
7
Connecting Patients to Transportation: Incentives and Return on Investment
The last panel of the workshop included several examples of current solutions for connecting patients to transportation. Valerie Lefler, the president and chief executive officer of Liberty Mobility Now, Inc., described Liberty Connect and Liberty Now, two customer-based transportation solutions that work together to facilitate trips. Alex Page, the lead transportation planner for Ride Connection in Portland, Oregon, discussed a dialysis transportation pilot project as an example of linking accessible, responsive transportation with individual and community needs. David Riley, the director of the Veterans Transportation Program at the U.S. Department of Veterans Affairs (VA), provided an overview of the Veterans Health Administration (VHA) travel authorities, which allow for transportation for the purposes of examination, treatment, or care.
The presentations were followed by comments from discussants Virginia Dize, the co-director of the National Aging and Disability Transportation Center at the National Association of Area Agencies on Aging (n4a); Ed Christopher, an independent consultant formerly with the Federal Highway Administration; and Joseph Cronin, the John R. Kerr Research Chair in Marketing in the Department of Marketing, and co-director of the Marketing Institute at the College of Business at Florida State University. The session was moderated by Marsha Regenstein, a professor in the Department of Health Policy at George Washington University. (Highlights are presented in Box 7-1.)
LIBERTY
During the time that Lefler was studying public transportation in the state of Nebraska, there were 58 Federal Transit Authority (FTA) Section 5311 rural public transit providers and almost 90 FTA Section 5310 (seniors and individuals with disabilities) public transportation providers, and numerous challenges to mobility were identified. There were some counties with no transit service at all, Lefler said. There were county/city jurisdictional barriers and challenges with coordinating schedules and pricing. Adding vehicles to increase capacity could take up to 2 years, she noted. There was limited night and weekend service and few options for paratransit service, and urban taxis were traveling to communities 200 to 300 miles away to provide service (charging regular taxi rates). Research also showed that there was a limited awareness of transit service.
Lefler and her colleagues sought to create a customer-based transporta-
tion solution that would optimize existing resources, use community-based staffing, plug in mobility options where needed, and be affordable and quick to implement. The technology would need to be able to function under conditions found in rural communities (e.g., low Internet connection bandwidth) and to work on any technology platform (e.g., iOS, Android, PC, etc.). They ultimately developed two solutions, Liberty Connect and Liberty Now.1 Liberty Connect uses a Software as a Service model that connects customers, transit agencies, and human service, medical, and care agencies. Liberty Now is an advanced centralized call center staffed by mobility managers using intelligent transportation systems.
Liberty Connect
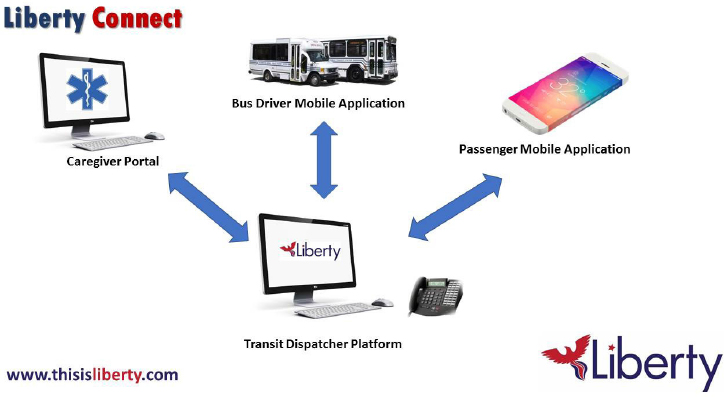
Liberty Connect is designed for agencies providing transportation service under FTA Section 5311 and 5310 programs and also for nonprofits. Liberty Connect includes a caregiver portal, a bus driver mobile application, and a mobile application for passengers, all connected to a transit dispatcher platform (see Figure 7-1).
The transit dispatcher dashboard shows the geographic information system (GIS) location of all vehicles currently in service. The dashboard also shows if a vehicle needs maintenance, based on a daily inspection checklist. Lefler emphasized that she and her team sought to make the platform intuitive and straightforward to use. All of the transportation requests, whether from the caregiver portal, the passenger mobile application, or the local call-in dispatcher, go into a pending request list. The transportation dispatcher at the local agency maintains control of the system. There is also a reporting function, including driver logs by day, week, month, and quarter; revenue miles; non-revenue miles; deadhead time (driving without a passenger); and passengers.
The caregiver portal allows the agencies (e.g., hospitals, doctors’ offices, nursing homes, assisted living facilities, community action agencies, etc.) to book transportation and track rides. The portal also provides flexible billing options and reporting and helps reduce stress on the agency and improve client transportation. The provider’s office can see who is coming for their appointments and where they are. The portal also allows the office to contact the driver when the patient is ready to be picked up to go home.
The bus driver mobile application works on iOS and Android mobile
___________________
1 Integrated Global Dimensions is the parent company that developed Liberty. Funding for research and development has come from the U.S. Department of Transportation, the Federal Transit Administration, and the Small Business Administration. The Texas Department of Transportation, NMotion, and Invest Nebraska have provided venture capital support. For more information see http://thisisliberty.com (accessed August 4, 2016).
SOURCE: Lefler presentation, June 7, 2016.
platforms, and it allows drivers to see details about their trips for the day. Drivers can enter updates at each step of the trip (e.g., passenger picked up, trip completed), and GIS data are pulled every 3 seconds, providing the place and time of each event that is happening. These data provide useful customer service information for reporting purposes, Lefler noted. They also allow for update notifications to the individuals using the passenger mobile application.
The passenger mobile application is very simple, Lefler said, comparing it to the applications used by Uber or Lyft. Passengers can see their upcoming trips and receive notifications.
Liberty Connect was launched in June 2016 and is currently being used in Scotts Bluff, Nebraska. Lefler said that it will be expanded to several new sites in the coming months, and additional functions will be added (e.g., credit card payment processing, customer satisfaction ratings, automated ticket tracking).
Liberty Now
Liberty Now is designed for nonemergency medical transportation (NEMT), nonmedical transportation, statewide and regional mobility management, and community hospital access to care centers. It is a centralized call center with dedicated mobility managers who search for the best solu-
tion for each individual, including public transit options, nonprofit service agencies, Liberty drivers, taxis, Uber or Lyft, volunteer drivers, and family members. Local Liberty mobility managers are hired from the community, so they know the micro-cultures and the roads, Lefler said, and Liberty drivers are independent contractors. Taking lessons from the railroads and the shipping and logistics industries, Lefler and colleagues designed intelligent transportation systems to collect and use data to track high-priority, high-vulnerability transports (e.g., dialysis patients, individuals in the late stages of Alzheimer’s disease) to make sure they arrive where and when needed. There is sophisticated trip scheduling technology and automated booking and routing. The emphasis is on using data to monitor customer service, identify gaps and opportunities, and improve passenger, caregiver, provider, and driver satisfaction.
Local Liberty mobility managers conduct local driver recruitment, screening, and training; follow up on customer service interventions if concerns are reported; and provide customer service and education. They gather constant business intelligence about mobility options. The Mobility Champions Circle includes local individuals and consumer advocates who work together to keep everyone apprised of any changes in options (e.g., rates, routes, and schedules of local public transportation agencies, which change frequently). Mobility managers also serve as emergency drivers of last resort. Lefler added that there is a launch team available to assist the Local Liberty mobility managers over the first 90 days, including a logistics specialist, a community engagement specialist, and a marketing strategist.
Liberty drivers are members of the local community, and they set their hours and service area on a weekly basis. Lefler added that the majority of trips are prescheduled. Customer service training, cardiopulmonary resuscitation, first aid, and lap belt training are required. Liberty drivers use their personal vehicles, which must be clean and well maintained, and are subject to random vehicle inspections. Drivers must also to pass a strict background check, including fingerprinting, driver’s license check, and vehicle title inspection. Lefler said that 80 percent of the ride fare stays in the community, paid to the local driver (the other 20 percent pays for Liberty infrastructure). This is very important in rural economic regions where there are very few part-time jobs, she said.
The two solutions now work together, and the Liberty Now automated or manual trip request appears in the Liberty Connect transit manager’s dispatch log, Lefler said in conclusion.
RIDE CONNECTION
Ride Connection is a nonprofit transportation provider in the Portland, Oregon, region that helps link accessible, responsive transportation with
individual and community needs, Page said. The vision is to create independence and community connectors through travel options. Ride Connection services include demand response (eg., curb-to-curb, door-to-door, door-through-door) using volunteer and paid drivers; community connectors (i.e., first-mile/last-mile connectors); shopping shuttles for seniors; travel training; and fare relief. Ride Connection also partners with more than 30 organizations in the Portland metropolitan area, providing resources such as driver training (e.g., lift operation, blood-borne pathogen training) and providing vehicles owned by Ride Connection.
Dahlia Dialysis Transportation Pilot
Page described the Dahlia Dialysis Transportation Pilot project as an example of a Ride Connection program. The project was funded by the Administration for Community Living, in partnership with the Community Transportation Association of America, Easterseals, and the n4a. The planning process was very inclusive, involving stakeholders, an advisory committee, focus groups, one-on-one interviews, caregiver surveys, patient surveys, a workshop, and workgroups. Months were spent researching the needs of the community, the clinics, and the transportation providers. Page said that dialysis patients are frequently asked to fill out surveys, and a common complaint is that they never hear back on the results of the survey. As part of this project, patients and clinic workers were provided with feedback throughout the process, he said. Patients and providers identified a variety of barriers to patient transport to and from dialysis, including the frequency of visits, the costs, scheduling, the special care needed, and the inflexibility of transportation providers.
Several community resource ideas emerged out of the planning process, Page said, all of them focused on education and volunteer recruitment. It was found that there was a lack of understanding among the transportation providers and the public of what dialysis is and what accommodations patients might need. For example, drivers had no idea that patients were in discomfort or pain and that they might be taking speed bumps too quickly for a patient’s comfort. Clinics did not understand the transportation options available to them. They knew them by name and phone number, but they were not advocates for the patients. To deal with these issues, the project included education for the transportation providers (i.e., classroom and online training, a video, patient dialogue) and outreach to the clinics. Page shared a clip from a video that is part of a full-day training program.2 The training has been very effective, he said, adding that some
___________________
2 The video is available at https://rideconnection.org/services/additional-programs/dahlia (accessed August 4, 2016).
transportation providers are giving their employees a small hourly wage increase to incentivize participation in the training.
From the inclusive planning process, Ride Connection implemented a pilot project with elements and changes designed to improve the effectiveness of transportation for dialysis patients. Elements of the pilot included, for example, a dedicated dispatcher, collaboration with partners, no costs to patients, allowing shared rides, training, and constant communication. A critical aspect of the pilot, Page said, is a quarterly assessment of the level of service for the patients.
Page reviewed the program costs, noting that the goal is not to be the cheapest ride, but to be the most appropriate ride for a dialysis patient. The average trip costs $16.32, which he suggested is low compared to other paratransit options. He said that the cost per ride has been increasing in recent months as the number of paid driver hours needed has increased. At the start, the project relied heavily on volunteer hours, but the number of volunteer hours has decreased over time, due in part to overworking of volunteers, slow recruitment, and having only one volunteer coordinator.
The ultimate goal is improved patient outcomes, and Page highlighted several key outcomes thus far. The majority of actual dialysis times more closely match the prescription times; missed appointments have decreased significantly; and patient health and quality of life have improved. Page acknowledged that quality of life is very difficult to assess, and the pilot relies on qualitative evidence from surveys. Patients have reported that the transportation project has improved their lives and that their stress is reduced by not having to worry about transportation.
Meanwhile, clinics are spending less time dealing with transportation issues, they have a better understanding of the transportation options for dialysis patients, and they are better advocates for their patients. All of this leads to saved time and money, Page said.
In closing, Page emphasized that collaboration is required for success and said that the educational component alone can help improve transportation. He cautioned against putting too much emphasis on financial return on investment; the focus should instead be a more holistic one, taking into account shared investments and shared values. Each stakeholder has different immediate needs, but all can agree to rally around better patient health outcomes. Going forward, Ride Connection is looking to replicate the dialysis transportation model with other chronic conditions and care facilities.
VETERANS TRANSPORTATION PROGRAM
The Veterans Transportation Program includes the Beneficiary Travel program, the Veterans Transportation Service, and the Highly Rural Trans-
portation Grants program. Riley focused his remarks on the VHA travel authorities that allow for transportation for the purposes of examination, treatment, or care.
The Beneficiary Travel program assists eligible veterans and other beneficiaries by offsetting the cost of their travel to VA and VA-authorized health care. Low-income and service-connected veterans are eligible for reimbursement for mileage or for third-party transportation. The Beneficiary Travel program costs were about $850 million in fiscal year 2015, and projected costs for fiscal year 2017 are about $924 million. A program of this size and visibility is frequently audited, and Riley said that errors in mileage reimbursement claim payments do occur. About 55 percent of enrolled veterans at the VA meet eligibility requirements for beneficiary travel. For the other 45 percent, the Veterans Transportation Service allows VA facilities to hire mobility managers, drivers, and ride schedulers as well as to purchase Americans with Disabilities Act (ADA)–compliant vehicles to transport beneficiaries to their health care appointments. However, Riley said, even with these two transportation authorities, there is a gap in coverage.
The Veterans Transportation Service was launched in 2010 with four sites, and today there are more than 100 sites participating (roughly two-thirds of the VA medical centers). This is not a mandatory program, Riley said, and uptake has required using metrics to convince leadership at VA hospitals that providing transportation is a good business decision.
One challenge is to demonstrate the sustainability of the Veterans Transportation Program. Although a few medical center directors will support anything that improves access, most need to see a benefit to their bottom line. If the program cannot pay for itself, Riley explained, directors will spend that money on other medical services and are likely to see transportation as a luxury. Since the inception of the Veterans Transportation Program, the program has collected data on trips and service miles; there have been more than 1 million trips, totaling more than 25 million service miles. One way to demonstrate value is to show how the Veterans Transportation Program offset costs from the $850 million Beneficiary Travel program. Costs are offset by intercepting some of the rides that would otherwise go to community providers. The mobility manager for the Veterans Transportation Program can compare the cost of using the set rate contract (for a third-party provider of a special mode of transportation) with the cost of using the VA’s own Veterans Transportation Program services. In addition, because the Veterans Transportation Program can transport more than one beneficiary at a time (e.g., in ADA-compliant vans), it is possible to also include veterans who are not beneficiary travel–eligible and transport them at the same time.
Another way to show value is to demonstrate a reduction in missed opportunities (e.g., missed appointments, cancellations made too late to
schedule another beneficiary in that time slot). Because the VHA has patient data from over the long term, it is able to demonstrate that transportation provided in a targeted manner can reduce missed opportunities. On an aggregate level, there has been about a 1 percent decrease in missed opportunities since the time before the implementation of the transportation program. The improvement was not uniform across facilities, Riley said, suggesting that it would be worthwhile to investigate why there is substantial improvement at some facilities and negative results at others. On an individual level, patients with high missed opportunity rates may be more likely to miss appointments because of transportation difficulties than patients with low missed opportunity rates, and perhaps the transportation program should be targeted at them.
Patient satisfaction is also used as a metric, and internal controls are used to demonstrate that the payments made are correct and that the services offered are for the appropriate population.
In closing, Riley highlighted several future needs. A longitudinal study is needed, he said, that includes specific subpopulations and focuses on quality of life and missed opportunities. Metrics are needed that include the degree of difficulty of the transport (e.g., rurality, traveler’s health condition, the need for enabling services). Riley suggested that the metrics should take into account the intended approach (i.e., access or cost offset). He also suggested that targeted resources are needed for sites focusing on special populations (e.g., the homeless and those with spinal cord injuries who are on dialysis or who have mental health issues). It is important to be able to demonstrate that these costly special populations are being served by the Veterans Transportation Service and that transporting them to care is saving money for the health care system in the long run. Transportation for patient flow is a potentially useful metric to consider (e.g., on-demand transport for discharged patients to reduce additional bed days of care). There is also a need for transportation for mental health 14-day follow-up visits, and Riley said that several VHA sites have shown that when transportation is provided, patients will come in for their follow-up appointments.
DISCUSSION
Following the presentations, participants continued the discussion of inclusive planning. Participants also expressed a range of opinions on how best to demonstrate the return on investment in health-related transportation in order to ensure the sustainability of programs, including the merits of sound economic arguments versus ethical and social arguments.
Inclusive Planning
The n4a has long had an interest in transportation, and its member Area Agencies on Aging around the country also consider transportation to be among their top priorities, Dize said. The National Aging and Disability Transportation Center is a partnership between n4a and Easterseals and is one of three federal transportation technical assistance centers funded by FTA. The center focuses on accessibility of transportation for older adults, people with disabilities of all ages, and family caregivers.
It is critically important, Dize emphasized, that individuals have access to information about the transportation that is available in their communities. The National Aging and Disability Transportation Center has a partnership with the Eldercare Locator, which provides information to older adults and caregivers about a wide variety of issues and resources. Transportation is the number one reason that people call the Eldercare Locator, Dize said, ranking above Social Security, Medicare, Medicaid, and other critical concerns. Between October 2015 and March 2016, the Eldercare Locator handled more than 16,000 calls on transportation issues, the majority of which were from older people who desperately needed a ride to medical services, Dize said.
It is also critically important to talk directly with the people who will be served by community transportation about what their needs are, Dize continued. Another way in which n4a is involved in transportation is through the Inclusive Coordinated Transportation Partnership Project, which is funded by the Administration for Community Living, and is being carried out in partnership with the Community Transportation Association of America and Easterseals. The project focuses on engaging older adults and people with disabilities in community transportation service planning. Dize said that Ride Connection (discussed above by Page) is one of the grantees. When considering return on investment, Dize said, it important to ensure that the investment being made is the “right” investment—that it is actually supporting the needs of people who are living in the community.
Page agreed and reiterated that the Dahlia Dialysis Transportation Pilot project focuses on providing the most appropriate ride, which is not necessarily the least expensive ride. Anyone whom Ride Connection partners with to provide rides receives training to ensure the highest levelof customer service. Page said he considers Ride Connection more as an advocate for the customer than a transportation provider. He added that the inclusive planning pilot project allowed Ride Connection to test its outreach capabilities and its ability to collaborate with multiple stakeholders and different interests and to work toward defining the shared value in the shared investment.
Lefler agreed with the importance of establishing shared goals at the start of a partnership and defining the population being served and the
desired outcomes. Working with the customer is the best way to determine what the goals are. Clearly defined goals are needed for monitoring progress on a regular basis and also for transparency. In establishing Liberty, eight focus groups were held to better understand the ecosystem in each environment. Participants included farmers, persons older than age 85, drivers, veterans, and other stakeholders. What is right in one community may be different from what is right in another community, Lefler said. Riley added that the Veterans Transportation Service also engages stakeholders in transportation to help guide the program.
Social Versus Economic Arguments in Demonstrating the Returns to Health from Investments in Transportation
There is stiff competition for limited transportation resources, Ed Christopher said, and Congress requires justification for the spending of public money to ensure that the money spent achieves a positive return. In assessing return on investment, Christopher said, it is important to carefully consider the questions that need to be answered as well as the metrics needed to answer them. He observed that return on investment is viewed differently by different stakeholders. For transportation access to care, he said, the questions revolve around whether the efforts are making people healthier.
Lefler noted that return on investment is difficult to ascertain in health care because it depends on illness, age, income level, and other factors of the many individuals involved. The ultimate question is whether quality of life is being improved. One of Liberty’s goals is to expand the ecosystem of transportation options. While the primary focus is on providing options to get to medical care, individuals might also find suitable options for visiting loved ones, for example, or for when driving themselves might not be a safe option for them. When making the business case to policy makers and legislators, the task is to show how transportation can be provided in the most efficient way possible. She agreed with Christopher that justifying the expense depends on the goals of the stakeholders.
Transportation is essential to quality of life, Riley agreed. He suggested that a long-term study using patient data and a quality-of-life scale could demonstrate the value of transportation, especially if that transportation was not limited to transport to medical care. From a business perspective, return on investment could be demonstrated by measuring the impact of transportation in those areas of health care that generate high costs. For example, can access to transportation eliminate the need to move an individual into a nursing home? Does access to transportation reduce the need for an extended inpatient hospital stay when discharge is possible? This is
a piecemeal approach, he acknowledged, but many such examples could make the case for investing in transportation.
Page emphasized that access to care is an equity issue as well and that people should not be denied health care because they cannot get to it. He suggested that there is a moral argument to be made as well, when justifying programs to Congress. Another participant agreed that there is a moral argument to be made for transportation to care, but said that it is economics that make the case for investment and that perhaps there is a moral imperative to make the economic case on behalf of those who are poor, marginalized, and disempowered.
Cronin highlighted the need for new and innovative cross-discipline research and stressed the need to “speak the language” of those you are trying to convince. He described some of his early work on return-on-investment calculations for medically related transportation services. One approach is to calculate cost avoidance (as a result of, for example, reduced ED visits, hospitalizations, or missed days of work). He said that much of the work at that time was based on assumptions about relationships between transportation and care (e.g., how many trips to care might correlate with avoidance of a 1-day in-hospital stay). He agreed that medical trips are about quality of life improvement, but he added that those controlling the funding (i.e., the tax dollars) want to show that they are generating a financial return. He encouraged participants to identify the economic benefits of getting people to care. These benefits range from eliminating missed appointments to keeping people out of the hospital. It is not making a profit, he emphasized—it is avoiding a cost, which can be a significant benefit for many businesses. Cronin encouraged participants from the health care field to engage business schools, which he said are willing to help.
A participant concurred with the need for a real collaboration between the transportation side and the health side. He acknowledged the challenges, including the fact that many in the health care field do not have an adequate understanding of the essential role of transportation assistance in getting people to care. He also agreed with the need to make a sound economic argument, but he suggested that the phrase “return on investment” is not ideal for this discussion. He noted the general aversion to viewing transportation to health care as a business model, but he asserted that there are financial savings to be realized when, for example, a child with asthma is well controlled in the primary care setting. One can compare the primary care visit and medication costs spent to the ED and hospitalizations avoided and demonstrate the return on investment.
Lefler agreed with the concept of demonstrating returns in terms of cost savings. She cited the example of using a Liberty driver who lives in
the community versus calling an urban taxi service to travel to a rural community. Page suggested thinking in terms of risk mitigation.
Riley also highlighted the need for a shared vocabulary and shared metrics that address concrete issues (i.e., established costs that can be intercepted or prevented). He called for both short- and long-term planning and suggested that there is an immediate need to demonstrate the business case to Congress and health and transportation leadership, to show them that investing in transportation to care is of value to them. Riley added that there is also the need for a long-term body of research that demonstrates improvement in quality of life and the impacts of prevention.
This page intentionally left blank.














