
8
Community Tools to Promote Health Equity
TOOLS FOR COMMUNITY SUCCESS
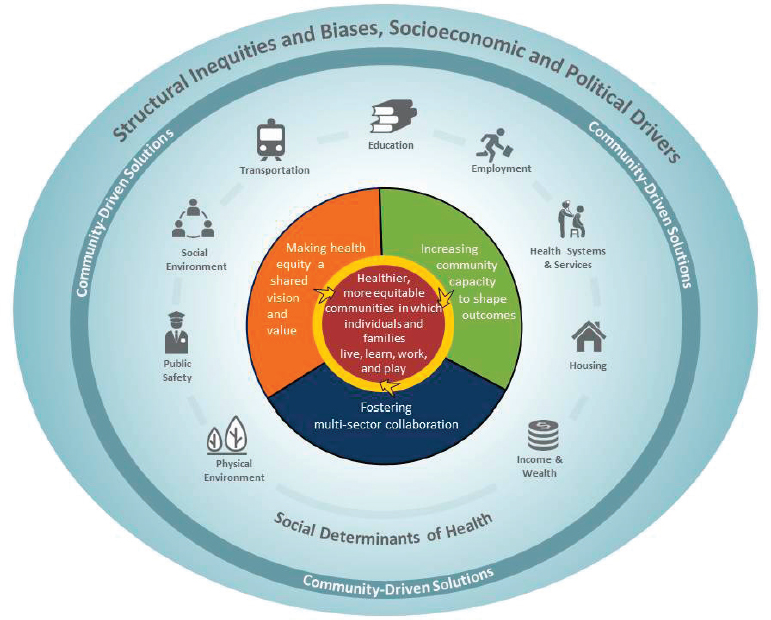
There are many tools available to communities to help them design, implement, and evaluate community-based solutions that advance health equity. These tools can be organized by the three elements identified in the committee’s conceptual model (see Figure 8-1): (1) creating a shared vision and value of health equity, (2) increasing community capacity to shape health outcomes, and (3) fostering multi-sector collaboration. The tools described here encompass approaches, methods, measures, and necessary infrastructure. The committee identified these tools based on the lessons learned from communities that have implemented solutions (see Chapter 5), a review of the literature, input from information-gathering meetings (see Appendix C for agendas), and committee expertise. This chapter first describes tools that support community-based solutions in a manner that applies across the three elements of this report’s conceptual model. Second, tools are organized according to the three elements in the report’s conceptual model. Third, widely available community toolboxes are summarized. Some of the tools shared in this chapter are explicitly designed to address social determinants of health, while others address the consequences of poor health outcomes, and some do both. The tools also vary in the time frame for implementation; some can be employed within a relatively short time, while others will take more time to plan and implement.
CROSSCUTTING TOOLS AND PROCESSES
A number of crosscutting tools provide a foundation for developing community-based solutions. Because each community is unique, the tools different communities need will vary. The tools described below are organized according to the types of actions that communities may need to take to address health equity, such as (1) making the case for health equity; (2) meeting information needs; (3) adopting or developing logic models or theories of change; (4) using civil rights law to promote health equity; (5) medical–legal partnerships; (6) using health impact assessments to understand policy implications; and (7) securing funding to support community action.
Making the Case for Health Equity
The Cost of Health Inequity
The cost of health inequity is usually calculated as a difference in cost, specifically, the excess burden that arises from certain groups
experiencing disparate levels of health. Health-related economic costs are higher among minority racial and ethnic groups than among whites both because they have more chronic conditions and because they have lower average education, which is correlated with poorer health and earlier death. By some calculations, the lower levels of self-reported health and higher levels of chronic disease among African Americans, Hispanics, and non-Hispanic whites relative to whites cost public and private insurers an estimated $24 billion in 2009 (Waidmann, 2009). But the costs are more widespread, affecting not just insurers but also families and employers (Dan et al., 2011; Gaskin et al., 2012). Combining the cost of lower health with the cost of lower productivity pushes the estimated 2009 economic burden to $82 billion (Gaskin et al., 2012). Factoring in early death raises the estimates even more. The economic burden for 2050, when the representation of minorities in the population will have increased substantially, is predicted to be more than twice as large as it is now (Gaskin et al., 2012; Waidmann, 2009).
Strategies for Investment
Recognizing that health inequities arise from many factors, decision makers face a challenge in weighing different strategies to improve health equity and health outcomes and decrease the cost of inequity. One model that informs health care cost reduction allows the user to simulate outcomes across geographic areas across a host of factors, such as changes to health care delivery, health care payment (e.g., global payments with reinvested savings), factors that influence healthier behaviors, some social determinants, and some socioeconomic factors. This approach, taken by the ReThink Health Dynamics Model, was used to simulate outcomes for typical midsize U.S. cities (Homer et al., 2016). In that work, a combination of approaches—expanding global payment, enabling healthier behaviors, and expanding socioeconomic opportunities—was estimated to lower health care costs by 14 percent and to improve productivity by 9 percent over 24 years. The most costly intervention component addressed socioeconomic opportunities, and the simulation assumed that the more costly investments occurred after savings from changes in health care delivery and payments. However, this was also the component that resulted in the greatest estimated improvements in the disadvantaged fraction of the population.
Participating in health equity improvement is a voluntary activity on the part of actors in the community. As such it is most likely to be maintained if there is a “business case,” meaning that benefits will accrue to the decision maker’s bottom line. What are the advantages of investments in improved health equity and raising awareness among
individuals, employers, and communities as a whole? While much of the health equity discussion rests on a moral argument, there are several economic arguments to support health equity promotion and improving the social determinants of health. One example of a social determinant of health for which there are large disparities among communities is education. By some estimates the annual economic value of better health from education is very high: if less educated populations improved their health and longevity to the level of college-educated Americans, the economic gain would be on the order of $1.02 trillion in 20061 (Schoeni et al., 2011).
Starting with education as an illustration, achieving health equity by reaching the poorest and most marginalized groups of people will require strong community ownership of the value and purpose of education, whether it be primary education, job training, or adult literacy. Disparities in education perpetuate disparities in income and health. What is the incentive—the business case—to improve education and training at individual, employer, and community levels? To individuals, education confers significant wage advantages; therefore, in theory, individuals have a strong incentive to pursue education (Blundell et al., 1999). Educational achievement is also shaped by ability; early childhood education; family background, including family income and parent education; and the local environment, including the quality of schools. The same amount of schooling could lead to very different skills, college experience, and earnings if one person goes to a much better school, with better teachers, instruction, and resources (Deming et al., 2014). Individuals can also achieve higher job earnings through employer training programs, but those most likely to receive additional training have greater skills and more education to begin with (Cappelli, 2004). This reinforcing nature of skills and education highlights how disparities can widen and create a “vicious circle” for those who do not have a strong start with initial qualifications.
Part of the reason a community’s commitment to education is important is that any one employer in the community is likely to invest in education, whether by supporting secondary education or general training. Using a standard model a typical firm’s calculus would be that education and training could improve worker productivity, making the firm more competitive and profitable (Becker, 1993). However, the more skilled workers could leave and work for a competing firm. Even if the firm were willing to pay a higher wage to retain the now higher-skilled worker, it would have “lost” its investment in training. In the real world, firms do
___________________
1 “[This estimate does] not capture the causal effects of education on health. Instead, [it estimates] the foregone benefıts if indeed the less-educated individuals experienced the same health and mortality as the college graduates” (Schoeni et al., 2011, p. S70).
support education and training, and this appears to be driven by contextual factors such as minimum wages, unionization, and employer competition in local areas (Acemoglu and Pischke, 1999; Autor, 2001). Firms also engage in particular or firm-specific training rather than general training. In contrast to general training, local employers may be more willing to invest in firm-specific training because the skills do not transfer to competitors as readily. Thus, the immediate business case for individual firms to act on behalf of general education and training in the community is somewhat narrow.
Mobilizing the Private Sector
While there is strong motivation at the individual level to pursue improvement, such as education, because of the prospect of higher incomes in the future, there is also a societal component at play. The spillover benefits of a more educated community accrue to everyone. Communities benefit from having an educated and literate population with greater civic engagement, lower crime, greater social cohesion, and economic growth. Firms can adapt their use of technology and equipment to the skills of a more educated, local work force, and more educated workers may exchange new ideas, furthering innovation. These spillover benefits mean that the community together, not just any one actor, should play an important role in supporting education. The challenge is that education benefits accrue over the long run and are thus investments that politically may be difficult to sustain. Private–public partnerships, such as Made in Durham, which works through a multi-sector collaborative to increase high school graduation rates and employment (NASEM, 2016; Stratton et al., 2012), have appeared to overcome some of the disincentives faced by any one actor operating in isolation.
Community momentum for changes in education, employment, or housing, whether through a school reform movement or a housing revitalization effort, may in part be understood as an attempt to mobilize the private sector on behalf of a public effort. The Aspen Institute describes such efforts as integrating social purposes with business methods (Sabeti, 2009). Such programs are often structured with public funding—for example, vouchers, grants, or tax credits—and private or shared public–private delivery of services and with public accountability structures. The impetus is often to introduce private-sector competition or innovation and to improve efficiency and performance. Frequently these mobilization efforts draw the attention of foundations, individual philanthropy, or private investors who provide additional resources and bolster further improvements. If these efforts around the social determinants of health
can lead to resources being more effectively and more equitably distributed, this could make inroads in health equity as well.
Other health drivers can be viewed through a similar lens. Often individuals have an incentive to improve their own situations, but this is shaped by local circumstances. Businesses have an interest in reducing the cost of health care; lowering the cost of employer-provided benefits, including workers compensation costs; lowering turnover; improving worker productivity; and reducing the number of sick days. A healthy workforce is less costly to employers. Yet, firms left to themselves may underinvest in health activities for workers. Thus, communities have a strong case for coming together and devising joint solutions.
Several investors have become involved in “social impact bonds,” also called “pay for success” programs (NASEM, 2016). Generally the programs are well-defined, are focused on “human capital” improvements over a 5- to 7-year span, and are limited in scope. For example, some such programs have addressed early childhood education, home visiting, prison avoidance, chronic homelessness, and foster care avoidance for children born to homeless mothers. They commonly involve private investors and foundations along with public payers. When early intervention programs yield desired outcomes—which means savings to the public down the line—the programs pay their investors from public or foundation funds. These solutions are appealing in part as a mechanism for community-building, for reinvigorating local dialogue on the social determinants of health, and for leveraging private institution participation and promoting transparency and efficiency. At the moment, however, because few such programs have run their course, there is relatively little empirical evidence concerning their effectiveness.
Another form of business-driven venture is the employment social enterprise. In this case, various entities, typically nonprofits, invest in disadvantaged groups, including those with low job skills and experience. They provide employment, training, and social services along with wages and experiential learning, working closely with local businesses (Maxwell et al., 2013; NASEM, 2016; Rotz et al., 2015). Social enterprises may also receive technical support and capital funding from entities such as REDF in California, which is itself grant-, foundation-, and donor-supported, as well as funding through tax credits. Social enterprises represent another form of public–private partnership and arise from a shared sense of purpose and common incentives.
Framing Outcomes and Success in Community Solutions
The major outcome of interest for community solutions is impact on health. Life expectancy can be a useful measure of impact on health because it is straightforward and easy to interpret, compare, and value.
However, it is less likely that community solutions will have data or measured impact on mortality indicators in the short term, as it takes considerable time to see changes in these long-term outcomes. In addition, the quantity of life is only one metric of health and does not capture quality, satisfaction, well-being, happiness, and opportunity. Instead, the committee sought out community-based solutions that target the social determinants of health with strong links to health outcomes as evidenced by the literature. However, community-level outcomes cannot be measured without community-level data. The section below outlines what is currently available to communities as well as the gaps in data and data tools.
Meeting Information Needs to Drive Community-Based Solutions
In 2011 the Institute of Medicine (IOM) Committee on Public Health Strategies to Improve Health highlighted the lack of accurate local data on the social, environmental, and behavioral determinants of health and recommended that the U.S. Department of Health and Human Services (HHS) support and implement: (1) a core, standardized set of indicators that can be used to assess the health of communities, including social determinants of health; (2) a core, standardized set of health outcome indicators for national, state, and local use; and (3) a summary measure of population health that can be used to estimate and track health-adjusted life expectancy (IOM, 2012). Since the publication of that report, there has been an increased emphasis on the use of common data elements (CDEs) in some parts of HHS, and a CDE resource portal is hosted by the National Library of Medicine (NIH, 2016). However, with a few exceptions (e.g., the National Health and Nutrition Evaluation Survey and the Patient Reported Outcomes Measurement Information System), CDE initiatives are disease-focused, and most are not linked to localities such as neighborhoods or census tracts. To address the issue of measurement heterogeneity, an IOM committee generated a framework, a core measure set, and an initial set of indicators (IOM, 2015b). Beyond addressing the challenges of what should be measured and how it should be measured, communities need data and interactive tools to easily access data as well as metrics that are specific to their situations and needs. Such data are critical to raising awareness to make health equity a shared vision and value, increasing a community’s capacity to design community-based solutions and shape outcomes, and fostering multi-sector collaboration and evaluation of solutions.
Data Sources
Increasingly, there are sources of electronic data that are publicly available and can be used to examine issues related to health and health
equity and to inform the development of community-based solutions. Some data sets are specific to health and others are from sectors relevant to health and health equity.
Thousands of data sets are accessible for public use through the U.S. government’s Health Data Initiative and the open data portal (HHS, n.d.-a). These include data sets from federal agencies, including U.S. Department of Health and Human Services agencies such as the U.S. Centers for Disease Control and Prevention (CDC), the Centers for Medicare & Medicaid Services, the Health Resources and Services Administration, the National Institutes of Health, and the U.S. Food and Drug Administration, as well as from states (e.g., Hawaii, Michigan, New York) and cities (e.g., Boston, Fort Collins). For instance, Boston’s open data portal includes data sets from many sectors that are relevant to health and health equity. These include hospital locations, healthy corner stores, farmers markets, community culinary and nutrition programs, crime incident reports, building code violations, and economic indicators (City of Boston Data Portal, 2013). Such data are sometimes organized into community dashboards that display key indicators. In Fort Collins, Colorado, for example, the dashboard includes quarterly summaries of factors that are related to a culture of health that advances health equity: neighborhood livability and social health, environment, transportation, economic health, environmental health, and safe community. The community dashboard for Travis County, Texas, presents data according to goals (CAN, 2016). For example, the municipality’s goal of “Being safe, just, and engaged” includes data related to crime, the proportions of jail bookings by race and ethnicity, and voting. The goal of “Realizing full potential” uses indicators related to kindergarten readiness, high school graduation, college success, and unemployment.
Some nongovernmental organizations also offer public access to various data sources relevant to community-based solutions that advance health equity. These include data sets from surveys such as the Robert Wood Johnson Foundation (RWJF) National Survey of Health Attitudes, which includes data on such values as health interdependence, sense of community, and social support; the University of Michigan’s Monitoring the Future series of youth surveys; and the Corporate Giving in Numbers survey. In other instances, data are available as files (e.g., the National Association of County and City Health Officials [NACCHO] National Profile of Local Health Departments) or reports (e.g., Best Complete Street Policies of 2015). Such resources (see Box 8-1) are currently more valuable for national-, state- or city-level assessments, as most of the data sets lack data at the neighborhood or community level. Moreover, many of these data sources are more suitable for use by researchers than by communities.
Indicators
For the purpose of this report, the committee uses the definition of indicator from the 2011 IOM report: a statistic or measure that is widely acknowledged to be useful for measuring something of concern to policy makers or the public (IOM, 2012). In the following section, indicators are summarized according to the components of the conceptual model for the report: (1) social determinants of health, (2) making health equity a shared vision and value, (3) increasing community capacity to shape outcomes, and (4) healthier, more equitable communities in which individuals and families live, learn, work, and play. The indicators selected for inclusion were based on a recent environmental scan on social-determinants-of-health indicators (Koo et al., 2016), an IOM report (IOM, 2012) that summarized national indicator sets for public health action, and a targeted literature search. The intent was to provide examples pertinent to community-based solutions rather than to provide an exhaustive summary. Further details of selected indicators by data set or index are provided in Appendix B.
Social determinants of health There are many data sources that contain indicators related to various social determinants of health. These include America’s Health Rankings, County Health Rankings, Community Health Status Indicators, and the National Equity Atlas. Indicators are most frequently available at the state or county level. Some cities have local equity atlases; Denver (Mile High Connects, 2016; Sadler et al., 2012) and Los Angeles (Reconnecting America, 2013) have noninteractive local equity atlases with a strong emphasis on transit. The Metro Atlanta Equity Analysis examines eight dimensions of community well-being (demographics, economic development, education, environment, health, housing, public safety, and transportation) through online tools.2 In some cases, such as the AARP Livability Index;3 the Brandeis University Diversity Data Kids dataset;4 the University of California, Davis, Regional Opportunity Index;5 and the Virginia Health Opportunity Index,6 data are available for smaller areas such as school districts or neighborhoods. Some indicators occur in the majority of the data sets reviewed. For example, high school
___________________
2 For more information, see http://atlantaequityatlas.com/about-maea (accessed December 19, 2016).
3 For more information, see https://livabilityindex.aarp.org (accessed December 19, 2016).
4 For more information, see http://www.diversitydatakids.org (accessed December 19, 2016).
5 For more information, see http://interact.regionalchange.ucdavis.edu/roi (accessed December 19, 2016).
6 For more information, see http://www.vdh.virginia.gov/health-equity/virginia-health-opportunity-index-hoi (accessed December 19, 2016).
graduation 4 years after starting 9th grade, health insurance, and air pollution are common indicators for education, health systems and services, and physical environment, respectively. There are also summarizing projects, such as Community Commons, that make these data available to a broader range of users (IP3, n.d.).
Making health equity a shared vision and value Although they were not conceptualized as explicit measures to demonstrate the extent to which health equity is a shared vision and value, some existing indicators are likely relevant. For instance, the Virginia Health Opportunity index includes a measure of segregation that includes community diversity and distances between communities with different racial or ethnic profiles. The JustSouth Index7 also includes a measure related to public school segregation along with measures of wage and employment equity. The National Equity Atlas8 characterizes diversity through the inclusion of a Diversity Index and a Culture of Health measure set that uses residential segregation.
None of these indicators explicitly measure attitudes or beliefs related to health equity, which are central to making health equity a shared vision and value. There is certainly the potential to construct indicators through standard techniques for survey development. However, attitudes and beliefs are sentiments or opinions that can be monitored through newer analytic techniques applied to social media. Sentiment analysis—the application of natural language processing, text mining, or computational linguistic tools to determine positive or negative effect—is widely used to assess opinions in written texts, including tweets. For example, it has been used to assess emotions associated with global warming and climate change (Lineman et al., 2015) and the moods of patients in online cancer communities (Rodrigues et al., 2016), and it has been used in the “Geography of Happiness” in combination with demographics and objective characteristics of place (Mitchell et al., 2013). Sentiment analysis tools are increasingly available as open sources or built into quantitative (e.g., R) or qualitative (e.g., NVivo) analysis programs.
In the short term, there will be a need to determine which existing indicators are most relevant for measuring and monitoring progress toward making health equity a shared vision and value. Moreover, new indicators are needed. The sentiment analysis of texts such as tweets and other social media communication represents a promising approach to capturing changes in popular opinions over time.
___________________
7 For more information, see http://www.loyno.edu/news/documents/just-south-index-2016.pdf (accessed December 19, 2016).
8 For more information, see http://nationalequityatlas.org (accessed December 19, 2016).
Increasing community capacity to shape outcomes As part of its culture of health agenda, RWJF developed measures organized by its action framework (Chandra et al., 2016). Four of those indicators relate to this report’s focus on increasing community capacity to shape outcomes: (1) a sense of community, (2) social support, (3) voter participation, and (4) volunteer engagement. The latter two are also present in several other data sources. Other aspects of community capacity building are leadership development, community organizing, organizational development, and fostering collaborative relations among organizations. These may be relevant areas for future measure development.
Fostering multi-sector collaboration RWJF’s culture of health metrics (Chandra et al., 2016) include nine indicators related to fostering multisector collaboration: local health department collaboration; opportunities to improve health for youth in schools; business support for workplace health promotion and culture of health; U.S. corporate giving; federal allocations for health investments related to nutrition and indoor and outdoor physical activity; community relations and policing; youth exposure to advertising for healthy and unhealthy food and beverage products; climate adaptation and mitigation; and health in all policies. In addition to the RWJF National Attitudes survey, the indicators reflect several novel data sources, including the Nielsen ratings for measuring youth exposure to advertising for health and unhealthy food and beverage products and community climate action plans for measuring climate adaptation and mitigation.
Healthier more equitable communities in which individuals and families live, learn, work, and play The measurement of progress toward “healthier more equitable communities in which members and families live, learn, work, and play” requires health indicators as well as equity indicators, including those related to the social determinants of health. National health indicator data sets contain a large variety of indicators for which health disparities exist (see Table B-1 in Appendix B for examples of indicators relevant to health equity in public data sources). These include indicators related to health behaviors (e.g., smoking, binge drinking), health status (e.g., poor mental health days, overall health status), morbidity (e.g., high blood pressure, diabetes), and mortality (e.g., premature death, addiction-related death). In addition, a report that RWJF commissioned from the Health Enhancement Research Organization proposed five indicators related to costs that could be used by collaborations wishing to engage nontraditional partners such as business entities: (1) annual end-of-life care expenditures, (2) family health care cost, (3) per capita expenditures on health care, (4) potentially preventable hospitalization
rates, and (5) social spending relative to health expenditure (May et al., 2016).
Interactive Tools
Although lists of indicators are useful in determining what to measure and how it should be measured, Web-based interactive tools make data sets more accessible to communities. Box 8-2 lists a collection of selected interactive tools, and their contents are summarized in Appendix B. Moreover, many of the interactive tools allow queries by geographic location, making it easy for communities to target their state, county, or neighborhood. In some instances, comparisons are made with other similar locations. For example, the CDC’s Community Health Status Indicators presents a target county’s data in comparison with “peer” counties and lists the indicators in three categories according to quartiles: better, moderate (middle two quartiles), and worse than the comparators (CDC, 2015). Other interactive tools display a composite index. The AARP Livability Index integrates multiple indicators in areas that are relevant to advancing health equity (housing, neighborhood, transportation, environment, health, engagement, and opportunity) to create an overall score (AARP Public Policy Institute, n.d.).
Some interactive tools are designed explicitly with health equity in mind. For example, the National Equity Access provides detailed demographic data as well as indicators in three key areas: economic vitality, readiness, and connectedness. In addition, it includes metrics related to the economic benefits of racial equity (gross domestic product gains with racial equity and income gains with racial equity) (PolicyLink and USC Program for Environmental and Regional Equity, 2016). Tools such as EJSCREEN (EPA, 2016) and the Food Access Research Atlas (U.S. Department of Agriculture Economic Research Service, 2016) focus on other important social determinants of health. While education level is found in many indexes, the Children’s Health and Education Mapping Tool explicitly links school population and resources, including school-based clinics, with health (School-Based Health Alliance, n.d.). The Diversity Data Kids interactive tool includes early childhood education and provides rankings and child opportunities by race and ethnicity for states, counties, large cities, and large school districts (Brandeis University, n.d.).
Another area of emphasis for interactive tools that is relevant to advancing health equity is opportunity indexes. Some indexes are at the state or county level. In contrast, the Virginia Health Opportunity Index has dashboards for counties, legislative districts, and health districts, thus providing a more local view of indicators to drive or evaluate community action (Virginia Department of Health, 2016).
The good news is there are many existing data sources, indicators, and interactive tools that can inform community-based solutions. Challenges include the facts that many communities may be unaware that such tools exist or may not be well positioned to use them effectively; that there is a need for indicators that can ascertain the extent to which health equity is a shared vision and value; that there is a persistent dearth of indicators and interactive tools based on neighborhood- or community-level data; and that although some interactive tools allow queries by racial or ethnic
group, gender, or age, they may not be informative for other groups for which health disparities exist, such as incarcerated, formerly incarcerated, and lesbian, gay, bisexual, and transgender (LGBT) populations.
Conclusion 8-1: Accessible and community-friendly interactive tools with data and metrics specific to individual communities are needed. Such data are critical to raising awareness to make health equity a shared vision and value, increasing community capacity to design community-based solutions and shape outcomes, and fostering multisector collaboration and the evaluation of solutions.
- In the short term there is a need to determine which existing indicators are most relevant for measuring and monitoring progress toward making health equity a shared vision and value, developing community capacity to shape outcomes, and encouraging multisector collaboration.
- Other aspects of community capacity building, including leadership development, community organizing, organizational development, and fostering collaborative relations among organizations are additional areas for potential indicator development.
Conclusion 8-2: There are many existing data sources, indicators, and interactive tools that are relevant to meeting the information needs that drive community-based solutions; however,
- Many communities may be unaware that such tools exist or lack some of the prerequisite skills for their effective use. Furthermore, these tools need to be made more user-friendly to facilitate use by community members.
- Many of the indicators and interactive tools provide data at the national, state, or county level. More tools are needed that provide interactive access to data at the neighborhood or community level.
Adopting or Developing Logic Models or Theories of Change
Engaging communities, developing community interventions, and developing projects addressing health equity all deal with very complex issues. To maximize the likelihood of success as well as of the potential for learning, those individuals, groups, and organizations pursuing such work must create and follow some sort of framework to guide strategies and activities. This framework might be as simple as project management, which involves identifying activities, specifying timelines, and measuring progress, or can involve more structured approaches such as logic models and theories of change.
Logic models are popular tools in the public health, nonprofit, and other fields. These models are frameworks that describe the different components of a program with the intent that the activities that make up a program are matched to the desired outcomes. Logic models graphically illustrate program components and usually include inputs, or what resources are used by the program; activities, or what the program does in terms of tasks, actions, etc.; outputs, or what the activities produce; outcomes, or the changes and benefits of the program in the short, medium, and long term; and impact, or the long-term intended change in organization, communities, or systems resulting from the program. These frameworks are outcomes-focused and assume causal links between activities and outcome. Using logic models helps stakeholders clearly identify a program’s components and intended results.
Another popular framework for complex interventions is the theory of change, which is specifically ideal for developing interventions to address complex social issues, such as health equity. In contrast to the logic model, which progresses from resources to outcomes, a theory of change starts by identifying a long-term goal and works backward to identify the preconditions that must be met in order to achieve the goal. Interventions to create the preconditions, as well as indicators of the performance of the interventions, are developed. Planners explicitly explain why the preconditions are necessary in order to achieved short-term objectives and why these are necessary to meet the long-term goal; in essence, the narrative concludes that the goal cannot be achieved unless the preconditions are met. Theories of change link outcomes and activities to explain how and why the desired change is expected to come about. Theories of change are dynamic and can be refined based on ongoing evaluation and strategic learning information; they provide guidance for stakeholders, support resource planning, and can help determine why an intervention worked—or did not. Done correctly, the process depends on the inclusion of different perspectives and participants in developing and implementing successful interventions. Additional details about specific approaches for change within organizations are provided later in this chapter. Box 8-3 highlights the development and application of theories of change in the community examples discussed in Chapter 5.
Using Civil Rights Law to Promote Health Equity
Civil rights laws can support community-based solutions to promote health equity and are an integral part of the culture of health in the United States. Chapter 6 contains a discussion on the broader context of using civil rights law to promote health equity, including background, the relationship to federal and state laws, and implementation of the
law—including many examples. As noted in Chapter 6, the Civil Rights Act of 1964 is an essential tool for addressing health disparities. (See below for a few civil rights law examples at the community level, and Box 8-4 provides an example from Baldwin Hills in Los Angeles County, California, of using the Clean Water Act for a civil rights, environmental justice, and health victory.) Civil rights laws offer tools that stakeholders working with public interest attorneys, public health professionals, community groups, government agencies, and recipients of federal, state, and local funds can use to promote health equity. As noted in Chapter 6, it is important to emphasize that these legal tools are not by any means limited to a litigation strategy. Voluntary compliance with civil rights laws can be preferable to litigation as a way of achieving equal justice goals. The civil rights movement uses many strategies to promote human dignity, equal justice, and just democracy and to overcome discrimination.9
___________________
9 DOJ Title VI Legal Manual at page II-3 (supporters of Title VI considered it an efficient alternative to ponderous, time-consuming, and uncertain litigation) (2016). Available at https://www.justice.gov/crt/fcs/T6manual (accessed July 15, 2016); Rodriguez et al. (2014).
Related Examples of Policies and Actions to Promote Health Equity
Agencies can also promote health equity through broad-based, more equitable community engagement. The National Park Service’s (NPS’s) Healthy Parks Healthy People U.S. program was established in 2011 to reframe the role of parks and public lands in terms of an emerging health and prevention strategy. The program seeks to work with national, state, and local parks as well as businesses, new health partners, funding resources, stakeholders, and advocacy organizations to foster and build upon the role that parks play in the health of our society (NPS, 2014). The NPS views civic engagement as an important part of its work and has created a number of tools, guides, and handbooks to promote engagement across diverse communities.10
___________________
10 See https://www.nps.gov/civic for tools such as Beyond Outreach Handbook: A Guide to Designing Effective Programs to Engage Diverse Communities; Learning to Make Choices for
Civil rights and health equity can also be promoted through programmatic priorities. For example, NPS recognizes that transportation is a significant barrier for many low-income communities and communities of color in reaching existing parks and open space. Many families do not have cars and do not live near efficient and reliable public transit that provides access to regional parks (NPS, 2015). Similarly, the NPS Every Kid in a Park provides every 4th grader in the nation and their families with a free pass to the national parks. NPS is providing transportation grants to schools with a high proportion of low-income students who qualify for free or reduced-price meals. In Los Angeles, 1 of 11 target cities in the nation, NPS and the U.S. Forest Service are working with the Los Angeles Unified School District, the second largest in the nation. Similarly, the Transit to Trails programs in the Los Angeles region provides transit and education materials for free, fun, healthy, and educational trips to mountains, beaches, rivers, and deserts (The City Project, n.d.-b).
Physical Education in Public Schools
A successful community-based effort to promote health equity through wellness and prevention is physical education in public schools. The IOM recommends monitoring physical education minutes, addressing disparities, improving teacher education, making physical education a core subject, and addressing physical activity in the whole school environment (IOM, 2013). Failure to provide physical education may adversely impact health outcomes as well as academic achievement. According to studies, physical education can have a neutral or positive effect on testing (Basch, 2011a; Diamant et al., 2011; HHS, 2002); cognitive function may be linked positively with physical activity among low-income and minority students in elementary and middle school (Efrat, 2011); physical education may be associated with reduced overweight or obesity, lower blood pressure, and improved bone health (Basch, 2011b); and physical education is an important component in the fight against obesity and other related chronic conditions (Diamant et al., 2011; Springer et al., 2009) The Los Angeles County Department of Public Health publishes a physical education model action plan (MAP) and a tool kit to support community action for compliance with physical education and civil rights requirements in public schools (LA County Department of Public Health, 2015). The Los Angeles Unified School District adopted a plan to comply with physical education and civil rights requirements in 2008 (Lafleur et al., 2013).
___________________
the Future: Strategies for National Parks and Other Special Places; and Leading in a Collaborative Environment: Six Case Studies Involving Collaboration and Civic Engagement.
A 2016 University of Southern California study analyzed physical education and physical fitness in almost 900 California public school districts. According to the report, there are significant racial and ethnic, economic, and achievement indicators that affect student fitness across all districts. The California Education Code mandates that all public schools both provide physical education for students and assess students’ physical fitness annually through the Fitnessgram standardized test. Yet many schools fail to meet physical education requirements, and less than half of all assessed students demonstrate full physical health. The major findings of the study include
- Fitnessgram passing rates differed significantly based on race and ethnicity.
- Non-Hispanic white students had the highest average passing rate, at 34 percent, followed by Asian students, at 31 percent. Students identifying as “Other” had an average passing rate of 29 percent. Hispanic students had a Fitnessgram passing rate of 26 percent. African American students had the lowest passing rate at 22 percent. Additionally, African American students had the highest percentage of poor scores, with nearly 400 districts reporting an overall passing rate of 10 percent or less among this racial group.
- School districts with more low-income students (eligible for free or reduced-price meals) tended to have lower Fitnessgram passing rates.
- Districts with higher API (academic performance index) scores tended to have higher Fitnessgram passing rates (Green et al., 2015).
According to the California Courts of Appeal, the state Education Code requires an average of 20 minutes of physical education per day in elementary schools, and parents and students have the right to sue a school district for not complying with that law. Half the public school districts audited in California from 2005 to 2009 did not comply with the minute requirements (Lafleur et al., 2013). According to a 2013 study, 83 percent of elementary schools in San Francisco reported that they met the minute requirements, but when the schools were monitored on-site only 5 percent met the requirements (Thompson, 2013). Districts that did not comply had a higher percentage of African American and Latino students than districts that did, according to a separate study (Rodriguez et al., 2014; Sanchez-Vaznaugh et al., 2012).
The shared use of parks, schools, and pools can help address the lack of places for healthy active living in underserved communities. In recent
years the Los Angeles Unified School District has raised $27 billion for new school construction and modernization. The school district has built more than 130 new schools, modernized hundreds more, cleaned up acres of polluted brownfields, and made the future brighter for generations of students (The City Project, n.d.-a).
Schools and parks can combine education materials on ethnic studies on places and people with studies of STEM (science, technology, engineering, and mathematics) subjects to make health and environmental quality and justice personal to students. According to a recent study from Stanford University, ethnic studies programs improve grade point averages across all subjects, increase school attendance, and increase courses taken (Dee and Penner, 2016).
There are national and community resources available for communities seeking help with civil rights issues. Community organizations are discussed throughout this report. National resources include the NAACP Legal Defense & Educational Fund, Inc., which works on racial and ethnic justice (NAACP LDF, n.d.). The American Bar Association lists many pro bono programs (ABA, 2009). The University of California, Los Angeles (UCLA), Civil Rights Project website houses many resources, including community tools for education, transportation, and housing (UCLA, 2016). The Human Rights Campaign is the largest civil rights organization with the goal of achieving LGBT equality (Human Rights Campaign, 2016). NOW, the National Organization for Women, is dedicated to women’s rights (NOW, 2016).
Medical–Legal Partnerships
In contrast to civil legal aid organizations that provide assistance to community members on issues that affect health through a justice-driven framework, medical–legal partnerships operate through a public health framework that includes the social determinants of health and values population outcomes as well as individual outcomes. Formally established in the early 1990s, medical–legal partnership is defined as “an approach to health that integrates the expertise of health care, public health and legal professionals, and staff to address and prevent health-harming social and legal needs for patients, clinics, and populations. By partnering together, health care, public health, and legal institutions transform the health care system’s response to social determinants of health” (National Center for Medical–Legal Partnership, 2014b, p. 2). The National Center for Medical–Legal Partnership reports the participants in U.S. medical–legal partnerships to be 155 hospitals, 139 health centers, 34 health schools, 52 law schools, 126 legal aid agencies, and 64 pro bono partners (National Center for Medical–Legal Partnership, 2016). The legal
care provided by medical–legal partnerships focuses on social, financial, or environmental problems that have a deleterious impact on a person’s health and can be addressed through civil legal aid. It is distinctive from that of civil legal aid organizations in five key ways (National Center for Medical–Legal Partnership, 2014b).
First, medical–legal partnerships train health care team members and often health professional students to recognize health-harming civil legal needs. The training can take the form of specialized training for medical champions (Pettignano et al., 2014), social workers (University of Colorado Law School, n.d.), family specialists (Sege et al., 2015), or broader training for a group of physicians and nurse practitioners in a particular clinical setting (Taylor et al., 2015). Sometimes, the medical–partnership includes a law school as well as community-based legal aid services, thus affording the opportunity for collaborative interprofessional training of law, medical, nursing, social work, and other types of students. For example, through a service learning project, law and medical students at Florida International University partnered with community members and Florida Legal Services to collect patient narratives, disseminate information on Medicaid expansion to community members, and present patient stories to state lawmakers (Martinez et al., 2016).
Second, medical–legal partnerships support screening patients for health-harming civil legal needs. Increasingly, this is done through formal checklists that screen for the breadth of civil legal needs rather than a single high-priority need (Pettignano et al., 2013; Taylor et al., 2015). In some instances, computer-based clinical decision support has been used to screen for health-harming legal and social needs as well as to improve the delivery of appropriate physician counseling and to streamline access to legal and social service professionals when nonmedical remedies are required (Gilbert and Downs, 2015).
Third, legal professionals and others with specialized training provide triage, consultation, and legal representation services for patients—most typically on-site. The Atlanta-based Health Law Partnership, comprised of three community partners—Children’s Healthcare of Atlanta, the Atlanta Legal Aid Society, and the Georgia State University College of Law—has attorneys in hospitals and clinics, and weekly interprofessional case conferences support triage of potential cases into those that require legal representation versus other types of services (Pettignano et al., 2014). Through the Colorado Health Equity Project, case management teams (physician, attorney, and social worker or behavior health specialist) provide on-site services to the Salud Family Health Center in Commerce City and the Colorado Center for Refugee Health (University of Colorado Law School, n.d.).
Fourth, changes to clinical or health care institution policy are made jointly by health care or legal professionals or both to treat and prevent health-harming legal needs. The Medical–Legal Partnership at Legal Aid of Western Missouri reported on the role of advocacy in occasioning community and organizational change in a medical–legal partnership (National Center for Medical–Legal Partnership, 2014a). Partners included a pediatric hospital, a federally qualified health center (FQHC), and a nonprofit social service organization focused on youth living in poverty. During a 3-year period, 158 advocacy efforts targeted 11 community sectors (e.g., civic groups, government, housing, education), resulting in multiple changes, including a community advisory board at the pediatric hospital and the establishment of a medical–legal partnership at a federally funded health care organization.
Fifth, health care or legal professionals or both jointly advance changes to local, state, and federal policies and regulations to improve population health. For example, to decrease injuries in motor vehicle accidents for children after they are too big for baby car seats, the Atlanta-based Health Law Partnership11 drafted state legislation to mandate that booster seats be used with seat belts for children under 8 years old. The key partners were Georgia State University students in a health legislation and advocacy course, who identified and researched the problem, assessed political will, and drafted the legislation, and government affairs staff of Children’s Healthcare of Atlanta, who found sponsors. The bill was subsequently signed into law.
Given the vulnerability of children, especially those with chronic diseases and who live in environments with inadequate heat, cooling, and light, children’s health has been a particularly fertile area for the implementation of medical–legal partnerships. Consequently, a number of medical–legal partnerships have targeted energy insecurity and demonstrated positive effects in preventing utility shut-offs. For example, the PhilaKids medical–legal partnership implemented a multifaceted intervention that included the training of health care staff, the implementation of a needs screener, and the development of consensus criteria for certification of medical need approvals for stable utilities (Taylor et al., 2015). During a 1-year period, this process increased the certification of medical need approvals by 65 percent, preventing utility shut-offs for 396 families with vulnerable children. Another study focused on children with asthma in Atlanta and demonstrated both financial and nonfinancial outcomes. Over 7 years, half of the nonfinancial outcomes achieved were in the area of housing (e.g., protection from foreclosure, improved housing,
___________________
11 For more information, see https://healthlawpartnership.org (accessed December 20, 2016).
and obtained or retained housing) and utilities (Pettignano et al., 2013). Recently, some authors have advocated for better integration of palliative medicine and medical–legal partnerships to address issues across the life course (Hallarman et al., 2014).
Medical–legal partnerships are growing and are currently present in all 50 states and the District of Columbia (National Center for Medical–Legal Partnership, 2016). Evidence, including the examples provided here, suggest that medical–legal partnerships play an important role in addressing the social determinants of health and are a relevant community-based solution for advancing health equity.
Using Health Impact Assessments to Understand Policy Implications
Health impact assessment (HIA) is a tool for analyzing the health effects of proposed programs, policies, and projects. The assessment process uses data and input from local stakeholders to understand the often overlooked benefits and consequences of a given proposal. HIA relies on the premise that most policy and programs will inevitably affect population health in some way and that it is better to understand those outcomes before final decisions are made. Recommendations to change a proposal based on HIA results can help improve health outcomes. To date, public health practitioners have conducted HIAs in a variety of policy areas—including, but not limited to, transportation, housing, land use, criminal justice, and development (NACCHO, 2016; The Pew Charitable Trusts, 2016).
Since the early 2000s when HIA was first used, the practice has become increasingly prominent as a method to apply a health context to policy decisions. At a 2002 meeting hosted by the CDC focused on the built environment’s effect on health, workshop participants identified HIA as a promising approach (Kemm, 2013). To date, more than 240 HIAs have been conducted within the United States, and there is movement to make the practice more widespread (Ross et al., 2014). The White House Task Force on Childhood Obesity, Health and Human Services’s Healthy People 2020 Policy, and the CDC’s Transportation and Healthy Policy all advocate for the use of HIA (Kemm, 2013).
HIA remains an optional tool for policy analysis, unlike environmental impact assessments, which can be required on federally funded or licensed projects (Ross et al., 2014). The Massachusetts legislature emerged as one of the few bodies mandating HIAs when it passed the Healthy Transportation Compact in 2009, which requires state agencies to “institute a health impact assessment for use by planners, transportation
administrators, public health administrators, and developers.”12 Due to HIA’s noncompulsory status, regulations guiding the practice do not exist. Practitioners are awarded much flexibility, and the resultant reports vary in content, methodology, messaging, and audience.
In 2007, a group of business and community leaders from North Omaha, Nebraska, formed a coalition to return the neighborhood to its former glory (CDC, 2013). The plan included improving Adams Park, a 68-acre green space next to the Malcolm X birthplace. The Douglas County Health Department led the HIA with its partners, the African American Empowerment Network and the North Omaha Neighborhood Alliance. They collected and analyzed data on health, demographics, food access, crime, traffic crashes, and land use; interviewed experts; and reviewed scientific research to understand how changes in Adams Park could impact health. The HIA showed that the Adams Park plan could greatly improve health in North Omaha in multiple ways: (1) provide greater access to affordable fruits and vegetables; (2) create space for social interaction and exercise; (3) increase physical activity levels; and (4) raise property values and reduce crime within a quarter-mile span. See Box 8-5 for an example of a community-driven health impact assessment of a rezoning proposal.
To make conducting an HIA more accessible and to increase the number of practitioners, members of the HIA community have begun to publish guidelines. A methodology that includes six main stages—screening, scoping, recommendations, assessment, reporting, and monitoring and evaluation—is often considered common practice and a useful way for approaching the HIA process. Recently, 12 equity metrics related to four HIA outcomes have been proposed (Heller et al., 2014):
- The HIA process and product focused on equity: (1) the proposal analyzed in the HIA was identified by or relevant to communities facing inequities; (2) the HIA scope—including goals, research questions, and methods—clearly addresses equity; (3) the distribution of health and equity impacts across the population was analyzed (e.g., existing conditions, impacts on specific populations predicted to address inequities; the HIA utilized community knowledge and experience as evidence); (4) the recommendations focus on impacts to communities facing inequities and are responsive to community concerns; (5) the findings and recommendations are disseminated in and by communities facing inequities using a range of culturally and linguistically appropriate media
___________________
12 The 189th General Court of the Commonwealth of Massachusetts. 2009. Chapter 25. An Act Modernizing the Transportation Systems of the Commonwealth.
- The HIA process built the capacity and ability of communities facing health inequities to engage in future HIA and in decision making more generally: (1) communities facing inequities lead or are meaningfully involved in each step of the HIA; and (2) as a result of the HIA, communities facing inequities have increased knowledge and awareness of decision-making processes and have attained greater capacity to influence decision-making processes, including the ability to plan, organize, fundraise, and take action within the decision-making context.
and other platforms; and (6) the monitoring and evaluation plan included clear goals to monitor equity impacts over time and an accountability mechanism (i.e., accountability triggers, actions, and responsible parties) to address adverse impacts that may arise.
- The HIA resulted in a shift in power benefiting communities facing inequities: (1) communities that face inequities have increased influence over decisions, policies, partnerships, institutions, and systems that affect their lives; and (2) government and institutions are more transparent, inclusive, responsive, and collaborative.
- The HIA contributed to changes that reduced health inequities and inequities in the social and environmental determinants of health: (1) the HIA influenced the societal and environmental determinants of health within the community and a decreased differential in these determinants between communities facing inequities and other communities; and (2) the HIA influenced physical, mental, and social health issues within the community and a decreased differential in these outcomes between communities facing inequities and other communities.
Funding Mechanisms for Communities
Regardless of the intended impact and the process of development and implementation of any community intervention to promote health equity, a key element is identifying the necessary fiscal resources for the project or program. Funding for community interventions can be described in terms of sources and mechanisms or strategies. Potential sources include federal, state, and local governmental agencies; business and other private-sector sources; and foundations or individual (or group) philanthropy. Mechanisms and strategies include grants, endowments and trusts, braided funding, leveraging or shared funding, investments (including social impact bonds and program-related investments or other low-interest loan programs or sub-market investments), and public–private partnerships. Community collaboratives working on health equity benefit from knowing the potential sources of funding and from using different strategies to diversify their revenue mix in order to bring more resources to bear and to increase the likelihood of success and sustainability.
Government funding sources are particularly attractive because, in general, they tend to be available for longer durations and can be quite substantial and even entirely sufficient for the development, implementation, and long-term sustainability of a program. Agencies have a broad set of potential funding mechanisms: including direct program or project funding, such as Medicaid and the U.S. Department of Housing and Urban Development (HUD) project grants; specific grant programs, such as community development block grants; low or below-market interest loan programs, such as the Federal Student Aid program; credit assistance, such as that provided by the Transportation Infrastructure Finance and Innovation Act; use fees, such as tolls; directly allocated taxes, such as the federal gasoline tax; and subsidies, such as HUD tenant and project-based assistance programs and public housing operating subsidies. Agencies can also pursue public–private partnerships where community services are financed by the government and provided by private agencies.
Many of the examples in Chapter 5 illustrate government as a source of funding for their initiatives. Both the Dudley Street Neighborhood Initiative and the Eastside Promise Neighborhood received Promise Neighborhood funding from the U.S. Department of Education through planning and implementation grants. In addition, Dudley Neighbors, Inc., as a certified state community development corporation, secured $100,000 in community tax investment credits. As an FQHC, Delta Health Center receives funding from the Health Resources and Services Administration Health Center Program through the Health Center Program Statute of the Public Health Service Act. Mandela MarketPlace has received essential funding support from the U.S. Department of Agriculture, specifically
from its Agricultural Marketing Service agency, the Food Insecurity Nutrition Incentive program, the Risk Management Agency, and the Healthy Food Financing Initiative.13 The Sustainable Neighborhoods Program of People United for Sustainable Housing (PUSH) was awarded a state grant to develop affordable housing units. In one example of city-level funding, during the first year of the Blueprint for Action, the city budget adopted by the Minneapolis mayor included $175,000 to support implementation.
The private sector is another potential funding source. Traditional mechanisms include corporate philanthropy, either voluntary or in response to regulated community benefit spending in support of a business’s nonprofit status, such as that required of nonprofit hospitals under the ACA. In order to sustain its work, the Indianapolis Congregation Action Network (IndyCAN) raises funds from corporations as well as others. The Dudley Street Neighborhood Initiative’s membership includes local businesses. Among Mandela MarketPlace’s partners is Mercury LLC, an advertising and marketing firm. A new and innovative mechanism is the social impact bond, with which private-sector investments pay for improved social outcomes that result in private-sector savings; these bonds are repaid contingent on attaining certain social outcomes. An example is the Denver Permanent Supportive Housing Social Impact Bond Initiative, which would decrease the cost associated with acute services for heavy-utilizing homeless persons by providing housing and on-site support services.
Philanthropy, often called the “third sector,” is another important source of funding for community interventions. Foundations have an advantage in terms of having greater flexibility to be more innovative and take greater risks than government agencies. Depending on the foundation, funding can be quite flexible, including providing “general operating support” which gives the grantee decision making concerning how best to bring resources to bear in addressing an issue. Foundation funding also presents challenges: compared to government sources, the total amount of dollars available is less. Projects much be aligned with the unique mission and vision of the foundation. Foundations are unlikely to be a source of sustainable funding over time, as foundation boards tend to be interested in moving on to new, innovative projects that promote their mission. And, despite the ability to be flexible and innovative, foundations can be as risk-averse and as proscriptive as any public agency—sometimes even more so. There are many types of foundations, with different sources of funding and different regulatory requirements, including
___________________
13 The Healthy Food Financing Initiative is operated jointly by the U.S. Department of Agriculture, the U.S. Department of Health and Human Services, and the U.S. Department of the Treasury.
private foundations, family foundations, community foundations, and corporate foundations, and each has myriad approaches to grant making. A relatively new foundation mechanism that has been used to support community health equity interventions is program-related investment, whereby a foundation makes a below-market loan or investment, such as in an affordable housing project, and any return on investment becomes a source for future grant making.
Foundations have been a prominent source of funding for the community examples in Chapter 5. For example, the Dudley Street Neighborhood Initiative was founded with assistance from the Boston-based Mabel Louise Riley Foundation. The Delta Health Care’s state and federal funding has been supplemented by the W.K. Kellogg Foundation. WE ACT’s development of the Northern Manhattan Climate Action Plan was supported through a $100,000 grant from The Kresge Foundation. The Magnolia Community Initiative recently received a $2 million collaborative gift from the Doris Duke Charitable Foundation and the Tikun Olam Foundation. Thunder Valley Community Development Corporation has secured funding from multiple foundations, including the Northwest Area Foundation, Doris Duke Charitable Foundation, Surdna Foundation, Novo Foundation, and W.K. Kellogg Foundation.
Community collaborations that are developing funding for a program or project will benefit from being aware of all potential funding sources. An affordable housing project might rely on more than half a dozen different sources, including private sources (such as traditional loans), government sources (such as community development funds), and philanthropic loans from foundations and individuals. All of the community examples in Chapter 5 relied on a diversity of funding sources to develop, implement, and maintain their activities. In many instances there was substantial governmental as well as philanthropic funding. There are financing strategies available to community organizations themselves, such as school districts and local public health agencies, as well as “braided” or “blended” funding, which refers to pooling funding from separate funding streams, usually created with different priorities but with enough flexibility and overlap to permit supporting a single intervention (Clary and Riley, 2016). A common strategy in attracting philanthropic funding is “leveraging,” whereby the investment from one foundation is used to attract additional grants from others. This also has the advantage of creating additional stakeholders and may translate to better chances of program sustainability as the ongoing costs are shared among a group of interested organizations.
In summary, an awareness of potential sources and creativity in financing are important in developing the resources required for community interventions. While sustainability is most often the intent of projects
and programs, communities should also be aware of the value of other enduring products that can come from interventions. Policy changes, for example, can endure and affect the health of a community for a long time. Leadership and collaborative relationships endure and can be repurposed to address new community issues. New knowledge of what works and what does not work is a key enduring product from any intervention. And, of course, the direct benefit to individuals affected by the intervention can be lifelong.
The following sections discuss the tools available to communities based on the three elements in the committee’s conceptual model: (1) making health equity a shared vision and value, (2) building community capacity to act, and (3) fostering multi-sector collaboration. The chapter then ends with examples of community tool kits that are readily available to communities and incorporate many of the tools outlined in this chapter.
MAKING HEALTH EQUITY A SHARED VISION AND VALUE
General Principles
Multiple approaches to making health equity a shared vision and value through community-based solutions share three characteristics:
- A shared sense of urgency about the issue to be addressed, and the need for a community-based solution (Hanleybrown et al., 2012).
- Clearly stated shared purpose and values. This may include a commitment to collective impact, which is described later in this chapter (Public Health Agency of Canada, 2016).
- A champion. An effective champion is trusted, respected, nonpartisan, and works effectively with political leaders; is strongly committed to the determinants of health philosophy; and welcomes, encourages, and successfully brokers multiple and varying perspectives to shape a health equity agenda (Public Health Agency of Canada, 2016).
A shared vision, aligned with a clearly stated purpose and values and fueled by a sense of urgency, is highlighted in the community examples in Chapter 5. Community-level data regarding the social determinants of health were essential in establishing a sense of purpose to facilitate a shared vision among all partners. In some instances, the shared vision targeted youth and families. For example, a shared vision of improved outcomes among children and families binds the Magnolia Community Initiative network of more than 70 government and private-sector partner
organizations. Driven by public safety concerns, Blueprint for Action was motivated by a shared vision of a unified city in which all youth are safe and able to thrive (Blueprint for Action, 2013). The Dudley Street Neighborhood Initiative has cultivated a shared vision among residents, families, local organizations, and local businesses regarding their power to achieve a healthier and more vibrant community. IndyCAN’s main platform, Opportunity for All, is based on a shared vision that every person should have equal opportunity to access the conditions and resources to achieve racial and economic equity. WE ACT has nurtured a shared vision of improved health in northern Manhattan through its environmental justice and climate activities.
The role of a champion or a group of champions is illustrated throughout the community examples. A prominent example of an individual champion was Jack Geiger’s role at both the policy level, to advocate to the Office of Equal Opportunity for the concept of neighborhood health centers, and later as project director of the Delta Health Center, the first FQHC. In contrast, the leaders who convened to develop the Blueprint for Action represented multiple champions from law enforcement, juvenile supervision, public health, youth programs, education, social services, faith communities, neighborhoods, and city and county government.
Public Will Building
Public will building differs in a number of ways from other approaches to making health equity a shared vision and value in that it is an explicit communication approach that “builds public support for social change by integrating grassroots outreach methods with traditional mass media tools in a process that connects an issue to the existing, closely held values of individuals and groups” (Metropolitan Group, 2009). In contrast to public opinion-based campaigns, which often target a short-term goal, public will-based approaches focus on long-term change building over time using four principles: (1) connecting through closely held core values rather than trying to change values; (2) respecting cultural context, including the dynamics of power, language, relationships, values, traditions, worldview, and decision making; (3) including target audiences in development and testing of key strategies and methods to ensure authenticity, clarity of message, and credibility of messengers; and (4) integrating grassroots and traditional communication methods. While not explicitly reflected in the Chapter 5 community examples, public will-based approaches have been applied to multiple topics, including the arts, behaviors that influence the outcomes of children and families (Leiderman et al., 2000), and out-of-school programs (Padgette et al., 2010). An example of the last topic is summarized in Box 8-6.
INCREASING COMMUNITY CAPACITY TO SHAPE HEALTH OUTCOMES
Successful and sustainable community interventions require the engagement of individuals and leaders from multiple sectors, not the least of which are the affected individuals in the community and the organizations that are perhaps closest to the affected population. In many instances, these individuals and grassroots organizations have less power, experience, and capacity to represent the unique goals and needs of the population that health equity interventions are meant to address. Community capacity refers to the ability of community members to make a difference over time and across different issues (Work Group for Community Health and Development, 2016b).
Capacity building enables an organization to be more effective in pursuing its mission, vision, and goals; to be sustainable; and to grow as needs require. Skill building includes such areas as basic business planning and practices, communication tools and strategies, strategic
planning, grant writing, and fundraising. Capacity building is a key element of sustainability. Strengthening community capacity to develop, implement, and sustain successful interventions depends on specific strategies, which include leadership development, community organizing, supporting the relationships between organizations necessary for collaboration, and organizational development (Chaskin, 1999).
Capacity Building for Leadership Development
Capacity building in regards to leadership development at the individual level includes building the skill sets that committed participants need to take a key role in representing the interests of their community and enhancing their effectiveness in helping shape intervention elements that respond to the specific community member needs. Leadership development, which usually includes specific skill building around communication and presentation skills as well as specific knowledge transfer and often project development, also creates lasting change for those individuals who engage in training.
Leadership development has different components within organizations. ISAIAH, located in Minneapolis, is a vehicle for congregations, clergy, and people of faith to act collectively and powerfully toward racial and economic equity in the state of Minnesota. ISAIAH’s mechanisms of change include three components (IOM, 2015a). The first component is grassroots leadership development. The second component builds upon the first: democratic, accountable, sustainable, and community-driven organizations, whose participants are “exercising democracy with each other” (IOM, 2014). The third component of community organizing emphasizes that the power or the ability to act drives change. In an IOM workshop, ISAIAH’s executive director Doran Schrantz explained, “Differentials in power do not change because somebody else who has more power gives it to you. Differentials in power change because you take ownership and collective and community responsibility for negotiating for the power and the resources you need. When that power structure is in place, that is when change happens” (IOM, 2014, p. 50).
Leadership development is an essential strategy emphasized in the community examples in Chapter 5. The Dudley Street Neighborhood Initiative offers internship programs to develop leadership capacity and provide career opportunities for talented youth in order to create the next generation of community leaders. Mandela Foods Cooperative, a venture of Mandela MarketPlace, has supported youth leadership development through the West Oakland Youth Standing Empowered program and also enabled employee leadership development through pathways from employment to ownership. WE ACT offers an 11-week environmental
health and justice leadership training program to educate community members about the environmental health issues confronting their northern Manhattan neighborhoods. WE ACT recently adapted its leadership training model for high school students in collaboration with academic partners and offers the Climate Change and Health Fellows program aimed at fostering climate literacy. Another example is Magnolia Community Initiative’s Belong Campaign,14 which is building social connections and creating leaders (“neighborhood ambassadors”) who can help connect residents to the resources available in the community. Box 8-7 outlines a multistep leadership development plan.
___________________
14 For more information, see https://www.youtube.com/watch?v=CUEtCD_I9iU (accessed October 21, 2016).
Capacity Building for Community Organizing
Community organizing through local outreach brings together individuals with shared interests and gives voice and power to individuals who traditionally are excluded and marginalized. Organizing can use grassroots approaches, often recruiting through one-on-one outreach interactions; faith- or congregation-based organizing, which works more at building networks of groups and institutions; and broad-based organizing, which may include secular, faith-based, or individual groups. Community organizing gives planners access to specific insights into what interventions are critical (and which are not) and increases the power and voice of community members in decision-making settings.
Community organizing may take different forms. In a seminal publication, Rothman characterized three models of practice: social planning, social action, and locality development (Rothman, 1996). Importantly for sustainability, the relationships created by community organizing often last longer than the lifespan of a program or project.
Social planning uses information and analysis to address substantive community issues and helps build agreement on common results. HIAs are one approach to social planning. Another strategy is the use of the variety of data sources described earlier in this chapter to characterize a particular issue.
Social action involves efforts to increase the power and resources of low-income, relatively powerless, or marginalized people. This may include the use of political action or disruptive events such as lawsuits, sit-ins, or boycotts to draw attention and focus to their concerns from those in power. IndyCAN’s Ticket to Opportunity field program mobilizes marginalized voters of color through large-scale voter engagement to build sustained capacity for transit equity. Community residents are also taught to use the tools of democracy to improve their communities.
Locality development is the process of reaching group consensus about common concerns and collaborating in problem solving. Promise Neighborhoods are an example of community organizing with an emphasis on locality development. The Dudley Street Neighborhood Initiative and Eastside Promise Neighborhood have received Promise Neighborhood funding, and their activities, which are described in Chapter 5, are exemplars of locality development. Another example of locality development is the Northside Achievement Zone (NAZ), which strives to permanently close the achievement gap and end generational poverty in North Minneapolis, a neighborhood with approximately 5,500 children with major educational achievement gaps at baseline. Only 29 percent of entering kindergartners living in North Minneapolis are ready to learn, 37 percent of African American youth graduate on time from Minneapolis Public Schools, 16 percent of African American youth graduate ready for
college, and 13 percent of those who attend a public university graduate in four years (Northside Achievement Zone, n.d.). This low achievement occurs in the context of other important social determinants of health: 73 percent of NAZ families earn $19,000 or less per year, single-parent families represent 51 percent of NAZ households, 25 percent of North Minneapolis students are homeless or highly mobile, and this small area is responsible for the majority of violent crime in Minneapolis. Consequently, the program’s community-based solutions are multi-sectoral and not solely focused on education:
- Education: early childhood, K–12, expanded learning, and mentoring
- Economic development: Emerge Community Development, Twin Cities RISE!
- Housing: Minneapolis Public Housing Authority, Project for Pride in Living, Urban Homeworks
- Health care: Visiting Nurse Agency, The Family Partnership, Northpoint Health & Wellness Center, Washburn Center for Children
In reality, community organizing often integrates aspects of multiple models, as reflected in several of the community examples in Chapter 5 (e.g., the Magnolia Community Initiative) and by Aim4Peace. Based in Kansas City, Missouri, Aim4Peace focuses on the neighborhood factors that most often contribute to violence, helping those who are considered at highest risk of committing offenses due to their living or employment situation. Aim4Peace includes locality development through its Life Skills Learning Program that works to prevent school delinquency and dropouts; supporting community actions to keep students in school; its Job Readiness Program that helps participants prepare for obstacles that can happen when they enter the workforce; and its Job Fair Initiative that links trainees and local employers. Through Aims4Peace’s Hospital Prevention Program, hospital workers respond to gunshot and violence-related trauma situations, intervene in conflicts, and aim to prevent further violence. Aim4Peace also engages in advocacy, a mechanism for social action.
Capacity Building for Organizational Development
In the United States, fairness is obtained by efforts that begin at the community level. Historically, in fact, advances in voting, education, and civil rights all followed from the efforts of people working first in specific communities. Some communities are issue-linked. Some are geographic.
It was the dedicated communities of women across the nation who won women’s right to vote. It was the efforts of teenagers in specific counties that set education equity in motion.15 Communities can be defined in many ways, including by geography, ethnicity, faith, race, need, age, and even aspiration.
Though communities vary greatly, successful change efforts are the same in key respects. They all involve people working together with a shared vision and commitment to improve some aspect of life. Importantly, the actions required to organize a community effort that has lasting effects are similar to those needed to restructure a company or an institution and to bring a group of people together to successfully achieve long-lasting desired change. Thinking and talking about systematic approaches to achieving health equity has several advantages. First, systematic efforts are more likely to be successful, and second, pursuing change in focused, orderly ways is more likely to attract the support of essential businesses, faith-based organizations, and the media.
Achieving change is a process. One well-documented process was developed at the Harvard Business School by Professor John Kotter. His “eight steps” for leading change have been used over the past 30 years to restructure and build successful private companies, public institutions, and nonprofit organizations. These steps, described from the perspective of errors that led to transformation failures in 1995 (Kotter, 1995), were further delineated in 1996 in the book Leading Change (Kotter, 1996). The eight steps provide a process for achieving desired changes and a foundation for community, business, faith, media, and other sectors to communicate effectively with each other to increase health equity in concrete ways.
Leading Change is the result of studying many thousands of companies and institutions and describes the steps required to change the culture of an organization. The steps are universal in that they are not about a single business or institution, but rather they are about human behavior and motivation. They apply to corporate, institutional, and even national restructuring efforts. The wording of the steps sometimes changes depending on the application, but the essential components are constant.
According to Kotter (1996), successful change requires close attention to these eight steps:
___________________
15 The April 1951 Farmville, Virginia, high school strike led by teenager Barbara Johns was followed by others in the south. Lawsuits were filed, the cases worked their way up the court system, and in May 1954, just 36 months after the Farmville walk-out, the Supreme Court handed down its landmark Brown v. Board of Education decision declaring that the principle of “separate but equal” is unconstitutional.
- Identify the urgency: Leaders need to describe health inequities and the high personal, social, political, and economic costs associated with them in ways that appeal to people’s heads and hearts and use this statement to raise a large army of volunteers.
- Build a guiding coalition: A volunteer army needs a coalition of effective people—coming from its own ranks—to guide it, coordinate it, and communicate its activities.
- Form a strategic vision and initiatives: Strategic initiatives are targeted and coordinated activities that, if designed and executed fast and well enough, will make the vision a reality.
- Enlist a volunteer army: Large-scale change can only occur when significant numbers of local, regional, or national citizens amass under a common opportunity and drive action in the same direction.
- Enable action by removing barriers: By removing barriers such as inefficient processes or hierarchies, leaders provide the freedom necessary for volunteers to work across boundaries and create real impact.
- Generate short-term wins: Wins are the molecules of results. They must be collected, categorized, and communicated—early and often—to track progress and energize volunteers to drive change.
- Sustain acceleration: Change leaders must adapt quickly in order to maintain their speed. Whether it is a new way of finding talent or removing misaligned processes, the leaders must determine what can be done—every day—to stay the course toward the vision.
- Institute change: To ensure that new behaviors are repeated over the long term, it is important to define and communicate the connections between these behaviors and society’s political and economic success (Kotter, 1996).
Other theories of organizational change (such as Lewin’s Change Management Model, Harvard Business Review’s Seven Steps to Change, and Managing Organizational Change in the Public Sector: Theory to Practice by Fernandez and Rainy) have many of the same elements and are relevant to communities as they consider their paths forward (Fernandez and Rainey, 2006; Harvard Business Review, 2002; Levasseur, 2001).
Building community capacity to shape health outcomes is an essential component of advancing health equity. Multiple groups have developed integrated resources for strengthening community capacity in leadership development, community organizing, supporting the relationships between organizations necessary for collaboration, and organizational development. One such multilingual resource is the Community Tool
Box at the University of Kansas (Work Group for Community Health and Development, 2016a). This resource and others are summarized in Table 8-2 later in this chapter.
FOSTERING MULTI-SECTOR COLLABORATION
Collaboration skills represent a specific area for capacity building and are key to bringing together the different sectors necessary to create, implement, and sustain a successful community intervention to achieve health equity. Convening strategies involve meetings that bring together representatives from different sectors to explore shared values, visions, and interventions; to identify roles and collaborative activities; and to braid different sources of funding to create greater impact than a single sector or organization can achieve alone. Collaboration is not always easy, given the disparate missions, goals, organizational cultures, and languages of the key participants, yet creating a shared and compelling vision can be successful in bringing individuals and organizations together to address critical health equity issues. As with all of the elements of community capacity building, the relationships created through collaboration can endure after specific projects or programs end.
Collaboration requires coalition building. A community coalition is a group of individuals or organizations with a common interest who agree to work together toward a common goal aimed at bettering their community (Community Health Innovation, n.d.; Community Tool Box, n.d.). The primary motivation for coalition building is to create a shared response to a community concern (e.g., an urgent issue, policy change, or release of new information) or opportunity (e.g., the availability of new funding) because the existing community response is either nonexistent or insufficient to meet the community’s need. Community coalitions vary in their scope and structure, but most often include the elements of influencing public policy, changing health behavior, and building healthy communities. They may be multi-issue or topic-specific.
Supported by the Greater Nashua Public Health Advisory Council, Plan4Health Nashua is a coalition of planning and public health professionals, including the Nashua Regional Planning Commission, the City of Nashua, the New Hampshire Public Health Association, and Healthy Eating Active Living (HEAL NH) (Plan4Health, n.d.). The Plan4Health Nashua goal is to advance street planning and design that support safer and easier ways to get around for pedestrians and bicyclists. During its 15-month grant period, the Plan4Health Nashua coalition conducted a street study to assess the bikeability and walkability of Nashua streets, developed a Complete Streets guidebook and policy recommendations,
and provided training to city staff, planners, elected officials, and other community members.
The DC Tobacco Free Coalition focuses on a single health issue, tobacco use and exposure (DC Tobacco Free Coalition, n.d.). Partners of the initiative include faith- and community-based organizations in Washington, DC, and individuals who employ multiple strategies spanning education, public policy, and advocacy using culturally and linguistically competent approaches.
The Prevention Institute describes eight steps to building an effective coalition among organizations within the same sector or across sectors (Cohen et al., 2002):
- Analyze the program’s objectives and determine whether or not to form a coalition.
- Recruit the right people.
- Devise a set of preliminary objectives and activities.
- Convene the coalition.
- Anticipate the necessary resources.
- Define elements of a successful coalition structure.
- Maintain coalition vitality.
- Make improvements through evolution.
The community examples in Chapter 5 highlight the important role of partnership building in the success of their organizations and the importance of investing in partnerships. Multi-sector collaboration was a criterion in the selection of the community examples. As part of community-based solutions, multi-sectoral collaborations can benefit from the following general principles that have been delineated by a number of authors:
- The ability of partners to commit resources: Multi-sectoral collaboration requires a human resource plan that is documented and agreed to by all partners, the identification of skill requirements and opportunities for training and development, the sharing of examples of innovative working methodologies, and consensus on a cost-sharing plan (Public Health Agency of Canada, 2016). Investment in partnership includes financial obligations such as time, personnel, and money and may also include forgoing other opportunities and taking on risks (Public Health Agency of Canada, 2016).
- The health sector as a leader or facilitator: Depending on the focus of the multi-sectoral community-based solution, the health sector may assume a leadership role when the solution is tied
-
to its primary interests and capacities or a facilitation or participant role when the necessary capacities belong to another sector such as education, transportation, or public safety (Public Health Agency of Canada, 2016).
- Political support and a public policy environment that supports collective action: A direct link to the political level facilitates visible political support, sustained partner participation, and access to necessary resources (Public Health Agency of Canada, 2016).
- Successful working relationships: Relationships are characterized by trust and mutual respect; being inclusive of all participants; reflecting clear and unambiguous communication; being transparent, clear, timely, and fair in the handling of issues; being supported by a clearly articulated vision; being enabled by effective leadership that ensures the various partners participate on an equitable footing; and having clarity around roles and responsibilities (Danaher, 2011).
- Ability to share leadership, accountability, and rewards among partners: Sharing should be supported through careful planning, mechanisms for monitoring progress and accountability, and plans for sharing anticipated gains (Public Health Agency of Canada, 2016).
These principles are illustrated in multiple community examples. PUSH has collaborated with multiple sectors, such as housing, energy, and parks departments, as well as more than 20 nongovernmental organizations ranging from national organizations and foundations to local nonprofits. The important aspects of Blueprint for Action’s partnerships have been communication to decrease redundancy in efforts across partners and the coordination of data collection from various sectors both to inform the Blueprint’s objectives and priorities and to systematically track progress. As with other case studies, the Dudley Street Neighborhood Initiative has multi-sector collaboration as a core organizational strength. The diversity of partnerships goes beyond nonprofits and governmental organizations to include businesses through the Dudley Workforce Collaborative as well as arts and cultural institutions through the Fairmont Cultural Corridor.
Different approaches may be used in developing community-based collaboration. One is the Framework for Collaborative Community Action on Health. This framework includes assess, prioritize, plan; implement targeted action; change community conditions and systems; achieve widespread change in behaviors and risk factors; and improve population health (IOM, 2003; Roussos and Fawcett, 2000). Collective impact is another approach for facilitating multi-sector collaboration through a focus on shared benefits that accrue to the participating organizations.
Beyond these general principles for fostering multi-sector collaboration, collective impact initiatives are long-term commitments by a group of important actors from different sectors to a common agenda for solving a specific social problem. Collective impact approaches are not needed for all social problems; they are best suited for adaptive problems (i.e., problems with a complex, unknown solution, for which no single entity has the resources nor authority to solve the problem alone) (Kania and Kramer, 2011).
Collective impact initiatives have three preconditions: (1) an influential champion or small group of champions, (2) financial resources to last for at least 2 to 3 years, and (3) a sense of urgency for change around a problem. These preconditions create the opportunity and motivation necessary to convene and maintain multi-sector collaborations. Collective impact initiatives are also characterized by five conditions relevant to advancing community-based solutions for health equity: a common agenda, shared measurement, mutually reinforcing activities, continuous communication, and backbone support.
The phases of collective impact and related activities are summarized in Table 8-1 according to the four components for success (Hanleybrown et al., 2012). The phases include activities that have been discussed elsewhere in this chapter, such as community engagement, public will building, and the data to meet community information needs. With Phases I
TABLE 8-1 Phases of Collective Impact
| Components for Success | Phase I Initiate Action | Phase II Organize for Impact | Phase III Sustain Action and Impact |
|---|---|---|---|
| Governance and infrastructure | Identify champions and form cross-sector group | Create infrastructure (backbone and processes) | Facilitate and refine |
| Strategic planning | Map the landscape and use data to make the case | Create a common agenda (goals and strategy) | Support implementation (align with goals and strategies) |
| Community involvement | Facilitate community outreach | Engage the community and build public will | Continue engagement and conduct advocacy |
| Evaluation and improvement | Analyze baseline data to identify key issues and gaps | Establish shared metrics (indicators, measurement, and approach) | Collect, track, and report progress (process to learn and improve) |
SOURCE: Hanleybrown et al., 2012.
and II taking up to 2 years for completion and Phase III lasting a decade or more, Hanleybrown et al. emphasize that collective impact is a “marathon, not a sprint” (Hanleybrown et al., 2012).
The Community Tool Box at the University of Kansas includes several assessments related to collective impact. The Collective Impact Readiness Impact assesses the extent to which preconditions are met or will require further investment. The Collective Impact Progress Assessment details progress on the five collective impact conditions (Work Group for Community Health and Development, 2016c).
The Magnolia Community Initiative exemplifies a collective impact approach, and a description of its efforts is also included in the Community Tool Box. Communication is facilitated through a shared website that offers access to discussion forums, group blogs, e-mail blasts, a shared calendar, and shared files and documents. Shared measurement is informed by a shared theory of change. Backbone support is provided by the network partners.
COMMUNITY TOOL KITS
In addition to individual strategies and tools, a number of tool kits have been developed. Koo et al. conducted an environmental scan and identified six tool kits that met their definition of a comprehensive resource for community health. Their criteria for inclusion were: (1) a conceptual model or theory of change for improving the community’s health, (2) a suggested set of actions or steps to improve community health, (3) resources to support collaboration with other sectors, and (4) examples of successful collaborative partnerships to improve health. In addition, they required that the tools targeted more than one sector and were freely available on the Internet. The six tool kits and their contents are summarized in Table 8-2 (Koo et al., 2016).
Other tool kits also provide guidance on various specific aspects of community-based solutions. For example, the National Partnership for Action to End Health Disparities Toolkit for Community Action was developed to help individuals, organizations, and policy makers: (1) raise awareness about health disparities by providing descriptions of health disparities and their causes; (2) engage others in conversations about the problem and solutions with tools to guide efforts to promote programs and policies for change; and (3) take action for change by providing information and tools to help individuals and organizations to address health in their communities (HHS, n.d.-b). The Health Equity and Social Justice Toolkit from NACCHO is targeted to local health departments and includes journal articles, video clips, reports, PowerPoint
TABLE 8-2 Comprehensive Tool Kits Supporting Community Health, United States, June 2014–December 2015
| Name | Lead Organization | Primary Audience | Features Unique to Tool Kit |
|---|---|---|---|
| Build Healthy Places Networka | Build Healthy Places Network | Health and community development sectors | Logic models for various health conditions; MeasureUp (mapping and measurement tools); community close-ups that highlight the role of community development |
| Community Commonsb | IP3 and CARES–University of Missouri | Broad | Access to and ability to visualize social determinants data in graphs, maps, and other formats; content from the field organized in “channels,” including economy, education, environment, equity, food, and health; houses (“hubs”) where organizations, initiatives, and collaboratives can share content, data, and resources |
| Community Health Improvement Navigatorc | U.S. Centers for Disease Control and Prevention | Hospitals, public health sector, community partners | Community health improvement infographic; key quotes from Internal Revenue Service final rule on community health needs assessments for charitable hospitals; search engine for evidence-based community interventions |
| Community Tool Boxd | University of Kansas | Broad | Online training, curriculum, community workstations; materials in multiple languages; troubleshooting guide; guestbook to describe use of toolbox |
| Name | Lead Organization | Primary Audience | Features Unique to Tool Kit |
|---|---|---|---|
| County Health Rankings and Roadmaps Action Center | University of Wisconsin Population Health Institute | Broad, community partners | County Health Rankings; What Works for Health database; model of population health; partner guides (including for public health) |
| Practical Playbooke | Duke University School of Medicine, Department of Community and Family Medicine | Public health sector, primary care providers | Similar content also published as a textbook: J. L. Michener, D. Koo, B. C. Castrucci, and J. B. Sprague (eds.), The Practical Playbook: Public Health and Primary Care Together, New York: Oxford University Press, 2016; first national meeting May 2016. |
a For more information, see http://buildhealthyplaces.org (accessed November 17, 2016).
b For more information, see http://www.communitycommons.org (accessed November 17, 2016).
c For more information, see http://www.cdc.gov/chinav (accessed November 17, 2016).
d For more information, see http://ctb.ku.edu/en (accessed November 17, 2016).
e For more information, see http://practicalplaybook.org (accessed November 17, 2016).
presentations, book references, action guides, and websites.16 Another example that is particularly relevant to fostering multi-sector collaboration is the Prevention Institute’s coalition and collaboration tools, including (1) Developing Effective Coalitions: An Eight Step Guide,17 (2) Collaboration Multiplier,18 (3) Collaboration Assessment Tool,19 and (4) The
___________________
16 For more information, see http://archived.naccho.org/topics/justice/hesj-tools.cfm (accessed November 17, 2016).
17 For more information, see https://www.preventioninstitute.org/publications/developing-effective-coalitions-an-eight-step-guide (accessed November 17, 2016).
18 For more information, see https://www.preventioninstitute.org/tools/collaboration-multiplier (accessed November 17, 2016).
19 For more information, see https://www.preventioninstitute.org/publications/collaboration-assessment-tool (accessed November 17, 2016).
Tension of Turf: Making it Work for the Coalition20 (Prevention Institute, 2016a). There are also specific guides that demonstrate the application of the tools in a specific domain: for example, multi-sector partnerships for preventing violence (Tsao and Davis, 2014). The Guide to Community Preventive Services is a collection of evidence-based findings from the Community Preventive Services Taskforce, a panel appointed by the CDC director. The resource is designed to help select interventions to improve health and prevent disease at the community level as well as at other levels. The Community Guide contains reviews designed to answer three questions of key relevance to those wishing to implement community-based solutions: (1) What has worked for others, and how well? (2) What might this intervention cost, and what am I likely to achieve through my investment? and (3) What are the evidence gaps?
In addition, another type of tool kit—collections of community exemplars—are useful to inform community-based solutions by highlighting successful practices at the local level through narrative. For example, the Prevention Institute offers a searchable database of more than 100 community profiles that address a variety of social determinants of health (Prevention Institute, 2016b). The Community Guide also provides stories featuring those who have used the Community Guide to make people safer and healthier.
CONCLUSION
Chapters 4 and 5 described why communities matter and highlighted nine examples of community-based solutions to promote health equity in the United States. This chapter outlines specific tools that communities can use to move toward health equity organized by: (1) those tools that apply across all three elements of health equity as a shared vision, cross-sector collaboration, and community capacity to shape outcomes; (2) those that apply specifically to one of the elements; and (3) prominent tool kits that can inform community-based efforts to promote health equity.
REFERENCES
AARP (American Association of Retired Persons) Public Policy Institute. n.d. Livability index. https://livabilityindex.aarp.org/categories/neighborhood (accessed October 18, 2016).
ABA (American Bar Association). 2009. Standing committee: Pro bono and public service. http://apps.americanbar.org/legalservices/probono/directory/programlinks.html (accessed November 21, 2016).
___________________
20 For more information, see https://www.preventioninstitute.org/publications/the-tension-of-turf-making-it-work-for-the-coalition (accessed November 17, 2016).
Acemoglu, D., and J. S. Pischke. 1999. Beyond Becker: Training in imperfect labour markets. Economic Journal 109(453):112–142.
Autor, D. H. 2001. Why do temporary help firms provide free general skills training? Quarterly Journal of Economics 116(4):1409–1448.
Basch, C. E. 2011a. Healthier students are better learners: A missing link in school reforms to close the achievement gap. Journal of School Health 81(10):593–598.
Basch, C. E. 2011b. Physical activity and the achievement gap among urban minority youth. Journal of School Health 81(10):626–634.
Becker, G. S. 1993 [1964]. Human capital: A theoretical and empirical analysis, with special reference to education. 3rd ed. Chicago, IL: The University of Chicago Press.
Blueprint for Action. 2013. Minneapolis Blueprint for Action to Prevent Youth Violence. Minneapolis, MN: City of Minneapolis Health Department.
Blundell, R., L. Dearden, C. Meghir, and B. Sianesi. 1999. Human capital investment: The returns from education and training to the individual, the firm and the economy. Fiscal Studies 20(1):1–23.
Brandeis University. n.d. Diversity data kids. http://www.diversitydatakids.org (accessed October 21, 2016).
CAN (Community Advancement Network). 2016. CAN dashboard. http://www.cancommunitydashboard.org (accessed December 20, 2016).
Cappelli, P. 2004. Why do employers pay for college? Journal of Econometrics 121(1):213–241.
CDC (U.S. Centers for Disease Control and Prevention). 2013. HIA stories from the field: Douglass County Health Department. https://www.cdc.gov/healthyplaces/stories/omaha.htm (accessed November 21, 2016).
CDC. 2015. The Community Health Status Indicators (CHSI).http://wwwn.cdc.gov/CommunityHealth/info/AboutProject (accessed October 18, 2016).
Chandra, A., J. Acosta, K. G. Carman, T. Dubowitz, L. Leviton, L. T. Martin, C. Miller, C. Nelson, T. Orleans, and M. Tait. 2016. Building a national culture of health. Santa Monica, CA: RAND Corporation.
Chaskin, R. J. 1999. Defining community capacity: A framework and implications from a comprehensive community initiative. Chicago, IL: Chapin Hall Center for Children at the University of Chicago.
City of Boston Data Portal. 2013. City of Boston data portal. https://data.cityofboston.gov (accessed October 18, 2016).
Clary, A., and T. Riley. 2016. Braiding and blending funding streams to meet health-related social needs of low-income persons: Considerations for state health policymakers. Washington, DC: National Academy for State Health Policy.
Cohen, L., N. Baer, and P. Satterwhite. 2002. Developing effective coalitions: An eight step guide. https://www.preventioninstitute.org/sites/default/files/uploads/8steps_040511_WEB.pdf (accessed October 21, 2016).
Community Health Innovation. n.d. Fundamentals of community coalition building. http://chsolutions.typepad.com/elevation/2010/04/community-coalition-building-part-1-fundamentals.html (accessed October 19, 2016).
Community Tool Box. n.d. Coalition building I: Starting a coalition. http://ctb.ku.edu/en/table-of-contents/assessment/promotion-strategies/start-a-coaltion/main (accessed October 19, 2016).
Dan, D., R. Finch, D. Harrison, and D. Kendall. 2011. An employer’s guide to reducing racial & ethnic health disparities in the workplace. Washington, DC: National Business Group on Health.
Danaher, A. 2011. Reducing health inequities: Enablers and barriers to inter-sectoral collaboration. Toronto, ON: Wellesley Institute.
DC Tobacco Free Coalition. n.d. DC Tobacco Free Coalition. http://www.dctfc.org (accessed October 19, 2016).
Dee, T., and E. Penner. 2016. The causal effects of cultural relevance: Evidence from an ethnic studies curriculum. National Bureau of Economic Research working paper no. 21865.
Deming, D. J., J. S. Hastings, T. J. Kane, and D. O. Staiger. 2014. School choice, school quality, and postsecondary attainment. The American Economic Review 104(3):991–1013.
Diamant, A. L., S. H. Babey, and J. Wolstein. 2011. Adolescent physical education and physical activity in California. Healthy policy brief, May. Los Angeles: University of California, Los Angeles, Center for Health Policy Research.
Efrat, M. 2011. The relationship between low-income and minority children’s physical activity and academic-related outcomes: A review of the literature. Health Education & Behavior 20(10):1–11.
EPA (U.S. Environmental Protection Agency). 2016. EJS: Environmental justice screening and mapping tool. https://www.epa.gov/ejscreen (accessed October 18, 2016).
Fernandez, S., and H. G. Rainey. 2006. Managing successful organizational change in the public sector. Public Administration Review 66(2):168–176.
Garcia, R., and R. Sivasubramanian. 2012. Environmental justice for all: Struggle in Baldwin Hills and south central Los Angeles. Clearinghouse Review: Journal of Poverty Law and Policy 46(7–8):374–378.
Gaskin, D. J., T. A. LaVeist, and P. Richard. 2012. The state of urban health: Eliminating health disparities to save lives and cut costs. New York: National Urban League Policy Institute.
Gilbert, A. L., and S. M. Downs. 2015. Medical–legal partnership and health informatics impacting child health: Interprofessional innovations. Journal of Interprofessional Care 29(6):564–569.
Green, G., J. Henry, and J. Power. 2015. Physical fitness disparities in California school districts: A practicum issue briefer for The City Project. University of Southern California: Price School of Public Policy. http://www.cityprojectca.org/blog/wp-content/uploads/2015/06/FINAL-Physical-Education-Briefer-20150601.pdf (accessed July 20, 2016).
Hallarman, L., D. Snow, M. Kapoor, C. Brown, K. Rodabaugh, and E. Lawton. 2014. Blueprint for success: Translating innovations from the field of palliative medicine to the medical–legal partnership. Journal of Legal Medicine 35(1):179–194.
Hanleybrown, F., J. Kania, and M. Kramer. 2012. Channeling change: Making collective impact work. Stanford Social Innovation Review. http://jcisd.org/cms/lib/MI01928326/Centricity/Domain/218/Making%20Collective%20Impact%20Work%20Stanford%202012.pdf (accessed October 31, 2016).
Harvard Business Review. 2002. Seven steps to change: A systematic approach. Cambridge, MA: Harvard Business School Press.
Heller, J., M. L. Givens, T. K. Yuen, S. Gould, M. B. Jandu, E. Bourcier, and T. Choi. 2014. Advancing efforts to achieve health equity: Equity metrics for health impact assessment practice. International Journal of Environmental Research and Public Health 11(11):11054–11064.
HHS (U.S. Department of Health and Human Services). 2002. Physical activity is fundamental to preventing disease. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services.
HHS. n.d.-a. Healthdata.gov. https://www.healthdata.gov (accessed October 18, 2016).
HHS. n.d.-b. National partnership for action to end health disparities: Toolkit for community action. http://minorityhealth.hhs.gov/npa/files/Plans/Toolkit/NPA_Toolkit.pdf (accessed October 31, 2016).
Homer, J., B. Milstein, G. B. Hirsch, and E. S. Fisher. 2016. Combined regional investments could sustainably enhance health system performance and be financially affordable. Health Affairs 35(8):1435–1443.
Human Rights Campaign. 2016. Human Rights Campaign. http://www.hrc.org (accessed October 21, 2016).
IOM (Institute of Medicine). 2003. The future of the public’s health in the 21st century. Washington, DC: The National Academies Press.
IOM. 2012. For the public’s health: The role of measurement in action and accountability. Washington, DC: The National Academies Press.
IOM. 2013. Educating the student body: Taking physical activity and physical education to school. Washington, DC: The National Academies Press.
IOM. 2014. Supporting a movement for health and health equity: Lessons from social movements: Workshop summary. Washington, DC: The National Academies Press.
IOM. 2015a. The role and potential of communities in population health improvement: Workshop summary. Washington, DC: The National Academies Press.
IOM. 2015b. Vital signs: Core metrics for health and health care progress. Washington, DC: The National Academies Press.
IP3. n.d. Community commons. http://www.communitycommons.org (accessed October 18, 2016).
Kania, J., and M. Kramer. 2011. Collective impact. Stanford Social Innovation Review Winter. https://ssir.org/images/articles/2011_WI_Feature_Kania.pdf (accessed October 24, 2016).
Kemm, J. R. 2013. Health impact assessment: Past achievement, current understanding, and future progress. Oxford, UK: Oxford University Press.
Koo, D., P. W. O’Carroll, A. Harris, and K. B. DeSalvo. 2016. An environmental scan of recent initiatives incorporating social determinants in public health. Preventing Chronic Disease 13:E86.
Kotter, J. P. 1995. Leading change: Why transformation efforts fail. Harvard Business Review March–April.
Kotter, J. P. 1996. Leading change. Cambridge, MA: Harvard Business Press.
LA (Los Angeles) County Department of Public Health. 2015. School district physical education model action plan (PE MAP) toolkit. http://publichealth.lacounty.gov/cardio (accessed October 7, 2016).
Lafleur, M., S. Strongin, B. L. Cole, S. L. Bullock, R. Banthia, L. Craypo, R. Sivasubramanian, S. Samuels, and R. García. 2013. Physical education and student activity: Evaluating implementation of a new policy in Los Angeles public schools. Annals of Behavioral Medicine 45(1):122–130.
Leiderman, S. A., W. C. Wolf, and P. York. 2000. Some thoughts about public will. Center for Assessment and Policy Development. http://www.racialequitytools.org/resourcefiles/leiderman.pdf (accessed August 15, 2016).
Levasseur, R. E. 2001. People skills: Change management tools—Lewin’s change model. Interfaces 31(4):71–73.
Lineman, M., Y. Do, J. Y. Kim, and G.-J. Joo. 2015. Talking about climate change and global warming. PLOS One 10(9):e0138996.
Martinez, I. L., N. Castellanos, C. Carr, C. J. Plescia, A. L. Rodriguez, S. Thommi, L. Zaremski, D. Weithorn, P. Maisel, and A. L. Wells. 2016. Increasing awareness in health care access in Florida: A community-based medical–legal practicum project. Progress in Community Health Partnerships: Research, Education, and Action 10(1):141–147.
Maxwell, N., D. Rotz, A. Dunn, L. Rosenberg, and J. Berman. 2013. The structure and operations of social enterprises in redf’s social innovation fund portfolio: Interim report. Oakland, CA: Mathematica Policy Research.
May, J., K. Moseley, and P. Terry. 2016. Developing culture of health metrics that really matter to companies and communities. Health Enhancement Research Organization.
Metropolitan Group. 2009. Building public will: Five-phase communication approach to sustainable change. http://www.metgroup.com/assets/Public-Will.pdf (accessed October 30, 2016).
Mile High Connects. 2016. Denver regional equity atlas. http://www.denverregionalequityatlas.org (accessed October 18, 2016).
Mitchell, L., M. R. Frank, K. D. Harris, P. S. Dodds, and C. M. Danforth. 2013. The geography of happiness: Connecting twitter sentiment and expression, demographics, and objective characteristics of place. PLOS One 8(5):e64417.
NAACP LDF (National Association for the Advancement of Colored People Legal Defense Fund). n.d. Home. http://www.naacpldf.org (accessed October 21, 2016).
NACCHO (National Association of County and City Health Officials). 2016. Health impact assessment.http://archived.naccho.org/topics/environmental/health-impact-assessment (accessed October 24, 2016).
NASEM (National Academies of Sciences, Engineering, and Medicine). 2016. Applying a health lens to business practices, policies, and investments: Workshop summary. Washington, DC: The National Academies Press.
National Center for Medical–Legal Partnership. 2014a. Medical–legal partnership at legal aid of Western Missouri. http://medical-legalpartnership.org/wp-content/uploads/2014/02/MLP-at-LAWMO-2013-Kansas-City-MO.pdf (accessed November 21, 2016).
National Center for Medical–Legal Partnership. 2014b. Medical–legal partnership toolkit.http://medical-legalpartnership.org/mlptoolkit (accessed October 21, 2016).
National Center for Medical–Legal Partnership. 2016. Partnerships across the U.S.http://medical-legalpartnership.org/partnerships (accessed October 21, 2016).
NIH (National Institutes of Health). 2016. U.S. National Library of Medicine: Common data element (CDE) resource portal. https://www.nlm.nih.gov/cde/summaries.html (accessed October 18, 2016).
Northside Achievement Zone. n.d. Northside Achievement Zone (NAZ). http://northsideachievement.org (accessed October 21, 2016).
NOW (National Organization for Women). 2016. National Organization for Women. http://now.org (accessed October 21, 2016).
NPS (National Park Service). 2014. Healthy parks healthy people community engagement eguide: Edition 1. https://www.nps.gov/public_health/hp/hphp/press/HealthyParksHealthyPeople_eGuide.pdf (accessed October 23, 2016).
NPS. 2015. Rim of the valley corridor special resource study and environmental assessment. https://parkplanning.nps.gov/document.cfm?documentID=65351 (accessed October 24, 2016).
Padgette, H., S. Deich, and L. Russell. 2010. Strengthening partnerships and building public will for out-of-school time programs. Washington, DC: National League of Cities’ Institute for Youth, Education, and Families.
Pettignano, R., L. R. Bliss, S. B. Caley, and S. McLaren. 2013. Can access to a medical–legal partnership benefit patients with asthma who live in an urban community? Journal of Health Care for the Poor and Underserved 24(2):706–717.
Pettignano, R., L. Bliss, and S. Caley. 2014. The health law partnership: A medical–legal partnership strategically designed to provide a coordinated approach to public health legal services, education, advocacy, evaluation, research, and scholarship. Journal of Legal Medicine 35(1):57–79.
Plan4Health. n.d. Plan4health Nashua: A collaborative project integrating planning and public health where we live, learn, work, and play. http://plan4health.us/plan4health-coalitions/nashua-nh-plan4health-nashua-an-initiative-of-the-greater-nashua-public-health-network (accessed November 21, 2016).
PolicyLink and USC (University of Southern California) Program for Environmental and Regional Equity. 2016. National equity atlas. http://nationalequityatlas.org (accessed October 18, 2016).
Prevention Institute. 2016a. Tools. https://www.preventioninstitute.org/tools (accessed October 21, 2016).
Prevention Institute. 2016b. Tools: Communities taking action: Profiles of health equity. https://www.preventioninstitute.org/tools/communities-taking-action-profiles-health-equity (accessed October 21, 2016).
Public Health Agency of Canada. 2016. Canadian best practices portal: Key element 6. http://cbpp-pcpe.phac-aspc.gc.ca/population-health-approach-organizing-framework/key-element-6-collaborate-sectors-levels (accessed October 21, 2016).
Realmuto, L., S. Owusu, and K. Libman. 2016. East Harlem neighborhood plan health impact assessment: Connecting housing affordability and health. New York: The New York Academy of Medicine.
Reconnecting America. 2013. Los Angeles equity atlas. http://reconnectingamerica.org/laequityatlas/index.php (accessed October 18, 2016).
Rodrigues, R. G., R. M. das Dores, C. G. Camilo-Junior, and T. C. Rosa. 2016. Sentihealth–cancer: A sentiment analysis tool to help detecting mood of patients in online social networks. International Journal of Medical Informatics 85(1):80–95.
Rodriguez, M., M. Brenman, M. E. Lado, and R. Garcia. 2014. Using civil rights tools to address health disparities. Los Angeles, CA: The City Project.
Ross, C. L., M. Orenstein, and N. Botchwey. 2014. Health impact assessment in the United States. New York: Springer.
Rothman, J. 1996. The interweaving of community intervention approaches. Journal of Community Practice 3(3–4):69–99.
Rotz, D., N. Maxwell, and A. Dunn. 2015. Economic self-sufficiency and life stability one year after starting a social enterprise job. Oakland, CA: Mathematica Policy Research.
Roussos, S. T., and S. B. Fawcett. 2000. A review of collaborative partnerships as a strategy for improving community health. Annual Review of Public Health 21:369–402.
Sabeti, H. 2009. The emerging fourth sector: Executive summary. Washington, DC: The Aspen Institute.
Sadler, B., E. Wampler, J. Wood, M. Barry, and J. Wirfs-Brock. 2012. The Denver regional equity atlas: Mapping access to opportunity at a regional scale. Denver, CO: Mile High Connects, Reconnecting America, and The Piton Foundation.
Sanchez-Vaznaugh, E. V., B. N. Sánchez, L. G. Rosas, J. Baek, and S. Egerter. 2012. Physical education policy compliance and children’s physical fitness. American Journal of Preventive Medicine 42(5):452–459.
Schoeni, R. F., W. H. Dow, W. D. Miller, and E. R. Pamuk. 2011. The economic value of improving the health of disadvantaged Americans. American Journal of Preventive Medicine 40(1):S67–S72.
School-Based Health Alliance. n.d. The children’s health and education mapping tool. http://www.sbh4all.org/resources/mapping-tool (accessed October 21, 2016).
Sege, R., G. Preer, S. J. Morton, H. Cabral, O. Morakinyo, V. Lee, C. Abreu, E. De Vos, and M. Kaplan-Sanoff. 2015. Medical–legal strategies to improve infant health care: A randomized trial. Pediatrics 136(1):97–106.
Springer, A. E., D. M. Hoelscher, B. Castrucci, A. Perez, and S. H. Kelder. 2009. Prevalence of physical activity and sedentary behaviors by metropolitan status in 4th-, 8th-, and 11th-grade students in Texas, 2004–2005. Preventing Chronic Disease 6(1):1–16.
Stratton, C., M. Rose, A. Parcell, and J. Mooney. 2012. Made in Durham: Building an education-to-career system. Durham, NC: MDC, Inc.
Taylor, D. R., B. A. Bernstein, E. Carroll, E. Oquendo, L. Peyton, and L. M. Pachter. 2015. Keeping the heat on for children’s health: A successful medical–legal partnership initiative to prevent utility shutoffs in vulnerable children. Journal of Health Care for the Poor and Underserved 26(3):676–685.
The City Project. n.d.-a. Quality education, physical education, and schools of hope. http://www.cityprojectca.org/quality-education-physical-education-and-shared-use#summary (accessed July 8, 2016).
The City Project. n.d.-b. Transit to trails. http://www.cityprojectca.org/transit-to-trails (accessed October 21, 2016).
The Pew Charitable Trusts. 2016. Issue brief: Is health impact assessment effective in bringing community perspectives to public decision-making? Lessons from 4 case studies in California. The Pew Charitable Trusts. http://www.pewtrusts.org/en/research-andanalysis/issue-briefs/2016/10/is-health-impact-assessment-effective-in-bringingcommunity-perspectives-to-public-decision-making (accessed October 24, 2016).
Thompson, H. R. 2013. Are physical education policies working?: A snapshot from San Francisco, 2011. Preventing Chronic Disease 10.
Tsao, B., and R. Davis. 2014. Multi-sector partnerships for preventing violence: A guide for using collaboration multiplier to improve safety outcomes for young people, communities, and cities. Oakland, CA: Prevention Institute.
UCLA (University of California, Los Angeles). 2016. The Civil Rights Project. https://www.civilrightsproject.ucla.edu (accessed October 21, 2016).
University of Colorado Law School. n.d. Colorado Health Equity Project (CHEP). http://chep.colorado.edu (accessed October 21, 2016).
USDA (U.S. Department of Agriculture) Economic Research Service. 2016. The food access research atlas. http://www.ers.usda.gov/data-products/food-access-research-atlas.aspx (accessed October 21, 2016).
Virginia Department of Health. 2016. Virginia health opportunity index (HOI). https://www.vdh.virginia.gov/OMHHE/policyanalysis/virginiahoi.htm (accessed October 21, 2016).
Waidmann, T. 2009. Estimating the cost of racial and ethnic health disparities. Washington, DC: Urban Institute.
Work Group for Community Health and Development. 2016a. The community tool box. http://ctb.ku.edu/en (accessed October 21, 2016).
Work Group for Community Health and Development. 2016b. The community tool box: Chapter 1, section 3. Our model of practice: Building capacity for community and system change. http://ctb.ku.edu/en/table-of-contents/overview/model-for-community-changeand-improvement/building-capacity/main (accessed October 21, 2016).
Work Group for Community Health and Development. 2016c. The community tool box: Chapter 13, section 1. Developing a plan for building leadership. http://ctb.ku.edu/en/table-ofcontents/leadership/leadership-ideas/plan-for-building-leadership/main (accessed October 21, 2016).
This page intentionally left blank.
























































