
4
The Role of Communities in Promoting Health Equity
The previous chapter provided evidence concerning the many social, economic, and environmental factors that shape health and contribute to health disparities, and indicating that successful community-level interventions to improve health equity need to target both people and places. (See Box 4-1 for definitions of community and community-based solution as used in this report.) These factors largely take place in communities but are also affected by larger forces such as state and federal policy (see Chapter 6 for more on the policy context). Community action plays a vital role in effecting sustainable change. This chapter will first discuss why communities and community-driven actions to promote health are essential components in promoting health equity. This is followed by a discussion of the evidence on community-based collaboration. Conditions to foster actions toward health equity are reviewed as are the evidence and data necessary to inform community-driven solutions.
Below, a first-person account of the Thunder Valley Community Development Corporation is provided as an example of the way in which one community organization is promoting health equity.
Taking Community Action to Promote Health Equity: The Thunder Valley Community Development Corporation
Written by Nick Tilsen, Founder and Executive Director of the Thunder Valley Community Development Corporation1

Thunder Valley Community Development Corporation2 (CDC) is a Lakota-led, grassroots, community development organization located on the Pine Ridge Indian Reservation in southwest South Dakota. Thunder Valley CDC has
___________________
1 Committee member Nick Tilsen is the founder and executive director of the Thunder Valley Community Development Corporation.
2 See more at http://thundervalley.org and https://www.youtube.com/watch?v=6aBQ09SjNI (both accessed December 5, 2016).
developed a comprehensive, innovative, and grassroots approach to collaborating with and empowering Lakota youth and families on the Pine Ridge Indian Reservation in order to improve the health, culture, and environment of our community in a way that heals and strengthens our identity. Our organization was founded by a group of young people who were reconnecting to Lakota spirituality and identity through ceremonies. They were presented with a challenge: “When are you going to make a way for your people, are you not warriors? It’s time to stop talking and start doing.” We recognized from that point that it would take systemic change to bring an ecosystem of opportunity to our community and solve the systemic and historic injustices we deal with daily.
The Pine Ridge Reservation is home to about 30,000 Oglala Lakota people. Eighty percent of the population is unemployed, and 50 percent lives below the federal poverty line. Life expectancy on the reservation is the lowest of anywhere in the Western Hemisphere besides Haiti, and the infant mortality rate is five times the national average. Fifty percent of the population is under the age of 18. To address these realities, we launched into deep community engagement with hundreds of hours of listening and visioning sessions with members of our community, including youth, elders, political leaders, and parents (see Figure 4-1 for the community theory of change). We challenged our community to think about what is possible and not just the challenges we face. We received a U.S. Department of Housing and Urban Development Sustainable Communities grant to facilitate this process and create a sustainable development plan for the region.
The community engagement process was at times very challenging—it is difficult to envision and dream about things that you have never seen before. This became evident in some intergenerational tensions. In one community engagement session, children were drawing what they believed was possible for the community on a white board. In the back of the room, there were a couple of elders grumbling that our community could never have these things, that we could not afford them. In that moment, the youth became angry that their hopes and dreams were being challenged. We were able to use that moment to create a mentality shift in the room by challenging the group and asking if it cost anything to dream, and what was the real cost if we did not? This mentality shift gave the elders a perspective in which to participate in the creation of what was possible. In going through this process, Thunder Valley CDC was able to create the Oyate Omniciye Oglala Regional Plan, which was adopted by the Oglala Sioux Tribe as the official Sustainable Regional Planning Document. Thunder Valley CDC has taken on a model community initiative through a 34-acre regenerative community development plan that provides the opportunity to begin to address the lack of physical, political, and economic infrastructure that exists and to create our own pathway out of poverty by building local skill and leadership capacity.
Along with our work to develop the regenerative community in a way that honors our cultural heritage and is adapted for the needs and vision of our local community, we are intentionally disrupting the status quo by creating models
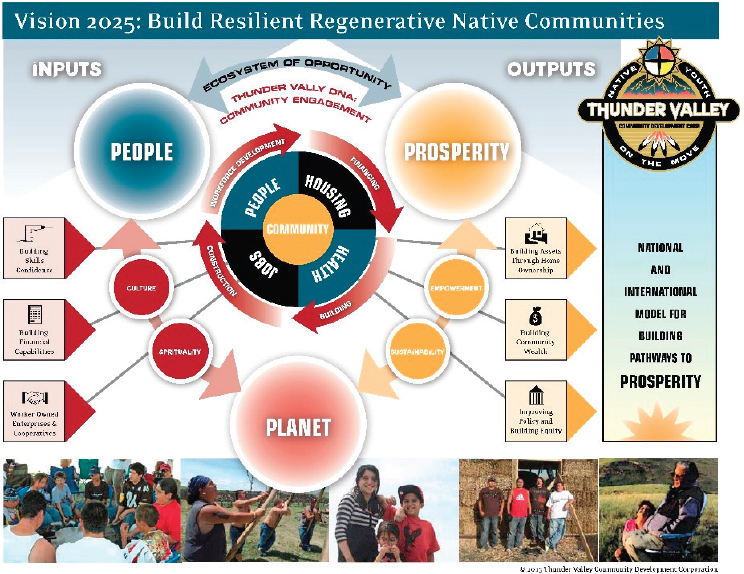
SOURCE: Thunder Valley CDC, 2016.
of change that will overcome intergenerational poverty and build momentum towards regional equity. These initiatives are focused on homeownership, food sovereignty, social enterprise, youth leadership development, regional equity, and the Lakota language.
Through our complex ecosystem of opportunity, the solutions we are creating will be able to address the root inequalities that negatively affect the social determinants of health.
Today, Thunder Valley CDC operates at about $4 million with support from multiple federal agencies, foundations, and individuals, including Northwest Area Foundation, Doris Duke Charitable Foundation, Surdna Foundation, Novo Foundation, W.K. Kellogg Foundation, Administration for Native Americans, and the U.S. Department of Agriculture. We are working to ensure the sustainability of our organization through building the capacity of our community to continue operating and growing the organization as well as ensuring sustainable funding. We also work diligently to try to diversify our funding streams and help shape trends in philanthropy.
To build the capacity of our organization we have been able to identify key people in our community who can be leaders in a specific area. This system builds power in our community by keeping our organization locally run. In addition, a core principle of our organization from the beginning is admitting what we do not know. This has allowed us to bring in consultants and experts from across the country to help build our knowledge of this work, especially in the areas of development and community design.
It is important to us that we are creating repeatable models—not a cookie cutter replica for other communities, but strategies that can be replicated in communities across the United States. To do this we have invested in the evaluation of our organization over the next five years, according to a sustainable triple bottom line, which holds people, planet, and prosperity in equal standing. For this evaluation we are measuring the impact of each of our initiatives and programs, the impact of the regenerative community, and the impact of our organization across the region. We also are measuring our community engagement. Ultimately, our work is aimed at improving health outcomes in our community by creating a healthy community and environment as a catalyst to decreasing health disparities across the reservation.
COMMUNITY ACTION: VITALLY NECESSARY
Community is any configuration of individuals, families, and groups whose values, characteristics, interests, geography, or social relations unite them in some way (adapted from Dreher, 20163). However, the word is used to denote both the people living in a place, and the place itself. In this report the committee generally focuses on shared geography—in other words, community is defined as the people living in a place, such as a neighborhood. Therefore, a community-based solution is an action, policy, program, or law that is driven by the community (members), affects local factors that can influence health, and has the potential to promote health equity.
The potential of community-based solutions to advance health equity is a focus because the Robert Wood Johnson Foundation asked the Committee on Community-Based Solutions to Promote Health Equity in the United States to consider solutions that could be identified, developed, and implemented at the local or community level. However, the report focus should not be interpreted to suggest that community-based
___________________
3 Draft manuscript from Melanie C. Dreher, Rush University Medical Center, provided to staff on February 19, 2016, for the Committee on Community-Based Solutions to Promote Health Equity in the United States. Available by request from the National Academies of Sciences, Engineering, and Medicine’s Public Access Records Office. For more information, email PARO@nas.edu.
solutions represent the primary or sole strategy or the best opportunity to promote health equity. Communities exist in a milieu of national, state, and local level policies, forces, and programs that enable and support or interfere with and impede the ability of community residents and their partners to address the conditions that lead to health inequity. Therefore, the power of community actors is a necessary and an essential, but not a sufficient, ingredient in promoting health equity.
In addition to the support of high level policies, such as those that address structural inequities (e.g., residential segregation), community-based solutions described in this report also rely on multi-sectoral and multilevel collaborations and approaches: for example, engaging business and other nontraditional partners. It is a strength of multi-sectoral collaboration and efforts that are not primarily health focused that they, by definition, ensure diverse approaches to improving community health equity and well-being. Such diverse approaches also are a manifestation of the fact that not all communities start out observing the unfair differences in life expectancy between one side of town and another and thereafter seek to address those inequities. Some communities aim to improve high school graduation or expand affordable housing or create jobs. This report is for communities that believe improving health among their residents is important, but it is also for communities that believe better transit, more affordable housing, safer streets, and more small businesses are important. Whether health is the end or the means to an end, communities can benefit by understanding how health is connected to other goals important to them, and improving education, housing, or employment can also help improve health and mitigate health inequity.
As illustrated in the Thunder Valley CDC example, and detailed in Chapter 3, the community serves as the bedrock of health, a foundation for achieving other important goals, and key to building a productive society. Communities differ in the causes of health inequity they experience, from the availability of health care providers, the affordability and quality of housing, and employment opportunities, to schools, transportation systems, safety, the availability of parks and green space, and other aspects of the physical environment. Some of the challenges faced by vulnerable communities are unique, while others may be common among multiple communities and populations, or they may be present in every community.
Not only is each community unique in the degree and nature of its health inequities, but so too are the means to address those issues, in terms of such resources as locus of power and community values. What communities share, however, is that they are each experts on their local needs and assets and thus need to drive community-based solutions. The nine community examples provided in Chapter 5 illustrate the ability of local community organizations to directly address the determinants of
health in order to improve health inequities. In each case, community action was supported, enabled, or facilitated by federal or state policies and programs because, as noted earlier in this report, community action is a necessary, but not sufficient, contributor to achieving health equity. Communities exist in a milieu of public- and private-sector policies, forces, and programs that enable and support or interfere with and impede the ability of community residents and their partners to address the conditions that lead to health inequity. Community action requires a supportive context, which may range from government policies and programs to the activities of an anchor institution4 such as a university or business.
Many communities strive to achieve greater well being and economic vibrancy. Communities might aim to improve high school graduation rates, expand affordable housing, create more jobs, or improve their children’s health. Whether health is a community’s ultimate goal or the means to an end, communities can benefit by pursuing health equity. Examining health outcomes in the community can help communities understand how health is connected to other desired objectives, and improving education or housing or employment can also help improve health. Communities can see the potential for win-wins. Although it is possible that some communities will notice health disparities and target them as a priority, that is not always the case. When it is not, it may be helpful to encourage communities to consider health equity as a potential co-benefit and to open up additional avenues for measurement, evaluation, and planning. For example, introducing a community coalition working to expand employment opportunities to the concept of health equity could help expand the ways in which members view the value of their collaborative undertaking: that is, not only are they creating jobs and helping to train people for them, this can also have positive effects on health equity in the community. In other words, this report is for communities that believe promoting health equity among their residents is important, but it is also for communities that believe better transit, more affordable housing, complete streets, and more small businesses are essential to a thriving community.
THE EVIDENCE ON COMMUNITY-BASED EFFORTS
Communities might not all be successful at building the type of organizational and collaborative capacity needed to achieve the changes they
___________________
4 Dubb et al. describe an anchor institution as a place-based institution that is tied to its location “by reason of mission, invested capital, or relationships to customers or employees and hence have a vested interest in improving the welfare of their surrounding communities” (Dubb et al., 2013, p. vii).
desire (e.g., improved educational attainment, a more widely accessible transit system) that can also improve health equity. What accounts for successful community interventions for promoting health equity? Why are some communities and organizations able to come together and effect change while others are not? The answers to these questions are complex and involve both the characteristics of the communities and organizations themselves and the broader aspects of the social, economic, environmental, and political context in which communities operate.
The evaluation of community efforts is extremely difficult and complex, both to identify the effects of community action on the determinants of health and to identify the effects on health and health equity (Fawcett et al., 2010). There are multiple barriers, including the complexity of webs of influence and causation and the existence of many confounding variables. Much of the existing research on community-based interventions and on the effectiveness of collaborative efforts to improve community health has been of limited usefulness.5 Research findings have been mixed or negative on the effectiveness of partnerships, and insufficient duration may be one challenge (Shortell et al., 2002). Research also has primarily focused on the “low-hanging fruits” in this space such as individual-level interventions, single interventions,6 and interventions implemented under highly controlled conditions not generalizable to socioculturally diverse communities (Trickett et al., 2011). Tobacco use is one case where the evidence of community-based interventions—along with the evidence on clinical interventions and integration of the two—is robust, as shown by the U.S. Preventive Services Task Force and the Community Task Force (Ockene et al., 2007). The evidence-based nonclinical interventions recommended by the Community Task Force included: smoking bans and restrictions, increasing the unit price for tobacco, and media campaigns.
In 2002, Shortell and colleagues conducted a study of 25 public–private community health partnerships (out of 283 partnerships in the Community Care Network that responded to a request for application from the Health Research and Educational Trust of the American Hospital Association. Between 1995 and 2000, the partnerships had grown from an average of 10 to an average of 22 member organizations, including “hospitals, health systems, managed care organizations, clinics, public health departments, physician organizations, nursing homes, schools and school districts, local government agencies, state health departments, citizen groups, chambers of commerce, social service agencies, and local businesses” (Shortell et al., 2002, p. 52). Based on both qualitative and
___________________
5 A growing body of research, not discussed here, focuses specifically on coalition functioning (see, for example, Shapiro et al., 2015).
6 See, for example, Holder et al., 1997.
quantitative analysis of the partnerships, researchers identified six characteristics shared by the five highest-performing partnerships and absent in the lowest-performing partnerships. These characteristics—“managing partnership size and diversity, developing multiple, approaches to leadership, maintaining focus, managing conflict, recognizing life cycles, and redeploying or patching resources are challenges faced by all community health coalitions in all types of environments”—they concluded (Shortell et al., 2002).
Fawcett and colleagues (2010) provide an overview of some of the factors that contribute to poor performance in achieving population health goals, including health equity, as established in Healthy People 2010, and some of the causes, including challenges in “engaging stakeholders at multiple ecologic levels in building collaborative partnerships for population health.” The authors offer seven recommendations for strengthening collaborative partnerships for population health and health equity: measure progress, “develop and use action plans that assign responsibility,” facilitate natural reinforcement for cross-sectoral collaboration, assure adequate base funding, provide training and technical support, establish participatory evaluation systems to document and review progress and make course corrections, and “arrange group contingencies to ensure accountability for progress and improvement” (Fawcett et al., 2010, p. 5).
A Cochrane Collaboration systematic review and meta-analysis by Hayes and colleagues (2012) examined 16 studies with a total of 28,212 participants “comparing local collaborative partnerships between health and government agencies with standard working arrangements” (Hayes et al., 2012, p. 2). Hayes et al. found only two good-quality studies: one showed no health improvement while the other showed modest benefit. The systematic review also included three studies that examined environmental changes, and two out of three showed some health benefit. In their recent study, Mays and colleagues (2016) examined 16 years worth of data from the National Longitudinal Survey of Public Health Systems based on a sample of 360 metropolitan communities and found decreased mortality from preventable causes in areas with a high level of comprehensive population health system capital. The researchers used a quasi-experimental research design and identified categories of system capital. Communities with comprehensive population health system capital had “a broad scope of population health activities supported through densely connected networks of contributing organizations” (Mays et al., 2016, p. 2007). The study authors noted that it is more challenging to develop comprehensive levels of system capital in rural, low-income, and minority communities, and they suggested that “efforts to build system capital in low-income, minority, and rural communities may go a long way toward reducing inequities in population health” (Mays et al., 2016, p. 2012).
Qualitative and practice-based studies have suggested that certain attributes—including leadership, a backbone or an integrator organization, an infrastructure for collaboration, a common vision, shared language, a strategy for diversifying funding—are required for communities to succeed in health improvement efforts (Community Tool Box, 2016; FSG, 2011, 2013; Hayes et al., 2012; Prybil et al., 2014; Verbitsky-Savitz et al., 2016), and many of these are likely to apply to community efforts to organize and mobilize for health equity as well. In addition to the three elements of health equity as a shared vision and value, collaboration, and capacity, findings suggest that the success of community organization and mobilization for health equity is a function of the following factors:
- the qualities of the community organization itself, such as committed, charismatic leaders, community support, and resources;
- the larger social, economic, environmental, and political conditions that set the stage for change.
These factors are briefly discussed in more detail below.
The characteristics of community organizations, such as having passionate and competent leadership (see, for example, the Delta Health Center and WE ACT for Environmental Justice community examples in Chapter 5), are important for successful interventions for health equity. However, as noted above, communities cannot always achieve sustainable change on their own. Successful community interventions are often not simply the product of extraordinary people doing extraordinary things. Research in sociology and political science indicates that the broader social, economic, environmental, or political context can influence whether organizations succeed, and it is likely that these contextual aspects can also affect the efforts of communities to bring about change (Hojnacki et al., 2012; Polletta, 2008). Evidence from the sociology of social movements may be useful in this context, given the centrality of community organizing to community-driven change efforts (Skocpol et al., 2000), the nearly three-decades-long Healthy Communities movement (Norris and Pittman, 2000), and the relationship between mobilization for political participation and shared membership in a voluntary organization (Campbell, 2013) such as a community health coalition. According to the predominant theories of political process, the political environment, often called the “political opportunity structure,” strongly shapes whether social movement mobilization is successful, sustainable, and leads to substantive policy change (Meyer, 2004; Polletta, 2008). Furthermore, researchers have shown that the ability of communities to organize successfully depends, in part, on the receptivity of local political actors and structures to the communities’ needs (McAdam, 1982).
Scholars measure the openness of political structures in a variety of ways, including the receptivity of elected officials to movement demands (Meyer and Minkoff, 2004), which may be greater if elected officials reflect the demographics of their communities (Browning et al., 1984); the extent to which policy makers have made policy decisions favorable to constituent needs (McAdam, 1982); the ability of minorities to have access to and influence over policy decisions (Eisinger, 1972); and the amenability of the audience, including the voting electorate, to movement issues (Santoro, 2008). These “opportunity structures” facilitate the ability of communities, even in the context of grave challenges, to come together to agree upon and solve problems, including those related to health equity.
For example, the greatest progress in reducing tobacco use in the United States came when local smoking-control ordinances were combined with state and federal efforts to increase tobacco taxes. The taxes not only made cigarettes more expensive, dampening demand; they also helped fund advertising campaigns warning people of the dangers of cigarettes and supported smoking quit lines. This multipronged effort to change policy, backed by a powerful communications and educational strategy, created a snowball of change that transformed norms and expectations around smoking (Prevention Institute, 2014). Ultimately, this changing policy environment sparked and facilitated effective community-led initiatives to reduce smoking-related illness.
Funding is another element of the larger policy context supporting community action. In the Thunder Valley CDC example described earlier, funding from the U.S. Department of Housing and Urban Development (HUD), the U.S. Department of Agriculture (USDA), and foundations allowed the community to create a sustainable development plan for the region. Both state and federal funding decisions can influence how collaboration and community participation unfold on the ground. Funding can also incentivize community participation. For example, the HUD Sustainable Communities Regional Planning Grant Program aims to support locally led collaborative efforts with partnerships that include a range of interests beyond traditional partners—such as arts and culture or recreation organizations, food systems, regional planning agencies, and public education entities—and which target such varied aims as housing and economic development in order to create jobs and regional economic activity (HUD, 2016).
In contrast, some policy environments can negatively affect community efforts to improve health equity. Certain areas suffer disproportionately from poor infrastructure that does not support healthy and walkable communities (e.g., a lack of sidewalks and fully accessible crosswalks). Although planning is a local issue, some states have policies in place to support complete streets policies (Smart Grow America, 2014) at the local
level. When there is not a supportive policy framework at the regional, state, or national level, creating community-level change can be more challenging.
These factors and examples can be applied across all of the determinants of health from a regional, state, and federal policy perspective. To build on the land use and transportation example, the U.S. Department of Transportation’s Transportation Investment Generating Economic Recovery (TIGER) discretionary grants program is helping jurisdictions such as Pittsburgh, Pennsylvania, build infrastructure that will, in Pittsburgh’s case, “reconnect the Hill District to downtown Pittsburgh, more than 60 years after highway and arena construction razed a middle income African American community” through a project that will improve neighborhood streets, sidewalks, and crosswalks, add a bus stop, a bike-sharing station, and Americans with Disabilities Act–compliant walkways, and will create open space for transportation and recreation (DOT, 2016).
ELEMENTS OF SUCCESSFUL COMMUNITY EFFORTS
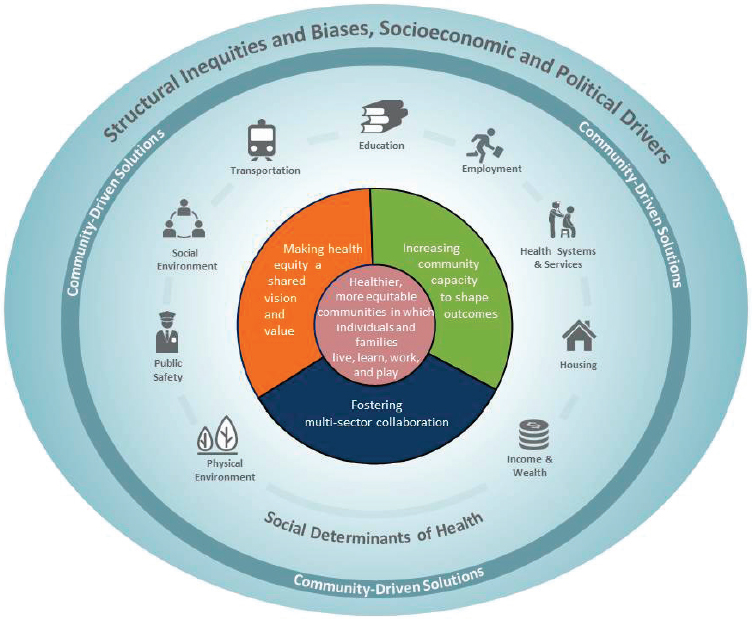
Communities working to promote health equity or to address social or environmental conditions in their neighborhoods may use different types of partnerships that include community-based organizations, local government agencies, and residents themselves. Such varied coalitions represent an important part of the opportunity structure for change. In the section that follows, the committee discusses in detail the three elements identified in its conceptual model introduced in Chapter 1 (see Figure 4-2), which were used to guide its review and selection of illustrative examples of community-based solutions detailed in Chapter 5:
- Multi-sector collaboration
- Health equity as a shared vision and value
- Community capacity to shape outcomes
1. Multi-Sector Collaboration
First, successfully addressing health inequities, like other community interventions, requires the committed collaboration of organizations situated in and outside the health and health care sector (Hoying et al., 2012). The Robert Wood Johnson Foundation (RWJF) Culture of Health Action Framework’s drivers for cross-sectoral collaboration are quality of partnerships, investment in collaboration, and policies that support collaboration (e.g., systems in place to encourage health as a mutual goal on an ongoing basis). Information on the roles of different sectors and
stakeholders is discussed in more detail in Chapter 7, including some examples of work on the horizon.
Many organizations have identified the fostering of cross-sector or multi-sector collaboration as a key ingredient for promoting health and health equity (Mattessich and Rausch, 2014; Prybil et al., 2014). Multisector collaboration—the partnership that results when government, nonprofit organizations, private entities, public organizations, community groups, and individual community members come together to solve problems that affect the whole community—has the potential to solve systemic problems that affect health outcomes. A multi-sector approach challenges the common silo approach to public health (and other fields), wherein advocates work only within their respective fields with little or no communication or alignment across fields. Although much can be learned from expertise in specific fields, the determinants of health do not reside in one sector alone, and no one sector, even health, holds the solution to improving health equity. Moreover, cross-sector collaboration
may also enable community actors to leverage a wider range of supports for community-driven work.
Drawing on the resources, perspectives, and insights of multiple sectors to address a problem increases the likelihood of effective and systemic impact. In their assessment of the association between multi-sector population health activities and health outcomes over time, Mays and colleagues found that communities with comprehensive system capital—rich networks of organizations working together to effect health improvement—experienced significantly lower death rates from preventable conditions (e.g., cardiovascular disease, diabetes, and influenza) compared to communities without this capital (Mays et al., 2016).
Achieving health equity depends on addressing the determinants of health in the broader context in which they are situated (see Figure 4-2). Although there are policy strategies that can have a significant impact on all of the determinants of health, programmatic approaches depend on the community for successful planning, implementation, and sustainability. If there is a focus on any one social or economic determinant, an intervention will require the involvement of the multiple sectors that overlap with the area of interest. For example, transportation affects (access to) housing, education, employment: thus, only a multi-sector collaboration that brings together stakeholders from these other areas will succeed. The overarching milieu in which all these disparate sectors come and work together is the community itself.
One implication of this is that openness is an important characteristic of successful community organizations. Open contexts (to use a term drawn from the sociology literature) encourage constituencies of historically marginalized populations to mobilize and advocate for government responses to their concerns. For example, the Dudley Street Neighborhood Initiative, the Indianapolis Congregation for Action, and WE ACT for Environmental Justice (see Chapter 5 for more information on these community examples) engage and empower traditionally excluded communities through leadership development. Open contexts can engender trust in the political system among historically marginalized populations and thus encourage residents of minority neighborhoods to become civically engaged, develop a sense of attachment to and ownership of their neighborhoods, and mobilize on behalf of neighborhood concerns (Bobo and Gilliam, 1990; Williams, 1998). Open contexts can also provide resources and opportunities across a myriad of domains that enhance community capacity and viability (Lyons et al., 2013). In contrast, closed contexts are less receptive and responsive to the claims and needs of marginalized constituencies. In relatively closed contexts, even the most impassioned leadership can fail to produce sustained and successful interventions (Lyons et al., 2013).
2. Health Equity as a Shared Vision and Value
Effective community partnerships have a “well-articulated and shared vision” (Shortell et al., 2002; see also Mattesich and Rausch, 2014), and it is reasonable to expect that success in addressing health inequities also requires a shared vision and shared values. Holding health equity as a shared vision and value is an aspirational notion; in many community-based partnerships to address any number of community challenges, health equity may simply be an implicit vision and value.
Shared value refers to two relevant concepts. One dimension of shared value refers to social or cultural values. In this context, the set of beliefs and ideas held in common that allow collaborators to work together despite differences (e.g., in social status, sector, philosophy, race and ethnicity, and ability) in order to craft interventions that have the sufficient resources, cultural awareness, and inclusiveness as well as a path to sustainability for lasting change (RWJF, 20157). The other dimension of shared value comes from the business literature—particularly the work of Porter and Kramer (2011)—and refers to “policies and operating practices that enhance the competitiveness of a company while simultaneously advancing the economic and social conditions in the communities in which it operates. Shared value creation focuses on identifying and expanding the connections between societal and economic progress” (Porter and Kramer, 2011). Combining the two meanings therefore means that a shared vision is the “glue” that holds multi-sector collaboration together, elevating the desired change above individual and organizational interests in order to improve the health and well-being of all those who are part of the community.
3. Community Capacity to Shape Outcomes
Third, increasing community capacity to shape outcomes is a recurring theme and need, as the committee found while reviewing community examples and the relevant literature (see, for example, Hargreaves et al., 2016; Hoying et al., 2012). Community capacity refers to the ability of communities to come together to identify common needs and to build
___________________
7 The RWJF Culture of Health Action Framework identifies making health a shared value as one of its four action areas for realizing a culture of health in the United States. The drivers identified for making health a shared value include “mindsets and expectations” that promote health and well-being as a priority, civic engagement, and a sense of community (the social connections needed for a community to thrive). The description of the framework’s first dimension states “Making Health a Shared Value emphasizes the importance of individuals, families, and communities in prioritizing and shaping a Culture of Health. Everyone should feel engaged with their community’s decisions and believe that they have a voice in the process” (RWJF, 2015).
social and political capital by drawing on ties with actors both inside (including residents, local businesses, and elected officials) and outside of the community (Chaskin, 1999). Thus defined, the concept of community capacity parallels other concepts central to research on different dimensions of community well-being. Notions of power, community empowerment, social network ties, and social capital are also relevant to this discussion of community capacity. In the organizational behavior literature, power is defined as asymmetrical control over valued resources (Anderson and Brion, 2014), and scholarship in political science reflects on power relations and on the formation of social capital (Campbell, 2013; Jacobs and Soss, 2010). Robert Putnam’s (2000) research identified and measured five broad dimensions of social capital: community organizational life, engagement in public affairs, community volunteerism, informal sociability, and social trust (see also NRC, 2014). In the sociology of community safety and crime, “collective efficacy” (Sampson et al., 1997) refers to the ability of residents of a given area to exert control over the behavior of individuals and groups and thereby create a safe and orderly environment. Collective efficacy, like community capacity, requires some degree of trust, cohesion, and shared norms of intervention for the common good of the community. Community members who come to know and trust their neighbors and have a sense of ownership and belonging in the place where they live are more likely to work collectively to solve common problems related to promoting health equity.
True community-led action is only possible insofar as communities have the capacity to organize for health equity. For a community to be able to change the conditions in which its members live, members need the capacity and ability to act—they need vision, leadership, voice, and power (see Box 4-2). Thus, building community capacity is the primary mechanism that ensures the democratization of decision making around health equity. Furthermore, community capacity (and community involvement more generally) is key for sustained change (Verbitsky-Savitz et al., 2016). For change to be long lasting, normative innovations need to be adopted into the very fabric of community social life. Communities with a greater capacity for social organization and collective efficacy are more adept at integrating change into community life because members of the community are themselves part of the intervention.
As discussed earlier, a community movement or action does not occur spontaneously. What Doran Schrantz from ISAIAH, a faith-based coalition, calls “invisible work” needs to be done first: “the work of organizers and organizations like ISAIAH or [the PICO Network] or countless other community organizations across this country. There are conversations at kitchen tables, in church basements, in little meeting rooms, [and] in your
neighborhood in which people go through the experience of being trained and how to have the public skills to pull that off” (Schrantz, 2016).
Depending on the community challenges being addressed, the appropriate range of knowledge and experience will need to be assembled. For example, a kindergarten-through-12th-grade intervention would ideally have expertise not only in education but also in cognitive development, the social environment, public safety, transportation, and other sectors, and the intervention would need to engage parents, caregivers, and, when appropriate, students themselves. Individuals participating from different sectors bring to the table a wide range of knowledge and skills, and there may well be a need for capacity to work collaboratively, with attention given to differences in power and status, in order to attain authentic partnerships with members of the affected community. See, for example, the Magnolia Community Initiative in Chapter 5 for a collaborative community initiative with partners across government, nonprofits, private entities, and faith organizations. Just as a shared vision is important to unite a multi-sector collaboration, authentic partnership with representatives from all affected community segments is essential to help community interventions succeed.
The current state of community health inequities did not emerge overnight or in a vacuum. Policies that intentionally or unintentionally create structural inequities based on bias, whether conscious or unconscious, and discrimination, whether blatant or subtle, continue to shape communities; some are decades old, and others are recent or under consideration. Communities working on interventions to achieve health equity need to engage in dialogue about or directly address these structural challenges in order to pursue effective and successful programs.
Conclusion 4-1: Making health equity a shared vision and value, building community capacity, and fostering multi-stakeholder collaboration are vital in the development of community-driven solutions for promoting health equity.
Conclusion 4-2: It is essential for entities initiating efforts to promote health equity in communities (e.g., government agencies, foundations, and other funders) to require explicit strategies for achieving authentic community engagement and ownership at each stage of such efforts. Specifically, it is important for leaders of such efforts to document and describe on an ongoing basis the engagement of different parts of the community, particularly residents not usually at the table and those most affected by inequitable health conditions.
BUILDING EVIDENCE TO SUPPORT COMMUNITY ACTION
There are numerous examples of successful community-based solutions that promote health equity. However, the partners involved in working to promote community-level intervention have faced challenges to achieving success. Based on the literature concerning the elements that support successful community-level intervention, on examining case examples, and on evaluating current gaps, it is clear that increasing the right kinds of evidence base (see Box 4-3), training, and access to experience would support further advancements in community-level action.
Evidence Base for Community Solutions
A major barrier to the spread of effective community solutions is the mismatch between what may be the most promising solutions and the knowledge base that is available for communities to draw on (Schorr, 2016). The current knowledge base consists primarily of programs or individualized interventions that have been shown to work with the use of experimental methods of evaluation, especially randomized controlled
trials. As with evidence-based public health practice and policy more broadly (Fielding and Briss, 2006), such traditional methods are a poor fit with the knowledge needed to design and implement cross-sector community solutions that will be effective in achieving health equity. Currently more is known about the problems of health inequities than about the solutions. Additionally, more is known about the programs that have worked in the past to marginally improve health equity than about the strategies and broad, interactive, crosscutting interventions that could bring greater and more widespread progress in the future.
Building an Evidence Infrastructure Toward Greater Impact
Efforts to design and implement cross-sector community solutions are hampered by the absence of an infrastructure to support knowledge development and dissemination, implementation, continuous improvement, and expanded data collection to inform this evidence base (see data discussions in Chapters 2 and 8 for more information). A strengthened infrastructure to guide community-level interventions will (1) identify the essential elements of successful interventions; (2) take account of the power of systems to determine results; and (3) assist all stakeholders to engage in ongoing disciplined inquiry.
1. Identify the essential elements of successful interventions.
An intervention’s essential elements—or core components, active ingredients, or effectiveness factors—are the functions or principles and activities necessary to achieve successful outcomes, including the implementation and contextual conditions of the solution (e.g., political and regulatory context or funding). When these attributes can be described, communities can be much more rigorous and intentional about what can be and needs to be adapted and what needs to be held constant. The National Scientific Council on the Developing Child reviewed the evidence on commonalities among child care environments that promote healthy development and found that the critical elements are ensuring “that relationships in child care are nurturing, stimulating, and reliable, [leading to] an emphasis on the skills and personal attributes of the caregivers, and on improving the wages and benefits that affect staff turnover” (National Scientific Council on the Developing Child, 2004). This finding is at odds with policies that predominantly define “quality” in terms of more easily quantified but less meaningful metrics such as adult–child ratios, group size, and physical facilities (National Scientific Council on the Developing Child, 2004).
Once identified, these essential elements can be re-bundled to fit a new population and unique circumstances. They are portable, effective guides to action, and can have a multiplying effect because they are more transferable to a wider range of settings than model programs. As noted earlier in the chapter, Thunder Valley CDC has invested in long-term evaluation plans to identify the core elements of its programs and inform strategies in other communities.
To systematically extract these essential elements requires good data, rigorous analysis, and thoughtful judgment as well as the infrastructure and desire to create a better understanding of the core elements of programs, contexts, and systems change aimed at significant outcomes.
2. Take account of the power of systems to determine results.
Much of what makes interventions effective is often undermined by the systems in which they operate, especially when the intervention is expanded to reach large numbers. As Patrick McCarthy, president of The Annie E. Casey Foundation, has pointed out, if the road to scale is to reach ambitious goals, it needs to run through public systems (McCarthy, 2014). And decades of experience, McCarthy says, “tell us that a bad system will trump a good program—every time, all the time” (McCarthy, 2014). Whether a community-based collaboration is concerned with youth in the juvenile justice system, students in public schools, families in the child welfare system, the youngest children and their families, or the survivors of domestic violence, even the greatest program cannot succeed in a lasting way if it is housed in a dysfunctional system. It is illusory to think
that an effective intervention can be scaled without full recognition of the power of the system that can determine program priorities, budget allocations, staffing levels, and eligibility criteria, and that can nurture or sabotage a culture of trust.
3. Assist all stakeholders to engage in “ongoing disciplined inquiry.”
To achieve greater impact in the future will require applying evidence that is generated by ongoing disciplined inquiry among practitioners, policy makers, and researchers. This ongoing disciplined inquiry needs to be based on a deep understanding of the problem it seeks to solve, of the systems that produce the current outcomes, of the detailed practical knowledge necessary for good ideas to actually work, and a willingness to constantly reassess operations and make changes that evidence and experience suggest will lead to improvement.
Community College Pathways (CCP) is an example of ongoing, disciplined inquiry in action. The Carnegie Foundation for the Advancement of Teaching created CCP in response to the extraordinarily high failure rates among the half million community college students annually assigned to remedial math instruction as a prerequisite to taking college-level courses. CCP consists of a network of college faculty, administrators, researchers, program designers, and implementers working together to “achieve big results, reliably and at scale” (CSSP, 2016b) for community college students struggling with remedial math. When CCP began, 80 percent of the students enrolled in these courses did not complete or pass them. Through monthly meetings to learn from the real-world experience of network participants and by adapting research-based ideas from diverse domains, CCP networks changed the way that remedial math classes are conducted, introduced new e-curricula, changed students’ own expectations about their ability to succeed at math, and developed support networks among students. Within 2 years, CCP tripled the success rates of remedial math students, who consistently outperformed comparison group students. CCP is now working in ever-wider circles to show how disciplined inquiry can develop effective responses to a problem previously perceived as intractable (Bryk et al., 2015).
In selecting interventions or elements of intervention to implement, communities attempting to draw from existing directories of effective programs find a severely limited knowledge base (Hayes et al., 2012; Schorr, 2016; Woulfe et al., 2010). Even when it comes to individual programmatic interventions that have been shown to have an impact in the contexts in which they have been tested, users cannot reliably conclude that the same intervention will produce similar results in their own system or community (CSSP, 2016a).
Communities determined to promote health equity by bridging the gaps among research, practice, and policy recognize the need to go beyond identifying and scaling up individual “evidence-based” programs. As they pursue broader change in the conditions for health, they find a dearth of systematic, organized information and guidance to help them set common goals and measures of success; select multifaceted and mutually reinforcing strategies, grounded in strong theory; align implementation efforts, and make the necessary system and community-level changes to adapt and continuously improve. A centralized resource for communities is needed, and several partially relevant models exist, some of which could potentially be modified to operate in an expanded capacity. These include the County Health Rankings (CHR) What Works for Health database, the CDC Community Health Improvement (CHI) Navigator, and also, perhaps, the Agency for Healthcare Research and Quality’s (AHRQ’s) Measures Clearinghouse and the National Library of Medicine (which serves as a knowledge curation resource through its special queries). The CHR What Works for Health database provides information for community health improvement organized by expected beneficial outcomes, potential beneficial outcomes, evidence of effectiveness, effect on disparities, implementation examples, implementation resources, and citations. The CHI Navigator8 is intended for individuals and groups who lead or participate in community health improvement work
within hospitals and health systems, public health agencies, and other community organizations. It is a one-stop shop that offers community stakeholders expert-vetted tools and resources for depicting visually the who, what, where, and how of improving community health; making the case for collaborative approaches to community health improvement; establishing and maintaining effective collaborations; and finding interventions that work for the greatest impact on health and well-being for all. (CDC, 2015)
Recommendation 4-1: A public–private consortium9 should create a publicly available repository of evidence to inform and guide efforts to promote health equity at the community level. The consortium should also offer support to communities, including technical assistance.
___________________
8 For more information, see http://www.cdc.gov/chinav (accessed December 5, 2016).
9 This could be done through such mechanisms as a collaboration among CDC (home of the Community Health Improvement Navigator initiative), university-based centers (see the example of the University of Wisconsin Population Health Institute that operates the County Health Rankings [CHR] What Works for Health database), and one or more philanthropic organizations.
The repository could include databases that provide and integrate information from multiple relevant sectors (e.g., education, health, housing) at the national, state, and metropolitan levels as well as for smaller local geographies such as census tracts; and information on effective intervention approaches and the knowledge necessary to strengthen the capacity of communities to take action on such needs as educational attainment, job training and job creation, civil rights, decent and stable housing, and other determinants of health by race, ethnicity, gender, disability status, age, sexual identity/orientation, and other demographic characteristics. Providing relevant assistance, guidance, and support to local community leaders (e.g., identifying data sources, accessing funding available from federal agencies, and using civil rights law) could improve the chances of success for community organizations. Creating or building on existing resources that could become a repository of information and a source of technical assistance could also be complemented by efforts to build learning networks, thus allowing communities to share experiences with other local community leaders (see, for example, the possibilities suggested by Community Commons10 and others).
REFERENCES
Anderson, C., and S. Brion. 2014. Perspectives on power in organizations. Annual Review of Organizational Psychology and Organizational Behavior 1(1):67–97.
Bobo, L., and F. D. Gilliam. 1990. Race, sociopolitical participation, and black empowerment. American Political Science Review 84(2):377–393.
Browning, R. P., D. R. Marshall, and D. H. Tabb. 1984. Protest is not enough: The struggle of blacks and Hispanics for equality in urban politics. Berkeley: University of California Press.
Bryk, A. S., L. M. Gomez, A. Grunow, and P. G. LeMahieu. 2015. Learning to improve: How America’s schools can get better at getting better. Cambridge, MA: Harvard Education Press.
Campbell, D. 2013. Social networks and political participation. Annual Review of Political Science 16:33–48.
CDC (U.S. Centers for Disease Control and Prevention). 2015. CDC community health improvement navigator. https://www.cdc.gov/chinav (accessed December 5, 2016).
CIL Management Center. 2005. Community organizing: Ground rules for grass roots organizers. Chapter 10: Leadership development. 10.3: Leadership development skills. http://wnyil.org/community-organizing/chapter10_3.html (accessed October 18, 2016).
Chaskin, R. J. 1999. Defining community capacity: A framework and implications from a comprehensive community initiative. Chicago, IL: Chapin Hall Center for Children at the University of Chicago.
___________________
10 For more information, see https://www.communitycommons.org (accessed December 5, 2016).
Community Tool Box. 2016. Chapter 1. Section 7. Working together for healthier communities: A framework for collaboration among community partnership, support organizations, and funders. http://ctb.ku.edu/en/table-of-contents/overview/model-for-community-change-and-improvement/framework-for-collaboration/main (accessed October 18, 2016).
CSSP (Center for the Study of Social Policy). 2016a. Better evidence for decision-makers. Washington, DC: Center for the Study of Social Policy.
CSSP. 2016b. Carnegie math pathways: Case study. http://www.cssp.org/policy/body/Carnegie-Math-Pathways.pdf (accessed October 26, 2016).
DOT (U.S. Department of Transportation). 2016. Tiger discretionary grants. https://www.transportation.gov/tiger (accessed October 13, 2016).
Dubb, S., S. McKinley, and T. Howard. 2013. Achieving the anchor promise: Improving outcomes for low-income children, families and communities. Takoma Park, MD: The Democracy Collaborative at the University of Maryland.
Eisinger, P. K. 1972. The conditions of protest behavior in American cities. Madison: University of Wisconsin.
Fawcett, S. B., J. Schultz, J. Watson-Thompson, M. Fox, and R. Bremby. 2010. Building multisectoral partnerships for population health and health equity. Preventing Chronic Disease 7(6):1–7.
Felitti, V. J., R. F. Anda, D. Nordenberg, D. F. Williamson, A. M. Spitz, V. Edwards, M. P. Koss, and J. S. Marks. 1998. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine 14(4):245–258.
Fielding, J. E., and P. A. Briss. 2006. Promoting evidence-based public health policy: Can we have better evidence and more action? Health Affairs (Millwood) 25(4):969–978.
FSG (Foundation Strategy Group). 2011. Collective impact. http://www.fsg.org/ideas-in-action/collective-impact (accessed October 18, 2016).
FSG. 2013. Using collective impact in a public health context: Introduction. http://www.fsg.org/blog/using-collective-impact-public-health-context-introduction (accessed October 18, 2016).
Hargreaves, M. B., N. Verbitsky-Savitz, B. Coffee-Borden, L. Perreras, P. J. Pecora, C. Roller White, G. B. Morgan, T. Barila, A. Ervin, L. Case, R. Hunter, and K. Adams. 2016. Advancing the measurement of collective capacity to address adverse childhood experiences and resilience. Gaithersburg, MD: Community Science.
Hayes, S. L., M. K. Mann, F. M. Morgan, H. Kitcher, M. J. Kelly, and A. L. Weightman. 2012. Collaboration between local health and local government agencies for health improvement. The Cochrane Database of Systematic Reviews (10):Cd007825.
Hojnacki, M., D. C. Kimball, F. R. Baumgartner, J. M. Berry, and B. L. Leech. 2012. Studying organizational advocacy and influence: Reexamining interest group research. Annual Review of Political Science 15(1):379–399.
Holder, H. D., R. F. Saltz, J. W. Grube, R. B. Voas, P. J. Gruenewald, and A. J.Treno. 1997. A community prevention trial to reduce alcohol-involved accidental injury and death: Overview. Addiction 92 (Suppl 2):S155–S171.
Hoying, A., N. Sambourskiy, and B. Sanders. 2012. A structured approach to effective partnering: Lessons learned from public and private sector leaders. Atlanta, GA: U.S. Centers for Disease Control and Prevention.
HUD (U.S. Department of Housing and Urban Development). 2016. Sustainable communities regional planning grants. http://portal.hud.gov/hudportal/HUD?src=/program_offices/economic_resilience/sustainable_communities_regional_planning_grants (accessed October 18, 2016).
Jacobs, L. R., and J. Soss. 2010. The politics of inequality in America: A political economy framework. Annual Review of Political Science 13(1):341–364.
Kania, L., and M. Kramer. 2011. Collective impact. Stanford Social Innovation Review Winter:36-41. https://ssir.org/articles/entry/collective_impact (accessed October 18, 2016).
Lyons, C. J., M. B. Velez, and W. A. Santoro. 2013. Neighborhood immigration, violence, and city-level immigrant political opportunities. American Sociological Review 78(4):604–632.
Mattessich, P. W., and E. J. Rausch. 2014. Cross-sector collaboration to improve community health: A view of the current landscape. Health Affairs 33(11):1968–1974.
Mays, G. P., C. B. Mamaril, and L. R. Timsina. 2016. Preventable death rates fell where communities expanded population health activities through multisector networks. Health Affairs (Millwood) 35(11):2005–2013.
McAdam, D. 1982. Political process and the development of black insurgency, 1930-1970. Chicago, IL: University of Chicago Press.
McCarthy, P. T. 2014. The road to scale runs through public systems. Stanford Social Innovation Review Spring:12-13. https://ssir.org/articles/entry/the_road_to_scale_runs_through_public_systems (accessed October 18, 2016).
Meyer, D. S. 2004. Protest and political opportunities. Annual Review of Sociology 30:125.
Meyer, D. S., and D. C. Minkoff. 2004. Conceptualizing political opportunity. Social Forces 82(4):1457–1492.
National Scientific Council on the Developing Child. 2004. Young children develop in an environment of relationships. Cambridge, MA: Harvard University Center on the Developing Child.
Norris, T., and M. Pittman. 2000. The healthy communities movement and the coalition for healthier cities and communities. Public Health Reports 115(2/3):118–124.
NRC (National Research Council). 2014. Civic engagement and social cohesion: Measuring dimensions of social capital to inform policy. Washington, DC: The National Academies Press.
Ockene, J. K., E. A. Edgerton, S. M. Teutsch, L. N. Marion, T. Miller, J. L. Genevro, C. J. Loveland-Cherry, J. E. Fielding, and P. A. Briss. 2007. Integrating evidence-based clinical and community strategies to improve health. American Journal of Preventive Medicine 32:244–252.
Polletta, F. 2008. Culture and movements. Annals of the American Academy of Political and Social Science 619(1):78–96.
Porter, M. E., and M. R. Kramer. 2011. Creating shared value. Harvard Business Review 89(1-2 January-February 2011):62–77.
Prevention Institute. 2014. Making connections for mental health and wellbeing among men and boys in the U.S. Oakland, CA: Prevention Institute.
Prybil, L., F. D. Scutchfield, R. Killian, A. Kelly, G. Mays, A. Carman, S. Levey, A. McGeorge, and D. W. Fardo. 2014. Improving community health through hospital-public health collaboration: Insights and lessons learned from successful partnerships. In Health management and policy faculty book gallery: Book 2. Lexington, KY: Commonwealth Center for Governance Studies, Inc.
Putnam, R. D. 2000. Bowling alone: The collapse and revival of American community. New York: Simon and Schuster.
RWJF (Robert Wood Johnson Foundation). 2015. From vision to action: A framework and measures to mobilize a culture of health. Princeton, NJ: Robert Wood Johnson Foundation.
Sampson, R. J., S. W. Raudenbush, and F. Earls. 1997. Neighborhoods and violent crime: A multilevel study of collective efficacy. Science 277(5328):918–924.
Santoro, W. A. 2008. The civil rights movement and the right to vote: Black protest, segregationist violence and the audience. Social Forces 86(4):1391–1414.
Schorr, L. B. 2016. Reconsidering evidence: What it means and how we use it. Stanford Social Innovation Review. https://ssir.org/articles/entry/reconsidering_evidence_what_it_means_and_how_we_use_it (accessed October 18, 2016).
Schrantz, D. 2016. PowerPoint presentation to the Committee on Community-Based Solutions to Promote Health Equity in the United States in Washington, DC, April 27, 2016. http://www.nationalacademies.org/hmd/~/media/Files/Activity%20Files/PublicHealth/COH_Community%20Based%20Solutions/April%20Meeting/Schrantz%20D.pdf (accessed October 18, 2016).
Shapiro, V. B., J. D. Hawkins, and S. Oesterle. 2015. Building local infrastructure for community adoption of science-based prevention: The role of coalition functioning. Prevention Science 16(8):1136–1146.
Shortell, S. M., A. P. Zukoski, J. A. Alexander, G. J. Bazzoli, D. A. Conrad, R. Hasnain-Wynia, S. Sofaer, B. Y. Chan, E. Casey, and F. S. Margolin. 2002. Evaluating partnerships for community health improvement: Tracking the footprints. Journal of Health Policy and Law 27(1).
Skocpol, T., M. Ganz, and Z. Munson. 2000. A nation of organizers: The institutional origins of civic voluntarism in the United States. The American Political Science Review 94(3):527–546.
Smart Grow America. 2014. State-level complete streets policies. https://www.smartgrowthamerica.org/app/legacy/documents/cs/policy/cs-state-policies.pdf (accessed October 18, 2016).
Thunder Valley CDC (Community Development Corporation). 2016. Theory of Change. http://thundervalley.org/change/theory-change (accessed October 23, 2016).
Trickett, E. J., S. Beehler, C. Deutsch, L. W. Green, P. Hawe, K. McLeroy, R. L. Miller, B. D. Rapkin, J. J. Schensul, A. J. Schulz, and J. E. Trimble. 2011. Advancing the science of community-level interventions. American Journal of Public Health 101(8):1410–1419.
Verbitsky-Savitz, N., M. B. Hargreaves, S. Penoyer, N. Morales, B. Coffee-Borden, and E. Whitesell. 2016. Preventing and mitigating the effects of aces by building community capacity and resilience: Appi cross-site evaluation findings. Washington, DC: Mathematica Policy Research.
Williams, M. S. 1998. Voice, trust, and memory: Marginalized groups and the failings of liberal representation. Princeton, NJ: Princeton University Press.
Woulfe, J., T. R. Oliver, S. J. Zahner, and K. Q. Siemering. 2010. Multisector partnerships in population health improvement. Preventing Chronic Disease 7(6):A119. https://www.cdc.gov/pcd/issues/2010/nov/10_0104.htm (accessed October 23, 2016).


























