
1
The Need to Promote Health Equity
INTRODUCTION
In the United States, health equity and equal opportunity are inextricably linked, and the burdens of disease and poor health and the benefits of wellness and good health are inequitably distributed among groups of people.
Although biology, genetics, and individual behaviors play a role in these differences, many health outcomes are more substantially affected by social, economic, and environmental factors. Understanding the social determinants of health requires a shift toward a more “upstream” perspective—that is, the conditions that constitute the context in which an individual’s behaviors are shaped. To put this more simply, Keyes and Galea (2016) describe the relationship between an individual and the conditions in which one lives using the metaphor of a fishbowl. If the bowl in which a fish lives is dirty, or the glass is cracked and the water is leaking, the fish will never reach its full health potential, despite any individual effort. Although the life of a person is clearly more complex than that of a fish, this metaphor illustrates the futility of only addressing individual behaviors without considering the context. People inhabit environments shaped by policies, forces, and actions that influence their individual choices and behaviors over a lifetime and over generations. Community-wide and national problems like poverty, unemployment, poor education, inadequate housing, poor public transportation, exposure to violence, and neighborhood deterioration (social or physical) are among the factors that shape people’s health, and they do so in unequal ways, thus contributing
to health inequities. The historic and ongoing interplay of structures, policies, norms, and demographic/geographic patterns shapes the life of every individual across the country. These factors are not intractable, and inequities in these factors can be mitigated by policies and community action in powerful ways (see Chapter 3 for a discussion of the evidence). Community assets can be built, leveraged, and modified to create a context to achieve health equity.
People are heavily influenced by the communities they work and live in, and the diverse actors that make up the community ecosystem can be powerful producers of health and well-being. Therefore, this report focuses on the promise of communities to create opportunities for their members to achieve their full health potential. By showcasing many creative, forward-looking, and bold community-led solutions for achieving health equity, this report aims to provide a new narrative about health in the United States. In addition to actors in communities, the report examines other elements that address the structures, policies, and norms needed to promote health equity.
DEFINING HEALTH EQUITY
This report makes frequent reference to a number of terms with meanings that vary depending on the context and the community of users. Such terms include “disparities,” “inequities,” “equity,” “racism,” and “bias,” and they are defined in the glossary of key terms and when first introduced in the report.
It is difficult to fully separate the concepts of equity and equality because they are intertwined. Different fields have used varying terminology in legal, public health, government, and other contexts. This report uses the term “health equity” by applying the term equity to the field of public health. Health equity is the state in which everyone has the opportunity to attain full health potential and no one is disadvantaged from achieving this potential because of social position or any other socially defined circumstance. In this report promoting health equity means creating the conditions where individuals and communities have what they need to enjoy full, healthy lives. Health equity requires focused and sustained societal efforts to confront historical and contemporary injustices and eliminate health disparities (Brennan Ramirez et al., 2008; HHS, n.d.). Health disparities are differences that exist among specific population groups in the attainment of full health potential and in incidence, prevalence, mortality, and burden of disease and other adverse health conditions (NIH, 2010), and they stem from systematic differences—that are preventable and unjust—among groups and communities occupying unequal positions in society (Graham, 2004).
As discussed later in this chapter, studies of health inequities have focused largely on health disparities across racial and ethnic populations. Although such studies have uncovered patterns of discrimination and inequitable health outcomes, enlarging this work to assess the effects of poverty, unemployment, toxic stress, and the many secondary unintended consequences (e.g., drug use and violence) for minority and other disproportionately impacted populations is needed. It is well documented that low socioeconomic status (SES) hampers an individual’s ability to achieve optimal health by limiting access to health-preserving resources (Williams and Purdie-Vaughns, 2015; Woolf and Braveman, 2011). However, SES does not fully explain health disparities based on race and ethnicity, sexual orientation and gender identity (Williams and Purdie-Vaughns, 2015).
In the following sections, the nature and implications of disparities on three key health indicators and for health care are discussed. This discussion is followed by a brief introduction to the social determinants of health and the impacts of health inequities on society. Next, the changing social and environmental context and the role of communities in addressing health inequity are described. Finally, this chapter highlights the ongoing support for accelerating the progress to achieve health equity before providing an overview of the rest of the report.
DISPARITIES IN HEALTH OUTCOMES
The existence of racial and ethnic disparities in morbidity, mortality, and many indicators of health for African Americans, Native Americans, Hispanics,1 and Asians/Pacific Islanders was first acknowledged by the federal government in the 1985 Report of the Secretary’s Task Force on Black and Minority Health (Heckler, 1985). Since then, research has sought to identify additional disparities and explain the mechanisms by which these disparities occur.
Three indicators provide summary information about the overall health of a population or subpopulation: infant mortality, age-adjusted death rates, and life expectancy. The United States ranks lower than most peer nations on these indicators; moreover, racial and ethnic disparities exist in quality and length of life among U.S. residents. The failure to address growing income inequality, along with health inequities by race
___________________
1 Hispanic/Latino identification with country of origin: Four decades after the U.S. government mandated the use of Hispanic or Latino for data collection (e.g., in the decennial census), most Americans with roots in Spanish-speaking countries prefer to be identified by their country (51 percent versus 24 percent who prefer a pan-ethnic term). Also, 69 percent respond that they believe there are multiple cultures, not one monolithic “Hispanic” or “Latino” culture (Taylor et al., 2012).
and ethnicity, contributes to the United States’ low health ranking among peer nations (Davis et al., 2014).
Infant mortality rates reflect the number of infants in a population who die before their first birthday per 1,000 live births. U.S. infant mortality rates have decreased since 2005 for the overall population and within each racial and ethnic group; however, sharp racial and ethnic disparities persist. In 2013, as in previous years, the infant mortality rate among African Americans (11.1 per 1,000 live births) was double the rate among whites (5.06 per 1,000 live births) (Mathews et al., 2015). American Indians/Alaska Natives and Puerto Ricans also experienced higher infant mortality rates (of 7.61 and 5.93 per 1,000 live births, respectively) than whites (Mathews et al., 2015). Infant mortality rates among Asians/Pacific Islanders and non-Puerto Rican Hispanics were lower than those of whites. If white America and black America were two separate nations, white America’s infant mortality rate would rank 49th in the world, while black America’s would be ranked 95th out of 224 nations listed by the U.S. Central Intelligence Agency’s World Factbook, following Botswana, Sri Lanka, the United Arab Emirates, and Turks and Caicos Islands (WHO, 2015).
Life expectancy, the average number of years a person is expected to live based on current mortality rates (typically reported as life expectancy at birth or average number of years a newborn would be expected to live), captures the degree to which all of the individual-level socioeconomic, environmental, and health care–related resources in a society enable members of that society to achieve a long and healthy life. Better living conditions and better access to health care–related resources throughout the lifespan extend longevity. From 1980 to 2014, U.S. life expectancy (at birth) increased by approximately 6 years for males, reaching 76.4 years, and increased 3 years for females, reaching 81.2 years. Racial and ethnic disparities decreased, but they were not eliminated. In 2014, the life expectancy for African American males was 72.0 years, while that for white males was 76.5 years and that for Latino males was 79.2 years. In the same year, life expectancy was 78.1 years for African American females, 81.1 years for white females, and 84.0 years for Latina females (Arias, 2016). Childhood obesity, which disproportionately affects Hispanic and African American youth (Asieba, 2016; Taveras et al., 2013), has been projected to reduce the steady increase in overall life expectancy in this century (Olshansky et al., 2005).
Age-adjusted mortality rates capture population deaths due to all causes, and especially those not due to old age. High death rates suggest that a population not only faces serious threats to health but also lacks the resources needed to address them. The 2012 to 2014 U.S. age-adjusted rates ranged considerably. By race and ethnicity, they ranged from 399.8
per 100,000 people among Asian/Pacific Islanders to 858.1 among African Americans. From 2007 to 2009, the rate was even higher (943.0 per 100,000) among American Indian/Alaska Natives (IHS, 2016). Although the overall death rate among whites (729.1 per 100,000) was substantially lower than the rate among African Americans, it exceeded that of Asian/Pacific Islanders and American Indian/Alaska Natives (NCHS, 2014) for causes including liver disease, suicide, and unintentional injury (Kochanek et al., 2016). Looking at more distal causes, research indicates that age-adjusted death rates among whites are higher for those who live in rural settings (Caldwell et al., 2016) and have lower incomes (HRSA, 2015).
The patterns of health disparities among immigrants and their children that emerge from available data are not straightforward. More than half of U.S. citizens of Asian/Pacific Islander and Hispanic background come from families that emigrated to the United States since 1965. Considerable socioeconomic and cultural heterogeneity exists within these groups, and some subpopulations (e.g., the Hmong population of Asian descent) experience particularly severe health disparities (Cho and Hummer, 2001; de Souza and Anand, 2014; Vang et al., 2015). However, recent immigrant status has also shown positive health impact in some populations (Hummer et al., 2007; Lee et al., 2013; Markides and Coreil, 1986).
Along with race and ethnicity, sexual orientation and gender identity have emerged as important factors in the study of health disparities. Recent epidemiologic surveys have attempted to comprehensively assess the physical and mental health of lesbian, gay, bisexual, and transgender (LGBT) persons (Hsieh and Ruther, 2016; IOM, 2011). The available evidence shows that the LGBT population does experience health disparities and that the disparities are exacerbated for those who hold multiple minority statuses: this “intersectional” perspective describes the recognition that when multiple identities intersect, they represent overlapping inequalities or types of disadvantage (IOM, 2011). Thus, LGBT persons who are also racial/ethnic minorities have worse outcomes than do white LGBT individuals (Hsieh and Ruther, 2016).
Health Care
It is becoming clearer that health insurance coverage alone will not address health disparities associated with race, ethnicity, SES, and geography (Kenney and Huntress, 2012; Ubri and Artiga, 2016). The Patient Protection and Affordable Care Act (ACA), passed in 2010, has accelerated progress toward improved health equity by expanding health insurance coverage to about 20 million Americans (Uberoi et al., 2016). However, challenges remain in fully addressing health care inequity, including policy hurdles affecting subgroups of the population (e.g., lack of coverage
for some immigrants and asylum seekers, or those subject to Deferred Action for Childhood Arrivals) (HealthCare.gov, n.d.); limited system capacity or competence to care for some populations, such as LGBT persons (e.g., newly covered partners of insured LGBT individuals); and the lack of health data to monitor the health needs of some populations (e.g., for American Indians, of whom approximately 20 percent live on rural reservations) (Kruse et al., 2016).
Merely increasing the availability of health care services does not necessarily reduce health care disparities. Consider how the availability of effective antiretroviral therapies has not reduced the rate of acquired immune deficiency syndrome (AIDS) equally across groups. In the U.S. context, the progression to AIDS may signal a failure to access treatment in a timely and appropriate manner as indicated by racial and ethnic trends that have been followed since the beginning of the epidemic, as shown in Figure 1-1.
Though AIDS diagnoses have decreased over time for all groups since the introduction of antiretroviral therapy, the proportion of diagnoses among whites has decreased substantially, while the percentage has increased for other groups, and most substantially for African Americans. Another striking example is found in the domain of clinical research,
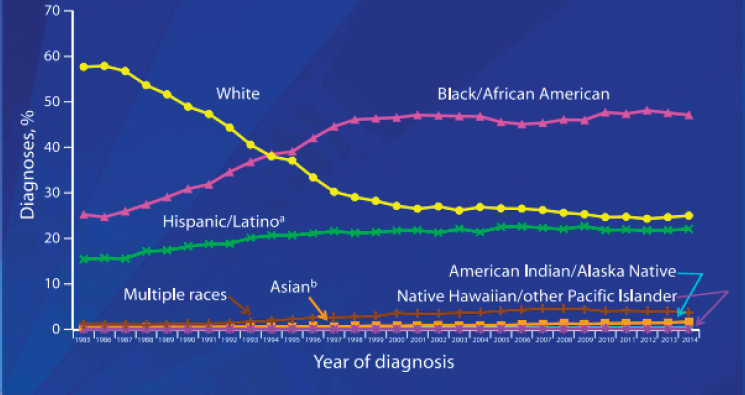
NOTE: All displayed data have been statistically adjusted to account for reporting delays, but not for incomplete reporting. a Hispanics/Latinos can be of any race. b Includes Asian/Pacific Islander legacy cases.
SOURCE: CDC, 2014.
where clinical trials of drugs and devices are not always carried out in diverse populations; therefore, the outcomes of trials may be biased toward the populations studied and fail to account for cultural or other factors that may influence effectiveness (George et al., 2014).
From a policy standpoint, the ACA has achieved its primary goal: the proportion of people who lack health insurance is lower than it has ever been. In the 29 states that have to date elected to participate in the ACA, Medicaid expansion has resulted in more than 10 million low-income individuals now being insured; furthermore, the associated reduction of cost-shifting for uncompensated care has benefited hospital budgets, particularly for disproportionate share hospitals (CMS, 2016; Cunningham et al., 2015). However, the costs of care for these patients are often greater than expected, and Medicaid’s reimbursement rates are a small fraction of the reimbursement rates from commercial payers; therefore, cost-shifting persists. The ACA has increased the availability of outpatient care for low-income persons through increased funding for the operation, expansion, and construction of community health centers.
Challenges remain, however. As noted above, access to insurance does not directly translate into health equity. The traditional fee-for-service system persists and influences utilization patterns more heavily than patient need or evidence-based practice guidelines (The National Commission on Physician Payment Reform, 2013; Page, 2013; Robinson, 2001). Patients need only to receive the care they want and need. Also, there is still a subset of people without adequate insurance, and some commercial payers are leaving the exchanges, premiums are on the rise again, and pharmaceuticals and specialty drugs are increasing in complexity and pricing, untouched by the ACA.
A significant group of workers earn too much to qualify for Medicaid, but too little to afford health insurance. Also, the law does not address the needs of undocumented residents who are among the poorest people in the United States. Nearly one-third of all noncitizen immigrants lack insurance (Barry-Jester and Casselman, 2015). Underutilization of health care services among subpopulations of Hispanic and Asian immigrants has been documented (Alegria et al., 2006). The reasons for underutilization are complex and include an inability to speak the language, differences in the circumstances of immigration (e.g., refugees versus recruited professionals), and the fear of inadvertently outing family members who are in the country without documentation (Ortega et al., 2015).
Because the law is still relatively new, researchers are investigating its outcomes, but there are concerns that some lower-income working class individuals remain underinsured but have had more cost of health care shifted to them (Saloner et al., 2014), and the variations in use and cost persist.
SOCIAL DETERMINANTS OF HEALTH
Although most of the research being conducted at the time of the Heckler Report sought to explain how behavioral and other individual-level factors contribute to health and health care disparities, the evidence accrued since 1985 has led the field toward examining the social, environmental, economic, and cultural determinants of health. These determinants are the conditions in which one lives, learns, works, plays, worships, and ages, and these conditions are shaped by historical and contemporary policies, law, governance, investments, culture, and norms. Addressing the root causes of health inequities, such as the social determinants of health, is important in part to help enable sustainable interventions by engaging multiple sectors and addressing multiple health outcomes simultaneously. The solutions highlighted in this report recognize that national and state leadership are important to effect change in these determinants, but the report specifically addresses these interrelated determinants at the community level (see Chapter 3 for a detailed discussion of the root causes of health disparities, including the social determinants of health).
IMPACTS OF HEALTH INEQUITY IN THE UNITED STATES
Although moral arguments to promote health equity exist2 advancing progress toward health equity could produce economic, national security, and other benefits for the nation. The premise that social mobility, opportunity to succeed with hard work, and opportunity to achieve prosperity exist is fundamental to the American Dream (Carr and Wiemers, 2016). However, recent literature demonstrates that worsening social, economic, and environmental factors are affecting health in serious ways that compromise opportunity for all (Chetty et al., 2016; Rudolph et al., 2015; Woolf et al., 2015). Health is more than life expectancy, infant health, and fitness and nutrition—it is the ability to lead a full and productive life. Additionally, an opportunity to achieve good health is crucial to U.S. democracy, national security, and economic vitality, as described below. The burden
___________________
2 For example, Jones and colleagues cite valuing all people equally as foundational to the concept of equity, noting that the equal worth of all people is at the core of the human rights principle that all human beings equally possess certain rights (Jones, 2009). Braveman and colleagues point out that health differences adversely affecting socially disadvantaged groups are particularly unacceptable because ill health can be an obstacle to overcoming social disadvantage. They further note that this “consideration resonates with common sense notions of fairness, as well as with ethical concepts of justice” (Braveman et al., 2011). Daniels argues for the moral importance of health by exploring the necessities for justice as it relates to health care and the social determinants of health (Daniels, 2008).
of disparities lowers the nation’s overall health status and its ranking relative to other nations.
Political and Economic Impacts of Health Disparities
In addition to the dollar cost of health care, because health inequities contribute to overall poor health for the nation, health inequity has consequences for the U.S. economy, national security, business workforce, and public finances.
Consequences for the Next Generation
American children rank behind their peers in most Organisation for Economic Co-operation and Development (OECD) nations in health status and on key determinants of health, and they experience growing disparities on multiple measures of child well-being (OECD, 2009; Seith and Isakson, 2011). Poverty, food insecurity, lack of stable housing, and lack of access to high-quality and developmentally optimal early childhood education are among the childhood factors that contribute to “chronic adult illnesses and to the intergenerational perpetuation of poverty and ill health found in many communities (e.g., obesity, diabetes, cardiovascular disease, poor educational outcomes, unemployment, poverty, early death)” (AAP, 2010, p. 839). Young children are most likely to live in poverty, and children from low-income and minority communities are most vulnerable (Burd-Sharps and Lewis, 2015). The nation’s growing racial and ethnic diversity, coupled with the conditions that lead to serious early life disadvantage, have serious implications for health and health disparities in later life, leading to squandering human lives and their potential (OECD, 2009).
Consequences for the Economy
The economic effects of health inequity are the result of both unsustainable and wasteful health care spending and diminished productivity in the business sector. Health care spending accounted for 17.5 percent of gross domestic product (GDP) in 2014, and health disparities contribute to a significant amount of financial waste in the health care system.
LaVeist and colleagues (2009) calculated that eliminating health disparities for minorities would have reduced indirect costs associated with illness and premature death by more than $1 trillion between 2003 and 2006. In 2009, the Urban Institute projected that from 2009 to 2018, racial disparities in health will cost U.S. health insurers approximately $337 billion in total (Waidmann, 2009). Disparities in access to health care and
in the quality of care can be costly to individuals, health care providers, health insurers, and taxpayers. Obtaining care late in the course of disease (i.e., delayed care) and inadequate health care coverage may increase the cost of care exponentially due to the exacerbation of complications, the need for more expensive care (e.g., emergency department services), and the need for more extensive care; furthermore, such treatment can increase longer-term reliance on the health care system for the management of unintended consequences on one hand and preventable chronic diseases on the other (IOM, 2009).
Consequences for National Security
For a nation that prizes military readiness, the effects of poor health status on entrance to military service and the readiness of the force matter. Military leaders reported that more than 75 percent of 17- to 24-year-olds—more than 26 million young adults—in the United States cannot qualify to serve in the armed forces because they have health problems ranging from obesity to dependencies on prescription and nonprescription drugs, are poorly educated, or are involved in crime (Christeson et al., 2009). According to more than 500 retired admirals, generals, and other senior military leaders, the health of our nation’s youth represents a serious national security concern (Christeson et al., 2009, 2010). Individuals who are not healthy enough to participate in the workforce will not be afforded the same employment opportunities as their healthy counterparts. Rear Admiral Robert Besal (ret.) has asserted that young people who are physically unfit for “productive employment or military service represent a staggering loss of individual potential and collective strength for the nation as well” (Council for a Strong America, 2016).
Consequences for Business
A healthy, productive workforce is a prerequisite to a thriving economy (HERO, 2015; IOM, 2015). The impact of poor health on private businesses is significant. Research from the Urban Institute shows that those young adults with health problems who can find jobs in the mainstream economy are less productive and generate higher health care costs for businesses than those without health problems (Woolf et al., 2015).
Consequences for Income Inequality
Research finds that people in counties with an inequitable distribution of opportunities for good health are more likely to die before the age of 75 than people in counties with more equitable opportunities for
health (health status), even if the average incomes are the same (University of Wisconsin Population Health Institute, 2015). Political scientists at Princeton and Georgetown University are finding that crippling political polarization and gridlock are linked to income and wealth inequality (Ferejohn, 2009; Voorheis et al., 2015). But income and wealth are not what worries Americans. Instead, it is what can be obtained with income and wealth that worries them most, and, of these, Gallup reports that health care is at the top of the list (Swift, 2015). Health problems often reduce personal income in ways that worsen inequity, which in turn may lead to further inequity. For states, it is well understood that as health care spending through state Medicaid increases, the funds available to support state universities decrease (Orszag and Kane, 2003).
CHANGING SOCIAL AND ENVIRONMENTAL CONTEXT
There are significant changes in the sociocultural (including demographic, economic, and political) and environmental landscapes affecting health disparities and the determinants of health.
The changing economic context is characterized by growing income inequality. According to an analysis performed by the Institute for Policy Studies, the income gap between higher- and lower-income individuals has increased substantially over the past 30 years, to the point that those with incomes in the top 10 percent average nine times the income of those in the bottom 90 percent, and those with incomes in the top 0.1 percent have incomes that are more than 184 times that of the bottom 90 percent (Asante-Muhammad et al., 2016). This income inequality has a remarkable impact on individual health, as higher-income earners have longer life expectancies than lower-income earners in every region of the United States. There are significant economic changes that affect other social determinants as well. For instance, urban centers across the country are dealing with shifting demographics that can result in the displacement of long-term residents. The economic advantages of changing land value due to these shifts largely benefit those who are already in higher-income brackets. In contrast, dislocated low-income households face overwhelming challenges in efforts to find new housing with access to high-quality schools, jobs, and other essential social services that are vital to optimal health. The lasting effects of the 2008 recession and the resulting displacement of vulnerable populations exacerbated the impact on both their health and their economic well-being—resulting in greater income inequality and wealth inequality (Smeeding, 2012).
Recent changes in U.S. demographics underscore the urgency of finding ways to attain health equity. For example, from 2000 to 2010 the African American population increased by 11 percent (Rastogi et al., 2010),
and the Hispanic population increased by 43 percent (Ennis et al., 2011), while the white population increased by only 1.2 percent (Hixson et al., 2011). By 2040 the number of U.S. counties in which the majority of the population is comprised of people of color is expected to more than double; those counties will then represent about one-third of the United States (Frey, 2015). Without significant and fundamental policy changes, these changes in the racial and ethnic composition of U.S. communities can be expected to further widen health inequities associated with race and class. Disparities in health, income, and education have also all been increasing over time (see Chapters 2 and 3 for more information).
Climate change will increasingly affect health. In 2015, at the United Nations Climate Change Conference—also known as COP 21—multiple nations, including the United States, came together to create an agreement to combat climate change and attempt to prevent the global temperature from rising more than 2 degrees Celsius. Health representatives played an integral role in the conference, as health is and will continue to be significantly affected by climate change. Climate change is happening in all areas, but its impacts are not distributed equally. It exacerbates vulnerabilities in communities that are already disproportionately affected by preexisting social, economic, and environmental factors. Extreme weather events are one of the many examples of the ways in which climate change will impact health. Hurricane Katrina was not necessarily the direct result of climate change. However, it offers many important lessons on mitigating risk and increasing resiliency in making plans to help the entire population, especially the most vulnerable. Although there is a risk that climate change could worsen health inequities, there is also great opportunity to integrate efforts to promote health into mitigation and adaptation efforts to support more resilient, healthy, and equitable communities (Rudolph et al., 2015).
Finally, recent events involving race and law enforcement relations have elucidated systematically unequal treatment in the criminal justice system (The President’s Task Force on 21st Century Policing, 2015). Moreover, there is a growing and bipartisan recognition that mass incarceration, which affects individuals of color disproportionately, plays a major role in the breakdown of families and communities, constitutes an unsustainable use of taxpayer dollars, and leads, in connection with the larger policy milieu in both the private and the public sector, to poor employment prospects and voter disenfranchisement (Clear, 2008; NRC, 2014). These current realities serve as reminders that the vision of an equitable society will be challenging to reach, but community-driven solutions, such as those this report highlights, can help move in that direction on a local scale.
WHY COMMUNITIES?
Individuals and families are part of communities, and the role of communities is crucial to promoting health equity for several reasons. First, as discussed earlier, medical interventions are insufficient to address health equity, and behavioral health promotion continues to show little success in reducing disparities (Baum and Fisher, 2014). Community-based and -driven efforts are needed to alter environmental, socioeconomic, and cultural conditions in ways that promote health equity. Community health refers to the overall well-being of a community at all levels (including the individuals within the community and the physical setting), which may involve multi-sector and multidisciplinary collaborative approaches to optimizing the health and quality of life of all persons who live, work, or are otherwise active in a defined community (Goodman et al., 2014). A healthy community is the foundation for achieving all other goals, as it is essential for a productive society. (For example, a community with a healthy workforce has a good base upon which to build its economy, and healthier students are more equipped to learn and be successful academically.) Furthermore, communities differ in the local quality and availability of health care providers, the affordability and quality of housing, employment opportunities, transportation systems, the availability of parks, green space, and other aspects of the physical environment. Communities are uniquely positioned to drive solutions tailored to their needs that target the multiple determinants of health.
MOMENTUM FOR ACHIEVING HEALTH EQUITY
There is a clear urgency for the nation to fully address health inequity. An analysis of current trends provides evidence of persistent health inequity, but there are reasons for optimism. Turning the tide is not only possible, it is imperative; many organizations in the public and private sectors have recognized this, making health equity an explicit or implicit priority. These organizations span the sectors of finance, philanthropy, public health, community development, academia, and beyond. Local, regional, and state governments have also taken on issues essential to achieving health equity. For example, the Federal Reserve Bank and community development financial institutions are engaging in improving community development, employment, and housing—which drive health improvement—and they are making investments that expand access to healthy and affordable foods and neighborhoods with open space to promote physical activity and community safety (Andrews and Erickson, 2012). Health equity is a guiding priority for the American Public Health Association in its initiative to make the United States the healthiest nation in a generation, with 2030 as a goalpost (APHA, n.d.). In
2016 the Association of State and Territorial Health Officials’ President’s Challenge is to “Advance health equity and optimal health for all,” and “Cultivating a culture of health equity” was the theme for the National Association of County and City Health Officials’ annual meeting. Numerous states, including California, Colorado, Massachusetts, Pennsylvania, and Wyoming, have created statewide offices of health equity that work in collaboration with other agencies and departments to inform policies that promote health equity. Health equity has become central to the goals of some of the nation’s largest philanthropic organizations, including The California Endowment, Ford Foundation, Kresge, and Kellogg. Advancing health equity is at the core of the Robert Wood Johnson Foundation’s (RWJF’s) new push for a culture of health (RWJF, 2015). The federal government is investing heavily in health equity as well, and it recently established a National Institutes of Health research program to address health disparities in chronic disease as well as the National Partnership for Action to End Health Disparities. These investments seek to “transform lives and places for disinvested people” (The Housing Fund, 2015), and at their core they are investments to create opportunity for all to achieve optimal health.
Conclusion 1-1: The persistent state of health disparities and health inequity in the United States has profound implications for the country’s overall health standing, economic vitality, and national security. Thus, addressing health inequities is a critical need that requires this issue to be among our nation’s foremost priorities.
ABOUT THIS REPORT
RWJF, as part of its Culture of Health Initiative,3 asked the Health and Medicine Division of the National Academies of Sciences, Engineering, and Medicine to help delineate the causes of and the solutions to health inequities in the United States. The charge to the committee is provided below (see Box 1-1 for the full statement of task). To respond to the charge, the Committee on Community-Based Solutions to Promote Health Equity in the United States was formed.
The focus of this report is on what communities can do to promote health equity and on the broader policy context and contributions of stakeholders that can support communities. In addition to the root causes and structural barriers that need to be overcome, the committee also examined levers and policies to support change, some of which span
___________________
3 For more information, see http://www.rwjf.org/en/culture-of-health.html (accessed October 28, 2016).
national, state, regional, and other contexts for the work of communities. To address its charge, the committee reviewed examples of community efforts across the country and was inspired by how these communities are rising to the challenge to address the difficult challenges and barriers to health and well-being.
Culture of Health Lens
RWJF defines a culture of health broadly “as one in which good health and well-being flourish across geographic, demographic, and social sectors; fostering healthy equitable communities guides public and private decision making; and everyone has the opportunity to make choices that lead to healthy lifestyles” (RWJF, n.d.). RWJF also says that “the exact definition of a culture of health can look very different to different people. A national culture of health must embrace a wide variety of beliefs, customs and values. Ultimately it will be as diverse and multifaceted as the population it serves” (RWJF, n.d.). The culture of health framework was developed by the foundation in collaboration with RAND Corporation through a combination of literature review and structured discussions with stakeholders (Chandra et al., 2016). The framework includes four action areas that are interdependent—none can be achieved alone (Plough and Chandra, 2016). The four action areas are
- Making health a shared value
- Fostering cross-sector collaboration to improve well-being
- Creating healthier, more equitable communities
- Strengthening the integration of health systems and services
The committee used the framework as a guide for this report and adapted it to apply specifically to its statement of task and at the community level.
The committee also referred to the ecological model illustrated in the 2003 Institute of Medicine (IOM)4 report The Future of the Public’s Health in the 21st Century. This figure shows the multiple determinants of health, beginning with an individual’s biology (and the biology of diseases) at the center, followed by individual behavior, and in the outermost layer, the highest level of social, economic, cultural, health, and environmental conditions and policy (IOM, 2003). The committee was charged with examining community-based solutions, and it developed a simple model to show what it concluded are three important elements of community-based efforts to promote health equity. The community-based level of intervention is situated in the second and third outermost circles of Figure 1-2 (i.e., social, family, and community networks; living and working conditions). As Figure 1-2 clearly indicates, community effort is necessary, but it is not a sufficient contributor to population health and, by extension, health equity. The outermost ring—the broad milieu of social,
___________________
4 As of March 15, 2016, the Health and Medicine Division (HMD) carries out the work previously undertaken by the IOM.
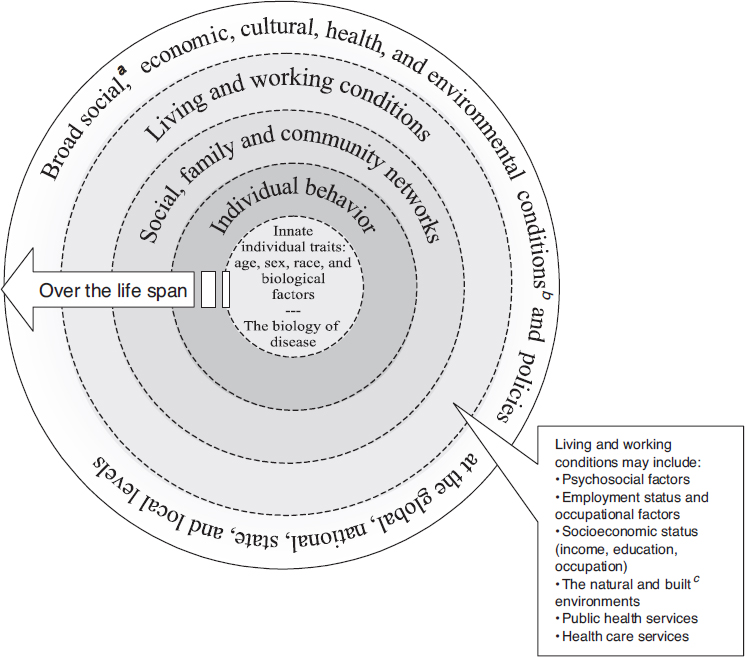
SOURCE: IOM, 2003.
economic, and environmental conditions and policies—is crucial to support community-level efforts.
Report Conceptual Model
Figure 1-3 is a conceptual model that grounds the committee’s report. The model adapts elements of the Culture of Health Action Framework
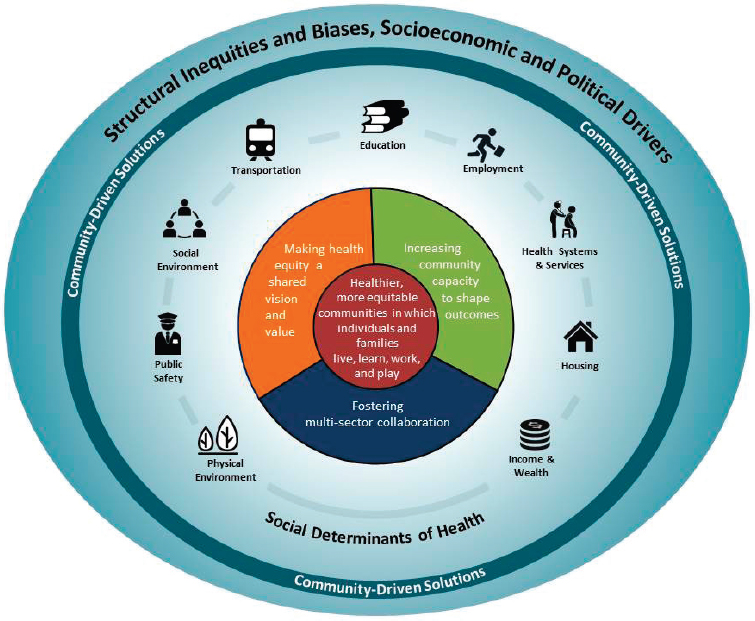
NOTES: Multi-sector collaboration includes partners from agriculture, banking/finance, business/industry, economic development, education, health care, housing, human/social services, justice, labor, land use and management, media, public health, transportation, and workforce development, among other sectors.
SOURCES: Informed by the Robert Wood Johnson Foundation (2015) Culture of Health Action Framework and the Prevention Institute’s (2016) Systems Framework to Achieve an Equitable Culture of Health.
(RWJF, 2015) and the Prevention Institute’s Systems Framework to Achieve an Equitable Culture of Health (Prevention Institute, 2016). The model applies the culture of health lens to the committee’s understanding of the underlying causes and conditions of health inequity in addition to the community-based solutions that promote health equity.
The model begins with the outer circle and background as the context in which health inequities and community-driven5 solutions exist.
___________________
5 The committee chose the term “community-driven solutions” because the community will be the driving force behind the solutions in this report.
The “socioeconomic and political context” was adapted from the World Health Organization Conceptual Framework for Action on the Social Determinants of Health (WHO, 2010) and encompasses policies, law, governance, and culture. In the report conceptual model, this socioeconomic and political context includes structural inequities and biases that are produced along the axes of race, gender, class, sexual orientation, and other social domains. These inequities are manifested in systematic disadvantages that lead to inequitable access to or experience of the determinants of health. The committee adapted the determinants of health identified by the Achieving Health Equity Team at the RWJF, separating the social and physical environments, and adding transportation. Although the framework incorporates transportation as part of the “physical and social environment,” transportation is vital to many areas of health (e.g., the ability to travel to health care facilities, community events, accessing jobs) and, alternatively, can have detrimental impacts on health (e.g., air pollution, unintentional injuries), and thus it has been highlighted in the model. (See Chapter 3 for a more detailed description of each determinant of health and the ways in which they affect health and well-being.)
The committee adapted two of the Culture of Health Action Framework Action Areas for community-level solutions: “Making health equity a shared vision and value” and “Fostering multi-sector collaboration.” Based on the committee’s information-gathering sessions, relevant literature, and committee deliberations, the committee also identified a third action area of importance for the framework when proposing solutions at the community level: “Increasing community capacity to shape outcomes.” This is a process that has emerged as essential for communities to have the power to address inequities and to sustain their efforts. (These three elements are discussed in more detail in Chapter 4.) To align with its statement of task, the committee incorporated equity at the community level in its conceptual model. The Culture of Health action area “Creating healthier, more equitable communities” has been incorporated into the conceptual model as the outcome of the community-driven solutions in the center of the diagram.
The community examples featured in this report will highlight solutions that have been implemented at the community level to target one or more of the nine determinants of health using the processes identified in the conceptual model (see Chapter 5). By making health equity a shared vision and value, increasing community capacity to shape outcomes, and fostering multi-sector collaboration, these solutions foster equal opportunity for health, which is the foundation for a vibrant, healthy community.
Community Health
This report does not focus on interventions that target a single health condition, but on community-level changes and impacts on health through a holistic lens. The development of a community-based solution is a community-driven process that includes fair participation by the community in the decision-making process, in which all people have access to the information necessary to understand the matter and the process and which produces outcomes that the people accept as fair, equitable, and nondiscriminatory in the context of addressing health disparities. Therefore, the terms “community-driven solutions” and “community-based solutions” will be used interchangeably for the remainder of this report (see Box 1-2 for definitions). The importance of communities and their role and potential to promote health equity is discussed in Chapter 4.
Overview of the Study Process
To address its charge, the committee gathered information through a variety of means. It held three information-gathering meetings that were open to the public and webcast live. The first, held in January 2016, focused on obtaining information on health disparities and their root causes, including an overview from the report sponsor. The second, held in March 2016, focused on many of the social determinants of health and
included presentations on how transportation, planning, environmental justice, and civil rights law affect health. The third meeting was held in April 2016, and presentation topics included faith-based community organizing, community-based participatory research, place-based factors and policy at the community level, and the economics of community development (meeting agendas are in Appendix C). The committee met in executive sessions for deliberative discussion throughout the study process. The committee received public submissions of materials for its consideration at the meetings and by e-mail throughout the course of the study.6 A website was created to provide information to the public about the committee’s work and to facilitate communication between the public and the committee.7 The process used to identify the community examples highlighted is outlined in the Chapter 5 Annex.
Overview of Report
Chapter 2 begins with a description of the state of health disparities in the United States by geography, income, race and ethnicity, and other categories. Chapter 3 discusses how structural and institutional inequities have led to disparate health outcomes and highlights historical issues that continue to affect health outcomes today, as well as the ways in which current and emerging issues ultimately affect communities. This is followed by a discussion on the multiple determinants of health and how they affect health equity. Chapter 4 discusses the role and capacity of communities to promote health equity and explains the larger context in which communities are situated, as well as the types of evidence needed to support communities. Chapter 5 provides nine examples of communities that are tackling health inequity and the lessons learned from these efforts. Chapter 6 addresses the policies that ultimately affect communities and that could either hinder or promote solutions at the level of individual communities. Chapter 7 discusses the roles of various stakeholders and the actions that these actors could undertake in their communities, with an emphasis on multi-sector collaboration. Chapter 8 is geared toward communities and provides an array of strategies, tools, and activities available to communities to help them promote health equity. Chapter 9 provides brief summarizing thoughts.
___________________
6 Public access materials can be requested from http://www8.nationalacademies.org/cp/projectview.aspx?key=IOM-BPH-15-15 (accessed December 23, 2016).
7 See http://www.nationalacademies.org/hmd/Activities/PublicHealth/Culture-ofHealth.aspx (accessed December 23, 2016).
CONCLUDING OBSERVATIONS
There are systemic root causes of health inequities in this country that can be overwhelming and that will take considerable time to address. It will require system-level changes to eliminate structural racism, reduce poverty, improve income equality, increase educational opportunity, and fix the laws and policies that perpetuate structural inequities. Until these root causes are addressed nationally, health equity will not be fully realized. However, actors at the community level—policy makers, businesses, state and local governments, anchor institutions, and community residents—are agents of local change who have the power to change the narrative and take action that will promote health equity. The latter is what this report will focus on, although, where possible, it will provide promising strategies to address these hard-to-tackle root causes at higher levels.
REFERENCES
AAP (American Academy of Pediatrics). 2010. Health equity and children’s rights. Pediatrics 125(4):838–849.
Alegria, M., Z. Cao, T. G. McGuire, V. D. Ojeda, B. Sribney, M. Woo, and D. Takeuchi. 2006. Health insurance coverage for vulnerable populations: Contrasting Asian Americans and Latinos in the United States. Inquiry 43(3):231–254.
Andrews, N. O., and D. J. Erickson. 2012. Investing in what works for America’s communities: Essays on people, place & purpose. Federal Reserve Bank of San Francisco and Low Income Investment Fund.
APHA (American Public Health Association). n.d. Health equity. https://www.apha.org/topics-and-issues/health-equity (accessed October 24, 2016).
Arias, E. 2016. Changes in life expectancy by race and Hispanic origin in the United States, 2013-2014. National Center for Health Statistics NCHS data brief no. 244.
Asante-Muhammad, D., C. Collins, J. Hoxie, and E. Nieves. 2016. The ever-growing gap: Without change, African-American and Latino families won’t match white wealth for centuries. Washington, DC: Institute for Policy Studies and CFED.
Asieba, I. O. 2016. Racial/ethnic trends in childhood obesity in the United States. Journal of Childhood Obesity 1(1):1–6.
Barry-Jester, A. M., and B. Casselman. 2015. 33 million Americans still don’t have health insurance. FiveThirtyEight, September 28. http://fivethirtyeight.com/features/33million-americans-still-dont-have-health-insurance (accessed January 9, 2017).
Baum, F., and M. Fisher. 2014. Why behavioural health promotion endures despite its failure to reduce health inequities. Sociology of Health and Illness 36(2):213–225.
Braveman, P. A., S. Kumanyika, J. Fielding, T. LaVeist, L. N. Borrell, R. Manderscheid, and A. Troutman. 2011. Health disparities and health equity: The issue is justice. American Journal of Public Health 101(Suppl 1):S149–S155.
Brennan Ramirez, L. K., E. A. Baker, and M. Metzler. 2008. Promoting health equity: A resource to help communities address social determinants of health. Atlanta: U.S. Department of Health and Human Services, U.S. Centers for Disease Control and Prevention.
Burd-Sharps, S., and K. Lewis. 2015. Geographies of opportunity: Ranking well-being by congressional district. New York: Social Science Research Council.
Caldwell, J. T., C. L. Ford, S. P. Wallace, M. C. Wang, and L. M. Takahashi. 2016. Intersection of living in a rural versus urban area and race/ethnicity in explaining access to health care in the United States. American Journal of Public Health 106(8):1463–1469.
Carr, M. D., and E. E. Wiemers. 2016. The decline in lifetime earnings mobility in the U.S.: Evidence from survey-linked administrative data. Washington, DC: Washington Center for Equitable Growth.
CDC (U.S. Centers for Disease Control and Prevention). 2014. Epidemiology of HIV infection through 2014. https://www.cdc.gov/hiv/pdf/library/slidesets/cdc-hiv-surveillancegenepi.pdf (accessed October 24, 2016).
Chandra, A., J. Acosta, K. G. Carman, T. Dubowitz, L. Leviton, L. T. Martin, C. Miller, C. Nelson, T. Orleans, M. Tait, M. Trujillo, V. Towe, D. Yeung, and A. L. Plough. 2016. Building a national culture of health: Background, action framework, measures, and next steps. Santa Monica, CA: RAND Corporation.
Chetty, R., M. Stepner, S. Abraham, S. Lin, B. Scuderi, N. Turner, A. Bergeron, and D. Cutler. 2016. The association between income and life expectancy in the United States, 2001–2014. JAMA 315(16):1750–1766.
Cho, Y., and R. A. Hummer. 2001. Disability status differentials across fifteen Asian and Pacific Islander groups and the effect of nativity and duration of residence in the U.S. Social Biology 48(3–4):171–195.
Christeson, W., A. D. Taggart, and S. Messner-Zidell. 2009. Ready, willing, and unable to serve: 75 percent of young adults cannot join the military; early education across America is needed to ensure national security. Washington, DC: Mission: Readiness.
Christeson, W., A. D. Taggart, and S. Messner-Zidell. 2010. Too fat to fight: Retired military leaders want junk food out of America’s schools. Washington, DC: Mission: Readiness.
Clear, T. R. 2008. The effects of high imprisonment rates of communities. Crime and Justice 37(1):97–132.
CMS (Centers for Medicare & Medicaid Services). 2016. Disproportionate share hospital (DSH). https://www.cms.gov/medicare/medicare-fee-for-service-payment/acuteinpatientpps/dsh.html (accessed October 24, 2016).
Council for a Strong America. 2016. New 50-state index from Council for a Strong America shows most young adults not “citizen-ready.” http://www.marketwired.com/press-release/new-50-state-index-from-council-strong-america-shows-most-young-adults-not-citizen-ready-2157947.htm (accessed October 24, 2016).
Cunningham, P. J., R. Garfield, and R. Rudowitz. 2015. How are hospitals faring under the Affordable Care Act? Early experiences from Ascension Health. The Kaiser Commission on Medicaid and the Uninsured. http://kff.org/health-reform/issue-brief/how-are-hospitals-faring-under-the-affordable-care-act-early-experiences-from-ascension-health/ (accessed October 24, 2016).
Daniels, N. 2008. Just health: Meeting health needs fairly. New York: Cambridge University Press.
Davis, K., K. Stremikis, D. Squires, and C. Schoen. 2014. Mirror, mirror on the wall, 2014 update: How the U.S. health care system compares internationally. The Commonwealth Fund.
de Souza, R. J., and S. S. Anand. 2014. Cardiovascular disease in Asian Americans: Unmasking heterogeneity. Journal of the American College of Cardiology 64(23):2495–2497.
Ennis, S. R., M. Rios-Vargas, and N. G. Albert. 2011. The Hispanic population: 2010. U.S. Census Bureau.
Ferejohn, J. 2009. Is inequality a threat to democracy? In The unsustainable American state, edited by L. R. Jacobs and D. S. King. New York: Oxford University Press. Pp. 34–60.
Frey, W. H. 2015. A pivotal period for race in America. In Diversity explosion: How new racial demographics are remaking America. Washington, DC: Brookings Institution Press.
George, S., N. Duran, and K. Norris. 2014. A systematic review of barriers and facilitators to minority research participation among African Americans, Latinos, Asian Americans, and Pacific Islanders. American Journal of Public Health 104(2):16–31.
Goodman, R. A., R. Bunnell, and S. F. Posner. 2014. What is “community health”? Examining the meaning of an evolving field in public health. Preventive Medicine 67(Suppl 1):S58–S61.
Graham, H. 2004. Social determinants and their unequal distribution: Clarifying policy understandings. Milbank Q 82(1):101–124.
HealthCare.gov. n.d. Immigration status and the marketplace. https://www.healthcare.gov/immigrants/immigration-status (accessed October 24, 2016).
Heckler, M. M. 1985. Report of the Secretary’s Task Force on Black & Minority Health. Washington, DC: U.S. Department of Health and Human Services.
HERO (Health Enhancement Research Organization). 2015. Exploring the value proposition for workforce health: Business leader attitudes about the role of health as a driver of productivity and performance. http://hero-health.org/wp-content/uploads/2015/02/HPP-Business-Leader-Survey-Full-Report_FINAL.pdf (accessed October 24, 2016).
HHS (U.S. Department of Health and Human Services). n.d. Disparities. https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities (accessed October 24, 2016).
Hixson, L., B. B. Hepler, and M. O. Kim. 2011. The white population: 2010. U.S. Census Bureau.
HRSA (Health Resources and Service Administration). 2015. Mortality and life expectancy in rural America: Connecting the health and human service safety nets to improve health outcomes over the life course. National Advisory Committee on Rural Health and Human Services.
Hsieh, N., and M. Ruther. 2016. Sexual minority health and health risk factors: Intersection effects of gender, race, and sexual identity. American Journal of Preventive Medicine 50(6):746–755.
Hummer, R. A., D. A. Powers, S. G. Pullum, G. L. Gossman, and W. P. Frisbie. 2007. Paradox found (again): Infant mortality among the Mexican-origin population in the United States. Demography 44(3):441–457.
IHS (Indian Health Service). 2016. Disparities. https://www.ihs.gov/newsroom/factsheets/disparities (accessed October 24, 2016).
IOM (Institute of Medicine). 2003. The future of the public’s health in the 21st century. Washington, DC: The National Academies Press.
IOM. 2009. America’s uninsured crisis: Consequences for health and health care. Washington, DC: The National Academies Press.
IOM. 2011. The health of lesbian, gay, bisexual, and transgender people: Building a foundation for better understanding. Washington, DC: The National Academies Press.
IOM. 2015. Business engagement in building healthy communities: Workshop summary. Washington, DC: The National Academies Press.
Jones, H. 2009. Equity in development: Why it is important and how to achieve it. London: Overseas Development Institute.
Kenney, G. M., and M. Huntress. 2012. The Affordable Care Act: Coverage implications and issues for immigrant families. https://aspe.hhs.gov/basic-report/affordable-care-act-coverage-implications-and-issues-immigrant-families (accessed October 24, 2016).
Keyes, K. M., and S. Galea. 2016. Population health science. New York: Oxford University Press.
Kochanek, K. D., E. Arias, and B. A. Bastian. 2016. The effect of changes in selected age-specific causes of death on non-Hispanic white life expectancy between 2000 and 2014. National Center for Health Statistics NCHS data brief no. 250.
Kruse, C. S., S. Bouffard, M. Dougherty, and J. S. Parro. 2016. Telemedicine use in rural Native American communities in the era of the ACA: A systematic literature review. Journal of Medical Systems 40(6):145.
LaVeist, T. A., D. J. Gaskin, and P. Richard. 2009. The economic burden of health inequalities in the United States. Washington, DC: Joint Center for Political and Economic Studies.
Lee, S., A. H. O’Neill, E. S. Ihara, and D. H. Chae. 2013. Change in self-reported health status among immigrants in the United States: Associations with measures of acculturation. PLOS One 8(10):e76494.
Markides, K. S., and J. Coreil. 1986. The health of Hispanics in the southwestern United States: An epidemiologic paradox. Public Health Reports 101(3):253–265.
Mathews, T. J., M. F. MacDorman, and M. E. Thoma. 2015. Infant mortality statistics from the 2013 period linked birth/infant death data set. National Vital Statistics Reports 64(9):1–28.
NCHS (National Center for Health Statistics). 2014. Health, United States, 2014: With special feature on adults aged 55–64. Hyattsville, MD: U.S. Centers for Disease Control and Prevention.
NIH (National Institutes of Health). 2010. NIH announces Institute on Minority Health and Health Disparities. https://www.nih.gov/news-events/news-releases/nih-announces-institute-minority-health-health-disparities (accessed October 24, 2016).
NRC (National Research Council). 2014. The growth of incarceration in the United States: Exploring causes and consequences. Washington, DC: The National Academies Press.
OECD (Organisation for Economic Co-operation and Development). 2009. United States country highlights: Doing better for children. https://www.oecd.org/unitedstates/43590390.pdf (accessed December 15, 2016).
Olshansky, S. J., D. J. Passaro, R. C. Hershow, J. Layden, B. A. Carnes, J. Brody, L. Hayflick, R. N. Butler, D. B. Allison, and D. S. Ludwig. 2005. A potential decline in life expectancy in the United States in the 21st century. New England Journal of Medicine 352(11):1138–1145.
Orszag, P. R., and T. J. Kane. 2003. Higher education spending: The role of Medicaid and the business cycle. https://www.brookings.edu/research/higher-education-spending-the-role-of-medicaid-and-the-business-cycle (accessed October 24, 2016).
Ortega, A. N., H. P. Rodriguez, and A. Vargas Bustamante. 2015. Policy dilemmas in Latino health care and implementation of the Affordable Care Act. Annual Review of Public Health 36:525–544.
Page, L. 2013. Will fee-for-service really disappear? Medscape. http://www.medscape.com/viewarticle/812672 (accessed November 17, 2016).
Plough, A., and A. Chandra. 2016. From vision to action: A framework and measures to mobilize a culture of health. Robert Wood Johnson Foundation. http://www.rwjf.org/content/dam/COH/RWJ000_COH-Update_CoH_Report_1b.pdf (accessed December 23, 2016).
Prevention Institute. 2016. Countering the production of health inequities: An emerging systems framework to achieve an equitable culture of health. Oakland, CA: The Prevention Institute.
Rastogi, S., T. D. Johnson, E. M. Hoeffe, and M. P. Drewery. 2010. The black population: 2010. U.S. Census Bureau.
Robinson, J. C. 2001. Theory and practice in the design of physician payment incentives. Milbank Quarterly 79(2):149–177.
Rudolph, L., S. Gould, and J. Berko. 2015. Climate change, health, and equity: Opportunities for action. Oakland, CA: Public Health Institute.
RWJF (Robert Wood Johnson Foundation). 2015. From vision to action: A framework and measures to mobilize a culture of health.
RWJF. n.d. What is a culture of health?http://www.evidenceforaction.org/what-culture-health (accessed October 24, 2016).
Saloner, B., L. Sabik, and B. D. Sommers. 2014. Pinching the poor? Medicaid cost sharing under the ACA. New England Journal of Medicine 370(13):1177–1180.
Seith, D., and E. Isakson. 2011. Who are America’s children: Examining health disparities among children in the U.S. New York: National Center for Children in Poverty.
Smeeding, T. 2012. Income, wealth, and debt and the Great Recession. Stanford, CA: Stanford Center on Poverty and Inequality.
Swift, A. 2015. Americans see healthcare, low wages as top financial problems. http://www.gallup.com/poll/181217/americans-healthcare-low-wages-top-financial-problems.aspx (accessed October 24, 2016).
Taveras, E. M., M. W. Gillman, K. P. Kleinman, J. W. Rich-Edwards, and S. L. Rifas-Shiman. 2013. Reducing racial/ethnic disparities in childhood obesity. JAMA Pediatrics 167(8):731–738.
Taylor, P., M. H. Lopez, J. Martinez, and G. Velasco. 2012. When labels don’t fit: Hispanics and their values of identity. Pew Hispanic Center. http://www.pewhispanic.org/2012/04/04/when-labels-dont-fit-hispanics-and-their-views-of-identity (accessed October 25, 2016).
The Housing Fund. 2015. The Housing Fund, Inc. wins $100,000 Wells Fargo next award for innovative strategy to improve consumer finance. http://thehousingfund.org/next-award (accessed October 24, 2016).
The National Commission on Physician Payment Reform. 2013. Report of the National Commission on Physician Payment Reform. Society of General Internal Medicine.
The President’s Task Force on 21st Century Policing. 2015. Final report of the President’s Task Force on 21st Century Policing. http://cops.usdoj.gov/pdf/taskforce/TaskForce_FinalReport.pdf (accessed October 18, 2016).
Uberoi, N., K. Finegold, and E. Gee. 2016. Health insurance coverage and the Affordable Care Act, 2010–2016. Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services.
Ubri, P., and S. Artiga. 2016. Disparities in health and health care: Five key questions and answers. http://files.kff.org/attachment/Issue-Brief-Disparities-in-Health-and-Health-Care-Five-Key-Questions-and-Answers (accessed October 24, 2016).
University of Wisconsin Population Health Institute. 2015. 2015 county health rankings: Key findings report. Madison: University of Wisconsin Population Health Institute.
Vang, Z. M., I. T. Elo, and M. Nagano. 2015. Preterm birth among the Hmong, other Asian subgroups and non-Hispanic whites in California. BMC Pregnancy and Childbirth 15:184.
Voorheis, J., N. McMaety, and B. Shor. 2015. Unequal incomes, ideology and gridlock: How rising inequality increases political polarization. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2649215 (accessed October 24, 2016).
Waidmann, T. A. 2009. Estimating the cost of racial and ethnic health disparities. Washington, DC: Urban Institute.
WHO (World Health Organization). 2010. A conceptual framework for action on the social determinants of health. Geneva: World Health Organization.
WHO. 2015. World health statistics 2015. Geneva, Switzerland: World Health Organization.
Williams, D. R., and V. Purdie-Vaughns. 2015. Social and behavioral interventions to improve health and reduce disparities in health. In Population health: Behavioral and social science insights. Rockville, MD: Agency for Healthcare Research and Quality and Office of Behavioral and Social Science Research.
Woolf, S. H., and P. Braveman. 2011. Where health disparities begin: The role of social and economic determinants—and why current policies may make matters worse. Health Affairs 30(10):1852–1859.
Woolf, S. H., L. Aron, L. Dubay, S. M. Simon, E. Zimmerman, and K. X. Luk. 2015. How are income and wealth linked to health and longevity? Washington, DC: Urban Institute and Virginia Commonwealth University.


























