transportation services
“The other element [to address] from a federal perspective—our customer is the same customer as a public transit customer. From Medicaid and FTA—anything we can do to make it easier to access those services is good. A lot of times we’re all serving the same customer, the payment and eligibly is different; are there ways to make that easier for the customer?” –Transportation services
“We’ll send as many trips as possible over to [public transit], and we get reduced complaints, better member service.” –Brokerage
Sharing Resources, Increasing Revenue
Although most interviewees described challenges in creating partnerships that involved cost sharing, several also shared examples of early partnerships that included in-kind donations of staff time and other resources. Cost allocation was suggested as one tool to help transportation and health care partnerships better understand inputs and outcomes to measure return on investment. Some transportation services staff discussed the revenue benefits of working more closely with health partners in terms of Medicaid transportation trips, too.
“One of the things I did at the brokerage was to try to support the public transit agencies to contract with us, keep them busy. The Medicaid transportation became an additional source of revenue that supplied match for the federal grants. I viewed that as being a win-win any time I could partner with those types of organizations.” –Transportation services
“We run the fixed-route bus service; also run the NEMT brokerage for the three counties—whatever is needed to get them to their health care appointments. That’s become a real big business for us dollar wise—bigger than general fund.” –Transportation services
“Program of all inclusive care for the elderly—we are the only type of transportation provider to provide this transportation service in the country. [The] operation is part of the local hospital. They pay the full cost of
the rides. Through the contract, we provide the vehicle, the driver, and an attendant on board, through your door to help and through your door to the health service. To the degree that the hospital is benefiting in their model and they utilize us, we can capture our full cost of providing that trip. It allows us to expand service without expanding the local subsidy.” –Transportation services
“Individual people who are eligible for these services—they know if they have an expectation for a demand response trip they can get it. Why bother with rail or bus in that case? In some environments, they know that the public transit agency is the option of choice, and they choose to just use fare—that means that the transit agencies doesn’t get the extra money they would from Medicaid (even though it saves Medicaid money from the demand response).” –Research/academia
“[We] launched a call center with a marketing team of board members and marketing director from [health services]—their phones, their computers, their office supplies—that’s their match. Expenses are my salary and the operating costs. [Health services] is doing all of my accounting and HR; I am a [health services] employee leased to [brokerage].” –Brokerage
“Our DOT public transit division is very supportive of the work we do. I’ve heard others talk about their 5310 money and how difficult it is to access it and use it—it’s often focused only on capital purchases. [The DOT public transit division has] receptiveness to maximize the use of federal dollars by leveraging state money and trying not to leave anything on the table. Regionally, having a transit agency willing to step outside of the box—using private, state, and federal programs—and having a transit authority that understands that public transit goes beyond a fixed-route system and beyond ADA is a benefit in our community.” –Transportation services
“The transit system has allowed the health workers to go on the bus with patients without charging us to get people used to it. Don’t know what that cost is to the transit agency.” –Health services
“First year of the [community health worker and transportation] program was funded by [CCO] as part of transformation money, now expired. Then the hospital took over the program—staff [is] hired by them and works for them.” –Health services
“[We have] two significant partnerships—both regional hospitals. As they looked at access, they saw loss of efficiency in the process by not having a centralized on-site presence to coordinate that effort. They both contract with [brokerage] and pay for a staff person to coordinate transportation; large part is Medicaid transportation, but it does spill over to
non-Medicaid clients also. So we have staff there on site to coordinate the transportation. They were able to demonstrate that in having that presence they were able to free up medical staff time to get out of the business of transportation. Rather than the social workers, discharge nurses doing it—now it’s transport staff.” –Brokerage
“Most of the operators had a positive experience—did it at a fully allocated cost. Role of NEMT has been leavening for rural transit has allowed rural communities to do amazing things.” –Consulting/technical assistance
“From the transit’s perspective, by setting up this model, compared to what it would have been if we had done it the traditional way of more individual rides which we are obligated to do, we’re saving between $25,000 and $30,000 a month.” –Transportation services
Sharing Data, Analyzing Solutions
While interviewees discussed many hurdles to sharing information between health care and transportation providers, some solutions emerged as well, ranging from Business Associates agreements to meet HIPAA requirements to housing transportation staff within the hospital or clinic. Others offered options for avoiding HIPAA issues by asking patients directly for information; some of these same solutions are included in the next section—“Available Information.”
“Main programming is the navigator, and the navigator will work for the clinic. [Nonprofit organization] will bring the coalition together, hire someone to analyze the data we get, but the clinic is going to implement the program. [This structure] got us a lot of things—they can watch someone from the day they walk in to the day they deliver, can follow people and see what their birth outcomes are, how are people who use the navigator working out, compare that to outcomes for people who aren’t using the navigator.” –Human services
“We also got a grant from [funders] who have come together looking at technology to get data. We’re going to collect feedback from patients through SMS. After somebody goes through the program, they’ll get a text, and we’ll ask them questions and get feedback outside of HIPAA. We’ll get information from them pretty close to the time they’re receiving the services; [a nonprofit organization] will be collecting that data—more about customer service than outcomes.” –Human services
“Some benefit to the transportation benefit being part of the CCOs—which is ultimately having the information in the same place will help be able to address those questions better.” –Transportation services
“[Health care providers] were very concerned about customer confidentiality and HIPAA. We clearly defined to them what the pilot would include—data sharing on customers that opted in. They’d be completely notified. We did incentivize it, because we asked participants if they were opting in to complete a pre-, post-, and quarterly survey. [Health care provider] was provided documentation on what the pilot would look like. There was a champion—a social worker who acted as the bridge and agreed to help facilitate the gathering of patient information. They agreed to let us have everybody’s prescribed treatment times and monthly or quarterly documentation on the actual time on the machine so we can compare those.” –Transportation services
“Going to track over time evaluation measures—mental and physical health (self-report). Since they’re going to get transit passes, we’re going to track where they use them and how often they use them.” –Transportation services
Some interviewees noted that brokers are or could be collecting and analyzing data in a more sophisticated way then other service providers. These data may be difficult to access, though.
“[Brokers] have more data than anyone we’ve ever seen. Even your small broker serving a small county has more information on individual riders—trends, cost, location. Brokers are the ones that are profit driven, so they’re really forced to collect that information.” –Research/academia
“[We] could potentially ask the clients themselves with notifications at the end of the trip. Or a phone call for individuals who do not use a smartphone to book their trip. Not just ask them about their trip but how they feel about their health; don’t want to collect specific information about the location of the doctor.” –Brokerage
“There is data sharing between us and the client [the health plan]. We do monthly dashboards; we’re pretty tight with the data we share outside of our clients. [We] don’t post average trip costs or how many trips we’re serving, but we have provided data for specific research projects that may come up.” –Brokerage
AVAILABLE INFORMATION
Interviewees shared information about national datasets or other relevant information that are currently available and will be available in the future. This section also includes representative snapshots from on-the-ground providers about information being collected at the local level.
Existing National Data
Integrated National Transit Database Analysis System
http://www.ftis.org/INTDAS/NTDLogin.aspx
“[RTAP] surveys the state DOT programs nationally and the transit program managers in states every 2 years. We ask them about their service and their issues. It gives us a clear picture of the challenges and issues that are relevant to our audience. We also ask about how they train and their technology. Rural operators and states have to report significant data as part of their grant agreement with FTA. National RTAP funds an analysis site so that systems and states can compare themselves and their numbers with other entities in the state and nationally.” –RTAP
General Transit Feed Specification, Google
http://maps.google.com/landing/transit/cities/index.html#NorthAmerica
“Lists the cities that have fixed-route service and accesses their itinerary builders. This gives you a picture of the availability of fixed-route transit in any given area of the use. Some states have taken more of a leadership role in assisting rural operators in becoming visible through Google maps.” –RTAP
National Transit Database
http://www.ntdprogram.gov/ntdprogram/data.htm
“Metrics: trip data, costs, revenue hours, revenue miles, vehicle miles, passengers per hour. These data elements can be down loaded from the NTD webpage or sliced and diced through the link I gave you. We are working with one of our board members who is going through an analysis process to identify health cost savings with enhancing access for people who are managing chronic illnesses.” –RTAP
AGing Integrated Database
http://www.agid.acl.gov/DataGlance/SPR
AGID is an “online query system that provides access to ACL-related program performance results, surveys and other data files.” Users can examine data, by state, that includes Census databases and Administration on Aging (AoA) databases. AoA databases include State Program Reports (SPR), Title VI Services by Tribal Organization, and Long-Term Care Ombudsmen reports. The SPR data may be of particular interest to health care and transportation partnerships. It includes information about one-way trips funded through the Older Americans Act, including demo-
graphic information about clients, client satisfaction, federal dollars spent, and the services accessed, including
- Personal Care
- Homemaker
- Chore
- Home-Delivered Meals
- Adult Day Care
- Case Management
- Congregate Meals
- Nutrition Counseling
- Assisted Transportation
- Health Promotion
- Cash and Counseling
–Administration for Community Living
NORC (National Opinion Research Center) University of Chicago National Social Life, Health, and Aging Project
http://www.norc.org/Research/Projects/Pages/national-social-life-healthand-aging-project.aspx
“The health of older adults is influenced by many factors. One of the least understood is the role that social support and personal relationships play in health and aging. The National Social Life, Health, and Aging Project (NSHAP) is a longitudinal, population-based study of health and social factors, aiming to understand the well-being of older, community-dwelling Americans by examining the interactions among physical health and illness, medication use, cognitive function, emotional health, sensory function, health behaviors, social connectedness, sexuality, and relationship quality. NSHAP provides policy makers, health providers, and individuals with useful information and insights into these factors, particularly on social and intimate relationships. The study contributes to finding new ways to improve health as people age.
To date there are two waves of NSHAP data available to researchers, and funding has now been awarded for a third wave of data collection. In 2005 and 2006, NORC and Principal Investigators at the University of Chicago conducted the first wave of NSHAP, completing more than 3,000 interviews with a nationally representative sample of adults born between 1920 and 1947 (aged 57 to 85 at the time of Wave 1 interview). In 2010 and 2011, nearly 3,400 interviews were completed for Wave 2 with these Wave 1 Respondents, Wave 1 Non-Interviewed Respondents, and their spouses or cohabiting romantic partners. The second wave of NSHAP
is essential to understanding how social and biological characteristics change. By eliciting a variety of information from respondents over time, NSHAP provides data that will allow researchers in a number of fields to examine how specific factors may or may not affect each other across the life course.
In 2015 and 2016, NSHAP plans to conduct more than 4,800 interviews for Wave 3. In the third wave of data collection, we will interview respondents that participated in a previous wave(s), which will improve the robustness of the study’s longitudinal data by adding a third time point. In addition, we will recruit and interview a new cohort of adults born between 1948 and 1965 and their spouses or cohabiting romantic partners to allow us to examine changes in trajectories of health across birth cohorts. As in Waves 1 and 2, Wave 3 will describe health and health transitions of respondents, and how they relate to a different kinds of social relationships in respondents’ lives.
For all waves, data collection includes/will include three measurements: in-home interviews, biomeasures, and leave-behind respondent-administered questionnaires. The face-to-face interviews and biomeasure collection take place in respondents’ homes.” –NORC
National Core Indicators
http://www.nationalcoreindicators.org
“National Core Indicators (NCI) is a collaborative effort between the National Association of State Directors of Developmental Disabilities Services (NASDDDS) and the Human Services Research Institute (HSRI). The purpose of the program, which began in 1997, is to support NASDDDS member agencies to gather a standard set of performance and outcome measures that can be used to track their own performance over time, to compare results across states, and to establish national benchmarks.” –National Association of States United for Aging and Disabilities (NASUAD)
Data Set Directory of Social Determinants of Health at the Local Level
http://www.cdc.gov/dhdsp/docs/data_set_directory.pdf
–Centers for Disease Control and Prevention
Health Indicators Warehouse
http://www.healthindicators.gov
Includes Nation Health Interview Survey data among others. –National Centers for Health Statistics
Coming Soon
National Core Indicators-Aging and Disabilities
http://nci-ad.org
“The National Core Indicators-Aging and Disabilities (NCI-AD) is an initiative designed to support states’ interest in assessing the performance of their programs and delivery systems in order to improve services for older adults and individuals with physical disabilities. NCI-AD is a collaborative effort between the National Association of States United for Aging and Disabilities (NASUAD) and the Human Services Research Institute (HSRI). NCI-AD’s primary aim is to collect and maintain valid and reliable data that give states a broad view of how publicly funded services impact the quality of life and outcomes of service recipients.
NCI-AD brings an important value proposition to the field of aging and disability services through development of indicators and outcomes that assess quality of life, community integration, and person-centered services. The project will help to address long-recognized gaps in assessing outcomes in long-term services and supports (LTSS) service systems that go beyond measures of health and safety to address important social, community, and person-centered goals as well as quality of life.
Data for the project are gathered through annual in-person surveys administered by state agencies to a sample of at least 400 older adults and individuals with physical disabilities accessing publicly funded services in skilled nursing facilities, Medicaid waivers, Medicaid state plan programs, and/or state-funded programs, as well as older adults served by Older Americans Act programs. The survey instrument includes a background survey, which gathers data about the consumer from agency records, and an in-person survey, which includes subjective satisfaction-related questions that can only be answered by the consumer, and objective questions that can be answered by the consumer or, if needed, their proxy. Project team interprets each state’s data and produces reports that can support state efforts to strengthen LTSS policy, inform quality improvement activities, and compare their performance with national norms.” –NASUAD
Survey questions include
- Do you have transportation when you want to do things outside of your home, like visit a friend, go for entertainment, or do something for fun?
- Do you have transportation to get to medical appointments/pick up medications when you need it?
- Can you see or talk to your family as often as you want to?
- With “transportation” offered as an option to choose in the followup question Why not?
Existing Local or Program-Specific Data
Most interviewees accessed and analyzed data from one sector. To understand value or return on investment, they rely on aggregate data, anecdotes, or only consider impacts within their own sector. Interviewees use surveys, aggregated data, anecdotes, and already completed analysis from other regions or sectors to help evaluate services and inform decisions.
“We can say—to what destination are they heading and circle different geographic coordinates. This many trips to hospital, this many to the shelter, this many to the bar—we can code the type of trips and know location-wise where are you going, how many miles, how long to get situated, what kind of money used—state, fed, donations. We do an MOU with all of the folks who have use of our corporate platform.” –Brokerage
“Short-term, [we’re] looking at access—number of trips and appointments successfully made. The impact on health care outcomes is going to have to be designed with more guidance from the health care side.” –Transportation services
“We own the software that the brokerage is using; we have access to all of the data. One of the things we want to look at is—how much transportation occurs within an individual’s county, and how much takes them outside of their county. [There is] limited information about the appointments in the software.” –Transportation services
“[They] have had increased behavioral health appointments—greater than they’ve ever had before. People are keeping their appointments; people are getting better and getting better faster. The big thing for the hospital [after a patient is discharged], they have no transportation to go home. The hospital can’t get that patient out of the bed, and keeps them from making money. Ability to get patients into a more appropriate setting after their care at the hospital is finished. For each $1 invested you save $9—calculating out the avoided health care cost. That hospital in 2015 had the best financial year they’d ever had; CEO attributed a big piece of that to this project.” –Consulting/technical assistance
“We have a health transportation coordinator paid through [health services], housed in hospital, coordinates rides for a large region, tracking financial impact for each patient. We know what billable revenue has been tied to the patients brought to the door through this project and what it costs us to get them there. The consideration on the health care side—just
because it was billed doesn’t mean it was what they netted. We need an actuarial study to figure it out.” –Human services
“Number of trips, average fare, what are patients paying—we will collect those data.” –Human services
“Did one survey via e-mail veterans. We can take that data and show that, according to the veterans, 25 percent wouldn’t have made it to their appointment. What is the cost of a missed appointment? Over a period of time, reducing the number of missed appointments saves the system a lot of money. Missed appointments are a big deal; access to care is limited to the time the clinic has to see veterans. If someone misses and that time goes unused, that’s a big deal.” –Veterans services
“One study demonstrated that VTS does impact missed appointments. [We did] one round of the survey, and now we’re authorized to do a second round. We’ll have some numbers that suggest [that] at least.” –Veterans services
“I’ve been told that through the Medicaid brokerage, appointments for preventive care—the no-show rate has dropped. [Have seen] a higher number of patients for preventative, which has overall savings.” –Brokerage
“When do people call, what kind of trips are they? Where are they going? What’s the ride for? If they’re a veteran, if they use a mobility device, their level of service? Not HIPAA related—trying to stay away from that issue.” –Brokerage
“When we first started our high-risk pregnancy program, a lot of our moms thought it was normal to take the ambulance to the ER every time they had pain. We’ve only had 134 people in our high-risk pregnancy program, but only 5 have had low-birth-weight babies. [We’ve] been able to see that and that there was a cost reduction of about $2,000 per case. Ambulance rides decreased dramatically.” –Health services
“The 98 highest utilizers were costing us $9 million, reduced by half. We saved them $2.4 million in ER costs. But this same group at that point only had had 1,500 primary care visits. Once we got them on the bus or [paratransit], their primary care visits increased to 6,500. So higher transportation and some care costs, and lower ED and ambulance usage.” –Health services
“The utilization of VA medical appointments has increased; the VA has reported no cancelations for people using this service.” –Veterans services
“It’s been highly successful with multiple ROI: decrease in no-show appointments, members are feeling more supported and satisfied with health care, 65 members have actually graduated from the program and have met their goals, decrease in emergency room and hospital readmissions, improved appointment compliance, medical compliance.” –Health services
“We were a participant for 4 years in a community-based transition program. Our job was to prevent readmission into hospital. Had coaches that met with patients in the hospital and followed them closely for 40 days. Part of that, we gave them the coaching, and we actually gave them free transportation to their follow-up medical appointments, meals, in-home assistance like housekeeping and things like that. We reduced readmissions. [We don’t know] if the people who got the transportation access had less missed appointments, more compliance—we didn’t really have a good control group.” –Transportation services
“In the last 4 years since 2011, the health care authority in [state] has been requiring the brokers to submit a report—data tracking and utilization system. It’s an extensive data base getting a lot of trip information for the Medicaid clients using transportation.” –Brokerage
“We commissioned a poll and came up with a survey. [We] determined that a significant percentage—20 percent of children under 200 percent poverty and 9 percent under poverty line—were missing routine health care because of transportation barriers.” –Foundation/funding
“We do collect data out of that program, but it’s principally the number of rides, associated health care visits for primary care and allied support services.” –Foundation/funding
Coming Soon
Ride Connection
Ride Connection, a nonprofit transportation services provider in Portland, Oregon, developed and is implementing a pilot program to improve outcomes for dialysis patients. In June 2016, Ride Connection will have a third round of survey data available. In addition, an article by Ride Connection staff discussing the program will be published in The Journal of Nephrology Social Work, National Kidney Foundation: https://www.kidney.org/professionals/CNSW/JNSWOnline (accessed September 27, 2016)
The Way to Wellville
“How do you get to Wellville? There are many roads and help from visionaries who’ve made great strides creating places where people enjoy healthier lives. Yet the Way to Wellville remains mostly unexplored.
That’s why HICCup is sponsoring The Way to Wellville, a national challenge among five communities over five years to make significant, visible and lasting improvement in five measures of health and economic vitality. In the end, we’ll map new paths for entire communities to make changes that result in healthier people and places.
Communities were required to submit a completed application in May 2014 to be considered for The Way to Wellville challenge. After reviewing 42 applications from 26 states, HICCup selected the Wellville Five communities in August 2014.
HICCup is a nonprofit founded by angel investor Esther Dyson to encourage a rethinking of how we produce health. Working together in Wellville, we will show the world how collective investment and action can return healthy dividends for communities—and their investors.” http://www.hiccup.co (accessed September 27, 2016)
RESEARCH AND RESOURCES
Completed Reports
GAO 12-647 Transportation-Disadvantaged Populations: Federal Coordination Efforts Could Be Further Strengthened
http://www.gao.gov/products/GAO-12-647
Findings: “Eighty federal programs are authorized to fund transportation services for the transportation disadvantaged, but transportation is not the primary mission of most of the programs GAO identified. Of these, the Department of Transportation administers 7 programs that support public transportation. The remaining 73 programs are administered by 7 other federal agencies and provide a variety of human services, such as job training, education, or medical care, which incorporate transportation as an eligible expense in support of program goals. Total federal spending on transportation services for the transportation disadvantaged remains unknown because, in many cases, federal departments do not separately track spending for these services. However, total funding for the 28 programs that do track or estimate transportation spending, including obligations and expenditures, was at least $11.8 billion in fiscal year 2010.
The interagency Coordinating Council on Access and Mobility, which the Secretary of Transportation chairs, has led government-wide transportation coordination efforts since 2003. The Coordinating Council has undertaken a number of activities through its ‘United We Ride’ initiative aimed at improving coordination at the federal level and providing assistance for state and local coordination. For example, its 2005 Report to the President on Human Service Transportation Coordination outlined collective and individual department actions and recommendations to decrease duplication, enhance efficiencies, and simplify access for consumers. Key challenges to federal interagency coordination efforts include a lack of activity at the leadership level of the Coordinating Council in recent years—the Coordinating Council leadership has not met since 2008—and the absence of key guidance documents for furthering agency coordination efforts. For example, the Coordinating Council lacks a strategic plan that contains agency roles and responsibilities, measurable outcomes, or required followup. GAO has previously reported that defining and articulating a common outcome and reinforcing agency accountability through agency plans and reports are important elements for agencies to enhance and sustain collaborative efforts.
State and local officials GAO interviewed use a variety of planning and service coordination efforts to serve the transportation disadvantaged. Efforts include state coordinating councils, regional and local planning, one-call centers, mobility managers, and vehicle sharing. For example, state coordinating councils provide a forum for federal, state, and local agencies to discuss and resolve problems related to the provision of transportation services to the transportation disadvantaged. In other examples, one-call centers can provide clients with transportation program information and referrals for appropriate service providers and mobility managers may serve many functions—as policy coordinators, operations service brokers, and customer travel navigators. However, state and local governments face several challenges in coordinating these services—including insufficient federal leadership, changes to state legislation and policies that may hamper coordination efforts, and limited financial resources in the face of growing disadvantaged populations.”
GAO 15-110 Transportation-Disadvantaged Populations: Nonemergency Medical Transportation Not Well Coordinated, and Additional Federal Leadership Needed
http://www.gao.gov/products/GAO-15-110
Findings: “Forty-two programs across six federal departments—Agriculture, Education, Health and Human Services (HHS), Housing and Urban Development, Transportation (DOT), and Veterans Affairs (VA)—
can provide funding for nonemergency medical transportation (NEMT) service, although NEMT is not their primary mission. Twenty-one of these programs, including Medicaid, are administered or overseen by HHS. The type of funding provided by these programs varies, but includes capital investments (such as bus purchases) and reimbursements of transportation costs (e.g., bus passes). Total federal spending on NEMT is unknown because federal departments do not separately track spending for these services. In some cases data were not available or NEMT was incidental to a program’s mission. However, one of the six departments (HHS) was able to provide estimates indicating that its spending totaled at least $1.3 billion in fiscal year 2012—most of this attributable to Medicaid.
Coordination of NEMT programs at the federal level is limited, and there is fragmentation, overlap, and potential for duplication across NEMT programs. The federal Interagency Transportation Coordinating Council on Access and Mobility (Coordinating Council)—chaired by the Secretary of DOT and tasked with promoting interagency cooperation and establishing mechanisms to minimize duplication and overlap of programs for the transportation disadvantaged—has taken some actions to improve coordination, such as developing a strategic plan. The strategic plan identified the council’s goal, priorities, and objectives for 2011 to 2013. However, the council has provided limited leadership and has not issued key guidance documents that could promote coordination. For example, the council has not met since 2008 and has not finalized a cost-sharing policy that would allow agencies to identify and allocate costs among programs. GAO has previously found that agencies providing similar transportation services to similar client groups may lead to duplication and overlap when coordination does not occur. This review found instances of fragmentation, overlap, and the potential for duplication, although the extent could not be quantified.
State and local officials in the selected states GAO visited identified a variety of ways they facilitate coordination of NEMT. These include state coordinating bodies (two states GAO visited), regional coordinating bodies (two states GAO visited), local metropolitan planning organizations, and local transit agencies. Cost and ride sharing and one-call/one-click information centers were also used to coordinate NEMT services. However, GAO found two programs—Medicaid and VA NEMT programs—largely do not participate in coordination activities. Requirements to serve only eligible individuals and ensuring proper controls are in place to prevent improper payments and fraud are among the challenges to coordination for these programs. These important NEMT programs provide services to potentially over 90 million individuals and coordination without the Medicaid and VA programs increases the risk for potential overlap and duplication of services.”
GAO 16-221 Medicaid: Efforts to Exclude Nonemergency Transportation Not Widespread, But Raise Issues for Expanded Coverage
http://www.gao.gov/products/GAO-16-221
Findings: “States’ efforts to exclude nonemergency medical transportation (NEMT) benefits from enrollees who are newly eligible for Medicaid under the Patient Protection and Affordable Care Act (PPACA) are not widespread. Of the 30 states that expanded Medicaid as of September 30, 2015, 25 reported that they did not undertake efforts to exclude the NEMT benefit for newly eligible enrollees, 3 states reported pursuing such efforts, and 2 states—New Jersey and Ohio—did not respond to GAO’s inquiry. However, the Centers for Medicare & Medicaid Services (CMS), within the U.S. Department of Health and Human Services (HHS), indicated that neither New Jersey nor Ohio undertook efforts to exclude the NEMT benefit.
Two of the three states pursuing efforts to exclude the NEMT benefit—Indiana and Iowa—have received waivers from CMS to exclude the benefit, and are in different stages of evaluating the effect these waivers have on enrollees’ access to care.
- Indiana’s draft evaluation design describes plans to survey enrollee and provider experiences to assess any effect from excluding the NEMT benefit.
- Iowa’s evaluation largely found comparable access between enrollees with and without the NEMT benefit; however, it also found that newly eligible enrollees beneath the federal poverty level tended to need more transportation assistance or have more unmet needs than those with higher incomes.
Officials from the groups that GAO interviewed identified potential implications of excluding the NEMT benefit, such as a decrease in enrollee access to services and an increase in the costs of coverage. For example, nearly all of the groups indicated that excluding the NEMT benefit would impede access to services, particularly for those living in rural areas, as well as those with chronic health conditions.”
GAO 16-238 Nonemergency Medical Transportation: Updated Medicaid Guidance Could Help States
http://www.gao.gov/products/GAO-16-238
Findings: “The nonemergency medical transportation (NEMT) benefits offered by Medicare and Medicaid differ. Medicare provides NEMT via ambulance only when other means of transportation, such as a taxi or wheelchair van, would jeopardize the health of the beneficiary. Medicaid
NEMT is generally available for beneficiaries who have no other means of transportation to medical services. States are responsible for the daily operations of their Medicaid programs and have discretion in how they deliver NEMT. Officials from 15 selected states reported using a variety of models to administer NEMT, including transportation brokers, which are entities that contract with states to administer NEMT services.
The Centers for Medicare & Medicaid Services (CMS), within the U.S. Department of Health and Human Services (HHS), oversees Medicare and Medicaid at the federal level, but this oversight varies by program. CMS generally uses regular program integrity activities—such as claims reviews—to oversee Medicare NEMT. Under Medicaid, CMS also uses regular oversight activities, and these include overseeing states’ program integrity activities and periodically issuing guidance. However, some of CMS’s guidance is outdated or may be of limited use because of legislative and other changes that affect Medicaid and states’ NEMT programs. For example, a 1998 guidebook on NEMT contains outdated information on implementing NEMT transportation broker programs. Other more recent guidance is targeted for patients and providers rather than state Medicaid programs. However, these programs also benefit from updated guidance on strategies to ensure compliance with federal requirements while incorporating current practices to meet beneficiaries’ needs. Guidance for state Medicaid programs is particularly important because NEMT is at high risk for fraud and abuse; some selected states and stakeholders GAO interviewed reported that updated guidance could be helpful. Standards for Internal Control in the Federal Government states that management should ensure adequate means of communicating with stakeholders. Effective communications can take many forms, including guidance. CMS officials reported that the agency is considering assessing whether additional NEMT guidance is needed, but has not set time frames for conducting this assessment.
GAO identified four types of challenges related to Medicaid NEMT and several steps taken by states to address some of these challenges. Challenges reported related to containing costs, maintaining program integrity, contracting with and overseeing vendors, and accessing NEMT. For example, states reported challenges containing NEMT costs due to increased NEMT utilization and reported implementing practices to help address these challenges. Such practices include setting fixed provider reimbursement fees that remained relatively constant in recent years. Officials from 7 of the 15 selected states and 6 stakeholders GAO interviewed reported that having information on how states administer NEMT and ways to address challenges could be helpful to states. Some of this information is available; for example, CMS reported collecting information on states’ approaches through state Medicaid plans and posting this information on CMS’s web-
site. Other organizations, such as the Transit Cooperative Research Program, have or are in the process of collecting such information.”
TCRP Synthesis 119 Use of Taxis in Public Transportation for People with Disabilities and Older Adults
http://onlinepubs.trb.org/Onlinepubs/tcrp/tcrp_syn_119.pdf
“The objective of the synthesis is to report on current practices, trends, advantages, and challenges of public transit agencies’ use of taxis to provide service for people with disabilities and older adults. Public transit agencies are increasingly interested in the use of taxis to serve their riders with disabilities and older adults. Factors contributing to the interest in taxis include the high cost of more traditional small bus and van service particularly for ADA paratransit service, economic strain on public budgets, and the advancement of technology to monitor and verify subsidized taxi trips. As communities and their public transit agencies explore the use of taxis for public transportation, there are lessons to be learned from those who sponsor and subsidize taxi programs for people with disabilities and older adults.”
TCRP Report 173 Improving Transit Integration Among Multiple Providers: Volume 1
http://onlinepubs.trb.org/onlinepubs/tcrp/tcrp_rpt_173v1.pdf
“The purpose of this Manual is to provide guidance to transit agencies; planning organizations; local, regional and state governments; and the array of organizations that are impacted by transit service or have a stake in the provision of transit service, based on the research presented in TCRP Report 173, Volume II.
The research shows that transit integration among multiple transit providers is not necessarily easy, but it is successfully practiced in regions around North America and around the world and yields significant benefits in the communities where it occurs. These anticipated benefits have led some regions to work toward integration of services to create a more seamless system in terms of how riders pay for fares, transfer between routes, and access information about what is available. Indeed, most transit riders do not think of travel in terms of jurisdictional boundaries or agency ownership, but in terms of origins and destinations. Successful integration can create a network that feels unified to the rider.”
National Academy of Sciences Empirical Redefinition of Comprehensive Health and Well-Being in the Older Adults of the United States
http://www.pnas.org/content/early/2016/05/10/1514968113.full.pdf
“The World Health Organization (WHO) defines health as a ‘state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.’ Despite general acceptance of this comprehensive definition, there has been little rigorous scientific attempt to use it to measure and assess population health. Instead, the dominant model of health is a disease-centered Medical Model (MM), which actively ignores many relevant domains. In contrast to the MM, we approach this issue through a Comprehensive Model (CM) of health consistent with the WHO definition, giving statistically equal consideration to multiple health domains, including medical, physical, psychological, functional, and sensory measures. We apply a data-driven latent class analysis (LCA) to model 54 specific health variables from the National Social Life, Health, and Aging Project (NSHAP), a nationally representative sample of U.S. community-dwelling older adults. We first apply the LCA to the MM, identifying five health classes differentiated primarily by having diabetes and hypertension. The CM identifies a broader range of six health classes, including two ‘emergent’ classes completely obscured by the MM. We find that specific medical diagnoses (cancer and hypertension) and health behaviors (smoking) are far less important than mental health (loneliness), sensory function (hearing), mobility, and bone fractures in defining vulnerable health classes. Although the MM places two-thirds of the U.S. population into “robust health’ classes, the CM reveals that one-half belong to less healthy classes, independently associated with higher mortality. This reconceptualization has important implications for medical care delivery, preventive health practices, and resource allocation.”
AARP Weaving It Together: A Tapestry of Transportation Funding for Older Adults
http://www.aarp.org/content/dam/aarp/research/public_policy_institute/liv_com/2013/weaving-it-together-report-transportation-funding-for-olderadults-AARP-ppi-liv-com.pdf
“This paper highlights the major sources of federal funding that providers can tap to fund transportation for these populations. As there is no comprehensive dataset that tracks state and local expenditures on specialized transportation, the authors have included seven case studies of local providers from around the country to illustrate how they combine federal, state, and local funding to put quality service on the street. The paper also provides examples of how local and state coordination efforts can expand the reach of services funded.”
AARP Policy Options to Improve Specialized Transportation
http://assets.aarp.org/rgcenter/ppi/liv-com/i39-specialized-transportation.pdf
“The congressional authorization of the surface transportation law, coupled with the growing demand for specialized transportation, presents an opportunity to improve the services targeted to Americans with mobility limitations caused by age, disability, or income constraints. Improvements would allow more of these vulnerable citizens to live in the settings of their choice, including their own homes and communities, and to access employment opportunities in the suburbs that are not well served by public transportation. Given this historic opportunity, the AARP Public Policy Institute is publishing this paper to
- describe specialized transportation, and how it is funded and delivered;
- highlight emerging best practices; and
- offer policy options for improving specialized transportation.”
AARP Expanding Specialized Transportation: New Opportunities Under the Affordable Care Act
http://www.aarp.org/content/dam/aarp/ppi/2015/AARP-New-ACATransportation-Opportunities.pdf
“Many states are taking advantage of new options within the Affordable Care Act (ACA) to improve access to care for the chronically ill and to promote community living for older adults and adults with physical disabilities. However, relatively few states are expanding transportation services through these new initiatives for low-income people with mobility limitations. This paper explores the ACA options that could expand specialized transportation for Medicaid and Medicare beneficiaries, and for people who are dually eligible for both forms of coverage. It also provides state examples and two case studies to illustrate how these options can work.”
CTAA Transit Planning 4 All: Inclusive Transportation Planning Grantee Case Studies
http://web1.ctaa.org/webmodules/webarticles/anmviewer.asp?a=3265
“The mission of this project, sponsored by the U.S. Department of Health and Human Services’ Administration for Community Living is to demonstrate the value that inclusive processes can bring to transportation efforts.
The Community Transportation Association of America, in partnership with Easterseals, National Association of Area Agencies on Aging, and Westat, is developing, testing and demonstrating ways to empower people with disabilities and older adults to be actively involved in designing and
implementing coordinated transportation systems. Our goal is to support communities nationwide in adopting sustainable, scalable, and replicable models that include participation of people with disabilities and older adults in the design and implementation of responsive, coordinated transportation systems.”
FTA Rides to Wellness
http://nationalcenterformobilitymanagement.org/rides-to-wellness-home
“The goals of the ‘Rides to Wellness’ initiative are to:
- increase access to care,
- improve health outcomes, and
- reduce health care costs.
Through this initiative the transportation community will become a recognized partner with the health/wellness and medical community. This initiative will demonstrate how partnerships across the transportation and health industries can reduce health care costs by leveraging public transportation assets.”
Smart Growth America Metrics for Transportation Investments That Support Economic Competitiveness, Social Equity, Environmental Stewardship, Public Health, and Livability
http://www.smartgrowthamerica.org/documents/mndot-working-paper-1august-2014.pdf
“This working paper provides a new framework for evaluating transportation projects in Minnesota based on established and emerging practices in the field of public sector teturn on investment (ROI). The working paper is organized around the following chapters:
Chapter 2: Project Purpose and Scope. This chapter describes the context and purpose for Transportation ROI including its relationship to previous and ongoing Minnesota Department of Transportation (MnDOT) work. Ultimately this study may provide direction for implementing a broad based ROI process that helps inform MnDOT’s policy and budget decisionmaking.
Chapter 3: Transportation ROI Categories and Metrics. This chapter provides an overview of well-established and emerging approaches to measuring ROI for transportation projects and programs that go beyond safety and system performance. The general categories addressed include
- Economic Competitiveness
- Social Equity
- Environmental Stewardship
- Public Health
- Livability
Chapter 4: Project/Program Selection and Analysis. This chapter considers various options for selecting an appropriate and manageable subset of MnDOT projects and programs that can best serve as a template to test the utility of ROI analysis going forward. It includes a preliminary description of candidate projects/programs followed by a discussion of various options for narrowing the analysis.
Chapter 5: Next Steps. This chapter solicits input from the Project Stakeholder Group (PSG) related to the overall purpose, content, and application of the ROI framework for MnDOT. It also provides a summary of the next steps in this study effort in terms of future meetings and related research and deliverables.”
Economic and Planning Systems Draft Memo on Analysis of Return-On-Investment (ROI) Practices in the United States
http://www.epsys.com/wp-content/uploads/2014/08/ROImm0117214.pdf
“This memorandum is designed to support legislative and other policy initiatives in the State of Washington that advance the effective use of return on investment (ROI) analysis for prioritizing transportation investments. It has been prepared by Economic & Planning Systems (EPS) to support Smart Growth America’s ongoing efforts to help states implement innovative transportation initiatives that maximize the benefits of transportation expenditures and grow economies. The analysis is based on a review of national practices and case studies of innovative strategies being employed and various levels of government.”
Reports Under Way or Planned for the Future
TCRP B-44 Examining the Effects of Separate Nonemergency Medical Transportation Brokerages on Transportation Coordination
http://apps.trb.org/cmsfeed/TRBNetProjectDisplay.asp?ProjectID=3541
“The research is nearing completion. The final draft report is expected spring 2016.”
“The objectives of this research are to present options for providing Medicaid-funded NEMT services and evaluate the effects of different options for providing NEMT on: (1) access to Medicaid services; (2) human services transportation (in particular, coordinated transportation services); and (3) public transit services, including ADA complementary paratransit services. The key audiences for this research include state-level policy makers and program administrators and other stakeholders affected by the different options for providing NEMT services.”
TCRP B-45 Transportation to Dialysis Centers: Health/Transportation Policy Intersection
http://apps.trb.org/cmsfeed/TRBNetProjectDisplay.asp?ProjectID=4116
RFP closed 07-13-2016.
“The objectives of this research are to quantify the current and projected demand and associated costs of transportation for kidney dialysis in the United States and identify current effective practices and new strategies for funding and providing transportation for dialysis. The research should address a number of important areas and answer the critical questions presented below. This research should consider and address differences that affect transportation for kidney dialysis in urban and rural areas.”
Health Outreach Partners Rides to Wellness Community Scan
https://outreach-partners.org/about-hop/transportation-initiative
“Will quantify financial impacts of missed appointments.
- National Survey: Implementation of a national survey of health centers, Veterans Affairs Medical Centers, and private providers to identify the impact of lack of transportation on health care costs. Key partners include the FTA, the Veterans Health Administration, and UnitedHealthcare.
- Community Profiles: Development of profiles illustrating local communities that are adopting transportation solutions that show promising opportunities for return on investment.”
Center for Medicare & Medicaid Innovation Accountable Health Communities Model
https://www.grantsolutions.gov/gs/preaward/previewPublicAnnouncement.do?id=55237
Applications for the Accountable Health Communities (AHC) grant closed in late May 2016. In early 2017, grantees will be announced. The “AHC model addresses a gap in the current delivery system by funding
interventions that connect community-dwelling beneficiaries with community services. The AHC model will test three community-focused interventions of varying intensity and their ability to impact total health care costs and inpatient and outpatient health care utilization. This model will engage community-dwelling Medicare and Medicaid beneficiaries of all ages (children and adults).” One of the five focus areas is “transportation needs beyond medical transportation.”
Center for Medicare & Medicaid Innovation Health Care Innovation Awards
https://innovation.cms.gov/initiatives/Health-Care-Innovation-Awards/Project-Profiles.html
https://innovation.cms.gov/initiatives/Health-Care-Innovation-Awards/Round-2.html
“The Health Care Innovation Awards are funding up to $1 billion in awards to organizations that are implementing the most compelling new ideas to deliver better health, improved care and, lower costs to people enrolled in Medicare, Medicaid, and Children’s Health Insurance Program (CHIP), particularly those with the highest health care needs.
The Health Care Innovation Awards Round Two are funding up to $1 billion in awards and evaluation to applicants across the country that test new payment and service delivery models that will deliver better care and lower costs for Medicare, Medicaid, and/or CHIP enrollees.”
Reports are available for Round 1 projects, and Round 2 evaluation reports should be available soon.
Tools and Resources
Children’s Fund Health Transportation Shortage Index
http://www.childrenshealthfund.org/publications/health-transportation-shortage-index-new-tool-identify-underserved-communities
“The HTSI is based on data from a national survey and a regional survey done in the rural Mississippi Delta. The national data show that each year 9 percent of children in families with income less than $50,000 (4 percent of children overall) missed at least one health care appointment annually because transportation was not available. In the regional survey, 10 percent missed a health care appointment because of lack of transportation. In both surveys, nearly one-third of these children later used a hospital emergency department for the condition associated with the missed appointment.
The national survey included a question asking parents if they had difficulty establishing a usual source of pediatric care. A positive response to this was used to identify families with problems accessing child health care services, because difficulty establishing a usual source of care is associated with higher rates of hospital emergency department use for routine illnesses. In the national survey, difficulty establishing a usual source of care was significantly associated with: (1) rural area, (2) low income, (3) longer travel distance to source of care (especially noted in rural areas), and (4) lack of public transportation. In the regional survey, it was associated with not having a car.
Children’s Health Fund developed the HTSI to serve as a tool to guide users in the assessment of the most important factors associated with transportation barriers to child health care access. The HTSI factors are: (1) population as a proxy for rural area and for travel distance; (2) poverty as a proxy for automobile ownership; (3) public transportation availability; and (4) health care provider workforce availability. Points are assigned for each factor based on area characteristics and are added together. Higher scores indicate greater risk for transportation barriers to child health care access.
To overcome these barriers, targeted communities should be prioritized for additional public transit resources and/or improved coordination between health care and transportation providers. Some potential strategies are suggested at the end of this report.”
Community Commons
http://www.communitycommons.org
“Community Commons is a place where data, tools, and stories come together to inspire change and improve communities. We provide public access to thousands of meaningful data layers that allow mapping and reporting capabilities so you can thoroughly explore community health.
As a mission-driven organization, the technology and resources that we develop directly provide innovation for the future. We aim to make our custom tools publicly available whenever possible and our partners understand and support this public-good mission.”
National Aging and Disability Transportation Center
http://www.nadtc.org
“To ensure that community transportation services are available to everyone, particular attention should be paid to the needs and preferences of older adults and people with disabilities.
A community’s ‘family of mobility/transportation options’ may include walking, biking, driving, and transitioning from driving, as well as fixed-route public transit, dial-a-ride services, volunteer transportation programs, taxis, and other shared-ride options. In addition, mobility management, one-call/one-click transportation resource centers, and travel training offer person-centered information and assistance that facilitate access to community transportation options.
To accommodate the unique issues older adults and people with disabilities face in accessing and using transportation options, NADTC promotes:
- Engaging older adults and people with disabilities before new transportation options are created and using their insights and experiences to improve transportation programs, design new program,s and ensure that services are of the highest quality.
- Ensuring that older adults and people with disabilities know about the transportation choices available in their community and understand how to access these options.
- Offering one-on-one assistance to assist older adults and people with disabilities to select the best transportation options to meet their needs and use the transportation options available in the community.
- Providing safe, efficient, predictable, and reliable transportation services that older adults and people with disabilities are comfortable using.
- Following the ADA to ensure that people with disabilities are able to stay connected to their communities.”
INTERVIEWEES
| Name | Agency |
|---|---|
| Suzanne Alewine |
Missouri Rural Health Association |
| Dr. Chisara Asomugha |
Center for Medicare & Medicaid Innovation |
| Erin Barbaro |
Institute for People, Place, and Possibility |
| Chris Barnett |
Community Commons |
| Diane Barr |
Cascade Health Alliance |
| Ed Benning |
Mass Transportation Authority, Flint, MI |
| Dr. Julie Bershadsky |
Human Services Research Institute |
| Doris Boeckman |
Community Asset Builders |
| Carrie Brown |
National Indian Justice Center |
| Amy Carmola |
United Way of Chittenden County |
| Charles Carr |
Mississippi DOT |
| Kathryn Chandler |
Northwest Valley Connect, AZ |
| Linda Cherrington |
Texas A&M Transit Mobility Program |
| Mary Comtois |
United Way of Buffalo and Erie County, Buffalo, NY |
| Dave Cooley |
OR Department of Veterans Affairs |
| Troyce Crucchiola |
patient advocate, OR |
| Dr. Moumita Dasgupta |
Amherst College |
| Kelly Dixon |
Greater Buffalo Niagara Regional Transportation Council |
| Virginia Dize |
National Aging and Disability Transport Center |
| Esther Dyson |
Way to Wellville |
| Jenna Estock |
Primary Health Network |
| David Faldmo |
Siouxland Community Health Center |
| Kathy Gale |
Interfaith Senior Programs, Inc., Waukesha, WI |
| Cheryl Goldstone |
Primary Health Network |
| Oscar Gomez |
Health Outreach Partners |
| Roy Grant |
Children’s Health Fund (formerly) |
| Yahaira Graxirena |
Central Mass Regional Planning Commission |
| Tabatha Harris |
Oklahoma State University, Southern Plains TTAP Center |
| Jeff Hazen |
Sunset Empire Transportation |
| Robert Hicks |
Pyramid Lake Paiute Tribe, Transportation Planning Department |
| Joshua Jinks |
Finger Lakes Performing Provider System, Rochester, NY |
| Dennis Johnson |
Children’s Health Fund |
| Angie Jones |
Grant County Transit, Oregon |
| Judith Kell |
Lakeshore Mercy Health, MI |
| Nancy Knopf |
Care Oregon |
| Dr. Alana Knudson |
Walsh Center for Rural Health Analysis at NORC |
| Dr. Katherine Kortum |
Transportation Research Board |
| Francois Larrivee |
Hopelink Brokerage, WA |
| Valerie Lefler |
Liberty System, Data & Collaboration |
| Doris Lookabill |
OmniRide, VA |
| Kris Lyon |
Lane Transit District, OR |
| Heather MacLeod |
U.S. General Accounting Office |
| Janet Malley |
Whatcom Transportation Authority |
| Randee Mason |
PYA Consulting |
| Kelly Myers |
National Indian Justice Center |
| Melanie Needle |
Chittenden County Regional Planning Commission |
| Alex Page |
Ride Connection |
| Ross Peterson |
GridWorks, Portland, OR |
| Robin Phillips |
National Rural Transit Assistance Program |
| Dennis Presley |
Southern Illinois University Center for Rural Health and Social Service |
| Amy Rauworth |
Lakeshore Foundation, Birmingham, AL |
| Dr. Marie Raven |
University of California San Francisco Medical Center |
| Julia Resnick |
American Hospital Association |
| David Riley |
Veterans Health Administration |
| Todd Robinson |
WSOS Community Action Commission, Inc., Fremont, OH |
| Mark Tadder |
CitiCare |
| Frank Thomas |
Northeast Oregon Public Transit, OR |
| Dan Schwanz |
Greater Oregon Behavioral Health, Inc. |
| Dr. Judy Shanley |
Easterseals |
| Rev. Sally Jo Snyder |
Consumer Health Coalition, PA |
| John Sorensen |
Centers for Medicare & Medicaid Services; Money Follows the Person |
| Maria Sotnikova |
Atlanta Regional Commission |
| Kelsey Walter |
National Association of States United for Aging and Disability |
| Jade Warren |
Access2Care |
| Eric Weakly |
Administration for Community Living |
| Elaine Wells |
Ride Connection, Portland, OR |
| Dace West |
Mile High Connects |
| Julie Wilcke |
Ride Connection, Portland, OR |
| Sally Wilson |
Project Access of Durham County, Durham, NC |
| Shirley Wilson |
Mississippi DOT |
| Chris Zeilenger |
Community Transportation Association of America |






























































