
EUTHANASIA IN THE NETHERLANDS
Bregje Onwuteaka-Philipsen
Professor of End-of-Life Research
Vrije University Medical Center
In the Netherlands, both euthanasia and physician-assisted suicide are legal, although the physician is expected to be present when the patient self-ingests the lethal medication. As Bregje Onwuteaka-Philipsen, a professor of end-of-life research at the Vrije University Medical Center and the Amsterdam Public Health Research Institute, explained, if something goes wrong after self-administration, the physician is then expected to perform euthanasia to complete the process. She also said that in the Netherlands there would be concern about the potential abuse of a prescription if a physician was not present to deliver the lethal medication at the time of death.
The current Dutch law was enacted in 2002, and it requires all physicians who perform either euthanasia or physician-assisted suicide to report each case to one of five regional euthanasia review committees. The review committees comprise a lawyer, a physician, and an ethicist who judge each case on the basis of criteria for due care. If there is a verdict of noncompliance, the case is referred to a public prosecutor who then investigates and makes a decision on whether to prosecute the physician. The criteria for due care include that the physician must
- be satisfied that the patient’s request is voluntary and well-considered;
- be satisfied that the patient’s suffering is unbearable, with no prospect of improvement;
- have informed the patient about his or her situation and prognosis;
- have come to the conclusion, together with the patient, that there is no reasonable alternative in the patient’s situation;
- have consulted at least one other, independent physician, who must see the patient and give a written opinion on whether the due care criteria set out above have been fulfilled; and
- have exercised due medical care and attention in terminating the patient’s life or assisting in the patient’s suicide.
Onwuteaka-Philipsen said that the law is primarily designed to protect the physician. She explained that suffering can be either psychological or physical, which can include a combination of complaints related to old age, and that there is no requirement that the patient be terminally ill. Since the law was enacted, there have been between 80 and 90 cases that were ruled to be noncompliant and referred to the public prosecutor, one of which went to trial.
There are several sources of information on the practice of euthanasia and physician-assisted suicide in the Netherlands. Annual reports from the five review committees include characteristics of all the reported cases. However, Onwuteaka-Philipsen said, these are limited to cases reported to the review committees, making it impossible to investigate instances of non-reporting. Furthermore, the annual reporting does not contain information on who has requested but been denied euthanasia or physician-assisted suicide. The report also lacks case details that would provide context for the end-of-life decision-making process. Onwuteaka-Philipsen said that the Dutch government has commissioned a nationwide evaluation study every 5 years since 1990, the first three of which led to changes in the regulation procedure and eventually to the Dutch law in 2002 regarding euthanasia. These studies consist of a death certificate analysis in which a questionnaire is sent to the attending physician of a stratified sample of deaths as well as a survey among a stratified sample of physicians in order to study trends in end-of-life decisions. Furthermore, specific topics are addressed with qualitative methods.
An analysis of 25 years of data on all deaths in the Netherlands found that the incidence of euthanasia rose significantly between 2010 and 2015, while physician-assisted suicide has remained low and the incidence of the illegal practice of ending life without an explicit request has fallen (van der Heide et al., 2017) (see Figure 4-1). Onwuteaka-Philipsen said that combining the results of this study with the number of reported cases of euthanasia and physician-assisted suicide shows that the notification rate has increased since the enactment of the 2002 law (see Figure 4-2).
Onwuteaka-Philipsen said that the percentage of deaths preceded by a request for euthanasia or physician-assisted suicide rose from 5.2 percent in 2005 to 8.4 percent in 2015 (van der Heide et al., 2017). At the same time, the percentage of requests that were granted also rose, from 39 percent in 2005 to 55 percent in 2015. It continues to be the case that most patients requesting either procedure have cancer or a serious somatic disease, she said, but the incidence of euthanasia has increased somewhat in older people (see Figure 4-3). Onwuteaka-Philipsen said that there is a growing debate in the Netherlands about whether euthanasia or physician-assisted suicide should be available to patients with dementia or psychiatric illness or who have no serious illness but feel that they
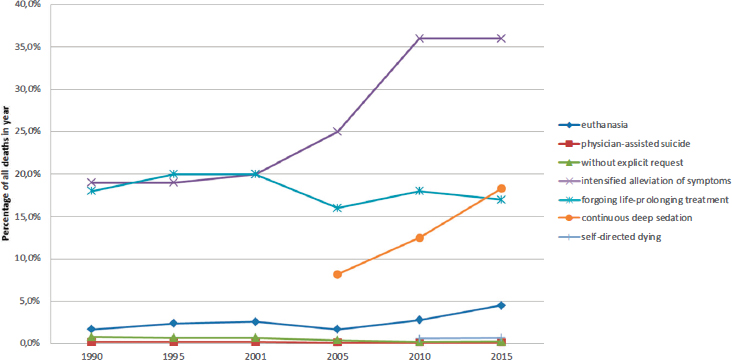
SOURCES: Onwuteaka-Philipsen presentation, February 13, 2018. Data from van der Heide et al., 2017.
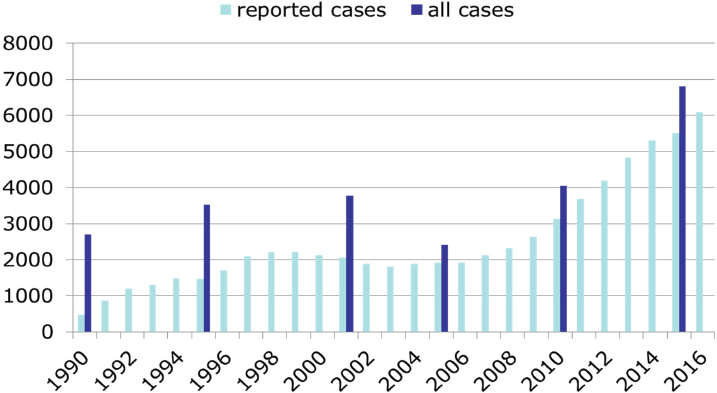
SOURCES: Onwuteaka-Philipsen presentation, February 13, 2018. Data from Onwuteaka-Philipsen et al., 2017.
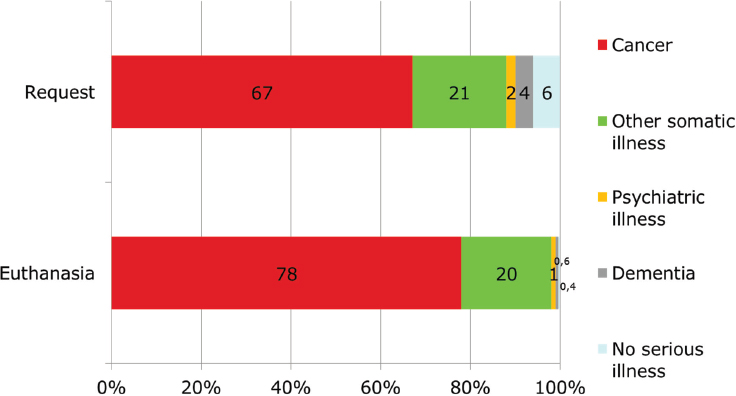
SOURCE: Onwuteaka-Philipsen presentation, February 13, 2018.
have completed their lives. To illustrate the types of information gathered in the Dutch process, she used the example of psychiatric illness. The absolute number of reported cases of patients with a psychiatric diagnosis completing either process has risen substantially over the past few years—from 13 in 2011 to 60 in 2016—but as a percentage of all cases, the numbers remain low (there were 6,091 reported cases in 2016) (Regional Euthanasia Review Committees, 2017). Surveys of psychiatrists in 1995, 2008, and 2016 found that there was an increasing number of requests from patients with a psychiatric diagnosis, though in all years most of those requests were refused (see Figure 4-4). The main reason that psychiatrists rejected 94 percent of these requests was because they did not meet the due care criteria.
Furthermore, Onwuteaka-Philipsen said, a survey of the Dutch public and Dutch physicians revealed how reluctant physicians are to grant a request for euthanasia or physician-assisted suicide for a patient with a psychiatric diagnosis. While 80 percent of the physicians said it was conceivable they would grant such a request from a cancer patient, only 37 percent said it was conceivable to ever grant a request from a psychiatric patient. In contrast, 53 percent of the public said euthanasia and physician-assisted suicide should be allowed for a patient with a psychiatric diagnosis, compared with 88 percent who said it should be allowed for cancer patients (Onwuteaka-Philipsen et al., 2017).
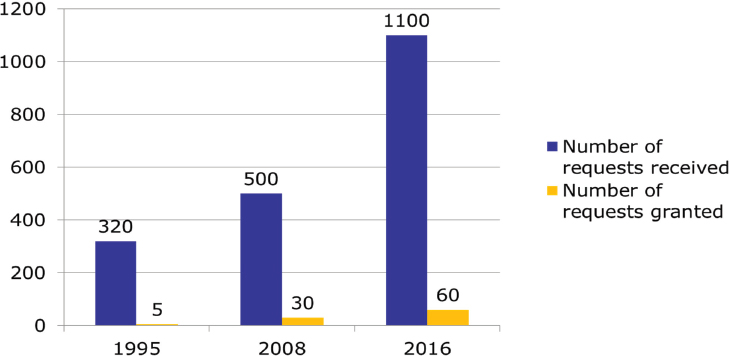
SOURCE: Onwuteaka-Philipsen presentation, February 13, 2018.
Frances Norwood
Assistant Research Professor of Anthropology
George Washington University
When Frances Norwood, an assistant research professor of anthropology at George Washington University, began studying euthanasia and end-of-life care, she went to the Netherlands. Norwood explained that what she discovered through her research in the Netherlands was not what she expected. The purpose of her study was to set aside the law, opinion studies, and the hypothetical and to go into people’s homes and find out what euthanasia really looks like in practice. She said she anticipated studying death and dying but what she found was actually something quite different.
Her study focused specifically on euthanasia, which is more widely used than physician-assisted suicide in the Netherlands. According to Norwood, Dutch doctors and families find physician-assisted suicide unpredictable, so they tend not to pursue it. Norwood spent 15 months between 1999 and 2001 in Amsterdam and in a cluster of small towns outside of the city sitting with people who were dying. Each day, she would sit in the office with a different general practice physician and go on house calls to see the more seriously ill and end-of-life patients. She returned to the Netherlands in 2008 and did follow-up interviews with some of the same family members and doctors.
Before discussing her findings, Norwood told the story of one patient,
an 80-year-old woman with terminal breast cancer that had spread to her lymph nodes. Over time, her symptoms worsened, and she was unable to eat with her husband or get outside in her garden, two things that were very important to her. When she requested euthanasia from her doctor, the doctor was shocked, as this woman felt like a grandmother to her. Nevertheless, she did what all of the doctors that Norwood met with in the Netherlands do, which was to schedule family meetings to discuss the euthanasia request. These meetings typically involved going from family member to family member and talking about how they feel about the request. Over the last 3 weeks of this woman’s life, her doctor visited almost daily, talking with her and listening to her life story. On her final day, in her hospital bed on the first floor of her own home, she said goodbye to her husband, son, and neighbors and died peacefully.
What this story illustrates, Norwood said, is that euthanasia in the Netherlands involves discussions taking place over weeks, months, and sometimes years and does not largely focus on the final day itself. A caveat to this conclusion, she noted, is that she was working with general practitioners and not specialists, so the patients tended not to be the sickest and thus had time to process their illnesses. As a result of this long discussion process, few patients actually followed through on their request for euthanasia, she said. The three main reasons she found for people not ultimately choosing euthanasia were that a family member was not ready, the person changed his or her mind over time, or the patient never restarted the process after the physician stalled on the initial request for assisted death.
In practice, Norwood said, patients get activated by the process and begin talking about what matters most to them. At the same time, physicians get more involved with the patient because now they have something to do in the wake of a terminal prognosis. Families become more involved, too, and social bonds are better maintained at a time when they are often slipping. In Norwood’s experience, she said, people typically did not go through with euthanasia because they received the satisfaction and contentment they needed through the dialogue occurring between themselves, their loved ones, and their physicians. In essence, talking euthanasia became a palliative practice, solidifying social bonds near the end of life and making a euthanasia death unnecessary for some.
Laws exist in the context of culture, Norwood noted, so she cautioned against extrapolating these findings to how physician-assisted death occurs in Oregon or any jurisdiction where it is legal. She explained that the ways in which Montana, Oregon, and Washington, DC, might practice physician-assisted death are all going to be slightly different. The practice of physician-assisted death is going to be based on cultural processes and cultural ways of thinking, feeling, acting, and understand-
ing, she said. She emphasized that the important question to ask regarding physician aid-in-dying is whether it is something that fits within U.S. culture. Norwood closed with a request to consider the cultural context and said that this is a practice that goes beyond what is written in law.
During the discussion period, Daniel Sulmasy of Georgetown University asked Norwood whether there is a connection between a request for assisted suicide or euthanasia and the meaningful family meetings, doctor visits, and opportunities for reconciliation. That is, Sulmasy said, why should it be that a patient only gets the opportunity for discussions with family and the possibility of reconciliation that Norwood mentioned if they ask for euthanasia? Norwood replied that Dutch practitioners generally are very involved with the families of patients from the beginning, but once a request for euthanasia is made, it gives practitioners more power to initiate difficult discussions.
THE CANADIAN EXPERIENCE
Jennifer Gibson
Sun Life Financial Chair in Bioethics
University of Toronto
Jennifer Gibson, the Sun Life Financial Chair in Bioethics and the director of the University of Toronto Joint Centre for Bioethics, agreed with Norwood on the importance of cultural and historical context. She told the audience that the context surrounding physician aid-in-dying in Canada will be different than the context in the Netherlands or in the United States. The Canadian story starts in 1993, when a woman in her early 40s with amyotrophic lateral sclerosis (ALS) sought an amendment to the criminal code so that her physician could help her die. At the time, the Supreme Court of Canada ruled 5-4 against physician-assisted death. Then, in 2015, the Supreme Court of Canada ruled 9-0 in favor of changing the criminal code to allow assisted death. As a result of this ruling, Canada enacted Bill C14, An Act to Amend the Criminal Code and to Make Related Amendments to Other Acts (Medical Assistance in Dying), in June 2016. Thus, Gibson said, physician aid-in-dying was part of Canadian conversation and consciousness for 22 years before a law concerning it was formalized.
What changed over time was public perspectives on the issue, Gibson said. In recent years a number of opinion polls have been conducted, and a convergence of public opinion emerged with 75 percent of Canadians supporting legalization of medically assisted death in Canada. One factor that drove the change in public attitude was the experience drawn from Oregon and the Benelux countries (Belgium, Luxemburg, and the
Netherlands), and the court noted this experience in making its ruling. Also influencing that decision was the Province of Quebec’s passing of integrated legislation related to end-of-life care which introduced the right to palliative care and the right to what the provincial legislation called medical aid-in-dying. Quebec’s legislation resulted from 5 years of consultation with residents and an iterative process to craft the law. The final factor, Gibson said, was that there were some shifts in clinical perspectives. In surveys conducted by the Canadian Medical Association, members supported legislation on medical aid-in-dying, but there was some reticence among those surveyed about being a provider of the practice.
One important factor in the Canadian context, said Gibson, is that criminal code amendments come under federal jurisdictions, but health care is primarily a provincial and territorial matter. This, Gibson said, created an interesting legal conundrum about the proper division of power. If Canada were to introduce legislation at the federal level, it would need to be translated in some way into the provincial and territorial practices in a coherent way, she explained. The diversity in the way that the Canadian provinces and territories organize their health systems means there is some heterogeneity in terms of how they provide medical aid-in-dying to residents.
Gibson said that geography is another key factor in the Canadian context. In the northern territories, for example, nurse practitioners are the primary caregivers, rather than physicians. Because of such differences, Gibson said, geographic diversity and diversity in jurisdictions will need to be considered by anyone who is serious about implementing medical aid-in-dying in Canada.
In Canada, the new law provides protections for both physicians and nurse practitioners whose scope of practice includes medication prescribing and administration. The law permits both clinician- and self-administration for a person over age 18 who is capable of making his or her own decisions related to health and who is legally eligible for health care in Canada. In addition, the individual must have a “grievous and irremediable” medical condition, must make a voluntary request that is not the result of external pressure, and must be informed of all available alternative options for his or her care.
Gibson said that the requirement of a “grievous and irremediable” medical condition has been a challenge for clinicians to interpret. In Canada, it has been interpreted as saying that the patient must have a condition that is serious or incurable and be in an advanced state or in irreversible decline. In addition, the individual must be experiencing enduring physical or psychological suffering that is intolerable and that cannot be addressed by means acceptable to the individual and
that the individual’s natural death is reasonably foreseeable under these circumstances.
The Canadian law also lays out a number of procedural requirements, including requirements related to the nature of the request, how the request is conducted, how it is signed, and how it is witnessed, while recognizing that not everyone can make a written request. The law requires two independent practitioners to confirm eligibility and 10 days between the request and the provision of the medication. The law allows for the 10-day waiting period to be shortened in the case of imminent death or imminent loss of competence. Gibson said that in his opinion, the Canadian law attempts to balance a respect for individual autonomy and suffering with protection for the vulnerable.
Since the law was passed, less than 1 percent of Canadian deaths have resulted from medically assisted death, with more than 99 percent of those deaths being clinician administered. The individuals who have taken advantage of the law have ranged in age from 18 to 102, with the average age being 73 and the majority over the age of 55. Approximately 60 percent of the patients had a cancer diagnosis, and another 18 percent had neurodegenerative disorders. About 50 percent of the deaths occurred in hospitals in large urban areas, Gibson said, though a movement is starting in favor of having deaths in private residences, hospices, or long-term care facilities.
REFERENCES
Onwuteaka-Philipsen, B. D. L., A. van der Heide, H. J. van Delden, K. Evenblij, I. El Hammoud, H. R. W. Pasman, C. Ploem, R. Pronk, S. van de Vathorst, and D. Willems. 2017. Third evaluation of the euthanasia law. ZonMw. The Hague, the Netherlands. [In Dutch].
Regional Euthanasia Review Committees. 2017. Regionaleuthanasia review committees annualreport2016. The Hague: Regional Euthanasia Review Committees. https://www.eutanasia.ws/_documentos/dossier_eutanasia/PaisesBajos_Balegica/17%20Netherland%20Annual%20Report%202016.pdf (accessed May 24, 2018).
van der Heide, A., J. J. M. van Delden, and B. D. Onwuteaka-Philipsen. 2017. End-of-life decisions in the Netherlands over 25 years. New England Journal of Medicine 377(5):492–494.










