
6
Policies to Support Community Solutions
Communities operate in the context of federal and state policies that can affect local government decisions relevant to health through laws and regulations, through the allocation of resources, and by shaping political will on issues and approaches. Among the more widely recognized policies are those that fund or regulate health care delivery services. But policies in a variety of areas, ranging from education to land use and housing, the environment, and criminal justice, can be relevant to health disparities. Policies can vary significantly across geographic areas and over time in establishing priorities, providing funding, or encouraging collaboration. They can provide important opportunities or constitute barriers to promoting health equity. The policy context shapes the levers that are available to communities to address change.
It seems reasonable to assume that the better informed communities are about the implications of federal and state policy and policy changes, the greater their ability will be to respond effectively to address health disparities and help achieve change in the determinants of health. And, conversely, the more the needs of communities are considered in decision making at the federal and state levels, the more effective those policies will be. In other words, policy makers have the opportunity to lay the groundwork for community success. This policy context (i.e., socioeconomic and political drivers) is highlighted in the report’s conceptual model in Figure 6-1.
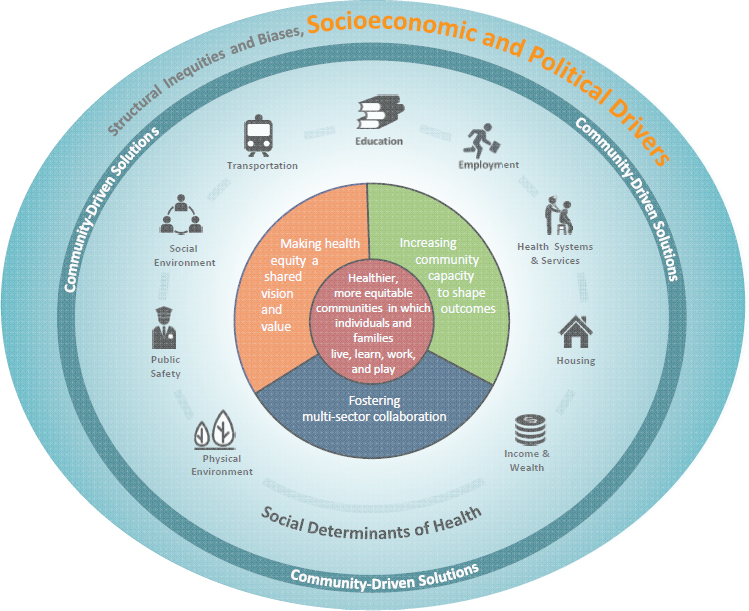
NOTE: The policy context is highlighted here to convey the focus of this chapter.
Frequently, community health initiatives, including collaborative activities, sometimes limit their vision and advocacy to policy changes related to health care and perhaps social services (Whittington et al., 2015). Communities—and the federal and state agencies that support them in their efforts to address health disparities—have multiple examples to follow in expanding their focus beyond health care and social services and examining opportunities in economic development, land use and housing, education, and criminal justice, areas which have not traditionally been the focus of health improvement efforts. Nevertheless, potential partners in those sectors are already working to improve outcomes, save money, and achieve other objectives that influence health. Examples include community development, justice reinvestment, and clean energy financing (Andrews et al., 2012; CSG, 2016; International Energy Agency, 2015). There are also policy changes that could be made at the federal and state level across non-health domains that would remove barriers
or create opportunities for communities to promote health equity. The committee asserts that to attain health equity in the long term, policies that create structural barriers need to be addressed—addressing the root cause of the problem, not only treating the inequities that result. In this chapter, specific policies in six areas are discussed for their high relevance to community-based solutions that advance health equity: taxation and income inequality, housing and urban planning, education, civil rights, health, and criminal justice policy.
TAXATION AND INCOME INEQUALITY
As discussed in Chapter 3, income has been identified as one of many drivers of population health and health inequity over the life course, along with factors that are closely related to income such as education, occupation, and place of residence (Adler and Rehkopf, 2008; Chow et al., 2006; Cutler and Lleras-Muney, 2006).
The distribution of income is shaped by general economic conditions and by federal and state policies: most notably, taxes and government transfer programs such as Social Security, Supplemental Security Income (SSI), unemployment insurance, veterans’ benefits, food stamps, the Supplemental Nutrition Assistance Program (SNAP), and the free and reduced-price school meal program. Thus, an individual’s or a household’s income results from a combination of reinforcing factors, including market conditions, government transfers, and taxes. A longitudinal analysis by the Congressional Budget Office (CBO) (2016) reviews changes in income inequality over time and notes that there has been increasing inequality along several measures: market income, “before-tax” income, and “after-tax” income. Market income (e.g., wages, salaries, business income, investment income, retirement pensions, and other money income), which excludes government transfers, rose over a 35-year period from 1979 to 2013 but grew 188 percent for households in the top 1 percent and only 18 percent for the bottom four income quintiles.
The CBO also examined before-tax income, which adds government transfers to market income. Government transfers reduce income inequality. Because government transfers largely benefit those at lower income levels, taking into account government transfers attenuates the income gap somewhat. So-called before-tax incomes rose between 32 and 39 percent in the lowest four quintiles, compared to 18 percent when government transfers are excluded. Because the highest quintile does not receive a significant amount of government transfers, its before-tax income grew at a similar rate as market income.
Finally, the CBO measured after-tax income, which takes into account both government transfers and taxes. Most federal revenues come from
individual income taxes ($1.6 trillion) and payroll taxes ($1.1 trillion), with corporate income taxes ($300 billion) and other taxes playing smaller roles ($309 billion) (CBO, 2016). Over 35 years, households in the top 1 percent of the income distribution experienced an average 3 percent annual growth in inflation-adjusted, after-tax income compared with 1 percent for households in the bottom quintile. Thus, over 35 years, incomes at the top increased by 192 percent compared with an increase of 46 percent at the bottom. Half of tax offsets, including exclusions, deductions, preferential rates, and credits, go to those in the highest fifth of incomes (CBO, 2016). In 2013 average federal tax rates were below the 35-year average for most households, despite recent changes in tax law. Thus, across all three measures examined by the CBO, income inequality has grown substantially. These analyses also demonstrate the important role of government transfers and tax policy, as well as general economic conditions, in shaping income inequality.
The steady upward trend of income inequality in the United States has been documented and examined in a range of scholarship, including political science. Jacobs and Soss (2010) offer a typology of frameworks for analyzing how “economic inequalities result from and influence politics in the United States,” one of which explores power relations, including how the state can create possibilities for agency (p. 345). A recent study underscores the stark relationship between income inequality and health and how this manifests locally. In the largest study of its kind, Chetty et al. (2016) examined more than 1 billion income tax and Social security records to report the association between income level and life expectancy from 1999 through 2014. Consistent with previous findings, they found that higher income is related to higher life expectancy and that lower income is related to lower life expectancy (NASEM, 2015; NRC and IOM, 2013; Waldron, 2007). The relationship found by Chetty et al. (2016) is dramatic: the gap in life expectancy for the richest and poorest 1 percent of the population was 14.6 years for men and 10.1 years for women. The relationship holds through the highest income percentiles, although the magnitude of the effect diminishes higher on the income distribution. Other studies have found that the income gradient also exists across racial and ethnic groups and that the relationship between income and health is stronger than between race and health (Woolf et al., 2015).
Chetty et al. (2016) examined the income-longevity relationship across time and across local areas. In certain local areas, the effect of being at the bottom of the income gradient is more pronounced than in others, with four- to fivefold differences. Trends in life expectancy also varied geographically, with some areas experiencing improvements and others declines.
There are a number of mechanisms through which income differences might drive local health patterns. Health behaviors, such as obesity and
smoking, have been identified (Chetty et al., 2016; Mathur et al., 2013), as has pollution (Mohai et al., 2009) and access to healthy foods (Kyureghian et al., 2013). Low-income families that are food-insecure have also been found to choose high-calorie, nutrient-poor foods, contributing to worse health outcomes (Burke et al., 2016).
Federal means-tested programs are based on income and, whether through cash or in-kind benefits, can have a significant impact on health outcomes and thereby redress health inequity. The largest of these programs is Medicaid, which is discussed later in the chapter. The second largest program by expenditures is the earned income tax credit (EITC), which provides a tax credit to low-income families and individuals, followed by SSI, which provides benefits to low-income individuals with disabilities. Other programs include subsidized housing of various forms; SNAP, which supports food expenditures for low-income families and individuals; and Temporary Assistance for Needy Families, a cash benefit program that has contracted in size and is currently less than one-quarter the size of the EITC in aggregate (GAO, 2015). Finally, there are school food programs, Early Education, and the Special Supplemental Nutrition Program for Women, Infants, and Children, the latter of which provides vouchers for nutritional foods, counseling, health screening, and referrals for low-income infants, young children, and pregnant and postpartum women.
The programs vary significantly in the size of their benefits and in the number of people they reach. Over time, their growth rates have changed with economic conditions and changes in program rules. The recent Great Recession led to increases in most of these programs’ spending between 2007 and 2011 and underscores the important role that these programs play in mitigating poverty (Bitler and Hoynes, 2013; Bitler et al., 2016). Program rules further shape the distribution of benefits among the low-income population: a study by Ben-Shalom et al. found that from 1984 to 2004, benefits to single mother households and non-employed1 families declined by 19 and 21 percent, respectively, while benefits going to employed families, the elderly, and the disabled grew by 61 percent, 12 percent, and 15 percent, respectively (Ben-Shalom et al., 2011).
In many states a federal program is augmented through benefits or eligibility expansions. States have expanded the EITC, SSI, and SNAP beyond federal provisions (Bartilow, 2016), creating less inequity within the state but greater inequity across states. Thus, local community conditions can vary significantly over time and across regions.
The evidence base concerning the health effects of these means-tested programs varies. SNAP plays a crucial role in reducing poverty and
___________________
1 Defined as families without a member over age 15 who worked in all 4 months prior to the interview.
food insecurity, particularly for children, and has also helped to reduce rates of obesity among its beneficiaries (Executive Office of the President, 2015). The U.S. Department of Agriculture (USDA), in collaboration with other organizations, released an obesity prevention tool kit, SNAP-Ed,2 for states to promote this goal. Programs and policies such as SNAP have the potential to reduce childhood and adulthood obesity and provide substantial economic returns on investment, and their effects could potentially be amplified by local sugar-sweetened beverage or “soda tax” policies. Soda taxes have shown promise in Philadelphia (CHOICES, 2016) and could significantly benefit other areas, including the Bay Area and Boulder (Goldberg, 2016), as shown by research conducted by the Childhood Obesity Intervention Cost Effectiveness Study3 initiative at the Harvard T.H. Chan School of Public Health.
In 2016 the federal EITC benefit, the largest means-tested federal program after Medicaid, provided cash transfers to 26 million people who work, primarily those with children (IRS, 2016). Studies have found that EITC benefits lead to improvements in a variety of health and mental health conditions for adults and children, as well as to reductions in smoking and other behaviors detrimental to health, improved parenting, and better school outcomes (Dahl and Lochner, 2005; Evans and Garthwaite, 2014; Hamad and Rehkopf, 2015, 2016; Strully et al., 2010). Twelve states play an important role in improving income and health equity by augmenting the EITC through state tax law. New York, for example, extends benefits to noncustodial parents, which has been found to increase employment and child support payments (Nichols and Rothstein, 2016). Because the EITC targets low- and middle-income workers, its expansion reduces income inequality and improves health equity.
In addition to the tax code and government transfers, federal and state laws shape incomes through minimum wage provisions. The federal government increased the minimum wage to $7.25 in 2009. In 21 states, the minimum wage is set higher than the federal level (Tax Policy Center, 2014). Given that minimum wages vary significantly due to state and local policies, such policies are another driver of health inequity at the community level. Declines in real minimum wages have been found to contribute to income inequality, particularly for women, between 1979 and 2012 (Autor et al., 2016). Studies of minimum wage and health have found that declining real minimum wage rates have contributed to increasing obesity rates in the United States (Meltzer and Chen, 2011) and that minimum wage policies are associated with lower maternal smoking and
___________________
2 Tool kit is available at https://snaped.fns.usda.gov/snap/SNAPEdStrategiesAndInterventionsToolkitForStates.pdf (accessed December 19, 2016).
3 For more information, see http://choicesproject.org (accessed December 19, 2016).
better birth outcomes (Wehby et al., 2016). A potential downside of minimum wage policies is their potential to decrease employment; research indicates that minimum wages can cause at least some unemployment, particularly for very low-skilled workers, including teenagers (Neumark et al., 2014).
HOUSING AND URBAN PLANNING POLICIES
Housing affordability has become a significant policy concern. From 2000 to 2012 the average rent burden for all renters grew from 26 percent of income to 29 percent of income, but for low-income families the burden has grown considerably more: renters in the bottom fifth of the income distribution spent about 63 percent of their income on rent in 2012, compared with 55 percent in 2000 (Collinson et al., 2015). In 2012, 49 percent of all renters and 89 percent of low-income renters spent more than 30 percent of their income on rent, an approximate 25 percentage point increase since 1960. This increase arose partly from improvements in housing and partly from stagnant incomes.
The federal government supports housing affordability through in-kind, means-tested programs and through the tax code. Roughly $42 billion is put toward numerous forms of means-tested housing assistance, such as vouchers to low-income families, subsidized rent in public housing projects, privately owned subsidized housing, and support for the construction of low-income housing. Two-thirds of federal subsidy recipients are either low-income elderly or people with disabilities. Significantly more support, roughly $228 billion, is given through tax deductions, such as mortgage interest deductions (OMB, 2016), the vast majority of which go to nonpoor households.
Among the earliest forms of housing assistance, public housing has faced numerous challenges. Historically, public housing developments were placed in disproportionately poor areas, distinct from their surrounding neighborhoods, which led to greater concentrations of poverty and racial segregation (Schill and Wachter, 1995). Today, funding for public housing is on the decline, and there are fewer than 1.1 million public housing units, down from 1.4 million units in the early 1990s, after an active effort to scale back public housing. The U.S. Department of Housing and Urban Development (HUD) HOPE VI program promoted demolition of public housing and sought to replace distressed public housing developments with lower-density, mixed-income developments (Schwartz, 2014); however, just over half of the demolished units have been replaced. Public housing units continue to be located in poorer neighborhoods than in other HUD programs (HUD, 2016b).
A number of other HUD-subsidized programs have supported privately owned, low-income housing by lowering construction costs or by providing rental subsidies to tenants. The Housing Choice Voucher (formerly Section 8) program awards vouchers to low-income families so that they can rent apartments on the private market. The program supports 2.4 million units for low-income households (HUD, 2016b). The remainder of the 5.3 million HUD-subsidized units is supported by project-based funding and other smaller programs. A significant policy issue is the low participation in housing assistance programs; only one in four eligible households currently receives a housing subsidy, and many areas report long waiting lists that combined are estimated to exceed 6.5 million households (Collinson et al., 2015). Finally, the Low Income Housing Tax Credit (LIHTC), begun in 1986, is now the largest federal housing program for the poor and has contributed to 2.78 million housing units becoming available from 1987 to 2014 (HUD, 2016a). The LIHTC program is administered by state entities that determine funding priorities within a federal framework.
A number of housing policies contribute to the economic status and welfare of low-income families. These include the overall size of federal housing assistance, which currently supports only one-quarter of eligible poor families; housing allocation processes; eligibility rules; and requirements on the quality of housing itself. At the same time, research findings on the impacts of housing policy on health equity are mixed. A recent review (Collinson et al., 2015) finds some evidence that families and children enjoy better health and overall well-being when living in more advantaged neighborhoods; however, housing subsidies do not necessarily move families to better neighborhoods. In particular, the public housing program appears to concentrate families in more economically and racially isolated neighborhoods than they would otherwise live in. In contrast, families receiving tenant-based subsidies like housing vouchers do not typically use them to move to neighborhoods that are substantially different from where they were previously living, although some research indicates that families receiving vouchers who have school-age children will move if housing is available near higher-performing schools (Ellen et al., 2016; Sanbonmatsu et al., 2011). Other research finds that although public housing is associated with reduced grade retention (i.e., repeating a grade) for African American students (but not for other students) (Currie and Yelowitz, 2000), housing vouchers were not found to improve educational attainment, crime, or health care use measured through Medicaid claims (Jacob et al., 2015). The HUD Moving to Opportunity experiment related to public housing found that children, mostly girls, benefited from moving out of public housing projects into a housing voucher program (Kessler et al., 2014; Sanbonmatsu et al., 2011). Relatively little research
exists examining the effect of the LIHTC on recipients’ living situations or health status.
Urban Planning Policies
Housing affordability and federal HUD policies are part of a larger dialogue concerning housing that also includes land use, residential and commercial development, natural resource use, transportation, and, even more broadly, changing neighborhoods and concerns over potential residential disruption. Urban planning policies shape the physical environment along with many other social determinants of health. Within federal and state initiatives, community actions can support local policy and implementation so that they benefit vulnerable populations.
Urban planning, while traditionally relying on geographic analytic tools, has the potential to influence health in a variety of ways, including access to health care services; disease outbreaks; physical activity among local residents; injuries related to motor vehicle, bicycle, and pedestrian traffic; air quality; crime; and employment (Kochtitzky et al., 2006). Increasingly, those involved in public health are being encouraged to include an urban planning lens, while those in urban planning are being encouraged to include a public health lens at the national level and in some states (Ricklin and Kushner, 2014).
One dimension of urban planning that can greatly influence health equity relates to so-called greening policies and programs. Two studies conducted in Philadelphia, including a randomized trial, found that programs to “green” and maintain vacant urban land—for example, through cleaning and plantings—led to lower rates of gun crime and vandalism; in addition, residents reported feeling safer, feeling less stress, and getting more exercise (Branas et al., 2011; Garvin et al., 2013; Huynh and Maroko, 2014). Because vacant lots are disproportionately situated in low-income areas, greening programs have the potential to promote health equity.
One of many urban planning challenges is around the larger issues of economic, job, and workforce development (Freeman, 2005; Newman and Wyly, 2006). Local economic development can revitalize blighted neighborhoods and create more jobs, but it can also lead to the displacement of low-income residents. In local areas where the housing supply is tight or where investment is improving the quality and amenities of the local housing stock, development can affect housing affordability, particularly for low-income residents, leading to displacement (Finch et al., 2016; PolicyLink, 2016b).
Displacement can exacerbate health inequities by limiting access to affordable housing, healthy food options, transportation, quality schools, bicycle and walking paths, exercise facilities, and social networks and
also by increasing financial hardship (CDC, 2009). The disruption of social ties and networks can affect mental and physical well-being, especially for households that have lived in their original neighborhood for a long period of time (Phillips et al., 2014). A recent study in Philadelphia found that residents in a gentrified area of Philadelphia who stayed in that area experienced improvements in their financial well-being, as measured by credit scores. However, vulnerable residents who moved from that area tended to move to lower-income neighborhoods and experienced a worsening in financial well-being (Ding and Hwang, 2016; Ding et al., 2015). Despite concerns around the negative impacts of potential displacement, research attempting to quantify the scale and nature of residential displacement is limited and existing studies have relatively limited time horizons (Zuk et al., 2015).
The changing landscape of a number of cities in the United States suggests increasing income and racial segregation. Wyly and Hammel mapped the effects of housing market and policy changes in the 1990s in 23 large U.S. cities (Wyly and Hammel, 2004). Along with a resurgence in capital investment in the urban core, the authors found increased racial and class segregation in addition to intensified discrimination and exclusion in gentrified neighborhoods (Wyly and Hammel, 2004). This has implications for health inequity, as evidenced by the body of literature that suggests the negative health impacts of segregation and discrimination on people of color. At the same time, a number of equitable development and housing policy tools have been developed that can assist communities to balance opportunities across local groups so that more can benefit from development efforts (PolicyLink, 2016a; Wilson et al., 2008). Local communities and governments across the country have started to integrate processes and policies to advance health equity within the urban planning and land use context. For example, Multnomah County, Oregon, applies an “equity and empowerment lens” to local policy (Multnomah County, 2014a, b, n.d.), and Seattle–King County implemented an “equity in all policies” approach to all decision making and annually reports on what it terms “the determinants of equity” in the county (Beatty and Foster, 2015).
In a 2011 Institute of Medicine (IOM) report, the authoring committee recommended that “states and the federal government develop and employ a ‘health in all policies’ (HIAP) approach to consider the health effects—both positive and negative—of major legislation, regulations, and other policies that could potentially have a meaningful impact on the public’s health” (IOM, 2011). The committee further recommended that “state and federal governments evaluate the health effects and costs of major legislation, regulations, and policies that could have a meaningful impact on health. This evaluation should occur before and after enactment.” The
recommendation below is made with an acknowledgment of the ongoing cross-sectoral work in many jurisdictions around the country and of the previous IOM recommendations.
Recommendation 6-1: All government agencies that support or conduct planning related to land use, housing, transportation, and other areas that affect populations at high risk of health inequity should:
- Add specific requirements to outreach processes to ensure robust and authentic community participation in policy development.
- Collaborate with public health agencies and others to ensure a broad consideration of unintended consequences for health and well-being, including whether the benefits and burdens will be equitably distributed.4
- Highlight the co-benefits of—or shared “wins” that could be achieved by—considering health equity in the development of comprehensive plans5 (e.g., improving public transit in transit-poor areas supports physical activity, promotes health equity, and creates more sustainable communities).
- Prioritize affordable housing, implement strategies to mitigate and avoid displacement (and its serious health effects), and document outcomes.
Strategies to expand affordable housing could include regulating the private housing market; establishing nonprofit-owned affordable housing; creating affordable home ownership opportunities; offering resident-controlled, limited-equity ownership; leveraging market rate development; and preserving publicly assisted affordable housing. Other policy tools to promote equitable development include the use of land trusts, legal covenants that protect and increase rent stabilization, inclusionary zoning, rent control, the use of Section 8 housing provisions, housing code enforcements, just-cause eviction controls, requirements for sufficient low-income housing to avoid displacement, and policies and tools that assist low-income residents in homeownership (ChangeLab Solutions, 2015). See Box 6-1 for an example of a community-driven neighborhood plan designed to make some of these changes.
___________________
4 See Recommendation 7 in For the Public’s Health: Revitalizing Law and Policy to Meet New Challenges (IOM, 2011).
5 See, for example, ChangeLab Solutions’ “Model Comprehensive Plan Language on Complete Streets” (ChangeLab Solutions, 2016).
EDUCATION POLICIES
The powerful role that education plays in producing—or reducing—inequitable health outcomes was discussed in Chapter 3. Educational attainment predicts life expectancy and such health status indicators as obesity and morbidity from acute and chronic diseases (see, for example, Woolf et al., 2007). The educational level of adults, particularly maternal educational achievement, is linked to their children’s health and wellbeing. In all regions of the United States (Montez and Berkman, 2014), the gradient in health outcomes by educational attainment has steepened over the last four decades (Goldman and Smith, 2011; Olshansky et al., 2012), producing a larger gap in health status between Americans with high and low education levels. Thus, policies and practices to increase academic achievement and reduce education disparities make a critical contribution to reducing health inequities.
An important insight emerges from looking broadly across the array of education-related policies and practices. Desired improvements in education and health outcomes are unlikely to be achieved by one-dimensional interventions. Both the community examples that the committee has examined and other information the committee has gathered suggest that achieving greater equity in health outcomes will require collaboration and collective action across sectors and new forms of community engagement and partnership. At the community level, there may be unique opportunities to work in a coordinated manner. Part of the committee’s charge was assessing and prioritizing these possibilities for more effective community-based efforts to improve health outcomes. In the context of education, there are a number of possibilities, including, notably, the opportunity to improve education outcomes themselves.
The current policy landscape in health and especially in education warrants serious consideration of policy as a key factor in shaping local action. New federal legislation, the Every Student Succeeds Act (ESSA),6 makes an important contribution to any effort to promote community-based strategies for reducing health inequities by recognizing the need for schools to improve educational achievement and to embrace and support “whole child” strategies. (See the Chapter 7 section on education for more details on ESSA and how communities can leverage it.) The act makes this contribution by specifically acknowledging the importance of promoting physical and mental health and wellness as essential to reducing inequities in academic achievement. Within this broad vision are numerous components of the law that represent opportunities to strengthen the linkages between education and health, thereby creating the local conditions to reduce health inequities through education.
___________________
6 S.1177 Every Student Succeeds Act. Public Law 114-95 (December 10, 2015), 114th Cong.
First, ESSA calls for the identification of evidence-based interventions. This is a significant development in education, a field that has been slow to make broad use of research as a basis for improving practice (West, 2016). The law sets forward specific tiers of evidence, ranging from randomized trials to correlational studies. There are current opportunities to expand significantly the evidence available to schools by making connections to the health community and scholars with interest in promoting educational equity.
School improvement plans represent another key feature of the new federal education legislation. Under Title I of ESSA, school districts, in partnership with stakeholders, must develop and implement plans that include evidence-based interventions. Their plans under Title IV, where Student Support and Academic Enrichment Grants (SSAEG) are awarded—a key local source of revenue for making more effective connections between education and health—must also be evidence-based. Furthermore, both Title I school improvement plans and Title IV plans must be informed by comprehensive needs assessments. Creating examples of needs assessments that effectively incorporate health and wellness will be of real value over the next 3 to 5 years as school districts work with community stakeholders in crafting these plans.
Finally, one of the most important components of ESSA pertains to its state and local accountability provisions. Historically these provisions have been preoccupied with testing and assessment in the hope that such data would ensure that more children were in fact doing well in school. States and localities are being given great latitude (without guidance) about how they should satisfy the ESSA accountability provisions going forward. The new education law provides an opportunity for communities to reframe how they think more broadly about student opportunity and student success in ways that embrace health and wellness. It is an opportunity, in this regard, to use additional types of data and use data in different ways. The law also reinforces the idea of thinking more broadly about who has a stake in student well-being. Because ESSA is clear that educators must work in partnership with their communities on behalf of children and youth, this is a chance for communities to seize these opportunities in ways that help them foster a genuine culture of health, which will improve education outcomes.
The Individuals with Disabilities Education Act (IDEA), first passed in 1975, is another federal law that promotes greater equity through the protection of rights for students with disabilities. A U.S. Department of Education (ED) analysis found that students of color are being identified as having a disability at increasingly more frequent rates and receive harsher discipline than their white peers (ED, 2016b). In early 2016, ED and the My Brother’s Keeper Task Force established in 2014 by President Barack Obama proposed the Equity in IDEA rule to address these
inequities by requiring standard approaches for identifying, disciplining, and supporting students with disabilities, particularly students of color with disabilities (ED, 2016c). Other efforts have been established to reduce inequity through early childhood intervention, including the Birth to Three Developmental Center7 in Washington State that serves infants and toddlers who qualify for services under IDEA through various programs to support these children and their families.
To aid in its enforcement and oversight of federal civil rights laws, ED collects data from school districts about student characteristics, academic offerings, and disciplinary actions. It compiles these data into a publicly available, national data set called the Civil Rights Data Collection so that researchers, states, and school districts can conduct their own analyses. Importantly, in 2000–2001, and again in 2011–2012 and 2012–2013, ED included all K–12 schools in its data collection rather than taking a sample. Maintaining the comprehensive, national data collection through education opens an important opportunity for communities to improve education and address disparities. In addition to data within the education sector, schools can benefit from partnering with others in the community to identify needs and plan and implement solutions. Examples have been highlighted in the work of the National Collaborative on Education and Health (Healthy Schools Campaign, 2016). Also, a joint initiative between ED and the U.S. Department of Health and Human Services (HHS) identifies “build[ing] local partnerships and participat[ing] in hospital community health needs assessments” as one of five high-impact opportunities. The Healthy Students, Promising Futures tool kit states
The community health needs assessments (CHNAs) that nonprofit hospitals are required to undertake include consultations with community members and public health experts, which can help launch productive partnerships between hospitals and schools. Schools and school districts can also partner with many other kinds of community-based organizations and institutions to enrich the health services available to students. (ED, 2016a)
Conducting community health needs assessments has long been an activity and role of local and state public health agencies. Public health accreditation, which a growing number of health departments undergo, requires that health departments conduct or participate in a collaborative process of comprehensive health needs assessment in their communities (PHAB, 2011).
An additional way to think about promoting community-based strategies for reducing education and health disparities is to consider the
___________________
7 For more information, see http://www.birthtothree.org/programs (accessed September 21, 2016).
existing infrastructure of policies and programs within the education sector with an eye toward how this infrastructure might be strengthened, modified, or expanded in the interest of improving health outcomes. Schools can take actions to improve the immediate health and well-being of their students. For example, there are a number of policies and practices that exist at the community level pertaining to air quality and environmental standards in educational settings. Policies exist widely that are related to physical activity and wellness. In what education administrators might think of as student services, policies and procedures exist concerning screening for health conditions as well as for counseling and mental health services. In the context of intergovernmental coordination and cooperation, many local education agencies (e.g., school districts) have established advisory councils, established school-based clinics, and employed school health coordinators. In the context of curriculum and instruction, there is a broad array of programs that connect education and health, to include asthma awareness education; emotional, social, and mental health education; nutrition education; and, of course, physical education.
Recommendation 6-2: State departments of education should provide guidance to schools on how to conduct assessments of student health needs and of the school health and wellness environment. This guidance should outline a process by which schools can identify model needs assessments, including those with a focus on student health and wellness.
Recommendation 6-3: To support schools in collecting data on student and community health, tax-exempt hospitals and health systems and state and local public health agencies should:
- Make schools aware of existing health needs assessments to help them leverage current data collection and analyses.8
- Assist schools and school districts in identifying and accessing data on key health indicators that should inform school needs assessments and any related school improvement plans.
Furthermore, ED could consider leveraging the needs assessment mandate of ESSA and require that schools and school systems collect such information on student and community health. One important factor to take into consideration would be the disproportionate burden that such
___________________
8 See, for example, the Healthy Students, Promising Futures tool kit from ED and HHS (ED, 2016a).
a requirement may place on schools already facing economic and infrastructure challenges.
CIVIL RIGHTS LAW AND POLICY
Civil rights, health, and environmental justice laws and policies provide a framework to promote equal access to publicly funded resources and prohibit discrimination based on race, color, national origin, income, gender, disability, and other factors. This crosscutting approach can be applied across different areas such as health, park access, education, housing, transportation, and others. Using the approach to support community-driven solutions draws on lessons from the civil rights movement and others such as the women’s movement. The civil rights movement includes community stakeholders; social science experts; attorneys working in and out of court; grassroots organizing; legislation by Congress; executive action by the president; implementation by administrative agencies; popular support through the right to vote; and philanthropic support (Ackerman, 2014; Rodriguez et al., 2014).
Resting upon a number of federal and state laws, including the Civil Rights Act of 1964, the Fair Housing Act of 1968, the Americans with Disabilities Act of 1990, the Patient Protection and Affordable Care Act (ACA) of 2010, related regulations, and executive orders, a civil rights approach can lead to changes in structural inequities, policies, and practices that perpetuate racial, ethnic, and other disparities. In their implementation, these laws and associated regulations require that agencies collect data, measure compliance, assess complaints, and allow for midcourse corrections. Data also need to be available to communities for holding officials accountable and advocating for change. A civil rights approach to alleviating health disparities is not synonymous with litigation. Voluntary compliance with and enforcement of equal justice laws and policies can be preferable to court action as a means to achieve equal justice goals, including health equity. A comprehensive civil rights approach to ensuring health equity relies on planning, data collection and analysis, media, negotiation, policy advocacy, and coalition building—all as part of a larger problem-solving strategy (Rodriguez et al., 2014). Civil rights attorneys may work with community allies, clients, social scientists and academics, experts, and broader coalitions to seek racial and ethnic equity and overcome discrimination and structural barriers to a more equitable society.
Through a civil rights lens, health equity involves the fair distribution of both the benefits and the burdens of programs and activities. Equal justice means more than freedom from unhealthy, environmentally degraded communities. Applying civil rights law to health equity includes a positive vision to meet the needs of communities at risk for
health inequity by reducing discriminatory burdens, removing barriers to participation in decision making, and increasing access to health and environmental benefits that help make all communities safe, vibrant, and healthy (USDA, 2012).
Federal Laws and Civil Rights
Numerous federal and state laws and policies support a civil rights approach to health equity. For example, Title VI of the Civil Rights Act of 1964 and corresponding regulations prohibit discrimination based on race, color, or national origin and promote equity in programs and activities by recipients of federal financial assistance.9 The Fair Housing Act of 1968 prohibits discrimination and promotes equal opportunity in housing.10 The ACA includes a provision, Section 1557, against health discrimination in federally funded or supported health programs or activities. Section 1557 and corresponding regulations prohibit discrimination based on race, color, national origin, limited English proficiency, gender, physical and mental ability, and age (HHS, 2016). The Americans with Disabilities Act affords similar protections against discrimination based on ability.11 The National Environmental Policy Act also provides protections that can be used to buttress equal justice laws.12 In addition, the President’s Executive Order 12898 on environmental justice and health requires federal agencies to address the effects of programs, policies, and activities on minority and low-income populations.13 Some states such as California have parallel laws that will become increasingly important to promote health equity,
___________________
9 42 U.S.C. § 2000d et seq.; 28 C.F.R. § 42.101 et seq. (U.S. Department of Justice regulations).
10 42 U.S.C. § 3601 et seq.
11 42 U.S.C. § 12101 et seq.
12 42 U.S.C. § 4321 et seq.
13 See Exec. Order No. 12898, 59 Fed. Reg. 32 (Feb. 16, 1994), Section 1-101, https://www.archives.gov/files/federal-register/executive-orders/pdf/12898.pdf (accessed June 24, 2016); White House Memo re: Executive Order on Federal Actions to Address Environmental Justice in Minority Populations and Low-Income Populations (February 11, 1994), www.epa.gov/sites/production/files/2015-02/documents/clinton_memo_12898.pdf (accessed June 24, 2016); Memorandum of Understanding on Environmental Justice and Executive Order 12898 (2011), www.epa.gov/sites/production/files/2015-02/documents/ejmou-2011-08.pdf (accessed June 24, 2016); and U.S. Department of Justice Guidance Concerning Environmental Justice (December 3, 2014), www.justice.gov/sites/default/files/ej/pages/attachments/2014/12/19/doj_guidance_concerning_ej.pdf (accessed June 24, 2016). See generally U.S. Department of Justice, Civil Rights Division, Title VI Legal Manual at pages 58–65 (January 11, 2001). Available at https://www.justice.gov/sites/default/files/crt/legacy/2011/06/23/vimanual.pdf (accessed June 24, 2016).
civil rights, and environmental justice and health with changes in federal enforcement and the political landscape in the years to come.14
The U.S. Commission on Civil Rights in 2016 issued a report emphasizing the need for the U.S. Environmental Protection Agency (EPA) to comply with and enforce civil rights and environmental justice laws.15 Similarly, civil rights and environmental justice practitioners widely and strongly criticize EPA for being derelict in pursuing enforcement actions. Government enforcement is particularly important to guard against discriminatory impact because there is no private cause of action for individuals and organizations to seek justice through the courts under the discriminatory impact standard, according to the U.S. Supreme Court (“the Sandoval problem”).16 This is widely held to be a major problem in rights enforcement, as it can be more difficult to show intentional discrimination. These concerns are supported by publicly available information regarding EPA’s failure to pursue filed administrative complaints, for example.17 EPA released its EJ 2020 Action Agenda in 2016 as a strategic plan to promote civil rights, environmental justice, and health. Its imple-
___________________
14 For example, California Government Code 11135 et seq. and corresponding regulations promote equal justice and prohibit discrimination by state agencies and state-funded programs and activities for specified classes, parallel to federal civil rights laws such as Title VI. Section 11135 was recently amended to strengthen compliance and enforcement. See, e.g., California Equal Justice Amendments Strengthen Law under 11135, http://www.cityprojectca.org/blog/archives/43834; and John Auyong et al., Opportunities for Environmental Justice in California Agency by Agency (Public Law Research Institute U.C. Hastings College of Law 2003), http://gov.uchastings.edu/public-law/docs/PLRI_Agency-by-Agency_03.pdf (accessed June 24, 2016).
15 U.S. Commission on Civil Rights, Environmental Justice: Examining the Environmental Protection Agency’s Compliance and Enforcement of Title VI and Executive Order 12898 (September 2016). Available at http://www.usccr.gov/pubs/Statutory_Enforcement_Report2016.pdf (accessed June 24, 2016).
16 According to the Court in Alexander v. Sandoval, 532 U.S. 275 (2001), the Title VI statute prohibits only intentional discrimination, and private individuals and organizations can enforce the statute in court. Congress did not intend to create a private cause of action to enforce the discriminatory impact regulations in court.
17 See, for example, Rosemere Neighborhood Association v. U.S. Environmental Protection Agency, 581 F.3d 1169 (9th Cir. 2009) (EPA failed to process a single complaint from 2006 or 2007 in accordance with its regulatory deadlines); Lawyer: EPA Has Failed Civil Rights Law: Attorney Marianne Engelman Lado argues that the Environmental Protection Agency should enforce civil rights law in the low-income communities of color that she says carry the burden of pollution, NBC News (August 2, 2015). Available at http://www.nbcnews.com/video/nbcnews.com/57693524#58380209 (accessed June 24, 2016). Kristen Lombardi, Talia Buford, Ronnie Greene, Environmental Justice, Denied: Environmental racism persists, and the EPA is one reason why (Center for Public Integrity September 4, 2015) (EPA has not made a formal finding of discrimination in 22 years, despite having received hundreds of complaints, some exhaustively documented). Available at https://www.publicintegrity.org/2015/08/03/17668/environmental-racism-persists-and-epa-one-reason-why (accessed June 24, 2016).
mentation remains to be evaluated.18 The recommendations and principles in the U.S. Commission on Civil Rights apply to other federal, state, and local agencies in addition to EPA. These and other examples demonstrate that environmental and civil rights laws can be used together, with the strengths in one body of policy and law shoring up challenges in the other.
A Planning Process
The following planning process is a policy and legal tool from the domain of civil rights and environmental justice—designed for use by federal, state, and local agencies and their grantees—that can be adapted to support community-based solutions to promote health equity. The process includes five major elements and can be used by community-based groups to assess both current policies and practices and those under consideration. This framework by public health, civil rights, and environmental justice experts is based on Title VI, Executive Order 12898, case law, and best practices by federal agencies19 (Environmental Justice Leadership Forum on Climate Change, 2016b; The City Project, 2016b):
- Describe what is planned in terms that are understandable to communities (for example, diversifying and broadening access to and support for healthy active living in parks and recreation areas).
- Analyze the benefits and burdens on all people.
- The analysis can include numerical disparities (in park access, for example), statistical evidence, anecdotal evidence, empirical studies and surveys, demographic data, geographical information system mapping, and financial analysis. Who benefits, and who is left behind? To do this, data needs to be collected and made publicly available for independent
___________________
18 See U.S. EPA, EJ 2020 Action Agenda (2016). Available at https://www.epa.gov/environmentaljustice/ej-2020-action-agenda-epas-environmental-justice-strategy; and Robert García and Marianne Engelman Lado, EPA Environmental Justice Action Agenda: Major Steps Forward, and Opportunities for More (NRPA Open Space Blog Nov. 4 2016),http://www.nrpa.org/blog/epa-environmental-justice-action-agenda-major-steps-forward-andopportunities-for-more (accessed June 24, 2016).
19 See, for example, Rodriguez et al., 2014, at pages 13–20 and authorities cited; Environmental Justice Leadership Forum on Climate Change, 2016b; and U.S. Department of Housing and Urban Development, Affirmatively Furthering Fair Housing, Final Rule, 24 C.F.R. Parts 5, 91, 92, et al., 80 Fed. Reg. 42272 (2015), https://www.gpo.gov/fdsys/pkg/FR-2015-07-16/pdf/2015-17032.pdf (accessed June 24, 2016).
-
-
analyses. Standards need to be defined to measure progress, allow for midcourse corrections, and hold officials accountable.
- The range of values at stake to be analyzed includes, for example, physical, mental, and social health; economic vitality, jobs, and displacement; climate and conservation; culture, history, art, and spiritual values; and equal justice and democratic participation.20
-
- Analyze alternatives to what is being considered.
- Include people of color, low-income people, and other stakeholders in every step in the decision-making process.
- Develop an implementation plan to distribute benefits and burdens fairly and avoid discrimination.
An implementation plan through monitoring, compliance, and enforcement helps promote health equity and avoids unjustified discriminatory impacts regardless of intent, as well as intentional discrimination and implicit bias (DOT, 2012a; The City Project, 2016b).
Planning for health equity needs to take place early enough in the process to meaningfully guide the decision-making process and outcomes. The following sections will expand on this process, with each step premised on the participation of diverse stakeholders.
Planning, Data, Standards, Implementation, and Stakeholders
The application of the civil rights approach depends on outlining explicit priorities in planning, data, standards, implementation, and participation. The need for public participation based on full and fair information needs to be addressed in the process and cannot be assumed (Christensen, 2016; Garcia et al., 2016). The experience with the investment of park bond funds in California illustrates why specific priorities matter. California voters have passed billions of dollars in statewide resource, park, and water bonds for almost 20 years. Yet people of color and low-income people throughout California disproportionately lack access to parks, beaches, and recreation areas. To address these concerns, in 2006 voters passed Proposition 84, a bond measure authorizing $5.4 billion in public investments to improve water, parks, coastal protection, and natural resources. Proposition 84 and Assembly Bill (AB) 31—implement-ing legislation for the proposition—defined “park poor” and “income
___________________
20 On the values at stake, see, for example, NPS, Healthy Parks, Healthy People Community Engagement eGuide at page 15 (2014). Available at www.nps.gov/public_health/hp/hphp/press/HealthyParksHealthyPeople_eGuide.pdf (accessed June 24, 2016).
poor” standards to prioritize the investment of $1.3 billion in local impact funds for park, water, and coastal projects (Garcia et al., 2016).21 Fully 88 percent of the $400 million in funds invested under the AB 31 standards were invested in communities that are disproportionately of color and low-income. In contrast, 69 percent of the remaining $1 billion that were not invested using those standards were disproportionately invested in communities that tend to be park-rich, wealthy, and white. Not taking equity and disparities into account through planning, standards, data, and implementation can result in policy failure. Good intentions and vague commitments to “equity” or “local parks and urban greening” alone can exacerbate rather than alleviate disparities.
Discriminatory Impacts and Data Analysis
An important starting point for promoting health equity is the analysis of disparities that bear more heavily on one group of people than another. This includes, for example, numerical disparities for people of color or women based on statistical studies or anecdotal evidence.22 Two recent cases by the U.S. Supreme Court emphasize the need to address civil rights compliance, enforcement, and data analysis by public agencies.23 Federal entities such as the U.S. Department of Justice address the need for data collection and analysis in their regulations and guidance documents.24
___________________
21 AB 31 is the Statewide Park Development and Community Revitalization Act of 2008, Pub. Res. Code §§ 5640 et seq. Prop 84 is the Safe Drinking Water, Water Quality and Supply, Flood Control, River and Coastal Protection Bond Act of 2006, Pub. Res. Code §§ 75001 et seq.
22 See, for example, Fisher v. University of Texas at Austin, 579—U.S.—, slip opinion at pages 13–15 (2016); Village of Arlington Heights v. Metropolitan Housing Dev. Corp., 429 U.S. 252, 265 (1977); Griggs v. Duke Power Co., 401 U.S. 424 (1971); U.S. Department of Justice, Civil Rights Division, Title VI Legal Manual at pages 42–58 and cases cited (2001), available at https://www.justice.gov/sites/default/files/crt/legacy/2011/06/23/vimanual.pdf (accessed June 24, 2016); and Robert García and Erica Flores Baltodano, Free the Beach! Public Access, Equal Justice, and the California Coast, 2 Stanford Journal of Civil Rights and Civil Liberties 143, 187–190 and authorities cited (2005), available at goo.gl/RVgbJ.
23 See Fisher v. University of Texas at Austin, 579—U.S.—(2016); Texas Department of Housing and Community Affairs v. Inclusive Communities Project, 576 U.S.–(2015); U.S. Department of Housing and Urban Development, Implementation of the Fair Housing Act’s Discriminatory Effects Standard, 24 C.F.R. Part 100, 78 Fed. Reg. 11460 (February 15, 2013). Available at https://portal.hud.gov/hudportal/documents/huddoc?id=discriminatoryeffectrule.pdf (accessed June 15, 2016).
24 The U.S. Department of Justice directs agencies to provide for “collection of data and information from applicants for and recipients of federal assistance sufficient to permit effective enforcement of Title VI.” 28 C.F.R. § 42.406(a). This includes, for example, “(1) The manner in which services are or will be provided by the program in question, and related data necessary for determining whether any persons are or will be denied such services on
The U.S. Supreme Court in Texas Department of Housing and Community Affairs v. Inclusive Communities Project held that the prohibition against unjustified discriminatory impacts plays an important role in moving the nation toward overcoming a legacy of residential segregation and promoting equal opportunity for all. Proof of intentional discrimination is not required. The disparate impact standard allows people to counteract disguised animus, unconscious prejudices, and implicit bias that may escape easy classification as intentional discrimination. “A thoughtless policy can be as unfair as, and functionally equivalent to, intentional discrimination” (Rodriguez et al., 2014). The prohibition against unjustified discriminatory impacts promotes equal opportunity for all in access to health, housing, parks, beaches, transportation, jobs, contracts for diverse business enterprises, and other infrastructure and ecosystem services.25 Overlapping evidence is relevant to prove discriminatory impact26 and intent.27
___________________
the basis of prohibited discrimination; (2) The population eligible to be served by race, color, and national origin; . . . (4) [R]elated information adequate for determining whether the [program] has or will have the effect of unnecessarily denying access to any person on the basis of prohibited discrimination.” 28 C.F.R. at § 42.406(b)(1), (2), (4). Similarly, FTA regulations address racial and ethnic data, demographic mapping, comparing benefits and burdens, public engagement, and planning. Federal Transit Administration, Title VI Requirements and Guidelines for Federal Transit Administration Recipients, Circular FTA C 4702.1B, pages IV -7, V-1 (Oct. 1, 2012); FTA, Environmental Justice Policy Guidance for Federal Transit Administration Recipients, Circular (FTA C 4703.1), pages 6, 8, 11 (August 15, 2012). Accord, Executive Order 12898 on Environmental Justice, Sec. 3-3 (research, data collection, and analysis).
25 See Texas Department of Housing and Community Affairs v. Inclusive Communities Project, 576 U.S.—2015. While the facts in that case involved the Fair Housing Act of 1968, the discriminatory impact standard is analogous under Title VI regulations and Affordable Care Act section 1557. See U.S. Department of Housing and Urban Development, Implementation of the Fair Housing Act’s Discriminatory Effects Standard, 24 C.F.R. Part 100, 78 Federal Register. 11460 (2013). Available at https://portal.hud.gov/hudportal/documents/huddoc?id=discriminatoryeffectrule.pdf (accessed June 15, 2016).
26 There are three prongs to the discriminatory impact inquiry: (1) Whether an action impacts one group more than another—numerical disparities based on race, ethnicity, or national origin shown through statistical studies or anecdotal evidence, for example. (2) If so, the funding recipient bears the burden of proving that an action is justified by business necessity—or by an analogous public policy in the case of a government agency. (3) Even if there is evidence of business necessity, the disparities are prohibited if there are less discriminatory alternatives to achieve similar objectives. See, for example, Inclusive Communities slip opinion at page 10.
27 To evaluate an intentional discrimination claim, circumstantial evidence includes (1) whether an action impacts one group more than another, including numerical disparities shown through statistical studies and anecdotal evidence; (2) a history of discrimination; (3) departures from substantive norms; (4) departures from procedural norms; (5) a pattern of discrimination; and (6) the decision maker knows the harm a decision will cause. See, for example, Village of Arlington Heights v. Metropolitan Housing Dev. Corp., 429 U.S. 252, 264–268 (1977); Adarand Constructors, Inc. v. Peña, 515 U.S. 200 (1995); and U.S. Department of Justice, Civil Rights Division, Title VI Legal Manual at pages 42–58 (2001). Available at https://
The U.S. Supreme Court in Fisher v. University of Texas at Austin in 2016 recognized the value of diversity in ways that support community-based solutions to promote health equity. Valuing diversity promotes cross-racial understanding, ending stereotypes, preparing for an increasingly diverse society and workforce, and cultivating leaders with legitimacy in the eyes of the public. The court emphasized the need to gather, analyze, and publish data based on race, color, and national origin in order to ensure that public benefits and burdens are distributed equally and to promote racial justice, human dignity, and diversity.28
Examples of the Planning Process in Action
Specific actions by several federal and local agencies illustrate how civil rights can be promoted to promote health equity through the planning process described above. The National Park Service (NPS) and the U.S. Army Corps of Engineers (the Corps) have used the systematic data-driven planning framework to analyze green access in the Los Angeles region. NPS and the Corps concluded as follows in the context of health and park access:
- There are disparities in green access based on race, color, or national origin;
- This contributes to health disparities based on those factors; and
- Environmental justice and civil rights laws require agencies to promote equity, compliance, and enforcement and alleviate these disparities.
These plans include the NPS plan to expand the Santa Monica Mountains National Recreation Area (“Rim of the Valley”) (NPS, 2015; The City Project, 2016a), the NPS plan to create the San Gabriel Mountains National Recreation Area (NPS, 2013; The City Project, 2014b), and the Corps’ plan to revitalize the Los Angeles River (The City Project, 2016c; U.S. Army Corps of Engineers, LA District, and Tetra Tech Inc., 2015).29 HUD provides another example of the planning framework in action. HUD
___________________
www.justice.gov/sites/default/files/crt/legacy/2011/06/23/vimanual.pdf (accessed June 24, 2016).
28Fisher v. University of Texas at Austin, 579—U.S.—, slip opinion at pages 11, 14–15 (2016). While the facts of the case involved narrowly tailored race conscious admissions to promote the compelling state interest of diversity in a university, the value of diversity and the need for data are analogous in promoting health equity.
29 The Corps has agreed to conduct a similar analysis of the benefits and burdens of, and alternatives to, the Dakota Access Pipeline, in consultation with the Standing Rock Sioux and with full public input before issuing any permits (Darcy, 2016). This is parallel to the Corps’s analysis for revitalization of the Los Angeles River. The decision was made in large part in response to community organizing by the Sioux and its supporters.
withheld federal subsidies for a proposed warehouse project in response to significant local community action, pending a full study under the civil rights and environmental justice laws to consider a park alternative and the impact on people of color and low-income people. This community initiation and decision by HUD contributed to the creation of the L.A. State Historic Park and the greening of the Los Angeles River (Garcia, 2013; The City Project, 2014a).30
With these laws, equal access to publicly funded resources, such as parks and recreation for healthy active living, can be viewed as core civil rights issues. In Brown v. Board of Education, the U.S. Supreme Court struck down segregation in schools when it held that schools separated on the basis of race are inherently unequal, in violation of the Equal Protection Clause.31 In Watson v. City of Memphis in 1963, the Supreme Court upheld equal access to public parks and recreation on equal justice grounds under Brown.32
The civil rights and equity framework is not limited to work in a single geographic area, such as Southern California, or to a specific substantive topic, such as health and park disparities (NPS, 2014). Echoing work by NPS and the Corps and recognizing the need for systematic data and analyses, EPA has released its online mapping and analysis tool called EJSCREEN. This tool includes nationwide data on health vulnerabilities, exposure to toxic chemicals and pollution, park access, and demographics, including race, color, national origin, income, and other variables and is described in more detail in Chapter 8 (EPA, 2016; The City Project, 2016d). WE ACT, a community example featured in Chapter 5, organized a coalition with 41 partners nationwide to address climate justice and health using the framework under Title VI of the 1964 Civil Rights Act (Environmental Justice Leadership Forum on Climate Change, 2016a,b).33
___________________
30 Community advocates settled a related lawsuit under state law. The state then bought the land and created the park.
31Brown v. Board of Education, 347 U.S. 483 (1954). Discrimination is not just a black and white issue. Also in 1954, the Supreme Court held the Equal Protection Clause protects against discrimination based on race, color, national origin, ancestry, or descent in Hernandez v. Texas, 347 U.S. 475 (1954).
32Watson v. City of Memphis, 373 U.S. 526 (1963).
33 A recent policy report explores the causes of such strong Latino support for environmental protection and government action to control climate change. Sam García, Latinos and Climate Change: Opinions, Impacts, and Responses (GreenLatinos and The City Project 2016), available at www.cityprojectca.org/blog/archives/43303 (accessed June 24, 2016). The communities that have shown the most consistent support for climate change, people of color, are generally marginalized or absent from the discussion by mainstream environmental organizations, academics, and government in carbon pricing schemes, including cap and trade, cap and dividend, and regulatory measures. The environmental justice movement has demonstrated that racially and ethnically identifiable communities are at a greater risk
The Federal Transit Administration addresses the framework in its civil rights and environmental justice guidance documents and has applied the framework to withhold federal funding in the transit context in Northern California (DOT, 2012a,b; The City Project, 2015). Box 6-2 describes an economic analysis of a policy intervention that advanced health equity.
Using Civil Rights Law
The following guidance can help civil rights attorneys, public health professionals, community groups, public agencies, recipients of public funding, foundations, and other stakeholders promote community-based solutions to promote health equity using civil rights tools and reinforce a culture of health (Rodriguez et al., 2014):
- Communities and other stakeholders can work together on compliance and equity plans for programs or activities by recipients of public funding that use the civil rights framework by describing what is to be done, analyzing the impact on all communities, analyzing alternatives, including full and fair participation by diverse communities, and promoting health equity.
- Compliance and equity plans can be used to guard against unjustified and unnecessary discriminatory impacts, as well as against intentional discrimination, in health and wellness programs and activities.
- Communities, when appropriate, can work with civil rights attorneys to use problem-solving strategies, including coalition building, planning, data collection and analysis, media, negotiation, policy and legal advocacy out of court, and access to justice through the courts.
- Communities can work with attorneys and public health experts together to promote a better understanding of the civil rights dimension of the challenge of health disparities and to show how to address these civil rights concerns for their communities to ensure that civil rights laws against discrimination in health and other publicly funded programs and activities are strengthened and not rolled back.
___________________
of environmental harms, disproportionately lack environmental benefits, pay a larger cost, and carry a heavier environmental burden than other communities regardless of class. Once these costs are considered the distribution of benefits must necessarily be structured to pay down that debt. Gerald Torres and Robert García, Impact of Pricing Schemes on Environmental Justice Communities (The City Project Policy Report 2016), available at www.cityprojectca.org/blog/archives/43641 (accessed June 24, 2016).
Conclusion 6-1: In the committee’s judgment, civil rights approaches have helped mitigate the negative impacts of many forms of social and health discrimination. Continuing this work is needed to overcome discrimination and the structural barriers that affect health.
Conclusion 6-2: The committee concludes that using civil rights approaches in devising and implementing community solutions to promote health equity can guard against unjustified and unnecessary discriminatory impacts, as well as against intentional discrimination in programs that affect health. For example, those implementing community solutions can employ methods and data in ways that include full and fair participation by diverse communities.
See Chapter 8 for additional discussion on how civil rights law can support community-based solutions.
HEALTH POLICY
The Patient Protection and Affordable Care Act
The ACA has changed the financing, organization, and delivery of U.S. health care services in a number of important ways. It not only expands private and public health insurance but also reforms how Medicare and Medicaid services are delivered and revises the tax code in important ways that encourage nonprofit hospitals to invest in their local communities in new ways. The following section briefly reviews selected features of the ACA and discusses both how these features affect communities and how federal policy could be changed to affect health equity at the community level.
The ACA has expanded access to Medicaid coverage and private insurance to millions of individuals. Nationally, since 2010, rates of uninsured have dropped from 16.0 percent in 2010 to 9.2 percent in 2015 (Cohen and Martinez, 2015). Significantly, in part because 32 states expanded their Medicaid programs and 19 did not, the rates of uninsured among the nonelderly population varies significantly from a low of 5 percent in Massachusetts to a high of 19 percent in Texas (Kaiser Family Foundation, 2015, 2016). State decisions regarding Medicaid expansion were controversial and highly politicized in many states (Jacobs and Callaghan, 2013). Yet, these state decisions have important implications for communities. The variation in uninsured rates is more dramatic across metropolitan areas; among the 25 largest metropolitan areas the rates range from 4 to 19 percent (U.S. Census Bureau, 2015). On average, urban and rural counties have higher rates of the uninsured than suburban counties. Moreover,
geographically uninsured whites are more likely to live in areas with high poverty census tracts, whereas minorities are more likely to be uninsured wherever they live (REACH Healthcare Foundation, 2016).
State policy around health insurance, particularly through Medicaid decision making, has serious implications for health and other disparities. On the one hand, the impact of health insurance on health outcomes has been found to be mixed, at least in the short run. For instance, while biometric measures of health were not found to improve in a study of the Oregon Medicaid expansion, self-reported health was found to improve. Other studies have also found improvements in self-reported health (Sommers et al., 2012), but not consistently (Wherry and Miller, 2016). On the other hand, health insurance is seen as a potential mechanism for increasing use of preventive and other medical care services. Although health insurance lowers the cost of care to individuals, other factors may also be important and counter lower costs, such as wait times for appointments, distances to services, and the perceived discomfort of the care itself. The empirical literature has found overwhelmingly that insurance expansions improve access to medical care (Finkelstein et al., 2012; Miller, 2012; Van Der Wees et al., 2013). Additionally, greater health insurance plays an important financial role by shielding individuals from out-of-pocket medical costs and improving their overall financial status (Hu et al., 2016). The annual cost of inpatient care for a person between the ages of 18 and 64 who was hospitalized in 2012 was approximately $15,000, and the annual cost of all types of care for that person in the same year was $25,000 (Hu et al., 2016). Individuals without health insurance often have difficulty paying medical expenses and may need to borrow money or forego other necessities such as food, heat, or rent. They are more likely to be contacted by collection agencies and are more likely to declare bankruptcy (Cunningham, 2008; Dobkin et al., 2016; Doty et al., 2008; Finkelstein et al., 2012). Thus, medical bills play a large role in individuals’ overall financial picture, including their ability to save and make other investments. The expansions of Medicaid, including expansions under the ACA, have been found to substantially reduce the financial burden of medical care on low-income individuals and to increase their financial well-being (Baicker et al., 2013; Gross and Notowidigdo, 2011; Hu et al., 2016).
The health insurance provisions of the ACA have important implications for local communities. Although communities individually may have little influence over state and federal policy change, they can leverage existing policies to their advantage. Thus, communities can actively promote health insurance enrollment activities and help increase the number of individuals with health insurance in their communities, leading to greater financial well-being.
Hospital Community Benefit
Another important provision of the ACA for communities relates to charitable or nonprofit hospitals (in 2014, 78 percent of approximately 5,000 U.S. hospitals were nonprofit, exempt from most federal, state, and local taxes [Berwick et al., 2008; James, 2016]). In particular, the ACA changed the Internal Revenue Code such that all charitable hospitals must conduct community health needs assessments (CHNAs) and adopt an implementation strategy that addresses the needs identified in that assessment. Furthermore, the process must include “persons who represent the broad interests of the community served by the hospital facility, including those with special knowledge of or expertise in public health.” Moreover, regulations issued in 2014 specify that the CHNA should include “the need to address financial and other barriers to accessing care, to prevent illness, to ensure adequate nutrition, or to address social, behavioral, and environmental factors that influence health in the community” (C.F.R. 501(r)3(4)), and it was later clarified in an executive update that this includes some forms of housing improvements. Nonetheless, federal reporting forms and instructions have caused some confusion related to community benefit, investments in improving the social determinants of health, and CHNAs. As health insurance coverage has expanded, the level of uncompensated care provided by hospitals has declined, leaving hospitals to consider other areas and ways to invest community benefit dollars. Some hospitals have shown greater interest in community-wide health investments and the underlying factors that affect population health rather than maintaining the more narrow focus on health care services and funding offsets (Rosenbaum and Choucair, 2016). In the report Can Hospitals Heal America’s Communities? Howard and Norris wrote that by “addressing these social determinants of health through their business and non-clinical practices (for example, through purchasing, hiring, and investments), hospitals and health systems can produce increased measurably beneficial impacts on population and community health” (Howard and Norris, 2015, pp. 1–2). Examples of efforts that have used community benefit investments to build, hire, and invest in the local community include Kaiser Permanente in California and elsewhere and Promedica in Cleveland (NASEM, 2016d).
Recommendation 6-4: Through multi-sectoral partnerships, hospitals and health care systems should focus their community benefit dollars to pursue long-term strategies (including changes in law, policies, and systems) to build healthier neighborhoods, expand access to housing, drive economic development, and advance other upstream initiatives aimed at eradicating the root causes of poor health, especially in low-income
communities. Hospital and health systems should also advocate for the expansion of efficient and effective services responding to health-related social needs34 for vulnerable populations and people living in poverty.
This work should include meaningful participation by members of low-income and minority populations in the community. In addition to leveraging federal tax provisions around community health benefit in order to improve the social determinants of health and health equity, work by the Institute for Healthcare Improvement has shown that hospitals effectively tackle health equity not only in the community but also within their own institutions (Wyatt et al., 2016). Box 6-3 features an example of policy-driven work to reduce disparities in Maryland.
Triple Aim
Another component of the ACA is an emphasis on improving care, improving population health, and reducing the per capita cost of care. This notion of the “Triple Aim” is a term coined by the Institute for Healthcare Improvement and incorporated in ACA implementation, becoming part of the U.S. national strategy for tackling health care issues (AHRQ, 2016a; Berwick et al., 2008; Whittington et al., 2015). States, such as Massachusetts, also focus on Triple Aim outcomes: for example, through the Massachusetts Quality and Cost Council (AHRQ, 2016b; Holahan and Blumberg, 2006).
In its original conception, the Triple Aim seeks to improve the individual experience of care, improve the health of populations, and reduce the per capita costs of care for populations (Berwick et al., 2008). The Triple Aim is notably silent on health disparities. Perhaps this perspective stems from an initial focus on the private actors in the United States carrying out the Triple Aim, by selecting populations of interest, improving quality, and lowering costs. In fact, the architects of the Triple Aim approach cautioned that equity could be sacrificed in pursuit of the Triple Aim: the health of one population could be achieved at the expense of another. More recently, others have called for a “triple aim for health equity” that broadens the focus and embeds health care in a community-based
___________________
34 Alley et al. describe services addressing health-related social needs, including transportation and housing (Alley et al., 2016). Others define services addressing such needs as “wraparound services,” referring to linkages or services health care providers can offer to ensure, for example, that patients have transportation to routine health care appointments, have adequate food in their homes, and obtain legal (e.g., for tenant-landlord disputes about environmental exposure to asthma triggers) or social service assistance. See, for example, Bell and Cohen (2009).
framework (Ehlinger, 2015). At issue is that the pursuit of the Triple Aim could perpetuate and even worsen disparities unless the concept is expanded to incorporate a health equity focus. A continued focus on rewarding health outcomes at the mean, without rewarding a compression in the variations in health, is likely to encourage interventions that target healthier, and socially less disadvantaged, populations in order to demonstrate improvements. Under such a reward system gaps in health between advantaged and disadvantaged populations may grow even wider.
Frequently, the pursuit of the Triple Aim is combined with an emphasis on care integration and bundled payment for services across settings in order to encourage efficiency and cost control (Berwick et al., 2008). The challenge from a health disparities standpoint is the skewed nature of health expenditures, with 1 percent of the population accounting for approximately 21.4 percent of health care expenditures, with average per-person annual expenditures of $87,570 (Cohen and Uberoi, 2013). Thus, there is a strong incentive for integrated health systems and those
receiving bundled payment to avoid the 1 percent of patients who present the highest costs. This subgroup also is disproportionately socially disadvantaged. Some evidence indicates the existence of potential challenges with respect to disadvantaged groups for programs such as the accountable care organizations that arose from the Triple Aim approach. In particular, a recent study found that commercial and Medicare accountable care organization networks were relatively less likely to include physicians in areas where a higher percentage of the population was African American, living in poverty, uninsured, disabled, or had a rate of high school education less than in other areas (Yasaitis et al., 2016). Even where variation in health outcomes is used as a performance metric, a strategy of encouraging the enrollment of those at low risk and avoiding those at high risk can artificially inflate performance measures. The implication is that high-powered financial incentives, such as capitation and bundled payment, may elicit unintended responses from delivery systems and perpetuate health inequities.
Recommendation 6-5: Government and nongovernment payers and providers should expand policies aiming to improve the quality of care, improve population health, and control health care costs35 to include a specific focus on improving population health for the most vulnerable and underserved. As one strategy to support a focus on health disparities, the Centers for Medicare & Medicaid Services could undertake research on payment reforms that could spur accounting for social risk factors in the value-based payment programs it oversees.
The National Academies Committee on Accounting for Socioeconomic Status in Medicare Payment Programs has shown in its reports (NASEM, 2016a,b,c,e) that value-based payment systems that do not account for social risk factors can have unintended adverse consequences, including providers and health plans avoiding low-income patients and underpayment to providers disproportionately serving socially at-risk populations (such as safety net providers). These unintended consequences could in turn lead to deterioration in the quality of health care for socially at-risk populations and widening health disparities. That committee has stated that reducing disparities in access, quality, and outcomes is one of four policy goals in accounting for social risk factors (NASEM, 2016a,b,c,e), and its reports suggest that reforms to value-based payment programs that compensate providers fairly and increase fairness and accuracy in
___________________
35 Better care, better population health, and lower cost are often described as the Triple Aim (Berwick et al., 2008).
public reporting can help achieve goals to reduce disparities and improve quality and efficiency of care for all patients.
CRIMINAL JUSTICE POLICY
The criminal justice system plays an important role in shaping health equity through multiple mechanisms. The first, which is conceptually straightforward, includes the health care screening and treatment services that the system provides to adult and juvenile prisoners and probationers. The second is more complex and far-ranging and includes the set of policies that determine if an individual becomes involved in the justice system, for how long, whether or not alternative sanctions will be offered, and how individuals will reenter the community after incarceration. These policies have long-term implications for education completion, employment, and income—all of which in turn affect health. Because the justice-involved population is disproportionately people of color and disproportionately comprises other vulnerable populations such as persons with mental illness, criminal justice policies have important implications for health equity.
The United States today has the highest rate of incarceration in the world, with a cost to states and the federal government of $80 billion in 2010 alone (DOJ, 2013). This remarkably high rate of incarceration stems from policies adopted by federal and state governments starting in the early 1980s, particularly around mandatory sentencing, “three strikes and you’re out,” and increasing drug-related incarceration (Blumstein and Beck, 1999; Mauer, 2001).
The current era of mass incarceration can be understood as a powerful policy intervention in the lives of the poor and people of color (Pettit and Western, 2004). Indeed, criminal justice policy and practice disproportionately affect minorities in a number of ways, and there is a large racial disproportionality at most stages of the criminal justice system for both adults and juveniles (Harris et al., 2009).
Policies related to the “war on drugs” since the 1980s have played an especially pivotal role in institutionalizing disproportionate minority contact with the criminal justice system. Many scholars have remarked that federal drug policies have targeted racial and ethnic minorities and especially African Americans and their communities. The differences in mandatory minimum sentencing guidelines for crack cocaine, which has been associated with poor and minority users, versus powder cocaine, whose users tend to be white (Palamar et al., 2015), is a case in point. Although the two substances are virtually identical on a molecular level, the Anti-Drug Abuse Act of 1986 stipulated a 100:1 weight ratio for powder versus crack cocaine when determining mandatory minimum sentences for
possession (Palamar et al., 2015). In practice, this meant that 5 grams of crack, for example, mandated the same sentence (5 years in prison) as 500 grams of cocaine. Although the disparity was recently revised to an 18:1 ratio by the 2010 Fair Sentencing Act, scholars and community advocates have long argued that any disparity targets crack and, by extension, poor and minority users (Palamar et al., 2015). As a result, federal drug policies that sanction crack more than powder cocaine have exacerbated a wide-scale racial inequity that characterizes criminal justice sanctions for drug use and possession.
Blumstein highlights several other mechanisms by which racial and socioeconomic disproportionality can compound itself in the criminal justice system (Blumstein, 2009). Because more serious crimes occur in poor neighborhoods, police patrol them more densely. This also leads individuals in these areas to be more likely to be arrested (Blumstein, 2009), and, because punishment is a function of prior police contact, the marginal arrest leads to greater punishment down the line. This disadvantage can build if it is combined with such police practices as racial profiling when deciding whom to stop, question, and search (Ridgeway and MacDonald, 2010). Hispanics and African Americans are disproportionately confined in jails and prisons than would be predicted by their arrest rates, and Hispanic and African American juveniles are more likely to be referred to adult court rather than juvenile court relative to white juveniles (Harris et al., 2009).
Disadvantage can further compound inequities in other ways. Youth who live in stable two-parent, higher-income families are more likely to be released than youth living in single-parent, lower-income families, which has implications also for further sanctions and for educational disruptions. Moreover, minority youth are more likely to face harsh disciplinary action in schools by being suspended or referred to court (Mizel et al., 2016), and schools with stringent disciplinary policies that favor suspension can also contribute to greater arrests among youth (Cuellar and Markowitz, 2015).
The high budgetary and social costs of imprisonment have led federal and state policy makers to reconsider sentencing and sanctioning rules. At the federal level, although there are mandatory minimum laws, changes were instituted to lower punishments for low-level, nonviolent drug offenses by individuals with no ties to large-scale organizations or gangs and to reduce sentences for certain inmates (DOJ, 2013). Texas and Arkansas also have reduced their prison populations by identifying alternative sanctions for low-level drug offenders. Kentucky similarly has shifted resources from prison beds to treatment services for offenders with behavioral health problems and greater community supervision. Other state initiatives, such as drug courts, have been found to
reduce disparities for Hispanics and, to some extent, for African Americans (Nicosia et al., 2013). At the juvenile level, states have also sought to promote treatment alternatives to incarceration for selected populations with behavioral health problems (Cuellar and Dave, 2016; Cuellar et al., 2006). Since 2007, the Justice Reinvestment Initiative—a public–private partnership that includes the DOJ Bureau of Justice Assistance—has also supported efforts in 33 states, all of which “aim to improve public safety and control taxpayer costs by prioritizing prison space for serious and repeat offenders and investing some of the savings in alternatives to incarceration for low-level offenders that are effective at reducing recidivism” (The Pew Charitable Trusts, 2016).
Recidivism is a large problem for the individuals who have been convicted. Recidivism has been linked in part to barriers faced by those with a criminal record. Federal, state, and local policies can exacerbate these barriers by stipulating legal sanctions and restrictions imposed on individuals with criminal records. The areas in which such challenges are faced include housing, employment, education, public benefits, and permission to travel. Some states “prohibit the employment of convicted felons in occupations ranging from child- and dependent-care service providers to barbers and hairdressers” (Bushway et al., 2007, p. 3). Some states also cut off their access to public employment, which has been an important source of work for inner-city minorities (Bushway et al., 2007). The American Bar Association has compiled the National Inventory of Collateral Consequences of Conviction, which catalogs the wide-ranging collateral consequences of criminal convictions contained in the numerous laws and regulations at the federal and state levels (ABA, 2016). As Bushway and colleagues suggest, policies like these can present formidable barriers to successful reintegration into society after release from prison (Bushway et al., 2007).
Recognizing the role that local policies play in marginalizing those with a criminal record, some communities have advocated for laws aimed at reducing the barriers to reentry for the formerly incarcerated. As of 2016 more than 150 cities and counties have adopted “ban the box” policies that prohibit employers from considering criminal records at the beginning of the application process. Ban-the-box policies instead require that employers first consider a job candidate’s qualifications (Rodriguez and Avery, 2016). However, recent data reveal that ban-the-box policies may have a negative effect on work opportunities for young, low-skilled African American and Hispanic men (Doleac and Hansen, 2016). Reentry is also a difficult transition for juveniles. Many states have developed special programs for youth, including mentoring, mental health counseling, education supports, and family reunification supports, to facilitate successful reintegration and the transition to adulthood, and some have
reformed their juvenile justice system (see, for example, The Pew Charitable Trusts, 2014).
While incarcerated, those confined to jail, prison, halfway houses, or juvenile facilities are reliant upon the justice system to provide for their health care needs. Many of these services are funded by criminal justice budgets. In addition, individuals may be eligible for Medicaid-funded services if they are not prisoners per se,36 such as when they reside in transitional reentry institutions or if they are not committed (Gupta et al., 2005). State and federal Medicaid policies can affect the available funding for health care services for these groups. With the recent expansion of Medicaid under the ACA, states and the federal government are revisiting Medicaid regulations related to the adult criminal justice population and facilitating access to Medicaid for eligible individuals prior to and after a stay in a correctional institution (CMS, 2016).
Beyond the far-reaching effects of a criminal record, criminal justice policies can play a role in health equity by influencing the odds of victimization (e.g., through gun policies). Clearly, firearm violence remains an important public health concern for many communities across the country (Monuteaux et al., 2015). With more than 10,000 Americans killed by firearms in 2014 (Kochanek et al., 2016), the United States suffers from the highest rate of firearm homicides among industrialized nations (IOM and NRC, 2013), and the burden of gun violence is borne disproportionately by economically disadvantaged communities, particularly communities of color (Altheimer, 2008). Exceptional levels of gun violence coexist alongside deeply polarized views over gun rights and gun policy. On the one hand, repeated episodes of large-scale gun violence in the United States have provoked proponents of gun control to argue for stricter policies to regulate the availability of guns in communities. On the other hand, proponents of gun rights argue that gun availability deters crime and enhances personal defense. Recent research in the American Journal of Preventive Medicine (Monuteaux et al., 2015) finds household gun ownership rates associate positively with various forms of violence across states. Other research concludes that living in a city with high rates of household gun ownership leads to greater odds of gun assault or gun robbery victimization (Altheimer, 2008). This research suggests that policies aimed at curbing firearm availability might help reduce violence in communities. However, the overall state of research on the relationship between gun availability and violence is mixed and offers contrasting views about the importance of gun regulation for violence. Furthermore, research that focuses specifically on how gun control policies influence firearm violence is also inconclusive (IOM and NRC, 2013).
___________________
36 Medicaid does not cover “inmates of a public institution.”
The recommendations of a recent IOM and National Research Council report that calls for more research on the potential efficacy of gun control policies in preventing firearm violence in U.S. communities continue to resonate (IOM and NRC, 2013). Chapter 7 includes a discussion of actions in public safety that could be considered to begin to bring about change from the community level up.
CONCLUDING OBSERVATIONS
Chapter 4 discussed the importance of communities and the fact that they not only are the locus for change, they also possess agency and can draw on their own power and assets to help effect change. However, as acknowledged in that chapter, it can be difficult for communities to promote health equity on their own. The present chapter describes the effects that policies and laws can have on communities. To sustain change over the long term, the broader context of issues that influence community efforts and success needs to be addressed.
REFERENCES
ABA (American Bar Association). 2016. National Inventory of Collateral Consequences of Conviction (NICCC). http://www.abacollateralconsequences.org (accessed May 13, 2016).
Ackerman, B. A. 2014. We the people, volume 3: The civil rights revolution, The civil rights revolution. Cambridge, Massachusetts: Belknap Press of Harvard University Press.
Adler, N. E., and D. H. Rehkopf. 2008. US disparities in health: Descriptions, causes, and mechanisms. Annual Review of Public Health 29:235–252.
AHRQ (Agency for Healthcare Research and Quality). 2016a. About the National Quality Strategy (NQS). http://www.ahrq.gov/workingforquality/about.htm#priorities (accessed October 14, 2016).
AHRQ. 2016b. Working for quality: National Quality Strategy (NQS). http://www.ahrq.gov/workingforquality (accessed October 17, 2016).
Alley, D. E., C. N. Asomugha, P. H. Conway, and D. M. Sanghavi. 2016. Accountable health communities—addressing social needs through Medicare and Medicaid. The New England Journal of Medicine 374(1):8.
Altheimer, I. 2008. Do guns matter—a multi-level cross-national examination of gun availability on assault and robbery victimization. Western Criminology Review 9:9.
Andrews, N. O., D. J. Erickson, I. Galloway, and E. Seidman. 2012. Investing in what works for America’s communities. San Francisco: Federal Reserve Bank of San Francisco and Low Income Investment Fund.
Autor, D. H., A. Manning, and C. L. Smith. 2016. The contribution of the minimum wage to U.S. wage inequality over three decades: A reassessment. NBER Working Paper No. 16533. http://www.nber.org/papers/w16533 (accessed October 24, 2016).
Baicker, K., S. L. Taubman, H. L. Allen, M. Bernstein, J. H. Gruber, J. P. Newhouse, E. C. Schneider, B. J. Wright, A. M. Zaslavsky, and A. N. Finkelstein. 2013. The Oregon experiment—effects of Medicaid on clinical outcomes. New England Journal of Medicine 368(18):1713–1722.
Bartilow, G. 2016. The safety net in Kentucky lifts 810,000 people out of poverty. Kentucky Center for Economic Policy Policy Blog. http://kypolicy.org/safety-net-kentucky-lifts-810000-people-poverty (accessed October 24, 2016).
Beatty, A., and D. Foster. 2015. The determinants of equity: Identifying indicators to establish a baseline of equity in King County. King County, WA.
Bell, J., and L. Cohen. 2009. The transportation prescription: Bold new ideas for healthy, equitable transportation reform in America, 2009. Commissioned by the convergence partnership. https://www.preventioninstitute.org/sites/default/files/publications/The%20Transportation%20Prescription_0.pdf (accessed December 1, 2016).
Ben-Shalom, Y., R. A. Moffitt, and J. K. Scholz. 2011. An assessment of the effectiveness of antipoverty programs in the United States. Cambridge, MA: National Bureau of Economic Research.
Berwick, D. M., T. W. Nolan, and J. Whittington. 2008. The triple aim: Care, health, and cost. Health Affairs 27(3):759–769.
Bitler, M., and H. Hoynes. 2013. The more things change, the more they stay the same? The safety net and poverty in the great recession. Cambridge, MA: National Bureau of Economic Research.
Bitler, M., H. Hoynes, and E. Kuka. 2016. Child poverty, the great recession, and the social safety net in the United States. Cambridge, MA: National Bureau of Economic Research.
Blumstein, A. 2009. Race and the criminal justice system. Race and Social Problems 1(4):183–186.
Blumstein, A., and A. J. Beck. 1999. Population growth in U.S. prisons, 1980–1996. Crime & Justice. 26:17.
Branas, C. C., R. A. Cheney, J. M. MacDonald, V. W. Tam, T. D. Jackson, and T. R. Ten Have. 2011. A difference-in-differences analysis of health, safety, and greening vacant urban space. American Journal of Epidemiology 174(11):1296–1306.
Burke, M. P., E. A. Frongillo, S. J. Jones, B. B. Bell, and H. Harline-Grafton. 2016. Household food insecurity is associated with greater growth in body mass index among female children from kindergarten through eighth grade. Journal of Hunger and Environmental Nutrition 11(2):227–241.
Bushway, S., D. F. Weiman, and M. A. Stoll. 2007. Barriers to reentry?: The labor market for released prisoners in post-industrial America. New York, NY: Russell Sage Foundation.
CBO (Congressional Budget Office). 2016. The distribution of household income and federal taxes, 2013. https://www.cbo.gov/sites/default/files/114th-congress-2015-2016/reports/51361-HouseholdIncomeFedTaxes_OneCol.pdf (accessed October 24, 2016).
CDC (U.S. Centers for Disease Control and Prevention). 2009. Health effects of gentrification. http://www.cdc.gov/healthyplaces/healthtopics/gentrification.htm (accessed July 7, 2016).
ChangeLab Solutions. 2015. Preserving, protecting, and expanding affordable housing: A policy toolkit for public health. http://www.changelabsolutions.org/sites/default/files/Preserving_Affordable_Housing-POLICY-TOOLKIT_FINAL_20150401.pdf (accessed October 24, 2016).
ChangeLab Solutions. 2016. Model comprehensive plan language on complete streets: A framework to embrace complete streets principle. http://www.changelabsolutions.org/publications/comp-plan-language-cs (accessed October 24, 2016).
Chetty, R., M. Stepner, S. Abraham, S. Lin, B. Scuderi, N. Turner, A. Bergeron, and D. Cutler. 2016. The association between income and life expectancy in the United States, 2001–2014. JAMA 315(16):1750–1766.
CHOICES (Childhood Obesity Intervention Cost-Effectiveness Study). 2016. Brief: Cost-effectiveness of a sugar-sweetened beverage excise tax in Philadelphia, PA. http://choicesproject.org/brief-cost-effectiveness-of-a-sugar-sweetened-beverage-excise-tax-in-philadelphia-pa (accessed November 23, 2016).
Chow, J. C.-C., M. A. Johnson, and M. J. Austin. 2006. The status of low-income neighborhoods in the post-welfare reform environment. Journal of Health & Social Policy 21(1):1–32.
Christensen, J. 2016. Environmental bonds should equitably benefit all communities: Looking forward based on an analysis of Prop 84. Los Angeles: University of California, Los Angeles, Institute of the Environment and Sustainability.
CMS (Centers for Medicare & Medicaid Services). 2016. State health official letter re: to facilitate successful re-entry for individuals transitioning from incarceration to their communities. Baltimore, MD: U.S. Department of Health and Human Services.
Cohen, R. A., and M. E. Martinez. 2015. Health insurance coverage: Early release of estimates from the National Health Interview Survey, January–March 2015. Hyattsville, MD: National Center for Health Statistics.
Cohen, S., and N. Uberoi. 2013. Differentials in the concentration in the level of health expenditures across population subgroups in the US, 2010. Statistical brief 421.
Collinson, R., I. G. Ellen, and J. Ludwig. 2015. Low income housing policy. In Economics of means-tested transfer programs in the United States, volume 2. Chicago, IL: University of Chicago Press.
CSG (Council of State Governments). 2016. States receiving technical assistance from the CSG Justice Center. https://csgjusticecenter.org/jr (accessed October 24, 2016).
Cuellar, A., and D. M. Dave. 2016. Causal effects of mental health treatment on education outcomes for youth in the justice system. Economics of Education Review 54:321–339.
Cuellar, A. E., and S. Markowitz. 2015. School suspension and the school-to-prison pipeline. International Review of Law and Economics 43:98–106.
Cuellar, A. E., L. S. McReynolds, and G. A. Wasserman. 2006. A cure for crime: Can mental health treatment diversion reduce crime among youth? Journal of Policy Analysis and Management 25(1):197–214.
Cunningham, P. J. 2008. Track report: Trade-offs getting tougher: Problems paying medical bills increase for U.S. families, 2003-2007. Washington, DC: Center for Studying Health System Change.
Currie, J., and A. Yelowitz. 2000. Are public housing projects good for kids? Journal of Public Economics 75(1):99–124.
Cutler, D. M., and A. Lleras-Muney. 2006. Education and health: Evaluating theories and evidence. Working paper no. 12352. Cambridge, MA: National Bureau of Economic Research.
Dahl, G. B., and L. Lochner. 2005. The impact of family income on child achievement. Working paper no. 11279. Cambridge, MA: National Bureau of Economic Research.
Darcy, J. 2016. Memorandum for commander, U.S. Army Corps of Engineers. Proposed Dakota Access Pipeline crossing at Lake Oahe, North Dakota. https://www.army.mil/e2/c/downloads/459011.pdf (accessed December 5, 2016).
Ding, L., and J. Hwang. 2016. The consequences of gentrification: A focus on residents’ financial health in Philadelphia: Working paper 16-22. Research Department, Federal Reserve Bank of Philadelphia 40.
Ding, L., J. Hwang, and E. Divringi. 2015. Gentrification and residential mobility in Philadelphia. Philadelphia, PA: Federal Reserve Bank of Philadelphia.
Dobkin, C., A. Finkelstein, R. Kluender, and M. J. Notowidigdo. 2016. The economic consequences of hospital admissions. Working paper no. 22288. Cambridge, MA: National Bureau of Economic Research.
DOJ (U.S. Department of Justice). 2013. Smart on crime: Reforming the criminal justice system for the 21st century. https://www.justice.gov/sites/default/files/ag/legacy/2013/08/12/smart-on-crime.pdf (accessed October 20, 2016).
Doleac, J. L., and B. Hansen. 2016. Does “ban the box” help or hurt low-skilled workers? Statistical discrimination and employment outcomes when criminal histories are hidden. Cambridge, MA: National Bureau of Economic Research.
DOT (U.S. Department of Transportation). 2012a. Environmental justice policy guidance for Federal Transit Administration recipients (FTA c 4703.1). U.S. government.
DOT. 2012b. Title VI requirements and guidelines for Federal Transit Administration recipients (FTA C4702. 1B). U.S. government.
Doty, M. M., S. R. Collins, S. D. Rustgi, and J. L. Kriss. 2008. Seeing red: The growing burden of medical bills and debt faced by U.S. families: Issue brief. The Commonwealth Fund 42(August).
ED (U.S. Department of Education). 2016a. Healthy students, promising futures: State and local action steps and practices to improve school-based health toolkit. http://www2.ed.gov/admins/lead/safety/healthy-students/index.html (accessed October 24, 2016).
ED. 2016b. Racial and ethnic disparities in special education: A multi-year disproportionality analysis by state, analysis category, and race/ethnicity. Washingon, DC: U.S. Department of Education.
ED. 2016c. U.S. Department of Education takes action to deliver equity for students with disabilities. http://www.ed.gov/news/press-releases/us-department-education-takes-action-deliver-equity-students-disabilities (accessed November 23, 2016).
Ehlinger, E. P. 2015. We need a triple aim for health equity. Minnesota Medicine: 28–29.
Ellen, I. G., K. M. Horn, and A. E. Schwartz. 2016. Why don’t housing choice voucher recipients live near better schools? Insights from big data. Journal of Policy Analysis and Management 35(4):884–905.
Environmental Justice Leadership Forum on Climate Change. 2016a. Clean power plan tool kit. http://www.ejleadershipforum.org/clean-power-plan-tool-kit (accessed October 24, 2016).
Environmental Justice Leadership Forum on Climate Change. 2016b. Environmental justice state guidance: How to incorporate equity and justice into your state clean power planning approach.http://www.eesi.org/files/EJ-State-Guidance-Final-v5-jan-15-2016.pdf (accessed October 24, 2016).
EPA (U.S. Environmental Protection Agency). 2016. EJScreen: Environmental justice screening and mapping tool (version 2016). https://ejscreen.epa.gov/mapper (accessed October 24, 2016).
Evans, W. N., and C. L. Garthwaite. 2014. Giving mom a break: The impact of higher EITC payments on maternal health. American Economic Journal: Economic Policy 6(2):258–290.
Executive Office of the President. 2015. Long-term benefits of the Supplemental Nutrition Assistance Program. https://www.whitehouse.gov/sites/whitehouse.gov/files/documents/SNAP_report_final_nonembargo.pdf (accessed November 23, 2016).
Finch, B. K., A. N. Beck, and H. Amaro. 2016. Does gentrification contribute to segregation? A study of urban displacement. Population Association of America Annual Meeting, Washington, DC. Poster presentation, March 18, 2016.
Finkelstein, A., S. Taubman, B. Wright, M. Bernstein, J. Gruber, J. P. Newhouse, H. Allen, K. Baicker, and Oregon Health Study Group. 2012. The Oregon health insurance experiment: Evidence from the first year. The Quarterly Journal of Economics 127(3):1057–1106.
Freeman, L. 2005. Displacement or succession? Residential mobility in gentrifying neighborhoods. Urban Affairs Review 40(4):463–491.
GAO (U.S. Government Accountability Office). 2015. Federal low-income programs: Multiple programs target diverse populations and needs. U.S. Government Accountability Office.
Garcia, R. 2013. The George Butler lecture, social justice and leisure: The usefulness and uselessness of research. Journal of Leisure Research 46:7–22.
Garcia, R., A. Collins, and C. De La Vega. 2016. Park funding for all! Parks & Recreation 32–33. http://www.cityprojectca.org/blog/archives/43709 (accessed October 24, 2016).
Garvin, E. C., C. C. Cannuscio, and C. C. Branas. 2013. Greening vacant lots to reduce violent crime: A randomised controlled trial. Injury Prevention 19(3):198–203.
Goldberg, D. 2016. Bay area and Boulder soda taxes would extend lives, avert millions in health care costs over 10 years, Harvard model projects. Healthy Food America. http://www.healthyfoodamerica.org/bay_area_and_boulder_soda_taxes_would_extend_lives_avert_millions_in_health_costs_over_10_years_harvard_model_projects (accessed November 23, 2016).
Goldman, D., and J. P. Smith. 2011. The increasing value of education to health. Social Science & Medicine 72(10):1728–1737.
Gross, T., and M. J. Notowidigdo. 2011. Health insurance and the consumer bankruptcy decision: Evidence from expansions of Medicaid. Journal of Public Economics 95(7-8):767–778.
Gupta, R. A., K. J. Kelleher, K. Pajer, J. Stevens, and A. Cuellar. 2005. Delinquent youth in corrections: Medicaid and reentry into the community. Pediatrics 115(4):1077–1083.
Hamad, R., and D. H. Rehkopf. 2015. Poverty, pregnancy, and birth outcomes: A study of the earned income tax credit. Paediatric and Perinatal Epidemiology 29(5):444–452.
Hamad, R., and D. H. Rehkopf. 2016. Poverty and child development: A longitudinal study of the impact of the earned income tax credit. American Journal of Epidemiology 183(9):775-784.
Harris, C. T., D. Steffensmeier, J. T. Ulmer, and N. Painter-Davis. 2009. Are blacks and Hispanics disproportionately incarcerated relative to their arrests? Racial and ethnic disproportionality between arrest and incarceration. Race and Social Problems 1(4):187–199.
Healthy Schools Campaign. 2016. A new national initiative highlights the link between health and education. Healthy Schools Campaign. https://healthyschoolscampaign.org/policy/a-new-national-initiative-highlights-the-link-between-health-and-education (accessed July 16, 2016).
HHS (U.S. Department of Health and Human Services). 2016. Summary: Final rule implementing Section 1557 of the Affordable Care Act.
Holahan, J., and L. Blumberg. 2006. Massachusetts health care reform: A look at the issues. Health Affairs 25(6):w432–w443.
Howard, T., and T. Norris. 2015. Can hospitals heal America’s communities?: “All in for mission” is the emerging model for impact. Washington, DC: The Democracy Collaborative.
Hu, L., R. Kaestner, B. Mazumder, S. Miller, and A. Wong. 2016. The effect of the Patient Protection and Affordable Care Act Medicaid expansions on financial wellbeing. Working paper no. 22170. Cambridge, MA: National Bureau of Economic Research.
HUD (U.S. Department of Housing and Urban Development). 2016a. Low-income housing tax credits (LIHTC) data sets (May 15, 2016). https://www.huduser.gov/portal/datasets/lihtc.html (accessed December 16, 2016).
HUD. 2016b. Picture of subsidized households datasets. https://www.huduser.gov/portal/datasets/picture/yearlydata.html (accessed December 19, 2016).
Huynh, M., and A. R. Maroko. 2014. Gentrification and preterm birth in New York City, 2008-2010. Journal of Urban Health 91(1):211–220.
International Energy Agency. 2015. Capturing the multiple benefits of energy efficiency.http://www.iea.org/publications/freepublications/publication/capturing-the-multiple-benefits-of-energy-efficiency.html (accessed October 20, 2016).
IOM (Institute of Medicine). 2011. For the public’s health: Revitalizing law and policy to meet new challenges. Washington, DC: The National Academies Press.
IOM and NRC (National Research Council). 2013. Priorities for research to reduce the threat of firearm-related violence. Washington, DC: The National Academies Press.
IRS (Internal Revenue Service). 2016. Statistics for tax returns with EITC. https://www.eitc.irs.gov/EITC-Central/eitcstats?_ga=1.80629535.982617637.1477348670 (accessed December 19, 2016).
Jacob, B. A., M. Kapustin, and J. Ludwig. 2015. The impact of housing assistance on child outcomes: Evidence from a randomized housing lottery. The Quarterly Journal of Economics 130(1):465–506.
Jacobs, L. R., and T. Callaghan. 2013. Why states expand Medicaid: Party, resources, and history. Journal of Health Politics, Policy and Law 38(5):1023–1050.
Jacobs, L. R., and J. Soss. 2010. The politics of inequality in America: A political economy framework. Annual Review of Political Science 13(1):341–364.
James, J. 2016. Health policy brief: Nonprofit hospitals’ community benefit requirements. Health Affairshttp://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_153.pdf (accessed August 8, 2016).
Kaiser Family Foundation. 2015. Health insurance coverage of nonelderly 0-64. http://kff.org/other/state-indicator/nonelderly-0-64/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D (accessed September 10, 2016).
Kaiser Family Foundation. 2016. Current status of state action on the Medicaid expansion decision, KFF state health facts. http://kff.org/health-reform/slide/current-status-of-the-medicaid-expansion-decision (accessed September 10, 2016).
Kessler, R. C., G. J. Duncan, L. A. Gennetian, L. F. Katz, J. R. Kling, N. A. Sampson, L. Sanbonmatsu, A. M. Zaslavsky, and J. Ludwig. 2014. Associations of housing mobility interventions for children in high-poverty neighborhoods with subsequent mental disorders during adolescence. JAMA 311(9):937–948.
Kochanek, K. D., S. L. Murphy, J. Q. Xu, and B. Tejada-Vera. 2016. Deaths: Final data for 2014. National Vital Statistics Reports 65(4).
Kochtitzky, C. S., H. Frumkin, R. Rodriguez, A. Dannenberg, J. Rayman, K. Rose, R. Gillig, and T. Kanter. 2006. Urban planning and public health at CDC. Morbidity and Mortality Weekly Report Supplements 55(2):34–38.
Kyureghian, G., R. M. Nayga, and S. Bhattacharya. 2013. The effect of food store access and income on household purchases of fruits and vegetables: A mixed effects analysis. Applied Economic Perspectives and Policy 35(1):69–88.
Mathur, C., D. J. Erickson, M. H. Stigler, J. L. Forster, and J. R. Finnegan. 2013. Individual and neighborhood socioeconomic status effects on adolescent smoking: A multilevel cohort-sequential latent growth analysis. American Journal of Public Health 103(3):543–548.
Mauer, M. 2001. The causes and consequences of prison growth in the United States. Punishment & Society 3(1):9–20.
Meltzer, D. O., and Z. Chen. 2011. The impact of minimum wage rates on body weight in the United States. In Economic aspects of obesity. Chicago, IL: University of Chicago Press. Pp. 17–34.
Miller, S. 2012. The impact of the Massachusetts health care reform on health care use among children. American Economic Review 102(3):502–507.
Mizel, M. L., J. N. Miles, E. R. Pedersen, J. S. Tucker, B. A. Ewing, and E. J. D’Amico. 2016. To educate or to incarcerate: Factors in disproportionality in school discipline. Children and Youth Services Review 70:102–111.
Mohai, P., P. M. Lantz, J. Morenoff, J. S. House, and R. P. Mero. 2009. Racial and socioeconomic disparities in residential proximity to polluting industrial facilities: Evidence from the Americans’ changing lives study. American Journal of Public Health 99(Suppl 3):S649–S656.
Montez, J. K., and L. F. Berkman. 2014. Trends in the educational gradient of mortality among US adults aged 45 to 84 years: Bringing regional context into the explanation. American Journal of Public Health 104(1):e82–e90.
Monuteaux, M. C., L. K. Lee, D. Hemenway, R. Mannix, and E. W. Fleegler. 2015. Firearm ownership and violent crime in the US: An ecologic study. American Journal of Preventive Medicine 49(2):207–214.
Multnomah County. 2014a. Foundational assumptions of the equity and empowerment lens logic model. https://multco.us/file/31824/download (accessed October 28, 2016).
Multnomah County. 2014b. Multnomah County Office of Diversity and Equity: Equity and empowerment lens. https://multco.us/diversity-equity/equity-and-empowerment-lens (accessed October 24, 2016).
Multnomah County. n.d. What is the equity and empowerment lens?https://multco.us/diversity-equity/equity-and-empowerment-lens (accessed October 28, 2016).
NASEM (National Academies of Sciences, Engineering, and Medicine). 2015. The growing gap in life expectancy by income: Implications for federal programs and policy responses. Washington, DC: The National Academies Press.
NASEM. 2016a. Accounting for social risk factors in Medicare payment: Identifying social risk factors. Washington, DC: The National Academies Press.
NASEM. 2016b. Accounting for social risk factors in Medicare payment: Criteria, factors, and methods. Washington, DC: The National Academies Press.
NASEM. 2016c. Accounting for social risk factors in Medicare payment: Data. Washington, DC: The National Academies Press.
NASEM. 2016d. The role of business in multisector obesity solutions: Working together for positive change: Workshop in brief. Washington, DC: The National Academies Press.
NASEM. 2016e. Systems practices for the care of socially at-risk populations. Washington, DC: The National Academies Press.
Neumark, D., J. I. Salas, and W. Wascher. 2014. More on recent evidence on the effects of minimum wages in the United States. IZA Journal of Labor Policy 3(1):26.
Newman, K., and E. K. Wyly. 2006. The right to stay put, revisited: Gentrification and resistance to displacement in New York City. Urban Studies 43(1):23–57.
Nichols, A., and J. Rothstein. 2016. The earned income tax credit from the economics of means-tested transfer programs in the United States, volume one. Edited by R. A. Moffitt. Vol. 1, Economics of means-tested transfer programs in the United States. Chicago, IL: University of Chicago Press.
Nicosia, N., J. M. MacDonald, and J. Arkes. 2013. Disparities in criminal court referrals to drug treatment and prison for minority men. American Journal of Public Health 103(6):e77–e84.
NPS (National Park Service). 2013. San Gabriel watershed and mountains special resource study. https://parkplanning.nps.gov/document.cfm?documentID=43639 (accessed September 16, 2016).
NPS. 2014. Healthy parks healthy people community engagement e-guide: Edition 1.
NPS. 2015. Rim of the valley corridor special resource study and environmental assessment. https://parkplanning.nps.gov/document.cfm?documentID=65351 (accessed October 24, 2016).
NRC and IOM (National Research Council and Institute of Medicine). 2013. U.S. health in international perspective: Shorter lives, poorer health. Washington, DC: The National Academies Press.
Olshansky, S. J., T. Antonucci, L. Berkman, R. H. Binstock, A. Boersch-Supan, J. T. Cacioppo, B. A. Carnes, L. L. Carstensen, L. P. Fried, D. P. Goldman, J. Jackson, M. Kohli, J. Rother, Y. Zheng, and J. Rowe. 2012. Differences in life expectancy due to race and educational differences are widening, and many may not catch up. Health Affairs 31(8):1803–1813.
OMB (Office of Management and Budget). 2016. Analytical perspectives, budget of the United States government, fiscal year 2017. https://www.whitehouse.gov/omb/budget/Analytical_Perspectives (accessed October 24, 2016).
Palamar, J. J., S. Davies, D. C. Ompad, C. M. Cleland, and M. Weitzman. 2015. Powder cocaine and crack use in the United States: An examination of risk for arrest and socioeconomic disparities in use. Drug and Alcohol Dependence 149:108–116.
Pettit, B., and B. Western. 2004. Mass imprisonment and the life course: Race and class inequality in US incarceration. American Sociological Review 69(2):151–169.
PHAB (Public Health Accreditation Board). 2011. Public Health Accreditation Board standards & measures, version 1.0. http://www.phaboard.org/wp-content/uploads/PHAB-Standards-and-Measures-Version-1.01.pdf (accessed December 2, 2016).
Phillips, D., L. Flores Jr., and J. Henderson. 2014. Development without displacement. Oakland, CA: Causa Justa.
PolicyLink. 2016a. Equity tools: Affordable housing. http://www.policylink.org/equity-tools/equitable-development-toolkit/affordable-housing (accessed October 21, 2016).
PolicyLink. 2016b. Equity tools: Economic opportunity. http://www.policylink.org/equitytools/equitable-development-toolkit/economic-opportunity (accessed October 21, 2016).
REACH Healthcare Foundation. 2016. Mid-America Regional Council Community Services Corporation. https://reachhealth.org/awarded-grants/mid-america-regional-council-community-services-corporation-9 (accessed October 14, 2016).
Ricklin, A., and N. Kushner. 2014. Healthy plan making—integrating health into the comprehensive planning process: An analysis of seven case studies and recommendations for change. Chicago, IL: American Planning Association.
Ridgeway, G., and J. MacDonald. 2010. Methods for assessing racially biased policing. Race, ethnicity, and policing: New and essential readings. Pp. 180–204.
Rodriguez, M. N., and B. Avery. 2016. Ban the box: U.S. Cities, counties, and states adopt fair-chance policies to advance employment opportunities for people with past convictions. National Employment Law Project. http://www.nelp.org/content/uploads/Ban-the-Box-FairChance-State-and-Local-Guide.pdf (accessed December 17, 2016).
Rodriguez, M., M. Brenman, M. E. Lado, and R. Garcia. 2014. Using civil rights tools to address health disparities. Los Angeles, CA: The City Project.
Rosenbaum, S., and B. Choucair. 2016. Expanding the meaning of community health improvement under tax-exempt hospital policy. In Health Affairs Blog. http://healthaffairs.org/blog/2016/01/08/expanding-the-meaning-of-community-health-improvement-under-tax-exempt-hospital-policy (accessed September 28, 2016).
Sanbonmatsu, L., J. Ludwig, L. F. Katz, L. A. Gennetian, G. J. Duncan, R. C. Kessler, E. Adam, T. W. McDade, and S. T. Lindau. 2011. Moving to opportunity for fair housing demonstration program--final impacts evaluation. Washington, DC: U.S. Department of Housing and Urban Development Office of Policy Development and Research.
Schill, M. H., and S. M. Wachter. 1995. The spatial bias of federal housing law and policy: Concentrated poverty in urban America. University of Pennsylvania Law Review 143(5):1285–1342.
Schwartz, A. F. 2014. Housing policy in the United States. New York: Routledge.
Sommers, B. D., K. Baicker, and A. Epstein. 2012. Mortality and access to care among adults after state Medicaid expansions. New England Journal of Medicine 367:1025–1034.
Strully, K. W., D. H. Rehkopf, and Z. Xuan. 2010. Effects of prenatal poverty on infant health: State earned income tax credits and birth weight. American Sociological Review 75(4):534–562.
Tax Policy Center. 2014. State minimum wage rates, 1983–2014. http://www.taxpolicycenter.org/sites/default/files/legacy/taxfacts/content/PDF/state_min_wage.pdf (accessed November 2, 2016).
The City Project. 2014a. Best practice HUD Los Angeles state historic park healthy green land use for all. In The City Project Blog. Los Angeles, CA: The City Project. http://www.cityprojectca.org/blog/archives/32984 (accessed June 3, 2016).
The City Project. 2014b. San Gabriel mountains best practice environmental justice framework for parks, health, and conservation values. In The City Project Blog. Los Angeles, CA: The City Project. http://www.cityprojectca.org/blog/archives/32899 (accessed June 3, 2016).
The City Project. 2015. Environmental justice and civil rights frequently asked questions FTA best practices. In The City Project Blog. Los Angeles, CA: The City Project. http://www.cityprojectca.org/blog/archives/38688 (accessed June 3, 2016).
The City Project. 2016a. National Park Service rim of the valley final study best practice environmental justice. In The City Project Blog. Los Angeles, CA: The City Project. http://www.cityprojectca.org/blog/archives/41777 (accessed June 3, 2016).
The City Project. 2016b. U.S. Civil rights commission civil rights and environmental justice and enforcement by EPA. In The City Project Blog. Los Angeles, CA: The City Project. http://www.cityprojectca.org/blog/archives/43798 (accessed June 3, 2016).
The City Project. 2016c. US Army Corps of Engineers best practice for revitalizing L.A. River for all. In The City Project Blog. Los Angeles, CA: The City Project. http://www.cityprojectca.org/blog/archives/41580 (accessed June 3, 2016).
The City Project. 2016d. US EPA EJSCREEN park access and health disparities civil rights and environmental justice best practice. In The City Project Blog. Los Angeles, CA: The City Project. http://www.cityprojectca.org/blog/archives/43843 (accessed June 3, 2016).
The Pew Charitable Trusts. 2014. Judging for juvenile justice: 3 judges share lessons of juvenile justice reform: The Pew Charitable Trusts. http://www.pewtrusts.org/~/media/assets/2014/11/pspp_juvenilejudges_qa_brief_web.pdf (accessed October 24, 2016).
The Pew Charitable Trusts. 2016. 31 states reform criminal justice policies through justice reinvestment: Fact sheet. http://www.pewtrusts.org/en/research-and-analysis/fact-sheets/2016/01/31-states-reform-criminal-justice-policies-through-justice-reinvestment (accessed October 24, 2016).
U.S. Army Corps of Engineers, LA District, and Tetra Tech Inc. 2015. Los Angeles River ecosystem restoration integrated feasibility report: Final feasibility report and environmental impact statement/environment impact report: Volume 1: Integrated feasibility report: Los Angeles County, California. Los Angeles, California.
U.S. Census Bureau. 2015. Latest local health insurance statistics available through Census Bureau’s American Community Survey. Suitland, MD: U.S. Census Bureau.
USDA (U.S. Department of Agriculture). 2012. Environmental justice strategic plan: 2012–2014. Washington, DC: U.S. Department of Agriculture.
Van Der Wees, P., A. Zaslavsky, and J. Ayanian. 2013. Improvements in health status after Massachusetts health care reform. The Millbank Quarterly 91(4):663–689.
Waldron, H. 2007. Trends in mortality differentials and life expectancy for male social security-covered workers, by socieoeconomic status. Social Security Bulletin 67(3):1–28.
Wehby, G., D. Dave, and R. Kaestner. 2016. Effects of the minimum wage on infant health: Working paper no. 22373. Cambridge, MA: The National Bureau of Economic Research.
West, M. R. 2016. From evidence-based programs to an evidence-based system: Opportunities under the Every Student Succeeds Act. Washington, DC: The Brookings Institution.
Wherry, L. R., and S. Miller. 2016. Early coverage, access, utilization, and health effects associated with the Affordable Care Act Medicaid expansions: A quasi-experimental study. Annals of Internal Medicine 164(12):795–803.
Whittington, J. W., K. Nolan, N. Lewis, and T. Torres. 2015. Pursuing the triple aim: The first 7 years. Milbank Quarterly 93(2):263–300.
Wilson, S., M. Hutson, and M. Mujahid. 2008. How planning and zoning contribute to inequitable development, neighborhood health, and environmental injustice. Environmental Justice 1(4):211–216.
Woolf, S. H., R. E. Johnson, R. L. Phillips, and M. Philipsen. 2007. Giving everyone the health of the educated: An examination of whether social change would save more lives than medicine. American Journal of Public Health 2007(97):4.
Woolf, S. H., L. Aron, L. Dubay, S. M. Simon, E. Zimmerman, and K. X. Luk. 2015. How are income and wealth linked to health and longevity? Washington, DC: Urban Institute and Virginia Commonwealth University.
Wright, G. 2013. Sharing the prize: The economics of the civil rights revolution in the American south. Cambridge, MA: Belknap Press of Harvard University Press.
WXY and Hester Street Collaborative. 2016. East Harlem neighborhood plan. http://www.eastharlemplan.nyc/EHNP_FINAL_FINAL_LORES.pdf (accessed December 4, 2016).
Wyatt, R., M. Laderman, L. Botwinick, K. Mate, and J. Whittington. 2016. Achieving health equity: A guide for health care organizations. Cambridge, MA: Institute for Healthcare Improvement.
Wyly, E. K., and D. J. Hammel. 2004. Gentrification, segregation, and discrimination in the American urban system. Environment and Planning 36:1215–1241.
Yasaitis, L. C., W. Pajerowski, D. Polsky, and R. M. Werner. 2016. Physicians’ participation in ACOs is lower in places with vulnerable populations than in more affluent communities. Health Affairs 35(8):1382–1390.
Zuk, M., A. H. Bierbaum, K. Chapple, K. Gorska, A. Loukaitou-Sideris, P. Ong, and T. Thomas. 2015 (unpublished). Gentrification, displacement, and role of public investment: A literature review. Federal Reserve Bank of San Francisco.
This page intentionally left blank.
















































