
1
Introduction
The United States has approximately 21 percent of the world’s coal resources (EIA, 2014). Despite recent declines in the number of active coal mines in the United States and the miners they employ, thermal coal, which is used to generate electricity from steam turbines, will continue to play an important role as an energy source for the foreseeable future. Coal is projected to produce 29 percent of electricity worldwide and 17 percent of U.S. electricity through 2050 (EIA, 2017c). Additionally, metallurgical coal used in steel production remains an important commodity produced in the United States. Coal is currently mined in 25 states. Production reached a high of 1,172 million tons in 2008 and declined to 728 million tons in 2016 (NMA, 2017a).
The two major types of coal extraction are surface mining and underground mining. In surface mining, soil and rock over the coal seam are removed to expose the coal, which is fragmented and removed. Underground mining involves accessing a coal seam by suitable openings from the surface, called shafts, slopes, or drifts. Surface mining’s share of coal production in the United States was about 66 percent in 2015 (EIA, 2012; NMA, 2017b). In absolute terms, surface coal production in 2015 was 589 million tons, representing a more than a fourfold increase from 139 million tons in 1950 (EIA, 2012; NMA, 2017b). In recent years, there has been an overall decline in coal production in the surface and underground sectors.
The trends toward increased surface mining, increased production and productivity from new technology, consolidation of mining companies, closure of smaller operations, and increased use of natural gas for electricity generation have all contributed over the years to a continuous decline in the number of underground mines and the number of miners employed in those mines. For the 12 months ending January 2010, there were 424 active underground coal mines and 47,004 active coal mine workers1 in those mines (including 6,685 independent contractors at 232 active mines, excluding office employees) (MSHA, 2014). (See Appendix E for additional details on coal mining in the United States.)
Following passage of the Coal Mine Health and Safety Act in 1969, improved ventilation and dust abatement strategies led to substantial declines in disease prevalence among U.S. coal miners. However, since around 2000, a resurgence in disease prevalence and severity (Antao et al., 2005; Suarthana et al., 2011), particularly in central Appalachia, has prompted renewed focus on the need for more effective exposure control in underground coal mines and is the underpinning for this report. This chapter provides a general overview of underground coal mining processes, inhalational exposures in coal mines, the spectrum of lung diseases related to respirable coal mine dust (RCMD) exposures, historical trends in the prevalence and severity of those diseases, and changes in U.S. coal mine dust regulations that are important in informing exposure control strategies aimed at disease prevention. This chapter lays a foundation for the committee’s statement of task addressed in this report.
___________________
1 The term “coal mine worker” often includes active miners as well as former (retired, disabled, or otherwise employed) coal miners; those who have worked for coal mine operators or their contractors; and those who have worked in various coal mine job duties.
COMMITTEE’S STATEMENT OF TASK
In response to a congressional request in the fiscal 2016 Congressional Appropriations (Public Law 114-113),2 the National Academies of Sciences, Engineering, and Medicine formed an ad hoc committee to assess monitoring and sampling approaches for informing underground coal mine operators’ decision making regarding the control of RCMD and mine worker exposure. (The committee’s formal statement of task is presented in Appendix A.) The committee’s task includes these components:
- Compare the monitoring technologies and sampling protocols (including sampling frequency) currently used or required in the United States, and in similarly industrialized countries, for the control of RCMD exposure in underground coal mines.
- Assess the effects of rock dust mixtures and their application for controlling explosions in mines, as required by current U.S. regulations, on RCMD measurements.
- Assess the efficacy of current monitoring technologies and sampling approaches and develop science-based conclusions regarding optimal monitoring and sampling strategies to aid mine operators’ decision making related to reducing RCMD exposure to miners in underground coal mines.
The committee was also asked to identify important research gaps regarding monitoring and sampling protocols for controlling miners’ RCMD exposures. The committee was specifically asked not to recommend changes to the requirements of the Mine Safety and Health Administration’s (MSHA’s) final rule, Lowering Miners’ Exposure to Respirable Coal Mine Dust, Including Continuous Personal Dust Monitors (79 Fed. Reg. 24,814 [2014]).3,4 The development of those requirements involves considerations beyond the scientific and technical focus of this report.
RESPIRABLE COAL MINE DUST: CONSTITUENTS AND SOURCES
RCMD comprises the size fraction of airborne particles in underground mines that can be inhaled by miners and deposited in the distal airways and lung gas-exchange region (WHO, 1999). The 2014 dust rule states, “Any respirable dust in the mine atmosphere is considered respirable coal mine dust to which miners are exposed and, when measured, is counted for determining compliance with the respirable dust standard” (79 Fed. Reg. 24,866). For regulatory purposes, RCMD is defined as “that dust collected with a sampling device approved by the Secretary (of Labor) and the Secretary of HHS in accordance with (30 CFR) part 74 (30 CFR 74).” The current regulation requires monitoring of RCMD mass concentrations (mg/m3) and the respirable quartz concentration in the RCMD. Aside from quartz content, there is no regulatory requirement related to the composition of RCMD mass, how the composition varies, and the sources of the constituents.
The constituents of RCMD are complex and heterogeneous and depend on mine geology and mining methods that generate the dust. There are three major sources of airborne dust particles in coal mines: particles entering the mine with the intake air; dust generated from cutting, drilling, or crushing coal and rock strata during the mining process; and application of rock dust products. Dust particles generated from abrasion of cutting or drill bits or other tools themselves may also be present in coal mines. Additionally, diesel exhaust represents another major source of airborne particles in many mines.
___________________
2 See Division H: Departments of Labor, Health and Human Services, and Education, and Related Agencies Appropriations Act, 2016.
3 The rule affects 30 Code of Federal Regulations (CFR) 70, 71, 72, 75, and 90.
4 In this report, the final rule is referred to as the 2014 dust rule.
Forms of coal range from soft (lignite) to hard coals (bituminous and anthracite) with higher carbon content. Anthracite, historically mined in Pennsylvania, has the highest carbon content (86 to 97 percent) and now accounts for only around 8 percent of coal production in the United States and 0.04 percent of the nation’s underground mining (EIA, 2017a,b). Bituminous and subbituminous coal (35 to 45 percent carbon) accounts for most coal production in the United States and 99 percent of underground mining production, the majority from mines west of the Mississippi (EIA, 2017a,b). Lignite (25 to 34 percent carbon) is mined mainly in Texas and North Dakota and constitutes 10 percent of U.S. coal production (EIA, 2017b). RCMD in underground coal mines is estimated to contain 40 to 95 percent coal (Walton et al., 1977; NIOSH, 1995).
In addition to coal, RCMD may contain crystalline silica5 and silicates, diesel exhaust particles, rock dust products (mainly calcium carbonate) used for explosion mitigation (see Chapter 2), metals, and other organic compounds. Other possible components of the coal mine atmosphere include gases, such as methane, radon, and carbon monoxide; chemicals, such as isocyanates used in roof bolting glues; microbial bioaerosols in water sprays used for dust suppression; and particles not otherwise specified (sometimes referred to as nuisance dust for which constituent-specific exposure limits are not specified).
Several studies have investigated specific characteristics that may be important in understanding health risks, such as bioavailable iron content of coal (Huang et al., 2005) and rare earth element concentration (Schatzel and Stewart, 2012), but few have considered the whole composition of RCMD. A recent study of RCMD particle characteristics analyzed 210 samples collected from stationary locations (that is, area samples) in eight underground coal mines from three regions in Appalachia (Johann-Essex et al., 2017). Overall, percentages of coal were relatively low (that is, less than 40 percent by number count), and statistically significant differences (95 percent confidence level) were observed between particle distributions between mine regions. Higher percentages of aluminosilicates and quartz6 were found in the samples from central Appalachia compared to those from northern Appalachia, which contained higher percentages of carbonate from rock dusting (that is, the application of rock dust products). Significant differences in particle mineralogy and size were also found between distinct sampling locations. For instance, samples collected near active cutting or drilling operations (for example, by roof bolters, continuous miners, or longwall shearers) and in the return airways had smaller and more elongated dust particles than those in intake airways or near the feeder breaker. Such findings highlight the variability in particle mineralogy, size, and shape that can exist in mine environments, and may be important in understanding health risks and devising exposure controls (Sellaro and Sarver, 2014). While diesel exhaust is not directly monitored in coal mine atmospheres (due to analytical interference that may be posed by coal particles), it is well established that diesel particulates tend to occur in the sub-micron range (about 10-1,000 nm); and represent a complex mixture of components, which tend to be dominated by elemental and organic carbon, with minor fractions of sorbed volatiles and metals (Kittelson, 1997).
OVERVIEW OF UNDERGROUND COAL MINING METHODS AND JOB DUTIES
The variability in RCMD composition and concentration is linked to coal mining processes and mine locations. To mine coal economically, mining companies seek to identify a sufficiently large seam of coal for extraction, either underground or at the surface. Underground coal mining, which occurs in an enclosed space, is associated with generally higher dust concentrations than
___________________
5 Crystalline silica is a collective term that refers to quartz, cristobalite, tridymite, and several other rare silica minerals. All of the crystalline silica minerals have the same chemical composition but have different crystal structures and are thus termed polymorphs.
6 The 2014 dust rule defines quartz as crystalline silicon dioxide (SiO2) not chemically combined with other substances and having a distinctive physical structure. Quartz is the most common form of crystalline silica.
surface mining. Geological features in underground mines, such as faults and seam splits containing noncoal layers together with the coal, might require cutting through rock to extract the coal.
Mining methods are important determinants of RCMD exposure. The two major methods of underground mining are the room-and-pillar method and the longwall method. In room-and-pillar mining, the roof is supported by pillars of coal and roof bolts are used to prevent rock falls from the roof strata. A continuous miner (a machine with a rotating cutter on a boom) cuts the coal. Longwall methods permit higher productivity, which creates the potential for greater dust generation. In longwall mining, a machine removes a strip of coal from the coal face, while shields support the roof. As the face advances, the mined out area is allowed to collapse. Details of underground mining methods are presented in Appendix F.
Miners’ job titles and duties are associated with different RCMD exposures. Miners working in proximity to the coal face, where a continuous miner or longwall machines liberate coal from surrounding rock, are likely to have the highest exposures (Colinet et al., 2010). As discussed below, for regulatory compliance purposes in the United States, personal monitors are required for miners working in designated occupations considered to have the highest RCMD exposures. Those occupations include the continuous miner operator, roof bolter operators, headgate and tailgate shearer operators, and jack setters (shield operators). In addition, RCMD samples are required to be collected from specific areas in the mine.
While RCMD exposures in surface mines are generally lower than those underground, the full spectrum of lung diseases related to RCMD exposure have been observed in surface miners (CDC, 2012; Halldin et al., 2015b). Surface mine workers involved in drilling have higher respirable quartz exposures (Amandus and Piacitelli, 1987; Piacitelli et al., 1990).
TOXICITY AND DISEASES ASSOCIATED WITH COAL MINE DUST EXPOSURE
There is a clear relationship between duration and intensity of RCMD exposure and risk of lung disease associated with coal mining. The most widely recognized respiratory disease from coal mining is coal workers’ pneumoconiosis (CWP). CWP can progress even after exposure removal (Halldin et al., 2015a), and risk for progression is related to concentration and duration of RCMD exposure and probably also to particular constituents of the dust. Estimated cumulative dust exposure has been found to be associated with higher prevalence of CWP and coal rank7 has shown some correlation with higher CWP disease prevalence for high rank coal (Attfield and Seixas, 1995).
Lung cellular damage and inflammation from exposure to RCMD results in injury that can lead to chronic lung disease, with disease progression likely a result of sustained inflammatory effects of retained mineral dust. Mechanisms of lung injury include (1) direct lung damage due to oxidant generation by RCMD particles and (2) stimulation of alveolar macrophages and lung epithelial cells by RCMD, with generation of oxidants, release of inflammatory mediators, and stimulation of fibrogenic factors (Lapp and Castranova, 1993; Castranova and Vallyathan, 2000). Exposure to high concentrations of respirable silica is associated with greater lung injury (Castronova, 2000). Additionally, researchers have examined potential biological pathways to explain higher CWP prevalence in workers from mining regions with higher concentrations of bioavailable iron in coal (Huang et al., 2002). A systematic review of scientific literature on occupational exposure to coal dust and the risk of interstitial lung diseases found evidence to suggest an independent effect of the nonquartz part of coal on disease development and progression (Beer et al., 2017).
The spectrum of coal mine dust lung diseases includes simple and complicated CWP; silicosis and mixed dust pneumoconiosis; dust-related diffuse fibrosis; and chronic obstructive pulmonary diseases, including emphysema and chronic bronchitis (Petsonk et al., 2013; Perret et al.,
___________________
7 Coal rank is a classification of coal based on fixed carbon, volatile matter, and heating value. It indicates the progressive geological alteration (coalification) from lignite to anthracite.
2017). All of those are diseases of long latency; that is, it typically takes at least 10 years (and often 20 to 30 years) before disease becomes clinically apparent. Effective diagnosis of a coal mine dust lung disease relies on a comprehensive occupational history; medical and social histories; findings on chest imaging, lung function testing, and arterial blood gas testing at rest and with exercise; and consideration of other diseases that may mimic these conditions.
Historically, the diagnosis of CWP relied mainly on findings from the chest radiograph. There are two main radiographic categories of classical CWP: simple and complicated CWP. Simple CWP is defined by the presence of opacities less than 10 mm in the longest dimension. Complicated CWP (also called progressive massive fibrosis [PMF]) is defined by the presence of radiographic opacities larger than 10 mm in size (Figure 1-1). The chest radiographic findings in simple and complicated silicosis are similar to and often indistinguishable from those of CWP, with a radiographic diagnosis of CWP based on the occupational history of exposure to RCMD, whereas a radiographic diagnosis of silicosis is based on the history of exposure to respirable silica in noncoal mining environments (for example, in metal/nonmetal mining, stone/sand/gravel mining, sandblasting, stone cutting industries, and others). Dust-related diffuse fibrosis is characterized on chest radiograph by irregular rather than rounded opacities and on lung tissue analysis by findings of bridging fibrosis connecting macular, nodular, or progressive massive fibrosis lesions, often with pigmented interlobular septal thickening (McConnonchie et al., 1988).
Obstructive lung diseases including emphysema and chronic bronchitis can occur in miners with and without radiographic pneumoconiosis, and emphysema can occur in nonsmoking coal miners (Attfield, 1985; Attfield and Hodous, 1992; Seixas et al., 1992). Emphysema severity in miners is related to cumulative RCMD exposure and lung dust content (Kuempel et al., 2009). Notably, coal mine dust injures the airways in an additive way with tobacco smoke exposure, and contributions from RCMD exposure and cigarette smoking are similar in predicting emphysema severity (Attfield and Hodous, 1992; Kuempel et al., 2009).
No specific medical treatment is effective in reversing coal mine dust lung diseases or in controlling disease progression. Consequently, efforts to minimize RCMD exposure along with medical surveillance for early disease detection and removal from exposure are the mainstays in protecting a miner’s health.
A number of Class I human carcinogens, including silica, radon, and diesel exhaust, are found in coal mine environments, and excess lung cancer mortality among coal miners (especially those exposed to respirable crystalline silica) remains a concern (Attfield and Keumpel, 2008; Miller and MacCalman, 2010; Blackley et al., 2016, 2018). In addition, exposure to RCMD, mainly particles less than 2.5 µm in aerodynamic diameter, may increase miners’ risk for cardiovascular diseases, particularly in combination with other occupational cardiovascular risk factors such as noise, vibration, and shift work (Enterline, 1972; Weiner et al., 2007; Eller et al., 2009; Skogstad et al., 2016; Eriksoon et al., 2018).
RECENT TRENDS IN COAL MINE DUST LUNG DISEASES AND IN MINING
Trends in Disease Epidemiology
The National Institute for Occupational Safety and Health (NIOSH) Coal Workers’ Health Surveillance Program was established by the Federal Coal Mine Health and Safety Act of 1969 to prevent early CWP from progressing to disabling disease. Since 1970, NIOSH has administered this program for eligible miners. Mandatory chest radiograph examinations must be provided by a NIOSH-approved facility for each miner at the beginning of their coal mine employment and within 3 years after the initial examination (42 CFR 37). Voluntary examinations must be offered at least every 5 years. Under the 2014 Coal Workers’ Health Surveillance Program, a coal miner or contractor working at an underground or surface mine receives a free chest x-ray, lung function test, and health assessment and symptom questionnaire.

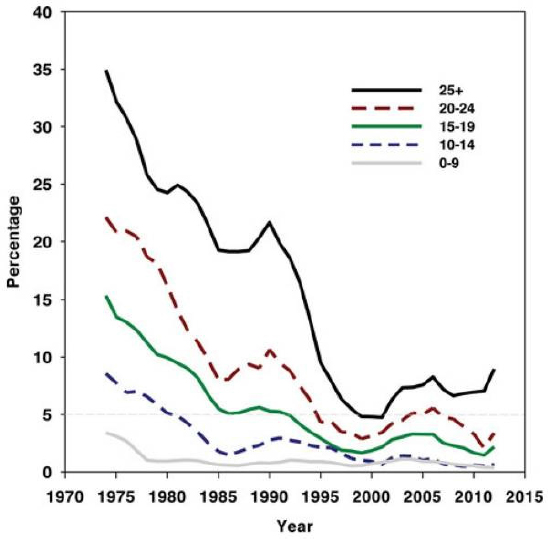
Beginning around 2000, data from the NIOSH Coal Workers’ Health Surveillance Program has shown an unexpected increase in the proportion of miners with CWP, based on abnormal chest radiographic findings (Laney and Attfield, 2010). That increase followed 30 years of decline in cases of CWP after the Federal Coal Mine Health and Safety Act of 1969 established limits on RCMD exposure (Figure 1-2).
In 2005, NIOSH found that, among miners with CWP, 35 percent showed rapidly progressive pneumoconiosis, including 15 percent with PMF (the most severe form of CWP) (Antao et al., 2005). Rapidly progressive pneumoconiosis is defined as an increase in small opacity profusion or development of progressive massive fibrosis within a period of less than 5 years, a substantially shorter period for disease progression than is typical for CWP.
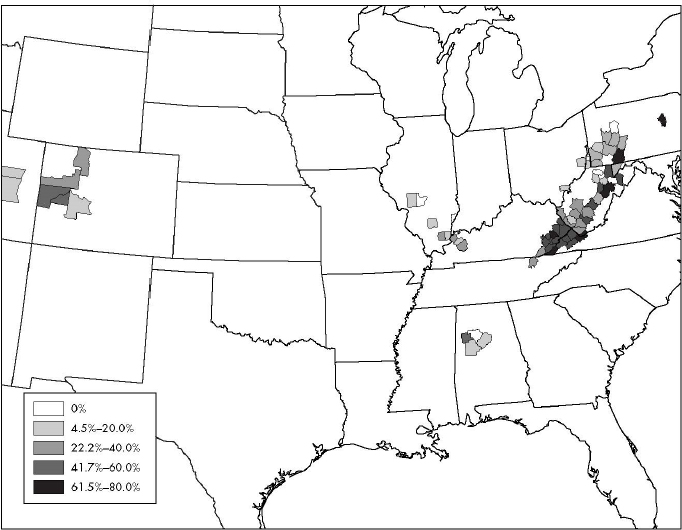
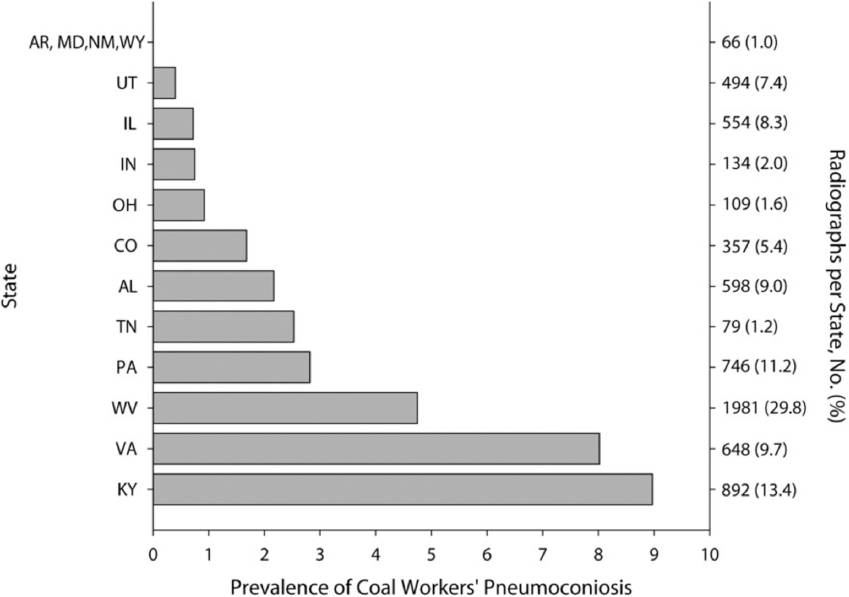
When the data on cases of rapidly progressive pneumoconiosis were mapped by geographic location, “hot spot” mining regions with high rates of the disease were identified (Figure 1-3), mainly in Appalachian coal fields in Kentucky, Virginia, and West Virginia (Figure 1-4). Compared to other miners, those with CWP in these three states were younger (median age 52 years compared to 55 years in other states) and more likely to be employed in smaller mines with fewer than 155 miners (Laney et al., 2012).
Because participation by active coal miners in the NIOSH Coal Workers’ Health Surveillance Program is voluntary, concern about potential bias in participation rates has been raised. However, differential participation by disease status is unlikely, as surveillance recruitment efforts by NIOSH have been aimed at all miners, and many miners are unaware that they have chest x-ray evidence of pneumoconiosis (which may be demonstrated on a chest x-ray in a miner without symptoms). Moreover, rates of participation in the NIOSH Coal Workers’ Health Surveillance Program have remained relatively stable over time (Laney and Attfield, 2013). Despite limitations from incomplete participation, findings of increased disease prevalence and severity underscore the need for effective dust control measures as well as the ongoing importance of medical surveillance of U.S. coal miners.
Trends in Underground Coal Mining and Employment That May Affect Disease Risk
Major changes have occurred over the past several decades in underground coal mining practices and coal mining conditions, some of which might have affected RCMD exposures and contributed to changing disease patterns. Lengths of continuous mining cuts and longwall passes (coal-face cutting) extended; cutting sequences changed to bi-directional cutting on longwalls and supersection continuous mining8 increased in use. Increased sizes and horsepower of mining equipment, more-efficient coal preparation methods, and an increased volume and speed of coal loading and transporting activities have led to increases in coal mine extraction productivity. Higher productivity certainly increases the total dust load generated.
___________________
8 The simultaneous operation of two sets of mining equipment that share a common dumping point on the same section, with each set being ventilated by a separate split of intake air.
Concurrent with changes in mining practices, there was a shift to thin seam mining, as relatively thick and high-quality coal seams became depleted in the United States. To ensure adequate head room for miners and equipment, more rock strata were mined as thin coal seams were being extracted for continuous mining and longwall mining. The actual section of strata mined may include portions of roof or floor or both. In some cases, the coal seam itself may contain partings of shale or clay materials that are mined along with coal. Mining surrounding rock along with the coal likely results in changes in particle size, shape, composition, and concentration, and probably increasing miners’ exposure to respirable crystalline silica from adjacent rock (Laney et al., 2010; Petsonk et al., 2013).
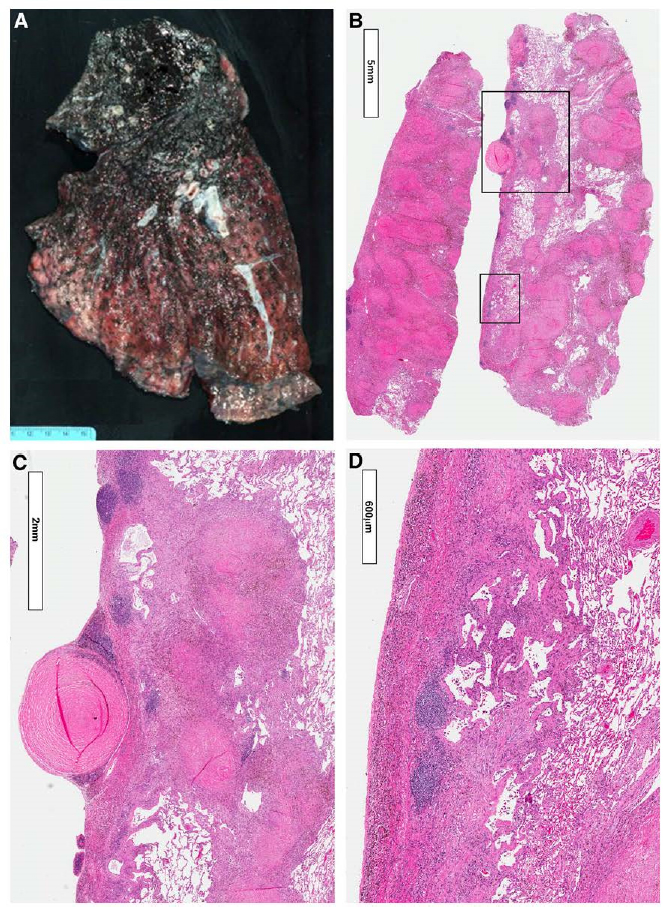
Increased silica exposure appears to explain at least some of the observed cases of rapidly progressive pneumoconiosis. Surveillance chest radiographs of Appalachian coal miners show an increasing proportion of r-type pneumoconiotic opacities (rounded pneumoconiotic opacities exceeding 3 mm), suggesting greater exposure to silica and silicates (Laney et al., 2010). A study of lung tissue specimens from 13 coal miners with rapidly progressive pneumoconiosis found that features of accelerated silicosis and mixed dust pneumoconiosis were common (Figure 1-5). Tissue samples contained a large amount of birefringent mineral dust particles suggestive for silica and silicates; carbonaceous coal dust was less prominent (Cohen et al., 2016).
Regarding employment factors, shifts in the mining economy (such as fluctuations in commodity price and decreases in mining jobs) resulted in a reduction of crew sizes on mine sections and extended work shifts, which tended to increase the duration of miners’ exposure. Economic shifts also have the potential to cause changes in the extent of workforce training, as well as experience and skill levels. If changes in the mining economy result in fewer unionized mines, the influence of mine safety committees could decrease. If more overtime, longer workweeks, and longer work shifts are relied upon to respond to economic changes, changes in patterns and
amounts of RCMD exposure are likely to occur. As miners who work for smaller mining companies tend to change employment locations and employers more frequently, their job duties also tend to vary and exposures during their mining tenures become more difficult to characterize. Also, smaller mining companies tend to have fewer health-directed resources. Those factors present challenges in understanding cumulative exposures over multiple years and other risk factors associated with coal mine dust lung diseases.
EARLY REGULATORY EFFORTS AND PAST RECOMMENDATIONS
With enactment of the Federal Coal Mine Health and Safety Act of 1969, mandatory standards for control of airborne RCMD were established for the first time in 30 CFR Part 70. In setting mandatory health standards in Title II of the Act (Interim Mandatory Health Standards), Congress stated that the purpose is “to provide to the greatest extent possible, that the working conditions in each underground coal mine are sufficiently free of respirable dust concentrations in the mine atmosphere to permit each miner the opportunity to work underground during the period of his entire adult working life without incurring any disability from pneumoconiosis or any other occupation-related disease during or at the end of such period.” That goal was to be achieved through mandatory RCMD exposure standards, medical examinations, and compensation programs, which were to be supported by enforcement as well as research and development programs. (Appendix G supplements the information provided in this section.)
According to the 1969 Coal Act, which became effective on June 30, 1970, the average RCMD concentration in the active sections of underground coal mines was to be maintained at or below 3.0 mg/m3. On December 30, 1972, the exposure limit was reduced to 2.0 mg/m3. The act also stated that the standard would be further reduced whenever the quartz content in RCMD was greater than 5 percent. The intended effect of the reduced limit was to keep the quartz concentration at or below 0.1 mg/m3. The significance of achieving those RCMD standards in mines was compelling, as a U.S. Bureau of Mines survey of 29 mines in 1968-1969 had found average dust concentrations in excess of 6 mg/m3 (Shepich, 1983). The Government Accountability Office (GAO, 1975) noted the general agreement among the miners, mine operators, union officials, and government agencies that significant reductions had been made in RCMD concentrations in mines. However, the report also identified weaknesses in the dust-sampling program that affect the accuracy and validity of the RCMD results and make it virtually impossible to determine how many mine sections complied with allowable dust concentration.
In the early 1990s, concerns were raised by MSHA, miners, and operators about the effectiveness of the regulatory dust program, including monitoring technology and sampling protocols, for meeting the stated purpose of the 1969 Coal Act in establishing the interim mandatory health standards. In May 1991, the Secretary of Labor directed MSHA to form a task force for conducting a review of the administration’s program to control RCMD concentrations and recommend program improvements. The review concluded that, even though there were significant reductions in RCMD concentrations since 1969, MSHA was not conducting the prescribed number of dust sampling inspections nor was it adequately monitoring the operator sampling program (MSHA, 1992).
A number of studies and program reviews were undertaken during that period to improve the effectiveness of the program from a compliance standpoint. At the same time, a search was under way for improved methods of dust control and new monitoring technology, sampling protocols, and compliance procedures.
In September 1995, NIOSH published a criteria document for occupational exposure to RCMD (NIOSH, 1995) that stated: “Excess prevalence of CWP, progressive massive fibrosis, and decreased lung function is estimated to be substantially reduced if lifetime average exposure to respirable coal mine dust is reduced from 2 mg/m3 to 0.5 mg/m3. However, even at a mean concentration of 0.5 mg/m3, miners have a greater than 1/1000 risk of developing these conditions.” The document presented the following recommendations:
- RCMD exposures should be limited to 1 mg/m3 as a time-weighted average concentration for up to 10 hours/day during a 40-hour workweek measured according to existing MSHA methods.
- The Recommended Exposure Limit (REL) represents the upper limit of exposure for each worker during each shift. For single, full-shift samples used to determine compliance, no upward adjustment of the REL should be made to account for measurement uncertainties.
- Exposures to respirable crystalline silica should not exceed 0.05 mg/m3 as a time-weighted average concentration for up to 10 hours/day during a 40-hour workweek.
Also in 1995, the Secretary of Labor established an Advisory Committee on the Elimination of Pneumoconiosis Among Coal Mine Workers. The report issued by the advisory committee recommended that MSHA exposure limits for coal mine dust and silica be lowered and established separately (MSHA, 1996). The report also concluded that continuous monitoring data are useful for evaluating the adequacy of dust control through hazard surveillance, in addition to using the data for compliance monitoring. The report emphasized the need for an appropriate balance among exposure monitoring and sampling strategies for determining compliance with RCMD exposure limits: personal (individual miner), occupational (such as a designated occupation), and environmental (such as a designated area). The report also noted the low participation rate of miners in the NIOSH Coal Worker’s Health Surveillance Program and recognized the difficulty in balancing out an individual miner’s right to confidentiality and the need for MSHA, NIOSH, mine operators, and fellow miners to know where and how much RCMD-related lung disease is occurring. The report concluded that “early recognition of hot spots where there is increased disease can further the primary preventive strategies.”
Monitoring technology and sampling strategies for respirable RCMD measurement have evolved to assist miners, mine management, and mine inspectors in their efforts to comply with the prevailing ambient airborne RCMD standards. In 2000, MSHA and NIOSH jointly proposed a rule to use a single, full-shift sample to determine the average concentration of RCMD. During that period, work had proceeded on the development of a continuous dust-monitoring device, including field-testing of prototypes. The eventual development of a continuous personal dust monitor (CPDM) for near-real-time measurement of RCMD concentrations was seen as the arrival of an important tool for exposure assessment and timely control (Volkwein et al., 2004). In 2010, MSHA and NIOSH published a final rule for approval requirements for the existing RCMD personal samplers, and new approval requirements for the CPDM. (See Chapter 4 for a description of the CPDM.)
DUST CONTROL MEASURES
While prevention of dust formation and prevention of dust from becoming airborne are two primary means to reduce the problem of airborne RCMD, the provision of adequate ventilating air to dilute the airborne dust and carry it away from the workers, and keeping the workers away from being downwind of the dust sources, are equally important to reduce exposure to RCMD. The application of those strategies has been greatly aided over the years by a number of developments in equipment design considerations and operating practices (for example, ventilation at the coal face and spray systems).
Every underground coal mining section in the United States operates under a MSHA-approved mine ventilation plan, which contains provisions for methane and dust control, as specified in 30 CFR 75.370. The dust control portion of the ventilation plan is specifically developed by the mine operator for each section in the mine and approved by the MSHA District Manager. Additional requirements for dust control provisions are specified in 30 CFR 90.300 and 90.301 for Part 90 miners, who have been diagnosed with coal mine dust disease. The dust control plan provides detailed descriptions of dust control measures to control miners’ exposures at less than
the allowable limit. In addition, it specifies sampling locations for monitoring purposes and serves to assess the performance of the process controls for respirable dust generation, entrainment, dispersion and control. The dust control plan provisions must be measurable and verifiable. (See Appendix F for information on dust control methods and examples items included in dust control plans.)
THE 2014 DUST RULE
MSHA’s 2014 dust rule changed the allowable limits, measurement technology, and sampling protocols for RCMD exposure (79 Fed. Reg. 85, May 1, 2014). The rule, which has been fully implemented, contains the following key features with respect to underground coal mines:
- The airborne RCMD concentration limit was lowered to 1.5 mg/m3. The RCMD limit is 0.5 mg/m3 for intake airways of the mine and in the mine atmosphere to which Part 90 miners are exposed (coal miners who have medical findings of pneumoconiosis and who opt to transfer to a less dusty job in the mine). The concentration limit for respirable quartz remained at 0.1 mg/m3 (100 micrograms per cubic meter or µg/m3).9,10
- Mine operators are required to use the CPDM to monitor RCMD exposures of underground coal miners in occupations associated with the highest concentrations. The CPDM also is to be used to monitor the exposures of Part 90 miners. Use of the CPDM is optional for nonproduction areas of underground coal mines.
- The term “normal production shift” is redefined to require that underground mine operators take RCMD samples in the mechanized mining unit (MMU) when production is at least 80 percent of the average production over the last 30 production shifts.
- The operator must collect RCMD samples for the full shift that a miner works. If a miner works a 12-hour shift, samples must be taken with an approved sampling device for the entire work shift. The previous RCMD regulation required monitoring for only 8 hours, even if shifts were longer.
- MSHA inspectors will use single, full-shift samples to determine compliance with the standard for RCMD concentrations.
- Immediate corrective actions to lower RCMD concentrations are required when a single, full-shift operator sample meets or exceeds the excessive concentration value for the RCMD standard. The excessive concentration value ensures that MSHA is 95 percent confident that the applicable standard has been exceeded and allows for the margin of error when measuring RCMD with an instrument. Tables of excessive concentration values are provided in the regulations for the applicable standard and device. See 30 CFR 70.206 and 70.207.
- Spirometry testing, occupational history, and symptom assessment have been added to the periodic chest radiographic (x-ray) examinations required to be offered by mine operators to underground miners through the NIOSH Coal Worker’s Health Surveillance Program.
- Certified persons who perform sampling of RCMD concentrations and who maintain and calibrate sampling equipment must complete an MSHA course of instruction and must pass an MSHA examination to demonstrate competency in the tasks needed for RCMD sampling procedures and in maintenance and calibration procedures. Procedures have been added that allow MSHA to revoke a person’s certification for failing to carry out the required sampling or maintenance and calibration procedures in a proper manner. Operators are required to provide training to all miners expected to wear a CPDM.
___________________
9 The Occupational Safety and Health Administration’s permissible exposure limit for crystalline silica is 50 µg/m3 (81 Fed. Reg. 16,286 [2016]).
10 Measured concentrations are to be expressed as equivalent concentrations. See 30 CFR 70.2.
Operators are required to collect all samples quarterly on consecutive shifts. The sampling frequency for each designated occupation (DO) and other designated occupation (ODO) is 15 consecutive shifts per quarter, and the sampling frequency for designated areas and Part 90 miners is five shifts per quarter.11 The DOs and ODOs must not be sampled concurrently. Sampling devices must be worn or carried directly to the MMU or designated area sampled and must be operated portal-to-portal. Sampling devices must remain with the occupation or designated area being sampled and must be operational during the entire shift, which includes the total time spent in the MMU or designated area and while traveling to and from the mining section or area being sampled (30 CFR 70.201). The operator’s approved ventilation plan must show the specific locations in the mine for taking the designated area samples.
If a single, full-shift sample measurement collected by a mine operator meets or exceeds the excess concentration value, the operator must make approved respiratory equipment available to affected miners. The operator also is required to take corrective action immediately. Examples of corrective actions include modifications of engineering or process controls (for example, ventilation and water sprays) and changes in work practices (for example, miner and equipment positioning). A violation is considered to occur when 3 out of 15 designated occupation or other designated occupation samples meet or exceed the excess concentration value or the average of all 15 samples meets or exceeds the excess concentration value. For operators’ samples of designated areas and Part 90 miners, noncompliance occurs when 2 out of 5 or the average of the 5 samples meets or exceeds the excess concentration value. Data from the CPDM sampling for regulatory compliance must be transmitted to MSHA within 24 hours after the sampling shift.
When sampling is done by MSHA, the instrument used is the personal respirable sampler with gravimetric analysis. The sample so collected is used to determine both compliance with the RCMD mass-based standard and the quartz concentration in the RCMD. Noncompliance occurs when one MSHA sample meets or exceeds the excess concentration value.
Trends in Regulatory Compliance Sampling
In contrast to the increasing rates of more severe and rapidly progressive forms of CWP, recent operator and MSHA samples in underground coal mines for regulatory compliance determinations show that measured airborne RCMD concentrations have decreased since implementation of the 2014 dust rule. A 2006 Morbidity and Mortality Weekly Report presented RCMD concentration data collected by MSHA inspectors and mine operators in Lee and Wise Counties, Virginia (Antao et al., 2006). In those two Appalachian counties, where cases of progressive massive fibrosis have been reported recently, samples collected for determining regulatory compliance showed that measured concentrations of RCMD and silica declined steadily.
Data provided to the committee by MSHA (Meikle, 2017) indicate that samples provided by mine operators showed a greater than 99 percent rate of regulatory compliance with the exposure limit in the 2014 dust rule. Since February 2016, all mine operator sampling underground has been performed with the CPDM; since August 1, 2016, the RCMD concentration limit has been 1.5 mg/m3. It is evident from the reported data from April 2016 to March 2017 that noncompliance is rare and that average RCMD concentrations of the submitted data were well below the allowable level (Table 1-1). Quarterly data for that period are presented in Appendix G. It is important to note, however, that 99 percent operator compliance with the RCMD allowable exposure limit of 1.5 mg/m3 over an entire shift does not mean that the exposures of 99 percent of the
___________________
11 Designated occupation is the occupation on a mechanized mining unit (MMU) that has been determined by results of RCMD samples to have the greatest respirable dust concentration. In addition, other occupations on an MMU that are designated for sampling are referred to as other designated occupations. Designated areas are specific locations in the mine where samples will be collected to measure sources of airborne RCMD in the active workings (that is, any place in a coal mine where miners are normally required to work or travel) (see 30 CFR 70.2).
| Mining Method | Type of Sample | Number of Samples | Average Concentration, mg/m3 | Number of Noncompliance | Percent Compliance |
|---|---|---|---|---|---|
| Longwall | DO | 2,474 | 0.907 | 15 | 99.4 |
| Longwall | ODO | 2,161 | 0.768 | 7 | 99.7 |
| Continuous Mining | DO | 27,758 | 0.679 | 58 | 99.8 |
| Continuous Mining | ODO | 25,248 | 0.647 | 46 | 99.8 |
NOTE: DO = designated occupation; ODO = other designated occupations.
SOURCE: Meikle, 2017.
miners are less than the allowable limit. Even stringent regulations cannot ensure that flaws in dust control practices are eliminated completely (Weeks, 2006; Pollock et al., 2010). It is also important to note that most miners incurred much of their exposures when previous regulations were in effect. Given that the latency period of CWP disease onset is typically 10 or more years, sufficient time has not elapsed to assess the effect of the 2014 requirements on disease rates and severity.
CONCLUSION
There are likely multiple factors that have contributed to an increase in the prevalence and severity of coal mine dust related lung diseases. Determining the causes of that increase and eliminating occupational lung disease in coal miners is a complex scientific, engineering, medical, regulatory, social, political, economic and legal problem. However, a full analysis of that problem is beyond the scope of this report. The primary focus of this report is an examination of monitoring and sampling approaches for the control of RCMD and miners’ exposure.
As dust-generating processes in mining have intensified over the past several decades associated health hazards might increase if there have been unanticipated changes in the characteristics of RCMD exposures that are important in the risk of coal mine dust lung diseases. Also, questions might arise as to whether the monitoring required by the 2014 dust rule is targeting the most important exposures metrics.
Currently, dust control technologies are widely available and have the potential to protect miners’ health from RCMD exposure. As discuss in later chapters, optimal strategies are needed to assure that the recent surge in prevalence and severity of coal mine dust lung diseases does not continue.
ORGANIZATION OF THE REPORT
In Chapter 2, the committee discusses the current technology and application for rock dusting to control explosions in coal mines, the composition and particle size distribution of available rock dust products, and the effect of rock-dusting practices on measurements of RCMD concentrations and compliance with respirable dust standards. Chapter 3 provides an overview of sampling and monitoring practices used in several major coal-producing countries. In considering the requirements for those practices and their implementation, the committee identified important commonalities and dissimilarities. Chapter 4 assesses the efficacy of current monitoring technologies and sampling approaches for informing decision making related to reducing RCMD exposures in the United States. In assessing efficacy, the chapter examines scientific and technical bases of key assumptions that those monitoring technologies and sampling approaches rely upon. As compliance sampling focuses mainly on the personal exposures of specific miners, the committee’s considerations included how those data might relate to airborne RCMD exposures of nonmonitored workers who share that mine environment. Chapter 5 discusses optimal monitoring
and sampling strategies to aid mine operators’ decision making related to lowering RCMD exposures. The committee considered strategies that go beyond strict compliance with current regulations and include consideration of other factors not reflected in the sampling results that may be important in understanding relationships between miners’ exposures and disease risk. Strategies were considered for maintainable reductions in RCMD exposures to all miners, not just particular mine workers wearing a CPDM during a particular shift. In addition to informing mine operators’ decision making, the committee considered strategies to aid mine workers’ decisions in responding to near-real-time CPDM measurements. Chapter 6 presents the committee’s overall conclusions, identifies important research gaps, and recommends research and development activities for addressing those gaps.
REFERENCES
Amandus, H. E., and G. Piacitelli. 1987. Dust exposures at U.S. surface coal mines in 1982-1983. Archives of Environmental Health 42(6):374-381.
Antao, V. C., E. L. Petsonk, L. Z. Sokolow, A. L. Wolfe, G. A. Pinheiro, and M. D. Attfield. 2005. Rapidly progressive coal workers’ pneumoconiosis in the United States: Geographic clustering and other factors. Occupational and Environmental Medicine 62(10):670-674. doi:10.1136/oem.2004.019679.
Antao, V., E. L. Petsonk, and M. D. Attfield. 2006. Advanced cases of coal workers’ pneumoconiosis—Two counties, Virginia, 2006. Morbidity and Mortality Weekly Report 55(33):909-913.
Attfield, M. D. 1985. Longitudinal decline in FEV1 in United States coalminers. Thorax 40(2):132-137.
Attfield, M. D., and T. K. Hodous. 1992. Pulmonary function of U.S. coal miners related to dust exposure estimates. American Review of Respiratory Disease 145(3):605-609.
Attfield, M. D., and E. D. Kuempel. 2008. Mortality among U.S. underground coal miners: A 23-year follow-up. American Journal of Industrial Medicine 51(4):231-245.
Attfield, M. D., and N. S. Seixas. 1995. Prevalence of pneumoconiosis and its relationship to dust exposure in a cohort of U.S. bituminous coal miners and ex-miners. American Journal of Industrial Medicine 27:137-151.
Beer, C., H. A. Kolstad, K. Søndergaard, E. Bendstrup, D. Heederik, K. E. Olsen, Ø. Omland, E. Petsonk, T. Sigsgaard, D. L. Sherson, and V. Schünssen. 2017. A systematic review of occupational exposure to coal dust and the risk of interstitial lung disease. European Clinical Respiratory Journal Blackley, D. J., C. N. Halldin, and A. S. Laney. 2014. Resurgence of a debilitating and entirely preventable respiratory disease among working coal miners. American Journal of Respiratory and Critical Care Medicine 190(6):708-709. doi:10.1164/rccm.201407-1286LE.
Blackley, D., J. Crum, C. Halldin, E. Storey, and A. Laney. 2016. Resurgence of progressive massive fibrosis in coal miners—Eastern Kentucky, 2016. Morbidity and Mortality Weekly Report 65:1385-1389. doi:10.15585/mmwr.mm6549a1.
Blackley, D. J., L. E. Reynolds, C. Short, R. Carson, E. Storey, and C. N. Halldin. 2018. Progressive massive fibrosis in coal miners from 3 clinics in Virginia. JAMA 319(1):500-501.
Castranova, V. 2000. From coal mine dust to quartz: Mechanisms of pulmonary pathogenicity. Inhalation Toxicology 12:7-14.
Castranova, V., and V. Vallyathan. 2000. Silicosis and coal workers’ pneumoconiosis. Environmental Health Perspectives 108(Suppl 4):675-684.
CDC (Centers for Disease Control and Prevention). 2012. Pneumoconiosis and advanced occupational lung disease among surface coal miners – 16 states, 2010–2011. Morbidity and Mortality Weekly Report 61(23):431.
Cohen, R. A., E. L. Petsonk, C. Rose, B. Young, M. Regier, A. Najmuddin, J. L. Abraham, A. Churg, and F. H. Green. 2016. Lung pathology in U.S. coal workers with rapidly progressive pneumoconiosis implicates silica and silicates. American Journal of Respiratory and Critical Care Medicine 193(6): 673-680.
Colinet, J. F., J. P. Rider, J. M. Listak, J. A. Organiscak, and A. L. Wolfe. 2010. Best Practices for Dust Control in Coal Mining. Pittsburgh, PA: NIOSH.
EIA (U.S. Energy Information Administration). 2012. Annual Energy Review 2011. Table 7.2 Coal Production, 1949-2011 (Million Short Tons) [online]. Available at https://www.eia.gov/totalenergy/data/annual/showtext.php?t=ptb0702 (accessed December 22, 2017).
EIA. 2014. Coal Recoverable Reserves 2014 [online]. Available at https://www.eia.gov/beta/international/rankings/#?cy=2014&aid=6&pid=1 (accessed December 22, 2017).
EIA. 2017a. Annual Coal Report 2016. Available online at https://www.eia.gov/coal/annual/pdf/acr.pdf (accessed December 22, 2017).
EIA. 2017b. Coal Data Browser. Aggregate Coal Mine Production: All Coal: Underground 2016. Available online at https://www.eia.gov/beta/coal/data/browser/ (accessed December 22, 2017).
EIA. 2017c. International Energy Outlook 2017. Data. Available online at https://www.eia.gov/outlooks/aeo/data/ (accessed December 22, 2017).
Eller, N. H., B. Netterstrøm, F. Gyntelberg, T. S. Kristensen, F. Nielsen, A. Steptoe, and T. Theorell. 2009. Work-related psychosocial factors and the development of ischemic heart disease: a systematic review. Cardiology in review 17(2): 83-97.
Enterline, P. E. 1972. A review of mortality data for American coal miners. Annals of the New York Academy of Sciences 200(1):260-272.
Eriksson, H. P., E. Andersson, L. Schiöler, M. Söderberg, M. Sjöström, A. Rosengren, and K. Torén. 2018. Longitudinal study of occupational noise exposure and joint effects with job strain and risk for coronary heart disease and stroke in Swedish men. BMJ open 8(4):e019160.
GAO (U.S. Government Accountability Office). 1975. Improvements Still Needed in Coal Mine Dust-Sampling Program and Penalty Assessments and Collections [online]. Available at http://www.gao.gov/assets/120/114174.pdf (accessed July 30, 2017).
Halldin, C. N., A. L. Wolfe, and A. S. Laney. 2015a. Comparative respiratory morbidity of former and current U.S. coal miners. American Journal of Public Health 105(12):2576-2577.
Halldin, C. N., W. R. Reed, G. J. Joy, J. F. Colinet, J. P. Rider, E. L. Petsonk, J. L. Abraham, A. L. Wolfe, E. Storey, and A. S. Laney. 2015b. Debilitating lung disease among surface coal miners with no underground mining tenure. Journal of Occupational and Environmental Medicine 57(1):62.
Huang, C., J. Li, Q. Zhang, and X. Huang. 2002. Role of bioavailable iron in coal dust-induced activation of activator protein-1 and nuclear factor of activated T cells: Difference between Pennsylvania and Utah coal dusts. American Journal of Respiratory Cell and Molecular Biology 27(5):568-574.
Huang, X., W. Li, M. D. Attfield, A. Nadas, K. Frenkel, and R. B. Finkelman. 2005. Mapping and prediction of coal workers’ pneumoconiosis with bioavailable iron content in the bituminous coals. Environmental Health Perspectives 113(8):964-968.
Johann-Essex, V., C. Keles, M. Rezaee, M. Scaggs-Witte, and E. Sarver. 2017. Respirable coal mine dust characteristics in samples collected in central and northern Appalachia. International Journal of Coal Geology 182:85-93.
Kittelson, D. 1997. Engines and Nanaoparticles: A Review. Journal of. Aerosol Science, 29(5):575–588.
Kuempel, E. D., M. W. Wheeler, R. J. Smith, V. Vallyathan, and F. H. Y. Green. 2009. Contributions of dust exposure and cigarette smoking to emphysema severity in coal miners in the United States. American Journal of Respiratory and Critical Care Medicine 180:257-264.
Laney, A. S. 2017. Presentation to Committee on the Study of the Control of Respirable Coal Mine Dust Exposure in Underground Mines, Morgantown, WV, June 29, 2017.
Laney, A. S., and M. D. Attfield. 2010. Coal workers’ pneumoconiosis and progressive massive fibrosis are increasingly more prevalent among workers in small underground coal mines in the United States. Occupational and Environmental Medicine 67(6):428-431.
Laney, A. S., and M. D. Attfield. 2013. Examination of potential sources of bias in the U.S. Coal Workers’ Health Surveillance Program. American Journal of Public Health 104(1):165-170.
Laney, A. S., E. L. Petsonk, and M. D. Attfield. 2010. Pneumoconiosis among underground bituminous coal miners in the United States: Is silicosis becoming more frequent? Occupational and Environmental Medicine 67(10):652-656.
Laney, A. S., E. L., Petsonk, J. M. Hale, A. L. Wolfe, and M. D. Attfield. 2012. Potential determinants of coal workers’ pneumoconiosis, advanced pneumoconiosis, and progressive massive fibrosis among underground coal miners in the United States, 2005-2009. American Journal of Public Health 102(Suppl 2):S279-283.
Laney, A. S., and D. N. Weissman. 2014. Respiratory diseases caused by coal mine dust. Journal of Occupational and Environmental Medicine 56 (Suppl 10):S18-S22.
Lapp, N. L., and V. Castranova. 1993. How silicosis and coal workers’ pneumoconiosis develop: A cellular assessment. Occupational Medicine 8(1):35-56.
McConnochie, K., F. H. Y. Green, V. Vallyathan, J. C. Wagner, R. M. E. Seal, and J. P. Lyons. 1988. Interstitial fibrosis in coal workers—experience in Wales and West Virginia. Annals of Occupational Hygiene 32:553-560.
Meikle, G. 2017. Presentation from the Chief of Health for Coal Mine Safety and Health, MSHA to Committee on the Study of the Control of Respirable Coal Mine Dust Exposure in Underground Mines, Morgantown, WV, June 29, 2017.
Miller, B. G., and L. MacCalman. 2010. Cause-specific mortality in British coal workers and exposure to respirable dust and quartz. Occupational and Environmental Medicine 67(4):270-276.
MSHA (Mine Safety and Health Administration). 1992. Review of the Program to Control Respirable Coal Mine Dust in the United States. Report of the Coal Mine Respirable Dust Task Group, June 1992 [online]. Available at https://arlweb.msha.gov/s&hinfo/blacklung/Reports/1992ReviewCoalMineDust.pdf (accessed November 17, 2017).
MSHA. 1996. Report of the Secretary of Labor’s Advisory Committee on the Elimination of Pneumoconiosis among Coal Mine Workers. Washington, DC: Department of Labor.
MSHA. 2014. Regulatory Economic Analysis For Lowering Miners’ Exposure to Respirable Coal Mine Dust Including Continuous Personal Dust Monitors Final Rule. Available online at https://arlweb.msha.gov/endblacklung/docs/REAFinalRule.pdf (accessed December 22, 2017).
NIOSH (National Institute for Occupational Safety and Health). 1995. Criteria for a Recommended Standard. Occupational Exposure to Respirable Coal Mine Dust. Cincinnati, Ohio: NIOSH.
NIOSH. 2008. Work-Related Lung Disease Surveillance System (eWoRLD). Respirable coal mine dust: Geometric mean exposures and percent exceeding designated occupational exposure limits by MSHA coal mine district and state, MSHA inspector and mine operator samples, 1979-2003. Available online at https://www.cdc.gov/eworld/Data/295 (accessed December 22, 2017).
NMA (National Mining Association). 2017a. U.S. Coal Production By State, 2005-2016. Available online at https://nma.org/wp-content/uploads/2017/06/coal_production_by_state_2016.pdf (accessed December 22, 2017).
NMA. 2017b. U.S. Coal Production Trends, 1980-2016 (Million Short Tons). Available online at https://nma.org/wp-content/uploads/2017/06/us_coal_production_trends_2016-2.pdf (accessed December 22, 2017).
Perret, J. L., B. Plush, P. Lachapelle, T. S. Hinks, C. Walter, P. Clarke, L. Irving, P. Brady, S. C. Dharmage, and A. Stewart. 2017. Respirology 22(4):662-670.
Petsonk, E. L., C. Rose, and R. Cohen. 2013. Coal mine dust lung disease. New lessons from old exposure. American Journal of Respiratory and Critical Care Medicine 187(11):1178-1185.
Piacitelli, G. M., H. E. Amandus, and A. Dieffenbach. 1990. Respirable dust exposures in U.S. surface coal mines (1982-1986). Archives of Environmental Health 45(4):202-209.
Pollock, D. E., J. D. Potts, and G. J. Joy. 2010. Investigation into dust exposures and mining practices in mines in the southern Appalachian Region. Mining Engineering 62(2):44-49.
Schatzel, S. J., and B. W. Stewart. 2012. A provenance study of mineral matter in coal from Appalachian Basin coal mining regions and implications regarding the respirable health of underground coal workers: A geochemical and Nd isotope investigation. International Journal of Coal Geology 94: 123-136.
Seixas, N. S., T. G. Robins, M. D. Attfield, and L. H. Moulton. 1992. Exposure-response relationships for coal mine dust and obstructive lung disease following enactment of the Federal Coal Mine Health and Safety Act of 1969. American Journal of Industrial Medicine 21(5):715-734.
Sellaro, R., and E. Sarver. 2014. Characterization of respirable dust in an underground coal mine in Central Appalachia. Transactions of the Society for Mining, Metallurgy & Exploration 336:457-466.
Shepich, T. J. 1983. Welcome remarks. Pp. 3-6 in Proceedings of the Symposium on Control of Respirable Coal Mine Dust, Mine Safety and Health Administration, Washington, DC.
Skogstad, M., H. A. Johannessen, T. Tynes, I. S. Mehlum, K. C. Nordby, and A. Lie. 2016. Systematic review of the cardiovascular effects of occupational noise. Occupational Medicine 66(1):10-16.
Suarthana, E., A. S. Laney, E. Storey, J. M. Hale, and M. D. Attfield. 2011. Coal workers’ pneumoconiosis in the United States: Regional differences 40 years after implementation of the 1969 Federal Coal Mine Health and Safety Act. Occupational and Environmental Medicine 68:908-913. doi:10.1136/oem.2010.063594.
Volkwein, J. C., R. P. Vinson, L. J. McWilliams, D. P. Tuchman, and S. E. Mischler. 2004. Performance of a new personal respirable dust monitor for mine use. Report of Investigations 9663:1-25. Pittsburgh, PA: NIOSH.
Walton, W. H., J. Dodgson, G. G. Hadden, and M. Jacobsen. 1977. The effects of quartz and other non-coal dusts in coal-workers’ pneumoconiosis. In Inhaled Particles IV, Part 2. W. H. Walton, Ed. Oxford, U.K.: Pergamon Press.
Weeks, J. L. 2006. The Mine Safety and Health Administration’s criterion threshold value policy increases miners’ risk of pneumoconiosis. American Journal of Industrial Medicine 49(6):492-498.
Weiner, J., L. Barlow, and B. Sjögren. 2007. Ischemic heart disease mortality among miners and other potentially silica‐exposed workers. American journal of industrial medicine 50(6):403-408.
WHO (World Health Organization). 1999. Hazard Prevention and Control in the Work Environment: Airborne Dust. Geneva, Switzerland: WHO.


















