
4
Real-World Business Cases for High-Value CPD
Transitioning from a broad discussion about the value proposition and how to define the elements of a business case, the workshop turned to concrete, real-world business cases for high-value continuing professional development (CPD) projects. There were four real-world cases presented,
followed by a discussion among the presenters and the workshop participants. For each case, the presenters described how the project was developed and implemented, and whether and how a business case was made for the project. Presenters discussed the outcomes of the projects, and offered reflection and lessons learned from the experiences.
SEPSIS CARE TRAINING
Lucy Savitz, Intermountain Healthcare
Savitz told workshop participants about her experience developing and implementing a CPD program for sepsis care at Intermountain Healthcare, a fully integrated delivery system in Salt Lake City, Utah. She noted that making the business case for high-value CPD at Intermountain may be “a little easier” than other health care organizations because Intermountain views CPD as “a responsibility of the delivery system.” This view, she added, is rooted in the notion that a clinician “will have to relearn their profession at least six different times” over the course of a career, and that it is “almost physically impossible” for busy professionals to keep up with new findings in the field on their own.
Sepsis is the leading cause of in-hospital mortality in the United States, and there is strong evidence that early identification and treatment of sepsis saves lives. However, Savitz went on to say there is a rapidly changing evidence base about sepsis, and some physicians have raised questions about the sepsis bundle (a set of evidence-based best practices that give maximum outcome benefit when instituted together).1 To improve sepsis care, the High Value Healthcare Collaborative (HVHC), of which Intermountain is a member, developed and tested a sepsis training program in emergency departments, inpatient units, and intensive care units. The objective of the program was to implement the 3-hour sepsis bundle reliably across these different patient care settings, said Savitz. The HVHC members—12 health delivery organizations across the country from Hawaii to New York City—worked collaboratively, but each implemented and tailored the sepsis program to their own unique systems and communities. Savitz said that differences between the communities include cultural issues, state regulations, payer mixes, and patient populations, all of which can affect the implementation of the program and “how you sell [the] business case locally.” For example, in Utah, state regulations require that nurses be paid overtime for training; this cost must be accounted for in a Utah business plan, but it may not apply in other states.
___________________
1 See https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2888324 (accessed November 2, 2017).
In describing the business case for the sepsis program, Savitz laid out some of the benefits and costs of implementation (see Table 4-1), and noted that one of the challenges was accounting for the indirect and intangible costs and benefits. For example, “increased positive patient experience” is a benefit of the sepsis program, but it is difficult to quantify or determine a dollar value for the benefit. Savitz said they were able to “sell” this benefit by theorizing that increased patient satisfaction would lead to increased patient loyalty and repeat business for the system. Savitz also noted that the business plan incorporates not only outcome measures but also process measures. Because some of the outcomes—for example, patient mortality—may be far removed from the time of training, the plan includes process measures such as compliance with the bundle or a decrease in time to treat. Including both outcome and process measures allows a delivery system to evaluate the progress that is being made. Regarding the costs of the program, Savitz noted that the collaboration between HVHC members reduced the costs and burdens of developing the program. For example, HVHC built an Internet platform for sharing resources; this enabled members to download training materials and substitute their own logo, rather than each organization spending time and money to create unique materials.
Savitz concluded her presentation with the story of the “Lipstick Lady.” At one health care delivery organization that Savitz visited, many providers
TABLE 4-1 Benefits and Costs of the Sepsis Care Training Program (from Savitz abstract)
| Benefits | Costs | |
|---|---|---|
| Decreased in-hospital mortality | Developing and testing training materials | |
| Decreased length of stay | Maintaining training materials | |
| Decreased ICU days | Staff time in training | |
| Increased discharge disposition to home | Analytic time to produce reports** | |
| Increased staff morale* | Chart abstraction time | |
| Increased positive patient experience | Dedicated staff time | |
| (Future) avoided payment penalty | Decision support tool development | |
| Increased bundle compliance (process) | EHR programming—CDS | |
| Decreased time to treat (process) | Refresher training/reinforcement | |
NOTE: CDS = clinical decision support; EHR = electronic health record; ICU = intensive care unit.
* “Lipstick Lady” example and decreased turnover.
** Value of measurable feedback.
SOURCE: Presented by Lucy Savitz, April 6, 2017.
shared the same story: a woman in the emergency department was identified and treated for sepsis early, and at the time she was supposed to be transferred to the intensive care unit (ICU), she was sitting up in her gurney applying lipstick. Savitz said that despite all the data that are gathered in support of CPD programs, these types of real-life patient stories are what serve as “enormous proof of the work and the value” of CPD. After seeing the Lipstick Lady survive and thrive after early sepsis intervention, “nobody was asking questions” about the value of these training programs.
PHYSICAL THERAPY RESIDENCY
Mark Bowden, Medical University of South Carolina
The Medical University of South Carolina (MUSC) has been in the process of developing a neurologic residency program for doctors of physical therapy over the last 4 years, said Bowden, director of the Division of Physical Therapy at MUSC. Physical therapy residencies, unlike medical residencies, are not part of the formal training process and have no external funding sources. Bowden explained that a physical therapy residency is a “voluntary program that individuals take up postprofessionally to . . . improve as clinicians.” He noted that while some participants of the residency may end up taking the neurologic clinical specialization exam, passing this exam is not the point of the residency. The goal is to alter clinical decision making and help participants become better therapists. That said, the exam does serve as a measurable by-product of the residency program.
Bowden commented that initially, there was no business model for the residency program. It was seen as an opportunity to improve education and clinical practice, and ultimately, to improve patient care. However, it soon became clear that funding would not be available for the residency program. Developing a business model and showing the value of the program became the only way to make the program a reality. To begin the process, four business students performed a survey of physical therapy students and recent graduates to learn about overall interest in a residency and the limitations to implementation. The survey revealed that 79 percent of students and 61 percent of therapists were either somewhat interested or highly interested in pursuing a residency. However, 94 percent of survey respondents were concerned about assuming the costs of the residency, and 56 percent were reluctant to relocate for the purpose of pursuing a residency.
In response to these concerns, the residency was designed in such a way that the tuition was covered by the employer, there was no relocation involved, there were minimal losses to productivity, and—perhaps most importantly to the business case—the program maintained revenue neutrality to MUSC while maximizing the investment of clinical partners.
The residency includes 64 hours of intensive study in Charleston (over four weekends), 120 hours of additional online content and interactive education, 160 hours of one-on-one mentoring, and three site visits by program faculty to observe the resident as well as resident–mentor interactions.
The mentorship requirement is a critically important part of the residency program, with mentors serving as “extensions of the faculty,” said Bowden. The relationship is collaborative rather than unidirectional, and the mentor helps facilitate the development of advanced professional behaviors, proficiency in communications, and consultation skills. To serve as a mentor, the therapist must complete an online mentorship certification course, participate in ongoing mentorship training, and have a specialty certification or at least 3 years in neurologic physical therapy. Mentors are invited to participate in all didactic learning opportunities and must be familiar with the content in order to reinforce the material with residents during patient care.
Over the last 4 years, the program has had 21 residents participate in seven different states. The hospitals that have hosted residents have seen dramatic benefits. One site, AnMed Health Rehabilitation Hospital, used to have difficulty recruiting therapists, with positions open for as long as 6 months, and recruitment and startup costing as much as $20,000. After it implemented the residency, the hospital’s recruitment and startup costs decreased to $3,000, and there is now a waiting list for new position openings. Three out of the last four hires sought the hospital out directly because of the residency opportunity, Bowden said. In addition, the hospital has seen improvements in patient care and patient satisfaction, with average length of stay decreasing by more than 2.5 days, improvements in a standardized measure for inpatient rehabilitation, and a higher discharge rate to the community. MUSC has seen benefits as well, with the creation of a revenue stream for Division of Physical Therapy strategic planning, creation of clinical education sites for their entry-level doctor of physical therapy students, and the development of clinical partners for comparative effectiveness and pragmatic clinical trials.
Bowden told workshop participants about plans to improve the business model and quantify the impact of the residency, including
- calculating the cost savings that are associated with shortening length of stay;
- expanding the outcomes data collected to include physical performance, patient satisfaction, and quality of life;
- developing a metric for “value” that includes costs, outcomes, and patient satisfaction data; and
- calculating costs per site for recruitment, retention, and marketing, and evaluating the effect of the residency.
COLLABORATION AND COORDINATION IN THE MRICU
Amy Dean, Virginia Commonwealth University
Kristin Miller, Virginia Commonwealth University
Dean and Miller presented their experience with developing and implementing an interprofessional training program aimed at improving patient care in the medical respiratory intensive care unit (MRICU) at Virginia Commonwealth University (VCU). Dean is the nurse clinician at VCU Health, and Miller is the assistant professor with the Division of Pulmonary Disease and Critical Care Medicine at VCU School of Medicine. Dean began by explaining how the MRICU operates. It is a 28-bed ICU that specializes in the care of critically ill patients; the patients are often on mechanical ventilation, require continuous renal replacement therapy, and/or have continuous infusions of sedatives and vasoactive medications. The MRICU is run by an established interprofessional team that includes nurses, physicians, advanced practice providers, physical therapists, occupational therapists, pharmacists, and respiratory therapists, and the unit is split into a “red team” and “blue team” to which patients are admitted on a rotating basis.
The Collaboration and Coordination in the MRICU project came out of the VCU Langston Quality Scholars Program (LQSP), which is a collaboration between the school of medicine, the school of nursing, and the health system at VCU. LQSP is an experiential learning program that is designed to deliver CPD that focuses on the science of improvement and leadership skills, said Dean. The curriculum for LQSP is planned by a collaborative team of education experts, and it is delivered through didactic and online modules, embedded quality improvement experiences in the workplace, and biweekly coaching by a health care science of improvement expert. LQSP is taught in a dyad format, with participants from different health professions learning and working together. Over the course of about 8 months, Dean and Miller participated in the LQSP as a dyad from the MRICU, and developed and implemented their project to improve MRICU care.
Miller explained that their project was grounded in the “ABCDEF bundles,” which are a series of best practices for patient care in the ICU (Marra et al., 2017):
A: Assess, prevent, and manage pain
B: Spontaneous awakening trial and spontaneous breathing trial (reduce sedation to test whether patient can be removed from ventilator)
C: Choice of analgesia and sedation
D: Assess, prevent, and manage delirium
E: Early mobility and exercise
F: Family engagement and empowerment
The MRICU project focused on three of these bundles: B, C, and E. Miller explained the reasoning behind these choices. The B bundle (spontaneous awakening and spontaneous breathing trial) was chosen because “studies have shown that synergistic use of both the spontaneous awakening trial and the spontaneous breathing trial decreases duration on the ventilator, decreases hospital lengths of stay, and decreases delirium.” The C bundle (choice of medication for analgesia and sedation) was chosen because, while sedation is important to keep patients comfortable and in sync with the breathing machines, deep sedation is often unnecessary and deleterious. Miller said,
Deep sedation has been found to reduce 6-month survival and to increase hospital mortality, ICU and hospital length of stay, time on the breathing machine or the ventilator, and physiologic stress to the patient.
To help providers find the ideal level of sedation for a patient, VCU uses evidence-based guidelines and the Richmond Agitation and Sedation Scale (RASS). Finally, the E bundle (early mobility and exercise) was chosen because ICU-acquired weakness is a problem that leads to decreased functional mobility, longer time on the ventilator, and increased mortality, said Miller.
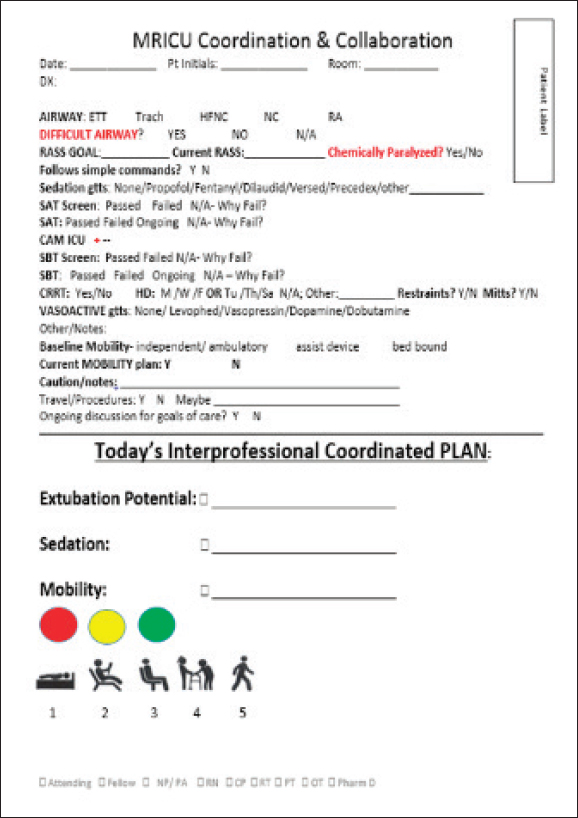
Dean added that despite the scientific evidence behind these best practice bundles, they were not being consistently and effectively implemented. Dean and Miller built an interdisciplinary team of providers from the MRICU to help bridge the gap between the scientific evidence and actual implementation of the practices. This team concluded that there was an issue with communication and coordination of the bundles, so a goal was set to “achieve daily interprofessional communication and coordination of the care relevant to the patient sedation level, liberation potential, and the mobility plan for all MRICU blue team patients.” The blue team served as the intervention group while the red team served as the control group. The blue intervention team used a Plan-Do-Study-Act (PDSA) cycle to develop and test different approaches to solving the problem. After several cycles, the team eventually developed a solution of interprofessional huddles held at 8 a.m., in which the team had a scripted conversation lasting 2 minutes per patient to develop a simple written plan for sedation, liberation potential, and mobility (see Figure 4-1).
Over the course of 3.5 months, the team held 269 huddles for 53 patients. The patients who had the “bundled huddle” had numerous improved outcomes: increased time at an appropriate sedation level, decreased use of
SOURCE: Presented by Amy Dean and Kristin Miller, April 6, 2017.
benzodiazepines (from 20 percent of patients to 5 percent), and increased provider compliance with spontaneous awakening trials and spontaneous breathing trials (from 45 percent to 92 percent and 41 percent to 89 percent, respectively). Postintervention, 99 percent of patients had a mobility plan, compared to 16 percent preintervention. The average observed inpatient length of stay was markedly decreased for patients who had the bundled huddle—from 11.01 days preintervention to 7.75 days postintervention (compared to 9.95 and 9.22 days in the red control group). Length
of stay in the ICU was similarly decreased, from 4.96 days to 3.14 days, compared to an increase in the red team’s patients from 3.76 days to 4.28 days.
With these data in hand, Dean and Miller estimated how much money was saved by implementing the program. The length of stay difference (1.14 days) was multiplied by the number of blue team admissions (183), and then by the average cost of a day in the ICU ($3,184).2 The cost savings over the course of the intervention was estimated to be $664,246; extrapolated out to an entire year, Dean and Miller estimated that the potential yearly savings was $2.26 million. In addition to the savings related to the length of stay, Dean and Miller also found significant savings related to the MRICU accommodation charges and respiratory therapy charges.
The cost savings must be compared to the cost of implementing the program, said Dean. The total cost—including LQSP faculty and staff, outside speakers, and supplies—was approximately $97,000, or about $12,000 per dyad. Dean said that it seems clear that the benefits of the program outweighed these costs, making a “great business case for high-value continuing professional development.” She noted that in addition to the quantifiable improvement in outcomes, there were other benefits, such as improved staff satisfaction, increased interprofessional collaboration, and a gain in skills and knowledge that can be used in other projects.
CPD COLLABORATIVE CONSORTIUM
Simon Kitto, University of Ottawa
Kitto shared a case study about an attempt at building a CPD consortium in Ontario, Canada. Kitto explained that because of the universal health care system in Canada, there are public-sector institutions in Ontario that work on CPD. However, these institutions have traditionally had no relationship with the Ministry of Health (MOH) of the Ontario Province. Rather, MOH had provided money for health care professional education directly to the hospitals, said Kitto. An Office of CPD in the Ontario Providence had the idea to approach MOH and present a business case for redirecting their CPD funding to the Office of CPD, instead of to the hospitals. MOH, said Kitto, had a limited understanding of what CPD was—it was a “completely new concept to them.” However, MOH had a great interest in quality improvement. Kitto said this was an opportunity for offices of CPD and MOH to “marry their interests.”
___________________
2 Based on Dasta, J. F., T. P. McLaughlin, S. H. Mody, and C. T. Piech. 2005. Daily cost of an intensive care unit day: The contribution of mechanical ventilation. Critical Care Medicine June, 1266–1271.
Six medical school CPD offices were chosen as participants to create a “consortium for the development, implementation, and evaluation of quality continuing education for the health professions.” The goal, said Kitto, was for all the medical schools in the province to begin to work together and present a united front to MOH to make the case for investing in CPD. The consortium planned to use a “walk in the woods” approach to develop their plan. This is a “method for multidimensional problem solving that is geared toward reaching a deal with necessary buy-in and support.” There are four stages in the method: (1) identify self-perceived needs, (2) agree on key interests, (3) explore options for meeting and prioritizing these interests, and (4) reach an agreement and develop a plan for moving forward (Marcus et al., 2012).
The consortium began the process by identifying some key value propositions about CPD, each centered around the overarching goals of social good, collaboration, and quality. The consortium agreed that CPD could bring more value to health care by being more
- responsive to critical emerging health issues (social good),
- strategically positioned to compete for provincial funding (collaboration),
- streamlined to create more efficiencies in administrative systems (quality),
- evidence based in the CPD needs assessment process (quality),
- innovative in the design of continuing education (quality), and
- collaborative.
Further discussions resulted in a list of shared interests for the consortium to effectively collaborate and move forward with its plan. The list included
- oversight coordination models,
- intellectual property,
- revenue sharing practice,
- accreditation models,
- implementation models, and
- memoranda of understanding for research collaboration.
Despite this initial success in identifying value propositions and shared interests, the project soon came to a halt, said Kitto. On the day that the consortium planned to begin the formal walk in the woods process, several key stakeholders failed to participate. As a medical sociologist, Kitto sought to learn some lessons from the stalled process; he identified three logistical,
cultural, and political issues that obstructed the consortium from successfully moving forward:
- Social desirability: Kitto remarked on the identified value propositions that centered on social good, collaboration, and quality. These are “pretty hard for anyone to reject” he said. Kitto speculated that the people involved in the consortium were reluctant to publicly disagree with such goals; yet, it is possible these goals were not aligned with their actual interests and beliefs. Because of this misalignment, some may not have perceived the value in participating in the process.
- Local concerns: Kitto said that asking these local, public institutions to help build a provincewide business case was problematic for several reasons. First, the offices of CPD are “lean machines;” they have a limited number of personnel, are heavily focused on local operations, and emphasize maintaining preexisting local relationships. Second, the cultures of the regions in which the offices were located were very different. The offices were driven by local issues and the needs of the health care professionals in their immediate environment rather than external collaborative efforts.
- Relationships between the stakeholders: Despite shared interests in improving CPD, the universities involved in the consortium and their representatives had a “quasi-competitive” relationship with each other. Kitto said that although they are public-sector institutions, universities compete with one another for students, funding, clients, and other resources. This history of competition, he added, “overshadowed the partnership” that could have been formed.
Kitto concluded that if he were to approach this process again, he would focus less on the technical aspects of building the business case and more on the stakeholders involved—who are they, what are their concerns, and where might there be sticking points? He said that while the technical methodology of the business case is ultimately important, it is essential to first fully understand and acknowledge the needs, concerns, and relationships of the stakeholders. Kitto argued that an “intercultural communication process” is necessary to bring the different CPD offices together. It is an intercultural process in that although there are similarities, each university stakeholder has its own organizational culture, history, and motivations, and these differences need to be addressed in order to build a successful collaboration.
DISCUSSION
Mike Rouse of the Accreditation Council for Pharmacy Education asked Dean and Miller to elaborate on the specific education and training that the providers received during the MRICU intervention. Dean explained that there were monthly didactic lectures that taught how to use quality improvement tools, such as process mapping, fishbone diagramming, and the PDSA cycle. In addition, the providers learned much from the biweekly coaching sessions with the science of improvement experts. Miller added that there was a lot of bedside education, in which the providers who were involved in the intervention could quickly educate the other members of the care team about topics such as mobility or sedation.
Brenda Zierler of the American Academy of Nursing pointed out that in her opinion, one of the best outcomes of the MRICU intervention was the interdisciplinary collaboration and communication that resulted in a clear and consistent plan of care. Miller agreed that the interdisciplinary aspect of the intervention was highly beneficial for everyone involved.
Julia Royall of the Global Health Information Specialist noted that Dean and Miller brought together a very diverse group of professionals to plan the intervention, and wanted to know the most challenging aspect of bringing these personalities and people together. Dean replied that the biggest challenge was “igniting the passion within the interdisciplinary team,” but said that focusing the group on the benefit to the patients made it “easy to bring people on board.” Miller added that the coaches from QSP were instrumental in helping them choose the right people for the team.
Savitz asked Bowden to elaborate on his goal of collecting data on patient quality of life. Bowden said that one of the challenges in getting clinical partners for the physical therapy residency has been getting people to recognize that things could be done better or differently, and that broadening the scope of outcomes that are measured—to include such aspects as quality of life—is critical to this conversation.
Darla Coffey from the Council on Social Work Education observed that none of the panelists mentioned continuing education credits as a primary driver or component of their projects. The panelists confirmed that participants in their programs do in fact receive CE credits, but that it tends to be “nontraditional CE,” such as discussion and learning during patient care rather than a standard lecture format. Coffey applauded the fact that these projects seemed to emerge from a commitment to learning and a systems perspective, and that any CE credits conveyed were simply added benefits.
Zohray Talib of The George Washington University had two questions for Bowden regarding how a project like the physical therapy residency might be translated for use in an area such as East Africa. First, she asked how leadership of hospitals can be incentivized to invest in the staff and to
recognize that there is value in upgrading staff. She noted that leadership is sometimes reluctant to invest in staff when there is no guarantee that the staff will continue working at the hospital. Bowden replied that the residents in his program make a 2-year commitment to the facility after the end of the residency, and if the resident leaves before that time, he or she must pay the investment back. However, he noted, he is “totally okay” with residents eventually moving on to other facilities, because it expands the impact of the program and puts the residents in a position to create culture change in their new workplace. Talib’s second question concerned the effectiveness of using a virtual classroom for some components of the program, noting that this model could be quite useful in a low-resource setting. Bowden responded by saying they struggled with the online portion of the residency in the first year, and have learned much about doing it effectively. He said that instead of continuously inundating the residents with content, they learned to ask residents to explore a small amount of content and then lead a practical discussion about it with their peers. For example, a resident might read an article about a specific approach to patient care, then try the approach in the clinic and report back to the other residents about whether and how the approach worked in the real-world environment.
Joel Nelson of the Health Resources and Services Administration asked the panelists about whether there has been “diffusion of innovation” with their programs; for example, has the red team in the MRICU adopted any of the practices of the blue team, or have new pilots of these projects been implemented elsewhere? Dean replied by saying that they are currently working to firmly establish their project in the ICU and hope to eventually take it hospital-wide and perhaps even community-wide. Dean commented that their MRICU dyad, one of eight dyads from different hospital departments, had seen great success and they were attempting to diffuse what they had learned. Miller added that a current focus of their work is on educating people within their ICU to make the program sustainable, noting that changing the way things have traditionally been done is very challenging. Bowden chimed in saying that one of their goals with the physical therapy residency is to “lay sod inside of rehab and then allow it to spread from there.” The hope, he said, is that people outside the residency program will take note of the benefits of the residency and want to make similar changes in their own area of practice as well. Bowden relayed a story about the diffusion of a resident innovation. One of the residents worked with the information technology department at his hospital to develop a menu of rehab-specific options in the electronic health record for his facility in Florida. Two years later, a site visit revealed that a facility in York, Pennsylvania, was using the menu in its electronic health record.
Savitz said that her evaluation and analysis of the HVHC project resulted in a “generalized framework for accelerated dissemination and
implementation” of this type of learning health care system. She relayed some key components of the framework:
- Use a clinical expert panel to address areas in which there is a dynamic evidence base, and answer questions about the data.
- Develop a tool and resource portal for people to share resources, such as clinical decision support tools or tools for comparative data analysis.
- Facilitate opportunities for providers to share examples of real-world learning.
Bjorg Palsdottir of the Training for Health Equity Network asked the panelists whether there was any opportunity for the lessons they have learned in their CPD programs to influence the education and training that health providers receive before they enter practice. Bowden responded that his group at MUSC has a formal process for collecting and analyzing feedback from the residents and the mentors, and that the feedback has “dramatically changed” how they approach entry-level education. Specifically, he said that it is “insufficient to focus so much on the didactic portion,” so they are making an attempt to use the classroom to teach clinical reasoning skills and pose practical patient scenarios.
Donald Moore, director of the Division of Continuing Medical Education and of Evaluation and Education at Vanderbilt University, observed that the CPD programs the panelists had described were largely focused on the kind of incidental and informal learning that takes place in the work environment, and that this move away from more traditional, formal education is an important part of the transition from CE to CPD.
REFERENCES
Dasta, J. F., T. P. McLaughlin, S. H. Mody, and C. T. Piech. 2005. Daily cost of an intensive care unit day: The contribution of mechanical ventilation. Critical Care Medicine 33(6):1266–1271.
Marcus, L. J., B. C. Dorn, and E. J. McNulty. 2012. The walk in the woods: A step-by-step method for facilitating interest-based negotiation and conflict resolution. Negotiation Journal July, 337–349.
Marra, A., E. W. Ely, P. P. Pandharipande, and M. B. Patel. 2017. The ABCDEF bundle in critical care. Critical Care Clinic 33(2):225–243.














