
3
Cannabis: Prevalence of Use, Regulation, and Current Policy Landscape
PREVALENCE OF CANNABIS USE IN THE UNITED STATES (1975–2014)
The popularity of cannabis has ebbed and flowed over the past century. Despite being outlawed in several states in the early 1900s and being federally prohibited in 1937, cannabis remained relatively obscure until the 1960s, when an upsurge in use among adolescents and young adults brought the drug into the mainstream. Since the early 1970s, two surveys, the National Survey on Drug Use and Health (NSDUH) and Monitoring the Future, have provided nationally representative data on self-reported use of cannabis. The NSDUH (called the National Household Survey on Drug Abuse until 2002) has polled Americans 12 years of age and older since 1971, and Monitoring the Future has polled high school seniors since 1976, adding 8th- and 10th-graders in 1991 (CBHSQ, 2014; ICPSR, 2016). Both national surveys include questions that ask respondents whether they have ever used cannabis and if they have used cannabis within the past year or within the past 30 days. These data have been used to categorize users, with those reporting use within the past month often considered to be “active” or “current” users. Monitoring the Future also asks youth about how easily they could access cannabis, whether they approve of its use, and how risky they perceive it to be. Other national surveys of interest include the Centers for Disease Control and Prevention’s (CDC’s) Youth Risk Behavior Survey, which surveys the health-risk behaviors of
9th- through 12th-grade students on a biannual basis,1 and the CDC’s Behavioral Risk Factor Surveillance System,2 which collects state and local data regarding health-related risk behaviors, chronic health conditions, and the use of preventive services. It is of note that many surveillance surveys differ in their design and methodology, which often limits the ability to compare and compile data across studies.
The prevalence of cannabis use peaked in the late 1970s, when more than one-third of high school seniors (37 percent in 1976) and one in eight Americans over 12 years old (12.8 percent in 1979) reported past-month use (Johnston et al., 2016). Self-reported past-month use declined throughout the 1980s and by 1992 was just one-third of the 1970s peak, both among high school seniors (12.1 percent) and the general population (4.4 percent). The recorded decline in use did not last long. The mid-1990s saw rapid increases, with use by high school seniors nearly doubling within just the 5 years from 1992 (11.9 percent) to 1997 (23.7 percent). Throughout the late 1990s and early 2000s, the rates of use largely stagnated, with trends among youth and the general population moving roughly in parallel (Johnston et al., 2016).
The years since 2007 have seen steady year-over-year increases in general population past-month use, rising from 5.8 percent to 8.4 percent in 2014 (a 45 percent increase). There is no single clear explanation for the post-2007 increases in use. Hypothesized causes include declining potency-adjusted prices on the illicit market; the proliferation of medical cannabis laws, especially those that allow for sale at brick-and-mortar dispensaries; and changing public perceptions about the harms of cannabis use (Sevigny et al., 2014).
Today, cannabis is the most popular illicit drug in the United States (in terms of past-month users), trailed by prescription-type drugs used for nonmedical purposes, such as pain relievers (3.8 million), tranquilizers (1.9m), and stimulants (1.7m), and by prohibited drugs such as cocaine (1.9m), hallucinogens (1.2m), and heroin (0.3m) (CBHSQ, 2016a). A recent survey showed that the primary use of cannabis in the United States remains recreational (89.5 percent of adult cannabis users), with only 10.5 percent reporting use solely for medical purposes, and 36.1 percent reporting a mixed medical/recreational use (Schauer et al., 2016).
In 2015, an estimated 22.2 million of more than 265 million Americans 12 years of age or older reported having used cannabis in the past month (8.3 percent) (CBHSQ, 2016a). Cannabis use is most prevalent among
___________________
1 For additional information see: http://www.cdc.gov/healthyyouth/data/yrbs/results.htm (accessed January 6, 2017).
2 For additional information see: http://www.cdc.gov/brfss/about/index.htm (accessed January 6, 2017).
young people ages 18 to 25 (19.8 percent using in the past month) (CBHSQ, 2016a). Interestingly, since 2002 the use of cannabis has decreased among 12- to 17-year-olds, while it has markedly increased in the senior population, that is, those over 55 years (Azofeifa et al., 2016).
Males are nearly twice as likely (10.6 percent) to use cannabis as females (6.2 percent) (see Table 3-1). Black Americans use cannabis at the highest rate among major ethnic groups (10.7 percent), followed by whites (8.4 percent) and Hispanics (7.2 percent) (CBHSQ, 2016b). Use is also more common among lower-income Americans and those without college degrees (Davenport and Caulkins, 2016).
Different demographics have different rates of cannabis use. For example, dividing the population by age yields stark differences. Data from the Monitoring the Future survey show that more than one-fifth (21.3 percent) of high school seniors reported past-month use in 2015
TABLE 3-1 Past-Month Use Rates by Demographic
| Past-Month Use Rate (%) | |
|---|---|
| Ethnicity | |
| White, Non-Hispanic | 8.4 |
| African American, Non-Hispanic | 10.7 |
| Hispanic | 7.2 |
| Asian Non-Hispanic | 3.0 |
| Gender | |
| Male | 10.6 |
| Female | 6.2 |
| Education | |
| Less Than High School | 8.2 |
| High School Graduate | 9.1 |
| Some College | 10.5 |
| College Grad | 5.9 |
| Family Incomea | |
| Less than $10k | 13.6 |
| $20k–$29.9k | 9.7 |
| $50k–$74.9k | 7.8 |
| $75k + | 6.6 |
| Agea | |
| 12–17 | 7.1 |
| 18–25 | 20.1 |
| 26–34 | 13.0 |
| 35–49 | 7.1 |
| 50+ | 3.9 |
a Calculated with the Substance Abuse and Mental Health Services Administration’s (SAMHSA’s) public online data analysis system (PDAS). Crosstab: IRMJRC × CATAG3 (CBHSQ, 2016b).
SOURCE: Derived from CBHSQ, 2016b.
(Johnston et al., 2016). According to NSDUH data, past-month use is highest among 18- to 25-year-olds (19.8 percent) and lower in older groups. All age groups have shown increases in past-month cannabis use since 2002, with the sole exception of adolescents between agees 12 and 17, whose use in 2015 (7.0 percent) was lower than that reported in 2002 (8.2 percent) (CBHSQ, 2016a).
Volume and Intensity of Cannabis Use Today
A different and often overlooked picture of cannabis use is painted when it is measured in terms of volume or intensity of use rather than the prevalence of current users. The NSDUH survey asks past-month cannabis users how many days in the past 30 they have used “marijuana or hashish,” allowing researchers to measure the volume of use by aggregating reported use-days or by tracking the number of users who report use on more than 20 days in the past 30, termed heavy or “daily/near-daily” users.
Today, 22.2 million Americans 12 years of age and older report current cannabis use (defined as “users in the past 30 days”) (CBHSQ, 2016a). As a proportion of past-month users, heavy users have grown from roughly one in nine in 1992 to more than one in three (35.4 percent) in 2014, indicating an increased intensity of use among current users.3 Furthermore, the population of heavy users has not only become larger, it has also become older. Burns et al. note an inversion of the ratio of youth (ages 12–17) to older adults (ages 50 and older): in 2002, more than three times as many youths as older adults were using cannabis on a daily or near-daily basis; by 2011, 2.5 times as many adults as youth were daily or near-daily cannabis users (Burns et al., 2013).
Generally, the intensity of use correlates with use prevalence: groups with high prevalence tend to be the same as those with high intensity. But some groups are noticeable exceptions. For example, Americans with less than a high school education are less likely to report past-month use than Americans with a high school diploma or with a partial college education, but in terms of past-month use, those with less than a high school education are most likely to report daily/near-daily use (44.8 percent). Likewise, among age demographics, 26- to 34-year-olds report less past-month use than 18- to 25-year-olds do, but they report substantially more
___________________
3 Computed by NSDUH cross-tabs for 1992 and 2014. For 1992: https://www.icpsr.umich.edu/icpsrweb/ICPSR/series/64/studies/6887?archive=ICPSR&sortBy=7 (accessed January 6, 2017). Compute “MRJMON” against “MJDAY30A,” recoded as “MJDAY30A(r: 0-20;21-30).” For 2014: http://www.icpsr.umich.edu/cgi-bin/SDA/NAHDAP/hsda?nahdap+36361-0001 (accessed January 6, 2017). Compute “IRMJRC” against “MJDAY30A,” recoded as “MJDAY30A (r: 0-20;21-30).”
heavy use among current users (42.2 percent). Heavy use among past-month users is lowest among 12- to 17-year-olds (7.4 percent). Younger users tend to have lighter habits. According to Monitoring the Future data, in 2015, 6 percent of high school seniors who used cannabis in the past month reported use on a daily basis, as did 3 percent of 10th-graders and 1.1 percent of 8th-graders (Johnston et al., 2016).
One result of the increased intensity of use among past-month users is that the bulk of cannabis consumption is increasingly concentrated among a small number of heavy users. By one estimate, the one-third of current cannabis users that use daily or near daily accounted for two-thirds of the reported days of past-month use and three-quarters of expenditures (Davenport and Caulkins, 2016).
CANNABIS REGULATION IN THE UNITED STATES
In the United States at the turn of the 20th century, cannabis was generally used for medical rather than recreational purposes. As such, the production and use of cannabis was regulated by consumer safety laws such as the Pure Food and Drug Act of 1906, which required producers to disclose and label the quantity of cannabis present in any product sold as food or medicine. Although several U.S. states enacted bans on cannabis between 1911 and 1930, it escaped early federal prohibitions, such as the Harrison Act of 1914, which regulated opium and derivatives of the coca plant (Musto, 1999).
Fear of “marihuana,” as cannabis was beginning to be called, grew during the 1920s and 1930s as immigration from Mexico steadily increased in southwestern states. In the mid-1930s, the federal government, through the Federal Bureau of Narcotics, endorsed state-level actions and encouraged states to adopt the Marihuana Tax Act as a means to criminalize the unregistered and untaxed production and use of cannabis. National prohibition did not take shape, however, until Congress passed the Marihuana Tax Act of 1937, which regulated the production, distribution, and use of cannabis via Congress’s power to tax commerce. The act required those dealing with cannabis to register with federal authorities and pay a tax (Booth, 2005; Musto, 1999). The supply and use of the drug was not criminalized, but nonmedical supply or use was a violation and subject to a fine and imprisonment.
Today, cannabis is regulated by local, state, federal, and international law. State laws often mirror federal law, enshrined in the Comprehensive Drug Abuse Prevention and Control Act of 1970, which includes the Controlled Substances Act (CSA). The CSA modernized and consolidated earlier federal drug laws, making them consistent with international drug control conventions, specifically the United Nations Single Convention
on Narcotic Drugs of 1961, which the United States ratified (Caulkins et al., 2016). The CSA placed cannabis in Schedule I, the most restrictive category reserved for substances that have no currently accepted medical use, alongside heroin and lysergic acid diethylamide (LSD). The federal government does not recognize the medical use of cannabis, citing no evidence of the accepted medical use of herbal cannabis. It bears mentioning that pharmaceutical-grade cannabinoids have been isolated and are scheduled apart from cannabis. For example, tetrahydrocannabinol (THC) is sold as Marinol®, available with prescription (a Schedule III drug). That THC, which is the principal active ingredient in cannabis, in its pure form is listed in Schedule III indicates that the placement of botanical or whole cannabis in Schedule 1 may be driven by the lack of recognition of medical use for the whole plant.
Federal criminal law prohibits the supply and use of cannabis with exceptions for medical and scientific purposes. The enforcement of cannabis prohibition by federal authorities has focused on international smuggling and domestic crop eradication as well as violations on federal lands. The federal government has relied on state and local authorities to enforce criminal prohibitions on cannabis retail and use. In 2014 there were more than 1.5 million arrests for drug law violations,4 approximately 30,000 of which were made by the U.S. Drug Enforcement Administration (DEA).5 However, federal law remains an important factor in regulating cannabis. While the National Institutes of Health (NIH) have funded cannabis research—$111 million on 281 cannabinoid research projects in 2015 alone (NIH, 2016)—the federal government has restricted research on cannabis by licensing a single producer under contract with the National Institute on Drug Abuse (NIDA) and requiring multiple administrative reviews on research proposals (Caulkins et al., 2016) (see Chapter 15—Challenges and Barriers in Conducting Cannabis Research for additional information).6 Federal law also prohibits the importation of and intra- and interstate trade in cannabis. Tangentially, federal banking and commercial laws impede the development of commercial cannabis businesses. Though
___________________
4 As a noteworthy caveat, within the United States there is evidence of racial, social, and economic status–based disparities in the enforcement and issued penalties related to cannabis sale and use (Austin and Ressler, 2016). Within this context, it is important to acknowledge the potential impact of these laws on the health outcomes of disenfranchised communities.
5 See https://ucr.fbi.gov/crime-in-the-u.s/2014/crime-in-the-u.s.-2014/tables/table-29 (accessed January 6, 2017) and https://www.dea.gov/resource-center/statistics.shtml#arrests (accessed January 6, 2017).
6 In August 2016, NIDA announced a policy change intended to support an increase in the number of DEA-registered marijuana manufacturers. This change was designed to ensure a larger and more diverse supply of marijuana for U.S. Food and Drug Administration (FDA) authorized research purposes (DEA, 2016).
legal at the state level, the federal prohibition on cannabis prevents businesses from accessing the banking sector, precluding entrepreneurs from accessing lines of credit, electronic funds transfer, checking accounts, and other financial goods and services available to contemporary businesses. Federal tax code also prohibits cannabis businesses from deducting typical costs of business (Caulkins et al., 2015; Oglesby, 2015). In summary, the legal changes in cannabis policy during the past 50 years have been characterized primarily by three types of policies, each implemented by various states, beginning with (1) decriminalization throughout the 1970s, which preceded (2) medical cannabis laws and (3) regulated and licensed recreational cannabis.
Decriminalization of Possession and Use
States and localities perform most of the legwork involved in enforcing the criminal prohibition on cannabis as they arrest and convict the vast majority of offenders. Each state maintains its own set of laws that regulate the supply and use of the drug. In most cases, acts involving cannabis are subject to criminal prohibition, but sanctions vary considerably by state, each of which is constitutionally entitled to establish its own criminal codes and penalties.
The reduction of statutory penalties for use-related acts, including personal possession, is referred to as decriminalization or depenalization. About a dozen U.S. states are often described as having decriminalized possession in the 1970s (Pacula et al., 2005), beginning with Oregon in 1973. This move to reduce penalties on cannabis use halted until 2001 when Nevada decriminalized possession of small amounts of cannabis. Today, 21 states and the District of Columbia have decriminalized possession of small amounts of cannabis (Caulkins et al., 2016).
During the 1970s, the federal government briefly considered abolishing criminal sanctions for use-related acts. The 1972 National Commission on Marihuana and Drug Abuse, appointed by President Nixon, recommended that federal law be amended to decriminalize cannabis possession, use, and low-level retail (Shafer Commission, 1972). Those recommendations were rejected by the Nixon administration. President Carter raised the issue again in a 1977 speech to Congress, calling for federal decriminalization of cannabis possession, but his administration did not succeed in changing policies (Musto, 1999).
Medical Cannabis Laws
The next major shift in state cannabis policy in the United States was the enactment of medical cannabis laws. Starting in 1996 California
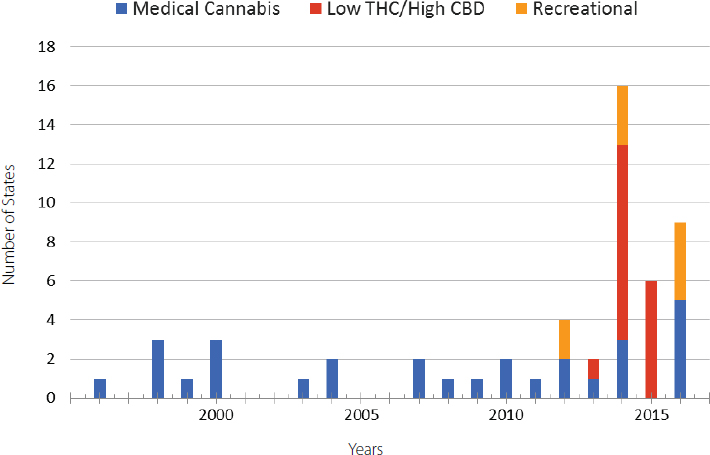
passed a popular referendum (Proposition 215) to allow individuals suffering from various illnesses to use herbal, whole plant cannabis, making California the first jurisdiction in the Western Hemisphere to legalize medical cannabis in some form. The law generally provides an affirmative defense for individuals using cannabis for medical purposes. Reforms at the state level continued in the waning years of the 20th century, with a handful of states passing laws to allow doctors to prescribe medical cannabis or allow for a legal defense for use of medical cannabis. The permission of use of the flower or products derived from the cannabis flower has now spread to 28 states and the District of Columbia. Another 16 states allow limited access to low-tetrahydrocannabinol (THC)/high-cannabidiol (CBD) products (NCSL, 2016). Figure 3-1 demonstrates that low-THC/high-CBD laws are a recent phenomenon.
Medical cannabis laws and policies vary greatly in terms of the regulations governing supply and use. Some are more restrictive than others, limiting the access of the drug to a certain class of individuals who suffer from certain illnesses or conditions, or establishing stricter limits on the production and distribution of the substance to at-home cultivation by patients and caregivers. Some states legally protect and regulate the
SOURCE: Adapted from NCSL, 2016.
operation of storefronts known as dispensaries. In these states, patients with a recommendation can enter stores and obtain a wide array of cannabis and cannabis products. Some dispensaries openly advertise their wares and services to patients at point of sale, with others aggressively promoting their business to the general public.
When it comes to the distribution of medical cannabis, some states, such as New York, restrict the sale of medical cannabis to non-smokable forms of the drug. Others require that patients register with the state and identify their source of cannabis. Even within states regulations may vary. Some states allow for local bans and municipal ordinances to help regulate additional aspects of the supply of cannabis.
Nonmedical, Adult Recreational Use
In 2010 California voted on legalizing recreational cannabis—in effect, permitting and regulating the supply and distribution of cannabis for adults to use nonmedically. Proposition 19 sought to repeal the state’s criminal prohibitions on cannabis, regulating it for recreational purposes for those over 21 years of age. The initiative failed, with 54 percent voting against. Two years later residents of Colorado, Oregon, and Washington went to the polls to vote on legalizing the adult recreational use of cannabis. Oregon’s initiative failed, with 53 percent of voters rejecting the measure7; however, Colorado and Washington State, after passing ballot initiatives in November 2012, became the first jurisdictions to legalize the large-scale commercial production of cannabis for recreational use for adults over 21, with Colorado also permitting home cultivation. In November 2014 similar initiatives were approved by voters in Alaska8 and Oregon. The District of Columbia took a narrower approach by legalizing only possession and home cultivation. The DC City Council subsequently attempted to permit and regulate a commercial market but was blocked by the U.S. Congress.
The liberalization of cannabis laws has been a gradual process. Early steps included medical cannabis, including the allowance and, sometimes, legal protection of dispensaries. Later, Alaska, Colorado, Oregon, and Washington State regulated the production and distribution of recreational cannabis by private, for-profit commercial actors along similar lines. Besides the general commercial design of these initiatives, the details of the regulations vary. Table 3-2 describes a few of the regula-
___________________
7 Oregon temporarily allowed sales of recreational cannabis through existing medical dispensaries beginning in October 2015, though licensed recreational stores are not expected to open until late 2016.
8 Alaska is expected to allow recreational cannabis sales in licensed stores by late 2016.
tory differences between Alaska, Colorado, Oregon, Washington, and the District of Columbia. With the exception of Washington State, all permit at-home cultivation. The District of Columbia follows a “grow and give” noncommercial model. None impose potency limits or require users to register.
In November 2016, California, Maine, Massachusetts, and Nevada voted to legalize adult measures related to recreational cannabis use
TABLE 3-2 Regulatory Differences Across Four States and the District of Columbia That Have Legalized Recreational Cannabis
| Alaska | Colorado | |
|---|---|---|
| Legal Process | Voter initiative, state statute | Voter initiative, amendment to state constitution |
| When Passed | November 2014 | November 2012 |
| When Implemented | February 2015: Personal possession, consumption, cultivation Late 2016 (expected): Retail sales |
December 2012: Personal possession, consumption, cultivation January 2014: Retail sales |
| Regulatory Authority | Marijuana Control Board (Alcoholic Beverage Control Board) | Marijuana Enforcement Division (Department of Revenue) |
| Minimum Age | 21 | 21 |
| Residency Requirement | None | None |
| Personal Possession Quantity | 28.5 g | 28.5 g |
| Home Cultivation | 6 plants, 3 of which can be flowering | 6 plants, 3 of which can be flowering |
| Interpersonal Sharing | 28.5 g | 28.5 g |
| Retail Transaction Limit | 28.5 g | Residents: 28.5 g Non-residents: 7 g |
| Retail Pricing Structure | Market | Market |
| Average Retail Price per Gram After Tax | No retail stores currently | $11.50 |
| Maximum THC Content | None | None |
and possession (NORML, 2016). Arkansas, Florida, Montana, and North Dakota voted in favor of medical marijuana initiatives. In order to develop and enforce regulations for a recreational cannabis industry, each state has appointed a regulatory agency. Alaska, Oregon, and Washington State delegated this responsibility to existing alcohol authorities, while Colorado expanded the responsibilities of the Medical Marijuana Enforcement Division under the Department of Revenue. To aid in drafting rules fol-
| Oregon | Washington | District of Columbia |
|---|---|---|
| Voter initiative, state statute | Voter initiative, state statute | Voter initiative |
| November 2014 | November 2012 | November 2014 |
| July 2015: Personal possession, consumption, cultivation October 1, 2015: Retail sales via medical dispensaries Late-2016 (expected): retail sales through licensed retailers |
December 2012: Personal possession, consumption July 2014: Retail sales |
February 2015: Personal possession, consumption, cultivation |
| Oregon Liquor Control Commission | Liquor and Cannabis Board (formerly the Liquor Control Board) | Not applicable |
| 21 | 21 | 21 |
| None | None | None |
| In public: 28.5 g At home: 228 g |
28.5 g | 57 g |
| 4 plants in flower | Not allowed | 6 plants per person 12 plants per household, 3 of which can be flowering |
| 28.5 g | Not allowed | 28.5 g |
| 7 g | 28.5 g | Not applicable |
| Market | Market | Not applicable |
| $10.00 | $10.00 | Not applicable |
| None | None | None |
| Alaska | Colorado | |
|---|---|---|
| Registration Requirements | None | None |
| Advertising | Final advertising regulations to be determined by the Alaska Department of Health and Social Services Division of Public Health | Restricted to media with no more than 30 percent of the audience under the age of 21 |
| Taxation | $50 excise tax per ounce on sales or transfers from cultivation facility to retail store or product manufacturer | 15 percent excise tax on cultivation; 10 percent retail marijuana sales tax; 2.9 percent state sales tax; local sales taxes |
| Cannabis Clubs | Not explicitly allowed or prohibited; ban on in-store consumption repealed in November 2015 | Not allowed |
| Medical Cannabis | 2000: Patient registry, possession, home cultivation | 2000: Patient registry, possession, consumption 2010: Commercial production and sales |
SOURCE: Adapted from UNODC World Drug Report 2016 (UNODC, 2016).
lowing the passage of their initiatives, state agencies held public hearings and working groups to solicit public input (Pardo, 2014).
The federal government has not challenged these state laws by invoking the supremacy clause of the U.S. Constitution. However, under the 10th Amendment, as reaffirmed by U.S. jurisprudence, the federal government cannot force a state to criminalize an act under state law (Garvey and Yeh, 2014). When the voters of these states passed initiatives to legalize, regulate, and tax recreational cannabis, they simultaneously repealed the penal provisions and sanctions prohibiting and criminalizing unauthorized cultivation, trafficking, and possession of cannabis. Under the Obama administration, the federal government seems to have opted for a more pragmatic solution which allows for a rules-based cannabis industry, as dictated by state regulations, while maintaining the future option to preempt.
| Oregon | Washington | District of Columbia |
|---|---|---|
| None | None | None |
| Entry sign required on exterior of dispensaries; Oregon Liquor Control Commission has authority to further regulate or prohibit advertising | Limited to one sign for retailers at business location | Not applicable, no commercial market |
| October–December 2015: No tax on retail sales; after January 5, 2016: 25 percent sales tax | July–June 2014: 25 percent tax at each stage (production, processing, retail) July 2015: 37 percent sales tax | Not applicable, no commercial market |
| Not allowed | Not allowed | Not allowed; currently under investigation by city task force. |
| 1999: Patient registry, possession, home cultivation | 1999: Possession 2012: Home cultivation, no patient registry |
2011: Patient registry |
POLICY LANDSCAPE
Most researchers recognize that a growing general public acceptance of the drug for medical and recreational purposes has been encouraging the changes at the state level. It remains to be seen if cannabis will be legalized at the national level or if such public opinion will continue. In 2015, according to a Gallup tracker poll, 58 percent of Americans favored legalizing cannabis, marking the third straight year that cannabis legalization found majority support (Gallup, 2015). Given that a large percentage of the U.S. population lives in states that permit some degree of access to THC-containing compounds via either the medical or the recreational market, it is important to examine the current policy landscape, which may shape future state and federal regulations of cannabis.
State-Level Changes
State-Regulated Use
Cannabis policy change has occurred at the state level in large part due to changing public sentiment. Many states have reformed their cannabis laws, not from a deliberative legislative process but through popular referendums. As discussed earlier, states have passed laws to allow qualifying individual’s access to medical cannabis. These laws can be broadly divided into three distinct categories: loose medical, restricted access, and non-THC.
Some of the earliest laws passed—and the laws generally found in most states west of the Mississippi River—are referred to as loose medical. In states with these policies, access to medical cannabis is not strictly limited to provable qualifying ailments, such as terminal cancer, HIV/AIDS, or glaucoma. A patient may access medical cannabis when his or her physician deems it necessary, and in some jurisdictions this amounts to little more than de facto legalization of recreational use. One study that surveyed more than 4,000 individuals seeking access to medical cannabis in California concluded that the typical patient was a white male in his early 30s who started using cannabis in his teens with fewer reported disabilities than the national average (O’Connell and Bou-Matar, 2007). Under restricted access, patients must meet certain qualifying criteria (such as a qualifying medical condition) or are restricted to what types of medical products are available, or both. For example, New York prohibits the use of smokable herbal cannabis, allowing only tinctures, oils, concentrates, and other forms of products. Non-THC laws permit the use of no-THC or low-THC/high-CBD products, such as CBD oil, to treat a short list of qualifying conditions, such as refractory epilepsy. This category is by far the most restrictive, and states that adopt these non-THC policies generally prohibit the supply and distribution of such products, granting only a legal defense for their use.
That said, 28 states and the District of Columbia fall in one or the other of the first two categories and allow for loose or restricted medical use, where patients may access some form of THC-containing compound. Sixteen states fall in the non-THC category. A total of 44 states and the District of Columbia have amended their laws to allow for some form of medical cannabis (NCSL, 2016) (see Figure 3-2).
Of all the jurisdictions that allow for some sort of access to THC-containing compounds, cancer, HIV/AIDS, multiple sclerosis, and glaucoma are among the most recognized qualifying ailments (NCSL, 2016). And examination of all jurisdictions shows that most list seizures and epileptic seizures within their statutes (NCSL, 2016). However, several states are open in their interpretation, allowing for medical cannabis to
be used to treat any illness for which the drug provides relief. Since few states maintain medical cannabis patient registries, the committee relied on data on the percentage of patients reporting certain qualifying illnesses in Oregon and Colorado (see Figure 3-3). As can be seen in the figure, the overwhelming majority obtained a recommendation on the basis of a claimed need to treat pain.
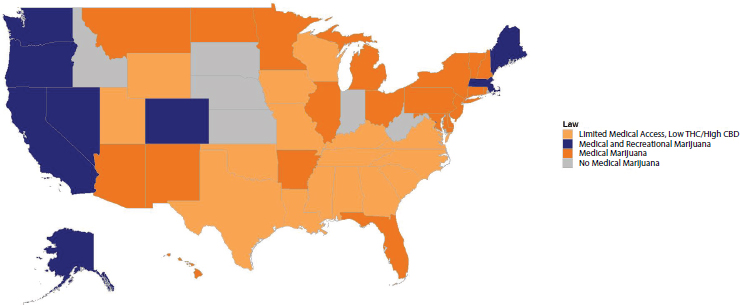
SOURCE: Adapted from NCSL, 2016.
State Research on Therapeutic Effects
In addition to state-level legal changes that regulate cannabis for either medical or recreational purposes, a few states have sought to expand research into cannabis’s therapeutic effects. The Center for Medicinal Cannabis Research (CMCR) at the University of California was created in 2000 to conduct clinical and preclinical studies of cannabinoids, including smoked cannabis, for conditions for which cannabis may be beneficial. With state funding, the CMCR approved 21 federally approved studies: 13 have been completed, and 6 have been discontinued (CMCR, 2016).
Departing from this, Colorado has started to conduct research into the medicinal value of cannabis that is neither federally funded nor federally approved. In 2014 Colorado passed legislation to promote research into cannabis’s medical benefits, creating the Medical Marijuana Scientific Advisory Council and appropriating $9 million in research grants. The advisory council approves research grants and evaluates research. As of early 2015, nine research grants have been approved, with six studies cur-
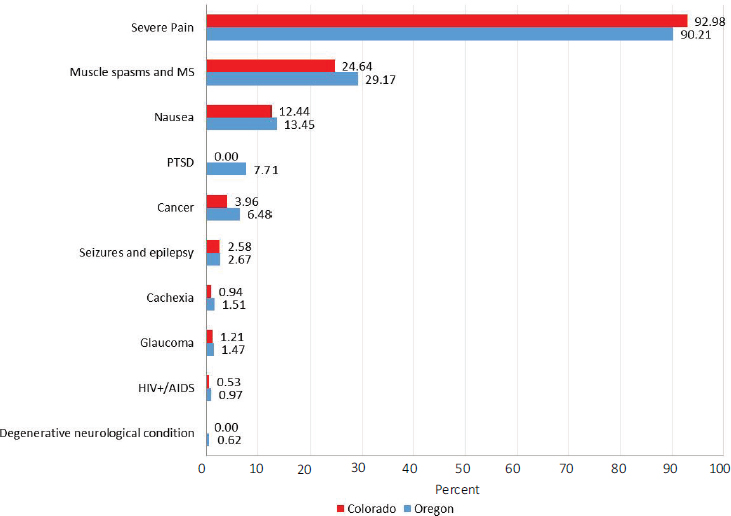
NOTE: Patients may report multiple qualifying ailments.
SOURCES: Adapted from CDPHE, 2016; OHA, 2016.
rently under way.9 Also in 2015, NIH provided $111 million in funding for 281 cannabinoid-related research efforts nationwide (NIH, 2016).
EXECUTIVE BRANCH POLICIES
Federal Regulated Use
As discussed earlier, the executive branch of the federal government has extensive influence and impact when it comes to regulating cannabis. Despite the complex domestic arrangements established by the U.S. Constitution and the current political climate, the executive branch has not challenged state-level laws that are in violation with federal drug laws. The Obama administration has issued a series of federal guidelines for
___________________
9 See the Colorado Department of Public Health and Environment’s Medical Marijuana Scientific Advisory Council: https://www.colorado.gov/pacific/cdphe/approved-medical-marijuana-research-grants (accessed January 6, 2017).
states that are reforming cannabis laws, granting limited space for such policies.
In 2009 the U.S. Department of Justice issued a policy memo declaring that it was not the federal government’s intent to prosecute individuals who abide by state medical cannabis laws (Ogden, 2009). That policy was later updated in August 2013 following the legalization of nonmedical cannabis in Colorado and Washington State. The current policy guidelines outline eight enforcement criteria whereby the federal government may intervene and prosecute an individual or group for violating the Controlled Substances Act (Cole, 2013). Furthermore, the U.S. Department of Justice stated that it expects states that have legalized cannabis to implement robust systems of enforcement and regulation to protect public health and safety; however, recent evaluations of the policy guidelines suggest that the U.S. Department of Justice has done little to evaluate how states comply with federal priorities (GAO, 2016).
Because cannabis is still federally prohibited, laws that govern other aspects of commerce—namely, banking and finance—have prevented businesses that deal in cannabis from accessing lines of credit or banking (McErlean, 2015). Money laundering laws and the CSA prevent many banks from interacting with cannabis businesses. In order to ease this conflict, the U.S. Department of the Treasury, through the Financial Crimes Enforcement Network (FinCEN), has issued a directive to financial establishments allowing them to deal with cannabis businesses that comply with state laws (FinCEN, 2014).
Federal Research
Despite ongoing federal funding for cannabinoid research ($111 million in 2015 alone), cannabis researchers have found federal research funds to be restricted and limited. Research proposals were required to undergo a thorough and rigorous assessment by the DEA, NIDA, the FDA, and the U.S. Department of Health and Human Services (HHS). If they were federally approved, researchers were limited in the type and quantity of cannabis available from the University of Mississippi, which was contracted by NIDA to act as the only licit supply of the drug for research. (See Chapter 15—Challenges and Barriers in Conducting Cannabis Research for additional information.) In 2015 the Obama administration, via HHS and the DEA, relaxed some regulatory restrictions, eliminating duplicative reviews of research proposals by the HHS as well as increasing the amount of cannabis available for research by raising the aggregate production quota of cannabis cultivated at the University of Mississippi (DEA, 2016).
In August 2016 the DEA denied a petition to reschedule cannabis to
Schedule II, citing that cannabis has no currently accepted medical use in treatment in the United States (DEA, 2016). The administration did, however, adopt a new policy to end the NIDA-contracted monopoly of research-grade cannabis by the University of Mississippi. Under new rules, the DEA will facilitate cannabis research by increasing the number of private entities allowed to cultivate and distribute research-grade cannabis (DEA, 2016).
CONGRESSIONAL BRANCH POLICIES
Recently the 113th Congress used its regulatory powers to shape cannabis policy at both the state and the subnational level. In the Consolidated and Further Continuing Appropriations Act of 2015 (Public Law No. 113-235), lawmakers precluded the U.S. Department of Justice from using fiscal year 2015 appropriated funds to enforce the Controlled Substances Act to prevent states from implementing their own laws that authorize the use, distribution, possession, or cultivation of medical cannabis (Sec 538). In the same piece of legislation, Congress precluded the District of Columbia from using appropriated funds to regulate, legalize, or otherwise reduce penalties for the possession, distribution, or use of any Schedule I substance, effectively blocking any citywide effort to regulate the trade in cannabis (Sec 908b). During the same session, Congress authorized the Secretary of Agriculture to promulgate rules to ensure that medical cannabis costs are not treated as a deduction in Supplemental Nutrition Assistance Program (SNAP) benefits as well as allowing universities and state departments of agriculture to cultivate industrial hemp for research purposes (Garvey et al., 2015).
Members of the current 114th Congress have proposed several pieces of legislation on cannabis. Some would remove cannabis from the Controlled Substances Act and treat the drug like alcohol. Others would end the civil asset forfeiture of real property of businesses that comply with state medical cannabis laws or authorize the U.S. Department of Veterans Affairs to offer recommendations regarding veterans’ use of cannabis in compliance with state regimes. One bill in particular, the Medical Marijuana Research Act, has gained bipartisan support from proponents and opponents of cannabis reform in Congress. The bill would increase cannabis research by making the drug and plant more accessible to researchers.
PUBLIC OPINION
Public opinion toward cannabis seems to be driving many of the policy changes that have taken place to date. Cannabis found mainstream market appeal in the late 1960s and early 1970s, and, as a result, polling
agencies started surveying the public opinion about the drug. In 1969 the Gallup Poll began asking Americans if they thought that the “use of cannabis should be made legal,” and the company has continued to ask Americans the same question for nearly 50 years.10
Gallup poll responses showed that support for legal cannabis use increased to 28 percent in 1977 (the same year President Carter called for national decriminalization). For about 20 years, support declined and then plateaued at around 24 percent, only to inch upward 4 years after California passed legislation in favor of medical cannabis. By 2000, 31 percent of respondents favored legal use. Over the past 6 years support has vacillated, but it averaged 48 percent from 2010 through 2012 and has averaged 56 percent since 2013. In 2015, 58 percent of respondents favored legal use.
Polling shows that the public is overwhelmingly in favor of the use of cannabis for medical purposes if prescribed by a doctor. No other company has tracked public opinion concerning medical cannabis over time in the same way as the Gallup Poll, but a collection of national surveys from ProCon indicate that since 1998, 60 to 85 percent of Americans have been supportive of the use of medical cannabis (ProCon, 2016). In a recent poll by Quinnipiac, 89 percent of respondents supported medical cannabis (Quinnipiac, 2016). However, it is of note that states attribute different medicinal value to different forms of the drug, restricting who can access what part of the plant. National surveys may not capture these distinctions that are made in state-level law or policy. Yet, the general shift over time suggests that the public is welcoming some changes in cannabis policy and law. There appears to be greater agreement that cannabis should be available as a medicine to those with certain qualifying conditions, but it is harder to find similar political agreement on recreational cannabis. It is unclear whether the wording of the Gallup Poll’s public opinion question paints an accurate picture of the current and ongoing sentiment with respect to states that are legalizing recreational cannabis.
POLICY AND RESEARCH
The political landscape for the commercialization, decriminalization, and use of cannabis is constantly evolving. As federal and state agencies continue to grapple with these important public policy issues, it is important to consider that each political decision may have significant public health implications.
___________________
10 It should be noted that the question is somewhat vague, implying “legalization” but referring to “use” of cannabis, not the legal production and distribution of the drug. This ambiguity may cloud respondents’ answers.
As laws and policies continue to change, research must also. Unfortunately, research on the health effects and potential therapeutic potential of cannabis use has been limited in this country, despite enormous changes at the state level. As such, there is currently limited research evidence to guide policy. This lack of aggregated knowledge is a significant impediment not only to the scientific understanding of cannabis but also to the advancement of public policy and the nation’s overall public health.
REFERENCES
Austin, W., and R. W. Ressler. 2016. Who gets arrested for marijuana use? The perils of being poor and black. Applied Economics Letters [Epub May 4, 2016], 1–3.
Azofeifa, A., M. E. Mattson, G. Schauer, T. McAfee, A. Grant, and R. Lyerla. 2016. National estimates of marijuana use and related indicators—National Survey on Drug Use and Health, United States, 2002–2014. Morbidity and Mortality Weekly Report 65(SS-11):1–25.
Booth, M. 2005. Cannabis: A history. New York: St. Martin’s Press (Macmillan Publishers).
Burns, R. M., J. P. Caulkins, S. S. Everingham, and B. Kilmer. 2013. Statistics on cannabis users skew perceptions of cannabis use. Front Psychiatry 4:138.
Caulkins, J. P., B. Kilmer, M. Kleiman, R. J. MacCoun, G. Midgette, P. Oglesby, R. L. Pacula, and P. H. Reuter. 2015. Considering marijuana legalization. http://www.rand.org/content/dam/rand/pubs/research_reports/RR800/RR864/RAND_RR864.pdf (accessed November 22, 2016).
Caulkins, J. P., B. Kilmer, A. Hawken, and M. Kleiman. 2016. Marijuana legalization: What everyone needs to know. New York: Oxford University Press.
CBHSQ (Center for Behavioral Health Statistics and Quality). 2014. National Survey on Drug Use and Health (NSDUH): Summary of methodological studies, 1971–2014. Rockville, MD: Substance Abuse and Mental Health Services Administration.
CBHSQ. 2016a. Key substance use and mental health indicators in the United States: Results from the 2015 National Survey on Drug Use and Health. Rockville, MD: Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR1-2015/NSDUH-FFR1-2015/NSDUH-FFR1-2015.pdf (accessed January 9, 2017).
CBHSQ. 2016b. 2015 National Survey on Drug Use and Health: Detailed tables. Rockville, MD: Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015.pdf (accessed December 27, 2016).
CDPHE (Colorado Department of Public Health and Environment). 2016. Medical Marijuana Registry Program statistics, July 31, 2016. https://www.colorado.gov/pacific/sites/default/files/CHED_MMR_Monthly_Report_Statistics_July_2016.pdf (accessed October 12, 2016).
CMCR (Center for Medical Cannabis Research). 2016. Research: Active studies, pending studies, completed studies, discontinued studies. http://www.cmcr.ucsd.edu (accessed December 16, 2016).
Cole, J. M. 2013. Memorandum for all United States attorneys. August 29. https://www.justice.gov/iso/opa/resources/3052013829132756857467.pdf (accessed November 10, 2016).
Davenport, S., and J. P. Caulkins. 2016. Evolution of the United States marijuana market in the decade of liberalization before full legalization. Journal of Drug Issues 46(4):411–427.
DEA (U.S. Drug Enforcement Administration). 2016. DEA announces actions related to marijuana and industrial hemp. https://www.dea.gov/divisions/hq/2016/hq081116.shtml (accessed November 10, 2016).
FinCEN (Financial Crimes Enforcement Network). 2014. BSA expectations regarding marijuana-related businesses. February 14. https://www.fincen.gov/sites/default/files/shared/FIN-2014-G001.pdf (accessed November 10, 2016).
Gallup (Gallup Tracking Poll). 2015. In U.S., 58% back legal marijuana use. http://www.gallup.com/poll/186260/back-legal-marijuana.aspx (accessed December 17, 2016).
GAO (U.S. Government Accountability Office). 2016. State marijuana legalization: DOJ should document its approach to monitoring the effects of legalization. February 1. GAO-16-1. http://www.gao.gov/products/GAO-16-1 (accessed November 10, 2016).
Garvey, T., and B. T. Yeh. 2014. State legalization of recreational marijuana: Selected legal issues. Congressional Research Service, January 13. https://fas.org/sgp/crs/misc/R43034.pdf (accessed November 10, 2016).
Garvey, T., C. Doyle, and D. H. Carpenter. 2015. Marijuana: Medical and retail—Selected legal issues. Congressional Research Service. April 8. https://fas.org/sgp/crs/misc/R43435.pdf (accessed November 10, 2016).
ICPSR (Interuniversity Consortium for Political and Social Research). 2016. Monitoring the Future (MTF) Series. https://www.icpsr.umich.edu/icpsrweb/ICPSR/series/35 (accessed January 9, 2017).
Johnston, L. D., P. M. O’Malley, R. A. Miech, J. G. Bachman, and J. E. Schulenberg. 2016. Monitoring the Future: National survey results on drug use, 1975–2015: Overview: key findings on adolescent drug use. Ann Arbor: Institute for Social Research, University of Michigan.
McErlean, E. D. 2015. The real green issue regarding recreational marijuana: Federal tax and banking laws in need of reform. DePaul Law Review 64(4):1079–1118.
Musto, D. F. 1999. The American disease: Origins of narcotic control. New York: Oxford University Press.
NCSL (National Conference of State Legislatures). 2016. State medical marijuana laws. November 9. http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx (accessed November 10, 2016).
NIH (National Institutes of Health). 2016. NIH research on marijuana and cannabinoids. https://www.drugabuse.gov/drugs-abuse/marijuana/nih-research-marijuana-cannabinoids (accessed December 16, 2016).
NORML. 2016. Election 2016—Marijuana Ballot Results. http://norml.org/election-2016 (accessed December 22, 2016).
O’Connell, T. J., and C. B. Bou-Matar. 2007. Long term marijuana users seeking medical cannabis in California (2001–2007): Demographics, social characteristics, patterns of cannabis and other drug use of 4,117 applicants. Harm Reduction Journal 4(1):16.
Ogden, D. 2009. Memorandum for selected United States attorneys on investigations and prosecutions in states authorizing the medical use of marijuana. October 19. https://www.justice.gov/opa/blog/memorandum-selected-united-state-attorneys-investigations-and-prosecutions-states (accessed November 10, 2016).
Oglesby, P. 2015. Supplemental thoughts about revenue from marijuana in Vermont (January 16, 2015). https://ssrn.com/abstract=2551029 or http://dx.doi.org/10.2139/ssrn.2551029 (accessed December 16, 2016).
OHA (Oregon Health Authority). 2016. Oregon Medical Marijuana Program Statistical Snapshot July, 2016. https://public.health.oregon.gov/DiseasesConditions/ChronicDisease/MedicalMarijuanaProgram/Documents/OMMP-Statistical-Snapshot%20-07-2016.pdf (accessed October 12, 2016).
Pacula, R. L., R. MacCoun, P. Reuter, J. Chriqui, B. Kilmer, K. Harris, L. Paoli, and C. Schäfer. 2005. What does it mean to decriminalize marijuana? A cross-national empirical examination. Advances in Health Economics and Health Services Research 16:347–369.
Pardo, B. 2014. Cannabis policy reforms in the Americas: A comparative analysis of Colorado, Washington, and Uruguay. International Journal of Drug Policy 25(4):727–735.
ProCon (ProCon.org). 2016. Votes and polls, national. http://medicalmarijuana.procon.org/view.additional-resource.php?resourceID=000151 (accessed December 10, 2016).
Quinnipiac (Quinnipiac University Poll). 2016. Allow marijuana for vets with PTSD, U.S. voters say 10-1, Quinnipiac University national poll finds; slim majority says legalize marijuana in general. https://poll.qu.edu/national/release-detail?ReleaseID=2354 (accessed December 16, 2016).
Schauer, G. L., B. A. King, R. E. Bunnell, G. Promoff, and T. A. McAfee. 2016. Toking, vaping, and eating for health or fun: Marijuana use patterns. American Journal of Preventive Medicine 50(1):1–8.
Sevigny, E. L., R. L. Pacula, and P. Heaton. 2014. The effects of medical marijuana laws on potency. International Journal on Drug Policy 25(2):308–319.
Shafer Commission. 1972. Marijuana: Signal of misunderstanding. First Report of the National Commission on Marijuana and Drug Abuse. Washington, DC: U.S. Government Printing Office.
UNODC (United Nations Office on Drugs and Crime). 2016. World Drug Report 2016. United Nations publication, Sales No. E.16.XI.7.
This page intentionally left blank.
























