
3
The Root Causes of Health Inequity
Health inequity, categories and examples of which were discussed in the previous chapter, arises from social, economic, environmental, and structural disparities that contribute to intergroup differences in health outcomes both within and between societies. The report identifies two main clusters of root causes of health inequity. The first is the intrapersonal, interpersonal, institutional, and systemic mechanisms that organize the distribution of power and resources differentially across lines of race, gender, class, sexual orientation, gender expression, and other dimensions of individual and group identity (see the following section on such structural inequities for examples). The second, and more fundamental root cause of health inequity, is the unequal allocation of power and resources—including goods, services, and societal attention—which manifest in unequal social, economic, and environmental conditions, also called the social determinants of health. Box 3-1 includes the definitions of structural inequities and the social determinants of health.
The factors that make up the root causes of health inequity are diverse, complex, evolving, and interdependent in nature. It is important to understand the underlying causes and conditions of health inequities to inform equally complex and effective interventions to promote health equity.
The fields of public health and population health science have accumulated a robust body of literature over the past few decades that elucidates how social, political, economic, and environmental conditions and
context contribute to health inequities. Furthermore, there is mounting evidence that focusing programs, policies, and investments on addressing these conditions can improve the health of vulnerable populations and reduce health disparities (Bradley et al., 2016; Braveman and Gottlieb, 2014; Thornton et al., 2016; Williams and Mohammed, 2013). This literature is discussed below in the sections on structural inequities and the social determinants of health.
HOW STRUCTURAL INEQUITIES, SOCIAL DETERMINANTS OF HEALTH, AND HEALTH EQUITY CONNECT
Health inequities are systematic differences in the opportunities groups have to achieve optimal health, leading to unfair and avoidable differences in health outcomes (Braveman, 2006; WHO, 2011). The dimensions of social identity and location that organize or “structure” differential access to opportunities for health include race and ethnicity, gender, employment and socioeconomic status, disability and immigration status, geography, and more. Structural inequities are the personal, interpersonal, institutional, and systemic drivers—such as, racism, sexism, classism, able-ism, xenophobia, and homophobia—that make those identities salient to the fair distribution of health opportunities and outcomes. Policies that foster inequities at all levels (from organization to community to county, state, and nation) are critical drivers of structural inequities. The social, environmental, economic, and cultural determinants of health are the terrain on which structural inequities produce health inequities. These multiple determinants are the conditions in which people live, including access to good food, water, and housing; the quality of schools,
workplaces, and neighborhoods; and the composition of social networks and nature of social relations.
So, for example, the effect of interpersonal, institutional, and systemic biases in policies and practices (structural inequities) is the “sorting” of people into resource-rich or resource-poor neighborhoods and K–12 schools (education itself being a key determinant of health (Woolf et al., 2007) largely on the basis of race and socioeconomic status. Because the quality of neighborhoods and schools significantly shapes the life trajectory and the health of the adults and children, race- and class-differentiated access to clean, safe, resource-rich neighborhoods and schools is an important factor in producing health inequity. Such structural inequities give rise to large and preventable differences in health metrics such as life expectancy, with research indicating that one’s zip code is more important to health than one’s genetic code (RWJF, 2009).
The impact of structural inequities follows individuals “from womb to tomb.” For example, African American women are more likely to give birth to low-birthweight infants, and their newborns experience higher infant death rates that are not associated with any biological differences, even after accounting for socioeconomic factors (Braveman, 2008; Hamilton et al., 2016; Mathews et al., 2015). Although the science is still evolving, it is hypothesized that the chronic stress associated with being treated differently by society is responsible for these persistent differential birth outcomes (Christian, 2012; El-Sayed et al., 2015; Strutz et al., 2014; Witt et al., 2015). In elementary school there are persistent differences across racial and ethnic divisions in rates of discipline and levels of reading attainment, rates that are not associated with any differences in intelligence metrics (Howard, 2010; Losen et al., 2015; Reardon et al., 2012; Skiba et al., 2011; Smith and Harper, 2015). There also are race and class differences in adverse childhood experiences and chronic stress and trauma, which are known to affect learning ability and school performance, as well as structural inequities in environmental exposures, such as lead, which ultimately can lead to differences in intelligence quotient (IQ) (Aizer et al., 2015; Bethell et al., 2014; Jimenez et al., 2016; Levy et al., 2016). One of the strongest predictors of life expectancy is high school graduation, which varies dramatically along class and race and ethnicity divisions, as do the rates of college and vocational school participation—all of which shape employment, income, and individual and intergenerational wealth (Olshansky et al., 2012). Structural inequities affect hiring policies, with both implicit and explicit biases creating differential opportunities along racial, gender, and physical ability divisions. Lending policies continue to create differences in home ownership, small business development, and other asset development (Pager and Shepherd, 2008). Structural inequities create differences in the ability to participate and
have a voice in policy and political decision making, and even to participate in the arguably most fundamental aspect of our democracy, voting (Blakely et al., 2001; Carter and Reardon, 2014). And implicit biases create differential health care service offerings and delivery and affect the effectiveness of care provided, including a lack of cultural competence (IOM and NRC, 2003; Sabin et al., 2009).
For many people, the challenges that structural inequities pose limit the scope of opportunities they have for reaching their full health potential. The health of communities is dependent on the determinants of health.
STRUCTURAL INEQUITIES
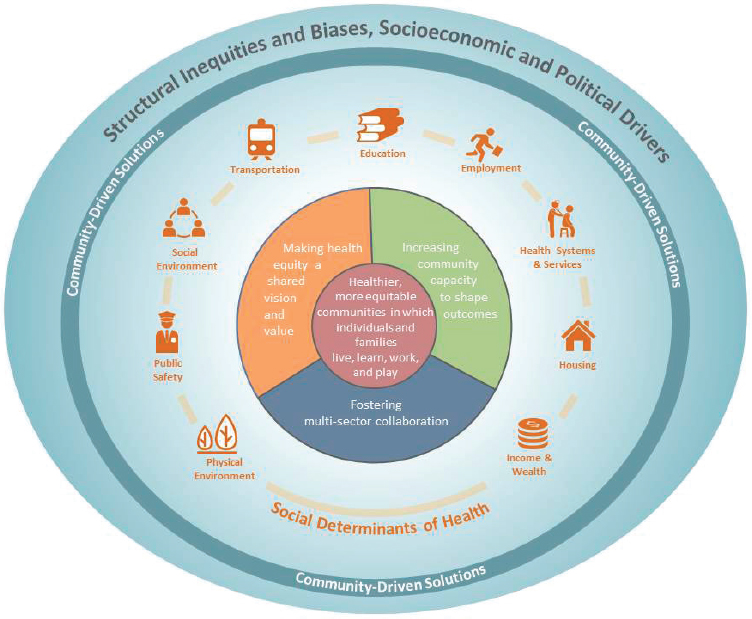
As described above, structural inequities refers to the systematic disadvantage of one social group compared to other groups with whom they coexist that are deeply embedded in the fabric of society. In Figure 3-1,
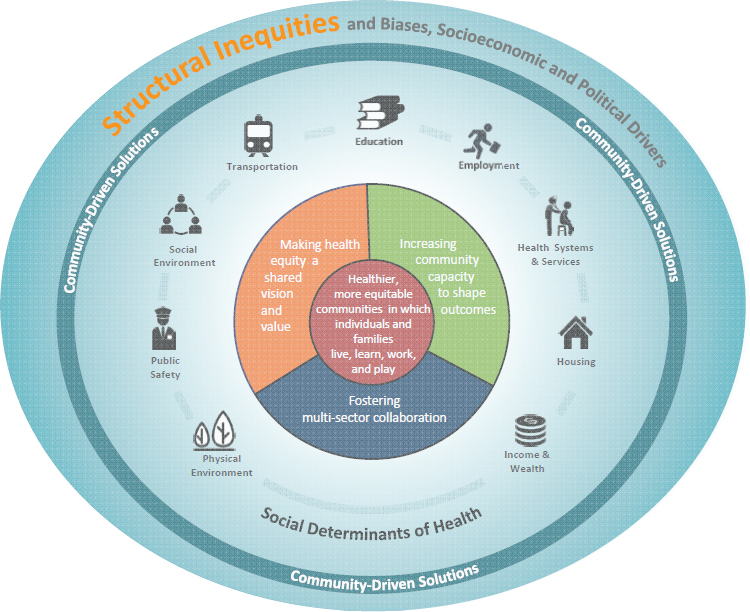
NOTE: Structural inequities are highlighted to convey the focus of this section.
the outermost circle and background indicate the context in which health inequities exist. Structural inequities encompass policy, law, governance, and culture and refer to race, ethnicity, gender or gender identity, class, sexual orientation, and other domains. These inequities produce systematic disadvantages, which lead to inequitable experiences of the social determinants of health (the next circle in the report model, which is discussed in detail later in this chapter) and ultimately shape health outcomes.
Historical Perspective and Contemporary Perceptions
Whether with respect to race, ethnicity, gender, class, or other markers of human difference, the prevailing American narrative often draws a sharp line between the United States’ “past” and its “present,” with the 1960s and 1970s marking a crucial before-and-after moment in that narrative. This narrative asserts that until the 1950s, U.S. history was shaped by the impacts of past slavery, Indian removal, lack of rights for women, Jim Crow segregation, periods of nativist restrictions on immigration and waves of mass deportation of Hispanic immigrants, eugenics, the internment of Japanese Americans, the Chinese exclusion policies, the criminalization of “homosexual acts,” and more (Gee and Ford, 2011; Gee et al., 2009). White women and people of color were effectively barred from many occupations and could not vote, serve on juries, or run for office. People with disabilities suffered widespread discrimination, institutionalization, and social exclusion.
Civil rights, women’s liberation, gay rights, and disability rights movements and their aftermaths may contribute to a narrative that social, political, and cultural institutions have made progress toward equity, diversity, or inclusion. Highlights of progress include the Civil Rights Act of 1964, the Voting Rights Act of 1965, the Fair Housing Act, Title IX of the Education Amendments of 1972, the Americans with Disabilities Act, the Patient Protection and Affordable Care Act, and, most recently, the Supreme Court case1 that legalized marriage equality in the United States. With a few notable exceptions—undocumented immigrants and Muslims, for example—these advances in law and policy have been mirrored by the liberalization of attitudes toward previously marginalized identity groups.
Today, polls and surveys indicate that most Americans believe that interpersonal and societal bias on the basis of identity no longer shapes individual or group social outcomes. For example, 6 in 10 respondents to a recent national poll said they thought the country has struck a
___________________
1Obergefell v. Hodges, 576 U.S. (2015).
“reasonable balance” or even gone “too far” in “accepting transgender people” (Polling Report, n.d.). In 2015, 72 percent of respondents, including 81 percent of whites, said they believe that “blacks have as good a chance as white people in your community to get any kind of job for which they are qualified” (Polling Report, n.d.). In another poll, a total of 72 percent agreed that “women and men have equal trouble finding good-paying jobs” (64 percent) or that men have more trouble (8 percent) (Ms. Foundation for Women, 2015). However, when broken down by racial and ethnic categories, the polls tell a different narrative. A recent survey revealed that 70 percent of African Americans, compared with 36 percent of whites, believe that racial discrimination is a major reason that African Americans have a harder time getting ahead than whites (Pew Research Center, 2016). Furthermore, African Americans (66 percent) and Hispanics (64 percent) are more likely than whites (43 percent) to say that racism is a big problem (DiJulio et al., 2015). Here, perceptions among African Americans and whites have not changed substantially; however, Hispanics are much more likely to now say that racism is a big problem (46 percent in 1995 versus 64 percent in 2015) (DiJulio et al., 2015).
Perceptions are confirmed by the persistence of disparities along the lines of socioeconomic position, gender, race, ethnicity, immigration status, geography, and the like has been well documented. Why? For one, historical inequities continue to ramify into the present. To understand how historical patterns continue to affect life chances for certain groups, historians and economists have attempted to calculate the amount of wealth transmitted from one generation to the next (Margo, 1990). They find that the baseline inequities contribute to intergenerational transfers of disadvantage and advantage for African Americans and whites, respectively (Chetty et al., 2014; Darity et al., 2001). The inequities also reproduce the conditions in which disparities develop (Rodriguez et al., 2015).
Racism
Though inequities may occur on the basis of socioeconomic status, gender, and other factors, we illustrate these points through the lens of racism, in part because disparities based on race and ethnicity remain the most persistent and difficult to address (Williams and Mohammed, 2009). Racial factors play an important role in structuring socioeconomic disparities (Farmer and Ferraro, 2005); therefore, addressing socioeconomic factors without addressing racism is unlikely to remedy these inequities (Kaufman et al., 1997).
Racism is an umbrella concept that encompasses specific mechanisms that operate at the intrapersonal, interpersonal, institutional, and systemic
levels2 of a socioecological framework (see Figure 3-2). Because it is not possible to enumerate all of the mechanisms here, several are described below to illustrate racism mechanisms at different socioecological levels. Stereotype threat, for example, is an intrapersonal mechanism. It “refers to the risk of confirming negative stereotypes about an individual’s racial, ethnic, gender, or cultural group” (Glossary of Education Reform, 2013). Stereotype threat manifests as self-doubt that can lead the individual to perform worse than she or he might otherwise be expected to—in the context of test-taking, for example. Implicit biases—unconscious cognitive biases that shape both attitudes and behaviors—operate interpersonally (discussed in further detail below) (Staats et al., 2016). Racial profiling often operates at the institutional level, as with the well-documented institutionalization of stop-and-frisk practices on Hispanic and African American individuals by the New York City Police Department (Gelman et al., 2007).
Finally, systemic mechanisms, which may operate at the community level or higher (e.g., through policy), are those whose effects are interactive, rather than singular, in nature. For example, racial segregation of neighborhoods might well be due in part to personal preferences and behavior of landlords, renters, buyers, and sellers. However, historically, segregation was created by legislation, which was reinforced by the policies and practices of economic institutions and housing agencies (e.g., discriminatory banking practices and redlining), as well as enforced by the judicial system and legitimized by churches and other cultural institutions (Charles, 2003; Gee and Ford, 2011; Williams and Collins, 2001). In other words, segregation was, and remains, an interaction and cumulative “product,” one not easily located in any one actor or institution. Residential segregation remains a root cause of racial disparities in health today (Williams and Collins, 2001).
Racism is not an attribute of minority groups; rather, it is an aspect of the social context and is linked with the differential power relations among racial and ethnic groups (Guess, 2006). Consider the location of environmental hazards in or near minority communities. Placing a hazard in a minority community not only increases the risk of adverse exposures for the residents of that community, it also ensures the reduction of risk for residents of the nonminority community (Cushing et al., 2015; Taylor, 2014). Recognizing this, the two communities could work together toward an alternative that precludes having the hazard in the first place, an alternative that disadvantages neither group.
___________________
2 In 2000 Dr. Camara Jones developed a theoretical framework for the multiple levels of racism and used an allegory of a garden to illustrate the mechanisms through which these levels operate (Jones, 2000).
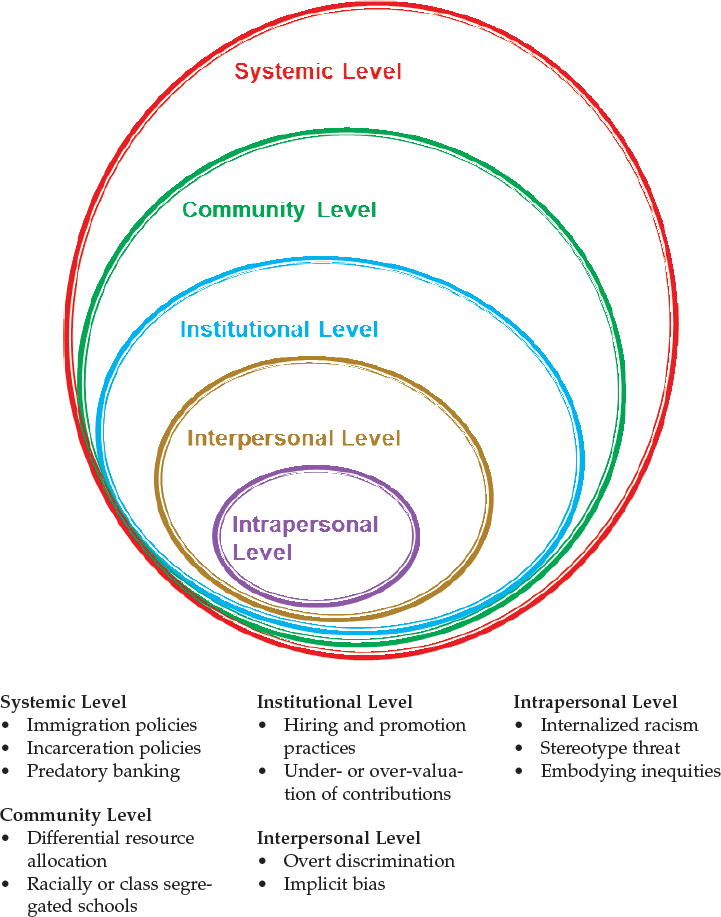
NOTES: The mechanisms by which the social determinants of health operate differ with respect to the level. For the intrapersonal level, these mechanisms are individual knowledge, attitudes/beliefs, and skills. At the interpersonal level, they are families, friends, and social networks. At the institutional level, they are organizations and social institutions. At the community level, they are relationships among organizations. At the systemic level, the mechanisms are national, state, and local policies, laws, and regulations.
SOURCE: Concept from McLeroy et al., 1988.
Most studies of racism are based on African American samples; however, other populations may be at risk for manifestations of racism that differ from the African American experience. Asians, Hispanics, and, more recently, Arabs and Muslims are subject to assumptions that they are not U.S. citizens and, therefore, lack the rights and social entitlements that other U.S. residents claim (Chou and Feagin, 2015; Cobas et al., 2009; Feldman, 2015; Gee et al., 2009; Johnson, 2002; Khan and Ecklund, 2013). The implications of this include threats or actual physical violence against members of these groups. For instance, researchers have found that in the months immediately following September 11, 2001, U.S. women with Arabic surnames who were residing in California experienced increases in both racial microaggressions (i.e., seemingly minor forms of “everyday racism”) and in poor birth outcomes compared to the 6 months preceding 9/11, while women of other U.S. ethnic groups did not (Kulwicki et al., 2008; Lauderdale, 2006). For Native Americans, because tribes are independent nations, the issues of racism need to be considered to intersect with those of sovereignty (Berger, 2009; Massie, 2016; Sundeen, 2016).
The evidence linking racism to health disparities is expanding rapidly. A variety of both general and disease-specific mechanisms have been identified; they link racism to outcomes in mental health, cardiovascular disease, birth defects, and other outcomes (Paradies, 2006a; Pascoe and Smart Richman, 2009; Shavers et al., 2012; Williams and Mohammed, 2009). Which racism mechanisms matter most depends in part on the disease and, to a lesser degree, the population. The vast majority of studies focus on the role of discrimination; that is racially disparate treatment from another individual or, in some cases, from an institution. Among the studies not focused on discrimination, the majority examine segregation. Generally, findings show that members of all groups, including whites, report experiencing racial discrimination, with levels typically, though not always, higher among African Americans and, to a lesser degree, Hispanics than among whites. Gender differences in some perceptions about and responses to racism have also been observed (Otiniano Verissimo et al., 2014). Three major mechanisms by which systemic racism influences health equity—discrimination (including implicit bias), segregation, and historical trauma—are discussed in more detail in the following paragraphs.
Discrimination
The mechanisms by which discrimination operates include overt, intentional treatment as well as inadvertent, subconscious treatment of individuals in ways that systematically differ so that minorities are treated worse than nonminorities. Recent meta-analyses suggest that
racial discrimination has deleterious effects on the physical and mental health of individuals (Gee et al., 2009; Paradies, 2006a; Pascoe and Smart Richman, 2009; Priest et al., 2013; Williams and Mohammed, 2009). Significant percentages of members of racial and ethnic minority populations report experiencing discrimination in health care and non-health care settings (Mays et al., 2007). Greater proportions of African Americans than members of other groups report either experiencing discrimination personally or perceiving it as affecting African Americans in general, even if they have not experienced it personally. Hate crimes motivated by race or ethnicity bias disproportionately affect Hispanics and African Americans (UCR, 2015) (see the public safety section in this chapter for more on hate crimes).
Discrimination is generally associated with worse mental health (Berger and Sarnyai, 2015; Gee et al., 2009; Paradies, 2006b; Williams and Mohammed, 2009); greater engagement in risky behaviors (Gee et al., 2009; Paradies, 2006b; Williams and Mohammed, 2009); decreased neurological responses (Harrell et al., 2003; Mays et al., 2007) and other biomarkers signaling the dysregulation of allostatic load; hypertension-related outcomes (Sims et al., 2012), though some evidence suggests racism does not drive these outcomes (Roberts et al., 2008); reduced likelihood of some health protecting behaviors (Pascoe and Smart Richman, 2009); and poorer birth-related outcomes such as preterm delivery (Alhusen et al., 2016). Paradoxically, despite higher levels of exposure to discrimination, the mental health consequences may be less severe among African Americans than they are among members of other groups, especially Asian populations (Gee et al., 2009; Williams and Mohammed, 2009). Researchers have suggested that African Americans draw on reserves of resilience in ways that temper the effects of discrimination on mental health (Brown and Tylka, 2011).
Though people may experience overt forms of racism (e.g., being unfairly fired on the basis of race), the adverse health effects of racism appear to stem primarily from the stress of chronic exposure to seemingly minor forms of “everyday racism” (i.e., racial microaggressions), such as being treated with less respect by others, being stopped by police for no apparent reason, or being monitored by salespeople while shopping (APA, 2016; Sue et al., 2007; Williams et al., 2003). The chronic exposure contributes to stress-related physiological effects. Thus, discrimination appears to exert its greatest effects not because of exposure to a single life traumatic incident but because people must mentally and physically contend with or be prepared to contend with seemingly minor insults and assaults on a near continual basis (APA, 2016). The implications appear to be greatest for stress-related conditions such as those tied to hypertension, mental health outcomes, substance abuse behaviors, and birth-related
outcomes (e.g., low birth weight and premature birth) than for other outcomes (Williams and Mohammed, 2009).
Higher socioeconomic status (SES) does not protect racial and ethnic minorities from discriminatory exposures. In fact, it may increase opportunities for exposure to discrimination. The concept of “John Henryism” is used to describe an intensely active way of tackling racial and other life challenges (James, 1994). Though the evidence is mixed, John Henryism may contribute to worse cardiovascular outcomes among African American males who respond to racism by working even harder to disprove racial stereotypes (Flaskerud, 2012; Subramanyam et al., 2013).
Implicit bias John Dovidio defines implicit bias—a mechanism of unconscious discrimination—as a form of racial or other bias that operates beneath the level of consciousness (Dovidio et al., 2002). Research conducted over more than four decades finds that individuals hold racial biases of which they are not aware and, importantly, that discriminatory behaviors can be predicted based on this construct (Staats et al., 2016). The effects are greatest in situations marked by ambiguity, stress, and time constraints (Bertrand et al., 2005; Dovidio and Gaertner, 2000). Implicit bias is not an arbitrary personal preference that individuals hold; for example, “I just happen to prefer pears over apples.” Rather, the nature and direction of individuals’ biases are structured by the racial stratification and norms of society. As a result, they are predictable.
Much of the public health literature has focused on the implicit biases of health care providers, who with little time to devote to each patient can provide care that is systematically worse for African American patients than for white patients even though the health care provider never intended to do so (IOM and NRC, 2003; van Ryn and Burke, 2000). The evidence is clear that unconscious racialized perceptions contribute to differences in how various individual actors, including health care providers, perceive others and treat them. Based on psychology lab experiments, functional magnetic resonance imaging (fMRI) pictures of the brain, and other tools, researchers find that white providers hold implicit biases against African Americans and that, to a lesser degree, some minority providers may also hold these biases (Hall et al., 2015). Although not limited to health care professionals, the biases lead providers to link negative characteristics (e.g., bad) and emotions (e.g., fear) with people or images they perceive as being African American (Zestcott et al., 2016). As a result of such implicit biases, physicians treat patients differently depending on the patient’s race, ethnicity, gender, or other assumed or actual characteristics (IOM and NRC, 2003; Zestcott et al., 2016).
Given the importance of implicit bias, researchers have considered the role of health care provider–patient racial and ethnic concordance. Even
if patients have similar clinical profiles, their care may differ systematically based on their race or ethnicity and that of their health care provider (Betancourt et al., 2014; van Ryn and Fu, 2003; Zestcott et al., 2016). The evidence on whether and how patient–provider concordance contributes to health disparities is mixed (van Ryn and Fu, 2003). Qualitative and quantitative findings suggest that patients do not necessarily prefer providers of the same race or ethnicity; they prefer a provider who treats them with respect (Dale et al., 2010; Ibrahim et al., 2004; Schnittker and Liang, 2006; Volandes et al., 2008). Providers appear to evaluate African American patients more negatively than they do similar white patients; seem to perceive them as more likely to participate in risky health behaviors; and may be less willing to prescribe them pain medications and narcotics medications (van Ryn and Fu, 2003). In a video-based study conducted among primary care providers, the odds ratio of providers referring simulated African American patients to otherwise identical white patients for cardiac catheterization was 0.6 (Schulman et al., 1999). Some evidence suggests minority providers deliver more equitable care to their diverse patients than white providers. For instance, a longitudinal study among African American and white HIV-positive patients enrolled in HIV care found that white doctors took longer to prescribe protease inhibitors (an effective HIV medication) for their African American patients than for their clinically similar white patients. Providers prescribed them on average 162 days earlier for white patients than for comparable African American patients (King et al., 2004). Among African American providers, there was no difference between African American and white patients in how long before providers prescribed the medications.
Racial and ethnic minority providers play an important role in addressing disparities because they help bridge cultural gulfs (Butler et al., 2014; Cooper et al., 2003; Lehman et al., 2012), and greater proportions of them serve minority and socially disadvantaged communities (Cooper and Powe, 2004); however, these providers are underrepresented in the health professions, and they face challenges that may constrain their professional development and the quality of care they are able to provide (Landrine and Corral, 2009). Specifically, they are more likely to serve patients in resource-poorer areas and lack professional privileges associated with academic and other resource-rich institutions. The structural inequities have implications not only for individual clinicians but also for the patients and communities they serve. Pipeline programs that grow the numbers of minority providers may help to address underrepresentation in the health professions. The available data suggest that pipeline participants are more likely to care for poor or underserved patients when they join the workforce (McDougle et al., 2015). Supporting the professional development of and expanding the resources and tools available to providers working in resource-poor communities seems to be one option for
improving access to and quality of care; however, the literature does not clearly elucidate the relationship between health care workforce pipeline programs (e.g., to grow the numbers of minority providers) and their impact on the social determinants of health for poor and underserved communities (Brown et al., 2005; Smith et al., 2009). A commitment to equity is not enough to remedy the discriminatory treatment that results from implicit biases because the inadvertent discriminatory behavior co-occurs alongside deeply held personal commitments to equity. Identifying implicit biases and acknowledging them is one of the most effective steps that can be taken to address their effects (Zestcott et al., 2016). Trainings can help health care providers identify their implicit biases. Well-planned allocations of resources, including time, may afford them sufficient opportunity to account for it while serving diverse persons/patients.
Segregation
Residential segregation—that is, the degree to which groups live separately from one another (Massey and Denton, 1988)—can exacerbate the rates of disease among minorities, and social isolation can reduce the public’s sense of urgency about the need to intervene (Acevedo-Garcia, 2000; Wallace and Wallace, 1997). The effects of racial segregation differ from those of socioeconomic segregation. Lower SES whites are more likely to live in areas with a range of SES levels, which affords even the poorest residents of these communities access to shared resources (e.g., parks, schools) that buffer against the effects of poverty (APA Task Force on Socioeconomic Status, 2007; North Carolina Institute of Medicine Task Force on Prevention, 2009). By contrast, racial and ethnic minorities are more likely to live in areas of concentrated poverty (Bishaw, 2011). Indeed, if shared resources are of poor quality, they may compound the low SES challenges an individual faces. Racial segregation contributes to disparities in a variety of ways. It limits the socioeconomic resources available to residents of minority neighborhoods as employers and higher SES individuals leave the neighborhoods; it reduces health care provider density in predominately African American communities, which affects access to health care (Gaskin et al., 2012); it constrains opportunities to engage in recommended health behaviors such as walking; it may be associated with greater density of alcohol outlets, tobacco advertisements, and fast food outlets in African American and other minority neighborhoods (Berke et al., 2010; Hackbarth et al., 1995; Kwate, 2008; LaVeist and Wallace, 2000); it increases the risk for exposure to environmental hazards (Brulle and Pellow, 2006); and it contributes to the mental and physical consequences of prevalent violence, including gun violence and aggressive policing (Landrine and Corral, 2009; Massey and Denton, 1989; Polednak, 1996).
Historical Trauma
Historical trauma, “a collective complex trauma inflicted on a group of people who share a specific group identity or affiliation” (Evans-Campbell, 2008, p. 320), manifests from the past treatment of certain racial and ethnic groups, especially Native Americans. This is another form of structural (i.e., systemic) racism that continues to shape the opportunities, risks, and health outcomes of these populations today (Gee and Ford, 2011; Gee and Payne-Sturges, 2004; Heart et al., 2011). The past consignment of Native Americans to reservations with limited resources continues to constrain physical and mental health in these communities; however, the methods to support research on this topic have not yet been fully developed (Heart et al., 2011). Additional details on the health of Native Americans are presented in Chapter 2 and Appendix A.
Interventions
The literature includes a small number of tested interventions. Interventions to address the health consequences of racism need not target racism in order to address the disparities it helps to produce. Furthermore, despite the deeply rooted nature of racism, communities are taking action to address the issue. (See Box 3-2 for a brief example of a community targeting structural racism and Box 3-3 for guidance on how to start a conversation about race.) Policy interventions and multi-sectoral efforts may be necessary to address structural factors such as segregation.
Examples of interventions that target racism include the following:
- Dismantling racism by addressing factors in organizational settings and environments that “directly and indirectly contribute to racial health care disparities” (Griffith et al., 2010, p. 370); see work by Derek Griffith (Griffith et al., 2007, 2010).
- The Undoing Racism project (Yonas et al., 2006), which integrates community-based participatory research with the “undoing racism” process, which is built around community organizing.
- The Praxis Project,3 a national organization whose mission is to build healthy communities by transforming the power relationships and structures that affect lives. The organization’s comprehensive strategy for change includes policy advocacy, local organizing, strategic communications, and community research.
___________________
3 For more information, see http://www.thepraxisproject.org (accessed October 20, 2016).
Although there is not a robust evidence base from which to draw solutions for implicit bias and its effects, there are promising strategies. For example, there is emerging evidence that mindfulness-based interventions have the potential to reduce implicit bias (Kang et al., 2014; Levesque and Brown, 2007; Lueke and Gibson, 2014). One promising avenue of research involves models of self-regulation and executive control on interracial interaction (Richeson and Shelton, 2003). Mindfulness has been shown to work on the cognitive brain function attentional processes involved in executive function, which is involved in decision making (Lueke and Gibson, 2014; Malinowski, 2013). A key component of mindfulness is paying attention with intention and without judgment.
There is also existing literature that points to the need for community-based interventions to mitigate implicit bias within the context of criminal justice and community safety (Correll et al., 2002, 2007; La Vigne et al., 2014; Richardson and Goff, 2013). According to the National Initiative for Building Community Trust and Justice, implicit bias can shape the outcomes of interactions between police and residents, which in turn result in pervasive practices that focus suspicion on specific populations (National Initiative for Building Community Trust and Justice, 2015). As discussed later in this chapter, the criminal justice system is a key actor and setting in shaping health inequity (see also Chapters 6 and 7 for more on criminal justice system as policy context and as a partner, respectively). Law enforcement agencies in communities around the country have employed strategies such as “principled policing” and policy changes and trainings to strengthen police–community relations (Gilbert et al., 2016; Jones, 2016).
The Perception Institute,4 an organization committed to generating evidence-based solutions for bias in education, health care, media, workplace, law enforcement, and civil justice, published a report authored by Godsil et al. (2014) in which promising interventions for implicit bias are highlighted (Godsil et al., 2014). Among these interventions was a multipronged approach to reducing implicit bias that Devine and colleagues (2012) found to be successful and the “first evidence that a controlled, randomized intervention can produce enduring reductions in implicit bias” (Devine et al., 2012, p. 1271). The multiple strategies of the intervention tested included stereotype replacement, counter-stereotype imaging, individuation, perspective taking, and increasing opportunities for contact. As discussed above, there is an emerging body of literature that is beginning to highlight promising solutions for implicit bias; however, that research base needs to be expanded further.
Recommendation 3-1: The committee recommends that research funders5 support research on (a) health disparities that examines the multiple effects of structural racism (e.g., segregation) and implicit and explicit bias across different categories of marginalized status on health and health care delivery; and (b) effective strategies to reduce and mitigate the effects of explicit and implicit bias.
This could include implicit and explicit bias across race, ethnicity, gender identity, disability status, age, sexual orientation, and other marginalized groups.
There have been promising developments in the search for interventions to address implicit bias, but more research is needed, and engaging community members in this and other aspects of research on health disparities is important for ethical and practical reasons (Minkler et al., 2010; Mosavel et al., 2011; Salway et al., 2015). In the context of implicit bias in workplaces and business settings, including individuals with relevant expertise in informing and conducting the research could also be helpful. Therefore, teams could be composed of such nontraditional participants as community members and local business leaders, in addition to academic researchers.
Conclusion 3-1: To reduce the adverse effects and the level of implicit bias among stakeholders in the community (such as health care workers,
___________________
4 For more information, see https://perception.org (accessed October 18, 2016).
5 Funders include government agencies, private foundations, and other sources such as academic centers of higher education.
social service workers, employers, police officers, and educators), the committee concludes, based on its judgment, that community-based programs are best suited to mitigate the adverse effects of implicit bias. Successful community programs would be tailored to the needs of the community. However, proven strategies and efficacious interventions to reduce the effects of or mitigate effects of implicit bias are lacking. Therefore:
Recommendation 3-2: The committee recommends that research funders support and academic institutions convene multidisciplinary research teams that include nonacademics to (a) understand the cognitive and affective processes of implicit bias and (b) test interventions that disrupt and change these processes toward sustainable solutions.
SOCIAL DETERMINANTS OF HEALTH
As described earlier, structural inequities are produced on the basis of social identity (e.g., race, gender, and sexual orientation), and the social determinants of health are the “terrain” on which the effects play out. Traditionally, the most well-known and cited of the factors that shape health outcomes are the individual-level behavioral factors (e.g., smoking, physical activity, nutrition habits, and alcohol and drug use) that the evidence shows are proximally associated with individual health status and outcomes. As stated in Chapter 1, understanding the social determinants of health requires a shift toward a more upstream perspective (i.e., the conditions that provide the context within which an individual’s behaviors are shaped). Again, consider the metaphor of a fish, and the role of the conditions of the fishbowl in influencing the fish’s well-being, and the analogy to human beings and conditions in which people live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks. These environments and settings (e.g., school, workplace, neighborhood, and church) have been referred to as “place.” In addition to the more material attributes of “place,” the patterns of social engagement, social capital, social cohesion, and sense of security and well-being are also affected by where people live (Braveman and Gottlieb, 2014; Healthy People 2020, 2016). Although the term “social determinants of health” is widely used in the literature, the term may incorrectly suggest that such factors are immutable. It is important to note that the factors included among the social determinants of health are indeed modifiable and that they can be influenced by social, economic, and political processes and policies. In fact, there are communities throughout the United States that have prioritized
NOTE: The social (and other) determinants of health are highlighted to convey the focus of this section.
addressing the social determinants of health and are demonstrating how specific upstream strategies lead to improved community conditions and health-related outcomes. (See Chapter 5 for an in depth examination of nine community examples.) Although it might be more accurate to refer to social “contributing factors” for health, the committee continues to use the widely accepted word “determinants” in this report.
For the purposes of this report, the committee has identified nine social determinants of health (see report conceptual model, Figure 3-3) that the literature shows fundamentally influence health outcomes at the community level. These determinants are education, income and wealth, employment, health systems and services, housing, the physical environment, transporation, the social environment, and public safety (Table 3-1 provides a brief definition of each).
There is a vast and growing body of literature on the social, economic, and environmental determinants of health and their impacts on health
TABLE 3-1 The Social (and Other) Determinants of Healtha
| Determinant of Health | Explanation |
|---|---|
| Education | The access or lack of access to learning opportunities and literacy development for all ages which effectively serves all learners. Education is a process and a product: as a process, education occurs at home, in school, and in the community. As a product, an education is the sum of knowledge, skills, and capacities (i.e., intellectual, socio-emotional, physical, productive, and interactive) acquired through formal and experiential learning. Educational attainment is a dynamic, ever-evolving array of knowledge, skills, and capacities. Education can influence health in many ways. Educational attainment can influence health knowledge and behaviors, employment and income, and social and psychological factors, such as the sense of control, social standing, and social networks. |
| Income and Wealth | Income is the amount of money earned in a single year from employment, government assistance, retirement and pension payments, and interest or dividends from investments or other assets. Income can fluctuate greatly from year to year, depending on life stage and employment status. Wealth, or economic assets accumulated over time, is calculated by subtracting outstanding debts and liabilities from the cash value of currently owned assets—such as houses, land, cars, savings accounts, pension plans, stocks and other financial investments, and businesses. |
| Wealth measured at a single point in time may provide a more complete picture of a person’s economic resources. Access to financial resources, be it income or wealth, affects health by safeguarding individuals against large medical bills while also making available more preventive health measures such as access to healthy neighborhoods, homes, land uses, and parks. | |
| Employment | The level or absence of adequate participation in a job or the workforce, including occupation, unemployment, and underemployment. Work influences health not only by exposing employees to physical environments, but also by providing a setting where healthy activities and behaviors can be promoted (An et al., 2011). The features of a worksite, the nature of the work, and how the work is organized can affect worker mental and physical health (Clougherty et al., 2010). Many Americans also obtain health insurance through their workplace, another potential impact on health and wellbeing. Health also affects one’s ability to maintain stable employment (Davis et al., 2016; Goodman, 2015). For most working adults, employment is the main source of income, providing access to homes, neighborhoods, and other goods and services that promote health. |
| Health Systems and Services | The access or lack of access to effective, affordable, culturally and linguistically appropriate, and respectful preventative care, chronic disease management, emergency services, mental health services, and dental care and the promotion of better community services and community conditions that promote health over the lifespan, including population health outcomes. It also refers to a paradigm shift that reflects health care over sick care and that promotes prevention. |
| Determinant of Health | Explanation |
|---|---|
| Housing | The availability or lack of availability of high-quality, safe, and affordable housing that is accessible for residents with mixed income levels. Housing also refers to the density within a housing unit and within a geographic area, as well as the overall level of segregation/diversity in an area based on racial and ethnic and/or socioeconomic status. Housing affects health because of the physical conditions within homes, the conditions in the neighborhoods surrounding homes, and housing affordability, which affects the overall ability of families to make healthy choices. |
| Physical Environment | The physical environment reflects the place, including the human-made physical components, design, permitted use of space, and the natural environment. It includes, for example, transportation/getting around, what’s sold and how it’s promoted, parks and open space, look and feel, air/water/soil, and arts and cultural expression. |
| Transportation | Transportation consists of the network, services, and infrastructure necessary for residents to get from one place to another. If designed and maintained properly, transportation promotes safe mobility and is accessible to all residents, regardless of geographic location, age or disability status. Unsafe transportation can result in unintentional injuries or death. Access or lack of access to quality transportation at the community level affects opportunity for employment and vital services such as health care, education, and social services. Active transportation—the promotion of walking and cycling for transportation, complemented by public transportation or any other active mode—is a form of transportation that reduces environmental barriers to physical activity and promotes positive health outcomes. Transportation can also have negative environmental impacts, such as air pollution, which can affect health. |
| Social Environment | The social environment, sometimes referred to as social capital, reflects the individuals, families, and businesses within a community, the interactions and kinship ties between them, and norms and culture. It also includes social networks and trust as well as civic participation and willingness to act for the common good. |
| Public Safety | Public safety refers to the safety and protection of the general public. Here it is characterized by the absence of violence in public settings and the role of the justice system. Violence is the intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community that either results in or has a high likelihood of resulting in injury, death, psychological or emotional harm, maldevelopment or deprivation, and trauma from actual and/or threatened, witnessed and/or experienced violence. |
a Determinants are listed in the order in which they are discussed in this section.
SOURCES: Davis et al., 2016; Mueller et al., 2015.
outcomes (Braveman and Gottlieb, 2014; Braveman et al., 2011; CSDH, 2008; Marmot et al., 2010). Often, the evidence is in the form of cross-sectional analyses, and the pathways to health outcomes are not always clearly delineated, in part due to the complexity of the mechanisms and the long time periods it takes to observe outcomes (Braveman and Gottlieb, 2014). Therefore, the literature is not sufficient to establish a causal relationship between each of these determinants and health, but the determinants certainly are correlated with and contribute to health outcomes. While this report focuses on the community level, it should be made clear that the social determinants of health operate at multiple levels throughout the life course (IOM, 2006). This includes the individual level (knowledge, attitudes/beliefs, skills), family and community level (friends and social networks), institutional level (relationships among organizations), and systemic level (national, state, and local policies, laws, and regulations) (see Figure 3-2, the social ecological model adapted from McLeroy et al. [1988]). Furthermore, the various levels of influence that the social determinants of health have can occur simultaneously and interact with one another (IOM, 2006). In addition to the multiple levels of influence, there is a diversity of actors, sectors, settings, and stakeholders that interact with and shape the social determinants of health. This adds an additional layer of complexity to the factors that shape health disparities.
The following sections describe each of these nine determinants and how they shape health outcomes, as well as the disparities within these social determinants of health that contribute to health inequity. To highlight the ongoing work of communities that seek to address the conditions in which members live, learn, work, and play, this section will feature brief examples of communities for each determinant of health.
Education
Education, as it pertains to health, can be conceptualized as a process and as an outcome. The process of educational attainment takes place in many settings and levels (e.g., the home/family, school, and community), while the outcome can be described as a sum of knowledge, skills, and capacities that can influence the other social determinants of health, or health, more directly (Davis et al., 2016). Within the current social determinants of health literature, the primary focus on education is on educational attainment as an outcome (i.e., years of schooling, high school completion, and number of degrees obtained) and how it relates to health outcomes.
There is an extensive body of research that consistently demonstrates a positive correlation between educational attainment and health status indicators, such as life expectancy, obesity, morbidity from acute and
chronic diseases, health behaviors (e.g., smoking status, heavy drinking physical activity, preventive services or screening behavior, automobile and home safety) and more (Baum et al., 2013; Cutler and Lleras-Muney, 2006, 2010; Feinstein et al., 2006; Krueger et al., 2015; Rostron et al., 2010). Educational attainment also has an intergenerational effect, in which the education of the parents, particularly maternal education, is linked to their children’s health and well-being (Cutler and Lleras-Muney, 2006). For example, research suggests that babies born to mothers who have not completed high school are twice as likely to die before their first birthday as babies who are born to college graduates (Egerter et al., 2011b; Mathews and MacDorman, 2007). Death rates are declining among the most-educated Americans, accompanied by steady or increasing death rates among the least educated (Jemal et al., 2008). The findings on the association between education and health are consistent with population health literature within the international context as well (Baker et al., 2011; Furnee et al., 2008; Marmot et al., 2010).
Even more noteworthy about the education and health relationship is the graded association that is observed across populations with varying education levels, commonly referred to as the “education gradient.” In the United States the gradient in health outcomes by educational attainment has steepened over the last four decades in all regions of the United States (Goldman and Smith, 2011; Montez and Berkman, 2014; Olshansky et al., 2012), producing a larger gap in health status between Americans with high and low education. Specifically, trends in data suggest that, over time, the disparities in mortality and life expectancy by education level have been increasing (Meara et al., 2008; Olshansky et al., 2012). Meara et al. found that approximately 20 percent of this trend was attributable to differential trends in smoking-related diseases in the 1980s and 1990s, despite the overall population increases in life expectancy during these two decades (Meara et al., 2008). Economic trends and shifting patterns of employment, in which skilled jobs linked to educational attainment are associated with increased income, also have implications for health (NRC, 2012). This makes the connection between education and health, mediated by employment opportunities, even more important and worth exploring.
Data from the Behavioral Risk Factor Surveillance System reveal that across all racial groups, adults with higher levels of educational attainment are less likely to rate their own health as less than very good (Egerter et al., 2011b). While the education gradient is present across racial and ethnic groups, it is important to keep in mind that the rates of educational attainment vary across different racial and ethnic groups. For the 2013–2014 academic year, the high school graduation rate for white students was 87.2 percent as compared with 76.3 percent among Hispanics, 72.5 percent among African Americans, and 70 percent among Native
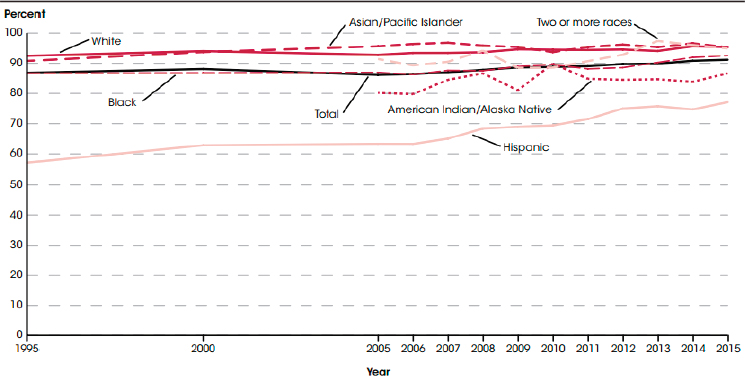
NOTE: Race categories exclude persons of Hispanic ethnicity. Prior to 2005, separate data on persons of two or more races were not available; data for American Indians/Alaska natives are not shown prior to 2005.
SOURCE: Kena et al., 2016.
Americans (Kena et al., 2016). These rates are consistent with high school diploma and bachelor degree achievement gaps that have persisted since the late 1990s (see Figures 3-4 and 3-5).
Although the literature linking education and health is robust, there is still some debate as to whether or not this relationship is a causal one (Baker et al., 2011; Fujiwara and Kawachi, 2009; Grossman, 2015). Issues that have been raised in the course of this debate include the role of reverse causation and the potential influence of any unobserved third variables (Grossman, 2015). The association between education and health is clearly bidirectional. Education outcomes are substantially affected by health (Cutler and Lleras-Muney, 2006). Students living in community conditions that contribute to hunger, chronic stress, or lack of attention to visual or hearing needs are likely to have problems concentrating in class (Evans and Schamberg, 2009). Unmanaged health conditions (e.g., asthma, dental pain, acute illnesses, mental health issues, etc.) give rise to chronic absenteeism, which in turn is highly correlated with underachievement (Ginsburg et al., 2014). In short, health issues are much more than minor distractions in the lives of students, especially students living in low-income communities.
SOURCE: Ryan and Bauman, 2016.
Disparities in Education
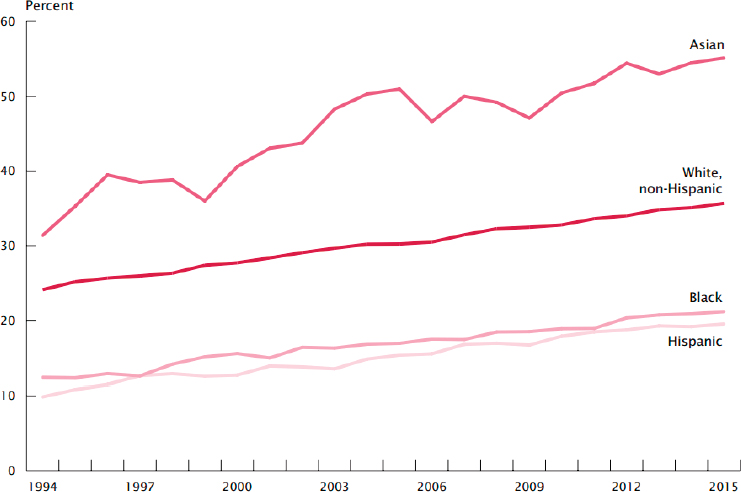
Educational attainment, common measures of which include high school diploma or bachelor’s degree, has increased for all race groups and Hispanics since 1988, according to U.S. Census estimates (Ryan and Bauman, 2016). Despite this overall progress, the gaps between these groups have remained the same for some and increased for others. For example, in 1988 African Americans and Hispanics attained bachelor’s degrees at very similar rates; however, by 2015 the percentage gap between African Americans and Hispanics had reached 7 percent, with rates of completion at 22 percent and 15 percent, respectively (Ryan and Bauman, 2016). Furthermore, there has been little to no progress in closing the gap of achievement between whites and African Americans (Ryan and Bauman, 2016).
A recent study of school trends conducted by the U.S. Government Accountability Office (GAO) found that there has been a large increase in schools that are distinguished by the poverty and race of their student bodies (GAO, 2016). The percent of K–12 schools with students who are poor and are mostly African American or Hispanic grew from 9 percent to 16 percent from 2000 to 2013. These schools were the most racially
and economically concentrated among all schools, with 75 to 100 percent of the students African American or Hispanic and eligible for free or reduced-price lunch—a commonly used indicator of poverty. Moreover, compared with other schools, these schools offered disproportionately fewer math, science, and college preparatory courses and had disproportionately higher rates of students who were held back in 9th grade, suspended, or expelled (GAO, 2016).
One gap in educational achievement that has successfully been narrowed over the past five decades is the gender disparity in bachelor’s degree attainment, in which men historically had higher achievement rates (Crissey et al., 2007). In 2015 the percentage of men ages 25 or older with a bachelor’s degree or higher was not statistically different from that of women, with women leading by one percentage point (Ryan and Bauman, 2016).
The evidence suggests that disparities in education are apparent early in the life course, which reflects broader societal inequities (Garcia, 2015). In education, these early disparities are evidenced by wide gaps in vocabulary between children from low-income and those from middle- or upper-income families. Children from low-income families may have 600 fewer words in their vocabulary by age 3, a gap that grows to as many as 4,000 words by age 7 (Christ and Wang, 2010). These word gaps directly affect literacy levels and reading achievement (Marulis and Neuman, 2010). There is substantial evidence that children who do not read at grade level by 7 or 8 years of age are much more likely to struggle academically (Chall et al., 1990). Both high school graduation rates and participation in postsecondary education opportunities are correlated with early literacy levels. Hence, attention to and investments in early childhood education are generally viewed as an important way to reduce disparities in education (Barnett, 2013).
Mechanisms
Although the association between education and health is clear, the mechanisms by which educational attainment might improve health are not so clearly understood. A keen understanding of the mechanisms could help to inform the most cost-effective and targeted policies or solutions that seek to improve health and, ultimately, promote health equity (Picker, 2007). Egerter et al. (2011b) identified multiple interrelated pathways through which education can affect health, based on the literature (see Figure 3-6). The three major pathways are the following:
- Education increases health knowledge, literacy, coping, and problem solving, thereby influencing health behaviors;
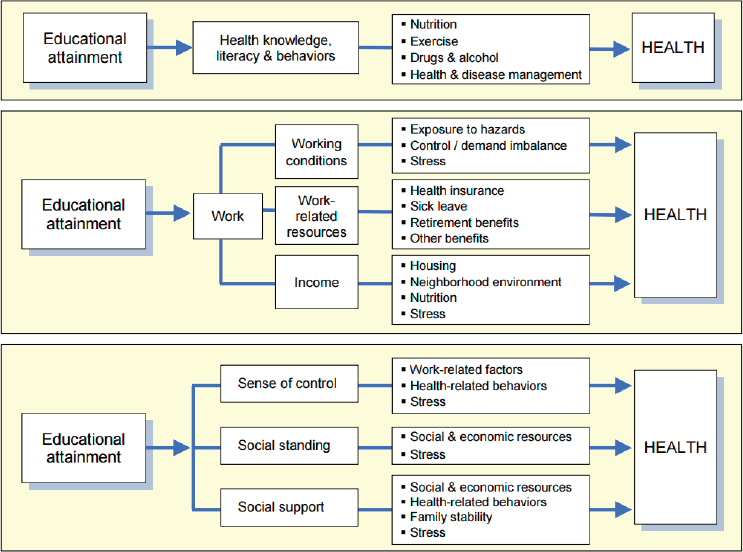
SOURCE: Egerter et al., 2011b. Used with permission from the Robert Wood Johnson Foundation.
- Educational attainment shapes employment opportunities and related benefits, such as income, working conditions, and other resources; and
- Research indicates that each additional year of education leads to almost 11 percent more income annually (Rouse and Barrow, 2006), which can secure safer working environments and benefits such as health insurance and sick leave.
- Education affects social and psychological factors that influence health (e.g., self-efficacy, social status, and social networks) (Egerter et al., 2011b).
- Education has also been linked to human capital, a systematic way of thinking that benefits every decision, which could positively affect health decisions (Cutler and Lleras-Muney, 2006; Lundborg et al., 2012, 2016).
In this framework, note that educational attainment is a predictor of health and can either improve or hinder health outcomes depending on
educational attainment. This suggests that policies and practices proven to increase academic performance and reduce education disparities are important to reducing health disparities. (See Box 3-4 for an example of a community school working to improve educational outcomes.) Intervening early is generally considered a high-impact strategy (Barnett, 2013). However, interventions that support academic achievement in high schools and in postsecondary settings are also important to increasing educational attainment (Balfanz et al., 2007; Carnahan, 1994; Kirst and Venezia, 2004; Louie, 2007). One of the key factors in both high school and college completion rates has to do with how well students transition from one level of the education system to another (Rosenbaum and Person, 2003).
Income and Wealth
Income can be defined broadly as the amount of money earned in a single year from employment, government assistance, retirement and pension payments, and interest or dividends from investments or other assets (Davis et al., 2016). Income can fluctuate greatly from year to year depending on life stage and employment status. Wealth, or economic assets accumulated over time, is calculated by subtracting outstanding debts and liabilities from the cash value of currently owned assets—such as houses, land, cars, savings accounts, pension plans, stocks and other financial investments, and businesses. Wealth measured at a single time period may provide a more complete picture than income of a person’s economic resources. Moreover, wealth has an intergenerational component, which can have implications for who has access to wealth and who does not (De Nardi, 2002).
Access to financial resources, be it income or wealth, affects health by buffering individuals against the financial threat of large medical bills while also facilitating access to health-promoting resources such as access to healthy neighborhoods, homes, land uses, and parks (Davis et al., 2016). Income can predict a number of health outcomes and indicators, such as life expectancy, infant mortality, asthma, heart conditions, obesity, and many others (Woolf et al., 2015).
Income Inequality and Concentration of Poverty
Income inequality is rising in the United States at a rate that is among the highest in the economically developed countries in the north (OECD, 2015). The past few decades have seen dramatic rises in income inequality. In 1970, 17 percent of families lived in upper-income areas, 65 percent in middle-income areas, and 19 percent in lowest-income areas; in 2012, 30 percent of families lived in upper-income areas, 41 percent in middle-income areas, and 30 percent in lowest-income areas (Reardon and Bischoff, 2016). In 2013, the top 10 percent of workers earned an average income 19 times that of the average income earned by the bottom 10 percent of workers; in the 1990s and 1980s, this ratio was 12.5 to 1 and 11 to 1, respectively (OECD, 2015). Furthermore, households earning in the bottom 10 percent have not benefited from overall increases in household income over the past few decades; the average inflation-adjusted income for this population was 3.3 percent lower in 2012 than in 1985 (OECD, 2015). Disparities in life expectancy gains have also increased alongside the rise in income inequality. From 2001 to 2014, life expectancy for the top 5 percent of income earners rose by about 3 years while life expectancy for the bottom 5 percent of income earners saw no increase (Chetty et al., 2016).
Not only are income and wealth determinants of health, but the concentration of poverty in certain neighborhoods is important to recognize as a factor that shapes the conditions in which people live. Concentrated poverty, measured by the proportion of people in a given geographic area living in poverty, can be used to describe areas (e.g., census tracts) where a high proportion of residents are poor (Shapiro et al., 2015). Concentrated poverty disproportionately affects racial and ethnic minorities across all of the social determinants of health. For example, National Equity Atlas data reveal that in about half of the largest 100 cities in the United States, most African American and Hispanic students attend schools where at least 75 percent of all students qualify as poor or low-income under federal guidelines (Boschma, 2016). Given that concentrated poverty is tightly correlated with gaps in educational achievement, this has implications for educational outcomes and health (Boschma and Brownstein, 2016).
Disparities Related to Income Inequality
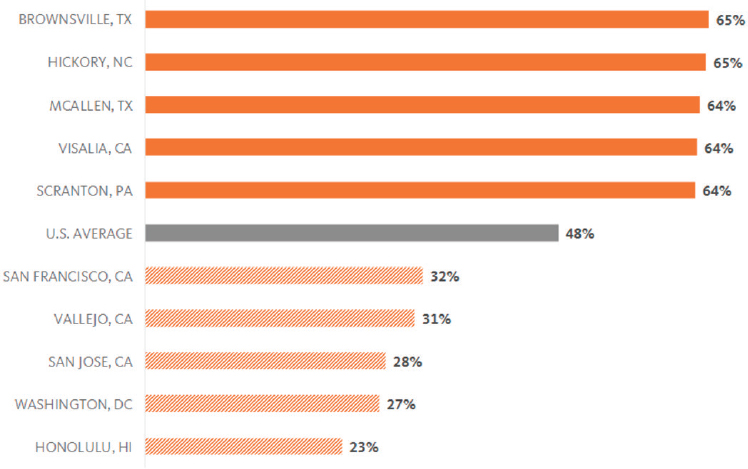
In 2012, of the 12 million full-time low-income workers between the ages of 25 and 64, 56 percent were racial and ethnic minorities (Ross, 2016b). Regional percentages varied from 23 percent in Honolulu, Hawaii, to 65 percent in Brownsville, Texas (Ross, 2016a). Figure 3-7 shows the proportion of low-income workers of racial and ethnic minority groups across different regions of the United States. The burden faced by low-income people suggests that efforts to advance health equity through income and wealth will need to take into consideration rising income inequality as well as significant geographic variation.
Chetty and colleagues published the largest study of its kind, using 1.4 billion income tax and Social Security records to report the association between income level and life expectancy from 1999 through 2014 (Chetty et al., 2016). Consistent with previous findings (NASEM, 2015; Waldron, 2007; Woolf et al., 2015), they found that higher income is related to higher life expectancy and that lower income is related to lower life expectancy. The gap in life expectancy for the richest and poorest 1 percent of individuals was 14.6 years for men and 10.1 years for women. A novel contribution of the study is its examination of the income–longevity relationship
SOURCE: Woolf et al., 2015. Used with permission from PolicyLink, figure from article by Angel Ross, New Data Highlights Vast and Persistent Racial Inequities in Who Experiences Poverty in America, http://nationalequityatlas.org/data-in-action/racial-inequitiespoverty-in-america (accessed December 27, 2016).
across time and local areas. In certain local areas, the effect of being at the bottom of the income gradient is more pronounced than in others, with four- to five-fold differences. This strong local component reinforces the notion suggested by the literature that place matters. Trends in life expectancy also varied geographically, with some areas experiencing improvements and others declines. Others have commented on the limitations of the study (Deaton, 2016; McGinnis, 2016; Woolf and Purnell, 2016).
Zonderman et al. take the findings of this study a step further by considering the role of race and gender differences in the relationship between poverty and mortality. They found that while African American men below poverty status had 2.66 times higher risk of mortality than African American men living above poverty status, white men below poverty status had approximately the same risk as white men living above poverty status (Zonderman et al., 2016). Both African American women and white women living below poverty status were at an increased mortality risk relative to those living above poverty status (Zonderman et al., 2016).
Infant mortality rates in the United States rank among the highest for developed nations (NRC and IOM, 2013), and mortality rates for infants born to low-income mothers are even higher. Studies have shown an inverse correlation between family income and infant mortality (Singh and Yu, 1995) as well as a positive correlation between income inequality (measured with the Gini coefficient) and infant mortality (Olson et al., 2010). Infants born to low-income mothers have the highest rates of low birth weight (Blumenshine et al., 2010; Dubay et al., 2001).
Chronic diseases are more prevalent among low-income people than among the overall U.S. population. Low-income adults have higher rates of heart disease, diabetes, stroke, and other diseases and conditions relative to adults earning higher levels of income (Woolf et al., 2015).
Mechanisms
Researchers have offered various hypotheses about the multiple mechanisms by which income can affect health. Woolf et al. suggest that among others, these mechanisms include more income providing the opportunity to afford health care services and health insurance; greater resources affording a healthy lifestyle and access to place-based benefits known as the social determinants of health; and economic disadvantage and hardship leading to stress and harmful physiological effects on the body (Woolf et al., 2015). Evans and Kim identify “multiple risk exposure” as a potential mechanism for the socioeconomic status and health gradient. This is the convergence among populations with low socioeconomic status of multiple physical and psychosocial risk factors such as poor housing and neighborhood quality, pollutants and toxins, crowding
and congestion, noise exposure, and adverse interpersonal relationships (Evans and Kim, 2010).
Wealth affects health through mechanisms that are not necessarily monetary, such as power and prestige, attitudes and behavior, and social capital (Pollack et al., 2013). Even in the absence of income, wealth can provide resources and a safety net that is not available to those without it. (See Box 3-5 for an example of an initiative seeking to build income and wealth in communities around the country.)
Employment
Employment is the level or absence of adequate participation in a job or workforce, including the range of occupation, unemployment, and underemployment. Work influences health not only by exposing employees to certain physical environments but also by providing a setting where healthy activities and behaviors can be promoted (An et al., 2011). For most adults, employment is the main source of income, thus providing access to homes, neighborhoods, and other conditions or services that promote health. The features of a worksite, the nature of the work, the amount of earnings or income, and how the work is organized can affect worker mental and physical health (An et al., 2011; Clougherty et al., 2010). Many Americans also obtain health insurance through their workplace, accounting for another potential impact on health and wellbeing. While the correlation between employment and health has been well established, there appears to be a bidirectional relationship between employment and health, as health also affects one’s ability to participate in and maintain stable employment (Davis et al., 2016; Goodman, 2015). Not only that, but a healthy workforce is a prerequisite for economic success in any industry (Doyle et al., 2005).
The existing literature on the social determinants of health makes it clear that there is a positive correlation between SES and health (Adler and Stewart, 2010a; Braveman et al., 2005; Conti et al., 2010; Dow and Rehkopf, 2010; Pampel et al., 2010; Williams et al., 2010). Occupational status, a composite of the power, income, and educational requirements associated with various positions in the occupational structure, is a core component of a person’s SES (Burgard and Stewart, 2003; Clougherty et al., 2010). Occupational status can be indicative of the types of tangible benefits, hazards, income, fringe benefits, degree of control over work, and level of exposure to harmful physical environments associated with a job (Clougherty et al., 2010). While the mechanisms by which occupational status influences health have not clearly been delineated, there is evidence that the type of job does affect such health outcomes as hypertension risk and obesity (An et al., 2011; Clougherty et al., 2010).
On the other end of the spectrum, unemployment is associated with poor psychological well-being (McKee-Ryan et al., 2005; Paul and Moser, 2009). Zhang and Bhavsar (2013) examined the literature to illuminate the causality, effect size, and moderating factors of the relationship between unemployment as a risk factor and mental illness as an outcome. The authors reported that unemployment does precede mental illness, but more research is required to determine the effect size (Zhang and Bhavsar, 2013). There is also evidence to suggest that emerging adults who are unemployed are three times as likely to suffer from depression as their employed counterparts (McGee and Thompson, 2015). Burgard and colleagues found that even after controlling for significant social background factors (e.g., gender, race, education, maternal education, income, and more), involuntary job loss was associated with poorer overall self-rated health and more depressive symptoms (Burgard et al., 2007).
Disparities in Employment
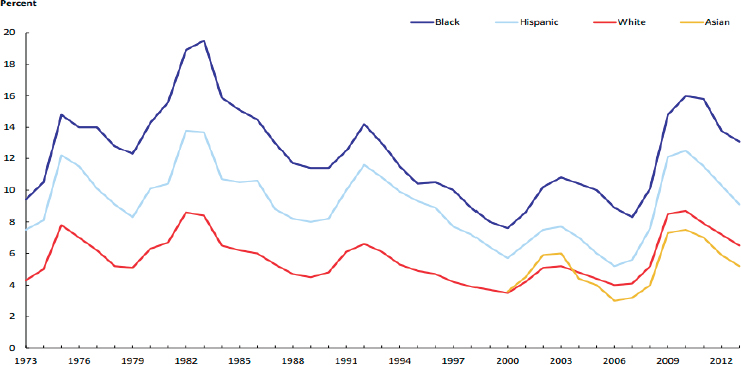
Employment data show disparities in unemployment rates across various racial and ethnic groups and geographic regions, despite the overall progress that has been made in reducing unemployment nationally (Wilson, 2016). During the fourth quarter of 2015, the highest state-level unemployment rate was 13.1 percent for African Americans (Illinois), 11.9 percent for Hispanics (Massachusetts), 6.7 percent for whites (West Virginia), and 4.3 percent for Asians (New York) (Wilson, 2016). Figure 3-8 shows how disparities in unemployment by race and ethnicity have persisted for more than 40 years, with the exception of whites and Asians. Disparities in employment between African Americans and whites persist even when level of education, a major predictor of employment, is held equal between the two groups (Buffie, 2015).
Among the employed, there are systematic differences in wages and earnings by race, ethnicity, and gender. According to the U.S. Bureau of Labor Statistics, in 2013 the median usual weekly earnings6 were $578 for Hispanics, $629 for African Americans, $802 for whites, and $942 for Asians (BLS, 2014). These disparities are consistent across almost all occupational groups. The widest gap in median usual weekly earnings was found between Hispanic women and Asian men, who made $541 and $1,059, respectively (BLS, 2014).
As with income, the distribution of occupations tends to differ across racial and ethnic groups (see Figure 3-9). Whereas half of Asians worked in management, professional, and related occupations in 2013, only 29
___________________
6 These represent earnings for full-time wage and salary workers only.
NOTE: People whose ethnicity is identified as Hispanic or Latino may be of any race. Data for Asians are only available since 2000.
SOURCE: BLS, 2014.
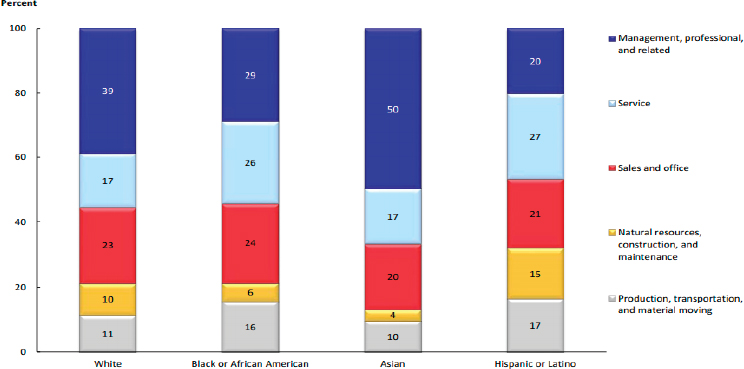
NOTE: People whose ethnicity is identified as Hispanic or Latino may be of any race. Data may not sum to 100 percent due to rounding.
SOURCE: BLS, 2014.
and 20 percent of African Americans and Hispanics, respectively, worked in those professions (BLS, 2014).
Mechanisms
The literature suggests that there are three potential mechanisms through which employment affects health:
- Physical aspects of work and the workplace
- Psychosocial aspects of work and how work is organized
- Work-related resources and opportunities (An et al., 2011; Clougherty et al., 2010)
The nature of work and the conditions of a workplace can increase the risk of injury or illness depending on the type of job. For employees in specific sectors (e.g., air transportation, nursing facilities, using motorized vehicles and equipment, trucking services, hospitals, grocery stores, department stores, food services), the risk of occupational injury is higher (An et al., 2011). This is especially true for operators, laborers, fabricators, and laborers (An et al., 2011). Occupational health can also be shaped by the physical nature of the tasks involved in a given work setting. For example, the health impact of a job that requires intense, laborious physical activity will be different than of a job in which the tasks are primarily sedentary. There is also emerging evidence suggesting that women working hourly jobs bear a larger burden due to hazardous conditions in the workplace than their male counterparts on outcomes such as hypertension, the risk of injury, injury severity, rates of absenteeism, and the time to return to work after illness (Clougherty et al., 2010; Hill et al., 2008).
The psychosocial aspects and organization of one’s job can influence both mental and physical health. The factors that make up this pathway can include work schedules, commute to work, degree of control in work, the balance between effort and rewards, organizational justice, social support at work, and gender and racial discrimination (An et al., 2011). Longer commute times specifically affect low-income populations, as the cost burden of commuting for the working poor is much higher than for other workers and makes up a larger portion of their household budgets (Roberto, 2008).
The resources and opportunities associated with work can have lasting implications for health. Higher-paying jobs are more likely than lower-paying jobs to provide workers with safe work environments and offer benefits such as health insurance, workplace health promotion programs, and sick leave (An et al., 2011). Box 3-6 briefly describes a program
that aims to increase “green” employment opportunities for underserved individuals in a community.
Health Systems and Services
Health care is arguably the most well-known determinant of health, and it is traditionally the area where efforts to improve health have been focused (Heiman and Artiga, 2015). Over the past few decades there has been a paradigm shift that reflects “health” care over “sick” care. The idea is to promote access to effective and affordable care that is also culturally and linguistically appropriate. Health care spans a wide range of services, including preventative care, chronic disease management, emergency services, mental health services, dental care, and, more recently, the promotion of community services and conditions that promote health over the lifespan.
Although screening, disease management, and clinical care play an integral role in health outcomes, social and economic factors contribute to health outcomes almost twice as much as clinical care does (Heiman and Artiga, 2015; Hood et al., 2016; McGinnis et al., 2002; Schroeder, 2007). For example, by some estimates, social and environmental factors proportionally contribute to the risk of premature death twice as much as health care does (Heiman and Artiga, 2015; McGinnis et al., 2002; Schroeder, 2007). That being said, in March 2002, the Institute of Medicine released a report that demonstrated that even in the face of equal access to health care, minority groups suffer differences in quality of health. The noted differences were lumped into the categories of patient preferences and clinical appropriateness, the ecology of health systems and discrimination, bias, and stereotyping (IOM and NRC, 2003). Our health systems are working to better understand and address these differences and appreciate the importance of moving beyond individualized care to care that affects families, communities, and populations (Derose et al., 2011). This new focus on improving the health of populations has been accompanied by a welcome shift from siloed care to a health care structure that is interprofessional, multisectoral and considers social, economic, structural and other barriers to health (NASEM, 2016).
Arriving at the place of shared understanding concerning the health care needs of individuals, families, and communities has required taking a broader look at health. The triple aim, a framework that aims to optimize health system performance, has helped conceptualize this look, bringing to the forefront the elements that matter most, considering per capita cost, improving the health care experience for patients, and focusing on population health (Stiefel and Nolan, 2012). In addition to helping create new health care opportunities, the Patient Protection and Affordable Care Act
(ACA) has helped mitigate the challenge of access to care. According to the U.S. Centers for Disease Control and Prevention (CDC), the proportion of people in 2015 without health insurance had dropped below 10 percent (Cohen et al., 2016c).
Continuing the momentum of improving access to culturally competent and linguistically appropriate care will be a crucial step to improving the health of populations. Culturally and linguistically appropriate care includes high-quality care and clear communication regardless of socioeconomic or cultural background (Betancourt and Green, 2010). There is limited research studying whether there is a link between culturally appropriate care and health outcomes, but data do exist that indicate that behavioral and attitudinal elements of cultural competence facilitate higher-quality relationships between physicians and patients (Paez et al., 2009). Making cultural competency training a part of the all types of providers’ (e.g., physicians, nurses, medical assistants, dentists, pharmacists, social workers, psychologists) education experience, as well as making it a requirement for licensure for providers (Like, 2011), may have the potential to link quality and safety. Continued work is needed to figure out how to translate increased access to care into improved health outcomes and increased health equity.
In light of the ACA’s emphasis on access to improving quality, health outcomes, and population health, it makes sense to look at the environments in which patients live.7 If the social determinants of health are not addressed in a multi-sectoral approach by educational systems, health systems, communities and others, the country will fall short of the triple aim. The Robert Wood Johnson Foundation’s Culture of Health Action Framework has identified action areas meant to work together to address issues of equity, well-being, and improved population health (RWJF, 2015b). Social determinants of health are woven through these action areas. In fact, research shows that social determinants of health play a larger role in health outcomes than do medical advances (Hood et al., 2016; Woolf et al., 2007).
Disparities
While some disparities in access to care have been narrowing, gaps persist among certain groups of the population. For example, the gaps in insurance that existed between poor and nonpoor households and between African Americans and whites or Hispanics and whites decreased
___________________
7 As access to care improves, it will be increasingly important to monitor potential disparities with respect to the nature of care that people receive. This is especially true for chronic conditions that require long-term engagement with the health care system.
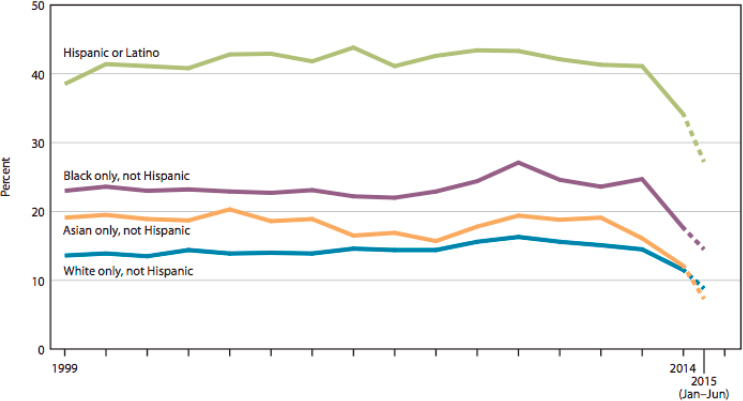
SOURCE: NCHS, 2016.
between 2010 and 2015 (AHRQ, 2016). However, systematic differences in access to care still exist and negatively affect poor households and racial and ethnic minority groups, including Hispanics and African Americans (NCHS, 2016) (see Figure 3-10). In fact, in 2013 people living below the federal poverty level had worse access to care than people in high-income households across all access measures8 (NCHS, 2016). People living in low-income households are at an elevated risk of poor health, and access to care is vital for this vulnerable population. The ACA authorized states to expand Medicaid coverage to adults with low incomes up to 138 percent of the poverty level. From 2013 to 2014, the percent of adults who were uninsured declined in all states, with the decline in the number of uninsured being greater in the states that opted to expand their Medicaid programs (NCHS, 2016).
Racial and ethnic disparities in mental health services exist as well. Members of racial and ethnic minority groups are less likely than whites to receive necessary mental health care and more likely to receive poor-quality care when treated. Specifically, minority patients are less likely than whites to receive the best available treatments for depression and anxiety (McGuire and Miranda, 2008). Among the barriers to access to care, the
___________________
8 Measures of access to care tracked in the 2015 National Healthcare Quality and Disparities Report include having health insurance, having a usual source of care, encountering difficulties when seeking care, and receiving care as soon as wanted.
lack of culturally competent care can be a barrier for specific racial and ethnic groups who face stigma due to cultural norms (Wahowiak, 2015).
The health care system has an important role to play in addressing the social determinants of health. At the community level, it can partner with community-based organizations and explore locally based interventions (Heiman and Artiga, 2015), creating payment models that take into account social determinants and implementing service delivery models that lend themselves to more community engagement and intervention. Health care systems can center equity by involving the community in decision making, allocating resources to act on the determinants of health in mind, and increasing community-based spending (Baum et al., 2009). Communities can be viewed as places of change for health systems, allowing for work both at micro and macro levels. (See Box 3-7 for an example of a community-based health system.) Cost-effective interventions to reduce health disparities and promote health equity should be recognized and explored, including attention to the structural barriers that affect access to health services.
Housing
Housing, as a social determinant of health, refers to the availability or lack of availability of high-quality, safe, and affordable housing for residents at varying income levels. Housing also encompasses the density within a housing unit and within a geographic area, as well as the overall level of segregation and diversity in an area based on racial and ethnic classifications or SES. Housing affects health because of the physical conditions within homes (e.g., lead, particulates, allergens), the conditions in a multi-residence structure (an apartment building or town home), the neighborhoods surrounding homes, and housing affordability, which affects financial stability and the overall ability of families to make healthy choices (Krieger and Higgins, 2002). The Center for Housing Policy has outlined 10 hypotheses on how affordable housing can support health improvement (Maqbool et al., 2015). These range from affordable housing freeing up resources for better nutrition and health care spending to stable housing reducing stress and the likelihood of poor health outcomes (e.g., for mental health or the management of chronic disease).
There is substantive evidence that the physical conditions in homes are important contributors to health outcomes (Cox et al., 2011; WHO, 2006). The World Health Organization (WHO) assessed the evidence in 2005 and found that sufficient evidence was available to estimate the burden of disease for physical factors, such as temperature extremes; chemical factors, such as environmental tobacco smoke and lead; biological factors, such as mold and dust mites; and building factors associated
with injuries and accidents. Since 2005 research has added to the areas where the WHO found some, but not sufficient, evidence to estimate the burden of disease, including more clarity on the relationship between rodent allergens and asthma (Ahluwalia et al., 2013; American College of Allergy Asthma and Immunology, 2014; Sedaghat et al., 2016). Data from the National Health and Nutrition Examination Survey show a decrease in blood lead levels between 1976 and 2002, with a steep drop between 1978 and 1988, probably due to lead being phased out of gasoline, and later a more gradual decrease, perhaps due to a reduction in the use of lead-based paint in housing (Jacobs et al., 2009). Conditions in multiunit residential buildings, including whether indoor smoking is permitted, are another dimension of housing that can affect health outcomes. Box 3-8
introduces the revitalization efforts of one multiunit apartment complex in a community in Minnesota.
Neighborhoods matter for a number of reasons, including their influence on physical safety and access to opportunity. The U.S. Department of Housing and Urban Development’s (HUD’s) Moving to Opportunity program was a 10-year demonstration program, which provided grants to public housing authorities in Baltimore, Boston, Chicago, Los Angeles, and New York City to implement an experimental study—a randomized controlled trial of a housing intervention. Housing authorities
randomly selected experimental groups of households with children [to] receive housing counseling and vouchers that must be used in areas with less than 10 percent poverty. Families chosen for the experimental group receive tenant-based Section 8 rental assistance that helps pay their rent, as well as housing counseling to help them find and successfully use housing in low-poverty areas. Two control groups are included to test the effects of the program: one group already receiving Section 8 assistance and another just coming into the Section 8 program. (HUD, n.d.)
Homeless Populations
For homeless people, a lack of stable housing contributes to disparities in the social determinants. In addition to having direct ties with lack of employment and income, a lack of housing is also associated with greater barriers to education, lower levels of food security, and reduced public safety. Compared to the overall population, homeless people have shorter life expectancies, which are attributable to higher rates of substance abuse, infectious disease, and violence (Baggett et al., 2013). Infectious diseases—including HIV, tuberculosis, and heart disease—have all been linked to shorter life expectancies among homeless people (Fazel et al., 2014). Other studies have found drug overdose, cancer, and heart disease to be the greatest causes of death among the homeless, with greater barriers to and lower rates of screening, diagnosis, and treatment as contributing factors (Baggett et al., 2013).
The Changing American City
Neighborhoods generally change slowly, but urban neighborhoods are seeing dramatic shifts in demographics and property value and over time are becoming more segregated by income (Zuk et al., 2015). Gentrification—the process of renewal and rebuilding, which precedes the influx of new, more affluent residents—is a trend that is being observed in urban centers around the country (McKinnish et al., 2010; Phillips et al., 2014; Sturtevant, 2014). While the literature linking the process of gentrification to health outcomes is not definitive, there is substantial evidence that connects displacement and health outcomes (Zuk et al., 2015). Displacement can occur as a direct result of a policy or program (Freeman and Braconi, 2002), because of recent development and property value increases in an area, or as a result of exclusion from a property for various reasons (Levy et al., 2006).
Displacement has major implications for housing, other social determinants, and the health of communities. According to the CDC, displacement exacerbates health disparities by limiting access to healthy housing, healthy food options, transportation, quality schools, bicycle and walk paths, exercise facilities, and social networks (CDC, 2013). Displacement
leads to poor housing conditions, including overcrowding and exposure to substandard housing with hazardous conditions (e.g., lead, mold, pests) (Phillips et al., 2014). Displacement can result in financial hardship, reducing disposable income for essential goods and services. This can have a negative impact on the health of the displaced population, with income being a significant determinant of health (CDC, 2013).
Physical Environment
The physical environment reflects the place, including the human-made physical components, design, permitted use of space, and the natural environment. Specific features of the physical or built environment include, but are not limited to, parks and open space, what is sold and how it is promoted, how a place looks and feels, air, water, soil, and arts and cultural expression (Davis et al., 2016). All of these physical factors shape the safety, accessibility, and livability of any locale, thus providing the context in which people live, learn, work, and play. This has direct implications for health. The physical environment contributes to 10 percent of health outcomes (Remington et al., 2015). Additionally, 40 percent of health outcomes depend on social and economic factors, which are intricately tied to the features of the physical environment (Remington et al., 2015). Inequities observed between the different physical environments of states, towns, and neighborhoods contribute to disparate health outcomes among their populations.
Exposure to a harmful physical environment is a well-documented threat to community health. Such threats include environmental exposures such as lead, particulate matter, proximity to toxic sites, water contamination, air pollution, and more—all of which are known to increase the incidence of respiratory diseases, various types of cancer, and negative birth outcomes and to decrease life expectancy (Wigle et al., 2007). Low-income communities and communities of color have an elevated risk of exposure to environmental hazards (Evans and Kantrowitz, 2002). In response to these inequities, the field of environmental justice seeks to achieve the “fair treatment and meaningful involvement of all people regardless of race, color, national origin, or income, with respect to the development, implementation, and enforcement of environmental laws, regulations, and policies” (EPA, 2016). Emerging considerations for low-income communities include the resulting gentrification and potential displacement of families when neighborhoods undergo revitalization that is driven by environmental clean-up efforts (Anguelovski, 2016).
Built Environment: Parks and Green Space
Access to green space has been demonstrated to positively affect health in many contexts. Such green space includes both parks and observable greenery. Living in the presence of more green space is associated with a reduced risk of mortality (Villeneuve et al., 2012). Nature has been shown to relieve stress and refocus the mind. Spending time in parks has been shown to improve mental health (Cohen et al., 2016a; Sturm and Cohen, 2014).
Beyond their benefits to mental health and reductions in stress, parks provide opportunities for increased physical activity. Local parks departments manage more than 108,000 outdoor public park facilities across the nation, many of them containing open space, jogging paths, and exercise equipment (Cohen et al., 2016b). According to Cohen et al., the average neighborhood park of 8.8 acres averaged 1,533 hours of active use per week (Cohen et al., 2016b). Individuals who are not as physically active face a greater risk of heart disease, diabetes, and cancer (James et al., 2016). In fact, about 9 percent of premature deaths in the United States are attributable to inactivity (Lee et al., 2012).
The usage of neighborhood parks and the associated health benefits are not equally distributed across communities. Research shows that recreational facilities are much less common in low-income and minority communities, though parks are more evenly distributed (Diez Roux et al., 2007). Moreover, the size and quality of park facilities vary based on race and income (Abercrombie et al., 2008). Accordingly, in low-income communities, residents are less likely to use parks (Cohen et al., 2016a). Beyond race and income, other disparities exist in park use. While seniors represent 20 percent of the population, they account for only 4 percent of park users (Cohen et al., 2016a). Proximity to park facilities also matters, as evidenced by a decrease in physical activity by more than half when distance between one’s home and the park doubles (Giles-Corti and Donovan, 2002).
Food Environment
The food environment refers to the availability of food venues such as supermarkets, grocery stores, corner stores, and farmer’s markets, including food quality and affordability. In communities described as food deserts, there is limited access to affordable and quality food. When there are fewer supermarkets, fruit and vegetable intake is lower, and prices are higher (Powell et al., 2007). This makes achieving a healthy diet difficult for local residents. Research indicates that a poor diet is associated with the development of cancer, diabetes, hypertension, birth defects, and heart disease (Willett et al., 2006).
The distribution of supermarkets is not equitable in the United States. Neighborhoods housing residents of lower socioeconomic status often have fewer supermarkets. Discrepancies also exist between racial and ethnic groups (Powell et al., 2007). Underserved communities turn to small grocery or corner stores to serve their food needs, but these businesses rarely provide the healthy selection offered by larger supermarkets. Moreover, food is most often higher priced in such stores.
Access to and the density of alcohol outlets are also associated with health outcomes in communities. In local areas where liquor store density is higher, alcohol consumption rates in the community are also higher (Pereiram et al., 2013). Alcoholism has been linked to diseases such as cancer, anemia, and mental illnesses. Moreover, alcohol outlets can serve as nuisance businesses, with their clientele bothering others in the neighborhood, decreasing the sense of security, and detracting from social cohesion. There is also evidence that links high-density alcohol outlet areas with higher rates of crime and substance use. In urban environments, a higher concentration of liquor stores is found in low-income, African American, and Hispanic communities, contributing to an elevated risk of alcohol-associated disorders in these neighborhoods (Berke et al., 2010).
A Changing Climate
Climate change has become a public health concern (Wang and Horton, 2015). There is a growing recognition that the physical environment is undergoing changes caused by human activity, such as through the production of greenhouse gases (IPCC, 2014). Human health is intricately linked to the places where we live, learn, work, and play. The air we breathe, the surrounding temperature, the availability of food, and whether there is access to clean water are all important ingredients to a healthy life, and the changing climate will affect all of these areas (Luber et al., 2014).
Not only do polluting emissions make air quality worse in the short term, but climate change itself will worsen air quality. Poor air quality exacerbates previous health conditions such as asthma and chronic obstructive pulmonary disease, and air pollution is associated with cardiovascular disease and many other illnesses. The changing climate is also causing a shift in seasons, which can affect pollen production and therefore seasonal allergies. Overall, with the changing climate there will be more extreme weather events such as increasing drought, vulnerability to wildfires, floods, hurricanes, and winter storms—all with subsequent health impacts from displacement, stress, or primary physical harm. The changing temperature is even having an impact on infectious diseases. New infectious diseases that spread via a vector, such as a tick or
mosquito, have the potential to emerge in previously non-affected areas. There is also a risk for an increase in food-related and waterborne illness caused by the changing temperatures and the survival of various infectious agents. Food insecurity, which is already a challenge in many locations, is at risk of worsening due to higher food prices, poorer nutritional content, and new challenges with distribution.
Although climate change will affect everyone, certain communities and groups will be more vulnerable to these effects. People with preexisting medical conditions, children, elderly populations, and low-income groups are at increased risk for poor outcomes. Existing health disparities that are due to social, economic, and environmental factors have the potential to be even more affected by climate change.
However, climate change also presents a significant opportunity. Given the existential threat to humanity, there is now a great deal of momentum to mitigate and adapt to climate change. Companies are pursuing new business opportunities, governments are forming international agreements, and policies are being implemented at the national, sub-national, state, regional, and local levels to affect change. Many of these policies to adapt to and mitigate climate change are also the key components in creating healthier, more equitable, and resilient communities. There are many co-benefits, and the policies, if implemented correctly, have the potential to significantly improve health outcomes and reduce health disparities (Rudolph et al., 2015). Examples of climate change mitigation and adaptation policies with co-benefits to build healthier, more equitable places include
- Improving access to public transit;
- Promoting flexible workplace transit;
- Creating more complete streets for better pedestrian and bicycle use;
- Implementing urban greening programs;
- Reducing urban heat islands through green space, cool roofs, and cool pavements;
- Promoting sustainable food systems and improved access;
- Building more walkable, dense, affordable housing and amenities;
- Reducing greenhouse gases;
- Promoting weatherizing homes, energy efficiency, and green buildings; and
- Greening fleets and reducing emissions.
Climate change will affect the physical environment in unprecedented ways. To mitigate and adapt to climate change will require multi-sector collaboration and approaches to effect systems change. Many of the same
multi-sector partners required to address the social determinants of health also are already partnering on related climate change work in their communities, creating a substantial opportunity for change (see Box 3-9 for an example of a community engaged in climate change–related work).
Transportation
In the social determinants of health literature, transportation is typically discussed as a feature of the physical (or built) environment (TRB and IOM, 2005). This report highlights transportation as a separate determinant of health because of its multifaceted nature: pollution and
greenhouse gas production; motor vehicle–related deaths and injuries; mobility and access to employment and vital goods and services; and active transportation. Transportation consists of the network, services, and infrastructure necessary to provide residents with the means to get from one place to another (Davis et al., 2016), and it is also vital to accessing goods, services (including health and social services), social networks, and employment. If designed and maintained properly, transportation facilitates safe mobility and is accessible to all residents, regardless of geographic location, age, or disability status. However, current research suggests that transportation costs are a barrier to mobility for households in poverty, which are disproportionately represented by African
Americans and Hispanics (FHWA, 2014). Long commute times and high transportation costs are significant barriers to employment and financial stability (Roberto, 2008). Brookings researchers have concluded, based on analyses of census data, that the suburbanization of poverty is disproportionately affecting proximity to jobs for poor and minority populations as compared with their nonpoor and white peers (Kneebone and Holmes, 2015; Zimmerman et al., 2015).
Transportation presents unevenly distributed negative externalities, including air pollution, noise, and motor vehicle–related injuries and deaths that are more prevalent in low-income and minority communities with poor infrastructure (Bell and Cohen, 2014; US DOT, 2015). Low-income and minority populations are more likely to live near environmental hazards, including transportation-related sources of pollution and toxic emissions such as roadways, bus depots, and ports (McConville, 2013; NEJAC, 2009; Perez et al., 2012). See, for example, Shepard (2005/2006) on the high concentration of bus depots in West Harlem, which also has one of the highest rates of asthma in the nation. The Regional Asthma Management and Prevention collaborative, in Oakland, California, and the California Environmental Protection Agency’s Air Resources Board, among others, have described the evidence on the relationship between asthma and exposures to diesel and other air pollution (California EPA, 2016; RAMP, 2009).
Active transportation—the promotion of walking and cycling for transportation complemented by public transportation or any other active mode—is a form of transportation that reduces environmental barriers to physical activity and can improve health outcomes (Besser and Dannenberg, 2005; Dannenberg et al., 2011). Since the mid-20th century, road design and transportation planning have centered on the automobile, with multiple and interconnected consequences for health and equity (IOM, 2014).
The relationship between physical activity and health is well established and was summarized by the U.S. Surgeon General’s 1996 report Physical Activity and Health (HHS, 1996) and the U.S. Task Force on Community Preventive Services (U.S. Task Force on Community Preventive Services, 2001). The evidence on the relationship among active transportation, physical activity, and health has been accumulating more recently. In a 2005 report from the Transportation Research Board and the Institute of Medicine, the authoring committee stated that “[r]esearch has not yet identified causal relationships to a point that would enable the committee to provide guidance about cost beneficial investments or state unequivocally that certain changes to the built environment would lead to more physical activity or be the most efficient ways of increasing such activity” (TRB and IOM, 2005, p. 10). Since then, Pucher et al. (2010) found
“statistically significant negative relationships” between active travel (walking and cycling) and self-reported obesity as well as between active travel and diabetes (Pucher et al., 2010).
McCormack and Shiell conducted a systematic review of 20 cross-sectional studies and 13 quasi-experimental studies and concluded that most associations “between the built environment and physical activity were in the expected direction or null” (McCormack and Shiell, 2011). They also found that physical activity was considerably influenced by “land use mix, connectivity and population density and overall neighborhood design” and that “the built environment was more likely to be associated with transportation walking compared with other types of physical activity including recreational walking” (McCormack and Shiell, 2011).
CDC has developed a set of transportation recommendations that address all of the facets described above and has also developed a Transportation Health Impact Assessment Toolkit.9 The CDC and the U.S. Department of Transportation (DOT) have also developed a Transportation and Health Tool to share indicator data on transportation and health.10
There have been multiple national initiatives in the past two to three decades aiming to improve livability and sustainability in places across the United States, and transportation equity is a mainstay of much of this work. (See Box 3-10 for an example of a regional transportation planning agency that seeks to improve access to transportation.) Initiatives have ranged from the federal Sustainable Communities Partnership,11 launched by the DOT, HUD, and the U.S. Environmental Protection Agency in 2009 to help U.S. communities “improve access to affordable housing, increase transportation options, and lower transportation costs while protecting the environment,” to Safe Routes to School, which aims to improve children’s safety while walking and riding bicycles.12
Social Environment
How the social environment is conceptualized varies depending on the source (Barnett and Casper, 2001; Healthy People 2020, 2016). However, there are common elements identified by the literature that collectively shape a community’s social environment as a determinant of health.
___________________
9 For more information, see https://www.cdc.gov/healthyplaces/transportation/hia_toolkit.htm (accessed September 21, 2016).
10 For more information, see https://www.transportation.gov/transportation-health-tool (accessed September 21, 2016).
11 For more information, see https://www.sustainablecommunities.gov/mission/about-us (accessed September 21, 2016).
12 For more information, see http://www.saferoutesinfo.org (accessed September 21, 2016).
For the purposes of this report, the social environment can be thought of as reflecting the individuals, families, businesses, and organizations within a community; the interactions among them; and norms and culture. It can include social networks, capital, cohesion, trust, participation, and willingness to act for the common good in relation to health. Social cohesion refers to the extent of connectedness and solidarity among groups in a community, while social capital is defined as the features of social structures (e.g., interpersonal trust, norms of reciprocity, and mutual aid) that serve as resources for individuals and facilitate collective action (Kawachi and Berkman, 2000).
A 2008 systematic review found associations between trust as an indicator of social cohesion and better physical health, especially with respect to self-rated health. Furthermore, it revealed a pattern in which the association between social capital and better health outcomes was especially salient in inegalitarian countries (i.e., countries with a high degree of economic inequity), such as the United States, as opposed to more egalitarian societies (Kim et al., 2008).
The social environment in a community is often measured as it relates to mental health outcomes. For example, social connections between neighbors (i.e., greater social cohesion, social capital, and reciprocal exchanges between neighbors) are protective against depression (Diez Roux and Mair, 2010). Factors such as exposure to violence, hazardous conditions, and residential instability are all associated with depression and depressive symptoms (Diez Roux and Mair, 2010).
It is important to note that high levels of social capital and a strong presence of social networks are not necessarily guarantors of a healthy community. In fact, they can be sources of strain as well as support (Pearce and Smith, 2003). Some studies explore the potential drawbacks of social capital, such as the contagion of high-risk behaviors (e.g., suicidal ideation, injection drug use, alcohol and drug use among adolescents, smoking, and obesity) (Bearman and Moody, 2004; Christakis and Fowler, 2007; Friedman and Aral, 2001; Valente et al., 2004).
Mechanisms
McNeill et al. (2006) postulate that the following are mechanisms by which features of the social environment influence health behaviors:
- Social support and social networks enable or constrain the adoption of health-promoting behaviors; provide access to resources and material goods; provide individual and coping responses; buffer negative health outcomes; and restrict contact to infectious diseases.
- Social cohesion and social capital shape the ability to enforce and reinforce group or social norms for positive health behaviors and the provision of tangible support (e.g., transportation).
The social environment interacts with features of the physical environment at the neighborhood level to shape health behaviors, stress, and, ultimately, health outcomes (Diez Roux and Mair, 2010). For example, a built environment that is poor in quality (i.e., low walkability, fewer parks or open space, unsafe transportation) can contribute to a lack of structural opportunities for social interactions, resulting in limited social networks
in a community (Suglia et al., 2016). Other research points to the role of physical activity as a potential pathway by which the social environment affects health outcomes such as obesity (Suglia et al., 2016).
At the community level, an important element of the social environment that can mediate health outcomes is the presence of neighborhood stressors. While the occurrence of stress is a daily facet of life that all people experience, chronic or toxic stress, in which the burden of stress accumulates, is a factor in the expression of disease (McEwen, 2012). Stressful experiences are particularly critical during early stages of life, as evidenced by the adverse childhood experiences study (Felitti et al., 1998), and are associated with abnormal brain development (IOM, 2000; Shonkoff and Garner, 2012). For low-income communities, stressors are salient because of the lack of resources, the presence of environmental hazards, unemployment, and exposure to violence, among other factors (McEwen, 2012; Steptoe and Feldman, 2001). (See Box 3-11 for an example of a community working to combat these stressors.) This applies as well to children in low-income households, who are more likely to experience multiple stressors that can harm health and development (Evans and Kim, 2010), mediated by chronic stress (Evans et al., 2011).
Chronic stress due to adverse neighborhood and family conditions has been linked to the academic achievement gap, in which children living in poverty fall behind those in better-resourced neighborhoods (Evans et al., 2011; Zimmerman and Woolf, 2014). Furthermore, stress and poor health in childhood are associated with decreased cognitive development, increased tobacco and drug use, and a higher risk of cardiovascular disease, diabetes, depression, and other conditions (County Health Rankings, 2016).
Public Safety
Public safety and violence are significant, intertwined social determinants of health, but they are also each significant indicators of health and community well-being in their own right. Public safety refers to the safety and protection of the public, and it is often characterized as the absence of violence in public settings (Davis et al., 2016). Since the late 1960s, homicide and suicide (another form of violence) have consistently ranked among the top leading causes of death in the United States (Dahlberg and Mercy, 2009).
Violent victimization affects health by causing psychological and physical injury, which can lead to disability and, in some cases, premature death. Beyond the risk of injury and death, violent victimization also has far-reaching health consequences for individuals, families, and neighborhoods. Furthermore, research shows that simply being exposed
to violence can have detrimental effects on physical and psychological well-being (Felitti et al., 1998; Pinderhughes et al., 2015). Violent victimization and exposure to violence have been linked to poor health outcomes, including chronic diseases (e.g., ischemic heart disease, cancer, stroke, chronic obstructive lung disease, diabetes, and hepatitis), asthma-related symptoms, obesity, posttraumatic stress disorder, depression, and substance abuse (Prevention Institute, 2011). For youth in schools, the data suggest that there is a cumulative effect of exposure to violence, with multiple exposures to violence being associated with higher rates of youth reporting their health as “fair” or “poor” (Egerter et al., 2011a). There is also research that indicates a link between neighborhood crime rates and adverse birth outcomes such as preterm birth and low birth weight (Egerter et al., 2011a).
Violence and the fear of violence can negatively affect other social determinants that further undermine community health. Violence rates can lead to population loss, decreased property values and investments in the built environment, increased health care costs, and the disruption of the provision of social services (Massetti and Vivolo, 2010; Velez et al., 2012). In addition, violence in communities is associated with reduced engagement in behaviors that are known to promote health, such as physical activity and park use (Cohen et al., 2010).
The perception of safety is a key indicator of violence in a community that is associated with health. For example, people who describe their neighborhoods as not safe are almost three times more likely to be physically inactive than those who describe their neighborhood as extremely safe (Prevention Institute, 2011). The perception of safety is also important for mental health. There is research that suggests that perceived danger and the fear of violence can influence stress, substance use, anger, anxiety, and feelings of insecurity—all of which compromise the psychological well-being of a community (Moiduddin and Massey, 2008; Perkins and Taylor, 1996). At the community level, fear of crime and violence can undermine social organization, social cohesion, and civic participation—all key elements in a social environment that is conducive to optimal health (Perkins and Taylor, 1996). Low perception of safety can also undermine the efforts of a community to improve the built environment through the availability of parks and open space to promote physical activity (Cohen et al., 2016a; Weiss et al., 2011).
Violence is not a phenomenon that affects all communities equally, nor is it distributed randomly. The widespread disparity in the occurrence of violence is a major facet of health inequity in the United States. Low-income communities are disproportionately affected by violence and by the many effects that it can have on physical and mental well-being. The conditions of low-income communities (concentrated poverty, low housing values, and high schools with low graduation rates among others), foster violence and put residents at an increased risk of death from homicide (Prevention Institute, 2011). This holds true for other types of violence as well. Living in poor U.S. neighborhoods puts African American and white women at an increased risk for intimate partner violence compared with women who reside in areas that are not impoverished (Prevention Institute, 2011).
Criminologists attribute the disparities in neighborhood violence not to the kinds of people living in certain neighborhoods but to the vast differences in social and economic conditions that characterize communities in the United States. Some refer to these differences as “divergent social worlds” and the “racial–spatial divide” (Peterson and Krivo, 2010). This is because there are specific racial and ethnic groups, such as African Americans, Hispanics, and Native Americans, who are vastly overrepresented
in communities that are at risk for violence because of the social and economic conditions. Residential segregation, which has been perpetuated by discriminatory housing and mortgage market practices, affects the quality of neighborhoods by increasing poverty, poor housing conditions, and social disorder and by limiting economic opportunity for residents (Prevention Institute, 2011).
As a result of the racial–spatial divide in community conditions, the violent crime rate in majority nonwhite neighborhoods is two to five times higher than in majority white neighborhoods. This is especially true for youth of color, particularly males. Overall homicide rates among 10- to 24-year-old African American males (60.7 per 100,000) and Hispanic males (20.6 per 100,000) exceed that of white males in the same age group (3.5 per 100,000) (Prevention Institute, 2011). African American males 15 to 19 years old are six times as likely to be homicide victims as their white peers (Prevention Institute, 2011). More specifically, African American males ages 15 to 19 are almost four times as likely to be victims of firearm-related homicides as white males (Prevention Institute, 2011). In terms of exposure to violence, African American and Hispanic youth are more likely to be exposed to shootings, riots, domestic violence, and murder than their white counterparts (Prevention Institute, 2011). This has major implications for trauma in communities that are predominantly African American or Hispanic. Native American communities also suffer from a disproportionately high violent crime rate that is two to three times higher than the national average (Prevention Institute, 2011). Box 3-12 briefly describes a public health–oriented model to address violence in communities.
Child Abuse and Neglect
Child abuse and neglect are two important measures of community violence that can affect physical and mental health. The Institute of Medicine and the National Research Council published a report (2014) that cited abuse and neglect during childhood as a contributor to the following health-related outcomes: problems with growth and motor development, lower self-reported health, gastrointestinal symptoms, obesity, delinquency and violence, and alcohol abuse (IOM and NRC, 2014).
In 1998, Felitti and colleagues published a pivotal study which demonstrated a link between adverse childhood experiences and the leading causes of death in adults at the time. The authors found a strong, graded association between the amount of exposure to abuse or household dysfunction and multiple risk factors (e.g., smoking, severe obesity, physical inactivity, depressed mood, and suicide attempts) for several leading causes of death (Felitti et al., 1998). Child abuse and neglect not only affect health directly, they also affect outcomes within the other social determinants of health, such as education, work, and social relationships (IOM and NRC, 2014). While the overall rates of child maltreatment have been declining since 2002, rates are still much higher for African American (14.3 per 1,000), Native American (11.4 per 1,000), multiracial (10.1 per 1,000), and Hispanic (8.6 per 1,000) children than for white children (7.9 per 1,000) (IOM and NRC, 2014; Prevention Institute, 2011). Child abuse and neglect are often accompanied by family stressors and other forms of family violence (IOM and NRC, 2014). As discussed above, the conditions of concentrated poverty in a neighborhood are associated with violence incidence. According to the Prevention Institute, the higher the percentage of families living below the federal poverty level in a neighborhood, the higher the rate of child maltreatment (Prevention Institute, 2011).
Hate Crimes
Hate crimes, which may or may not involve physical violence, are often motivated by some bias against a perceived characteristic.13 An FBI analysis of single-bias hate crime incidents revealed that in 2014, 48.3 percent of victims were targeted because of the offender’s bias against race, and 62.7 percent of those victims were targeted because of anti-African American bias (UCR, 2015). Among hate crimes motivated by bias toward a particular ethnicity in 2014, almost 48 percent of the victims were targeted because of anti-Hispanic bias (UCR, 2015).
___________________
13 The Hate Crimes Statistics Act (28 U.S.C. § 534) defines hate crimes as “crimes that manifest evidence of prejudice based on race, gender or gender identity, religion, disability, sexual orientation, or ethnicity.”
As is the case with other types of violence, exposure to hate crime violence can have pernicious effects on health. For lesbian, gay, bisexual, and transgender (LGBT) persons specifically, exposure to hate crimes at the community level has been linked to increased rates of suicide among youth, marijuana use, and all-cause mortality (Duncan and Hatzenbuehler, 2014; Duncan et al., 2014; Hatzenbuehler et al., 2014). Discrimination in general, which by definition is the driving factor behind the perpetration of hate crimes, has been shown to affect the health of individuals and communities. Whether it be perceived discrimination in everyday encounters or systemic discrimination in housing policies, this type of unequal treatment has been associated with major depression, psychological distress, stress, increased pregnancy risk, mortality, hypertension, and more health-related outcomes (Dolezsar et al., 2014; Galea et al., 2011; Kessler et al., 1999; Padela and Heisler, 2010; Sims et al., 2012).
Criminal Justice System
The criminal justice system is a key actor, setting, and driver of public safety as it relates to health equity. Specifically, the criminal justice system’s role in the mass incarceration of racial and ethnic minorities is an important factor when examining the social determinants of health (NRC, 2014). The past 40–50 years have seen a large-scale expansion of incarceration, which has had lasting effects on families and communities (Cloud, 2014; Drake, 2013). This expansion has affected racial and ethnic minority groups, and particularly men (Drake, 2013). Research suggests that disproportionately more Hispanics and African Americans are confined in jails and prisons than would be predicted by their arrest rates and that Hispanic and African American juveniles are more likely than white juveniles to be referred to adult court rather than juvenile court (Harris, 2009).
When those who were formerly incarcerated are released back into their communities, successful reentry is hindered by a number of obstacles, such as stigma, limited employment and housing opportunities, and the lack of a cohesive social network (Lyons and Pettit, 2011). All of these factors are vital to achieving optimal health, and for communities with high rates of incarceration, the absence of these opportunities can lead to a diminished capacity to combat crime and mobilize for resources (Clear, 2008). It is important to examine the patterns and effects of mass incarceration because it not only affects the health of incarcerated populations but also has a detrimental effect on multiple determinants of health in communities. Mass incarceration has contributed to the breakdown of educational opportunities, family structures, economic mobility, housing options, and neighborhood cohesion, especially in low-income communities of color (Cloud, 2014). Neal and Rick examined U.S. Census data from
1960 to 2010 and found that although great progress was made in closing the black–white education and employment gap up until the 1980s, that progress then came to a halt in large part due to rising incarceration rates (Neal and Rick, 2014). In addition, communities with high levels of incarceration have higher rates of lifetime major depressive disorder and generalized anxiety disorder (Hatzenbuehler et al., 2015).
Wildeman estimated the effects of incarceration on population-level infant mortality rates, and his findings suggest that if incarceration rates remained the same as they were in 1973, the infant mortality rate in 2003 would have been 7.8 percent lower and the absolute African American–white disparity in infant mortality would have been 14.8 percent lower (Wildeman, 2012). A keen understanding of the precise mechanisms by which incarceration affects the health of specific populations and contributes to health inequity is needed to reduce disparities in key health outcomes such as infant mortality.
CONCLUDING OBSERVATIONS
The root causes of health inequity begin with historical and contemporary inequities that have been shaped by institutional and societal structures, policies, and norms in the United States. As discussed in this chapter, these deeply rooted inequities have shaped inequitable experiences of the social and other determinants of health: education, income and wealth, employment, health systems and services, housing, the physical environment, transportation, the social environment, and public safety.
Conclusion 3-2: Based on its review of the evidence, the committee concludes that health inequities are the result of more than individual choice or random occurrence. They are the result of the historic and ongoing interplay of inequitable structures, policies, and norms that shape lives.
These structures, policies, and norms—such as segregation, redlining and foreclosure, and implicit bias—play out on the terrain of the social, economic, environmental, and cultural determinants of health.
What Can Academic Research Do?
The current public health interest in the role of place, including communities, stems from significant empirical epidemiological evidence. As discussed in this chapter, there are a range of factors that contribute to health and that need to be more extensively studied. These include factors beyond the individual domain, such as living and working conditions and economic policies at the local, state, and national levels that are
intimately connected to health and well-being. Likewise, the American Public Health Association’s (APHA’s) 2014 and 2015 conference themes on the geography of health and health in all policies, respectively, reflect a growing recognition of the need for action on social and environmental factors in order to achieve the goal of becoming the healthiest nation in one generation (APHA, 2016).
At a meeting of the National Academies of Sciences, Engineering, and Medicine’s Roundtable on Population Health Improvement in 2013, David Williams asked, “How could we expect that the lives and health of our patients would improve if they continued to live in the same conditions that contributed to their illness?” (IOM, 2013). His question points to a fundamental challenge to improving the public’s health and promoting health equity. This recognition that inequities in social arrangements and community factors shape life opportunities is not new; it was asserted as early as 1906 by W. E. B. Du Bois in his address regarding the role of social status and life conditions in shaping health and inequities. Du Bois reported findings from the 11th Atlanta Conference on the Study of the Negro Problem held at Atlanta University, which in part concluded that “the present difference in mortality seems to be sufficiently explained by conditions of life” (DuBois, 1906).
Despite the increasingly widespread recognition in the field, many public health efforts continue to target individuals and are most often disease specific. The existing approaches to prevention and health promotion are still “catching up” with what is known about the social determinants of health and population health. Kindig and Stoddart pointed out that “much of public health activity, in the United States at least, does not have such a broad mandate” (Kindig and Stoddart, 2003, p. 382). Building the science base for how to move upstream to improve population health has begun. While our understanding of the role of the social determinants of health, including features of the physical and social environments, has greatly improved over the last several decades, the scientific progress has not been so great on how, when, and where to intervene. Progress on how to move upstream in taking action has developed much more slowly than progress in the ability to describe the role of context and community-level factors that shape the major causes of morbidity, mortality, and well-being (Amaro, 2014).
Improving the science of population health interventions, place-based approaches, and strategies to improve health equity will require a workforce of scientists and practitioners equipped to develop the requisite knowledge base and practice tools. As Kindig and Stoddart noted, social epidemiology has made highly important contributions to our understanding of the social determinants of health and population health but “does not have the breadth, or imply all of the multiple interactions and
pathways” involved in population health (Kindig and Stoddart, 2003, p. 382). Diez Roux and Mair describe social epidemiology’s most critical conceptual and methodological challenges as well as promising directions in studying neighborhood health effects (Diez Roux and Mair, 2010). Specifically, models for the training of population and place-based scientists and practitioners are needed to develop the research required to guide upstream approaches—including place-based interventions—that will address the contextual factors that shape major public health problems such as obesity, interpersonal violence, infant and maternal health, cardiovascular diseases, infectious diseases, substance abuse, and mental health disorders. For example, training models such as the interdisciplinary team science McArthur Model described by Adler and Stewart could be expanded to integrate public health practitioners and community leaders alongside research leaders (Adler and Stewart, 2010b).
Translating knowledge on the social determinants of health into practice requires at least four essential areas of expertise:
- An understanding of theories that articulate the complex mechanisms of action in the social determinants of health and how place influences health.
- Expertise in the design of community-level interventions and in models of community–academic partnerships.
- Expertise in the complex issues of study design, measurement, and analytic methods in assessing changes resulting from interventions focused on population-level impacts and community-level health improvement.
- Expertise and understanding of various socio-demographic groups, cultures, and varied sector stakeholders and drivers that shape sustained stakeholder engagement in improving population health and community conditions.
Considering the distinct fields of expertise required for these components and theory, the approaches to intervention and measurement stem from different disciplines and have often been developed without significant interchange. Researchers face significant challenges. Thus, academic institutions involved in the training of population and place-based scientists need to integrate these diverse bodies of knowledge—including theory, methods, and tools from diverse disciplines. Models for the transdisciplinary training of researchers, practitioners, and community partners are needed. Academic institutions need to develop models for intra-professional workforce training on place-based and community-level implementation science and evaluation that target improving population health and addressing health inequities. See Chapter 7 for more on
the role of academic research in community solutions to promote health equity.
The social determinants of health, while interdependent and complex, are made up of mutable factors that shape the conditions in which one lives, learns, works, plays, worships, and ages. As highlighted in the boxes throughout this chapter, communities around the country are taking it upon themselves to address these conditions. Chapter 4 will discuss why communities are powerful agents of change, along with discussing the conditions necessary for successful and sustainable outcomes. Chapter 5 will provide an in-depth overview of nine communities that are addressing the root causes of health inequities.
REFERENCES
Abercrombie, L. C., J. F. Sallis, T. L. Conway, L. D. Frank, B. E. Saelens, and J. E. Chapman. 2008. Income and racial disparities in access to public parks and private recreation facilities. American Journal of Preventive Medicine 34(1):9–15.
Acevedo-Garcia, D. 2000. Residential segregation and the epidemiology of infectious diseases. Social Science & Medicine 51(8):1143–1161.
Adler, N. E., and J. Stewart. 2010a. Preface to the biology of disadvantage: Socioeconomic status and health. Annals of the New York Academy of Sciences 1186(1):1–4.
Adler, N. E., and J. Stewart. 2010b. Using team science to address health disparities: MacArthur network as case example. Annals of the New York Academy of Sciences 1186: 252–260.
Ahluwalia, S. K., R. D. Peng, P. N. Breysse, G. B. Diette, J. Curtin-Brosnan, C. Aloe, and E. C. Matsui. 2013. Mouse allergen is the major allergen of public health relevance in Baltimore City. Journal of Allergy and Clinical Immunology 132(4):830–835, e831–e832.
AHRQ (Agency for Healthcare Research and Quality). 2016. 2015 National Healthcare Quality and Disparities Report and 5th anniversary update on the National Quality Strategy. AHRQ Pub., No. 16-0015. Rockville, MD: U.S. Department of Health and Human Services.
Aizer, A., J. Currie, P. Simon, and P. Vivier. 2015. Inequality in lead exposure and the black-white test score gap. Institute for Public Policy and Social Research. https://www.ippsr.msu.edu/research/inequality-lead-exposure-and-black-white-test-score-gap (accessed December 9, 2016).
Alhusen, J. L., K. M. Bower, E. Epstein, and P. Sharps. 2016. Racial discrimination and adverse birth outcomes: An integrative review. Journal of Midwifery and Women’s Health October:1–14.
Amaro, H. 2014. The action is upstream: Place-based approaches for achieving population health and health equity. American Journal of Public Health 104(6):964.
American College of Allergy Asthma and Immunology. 2014. Mouse infestations cause more asthma symptoms than cockroach exposure. https://www.sciencedaily.com/releases/2014/11/141107091226.htm (accessed September 21, 2016).
An, J., P. Braveman, M. Dekker, S. Egerter, and R. Grossman-Kahn. 2011. Work, workplaces, and health. Princeton, NJ: Robert Wood Johnson Foundation.
Anguelovski, I. 2016. From toxic sites to parks as (green) LULUs? New challenges of inequity, privilege, gentrification, and exclusion for urban environmental justice. Journal of Planning Literature 31(1):23–36.
APA (American Psychological Association). 2016. Stress in America: The impact of discrimination. Stress in America™ Survey. Washington, DC: American Psychological Association.
APA Task Force on Socioeconomic Status. 2007. Report of the APA Task Force on Socioeconomic Status. Washington, DC: American Psychological Association.
APHA (American Public Health Association). 2016. Past and future annual meetings. American Public Health Association. https://www.apha.org/events-and-meetings/annual/past-and-future-annual-meetings (accessed December 12, 2016).
Baggett, T. P., S. W. Hwang, J. J. O’Connell, B. C. Porneala, E. J. Stringfellow, E. J. Orav, D. E. Singer, and N. A. Rigotti. 2013. Mortality among homeless adults in Boston: Shifts in causes of death over a 15-year period. JAMA Internal Medicine 173(3):189–195.
Baker, D. P., J. Leon, E. G. Smith Greenaway, J. Collins, and M. Movit. 2011. The education effect on population health: A reassessment. Population and Development Review 37(2):307–332.
Balfanz, R., L. Herzog, and D. J. Mac Iver. 2007. Preventing student disengagement and keeping students on the graduation path in urban middle-grades schools: Early identification and effective interventions. Educational Psychologist 42(4):223–235.
Barnett, E., and M. Casper. 2001. A definition of “social environment.” American Journal of Public Health 91(3):465.
Barnett, W. S. 2013. Getting the facts right on pre-K and the President’s pre-K proposal. New Brunswick, NJ: National Institute for Early Education Research.
Baum, F. E., M. Begin, T. A. J. Houweling, and S. Taylor. 2009. Changes not for the fainthearted: Reorienting health care systems toward health equity through action on the social. American Journal of Public Health 99(11):1967–1974.
Baum, S., J. Ma, and K. Payea. 2013. Education pays: The benefits of higher education for individuals and society. Trends in Higher Education. The College Board. http://trends.collegeboard.org/sites/default/files/education-pays-2013-full-report.pdf (accessed October 31, 2016).
Bearman, P. S., and J. Moody. 2004. Suicide and friendships among American adolescents. American Journal of Public Health 94(1):89–95.
Bell, J., and L. Cohen. 2014. The transportation prescription: Bold new ideas for healthy, equitable transportation reform in America. Oakland, CA: PolicyLink and Prevention Institute.
Berger, B. R. 2009. Red: Racism and the American Indian. UCLA Law Review 56(3):591–656.
Berger, M., and Z. Sarnyai. 2015. “More than skin deep”: Stress neurobiology and mental health consequences of racial discrimination. Stress 18(1):1–10.
Berke, E. M., S. E. Tanski, E. Demidenko, J. Alford-Teaster, X. Shi, and J. D. Sargent. 2010. Alcohol retail density and demographic predictors of health disparities: A geographic analysis. American Journal of Public Health 100(10):1967–1971.
Bertrand, M., D. Chugh, and S. Mullainathan. 2005. Implicit discrimination. American Economic Review 95(2):94–98.
Besser, L. M., and A. L. Dannenberg. 2005. Walking to public transit: Steps to help meet physical activity recommendations. American Journal of Preventive Medicine 29(4):273–280.
Betancourt, J. R., and A. R. Green. 2010. Linking cultural competence training to improved health outcomes: Perspectives from the field. Academic Medicine 85(4):583–585.
Betancourt, J. R., J. Corbett, and M. R. Bondaryk. 2014. Addressing disparities and achieving equity: Cultural competence, ethics, and health-care transformation. Chest 145(1):143–148.
Bethell, C. D., P. Newacheck, E. Hawes, and N. Halfon. 2014. Adverse childhood experiences: Assessing the impact on health and school engagement and the mitigating role of resilience. Health Affairs 33(12):2106–2115.
Bishaw, A. 2011. Areas with concentrated poverty: 2006–2010. U.S. Cenus Bureau. http://www.census.gov/prod/2011pubs/acsbr10-17.pdf (accessed November 21, 2016).
Blakely, T. A., B. P. Kennedy, and I. Kawachi. 2001. Socioeconomic inequality in voting participation and self-rated health. American Journal of Public Health 91(1):99–104.
Blount-Hill, K.-L., and J. A. Butts. 2015. Respondent-driven sampling: Evaluating the effects of the Cure Violence model with neighborhood surveys. New York: John Jay College of Crimincal Justice, City University of New York.
BLS (U.S. Bureau of Labor Statistics). 2014. Labor force characteristics by race and ethnicity, 2013. Report 1050. U.S. Bureau of Labor Statistics.
Blumenshine, P., S. Egerter, C. J. Barclay, C. Cubbin, and P. A. Braveman. 2010. Socioeconomic disparities in adverse birth outcomes: A systematic review. American Journal of Preventive Medicine 39(3):263–272.
Boschma, J. 2016. Separate and still unequal. The Atlantic, March 1. http://www.theatlantic.com/education/archive/2016/03/separate-still-unequal/471720 (accessed December 12, 2016).
Boschma, J., and R. Brownstein. 2016. The concentration of poverty in American schools. The Atlantic. February 29. http://www.theatlantic.com/education/archive/2016/02/concentration-poverty-american-schools/471414 (accessed December 2, 2016).
Bradley, E. H., M. Canavan, E. Rogan, K. Talbert-Slagle, C. Ndumele, L. Taylor, and L. A. Curry. 2016. Variation in health outcomes: The role of spending on social services, public health, and health care, 2000–09. Health Affairs 35(5):760–768.
Braveman, P. 2006. Health disparities and health equity: Concepts and measurement. Annual Review of Public Health 27:167–194.
Braveman, P. 2008. Racial disparities at birth: The puzzle persists. Issues in Science and Technology 24(2):23–30.
Braveman, P., and L. Gottlieb. 2014. The social determinants of health: It’s time to consider the causes of the causes. Public Health Reports 129(Suppl 2):19–31.
Braveman, P. A., C. Cubbin, S. Egerter, S. Chideya, K. S. Marchi, M. Metzler, and S. Posner. 2005. Socioeconomic status in health research: One size does not fit all. JAMA 294(22):2879–2888.
Braveman, P., S. Egerter, and D. R. Williams. 2011. The social determinants of health: Coming of age. Annual Review of Public Health 32:381–398.
Brown, D., and T. Tylka. 2011. Racial discrimination and resilience in African American young adults: Examining racial socialization as a moderator. Journal of Black Psychology 37(3):259–285.
Brown, D. J., A. L. DeCorse-Johnson, M. Irving-Ray, and W. W. Wu. 2005. Performance evaluation for diversity programs. Policy, Politics & Nursing Practice 6(4):331–344.
Brulle, R. J., and D. N. Pellow. 2006. Environmental justice: human health and environmental inequalities. Annual Review Public Health 27:103–124.
Buffie, N. 2015. The problem of black unemployment: Racial inequalities persist even amongst the unemployed. CEPR Blog, November 4. Washington, DC: Center for Economic and Policy Research. http://cepr.net/blogs/cepr-blog/the-problem-of-black-unemployment-racial-inequalities-persist-even-amongst-the-unemployed (accessed October 31, 2016).
Burgard, S., and J. Stewart. 2003. Occupational status. MacArthur Research Network on SES & Health. http://www.macses.ucsf.edu/research/socialenviron/occupation.php (accessed December 2, 2016).
Burgard, S., J. E. Brand, and J. S. House. 2007. Toward a better estimation of the effect of job loss on health. Journal of Health and Social Behavior 48(December):369–384.
Butler, M., E. McCreedy, N. Schwer, D. Burgess, K. Call, J. Przedworski, S. Rosser, S. Larson, M. Allen, S. Fu, and R. L. Kane. 2014. Improving cultural competence to reduce health disparities. AHRQ Publication No. 16-EHC006-EF. Prepared by Minnesota Evidence-based Practice Center for Agency for Healthcare Research and Quality. https://effectivehealthcare.ahrq.gov/ehc/products/573/2206/cultural-competence-report-160327.pdf (accessed December 2, 2016).
Butts, J. A., C. G. Roman, L. Bostwick, and J. R. Porter. 2015. Cure Violence: A public health model to reduce gun violence. Annual Review of Health 36:39–53.
California EPA (Environmental Protection Agency). 2016. Asthma and air pollution. https://www.arb.ca.gov/research/asthma/asthma.htm (accessed September 21, 2016).
Carnahan, S. 1994. Preventing school failure and dropout. In Risk, resilience, and prevention: Promoting the well-being of all children, edited by R. Simeonsson. Baltimore, MD: Brookes. Pp. 103–123.
Carter, P. L., and S. F. Reardon. 2014. Inequality matters. William T. Grant Foundation.
CDC (U.S. Centers for Disease Control and Prevention). 2013. Health effects of gentrification. http://www.cdc.gov/healthyplaces/healthtopics/gentrification.htm (accessed October 31, 2016).
Chall, J. S., V. A. Jacobs, and L. E. Baldwin. 1990. The reading crisis: Why poor children fall behind. Cambridge, MA: Harvard University Press.
Charles, C. Z. 2003. The dynamics of racial residential segregation. Annual Review of Sociology 29(1):167–207.
Chetty, R., N. Hendren, R. Chetty, N. Hendren, P. Kline, E. Saez, P. Kline, and E. Saez. 2014. Where is the land of opportunity? The geography of intergenerational mobility in the United States. Quarterly Journal of Economics 129(4):1553–1623.
Chetty, R., M. Stepner, S. Abraham, S. Lin, B. Scuderi, N. Turner, A. Bergeron, and D. Cutler. 2016. The association between income and life expectancy in the United States, 2001–2014. JAMA 315(16):1750–1766.
Chou, R. S., and J. R. Feagin. 2015. Myth of the model minority: Asian Americans facing racism, second edition. Boulder, CO: Paradigm Publishers..
Christ, T., and X. C. Wang. 2010. Bridging the vocabulary gap: What the research tells us about vocabulary instruction in early childhood. Young Children, 84–91.
Christakis, N. A., and J. H. Fowler. 2007. The spread of obesity in a large social network over 32 years. The New England Journal of Medicine 357(4):370–379.
Christian, L. M. 2012. Psychoneuroimmunology in pregnancy: Immune pathways linking stress with maternal health, adverse birth outcomes, and fetal development. Neuroscience & Biobehavioral Reviews 36(1):350–361.
Clear, T. R. 2008. The effects of high imprisonment rates on communities. Crime and Justice 37(1):97–132.
Cloud, D. 2014. On life support: Public health in the age of mass incarceration. New York: Vera Institute of Justice.
Clougherty, J. E., K. Souza, and M. R. Cullen. 2010. Work and its role in shaping the social gradient in health. Annals of the New York Academy of Sciences 1186:102–124.
Cobas, J. A., J. Duany, and J. R. Feagin. 2009. How the United States racializes Latinos: White hegemony and its consequences. Boulder, CO: Paradigm.
Cohen, D. A., B. Han, K. P. Derose, S. Williamson, T. Marsh, L. Raaen, and T. L. McKenzie. 2016a. The paradox of parks in low-income areas: Park use and perceived threats. Environment and Behavior 48(1):230–245.
Cohen, D. A., B. Han, C. J. Nagel, P. Harnik, T. L. McKenzie, K. R. Evenson, T. Marsh, S. Williamson, C. Vaughan, and S. Katta. 2016b. The first national study of neighborhood parks. American Journal of Preventive Medicine 51(4):419–426.
Cohen, L., R. Davis, V. Lee, and E. Valdovinos. 2010. Addressing the intersection: Preventing violence and promoting healthy eating and active living. Oakland, CA: Prevention Institute.
Cohen, R. A., M. E. Martinez, and E. P. Zammitti. 2016c. Health insurance coverage: Early release of estimates from the National Health Interview Survey, 2015. Hyattsville, MD: National Center for Health Statistics.
Conti, G., J. Heckman, and S. Urzua. 2010. The education-health gradient. American Journal of Economic Review 100(2):234–238.
Cooper, L. A., and N. R. Powe. 2004. Disparities in patient experiences, health care processes, and outcomes: The role of patient-provider racial, ethnic, and language concordance. New York: The Commonwealth Fund.
Cooper, L. A., D. L. Roter, R. L. Johnson, D. E. Ford, D. M. Steinwachs, and N. R. Powe. 2003. Patient-centered communication, ratings of care, and concordance of patient and physician race. Annals of Internal Medicine 139(11):907–915.
Correll, J., B. Park, C. M. Judd, and B. Wittenbrink. 2002. The police officer’s dilemma: Using ethnicity to disambiguate potentially threatening individuals. Journal of Personality and Social Psychology 83(6):1314–1329.
Correll, J., B. Park, C. M. Judd, and B. Wittenbrink. 2007. The influence of stereotypes on decisions to shoot. European Journal of Social Psychology 37:1102–1117.
County Health Rankings. 2016. Health factors. http://www.countyhealthrankings.org/our-approach/health-factors (accessed October 11, 2016).
Cox, D. C., G. Dewalt, G. O’Haver, and B. Salatino. 2011. American healthy homes survey: Lead and arsenic findings. U.S. Department of Housing and Urban Development. http://portal.hud.gov/hudportal/documents/huddoc?id=AHHS_Report.pdf (accessed October 31, 2016).
Crissey, S., N. Scanniello, and H. B. Shin. 2007. The gender gap in educational attainment: Variation by age, race, ethnicity, and nativity in the United States. Housing and Household Economic Statistics Division, U.S. Census Bureau. Presented at the Annual Meeting of the Population Association of America, New York, NY, March 29–31, 2007. https://www.census.gov/hhes/socdemo/education/data/acs/CrisseyScannielloShin_poster.pdf (accessed December 12, 2016).
CSDH (Commission on Social Determinants of Health). 2008. Closing the gap in a generation: Health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. Geneva, Switzerland: World Health Organization.
Cure Violence. n.d.-a. The Cure Violence health model. http://cureviolence.org/the-model/essential-elements (accessed December 2, 2016).
Cure Violence. n.d.-b. Summary of findings on Cure Violence. http://cureviolence.org/results/summary-of-findings (accessed December 2, 2016).
Cushing, L., R. Morello-Frosch, M. Wander, and M. Pastor. 2015. The haves, the have-nots, and the health of everyone: The relationship between social inequality and environmental quality. Annual Review of Public Health 36:193–209.
Cutler, D. M., and A. Lleras-Muney. 2006. Education and health: Evaluating theories and evidence. National Bureau of Economic Research working paper no. 12352. http://www.nber.org/papers/w12352 (accessed October 31, 2016).
Cutler, D. M., and A. Lleras-Muney. 2010. Understanding differences in health behaviors by education. Journal of Health Economics 29(1):1–28.
Dahlberg, L. L., and J. A. Mercy. 2009. History of violence as a public health problem. American Medical Association Journal of Ethics 11(2):167–172.
Dale, H. E., B. J. Polivka, R. V. Chaudry, and G. C. Simmonds. 2010. What young African American women want in a health care provider. Qualitative Health Research 20(11):1484–1490.
Dannenberg, A. L., H. Frumkin, and R. J. Jackson. 2011. Making healthy places: Designing and building for health, well-being, and sustainability. Washington, DC: Island Press.
Darity, W. A., J. Dietrich, and D. Guilkey. 2001. Persistent advantage or disadvantage?: Evidence in support of the intergenerational drag hypothesis. American Journal of Economics and Sociology 60(2):435–470.
Davis, R., S. Savannah, M. Harding, A. Macaysa, and L. F. Parks. 2016. Countering the production of inequities: An emerging systems framework to achieve an equitable culture of health. Oakland, CA: Prevention Institute.
De Nardi, M. 2002. Wealth inequality and intergenerational links. Minneapolis: Federal Reserve Bank of Minneapolis.
Deaton, A. 2016. On death and money: History, facts, and explanations. JAMA 315(16):1703–1705.
Derose, K. P., C. R. Gresenz, and J. S. Ringel. 2011. Understanding disparities in health care access—and reducing them—through a focus on public health. Health Affairs 30(10):1844–1851.
Devine, P. G., P. S. Forscher, A. J. Austin, and W. T. Cox. 2012. Long-term reduction in implicit race bias: A prejudice habit-breaking intervention. Journal of Experimental Social Psychology 48(6):1267–1278.
Diez Roux, A. V., and C. Mair. 2010. Neighborhoods and health. Annals of the New York Academy of Sciences 1186(1):125–145.
Diez Roux, A. V., K. R. Evenson, A. P. McGinn, D. G. Brown, L. Moore, S. Brines, and D. R. Jacobs. 2007. Availability of recreational resources and physical activity in adults. American Journal of Public Health 97(3):493–499.
DiJulio, B., M. Norton, S. Jackson, and M. Brodie. 2015. Kaiser Family Foundation/CNN survey of Americans on race. Washington, DC: The Henry J. Kaiser Family Foundation.
Dolezsar, C. M., J. J. McGrath, A. J. Herzig, and S. B. Miller. 2014. Perceived racial discrimination and hypertension: A comprehensive systematic review. Health Psychology 33(1):20–34.
Dovidio, J., and S. L. Gaertner. 2000. Aversive racism and selection decisions: 1989 and 1999. Psychological Science 11(4):315–319.
Dovidio, J., S. L. Gaertner, K. Kawakami, and G. Hodson. 2002. Why can’t we just get along? Interpersonal biases and interracial distrust. Cultural Diversity and Ethnic Minority Psychology 8(2):88–102.
Dow, W. H., and D. H. Rehkopf. 2010. Socioeconomic gradients in health in international and historical context. Annals of the New York Academy of Sciences 1186:24–36.
Doyle, C., P. Kavanagh, O. Metcalfe, and T. Lavin. 2005. Health impacts of employment: A review. Dublin, IE: The Institute of Public Health in Ireland.
Drake, B. 2013. Incarceration gap widens between whites and blacks. Pew Research Center, September 6. http://www.pewresearch.org/fact-tank/2013/09/06/incarceration-gap-between-whites-and-blacks-widens (accessed September 6, 2016).
Dubay, L., T. Joyce, R. Kaestner, and G. M. Kenney. 2001. Changes in prenatal care timing and low birth weight by race and socioeconomic status: Implications for the Medicaid expansions for pregnant women. Health Services Research 36(2):373–398.
DuBois, W. E. B. 1906. Report of a social study made under the direction of Atlanta University. Paper read at The Eleventh Conference for the Study of the Negro Problems, Atlanta, GA.
Duncan, D. T., and M. L. Hatzenbuehler. 2014. Lesbian, gay, bisexual, and transgender hate crimes and suicidality among a population-based sample of sexual-minority adolescents in Boston. American Journal of Public Health 104(2):272–278.
Duncan, D. T., M. L. Hatzenbuehler, and R. M. Johnson. 2014. Neighborhood-level LGBT hate crimes and current illicit drug use among sexual minority youth. Drug and Alcohol Dependence 135:65–70.
Egerter, S., C. Barclay, R. Grossman-Kahn, and P. A. Braveman. 2011a. Violence, social disadvantage and health. Princeton, NJ: Robert Wood Johnson Foundation.
Egerter, S., P. Braveman, T. Sadegh-Nobari, R. Grossman-Kahn, and M. Dekker. 2011b. Education and health. Princeton, NJ: Robert Wood Johnson Foundation.
El-Sayed, A. M., D. W. Finkton, M. Paczkowski, K. M. Keyes, and S. Galea. 2015. Socioeconomic position, health behaviors, and racial disparities in cause-specific infant mortality in Michigan, USA. Preventive Medicine 76:8–13.
EPA (U.S. Environmental Protection Agency). 2016. Environmental justice. https://www.epa.gov/environmentaljustice (accessed October 11, 2016).
Erro, P. n.d. Fresno Hunger Count: Survey methodology. Fresno Hunger Count. http://www.hunger-count.org/uploads/1/3/5/7/13572364/fhc_survey_methodology.pdf (accessed December 12, 2016).
Evans, G. W., and E. Kantrowitz. 2002. Socioeconomic status and health: The potential role of environmental risk exposure. Annual Review of Public Health 23:303–331.
Evans, G. W., and P. Kim. 2010. Multiple risk exposure as a potential explanatory mechanism for the socioeconomic status-health gradient. Annals of the New York Academy of Sciences 1186:174–189.
Evans, G. W., and M. A. Schamberg. 2009. Childhood poverty, chronic stress, and adult working memory. Proceedings of the National Academy of Sciences 106(16):6545–6549.
Evans, G. W., J. Brooks-Gunn, and P. K. Klebanov. 2011. Stressing out the poor: Chronic physiological stress and the income-achievement gap. Pathways. Stanford, CA: Stanford Center on Poverty and Inequality Winter. Pp. 17–21.
Evans-Campbell, T. 2008. Historical trauma in American Indian/Native Alaska communities: A multilevel framework for exploring impacts on individuals, families, and communities. Journal of Interpersonal Violence 23(3):316–338.
Farmer, M. M., and K. F. Ferraro. 2005. Are racial disparities in health conditional on socioeconomic status? Social Science & Medicine 60(1):191–204.
Fazel, S., J. R. Geddes, and M. Kushel. 2014. The health of homeless people in high-income countries: Descriptive epidemiology, health consequences, and clinical and policy recommendations. The Lancet 384(9953):1529–1540.
Feeding America. 2014a. Hungerin America 2015: Executive summary. Feeding America. http://www.feedingamerica.org/hunger-in-america/our-research/hunger-in-america/hia-2014-executive-summary.pdf (accessed December 12, 2016).
Feeding America. 2014b. Map the meal gap 2016: Child food insecurity in California by county in 2014. http://www.feedingamerica.org/hunger-in-america/our-research/map-the-meal-gap/2014/CA_AllCounties_CDs_CFI_2014.pdf (accessed December 12, 2016).
Feinstein, L., R. Sabates, T. M. Anderson, A. Sorhaindo, and C. Hammond. 2006. What are the effects of education on health? Paper presented at Social Outcome of Learning Project Symposium, Copenhagen, Denmark.
Feldman, K. P. 2015. A shadow over Palestine: The imperial life of race in America. Minneapolis: University of Minnesota Press.
Felitti, V. J., R. F. Anda, D. Nordenberg, D. F. Williamson, A. M. Spitz, V. Edwards, M. P. Koss, and J. S. Marks. 1998. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine 14(4):245–258.
FHWA (Federal Highway Administration). 2014. Mobility challenges for households in poverty: 2009 National household travel survey. U.S. Department of Transportation, Federal Highway Administration.
FII (Family Independence Initiative). n.d.-a. About. http://www.fii.org/about (accessed December 2, 2016).
FII. n.d.-b. Mission and vision. http://www.fii.org/mission-and-vision (accessed December 2, 2016).
FII. n.d.-c. Our approach in action. http://www.fii.org/our-approach-in-action (accessed December 2, 2016).
FII. n.d.-d. Resource bank. http://www.fii.org/resource-bank (accessed December 2, 2016).
Flaskerud, J. H. 2012. Coping and health status: John Henryism. Issues in Mental Health Nursing 33(10):712–715.
Freeman, L., and F. Braconi. 2002. Gentrification and displacement. The Urban Prospect 8(1):1–4.
Friedman, S. R., and S. Aral. 2001. Social networks, risk-potential networks, health, and disease. Journal of Urban Health 78(3):411–418.
Fujiwara, T., and I. Kawachi. 2009. Is education causally related to better health? A twin fixed-effect study in the USA. International Journal of Epidemiology 38(5):1310–1322.
Furnee, C. A., W. Groot, and H. M. van den Brink. 2008. The health effects of education: A meta-analysis. European Journal of Public Health 18(4):417–421.
Galea, S., M. Tracy, K. J. Hoggat, C. DiMaggio, and A. Karpati. 2011. Estimated deaths attributable to social factors in the United States. American Journal of Public Health 101(8):1456–1465.
GAO (U.S. Government Accountability Office). 2016. K-12 education: Better use of information could help agencies identify disparities and address racial discrimination. GAO-16-345. U.S. Government Accountability Office. http://www.gao.gov/products/GAO-16-345 (accessed October 31, 2016).
Garcia, E. 2015. Inequalities at the starting gate: Cognitive and noncognitive skills gaps between 2010-2011 kindergarten classmates. Washington, DC: Economic Policy Institute.
Gaskin, D. J., G. Y. Dinwiddie, K. S. Chan, and R. R. McCleary. 2012. Residential segregation and the availability of primary care physicians. Health Services Research 47(6):2353–2376.
Gee, G. C., and C. L. Ford. 2011. Structural racism and health inequities: Old issues, new directions. Du Bois Review: Social Science Research on Race 8(1):115–132.
Gee, G. C., and D. C. Payne-Sturges. 2004. Environmental health disparities: A framework integrating psychosocial and environmental concepts. Environmental Health Perspectives 112(17):1645–1653.
Gee, G. C., A. Ro, S. Shariff-Marco, and D. Chae. 2009. Racial discrimination and health among Asian Americans: Evidence, assessment, and directions for future research. Epidemiology 31:130–151.
Gelman, A., J. Fagan, and A. Kiss. 2007. An analysis of the New York City police department’s “stop-and-frisk” policy in the context of claims of racial bias. Journal of the American Statistical Association 102(479):813–823.
Gilbert, D., S. Wakeling, and V. Crandall. 2016. Strengthening community-police relationships: Training as a tool for change. Oakland: California Partnership for Safe Communities.
Giles-Corti, B., and R. J. Donovan. 2002. The relative influence of individual, social and physical environment determinants of physical activity. Social Science & Medicine 54(12):1793–1812.
Ginsburg, A., P. Jordan, and H. Chang. 2014. Absences add up: How school attendance influences student success. Attendance Works. http://www.attendanceworks.org/research/absences-add (accessed October 19, 2016).
Glossary of Education Reform. 2013. Stereotype threat. http://edglossary.org/stereotype-threat (accessed December 2, 2016).
Godsil, R. D., L. R. Tropp, P. A. Goff, and j. a. powell. 2014. Addressing implicit bias, racial anxiety, and stereotype threat in education and health care. The Perception Institute. http://perception.org/wp-content/uploads/2014/11/Science-of-Equality.pdf (accessed October 31, 2016).
Goldman, D., and J. P. Smith. 2011. The increasing value of education to health. Social Science & Medicine 72(10):1728–1737.
Goodman, N. 2015. The impact of employment on the health status and health care costs of working-age people with disabilities. The National Center on Leadership for the Employment and Economic Advancement of People with Disabilities. http://www.leadcenter.org/system/files/resource/downloadable_version/impact_of_employment_health_status_health_care_costs_0.pdf (accessed October 31, 2016).
Griffith, D. M., M. Mason, M. Yonas, E. Eng, V. Jeffries, S. Plihcik, and B. Parks. 2007. Dismantling institutional racism: Theory and action. American Journal of Community Psychology 39(3–4):381–392.
Griffith, D. M., M. Yonas, M. Mason, and B. E. Havens. 2010. Considering organizational factors in addressing health care disparities: Two case examples. Health Promotion Practice 11(3):367–376.
Grossman, M. 2015. The relationship between health and schooling: What’s new? Cambridge, MA: National Bureau of Economic Research.
Guess, T. J. 2006. The social construction of whiteness: Racism by intent, racism by consequence. Critical Sociology 32(4):649–673.
Hackbarth, D. P., B. Silvestri, and W. Cosper. 1995. Tobacco and alcohol billboards in 50 Chicago neighborhoods: Market segmentation to sell dangerous products to the poor. Journal of Public Health Policy 16(2):213–230.
Hall, J., L. Porter, D. Longhi, J. Becker-Green, and S. Dreyfus. 2012. Reducing adverse childhood experiences (ACE) by building community capacity: A summary of Washington Family Policy Council research findings. Journal of Prevention & Intervention in the Community 40(4):325–334.
Hall, W. J., M. V. Chapman, K. M. Lee, Y. M. Merino, T. W. Thomas, B. K. Payne, E. Eng, S. H. Day, and T. Coyne-Beasley. 2015. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: A systematic review. American Journal of Public Health 105(12):e60–e76.
Hamilton, B. W., J. A. Martin, and M. J. K. Osterman. 2016. National vital statistics reports. Hyattsville, MD: National Center for Health Statistics 65(3).
Harrell, J. P., S. Hall, and J. Taliaferro. 2003. Physiological responses to racism and discrimination: An assessment of the evidence. American Journal of Public Health 93(2):243–248.
Harris, A. 2009. Attributions and institutional processing: How focal concerns guide decision-making in the juvenile court. Race and Social Problems 1(4):243–256.
Hatzenbuehler, M. L., A. Bellatorre, Y. Lee, B. K. Finch, P. Muennig, and K. Fiscella. 2014. Structural stigma and all-cause mortality in sexual minority populations. Social Science & Medicine 103:33–41.
Hatzenbuehler, M. L., K. Keyes, A. Hamilton, M. Uddin, and S. Galea. 2015. The collateral damage of mass incarceration: Risk of psychiatric morbidity among nonincarcerated residents of high-incarceration neighborhoods. American Journal of Public Health 105(1):138–143.
Healthy People 2020. 2016. Social determinants of health. https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health (accessed October 24, 2016).
Heart, M. Y., J. Chase, J. Elkins, and D. B. Altshul. 2011. Historical trauma among Indigenous Peoples of the Americas: Concepts, research, and clinical considerations. Journal of Pyschoactive Drugs 43(4):282–290.
Heiman, H. J., and S. Artiga. 2015. Beyond health care: The role of social determinants in promoting health and health equity. Menlo Park, CA: The Henry J. Kaiser Family Foundation.
HHS (U.S. Department of Health and Human Services). 1996. Physical activity and health: A report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, U.S. Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion.
Hill, J. J., 3rd, M. D. Slade, L. Cantley, S. Vegso, M. Fiellin, and M. R. Cullen. 2008. The relationships between lost work time and duration of absence spells: Proposal for a payroll driven measure of absenteeism. Journal of Occupational and Environmental Medicine 50(7):840–851.
Hood, C. M., K. P. Gennuso, G. R. Swain, and B. B. Catlin. 2016. County Health Rankings: Relationships between determinant factors and health outcomes. American Journal of Preventive Medicine 50(2):129–135.
Howard, T. C. 2010. Why race and culture matter in schools: Closing the achievement gap in America’s classrooms. New York: Teachers College Press.
HUD (U.S. Department of Housing and Urban Development). n.d. Moving to opportunity for fair housing. http://portal.hud.gov/hudportal/HUD?src=/programdescription/mto (accessed September 21, 2016).
Ibrahim, S. A., A. Zhang, M. B. Mercer, M. Baughman, and C. K. Kwoh. 2004. Inner city African-American elderly patients’ perceptions and preferences for the care of chronic knee and hip pain: Findings from focus groups. Journals of Gerontology 59(12):1318–1322.
IEL (Institute for Educational Leadership). n.d. What is a community school? Coalition for Community Schools, Institute for Educational Leadership. http://www.communityschools.org/aboutschools/what_is_a_community_school.aspx (accessed December 12, 2016).
IOM (Institute of Medicine). 2003. Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, DC: The National Academies Press.
IOM. 2006. Genes, behavior, and the environment: Moving beyond the nature/nurture debate. Washington, DC: The National Academies Press.
IOM. 2013. Roundtable on Population Health Improvement: April 2013. http://nationalacademies.org/hmd/Activities/PublicHealth/PopulationHealthImprovementRT/2013-APR-09/Videos/Panel%20Presentations%20and%20Discussion/8-Williams-Video.aspx (accessed December 14, 2016).
IOM. 2014. Applying a health lens to decision making in non-health sectors: Workshop summary. Washington, DC: The National Academies Press.
IOM and NRC (Institute of Medicine and National Research Council). 2000. From neurons to neighborhoods: The science of early childhood development. Washington, DC: National Academy Press.
IOM and NRC. 2014. New directions in child abuse and neglect research. Washington, DC: The National Academies Press.
IPCC (Intergovernmental Panel on Climate Change). 2014. Climate change 2014 synthesis report: Summary for policy. Geneva, Switzerland: Intergovernmental Panel on Climate Change.
Jacobs, D. E., J. Wilson, S. L. Dixon, J. Smith, and A. Evens. 2009. The relationship of housing and population health: A 30-year retrospective analysis. Environmental Health Perspectives 117(4):597–604.
James, P., J. E. Hart, R. F. Banay, and F. Laden. 2016. Exposure to greenness and mortality in a nationwide prospective cohort study of women. Environmental Health Perspectives 124(9):1344–1352.
James, S. A. 1994. John Henryism and the health of African-Americans. Culture, Medicine & Psychiatry 18(2):163–182.
Jemal, A., E. Ward, R. N. Anderson, T. Murray, and M. J. Thun. 2008. Widening of socioeconomic inequalities in U.S. death rates, 1993-2001. PLOS One 3(5):e2181.
Jimenez, M. E., N. E. Reichman, R. Wade, Y. Lin, and L. M. Morrow. 2016. Adverse experiences in early childhood and kindergarten outcomes. Pediatrics 137(2).
Johnson, K. R. 2002. Race and the immigration laws: The need for critical inquiry. In Crossroads, directions and a new critical race theory, edited by F. Valdes, J. M. Culp, and A. P. Harris. Philadelphia, PA: Temple University Press. Pp. 187–198.
Jones, C. P. 2000. Levels of racism: A theoretic framework and a gardener’s tale. American Journal of Public Health 90(8):1212–1215.
Jones, E. 2016. Principled policing. California Police Chief Spring:40–41.
Kang, Y., J. R. Gray, and J. F. Dovidio. 2014. The nondiscriminating heart: Lovingkindness meditation training decreases implicit intergroup bias. Journal of Experimental Psychology 143(3):1306–1313.
Kaufman, J. S., R. S. Cooper, and D. L. Mcgee. 1997. Socioeconomic status and health in blacks and whites: The problem of residual confounding and the resiliency of race. Epidemiology 8:621–628.
Kawachi, I., and L. Berkman. 2000. Social cohesion, social capital, and health. In Social epidemiology, edited by I. Kawachi and L. Berkman. New York: Oxford University Press. Pp. 174–190.
Kena, G., W. Hussar, M. J., C. de Brey, L. Musu-Gillette, X. Wang, J. Zhang, A. Rathbun, S. Wilkinson-Flicker, M. Diliberti, A. Barmer, F. Bullock Mann, and E. Dunlop Velez. 2016. The condition of education 2016 (NCES 2016-144). Washington, DC: U.S. Department of Education, National Center for Education Statistics.
Kessler, R. C., K. D. Mickelson, and D. R. Williams. 1999. The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. Journal of Health and Social Behavior 40:208–230.
Khan, M., and K. Ecklund. 2013. Attitudes toward Muslim Americans post-9/11. Journal of Muslim Mental Health 7(1).
Kim, D., S. Subramanian, and I. Kawachi. 2008. Social capital and physical health: A systematic review of the literature. In Social capital and health, edited by I. Kawachi, S. Subramanian, and D. Kim. New York: Springer Science + Business Media. Pp. 139–190.
Kindig, D., and G. Stoddart. 2003. What is population health? American Journal of Public Health 93(3):380–383.
King, W. D., M. D. Wong, M. F. Shapiro, B. E. Landon, and W. E. Cunningham. 2004. Does racial concordance between HIV-positive patients and their physicians affect the time to receipt of protease inhibitors? Journal of General Internal Medicine 19(11):1146–1153.
Kirst, M. W., and A. Venezia. 2004. From high school to college: Improving opportunities for success in postsecondary education. San Francisco, CA: Jossey-Bass.
Kneebone, E., and N. Holmes. 2015. The growing distance between people and jobs in metropolitan America. Washington, DC: Metropolitan Policy Program at Brookings.
Kokua Kalihi Valley. n.d. Kokua Kalihi Valley. http://www.kkv.net (accessed December 2, 2016).
Krieger, J., and D. L. Higgins. 2002. Housing and health: Time again for public health action. American Journal of Public Health 92(5):758–768.
Krueger, P. M., M. K. Tran, R. A. Hummer, and V. W. Chang. 2015. Mortality attributable to low levels of education in the United States. PLOS One 10(7):e0131809.
Kulwicki, A., R. Khalifa, and G. Moore. 2008. The effects of September 11 on Arab American nurses in metropolitan Detroit. Journal of Transcultural Nursing 19(2):134–139.
Kwate, N. O. A. 2008. Fried chicken and fresh apples: Racial segregation as a fundamental cause of fast food density in black neighborhoods. Health and Place 14(1):32–44.
La Vigne, N. G., P. Lachman, S. Rao, and A. Matthews. 2014. Stop and frisk: Balancing crime control with community relations. Washington, DC: Office of Community Oriented Policing Services.
Landrine, H., and I. Corral. 2009. Separate and unequal: Residential segregation and black health disparities. Ethnicity & Disease 19(2):179–184.
Lauderdale, D. S. 2006. Birth outcomes for Arabic-named women in California before and after September 11. Demography 43(1):185–201.
LaVeist, T. A., and J. M. Wallace. 2000. Health risk and inequitable distribution of liquor stores in African American neighborhood. Social Science and Medicine 51:613–617.
Lee, I. M., E. J. Shiroma, F. Lobelo, P. Puska, S. N. Blair, and P. T. Katzmarzyk. 2012. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. The Lancet 380(9838):219–229.
Lehman, D., P. Fenza, and L. Hillinger-Smith. 2012. Diversity & cultural competency in health care settings. A Mather LifeWays orange paper. Racial and ethnic minority providers disparities cultural competence. https://www.matherlifewaysinstituteonaging.com/wp-content/uploads/2012/03/Diversity-and-Cultural-Competency-in-Health-Care-Settings.pdf (accessed December 2, 2016).
Levesque, C., and K. W. Brown. 2007. Mindfulness as a moderator of the effect of implicit motivational self-concept on day-to-day behavioral motivation. Motivation and Emotion 31(4):284–299.
Levy, D. K., J. Comey, and S. Padilla. 2006. In the face of gentrification: Case studies of local efforts to mitigate displacement. Washington, DC: Urban Institute.
Levy, D. J., J. A. Heissel, J. A. Richeson, and E. K. Adam. 2016. Psychological and biological responses to race-based social stress as pathways to disparities in educational outcomes. American Psychologist 71(6):455–473.
Like, R. C. 2011. Educating clinicians about cultural competence and disparities in health and health care. Journal of Continuing Education in the Health Professions 31(3):196–206.
Losen, D. J., C. L. Hodson, I. Keith, A. Michael, K. Morrison, and S. Belway. 2015. Are we closing the school discipline gap? The Center for Civil Rights Remedies at The Civil Rights Project, UCLA, February. https://www.civilrightsproject.ucla.edu/resources/projects/center-for-civil-rights-remedies/school-to-prison-folder/federal-reports/are-we-closing-the-school-discipline-gap/AreWeClosingTheSchoolDisciplineGap_FINAL221.pdf (accessed December 14, 2016).
Louie, V. 2007. Who makes the transition to college? Why we should care, what we know, and what we need to do. Teachers College Record 109(10):2222–2251.
Luber, G., K. Knowlton, J. Balbus, H. Frumkin, M. Hayden, J. Hess, M. McGeehin, N. Sheats, L. Backer, C. B. Beard, K. L. Ebi, E. Maibach, R. S. Ostfeld, C. Wiedinmyer, E. A. Zielinski-Gutiérrez, and L. Ziska. 2014. Chapter 9: Human health. In Climate change impacts in the United States: The third national climate assessment, edited by J. M. Melillo, T. C. Richmond, and G. W. Yohe. U.S. Global Change Research Program.
Lueke, A., and B. Gibson. 2014. Mindfulness meditation reduces implicit age and race bias: The role of reduced automaticity of responding. Social Psychological and Personality Science 6(3):284–291.
Lundborg, P., C. H. Lyttkens, and P. Nystedt. 2012. Human capital and longevity: Evidence from 50,000 twins. Health, Econometrics and Data Group (HEDG). The University of York. https://www.york.ac.uk/media/economics/documents/herc/wp/12_19.pdf (accessed December 12, 2016).
Lundborg, P., C. H. Lyttkens, and P. Nystedt. 2016. The effect of schooling on mortality: New evidence from 50,000 Swedish twins. Demography 53(4):1135–1168.
Lyons, C. J., and B. Pettit. 2011. Compounded disadvantage: Race, incarceration, and wage growth. Social Problems 58(2):257–280.
Malinowski, P. 2013. Neural mechanisms of attentional control in mindfulness meditation. Frontiers in Neuroscience 7(8).
Maqbool, N., J. Viveiros, and M. Ault. 2015. The impacts of affordable housing on health: A research summary. Washington, DC: Center for Housing Policy, National Housing Conference.
Margo, R. A. 1990. Race and schooling in the south, 1880–1950. Chicago, IL: The University of Chicago Press.
Marmot, M., J. Allen, P. Goldblatt, T. Boyce, D. McNeish, M. Grady, and I. Geddes. 2010. Fair society, healthy lives: Strategic review of health inequalities in England post 2010. London: University College London.
Marulis, L. M., and S. B. Neuman. 2010. The effects of vocabulary intervention on young children’s world learning: A meta-analysis. Review of Educational Research 80(3):300–335.
Massetti, G. M., and A. M. Vivolo. 2010. Achieving public health impact in youth violence prevention through community-research partnerships. Progress in Community Health Partnerships: Research, education, and action 4(3):243–251.
Massey, D. S., and N. A. Denton. 1988. The dimensions of residential segregation. Social Forces 67(2):281–315.
Massey, D. S., and N. A. Denton. 1989. Hypersegregation in U.S. metropolitan areas: Black and Hispanic segregation along five dimensions. Demography 26(3):373–391.
Massie, V. M. 2016. To understand the Dakota Access Pipeline protests, you need to understand tribal sovereignty. Vox, October 28. http://www.vox.com/2016/9/9/12851168/dakota-access-pipeline-protest (accessed December 2, 2016).
Mathews, T. J., and M. F. MacDorman. 2007. Infant mortality statistics from the 2004 period linked birth/infant death data set. National Vital Statistics Reports. Hyattsville, MD: National Center for Health Statistics 55(15):1–32.
Mathews, T. J., M. F. MacDorman, and M. E. Thoma. 2015. Infant mortality statistics from the 2013 period linked birth/infant death data set. National Viral Statistics Reports. Hyattsville, MD: National Center for Health Statistics 64(9):1–30.
Mays, V. M., S. D. Cochran, and N. W. Barnes. 2007. Race, race-based discrimination, and health outcomes among African Americans. Annual Review of Psychology 58:201–225.
McConville, M. 2013. Creating equitable, healthy, and sustainable communities: Strategies for advancing smart growth, environment justice, and equitable development. U.S. Environmental Protection Agency. https://www.epa.gov/sites/production/files/2014-01/documents/equitable-development-report-508-011713b.pdf (accessed October 12, 2016).
McCormack, G. R., and A. Shiell. 2011. In search of causality: A systematic review of the relationship between the built environment and physical activity among young adults. International Journal of Behavioral Nutrition and Physical Activity 8(125).
McDougle, L., D. P. Way, W. K. Lee, J. A. Morfin, B. E. Mavis, D. Matthews, B. A. LathamSadler, and D. M. Clinchot. 2015. A national long-term outcomes evaluation of U.S. premedical postbaccalaureate programs designed to promote health care access and workforce diversity. Journal of Health Care for the Poor and Underserved 26(3):631–647.
McEwen, B. S. 2012. Brain on stress: How the social environment gets under the skin. Proceedings of the National Academy of Sciences 109(Suppl 2):17180–17185.
McGee, R. E., and N. J. Thompson. 2015. Unemployment and depression among emerging adults in 12 states, Behavioral Risk Factor Surveillance System. Preventing Chronic Disease 12(3):140451.
McGinnis, J. M. 2016. Income, life expectancy, and community health: Underscoring the opportunity. JAMA 315(16):1709–1710.
McGinnis, J. M., P. Williams-Russo, and J. R. Knickman. 2002. The case for more active policy attention to health promotion. Health Affairs 21(2):78–93.
McGuire, T. G., and J. Miranda. 2008. New evidence regarding racial and ethnic disparities in mental health: Policy implications. Health Affairs 27(2):393–403.
McKee-Ryan, F., Z. Song, C. R. Wanberg, and A. J. Kinicki. 2005. Psychological and physical well-being during unemployment: A meta-analytic study. Journal of Applied Psychology 90(1):53–76.
McKinnish, T., R. Walsh, and T. K. White. 2010. Who gentrifies low-income neighborhoods? Journal of Urban Economics 67(2):180–193.
McLeroy, K. R., D. Bibeau, A. Steckler, and K. Glanz. 1988. An ecological perspective on health promotion programs. Health Education Quarterly 15:351–377.
McNeill, L. H., M. W. Kreuter, and S. V. Subramanian. 2006. Social environment and physical activity: A review of concepts and evidence. Social Science & Medicine 63(4):1011–1022.
Meara, E., S. Richards, and D. Cutler. 2008. The gap gets bigger: Changes in mortality and life expectancy by education, 1981–2000. Health Affairs 27(2):350–360.
Miller, J. 2015. Community close up: Rolling Hills Apartments, St. Paul, Minnesota. http://buildhealthyplaces.org/whats-new/rolling-hills-apartments-st-paul-minnesota-2 (accessed October 19, 2016).
Minkler, M., A. P. Garcia, J. Williams, T. LoPresti, and J. Lilly. 2010. Si se puede: Using participatory research to promote environmental justice in a Latino community in San Diego, California. Journal of Urban Health 87(5):796–812.
Moiduddin, E., and D. S. Massey. 2008. Neighborhood disadvantage and birth weight: The role of perceived danger and substance abuse. International Journal of Conflict and Violence 2(1):113–129.
Montez, J. K., and L. F. Berkman. 2014. Trends in the educational gradient of mortality among US adults aged 45–84 years: Bringing the regional context into the explanation. American Journal of Public Health 104(1):e82–e90.
Mosavel, M., R. Ahmed, D. Daniels, and C. Simon. 2011. Community researchers conducting health disparities research: Ethical and other insights from fieldwork journaling. Social Science & Medicine 73(1):145–152.
Ms. Foundation for Women. 2015. A Ms. Foundation for Women survey: A fresh look at the public’s view toward issues and solutions. https://d18t6orusej5w.cloudfront.net/wp-content/uploads/2015/10/Ms-National-Survey-Executive-Summary.pdf (accessed December 2, 2016).
Mueller, N., D. Rojas-Rueda, T. Cole-Hunter, A. de Nazelle, E. Dons, R. Gerike, T. Gotschi, L. Int Panis, S. Kahlmeier, and M. Nieuwenhuijsen. 2015. Health impact assessment of active transportation: A systematic review. Preventive Medicine 76:103–114.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2015. The growing gap in life expectancy by income: Implications for federal programs and policy responses. Washington, DC: The National Academies Press.
NASEM. 2016. Systems practices for the care of socially at-risk populations. Washington, DC: The National Academies Press.
Nashville Area Metropolitan Planning Organization. n.d. Nashville Area Metropolitan Planning Organization. http://nashvillempo.org (accessed October 17, 2016).
National Initiative for Building Community Trust and Justice. 2015. Implicit bias. Community-oriented trust and justice briefs. Washington, DC: Office of Community Oriented Policing Services.
NCHS (National Center for Health Statistics). 2016. Health, United States, 2015: With special feature on racial and ethnic health disparities. Hyattsville, MD: U.S. Centers for Disease Control and Prevention.
Neal, D., and A. Rick. 2014. The prison boom and the lack of black progress after Smith and Welch. Working paper 20283. Cambridge, MA: National Bureau of Economic Research.
NEJAC (National Environmental Justice Advisory Council). 2009. Reducing air emissions associated with goods movement: Working towards environmental justice. Washington, DC: U.S. Environmental Protection Agency.
North Carolina Institute of Medicine Task Force on Prevention. 2009. Chapter 11: Socioeconomic determinants of Health. In Prevention for the health of North Carolina: Prevention action plan. Morrisville: North Carolina Institute of Medicine.
NRC (National Research Council). 2012. Education for life and work: Developing transferable knowledge and skills for the 21st century. Washington, DC: The National Academies Press.
NRC. 2014. The growth of incarceration in the United States: Exploring causes and consequences. Washington, DC: The National Academies Press.
NRC and IOM (National Research Council and Institute of Medicine). 2013. U.S. health in international perspective: Shorter lives, poorer health. Washington, DC: The National Academies Press.
OECD (Organisation for Economic Co-operation and Development). 2015. In it together: Why less inequality benefits all . . . in the United States. Organisation for Economic Cooperation and Development. https://www.oecd.org/unitedstates/OECD2015-In-It-Together-Highlights-UnitedStates-Embargo-21May11amPArisTime.pdf (accessed December 1, 2016).
Olshansky, S. J., T. Antonucci, L. Berkman, R. H. Binstock, A. Boersch-Supan, J. T. Cacioppo, B. A. Carnes, L. L. Carstensen, L. P. Fried, D. P. Goldman, J. Jackson, M. Kohli, J. Rother, Y. Zheng, and J. Rowe. 2012. Differences in life expectancy due to race and educational differences are widening, and many may not catch up. Health Affairs 31(8):1803–1813.
Olson, M. E., D. Diekema, B. A. Elliott, and C. M. Renier. 2010. Impact of income and income inequality on infant health outcomes in the United States. Pediatrics 126(6):1165–1173.
Otiniano Verissimo, A. D., C. E. Grella, H. Amaro, and G. C. Gee. 2014. Discrimination and substance use disorders among Latinos: The role of gender, nativity, and ethnicity. American Journal of Public Health 104(8):1421–1428.
Padela, A. I., and M. Heisler. 2010. The association of perceived abuse and discrimination after September 11, 2001, with psychological distress, level of happiness, and health status among Arab Americans. American Journal of Public Health 100(2):284–291.
Paez, K. A., J. K. Allen, M. C. Beach, K. A. Carson, and L. A. Cooper. 2009. Physician cultural competence and patient ratings of the patient-physician relationship. Journal of General Internal Medicine 24(4):495–498.
Pager, D., and H. Shepherd. 2008. The sociology of discrimination: Racial discrimination in employment, housing, credit, and consumer markets. Annual Review of Sociology 34(1):181–209.
Pampel, F. C., P. M. Krueger, and J. T. Denney. 2010. Socioeconomic disparities in health behaviors. Annual Review of Sociology 36:349–370.
Paradies, Y. 2006a. A systematic review of empirical research on self-reported racism and health. International Journal of Epidemiology 35(4):888–901.
Paradies, Y. 2006b. Defining, conceptualizing and characterizing racism in health research. Critical Public Health 16(2):143–157.
Pascoe, E. A., and L. Smart Richman. 2009. Perceived discrimination and health: A meta-analytic review. Psychological Bulletin 135(4):531–554.
Paul, K. I., and K. Moser. 2009. Unemployment impairs mental health: Meta-analyses. Journal of Vocational Behavior 74(3):264–282.
Pearce, N., and G. D. Smith. 2003. Is social capital the key to inequalities in health? American Journal of Public Health 93(1):122–129.
Pereiram, G., L. Wood, S. Foster, and F. Haggar. 2013. Access to alcohol outlets, alcohol consumption and mental health. PLOS One 8(1).
Perez, L., F. Lurmann, J. Wilson, M. Pastor, S. J. Brandt, N. Kunzli, and R. McConnell. 2012. Near-roadway pollution and childhood asthma: implications for developing “win-win” compact urban development and clean vehicle strategies. Environmental Health Perspectives 120(11):1619–1626.
Perkins, D. D., and R. T. Taylor. 1996. Ecological assessments of community disorder: Their relationship to fear of crime and theoretical implications. American Journal of Community Psychology 24(1):63–107.
Peterson, R. D., and L. J. Krivo. 2010. Divergent social worlds: Neighborhood crime and the racial-spatial divide. New York: Russell Sage Foundation.
Pew Research Center. 2016. On views of race and inequality, blacks and whites are worlds apart. Pew Research Center. June 27. http://www.pewsocialtrends.org/2016/06/27/on-views-of-race-and-inequality-blacks-and-whites-are-worlds-apart (accessed October 31, 2016).
Phillips, D., L. Flores, Jr., and J. Henderson. 2014. Development without displacement. Oakland, CA: Causa Justa.
Picard-Fritsche, S., and L. Cerniglia. 2013. Testing a public health approach to gun violence: An evaluation of Crown Heights Save Our Streets, a replication of the Cure Violence model. New York: Center for Court Innovation.
Picker, L. 2007. The effects of education on health. The NBER Digest. National Bureau of Economic Research. March. http://www.nber.org/digest/mar07/w12352.html (accessed October 31, 2016).
Pinderhughes, H., R. A. Davis, and M. Williams. 2015. Adverse community experiences and resilience: A framework for addressing and preventing community trauma. Oakland, CA: Prevention Institute.
Polednak, A. P. 1996. Segregation, discrimination and mortality in U.S. blacks. Ethnicity & Disease 6(1–2):99–108.
Pollack, C. E., C. Cubbin, A. Sania, M. Hayward, D. Vallone, B. Flaherty, and P. A. Braveman. 2013. Do wealth disparities contribute to health disparities within racial/ethnic groups? Journal of Epidemiology & Community Health 67(5):439–445.
Polling Report. n.d. LGBT. http://pollingreport.com/lgbt.htm (accessed December 2, 2016).
Powell, L. M., S. Slater, D. Mirtcheva, Y. Bao, and F. J. Chaloupka. 2007. Food store availability and neighborhood characteristics in the United States. Preventive Medicine 44(3):189–195.
Prevention Institute. 2011. Fact sheet: Links between violence and health equity. Oakland, CA: Prevention Institute.
Priest, N., Y. Paradies, B. Trenerry, M. Truong, S. Karlsen, and Y. Kelly. 2013. A systematic review of studies examining the relationship between reported racism and health and wellbeing for children and young people. Social Science & Medicine 95:115–127.
Pucher, J., R. Buehler, D. R. Bassett, and A. L. Dannenberg. 2010. Walking and cycling to health: A comparative analysis of city, state, and international data. American Journal of Public Health 100(10):1986–1992.
RAMP (Regional Asthma Management and Prevention). 2009. Asthma and diesel. Oakland, CA: Regional Asthma Management and Prevention.
Reardon, S. F., and K. Bischoff. 2016. The continuing increase in income segregation, 2007-2012. Stanford, CA: Stanford Center for Education Policy Analysis.
Reardon, S. F., R. A. Valentino, and K. A. Shores. 2012. Patterns of literacy among U.S. students. Future of Children 22(2):17–37.
Remington, P. L., B. B. Catlin, and K. P. Gennuso. 2015. The County Health Rankings: Rationale and methods. Population Health Metrics 13:11.
Richardson, L. S., and P. A. Goff. 2013. Implicit racial bias in public defender triage. The Yale Law Journal 122(8):2626–2649.
Richeson, J. A., and N. Shelton. 2003. When prejudice does not pay: Effects of interracial contact on executive function. Psychological Science 14(3):287–290.
Roberto, E. 2008. Commuting to opportunity: The working poor and commuting in the United States. Washington, DC: Brookings Institution, Metropolitan Policy Program.
Roberts, C. B., A. I. Vines, J. S. Kaufman, and S. A. James. 2008. Cross-sectional association between perceived discrimination and hypertension in African-American men and women: The Pitt County Study. American Journal of Epidemiology 167(5):624–632.
Rodriguez, J., A. Geronimus, J. Bound, and D. Dorling. 2015. Black lives matter: Differential mortality and the racial composition of the U.S. electorate, 1970–2004. Social Science & Medicine 136–137:193–199.
Rosenbaum, J. E., and A. E. Person. 2003. Beyond college for all: Policies and practices to improve transitions into college and jobs. Professional School Counseling 6(4):252–260.
Ross, A. 2016a. New data highlights vast and persistent racial inequities in who experiences poverty in America. National Equity Atlas. http://nationalequityatlas.org/data-inaction/racial-inequities-poverty-in-america (accessed August 30, 2016).
Ross, A. 2016b. An overview of America’s working poor. National Equity Atlas. http://nationalequityatlas.org/data-in-action/overview-america-working-poor (accessed December 16, 2016).
Rostron, B. L., J. L. Boies, and E. Arias. 2010. Education reporting and classification on death certificates in the United States. National Center for Health Statistics. Vital and Health Statistics 151:1–21.
Rouse, C. E., and L. Barrow. 2006. U.S. elementary and secondary schools: Equalizing opportunity or replicating the status quo? The Future of Children 16(2):99–123.
Rudolph, L., S. Gould, and J. Berko. 2015. Climate change, health, and equity: Opportunities for action. Oakland, CA: Public Health Institute.
RWJF (Robert Wood Johnson Foundation). 2009. Beyond health care. Robert Wood Johnson Foundation Commission to Build a Healthier America.
RWJF. 2015a. Everett culture of health story. http://www.rwjf.org/en/library/articles-and-news/2015/10/coh-prize-everett-ma-story.html (accessed October 21, 2016).
RWJF. 2015b. From vision to action: A framework and measures to mobilize a culture of health. Robert Wood Johnson Foundation. http://www.rwjf.org/content/dam/COH/RWJ000_COH-Update_CoH_Report_1b.pdf (accessed February 7, 2016).
Ryan, C. L., and K. Bauman. 2016. Educational attainment in the United States: 2015. Current Population Reports. U.S. Census Bureau. http://www.census.gov/content/dam/Census/library/publications/2016/demo/p20-578.pdf (accessed October 31, 2016).
Sabin, J., B. A. Nosek, A. Greenwald, and F. P. Rivara. 2009. Physicians’ implicit and explicit attitudes about race by MD race, ethnicity, and gender. Journal of Health Care for the Poor and Underserved 20(3):896–913.
Salway, S., P. Chowbey, E. Such, and B. Ferguson. 2015. Researching health inequalities with community researchers: Practical, methodological and ethical challenges of an “inclusive” research approach. Research Involvement and Engagement 1(1).
Schnittker, J., and K. Liang. 2006. The promise and limits of racial/ethnic concordance in physician-patient interaction. Journal of Health Politics, Policy and Law 31(4):811–838.
Schroeder, S. A. 2007. We can do better—Improving the health of the American people. The New England Journal of Medicine 357:1221–1228.
Schulman, K. A., J. A. Berlin, W. Harless, J. F. Kerner, S. Sistrunk, B. J. Gersh, R. Dubé, C. K. Taleghani, J. E. Burke, S. Williams, J. M. Eisenberg, and J. J. Escarce. 1999. The effect of race and sex on physicians’ recommendations for cardiac catheterization. The New England Journal of Medicine 340(8):618–626.
Sedaghat, A. R., E. C. Matsui, S. N. Baxi, M. E. Bollinger, R. Miller, M. Perzanowski, and W. Phipatanakul. 2016. Mouse sensitivity is an independent risk factor for rhinitis in children with asthma. Journal of Allergy and Clinical Immunology: In Practice 4(1):82–88.
Shapiro, I., C. Murray, and B. Sard. 2015. Basic facts on concentrated poverty. Washington, DC: Center on Budget and Policy Priorities.
Shavers, V. L., P. Fagan, D. Jones, W. M. Klein, J. Boyington, C. Moten, and E. Rorie. 2012. The state of research on racial/ethnic discrimination in the receipt of health care. American Journal of Public Health 102(5):953–966.
Shepard, P. 2005/2006. Breathe at your own risk: Transit justice in West Harlem. Race, Poverty, and the Environment (Winter):51–53.
Shonkoff, J. P., and A. S. Garner. 2012. The lifelong effects of early childhood adversity and toxic stress. Pediatrics 129(1):e232–e246.
Sims, M., A. V. Diez-Roux, A. Dudley, S. Gebreab, S. B. Wyatt, M. A. Bruce, S. A. James, J. C. Robinson, D. R. Williams, and H. A. Taylor. 2012. Perceived discrimination and hypertension among African Americans in the Jackson Heart Study. American Journal of Public Health 102(Suppl 2):S258–S265.
Singh, G. K., and S. M. Yu. 1995. Infant mortality in the United States: Trends, differentials, and projections, 1950 through 2010. American Journal of Public Health 85(7):957–964.
Skiba, R. J., R. H. Horner, C.-G. Chung, M. K. Rausch, S. L. May, and T. Tobin. 2011. Race is not neutral: A national investigation of African American and Latino disproportionality in school discipline. School Psychology Review 40(1):85–107.
Smith, E. J., and S. R. Harper. 2015. Disproportionate impact of K-12 school suspension and expulsion on black students in southern states. Philadelphia: University of Pennsylvania, Center for the Study of Race and Equity in Education.
Smith, S. G., P. A. Nsiah-Kumi, P. R. Jones, and R. J. Pamies. 2009. Pipeline programs in the health professions, part 1: Preserving diversity and reducing health disparities. Journal of the National Medical Association 101(9):836–840, 845–851.
Staats, C., K. Capatosto, R. A. Wright, and V. W. Jackson. 2016. State of the science: Implicit bias review. Columbus, OH: Kirwan Institute for the Study of Race and Ethnicity.
Steptoe, A., and P. J. Feldman. 2001. Neighborhood problems as sources of chronic stress: Development of a measure of neighborhood problems, and associations with socioeconomic status and health. Annals of Behavioral Medicine 23(3):177–185.
Stiefel, M., and K. Nolan. 2012. A guide to measuring the Triple Aim: Population health, experience of care, and per capita cost. Cambridge, MA: Institute for Healthcare Improvement.
Strutz, K. L., V. K. Hogan, A. M. Siega-Riz, C. M. Suchindran, C. T. Halpern, and J. M. Hussey. 2014. Preconception stress, birth weight, and birth weight disparities among US women. American Journal of Public Health 104(8):125–132.
Sturm, R., and D. Cohen. 2014. Proximity to urban parks and mental health. Journal of Mental Health Policy and Economics 17(1):19–24.
Sturtevant, L. 2014. The new District of Columbia: What population growth and demographic change mean for the city. Journal of Urban Affairs 36(2):276–299.
Subramanyam, M. A., S. A. James, A. V. Diez-Roux, D. A. Hickson, D. Sarpong, M. Sims, H. A. Taylor, Jr., and S. B. Wyatt. 2013. Socioeconomic status, John Henryism and blood pressure among African-Americans in the Jackson Heart Study. Social Science & Medicine 93:139–146.
Sue, D. W., C. M. Capodilupo, G. C. Torino, J. M. Bucceri, A. M. Holder, K. L. Nadal, and M. Esquilin. 2007. Racial microaggressions in everyday life: Implications for clinical practice. American Psychologist 62(4):271–286.
Suglia, S. F., R. C. Shelton, A. Hsiao, Y. C. Wang, A. Rundle, and B. G. Link. 2016. Why the neighborhood social environment is critical in obesity prevention. Journal of Urban Health 93(1):206–212.
Sundeen, M. 2016. What’s happening in Standing Rock? Outside, September 2. https://www.outsideonline.com/2111206/whats-happening-standing-rock (accessed December 2, 2016).
Taylor, D. E. 2014. Toxic communities: Environmental racism, industrial pollution, and residential mobility. New York: NYU Press.
Thornton, R. L., C. M. Glover, C. W. Cene, D. C. Glik, J. A. Henderson, and D. R. Williams. 2016. Evaluating strategies for reducing health disparities by addressing the social determinants of health. Health Affairs 35(8):1416–1423.
TRB and IOM (Transportation Research Board and Institute of Medicine). 2005. Does the built environment influence physical activity? Examining the evidence. TRB special report 282. Washington, DC: The National Academies Press.
UCR (Uniform Crime Report). 2015. Hate crime statistics, 2014. Washington, DC: U.S. Department of Justice, Federal Bureau of Investigation. https://ucr.fbi.gov/hatecrime/2014/topic-pages/victims_final.pdf (accessed October 28, 2016).
U.S. Census Bureau. 2015. QuickFacts: Fresno County, California. http://www.census.gov/quickfacts/table/PST045215/06019 (accessed December 12, 2016).
US DOT (U.S. Department of Transportation). 2015. Equity. https://www.transportation.gov/mission/health/equity (accessed September 20, 2016).
U.S. News & World Report. n.d. Reagan High School. http://www.usnews.com/education/best-high-schools/texas/districts/austin-independent-school-district/reagan-high-school-18613 (accessed December 12, 2016).
U.S. Task Force on Community Preventive Services. 2001. Increasing physical activity: A report on recommendations of the Task Force on Community Preventive Services. Morbidity and Mortality Weekly Report 50(RR18):1–16.
Valente, T. W., P. Gallaher, and M. Mouttapa. 2004. Using social networks to understand and prevent substance use: A transdisciplinary perspective. Substance Use & Misuse 39(10-12):1685–1712.
van Ryn, M., and J. Burke. 2000. The effect of patient race and socio-economic status on physicians’ perceptions of patients. Social Science & Medicine 50:813–828.
van Ryn, M., and S. S. Fu. 2003. Paved with good intentions: Do public health and human service providers contribute to racial/ethnic disparities in health? American Journal of Public Health 93(2):248–255.
Velez, M. B., C. J. Lyons, and B. Boursaw. 2012. Neighborhood Housing Investments and Violent Crime in Seattle, 1981-2007. Criminology 50(4):1025–1056.
Villeneuve, P. J., M. Jerrett, J. G. Su, R. T. Burnett, H. Chen, A. J. Wheeler, and M. S. Goldberg. 2012. A cohort study relating urban green space with mortality in Ontario, Canada. Environmental Research 115:51–58.
Volandes, A. E., M. Paasche-Orlow, M. R. Gillick, E. F. Cook, S. Shaykevich, E. D. Abbo, and L. Lehmann. 2008. Health literacy not race predicts end-of-life care preferences. Journal of Palliative Medicine 11(5):754–762.
Wahowiak, L. 2015. Addressing stigma, disparities in minority mental health: Access to care among barriers. The Nation’s Health 45(1). http://thenationshealth.aphapublications.org/content/45/1/1.3.full (accessed October 27, 2016).
Waldron, H. 2007. Trends in mortality differentials and life expectancy for male social security-covered workers, by socieoeconomic status. Social Security Bulletin 67(3):1–28.
Wallace, R., and D. Wallace. 1997. Socioeconomic determinants of health: Community marginalisation and the diffusion of disease and disorder in the United States. BMJ 314(7090):1341–1345.
Wang, H., and R. Horton. 2015. Tackling climate change: The greatest opportunity for global health. The Lancet 386(10006):1798–1799.
Weiss, C. C., M. Purciel, M. Bader, J. W. Quinn, G. Lovasi, K. M. Neckerman, and A. G. Rundle. 2011. Reconsidering access: Park facilities and neighborhood disamenities in New York City. Journal of Urban Health 88(2):297–310.
WHO (World Health Organization). 2006. Report of the WHO technical meeting on quantifying disease from inadequate housing (November 28-30, 2005). Bonn, Germany: World Health Organization, European Centre for Environment and Health.
WHO. 2011. 10 facts on health inequities and their causes. http://www.who.int/features/factfiles/health_inequities/en (accessed December 2, 2016).
Wigle, D. T., T. E. Arbuckle, M. Walker, M. G. Wade, S. Liu, and D. Krewski. 2007. Environmental hazards: Evidence for effects on child health. Journal of Toxicology and Environmental Health 10(1–2):3–39.
Wildeman, C. 2012. Imprisonment and infant mortality. Social Problems 59(2):228–257.
Willett, W. C., J. P. Koplan, R. Nugent, C. Dusenbury, P. Puska, and T. A. Gaziano. 2006. Prevention of chronic disease by means of diet and lifestyle changes. In Disease control priorities in developing countries. New York: Oxford University Press.
Williams, D. R., and C. Collins. 2001. Racial residential segregation: A fundamental cause of racial disparities in health. Public Health Reports 116(September–October):404–416.
Williams, D. R., and S. A. Mohammed. 2009. Discrimination and racial disparities in health: Evidence and needed research. Journal of Behavioral Medicine 32(1):20–47.
Williams, D. R., and S. A. Mohammed. 2013. Racism and health II: A needed research agenda for effective interventions. American Behavioral Scientist 57(8).
Williams, D. R., H. W. Neighbors, and J. S. Jackson. 2003. Racial/ethnic discrimination and health: Findings from community studies. American Journal of Public Health 93(2):200–208.
Williams, D. R., S. A. Mohammed, J. Leavell, and C. Collins. 2010. Race, socioeconomic status, and health: Complexities, ongoing challenges, and research opportunities. Annals of the New York Academy of Sciences 1186:69–101.
Wilson, V. 2016. State unemployment rates by race and ethnicity at the end of 2015 show a plodding recovery. Washington, DC: Economic Policy Institute.
Witt, W. P., H. Park, L. E. Wisk, E. R. Cheng, K. Mandell, D. Chatterjee, and D. Zarak. 2015. Neighborhood disadvantage, preconception stressful life events, and infant birth weight. American Journal of Public Health 105(5):1044–1052.
Woolf, S. H., and J. Q. Purnell. 2016. The good life: Working together to promote opportunity and improve population health and well-being. JAMA 315(16):1706–1708.
Woolf, S. H., R. E. Johnson, R. L. Phillips, and M. Philipsen. 2007. Giving everyone the health of the educated: An examination of whether social change would save more lives than medicine. American Journal of Public Health 2007(97):4.
Woolf, S. H., L. Aron, L. Dubay, S. M. Simon, E. Zimmerman, and K. X. Luk. 2015. How are income and wealth linked to health and longevity? Washington, DC: Urban Institute and Virginia Commonwealth University.
Yonas, M. A., N. Jones, E. Eng, A. I. Vines, R. Aronson, D. M. Griffith, B. White, and M. DuBose. 2006. The art and science of integrating Undoing Racism with CBPR: Challenges of pursuing NIH funding to investigate cancer care and racial equity. Journal of Urban Health 83(6):1004–1012.
Zestcott, C. A., I. V. Blair, and J. Stone. 2016. Examining the presence, consequences, and reduction of implicit bias in health care: A narrative review. Group Processes & Intergroup Relations 19(4):528–542.
Zhang, S., and V. Bhavsar. 2013. Unemployment as a risk factor for mental illness: Combining social psychiatric literature. Advances in Applied Sociology 03(02):131–136.
Zimmerman, E., and S. H. Woolf. 2014. Understanding the relationship between education and health. Discussion paper. Washington, DC: Institute of Medicine.
Zimmerman, R., C. E. Restrepo, H. B. Kates, and R. Joseph. 2015. Final report: Suburban poverty, public transit, economic opportunities, and social mobility. New York: University Transportation Research Center.
Zonderman, A. B., N. A. Mode, N. Ejiogu, and M. K. Evans. 2016. Race and poverty status as a risk for overall mortality in community-dwelling middle-aged adults. JAMA Internal Medicine 176(9):1394–1395.
Zuk, M., A. H. Bierbaum, K. Chapple, K. Gorska, A. Loukaitou-Sideris, P. Ong, and T. Thomas. 2015. Gentrification, displacement, and role of public investment: A literature review. Federal Reserve Bank of San Francisco working paper no. 2015-05. Community Development Investment Center working paper series. http://www.frbsf.org/community-development/publications/working-papers/2015/august/gentrification-displacement-role-of-public-investment (accessed October 31, 2016).






















































































