
4
Translating Conceptual Models of Infectious Disease Transmission and Control into Practice
The second half of session 1 featured case studies for translating conceptual models of infectious disease control and transmission into practice. The session was moderated by Marcos Espinal, director of communicable diseases and health analysis at the Pan American Health Organization. Frank Mahoney, senior immunization officer at the International Federation of Red Cross and Red Crescent Societies, described the effect the West Africa Ebola virus disease (EVD) outbreak had on the epidemiology of other infectious diseases. Emily Gurley, associate scientist in the Department of Epidemiology at the Johns Hopkins Bloomberg School of Public Health, described efforts to control the transmission of waterborne diseases in Dhaka, Bangladesh. Albert Ko, professor and chair of the Department of Epidemiology of Microbial Diseases at the Yale School of Public Health, examined the transmission and control of leptospirosis and Zika virus in Brazilian slums. Robin Wood, chief executive officer of the Desmond Tutu HIV Centre and Foundation at the University of Cape Town, explored transmission and control of tuberculosis (TB) in Cape Town, South Africa.
EFFECT OF THE WEST AFRICA EBOLA VIRUS DISEASE OUTBREAK ON OTHER INFECTIOUS DISEASES
Frank Mahoney, senior immunization officer at the International Federation of Red Cross and Red Crescent Societies, spoke about the effect of the West Africa EVD outbreak on the epidemiology of other infectious diseases based on his experience as a medical epidemiologist with the U.S.
Centers for Disease Control and Prevention (CDC) during the epidemic. He began his presentation by sharing the case of diplomat Patrick Sawyer who was being monitored in Monrovia, Liberia, for suspected EVD in July 2014. Sawyer left the country and traveled to Lagos, Nigeria, where he was admitted to a local hospital with a provisional diagnosis of malaria. The chief medical officer at the hospital suspected EVD, and the diagnosis was confirmed 2 days before Sawyer died. Mahoney reported that 72 health care workers and airport staff overall were exposed to the disease through Sawyer. To illustrate how the exposure occurred, he cited a statement from the case investigation form made by a health care worker who cared for Sawyer:
On getting to the patient, I discovered his intravenous line was by his side and picked it up with bare hands to hang on the drip stand. I called the nurse to assist the patient to [the] toilet. I had a cut on my hand and did not remember to wash my hands until much later in the shift.
At the time, he said, many health care workers in the area were not trained to scrupulously reduce exposure to infectious bodily fluids.
Effect of the Outbreak on the Health Workforce and Health Services Provision
According to Mahoney, the EVD outbreak in West Africa had a substantial effect on the health systems in the region between 2014 and 2015, affecting both the health workforce and the provision of health services in the region. During the epidemic, he said, a total of 815 health care workers were infected, and of the known outcomes, the mortality rate was 66 percent (WHO, 2015). Early in the outbreak, he reported, a high proportion of the EVD cases occurred among the health workforce (see Figure 4-1). However, training on infection control for every health worker helped to reduce the proportion of health care worker deaths to around 1 percent by the end of the outbreak (WHO, 2015). The geographic distribution of EVD infection among health care workers in West Africa spanned both urban and rural settings, noted Mahoney. A diverse range of health care workers were infected, he said, mainly workers who had primary contact with patients, such as nurses and nurse aids. He explained that this had a major effect on the health care system, such as limiting the provision of services, closing many facilities, and raising concerns among the health care workers about becoming infected in health care settings—especially when managing patients with febrile illness and/or hemorrhage. At the community level, he said that people also had fears of becoming infected by receiving treatment
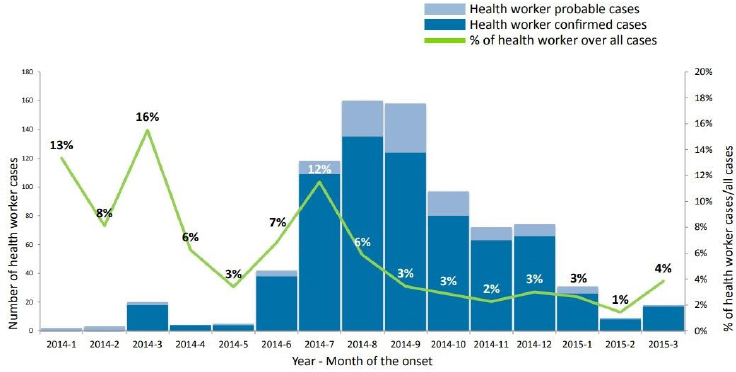
NOTE: All cases include health worker and nonhealth worker confirmed and probable cases.
SOURCES: Mahoney presentation, December 12, 2017; WHO, 2015. Reprinted from Health worker Ebola infections in Guinea, Liberia, and Sierra Leone, preliminary report, page 3, Copyright (2015).
in health care settings and would tend to seek care from community health care workers.
Mahoney reported that there was a subsequent decrease in the use of health care services during the outbreak, which has been documented by multiple studies on the effect of the EVD outbreak on health care delivery in West Africa. For example, he cited a study that investigated the average monthly consultations for children under 5 years of age before and during the EVD outbreak in Sierra Leone, finding reductions in visits for malaria (–27 percent), acute respiratory infection or pneumonia (–27 percent), and acute watery diarrhea (–38 percent); however, there was an 80 percent increase in the number of patients who came in with measles (Sesay et al., 2017). He also described a community-level, population-based survey assessing health care use during and after the EVD outbreak in Liberia, which found that in December 2014 (around the peak of the outbreak), among the 25 percent of households reporting a sick child in the previous 2 weeks, only 40 percent of them sought care for the sick children in the health care system; this rebounded to between 80 and 90 percent by March 2015 (Morse et al., 2016). During the peak of the epidemic, people stopped accessing care, he said, but it seemed that they quickly recovered. He cited
several more studies documenting the negative effects of EVD on health care delivery in the region:
- In hospitals and public health clinics in Guinea, there were decreases in HIV testing, in Pentavalent 1 and 3 vaccinations, and in visits for acute respiratory infections and acute watery diarrhea (Barden-O’Fallon et al., 2015).
- Across 15 facilities in Sierra Leone, there was a decrease in outpatient visits (Elston et al., 2016).
- In a hospital setting in Guinea, there were decreases in clinic or pharmacy visits and in antiretroviral compliance (Cisse et al., 2015).
- In mobile treatment facilities in Guinea, there were decreases in outpatient visits (–40 percent), in HIV testing (–46 percent), in enrollment in HIV care (–47 percent), and in new diagnoses of HIV (–53 percent) (Leuenberger et al., 2015).
Changes in the Epidemiology of Priority Diseases
Mahoney explained that changes in health care use caused by the EVD outbreak in West Africa gave rise to concerns about changes in the epidemiology of priority diseases in the region—HIV, malaria, and TB. He described a study that modeled the effect of the EVD outbreak on the malaria, HIV, and TB disease burdens in Guinea, Liberia, and Sierra Leone. He said that the analysis attributed approximately 7,000 additional deaths from malaria as a result of the outbreak and a change of approximately 50 percent in malaria-attributable mortality rates in all three countries.1 For HIV, he said, they estimated around 1,000 additional deaths and a change in the HIV-attributable mortality rate of around 15 percent.2 He added that for TB they estimated around 3,000 additional deaths and a subsequent 50 to 60 percent change in the TB-attributable mortality rate (Parpia et al., 2016).3 He described a different study that found increases in untreated malaria cases of 45 percent in Guinea, 88 percent in Sierra Leone, and 140 percent in Liberia in 2014; researchers estimated the disease burden at 3.5 million additional untreated cases and 10,900 additional malaria-attributable deaths (Walker et al., 2015).
Other diseases were affected as well, noted Mahoney. People stopped
___________________
1 Based on an estimated 50 percent reduction in treatment coverage among children less than 5 years of age.
2 Based on 50 percent reduction in antiretroviral coverage among persons 15 to 49 years of age.
3 Based on 50 percent reduction in treatment coverage for both drug-susceptible and drug-resistant TB.
coming for their immunizations, he said, and Guinea, Liberia, and Sierra Leone all experienced reductions in coverage for both diphtheria-tetanus-pertussis and measles, leading to an increase in susceptibility, based on World Health Organization (WHO)-United Nations Children’s Fund (UNICEF) estimates of vaccination coverage. According to 2015 estimates, he reported, there were large numbers of children up to 3 years of age in Liberia who were susceptible to measles, and as expected, all of the countries experienced measles outbreaks in 2015; he noted that they all implemented measles supplemental immunization campaigns to mitigate those outbreaks. He described another study on all-cause mortality in Moyamba District, Sierra Leone, which reviewed burial team data for a 5-month period (November 2014 to April 2015). He said they reported 496 deaths among children less than 1 year of age, 786 among children less than 5 years of age, and around 1,300 deaths among persons less than 50 years of age. He noted that Ebola caused only 2 percent of these deaths and that mortality was 3.4 times higher than the average mortality in the preceding 3 years. Although death registration may not be entirely accurate, he added, it still represents a threefold increase (Elston et al., 2016).
Mahoney reiterated that the EVD outbreak had major effects on the health workforce and on health service delivery in the region, which led to decreases in access and use of services for major infectious diseases. He noted that models predicted an increase in subsequent mortality that was difficult to measure in practice, with only limited data showing resulting increases in mortality. However, he suggested that local measures may have mitigated this effect, such as interventions against measles and mass drug administration for malaria.
Management of Outbreaks in Urban Settings
Mahoney discussed some potential lessons that might be gleaned from the management of the EVD outbreak in West Africa, using specific examples from the outbreak management in Liberia and in Nigeria. He related that early in the outbreak in Liberia—when the number of suspect cases was doubling every 2 weeks—a presidential task force was deployed to manage the situation. He explained that the task force implemented quarantine in West Point, the largest slum in the capital of Liberia, which led to conflict with and resistance from the community. He said that it ultimately created mistrust in the government regarding the whole epidemic response. Providers participating in the response were also concerned, he added, as Montserrado County was overwhelmed with cases: there were not enough Ebola treatment unit (ETU) beds, people were dying in the streets, and models were predicting hundreds of thousands of EVD cases. Responders debated about the type of care that should be provided (ETU model of
care, home care, or transit centers), he said, and they were concerned about managing patients within a health care system that had already been hugely affected by the beginning of the outbreak.
To develop a Liberian strategy, Mahoney said meetings were convened with international partners in August 2014. He said the key elements of the strategy were early identification and isolation of suspect patients (through intensified surveillance, contact tracing, and clinical management in dedicated treatment centers); safe transportation; prevention of transmission in the health care setting; and safe burials. He noted that the strategy did not include treatment within the existing health care system, distribution of home health care kits, wide-scale support for water and distribution of hygiene kits, or the involuntary quarantine of infected households.
Mahoney presented a range of challenges related to the construction of ETUs in Liberia. He said they are costly, in terms of both money and human resources, because 400 health care workers were required per 100-bed ETU, and few support organizations had the relevant experience. One strategy for addressing these challenges, he said, was to set up an ETU in an abandoned hospital. He explained that the Island Clinic in Montserrado County, Liberia, was renovated into a 100-bed hospital with WHO support and was managed by the government. He reported that it was filled within hours of opening and had more than 200 admissions in the first week, but within 2 months of opening in 2014, there was a remarkable drop in admissions in Montserrado County (WHO, 2014). He reported that Nigeria also experienced a crisis when faced with several highly probable cases of EVD but had nowhere to care for them. He explained that they resolved this by setting up an ETU in an abandoned hospital ward in Lagos, where they set up improvised hygiene stations and clinical staff were mentored by people with previous ETU experience (Shuaib et al., 2014).
After the initial decline of EVD cases in more populated areas, Mahoney said they faced rural outbreaks of EVD in isolated communities in Liberia caused by infected people leaving the city and seeding outbreaks in these areas. He explained that the response to those rural outbreaks was called the Rapid Isolation and Treatment of Ebola strategy, which served as a complement to the other outbreak response activities. Over time, he said, the strategy helped reduce the intervention period interval quite substantially over the course of the epidemic. Mahoney concluded by suggesting the following set of strategies for maintaining the capacity for preparedness moving forward:
- Rapidly detect and isolate patients.
- Identify—in advance—facilities to manage patients with hemorrhagic fever.
- Embed infection control practices into everyday practice.
- Maintain skills of clinical staff.
- Engage with communities for effective management of response.
WATERBORNE DISEASES IN DHAKA, BANGLADESH
Emily Gurley, associate scientist in the Department of Epidemiology at the Johns Hopkins Bloomberg School of Public Health, gave a presentation on the waterborne transmission of cholera in the urban built environment, illustrating practical strategies for preventing and mitigating the transmission of cholera that have been used in Dhaka, Bangladesh. She opened by lamenting that, from an epidemiological perspective, not enough progress has been made since John Snow’s seminal work tracing the 1854 cholera epidemic in London to the Broad Street pump by mapping the hotspots of disease. She noted that many current strategies for cholera remain similar to Snow’s work. Gurley said that progress has been made in many other ways, however. For example, she reported that Millennium Development Goal (MDG) 7c, which aimed to halve the population without sustainable access to safe drinking water, was achieved through collaborative efforts and commitment to the goal. That said, she noted that achieving sustainability of access and safety of drinking water remains a struggle—not only in how to go about it but how to measure it. For the purposes of the MDGs, she noted, sustainable access to safe water was defined as the proportion of the population using improved drinking water sources. She explained that improved sources are designed and constructed to deliver safe water, such as covered sources that are expected to be protected from microbial contamination (for example, this would not include a lake or an open shallow well).
Gurley reported that worldwide there is still a large degree of heterogeneity and inequity in terms of access to safe drinking water. In many countries, she said, the situation may appear relatively good, but within a country’s political boundaries, there is often substantial heterogeneity in access to safe water. She explained that this is the case in Bangladesh, where WHO data estimate that between 76 and 85 percent of the population have been using improved drinking water sources since 2000, but there are reasons to be skeptical that this trend is reflected countrywide (WHO, 2017c).
Reducing Cholera Transmission in Arichpur of Dhaka, Bangladesh
Since 2009, Gurley has been working on reducing waterborne infections in Arichpur of Tongi Township in Dhaka, Bangladesh. She explained that Arichpur is densely populated, with around 50,000 residents in an area of roughly one-half of a square kilometer. She added that the community has few high-rise buildings, but adjacent to the community is a
large open campground where 5 million people converge from Bangladesh and 150 countries every January for Bishwa Ijtema, the largest gathering of Muslims in the world. Gurley explained that Arichpur is a very wet place, bounded to the south by a river and subject to monsoon floods; the drainage is poor and streets are prone to flooding, which makes them difficult to navigate.
Despite its wet climate, Gurley noted, it is difficult to access safe drinking water in Arichpur. She noted that Bangladesh has done much work to improve access to drinking water: cities have improved their water sources and the majority of the country’s residents have access to improved water sources, mostly from municipal water supplies (57 percent) (Gurley et al., 2014). However, she said that the safety of those municipal water supplies is uncertain because they are relatively old, and the population has grown faster than the supply and infrastructure can keep up with. She said that many people resort to finding the main water line and creating their own access. She explained that open sewers running through the streets often contain makeshift hoses that run the municipal water supply into homes. She said that this creates many opportunities for contamination, such as breaches in the municipal water lines. She was initially called to work in Arichpur because of an outbreak of hepatitis E caused by a mass contamination of the municipal water supply, which spread quickly through the community and infected around 4,000 people (Gurley et al., 2014).
Gurley explained that they began considering how to address cholera in Arichpur and how to better understand the drivers of the established cholera risk. Understanding those drivers, she said, requires strategies to improve surveillance and to predict the areas and populations that are at the highest risk in the community. She explained that the current standard of cholera surveillance is to wait for people to visit a health facility and be diagnosed, at which point they are usually quite ill already. She deemed this strategy unsatisfactory for multiple reasons. She said that it identifies only severe cases, especially in areas with poor access to care. She added that it is not timely, because by the time severe cases present themselves, it is likely that a number of other cases in the community already occurred, and the opportunity to prevent the outbreak may have been lost. To improve their strategy, she said, they aimed to build a cholera surveillance system that would ideally be able to identify the etiologies—including being able to find mild and severe cases to study—and would enable notification as close to the time of infection as possible. They carried out studies on three potential surveillance strategies: cholera prediction through pharmacy sales; the Choleraphone community surveillance intervention; and cluster analysis of cholera risk factors in the community.
Cholera Prediction Through Pharmacy Sales
Gurley described the first study, where she and her colleagues decided to try a cholera surveillance strategy using data on sales of oral rehydration solution (ORS) among pharmacies and drug sellers as an early warning system for cholera. In a survey study, she said, they enrolled 50 of the 120 drug sellers identified in Arichpur and asked them to send the researchers a daily text message with the number of ORS packets sold at the end of the day. She explained that the ORS sales data were compared to the traditional cholera surveillance system that was already in place in Dhaka. The study found that between April and October 2013, cholera cases represented about 22 percent of total diarrhea hospitalizations, she reported, and analysis revealed seasonality to ORS sales that corresponded with the seasonality of diarrhea and cholera (Azman et al., 2015). It also revealed the spatial distribution of cholera sales, she added, when they aligned all the pharmacies based on their locations in the community and found spatial heterogeneity in where the ORS packets were being sold. She said that this spatial heterogeneity also corresponded with where they found cases of diarrhea and cholera. Although they found significant correlations between ORS sales and cholera, she noted, it was not a great predictor because it was only able to provide an early signal 1 day ahead of the cholera. Furthermore, she noted that the data are noisy and not specific enough because ORS interventions in Bangladesh have been so successful that the packets are readily available and commonly used for reasons other than diarrhea treatment.
Choleraphone Surveillance Intervention
Gurley continued to describe another approach in the same community using a surveillance intervention called Choleraphone. They enrolled a cohort of 400 households nested within a study on access to water, she said, and each household was provided with a phone that was recharged every month. Households were asked to call the study team when someone in the house had diarrhea, she explained, and then a health care worker would visit that home to provide ORS and request that the person self-collect a rectal swab. The incidence of diarrhea found through the Choleraphone was compared to a household survey, but she hoped that this approach would provide the etiology and offer a real-time picture of cholera in the community. She said that people did report diarrhea over the phone, but overall the incidence was much lower than expected. She noted that the study population is highly mobile and difficult to study; many enrolled households dropped out for various reasons, such as leaving or moving elsewhere in the community or reluctance to self-collect a rectal swab.
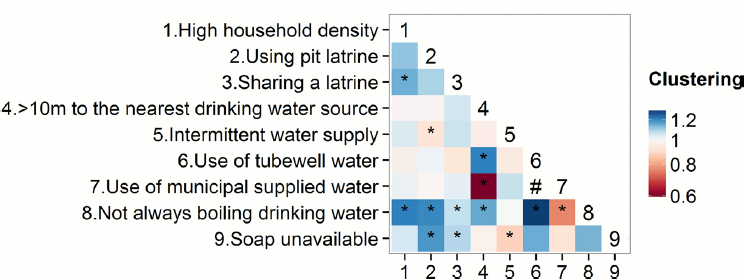
NOTES: Shading of cells indicates estimates of co-occurrence of different exposures and denotes intraclass correlation coefficient estimates between 0.6 and 1.2. Values above 1 suggest a tendency for two exposures to appear in the same households or matched-set closer to each other (co-occurrence of two exposures). Values less than 1 suggest a tendency for two exposures not to appear together. Numbers on the x-axis refer to the corresponding number listed as the high-risk factors for cholera on the y-axis. * Statistically significant estimates based on 1,000 bootstrap iterations. # Result not shown because the “Use of municipal supplied water” risk factor was structurally correlated to the “Use of tubewell water” risk factor. SOURCES: Gurley presentation, December 12, 2017; Bi et al., 2016.
Cluster Analysis of Cholera Risk Factors in the Community
Gurley explained that the third strategy was a study looking at clustering of risk factors for cholera within the community (Bi et al., 2016). For every confirmed case, she explained, they enrolled sets of spatially matched control households and then compared households distributed throughout these communities, looking for spatial clustering of high-risk factors for waterborne disease in general and cholera in particular. She reported that they found a large amount of clustering (see Figure 4-2); for example, households without hand soap were highly clustered with those using pit latrines. Spatially, those risk factors were clustered together within households, she noted, and added that even within this area of high risk, there were pockets that were at much higher risk than others based on what is known about transmission.
Gurley concluded by suggesting that it is useful to appreciate and under-
stand these types of substantial and important spatial heterogeneities in risk, even within a single community, because those clusters of exposure can be targeted for interventions, such as vaccination. She noted that, although good vaccines are available, the ability to deploy them well and in a timely way is an ongoing struggle. They are considering carrying out seroprevalence surveys that could identify where people have been infected previously and help think about risk going forward, she added.
She also suggested that creative, context-specific surveillance solutions are useful. For example, she said that they are interested in looking at intravenous fluids provided by drug sellers when people are feeling particularly sick. Finally, she noted an ongoing struggle to sustain the gains in improved water source access over time. She explained that reduced exposure creates new outbreak opportunities because it reduces the population-level risk of some of these diseases, which creates large pools of susceptible people. In this scenario, breaches and contamination in municipal water supplies and other water sources will likely cause even larger outbreaks than those seen now in places like Dhaka, where people are regularly exposed to those diseases.
EMERGING VECTOR-BORNE AND ZOONOTIC DISEASES IN BRAZILIAN SLUMS
Albert Ko, professor and chair of the Department of Epidemiology of Microbial Diseases at the Yale School of Public Health, discussed emerging vector-borne and zoonotic diseases in Brazilian slum communities. He described some of the challenges related to identifying drivers of transmission in urban slum environments and highlighted the contribution of gradients to disease risk, both between seemingly disparate communities in the urban macroenvironment as well as the slum microenvironment within communities.
Bottlenecks to Spillover Transmission
Providing another conceptual model that was translated into practice, Ko presented a model of bottlenecks to spillover transmission that facilitate or constrain transmission of different diseases between species (Plowright et al., 2017) (see Figure 4-3). He explained that the model traces the bottlenecks through the following path: reservoir distribution, reservoir density, pathogen prevalence, infection intensity, pathogen release, pathogen survival and spread in environmental reservoirs, human exposure, and finally within-host barriers. He said these bottlenecks pose challenges to identifying drivers of transmission and there are further challenges to identifying drivers of transmission in complex urban slum environments. For
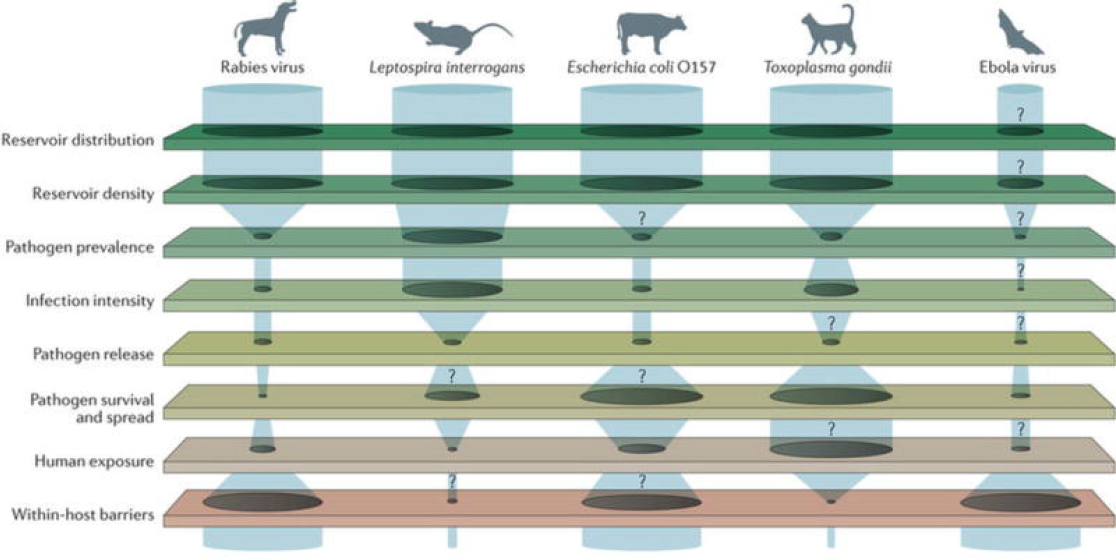
NOTES: The width of the gaps between barriers signifies the ease of spillover transmission depending on context. The question marks represent the knowledge gaps in specific pathogens’ points of transmission.
SOURCES: Ko presentation, December 12, 2017; Plowright et al., 2017. Reprinted by permission from Springer Customer Service Centre GmbH: Springer Nature. Nature Reviews Microbiology. Pathways to zoonotic spillover, Plowright, R. K., C. R. Parrish, H. McCallum, P. J. Hudson, A. I. Ko, A. L. Graham, and J. O. Lloyd-Smith. © 2017.
example, he said, slum environments are not homogeneous communities, but extremely heterogeneous communities. Although heterogeneity can be a challenge, he added, this variation can also provide insight into designing and implementing interventions.
Ko outlined some research challenges related to identifying drivers of transmission. He said that the standard methods for identifying reservoir distributions and reservoir densities are impractical, infeasible, and imprecise. He added that there is a lack of sound environmental sampling methods, particularly for pathogens, and poor linkage between environmental sampling data and human outcomes. He noted that human exposures are highly stochastic processes in urban slum communities, and that researchers must rely on imprecise proxies. Further challenges, according to Ko, are posed by the complex synergisms and the covariation at hand, such as defining the concept of poverty. He believed that a major challenge is that researchers have been limited to modeling static processes rather than dynamic processes because of the difficulty and intensity of the work; as a result, the models exclude dynamic processes of movement or migration including reservoirs, pathogens, and humans.
Release of Bottlenecks: Spillover of Environmentally Transmitted Pathogens
Ko described how the release of bottlenecks leads to the spillover of environmentally transmitted pathogens, including leptospirosis. He explored how ecological changes from urbanization and the growth of slums can contribute to spillover breakthrough via the release of bottlenecks, using the example of work that he and his colleagues have been carrying out in the city of Salvador, Brazil’s third largest city at 3 million people. He explained that in Salvador’s Pau da Lima periurban slum community, half of the population lives below the poverty line, and because of open sewers and other factors, rats (not humans) are the dominant, biologically successful mammal. He said that rats reside in burrows under earthen stairwells in close proximity to where people live (Cornwall, 2016).
New Epidemiological Pattern of Leptospirosis
Ko said that leptospirosis has emerged as a slum health problem in a new epidemiological pattern that is a consequence of ecological changes juxtaposed with demographic and social changes. He explained that leptospirosis was traditionally a rural-based zoonotic spirochetal disease in which the pathogen (the spirochete) is harbored in the renal tube and shed into the environment, where humans come into contact either directly with the reservoir or indirectly through the environment. He said that under this
new epidemiological pattern, which is evident in Salvador and many other major Brazilian urban centers, there are rainfall-associated leptospirosis epidemics that attack the same urban slum communities in a predictable pattern each year. Transmission of leptospirosis in Salvador is primarily rat-borne (primarily Rattus norvegicus) and due to a single serovar agent, he said. There are similar conditions of poverty and climate in communities throughout the developing world, he added. In Brazil alone, there are more than 12,000 cases, with high case fatality rates: more than 10 percent for Weil’s disease,4 and more than 50 percent for leptospirosis-associated severe pulmonary hemorrhagic syndrome (Ko et al., 1999; McBride et al., 2005).
The dynamics of rat reservoirs are key drivers of transmission, explained Ko. His team has carried out extensive rat-trapping surveys in Salvador, and has determined that the predominant mode of intraspecific transmission is environmentally mediated. He reported that carriage rates in the rat populations are more than 80 percent, and that each rat sheds approximately 1010 bacteria per day (Costa et al., 2015). He said that traditional capture–recapture methods do not work for Rattus norvegicus to estimate rat abundance, so they use an inexpensive tracking board method as a proxy for abundance (Hacker et al., 2016). Ceramic tiles painted with lampblack are set out overnight to capture rat paw prints, tail marks, and scratches, which are used toward densely sampling rat abundance. He reported that population abundance and pathogen shedding vary significantly across slum environments, yet the rat-related factors do not vary over season and time.
Rainfall as a Driver for Exposure to the Leptospiral Pathogen
Ko explained that they searched for potential temporal factors or drivers that cause seasonality of leptospirosis epidemics in humans, despite the rat-related factors themselves not appearing to be seasonal. They conducted a 10-year time series analysis of more than 2,000 leptospirosis hospitalizations to generate a fairly robust predictive model, he reported, which is being used in Salvador to identify outbreaks and allocate resources in real time. He said they found that lower temperatures may actually promote pathogen survival in the environment, and subsequently infection risks. They also found that even small amounts of rainfall—not only extreme events—also contribute to risk, he added, with increases in cases (including a lag time of 1 to 2 weeks that is roughly the incubation period for leptospirosis) indicating that exposures occur during or shortly after rainfall events in urban slum communities.
___________________
4 Weil’s disease occurs when leptospirosis infection in humans causes life-threatening complications, including jaundice, renal dysfunction, and hemorrhaging.
Ko said they conducted a study based on their finding that higher leptospiral pathogen loads are also associated with seasonal periods of heavy rainfall in urban slum communities (Casanovas-Massana et al., 2018). They used longitudinal sampling of open sewage and standing water and used quantitative polymerase chain reaction (qPCR) to detect genome equivalents of leptospirosis, he explained. He reported that high probabilities of quantitative PCR-positive samples and higher loads of leptospirosis were associated with the rainy season, and particularly associated the leptospirosis load or the probability of finding leptospirosis in sewage with the rainy season. He added that morning sampling during the rainy season detected higher loads than in the afternoon—probably because rats tend to be nocturnal, so there is probably more shedding over time in the evenings. The valley bottoms in the community also had higher loads of leptospirosis, he said. He suggested that, based on these findings, open sewers serve as transmission sources of leptospirosis in slum communities. According to Ko, the findings also illustrate the contribution of hydrology and the movement of the pathogen through water, sewage, and soil as potential drivers for leptospirosis during the rain seasons.
Potential Influences of the Environment and Social Gradients on Infection Transmission
Ko described a study that demonstrates the influence of the environment and social gradients on Leptospira infection. A long-term cohort study in Pau da Lima used tracking boards and surveys to identify risk factors associated with spillover infections or exposures, he said, and analysis found several significant covariates (Reis et al., 2008). The rat linear predictor (based on tracking board outputs) was significant, he reported, as was the cumulative rainfall experienced by the cohort participants. He said that greater distance to a public trash dump lowered the risk for infection, probably because trash is a food source for rats. He suggested that this finding is an example of a definable infrastructure deficiency that drives transmission. In the context of synergisms and covariation, he reported that the logarithm of household income per capita, which captures both environmental and social factors, was also significantly associated with risk. He said that the poorest land quality is at the bottom of valleys in the slum community, which is consistent with a larger pattern of vulnerable populations within slums residing in areas with the worst land quality.
Ko reported that the social gradient was captured in this study by socioeconomic status, which was associated with risk for leptospirosis. He explained that, for every $1 per capita household income per day, there is a decrease in risk of exposure to leptospirosis. He added that they also found a linear increase in risk among people until they reach 30 years of
age, after which it plateaus. He said that males had significantly increased risk, suggesting that adult young males tend to engage in risky behaviors that lead to exposures; for example, he added, after a rainfall people dig out the open sewers to create a barrier so that it does not overflow and flood their households in the next rainfall event.
Ko suggested that disparities in Zika and congenital Zika syndrome outcomes in slum versus nonslum communities in Pau da Lima illustrate the broad effect of inequities related to infectious disease transmission, both within slum communities and between slum and nonslum communities. He said that the Zika epidemic in Pau da Lima is an example of an epidemic that breaks the typical paradigm of focusing on disease rather than process. He reported that seroincidence surveys indicate that the social gradient is the opposite of those for leptospirosis—that is, the much more marginalized areas were protected rather than the wealthier areas. According to Ko, this suggests that movement plays an important role in Zika transmission. At the epicenter of the Zika epidemic, he said, they carried out hospital-based surveillance for microcephaly. He reported on unpublished data that revealed at a private hospital not supported by the national health plan the prevalence of microcephaly among all newborns was 1.2 percent; at a public hospital, the rate was about 10 times higher at 12.0 percent. He suggested that much of this was driven by exposure: in the public hospital, 63.1 percent of mothers were seropositive compared to 18.8 percent of mothers from wealthier communities in the private hospital. He cautioned that, beyond these figures, the brunt of the Zika epidemic—caring for the children with neurodevelopmental problems—will be borne by the public health system.
Community-Driven Initiative for Social Equity and Urban Leptospirosis Prevention
Ko emphasized that the transmission of infectious diseases in the slums is a complex interaction of poverty, geography, and climate, but he described opportunities to identify defined structural determinants, both environmental and social, that could be targeted for intervention. Addressing open sewers and rainwater drainage are two such opportunities, he said. He noted that addressing the issue of social gradient to risk is more complex, but strategies might include a better understanding of the psychosocial factors that place young males at risk for leptospirosis, sexually transmitted infections, violence, and drug use in poor urban slum communities. He described the Fiocruz-Cornell Global Infectious Disease Training Program, a community-driven initiative for social equity and urban leptospirosis prevention that has been under way over the last 20 years in collaboration with the government of Brazil. It aims to mount multilevel interventions
based on forecasting, health education to address high-risk behaviors, and targeted rodent control. This initiative reported a fourfold decrease in leptospirosis during the program. Social participation and community buy-in are keys to the success of such initiatives, he said. For example, Pau da Lima community leaders convinced the government to invest $36 million to build closed sewage systems on the periphery of the community.
TUBERCULOSIS TRANSMISSION IN CAPE TOWN, SOUTH AFRICA
Robin Wood, chief executive officer of the Desmond Tutu HIV Centre and Foundation at the University of Cape Town, focused his presentation on the transmission of TB in Cape Town, South Africa, where the country is estimated to have the highest burden of TB in the world. The city of Cape Town alone has more TB case notifications per year (around 26,000) than Canada, France, United Kingdom, and the United States combined (WHO, 2016). He said that, compared to the age-adjusted TB rates in New York City over the past 100 years (which have dropped overall, especially among young people), the same rates in Cape Town have changed very little. He reported that today there is as much TB in children and more TB among young adults in South Africa and suggested that the HIV epidemic is a contributing factor (Hermans et al., 2015).
Wood noted that, although TB was made a notifiable disease in Cape Town in 1904—a decade before it became notifiable in the United Kingdom—the massive TB burden persists despite every advance in TB control measures having been implemented in Cape Town since the beginning of the 20th century. According to cross-sectional infection rates for proportions in different age groups in Cape Town, said Wood, 20 percent of the population is infected by the time they enter school at 5 years of age, 50 percent are infected by age 14, and by adulthood, most people are either infected or have active TB disease (Wood et al., 2010).
Airborne Component of Mycobacterium tuberculosis Life Cycle
Wood explained that the Mycobacterium tuberculosis (MTB) life cycle has an airborne component. He said that the Wells-Riley equation, developed in the 1950s, can be used to predict the number of new cases of airborne infections in a steady-state, single-transmission environment (Wells, 1955). He added that the equation can be generalized to take into account multiple transmission factors and model the transmission of MTB within a given population. The modified version of the Wells-Riley equation can be used to estimate the annual risk of TB infection, he said, which is determined by the number of inhaled TB infectious quanta per year.
He highlighted three parts of the modified equation. The first part is the
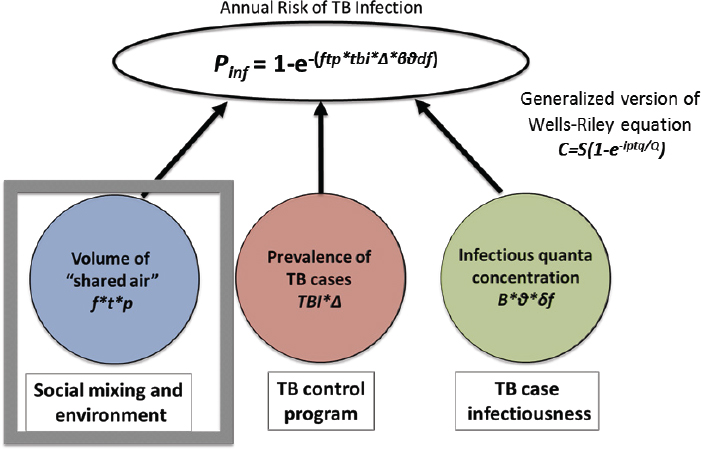
NOTES: The generalized Wells-Riley equation C = S(1-e-iptq/Q) calculates number of new infected cases; i = number of infectious people; p = ventilation rate of susceptible people; q = quantum of infection; Q = constant rate of ventilation in an indoor environment; S = number of susceptible people; t = time; TB = tuberculosis.
SOURCE: Wood presentation, December 12, 2017.
volume of air breathed from others; this is relevant to an airborne disease like TB, he said, because the volume of air exchanged between people is likely a key factor that is driven by social mixing and the environment. The second part is the population prevalence of infectious TB cases, he said, which is relevant because TB control programs try to decrease prevalence by putting people onto effective therapy. The third part—the infectiousness of the range of TB cases—is also known as the infectious quanta concentration, said Wood; he noted that there is ongoing work to better understand this component of TB transmission (see Figure 4-4).
Modeling the Risk of Airborne Infectious Disease Using Exhaled Air
Wood focused more closely on the component of the modified Wells-Riley equation that represents social mixing and the environment. He described how the equation can be used to model the risk of airborne disease transmission by using measurements of exhaled air. Carbon diox-
ide is often used to measure ventilation, he noted, because a single person produces about 8 liters (40,000 parts per million) of carbon dioxide each minute. If the carbon dioxide level in an indoor room increases to 4,000 parts per million, he explained, then around 10 percent of every breath taken by a person in that room has been breathed out by somebody else. He added that, by using measurements of room volume, ventilation, and carbon dioxide production rate, it is possible to calculate the total amount of air that was exchanged in a room. It is also possible to calculate how long it will take for a room to reach steady-state equilibrium of carbon dioxide concentration, he said; the final steady state is defined as the carbon dioxide production of everyone in the room divided by the per-person ventilation. He noted that it takes longer to reach equilibrium in a large room and less time in a room with a greater amount of ventilation (Issarow et al., 2015).
Using Continuous Personal Carbon Dioxide Monitors to Calculate Shared Air
Wood explained that carbon dioxide disseminates rapidly, and he and his colleagues believe that carbon dioxide behaves in a similar way to the small particles (1 to 2 microns in size) that are thought to be transmitters of mycobacteria and TB. He said his team created a small device for people to wear that measures carbon dioxide levels continuously and enables location tracking, which allows researchers to calculate the amount of air exchanged between individuals in a variety of environments. He described a set of studies that used these continuous personal carbon dioxide monitors to calculate the volume of shared air in different settings and to determine if those settings reached carbon dioxide equilibrium.
Wood reported that in one study the device was used by an adolescent girl living in a relatively dense community (25,000 people in one square kilometer) as she traveled to school by taxi and public transportation and spent her day in school (Richardson et al., 2014). The researchers found that the carbon dioxide levels were dramatically different in various classrooms within the school in which she spent time. In two of those classrooms in particular, he said, the rates of rebreathed air peaked at around 0.35 to 0.375 liters per minute by the end of the classroom periods. In these two classrooms, the carbon dioxide concentrations in the rooms did not reach steady-state equilibrium during the class periods she attended, which indicates that the ventilation rates were very low. He noted that those two classrooms only had windows on one side, while the other rooms had cross flow from windows on both sides.
In another study, Wood said, the devices were used by a large group of adolescents in the township of Masiphumelele. He reported that the results showed that most of the rebreathed air was at home and in school; there
was also a difference between the liters of rebreathed air in summer and winter (Wood et al., 2014). He said that in the winter, the adolescents in the study were rebreathing between 150 and 300 liters per day on average, mainly at school; in the summer, the students averaged between around 50 and 90 liters of rebreathed air per day. For reference, he estimated that most people in attendance at the workshop rebreathe around 25 liters per day.
Wood described a subsequent study that placed the carbon dioxide measurement devices throughout the township. He said that this allowed the investigators to compare concentrations of carbon dioxide with the locations of the adolescents, the locations of people who had just been diagnosed with TB, and the locations of people who had completed therapy for acute sickness of TB (Patterson et al., 2017). Wood reported that the locations of those three groups did not seem to overlap, suggesting that the people identified as having TB did not appear to be the same people who were transmitting the infection to adolescents. He said that a member of his research team created a model to integrate social contact and environmental data to evaluate TB transmission in the township (Andrews et al., 2014). He explained that, for any given age group, the model calculates the social mixing and carbon dioxide data to estimate where people are becoming infected. The results showed that between 10 and 20 percent of transmission was taking place in households, but the model estimated that among young people ages 15 to 19, more than 50 percent of transmission was taking place in schools. He attributed this to the associative nature of households—where a person meets the same people every day—versus the more generalized mixing that occurs in public spaces.
Ventilation in School Classrooms
Spurred by the finding that a high level of transmission was taking place in schools in the township of Masiphumelele, Wood said that he investigated ventilation in school classrooms. He found a study from 1924 that measured carbon dioxide levels in schools in New York City and found that they rarely exceeded 1,000 parts per million (Simpson, 1924). Wood surmised that one of the reasons the carbon dioxide concentrations were maintained at safe levels—even though the rooms appear small and crowded by modern standards—is that the classrooms had high windows with ventilation driven by temperature gradients rather than the current reliance on cross flow from windows on two sides of a room.
To illustrate the conditions of classroom ventilation in modern schools, Wood used a figure adapted from a 2008 study that plotted the correlation between mean indoor carbon dioxide concentrations against airflow rate per person in 62 naturally ventilated classrooms in Europe and North America (Santamouris et al., 2008) (see Figure 4-5). Wood noted that the
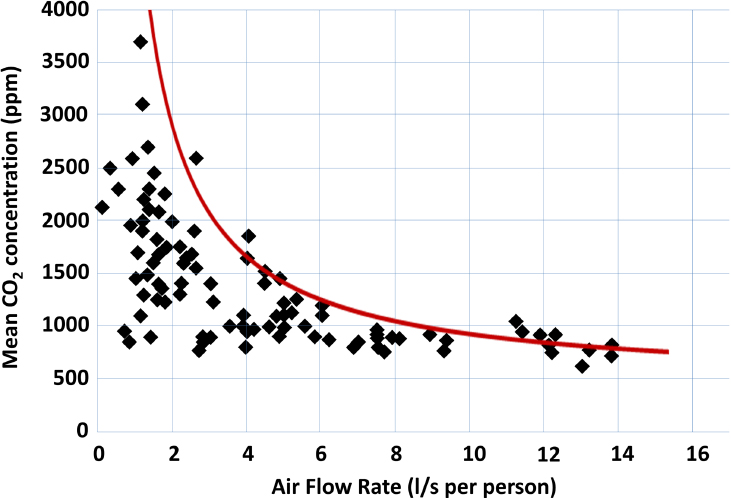
NOTES: The red line represents idealized values of ventilation having reached steady-state values of carbon dioxide concentrations; x-axis is the ventilation rate per occupant; y-axis is the measured concentration of carbon dioxide (parts per million); CO2 = carbon dioxide; l/s = liters per second; ppm = parts per million.
SOURCES: Wood presentation, December 12, 2017; Richardson et al., 2014.
idealized steady-state ventilation was rarely achieved in the classrooms surveyed in the study, as indicated by the red line he overlaid on Figure 4-5. He explained that equilibrium is achieved rapidly when airflow is high, but equilibrium is not achieved when airflow is low. He also noted that the carbon dioxide levels in the classrooms were high, reaching nearly 4,000 parts per million. Therefore, he said, people are being forced to rebreathe around 300 liters of air during an 8-hour school day. He noted that international recommendations for carbon dioxide levels in schools tend to advise a median peak carbon dioxide concentration of around 1,000 parts per million (Richardson et al., 2014).
Wood concluded by arguing that air volumes exchanged are major drivers of TB, especially in South Africa, and that rebreathing is facilitated by social mixing and environmental conditions. For example, he said that an ideal environment for TB would be an overcrowded prison where people
spend 23 hours per day with no ventilation and breathe between 1,000 and 2,000 liters of other people’s air per day. Wood maintained that the main role of TB control programs should be to address the prevalence of TB transmitters in the population, but he noted that it can be difficult to find the transmitters who are infecting the groups of people with the highest infection rates. Wood also suggested examining the infectiousness of TB transmitters. He explained that when social circumstances are relatively good, and people are not rebreathing large amounts of air, TB outbreaks can only be caused by superspreaders and the outbreaks do not develop into endemic disease, because the next generation will not be infectious. When there is endemic TB, he warned, the entire spectrum of MTB infectiousness can transmit disease.
DISCUSSION
Jay Siegel, recently retired chief biotechnology officer and head of scientific strategy and policy at Johnson & Johnson, noted that in Bethesda, Maryland, there is a county building code that does not require air exchange, but actually caps air exchange. He explained that when a new home is built, sealed door and air pressure tests are required to ensure that the home is airtight to minimize gas exchange to attempt to decrease energy consumption. He remarked that such construction codes have led to an increase in buildings with sick people and where carpeting or insulation are degassing volatile organic compounds. He asked Wood if such building codes are in place in South Africa or elsewhere and whether those codes are increasing the infectious disease risk.
Wood replied that in the United States there have been some extraordinary contact numbers of children in schools. To illustrate, he described a respiratory virus epidemic in Colorado where hundreds of people were infected by one person, which suggests a superspreader story, he said. He suggested that part of the problem is that architects have not been provided with the medical and disease-related reasons for not decreasing the ventilation per current trends. The building codes in South Africa, he added, require that a portion of the floor area must be open to the outdoors. He suggested that disease-related factors need to be taken into consideration and architects need to be advised about how design is important for health. Wood provided another example of the Pollsmoor Prison in Cape Town, South Africa, where hundreds of people are housed in a single room with no ventilation—that room in the prison is subject to exactly the same building code as a domestic bedroom in the same area, he said. Wood suggested that TB control programs should be tailored to social circumstances to achieve their aim of decreasing TB prevalence. If there are poor ventilation systems
in places like prisons, he said, then the TB control program needs to be able to identify cases quickly to prevent rapid spread.
He elaborated that passive case-finding strategies, for example, are not suitable for groups of people with TB-HIV coinfection with rapidly progressing TB or for TB patients who are living in poor circumstances. He suggested that more active case-finding strategies should be used to look for cases that occur in those types of circumstances. He said that this was done in Cape Town in the 1970s during the lowest point of the TB epidemic, when millions of chest X-rays were carried out. He added that the TB control program was ordered to stop the campaign because it was no longer cost-effective according to global guidelines, even though it was effective for the specific context.
David Nabarro, advisor for health systems and sustainability at 4SD, suggested that the superspreader issue should be considered in every effort against infectious diseases, be it cholera, influenza, or TB. He suggested focusing on the significance of superspreaders as key individuals infected with bacteria, viruses, or other microorganisms who transmit them to an unusually large number of other people. Wood replied that superspreaders are important and disease specific; for example, he explained that in measuring the infectivity of TB individuals and measuring their production rate of appropriately sized particles, superspreaders have only been found historically because the sensitivities in systems for finding them are low. He suggested that the problem of superspreaders needs to be defined properly and disease specifically in addition to having appropriate, sensitive systems.
Wood continued that part of the success of the TB control achieved in New York was because of the spectrum of people—many people with low infectivity and a few people with high infectivity—which allowed efforts to focus on those few high-infectivity cases. In Cape Town, he explained, there is a situation of endemic TB spread in which everybody is transmitting rather than a single superspreader, because there are more than 500 TB strains in the community. Gurley noted that it is difficult to identify superspreaders for cholera, because it is related to both host infectiousness and social context.
Peter Daszak, president of EcoHealth Alliance, asked Gurley about current interventions for cholera and if new interventions will be informed by knowing more about where cases start. Gurley replied that the long-term goal of getting people safe water to drink should be pursued doggedly or progress will never be made. She noted that there is now a good vaccine for cholera, but it is not used widely enough; she explained that vaccine strategies are often based on administrative units rather than high-risk areas and populations, and that many of the current intervention strategies and systems are not flexible enough to take risk into account. If more flexibility can be cultivated, she suggested, then interventions like vaccines may help
reduce hot spots of risk by addressing them at early stages and thus reducing the risk for everyone else. Nabarro asked Gurley to elaborate on the issue of water versus sanitation for cholera intervention.
Gurley replied that cholera is often spread through contaminated hands within a household, and the first person infected in a given household was probably infected by water. She said that household spread is also water related because good access to water is needed for hand washing. Sanitation is part of good infrastructure, she said, but ensuring clean water would go a long way. Nabarro responded that the delay in globally advancing sanitation is distressing and suggested that water is often put ahead of sanitation in public health. Sanitation is an integral issue in the built environment, he said, and suggested pushing for better sanitation that is not necessarily water based, such as the separation of feces, particularly children’s feces and particularly during the rainy seasons.
Espinal noted that the internationally cited death toll from EVD is approximately 11,000 people, but the conclusion of one report was that the true number of people who died will never be known because the West Point slum was so complicated to deal with, and the bodies were being disposed of without being counted. He also noted that EVD was quickly contained in Nigeria, including Lagos, a huge and poor city. He asked if there are lessons to be gained regarding slums and big cities by comparing the control of EVD in Nigeria versus Liberia. Mahoney replied that there were many occult burials on an island outside of West Point. He said that the case of West Point was striking because EVD did not spread there in expected geographic ways for an infectious disease: the outbreaks were geographically tight, with a cluster around households in West Point, beyond which it did not spread much. He added that, unlike the way that cholera spreads, for example, EVD exposure was family related. Mahoney said that in the example of Nigeria they were lucky in having the right people at the right time to help mentor clinical staff, although he noted that Nigeria did experience critical issues, including a doctor strike. Mahoney said that, at one point, a contact showed up in another city, and the staff from that city called Lagos and said they had sufficient personal protective equipment and were going to see the patient. Mahoney said that they were told not to see the patient, to lock the door, and to wait for people who were experienced in managing an EVD patient; the patient was retrieved and brought back to Lagos via an 8-hour taxi ride.
He reiterated that the people managing Ebola patients need to be mentored by those with experience and said that Nigeria was fortunate to have experienced people as part of the effort. Mahoney added that Nigeria’s Field Epidemiology Training Program did a great job contact tracing, that the Polio Incident Management Team was brought in to help manage the outbreak response, and that the response had a strong infrastructure of
data-driven management. Mahoney outlined some lessons learned in the Nigerian response. He said that there was a program to trace EVD contact on a daily basis, but some contacts would present with the disease after several days without contact and claim that they had forgotten they were being traced; in other cases, people who were supposed to take temperatures of contacts daily were not actually doing so. From this they learned that they needed to directly observe temperature monitoring of contacts, he said.
Christopher Braden, deputy director of the National Center for Emerging and Zoonotic Infectious Diseases, CDC, asked if new technologies will enable more sensitive types of environmental sampling. Ko replied that this is a critical research need and technology is improving, but there are several barriers. He said many of the technological advances are in detection rather than processing—for example, that the volume of the infectious dose is small for toxoplasmosis and cryptosporidiosis, but processing requires 20 to 40 liters of water. Ko said that the sampling design is also challenging: exposures are highly probabilistic for highly stochastic processes, as with leptospirosis. He added that further issues are related to obtaining the sample density needed to get a signal as well as how to get the signal above the noise in a spatial grid.
Wood reported that environmental sampling is being done, but a problem is that large droplets fall out of the air and leave evidence of TB on floors and walls. However, he said that the relevance of this type of sampling to transmission is unknown, although signals can be detected. He noted that biodefense machines are used to sample large volumes of air (by cubic meter per minute) in community and health settings, and PCR has shown positive signals. He suggested that this is useful for children in classrooms, compared to other settings such as churches, because the identities of the schoolchildren in the classroom are known and they can be resampled later. Ko noted that this type of environmental pathogen sampling is somewhat locked into risk assessment, rather than linking those environmental signals and risks to human outcomes. Mahoney added that environmental sampling in work on polio has advanced far enough to track chains of transmission due to genetic clades, although he noted that this is probably unique to that virus.
Christopher Dye, director of strategy, policy, and information at the Office of the Director-General of WHO, remarked that John Snow fixed the water supply but did not recommend active surveillance; he noted that water and sanitation sectors tend to be confined to the health domain and may be reluctant to get into active surveillance. He asked if the inclusion of safe water and sanitation in the Sustainable Development Goals (SDGs) framework is an advance over the MDG framework, because the word “safe” ties health to water and sanitation in a way that was not present in
the MDG era.5 Gurley replied that John Snow may not have fixed the water supply, but he cut it off for a time while the problem was addressed. She agreed that the emphasis on safety is important and suggested that checking the veracity of sources should be incorporated going forward: that is, rather than saying “This person told me this is their water source; therefore their water is safe,” better ways are needed to measure that safety. She noted that surveillance for cholera is one way to implement that, but there are many other potential ways.
Espinal concluded the discussion by remarking that the presentations underscored the importance of the International Health Regulations and the Global Health Security Agenda in ensuring that countries implement essential public health functions to contain outbreaks and emergencies. The presentations also highlighted the need for more support for research about the drivers of infectious disease, he said. He suggested there are other systemic issues at hand, noting that rainfall, climate change, and housing are related to the SDGs and that progress might be made by addressing them.
___________________
5 Since the MDGs, the WHO-UNICEF Joint Monitoring Programme for Water Supply, Sanitation, and Hygiene has introduced more categories for safe water and sanitation facilities: limited, basic, or safely managed.


























