
6
Department of Veterans Affairs Mental Health Services: Need, Usage, and Access and Barriers to Care
Since Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) began in 2001, 2003, and 2010, respectively, an increasing number of veterans from this era have been receiving health care services through the Department of Veterans Affairs (VA). These services have included care to address mental health conditions that developed following their military service (Mott et al., 2014; VA, 2014). The purpose of this chapter is to detail the characteristics of the OIF, OEF, and OND veteran population, describe the mental health needs that exist within this population, and explore how these veterans are using mental health services, including treatment provided by the VA and other non-VA sources of care. To address a key task in the committee’s charge, this chapter relies on its own survey to examine in depth the mental health service needs and treatment patterns for OIF, OEF, and OND veterans who are not currently enrolled to receive mental health services at a VA facility. The committee examines survey and site visit findings on the experience of veterans with VA mental health services, barriers to accessing these services, current attitudes toward VA mental health services, and the factors influencing veterans’ future use of these services. The chapter concludes with a summary and the committee’s conclusions regarding the use of VA mental health services.
The specific questions addressed in the major sections of this chapter are
- How is eligibility for and access to VA health services, including mental health services, determined?
- What are the key demographic, service-related, and geographic characteristics of the 2016 pool of approximately 4.1 million OEF/OIF/OND-era veterans?
- What is the need for mental health services among OEF/OIF/OND-era veterans?
- What share of those veterans in need are accessing mental health treatment services and where are those in treatment receiving services?
- Among veterans who have used the VA mental health services, what are their experiences with respect to various dimensions of access and quality, such as the availability, timeliness, and effectiveness of the care they received?
- Among those in need, what are the barriers and facilitators to use of mental health services?
- What factors may influence the future use of mental health services?
ELIGIBILITY AND PRIORITY FOR DEPARTMENT OF VETERANS AFFAIRS HEALTH CARE SERVICES
The VA serves 8.76 million veterans per year at more than 1,700 health care sites throughout the United States (VA, 2015e). Not all veterans, however, are eligible for care through the VA. Veterans may be eligible for health care services if they
- Served in the active military service and were separated under any condition other than dishonorable.
- Served in the Reserves or National Guard, or are currently serving, and were called to active duty by a federal order and completed the full period for which they were called or ordered to active duty (VA, 2015c).
The VA has minimum duty requirements for eligibility for health care services. For example, most veterans who enlisted after September 7, 1980, or entered active duty after October 16, 1981, must have served 24 continuous months or the full period for which they were called to active duty in order to be eligible (VA, 2015c). A number of exceptions to the minimum duty requirements exist and, therefore, veterans must apply for health care services to determine eligibility. An enhanced eligibility status exists for any veteran who falls into one or more of the following categories:
- Is a former prisoner of war.
- Has received the Purple Heart medal.
- Has received the Medal of Honor.
- Has a compensable VA awarded service-connected disability of 10 percent or more.
- Receives a VA pension.
- Was discharged from the military because of a disability (not pre-existing), early out, or hardship.
- Served in a theater of operations for 5 years post discharge.
- Served in the Republic of Vietnam from January 9, 1962 to May 7, 1975 (or on qualifying U.S. Navy and Coast Guard ships associated with military service in Vietnam).
- Served in the Persian Gulf from August 2, 1990, to November 11, 1998.
- Was stationed or resided at Camp Lejeune for 30 days or more between August 1, 1953, and December 31, 1987.
- Is found by VA to be catastrophically disabled.
- Previous years’ household income was below VA’s National Income or Geographical-Adjusted Thresholds (VA, 2015c).
Veterans must apply for VA health care services, and then the VA reviews the application and makes a determination on eligibility for enrollment. Once a veteran is enrolled, the veteran is assigned an enrollment priority group (see Box 6-1). Priority groups are used because Congress annually allocates funds for VA and, given the limited funds it must work with, the agency needs a way to prioritize who should receive health care services. The priority groups range from 1 to 8, with those in group 1 receiving the highest priority. On the basis of eligibility and income, some veterans may have to pay a copay when using services.
Veterans who served in a combat theater after November 11, 1998, and were discharged from active duty on or after January 28, 2003, are eligible for comprehensive VA health care services for 5 years following their discharge under the “combat veteran” authority in the National Defense Authorization Act of 2008. Veterans in this group would include veterans serving in combat theaters in support of OEF/OIF/OND (unless they were discharged before January 28, 2003). During the 5 years, veterans are allowed to enroll for health care services without first establishing their priority group. After 5 years, these veterans are assigned to a priority group based on their income and degree of disability due to their service-related condition at that time (IOM, 2014). Combat veterans who did not enroll within the 5-year window of eligibility and were discharged from service between January 1, 2009, and January 1, 2011, were granted 1 additional year of eligibility under the Clay Hunt Suicide Prevention for American Veterans Act in 2015.1
In general, the VA does not provide health care services or coverage to spouses or dependents. However, with the Program of Comprehensive Assistance for Family Caregivers, veterans’ family members caring for seriously injured veterans, including veterans who have mental health conditions, are eligible for certain VA services including caregiver training, a financial stipend, mental health services and counseling, and access to health insurance (VA, 2017f).
Legal veteran status is earned by individuals who complete at least 2 consecutive years of active-duty military service and are discharged or separate from service under conditions other than dishonorable.2 Under VA regulations (although not mandated by federal law), individuals who receive an other-than-honorable (OTH) discharge are not eligible to receive VA medical care, including mental health care (Commission on Care, 2016). This includes veterans who received an OTH discharge because of actions or behavior that resulted from a health condition (such as a traumatic brain injury [TBI], posttraumatic stress disorder [PTSD], or substance use) that may have been caused or aggravated by their service. Individuals with OTH discharges have some level of misconduct on their records, but no court martial convictions. Nearly 7 percent of OEF/OIF/OND veterans have received an OTH discharge (Swords to Plowshares, 2016). A recent Government Accountability Office report (GAO, 2017) found that of the 91,764 service members who received a misconduct separation between fiscal years (FY) 2011 and 2015, 62 percent (57,141) were diagnosed with PTSD or a TBI within 2 years of their separation. Of the 57,141, 23 percent (12,283) received an OTH discharge, making them potentially ineligible to receive VA health care services. This finding is consistent with findings of a 2016 report by the congressionally appointed Commission on Care, which reported that many former service members who received an OTH discharge as a result of a regulatory bar (which could be the result of behavioral misconduct related to a service-connected mental health condition) are legally veterans, but are routinely denied health care unless they request, receive, and prevail in eligibility adjudication with the Veterans Benefits Administration (VBA) that their discharge was not dishonorable (Commission on Care, 2016). However, very few veterans who request eligibility adjudication receive it. For those veterans who are granted adjudication proceedings, the process can take about 4 years to complete (Swords to Plowshares, 2016). The Commission on Care recommends that the VA eliminate the regulation that automatically prohibits veterans with an OTH discharge from receiving health care from the VA. Furthermore, it recommends that the VA award tentative eligibility for services to individuals with OTH discharge who have completed substantial honorable service, including (but not limited to) serving in a combat theater. Finally, it recommends that the VA should provide an opportunity to recognize that misconduct that leads to the OTH discharge may itself be related to a service-connected condition (Commission on Care, 2016). As mentioned in Chapter 4,
___________________
1 Public Law 114-2.
2 38 U.S.C. § 101(2).
in 2017 VA Secretary David Shulkin announced that the VA would offer emergency mental health care to veterans with an OTH discharge status as part of its ongoing efforts to prevent veteran suicides (VA, 2017e). Under this initiative, veterans with OTH discharges will be eligible to seek treatment at a VA emergency department, Vet Center, or contact the Veterans Crisis Line. The VA will provide a full array of mental health services for up to 90 days. The VA estimated that 30,000 to 50,000 OTH veterans per year (out of the total 505,000) would use emergency mental health services, requiring an estimated
150,000 to 240,000 additional bed days of inpatient care as well as approximately 375 to 675 full-time equivalent provider-years of outpatient mental health services (VA, 2017d).
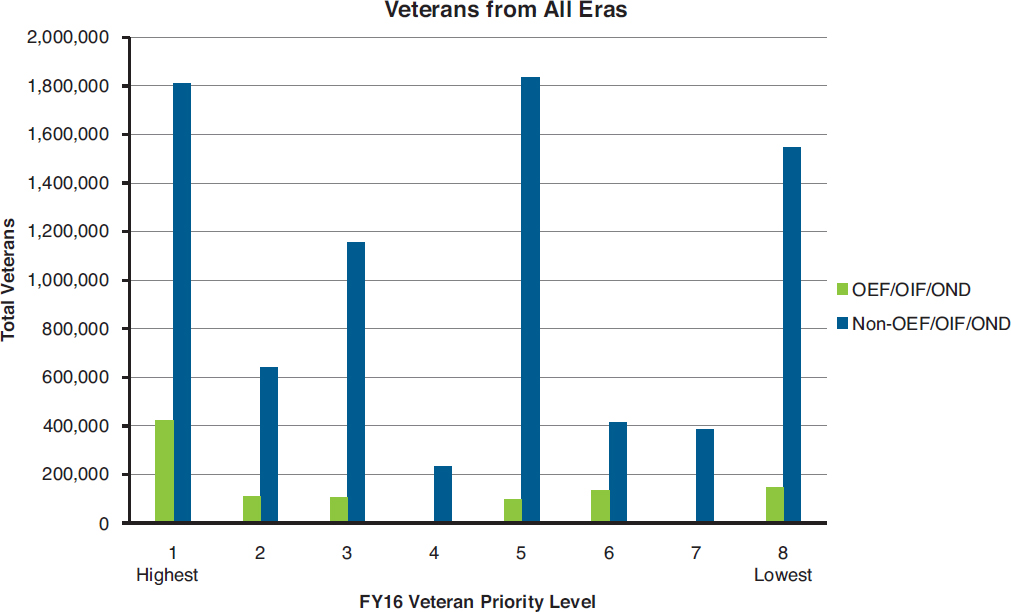
In FY 2016, 9,040,675 veterans of all eras were enrolled in the VA health system and assigned to priority groups 1–8 (see Box 6-1).3 Of those, 1,024,330 are OEF/OIF/OND veterans (that is, veterans who served in the U.S. Armed Forces after September 2001), and 8,016,345 are veterans of other eras.
___________________
3 Personal communication, Stacy Gavin, VA, May 25, 2017.
SOURCE: Adapted from personal communication, Stacy Gavin, Department of Veterans Affairs, May 25, 2017.
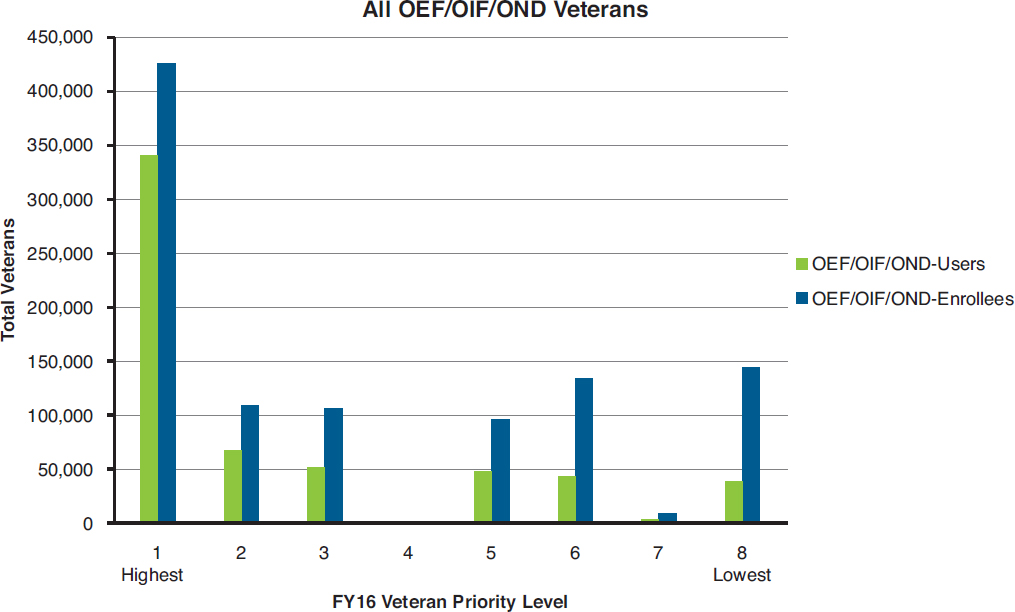
Figure 6-1 shows the distribution of enrolled OEF/OIF/OND veterans and other-era veterans among the priority groups. Priority groups 1, 6, and 8 have the highest numbers of OEF/OIF/OND veterans enrolled; priority groups 1, 5, and 8 have the highest numbers of veterans of other eras. Of the 1,024,330 OEF/OIF/OND veterans who are enrolled in VA health care, 604,871 of them used VA health care services in FY 2016. Figure 6-2 shows the distribution among the priority groups of OEF/OIF/OND veterans who are enrolled in VA health care and also use the health care services. Not all enrolled veterans actively use the health care services. The highest number of OEF/OIF/OND enrollees and users are in priority groups 1, 2, and 3. About 60 percent of OEF/OIF/OND enrollees use VA health services. This number is lower than the number of other-era enrollees who use VA health services, which is about 72 percent.
KEY CHARACTERISTICS OF THE OPERATION ENDURING FREEDOM, OPERATION IRAQI FREEDOM, AND OPERATION NEW DAWN COHORT WHO USE AND DO NOT USE VETERANS HEALTH ADMINISTRATION SERVICES
Mental health conditions are the third most frequently diagnosed category of conditions at the VA, for both men and women (Frayne et al., 2014; VA, 2015b). Among veterans not using the VA for mental
SOURCE: Adapted from personal communication, Stacy Gavin, Department of Veterans Affairs, May 25, 2017.
health services, many may not need mental health services. However, as described in Chapter 11, there are veterans who would benefit from mental health services but are not using them.
Demographic data on veterans not using VA health services are often difficult to come by because there is no standardized way of tracking all service members once they separate from the military. Because data on veterans not using VA services are not often collected, the committee was instructed in the congressional legislation mandating this study to specifically seek out and survey OEF/OIF/OND veterans who are not currently or have never used VA mental health services. As a result, many of the demographic data for non-users come from the survey conducted for this study, as described in Chapter 5, and these data are presented below. It is important to note that all weighted numbers from the committee’s survey reported in this chapter and the following chapters represent estimates of the numbers of veterans, unless otherwise specified.
Demographics and Service Branch
This section summarizes the committee’s survey results related to the demographics of the OEF/OIF/OND cohort. Table 6-1 presents the demographics of the OEF/OIF/OND veterans from the committee’s survey. Most OEF/OIF/OND veterans are under 50 (72 percent); the most common age category is 30–39 years of age, representing 35 percent of the total population. Twenty-one percent of
OEF/OIF/OND veterans are female. Among the chosen race/ethnicity categories, 66 percent of the veterans in the study are non-Hispanic white; 13 percent are non-Hispanic black, 12 percent are Hispanic, and the remaining 9 percent are various other races. Almost half (47 percent) of OEF/OIF/OND veterans have a 4-year college degree or more. Almost two-thirds are married or in a civil commitment or union (64 percent), and the rest of the cohort is split relatively evenly between never married and formerly married. About three-quarters of these veterans are employed. The income of these veterans varies widely, with a similar percentage making less than $25,000 per year (12 percent) as there are making more than $150,000 (11 percent) per year. Allowing for missing responses to the survey question, 10 to 11 percent of the OEF/OIF/OND veterans surveyed do not have health insurance.
The descriptive statistics in Table 6-1, which are estimates derived from the committee’s survey, are reasonably comparable to estimates produced by the VA for the OEF/OIF/OND veteran population (VA, 2017c). About 74 percent of OEF/OIF/OND veterans in the VA estimates are under age 45, whereas in Table 6-1, 72 percent of OEF/OIF/OND veterans are under 50. A greater percentage of OEF/OIF/OND veterans in the study population from the committee’s survey are married or in a civil commitment or union (64 percent; Table 6-1) than among OEF/OIF/OND veterans (54 percent) in the VA estimates. In the study population, 66 percent were white non-Hispanic (see Table 6-1), versus 67 percent of OEF/OIF/OND male veterans and 56 percent of OEF/OIF/OND female veterans from the VA estimates. More of the OEF/OIF/OND veterans in Table 6-1 had a 4-year college degree or more than did OEF/OIF/OND veterans in the VA estimates (47 versus 30 percent). The percentage of OEF/OIF/OND veterans without health insurance in Table 6-1 (10 percent) was similar to that of OEF/OIF/OND veterans in the VA estimates (6.7 percent).
The distribution of demographic characteristics for the OEF/OIF/OND population (the population used in the committee’s survey that includes veterans who began their service prior to 9/11 but who served in OEF/OIF/OND) differs from that of the broader veteran population (veterans of all eras). The OEF/OIF/OND population is much younger, as 79 percent of all other veterans are age 55 or older (VA, 2017c). While 21 percent of OEF/OIF/OND veterans are female, 9 percent of the overall veteran population is female (VA, 2017b). The percentages of white non-Hispanic veterans in OEF/OIF/OND versus all veterans are 66 versus 77 percent (VA, 2017b). The OEF/OIF/OND population has a higher level of educational attainment (4-year college degree or more) than the overall veteran population (47 versus 27 percent) (VA, 2017c). Similar percentages of OEF/OIF/OND veterans and all other veterans are married (64 versus 65 percent) (VA, 2017c). The percentage of all other veterans without health insurance coverage is lower than among OEF/OIF/OND veterans (3 versus 10 percent) (VA, 2017c).
Table 6-2 presents the military characteristics of OEF/OIF/OND veterans, which are estimates derived from the committee’s survey. An overwhelming majority served on active duty (79 percent), with 20 percent being in the National Guard or Reserve forces. The Army is the most common branch of service (46 percent), followed by the Air Force (20 percent), Navy or Coast Guard (19 percent), Marine Corps (9 percent), and multiple branches (5 percent). Only 20 percent were officers, and 79 percent were enlisted personnel. A slight majority (53 percent) of the veterans were deployed in support of OEF/OIF/OND (includes deployments to combat area, non-combat area, or training mission). Twenty-five percent of the veterans were deployed for 12 months or less and 28 percent for more than 12 months.
Most veterans—59 percent—were never deployed into a combat area, while 18 percent had one combat deployment and 22 percent had more than one. Among those veterans who were deployed to a combat area, the deployment locations varied. Twenty-three percent were deployed to more than one location, 26 percent were deployed to Iraq only, 10 percent were deployed to Afghanistan only, and 16 percent were deployed to other areas. Most veterans reported a low combat exposure (81 percent). The combat exposure variable is based on the Deployment Risk and Resilience Inventory (DRRI) Com-
| Demographic Characteristics | Unweighted n | Weighted N | Weighted % | Standard Error % |
|---|---|---|---|---|
| Total | 4,180 | 4,179,998 | 100% | |
| Age | ||||
| 17 to 29 years old | 617 | 633,990 | 15.2% | 0.5% |
| 30 to 39 years old | 1,502 | 1,444,386 | 34.6% | 0.9% |
| 40 to 49 years old | 939 | 923,549 | 22.1% | 0.6% |
| 50 years old and older | 1,086 | 1,104,789 | 26.4% | 0.8% |
| Missing | 36 | 73,284 | 1.8% | 0.4% |
| Gender | ||||
| Male | 2,946 | 3,303,305 | 79.0% | 0.8% |
| Female | 1,220 | 859,250 | 20.6% | 0.8% |
| Missing | 14 | 17,442 | 0.4% | 0.1% |
| Race/Ethnicity | ||||
| Non-Hispanic White only | 2,636 | 2,762,440 | 66.1% | 0.8% |
| Non-Hispanic Black only | 644 | 537,059 | 12.8% | 0.5% |
| Hispanic | 503 | 490,740 | 11.7% | 0.6% |
| Other or multiple races | 349 | 355,834 | 8.5% | 0.6% |
| Missing | 48 | 33,924 | 0.8% | 0.1% |
| Education | ||||
| Less than a 4-year college degree | 2,204 | 2,218,603 | 53.1% | 1.0% |
| 4-year college degree or more | 1,969 | 1,956,133 | 46.9% | 1.0% |
| Refused | 1 | 796 | 0.0% | 0.0% |
| Don’t know | 1 | 463 | 0.0% | 0.0% |
| Missing | 5 | 4,002 | 0.1% | 0.1% |
| Marital status | ||||
| Married or civil commitment or union | 2,585 | 2,688,394 | 64.3% | 0.7% |
| Never married | 711 | 745,414 | 17.8% | 0.6% |
| No longer married | 868 | 732,858 | 17.5% | 0.7% |
| Don’t know | 5 | 1,959 | 0.0% | 0.0% |
| Missing | 11 | 11,373 | 0.3% | 0.1% |
| Employment | ||||
| Not employed | 1,092 | 959,181 | 22.9% | 0.7% |
| Employed | 2,992 | 3,104,253 | 74.3% | 0.8% |
| Missing | 96 | 116,563 | 2.8% | 0.4% |
| Annual income | ||||
| Less than $10,000 | 117 | 104,291 | 2.5% | 0.2% |
| $10,000 to $24,999 | 418 | 386,506 | 9.2% | 0.6% |
| $25,000 to $49,999 | 867 | 789,738 | 18.9% | 0.8% |
| $50,000 to $74,999 | 927 | 919,022 | 22.0% | 0.7% |
| $75,000 to $99,999 | 647 | 679,617 | 16.3% | 0.7% |
| $100,000 to $149,999 | 679 | 739,934 | 17.7% | 0.8% |
| $150,000 or more | 427 | 471,177 | 11.3% | 0.5% |
| Refused | 27 | 20,528 | 0.5% | 0.1% |
| Don’t know | 26 | 18,778 | 0.4% | 0.1% |
| Missing | 45 | 50,406 | 1.2% | 0.2% |
| Health insurance | ||||
| Not insured | 644 | 427,500 | 10.2% | 0.4% |
| Insured | 3,357 | 3,519,268 | 84.2% | 0.4% |
| Missing | 179 | 233,229 | 5.6% | 0.5% |
NOTE: Individual item counts may not sum to total counts due to rounding. Missing includes skipped items.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| Military Experience Characteristics | Unweighted n | Weighted N | Weighted % | Standard Error % |
|---|---|---|---|---|
| Total | 4,180 | 4,179,998 | 100% | |
| Military status | ||||
| Active | 3,409 | 3,302,287 | 79.0% | 0.9% |
| Reserve/Guard | 751 | 843,162 | 20.2% | 0.8% |
| Refused | 2 | 3,271 | 0.1% | 0.1% |
| Missing | 18 | 31,278 | 0.7% | 0.2% |
| Branch of service | ||||
| Army | 2,000 | 1,903,401 | 45.5% | 0.8% |
| Marine Corps | 382 | 385,290 | 9.2% | 0.5% |
| Navy/Coast Guard | 727 | 806,405 | 19.3% | 0.7% |
| Air Force | 816 | 842,734 | 20.2% | 0.7% |
| Multiple branches | 239 | 214,173 | 5.1% | 0.4% |
| Refused | 1 | 320 | 0.0% | 0.0% |
| Missing | 15 | 27,675 | 0.7% | 0.2% |
| Rank | ||||
| Officer | 751 | 831,056 | 19.9% | 0.9% |
| Enlisted | 3,411 | 3,319,462 | 79.4% | 0.8% |
| Refused | 4 | 6,784 | 0.2% | 0.1% |
| Don’t know | 1 | 463 | 0.0% | 0.0% |
| Missing | 13 | 22,231 | 0.5% | 0.1% |
| Total length of deployments | ||||
| No deployment | 1,195 | 1,925,786 | 46.1% | 0.7% |
| 1 to 12 months | 1,317 | 1,053,685 | 25.2% | 0.7% |
| More than 12 months | 1,643 | 1,173,158 | 28.1% | 0.7% |
| Refused | 10 | 8,822 | 0.2% | 0.1% |
| Missing | 15 | 18,546 | 0.4% | 0.1% |
| Number of deployments to combat area | ||||
| None | 1,643 | 2,473,530 | 59.2% | 0.5% |
| One | 1,170 | 762,825 | 18.2% | 0.5% |
| More than one | 1,330 | 909,445 | 21.8% | 0.6% |
| Refused | 11 | 5,331 | 0.1% | 0.0% |
| Missing | 26 | 28,865 | 0.7% | 0.1% |
| Location of deployments among the deployed | ||||
| Iraq only | 942 | 577,324 | 25.9% | 0.9% |
| Afghanistan only | 325 | 224,833 | 10.1% | 0.6% |
| Other combat area | 472 | 360 752 | 16.2% | 0.8% |
| Multiple combat areas | 765 | 511,755 | 23.0% | 0.9% |
| No combat deployments | 450 | 546,537 | 24.5% | 1.1% |
| Missing | 6 | 5,643 | 0.3% | 0.1% |
| Exposure to combat and aftermath of battle | ||||
| Low | 3,007 | 3,380,131 | 80.9% | 0.5% |
| Moderate | 868 | 599,552 | 14.3% | 0.4% |
| High | 214 | 147,050 | 3.5% | 0.3% |
| Don’t know | 1 | 583 | 0.0% | 0.0% |
| Missing | 90 | 52,681 | 1.3% | 0.1% |
| Military Experience Characteristics | Unweighted n | Weighted N | Weighted % | Standard Error % |
|---|---|---|---|---|
| Service-connected disability | ||||
| Less than 50% disability | 830 | 745,488 | 17.8% | 0.6% |
| 50% or more disability | 1,174 | 737,603 | 17.6% | 0.5% |
| No disability | 2,095 | 2,605,612 | 62.3% | 0.6% |
| Refused | 51 | 56,024 | 1.3% | 0.2% |
| Don’t know | 1 | 556 | 0.0% | 0.0% |
| Missing | 29 | 34,715 | 0.8% | 0.2% |
| Treatment for physical condition(s) during the past 24 months | ||||
| Yes | 1,761 | 1,123,721 | 26.9% | 0.5% |
| No | 2,330 | 2,971,336 | 71.1% | 0.5% |
| Missing | 89 | 84,940 | 2.0% | 0.2% |
NOTE: Individual item counts may not sum to total counts due to rounding. Missing includes skipped items.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
bat Exposure and Aftermath of Battle subscale grouped into the following categories: low (0 to 17), moderate (18 to 35), and high (36 to 45). Looking at the reported treatment for services, most of these veterans did not report having a service-connected disability (62 percent), and the proportion of veterans having a service-connected disability of less than 50 percent (18 percent) was the same as those with more than 50 percent disability (18 percent). Just over one-quarter (27 percent) of the veterans reported having been in treatment for a physical condition during the previous 24 months.
Geographic Distribution of Operation Enduring Freedom, Operation Iraqi Freedom, and Operation New Dawn Veterans
The committee’s survey was not designed to describe the geographic distribution of OEF/OIF/OND veterans. However, the U.S. Bureau of the Census American Community Survey (ACS) can be used to obtain that distribution, which can then be compared to the geographic distribution of all veterans. The ACS survey data are based on self-report of veteran status and service period and, therefore, do not align perfectly with the sample frame used for the committee’s survey, which used administrative records from the VA.
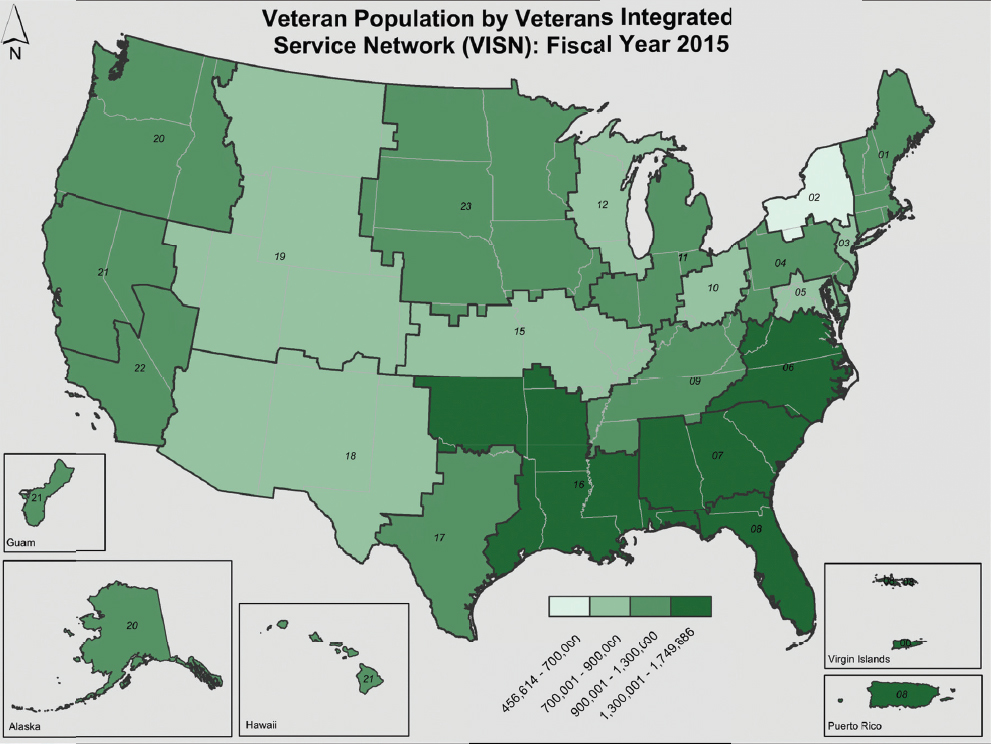
With regard to where veterans are living, Figure 6-3 shows the most populated Veterans Integrated Service Networks (VISNs) in 2014. As noted in Chapter 2, the VA is in the process of realigning its VISNs and, therefore, the current numbers and borders of the VISNs may differ from those in Figure 6-3. VISN 16 (South Central VA Health Care Network) is the most populated with veterans, and it contains the states of Arkansas, Louisiana, and Mississippi, as well as parts of Texas, Missouri, Alabama, and Florida. VISN 16 is projected by the VA to remain the most populated VISN for the next 25 years (VA National Center for Veterans Analysis and Statistics, 2016). For all veterans in total, as well as veterans under age 50, VA predicts that the south will remain the most heavily populated region by veterans, with clusters of veteran populations scattered throughout the rest of the country.
The ACS routinely collects data on U.S. adults’ self-reports of veteran status and service era. In 2015, the ACS estimated that approximately 1.2 percent of the U.S. population 18 and older is a U.S. military veteran. As shown in Table 6-3, on the basis of ACS self-reports, about 1 in 6 (16.7 percent) of all surviving U.S veterans included in the 2015 ACS sample report having served in the U.S. Armed Forces after September 2001.
SOURCE: VA, 2015f.
Likely due to the all-volunteer nature of the force and how recently they have served, OEF/OIF/OND-era veterans are numerically most concentrated in large, more populous states that also have large active U.S. military installations. In terms of absolute numbers, the top six states (see Table 6-4) account for an estimated 40 percent of the total OEF/OIF/OND veteran population.
TABLE 6-3 Percent of U.S Armed Forces Veterans by Service Era
| Service Era | % of Total Surviving Veterans |
|---|---|
| Total | 100% |
| OIF/OEF/OND | 16.7% |
| Persian Gulf War | 19.3% |
| Vietnam War | 36.0% |
| Korean War | 9.5% |
| WW II | 5.0% |
| All other periods | 13.5% |
NOTE: Population estimates from the 2015 American Community Survey.
SOURCE: U.S. Census Bureau, 2015.
TABLE 6-4 Six States with Largest Populations of OEF/OIF/OND Veterans
| State of Residency | 2015 ACS Estimated Percent of OEF/OIF/OND Veterans |
|---|---|
| Texas | 10% |
| California | 9% |
| Florida | 7% |
| Virginia | 6% |
| Georgia | 4% |
| North Carolina | 4% |
| All other states/territories | 60% |
| Total | 100% |
NOTE: Population estimates from the 2015 American Community Survey.
SOURCE: U.S. Census Bureau, 2015.
Mental Health Profile and Classification of Mental Health Care Need
This section summarizes the mental health profile of the group of OEF/OIF/OND veterans using estimates derived from the committee’s survey of veterans. The results are used to identify the need for mental health services among the OEF/OIF/OND veteran population. Estimating the need for mental health services is important to the question of why some veterans who need mental health care are not enrolled in VA mental health services. Many of the committee’s survey analyses in the report use the findings reported here.
The committee’s survey assessed the need for mental care using an analytic approach that dichotomized all OEF/OIF/OND veterans into two need groups—those who have a mental health need and those without a mental health need. Mental health need was determined on the basis of a survey respondent’s answers to (1) validated mental health screeners included in the survey, and (2) a survey question about having received a mental health diagnosis from a health care provider in the past 24 months. The five mental health screeners used in the study assessed possible recent or current symptoms of psychological distress, PTSD, major depression, alcohol dependence, and drug dependence. They are validated instruments widely used in the VA and elsewhere for identifying individuals needing further clinical assessment. Details about the screeners are in Chapter 5. A positive screening result indicates that an individual’s symptoms suggest a possible problem that warrants a comprehensive assessment by a mental health professional to determine a diagnosis and whether there is a need for treatment. A diagnosis cannot be made on the basis of screening results, and, therefore, it is important to note that the committee’s research did not produce an estimate of the prevalence of mental disorder diagnoses in this population. Chapter 4 has more information about VA mental health screening.
A veteran was classified as having a need for mental health care if the result on at least one mental health screener was positive or if the veteran reported receiving a mental health diagnosis from a health care provider in the previous 24 months. Table 6-5 shows percentage of OEF/OIF/OND veterans who screened positive on each mental health screener and the percentage who reported having received a mental health diagnosis in the past 24 months. Overall, 41 percent of veterans were found to have a potential need for mental health care. This estimate of mental health care need derived from the committee’s survey is consistent with results found in another national survey of Iraq and Afghanistan veterans, which reported that 43 percent of Iraq and Afghanistan veterans had probable PTSD, major depression, or alcohol misuse (Elbogen et al., 2013).
TABLE 6-5 Percentage of OEF/OIF/OND Veterans Who Have a Mental Health Need* by Screener and/or Received a Mental Health Diagnosis
| Mental Health Screener or Diagnosis | Unweighted n | Weighted N | Weighted % | Standard Error % |
|---|---|---|---|---|
| Total | 4,180 | 4,179,998 | – | – |
| Any mental health need based on positive screener or diagnosis: | 2,007 | 1,705,168 | 41.0% | 1.0% |
| Screened positive on: | ||||
| Psychological distress (Kessler) screener | 661 | 541,956 | 13.0% | 0.6% |
| PTSD screener | 1,279 | 965,520 | 23.2% | 0.8% |
| Depression screener | 795 | 682,963 | 16.4% | 0.7% |
| Alcohol dependence screener | 239 | 220,025 | 5.3% | 0.5% |
| Drug dependence screener | 116 | 111,223 | 2.7% | 0.3% |
| Mental health diagnosis in past 24 months | 1,502 | 1,179,971 | 28.4% | 0.9% |
NOTES: Percentages will not sum to 100 percent because OEF/OIF/OND veterans may screen positive for more than one condition.
*Mental health need could not be determined for 16 cases.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
Results from the individual mental health screeners in the committee’s survey showed 23 percent of the veterans screened positive for PTSD, 16 percent screened positive for major depression, and 13 percent screened positive on the Kessler six-item measure of general psychological distress. Five percent screened positive for alcohol dependence and 3 percent for drug abuse. In the survey by Elbogen et al. (2013), 20 percent screened positive for PTSD, 24 percent for major depression, and 27 percent for alcohol misuse. The large discrepancy between these two studies in the percentage scoring positive for problem drinking is likely accounted for by the different cut-offs each study used to score the Alcohol Use Disorder Identification Test scale, which assesses problems with drinking.
In the committee’s survey, 28 percent of OEF/OIF/OND veterans self-reported that they had received at least one mental health diagnosis in the previous 24 months. Among those who had a positive result on the mental health screeners, nearly 7 in 10 reported having had received a mental health diagnosis. Information on mental health and substance use disorders in the U.S. general population can be found in Chapter 4.
NEED FOR AND USE OF DEPARTMENT OF VETERANS AFFAIRS HEALTH CARE SERVICES
OEF/OIF/OND veterans have enrolled in VA health care at a higher rate than veterans from previous service eras. Since October 2001, approximately 61 percent of OEF/OIF/OND veterans have obtained some sort of health care (not just mental health care) at the VA (VA, 2015b). OEF/OIF/OND veterans are also more likely than members of other cohorts to have service-connected disabilities that bring them to the VA for care (RAND Corporation, 2015). Concerning veterans who do not use VA health services, it is estimated that “approximately 140,000 new veterans become eligible each year to receive health care through the VA,” but as noted above only slightly more than half of those veterans go on to actually use any of VA’s health care services (Lee et al., 2015). The VA itself similarly estimates that just under 40 percent of veterans have never used the VA for any health care service (VA, 2015b).
Distribution of Mental Health Service Need and Use
Estimates derived from the committee’s survey results provide insight into whether the VA is addressing the mental health care needs of OEF/OIF/OND veterans. Survey respondents, which included both users and non-users of VA services, were categorized in terms of (1) their possible need for mental health services (see discussion in previous section) and (2) their actual use of mental health services. Veterans were classified as users if they had received mental health care in the past 24 months from either the VA or from a non-VA provider. Veterans who did not receive mental health care in the past 24 months were considered non-users.
Table 6-6 shows the results of the analyses of the need for and use of mental health services. According to Table 6-5 above, 6 in 10 (59 percent) of OEF/OIF/OND veterans did not have a need for mental health services. Table 6-6 shows that among the remaining 41 percent who did have a mental health need, over half (55 percent) did not seek care, while 28 percent used VA services, and an additional 16 percent (8 percent of all OEF/OIF/OND veterans) sought non-VA care only. Among those who did not have a mental health need, there was negligible use of services, either VA or non-VA—that is, there were few false positives.
The presence of demographic differences between veterans who needed mental health services and those who did not are evident in Table 6-6. The differences by gender and race/ethnicity are quite modest. Only small differences were found for women relative to men, as well as for blacks and Hispanics relative to non-Hispanic whites. In contrast, much larger differences are evident by education, marital and employment status, and having or not having health insurance. Those with less than a college degree, who are no longer married, who are unemployed, and do not have health insurance are all disproportionately represented among those having a mental health need versus those with a college degree or more, who are married, employed, and who have health insurance, respectively. That is, the latter are all more likely to be among those with no need for mental health services.
To summarize Tables 6-5 to 6-7, the survey data demonstrate several important relationships between the need for and use of mental health care services among OEF/OIF/OND veterans. First, about 41 percent, or about 1.7 million veterans, in this cohort have a mental health need, as shown Table 6-5. Second, of the remaining 2.5 million or so veterans who do not have a mental health need, the overwhelming majority (96 percent) do not use either VA or non-VA mental health services; see Table 6-6. Third, Table 6-6 also shows that of those 1.7 million or so veterans who do have a mental health need, over half (55 percent) are not using any mental health services; that is, there is a substantial level of potential unmet need for mental health services in this cohort. Finally, Table 6-7 shows that of those veterans who have a mental health need and do use mental health services, about 36 percent use non-VA mental health services, but the majority (64 percent) use the VA’s mental health services.
User Groups and Sources of Service Use
The committee’s survey also allowed for a more detailed breakdown of these user groups by the sources the veterans used for mental health services. Specifically, to further examine where OEF/OIF/OND veterans were receiving these services, the committee described the types of health care providers seen by veterans in each use group, as shown in Table 6-7. Overall, 64 percent of all OEF/OIF/OND veterans who had a mental health need and sought care used the VA. Within that group, about 62 percent (or 39 percent of all veterans with need who use the VA) access mental services through a combination of a VA primary care provider, VA mental health treatment facilities, and Vet Centers, while 23 percent (15 percent out of the 64 percent) use a VA primary care provider only, and 8 percent (4.8 percent out of the 64 percent) use VA mental health facilities only, and 4 percent (2.5 percent out of 64 percent) use Vet Centers only.
TABLE 6-6 Percentage of OEF/OIF/OND Veterans by Mental Health Need,* Service Use, and Demographic Characteristics
| Demographic Characteristics | All OEF/OIF/OND Veterans | Mental Health Need | No Mental Health Need | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | |
| Total | 4,180 | 4,179,998 | 100% | – | 2,007 | 1,705,168 | 100% | – | 2,157 | 2,453,388 | 100% | – |
| Mental health service use | ||||||||||||
| No use | 2,915 | 3,296,850 | 79.3% | 0.6% | 890 | 941,504 | 55.2% | 1.2% | 2,025 | 2,355,346 | 96.0% | 0.6% |
| VA use | 913 | 515,925 | 12.4% | 0.4% | 849 | 476,654 | 28.0% | 0.9% | 64 | 39,270 | 1.6% | 0.3% |
| Non-VA use only | 308 | 317,086 | 7.6% | 0.5% | 256 | 272,799 | 16.0% | 1.2% | 52 | 44,287 | 1.8% | 0.4% |
| Missing | 28 | 28,694 | 0.7% | 0.2% | 12 | 14,210 | 0.8% | 0.3% | 16 | 14,484 | 0.6% | 0.2% |
| Gender | ||||||||||||
| Male | 2,946 | 3,303,305 | 79.0% | 0.8% | 1,359 | 1,312,186 | 77.0% | 1.1% | 1,572 | 1,969,877 | 80.3% | 1.2% |
| Female | 1,220 | 859,250 | 20.6% | 0.8% | 642 | 386,589 | 22.7% | 1.1% | 577 | 472,461 | 19.3% | 1.2% |
| Missing | 14 | 17,442 | 0.4% | 0.1% | 6 | 6,393 | 0.4% | 0.2% | 8 | 11,050 | 0.5% | 0.2% |
| Race/Ethnicity | ||||||||||||
| Non-Hispanic white only | 2,636 | 2,762,440 | 66.1% | 0.8% | 1,187 | 1,071,175 | 62.8% | 1.3% | 1,441 | 1,681,093 | 68.5% | 1.0% |
| Non-Hispanic black only | 644 | 537,059 | 12.8% | 0.5% | 371 | 254,662 | 14.9% | 0.8% | 271 | 280,705 | 11.4% | 0.7% |
| Hispanic | 503 | 490,740 | 11.7% | 0.6% | 263 | 223,566 | 13.1% | 1.1% | 238 | 265,738 | 10.8% | 0.5% |
| American Indian/Alaska | 109 | 108,708 | 2.6% | 0.4% | 69 | 54,395 | 3.2% | 0.5% | 40 | 54,313 | 2.2% | 0.5% |
| Native | ||||||||||||
| Other or multiple races | 240 | 247,127 | 5.9% | 0.6% | 92 | 86,354 | 5.1% | 0.6% | 144 | 152,630 | 6.2% | 0.7% |
| Missing | 48 | 33,924 | 0.8% | 0.1% | 25 | 15,015 | 0.9% | 0.2% | 23 | 18,909 | 0.8% | 0.2% |
| Education | ||||||||||||
| Less than a 4-year college degree | 2,204 | 2,218,603 | 53.1% | 1.0% | 1,233 | 1,086,043 | 63.7% | 1.2% | 960 | 1,117,194 | 45.5% | 1.4% |
| 4-year college degree or more | 1,969 | 1,956,133 | 46.8% | 1.0% | 770 | 617,723 | 36.2% | 1.2% | 1,194 | 1,332,334 | 54.3% | 1.4% |
| Refused | 1 | 796 | 0.0% | 0.0% | – | – | – | – | 1 | 796 | 0.0% | 0.0% |
| Don’t know | 1 | 463 | 0.0% | 0.0% | 1 | 463 | 0.0% | 0.0% | – | – | – | – |
| Missing | 5 | 4,002 | 0.1% | 0.1% | 3 | 938 | 0.1% | 0.0% | 2 | 3,064 | 0.1% | 0.1% |
| Marital status | ||||||||||||
| Married or civil commitment or union | 2,585 | 2,688,394 | 64.3% | 0.7% | 1,119 | 961,783 | 56.4% | 1.4% | 1,457 | 1,713,737 | 69.9% | 0.9% |
| Never married | 711 | 745,414 | 17.8% | 0.6% | 356 | 337,130 | 19.8% | 1.3% | 351 | 403,114 | 16.4% | 0.8% |
| No longer married | 868 | 732,858 | 17.5% | 0.7% | 522 | 399,266 | 23.4% | 1.2% | 344 | 332,230 | 13.5% | 0.8% |
| Don’t know | 5 | 1,959 | 0.0% | 0.0% | 5 | 1,959 | 0.1% | 0.1% | – | – | – | – |
| Missing | 11 | 11,373 | 0.3% | 0.1% | 5 | 5,031 | 0.3% | 0.2% | 5 | 4,306 | 0.2% | 0.1% |
| Employment | ||||||||||||
| Not employed | 1,092 | 959,181 | 22.9% | 0.7% | 716 | 546,752 | 32.1% | 1.1% | 371 | 405,989 | 16.5% | 1.0% |
| Employed | 2,992 | 3,104,253 | 74.3% | 0.8% | 1,244 | 1,117,750 | 65.6% | 1.2% | 1,740 | 1,975,355 | 80.5% | 1.1% |
| Missing | 96 | 116,563 | 2.8% | 0.4% | 47 | 40,666 | 2.4% | 0.4% | 46 | 72,043 | 2.9% | 0.5% |
| Health insurance | ||||||||||||
| Not insured | 644 | 427,500 | 10.2% | 0.4% | 464 | 292,944 | 17.2% | 0.9% | 178 | 133,309 | 5.4% | 0.6% |
| Insured | 3,357 | 3,519,268 | 84.2% | 0.6% | 1,450 | 1,295,612 | 76.0% | 1.2% | 1,894 | 2,205,496 | 89.9% | 0.9% |
| Missing | 179 | 233,229 | 5.6% | 0.5% | 93 | 116,612 | 6.8% | 0.7% | 85 | 114,582 | 4.7% | 0.5% |
NOTES: Columns and rows may not sum to totals due to missing values. Missing includes skipped items. SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
*Mental health need could not be determined for 16 cases.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| User Group and Source of Service Use | Unweighted n | Weighted N | Weighted % | Standard Error % |
|---|---|---|---|---|
| Total users of mental health services | 1,105 | 749,453 | 100% | – |
| Need, VA user | 849 | 476,654 | 63.6% | |
| VA primary care provider only | 189 | 110,095 | 14.7% | 1.1% |
| VA mental health treatment facility only | 73 | 36,155 | 4.8% | 0.6% |
| Vet Center only | 33 | 19,032 | 2.5% | 0.6% |
| A combination of the above sources | 521 | 294,341 | 39.3% | 1.7% |
| Unspecified service use | 30 | 16,056 | 2.1% | 0.5% |
| Missing | 3 | 974 | 0.1% | 0.1% |
| Need, non-VA user | 256 | 272,799 | 36.4% | |
| Non-VA provider, paid for by the VA | 9 | 9,145 | 1.2% | 0.6% |
| Other, not paid for by the VA | 241 | 259,356 | 34.6% | 2.1% |
| A combination of the above sources | 6 | 4,299 | 0.6% | 0.3% |
NOTE: Responses may not sum to 100% due to rounding. Missing includes skipped items.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
Thirty-six percent of veterans who have a mental health need and who seek care use non-VA providers. Nearly all of these veterans (35 percent of the 36 percent) use care in the private sector that is completely independent of the VA (that is, is not paid for by the VA).
Potential and Perceived Need for Mental Health Services
In addition to measuring the potential need for mental health care on the basis of screening results or a reported diagnosis as previously described under Mental Health Profile and Classification of Mental Health Care Need, the committee’s survey of users and non-users of VA health services assessed whether veterans perceived a need for professional help. To measure perceived need for mental health care, veterans were asked, “Was there ever a time in the past 24 months when you felt you might need to see a professional because of your problems with emotions or nerves or your use of alcohol or drugs?” The committee was interested in exploring this perception of need because it could be critically important in understanding whether help is actually sought.
Table 6-8 shows (1) the number of veterans who have a mental health need based on the screeners and diagnoses, (2) the percentage who report having a perceived mental health care need, and (3) their combined relationships with use of mental health services. Table 6-8 highlights several important facts. One is that of the estimated 1.7 million OEF/OIF/OND veterans who have a mental health need, only about half (47 percent) perceive that they might have a mental health care need, suggesting that self-awareness regarding one’s mental health is not synonymous with screening positive or being told by a medical professional that one has such a need. Indeed, since over half of the veterans (52 percent) who have a positive screen or a reported diagnosis did not perceive a need for mental health services, it seems likely that a major reason for veterans not seeking care is that they personally do not perceive a need for such services.
While a veteran’s perceptions about whether he or she needs mental health services are not the same as assessed need according to a clinician’s diagnosis or a positive result on a screening test, veterans’ perceptions are reasonably well correlated with assessed need, in the following sense. If a veteran perceives
TABLE 6-8 Percentage of OEF/OIF/OND Veterans by Mental Health Need, Perceived Need,* and User Group
| Demographic Characteristics | All OEF/OIF/OND Veterans | Mental Health Need | No Mental Health Need | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | |
| Total | 4,180 | 4,179,998 | 100% | – | 2,007 | 1,705,168 | 100% | – | 2,157 | 2,453,388 | 100% | – |
| Perceived need | 1,100 | 915,775 | 21.9% | 0.9% | 961 | 799,982 | 46.9% | 1.6% | 139 | 115,793 | 4.7% | 0.5% |
| No use | 453 | 452,189 | 10.8% | 0.7% | 338 | 353,079 | 20.7% | 1.1% | 115 | 99,110 | 4.0% | 0.5% |
| VA use | 456 | 260,502 | 6.2% | 0.3% | 456 | 260,502 | 15.3% | 0.7% | – | – | – | – |
| Non-VA use only | 159 | 177,910 | 4.3% | 0.4% | 159 | 177,910 | 10.4% | 0.9% | – | – | – | – |
| Missing user group | 32 | 25,174 | 0.6% | 0.1% | 8 | 8,491 | 0.5% | 0.2% | 24 | 16,683 | 0.7% | 0.2% |
| No perceived need | 3,042 | 3,223,961 | 77.1% | 0.9% | 1,032 | 891,739 | 52.3% | 1.5% | 2,008 | 2,328,150 | 94.9% | 0.5% |
| No use | 2,448 | 2,828,944 | 67.7% | 0.9% | 547 | 581,244 | 34.1% | 1.4% | 1,901 | 2,247,700 | 91.6% | 0.7% |
| VA use | 386 | 212,964 | 5.1% | 0.3% | 386 | 212,964 | 12.5% | 0.7% | – | – | – | – |
| Non-VA use only | 95 | 91,812 | 2.2% | 0.3% | 95 | 91,812 | 5.4% | 0.7% | – | – | – | – |
| Missing user group | 113 | 90,241 | 2.2% | 0.3% | 4 | 5,719 | 0.3% | 0.2% | 107 | 80,450 | 3.3% | 0.5% |
NOTES: Responses may not sum to totals due to rounding. Columns and rows may not sum to totals due to rounding or due to missing values in perceived need or mental health need. SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
*As measured by the survey item, “Was there ever a time in the past 24 months when you felt you might need to see a professional because of your problems with emotions or nerves or your use of alcohol or drugs?”
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
that he or she has a mental health need, the perception agrees with the screening result about 87 percent of the time (799,982 veterans with positive screens or a reported diagnosis out of 915,775 veterans with perceived need). On the other hand, if a veteran perceives that he or she does not have a mental health need, this agrees with the screening result about 72 percent of the time (2,328,150 veterans who do not have a positive screen or a reported diagnosis out of 3,223,961 with no perceived need).
In keeping with this relatively strong association between assessed and perceived need, Table 6-8 further explores the role of perceived need on the relationship between assessed need and service use. First, for those estimated 2.5 million veterans with no assessed mental health care needs, the overwhelming majority of 96 percent (2,346,810 non-users out of 2,453,388) do not use mental health services. This is true whether or not they perceive need (86 percent or 99,110 non-users out of 115,793 veterans with perceived need and no mental health need; 97 percent or 2,247,700 non-users out of 2,328,150 veterans with no perceived need and no mental health need).
Next, consider those estimated 1.7 million veterans with mental health care needs. Among these veterans with assessed needs, about half (52 percent) do not perceive a need and about half (47 percent) do perceive a need, as mentioned above. Of those who have a need but do not perceive it, about 65 percent do not seek care (581,244 veterans out 891,739). One might expect that none of these veterans would seek care if they do not believe that they need to see a mental health provider, but in fact about one-third (34 percent or 304,776 veterans out of 891,739) still seek care.
Finally, of these estimated 799,982 veterans who have an assessed need and perceive a need, about 44 percent (353,079 veterans out of 799,982) do not seek care, despite their perception. About 55 percent of veterans with assessed and perceived need do seek care (438,412 veterans out of 799,982), in contrast with only 34 percent of veterans with assessed need but no perceived need.
The results in Table 6-8 show that the perception of a mental health condition is an important factor in the likelihood of getting care, although some veterans who do not perceive that they need mental health care still do seek mental health services. It could be possible that these veterans may not perceive a need for care because their needs are being met and the care is working. Veterans who have an assessed need and perceive such a need are more likely to seek care than those who do not perceive their need, but there remains a substantial chance that they will not seek care despite their perceived need. This lack of perception of need for mental health care is among the barriers to accessing care. Other barriers are discussed below.
Table 6-9 examines the relationship between assessed need (positive screen or reported diagnosis) and perceived need for mental health care. A veteran’s likelihood of perceiving a need for mental health care varies by the different screeners that the committee used to assess need. Looking at mental health care need by the individual screeners, Table 6-9 shows that, among those who screened positive for PTSD, 53 percent perceived they had a need for care. The same percentage reported having received a diagnosis. Veterans who screened positive for drug dependence or alcohol dependence are the most likely to have a perceived need for care (75 and 67 percent, respectively). Forty-seven percent of veterans had a positive screener or diagnosis and had a perceived need. Sixty percent of veterans with two or more positive screeners or one or more positive screeners and a reported diagnosis perceived a need for mental health care.
Logistic regression analysis was used to examine how demographic characteristics and experiences affect the likelihood of having a mental health care need and the perception of a mental health care need, while adjusting for other factors such as race/ethnicity, age, and sex. This approach permits exploring the effect of any one variable on the probability of need (either perceived or assessed) while controlling for other attributes.
| Screener or Diagnosis | Perceived Need and Positive Screener: Unwgt n | Perceived Need and Positive Screener: Wgt N | Positive Screener: Unwgt n | Positive Screener: Wgt N | Perceived Need Among Those Screening Positive: Wgt % | Standard Error |
|---|---|---|---|---|---|---|
| Any mental health care need based on positive screener or diagnosis | 961 | 799,982 | 2,007 | 1,705,168 | 46.9% | 1.6 |
| Psychological distress (Kessler) screener | 435 | 351,815 | 661 | 541,956 | 64.9% | 1.9 |
| PTSD screener | 681 | 511,504 | 1,279 | 965,520 | 53.0% | 1.7 |
| Depression screener | 467 | 380,048 | 795 | 682,963 | 55.6% | 2.0 |
| Alcohol dependence screener | 167 | 148,347 | 239 | 220,025 | 67.4% | 4.1 |
| Drug dependence screener | 90 | 83,825 | 116 | 111,223 | 75.4% | 4.3 |
| Diagnosed in past 24 months | 778 | 619,125 | 1,502 | 1,179,971 | 52.5% | 1.6 |
| A combination of 2 or more of the above | 737 | 582,227 | 1,251 | 969,428 | 60.1% | 1.5 |
NOTE: Weighted % will not sum to 100% because veterans may screen positive for more than one condition. Unwgt n = unweighted n; Wgt = weighted.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
All logistic regression models were fitted using SAS proc surveylogistic to account fully for the complex survey design. Furthermore, model fit for each logistic regression was examined using the Hosmer-Lemeshow Goodness of Fit more(GOF) test (Hosmer and Lemeshow, 1980). Because this GOF test is not a feature of surveylogistic, the fits were recomputed using proc logistic with the sampling weights. This approach produces the same weighted point estimates as proc surveylogistic and allows calculation of the observed and expected frequencies used in the GOF test. A significant chi-square statistic indicates evidence of lack of model fit.
Table 6-10 describes the independent variables used in the regression models discussed here and in other sections of the report. These variables include demographic, socioeconomic, military/service-related experience, and clinical measures; the reference category for each variable is shown in the table. (The regression models discussed later use additional independent variables, which are shown in Table 6-20.) The combat-exposure variable was based on the DRRI Combat Exposure subscale that is discussed in more detail in Chapter 5. Because of the availability of two distinct measures of deployment (length and number of deployments), an alternative set of regression models that include the number of deployments (0, 1, 2 or more) was also estimated. Veterans who had missing data on one or more of the variables in the regression were excluded from the analysis, and, for this reason, the effective sample size varies across regression models. In the regression models, the association of each independent variable with the dependent variable was examined in bivariate regression. Only the independent variables that were statistically significant at the bivariate, or the full-model stage, were included in the final model. There were no observed changes in coefficients or standard errors between the bivariate and full models that would suggest a serious problem with multicollinearity.
TABLE 6-10 Core Independent Variables Used in the Multivariate Analyses
| Variable | Description | Missing n |
|---|---|---|
| Female | Male (reference), Female | 14 |
| Educational level | Less than college (reference), some college, associate’s or bachelor’s degree, master’s degree or higher | 7 |
| Marital status | Married (reference), Never married, No longer married | 16 |
| Age | 18 to 29 (reference), 30 to 39, 40 to 49, 50+ | 36 |
| Race | Non-Hispanic white (reference), Non-Hispanic black, Hispanic, American Indian/Alaska Native, other or multiple races | 48 |
| Income | Less than $25,000 (reference), $25,000 to $49,999, $50,000 to $74,999, $75,000+ | 98 |
| Employment status | Employed (reference), unemployed, out of the labor force | 96 |
| Unit component | Active duty (reference), Reserve/Guard | 20 |
| Branch of service | Army (reference), Air Force, Navy/Coast Guard, Marine Corps, multiple branches | 16 |
| Rank | E4 or less (reference), E5–E6, E7–E9, Officer | 18 |
| Cumulative length of deployment | Not deployed (reference), 0–6 months, 7–12, 25–36, 37–48, more than 48 months | 25 |
| Number of combat deployments | Not deployed (reference), 1, 2 or more | 37 |
| DRRI combat exposure | Low: 0 to 17 (reference), Moderate: 18 to 35, High: 36 to 54 | 91 |
| Disability rating | No disability (reference), less than 50%, 50% or more | 81 |
| PTSD score | Sum of four items such as In the past month were you constantly on guard, watchful, or easily startled? or, Felt numb, detached from others, activities, or your surroundings? | 17 |
| Drug dependence score | Sum of ten items such as In the past 12 months have you abused more than one drug at a time? or, Have you neglected your family because of your drug use? | 35 |
| Alcohol dependence score | Sum of ten items such as How often do you have six or more drinks on one occasion? or, Have you or someone else ever been injured as a result of your drinking? | 32 |
| Depression score | Sum of two items: Over the past two weeks, how often have you been bothered by any of the following problems: Little interest or pleasure in doing things? Feeling down, depressed, or hopeless? | 13 |
| Perceived mental health need | No (reference), Yes | 38 |
| Insured | Not insured (reference), Insured | 179 |
NOTE: The Kessler scale was not included in the regressions because it is not a screener for any specific condition but rather general psychological distress.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
Positive Screen for Mental Health Care Need
A logistic regression was first used to examine how demographic and military characteristics were associated with the odds of screening positive for any mental health disorder. In a second step, the committee examined each screen separately. The dependent variables in these regressions are indicators for (1) whether a veteran screened positive for any mental health disorder and (2) separately, whether he or she screened positive for specific disorders—PTSD, depression, alcohol use disorders, and drug use disorders.4 An additional six logistic regression models were fitted using perceived need as the dependent variable; those results are discussed in the next section.
___________________
4 Results from the Kessler Screening Scale for Psychological Distress were not included in the regressions because it is not a screener for any specific condition but rather for general psychological distress. Only screeners for specific conditions were
| Variable | Variable Value | Odds Ratio | Lower CL | Upper CL |
|---|---|---|---|---|
| Female | Female | 1.491** | 1.134 | 1.960 |
| Age | 50+ years old | 0.657* | 0.474 | 0.911 |
| Marital status | No longer married | 1.621** | 1.259 | 2.088 |
| Unit component | Reserves/Guard | 0.748* | 0.577 | 0.969 |
| Rank | E5–E6 | 0.724* | 0.541 | 0.969 |
| Rank | E7–E9 | 0.543** | 0.382 | 0.771 |
| Rank | Officers | 0.340** | 0.217 | 0.533 |
| Branch | Air Force | 0.764** | 0.623 | 0.937 |
| Branch | Multiple branches | 1.874** | 1.427 | 2.462 |
| DRRI Combat | Moderate | 2.609** | 2.026 | 3.359 |
| DRRI Combat | High | 8.544** | 4.607 | 15.845 |
| Employment | Not employed | 2.310** | 1.609 | 3.316 |
| Employment | Not in labor force | 1.861** | 1.404 | 2.467 |
| Income | $75,000 or more | 0.649* | 0.465 | 0.905 |
| Disability rating | Disability 50 percent or higher | 3.837** | 3.032 | 4.856 |
| Disability rating | Disability less than 50 percent | 1.477** | 1.191 | 1.833 |
NOTES: *p<.05; **p<.01; 95 percent confidence limits (CL) for the odds ratios.
4,180 unweighted cases initially available, 613 unweighted cases excluded due to missing responses.
Model includes 3,567 unweighted cases representing weighted N of 3,493,024.
The reference category for each variable is shown in Table 6-10.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
Table 6-11 shows the adjusted odds ratios from the logistic regression model of the probability of having a mental health care need that includes the cumulative length of deployment instead of the number of deployments as a covariate. Odds ratios greater than 1 indicate that the factor (variable value) is associated with an increased risk of the mental health condition relative to the base case; odds ratios less than 1 indicate that the factor is associated with a decreased risk; odds ratios equal to 1 indicate parity, that is, that there is no difference in risk. The table also shows the 95 percent confidence limits (CL) for the odds ratios. When the confidence interval includes the value 1, the odds ratio is not significantly different from 1. Reported odds ratios are adjusted for all other variables shown in the model.
Overall, this model of the probability of having a mental health care need shows that most of the independent variables are statistically significantly related to need. Combat exposure is the strongest predictor of screening positive for a mental health condition. Odds of screening positive for a mental health condition were eight times higher for veterans who were high on the DRRI combat exposure scale compared to those who scored low on the DRRI, and the odds were two times higher even among those with moderate exposure. Disability status is also a strong predictor; the odds of screening positive for a mental health need were close to four times higher among those having a disability rating of more than 50 percent compared to those with no disability, and the odds were one and a half times greater among those with less than 50 percent. Other factors associated with the increased odds of a positive mental health screen are being female, being divorced, being out of the labor force or unemployed, and having served in multiple branches of service. In contrast, being over 50, having higher income, being in the Reserves or National Guard, in the Air Force relative to the Army, and being a senior enlisted person
___________________
included in order to identify the unique effects of depression, PTSD, etc., and including results from the Kessler screener would have possibly confounded the effects, making the results difficult to interpret.
| Screener Score | Odds Ratio | Lower CL | Upper CL |
|---|---|---|---|
| Psychological distress (Kessler) | 1.255** | 1.233 | 1.278 |
| PTSD | 2.041** | 1.940 | 2.148 |
| Depression | 1.797** | 1.705 | 1.893 |
| Alcohol dependence | 1.128** | 1.108 | 1.148 |
| Drug dependence | 1.779** | 1.564 | 2.024 |
| Number of positive screeners | 2.634** | 2.454 | 2.828 |
NOTES: *p<.05; **p<.01; 95 percent confidence limits (CL) for the odds ratios.
4,180 unweighted cases initially available, 655 unweighted cases excluded due to missing responses.
Model includes 3,525 unweighted cases representing weighted N of 3,463,029.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
or officer ranks lowers the odds of screening positive for a mental health condition. Factors which are not significantly related to mental health need—when these other predictors are taken into account—are education level, race, cumulative length of deployments, having health insurance, scores on the individual mental health screeners, and perceived need.
Perceived Mental Health Care Need
Two additional logistic regression models were used to examine perceived need and its relationship with factors such as screener scores and demographic and military attributes, as shown in Tables 6-12 and 6-13. Refer to Table 6-10 for a list of independent variables used in the regression models. Only the independent variables that were statistically significant at the bivariate stage, or the full-model stage, were included in the final model.
The model summarized in Table 6-12 regressed perceived need against the screener results, and produced unadjusted odds ratios for the effect that each positive screen has on the probability that a person perceives that he or she has a mental health problem. This model included the continuous scores on five screener variables: psychological distress, PTSD, depression, alcohol use disorder, and drug use disorder. These variables were included to examine whether veterans with specific mental health symptoms are more or less likely to have a perceived need, as this likely affects the decision to seek
| Variable | Variable Value | Odds Ratio | Lower CL | Upper CL |
|---|---|---|---|---|
| Female | Female | 2.196** | 1.648 | 2.927 |
| Unit component | Reserve/Guard | 0.655* | 0.470 | 0.911 |
| Income | $50,000 to $74,999 | 1.864** | 1.337 | 2.599 |
| PTSD score | Continuous | 1.614** | 1.492 | 1.747 |
| Depression score | Continuous | 1.418** | 1.326 | 1.517 |
| Alcohol dependence score | Continuous | 1.090** | 1.066 | 1.114 |
| Drug dependence score | Continuous | 1.346** | 1.182 | 1.533 |
NOTES: *p<.05; **p<.01; 95 percent confidence limits (CL) for the odds ratios.
4,180 unweighted cases initially available, 655 unweighted cases excluded due to missing responses.
Model includes 3,525 unweighted cases representing weighted N of 3,463,029.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
care. By contrast, the second model included demographic variables, military experience measures, and a categorical measure of the number of mental health conditions for which a veteran screened positive (0, 1, 2 or more). This model allows us to examine the dose–response association between the number of elevated screens and the perceived need.
Table 6-12 shows the unadjusted odds ratios for the relationship between the continuous screener scores and perceived need. All of the odds ratios are positive and statistically significant, indicating that higher screener scores are associated with a higher probability of perceived need for mental health treatment. PTSD was most strongly associated with perceived need. The number of positive screens was also a strong predictor of perception of need.
Table 6-13 shows the estimated adjusted odds of perceiving a mental health care need when demographic and military experience variables are included in the model. As that table shows, few demographic factors are significantly associated with perceived need once the screener scores are taken into consideration. The only variables other than screeners associated with perceived need are gender, income, and service in the Guard/Reserve. As the results show, females have more than double the odds of perceiving a need than males and those in middle-income brackets ($50,000 to $75,000) have close to double the odds of perceiving a mental health need compared those in the lowest income bracket. Also, those in the Reserve/National Guard are significantly less likely than those classified as active duty to report a perceived need.
Other than these three results, none of the demographic and military experience variables were significantly associated with perceived need. In contrast, each of the continuously scored screener scales was significantly associated with perceived need leading to the conclusion that the perception of need is primarily associated with the cumulative burden or severity of the need as indicated by the screeners.
Finally, the committee notes that neither having a mental health care need nor perceiving that one has a need necessarily translates into use of services. Therefore, to identify factors that may influence the use of mental health care services in the future, the committee examined barriers and facilitators that are associated with mental health care service use at present. The committee focused on veterans who have a mental health care need.
BARRIERS AND FACILITATORS TO SERVICE USE
There are numerous types of potential barriers and facilitators to using health care, including VA system factors such as awareness of eligibility for services, understanding how VA is organized, access factors (for example, the distance to services, the ease of getting appointments, and the availability of providers and services), individual factors (for example, opinions about VA health services, attitudes toward mental health treatment, concerns about confiscation of firearms, employment, and other competing personal demands), and combination factors (for example, the perceived availability of services and providers).
This section presents both survey and site visit interview results about barriers and facilitators to service use.
Eligibility Knowledge
Perhaps the first requirements to obtain VA mental health care are having an awareness of its existence and having knowledge about one’s eligibility. Unfortunately, many veterans appear to be unaware of both the existence of services and their own eligibility. For example, of the survey respondents who have had a mental health need but did not use VA mental health services, 33 percent reported that they were not aware that VA offered mental health services and 42 percent did not know how to apply for
VA mental health benefits. An additional 30 percent of survey respondents “did not feel they deserved” to receive mental health care from the VA and 40 percent did not think they were “entitled to or eligible for” VA mental health care. These results are shown in Table 6-15. Given how complex the VA eligibility guidelines are, it is quite possible that this complexity contributes to veterans’ uncertainty; see Box 6-1 for a summary of eligibility categories.
The site visit interviews reinforced the supposition that a veteran needs to have a significant amount of information to successfully enroll with the VA, starting with the understanding that he or she is, indeed, a “veteran”:
[It] took me a very, very long time to realize I even qualify as a veteran. . . . I considered veterans somebody who had been to combat. . . . [Battle Creek, Michigan]
Probably 50 percent of the folks that I talk to that have not come into the VA believe they can’t come unless they’re service-connected, which is not true. [Topeka, Kansas]
The expanded eligibility criteria described earlier in this chapter, which affect veterans serving in combat theaters in support of OEF, OIF, and OND, adds to veterans’ confusion about whether they qualify for services. Many veterans reported a lack of knowledge about the VA and eligibility for services, despite the fact that all service members must attend a Transitional Assistance Program (TAP) before leaving active duty. Interviewees often said that the information about the VA shared at TAP was sparse or non-existent. The following quotes are typical of what site visitors heard:
No one explained to us how to enter the VA system or how to access the health care benefits we had. A group of at least 140 were in my week-long transition class. At no point did we hear that information. [Seattle, Washington]
Similarly, interviewees reported a lack of information about eligibility for services under military sexual trauma (MST) policies:
It’s always been the case that veterans who report MST can be eligible for mental health-related care. . . . Some veterans tell me they think only combat veterans can come to the VA or poor veterans. [Charleston, South Carolina]
Yet even if the information were shared, interviewees indicated that TAP classes are at the wrong time for a service member to try to retain critical information about such things as health care eligibility; veterans say they feel overwhelmed. Such “information overload” is even more difficult for individuals with cognitive challenges from PTSD or a TBI.
Transitioning from the military to the VA system is often challenging for veterans who entered the military shortly after high school. Many are on their own and paying rent and bills for the first time, while lacking the camaraderie and identity they just spent years building. A Veterans’ Service Organization staff member summed up the difficult transition in this manner:
You go from mom and dad’s house to the military . . . get out after 4 years . . . without somebody providing you structure. . . . I always say, “The VA is not your NCO [non-commissioned officer]. They’re not going to give you that structure.” . . . A lot of them have what I call culture shock. [Battle Creek, Michigan]
A veteran offered a similar perspective, saying, “It’s been my experience with the VA that they stand up and say, ‘We’re here to help you . . . but you’ve got to navigate the maze.’” [El Paso, Texas]
During the site visits, veterans also reported frustration with inconsistent information or misinformation about VA eligibility. One caregiver of a veteran in Charleston, South Carolina, said, “He’s gone to
the VA in Columbia. He’s gone to the VA in Salisbury. He’s hitting different VAs, and they’re all telling him different things.” Similarly, another caregiver in San Diego, California, said, “She was just trying to get her VA ID card. . . . Every time she called, she was given different information, even though she was asking the same question.” The caregiver added, “How do you have confidence in a system that can’t get you consistent information?”
Understanding the Veterans Health Administration and the Veterans Benefits Administration
Understanding how various benefits and services are organized within the VA system is a major hurdle for many veterans seeking VA care. Across all the sites visited, veterans conveyed confusion about the differences between the VBA and the Veterans Health Administration (VHA), two operating components of the VA. Most veterans appeared to understand that they need to go through VBA’s disability compensation process to document their service-connected disabilities. Many veterans, however, incorrectly assumed that this process, which involves medical assessments by VA clinicians, sets them up for health care through the VA. These veterans are unaware that enrollment in the VHA is a completely separate process, and they are often waiting in vain for someone to contact them about mental health appointments.
Some VA medical centers (VAMCs) are making an effort to reduce the confusion between VHA and VBA services. For example, because many veterans apply for disability, but never enroll for health care, the Palo Alto VAMC has started a program where staff are notified each time an OEF/OIF/OND veteran in that location goes through a disability examination. A member from the transition team then calls the veteran and works to engage him or her in health care. The VA staff referred to this program as “groundbreaking because they [VBA and VHA] have always maintained that the two systems have to be separate.”
A related issue is that if veterans have a negative experience with the disability claims process, they may be turned off from seeking care from the VA because they assume that it will be unsatisfactory. A clinician in Charleston said, “I think the biggest thing is that the veterans get it all confused. They hear one thing about claims not going through, and they think that’s how the VA doctors are going to be.”
In addition to the confusion between the VHA and VBA, both veterans and staff raised the possibility that disability compensation may be affecting veteran treatment-seeking behavior. For example, in several locations, clinical staff expressed the view that the disability and compensation system incentivizes veterans to be “sick” and to continue to use clinical resources that might better serve someone else.
Some veterans similarly expressed their fears that if they stop getting services or show signs of improvement, they will lose some or all of their disability compensation:
I notice that in order for me to keep my benefits I have to stretch the truth a little bit. . . . I’m still struggling, but it’s getting better . . . if I lose my percentages, then I lose a lot more benefits that the VA has to offer. [Palo Alto, California]
Interestingly, other VA staff and veterans countered this perspective. Their view was that veterans were avoiding care in order to maintain their incomes:
Some people are afraid to go get care from the VA. . . . Because if you get better in any way. . . they lower your rate. . . . I do my mental health care mainly through the Vet Center because they don’t report back to Comp and Pen on everything. [Palo Alto, California]
Many veterans who use VA health care are low income and their disability compensation is financially important to them. As one clinician in Nashville said, “When they call these veterans for a reevaluation, these veterans get desperate . . . afraid they are going to lose their disability payment. For a lot of them, that’s all they have to eat.” From these reports, it seems the disability system can leave many veterans conflicted about how best to proceed in treatment.
The VA’s Veterans Satisfaction Survey (VSS), an annual survey of veterans served by the VA, also asks veterans about mental health services and disability compensation. Veterans are asked to rate the statement, “I believe it is necessary for me to stay in mental health treatment to keep my service connected disability,” on a scale of 1 to 5, where 1 is strongly disagree, 5 is strongly agree, and 3 is neither. For FY 2016,5 the VA reported a mean rating of 3.26 (standard deviation = 1.27) among OEF and OIF respondents (VA, 2016). This result and veterans’ perspectives reported in the site visits may suggest a closer examination of veterans’ understanding of disability compensation and treatment-seeking behavior is warranted. See Chapter 15 for details about the VSS.
Veteran Perspectives Regarding Barriers and Facilitators to Service Use
In its survey of veterans, the committee examined barriers and facilitators to VA service use for three groups of veterans who have a mental health care need. Each user group reported on various topics:
Among users of VA mental health services
- Reasons for using VA services
- Experiences with the VA
Among non-users of VA mental health services
- Reasons for not using VA services
Among all veterans who have a mental health need
- Ease of use
- Availability of mental health services
- Obstacles to obtaining services
- Attitudes about mental health treatment
Users’ Perspectives
The survey asked VA users of mental health services who have a mental health need about the reasons they use VA mental health services. Table 6-14 summarizes these reasons. The most frequently endorsed reasons for using the VA were the provision of prescription benefits (87 percent), entitlement to services (85 percent), and lower cost (83 percent). About three-quarters of the users indicated that getting care for a service-connected disability was a reason for using the VA. Other reasons for using the VA among veterans who have a mental health need included the convenience of the VA location (68 percent), liking the VA doctors or already using the VA for years (64 percent), and the VA being
___________________
5 The FY 2016 report reviewed by the committee covers survey data collected through June 2016.
| Reasons Veterans Use VA Mental Health Services | Unweighted n | Weighted N | Weighted % Agree | Standard Error % |
|---|---|---|---|---|
| Total | 849 | 476,654 | – | – |
| VA provides prescription benefits | 732 | 413,337 | 86.7% | 1.4% |
| You are entitled to it | 724 | 404,614 | 84.9% | 1.4% |
| VA costs less than other options for care | 702 | 396,222 | 83.1% | 1.5% |
| Can get care for a service-connected disability | 649 | 356,734 | 74.8% | 1.9% |
| VA location is convenient | 581 | 322,712 | 67.7% | 1.9% |
| You like the doctors at the VA or have been going for years | 548 | 306,095 | 64.2% | 2.0% |
| VA is the only source of mental health care available | 522 | 303,496 | 63.7% | 1.8% |
| Spouse or friends suggested you get care at the VA | 448 | 265,517 | 55.7% | 1.9% |
| VA provides services cannot get elsewhere | 390 | 231,985 | 48.7% | 1.8% |
| VA provides a higher quality of care | 401 | 220,917 | 46.3% | 1.9% |
| Lost or had inadequate private health insurance | 337 | 200,252 | 42.0% | 1.9% |
NOTE: Weighted % agree includes responses of strongly and somewhat agree.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
the only available source of mental health care (64 percent). The last reason is consistent with the fact that 42 percent of the veterans reported having lost insurance coverage or having inadequate levels of coverage as their reason for using the VA. Slightly less than half (49 percent) sought care at the VA because the VA provides services that they could not get elsewhere. The belief that the VA provides higher quality care also motivated 46 percent of veterans. These latter two findings are consistent with a theme found in the qualitative interviews, discussed in later chapters, that many veterans believe that the mental health professionals at the VA are familiar with veteran issues.
Non-Users’ Perspectives
The survey also asked those who have a mental health need but do not use VA mental health services what their reasons were for not using services. Table 6-15 summarizes the responses and shows that the most commonly cited reasons for not using the VA were a lack of knowledge about how to apply for benefits (42 percent) and the belief by the veteran that he or she was not eligible or entitled to services (40 percent). In addition, about one-third of veterans who had a mental health need indicated they do not use the VA because they were not aware that the VA offers mental health services (33 percent) and a similar percentage (30 percent) did not feel they deserved to receive mental health care benefits from the VA. Taken together, these responses suggest that enhancements in the VA’s outreach strategies are needed, even though all service members go through the TAP before separation. TAP includes a 6-hour module on VA benefits. Notably, 30 percent do not trust the VA, 23 percent had a bad prior experience at the VA, and 19 percent indicated they do not feel welcome at the VA.
All Veterans Who Have a Mental Health Need
Access to Care and Ease of Use
The committee’s survey explored how easy it is for veterans to use the VA in terms of location and transportation, access to timely appointments, the availability of providers and services, specific
| Reasons Veterans Do Not Use VA Mental Health Services | Unweighted n | Weighted N | Weighted % Yes | Standard Error % |
|---|---|---|---|---|
| Total | 1,146 | 1,214,303 | – | – |
| Do not know how to apply for VA mental health care benefits | 411 | 506,957 | 41.7% | 1.3% |
| Do not believe entitled or eligible for VA mental health care benefits | 357 | 479,555 | 39.5% | 1.8% |
| Not aware VA offers mental health care benefits | 314 | 401,674 | 33.1% | 1.7% |
| Use other sources of mental health care | 361 | 399,701 | 32.9% | 1.6% |
| Do not need care | 338 | 384,146 | 31.6% | 1.6% |
| Feel do not deserve to receive mental health care benefits from the VA | 282 | 358,479 | 29.5% | 1.4% |
| Do not trust the VA | 360 | 357,804 | 29.5% | 1.9% |
| Some other reason | 327 | 318,751 | 26.2% | 1.5% |
| Had a bad prior experience at VA | 300 | 276,663 | 22.8% | 1.3% |
| Do not feel welcome at the VA | 223 | 225,174 | 18.5% | 1.3% |
| Do not want assistance from the VA | 203 | 207,205 | 17.1% | 1.0% |
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
obstacles to getting care, and attitudes about getting mental health treatment. Table 6-16 shows accessibility (measured as travel distance, travel time, and ease of transport) to the nearest VA facility that offers mental health service among veterans who screen positive for a mental health need and use mental health services. In general, the majority of veterans who had a mental health need and used the VA did not consider the location of and transportation to the VA for mental health services to be barriers. However, among those screening positive who used mental health services but not the VA (non-VA users), the location may be a barrier. Seventy-three percent of VA users who had a mental health need reported that they live within 30 miles of a VA facility that offers mental health services; among non-VA users who had a mental health need, only 45 percent reported living within 30 miles from a VA facility with mental health services. Not surprisingly, among those veterans who had a mental health need, a much larger percentage of non-VA users than VA users (28 versus 3 percent) were unsure of the location of the nearest facility, but after restricting attention to those who specified a distance, 75 percent of VA users with a mental health need reported that they live within 30 miles of a VA facility that offers mental health services; among non-VA users with a mental health need, only 64 percent reported living within 30 miles of a VA facility with mental health services.
Among VA users with a mental health need, Table 6-16 shows, 76 percent indicated that they live 45 minutes or less from a VA facility; only 44 percent among non-VA users with a mental health need reported living 45 minutes or less from a VA facility. This is a statistically significant difference, and this may be one of the reasons some veterans do not use mental health services at the VA even though they have a need. Note that non-VA users with a mental health need were often unsure about the travel time to the nearest VA facility (33 versus 3 percent for VA users with a mental health need), but differences persist after restricting attention to those who specified a time: 78 percent of VA users with a mental health need reported living 45 minutes or less from such a facility, versus 66 percent for non-VA users with a mental health need. Overall, 75 percent of the veterans with a mental health need who used VA
| Geographic Accessibility to VA Facility | All OEF/OIF/OND Veterans | VA Users | Non-VA Users* | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | |
| Distance from VA facility | ||||||||||||
| 0–10 miles | 482 | 357,662 | 21.0% | 1.1% | 274 | 153,011 | 32.1% | 2.1% | 45 | 43,621 | 16.0% | 2.4% |
| 11–20 miles | 464 | 366,666 | 21.6% | 1.0% | 219 | 121,548 | 25.5% | 1.7% | 47 | 48,411 | 17.7% | 2.4% |
| 21–30 miles | 272 | 202,208 | 11.9% | 0.7% | 139 | 74,406 | 15.6% | 1.2% | 33 | 29,889 | 11.0% | 2.3% |
| 31–40 miles | 145 | 112,004 | 6.6% | 0.7% | 70 | 40,650 | 8.5% | 1.2% | 23 | 21,595 | 7.9% | 1.8% |
| 41–50 miles | 123 | 102,664 | 6.0% | 0.6% | 53 | 31,489 | 6.6% | 1.0% | 16 | 18,604 | 6.8% | 1.5% |
| >50 miles | 230 | 208,362 | 12.3% | 0.8% | 72 | 42,684 | 9.0% | 1.3% | 26 | 30,129 | 11.0% | 2.0% |
| Not sure | 276 | 335,965 | 19.8% | 0.9% | 21 | 12,463 | 2.6% | 0.7% | 64 | 77,473 | 28.4% | 2.8% |
| Missing | 11 | 14,136 | 0.8% | 0.2% | 1 | 402 | 0.1% | 0.1% | 2 | 3,078 | 1.1% | 0.8% |
| Time to VA facility | ||||||||||||
| <10 minutes | 174 | 133,386 | 7.8% | 0.7% | 93 | 54,522 | 11.4% | 1.4% | 15 | 11,666 | 4.3% | 1.5% |
| 10–20 minutes | 415 | 303,647 | 17.9% | 1.0% | 233 | 128,657 | 27.0% | 2.0% | 37 | 42,673 | 15.6% | 2.3% |
| 21–30 minutes | 335 | 246,356 | 14.5% | 0.9% | 177 | 93,561 | 19.6% | 1.4% | 34 | 28,832 | 10.6% | 2.3% |
| 31–45 minutes | 297 | 227,472 | 13.4% | 0.8% | 148 | 84,999 | 17.8% | 1.5% | 36 | 35,385 | 13.0% | 2.6% |
| 46–60 minutes | 205 | 163,924 | 9.6% | 0.7% | 91 | 52,441 | 11.0% | 1.3% | 28 | 24,021 | 8.8% | 1.9% |
| >1 hour | 260 | 232,297 | 13.7% | 0.9% | 83 | 47,773 | 10.0% | 1.3% | 34 | 38,255 | 14.0% | 2.6% |
| Not sure | 303 | 378 321 | 22.3% | 1.0% | 19 | 12 172 | 2.6% | 0.7% | 70 | 88 890 | 32.6% | 3.5% |
| Missing | 14 | 14,265 | 0.8% | 0.2% | 5 | 2,530 | 0.5% | 0.3% | 2 | 3,078 | 1.1% | 0.8% |
| Ease of transport to the VA | ||||||||||||
| Very easy/Somewhat easy/Neither easy nor hard | 1,281 | 989,867 | 58.2% | 1.1% | 641 | 357,353 | 75.0% | 1.7% | 134 | 134,654 | 49.4% | 2.9% |
| Very hard/Somewhat hard | 290 | 244,868 | 14.4% | 0.9% | 127 | 78,166 | 16.4% | 1.6% | 45 | 47,073 | 17.3% | 2.1% |
| Not sure | 418 | 450,580 | 26.5% | 1.1% | 76 | 38,516 | 8.1% | 1.0% | 75 | 87,994 | 32.3% | 2.9% |
| Missing | 14 | 14,353 | 0.8% | 0.2% | 5 | 2,618 | 0.5% | 0.3% | 2 | 3,078 | 1.1% | 0.8% |
NOTES: Responses may not sum to 100% due to rounding. SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
*“Non-VA user” denotes veterans who receive mental health services but not at a VA facility.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
mental health services (or 82 percent adjusted for not sure and missing) reported that it is very easy, somewhat easy, or neither easy nor hard to get to the nearest VA facility with mental health services; among non-VA users with a mental health need, only 49 percent (or 74 percent after adjustment) reported the same ease of access. Though transportation may not be an issue for the majority of veterans with a mental health need, a noteworthy minority indicated that they were located a considerable distance from the nearest VA offering mental health care. For 9 percent of VA users with a mental health need (9 percent after adjustment) and 11 percent of non-VA users with a mental health need (16 percent after adjustment), the nearest facility with mental health services was more than 50 miles away, and 10 percent of VA users with a mental health need (10 percent after adjustment) and 14 percent of non-VA users with a mental health need (21 percent after adjustment) indicated that they lived more than 1 hour from such a facility.
While the majority of veterans surveyed live reasonably close to the nearest VA facility offering mental health care, the committee found on its site visits that transportation can be a significant challenge and a barrier for veterans in rural locations. In some locations veterans reported travel times of more than an hour to reach needed services. Among veterans who rely on public transportation in rural locations, seeking services and returning home can take an entire day.
Financial distress experienced by many veterans can result in an inability to pay for gas for the trip, ownership of an unreliable vehicle or lack of a vehicle, or a lack of affordable or reliable public transportation. As one VA clinician in Battle Creek, Michigan, bluntly said, “There’s a natural assumption that all these veterans have drivers licenses, they have money for gas, and they have their own vehicle. They don’t.”
Many sites reported that Disabled American Veterans (DAV) runs vans to assist veterans with getting to the VA for appointments. Although this was praised as a great service, it is still difficult for many veterans to use because it often requires them to spend an entire day traveling to and from an appointment since the vans run one route in and one route out each day. Additionally, DAV requires telephone confirmation the day before, something that is challenging for veterans without consistent phone access or the ability to afford cell phone minutes.
Further complicating the transportation options are the symptoms of PTSD themselves. VA clinicians noted that those who are apprehensive about being in crowded places have a hard time using public transportation even if it is otherwise a viable option. They also noted that many veterans suffering from PTSD are nervous drivers, and many veterans commented that their anger management issues lead to road rage, making it hard to safely drive long distances. One veteran said, “A lot of OIF veterans and OEF veterans aren’t really happy about driving. With all the roadside bombs and stuff, I think it made a lot of paranoid drivers” [Topeka, Kansas]. Many mental health care service recipients also deal with multiple comorbidities, including chronic pain, adding additional barriers to making long drives. As discussed below in the section on factors that may influence future use, the committee’s survey showed that the farther a veteran resides from a VA facility offering mental health services, the odds they use services decreases despite having a mental health care need (see Table 6-38). This suggests that further expanding telemedicine options to rural-dwelling veterans may improve access for those who see distance to the nearest mental health facility as a barrier to their care. Overall, about half of the veterans in the survey said they would be willing to receive Internet-delivered mental health care in the future (see Table 6-35).
Veterans also reported issues with the process of getting mental health care, ease of getting appointments, the availability of staff to answer questions, and the time between requests and actual appointments. Table 6-17 shows ratings for access to mental health care and for the availability of mental health care among veterans who screen positive for a mental health need and who use the VA for mental health
| Ease of Access to VA Mental Health Care | Unweighted n | Weighted N | Weighted % | SE % |
|---|---|---|---|---|
| Process of getting mental health care | ||||
| Very or somewhat burdensome | 457 | 258,287 | 54.2% | 1.8% |
| Not very or at all burdensome | 353 | 192,381 | 40.4% | 1.8% |
| Not sure | 34 | 23,703 | 5.0% | 1.1% |
| Easy to get appointment | ||||
| Never or sometimes | 366 | 203,084 | 42.6% | 2.0% |
| Always or usually | 410 | 233,211 | 48.9% | 2.1% |
| Have not tried | 61 | 35,263 | 7.4% | 1.1% |
| Not sure | 8 | 4,068 | .9% | 0.3% |
| Evening/weekend/holiday care available | ||||
| Never or sometimes | 271 | 154,680 | 35.4%a | 1.8% |
| Always or usually | 129 | 75,317 | 17.2%a | 1.5% |
| Have not tried | 374 | 205,445 | 47.0%a | 1.8% |
| Time between request and appointment | ||||
| Very or somewhat dissatisfied | 260 | 146,684 | 33.6%b | 1.9% |
| Very or somewhat satisfied | 506 | 284,621 | 65.1%b | 1.9% |
| Availability of VA personnel to answer questions by phone | ||||
| Very or somewhat dissatisfied | 214 | 117,793 | 24.7% | 1.6% |
| Very or somewhat satisfied | 387 | 216,132 | 45.3% | 1.8% |
| Does not apply | 229 | 132,513 | 27.8% | 2.0% |
| Availability of VA personnel to answer questions in person | ||||
| Very or somewhat dissatisfied | 139 | 82,076 | 17.2% | 1.5% |
| Very or somewhat satisfied | 642 | 360,390 | 75.6% | 1.5% |
| Does not apply | 46 | 23,063 | 4.8% | 0.8% |
NOTES: Individual item counts may not sum to total counts due to item non-response. SE = standard error of percentage.
aPercentage among those estimated 436,969 veterans who had tried to get an appointment with a VA mental health provider in the past 24 months.
bPercentage among those estimated 431,305 veterans who answered the question.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
services. Despite the convenient location for many, among those who responded, only 40 percent of VA users with a mental health need indicated that obtaining mental health care through the VA was not very or not at all burdensome. Among responding VA users with a mental health need who had tried to obtain an appointment in the last 24 months, only about half (49 percent) indicated it was always or usually easy to get an appointment. Of VA users (N = 435,442) with a mental health need who responded to the question about availability of care during evenings and weekends, only 17 percent of them indicated that they could always or usually get an appointment. Of VA users (N = 431,305) with a mental health need who responded to the question about the time between the request and an appointment, 65 percent of them indicated that they were very or somewhat satisfied with the time between request and appointment for mental health services. Only 45 percent of VA users with a mental health need reported that
they were satisfied with the availability of VA personnel to answer questions by phone. Overall, the table shows, a large proportion of veterans reported difficulty getting convenient and timely appointments for their mental health needs.
Availability of Mental Health Providers and Specific Mental Health Services
The survey also inquired about the availability of a range of VA mental health providers and services. These results are shown in Table 6-18 for VA users who have a mental health need. Just over half of veterans who use VA services (52 percent) were satisfied with the availability of psychiatrists. This is significantly larger than the proportion who reported being very or somewhat dissatisfied (24 percent) or who had no opinion (23 percent). Similarly, a significantly larger proportion (46 percent) of respondents were satisfied with the availability of psychologists and of nurse practitioners when compared with those who were dissatisfied or had no opinion. The large proportion of veterans with mental health needs who use the VA but had no opinion about availability of social workers, addiction counselors, or chaplain/pastoral care suggests that these veterans did not seek those services or that these services were not available in the veterans’ specific VA facilities.
Table 6-18 also shows that 40 percent of veterans with a mental health need were satisfied with the availability of specialized mental health services. However, the proportion who was dissatisfied was only 28 percent, meaning that among respondents with an opinion, the proportion of veterans who are satisfied with their access to specialized mental health care is 1.4 times higher than those who are not satisfied. In every type of services rated, among veterans who responded, a significant percentage were satisfied or very satisfied with availability of the service. In the case of medication management, respondents were 2.4 times more likely to be satisfied than not satisfied. Table 6-19 shows the responses of VA users with a mental health need when asked to rate five different aspects of the VA’s delivery of mental health services. Seventy to 84 percent of veterans in this category responded to the questions. Among those who responded, the overwhelming majority had a somewhat or very positive opinion about those particular aspects of mental health care. The only exception was the availability of needed services, about which only 43 percent of respondents had a somewhat or very positive opinion. Over 60 percent of respondents had a somewhat or very positive opinion of the way the VA maintained the confidentiality of patient records and of the VA staff’s courtesy and respect toward patients. This finding somewhat contradicts some of the comments that were offered during the site visits regarding staff attitudes toward patients (see Chapter 10). On the whole, however, veterans with a need who use the VA mental health services appear to be satisfied with these aspects of service delivery.
Predictors of Access to Care
Because access to care is such a crucial component of the quality of care and because studies have identified significant difficulties for veterans in this area, the committee used the survey data to conduct logistic regression analyses to identify predictors of difficulties accessing care, including the availability of mental health providers and services. The committee was especially interested in race/ethnicity and gender as potential predictors, but it included other veteran characteristics as potential predictors as well. These included age, marital status, employment status, the branch of service, deployment time, and combat exposure. Refer to Table 6-10 above for a list of the core independent variables used in the regression models, including the reference categories for those variables. In addition, the regressions in this section (and in Factors That May Influence Future Use below) use several additional variables, described in Table 6-20, that assess potential attitudes and beliefs that may pose barriers to treatment
| Availability of Providers and Services | Very or Somewhat Satisfied | Very or Somewhat Dissatisfied | No Opinion | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Satisfaction with Mental Health Provider Availability for: | Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % |
| Psychiatrist | 444 | 246,018 | 51.6% | 1.9% | 201 | 113,166 | 23.7% | 1.8% | 193 | 111,812 | 23.5% | 1.8% |
| Psychologist | 396 | 219,136 | 46.0% | 1.8% | 175 | 99,452 | 20.9% | 1.7% | 267 | 152,594 | 32.0% | 1.8% |
| Social workers | 305 | 169,104 | 35.5% | 1.9% | 134 | 73,217 | 15.4% | 1.4% | 385 | 222,176 | 46.6% | 1.9% |
| Nurse practitioners | 419 | 230,232 | 48.3% | 1.8% | 116 | 68,893 | 14.5% | 1.4% | 296 | 168,062 | 35.3% | 2.0% |
| Addictions counselors | 105 | 61,420 | 12.9% | 1.1% | 45 | 29,359 | 6.2% | 1.0% | 672 | 373,365 | 78.3% | 1.5% |
| Chaplain services/Pastoral care | 101 | 59,039 | 12.4% | 1.2% | 31 | 18,073 | 3.8% | 0.8% | 685 | 381,784 | 80.1% | 1.5% |
| Satisfaction with health care services availability for: | ||||||||||||
| Primary care services | 496 | 284,033 | 59.6% | 1.8% | 285 | 153,046 | 32.1% | 1.8% | 2 | 475 | 0.1% | 0.1% |
| General mental health services | 526 | 296,672 | 62.2% | 1.9% | 240 | 136,297 | 28.6% | 1.8% | 1 | 379 | 0.1% | 0.1% |
| Specialized mental health care services | 351 | 189,121 | 39.7% | 2.0% | 224 | 131,262 | 27.5% | 1.6% | 5 | 2,935 | 0.6% | 0.3% |
| Satisfaction with mental health services availability for: | ||||||||||||
| Medication management | 482 | 267,108 | 56.0% | 2.1% | 195 | 112,157 | 23.5% | 1.7% | 1 | 538 | 0.1% | 0.1% |
| Psychotherapy (talk therapy) | 344 | 187,708 | 39.4% | 1.5% | 168 | 98,300 | 20.6% | 1.6% | 8 | 4,163 | 0.9% | 0.4% |
| Group therapy | 173 | 100,104 | 21.0% | 1.6% | 102 | 59,725 | 12.5% | 1.3% | 14 | 6,318 | 1.3% | 0.4% |
| Emergency services (e.g., crisis hotline and other 24-hour services) | 204 | 116,747 | 24.5% | 1.7% | 108 | 63,758 | 13.4% | 1.4% | 11 | 5,468 | 1.1% | 0.4% |
| Case management | 270 | 149,124 | 31.3% | 1.6% | 146 | 88,589 | 18.6% | 1.6% | 13 | 5,970 | 1.3% | 0.4% |
NOTES: Responses may not sum to 100% due to rounding or due to the omission of the percentages of missing or refused in the table. SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| Aspects of VA Mental Health Care | Very or Somewhat Negative | Somewhat or Very Positive | Refused or Missing | Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | Wgt N | Unwgt n | |
| Availability of needed services | 279 | 161,822 | 33.9% | 1.7% | 363 | 203,751 | 42.7% | 1.6% | 207 | 111,081 | 23.3% | 1.5% | 476,654 | 849 |
| Privacy and confidentiality of medical records | 88 | 49,209 | 10.3% | 1.1% | 549 | 306,577 | 64.3% | 1.9% | 211 | 120,597 | 25.3% | 1.9% | 476,654 | 849 |
| Ease of using VA mental health care | 239 | 140,221 | 29.4% | 1.9% | 428 | 236,069 | 49.5% | 2.0% | 181 | 100,093 | 21.0% | 1.8% | 476,654 | 849 |
| Mental health care staff’s skill and expertise | 160 | 92,679 | 19.4% | 1.5% | 468 | 261,843 | 54.9% | 1.9% | 221 | 122,132 | 25.6% | 2.3% | 476,654 | 849 |
| Staff’s courtesy and respect toward patients | 140 | 78,043 | 16.4% | 1.5% | 569 | 319,881 | 67.1% | 2.0% | 140 | 78,731 | 16.5% | 1.9% | 476,654 | 849 |
NOTE: SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
TABLE 6-20 Additional Independent Variables Included in the Regression Models
| Variable | Description | Unavailable n |
|---|---|---|
| Attitudes Toward Seeking Professional Psychological Help Scale (ATSPPH) | Sum of 10 items such as “If I believed I was having a mental breakdown, my first inclination would be to get professional attention” and “The idea of talking about problems with a psychologist strikes me as a poor way to get rid of emotional conflicts.” | 2,077 |
| Stigma | Sum of nine items, such as “It could harm my career” and “My coworkers would have less confidence in me if they found out.” | 2,210 |
| Barriers | Sum of two items: “It would be difficult to get childcare or time off of work” and “Mental health care would cost too much money.” | 2,117 |
| Encouraged to get help | No one (reference), Relative or friend encouraged respondent to get help | 2,077 |
| Distance to VA facility | 0–10 miles (reference), 11–20 miles, 21–30 miles, 31–40 miles, 41–50 miles, more than 50 miles | 2,314 |
| Time to VA facility | Less than 10 minutes (reference), 10–20 minutes, 21–30 minutes, 31–45 minutes, 46–60 minutes, more than 1 hour | 2,349 |
NOTE: Unavailable n includes responses of don’t know, refused, missing, and those who were never asked the question.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
seeking. The variables Distance to VA and Time to VA are not used simultaneously in any models in order to avoid collinearity issues. Only the independent variables that were statistically significant at the bivariate, or the full-model stage, were included in the final model.
Four responses to accessing mental health care survey items were selected as dependent variables for logistic regression analysis: (1) The process for getting mental health care through the VA is very or somewhat burdensome; (2) In the past 24 months it was never easy to get appointments with VA mental health providers; (3) In the past 24 months I was never able to get mental health care from a VA facility during evenings, weekends or holidays; and (4) During the past 24 months I was very or somewhat dissatisfied with the time between requesting a VA appointment for mental health care and the actual appointment date. In addition, to examine predictors of veterans’ satisfaction with availability of services and providers, three composite variables were created using linear regression as these composites were continuous variables. The first composite included satisfaction with the availability of primary care, general mental health services, and specialized mental health services. The second included satisfaction with the availability of psychiatrists, psychologists, social workers, nurse practitioners, addiction counselors, and chaplains or pastoral counselors. The third included satisfaction with the availability of medication management, psychotherapy, group therapy, emergency services, and case management.
Results showing odds ratios and the corresponding lower and upper bounds of the confidence intervals of statistically significant predictors are presented in Tables 6-21 through 6-24. Gender did not significantly predict any of the four access variables, suggesting that these aspects of access to care did not differ for men and women. Statistically significant effects for race indicated that veterans who are Hispanic and American Indians or Alaska Natives were more likely to report that they were dissatisfied with the period of time between their request for an appointment at the VA and the appointment date (see Table 6-24). It should be noted, however, that American Indian or Alaskan Native race may be confounded with living in a rural area, which may be associated with dissatisfaction with access to care. Other variables significantly associated with dissatisfaction with time to appointment were never having been married or being divorced, having an associate’s or bachelor’s degree, being an officer, having to travel more than an hour to a VA facility, and perceived need. Generally, variables that predicted only one measure of satisfaction with access to care should be used only if they are replicated in other
| Variable | Variable Value | Odds Ratio | Lower CL | Upper CL | Standard Error |
|---|---|---|---|---|---|
| Age | 50+ years old | 0.379** | 0.213 | 0.675 | 0.292 |
| Insured | Insured | 2.094** | 1.327 | 3.305 | 0.231 |
| PTSD score | Continuous | 1.168* | 1.016 | 1.342 | 0.071 |
| ATSPPH | Continuous | 0.952* | 0.915 | 0.990 | 0.020 |
| Barriers score | Continuous | 1.608** | 1.192 | 2.168 | 0.152 |
| Encouraged to get help | Continuous | 0.543* | 0.320 | 0.921 | 0.268 |
| Disability rating | Disability less than 50 percent | 0.479* | 0.262 | 0.875 | 0.305 |
| Disability rating | Disability 50 percent or higher | 0.418** | 0.276 | 0.633 | 0.211 |
NOTES: *p<.05; **p<.01; 95 percent confidence limits (CL) for the odds ratios.
2,007 unweighted cases initially available, 621 unweighted cases excluded due to missing responses.
Model includes 1,386 unweighted cases representing weighted N of 1,062,004.
Reference categories for the variables are shown in Tables 6-10 and 6-20.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
studies, whereas variables that predicted multiple measures are likely to be more reliable and consistent indicators of veteran-perceived satisfaction with access to care. Not surprisingly, the most consistent predictor of access to care was reported barriers to care. Veterans who reported more barriers to care were more likely to report difficulties and dissatisfaction with access to care (see Tables 6-21 and 6-24). Depression scores significantly predicted three of the four access variables (see Tables 6-22, 6-23, and 6-24) and PTSD predicted one (see Table 6-21). Veterans with higher depression or PTSD levels were more likely to report access difficulties. Veterans with a high score on the DRRI combat scale report that it is never easy to get appointments with a VA mental health provider (see Table 6-22). Veterans with insurance are more likely to report that the process of obtaining care through the VA is burdensome (see Table 6-21). Other variables that significantly predicted at least one measure of access included age, score on the Attitudes Toward Seeking Professional Psychological Help (ATSPPH), having been encouraged to get help, disability rating, and deployment time.
| Variable | Variable Value | Odds Ratio | Lower CL | Upper CL | Standard Error |
|---|---|---|---|---|---|
| Deployment time | More than 48 months | 0.199* | 0.051 | 0.771 | 0.687 |
| DRRI combat | High | 2.716* | 1.178 | 6.259 | 0.423 |
| Depression score | Continuous | 1.315** | 1.170 | 1.476 | 0.059 |
| Encouraged to get help | Continuous | 0.482* | 0.265 | 0.876 | 0.303 |
| Disability rating | Disability 50 percent or higher | 0.347** | 0.174 | 0.695 | 0.352 |
NOTES: *p<.05; **p<.01; 95 percent confidence limits (CL) for the odds ratios.
Respondents who had not tried to get an appointment with a VA mental health provider in the past 24 months were excluded.
1,060 unweighted cases initially available, 288 unweighted cases excluded due to missing responses.
Model includes 772 unweighted cases representing weighted N of 485,150.
Reference categories for the variables are shown in Tables 6-10 and 6-20.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| Variable | Variable Value | Odds Ratio | Lower CL | Upper CL | Standard Error |
|---|---|---|---|---|---|
| Deployment time | 7–12 months | 0.427* | 0.194 | 0.938 | 0.400 |
| Deployment time | 25–36 months | 0.381* | 0.160 | 0.908 | 0.440 |
| Depression score | Continuous | 1.192** | 1.055 | 1.348 | 0.062 |
| ATSPPH | Continuous | 0.949* | 0.903 | 0.997 | 0.025 |
NOTES: *p<.05; **p<.01; 95 percent confidence limits (CL) for the odds ratios.
Respondents who had not tried to get a mental health care appointment at the VA during evenings, weekends, or holidays in the past 24 months were excluded.
542 unweighted cases initially available, 162 unweighted cases excluded due to missing responses.
Model includes 380 unweighted cases representing weighted N of 250,393.
Reference categories for the variables are shown in Tables 6-10 and 6-20.
ATSPPH = Attitudes Toward Seeking Professional Psychological Help scale.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
The results of the linear regression analyses of veterans’ satisfaction with the availability of VA mental health providers and services are summarized in Tables 6-25 through 6-27. Neither race nor gender significantly predicted satisfaction with the availability of mental health services or providers. However, depression, PTSD, and barriers to care were all consistently associated with lower satisfaction with the availability of VA mental health services. That is, veterans with higher levels of depression or PTSD and those who reported more barriers to care were less satisfied with availability of VA mental
| Variable | Variable Value | Odds Ratio | Lower CL | Upper CL | Standard Error |
|---|---|---|---|---|---|
| Age | 50+ years old | 0.293* | 0.106 | 0.810 | 0.516 |
| Marital status | Never married | 1.907* | 1.035 | 3.514 | 0.310 |
| Marital status | No longer married | 1.694* | 1.031 | 2.782 | 0.252 |
| Education | Associate’s or Bachelor’s degree | 1.948* | 1.032 | 3.677 | 0.322 |
| Race | American Indian/Alaska Native | 5.093* | 1.427 | 18.182 | 0.645 |
| Race | Hispanic | 1.766* | 1.034 | 3.016 | 0.271 |
| Rank | Officers | 2.605* | 1.067 | 6.361 | 0.453 |
| Depression score | Continuous | 1.120* | 1.017 | 1.235 | 0.049 |
| Barriers score | Continuous | 1.756** | 1.272 | 2.425 | 0.164 |
| Time to VA facility | More than 1 hour | 2.268* | 1.139 | 4.516 | 0.349 |
| Perceived need | Yes | 1.855** | 1.246 | 2.761 | 0.202 |
NOTES: *p<.05; **p<.01; 95 percent confidence limits (CL) for the odds ratios.
Respondents who had not tried to get an appointment with a VA mental health provider in the past 24 months were excluded.
1,060 unweighted cases initially available, 307 unweighted cases excluded due to missing responses.
Model includes 753 unweighted cases representing weighted N of 472,271.
Reference categories for the variables are shown in Tables 6-10 and 6-20.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| Variable | Variable Value | Estimate | Standard Error | t-score | p-value |
|---|---|---|---|---|---|
| PTSD score | Continuous | −0.088** | 0.026 | −3.374 | 0.001 |
| Drug dependence score | Continuous | −0.055* | 0.026 | −2.114 | 0.036 |
| Depression score | Continuous | −0.082** | 0.027 | −3.039 | 0.003 |
| ATSPPH | Continuous | 0.020** | 0.007 | 2.718 | 0.007 |
| Barriers score | Continuous | −0.212** | 0.046 | −4.608 | 0.000 |
| Disability rating | Disability 50 percent or higher | 0.288* | 0.131 | 2.197 | 0.029 |
NOTES: *p<.05; **p<.01. ATSPPH = Attitudes Toward Seeking Professional Psychological Help scale.
Responses of no opinion were excluded.
1,435 unweighted cases initially available, 335 unweighted cases excluded due to missing responses.
Model includes 1,100 unweighted cases representing weighted N of 733,848.
Reference categories for the variables are shown in Tables 6-10 and 6-20.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| Variable | Variable Value | Estimate | Standard Error | t-score | p-value |
|---|---|---|---|---|---|
| Depression score | Continuous | −0.106** | 0.021 | −5.128 | 0.000 |
| ATSPPH | Continuous | 0.031** | 0.008 | 3.944 | 0.000 |
| Barriers score | Continuous | −0.143* | 0.059 | −2.436 | 0.016 |
NOTES: *p<.05; **p<.01. ATSPPH = Attitudes Toward Seeking Professional Psychological Help scale.
Responses of no opinion were excluded.
1,121 unweighted cases initially available, 270 unweighted cases excluded due to missing responses.
Model includes 851 unweighted cases representing weighted N of 533,652.
Reference categories for the variables are shown in Tables 6-10 and 6-20.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| Variable | Variable Value | Estimate | Standard Error | t-score | p-value |
|---|---|---|---|---|---|
| Insured | Insured | −0.262** | 0.091 | −2.859 | 0.005 |
| PTSD score | Continuous | −0.081* | 0.038 | −2.105 | 0.037 |
| Depression score | Continuous | −0.092** | 0.025 | −3.634 | 0.000 |
| ATSPPH | Continuous | 0.038** | 0.008 | 4.853 | 0.000 |
| Barriers score | Continuous | −0.229** | 0.057 | −4.019 | 0.000 |
NOTES: *p<.05; **p<.01. ATSPPH = Attitudes Toward Seeking Professional Psychological Help scale.
Responses of no opinion were excluded.
1,089 unweighted cases initially available, 256 unweighted cases excluded due to missing responses.
Model includes 833 unweighted cases representing weighted N of 519,440.
Reference categories for the variables are shown in Tables 6-10 and 6-20.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
The results of the linear regression analyses of veterans’ satisfaction with the availability of VA mental health providers and services are summarized in Tables 6-25 through 6-27. Neither race nor gender significantly predicted satisfaction with the availability of mental health services or providers. However, depression, PTSD, and barriers to care were all consistently associated with lower satisfaction with the availability of VA mental health services. That is, veterans with higher levels of depression or PTSD and those who reported more barriers to care were less satisfied with availability of VA mental health services. In contrast, those with more favorable attitudes toward getting help were more satisfied with the availability of mental health services.
BARRIERS: INDIVIDUAL FACTORS
There are many aspects of life that can influence a veteran’s use of the VA and which affect his or her health care–seeking behavior. The committee’s research, both the survey and the site visit interviews, revealed some of these more personal factors—obstacles reported, attitudes toward mental health care, firearm ownership, employment concerns, and other competing demands—which are characteristic of a veteran’s life, and, as the committee’s research shows, can influence treatment-seeking behavior.
The survey explores barriers to care by asking respondents directly about potential obstacles to getting care. Table 6-28 presents the percentage of veterans with a mental health need who agree with statements regarding obstacles to getting mental health care. Most of the items in Table 6-28 relate to stigma; the two exceptions are “Would be difficult to get childcare or time off work” and “Mental health care would cost too much money.” The two obstacles cited by the greatest number of veterans were being denied security clearance (N = 557,000) and mental health care costing too much money (N = 533,000). It should be noted, however, that several of the items included “not applicable” as a response option. For items with a “not applicable” response option, Table 6-28 shows results calculated with and without “not applicable” responses in the total N.
Veterans’ attitudes toward the effectiveness of mental health treatment and seeking professional mental health care may be another barrier to getting help. Table 6-29 shows the attitudes toward receiving psychological treatment among veterans who screen positive for a mental health need. Most who screen positive for a mental health need indicated that they would seek psychological help if they were worried or upset for a long period of time (77 percent). Similarly, 71 percent of veterans who have a mental health need indicated that they would seek professional attention if they believed that they were having a mental breakdown. Additionally, 69 percent strongly or somewhat agreed with the statement that they might want psychological counseling in the future, and 67 percent reported that someone with an emotional problem is not likely to solve it alone, but would with professional help. Though some discomfort with professional help is evident in the almost evenly split response to admiring someone who copes without professional help, overall the veterans indicated an openness toward seeking professional help if they thought that they needed it. At the same time, significant percentages of veterans indicated that they somewhat or strongly disagreed with statements saying they would seek help or that they believed that they could benefit from such help. This skepticism about the personal utility and benefit of mental health treatment could represent a significant barrier to the receipt of services for a significant minority of veterans.
Employment Concerns
A commonly reported concern among veterans is the effects that seeking mental health care may have on their employment. Veterans participating in the survey and site visit interviews expressed
| Perceived Obstacles | Total n | Unweighted n | Weighted N | Weighted % Yes | Standard Error % |
|---|---|---|---|---|---|
| Total | 2,007 | 2,007 | 1,705,168 | – | – |
| Could be denied security clearance in the future | 2,007 | 687 | 556,869 | 32.7% | 1.2% |
| Mental health care would cost too much money | 2,007 | 616 | 533,015 | 31.3% | 1.0% |
| Would be seen weak by others | 2,007 | 585 | 472,258 | 27.7% | 0.9% |
| Would think less of myself if I could not handle it on my own | 2,007 | 587 | 468,625 | 27.5% | 1.1% |
| Would be too embarrassing | 2,007 | 567 | 466,744 | 27.4% | 1.1% |
| Could harm my career | 2,007 | 473 | 397,254 | 23.3% | 1.2% |
| [excluding not applicable] | [1,295] | [36.7%] | [1.6%] | ||
| Co-worker would have less confidence in me | 2,007 | 461 | 390,954 | 22.9% | 1.4% |
| [excluding not applicable] | [1,313] | [35.8%] | [1.6%] | ||
| Supervisor may respect me less or treat me differently | 2,007 | 457 | 378,530 | 22.2% | 1.2% |
| [excluding not applicable] | [1,313] | [34.8%] | [1.6%] | ||
| Personal firearms could be taken away | 2,007 | 425 | 352,810 | 20.7% | 1.4% |
| [excluding not applicable] | [1,215] | [34.5%] | [2.0%] | ||
| Would be too difficult to get childcare or time off work | 2,007 | 361 | 303,434 | 17.8% | 1.3% |
| [excluding not applicable] | [984] | [36.9%] | [2.0%] | ||
| Friends and family would respect me less | 2,007 | 345 | 280,688 | 16.5% | 1.1% |
| Could lose medical or disability benefits | 2,007 | 143 | 120,618 | 7.1% | 0.8% |
| [excluding not applicable] | [1,260] | [11.8%] | [1.3%] | ||
| Could lose contact with or custody of my children | 2,007 | 120 | 102,760 | 6.0% | 0.6% |
| [excluding not applicable] | [829] | [15.0%] | [1.4%] |
NOTES: Percentages do not sum to 100% percent because respondents could mark all that apply. The items for which “not applicable” was a response option, analyses were completed both with and without “not applicable” responses in the total N.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
concerns that having a documented mental health issue would either cause them to lose their current job, or prevent them from obtaining employment in the future. As shown in Table 6-28 above, among those who indicated the item was applicable to them, 37 percent of the veterans in the committee’s survey who had mental health needs reported that seeking mental health services could harm their careers, 36 percent indicated that seeking care would lead to co-workers having less confidence in them if they found out, and 35 percent indicated that it would result in supervisors losing respect or treating them differently.
One-third (33 percent) of the survey respondents who had a mental health need cited fear of being denied a security clearance in the future as an obstacle to seeking care. That finding is consistent with what veterans said in the site visit interviews; in particular, they stated that much of their concern was related to getting jobs in law enforcement, which would require possession of a firearm, or other jobs
| Statement About Mental Health Care | Agree | Disagree | ||||||
|---|---|---|---|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | |
| Total | 2,007 | 1,705,168 | – | – | 2,007 | 1,705,168 | – | – |
| I would want to get psychological help if I were worried or upset for a long period of time. | 1,570 | 1,307,513 | 76.7% | 1.7% | 335 | 310,960 | 18.2% | 1.6% |
| If I believed I was having a mental breakdown, my first inclination would be to get professional attention. | 1,448 | 1,212,405 | 71.1% | 1.3% | 471 | 419,434 | 24.6% | 1.2% |
| I might want to have psychological counseling in the future. | 1,434 | 1,183,242 | 69.4% | 1.6% | 467 | 430,121 | 25.2% | 1.5% |
| A person with an emotional problem is not likely to solve it alone; he or she is likely to solve it with professional help. | 1,366 | 1,139,951 | 66.9% | 1.4% | 532 | 474,621 | 27.8% | 1.3% |
| If I were experiencing a serious emotional crisis at this point in my life, I would be confident that I could find relief in psychotherapy. | 1,304 | 1,091,558 | 64.0% | 1.4% | 591 | 517,596 | 30.4% | 1.4% |
| There is something admirable in the attitude of a person who is willing to cope with his or her conflicts and fears without resorting to professional help. | 962 | 824,517 | 48.4% | 1.7% | 930 | 785,679 | 46.1% | 1.4% |
| Personal and emotional troubles, like many things, tend to work out by themselves. | 705 | 610,928 | 35.8% | 1.6% | 1,203 | 1,009,860 | 59.2% | 1.5% |
| Considering the time and expense involved in psychotherapy, it would have doubtful value for a person like me. | 681 | 595,704 | 34.9% | 1.5% | 1,201 | 1,008,242 | 59.1% | 1.4% |
| A person should work out his or her own problems; getting psychological counseling would be a last resort. | 655 | 568,940 | 33.4% | 1.3% | 1,249 | 1,050,610 | 61.6% | 1.4% |
| The idea of talking about problems with a psychologist strikes me as a poor way to get rid of emotional conflicts. | 593 | 496,963 | 29.1% | 1.2% | 1,319 | 1,127,213 | 66.1% | 1.1% |
NOTES: Weighted % agree includes responses of strongly and somewhat agree. Weighted % disagree includes responses of Strongly and Somewhat Disagree.
SE = standard error of percentage; Unwgt = unweighted; Wgt = Weighted.
Rows may not sum to 100% due to the omission of the percentages of missing or refused in the table.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
that would require obtaining a security clearance. In addition, individuals still in the Reserves or the National Guard expressed concern that a mental health diagnosis could prematurely end their military careers. (For more details about mental health treatment and access to VA health care among National Guard and Reserve forces serving in Iraq and Afghanistan see IOM, 2013, 2014.)
Similar to the gun ownership issue discussed below, it is difficult to tease out reality from the rumors that circulate in the veteran community. For example, during the committee’s site visits, one veteran said that a friend of his was fired from his job as a police officer when the police department found out he had sought care from a VA therapist. And a VA clinician in Washington, DC, said, “I was talking to a veteran this morning who was telling me that their job is beginning to do an investigation around people who have mental health services because of the nature of the job.” What is certain is that the concern is keeping some veterans from seeking VA services. As one veteran in East Orange, New Jersey, noted, “I certainly did not want to talk to a mental health professional because if it’s in the government’s mental health log, someway, somehow, somebody is going to get ahold of that.” This issue was the reason some veterans were willing to seek services from Vet Centers and not the VA, since their records are separate and perceived by veterans to be more confidential.
Employment concerns were more salient in certain parts of the country than in others. Trepidation about the loss of security clearances was more relevant in areas of the country with large numbers of government and defense-industry jobs, such as the Washington, DC, and Hampton Roads, Virginia, areas. Veterans spoke about law enforcement implications in many parts of the country, but particularly in southern Texas where Customs and Border Protection is a large employer, especially of veterans.
Competing Demands
Many veterans in the OEF/OIF/OND cohort are working hard to balance jobs, school, and young families. Life’s demands leave little time to either acknowledge a mental health issue or, if it is identified, participate in the necessary treatment to address the problem. Data from the committee survey underscore this point: 37 percent of the veterans with mental health needs who indicated the item was applicable to them reported that difficulty getting childcare or time off from work is an obstacle to seeking services (see Table 6-28). Among all veterans with mental health needs, including those who indicated the issue was not applicable to them, 18 percent indicated that finding childcare or getting time off of work was an obstacle to their care.
The committee notes similar concerns from its site visits. Even those who do “worry about their mental health” simply can’t find the time to fit in a treatment regimen, as one VA clinician in Biloxi, Mississippi, commented: “They’re busy trying to go to school, trying to be married, trying to raise children, so they put themselves on the backburner because they’re trying to work and make a living.” During the site visits, one veteran in Pennsylvania explained, “I can’t take time off work. Nobody pays for time off work.” Many of the evidence-based treatments require multiple weeks of regular treatment, and veterans said that taking time off from work for 12 weeks in a row is not possible for them. Additionally, many veterans work variable shifts, making it nearly impossible to schedule the appointments for an entire treatment regimen.” One VA clinician in Palo Alto, California, said, “[I]f you can’t feed your family, you can’t really worry about your mental health.”
Those who are in school did not report faring any better. Many commented that they cannot afford to miss their classes. A veteran in Pennsylvania who was interviewed on his campus commented, “[A] class here costs me $8,000. If I miss 4 days, I’m out of the course. I have to wait 6 weeks to come back through the course again.” VA staff noted that the GI Bill is a huge financial asset for OEF/OIF/OND veterans, leading a large number of this cohort of veterans to attend college. Yet veterans used the word
“impossible” to explain the ability to seek mental health treatment and maintain their busy schedules: “It’s impossible to have a job or go to school, and go to these appointments.” [Washington, DC]
Taking care of children is a responsibility that prevents many veterans from seeking care. A related issue among those with mental health needs is that seeking treatment may lead to their losing contact with or custody of their children (15 percent among veterans with mental health needs who indicated this item was applicable to them) (see Table 6-28). Since most VA facilities lack childcare, veterans with children are limited in their treatment options. On the site visit interviews, VA clinicians said that this often disproportionately affects female veterans, some of whom lack the ability to come in for treatment. As a VA clinician in Biloxi, Mississippi, noted, “I’ve had some female veterans who wouldn’t enter treatment because they couldn’t get anyone to watch their child.” Many VA clinicians reported allowing children into appointments if there was no other option, but they noted that what they can achieve in an appointment with a child is limited. Another clinician from Biloxi explained,
I’ve tried to see some veterans with their 2-year-old in the stroller in the office, and it makes it much more challenging. Or if the child’s a little bit older, I’m spelling words because we don’t want to say inappropriate things in front of children.
VA staff interviewees in Seattle reported that they had on-site childcare for veterans to use during their appointments. They reported that they were one of only three VAMCs in the country to have this asset and reported that it was “fabulous.” Many Vet Centers also reported having turned a room into a child-friendly space, with things like coloring books, video games, and TVs. They allow patients to leave their children in these rooms while they have their appointment.
Firearms and Mental Health
Results from the committee’s survey showed that, among those veterans who have a mental health need who indicated the obstacle was applicable to them, 35 percent saw the potential of having their personal firearms taken away as an obstacle to using VA mental health services (see Table 6-28). Among all veterans with mental health needs (including those who indicated the item was not applicable), 21 percent saw this as an obstacle to use VA mental health services. Similarly, interviewees in many site visit locations expressed concern that seeking care and receiving a mental health diagnosis would result in the veteran not being able to own or purchase firearms. This section presents what we heard from veterans. It begins with background information about federal and state firearm laws.
Federal and State Firearm Laws
The Gun Control Act of 19686 prohibits certain categories of people from possessing, shipping, transporting, and receiving firearms and ammunition. Prohibited categories include individuals “adjudicated to be mentally defective,” or who have been committed to a mental institution as well as individuals who are unlawful users or addicts of any controlled substance and persons dishonorably discharged from the U.S. Armed Forces. Merely having a mental health diagnosis or receiving treatment for a mental health condition is not enough on its own to qualify a person as “adjudicated as mentally defective” according to federal law (Liu et al., 2013). The Federal Bureau of Investigations (FBI) manages the National Instant Criminal Background Check System (NICS), which is used to determine the eligibility for gun ownership in the United States.
___________________
6 27 C.F.R. § 478.11.
State laws regarding mental health and gun possession and transfer vary greatly, although many states essentially mirror federal regulations or provide further specifications related to the purchase, possession, transfer, revocation, or restoration of firearms (Simpson, 2007). In addition to federal and state firearm laws, there are gun restrictions under Public Law 110-180 that apply to veterans who receive monetary benefits from the VA and are assigned a fiduciary to manage their finances because they are not able to manage their own affairs (as determined by the VA or a court). These veterans are deemed mentally defective by the VA and reported to NICS and, under federal law, are not permitted to purchase, possess, transfer, or ship a firearm or ammunition (McNiel et al., 2007). As of December 31, 2015, there were 263,492 files on mentally defective veterans referred to the FBI by the VA (Krouse, 2017). Veterans may apply for relief from this designation to possibly restore their right to possess or purchase firearms.
If a veteran is ordered by a state court to be involuntarily committed because he or she poses a danger to himself or herself or to others, the state in which the court resides—not the VA—would submit the veteran’s disqualifying record to the FBI (in accordance with the state law) to be added to NICS. The VA itself has rarely (if ever) submitted a veteran’s record for inclusion in NICS for a mental health or medical diagnosis only (Krouse, 2015).
Gun Laws and Veteran Treatment Seeking
As explained above, under federal and state law a mental health diagnosis absent an involuntary hospitalization or a judicial order does not result in loss of gun ownership rights. Of course, a veteran may not know if treatment seeking might lead to hospitalization or a judicial order; however, in the survey and on the site visits, the committee found that veterans may not have an accurate understanding of how seeking mental health care may affect gun purchase and ownership. The committee’s research suggests that a lack of accurate information can have a negative effect on treatment-seeking behavior:
[My friend] went in to talk to somebody about his [PTSD]. He got a letter [from the VA]. . . . If he attempted to purchase firearms after being told he had to surrender them, it constituted some kind of felony and he would be detained. Now he’s like, “Why would I have any of my friends go and tell them that they have any kind of PTSD issues when I was just told I’m going to get arrested for keeping my firearms?” . . . . It’s why, when vets get out, a lot of them don’t want to go and talk to the VA. . . . [Altoona, Pennsylvania]
Additionally, many veterans reported that they believed that new laws were going into effect that would limit their ability to own firearms, such as this one reported by a veteran, “I was under the assumption that a law had been passed that if you have mental disorders, you can’t get a weapon” [Altoona, Pennsylvania].
By what veterans conveyed to the interviewers, it is difficult to understand the exact circumstances regarding veteran’s understanding of gun ownership laws and the supposed loss of weapons. As in the examples above, several first-hand accounts indicated that veterans had made assumptions about the VA’s actions, and many other accounts shared with site visitors were secondhand, from “a friend of a friend.” The issue is further complicated by varying state laws.
What is certain is that a loss of weapons is a serious concern for many veterans (especially in rural regions of the country), and this concern constitutes a barrier to seeking care for mental health concerns.
A staff member in Iowa said: “I’ve also had people decline mental health services because they’re afraid that we’ll infringe on their gun rights.”
The VA indicated in communication to the committee that it does not actively provide information to veterans regarding laws surrounding gun ownership and mental illness. The VA does, however, actively promote safe gun ownership and the safe use of guns as part of its suicide prevention strategy, and it has distributed over 3 million gun locks. Furthermore, it disseminates gun safety education materials to at-risk veterans and their families and offers lethal means counseling training for suicide prevention coordinators and other providers (VA, 2017a,d).
FACTORS THAT MAY INFLUENCE FUTURE USE
The committee’s survey of OEF/OIF/OND veterans examined the potential future use of VA mental health services based on the veterans’ responses to hypothetical questions regarding their expected use and their actual current or recent use patterns. Hypothetical questions about future use can reveal attitudes about the VA along various dimensions and are likely to elicit responses that are correlated with actual use. They can also reveal potential differences among various subgroups of veterans that may facilitate our understanding of these various influences. However, the estimates of hypothetical use alone are unlikely to be good predictors of future use. Instead, the current patterns and trends in use behavior are likely to be the best predictors of actual future use. The committee explored both types of measures of future use.
Hypothetical Future Use of the Department of Veterans Affairs Services
The committee first asked all veterans how likely they are to use any VA service in the future. Seventy-one percent of veterans indicated that they were somewhat likely, likely, or very likely to use a VA service in the future. The survey then asked if they had a mental health need in the future, how likely they would be to use the VA for mental health services. Thus, this question is conditional on having a potential need and an unspecified time frame in the future. Table 6-30 shows that, under these assumptions, nearly two-thirds (an estimated 2.7 million) of all veterans indicated they were somewhat likely, likely, or very likely to use VA mental health services if they have such a need. This estimate substantially overstates the actual current perceived need and use of these services by veterans, as can be seen by comparing the hypothetical responses with the actual behavior shown by veterans, detailed in Table 6-8. In particular, Table 6-8 shows that among those veterans with an assessed mental health need and who have a perceived need (19 percent of all veterans, an estimated 800,000), slightly more
| Use of VA Mental Health Services | Unweighted n | Weighted N | Weighted % Likely | Standard Error % |
|---|---|---|---|---|
| Need/VA Users (N=473,466) | 748 | 423,600 | 88.9% | 1.1% |
| Need/Non-VA users (N=269,722) | 129 | 139,524 | 51.1% | 3.1% |
| Need/Non-users (N=934,323) | 595 | 580,644 | 61.7% | 1.8% |
| No need, no use (N=2,346,810) | 1,332 | 1,440,543 | 61.2% | 1.2% |
NOTE: Weighted % Likely includes responses of Very Likely, Likely, and Somewhat Likely.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
than half of them use any mental health care (about 438,000)—VA or non-VA—and about 70 percent of those veterans use the VA. Therefore, of those who both have and perceive they have a need for care, only 33 percent (about 260,500) use the VA, substantially below the 64 percent who report they would use the VA in the future if they have a mental health need.
Table 6-30 exhibits future use intentions by the current user group. As scan be seen, nearly all VA users (89 percent) said that they were at least somewhat likely to use VA mental health services if in need, while only 51 percent of non-VA users and 62 percent of non-users reported they are at least somewhat likely to use the VA in the future if they had a mental health need. Among all veterans (regardless of need and user group), 64 percent (SE 0.8 percent) reported they were at least somewhat likely to use VA mental health services if in need.
Veterans who said they were not at all likely to use VA mental health services—even if they were in need at some time in the future—were asked about their reasons. Some important differences by user group can be seen in Table 6-31, which includes all veterans who reported that they were not at all likely to use the VA in the future even if they had a mental health need. More than half (54 percent) of current VA users reported having had a bad experience with the VA, and only slightly fewer (46 to 48 percent) reported having waited too long for an appointment, having used the VA before and not seeing improvement, or that VA doctors or staff did not provide good quality treatment. Among non-VA users, 30 percent reported having had a bad experience with the VA, and 13 percent reported having used the VA before and having not seen improvement. A majority of non-VA users (57 percent), perhaps not surprisingly, are most likely to report a preference for a civilian health provider, an option that is also highly endorsed by those who have a mental health need who do use mental health services (49 percent), and even more so by those with no need and no use (64 percent).
Among veterans who have a mental health need, Table 6-32 presents the factors these veterans offered for being unlikely to use VA mental health services in the future. The most frequently cited reason was that veterans prefer a civilian mental health care provider (61 percent). Other common reasons included waiting too long for an appointment (38 percent) and difficulty reaching facilities (25 percent). Quality of treatment is an issue for 19 percent of veterans.
The survey asked all veterans whether they would like to see certain changes at the VA. Table 6-33 presents the percentages of all veterans by the importance they place on select changes the VA could make. For each proposed change, more than half of veterans indicated that the potential change was very or moderately important. The change they most frequently cited as one they would like the VA to undertake is to make the appointment process easier: 80 percent indicated this change was very or moderately important. This is consistent with the findings discussed earlier regarding barriers. Nearly 78 percent said that they would like better quality services and customer service, and 75 percent would like more available services or facilities. Among the desired changes, the desire for nicer facilities was least frequently endorsed, with 56 percent indicating that this is very or moderately important.
Analyses by user group about whether veterans would like to see certain changes at the VA are presented in Table 6-34. Overall, there are no significant differences by user group in the ratings of the importance of ease of the appointment process, better quality services, and better quality customer service, but there are some modest differences between VA users and non-users on the other three variables: VA users consistently rate greater availability of services or facilities as important, and they rate closer and nicer facilities as less important than non-users. While the importance ratings of non-VA users show the same general trends, the sample size for this group is too small to draw reliable conclusions. The survey also explored how various modes of delivery affected veterans’ likelihood of using VA mental health services. As shown in Table 6-35, 60 percent of all veterans would like to receive the services in
| Reasons Not to Use VA Mental Health Services | Need, VA Users | Need, Non-VA Users | Need, Non-Users | No Need, Non-Users | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | |
| Total | 98 | 51,935 | – | – | 127 | 134,387 | – | – | 287 | 350,723 | – | – | 683 | 904,519 | – | – |
| Used VA before and had a bad experience | 52 | 28,028 | 54.0% | 6.6% | 47 | 39,829 | 29.6% | 4.2% | 81 | 79,274 | 22.6% | 2.8% | 61 | 60,938 | 6.7% | 1.4% |
| VA doctors/staff did not provide good quality treatment | 45 | 25,103 | 48.3% | 6.9% | 44 | 32,712 | 24.3% | 4.2% | 77 | 77,344 | 22.1% | 2.7% | 117 | 122,393 | 13.5% | 1.6% |
| Used VA before and did not improve | 42 | 24,412 | 47.0% | 6.6% | 27 | 17,402 | 12.9% | 3.0% | 54 | 42,764 | 12.2% | 1.9% | 31 | 23,315 | 2.6% | 0.5% |
| You would wait too long for an appointment | 47 | 24,056 | 46.3% | 6.9% | 61 | 55,106 | 41.0% | 5.4% | 127 | 134,586 | 38.4% | 2.7% | 260 | 305,662 | 33.8% | 2.1% |
| Prefer civilian health care provider | 38 | 19,371 | 37.3% | 5.8% | 81 | 76,450 | 56.9% | 7.0% | 142 | 170,101 | 48.5% | 2.9% | 441 | 575,883 | 63.7% | 2.1% |
| Facilities are too far away/too hard to get to | 22 | 12,120 | 23.3% | 5.0% | 34 | 30,193 | 22.5% | 4.2% | 68 | 80,897 | 23.1% | 2.2% | 186 | 220,593 | 24.4% | 1.9% |
| Mental health treatment generally does not work | 14 | 8,855 | 17.1% | 4.4% | 11 | 8,028 | 6.0% | 2.5% | 40 | 43,588 | 12.4% | 1.9% | 46 | 43,561 | 4.8% | 0.7% |
| Facilities are not clean or attractive | 6 | 2,593 | 5.0% | 2.1% | 15 | 9,449 | 7.0% | 2.4% | 31 | 31,346 | 8.9% | 1.5% | 54 | 62,147 | 6.9% | 1.1% |
NOTES: Percentages do not sum to 100% percent because respondents could mark all that apply. “Non-VA user” denotes veterans who receive mental health services but not at a VA facility.
SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| Reasons Not to Use VA Mental Health Services | All OEF/OIF/OND Veterans | |||
|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | |
| Total | 1,140 | 1,398,993 | – | – |
| Prefer civilian health care provider | 722 | 858,983 | 61.4% | 1.4% |
| You would wait too long for an appointment | 509 | 528,528 | 37.8% | 1.5% |
| Facilities are too far away/too hard to get to | 317 | 348,597 | 24.9% | 1.1% |
| VA doctors/staff did not provide good quality treatment | 291 | 260,941 | 18.7% | 1.3% |
| Used VA before and had a bad experience | 253 | 213,288 | 15.2% | 1.2% |
| Used VA before and did not improve | 160 | 109,782 | 7.8% | 0.7% |
| Facilities are not clean or attractive | 110 | 107,181 | 7.7% | 0.8% |
| Mental health treatment generally does not work | 114 | 105,132 | 7.5% | 0.6% |
NOTE: SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
person, although a significant proportion, 45 percent, indicated they would likely use Internet. Similarly, 44 percent indicate they would likely use phone as a means to receive care in the future.
Among all veterans with a mental health need (not shown in the table), 70 percent indicated that they prefer to receive mental health services in person, and 91 percent of VA users with a mental health need prefer services in person, although in both these groups over half said they would definitely or probably use the Internet or phone.
While more veterans indicated they were willing to use in-person services than other modalities, Internet and phone service offerings were endorsed by large groups and will likely become more popular in future especially with younger veterans from the OEF/OIF/OND cohort. In Table 6-36 the survey results confirm this assertion—50 percent of younger veterans (ages 17–29), 46 percent of 30- to 39-year-old veterans, and 50 percent of 40- to 49-year-old veterans reported they were willing to use the Internet
| Changes the VA Could Make | Important | Not Important | ||||||
|---|---|---|---|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | |
| Total | 4,180 | 4,179,998 | 100% | – | 4,180 | 4,179,998 | 100% | – |
| Easier appointment process | 3,395 | 3,331,735 | 79.7% | 0.9% | 622 | 689,116 | 16.5% | 0.9% |
| Better quality services | 3,273 | 3,252,381 | 77.8% | 1.0% | 730 | 755,576 | 18.1% | 0.9% |
| Better quality customer service | 3,222 | 3,200,648 | 76.6% | 0.9% | 787 | 805,185 | 19.3% | 0.8% |
| More available services or facilities | 3,177 | 3,139,848 | 75.1% | 0.9% | 835 | 869,074 | 20.8% | 0.9% |
| Closer facilities | 2,663 | 2,656,245 | 63.5% | 0.6% | 1,352 | 1,353,561 | 32.4% | 0.6% |
| Nicer facilities | 2,294 | 2,331,728 | 55.8% | 1.0% | 1,698 | 1,661,128 | 39.7% | 0.9% |
NOTES: Weighted % important includes responses of very and moderately important. Weighted % not important includes responses of slightly and not at all important. SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
Rows may not sum to 100% due to the omission of the percentages of missing or refused in the table.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| Changes the VA Could Make | Important | Not Important | ||||||
|---|---|---|---|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | |
| All OEF/OIF/OND Veterans (N=4,179,998) | ||||||||
| Easier appointment process | 3,395 | 3,331,735 | 79.7% | 0.9% | 622 | 689,116 | 16.5% | 0.9% |
| Better quality services | 3,273 | 3,252,381 | 77.8% | 1.0% | 730 | 755,576 | 18.1% | 0.9% |
| Better quality customer service | 3,222 | 3,200,648 | 76.6% | 0.9% | 787 | 805,185 | 19.3% | 0.8% |
| More available services or facilities | 3,177 | 3,139,848 | 75.1% | 0.9% | 835 | 869,074 | 20.8% | 0.9% |
| Closer facilities | 2,663 | 2,656,245 | 63.5% | 0.6% | 1,352 | 1,353,561 | 32.4% | 0.6% |
| Nicer facilities | 2,294 | 2,331,728 | 55.8% | 1.0% | 1,698 | 1,661,128 | 39.7% | 0.9% |
| All Veterans with Mental Health Need VA Users (N=476,654) | ||||||||
| Easier appointment process | 701 | 387,386 | 81.3% | 1.5% | 105 | 65,209 | 13.7% | 1.3% |
| More available services or facilities | 681 | 376,505 | 79.0% | 1.6% | 130 | 79,802 | 16.7% | 1.5% |
| Better quality services | 681 | 373,441 | 78.3% | 1.6% | 131 | 82,450 | 17.3% | 1.5% |
| Better quality customer service | 648 | 355,353 | 74.6% | 1.4% | 164 | 101,095 | 21.2% | 1.5% |
| Closer facilities | 527 | 279,738 | 58.7% | 1.9% | 285 | 176,153 | 37.0% | 1.8% |
| Nicer facilities | 432 | 229,542 | 48.2% | 1.9% | 375 | 223,383 | 46.9% | 1.9% |
| Non-VA Users (N=272,799) | ||||||||
| Easier appointment process | 208 | 218,407 | 80.1% | 4.4% | 32 | 38,754 | 14.2% | 3.9% |
| Better quality services | 195 | 209,735 | 76.9% | 5.2% | 43 | 45,710 | 16.8% | 3.9% |
| More available services or facilities | 192 | 206,249 | 75.6% | 4.3% | 47 | 50,249 | 18.4% | 3.2% |
| Better quality customer service | 191 | 200,735 | 73.6% | 4.2% | 47 | 52,356 | 19.2% | 3.2% |
| Closer facilities | 155 | 163,801 | 60.0% | 3.9% | 86 | 95,396 | 35.0% | 3.6% |
| Nicer facilities | 127 | 128,624 | 47.1% | 4.8% | 113 | 128,538 | 47.1% | 4.4% |
| Non-Users (N=941,504) | ||||||||
| Easier appointment process | 726 | 746,952 | 79.3% | 1.6% | 118 | 143,630 | 15.3% | 1.7% |
| Better quality services | 687 | 723,961 | 76.9% | 1.8% | 147 | 160,366 | 17.0% | 1.8% |
| Better quality customer service | 672 | 706,063 | 75.0% | 1.8% | 165 | 179,504 | 19.1% | 1.7% |
| More available services or facilities | 658 | 694,299 | 73.7% | 1.7% | 181 | 190,960 | 20.3% | 1.7% |
| Closer facilities | 567 | 606,545 | 64.4% | 1.9% | 271 | 280,893 | 29.8% | 1.7% |
| Nicer facilities | 464 | 509,800 | 54.1% | 2.2% | 370 | 375,180 | 39.8% | 2.1% |
NOTES: Weighted % important includes responses of very and moderately important. Weighted % not important includes responses of slightly and not at all important. SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| Mode | Yes | No | ||||||
|---|---|---|---|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | |
| All OEF/OIF/OND Veterans (N=4,179,998) | ||||||||
| In person | 2,739 | 2,515,812 | 60.2% | 0.9% | 1,297 | 1,527,735 | 36.5% | 0.9% |
| Internet | 1,944 | 1,875,473 | 44.9% | 0.8% | 2,080 | 2,159,905 | 51.7% | 0.8% |
| Phone | 1,980 | 1,845,485 | 44.2% | 1.1% | 2,045 | 2,188,405 | 52.4% | 1.1% |
| VA Users (N=476,654) | ||||||||
| In person | 744 | 414,556 | 87.0% | 1.3% | 67 | 41,189 | 8.6% | 1.2% |
| Internet | 424 | 238,026 | 49.9% | 2.0% | 380 | 212,738 | 44.6% | 1.9% |
| Phone | 499 | 276,470 | 58.0% | 2.3% | 307 | 175,787 | 36.9% | 2.2% |
| Non-VA Users (N=272,799) | ||||||||
| In person | 143 | 155,772 | 57.1% | 3.4% | 96 | 99,354 | 36.4% | 3.3% |
| Internet | 132 | 143,935 | 52.8% | 3.7% | 107 | 111,191 | 40.8% | 3.4% |
| Phone | 108 | 114,465 | 42.0% | 3.8% | 129 | 138,246 | 50.7% | 4.3% |
| Non-Users (N=941,504) | ||||||||
| In person | 548 | 554,019 | 58.8% | 1.8% | 297 | 339,709 | 36.1% | 1.7% |
| Internet | 404 | 419,563 | 44.6% | 1.5% | 438 | 473,337 | 50.3% | 1.6% |
| Phone | 405 | 423,669 | 45.0% | 2.1% | 439 | 469,498 | 49.9% | 2.2% |
NOTES: Weighted % yes includes responses of probably and definitely yes. Weighted % no includes responses of probably and definitely no. SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
for future services, whereas only 37 percent of veterans 50 years and older reported being willing to use Internet-based mental health services in the future.
Comparison of Use of Mental Health Services Among Veterans with Need
Although the responses to hypothetical use questions suggest a large share of veterans would use VA services if they had a mental health need, intentions and actions do not always align. As such, the committee sought to develop and estimate a model of actual mental health use to understand the factors that influence the decision to seek help for mental health problems. Of particular interest were veterans who were assessed as having mental health need but who were not receiving treatment. Why are veterans with need not in treatment that might address those needs? The previous sections of this chapter have explored some of those reasons. This section describes a multivariable model that was used to identify predictors of service use and type of use by comparing three groups of veterans with mental health need: (1) users of the VA, (2) users of mental health services but not the VA, and (3) non-users.
The committee first considered how best to model mental health service use. Mental health service use includes three possible outcomes that can be investigated: no use, VA use, and non-VA use only. A multinomial logit specification views the choice to use a VA provider, a civilian provider, or no care at all as occurring simultaneously. In other words, veterans who have a mental health problem make their
| Mode | Yes | No | ||||||
|---|---|---|---|---|---|---|---|---|
| Unwgt n | Wgt N | Wgt % | SE % | Unwgt n | Wgt N | Wgt % | SE % | |
| All OEF/OIF/OND Veterans (N=4,179,998) | ||||||||
| In person | 2,739 | 2,515,812 | 60.2% | 0.9% | 1,297 | 1,527,735 | 36.5% | 0.9% |
| Internet | 1,944 | 1,875,473 | 44.9% | 0.8% | 2,080 | 2,159,905 | 51.7% | 0.8% |
| Phone | 1,980 | 1,845,485 | 44.2% | 1.1% | 2,045 | 2,188,405 | 52.4% | 1.1% |
| 17 to 29 years old (N=633,990) | ||||||||
| In person | 388 | 386,589 | 61.0% | 2.2% | 207 | 228,406 | 36.0% | 2.1% |
| Internet | 294 | 318,469 | 50.2% | 1.8% | 300 | 296,323 | 46.7% | 1.7% |
| Phone | 284 | 299,700 | 47.3% | 2.3% | 311 | 315,295 | 49.7% | 2.3% |
| 30 to 39 years old (N=1,444,386) | ||||||||
| In person | 974 | 885,253 | 61.3% | 1.9% | 464 | 502,911 | 34.8% | 1.9% |
| Internet | 724 | 660,966 | 45.8% | 1.8% | 715 | 726,559 | 50.3% | 1.9% |
| Phone | 715 | 646,521 | 44.8% | 2.0% | 723 | 740,384 | 51.3% | 2.0% |
| 40 to 49 years old (N=923,549) | ||||||||
| In person | 642 | 582,026 | 63.0% | 1.7% | 276 | 318,137 | 34.4% | 1.9% |
| Internet | 471 | 459,972 | 49.8% | 1.9% | 442 | 436,069 | 47.2% | 1.9% |
| Phone | 469 | 435,535 | 47.2% | 2.2% | 445 | 461,387 | 50.0% | 2.4% |
| 50 years old and older (N=1,1 | 3,789) | |||||||
| In person | 722 | 635,480 | 57.5% | 1.5% | 331 | 439,603 | 39.8% | 1.5% |
| Internet | 442 | 409,603 | 37.1% | 2.0% | 604 | 662,277 | 59.9% | 2.1% |
| Phone | 503 | 445,408 | 40.3% | 1.8% | 544 | 626,554 | 56.7% | 1.8% |
| Missing (N=73,284) | ||||||||
| In person | 13 | 26,464 | 36.1% | 10.1% | 19 | 38,678 | 52.8% | 10.5% |
| Internet | 13 | 26,464 | 36.1% | 8.9% | 19 | 38,678 | 52.8% | 8.9% |
| Phone | 9 | 18,321 | 25.0% | 5.9% | 22 | 44,785 | 61.1% | 5.5% |
NOTES: Weighted % yes includes responses of probably and definitely yes. Weighted % no includes responses of probably and definitely no. SE = standard error of percentage; Unwgt = unweighted; Wgt = weighted.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
decision about whether to get care and where to get care together, rather than as separate components. An alternative view is that these decisions are sequential rather than simultaneous. In this view, veterans first decide to get care and then choose whether to use a VA or civilian provider. This latter view implies that one should use nested models, with the first model predicting the decision to get any care and the second model predicting, among those who get care, the chosen provider (VA or non-VA). There is no a priori reason for selecting one specification over the other, and both types of model specifications obtain similar results.
The committee preferred nested models because the results are easier to interpret and felt these models more accurately reflect the nature of the veteran’s choice. The results from the multinomial model are more difficult to interpret because they blend, to some degree, the decision to seek care with the decision on the provider.
In addition to the demographic, socioeconomic, and military experience variables shown in Table 6-10, the models also included several variables assessing potential attitudes and beliefs that could pose barriers to treatment seeking, which are described in Table 6-20 above. The analysis is of particular importance because of the possibility of identifying factors that may distinguish high-need users from high-need nonusers, thereby giving clues as to why veterans may not be receiving the treatment they need. As before, the analyses exclude veterans who had missing data on one or more of the variables in the regression from the analysis, and therefore the sample size varies across regression models. Only the independent variables that were statistically significant at the bivariate, or the full-model stage, were included in the final model.
The discussion focuses on the two-stage model with the screener scores included as independent variables. Tables 6-37 and 6-38 show the first and second regressions of the two-stage model. Table 6-37 shows the model for predicting use and then Table 6-38 shows the model predicting VA versus non-VA use among veterans with a need who used mental health services. As Table 6-37 shows, among the sociodemographic predictors, only income and having health insurance are statistically significant in predicting use, given a mental health need: having a higher income and having insurance lower the likelihood of using mental health services. However, having a non-zero disability rating is significantly associated with mental health service use, and places veterans in higher priority categories for receiving care from the VA, and thus is regarded as insured in this analysis. Among the military/service-related variables being in the Navy/Coast Guard also lowered the likelihood of using mental health services. Interestingly, longer deployments tended to be associated with lower odds of mental health treatment among those who needed mental health services. The odds of service use decline in a monotonic fashion from the reference group of veterans who were never deployed through categories with a deployment
| Variable | Variable Value | Odds Ratio | Lower CL | Upper CL |
|---|---|---|---|---|
| Income | $75,000 or more | 0.514* | 0.288 | 0.917 |
| Insured | Insured | 0.660* | 0.467 | 0.932 |
| Branch | Navy/Coast Guard | 0.652* | 0.451 | 0.944 |
| Deployment time | 13–24 months | 0.620* | 0.399 | 0.962 |
| Deployment time | 25–36 months | 0.530* | 0.322 | 0.873 |
| ATSPPH | Continuous | 1.080** | 1.050 | 1.112 |
| Encouraged to get help | Continuous | 3.361** | 2.298 | 4.917 |
| Perceived need | Yes | 1.991** | 1.503 | 2.638 |
| Disability rating | Disability 50 percent or higher | 4.504** | 2.853 | 7.111 |
| Disability rating | Disability less than 50 percent | 1.905** | 1.231 | 2.948 |
| Distance from VA | Don’t know | 0.406** | 0.217 | 0.759 |
NOTES: *p<.05; **p<.01; 95 percent confidence limits (CL) for the odds ratios. ATSPPH = Attitudes Toward Seeking Professional Psychological Help scale.
2,007 unweighted cases initially available, 520 unweighted cases excluded due to missing responses.
Model includes 1,487 unweighted cases representing weighted N of 1,252,699.
Reference categories for the variables are shown in Tables 6-10 and 6-20.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
| Variable | Variable Value | Odds Ratio | Lower CL | Upper CL |
|---|---|---|---|---|
| Female | Female | 0.471* | 0.239 | 0.929 |
| Income | $50,000 to $74,999 | 0.310* | 0.128 | 0.754 |
| Income | $75,000 or more | 0.300** | 0.136 | 0.665 |
| Insured | Insured | 0.111** | 0.035 | 0.355 |
| Deployment time | More than 48 months | 3.430* | 1.270 | 9.260 |
| Perceived need | Yes | 0.549* | 0.314 | 0.961 |
| Disability rating | Disability 50 percent or higher | 17.761** | 8.184 | 38.542 |
| Disability rating | Disability less than 50 percent | 5.984** | 2.792 | 12.823 |
| Distance from VA | 21–30 miles | 0.434* | 0.192 | 0.978 |
| Distance from VA | 31–40 miles | 0.357* | 0.138 | 0.928 |
| Distance from VA | More than 50 miles | 0.269** | 0.102 | 0.712 |
| Distance from VA | Don’t know | 0.046** | 0.017 | 0.127 |
NOTES: *p<.05; **p<.01; 95 percent confidence limits (CL) for the odds ratios.
1,105 unweighted cases initially available, 257 unweighted cases excluded due to missing responses.
Model includes 848 unweighted cases representing weighted N of 582,306.
Reference categories for the variables are shown in Tables 6-10 and 6-20.
SOURCE: Committee to Evaluate VA Mental Health Services, Veteran Survey, 2017.
of 25 to 36 months. The reasons for this association are not clear, but from a health services perspective it helps identify a group that is currently being underserved.
A particularly strong predictor of using mental health services is having a disability rating of 50 percent or more, as veterans with this disability rating were more likely to use the services as veterans who were not disabled (odds ratio [OR] = 4.504). Disabled veterans with a disability rating less than 50 were also more likely to use mental health services (OR = 1.905). In other words, veterans with a mental health need but without a disability rating were substantially less likely to be receiving mental health services than those who did have a disability rating.
As Table 6-37 shows, the analysis also provided some critical information as to whether service use was predicted by several barriers to mental health help seeking that could be potentially modified. Four variables were of particular interest as they might be useful in shaping policy or designing intervention strategies that might bring more veterans with need to mental health treatment. The first is recognizing a need for mental health treatment. As Table 6-37 shows, veterans who perceive such a need have nearly double the odds (OR = 1.99) of actually seeking treatment, which suggests the possibility that if this perception of need could be altered, more veterans with need would enter treatment. A second variable that the committee tested is stigma, and while stigma is clearly an issue of substantial concern to many veterans, the analysis did not find that it significantly predicted service use. A third variable, the ATSPPH Scale, examined whether veterans who believed treatment to be appropriate and potentially helpful for addressing mental health problems were more likely to be users of services. The highest score achievable on this scale is 30 points higher than the lowest score, and each point on the scale associated with an 8 percent increase (OR 1.08 for a one-unit change in the scale score) in the odds of seeking services. Thus, a veteran scoring 20 points higher would have a 160 percent increase in the odds of treatment seeking compared to the veteran scoring 20 points lower. Because the beliefs measured in this scale are potentially modifiable, this finding could be useful in guiding interventions aimed at bringing more veterans with need into treatment. Finally, a fourth potentially modifiable variable concerns whether or not a veteran reports having a friend or relative who encouraged mental health
help seeking. As Table 6-37 shows, veterans who had such support had more than three times the odds of seeking treatment than those who did not. Again, such a finding could be useful for policy and intervention if only by letting the people close to veterans know how important their support is and how helpful it could be in encouraging veterans to seek services.
Among veterans who have chosen to use mental health services, Table 6-38 shows the odds of choosing to use VA care versus non-VA care only. A factor that greatly increases the odds of using VA care is having a disability rating, whether less than 50 percent (which increased the odds by almost 6 times) or 50 percent or more (nearly 18 times). A second factor that substantially increases likelihood of using of the VA is having a cumulative deployment period of more than 4 years. Several other factors significantly reduce the likelihood of using the VA; the strongest such factor is insurance status. Veterans who have insurance are far less likely (about one-tenth as likely) to use VA care than those who do not have insurance. Among veterans who seek care, having higher income is another factor that makes them much less likely to use the VA. These findings suggest that veterans with resources—income or insurance access—use those resources to seek needed care outside of the VA. As might be expected, being at a distance from the nearest VA facility with mental health care services also decreases the odds of using VA services rather than non-VA services. This finding suggests that providing options for telemedicine and other remote access services could increase the number of veterans who choose to use VA for their mental health care. Finally, female veterans who use mental health services have significantly lower odds (about half) of using services compared to male veterans.
Existing Data from the Department of Veterans Affairs and the Broader Literature
As of 2015, VA data collection systems did not assess health care use patterns, which further complicates the already difficult task of predicting factors that may increase or decrease future use of VA health services (RAND Corporation, 2015). The committee notes, however, that delay-onset PTSD is one possible factor to consider when projecting the need of VA mental health services for OEF/OIF veterans in the future. The VA has seen many cases of veterans from previous eras presenting with PTSD and other mental health symptoms later in life (VA, 2015a), and the new cohort of Iraq and Afghanistan veterans may be no different. Maguen and colleagues (2012) found that it often takes more than 2 years from the last deployment to seek mental health care. Furthermore, they found that there was a median lag time of 7.5 years between an initial first visit for mental health care and beginning “minimally adequate” mental health treatment.
The predictors of use that have previously been studied could be informative in identifying factors that may increase the use of VA mental health services by OEF/OIF/OND veterans. Di Leone and colleagues (2013) found that some predictors, such as PTSD symptomatology and positive perceptions of VA care, were similar for both male and female OEF/OIF veterans. For men, however, being a minority was also significantly associated with the use of VA mental health services, whereas low income and having been sexually harassed were additional predictive variables for women. For all VA health services (not just mental health), Lee et al. (2015) found that OEF/OIF/OND veterans who were over age 50 or who had been in the Army or Marine Corps or had a “combat” or “logistics” military occupation had the highest proportion of VA use. Additionally, the study found a positive correlation between increasing cumulative deployment time and VA health services use.
It is well established that young adults, especially males, tend to use heath care less in general (Fasoli et al., 2010; Hoge et al., 2004; Mackenzie et al., 2006), and therefore, because many OEF/OIF/OND veterans are males and still quite young, it is conceivable that they may now have a predisposition toward not accessing any health care services at all, including mental health care. A study by Maguen et al. (2012)
similarly found that “men waited nearly 2 years longer than women” to seek mental health care, and also that younger age and racial/ethnic minority status were factors in delaying an initial mental health visit.
Conversely, being a female veteran is a predictor of increased use. A VA study focusing specifically on women veterans found that as a result of more women opting to join the military in recent years, there had been an 80 percent increase from FY 2003 to FY 2012 in the number of women using VA health services, with nearly one in five of all female VA patients having served in OEF/OIF/OND (Frayne et al., 2014). The study also reported that, in general, “women tend to use the full range of outpatient services” at the VA (p. 9) more than men, including mental health and substance use disorder services (37 versus 24 percent for any mental health/SUD service; 14 versus 8 percent for at least six visits) (Frayne et al., 2014).
Elbogen et al. (2013) found that the veterans who needed services the most were the ones who were most likely to actually access services. And, not surprisingly, OEF/OIF veterans who go to the VA for mental health services and also express a greater readiness for change tend to be those who make greater use of the services by attending more appointments (Jakupcak et al., 2013).
Kehle-Forbes and colleagues (2015) studied the two most prominent evidence-based psychotherapies endorsed at the VA, and reported that while 82 percent of the veterans in their study had agreed to start prolonged exposure therapy or cognitive processing therapy, 38.5 percent of those eventually dropped out of treatment. Younger veterans were more likely to drop out than older ones.
One possible reason for OEF and OIF veterans not using VA mental health services is simply that some of these veterans are not currently in need of those services. A study by Vaughan et al. (2014) reported that while veterans who had received VA mental health services did show high proportions of probable PTSD or depression (23 percent for PTSD; 21 percent for depression), those who had not sought such services did not have nearly as high a prevalence of the disorders (6 percent for PTSD; 8 percent for depression).
SUMMARY
This chapter details key characteristics of the OEF/OIF/OND veteran population, its potential need for mental health care services, the reasons why veterans may not be seeking mental health care (that is, what are the barriers to access to care?), and the factors that may influence the future use of VA mental health care services. The information presented in this chapter comes primarily from the committee’s survey of veterans; however, information from the committee’s site visits and from the literature also is included. A summary of the committee’s findings is outlined below.
Key Characteristics of the Operation Enduring Freedom, Operation Iraqi Freedom, and Operation New Dawn Cohort Who Use and Do Not Use the Department of Veterans Affairs Services
- Important demographic differences exist between the OEF/OIF/OND veteran population and the overall veteran population (that is, veterans from all eras).
- The OEF/OIF/OND veteran population is younger than the overall veteran population. Seventy-two percent of OEF/OIF/OND veterans are under age 50 while 79 percent of the overall veteran population is over 55 years of age.
- More OEF/OIF/OND veterans are women than in previous eras. Twenty-one percent of OEF/OIF/OND veterans are women versus 9 percent of the overall veteran population. From FY 2003 to FY 2012, there was an 80 percent increase in the numbers of women veterans using VA health services.
- The OEF/OIF/OND veteran population is more racially and ethnically diverse than the overall veteran population. Sixty-six percent of OEF/OIF/OND veterans are non-Hispanic white versus 77 percent of the overall veteran population.
Need for and Use of the Department of Veterans Affairs Mental Health Care Services
- Evidence from the committee’s survey suggests the OEF/OIF/OND veteran population potentially has a substantial need for mental health care services.
- Of the estimated 4.2 million OEF/OIF/OND veterans, 41 percent screen positive on at least one of the mental health screening measures used in the survey or reported that they were told by a health professional that they have a mental health condition. (A positive screen does not necessarily mean that a veteran has a mental health condition. The screeners used in the survey cannot be used to make a diagnosis; rather, they indicate a need for further assessment by a mental health professional to determine a diagnosis and whether there is a need for treatment.) These data are consistent with the results from another national survey of OEF/OIF/OND veterans (Elbogen et al., 2013).
- Over two-thirds (69 percent) of OEF/OIF/OND veterans who had a positive result on one or more mental health screeners reported having been told recently by a health professional that they have a least one mental health disorder.
- Of the veterans who screened negative on the all of the screening measures in the survey, the overwhelming majority (96 percent) do not use either VA or non-VA mental health services.
- An estimated 22 percent of OEF/OIF/OND veterans perceive a need for care (as measured by responses to a question about whether the veterans felt a need to see a professional because of mental health problems). Fewer veterans express a perceived need than the estimated number of veterans with an assessed need (positive screens or reported diagnosis), but perceived need also indicates a potential need for follow-up assessment among a substantial number of veterans.
- Over half of veterans with a positive screen do not perceive a need for mental health services, which suggests that some veterans do not seek care because they do not perceive that they personally have a need.
- Combat exposure and cumulative deployment time are among the strongest predictors associated with having a mental health need.
- Higher scores on the screening measures are associated with a higher probability of perceived need for mental health care. The number of positive screens also was a strong predictor of the perception of need.
- The variables other than the screening measures that have a statistically significant association with perceived need are gender, income, and service in the National Guard/Reserves. Women have more than double the odds of perceiving a mental health need than men, veterans earning $50,000–$75,000 per year have nearly double the odds of perceiving a mental health need than veterans in the lowest income bracket, and those in the National Guard/Reserves are less likely to perceive a mental health need than those on active duty.
- Given the estimates of potential need found in the survey, the committee examined the degree to which these needs are addressed or met. The survey data suggest there is potentially substantial unmet need for mental health care services in the OEF/OIF/OND population.
- Of those who have an assessed mental health need (as determined by positive mental health screens or reported diagnosis), less than half (44 percent) of OEF/OIF/OND veterans have
-
-
sought either VA or non-VA mental health care services. While all of the remaining estimated 940,000 veterans cannot definitively be categorized as having unmet needs, the survey results suggest that a substantial number do have unmet needs.
- Among the 22 percent of veterans reporting a perceived mental health need, 48 percent have sought either VA or non-VA mental health care services. When restricted to those veterans with a perceived need who also had an assessed need, 55 percent sought such care.
- Therefore, depending on which measure of potential need is used (assessed need or assessed need in combination with perceived need), the proportions using VA or non-VA mental health care services varies from 44 to 55 percent, a range that suggests that a large number of veterans are not getting care and that the potential unmet may be substantial.
- Veterans who have a mental health need but do not have a disability rating are substantially less likely to be receiving mental health services than those who do have a disability rating.
-
- OEF/OIF/OND veterans who have a mental health need are more likely to use VA mental health care services than to use non-VA mental health care services.
- Among the OIF/OIF/OND veterans with a mental health need who used mental health care services, an estimated two-thirds (64 percent) used VA mental health services, with the remainder using only non-VA providers.
- Among the OEF/OIF/OND veterans with a perceived need who used mental health care services, the percent using VA services is somewhat lower (59 percent).
Barriers and Facilitators to Service Use
- The most common reasons reported by veterans with a mental health need for using VA mental health care services include
- Prescription benefits (87 percent).
- Entitlement to services (85 percent).
- Lower cost of care (83 percent).
- Convenience of the VA location (68 percent).
- Liking the VA doctors or already using the VA for years (64 percent).
- The VA is the only available source of mental health care (64 percent).
- The most common reasons reported by veterans with a mental health need for not using VA mental health care services include
- Lack knowledge about how to apply for benefits (42 percent).
- Believe that they are not eligible or entitled to services (40 percent).
- Not aware that the VA offers mental health services (33 percent).
- Use other sources of mental health care (33 percent).
- Do not need care (32 percent).
- Feel that they do not deserve to receive mental health care benefits from the VA (30 percent).
- Do not trust the VA (30 percent).
- Had a prior bad experience at the VA (23 percent).
- Do not feel welcome at the VA (19 percent).
-
Several possible barriers to accessing VA mental health care were identified in the committee’s research, particularly for OEF/OIF/OND veterans with mental health need who do not use the VA for mental health services.
- Transportation challenges.
-
-
- Physical distance to a VA facility. A lower percentage of non-VA users with a mental health need live within 30 miles of a VA facility than VA users with a mental health need (45 versus 73 percent). Eleven percent of non-VA users with a mental health need report living more than 50 miles compared with 9 percent of VA users with a mental health need.
- Travel time to a VA facility. A lower percentage of non-VA users with a mental health need live within a 45-minute drive from a VA facility, compared with VA users with a mental health need (44 versus 76 percent). Fourteen percent of non-VA users with a mental health need live more than 1 hour from a VA facility, compared with 10 percent of VA users with a mental health need.
- Overall ease of access to a facility. A lower percentage of non-VA users with a mental health need reported that it is very easy, somewhat easy, or neither easy or hard to get to the nearest VA facility that offers mental health services than VA users with a mental health need (49 versus 75 percent).
- Additional transportation challenges include the facts that some veterans have to rely on public transportation or rides from organizations such as the Disabled American Veterans and that some veterans who have PTSD and/or chronic pain may not be comfortable using public transit or driving long distances.
- Challenges associated with accessing care (for example, making appointments).
- More than half (54 percent) of VA users with a mental health care need find the process of getting mental health care to be very or somewhat burdensome. Regression analysis shows that predictors for finding the process of getting mental health care to be very or somewhat burdensome are having insurance, having PTSD, and having a higher barriers score.
- Only about half (49 percent) of VA users with a mental health care need reported that it was always or usually easy to get an appointment, and only 17 percent reported that evening, weekend, and holiday appointments were always or usually available. Regression analysis shows that predictors for finding the process of getting an appointment with a mental health provider never easy are a high score on the DRRI combat scale and having depression. Having depression is also a predictor for never being able to get VA mental health care on evenings, weekend, and holidays.
- About one-third (34 percent) of VA users with a mental health care need reported that they were very or somewhat dissatisfied with the time between their requests and the appointments. Regression analysis shows several statistically significant predictors for being dissatisfied with time to appointment (never having been married or being divorced, having an associate’s or bachelor’s degree, being an officer, having to travel more than an hour to a VA facility, and perceived need).
- Other obstacles that present challenges to obtaining mental health care.
- Employment concerns such as time off from work (37 percent of veterans who have a mental health need; this number also includes concerns about getting child care), harm to career (37 percent), denial of security clearance (33 percent), and less confidence and respect from co-workers (36 percent) and supervisors (35 percent).
- Fear of discrimination in domains such as gun ownership (35 percent), loss of contact with or custody of children (15 percent), and loss of medical or disability benefits (12 percent).
-
- In general, VA users with a mental health need are satisfied with their mental health providers and with the services they receive from the VA.
- The overwhelming majority of VA users with a mental health need are somewhat or very positive about VA’s delivery of services (availability of needed services, privacy and confidentiality of medical records, ease of using VA mental health care, mental health care staff’s skill and expertise, and staff’s courtesy and respect toward patients).
- Among OEF/OIF/OND veterans with a mental health need, veterans were more likely to use VA mental health services if they had a disability rating of 50 percent or higher, perceived a need for mental health treatment, believed mental health treatment is appropriate and potentially helpful, and were encouraged to seek help by a relative or friend.
Future Use of the Department of Veterans Affairs Mental Health Services
- It is estimated that nearly two-thirds of OEF/OIF/OND veterans indicated that they might use VA mental health care services in the future, although the committee believes that this finding may be overstating future use because only about one-third of veterans who have mental health care need and perceive that they need care use the VA for mental health care services.
- Among OEF/OIF/OND veterans who do not plan to use VA mental health care services, the reasons for not doing so include that they prefer to see a non-VA mental health provider (61 percent), the wait times for appointments at the VA are too long (38 percent), the physical distance to a VA medical facility is too great (25 percent), and the VA does not provide good quality treatment (19 percent).
- Changes that OEF/OIF/OND veterans would like to see at the VA include making the process for scheduling appointments easier, better quality services and customer service, and more available services or facilities.
- Regarding the mode of delivery, 45 percent of OEF/OIF/OND veterans would likely use the Internet and 44 percent would likely use the phone to receive mental health care. Younger veterans tended to be more open to obtaining mental health care using the Internet.
REFERENCES
Commission on Care. 2016. Final report of the commission on care. Washington, DC: Commission on Care.
Di Leone, B. A., D. Vogt, J. L. Gradus, A. E. Street, H. L. Giasson, and P. A. Resick. 2013. Predictors of mental health care use among male and female veterans deployed in support of the wars in Afghanistan and Iraq. Psychological Services 10(2):145–151.
Elbogen, E. B., H. R. Wagner, S. C. Johnson, P. Kinneer, H. Kang, J. J. Vasterling, C. Timko, and J. C. Beckham. 2013. Are Iraq and Afghanistan veterans using mental health services? New data from a national random-sample survey. Psychiatric Services 64(2):134–141.
Fasoli, D. R., M. E. Glickman, and S. V. Eisen. 2010. Predisposing characteristics, enabling resources and need as predictors of utilization and clinical outcomes for veterans receiving mental health services. Medical Care 48(4):288–295.
Frayne, S. M., C. S. Phibbs, F. Saechao, N. C. Maisel, S. A. Friedman, A. Finlay, E. Berg, V. Balasubramanian, S. K. Dally, L. Ananth, Y. Romodan, J. Lee, S. Iqbal, P. M. Hayes, L. Zephyrin, A. Whitehead, A. Torgal, J. G. Katon, and S. Haskell. 2014. Sourcebook: Women veterans in the Veterans Health Administration. Volume 3. Sociodemographics, utilization, costs of care, and health profile. Washington, DC: Women’s Health Evaluation Initiative, Women’s Health Services, Veterans Health Administration, Department of Veterans Affairs.
GAO (Government Accountability Office). 2017. DcD health: Actions needed to ensure post-traumatic stress disorder and traumatic brain injury are considered in misconduct separations. Washington, DC: Government Accountability Office.
Hoge, C. W., C. A. Castro, S. C. Messer, D. McGurk, D. I. Cotting, and R. L. Koffman. 2004. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. New England Journal of Medicine 351(1):13–22.
Hosmer, D. W., and S. Lemeshow. 1980. A goodness-of-fit test for the multiple logistic regression model. Communications in Statistics A10:1043–1069.
IOM (Institute of Medicine). 2013. Returning home from Iraq and Afghanistan: Assessment of readjustment needs of veterans, service members, and their families. Washington, DC: The National Academies Press.
IOM. 2014. Treatment for posttraumatic stress disorder in military and veteran populations: Final assessment. Washington, DC: The National Academies Press.
Jakupcak, M., K. D. Hoerster, R. K. Blais, C. A. Malte, S. Hunt, and K. Seal. 2013. Readiness for change predicts VA mental healthcare utilization among Iraq and Afghanistan war veterans. Journal of Traumatic Stress 26(1):165–168.
Kehle-Forbes, S. M., L. A. Meis, M. R. Spoont, and M. A. Polusny. 2015. Treatment initiation and dropout from prolonged exposure and cognitive processing therapy in a VA outpatient clinic. Psychological Trauma 8(1):107–114.
Krouse, W. J. 2015. Gun control legislation in the 113th Congress. Washington, DC: Congressional Research Service.
Krouse, W. J. 2017. Gun control: Federal law and legislative action in the 114th Congress. Washington, DC: Congressional Research Service.
Lee, S. E., V. P. Fonseca, C. L. Wolters, D. D. Dougherty, M. R. Peterson, A. I. Schneiderman, and E. K. Ishii. 2015. Health care utilization behavior of veterans who deployed to Afghanistan and Iraq. Military Medicine 180(4):374–379.
Liu, E. C., E. Bagalman, V. S. Chu, and C. S. Redhead. 2013. Submission of mental health records to NCIS and the HIPAA privacy rule. Washington, DC: Congressional Research Service.
Mackenzie, C., W. Gekoski, and V. Knox. 2006. Age, gender, and the underutilization of mental health services: The influence of help-seeking attitudes. Aging and Mental Health 10(6):574–582.
Maguen, S., E. Madden, B. E. Cohen, D. Bertenthal, and K. H. Seal. 2012. Time to treatment among veterans of conflicts in Iraq and Afghanistan with psychiatric diagnoses. Psychiatric Services 63(12):1206–1212.
McNiel, D. E., C. M. Weaver, and S. E. Hall. 2007. Base rates of firearm possession by hospitalized psychiatric patients. Psychiatric Services 58(4):551–553.
Mott, J. M., K. M. Grubbs, S. Sansgiry, J. C. Fortney, and J. A. Cully. 2014. Psychotherapy utilization among rural and urban veterans from 2007 to 2010. Journal of Rural Health 31(3):235–243.
RAND Corporation. 2015. Assessment A (Demographics). Santa Monica, CA: RAND Corporation.
Simpson, J. R. 2007. Bad risk? An overview of laws prohibiting possession of firearms by individuals with a history of treatment for mental illness. Journal of the American Academy of Psychiatry and Law 35(3):330–338.
Swords to Plowshares. 2016. Presentation to the Commission on Care. https://commissiononcare.sites.usa.gov/files/2016/03/Presentation-on-OTH-Discharges.pdf (accessed July 20, 2016).
U.S. Census Bureau. 2015. American Community Survey: Veterans statistics. https://www.census.gov/library/visualizations/2015/comm/veterans-statistics.html (accessed June 9, 2017).
VA (Department of Veterans Affairs). 2014. Selected Veterans Health Administration characteristics: FY 2002 to FY 2014. http://www.va.gov/vetdata/Utilization.asp (accessed November 12, 2015).
VA. 2015a. Aging veterans and posttraumatic stress symptoms. http://www.ptsd.va.gov/public/types/war/ptsd-older-vets.asp (accessed November 12, 2015).
VA. 2015b. Analysis of VA health care utilization among Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) veterans: Cumulative from 1st qtr FY 2002 through 2nd qtr FY 2015 (October 1, 2001–March 31, 2015). Washington, DC: Department of Veterans Affairs.
VA. 2015c. Health benefits. http://www.va.gov/HEALTHBENEFITS/apply/veterans.asp (accessed October 23, 2015).
VA. 2015d. Health benefits—Priority groups. http://www.va.gov/HEALTHBENEFITS/resources/priority_groups.asp (accessed October 23, 2015).
VA. 2015e. Veterans Health Administration. http://www.va.gov/health/ (accessed October 23, 2015).
VA. 2015f. Veterans population by veterans integrated service network (VISN): Fiscal year 2015. https://www.va.gov/vetdata/docs/Maps/Vetpop14_VISN.pdf (accessed February 2, 2017).
VA. 2016. Mental Health Satisfaction Survey: Veteran Satisfaction Survey (VSS) National Results. Department of Veterans Affairs.
VA. 2017a. Follow up: Information request from NASEM Committee to Evaluate VA’s Mental Health Services. Department of Veterans Affairs.
VA. 2017b. National Center for Veterans Analysis and Statistics: The veteran population model. https://www.va.gov/vetdata/veteran_population.asp (accessed July 19, 2017).
VA. 2017c. Profile of post-9/11 veterans: 2015. https://www.va.gov/vetdata/docs/SpecialReports/Post_911_Veterans_Profile_2015.pdf (accessed July 19, 2017).
VA. 2017d. Response to committee request for information. Department of Veterans Affairs.
VA. 2017e. VA secretary announces intention to expand mental health care to former service members with other-than-honorable discharges and in crisis. Washington, DC: Department of Veterans Affairs.
VA. 2017f. VA caregiver support.https://www.caregiver.va.gov/support/support_benefits.asp. (accessed October 6, 2017).
VA National Center for Veterans Analysis and Statistics. 2016. Table 11l: Vetpop2014: Living veterans by Veteran Integrated Service Network, age group, gender, 2013–2043. https://www.va.gov/vetdata/veteran_population.asp (accessed November 6, 2017).
Vaughan, C. A., T. L. Schell, T. Tanielian, L. H. Jaycox, and G. N. Marshall. 2014. Prevalence of mental health problems among Iraq and Afghanistan veterans who have and have not received VA services. Psychiatric Services 65(6):833–835.
This page intentionally left blank.































































