5
Background on Selected Epidemiologic Studies and Populations
The process of updating the evidence base of possible health effects of the chemicals of interest (COIs)—2,4-dichlorophenoxyacetic acid (2,4-D); 2,4,5-trichlorophenoxyacetic acid (2,4,5-T) and its contaminant 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD); 4-amino-3,5,6-trichloropicolinic acid (picloram); and dimethyl arsenic acid (DMA or cacodylic acid)—has involved the evaluation and integration of thousands of epidemiologic publications over successive reports. The search strategy used to identify these publications, along with refinements that have been made since the initial volume of the series was prepared, are described in Chapter 3.
In addition to reviewing studies involving exposures to the specific COIs, the current and previous Veterans and Agent Orange (VAO) committees have considered studies that examined compounds chemically related to the herbicides used in Vietnam, such as 2-(2-methyl-4-chlorophenoxy) propionic acid, hexachlorophene, and chlorophenols, particularly 2,4,5-trichlorophenol. If a publication did not specify the herbicides or polychlorinated biphenyls (PCBs) with dioxin-like actions to which study participants were exposed or the magnitude of exposure, those limitations were considered when weighing the evidence of each publication. The committee considers studies of exposure to PCBs and other dioxin-like chemicals informative if their results were reported in terms of TCDD toxic equivalents (TEQs) or concentrations of specific congeners of dioxin-like chemicals. The details of the exposure assessments conducted within individual studies are presented in this chapter, whereas generic issues of exposure assessment are discussed in Chapter 3 along with the special challenges involved in characterizing and reconstructing the herbicide exposures of Vietnam veterans.
This chapter presents study design and other important methodologic information on populations of Vietnam veterans, occupational cohorts, and
environmentally exposed groups that have been reported on repeatedly, often for many health outcomes, as well as on case-control studies that have generated multiple epidemiologic publications relevant to the VAO series. This integrative approach has been taken to avoid repeating design information in multiple health-outcomes chapters and to make evident to the reader the extensive degree of interrelationship among many of the published analyses that have been reviewed in the course of the VAO series. If new results are based on updating information from or adding subjects to previously studied populations or use a subset of the original study population, then this synthesis considers the redundancy among studies while recognizing that separately reported information can impart new relevance to other data on a study population. Such clusters of studies are useful in describing the course of a population’s response to an exposure, and joint consideration of an entire body of research on a population may yield insights into relationships with potential confounding factors. The various study designs have strengths and weaknesses that influence the evidentiary weight that they contribute, and these factors are addressed in the health-outcomes chapters. One-time reports on a study population that addressed only a single health outcome are not described in this chapter, but instead are described and critiqued in the sections of the report that discuss the results related to that particular health outcome.
Many of the cohorts that have contributed to the cumulative findings of the VAO committees, occupational cohorts in particular, are no longer being followed. For completeness, these cohorts are mentioned briefly in this chapter and, where relevant, in the body of this report. Additional detailed background information on them is available in the earlier volumes of the series. This chapter is intended to give a brief overview of those major cohorts and studies that have contributed to the evidence base of potential health outcomes that stem from exposure to the COIs and for which new information has become available on the incidence or prevalence of disease and other health outcomes since Update 2014. It is not intended to be a compendium of every study or population ever reviewed in the VAO series.
Many groups potentially exposed to the COIs have been monitored periodically, including the cohorts of the International Agency for Research on Cancer (IARC) and the National Institute for Occupational Safety and Health (NIOSH); residents of Seveso, Italy; and Ranch Hand and Army Chemical Corps (ACC) personnel who served in Vietnam. Discussions of the specific cohorts in this chapter include references both to publications discussed in previous VAO reports and to new publications. In drawing its conclusions, the committee combined the evidence in new publications and the evidence synthesized from Update 2014, taking into account the interdependence of related publications.
Individual researchers who belong to the research consortia that are evaluating cohorts in large multicenter studies (such as the IARC and NIOSH cohort studies) sometimes publish reports based on subsets of study participants who they themselves are monitoring. VAO committees consider all published reports, including those based on entire cohorts and those based on subcohorts.
In drawing its conclusions, the committee factored in both types of studies, taking into consideration the interdependence among related studies. In particular, some subcohort studies have access to information not available for the entire cohort, such as data on individual serum TCDD concentrations and personal information that can be used to adjust for additional confounders. Furthermore, in the case of analyses based on an entire cohort that include data from a subcohort as a subset, using the reports on the subcohort as part of the evaluation might provide additional information on the consistency of the relationships among subcohorts, such as whether there are important subcohort-by-exposure interaction effects that were not considered in the full-cohort analysis. As long as the design and analysis methods of the study populations are recognized, VAO committees have been less concerned about over-weighting unstable positive findings based on small subgroups or giving “repeated consideration” to duplicative results than they would have been if a quantitative meta-analysis were being undertaken.
The chapter is organized to present the study populations in the order that roughly reflects the importance attributed to the data generated (Vietnam veterans, occupationally exposed workers, and people who have been environmentally exposed). It begins with Vietnam veterans and first covers studies conducted in the United States by the Air Force, the Centers for Disease Control and Prevention (CDC), the Department of Veterans Affairs (VA), and other groups, before describing studies of veterans from other countries (particularly Australia, New Zealand, and South Korea) who served in Vietnam. The section “Occupational Studies” covers studies of workers who, through employment or other work (other than military service), were exposed to the COIs and dioxin-like chemicals, including production workers, agriculture and forestry workers (including herbicide and pesticide applicators), and other groups (e.g., sawmill and paper and pulp workers). Again, studies of U.S. workers are presented before those of international cohorts. The section “Environmental Studies” covers studies of populations exposed to the COIs and dioxin-like chemicals from non-occupational sources and includes assessments of the general population, such as the National Health and Nutrition Examination Survey (NHANES), and also assessments of people who had unusually high exposures because of war-related or industrial sources in their residential neighborhoods (such as the residents of southern Vietnam; suburban Taichung, Taiwan; and Chapaevsk, Russia) or accidents (such as Seveso, Italy, and the Yusho poisoning in Western Japan). The chapter ends with a section that addresses the publications that are based on repeatedly mentioned case-control study populations; the case-control studies that assessed Vietnam-veteran status, however, are included in the section on veteran studies, and nested case-control studies are presented along with the cohorts from which they were derived.
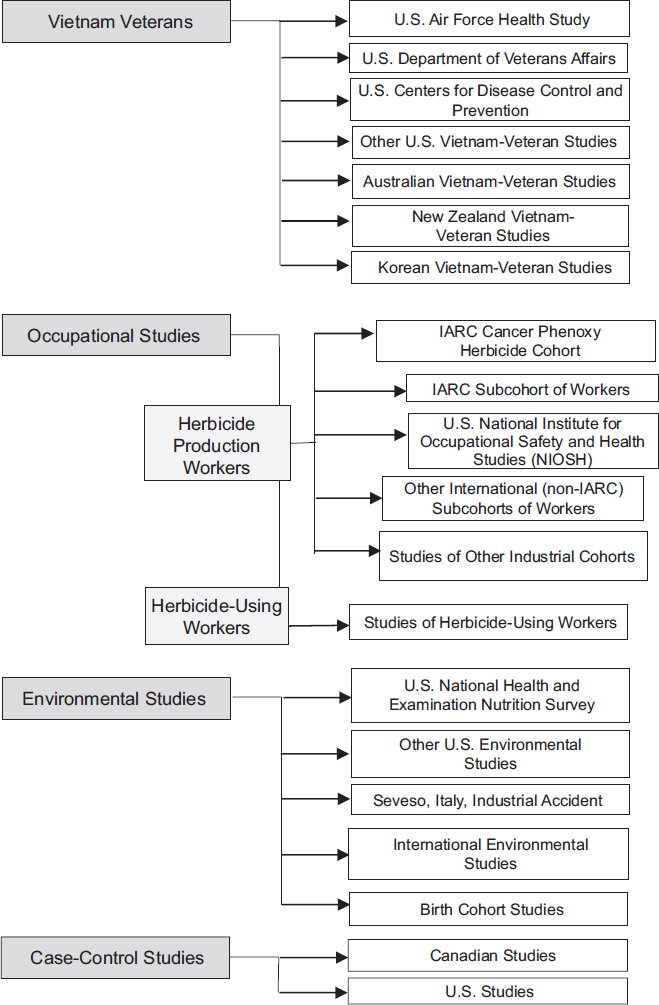
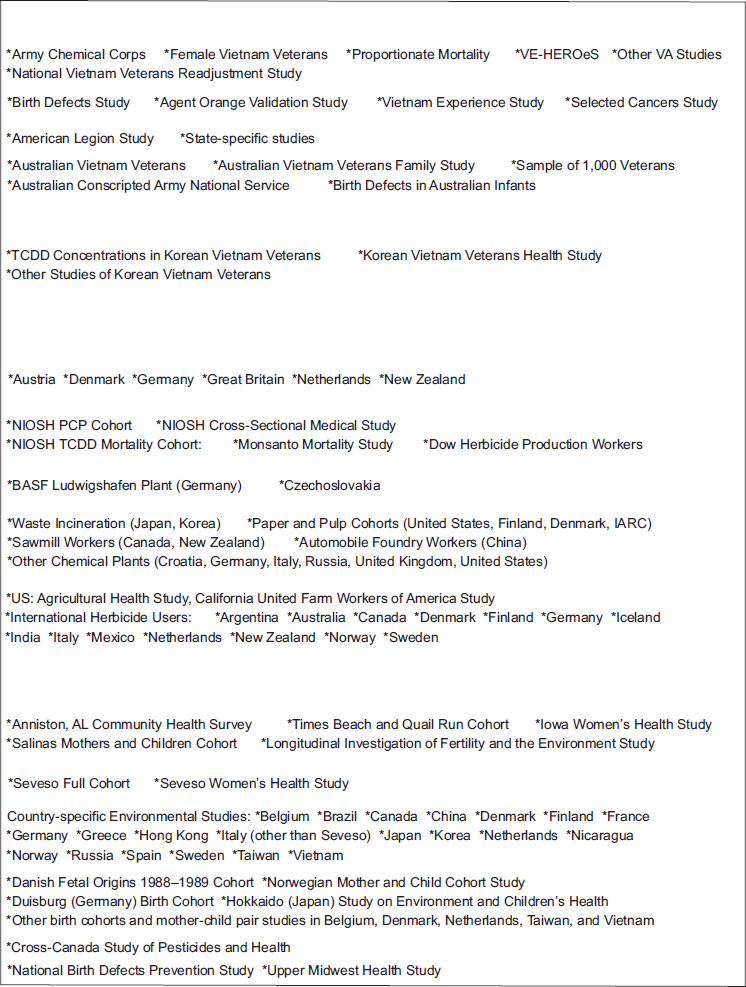
Because of the breadth of literature reviewed in this chapter, Figure 5-1 provides the reader with a comprehensive overview of the individual study populations that have been reviewed in the course of the VAO series, although not all of these populations are discussed in this chapter or even in this volume.
VIETNAM-VETERAN STUDIES
Studies of Vietnam veterans who might have been exposed to herbicides, including Agent Orange, have been conducted in the United States at the national and state levels and in Australia, South Korea, and New Zealand. Exposures have been defined in various ways, and health outcomes have been evaluated with reference to various comparison or control groups. This section is organized primarily by research organization or sponsor because it is more conducive to a methodical presentation of the studies. The means by which herbicide or dioxin exposures were characterized varies from the individually specified exposures of Ranch Hand and ACC personnel, as reflected in serum TCDD measurements, to the use of service in Vietnam as a surrogate for TCDD exposure in some studies.
Several comparison groups have been used for veteran cohort studies: Vietnam veterans who were stationed in areas where herbicide-spraying missions were unlikely to have taken place; Vietnam-era veterans who were in the military at the time of the conflict but did not serve in Vietnam; veterans who served in other wars or conflicts, such as the Korean War and World War II; and various state and national populations. In all of the studies of Vietnam veterans, whether or not the study participants were American, the study participants were the target population of the committee’s charge, and they were assumed to have had a higher probability of exposure to the COIs than people who did not serve in Vietnam, regardless of whether there was any information on individual exposures beyond the mere fact that they were deployed to Vietnam.
The studies in the publication period considered in the present update examined a range of health outcomes among Vietnam veterans with service history from the United States as well as those from New Zealand. These included new analyses of the Air Force Health Study cohort (AFHS) (Landgren et al., 2015; Mazur et al., 2013, 2014), ACC personnel (Cypel et al., 2016), several publications from VA Medical Centers (Krishnamurthy et al., 2016; Nosrati et al., 2014; Ovadia et al., 2015), and a 20-year hospitalization study of New Zealand Vietnam veterans (Cox et al., 2015).
Air Force Health Study
Reports and findings from the AFHS have provided important information that has been incorporated throughout the VAO series, including the current volume, and it continues to be considered an important cohort in the committee’s assessment of the overall evidence of exposure to the COIs and health outcomes. Active data collection from this cohort was completed in 2002, but VAO committees have remained interested in reviewing additional publications that provide longitudinal analysis of the vast amount of information assembled or that make use of the collection of preserved biologic samples. As yet, the few new published findings have been disease specific and not always focused on the effects of
exposure to the herbicides, but have grouped all participants to examine outcomes related to aging (IOM, 2015).
Major defoliation activities in Vietnam were conducted by Air Force personnel as part of Operation Ranch Hand. Veterans who took part in the defoliation activities became the first subpopulation of Vietnam veterans to receive special attention with regard to herbicide exposure and have become known as the Ranch Hand cohort within the AFHS. To determine whether exposure to herbicides, including Agent Orange, had adverse health effects on these veterans, the Air Force made a commitment to Congress and the White House in 1979 to conduct an epidemiologic study of Ranch Hand personnel (AFHS, 1982). The study protocol had three components: a retrospective mortality study, a retrospective morbidity study, and a 20-year prospective follow-up study with longitudinal data and biospecimens collection. Details on the mortality and retrospective morbidity arms can be found in prior reports (IOM, 2006b, 2015). The prospective study arm has been the focus of multiple reports on a variety of health outcomes in the cohort as well as new research using these assets.
Prospective Study Design and Data Collection
Records from the National Personnel Records Center and the Air Force Human Resources Laboratory were searched and cross-referenced to identify all Ranch Hand personnel (AFHS, 1982; Michalek et al., 1990). The exact number of Ranch Hands varies among published reports, depending on the time frame of identification, but the most widely used estimate is 1,242, which reflects the number who served in Vietnam and who were not killed in action. Ultimately, however, not all of those who have been identified actually participated in the AFHS (some were deceased before the study began, others were unlocatable, and a small number refused to participate) (IOM, 2015). A comparison population of 24,971 C-130 crew members and support personnel who served in the U.S. Air Force between 1962 and 1971 and were assigned to duty in Southeast Asia but who were not occupationally exposed to tactical herbicides (AFHS, 1983, 1984a) was selected from the same data sources. Each Ranch Hand was matched to a pool of 8 to 10 comparisons, who were selected based on the first living and compliant person randomly selected from the individual-level pool. Individual comparison participants remained associated with their matched Ranch Hand for the duration of the study, but those who died, dropped out, or were lost to follow-up were replaced with the next best comparable control who was living and agreed to participate (AFHS, 1982). Comparison participants were individually matched for age, type of job (differentiated into five categories: officer/pilot, officer/navigator, officer/other, enlisted/flight engineer, and enlisted/other), and race (white or not white) to control for possible differences in the development of chronic disease that may relate to age, race, or educational and socioeconomic status (AFHS, 1984a). To control for the many potential confounders related to the physical and
psycho-physiologic effects of combat stress and the Southeast Asia environment, Ranch Hands were matched to control participants who performed similar combat or combat-related jobs (AFHS, 1982). Comparisons were assumed to be similar to the Ranch Hands regarding lifestyle, training profiles, and socioeconomic factors. Although not representative of the U.S. population, the sample was diverse in terms of socioeconomic status and educational background (IOM, 2015).
The prospective follow-up consisted of six comprehensive exams that began with the baseline exam in 1982 and occurred thereafter in years 3, 5, 10, 15, and 20 of the study (the final physical exam was conducted in 2002 and final analysis for the formal AFHS study was completed in 2006). Morbidity was ascertained through comprehensive questionnaires and accompanying physical examination, which included more than 200 laboratory and clinical tests (although the number and type of laboratory tests performed at each physical examination changed over time, reflecting changes in science and technology). Questionnaire data included information relating to demographics; employment; child and family health; health habits; recreation, leisure, and physical activities; toxic exposures; military experience; and wartime herbicide exposure. Data collected during the physical examinations included indices of health status that encompassed general health and endpoints by major organ system. Additional sources of data collected in the course of the AFHS included medical records from the participants’ physicians, dentists, and other health providers; vital status records, such as birth and death certificates; information on the participants’ families, including spouses and children who were under 18 years old at the time of the exam; and military administrative records that contained duty station orders, flight records, performance reports, awards and decorations, and discharge documents (IOM, 2015). The number of Ranch Hand and comparison participants who completed the questionnaire and physical exam differed at each follow-up. In all, 2,758 individuals participated in at least one exam cycle.
Over the course of the AFHS, more than 91,000 unaliquoted biospecimens were collected as part of the physical exam component. The number of samples varied by type of specimen, participant, and cycle. Although some samples were collected as part of the laboratory testing and work-ups, additional biospecimens samples were collected from study participants at each exam cycle and preserved to be used for future analyses. Serum and urine were collected longitudinally across multiple cycles, while semen and whole blood were collected at a single exam cycle. Adipose tissue was collected from a subset of individuals at one exam cycle. To obtain samples for a TCDD assay carried out by the CDC on 777 Ranch Hand and 1,174 matched comparisons, a separate blood draw was performed during cycles 3–6 (see discussion on estimating exposure in the cohort, below). Multiple blood samples were drawn for a subset of the population for use in dioxin biological half-life and other studies.
Results have been published for baseline morbidity (AFHS, 1984a) and baseline mortality (AFHS, 1983) and for reproductive outcomes (AFHS, 1992;
Michalek et al., 1998a,c; Wolfe et al., 1995). Mortality updates have been published for 1984–1986, 1989, and 1991 (AFHS, 1984b, 1985, 1986, 1989, 1991b). An interim technical report updated cause-specific mortality in Ranch Hands through 1993 (AFHS, 1996). Michalek et al. (1998b) and Ketchum and Michalek (2005), respectively, reported on 15-year and 20-year follow-ups of post-service mortality in the Ranch Hand veterans, updating an earlier cause-specific mortality study by Michalek et al. (1990). Many analyses presented in the voluminous reports on the follow-up examinations of 1984, 1987, 1992, 1997, and 2002, which are cited as AFHS (1987, 1990, 1995, 2000, 2005), have been deemed not useful for the purposes of the VAO reviews because they were limited to comparisons of data on those in the cohort who were still alive and participated in a particular examination.
Exposure Estimation
As described in Chapter 2, the results of biologic-marker studies of Ranch Hand personnel have been consistent with their being exposed, as a group, to TCDD. When the Ranch Hand cohort was classified by military occupation, a higher level of serum TCDD was detected in people whose jobs involved more frequent handling of herbicides (AFHS, 1991a). The exposure index initially proposed in the AFHS relied on military records that documented spraying missions of TCDD-containing herbicides (Agent Orange, Agent Purple, Agent Pink, and Agent Green) as reported in the Herbicide Reporting System tapes for the period starting in July 1965. For exposure before July 1965, exposure information would be based on military procurement records and dissemination information. In 1991 the record-based exposure index was compared with the results of the Ranch Hand serum-TCDD sampling conducted on personnel at least 10 years after their service in Vietnam. The exposure index and the TCDD serum levels, which the authors referred to as body burden, correlated weakly.
Blood samples for use in determining serum TCDD concentrations were drawn at the periodic examinations conducted in 1982 (cycle 1) from 36 Ranch Hands (Pirkle et al., 1989), in 1987 (cycle 3) from 866 Ranch Hands (AFHS, 1991a), in 1992 (cycle 4) from 455 Ranch Hands (AFHS, 1995), and in 1997 (cycle 5) from 443 Ranch Hands (AFHS, 2000). For veterans whose TCDD was not measured in 1987 but was measured later, the later measurement was extrapolated to 1987 by using a first-order kinetics model with a constant half-life of 7.6 years.
Michalek et al. (1995) developed several indexes of herbicide exposure of members of the Ranch Hand cohort and tried to relate them to the measurements of serum TCDD from 1987 to 1992. Self-administered questionnaires completed by the Ranch Hand veterans were used to develop several indexes of herbicide or TCDD exposure: the number of days of skin exposure, the percentage of skin area exposed, and the product of the number of days of skin exposure, the percentage
of skin exposed, and a factor for the concentration of TCDD in the herbicide. A fourth index, which used no information gathered from individual study participants, was calculated by multiplying the volume of herbicide sprayed during a person’s tour of duty by the concentration of TCDD in herbicides sprayed in that period and then dividing the product by the number of crew members in each job specialty at the time.
Each of the four indexes tested was significantly related to serum TCDD concentrations, although the models explained only 19% to 27% of the variability in serum TCDD concentrations. Days of skin exposure had the highest correlation. Military job classification (for example, Ranch Hand combat troops, Ranch Hand administrators, Ranch Hand flight engineers, and Ranch Hand ground crew), which is not included in any of the four indexes, explained 60% of the variability in serum TCDD. When the questionnaire-derived indexes were applied within each job classification, days of skin exposure added statistical significance, but not substantially, to the variability explained by job alone.
Ranch Hands were divided into three categories on the basis of their potential exposure:
- Low potential. Pilots, copilots, and navigators. Exposure was primarily through preflight checks and spraying missions.
- Moderate potential. Crew chiefs, aircraft mechanics, and support personnel. Exposure could occur by contact during de-drumming and aircraft loading operations, onsite repair of aircraft, and repair of spray equipment.
- High potential. Spray-console operators and flight engineers. Exposure could occur during operation of spray equipment and through contact with herbicides in the aircraft.
At times, other metrics of exposure were also applied. For example, rank was used as a surrogate of exposure because officers (pilots, copilots, and navigators) were unlikely to handle the herbicides.
Pavuk et al. (2014) analyzed serum concentrations of TCDD and dioxin-like chemicals (i.e., polychlorinated dibenzo-p-dioxins [PCDDs], polychlorinated dibenzofurans [PCDFs], and PCBs) from samples collected in 2002 from 777 Ranch Hand and 1,173 comparison subjects. In addition, the results were compared with serum samples from 436 age- and gender-matched adults from the NHANES research initiative. The main findings showed that median serum TCDD levels were more than two times higher in the Ranch Hand veterans than in either the AFHS comparison veterans or the NHANES comparison group. However, the absolute values of serum TCDD levels, as well as the group differences in median serum TCDD levels, were substantially lower than results from prior serum samples collected in 1987. For the other dioxin-like chemicals, the concentrations in 2002 were similar in all three groups. These data demonstrate the unique TCDD signature experienced from herbicide exposure in Vietnam and
indicate that, over time, the elimination rate is higher than the ongoing intake rate from background exposure to TCDD in both groups of AFHS veterans.
Analyses of the serum TCDD readings were included in the 1987 examination report (AFHS, 1991a). Other Ranch Hand publications have addressed the relationship between serum TCDD and reproductive hormones (Henriksen et al., 1996); diabetes mellitus, glucose, and insulin (Henriksen et al., 1997); skin disorders (Burton et al., 1998); preterm birth and infant death (Michalek et al., 1998a); sex ratios (Michalek et al., 1998c); skin cancers (Ketchum et al., 1999); insulin, fasting glucose, and sex-hormone-binding globulin (Michalek et al., 1999a); immunologic responses (Michalek et al., 1999b); diabetes mellitus (Longnecker and Michalek, 2000; Steenland et al., 2001); cognitive function (Barrett et al., 2001); hepatic abnormalities (Michalek et al., 2001b); peripheral neuropathy (Michalek et al., 2001c); hematologic results (Michalek et al., 2001a); psychologic functioning (Barrett et al., 2003); correlations between diabetes and TCDD elimination (Michalek et al., 2003); thyroid function (Pavuk et al., 2003); cancer incidence (Akhtar et al., 2004; Pavuk et al., 2005); insulin sensitivity (Kern et al., 2004); prostate cancer (Pavuk et al., 2006); serum testosterone and the risk of benign prostate hyperplasia (Gupta et al., 2006); and diabetes and cancer incidence (Michalek and Pavuk, 2008).
The tendency of the AFHS researchers to use different cutpoints and population definitions for analogous analyses suggests that they used an a posteriori selection that may have influenced the results. For example, Michalek and Pavuk (2008) allude to the commonly held assumption that Agent Orange was more heavily contaminated earlier in the war as the motivation for making various temporal partitions in their analyses, but the choices were not consistent among studies. With respect to the development of cancer, service in 1968 or earlier was considered to have been in the critical exposure period, whereas for diabetes, the critical exposure period was considered to be 1969 or earlier. Additionally, the construction of low- and high-exposure variables based on “days of spraying” was done differently for cancer than it was diabetes. Days of spraying were grouped into 30-day blocks for cancer, and into blocks of 90 or more days for diabetes.
Impact of the AFHS on VAO Reviews
Ostensibly, the AFHS was designed to answer exactly the question that the VAO series is asking: Is exposure to the herbicides used during the Vietnam War associated with long-term health outcomes or outcomes in the offspring of exposed veterans? The AFHS is perceived by many to be the central piece of research for decision making by the VAO committees because it used longitudinally collected data and objective, quantifiable measures of TCDD exposure through serum samples, on a population that was directly exposed to the COIs in the Vietnam theater. Unlike many other studies of Vietnam veterans, data on alcohol
use and smoking status were collected and included in the analysis when they were known risk factors for the outcome of interest. However, the AFHS also has important limitations that all VAO committees have had to consider.
Although the study was carefully designed to match Ranch Hand and comparison subjects to minimize bias to the extent possible, the AFHS population is likely not representative of the entire population of Vietnam veterans, so its findings might not be generalizable to all Vietnam veterans. The 1987 TCDD serum assay found the comparison subjects to also have elevated levels of TCDD, although the exposure was significantly higher in the Ranch Hand group than in the comparison group. Therefore, the comparison is not an ideal exposed-versus-unexposed comparison but rather a high-exposure-versus-low-exposure comparison (IOM, 2006b, 2015). The exposure in the comparison group might also make the study findings vulnerable to bias toward the null if the difference in exposures between the AFHS group and the comparison group was not large enough to allow an association between exposure and outcome to be detected. That problem does not affect the validity of positive findings, however. Similarly, for AFHS analyses that used non-AFHS Vietnam veterans as the comparison group, those individuals might also have been exposed to the COIs, which would likewise influence results toward the null.
The AFHS might be underpowered for detecting small effects, especially rare outcomes, because of its relatively small sample size. Therefore, its findings are vulnerable to false negatives (failure to detect an important association). This also raises questions about the stability of positive findings; this is somewhat less of a problem if the findings are repeated over examination cycles, although the results of the examination cycles themselves are not fully independent repetitions.
Three new studies have been published using AFHS data since Update 2014. In the first study, Landgren et al. (2015) used data and serum samples from 479 Ranch Hands and 479 comparison veterans to examine the association between serum TCDD levels and the presence of monoclonal gammopathy of undetermined significance (MGUS). After the model had been adjusted for several demographic and clinical factors, Ranch Hands were found to have a 2.4-fold increased risk for MGUS. This study is the first to correlate an objective measurement of levels of TCDD exposure with MGUS and additional detail of it is found in Chapter 7. The second study used AFHS data from 991 AFHS participants to examine the relationship between testosterone levels and the levels of fasting glucose and, therefore, a diagnosis of type 2 diabetes (Mazur et al., 2014). The authors found that low testosterone levels in men were an independent risk factor (comparable to aging and obesity) for high fasting glucose and, therefore, that testosterone was a weak predictor of a diagnosis of type 2 diabetes. In a second publication based on AFHS data, Mazur et al. (2013) used data from the same 991 AFHS subjects to examine the relationship of obesity to individual and population-level declines in testosterone. Over 20 years of followup, mean testosterone levels declined at least twice as much as would have been
expected from cross-sectional estimates of the decline usually associated with aging. However, because neither of the Mazur studies considered exposure status or TCDD levels in the analysis, these studies were not considered to be relevant to the committee’s charge even though they were conducted using AFHS data.
Department of Veterans Affairs
Army Chemical Corps Cohort
Analyses of members of the ACC were conducted by VA, whose other research efforts on Vietnam veterans are discussed together below. Like the Ranch Hand personnel, ACC personnel performed chemical operations involving the direct handling and distribution of herbicides, but instead of using planes, they performed these tasks on the ground and by helicopter in Vietnam. Nearly 1,000 men serving in ACC units were deployed to Vietnam between 1966 and 1971. ACC members were responsible for the storage, preparation (handling and mixing), and application of herbicides, tear gas, and napalm among other chemicals. ACC units were also tasked with cleaning and maintenance of the equipment used to prepare and apply the chemicals (Thomas and Kang, 1990). Because the ACC personnel were expected to have been highly exposed to herbicides, VAO committees recommended studying this important group of Vietnam veterans (IOM, 1994) and later encouraged the publication of the study’s findings (IOM, 2005). The availability of serum TCDD concentrations in a subset of this cohort of Vietnam veterans has made its findings particularly useful in appraising possible associations with various health outcomes. The primary strengths and limitations of the ACC studies are similar to those of the AFHS.
ACC service members were belatedly identified using morning reports for all ACC units known to have been assigned to Vietnam between 1966 and 1971 for a study of health effects and mortality related to herbicide exposure (Thomas and Kang, 1990). However, the findings of increased risk of certain outcomes, such as digestive diseases, were based on small numbers of cases and cannot be associated with particular exposures since serum samples or other objective measures of exposure were not collected. In an extension of that study, Dalager and Kang (1997) compared the mortality of ACC veterans who deployed to Vietnam with the mortality of those who did not. For that study, ACC veterans were identified using a combination of the same morning reports for ACC units stationed in Vietnam as used by Thomas and Kang (1990), Defense Manpower Data Center tapes of Vietnam-era Army personnel with a military occupational specialty code indicating a chemical operations position between 1971 and 1974, and class rosters for chemical courses conducted at the Army Chemical School at Fort McClellan, Alabama, from 1965 to 1972. Analyses compared cause-specific mortality among Vietnam-deployed ACC men (n = 2,872) and those who never deployed to Southeast Asia (n = 2,737), and also compared each group to the
standardized U.S. population. Because all men who served in ACC units were stationed at Fort McClellan for at least some time, and Fort McClellan is in close proximity to Anniston, Alabama, where Monsanto operated a plant that produced PCBs, all ACC veterans were likely exposed to at least low levels of these and other chemicals. Therefore, comparisons using deployed and non-deployed ACC men are likely to be biased toward the null due to this baseline of increased exposure, but this bias is not the case for analyses that used the standardized U.S. population as the comparison group.
The results of an initial feasibility study that measured serum dioxin levels in a subset of Vietnam-deployed and nondeployed ACC veterans were reported by Kang et al. (2001). The researchers recruited 565 veterans: 284 Vietnam veterans and 281 non-Vietnam veterans as controls. Blood samples were collected in 1996 from 50 Vietnam veterans and 50 control veterans, and 95 of the samples met CDC standards of quality assurance. A comparison of both groups showed that the geometric mean TCDD concentrations did not differ between groups (p = 0.6). The 50 Vietnam-deployed veterans were then stratified into those who sprayed herbicides and those who did not, based on self-reported information. The sprayers had higher TCDD concentrations than those who reported no spraying activities. The authors concluded that Agent Orange exposure was a likely contributor to TCDD concentrations in Vietnam veterans who had a history of spraying herbicides.
Following the 2001 feasibility study Kang et al. (2006) reported the findings from the larger study of this population of ACC veterans. A health survey was administered by telephone to 1,499 Vietnam-deployed veterans and 1,428 non-Vietnam-deployed veterans. Exposure to herbicides was assessed by analyzing serum specimens from a sample of 897 veterans for dioxin. Consistent with the findings from the feasibility study, veterans who reported spraying herbicides had significantly higher TCDD serum concentrations than veterans who did not report herbicide spraying.
Having determined the vital status—that is, whether an individual was alive or had died—of the ACC personnel through 2005, Cypel and Kang (2010) presented results on mortality from the following causes: cancers (oral and pharyngeal, digestive, respiratory, prostate, testicular, skin, brain, and lymphopoietic [leukemia]), diabetes, circulatory conditions (hypertension and cerebrovascular), respiratory conditions (pneumonia, influenza, and chronic obstructive pulmonary disease), and cirrhosis of the liver. The study compared 2,872 ACC personnel who served in Vietnam with 2,737 ACC personnel who did not serve in Vietnam, using survival analysis that controlled for race, age at entry into follow-up, rank, and duration of military service. It also compared 662 ACC personnel who served in Vietnam and reported spraying herbicides with 811 who did not serve in Vietnam and did not report spraying herbicides, controlling for additional covariates of body mass index (BMI) and smoking status obtained in the telephone survey. Mortality in both cohorts was also compared with the expected mortality
in U.S. males. Concerns were raised over the lack of adjustment for smoking status in the analysis of respiratory diseases in Vietnam-deployed veterans and non-Vietnam-deployed veterans. (The subcohort analyses that compared sprayers with nonsprayers were adjusted for smoking status.)
In a new study of ACC veterans, Cypel et al. (2016) analyzed the results of a 2013 survey of 3,086 ACC veterans that compared prevalence of self-reported, physician-diagnosed hypertension in both Vietnam-deployed and non-Vietnam-deployed herbicide sprayers and non-sprayers. This study, which is reviewed in Chapter 10, reports that the mean serum TCDD level in ACC Vietnam-service sprayers was 4.3 parts per trillion (ppt) (lipid based) as compared with a mean level of 9.5 ppt in AFHS participants.
U.S. Female Vietnam Veterans Cohort
Although estimates have varied, the most recent estimates from VA are that 7,500 U.S. women served in Vietnam between August 1964 and May 1975 (VA, 2017a). The vast majority of them served as combat nurses—mostly in the Army Nurse Corps—but some also served in the Women’s Army Corps and the Air Force, Navy, and Marine Corps (Spoonster-Schwartz, 1987; Thomas et al., 1991; VA, 2017a).
In 1986, Public Law (PL) 99-972 was enacted. It required that an epidemiologic study be conducted to examine the long-term adverse health effects on female Vietnam veterans who had exposure to traumatic events, exposure to herbicides such as Agent Orange or other chemicals or medications, or any other related experience or exposure during such service. The first study that VA conducted to assess mortality in female Vietnam veterans was by Thomas et al. (1991). No comprehensive record of female personnel who served in Vietnam in 1964–1972 existed, so the researchers gathered military service data from each branch of the armed forces through December 31, 1987. Female Army and Navy personnel were identified from morning reports and muster rolls of hospitals and administrative support units where women were likely to have served. Military personnel were identified as female by their names, leaving open the possibility that some women may have been inadvertently excluded from the analysis. Women who served in the Air Force and Marine Corps were identified through military records. The combined roster of all female personnel from the military branches was considered by the researchers to be generally complete. A comparison group of female veterans was identified through the same process as the women who served in Vietnam but the comparison group had not served in Vietnam during their military service. Demographic information and information on overseas tours of duty, unit assignments, jobs, and principal duties were abstracted from military records. Mortality information was obtained from VA’s Beneficiary Identification Records Locator Subsystem, the Social Security Administration, the Internal Revenue Service, the National Death Index (NDI),
and military personnel records. Women whose service in the military fell outside the period of interest, whose records were missing data, or who served in Southeast Asia but not in Vietnam were excluded. The analysis included 132 deaths among 4,582 female Vietnam veterans and 232 deaths among 5,324 comparison veterans who served in the military from July 4, 1965, to March 28, 1973, which was when combat operations occurred. Cause-specific mortality was derived for both groups of veterans and compared with mortality in U.S. women with adjustments for race, age, and calendar period. Dalager et al. (1995a) updated mortality in the original cohort through December 31, 1991, using the same study protocol as Thomas et al. (1991). After updating the mortality figures and adjusting the existing cohort on the basis of new information about the study groups based on the inclusion criteria, an additional 4 Vietnam-deployed veterans and 1 comparison veteran were included in the final study population (Dalager et al., 1995a).
Updates of mortality among women Vietnam veterans have been published periodically. Cypel and Kang (2008) conducted a mortality study of female veterans who deployed to Vietnam, comparing them with a control group of women veterans matched on rank and military occupation who were in the military at the same time period but who were not deployed to Vietnam. Kang and colleagues (2014a) updated total and cause-specific mortality analyses of female U.S. Vietnam-era veterans through December 31, 2010, using the same sources to determine vital status as were used by Thomas et al. (1991) and Dalager et al. (1995a). For deaths that occurred before 1992, the cause of death was ascertained from official death certificates. For deaths occurring on or after January 1, 1992, cause-of-death information was obtained from NDI Plus, which codes the cause of death by the International Classification of Diseases (ICD) system. The underlying causes of death were formally assigned by a qualified nosologist. This mortality update was structured as a retrospective cohort study consisting of three study groups of female veterans who served during the Vietnam era using the same dates as Thomas et al. (1991) and Dalager et al. (1995a). The first group included 4,734 female veterans who served in Vietnam, the second group consisted of 2,062 female veterans who served near Vietnam, and the third group included 5,313 female veterans who did not deploy outside of the United States. Mortality comparisons were made using either the non-deployed U.S. cohort or women of the U.S. general population, adjusted for age, race, and calendar year, as the reference group. Of the total sample of 12,109 female veterans, 2,743 (23%) were deceased by the study end date of December 31, 2010, and the cause of death was available for 96.2% of the deaths. The adjusted total mortality and heart-disease-specific rates were lower in the female Vietnam veterans than in the U.S. Vietnam-era female veterans or in the U.S. general population. The cancer mortality rate was approximately equal between the female Vietnam veterans group and both the U.S. cohort of female veterans and the U.S. general population. When the analysis was constrained to nurses only (approximately two-thirds of the study cohort), higher adjusted mortality rates for pancreatic, brain, and
other nervous system cancers were reported for the female Vietnam veterans. Whereas all reports from the female U.S. Vietnam-veteran cohort provide direct information on the health and mortality status of female military personnel who served in Vietnam, the limitations of the results must be kept in mind. Specifically, female veterans likely experienced low herbicide exposure because they were not involved in applying herbicides or engaged in direct combat, and their in-country tours of duty were generally limited to 1 year and at fixed locations that were not in proximity to known defoliated areas. In summary, this analysis does not provide evidence of a higher risk of total or cause-specific mortality in female Vietnam-deployed veterans compared with non-deployed female Vietnam veterans and the U.S. general population. The suggestion of higher rates of mortality from pancreatic, brain, and other nervous system cancers among Vietnam nurse veterans should be cautiously interpreted, given the study’s limitations and the large number of causes of mortality examined.
VA also published studies of pregnancy outcomes and gynecologic cancers—namely, neoplasms of the cervix, uterus, and ovary—in U.S. female Vietnam veterans (Kang et al., 2000a,b). Army veterans were identified from a list obtained by the Army and Joint Services Environmental Support Group; computerized lists were also provided by the Air Force, Navy, and Marine Corps. Military-service data were abstracted from personnel records. Of 5,230 eligible veterans, 4,390 with a documented tour of duty in Vietnam were alive on January 1, 1992. From a pool of 6,657 women whose military units did not serve in Vietnam, 4,390 veterans who were alive on January 1, 1992, were randomly selected as controls. After the research group excluded 250 veterans and 250 nonveterans who participated in a pilot study as well as those who could not be located (n = 370), who were deceased (n = 339), or who declined to participate (n = 775, 13% of Vietnam veterans and 17% of non-Vietnam veterans), 6,430 women completed a full telephone interview, and another 366 women completed only a short, written questionnaire. The information collected included demographic background, general health, lifestyle, menstrual history, pregnancy history, pregnancy outcomes, and military experience, including nursing occupation and combat exposure. Information on pregnancy risks and complications—including smoking, infections, medications, exposure to X-rays, occupational history, and exposure to anesthetic gases, ethylene oxide, herbicides, and pesticides—was collected for each pregnancy. In Kang et al. (2000a), for each woman veteran, the first pregnancy following the beginning of Vietnam service was designated as the index pregnancy. For the comparison group, the first pregnancy after July 4, 1965, was designated as the index pregnancy. The study analyzed data on 3,392 Vietnam and 3,038 non-Vietnam veterans and on 1,665 Vietnam and 1,912 non-Vietnam veteran index pregnancies. In Kang et al. (2000b), a self-reported history of gynecologic cancers (defined by the authors as cancers of the breast, ovary, uterus, and cervix) was collected. The authors attempted to “retrieve hospital records on all reported cancers as far back as 30 years.” Of records successfully
found, 99% of the breast cancer and 90% of all cancer diagnoses were confirmed. The authors did not provide specific data on diagnosis confirmation for the three sites other than the breast, but they stated that Vietnam status was not associated with a greater likelihood of finding confirmatory medical records.
After the publications by Kang et al. (2000a,b), Congress passed PL 106-419, which provides compensation for the children of female Vietnam veterans who are born with birth defects unrelated to an existing familial disorder, to a birth-related injury, or to a fetal or neonatal infirmity with a well-established cause. The legislation covers 18 birth defects, including cleft lip or palate, congenital heart disease, hypospadias, neural-tube defects, and Williams syndrome. A complete list of covered birth defects can be found in 38 CFR 3.815.
Proportionate-Mortality Cohort
Among the earliest reports on health outcomes in Vietnam veterans was a proportionate-mortality study by Breslin et al. (1988). The participants were Army and Marine Corps ground troops (all men) who served at any time from July 4, 1965, through March 1, 1973. A list of 186,000 Vietnam-era Army and Marine Corps veterans who were reported deceased as of July 1, 1982, was assembled from VA’s Beneficiary Identification Records Locator Subsystem. From this list, 75,617 individuals were randomly selected for inclusion in the study. The information extracted from the selected military records included duty stations, dates of tours, branch of military service, date of birth, sex, race, military occupation specialty codes, education level, type of discharge, and confirmation of service in Vietnam. Additional information was extracted on veterans who served in Southeast Asia, including the first and last dates of service in Southeast Asia, the military unit, and the country where the veteran served. For the final sample of Army and Marine Corps veterans, the cause of death was ascertained from death certificates or Department of Defense (DoD) Report of Casualty forms for 24,235 men who served in Vietnam and 26,685 men who did not serve in Southeast Asia. Each veteran’s cause of death was coded by a nosologist who used ICD-8. Exposue to herbicides or other environmental factors was not considered in the analysis. Deaths from external causes (accidents, poisonings, and violence) were slightly eleveated among Vietnam veterans who served in the Army but not among marines who served in Vietnam. Death from any cancer was elevated among marines who served in Vietnam but not Army veterans. When examined by type of cancer, proportionate mortality ratios were not elevated for Army veterans, but proportionate mortality ratios for lung and non-Hodgkin lymphoma (NHL) were elevated among the Marine Corps veterans.
Using the proportionate-mortality cohort assembled by Breslin et al. (1988), Burt et al. (1987) conducted a nested case-control study of NHL with controls selected from among the cardiovascular-disease deaths. Although unrecognized at the time of that publication, using cardiovascular deaths as the control group
biased estimates of NHL toward the null because some cardiovascular diseases, such as hypertension, are associated with exposure to herbicides, see Chapter 10. When all Army and Marine Corps veterans who were deployed to Vietnam were compared with veterans who did not serve in Vietnam, no excess of mortality from NHL was found. When stratified by service branch and age, only marines with combat roles or who served in Vietnam from 1967 to 1969 (when herbicide spraying was greatest) had statistically significant increased odds of death from NHL. In a follow-up of the Breslin et al. (1988) study, Bullman et al. (1990) compared cause-specific proportionate mortality of 6,668 Army I Corps Vietnam veterans, who served in the northernmost part of South Vietnam in a combat zone designated as Military Region I by the U.S. military, with 27,917 Army Vietnam-era veterans who had not served in Vietnam. The subjects studied by Bullman et al. included the study population identified by Breslin et al. and an additional 9,555 Army Vietnam-era veterans whose deaths were identified after VA’s Beneficiary Identification Records Locator Subsystem database was searched for mortality data through December 31, 1984. Deaths from external causes (accidents, poisonings, and violence) were found to be slightly eleveated among Army I Corps Vietnam veterans, particularly deaths attributed to motor vehicle accidents and accidental poisonings. Similarly, Watanabe et al. (1991) updated the Vietnam-veteran mortality experience reported by Breslin et al. (1988) by extending the follow-up from January 1, 1982, to December 31, 1984. An additional 11,325 deceased Army and Marine Corps Vietnam-era veterans were identified from the period and included in the study. The study population for Watanabe et al. consisted of 62,068 military veterans, of whom 29,646 served in Vietnam and 32,422 never served in Southeast Asia. Proportionate-mortality ratios were calculated for three referent groups: branch-specific (Army and Marine Corps) non-Vietnam veterans, all non-Vietnam veterans combined, and the U.S. male population. Deaths from external causes were again statistically significantly elevated among Vietnam-deployed marines compared with non-Vietnam veterans and Army veterans who served in Vietnam compared with Army veterans who did not serve in Vietnam and all non-Vietnam veterans. Cancer of the larynx was statistically significantly higher among Vietnam-deployed Army veterans than either non-Vietnam Army veterans or all non-Vietnam veterans but lung cancer was only significantly different for Army Vietnam veterans compared with all non-Vietanm veterans. Deaths from lung cancer, NHL, and Hodgkin disease were all statistically significantly elevated for Marine Corps veterans who had served in Vietnam compared with marines who had not served in Vietnam only. A third follow-up proportionate-mortality study (Watanabe and Kang, 1996) used the veterans from Breslin et al. (1988) and Watanabe et al. (1991) and included an additional 9,040 randomly selected Vietnam-era veterans who died from July 1, 1984, through June 30, 1988. The final study included 70,630 veterans—33,833 who had served in Vietnam and 36,797 who had never served in Southeast Asia. The analyses were performed using the same referent groups described in Watanabe
et al. (1991). Just as in the previous analyses of mortality, Army and Marine Corps Vietnam veterans had statistically significant excesses of deaths from external causes. Army Vietnam veterans had statistically significant excesses of deaths for laryngeal cancer and lung cancer when compared to both Army non-Vietnam veterans and all non-Vietnam veterans. Results showing statistical significance for Marine Corps Vietnam veterans varied according to the referent population used (non-Vietnam marine veterans or all non-Vietnam veterans). When compared with non-Vietnam marine veterans, marine Vietnam veterans had significantly elevated proportionate mortality ratios for deaths from NHL, Hodgkin disease, and cancers of the pancreas, lung, and skin. Deaths from circulatory diseases were statistically significantly lower among Marine Corps Vietnam veterans than marines who did not serve in Vietnam and all non-Vietnam veterans. Marine Corps Vietnam veterans also had significant excesses for lung cancer and skin cancer compared with all non-Vietnam veterans. Proportionate mortality ratios for deaths due to respiratory and digestive diseases were statistically significantly lower among marine Vietnam veterans than all non-Vietnam veterans. Compared with the standardized U.S. population, deaths from many of the major categories of organ systems were statistically significantly lower among both the Vietnam-deployed and non-deployed veterans. However, cancers overall were higher among the Vietnam-deployed and non-deployed Army veteran groups and the Marine Corps non-Vietnam veteran group. Lung cancer deaths were significantly higher among both Army veteran groups and the Marine Corps Vietnam-deployed group compared with the U.S. population. Using the U.S. population for comparison, proportionate mortality ratios were statistically significantly higher for prostate cancer in Army non-deployed veterans and skin cancer for Marine Corps veterans that served in Vietnam.
National Vietnam Veterans Readjustment and Longitudinal Studies
In response to concerns about the health and well-being of Vietnam veterans, in 1983 Congress passed PL 98-60, which directed VA to contract for an independent national study looking at the frequency and effects of posttraumatic stress disorder (PTSD) and related postwar psychological issues. In 1984 the contract for the National Vietnam Veterans Readjustment Study was awarded to the Research Triangle Institute (RTI). Several publications resulted from that work (Currier and Holland, 2012; Schlenger et al., 2015a; Yager et al., 2016) but given the focus on mental health, most are not relevant to the VAO series.
In 2000 Congress passed PL 106-419, which directed VA to contract for a follow-up study, the National Vietnam Veterans Longitudinal Study, to determine the effects of PTSD over a 25-year period and postservice adjustment. The study was awarded to Abt Associates (VA, 2018b). A total of 1,450 veterans participated in at least one of the study phases of the National Vietnam Veterans Longitudinal Study, which included a self-administered paper health questionnaire,
a computer-assisted telephone health interview, and a telephone mental health interview conducted by a professional clinical interviewer (Marmar et al., 2015). Results from this second effort have been recently published (Marmar et al., 2015; Schlenger et al., 2015b, 2016; Steenkamp et al., 2017). But because the focus of this research is mental health outcomes, the results are not considered by VAO update committees. The data collected from veterans who participated in both the National Vietnam Veterans Readjustment Study and the National Vietnam Veterans Longitudinal Study are now part of the National Vietnam Veterans Longitudinal Study Registry, which was acquired in 2015 and is housed at VA’s Seattle Epidemiologic Research Information Center in Seattle, Washington (VA, 2018a). However, as noted previously, VAO committees do not consider mental health conditions in their review of health outcomes of Vietnam veterans.
Most recently, VA has undertaken a new research initiative to assess the current health of Vietnam veterans who served on the ground, Blue Water Navy veterans, and veterans who served elsewhere during the Vietnam Era (1961–1975). The Vietnam Era Health Retrospective Observational Study (VE-HEROeS) is designed to compare the overall health, lifestyle characteristics, and aging-related conditions of these veterans with similarly aged U.S. residents who never served in the military. The committee invited the lead investigator, Dr. Victoria Davey, to discuss the project. The study was designed to compare a retrospective cohort of Vietnam veterans, with all service branches represented, with Vietnam-era veterans who were deployed to countries other than Vietnam, Cambodia, or Laos and with members of the U.S. general population who never served in the military. Recruitment was based on a sampling frame that was constructed to be a randomly selected sample of persons from VA’s database of all veterans (both users of VA health care or benefits and those not using VA services). The questionnaire collected information on the following topics: military service (combat experience, chemical and other exposures, re-entry into civilian life, or no military service), general health (neurologic conditions, infections, presumptive conditions, cancer, hypertension, and mental health conditions), experience with aging, lifestyle factors (tobacco use, health care use, living arrangements), and health experiences of descendants (nine questions on birth defects and other conditions of children and grandchildren). A medical records review is being conducted of a small subset of participants (n = 4,000) to validate the questionnaire information (Davey, 2017). The data are being analyzed, and although some abstracts and posters containing a few findings have been submitted to VA research and outside conferences, no results had been published in the peer-reviewed literature as of January 31, 2018.
Other VA Studies
VA also conducted studies that focused on specific health outcomes, using data from VA’s Agent Orange Registry, a computer database containing health information on Vietnam veterans who voluntarily undergo examinations in a
VA hospital. This registry was established in 1978 to monitor health complaints or problems of Vietnam veterans that potentially could be related to herbicide exposure during their military service in Vietnam, but it was not intended to be a research program (Dick, 2015). The registry was established also as a means to facilitate increased access of Vietnam veterans to the VA health care system. Veterans are eligible to participate if they had any active military service in the Republic of Vietnam between 1962 and 1975 and express a health concern related to herbicide exposure. Beginning in 2011, eligibility has been expanded to include veterans who served along the Korean Demilitarized Zone between 1968 and 1971, veterans who served in certain units in Thailand, and veterans who were involved in the testing, transporting, or spraying of herbicides for military purposes (Dick, 2015). The examinations that these veterans undergo consist of an exposure history (based on self-reports that are not verified by DoD records), a medical history, laboratory tests if indicated, and an examination of the organ systems most commonly affected by toxic chemicals. The quality, consistency, and usability of data from this registry—and indeed from all registries with voluntary participation that rely on self-reported information—are limited. As of July 6, 2017, this registry contained information on 676,774 veterans who had undergone an initial examination and there had been 79,846 follow-up evaluations, for a total of 756,620 examinations (VA, 2017b). Some VA investigators have used participation in the registry as a surrogate of herbicide exposure (Clemens et al., 2014; Nosrati et al., 2014; Ovadia et al., 2015).
Other VA analyses have relied on self-reported exposure to herbicides (Beard et al., 2016, 2017; Krishnamurthy et al., 2016; Le et al., 2016; Q. Li et al., 2013). Two other VA studies (Baumann Kreuziger et al., 2014; Mescher et al., 2018) determined exposure to Agent Orange (or presumably other herbicides) by reviewing claims of exposure submitted by veterans that were reviewed by VA benefits and compensation officers who used service records to confirm that locations and timeframes of deployment corresponded to sprayed areas.
VA has evaluated specific health outcomes, including carrying out case-control studies of soft-tissue sarcoma (STS) (Kang et al., 1986, 1987), NHL (Dalager et al., 1991), Hodgkin lymphoma (HL) (Dalager et al., 1995b), testicular cancer (Bullman et al., 1994), and lung cancer (Mahan et al., 1997). Each study created and applied a different measure of surrogate herbicide exposure because objective measures, such as serum TCDD analyses, were not available. Other VA studies included a post-service mortality analysis (separate from the proportionate mortality cohort) of marines that compared those who served in Vietnam (n = 10,716) with Vietnam-era marines (n = 9,346) (Watanabe and Kang, 1995), and a small case-control study that compared dioxin and dibenzofuran concentrations in the adipose tissue of 36 Vietnam veterans and 79 non-Vietnam veterans and a sample of U.S. men born in 1936–1954 (Kang et al., 1991). All tissue samples were archived specimens from the EPA’s National Human Adipose Tissue Survey and
had been collected by hospitals and medical examiners from men who died from external (non-combat) causes or surgical procedures.
VA has examined other outcomes in Vietnam veterans: PTSD (Bullman et al., 1991; Goldberg et al., 1990; True et al., 1988), suicide and motor-vehicle crashes (Bullman and Kang, 1996; Farberow et al., 1990), tobacco use (McKinney et al., 1997), and self-reported physical health (Eisen et al., 1991). The studies have been included for completeness, but the outcomes that they address are outside the purview of this committee. VAO and Update 1998 discussed them in detail; most did not deal with exposure to herbicides specifically, and the exposure to “combat” was evaluated as the risk factor of interest. As noted VA has also initiated a study to update the mortality experience of Vietnam veterans. This update is expected to update the rates, causes, and patterns of overall and cause-specific mortality from 1979 through 2014 of all Vietnam veterans compared with all Vietnam-era veterans and the general U.S. population (Davey, 2017).
Centers for Disease Control and Prevention Studies
Surveys of U.S. Vietnam veterans who were not part of the Ranch Hand or ACC groups indicated that 25% to 55% believed they were exposed to herbicides (CDC, 1989b; Erickson et al., 1984a,b; S. D. Stellman and J. M. Stellman, 1986). Several attempts have been made to estimate the exposures of Vietnam veterans who were not part of the Ranch Hand or ACC groups. CDC has undertaken a series of studies to examine various health outcomes in Vietnam veterans as directed by Congress in the Veterans Health Programs Extension and Improvement Act of 1979 (PL 96-151) and the Veterans’ Health Care, Training, and Small Business Loan Act of 1981 (PL 97-72). The first of these CDC studies was a case-control interview study of birth defects in the offspring of men who served in Vietnam, which included developing an exposure opportunity index to score herbicide exposure (Erickson et al., 1984a,b).
Agent Orange Validation Study
The CDC Agent Orange study (CDC, 1985) was initiated in response to a 1983 request by the U.S. government to conduct a study of possible long-term health effects in Vietnam veterans exposed to herbicides. The study attempted to classify veterans’ service-related exposures to herbicides by determining the proximity of troops to herbicide spraying through the use of military records to track troop movement and the use of the HERBS tapes1 to locate herbicide-spraying patterns.
___________________
1 The HERBS tapes were a digital record of herbicide spray missions compiled by the Department of Defense in the early 1970s. Information on them is presented in the original VAO report (IOM, 1994).
In 1987, CDC conducted the CDC Agent Orange Validation Study to test the validity of the various indirect methods used to estimate the exposure of ground troops to herbicides in Vietnam. The study measured serum TCDD in a non-random sample of Vietnam veterans and in Vietnam-era veterans who did not serve in Vietnam (CDC, 1988b). Vietnam veterans were selected for the study on the basis of the number of herbicide exposure events that they were thought to have experienced, based on the number of days their unit was within 2 kilometers and 6 days of a recorded herbicide-spraying event. Blood samples were obtained from 66% of 646 Vietnam veterans and from 49% of the eligible comparison group of 97 veterans. More than 94% of those whose serum was obtained had served in one of five battalions.
The median serum TCDD concentration in Vietnam veterans in 1987 was 4 ppt (range: < 1 to 45 ppt, but only two veterans had concentrations above 20 ppt). The “low” exposure group consisted of 298 Vietnam veterans, the “medium” exposure group 157 veterans, and the “high” exposure group 191 veterans. The distribution of TCDD measurements was nearly identical to that in the control group of 97 non-Vietnam veterans. The CDC validation study concluded that study participants could not be distinguished from controls on the basis of serum TCDD. In addition, neither record-derived estimates of exposure nor self-reported exposure to herbicides could predict which Vietnam veterans would have high serum TCDD at the time of the study (CDC, 1988b, 1989a). The report concluded that it was unlikely that military records alone could be used to identify a large number of veterans who might have been heavily exposed to TCDD in Vietnam. The serum TCDD measurements in Vietnam veterans also suggested that the exposure to TCDD in Vietnam was substantially lower, on average, than that of persons exposed as a result of the industrial explosion in Seveso, Italy, or that of the heavily exposed occupational workers who have been the focus of many of the studies evaluated by VAO committees. The assessment of average exposure does not eliminate the possibility that some Vietnam veterans had heavy exposures.
Vietnam Experience Study
Using exposure estimates from the Agent Orange Validation Study, CDC conducted the CDC Vietnam Experience Study, a historical cohort study of the health experience of Vietnam veterans (CDC, 1989b). The study was divided into three parts: physical health, reproductive outcomes and child health, and psychosocial characteristics (CDC, 1988a,c,d). CDC examined post-service mortality (through 1983) in a cohort of 9,324 U.S. Army veterans who served in Vietnam and in 8,989 Vietnam-era Army veterans who served in Germany, Korea, or the United States (Boyle et al., 1987; CDC, 1987). In other studies using the data collected from the Agent Orange Validation Study, O’Brien et al. (1991) combined the mortality and interview data to identify veterans who developed
NHL. Decoufle et al. (1992) evaluated the influence of self-reported exposure to herbicides on self-reported adverse health outcomes. Finally, in a follow-up of CDC’s Vietnam Experience Study cohort, Boehmer et al. (2004) reported findings on mortality from 1965 through 2000.
Selected Cancers Study
The CDC Selected Cancers Study (CDC, 1990a) was designed to investigate the effects of military service in Vietnam and of exposure to herbicides on the health of American veterans, with a specific focus on the risk of developing NHL (CDC, 1990b), STS and other sarcomas (CDC, 1990c), HL (CDC, 1990d), and nasal, nasopharyngeal, and primary liver cancers (CDC, 1990d).
Other U.S. Vietnam-Veteran Studies
American Legion Study
The American Legion, a voluntary service organization for veterans, conducted a cohort study of the health and well-being of Vietnam veterans who were members. The studies examined physical health and reproductive outcomes, social-behavioral consequences, and PTSD in veterans who had served in Southeast Asia and elsewhere (Snow et al., 1988; J. M. Stellman et al., 1988; S. D. Stellman et al., 1988a,b). No additional studies have been published on the cohort.
State Studies
Several states have conducted studies of Vietnam veterans, most of which have not been published in the scientific literature. The VAO and Update 1996 committees reviewed studies of veterans of Hawaii (Rellahan, 1985), Iowa (Wendt, 1985), Maine (Deprez et al., 1991), Massachusetts (Clapp, 1997; Clapp et al., 1991; Kogan and Clapp, 1985, 1988; Levy, 1988), Michigan (Visintainer et al., 1995), New Jersey (Fiedler and Gochfeld, 1992; Kahn et al., 1988, 1992a,b,c), New Mexico (Pollei et al., 1986), New York (Greenwald et al., 1984; Lawrence et al., 1985), Pennsylvania (Goun and Kuller, 1986), Texas (Newell, 1984), West Virginia (Holmes et al., 1986), and Wisconsin (Anderson et al., 1986a,b). Chamie et al. (2008) examined the association between herbicide exposure and prostate cancer in Vietnam-era veterans using the VA health system in northern California; the reliability of this study of about 13,000 men is limited by its reliance on self-reported exposure status and by the exclusion of prostate cases diagnosed before 1998, before computerized records became available. No additional single-state studies have been identified.
Grufferman et al. (2014) evaluated the role of parental military service in Vietnam and service-related exposures and the risk of rhabdomyosarcoma in
offspring using data from the Intergroup Rhabdomyosarcoma Study Group clinical trial, which included hospitals in 46 U.S. states and the District of Columbia from 1982 to 1988.
Australian Vietnam-Veteran Studies
The Australian government has commissioned a number of studies to follow the health outcomes of Australian veterans who served in Vietnam. Although the Australians did not participate in herbicide spraying, there is a possibility that they may have been exposed to the herbicides if stationed or passing through areas that were sprayed.
Australian Vietnam Veterans
The Australian Vietnam veterans study population corresponds to the cohort defined by the Nominal Roll of Vietnam Veterans, which lists Australians who served on land or in Vietnamese waters from May 23, 1962, to July 1, 1973, including military and some non-military personnel of both sexes. People who served in any branch of service in the defense forces and citizen military forces (such as diplomatic, medical, and entertainment personnel) were considered. The comprehensive studies, however, are limited to male members of the military, and most of the analyses focus on men in the defense forces—the Army (41,084), the Navy (13,538), and the Air Force (4,570). One investigation examined the possibility of an association between Vietnam service and cancer incidence by comparing diagnoses from 1982 to 2000 among male Vietnam veterans with those in the general population of Australia (ADVA, 2005a). The results in that report supersede those reported by the Australian Department of Veterans’ Affairs (CDVA 1998a). Morbidity in female Vietnam veterans had also been studied (CDVA, 1998b). Additional case-control studies of the incidence of adrenal gland cancers, leukemias, and NHL were conducted in this population (AIHW, 1999, 2000, 2001).
There have been several studies of mortality among Australian Vietnam veterans (CDVA, 1997; CIH, 1984a,b,c; Crane et al., 1997a,b; Evatt, 1985; Fett et al., 1987a,b; Forcier et al., 1987). The latest one (ADVA, 2005b), which considered the causes of death of men in all branches of service through 2001 compared with that of the general Australian population and reported by branch of service, supersedes the others.
Australian Vietnam Veterans Family Study
The Australian Department of Veterans’ Affairs has published four large volumes that summarize the results of studies conducted among family members of Vietnam-era veterans (ADVA, 2014a,b,c,d). The purpose of this study was to
better understand the long-term impacts of service on the health and welfare of the families of Australian Vietnam veterans. The first volume (2014a) provided an overview of the entire effort. The second (2014b) assessed the health of the family members with more emphasis placed on the details of psychological and social well-being, rather than adverse impacts on physical health. The third (2014c) investigated mortality among members of the veterans’ families, while the final volume (2014d) discussed qualitative information gathered in the course of the entire study. Although responses were collected on spouses and partners of the veterans, the analyses focused on outcomes reported by the children of the veterans. The wide range of outcomes examined for the family members themselves included mental health outcomes, pregnancy and birth defect outcomes, physical health, social functioning, and mortality. Because many of the health outcomes reported for these family members are not central to the charge of the committee (e.g., mental health and social functioning), minimal consideration was given to these publications.
From the roster of Australian Vietnam veterans, more than 10,000 Australians who had served in the Vietnam War were randomly selected and contacted, along with their family members, for potential participation in the study. The Vietnam veterans who were identified and ultimately selected included 3,940 who were randomly selected and 2,569 who self-selected into the study based on media publications announcing that the study would be conducted.
The primary comparison group consisted of family members of nondeployed Vietnam-era personnel. These personnel comprised 3,967 randomly selected non-deployed era veterans and 418 who self-selected into the study. Thus, there were far more Australian Vietnam veterans who self-selected into the study than non-deployed Australian Vietnam-era veterans who self-selected, and the percentage of the Vietnam veterans who self-selected was much higher than the percentage of non-deployed Vietnam-era veterans who self-selected. In total, the family members of Vietnam veterans included 2,199 sons and daughters, of whom 1,385 were examined for pregnancy and birth defect–related outcomes.
When there is no specific exposure information provided, the VAO series has considered these comparisons of deployed versus non-deployed groups to cover potential exposure to all the COIs and thus the most relevant measures for their task. Such contrasts, however, also cover all aspects of the deployment experience, and in this set of Australian studies there was considerably more concern about the psychological effects on the veterans (especially PTSD) and their secondary impact on the veterans’ family members, which would not be expected to be an effect of herbicide exposure. Some analyses have been conducted among all study participants, and some analyses were stratified by the type of enrollment (random versus self-selected). The committee fully recognized the potential reporting biases that may have emanated from the self-selected cohort, and thus it placed considerably more weight on the results derived for the randomly selected cohort, as did the researchers themselves.
Australian Conscripted Army National Service
The Australian Conscripted Army National Service study population is a subset of the veterans considered in the overall Australian Vietnam Veterans study group. The 19,240 conscripted male Army veterans deployed to Vietnam (“National Service” veterans) were compared with 24,729 non-deployed counterparts (“National Service non-veterans”). The results on death and cancers in the Australian conscripted Army National Service veterans (ADVA, 2005c) supersede those of earlier internal comparisons of deployed and non-deployed Vietnam War–era National Service veterans (CIH, 1984a,b,c; Crane et al., 1997b; Fett et al., 1987a,b). Those government-sponsored studies of Australian Vietnam veterans did not characterize the veterans’ exposure to the herbicides sprayed in Vietnam beyond the fact that they had served on land or in Vietnamese waters from May 23, 1962, through July 1, 1973. It is the convention of VAO committees to regard Vietnam veterans in general as being more likely to have received higher exposures to the COIs than the general public, but ideally that assumption should have been validated by more objective measurements of exposure, such as serum measurements, in a sample of Australian Vietnam veterans.
Sample of 1,000 Australian Vietnam Veterans
O’Toole et al. (1996a,b,c) studied a broad spectrum of health issues in a random sample of 1,000 Australian Vietnam veterans (both regular enlisted and conscripted Army National Service members) selected from Australia’s comprehensive roster of 57,643 service members who were deployed to Vietnam. In wave 1, conducted in 1990–1993, 641 members of the sample were located and interviewed. In wave 2, conducted in 2005–2006, O’Toole et al. (2009) obtained responses from 450 (51.4% of those not known to have died). A total of 391 veterans responded to both waves. The Australian Bureau of Statistics’ National Health Survey was administered in both waves, and additional data were collected on combat experience, PTSD, and general psychiatric status. The veterans’ self-reported health status was compared with that of the general male Australian population gathered during the government’s administration of the same survey in 1989–1990 and 2004–2005; it is not clear that this instrument was administered to the two groups under comparable conditions. The low response rates make the findings vulnerable to nonresponse bias, and the self-report measures of health conditions might be of low validity and subject to recall bias. The committee for Update 2010 was skeptical about the reliability of the nearly uniform findings of statistically increased prevalence of nearly 50 health conditions.
O’Toole et al. (2010) reported on mortality in the sample through 2004 as related to previously gathered information on psychosocial factors that are not within the scope of VAO reviews. It is of interest, however, that they found that 11.7% of the veterans in the sample had died by the end of 2004. Additional
publications using the survey results from waves 1 and 2 have been published on the course of combat-related PTSD (O’Toole and Catts, 2017) and the intergenerational transmission of PTSD in the offspring of these veterans (O’Toole et al., 2017). However, as mental health outcomes related to combat cannot easily be teased apart from any potential effects of herbicide exposure, such publications are not reviewed in depth.
Birth Defects in Australian Infants
The Australian government sponsored a case-control study of 8,517 infants with congenital anomalies born in 1966–1979 at 34 hospitals in New South Wales, Victoria, and in the Australian Capital Territory; the infants were matched by period of birth, mother’s age, hospital, and means of hospital payment to live-born infants without diagnosed birth defects (Donovan et al., 1983, 1984; Evatt, 1985). The fathers of infants in both groups were identified and their names compared with those on the roster of men who had served in the Australian Army in 1962–1972; additional means of verification were used to determine whether a child’s father was in the Army during this interval (329 cases and 338 controls) and also whether the father was deployed to Vietnam (127 cases and 123 controls). After adjustments were made for maternal age, infant sex, multiple births, and father’s place of birth, conditional logistic regression was used to compare the Vietnam veterans (National Service or regular Army) to other era veterans and to all other fathers for all birth anomalies and for seven diagnostic groups.
Korean Vietnam-Veteran Studies
Military personnel of the Republic of Korea served in Vietnam from 1964 through 1973. Studies of the health of these personnel have been pursued by several researchers.
Study of TCDD Concentrations in Korean Vietnam Veterans
J. S. Kim et al. (2001) attempted to use serum dioxin concentrations to validate an index for estimating group exposure. The study involved 720 veterans who served in Vietnam and 25 veterans who did not. The exposure index was based on herbicide-spraying patterns in military regions where Korean personnel served, time and location data on the military units stationed in Vietnam, and an exposure score derived from self-reported activities during service. A total of 13 pooled samples were submitted to CDC for serum dioxin analyses. One analytic sample was prepared from the pooled blood of the 25 veterans who did not serve in Vietnam. The remaining 12 samples were intended to correspond to 12 exposure categories; each was created by pooling blood samples from 60 veterans. The 12 exposure categories ultimately were reduced to four exposure groups, each
representing a quartile of 180 Vietnam veterans but characterized by only three serum TCDD measurements.
The paper by J. S. Kim et al. (2001) reported highly significant Pearson correlation coefficients and results of multiple logistic-regression analysis. The statistical analyses apparently were based on the assignment of the pooled serum dioxin value to each individual in the exposure group. The multiple regression analysis evaluated such variables as age, BMI, and consumption of tobacco or alcohol. In a later report on the same exposure groups and serum dioxin data, the authors corrected their analysis (J. S. Kim et al., 2003). A correlation was observed between serum dioxin concentrations and ordinal exposure categories, but the correlation was not statistically significant. The authors attributed the lack of statistical significance to the small sample size, and they noted that the data exhibited a distinct monotonic upward trend; the average serum dioxin concentrations were 0.3, 0.6, 0.62, 0.78, and 0.87 pg/g (lipid-adjusted) for, respectively, exposure categories 0 through 4. The decision to pool blood samples from a large number of persons in each exposure set (J. S. Kim et al., 2001) greatly reduced the power of the validation study. Instead of 180 samples in each of the final exposure categories, the pooled analysis produced only three samples in each category. The lipid-adjusted serum TCDD concentrations in the 12 pooled samples from Vietnam veterans ranged from 0.25–1.2 pg/g, whereas the single sample from the non-Vietnam veterans contained 0.3 pg/g. The narrow range of results makes the biologic relevance of any differences questionable.
Thus, it appears that there was not a clear separation in terms of TCDD levels between Korean Vietnam veterans and non-Vietnam veterans. Furthermore, the range of mean values in the four Vietnam veteran exposure categories was narrow, and all concentrations were relatively low (less than 1 pg/g). The relatively low serum dioxin concentrations observed in the 1990s in those people are the residuals of substantially higher initial concentrations, as has been seen in other Vietnam veteran groups. However, the concentrations reported in the Korean veterans study are significantly lower than those reported in American Vietnam veterans in the 1988 CDC Agent Orange Validation Study, which was nonetheless unable to distinguish Vietnam veterans from non-Vietnam veterans on the basis of serum dioxin (CDC, 1988b). The Korean authors were able to construct plausible exposure categories based on military records and self-reporting, but they were unable to validate the categories with serum dioxin measurements.
Korean (Vietnam) Veterans Health Study
Six publications have been reviewed from an exceptionally large epidemiological study of more than 180,000 Korean Vietnam veterans, denoted herein as the “Korean study.” It is much larger in scope than all of the other published epidemiological studies conducted among Vietnam veterans. The Korean study provides results for a very large set of health outcomes, including rare conditions,
as well as non-fatal outcomes and cause-specific mortality. The research methodology used in the Korean study was very carefully evaluated by the Update 2014 committee (the first committee to examine these publications) because the study used multiple methods of exposure ascertainment and health outcome ascertainment. The careful evaluation was done so that across all health outcomes, committee members would weigh the results from the Korean study in a consistent manner and take into account the strengths and limitations from this large body of data.
For the Assessment of the Potential Exposure to Herbicides Publications on the Korean study have relied on multiple methods for the exposure assessment (referred to imprecisely in the Yi articles as Agent Orange). First, a self-report perceived exposure index was used to query Korean veterans as to how they might have been exposed to herbicides in Vietnam (Yi et al., 2013a,b). Responses to six questions on a postal survey were used to derive a four-tiered categorization of self-perceived herbicide exposure (Yi et al., 2013a); see Table 5-1. The initial four-tier scale (high, moderate, low, and none) was further compressed into simply “high” or “low” for many analyses. The perceived herbicide exposure estimates were highly correlated with the health outcomes, indicating the possibility of recall bias.
In the second method, an objective exposure opportunity index (EOI) score of exposure potential was calculated for each veteran based on the proximity of the veteran’s military unit to herbicide-sprayed areas (Yi et al., 2014a,b). The Korean investigators obtained locations and calendar date histories for the military units represented in their cohort and used this information as input to obtain EOI scores from its model (J. M. Stellman et al., 2003b), which consolidates all the temporal and spatial information gathered from the original military records on the herbicide spray missions conducted in Vietnam. The investigators classified the resulting EOI scores using two- and four-group categorizations
TABLE 5-1 Distribution of Perceived Herbicide Exposure Among 114,562 Korean Vietnam Veteransa
| 2 Groups | Exposure Questions | 4 Groups | Prevalence |
|---|---|---|---|
| High | 1. Sprayed herbicides | High | 16.1% |
| 2. Handled herbicide spray equipment | |||
| 3. Present during herbicide spraying | Moderate | 35.7% | |
| 4. Got herbicide on skin or clothing | |||
| Low | 5. Walked through sprayed area | Low | 13.2% |
| 6. Exposed in other ways (not listed above) | |||
| Answered “no” to all six questions | None | 34.9% |
aExposure assigned based on their self-reported responses to a postal survey.
SOURCE: Adapted from Yi et al., 2013a.
and multiple aggregations of military units. The initial four-tier scale (high, moderate, low, and none) was further compressed into simply “high” or “low” for many analyses, the details of which are presented in Tables 5-2 and 5-3. The self-reported perceived exposures are not directly comparable to the objective EOI scores, which were designed to assess the exposure opportunity that would result from unintended proximity to herbicide spraying and not the direct result of duties that required handling or applying herbicides (IOM, 2008).
TABLE 5-2 Distribution of EOI Scores on Two-Level Scale in Epidemiology Studies Among Korean Vietnam Veteransa
| Exposure Category (log10 EOI Score) | Yi et al. (2014a)b Division/Brigade or Battalion/Company (n = 111,726)d | Yi et al. (2014b)c Division/Brigade (n = 180,251)e |
|---|---|---|
| Low (< 4.0) | 62.0% | 52.4% |
| High (≥ 4.0) | 38.0% | 47.6% |
aDetails of the two-level exposure classification is described in the Ohrr et al. (2006, publication in Korean).
bBattalion/company level EOI score assigned for combat units only.
cThe overall range of log EOI scores in Yi et al. (2014b) is 0.0–5.8.
dYi et al. (2014a), 111,726 veterans analyzed for disease prevalence.
eYi et al. (2014b), 180,251 veterans analyzed for cancer outcomes.
SOURCES: Adapted from VAO Update 2014 (NASEM, 2016a).
TABLE 5-3 Distribution of EOI Scores on Four-Level Scalea
| Source | Yi et al. (2013a) | Yi et al. (2014a) | ||
|---|---|---|---|---|
| Exposure Category (log10 EOI score) | Division/Brigade (n = 96,126)b | Battalion/Company (n = 96,126) | Division/Brigade or Battalion/Companyc (n = 111,726)d | Division/Brigade (n = 180,251)e |
| None (< 0.1) | 20.1% | 26.1% | 30.9% | 25.2% |
| Low (0.1 ≤ EOI < 4.0) | 28.2% | 33.1% | 31.2% | 27.2% |
| Medium (4.0 ≤ EOI < 5.0) | 31.1% | 21.5% | 20.1% | 28.3% |
| High (≥ 5.0) | 20.6% | 19.3% | 17.9% | 19.3% |
aDetails of the four-level exposure classification is described in Ohrr et al. (2006, publication in Korean).
bYi et al. (2013a), 96,126 veterans analyzed for self-reported disease prevalence. Log (EOI score) mean and range not reported.
cBattalion/company level EOI score assigned for combat units only.
dYi et al. (2014a), 111,726 veterans analyzed for disease prevalence. Log (EOI score) mean 2.6 ± 2.2 (range 0.0–6.2).
eYi et al. (2014b), 180,251 veterans analyzed for cancer outcomes. Log (EOI score) range 0.0–5.8.
SOURCE: Adapted from VAO Update 2014 (NASEM, 2016a).
In developing the EOI scores, military units were aggregated at two levels: the larger brigade/division level and the smaller battalion/company level. The distributions of EOI scores are similar across the Korean study publications, regardless of military unit aggregation. The Update 2014 committee noted that the proportion of veterans in the “high” exposure category may be too large and the individuals too similar to the lower categories to detect the true strength of associations between exposure and adverse health conditions. The committee proposed that an exposure classification that put only the top 10% or 15% of individuals in the “high” category would have been better for the purpose of identifying adverse health effects due to exposure.
The Korean study overcame significant logistical challenges in applying the EOI model to a large-scale epidemiologic study of a broad spectrum of health effects. The Update 2014 committee found that although there were likely sources of error in the EOI method for modeling herbicide exposures of Vietnam veterans, there was no indication of systematic bias in the rank ordering of exposure scores developed by this method. Furthermore, since nondifferential misclassification of exposure would bias measures of association toward the null, the observed statistically significant relationships found between EOI scores and health effects are likely to be real.
For the Assessment of the Health Outcomes of Interest As with exposure assessment, multiple methods were used to ascertain health outcomes in the Korean study. First, veterans self-reported all current and physician-diagnosed diseases. The diseases were classified into seven groups of diseases: cancers, circulatory diseases, respiratory diseases, digestive diseases, neuromuscular diseases, endocrine diseases, and other diseases. Within the major disease groups, self-reporting was further provided for 17 cancers (including stomach cancer, liver cancer, and lung cancer), 13 circulatory diseases (including hypertension, myocardial infarction, and angina), 5 respiratory diseases (including chronic bronchitis and emphysema), 6 digestive diseases (including gastritis and peptic ulcer), 4 neuromuscular diseases (including central nervous system disorders and peripheral neuropathy), 2 endocrine diseases (diabetes and hypothyroidism), and 4 other diseases (including renal failure and skin disease).
Second, incidence data for the specific types of cancer reported in the cohort were obtained from the Korean Cancer Incidence Database (1992–2003) and classified according to ICD-10.
Third, prevalent cases of individual disease conditions were identified by extracting claims data from the Korea National Health Insurance service during the period January 1, 2000, to September 30, 2005. Data on health outcomes were also obtained through a review of medical care covered directly by the Korean government through the Veterans Health Service during the same period. The health outcomes that were examined included the prevalence of endocrine
diseases (ICD-10 E00–E90), neurologic diseases (G00–G99), circulatory diseases (I00–I99), respiratory diseases (J00–J99), and digestive diseases (K00–K93).
Fourth, vital status of Korean Vietnam veterans and the underlying causes of deaths were ascertained by use of the 1992–2005 death records of the National Statistical Office. Categories included all causes of death, 23 specific cancers, and 36 specific causes other than cancer.
Using these multiple methods for exposure classification and health outcome ascertainment, associations between metrics of herbicide exposure potential and health outcomes were derived. First, in some analyses, the health experiences of Korean Vietnam veterans, as a function of their exposure status, was compared to the health status of age-matched adults in the Korean general population. This method is known as an “external” control group. Second, some analyses were performed among Korean Vietnam veterans with the lowest herbicide exposure classification serving as the comparison group. This method is known as an “internal” control group.
The above variations in exposure assessment, health outcome ascertainment, and the use of internal and external comparison groups have significant implications for the appropriate interpretation of results from the Korean study. In considering these variations, the committee kept in mind the following methodological principles and empirical observations:
- Whereas self-reported exposure may be reliable and valid in some research circumstances, it is generally considered less reliable and valid than objectively obtained estimates of exposure (Zajacova and Dowd, 2011). The potential for recall bias is of particular concern, and the likelihood of this bias occurring increases with the length of time from the potential exposure to the incidence of disease.
- In acquiring health outcome data, objective sources (e.g., a cancer registry or health claims system) are generally preferred over self-report outcome data, assuming that the objective source of outcome data is largely comprehensive.
- For morbidity and mortality analyses, the estimation and validity of relative risk may be more prone to bias when an external control group is used (e.g., the general population) than when an internal control group is used (Monson, 1990). This may be due to the “healthy warrior” effect. That is, in order to be accepted to military service and deploy, members must meet a high standard of general and physical fitness, whereas the general population includes some individuals of poor health. Using an internal control group, so long as the veteran groups are similar or adjusted for potential confounding variables, alleviates concerns of bias due to the healthy warrior effect.
- Relative risk estimates that are only slightly above (e.g., 1.1) or below (e.g., 0.9) the null value of 1.0 may achieve statistical significance because of the large number of subjects in the study population, but may
- still reflect bias (e.g., selection or confounding bias) and be of less clinical significance than relative risk estimates of larger magnitude.
Therefore, when reviewing results within and across publications from the Korean study, the Update 2014 committee gave very limited overall weight to self-reported exposure data and self-reported health-outcomes data compared to objective measurements of the chemicals and health outcomes of interest. Also, more weight was given to the relative risk estimates of mortality and cancers derived from the use of an internal control group than from the use of the general population in order to minimize concern about a healthy warrior effect. Finally, less weight was afforded to statistically significant associations close to the null value (e.g., ranging from 0.9 to 1.1) than to those further from the null in order to account for differences of questionable clinical significance arising from this large study’s statistical power and to account for modest selection bias and confounding.
Brief Reviews of Individual Publications on the Korean Veterans Health Study
No new publications on the Korean study were identified for the current update. Relevant results from these publications are presented in each of the applicable health outcome sections under the heading of Conclusions from VAO and Previous Updates. However, to avoid redundancy, each of the publications is reviewed here, with a focus on the methods used.
In Yi (2013), a total of 185,265 Korean men, who had served in Vietnam from 1964 to 1973 and who were alive in 1992 were followed for cancer incidence from 1992 to 2003. Cancer diagnoses were ascertained via linkage with the Korean National Cancer Incidence Database, whereas cancer deaths were identified using National Statistical Office records. Cancer incidence and cancer mortality were not examined in terms of the veterans’ herbicide exposure during military service in Vietnam. Age-adjusted incidence and standardized incidence ratios were calculated using the Korean male population during 1992 to 2003 as the reference population (Yi, 2013). The overall cancer incidence among Vietnam veterans was not higher than in the general male population. However, when the incidence was analyzed by cancer type, Vietnam veterans and subgroups of the study population classified by military rank (enlisted; non-commissioned officer; officer) experienced a higher incidence of several cancers, including prostate cancer, T-cell lymphoma, lung cancer, bladder cancer, kidney cancer, and colon cancer, than the general Korean population. In Yi et al. (2013a), exposure of 114,562 Korean Vietnam veterans was assessed using two methods, as previously described in the section For the Assessment of the Potential Exposure to Herbicides. The first method was perceived self-report herbicide exposure in which veterans were categorized as having either “low” or “high” perceived exposure.
The second method used to estimate herbicide exposure was more objective and based on the proximity of each veterans’ military unit to herbicide-sprayed areas using the EOI model developed by J. M. Stellman et al. (2003b) and veterans were again classified using “high” and “low” group exposure categorizations. Associations were reported between self-reported diseases and high versus low exposures. All disease outcomes were based on self-report and classified into seven groups of diseases: cancers, circulatory diseases, respiratory diseases, digestive diseases, neuromuscular diseases, endocrine diseases, and other diseases. Subtypes of disease were reported for each disease condition. The Update 2014 committee was concerned about the reliability of self-reported exposure and health data because the use of such data in Yi et al. (2013a) uniformly yielded highly significant statistical associations across an exhaustive spectrum of disease conditions, while the use of the objective EOI method of exposure classification and documented reports of adverse health outcomes in the later publication on this population produced more variable results. The observation of inconsistencies when theoretically more reliable measures of health and exposure were analyzed reinforced the concern about the findings based on self-report in the Korean study.
Yi et al. (2013b) examined the serum levels of TCDD in 102 of these Korean Vietnam veterans for three purposes:
- to assess their use as a potential objective tool for herbicide exposure;
- to determine their correlation to self-reported exposure (six-item questionnaire); and
- to evaluate how they related to age, BMI, and smoking.
In 2002 serum samples were collected, and a health examination was performed. For an objective assessment of herbicide exposure, EOI scores were again derived using the model by J. M. Stellman et al. (2003b), and veterans were classified as low versus high exposure or in four categories consisting of none, low, moderate, or high exposure. The serum TCDD concentrations among the Korean Vietnam veterans were lower than those reported in other studies of Korean and U.S. Vietnam veterans, and concentrations were not associated with herbicide exposure indices or with age, BMI, or smoking. The net value of this study is the observation that the assessment of serum levels of TCDD among veterans long after service in Vietnam (e.g., 40 years or more) may be of very limited value as a metric for herbicide exposure unless individuals were exposed to very high levels during military service.
Yi and Ohrr (2014) examined the incidence of cancer among 180,251 Korean Vietnam veterans from 1992 through 2003 using EOI scores for exposure assessment. The incidence of cancer was determined through a review of records from the Korea National Cancer Incidence Database. Overall, the veterans classified with high exposure had a small yet statistically significant higher risk of cancer
than the veterans classified with low exposure. Compared with low exposure, high herbicide exposure appeared to be most related to an elevated risk of cancers of the mouth, salivary glands, stomach, and small intestine. The objective classification of both herbicide exposure and cancer incidence is considered a strength of this study over other publications from this cohort that used self-report data for analyses.
Again, using EOI scores to estimate herbicide exposure, Yi et al. (2014a) examined the prevalences of a wide range of disease conditions, specifically, those pertaining to the endocrine, nervous, circulatory, respiratory, and digestive systems. Health information was derived through a review of claims data from the Health Insurance Review and Assessment Service of Korea from January 1, 2000, to September 30, 2005. Overall, and compared with low exposure, high herbicide exposure was associated with a statistically significantly higher prevalence of hypothyroidism, autoimmune thyroiditis, other endocrine gland disorders including pituitary gland disorders, as well as amyloidosis and Alzheimer disease. As with Yi and Ohrr (2014), the objective classification of both herbicide exposure and disease prevalence is considered a strength of this study.
Finally, Yi et al. (2014b) used objective classifications of both herbicide exposure and cause-specific mortality to analyze cause-specific mortality in 180,639 Korean Vietnam veterans. The EOIs were used as the basis for two characterizations of herbicide exposure: as “low” versus “high” and as per unit increase based on a log-transformed scale. The incidence of mortality and cause of death were ascertained by the use of death records from the National Statistical Office for the period 1992–2005. Veterans with high herbicide exposure were found to have 10% increased long-term risk of mortality and 13% increased cancer mortality. The observed cause-specific cancer mortality estimates were very imprecise, but were highest for thyroid cancer, chronic myeloid leukemia, small intestine cancer, and bladder cancer.
Other Studies of Korean Vietnam Veterans
Epidemiologic studies have also looked at immunotoxicologic outcomes (H. A. Kim et al., 2003) and skin and general disease patterns (Mo et al., 2002) in Korean Vietnam veterans who were exposed to herbicides during the Vietnam War. One case-control study of the association between exposure to TCDD and recovery outcomes (hypertension, hyperlipidemia, and the rate and severity of major adverse coronary events) in male veterans who presented with acute coronary syndrome was also examined, but the study findings are not informative about associations between TCDD and acute coronary syndrome itself. Two new studies of Korean veterans who served in Vietnam were identified for the current update. Y. S. Yang et al. (2016) used a case-control design to examine the association between exposure to Agent Orange and Parkinson disease. Han et al. (2016) conducted a small hospital-based case-control study of acute ischemic
stroke to compare vascular features among those presumed to have been exposed to Agent Orange (based on deployment in Vietnam) and those veterans who did not serve in Vietnam.
New Zealand Vietnam-Veteran Studies
McBride et al. (2013) followed 2,783 male veterans from New Zealand who served in Vietnam between 1964 and 1972. Their status with respect to cancer incidence and mortality was determined from 1988 through 2008. This cohort included 84% of all 3,322 Vietnam veterans from New Zealand who had survived service in Vietnam. Standardized incidence and mortality ratios were generated by comparing the observed incident cases and deaths in this cohort with the corresponding expected numbers of new cases and deaths rates from the general male population of New Zealand. For all-cause mortality, the Vietnam veterans had significantly lower rates than the New Zealand general population. Cancer mortality and overall incidence were similar between Vietnam veterans and the New Zealand general population, as was heart disease mortality. In contrast, New Zealand Vietnam veterans appeared to be at higher risk of cancers of the head and neck and oral cavity, pharynx, and larynx as well as of incident chronic lymphoid leukemia (also known as chronic lymphocytic leukemia) than was the New Zealand general population. Although the follow-up of this cohort was long (20 years), the study did not have information on cancer incidence and mortality in the time period immediately after the service (i.e., between 1972 and 1988). It also lacked an internal comparison group, and information on potential confounding factors including smoking, drinking habits, and human papilloma virus status was not available, which limits the interpretation of the data, particularly regarding incident cancers. Moreover, it was assumed that any veteran who had been deployed had been exposed to the herbicides, and the presumed exposure was not validated through more objective measures such as serum concentrations or even more targeted self-reported questions of exposure.
For the current report, one new follow-up publication of the New Zealand Vietnam veteran cohort was identified. Cox et al. (2015) used hospital discharge records from 1988 to 2009 to report the prevalent health conditions among the same cohort of 2,783 New Zealand Vietnam veterans used by McBride et al. (2013). For participants 30 years of age or older, person-years of follow-up were calculated by 5-year age categories. Age-specific hospitalization rates were calculated using the total number of annual hospitalizations published by the Ministry of Health and the average annual resident population. The comparison group was the standardized general population of New Zealand. Standardized hospitalization ratios and 99% confidence limits were calculated and reported as a means to control for the multiple tests performed for various outcomes. Overall, this study found that hospital admissions due to all causes combined was slightly higher for Vietnam veterans than for the standardized population of New Zealand. Multiple
outcomes by system and specific conditions were reported; however, several of the outcomes are not generally conditions for which an individual would be hospitalized (e.g., diabetes, cataract, anxiety disorder), thereby limiting the utility of some of the findings reported. This study is also subject to the same limitations discussed for McBride et al. (2013).
OCCUPATIONAL STUDIES
Several occupational groups in the United States and elsewhere have been exposed to the COIs. Exposure characterization in studies of these groups varies widely in the metric used, the extent of detail, confounding exposures, and whether individual, surrogate, or group (ecologic) measures are used. Some studies reviewed in earlier VAO reports used job titles as broad surrogates of exposure; others rely on disease-registry data.
The VAO committees have reviewed many epidemiologic studies of occupationally exposed groups for evidence of an association between exposure to TCDD or to the herbicides used in Vietnam and health risks. In reviewing the studies, the committee considered two types of exposure separately: exposure to 2,4-D or 2,4,5-T and exposure to TCDD from 2,4,5-T or other sources. That separation is necessary because some health effects could be associated with an exposure to 2,4-D or 2,4,5-T in the absence of substantial TCDD exposure. After the dioxin contamination of phenoxy herbicides was recognized, production conditions were modified to minimize that contamination, and the use of the products most likely to contain TCDD (2,4,5-T and Silvex) was banned. As a result, workers who were exposed to phenoxy herbicides only after the late 1970s are not assumed to have been at risk for exposure to TCDD. The distinction is particularly important for workers in agriculture and forestry, including farmers and herbicide appliers, whose exposure is primarily the result of mixing, loading, and applying herbicides.
The committee also considered studies of occupational exposure to dioxins, focusing on workers in chemical plants that produced phenoxy herbicides or chlorophenols, which tend to be contaminated with PCDDs. Waste-incineration workers were also included in the occupation category because they can come into contact with dioxin-like chemicals while handling the byproducts of incineration. Other occupationally exposed groups included were pulp-and-paper workers exposed to dioxins through bleaching processes that use chlorinated compounds and sawmill workers exposed to chlorinated dioxins, which can be contaminants of the chlorophenates used as wood preservatives.
Because no new information has been published on several of these cohorts for years or decades and detailed information on them is available in previous volumes of the series, this section offers only a brief overview of those major occupational cohorts and studies that have contributed to the evidence base on potential health outcomes stemming from exposure to the COIs but for which no
new information for the current volume is available. Instead, the focus here is on the design and methodology of studies for those occupational cohorts for which new information is available in this report.
Studies of Herbicide Production Workers
International Agency for Research on Cancer (IARC)
A multisite study by IARC involved 18,390 production workers and phenoxy herbicide sprayers working in 10 countries (Saracci et al., 1991). The full cohort was established by using the International Register of Workers Exposed to Phenoxy Herbicides and Their Contaminants. Twenty cohorts were combined for the analysis: one each in Australia, Austria, Canada, Finland, and Sweden; two each in Denmark, Italy, the Netherlands, and New Zealand; and seven in the United Kingdom. There were 12,492 production workers and 5,898 sprayers in the full cohort. Several studies published using data from this cohort were reviewed by the first few VAO committees and contributed to conclusions on some cancers (Kogevinas et al., 1992, 1993, 1995, 1997), but no new studies of the IARC cohort have been published since Update 1998.
Several of the subcohorts that make up the IARC cohort have generated independent reports that have been evaluated separately by VAO committees to garner additional insights, such as the results associated with TCDD concentrations measured in various subjects: Austrian production workers (Jäger et al., 1998; Neuberger et al., 1998, 1999), British production workers (Coggon et al., 1986, 1991, 2015), Danish production workers (Lynge, 1985, 1993), Dutch production workers (Boers et al., 2010, 2012; Bueno de Mesquita et al., 1993; Hooiveld et al., 1998), German production workers (Becher et al., 1992, 1996; Flesch-Janys, 1997; Flesch-Janys et al., 1995, 1996; Manz et al., 1991), and New Zealand production workers (Burns et al., 2010; Collins et al., 2009a; McBride et al. 2009a,b; 't Mannetje et al., 2005, 2017, 2018). Several of the component cohorts have not been the subject of any separate publications: Australian herbicide sprayers, Canadian herbicide sprayers, Finnish production workers, two cohorts of Italian production workers, and Swedish production workers. The U.S. NIOSH cohort was added to the IARC cohort as of the 1997 publication by Kogevinas et al. and is discussed after the international production-worker cohorts.
Previous committees have examined studies of several international production-worker or herbicide-using worker cohorts, including many that were subcohorts of IARC. No new studies were identified by the committee for inclusion in the current report on many of these groups, including
- BASF Ludwigshafen Plant workers, Germany, who were involved in an accident in 1953 when some of the workers experienced extremely high
- exposures to TCDD during the manufacture of trichlorophenol (TCP), or as a result of the accident, or following the accident during reactor cleanup, maintenance, or demolition (Ott and Zober, 1996; Thiess et al., 1982; Zober et al., 1990, 1994, 1997). (This group was not in the IARC cohort.)
- Two Dutch subcohorts of the IARC cohort consisting of 2,106 male workers employed in two manufacturing factories producing and formulating chlorophenoxy herbicides: 2,4,5-T in factory A from 1955 through 1985, and 2-methyl-4-chlorophenoxyacetic acid (MCPA), 2-(2-methyl-4-chlorophenoxy) propionic acid (Mecoprop, MCPP), and 2,4-D in factory B from 1965 through 1986. Accordingly, members of both subcohorts had potential exposure to phenoxy herbicides, but only those in factory A would have been exposed to TCDD. Several analyses have been made using the entire cohort population or subsets of workers from chemical production factory A and factory B—these have examined different endpoints and applied different methods and measures to estimate exposure to TCDD (Boers et al., 2010, 2012; Bueno de Mesquita et al., 1993; Hooiveld et al., 1998; Saberi Hosnijeh et al., 2011, 2012a,b,c, 2013a,b).
- German production workers consisting of four German cohorts added to the IARC cohort as of 1997: the Boehringer–Ingelheim cohort, which had a high potential for TCDD exposure from the production of TCP and 2,4,5-T from 1951 to 1954 and from 1957 to 1984 (Flesch-Janys, 1997; Flesch-Janys et al., 1995; Manuwald et al., 2012; Manz et al., 1991), a cohort in the BASF Ludwigshafen plant that did not include those involved in the 1953 accident, and cohorts in two Bayer plants (Becher et al., 1992, 1996). All the plants were involved in the production of phenoxy herbicides or chlorophenols.
- Workers in Czechoslovakia (n > 80) who were exposed to TCDD during the production of 2,4,5-T (Pazderova-Vejlupková et al., 1981; Pelclová et al., 2001, 2002, 2007, 2009, 2011; Urban et al., 2007).
New Zealand Production Workers Two new studies on this cohort were identified ('t Mannetje et al., 2017, 2018). The Dow AgroSciences plant in New Plymouth, New Zealand, produced phenoxy herbicides from the late 1950s through the mid-1980s. This plant also produced picloram, one of the COIs about which very little information is available. The New Zealand cohort was incorporated into the original IARC cohort.
Complete employment records for 1969–1984 (referred to as the 1984 cohort) were available and 't Mannetje et al. (2005) used them to report on the mortality experience through 2000 of the 713 men and 100 women who had worked at least 1 month in that period. McBride et al. (2009a) conducted expanded analyses and updated previous analyses of cause-specific mortality from both cancers and other conditions. The cohort was increased to 1,599 participants (the 1988 cohort),
including a substantial number of people who had minimal opportunity for exposure, by extending the employment period for eligibility to November 1, 1988, and removing the requirement that employment lasted at least 1 month. A subsample of the 1988 cohort participated in a serum-dioxin analysis that found that 70% had been exposed. McBride et al. (2009b) further expanded the cohort to 1,754 participants (the 2003 cohort) by further extending eligibility to anyone who had worked at the site at any time until October 1, 2003. Both enlarged cohorts were followed through 2004. The New Zealand Health Information Service Mortality Collection was used to identify deaths, and exposure status was classified according to work experience. Collins et al. (2009a) described the group’s serum TCDD concentrations overall, and Burns et al. (2010) performed analyses to determine what factors might predict serum TCDD: age, BMI, and employment history were found to be significant determinants. Both Collins et al. (2009a) and C. J. Burns et al. (2010) reported standardized mortality ratios adjusted for age, sex, and calendar age and used the New Zealand general population as the reference population. For the 1988 cohort, effect estimates were stratified by exposure status (ever exposed and never exposed) and by predicted cumulative exposure categories. For the 2003 cohort, standardized mortality ratios were reported for the entire cohort and stratified by employment duration (less than 3 months and at least 3 months) and by latency (15 years of latency and less than 15 years of latency). For the 1988 cohort, proportional-hazards survival analysis was also used to test the association between mortality and predicted cumulative exposure categories.
The New Zealand studies have several important limitations. The sample loss was substantial: 13% were lost to follow-up in both cohorts, and 8% of the 1988 cohort and 9% of the 2003 cohort emigrated. If subject loss was nonrandom, then the study findings might be vulnerable to sample selection bias. In addition, the inclusion in the 2003 cohort of the employees hired as recently as 2003 is questionable. It appears that no deaths were observed in the increment between the 1988 cohort and the 2003 cohort (those hired since 1988), presumably because these participants were relatively young. The inclusion of the incremental participants might dilute the power of the study to detect the effects of TCDD exposure on health outcomes that require a long latent period; participants who have not yet “matured” through the latent period might be contributing noise rather than signal to the analyses. The Update 2010 committee, therefore, did not give substantial weight to the dose–response findings of McBride et al. (2009b). The serum concentrations of dioxins and furans observed in a subset of the workers in the Dow phenoxy-herbicide plant in New Zealand have been used in estimating individual exposure (Aylward et al., 2010; Collins et al., 2009a).
National Institute for Occupational Safety and Health (NIOSH) Studies
NIOSH has collected data on and followed several groups of U.S. workers exposed to the committee’s COIs, including the dioxin registry; the
pentachlorophenol (PCP) cohort (Ruder and Yiin, 2011); the cross-sectional medical study of workers in plants producing 2,4,5-TCP and 2,4,5-T or 2,4,5-TCP, 2,4,5-T, and hexachlorophene (Alderfer et al., 1992; Calvert et al., 1991, 1992, 1994, 1998, 1999; Egeland et al., 1994; Halperin et al., 1995, 1998; Kayajanian, 2002; Lawson et al., 2004; Sweeney et al., 1993, 1996, 1997–1998); and the TCDD mortality cohort. The NIOSH cohort was added to the IARC cohort as of the 1997 publication by Kogevinas et al. No new studies on the entire NIOSH cohort have been published since those reviewed in Update 2006.
NIOSH TCDD Mortality Cohort Since 1978, NIOSH has compiled an extensive set of data on chemical production workers potentially contaminated with TCDD in 1942–1984. More than 5,000 workers who were involved in production or maintenance in any of 12 companies were identified from personnel and payroll records; 172 additional workers identified previously by their employers as being exposed to TCDD were also included in the study cohort (Suskind and Hertzberg, 1984). The employees’ possible exposure resulted from working with various substances of which TCDD was a contaminant: 2,4,5-TCP, 2-(2,4,5-trichlorophenoxy) propionic acid (Silvex, 2,4,5-TP), 2-(2,4,5-trichlorophenoxy) ethyl 2,2-dichloropropionate (Erbon), O,O-dimethyl O-(2,4,5-trichlorophenyl) phosphorothioate (Ronnel®), and hexachlorophene. The 12 plants involved were large manufacturing sites of major chemical companies, so many of the participants were potentially exposed to many other compounds, some of which could be toxic and carcinogenic.
Exposure status was determined initially through a review of process operating conditions, employee duties, and analytic records of TCDD in industrial hygiene samples, process streams, products, and waste (Fingerhut et al., 1991). Occupational exposure to TCDD-contaminated processes was confirmed by measuring serum TCDD in 253 cohort members. The duration of exposure, defined as the number of years an employee had worked in processes contaminated with TCDD, was used as the primary exposure metric in the study. The use of duration of exposure as a surrogate for cumulative exposure was based on a correlation (Pearson correlation efficient, 0.72) between log-transformed serum TCDD levels and the number of years worked in TCDD-contaminated processes. The duration of exposure of individual workers was calculated from work records, and exposure-duration categories were created: < 1 year, 1–<5 years, 5–<15 years, and ≥15 years. In some cases, information on the duration of exposure was not available, so a separate metric, duration of employment, was defined as the total time that each worker was employed at the study plant. Fingerhut et al. (1991) used the exposure measures in assessing mortality through 1987.
A follow-up study (Steenland et al., 1999) examined the association between TCDD exposure and cause of death through 1993; it examined specific health outcomes, including cancers (all and site-specific), respiratory disease, cardiovascular disease, and diabetes. The researchers used a more refined exposure
assessment than had previous analyses. It excluded workers whose records were inadequate to determine the duration of exposure, and this reduced the number of study participants to a subcohort of 3,538 workers (69% of the overall cohort). The exposure assessment for that subcohort was based on a job–exposure matrix that assigned each remaining worker a quantitative exposure score for each year of work (Piacitelli and Marlow, 1997).
Subcohorts of the NIOSH TCDD Mortality Cohort
Monsanto The NIOSH study cohort (Fingerhut et al., 1991) included employees of the Monsanto facility in Nitro, West Virginia, which produced 2,4,5-T in 1948–1969. Zack and Suskind (1980) examined the mortality experience of the 121 men who had chloracne associated with an unintentional release that occurred on March 8, 1949. Other studies considered mortality and other health outcomes in additional workers involved in numerous aspects of 2,4,5-T production at the Monsanto plant (Collins et al., 1993; Moses et al., 1984; Suskind and Hertzberg, 1984; Zack and Gaffey, 1983). No additional studies on those participants alone have been published; they have since been followed as part of the NIOSH and IARC cohorts.
Dow Production Workers At the Dow plant in Midland, Michigan, 2,4-D, TCP, and PCP were manufactured over different, overlapping time periods and exposed different populations of workers. The cohort of TCP workers who were potentially exposed specifically to TCDD is one of the eight cohorts in the NIOSH cohort of dioxin-exposed U.S. workers that were entered into the IARC phenoxy herbicides cohort. Dow PCP workers who were not exposed to TCDD are not in the IARC or NIOSH cohorts for TCDD, but this group is one of four cohorts included in NIOSH’s PCP cohort (Fingerhut et al., 1984; Ruder and Yiin, 2011). Dow assembled a large cohort at the Midland, Michigan, plant (Bond et al., 1989a; Cook et al., 1986, 1987). TCDD exposure in the cohort was defined by chloracne diagnosis (Bond et al., 1989b). Within the cohort, a subcohort study of women (Ott et al., 1987) and a case-control study of STS (Sobel et al., 1987) were conducted. The Dow cohorts have been followed as part of the NIOSH and IARC cohorts since 1991 and 1997, respectively.
C. J. Burns et al. (2011) reported on cancer incidence in 2,4-D production workers in the Dow Midland plant. The exposed cohort consisted of 1,316 men who worked in 2,4-D operations from 1945 through 1994 and who were alive on January 1, 1985, when the Michigan statewide cancer registry was initiated. Exposure was considered both as a discrete category (exposed cohort members versus a non-exposed reference population) and as a cumulative variable estimated as (job-specific exposure estimate) × (duration on the job) summed over all jobs held since 1945. Workers were stratified into three categories according to their estimated cumulative exposure. The cohort was followed from 1985
through 2007. Cancer incidence was ascertained from the Michigan statewide cancer registry, and data were linked to two other states where cohort members might reside. Three nested cohorts were used for statistical analyses in order to address potential problems with missing data due to migration outside the three states, with data linkage. Cohort 1 consisted of the entire exposed cohort regardless of residency (1,316 people who had 25,267 person-years of follow-up). Cohort 2 required Michigan residency: follow-up was terminated when a person was no longer a Michigan resident because company records showed a permanent non-Michigan address (those who died were classified as residents if Michigan was listed as the state of residency on their death certificates) (1,256 who had 23,354 person-years). Cohort 3 was the most restrictive and required Michigan residency; follow-up was terminated as soon as a person was no longer known to be a Michigan resident (1,108 who had 18,897 person-years). People of unknown residency status were assumed to remain Michigan residents and were included in the follow-up for Cohort 2 but were excluded from Cohort 3. Standardized incidence ratios were derived for all three cohorts, with Michigan white males as the reference population; Fisher’s exact confidence intervals were used to characterize the uncertainty. For Cohort 2, additional analyses were conducted by using the National Cancer Institute’s Surveillance, Epidemiology, and End Results registry population and a regional population as the reference populations. The cohort was stratified according to cumulative duration and cumulative exposure categories. There were several concerns that the study findings might be biased. First, the study cohort might be healthier than the general population being used as the reference population. Second, the lack of a latency period in the study design might lead to an attenuation effect on the risk estimates. Third, Cohort 2, which was the researchers’ focus in the study, might be vulnerable to an attenuation effect because of the uncertainty in residency status. The results on Cohort 3 are considered the least subject to bias and therefore the most reliable. Although Cohort 3 was the smallest group and as such is also subject to the most variability, consistency in results among the three cohorts was considered confirmatory.
All Dow TCP-Exposed Workers TCP was produced in Dow’s Midland facility from 1942 to 1979, and 2,4,5-T was produced there from 1948 to 1982. Collins et al. (2009b) reported on the vital status through 2003 of 1,615 people who worked with TCP or 2,4,5-T from 1942 through 1982; 58,743 person-years were accumulated, and 662 deaths were observed. Standardized mortality ratios for cause-specific mortality in the cohort—with and without the overlap of 196 people who were also part of the PCP cohort (reviewed in Collins et al., 2009c)—were calculated by using the U.S. population as the reference population and using the Occupational Mortality Analysis Program. Work history records were used to determine length of exposure. Serum samples used for measuring the levels of six types of dioxins were collected for 431 TCP and PCP workers. Historic concentrations for each dioxin congener were calculated
from the median concentrations from the serum samples and the known half-lives associated with each congener. A job exposure matrix was created for both the TCP and PCP production facilities based on measured concentrations for workers in different jobs. A pharmacokinetic model was applied to job-specific concentrations to the work history of each member of the study group to estimate their time-dependent serum concentration profiles for each dioxin congener (i.e., TCDD, as well as Hexa-CDD, Hepta-CDD, and Octa-CDD). Collins et al. (2016) reported the results of an additional follow-up of vital status to TCP and PCP production workers. Vital status was determined for the cohort through December 2011; a total of 1,198 deaths since 1979 were found.
Dow PCP Production Workers These workers were engaged in the manufacture of PCP from 1937 to 1980 in the same plant where the TCP cohort worked. Unlike TCP, PCP did not contain TCDD, but it did contain other highly chlorinated dioxin congeners, and 20% of the PCP workers had suffered from chloracne. Dow performed an exposure risk assessment on the subset of its manufacturing workers who were exposed to PCP (Ramlow et al., 1996). The exposure assessment evaluated the available industrial-hygiene and process data, including recollections from employees about their job, processes, and changes in processes as well as data from engineering controls, measurements from surface wipes, and exposure-monitoring data from area sampling and personal breathing zones. Jobs in the “flaking/prilling/packaging area” were determined to have a higher potential exposure because of dermal exposure to airborne PCP; the industrial-hygiene data suggested a difference of about a factor of 3 between the areas of highest and lowest potential exposure. An estimated exposure-intensity score of between 1 and 3 (from lowest to highest potential exposure intensity) was assigned to each job. Information concerning the use of personal protective equipment was deemed to be unreliable. For each participant, cumulative PCP and TCDD exposure indexes were calculated by multiplying the duration of each exposed job by its estimated exposure intensity and then summing across all exposed jobs.
Collins et al. (2009c) conducted a mortality study of the Dow PCP production workers with the accrual of years at risk starting at the beginning of 1940 and followed through 2003; the TCP workers were followed over the same years (Collins et al., 2009b). The cohort consisted of 773 PCP workers; 27,035 person-years were accumulated, and 370 deaths were observed. Standardized mortality ratios for the PCP cohort (with and without the overlap of 196 people in the TCP cohort) were reported for cause-specific mortality, with the U.S. population as the referent population. Proportional-hazards survival analysis was also used to assess the association between mortality and predicted cumulative exposure as a function of the total TCDD TEQ. An updated mortality analysis that follows the cohort of PCP and TCP workers though 2011 and reports cause-specific mortality on several cancers and other diseases (Collins et al., 2016) is reviewed in the current update.
Dow TCDD-Exposed Production Workers Dow conducted a study of 204 workers engaged in the production of 2,4,5-T (Ott et al., 1980) and another study of 61 TCP manufacturing workers who had chloracne (Cook et al., 1980). Industrial hygienists developed a job-exposure matrix that ranked employee exposures as low, moderate, or high on the basis of available air-monitoring data and professional judgment. The matrix was merged with employee work histories to assign an estimate of exposure to each job. A cumulative dose was then developed for each of the 878 employees by multiplying the representative 8-hour time-weighted average exposure value for each job by the number of years in the job and then adding the products for all jobs. A 2,4-D time-weighted average of 0.05 mg/m3 was used for low, 0.5 mg/m3 for moderate, and 5 mg/m3 for high exposure. The exposure estimates do not appear to have taken into account the role of dermal exposure in the facilities. It is not clear to what extent the use of air measurements alone can provide accurate classification of workers into low-, moderate-, and high-exposure groups. The study apparently did not include biologic monitoring of 2,4-D.
Bond et al. (1983) investigated potential exposure to TCDD and morbidity in the sets of workers reported on by Cook et al. (1980) and Ott et al. (1980). Potential TCDD exposure and reproductive outcomes were studied in the offspring of 930 men who worked with chlorophenol from 1939 through 1975 (Townsend et al., 1982). Dow employees who had a diagnosis of chloracne or who were classified as having chloracne on the basis of a clinical description were followed prospectively for mortality (Bond et al., 1987). There was a succession of mortality studies of workers involved in 2,4-D production in several of the plants (Bloemen et al., 1993; Bond et al., 1988; C. J. Burns et al., 2001). These studies also used the same exposure-assessment procedures.
Bodner et al. (2003) published a 10-year follow-up of the work of Cook et al. (1986), comparing the mortality experience of 2,187 male workers at Dow who were potentially heavily exposed to dioxin before 1983 with that of the NIOSH and IARC cohorts. Dow researchers have published a study of serum dioxin concentrations measured in 2002 in former chlorophenol workers (Collins et al., 2006). Most of the workers in the study were included in the NIOSH and IARC cohorts. The authors used their data to estimate worker exposure at the time of exposure termination by using several pharmacokinetic models. They concluded that their findings were consistent with those of other studies that reported high serum dioxin concentrations in chlorophenol workers after occupational exposure.
Aylward et al. (2013) examined the elimination rates of dioxin congeners in former chlorophenol workers from the Midland plant. Blood samples from 56 former chlorophenol workers were taken and examined in 2004–2005 and then resampled in 2010. The purpose of this analysis was to estimate half-life reductions for TCDD TEQs, which, in aggregate, were 9.3 years for the dioxin congeners analyzed. This analysis is informative with respect to estimating elimination rates over time for the COIs as the Vietnam-veteran cohort continues to age.
Studies of Other Industrial Cohorts
VAO committees have reviewed several other occupational cohorts and studies of industrial workers over the series. The countries and industries have included
- Chinese automobile foundry workers (L. Wang et al., 2013);
- pulp and paper workers exposed to TCDD and other dioxins that can be generated by the bleaching process during the production and treatment of paper and paper products in the United States (Henneberger et al., 1989; Robinson et al., 1986; Solet et al., 1989), Finland (Jäppinen and Pukkala, 1991), Denmark (Rix et al., 1998), and an IARC cohort of paper and pulp workers in 11 countries (McLean et al., 2006);
- sawmill workers with dermal and inhalation exposure through the use of pentachlorophenates (which are contaminated with higher-chlorinated PCDDs [Cl6–Cl8]) in British Columbia, Canada (Dimich-Ward et al., 1996; Heacock et al., 1998; Hertzman et al., 1997), and New Zealand (McLean et al., 2009), or to tetrachlorophenates (which are less contaminated with higher-chlorinated PCDDs) (McLean et al., 2009) in New Zealand; and
- waste incineration workers in Japan (Yamamoto et al., 2015; Yoshida et al., 2006) and Korea (Oh et al., 2005).
Studies of U.S. workers in other chemical plants have also included studies of 2,4-D and 2,4,5-T production workers (Poland et al., 1971), white men employed at a chemical plant that manufactured flavors and fragrances (Thomas, 1987), and workers producing PCP, lower-chlorinated phenols, and esters of chlorophenoxy acids (Hryhorczuk et al., 1998).
International cohorts of chemical workers exposed to the COIs have included UK chemical workers exposed to TCDD as a result of an industrial accident in 1968 (Jennings et al., 1988; May, 1973, 1982, 1983), 2,4-D production workers in the former Soviet Union (Bashirov, 1969), and Croatian workers exposed to a complex mixture of pesticides (atrazine, alachlor, cyanazine, 2,4-D, and malathion) during the production process (Garaj-Vrhovac and Zeljezi, 2002). Some of these worker populations, such as the Chinese automobile foundry workers, were reported on only once, and others were prospectively or retrospectively followed for years, such as waste incineration workers in Japan (Yamamoto et al., 2015; Yoshida et al., 2006). Summaries of these studies are included in the update in which they were first identified. For the current volume, morbidity and mortality outcomes of worker cohorts at an electric arc furnace in Italy (Cappelletti et al., 2016) and at a transformer and capacitor recycling plant in Germany (Fimm et al., 2017; Haase et al., 2016; Putschogl et al., 2015) are reviewed.
Inadequate occupational hygiene at a recycling plant for capacitors and transformers in Dortmund, Germany, led to a significant body burden of PCBs
in workers, their family members, and people working or living in the immediate vicinity of the plant. A medical surveillance program, Health Effects in High-Level Exposure to PCB, was initiated to provide biomonitoring to identify potential health risks related to PCB exposure for the affected population (Kraus et al., 2012). Workers of and residents around this plant were exposed to both dioxin-like (PCBs 105, 114, 123, 156, 157, 167, and 189) and non-dioxin-like PCBs as a result of contamination of the area. Participation in the surveillance program was voluntary, and data and blood samples were collected at three time points: immediately (beginning in 2010), 1 year, and 2 years after exposure. PCB congeners were measured in serum using blood samples collected from the participants, and urine samples were also collected at the three time points. Of the eligible 294 adults, 148 participated at all three time points. Three studies using these data were published and are reviewed in this update. Putschogl et al. (2015) studied associations with neurotransmitter metabolites of dopamine and norepinephrine in urine as markers of targeted effects on these specific neurotransmission pathways, and Haase et al. (2016) confirmed that PCB exposure can modify lymphocyte profiles. However, neither of these analyses of metabolites or immune cells is diagnostic of a specific health outcome, and they are therefore only of tangential relevance to the committee’s charge. Fimm et al. (2017) examined a broad range of cognitive functions covering attention, executive processing, reasoning, memory, and motor performance in this cohort.
Studies of Herbicide-Using Workers
The original VAO committee and committees up through Update 2006 were more inclusive of identified studies from the literature searches. Several of the early studies reviewed and included in the updates had nonspecific, inferred exposure characterizations based on “usual occupation” from death certificates, self-reported “current occupation,” or census tract or area of residence (e.g., rural or farming areas). The studies focused primarily on farmers and people employed in the agricultural industry, but workers in forestry and other outdoor occupations, such as highway-maintenance workers, are also likely to have been exposed to herbicides and other chemicals. The problem with using such nonspecific surrogates of exposure is that it will influence and change the effect estimates (either toward or away from the null depending on the types of bias present) making it impossible to know the true effect of the COIs. Occupation or job titles do not provide information on the duration or the intensity of the exposure, and they cannot be used to determine whether a worker was exposed to a specific agent. Even those studies that collected more details on the number of years of employment in the agriculture industry, broad categories of the chemicals used (e.g., herbicides, insecticides, fungicides, etc.), specific classes of chemicals or names, the frequency of application, the use of personal protective equipment, and the method of application may be limited by recall or information bias (depending on
whether other records are available) and do not provide much evidentiary weight if the specific agents and chemicals used are not collected.
Since the first VAO report, exposure assessments in epidemiology studies have been increasingly exact in both specificity and amount, enabling the committees of the more recent updates to establish stricter criteria for accepting exposure as sufficiently specific for results to be added to the evidentiary database. The current committee now seeks results expressed in terms of the five COIs for this project or their analogues, and it regards classification based only on job title as inadequate. Data derived from studies in which exposure is described non-specifically as “herbicide” can at most be used as supportive evidence. According to the policy established by the Agent Orange Act of 1991, studies of Vietnam veterans are presumed to involve relevant exposure, as are studies of workers at a particular plant during a period when it is known to have been producing phenoxy herbicides or other chemicals recognized as having been contaminated with TCDD.
The most reliable information on health effects among American herbicide applicators and users exposed to the COIs has come from prospective investigations of the Agricultural Health Study (AHS). More than 200 publications have reported on outcomes from this cohort, although not all have focused on the use of 2,4-D or other COIs. Several new publications from the AHS were reviewed in the current update. VAO and update committees have also reviewed studies of other populations of farmers and agricultural workers conducted among state populations and as part of larger cohorts such as the CropLife America Farm Family Exposure Study (Mandel et al., 2005) and the California United Farm Workers of America Study (Mills and Yang, 2005, 2007; Mills et al. 2005). In addition to studies of herbicide users in the United States, several international publications have been reviewed by VAO committees.
Agricultural Health Study
The AHS is a prospective investigation of cohorts of private pesticide applicators (farmers), their spouses, and commercial pesticide applicators in Iowa and North Carolina, with a total of 89,658 participants, including 57,311 applicators (82% of those seeking licensing) and 32,347 spouses (75% of all spouses). The applicators are predominantly male, and the spouses are predominantly female. The AHS is sponsored by the National Cancer Institute, the Environmental Protection Agency, and the National Institute of Environmental Health Sciences. Enrollment in the study was offered to applicants for applicator certification in Iowa and North Carolina. The project’s website (www.aghealth.nih.gov) provides many details about the study, including a specification of which pesticides were the subject of information gathered from the enrollment forms and mailed questionnaires (Alavanja et al., 1994).
In phase I (1993–1997), the enrollment form for both commercial (8.6%) and private (largely farmers) applicators asked for details on the use of 22 pesticides (10 herbicides, including 2,4-D; 9 insecticides; 2 fungicides; and 1 fumigant) and yes–no responses as to whether 28 other pesticides (8 herbicides, including 2,4,5-T and Silvex; 13 insecticides; 4 fungicides; and 3 fumigants) had ever been used. A subset of 24,034 applicators also completed and mailed back a take-home questionnaire (response rate 42%). The questionnaire asked for details about use of the 28 pesticides with yes–no information on the enrollment form and for yes–no responses as to whether 108 other pesticides (34 herbicides, including organic arsenic, which would cover cacodylic acid; 36 insecticides; 29 fungicides; and 9 fumigants) had ever been “frequently” used. Although no pronounced differences in demographics, medical histories, or farming practices were found between those who completed the questionnaire and those who did not (Tarone et al., 1997), it is still possible that selection bias might have compromised the validity of any studies based on the questionnaire because of differences that might not have been captured in the enrollment form. Dosemeci et al. (2002) published an algorithm designed to characterize the personal exposures of that population. Weighting factors for the key exposure variables were developed from the literature on pesticide exposure. This quantitative approach has the potential to improve the accuracy of exposure classification for the cohort, but the published epidemiologic studies reviewed as part of the VAO series do not appear to have used that method.
Phase II was a 5-year follow-up conducted in 1999–2003. Computer-assisted telephone interviews were completed by 60,138 participants. The interviews specified “pesticides” in general to include herbicides. They asked about specific pesticides on individual crops; for several crops, only if atrazine or 2,4-D was specified was a participant asked whether it had been used alone or as part of the manufacturer’s mixture. A full pesticide list was not posted on the website with the follow-up questionnaire. In addition, dietary histories were completed by 35,164 respondents, and buccal-cell samples were gathered from 34,810 participants. The rate of response to the phase II survey—67% overall and 63% of the original cohort of 55,748 male applicators—was modest and leaves some room for selection bias to compromise the validity of studies based on the survey. In phase III (2005–2010), responses to an updated computer-assisted telephone interview were provided by 43,426 participants.
Numerous reports on the AHS cohort have been considered in the VAO series, and several new published studies have been reviewed in the current update (Bonner et al., 2017; Christensen et al., 2016; Henneberger et al., 2014; Koutros et al., 2016; LaVerda et al., 2015; Lebov et al., 2015, 2016; Parks et al., 2016). All have developed pesticide-exposure estimates or exposure categories from self-administered questionnaires, but only those studies that have considered exposure to the COIs are considered most relevant to VAO committees. The results on the relative rates of individual conditions seem comparable in exposure specificity
with findings in production cohorts in which not all of the workers included were necessarily exposed to the COIs and may have had additional toxic exposures. The AHS questionnaire collected detailed information regarding herbicide use; 2,4-D was the most commonly reported herbicide. Because all relevant studies have been reviewed in detail in the VAO report that corresponded to their publication date, only an overview is presented here. Details of the studies reviewed for the first time in the current volume are presented in the section corresponding to the health outcome of interest. Using various subsets of the study population, they have addressed a variety of health outcomes associated with one or more of the COIs, including
- all-cause and cause-specific mortality (Blair et al., 2005a; Waggoner et al., 2011) and morbidity (Alavanja et al., 2005; Blair et al., 2005b);
- incidence of prostate cancer (Alavanja et al., 2003, 2005), lung cancer (Alavanja et al., 2004), breast cancer (Engel et al., 2005), colorectal cancer (W. J. Lee et al., 2007), cutaneous melanoma (Dennis et al., 2010), all cancers (Alavanja et al., 2005; Koutros et al., 2010a, Samanic et al., 2006), and risk factors for pancreatic cancer (Andreotti et al., 2009);
- neurotoxicity of chronic exposure to modest amounts of pesticides (Kamel et al., 2005), neurologic symptoms including memory and concentration problems (Kamel et al., 2007a), Parkinson disease (Kamel et al., 2007b, 2014; Tanner et al., 2011), and amyotrophic lateral sclerosis (Kamel et al., 2012);
- reproductive effects (Farr et al., 2004, 2006) and cancer risk in the 21,375 children of pesticide appliers born in 1975 or later (Flower et al., 2004);
- diabetes in applicators and their wives (Montgomery et al., 2008; Starling et al., 2014) and history of gestational diabetes (Saldana et al., 2007);
- incidence of and mortality from myocardial infarction (Mills et al., 2009) and mortality from stroke (Rinsky et al., 2013);
- respiratory symptoms and disorders: chemical predictors of wheeze (Hoppin et al., 2002, 2006b), hypersensitivity pneumonitis (Hoppin et al., 2007b), chronic bronchitis (Hoppin et al., 2007a; Valcin et al., 2007), atopic and nonatopic asthma in women (Hoppin et al., 2008), and allergic and nonallergic adult-onset asthma (Hoppin et al., 2009);
- thyroid disease among AHS female spouses (Goldner et al., 2010) and male pesticide applicators (Goldner et al., 2013); and
- genetic markers (single nucleotide polymorphisms and candidate genes) and outcomes of prostate cancer risk (Andreotti et al., 2012; Barry et al., 2011, 2012; Karami et al., 2013; Koutros et al., 2010b, 2011), and telomere length (Hou et al., 2013).
Health outcomes examined by a single study that have accounted for and presented results on relevant COI exposures include doctor visits resulting from
pesticide exposure (Alavanja et al., 1998), rheumatoid arthritis (De Roos et al., 2005b), hearing loss (Crawford et al., 2008), and rhinitis in the past 12 months (Slager et al., 2009).
Several additional publications have discussed pesticide-use patterns in the population (Hoppin, 2005; Hoppin et al., 2006a; Kirrane et al., 2004; Samanic et al., 2005), estimated amounts of absorption of 2,4-D and chlorpyrifos exposures (Thomas et al., 2010), and have developed (Dosemeci et al., 2002) or refined (Coble et al., 2011) an algorithm for estimating pesticide exposure intensity. Other studies have focused on examining a variety of exposure issues, including the effect of exposure misclassification in the AHS (Blair et al., 2011) and using multiple imputation methods to assign pesticide use values for nonresponders and other missing data (Heltshe et al., 2012).
International Studies of Herbicide Users
Several studies have been reviewed in the VAO series that have published results of health effects on herbicide users in many different countries. In some countries, large studies were designed and large cohorts were followed, producing several publications that have been reviewed in the VAO series; those cohorts are described in brief by country of origin.
The Canadian Ontario Farm Family Health Study examined exposure to phenoxyacetic acid herbicides, including 2,4-D, and several fertility, reproductive, and pregnancy outcomes (Arbuckle et al., 1999a,b, 2001; Curtis et al., 1999; Savitz et al., 1997) and birth defects (Weselak et al., 2008). Biomonitoring was conducted in a subset of participants to evaluate the validity of the self-reported predictors of exposure (Arbuckle and Ritter, 2005; Arbuckle et al., 2002, 2005) and to examine other potential indirect sources of exposure to herbicides (Arbuckle et al., 2006). A second large cohort of 156,242 Canadian male farmers from three provinces, known as the Canadian Farm Operator Study, was assembled, and information on herbicide use in the cohort was used to determine the risk of specific causes of death in that population: NHL (Morrison et al., 1994; Wigle et al., 1990), prostate cancer (Morrison et al., 1993), brain cancer (Morrison et al., 1992), multiple myeloma (Semenciw et al., 1993), and leukemia (Semenciw et al., 1994). Other Canadian studies of agricultural workers have evaluated immune, neurobehavioral, and lung function of farmers who mixed and applied commercial formulations that contained chlorophenoxy herbicides and of residents in an agricultural area of Saskatchewan, Canada (Faustini et al., 1996), as well as asthma and pesticide use among male farmers in Saskatchewan (Senthilselvan et al., 1992). Mortality in men employed by a Canadian public utility, who were likely exposed to herbicides similar to those used in Vietnam, has also been reviewed (Green, 1987, 1991).
In Denmark, three studies reported on a cohort of Danish gardeners who had been exposed to herbicides (E. S. Hansen et al., 1992, 2007; Kenborg et
al., 2012), and one study examined cancer incidence among Danish farmers (Ronco et al., 1992). Danish gardeners were identified from union worker records on May 1, 1975. Most of the women (n = 859) worked in greenhouses, where herbicides are not routinely used; the men (n = 3,156), however, were known to be highly exposed to pesticides and herbicides, which included the phenoxy herbicides 2,4-D, 2,4,5-T, and MCPA. Vital status of the entire cohort through 1984 was achieved. Person-years at risk were calculated and reported for a latent period of 10–15 years. E. S. Hansen et al. (1992) determined the incidence of cancer in this cohort from 1975 to 1984 and compared those numbers with expected numbers calculated from incidence rates in the general Danish population. E. S. Hansen et al. (2007) used analogous methods to extend the follow-up period for the men through 2001 but used year of birth as a surrogate for intensity of exposure, with high exposures assumed for those who had been born before 1915, low exposures for those born in 1934 or later, and intermediate exposure for those born in between. Using this same cohort of Danish gardeners but restricted to men alive and living in Denmark at the beginning of 1977 (n = 3,124), Kenborg et al. (2012) reported on the incidence of Parkinson disease as a primary diagnosis from 1977 through 2008 and compared the results with the observed incidence of Parkinson disease in all Danish men by calendar period and age group. Kenborg et al. (2012) also reported on the incidence of lung, larynx, and bladder cancers in the cohort compared with the incidence in the general male Danish population. For the current update, a study of parental employment in farming and agriculture and cryptorchidism in offspring using the Danish National Patient Registry (Jorgensen et al., 2014) was identified and reviewed.
Three studies reporting on or updating mortality or cancer morbidity in Finnish men who had applied 2,4-D and 2,4,5-T for at least 2 weeks in 1955–1971 through work removing brush have been reviewed in the VAO series (Asp et al., 1994; Riihimaki et al., 1982, 1983).
Studies of Italian herbicide users have primarily been conducted among farmers in particular regions. Gambini et al. (1997) examined cancer mortality in a cohort of rice growers in northern Italy. Two studies reported on a cohort of male farmers in Italy’s southern Piedmont region who were licensed to use agricultural pesticides in 1970–1974, and the use of phenoxy herbicides in the area was reported to be twice the national average. Corrao et al. (1989) evaluated cancer incidence in the 25,945 men in the cohort on the basis of new diagnoses from hospital admissions in 1976–1983. In a continuation of that study, Torchio et al. (1994) reported on mortality through 1986 in the 23,401 men who were residents of the Piedmont area at the time of registration, stratified by the location of their residences (lived near arable land, near woodlands, and near mixed-use land).
The original VAO committee reviewed several studies that used data from the Swedish Cancer-Environment Register, which contained data from the Swedish Cancer Registry and individual responses from the 1960 and 1970 national censuses, including data on current occupation. Publications that used the Swedish
Cancer-Environment Register included a study of cancer incidence and farm work (Wiklund, 1983); studies of STS and malignant lymphoma in agricultural and forestry workers (Wiklund and Holm, 1986; Wiklund et al., 1988a); and a study of the risk of multiple myeloma in relation to various occupational activities (Eriksson and Karlsson, 1992). Two studies of cancer mortality in Swedish railroad workers who were exposed to 2,4-D, 2,4,5-T, and other herbicides were also examined (Axelson and Sundell, 1974; Axelson et al., 1980). Other studies reviewed by the committee addressed mortality and cancer incidence in a cohort of Swedish lumberjacks (Thörn et al., 2000) and cancers in Swedish pesticide and herbicide applicators (Dich and Wiklund, 1998; Wiklund et al., 1987, 1988b, 1989a,b).
For some countries, only one or two studies have been published on exposure to the COIs and health outcomes (mortality, prevalence, or incidence) among herbicide handlers. Many of these studies were small and, especially the earlier studies, lacked adequate or specific exposure information. These have included: Argentinian farmers (Butinof et al., 2015; Lerda and Rizzi, 1991); Australians exposed to phenoxy herbicides (Fritschi et al., 2005); Dutch forestry workers exposed to 2,4,5-T (van Houdt et al., 1983) and Dutch male herbicide applicators (Swaen et al., 1992, 2004); German male agricultural plant-protection workers in the former German Democratic Republic who spent at least 5 years during 1948–1972 applying pesticides, some of which were phenoxy herbicides (Barthel, 1981); Icelanders whose occupation may have exposed them to 2,4-D (Zhong and Rafnsson, 1996); Indian herbicide sprayers and warehouse employees (Linga Reddy et al., 2015); Mexican agricultural workers (Carbajal-López et al., 2016); New Zealand forestry workers (Reif et al., 1989); and offspring of Norwegian farmers (Kristensen et al., 1997).
ENVIRONMENTAL STUDIES
Industrial accidents have led to the evaluation of long-term health effects in non-worker populations that live near areas with fairly high environmental concentrations of the COIs. Effects on residents around normally operating industrial operations, such as waste incinerators, and even on people exposed only to “background” concentrations have also been studied. The systematic follow-up studies that have been conducted on the Seveso population and the numerous analyses of the population-level data collection effort of NHANES have contributed prominently to the evidence base considered by VAO committees.
Environmental exposures to the COIs almost never occur in isolation. Exposures to dioxin-like chemicals generally occur as part of mixtures that also include non–dioxin-like chemicals that tend to correlate with the dioxin-like chemicals, so it is not surprising that specific chemicals measured in a person’s serum also tend to correlate with one another; this collinearity means that it is difficult for epidemiologic studies to attribute any observed association to a particular chemical configuration (Longnecker and Michalek, 2000).
Environmental studies are presented below, beginning with the United States, then summarizing major international cohorts.
U.S. Environmental Studies
Several populations with environmental exposures to the COIs have been reviewed in the course of the VAO series. Descriptions of those populations and cohorts for which no new information has been identified since the last VAO update report (e.g., Anniston, Alabama, Community Health Survey; the Great Lakes Fish Consumption Study; the Iowa Women’s Health Study; and Times Beach and Quail Run, Missouri) can be found in Chapter 6 of Update 2014 (NASEM, 2016a) and the volume that first reviewed the study following its publication. Studies of U.S. populations that the committee identified and that have not been the focus of multiple ongoing follow-up or publications are summarized in the chapters related to the health outcome of interest.
National Health and Nutrition Examination Survey
In the early 1960s the CDC National Center for Health Statistics began the NHANES program as a means of monitoring and assessing the health and nutritional status of people of all ages living in the United States. In 1999 the survey became a continuous program that has a changing focus on a variety of health and nutrition measurements in order to meet emerging needs. A rich variety of data—demographic and socioeconomic data; dietary information; medical, dental, and physiologic assessments; and the serum concentrations of persistent organic pollutants (POPs), including specific congeners of dioxins, furans, and PCBs—are collected through in-person interviews, health examinations, and blood samples obtained from a nationally representative sample of adults and children in the noninstitutionalized U.S. population. Information obtained from NHANES data is used to determine the prevalences of diseases, to assess nutritional status, and to establish national standards of height, weight, and blood pressure. Researchers also conduct analyses of the NHANES data for epidemiologic studies and medical research on various health outcomes using serum concentrations of various compounds to determine associations.
Starting with the preparation of Update 2008, VAO committees began seeing a stream of publications addressing the possible association of some pesticides and various individual and grouped dioxin-like chemicals with the occurrence of a variety of health outcomes as assessed by the surveys for particular temporal spans. NHANES data from 1999 to 2002 were used to evaluate the relationships of the COIs with cardiovascular disease (Ha et al., 2007); diabetes, metabolic syndrome, insulin resistance, and arthritis (D. H. Lee et al., 2006, 2007a,b,c); peripheral neuropathy and poor glycemic control (A1C ≥ 7.0%) (D. H. Lee et al., 2008); obesity via BMI and waist circumference (Elobeid et al., 2010); and
thyroid-hormone concentrations (Turyk et al., 2007). Hypertension over this time period was examined by Ha et al. (2009) and Everett et al. (2008a), but Everett et al. also provided additional information for the years 2003–2004 in a subsequent commentary (Everett et al., 2008b). Peters et al. (2014) added NHANES data for 2005–2008 to the sets for 1999–2002 and 2003–2004 previously analyzed by Everett et al. (2008a,b) for the association of blood pressure with blood concentrations of dioxin-like PCBs 126 and 169 and mono-ortho PCBs 118 and 156. Using this expanded data set, they developed a model to predict blood PCB concentrations using generally available variables (age, sex, ethnicity, and blood lipid levels). However, because only a single mono-ortho dioxin-like PCB was used in combination with PBCs having no dioxin-like activity, this work does not augment the results previously published by Everett et al. (2008a,b) for VAO purposes.
As additional cycles of NHANES were conducted and became available for research, new analyses used data collected over multiple cycles. For example, serum samples collected from NHANES participants between 1999–2004 were analyzed for organochlorine pesticides, POP residues, and dioxin-like chemicals, including PCDDs, PCDFs, and PCBs. M. R. Cho et al. (2011) reported on the associations between bone mineral density and exposures to POPs and organochlorine pesticides. Y. S. Lin et al. (2012) examined samples for levels of dioxin-like chemicals (PCDDs, PCDFs, and PCBs based on TEQs) and their associations with total and cause-specific (cardiovascular and cancer) mortality, through 2006, based on ICD-10 codes. Everett and Thompson (2014) examined the relationship between dioxins (including TCDD) and dioxin-like PCBs (TEQs were calculated for six different dioxins and eight dioxin-like PCBs) and the prevalence of diabetic nephropathy. Using 2003–2004 NHANES data, Y. M. Lee et al. (2013) evaluated the associations between toxic equivalency factors (TEFs) for organochlorine pesticides as well as PCDDs, PCDFs, and PCBs and the risk of hyperuricemia in subjects 20 years of age and older. Jones et al. (2011) examined the association between urinary arsenic and hypertension and blood pressure in NHANES 2003–2008 participants. Each of the relevant NHANES studies and their results have been summarized in detail previously. For the current update, 1999–2004 NHANES data were used to examine the relationship of serum concentrations of dioxin-like PCBs and other relevant chemicals with cancer (S. A. Kim et al., 2015; Morgan et al., 2017), diabetes and nephropathy (Everett and Thompson, 2016), cardiovascular outcomes (S. A. Kim et al., 2015), and possible indicators of immune dysfunction (Serdar et al., 2014). NHANES data from cycles 1999–2000 and 2001–2002 were used to examine the correlation between serum concentrations of dioxin-like PCBs and cognitive impairment in adults (Przybyla et al., 2017), and NHANES data from the 2011–2012 cycle were used to study whether different sets of urinary environmental chemical concentrations are risk factors of high blood pressure (Shiue et al., 2014).
Priority Toxicant Reference Range Study The study population for the Priority Toxicant Reference Range Study was a subgroup of participants aged 20–59 years in NHANES III (1988–1994), which was established to characterize the levels of 44 environmental toxicants (including 2,4-D and its metabolite 2,4-dichlorophenol) in urine and blood (regarded as indicators of internal dose). Unlike overall NHANES samples, which were established by rigorous statistical sampling procedures to be representative samples of the U.S. population, this study sample is regarded as a convenience sample because its 1,338 members had voluntarily provided an additional 20 ml of blood and had responded to an extra questionnaire during their regular NHANES medical examination (Needham et al., 1995).
Schreinemachers (2010) examined the association in 727 healthy adults between exposure to 2,4-D, as indicated by its presence in urine, and biomarkers that are linked to the pathogenesis of acute myocardial infarction and type 2 diabetes, namely, serum high density lipoprotein, triglycerides, total cholesterol minus high density lipoprotein, insulin, C-peptide, plasma glucose, and thyroid-stimulating hormone. Urinary 2,4-D was detectable in 102 (14%) samples, with concentrations of 1–28 mg/dL. The outcome variables were compared between participants with and without detectable urinary 2,4-D by using Wilcoxon’s rank-sum test.
Krieg (2013) performed a limited assessment of cognition in 700 adults. Twelve pesticide metabolites were measured in the urine, including two chemicals found in the urine after 2,4-D exposure: unmetabolized 2,4-D and 2,4-dichlorophenol. The analysis investigated the association of urine pesticide metabolite concentrations with the results of three neurobehavioral tests (simple reaction time, symbol-digit substitution, and serial digit learning).
Longitudinal Investigation of Fertility and the Environment Study
The Longitudinal Investigation of Fertility and the Environment (LIFE) Study examined environmental influences on human fecundity and fertility. Participants were 501 male partners of couples discontinuing contraception for the purposes of becoming pregnant who were recruited in Michigan and Texas during 2005–2009. Upon enrollment, in-person interviews were conducted with each male partner to ascertain health, demographic, and reproductive histories. All data and biospecimens were collected in the home, and baseline interviews were followed by a standardized anthropometric assessment for the determination of BMI conducted by research nurses who also obtained non-fasting blood (10 mL) for quantification of serum chemicals and lipids. The quantification of POPs in serum included polybrominated biphenyl 153, 9 organochlorine pesticides, and 10 polybrominated diphenyl ethers. PCBs with TEFs included 105, 114, 118, 156, 157, 167, and 189. A baseline semen sample was obtained followed by a second sample approximately 1 month later irrespective of couples’ pregnancy status. A total of 35 semen parameters were measured including 5 that reflected general characteristics
(volume, straw distance, sperm concentration, total sperm count, hypo-osmotic swollen), 8 motility measures, 12 morphometry measures, 8 morphology measures, and 2 sperm chromatin stability assay measures. Two publications from this study were identified and are reviewed in detail in Chapter 8: Mumford et al. (2015) examined the relationship between exposure to a number of persistent organic pollutants and semen quality, and Robledo et al. (2015) used blood samples from adult couples to characterize the relationship between the concentrations of a number of persistent organic pollutants and birth outcomes.
International Environmental Studies
Several studies of international populations that were environmentally exposed to the COIs have been reviewed by VAO committees. As this chapter is not intended to be a compendium of every study ever reviewed in the VAO series, only those cohorts and groups with environmental exposures that have contributed more than one study for review by VAO committees and for which new information is available are considered here. A number of reviewed studies have used data analyzed from birth cohorts. For example, results from the Norwegian Mother and Child Cohort Study on prenatal exposure to dioxin-like PCBs and health outcomes have been previously reviewed (Papadopoulou et al., 2013; Stølevik et al., 2011). The Norwegian Mother and Child Cohort Study is a prospective, population-based pregnancy cohort that recruited more than 100,000 pregnant women (resulting in about 114,000 children) and more than 75,000 fathers from 1998 to 2008 to study the causes, variability, and trajectories of diseases over the life course. The participation rate was relatively low (41%), perhaps due, in part, to the requirement to be able to fluently read Norwegian. Questionnaires were administered to collect health data, demographic factors, lifestyle exposures, and developmental progress (Magnus et al., 2016). Blood samples were collected twice from the mothers (first at the ultrasound appointment at 17–18 weeks of gestation and later after delivery) and were processed and stored. A single blood sample was collected from fathers at the ultrasound appointment. A sample from the cord blood was drawn at delivery (Paltiel et al., 2014). New results from Caspersen et al. (2016) are presented in Chapter 8.
A second birth cohort for which several published studies have been reviewed in the VAO series is the Duisburg Birth Cohort Study (Nowack et al., 2015; Rennert et al., 2012; Winneke et al., 2014). This cohort consists of 232 healthy mother–infant pairs, in which the mothers were recruited between 2000 and 2002 in Duisburg, Germany; had no serious complications or illnesses during pregnancy or parturition; and gave birth to children who were born at term (weeks 38–42 of pregnancy). Maternal blood samples were taken during weeks 28–43 of gestation, and samples of maternal milk were collected from nursing mothers during the first 3 weeks after parturition. Both samples were tested for dioxins, dioxin-like PCBs, and six indicator PCBs (Wilhelm et al., 2008).
Other prenatal exposures studies have examined exposure to endocrine-disrupting chemicals (including dioxins) in Belgian children (Delvaux et al., 2014) and birth weight and development (Halldorsson et al., 2009; Olsen et al., 2001) and childhood growth (Wohlfahrt-Veje et al., 2014) in Danish children who were exposed prenatally to dioxins and dioxin-like chemicals. Two publications that used data from the Danish Fetal Origins 1988–1989 Cohort, in which offspring were followed for 20 years, were identified for the current update. The first study examined prenatal levels of maternal POPs in serum and the risk of asthma in offspring (S. Hansen et al., 2014), and the second examined allergic sensitization and lung function in offspring (S. Hansen et al., 2016). The effects of prenatal and lactational dioxin and PCB exposure on several neurodevelopment and functioning parameters have been examined in a longitudinal assessment of Dutch children (Berghuis et al., 2014; ten Tusscher et al., 2014). However, these Belgian, Danish, and Dutch studies have potential relevance only to female Vietnam veterans with pregnancy subsequent to military service.
In addition to the many studies that used birth cohorts to examine point-in-time or longitudinal health effects of prenatal exposure to dioxins and dioxin-like chemicals, several cohorts of people who were exposed as adults to the COIs from their residential environments have been established and followed. These have included studies from the Dutch LifeLines cohort study, a multidisciplinary prospective population-based cohort study examining health and health-related behaviors of persons living in the northern region of the Netherlands (de Jong et al., 2014); Finnish fishermen and their wives who were exposed to higher amounts of dioxins and PCBs through consumption of contaminated fish (Turunen et al., 2008, 2012); and French residents in the vicinity of municipal solid-waste incinerators that had high levels of TCDD emissions, who were examined for cancer (Floret et al., 2003; Viel et al., 2000, 2008a,b, 2011) or birth defects (Cordier et al., 2004, 2010). For the current update, the subjects of studies of the effects of environmental exposures have included populations in Belgium (Den Hond et al., 2015; Van Larebeke et al., 2015), Brazil (Cremonese et al., 2017; Ueker et al., 2016), Canada (Singh and Chan, 2017; Thomas et al., 2015), China (J. Z. Yang et al. 2015; X. L. Yang et al., 2015; J. Zhang et al., 2014), France (Danjou et al., 2015; Kalfa et al., 2015; Mayhoub et al., 2014; Nicolle-Mir, 2014; Ploteau et al., 2017), Germany (Fimm et al., 2017; Haase et al., 2016; Putschogl et al., 2015), Greece (Vafeiadi et al., 2017), Hong Kong (Hui et al., 2016), Italy (Cappelletti et al., 2016), Korea (Lim et al., 2017), Nicaragua (Raines et al., 2014), Norway (Koutros et al., 2015), Russia (Galimova et al., 2015), and Spain (Martínez-Zamora et al., 2015; Paul et al., 2017).
Some environmental exposures, such as the large accidental release of TCDD in Seveso, Italy, have been the subject of multiple studies and long-term followup. For many of these populations new studies continue to be published, and those that have adequate exposure specificity and assessment are reviewed by
VAO committees. Additional background on those groups is summarized in more detail below.
Seveso, Italy
On July 10, 1976, a large industrial accident caused by an uncontrolled reaction during TCP production in Seveso, Italy, resulted in chemical release to the surrounding area that created an environmental exposure to TCDD. The degree of TCDD contamination in the soil has been used extensively as a means of imputing exposures of members of the population. Three areas were defined on the basis of soil sampling: Zone A (556 people), the most heavily contaminated, from which all residents were permanently evacuated within 20 days; Zone B (3,920), an area of lower contamination that all children and women in the first trimester of pregnancy were urged to avoid during daytime; and Zone R (26,227), a region with some contamination in which the consumption of local crops was prohibited (Bertazzi et al., 1989a,b). The sample sizes differ among follow-up studies, presumably because of migration; the sample sizes given above were reported in Bertazzi et al. (1989b).
Cohort of Entire Exposed Population
Data on serum TCDD concentrations in Zone A residents have been presented by Mocarelli et al. (1990, 1991) and by CDC (1988e). In the 10 residents who had severe chloracne, TCDD concentrations were 828–56,000 ppt of lipid weight (median 16,600 ppt). In 9 residents without chloracne (one sample was lost), TCDD concentrations were 1,770–10,400 ppt (median 4,540 ppt). TCDD was undetectable in all control participants but one. The highest of the concentrations exceeded any that had been estimated at the time for TCDD-exposed workers on the basis of backward extrapolation and a half-life of 7 years. Data on nearby soil concentrations, the number of days that a person stayed in Zone A, and whether local food was consumed were considered in evaluating TCDD, but none of those data correlated with serum TCDD, which suggested strongly that the important exposure was from fallout on the day of the accident. The presence and degree of chloracne correlated with TCDD. Adults seemed much less likely than children to develop chloracne after acute exposure, but surveillance bias could have affected that finding. More recent updates (Bertazzi et al., 1998, 2001) have not changed the exposure-assessment approach.
A number of studies of the Seveso population have used lipid-adjusted serum TCDD concentrations as the primary exposure metric (Baccarelli et al., 2002; Eskenazi et al., 2002a,b, 2003, 2004, 2005, 2007, 2010, 2014; Landi et al., 2003). Fattore et al. (2003) measured the current air concentrations of PCDDs in Zones A and B and compared them with measurements in a control area near Milan.
The authors concluded that a release from PCDD-contaminated soil did not add appreciably to air concentrations in the Seveso study area. Finally, Weiss et al. (2003) collected breast milk from 12 mothers in Seveso and compared TCDD concentrations in the milk with concentrations in a control population near Milan, and they found that the TCDD concentrations in milk from mothers in Seveso were twice as high as in controls. The authors concluded that breastfed children in the Seveso area were likely to have higher body burdens of TCDD than children in other areas.
Several cohort studies have been conducted using the Zone A, Zone B, and Zone R exposure categories. There have been multiple long-term follow-up investigations of the health outcomes, especially cancers, of Seveso residents. Bertazzi and colleagues, for example, conducted 10-year mortality follow-up studies of adults (Bertazzi et al., 1989a) and children who were 1–19 years old at the time of the accident (Bertazzi et al., 1989b, 1992), 15-year follow-up studies (Bertazzi et al., 1997, 1998), and a 20-year follow-up study (Bertazzi et al., 2001). Pesatori et al. also conducted a 15-year follow-up study to update non-cancer mortality (1998), and a 20-year follow-up of incident cancers (2009). Consonni et al. (2008) reported on the 25-year follow-up (through 2001) vital status of residents (“present”) in the Seveso area and reference territory at the time of the Seveso accident and of immigrants and newborns (“non-present”) in the 10 years thereafter. Cause-specific mortality was determined for each zone, compared with that in the comparison cohort, and adjusted for presence at the accident, sex, age, and time since the Seveso accident. Most recently, Eskenazi et al. (2018) published a review summarizing the results of research studies conducted in this population over the 40 years since the explosion as well as areas of continuing investigation, including effects in children and grandchildren of both men and women exposed to dioxin in the three zones of exposure.
In addition to a 2-year prospective controlled study of workers potentially exposed to TCDD during the cleanup of the most highly contaminated areas after the accident (Assennato et al., 1989a), other studies have examined specific health effects associated with TCDD exposure in Seveso residents—chloracne, birth defects, and spontaneous abortion—as well as crude birth and death rates (Bisanti et al., 1980); the distribution of chloracne in Seveso children (Caramaschi et al., 1981); chemicals in the blood and urine of children who had chloracne (Mocarelli et al., 1986); chloracne and peripheral nervous system conditions (Barbieri et al., 1988); dermatologic and laboratory tests in a group of the children who had chloracne and in a group of controls (Assennato et al., 1989b); health status and TCDD concentrations in chloracne cases and non-cases (Baccarelli et al., 2005a) that had been recruited previously by Landi et al. (1997, 1998); hepatic enzyme–associated conditions (Ideo et al., 1982, 1985); abnormal pregnancy outcomes (Mastroiacovo et al., 1988); cytogenetic abnormalities in maternal and fetal tissues (Tenchini et al., 1983); neurologic disorders (Boeri et al., 1978; Filippini et al., 1981); cancers (Bertazzi et al., 1993; Pesatori et al., 1992,
1993, 2008, 2009); the sex ratio of offspring who were born in Zone A (Mocarelli et al., 1996); birth weight and neonatal thyroid function (Baccarelli et al., 2008); immunologic effects (Baccarelli et al., 2002); effects on reproductive hormones and sperm quality (Mocarelli et al., 2008, 2011); aryl hydrocarbon receptor (AHR)-dependent pathway and toxic effects of TCDD in humans (Baccarelli et al., 2004); effects of TCDD-mediated alterations in the AHR-dependent pathway in people who lived in Zones A and B (Landi et al., 2003); and NHL-related (14;18) translocation prevalence and frequency in dioxin-exposed healthy people in Seveso (Baccarelli et al., 2006). Baccarelli et al. (2005b) reviewed statistical strategies for handling non-detectable readings or readings near the detection limit in dioxin-measurement datasets. They recommended that a distribution-based multiple-imputation method be used to analyze environmental data when substantial proportions of observations have non-detectable readings.
Seveso Women’s Health Study
The Seveso Women’s Health Study (SWHS) was undertaken to evaluate the association between individual serum TCDD concentrations and reproductive effects in women who resided in Seveso at the time of the 1976 accident. From a pool of 1,271 eligible women who were between infancy and 40 years old at the time of the accident, who had resided in Zone A or B at that time, and for whom adequate serum remained from the samples collected shortly after the explosion, 981 were enrolled in the study group in 1996–1998 (80% participation rate). All the women were interviewed by a nurse blinded to their exposure status, and each subset received gynecologic examinations. Medical records of those who reported ever having received a diagnosis of cancer were obtained and subjected to blind review by a pathologist. The stored samples were used for new TCDD analyses with improved analytic techniques that had become available.
As an initial step in the SWHS, Eskenazi et al. (2001) tested the validity of exposure classification by zone. Investigators measured serum TCDD in samples collected in 1976–1980 from 601 residents (97 in Zone A and 504 in Zone B). A questionnaire that the women completed in 1996–1998 included age, chloracne history, animal mortality in the vicinity, consumption of homegrown food, and the woman’s location at the time of the explosion. Participants did not know their TCDD concentrations at the time of the interview, but most knew their zones of residence. Interviewers and TCDD analysts were blinded to the participants’ zones of residence. The zone of residence explained 24% of the variability in serum TCDD. Adding the questionnaire data improved the regression model to the point that it explained 42% of the variability. Those findings demonstrate a significant association between zone of residence and serum TCDD, but much of the variability in TCDD concentration is still unexplained by the models. Warner et al. (2005) used a chemical-activated luciferase-gene expression bioassay and a high-resolution isotope-dilution gas-chromatography mass-spectrometry assay
to measure PCDDs, PCDFs, and PCBs in the serum of 78 women who resided near Seveso in order to determine average total dioxin-like chemical TEQs; the two methods produced similar results. Warner et al. (2014) compared the concentrations of TCDD in serum samples taken in 1976 and in 1996 to examine characteristics that could be used to predict 1996 TCDD concentrations. They also presented an updated estimate of the TCDD elimination half-life over the 20-year period since the uncontrolled release took place.
In one study, the women enrolled in the SWHS were assessed for cancer incidence in the 20 years following the accident (Warner et al., 2002). Warner et al. (2011) later added more than 10 years of observations on cancer incidence in the women in the SWHS, covering the period from the 1976 explosion through 2009. Of the 981 women who had participated in the first study, 833 were located, alive, and willing to participate in the second. Each was re-interviewed, provided clinical measurements, and consented to a medical record review to confirm her cancer diagnosis. A subset underwent bone-density testing. The average age was 50.8 years. An additional 45 cancers had been diagnosed, for a total of 66 cases, of which 33 were breast cancers. Thyroid cancer was the next most prevalent, with 7 cases, and the 15 other types of cancer observed had at most 3 cases. After adjusting for the women’s age at the time of the accident and for marital status, the researchers found that the association between the risk of any cancers and the lipid-adjusted, log-transformed serum TCDD concentrations at the time of the accident was significantly higher in the subjects than in controls. The availability of serum TCDD concentrations measured from blood samples gathered fairly soon after the single-substance accident (which minimizes uncertainty about what exposure had been experienced and reduces the need for back-extrapolation) contributes substantially to the value of the results.
A series of studies have examined the associations between serum TCDD and a variety of endpoints related to female reproductive functioning: menstrual cycle (Eskenazi et al., 2002a), endometriosis (Eskenazi et al., 2002b), pregnancy outcome (Eskenazi et al., 2003a), age at menarche and age at menopause (Eskenazi et al., 2005), and age at menarche in women who were premenarcheal at the time of the explosion (Warner et al., 2004). Eskenazi et al. (2007) and Warner et al. (2007) examined the incidence of fibroids and ovarian function, respectively, in SWHS participants.
Eskenazi et al. (2010) examined the relationship between serum TCDD around the time of the accident and time to pregnancy in 463 SWHS participants who had attempted pregnancy since the accident and who were no more than 40 years old at the time of the accident. The main analysis was restricted to the 278 women who had delivered live births that were not the results of contraceptive failure. Effect estimates for the associations between TCDD and fecundity and between TCDD and infertility were adjusted for several factors including maternal age, maternal smoking in the year before conception, parity, menstrual-cycle irregularity, oral-contraceptive use in the year before attempt, paternal age near
the time of conception, and the history of reproductive and endocrine conditions. Wesselink et al. (2014) examined the risk of adverse pregnancy outcomes in relation to TCDD concentrations (measured in 1996) in the SWHS among 1,211 post-chemical-explosion pregnancies through the 2008–2009 follow-up assessment. The birth outcomes that were examined included gestational age, pre-term delivery, and birth weight. Of note, only 35% of women in the analysis were age 21 or older at the time of explosion, thereby limiting the inference of this work to female veterans who served in Vietnam.
Several publications from the SWHS have been reviewed by the committee that examined health outcomes in addition to reproductive and pregnancy outcomes. These have included risk for the development of diabetes and metabolic syndrome 30 years after the accident (Warner et al., 2013), thyroid hormone levels (and disruption) in relation to TCDD concentrations measured over time (Chevrier et al., 2014), and TCDD concentrations measured in 1996 versus the bone mineral density of the spine and hip measured in 2008 (Eskenazi et al., 2014). A study of neurocognitive and physical functioning among the SWHS participants is reviewed in the current volume (Ames et al., 2018).
Japanese Environmental Studies
Several population-based studies of relevant exposures in Japan have been considered by VAO committees, including investigations of serum concentrations of PCDDs, PCDFs, and dioxin-like PCBs relative to the prevalence of diabetes (Uemura et al., 2008a), distributions with respect to various demographic characteristics (Uemura et al., 2008b), and the prevalence of metabolic syndrome (Uemura et al., 2009). In a separate analysis representative of the Japanese population, Nakamoto et al. (2013) gathered fasting blood samples from a cross-sectional sample of 1,063 men and 1,201 women (aged 15–76 years) who were living in 125 areas of 45 prefectures throughout Japan and who were not occupationally exposed to dioxins (including TCDD). The full WHO 2005 set of dioxin-like PCDDs, PCDFs, and PCBs were measured in the samples and assessed in relation to a range of self-reported history of diseases, including allergic diseases, hypertension, diabetes, hyperlipidemia, gout, thyroid disease, kidney disease, gastric ulcer, and gynecological disease. Fukuda et al. (2003) examined mortality and incinerator dioxin emissions in municipalities in Japan. The associations of adverse pregnancy outcomes and proximity of maternal residence (10 kilometers or fewer) with municipal solid waste incinerators with high dioxin emission levels at the time of birth have also been examined (Tango et al., 2004).
The emphasis of environmental studies in Japan has been on the long-term follow-up of the 1968 Yusho rice oil poisoning accident. The accident occurred in western Japan, where the rice oil intended for cooking was contaminated during processing with PCBs and PCDFs, exposing more than 1,900 people (Kuratsune et al., 1972). Based on unusual symptoms following exposure, a total of 1,961
cases of “Yusho Disease” were registered and subsequently followed for more than 40 years. Because of changes in the symptoms and advances in analytic techniques, the diagnostic criteria have changed several times since they were first published in 1968 (Akahane et al., 2017). Several studies have considered exposure status based on designation as a Yusho case, but VAO committees have generally not reviewed such studies unless the concentrations of dioxins and dioxin-like chemicals were presented, such as in Tsukimori et al. (2012, 2013) (reviewed in Update 2012), and M. C. Li et al. (2015) and Mitoma et al. (2015), which are both reviewed in the current update.
Hokkaido Study on Environment and Children’s Health
The Hokkaido Study on Environment and Children’s Health is a prospective birth cohort study that began in 2002 and includes two cohorts (Kishi et al., 2017). The first is the Sapporo (Toho Hospital) cohort with one obstetric hospital, and the second cohort is the much larger Hokkaido cohort, which has 37 hospitals and clinics. The primary study goals are to examine the effects of low-level environmental chemical exposures on birth outcomes; to follow the development of allergies, infectious diseases, and neurobehavioral developmental disorders and perform a longitudinal observation of child development; to identify high-risk groups based on genetic susceptibility to environmental chemicals; and to identify the additive effects of various chemicals, including tobacco smoking (Kishi et al., 2017).
The Sapporo cohort consists of 514 women who enrolled at 23–35 weeks of gestation and who had planned to deliver at Toho Hospital in Sapporo city between July 2002 and October 2005 (participation rate of 26.6%). A self-administered questionnaire was completed at the time of enrollment to obtain parental baseline information. Various specimens, including maternal and cord blood, maternal hair, and breast milk, were collected for the assessment of exposures to 29 dioxin and dioxin-like PCB congeners, 58 other PCB congeners, and 5 hydroxylated PCB congeners. Maternal medical and infant birth records were obtained from the hospital. Follow-ups and the administration of neurobehavioral developmental tests were conducted at ages 6 and 18 months and 3.5 and 7 years. The focus of investigations using the Sapporo cohort are on child neurobehavioral development, but the development of asthma, allergies, and infectious diseases is also examined.
The Hokkaido cohort enrolled 20,926 pregnant women before 13 weeks of gestational age who visited one of the associated hospitals or clinics in the Hokkaido prefecture between February 2003 and March 2012 (participation rate of 55%). A simultaneous analysis of 11 perfluorinated alkyl substances in maternal plasma collected during the third trimester of pregnancy was conducted. The Hokkaido cohort focuses on rare diseases such as birth defects and developmental disorders as well as on the prevalence of complicated pregnancies and birth
outcomes, such as miscarriage, stillbirth, low birth weight, preterm birth, and small for gestational age. Follow-ups of the children were conducted at 18 months and 3 years of age and began in October 2013 and January 2015, respectively. The follow-ups of 5- and 6-year-old participants started in October 2014 (Kishi et al., 2017).
Previous VAO volumes have reviewed publications from the Sapporo and Hokkaido cohorts. Four publications using subsets of the cohort data were identified and reviewed in this volume. Kobayashi et al. (2017) obtained maternal blood samples during the third trimester or within a week of delivery. The samples were tested for total dioxin levels (as the sum of 29 congeners) and genotyping for genes coding three enzymes involved in dioxin metabolism. The genotype status was previously shown to be related to birth weight in 484 children in the Hokkaido cohort. Miyashita et al. (2015a,b) investigated 70 PCB congeners, including dioxin-like PCBs, in the blood of 367 mother–child pairs from the Hokkaido Study cohort and the relationship with newborn anthropometric measurements of birth weight (small for gestational age), length, chest circumference, and head circumference. Finally, Nakajima et al. (2017) examined sex-specific differences in the effect of prenatal exposure to dioxin-like chemicals on neurodevelopment in children who were participants in the Sapporo cohort; 190 mother–infant pairs in the 6-month-old group and 122 mother–child pairs in the 18-month-old group were studied.
Russian Environmental Studies
Chapaevsk
Several studies in the Samara region of Russia have identified the Middle Volga Chemical Plant (also known as SZVH or Khimprom) in Chapaevsk, about 950 kilometers southeast of Moscow, as a major source of TCDD pollution (Revazova et al., 2001; Revich et al., 2001). From 1967 to 1987 the plant produced γ-hexachlorocyclohexane (lindane) and its derivatives, and many of the workers experienced chloracne. Since then, it has produced various chlorinated products. Dioxins were detected in the small number of air, soil, drinking-water, and cow’s-milk samples gathered in the region, but no description of how these media were sampled was given. When Revich et al. (2001) compared the samples with measurements from four other Russian cities that had industrial facilities, the TCDD concentrations observed in Chapaevsk exceeded all reported maximums. Revich et al. (2001) presented rudimentary comparisons of cancer incidence and mortality and reproductive outcomes with regional and national rates; residence in the city of Chapaevsk was used as a surrogate for exposure, and no attempt was made to create exposure categories based on factors that might have influenced the degree of TCDD exposure. The analyses of chromosomal aberrations and other cytologic indicators of genetic damage partitioned the women studied
into three groups on the basis of worker status or distance of residence from the factory (Revazova et al., 2001).
Chapaevsk Children’s Study Later research efforts on Chapaevsk residents have focused on quantifying the serum concentrations of dioxins and TEQs associated with furans and PCBs. Akhmedkhanov et al. (2002) reported on a convenience sample of 24 volunteers. The Russian Children’s Study was designed to assess the effect of in utero and childhood exposure on development. Although 516 peripubertal boys (identified through health insurance and clinic records) were enrolled, the final cohort consisted of 499 boys and 449 mothers. This prospective longitudinal study enrolled boys at age 8–9 years (in 2003–2005) who then underwent a physical exam and blood sampling and who, together with the mother or guardian, completed a questionnaire. Annual follow-up examinations were also conducted (9-year retention rate of 73%), blood is collected biennially, urine is collected annually, and semen collection began in 2012. Serum samples were used to measure 7 PCDDs, 10 PCDFs, 4 non-ortho-substituted PCBs, 6 mono-ortho-substituted PCBs, and 31 other non-dioxin-like PCBs.2 Although the design does not allow researchers to isolate possible in utero exposure and postnatal exposure and its utility is further limited by the fact that subjects were exposed to dioxins in a different period of their lives (infancy, childhood, and adolescence) than Vietnam veterans, the exposures are well characterized. The information generated by this cohort will be relevant to VAO reports only in conjunction with effects in offspring after maternal exposure to the extent that the consequences of gestational and childhood exposure can be distinguished. The published findings have detailed the characterizations of serum concentrations in the boys (J. S. Burns et al., 2009) and their mothers (Humblet et al., 2010), and the first papers that examine semen parameters are detailed in Chapter 8 (Mínguez-Alarcón et al., 2017). The committee also heard an invited presentation from the lead researcher, Dr. Russ Hauser, and is able to offer a bit more detail regarding initial findings based on his presentation.
Swedish Environmental Studies
Most Swedish environmental studies have focused on results from the Prospective Investigation of the Vasculature in Uppsala Seniors (PIVUS) study. Participants were recruited within 2 months after their 70th birthdays randomly from the registry of residents of the community of Uppsala, Sweden, between April 2001 and June 2004. The primary aim was to investigate cardiovascular disease (CVD) in an elderly population. Of the 2,025 subjects who were invited to participate, 1,016 were included, for a participation rate of about 50%; half
___________________
2 Dr. Russ Hauser, Harvard T.H. Chan School of Public Health, presentation to the committee November 30, 2017.
of the participants were female. All participants answered a questionnaire about their medical history, medications, diet, and smoking habits. The burden of POPs, including several dioxin-like PCBs, was assessed from blood serum or plasma. However, the results are limited by the fact that participants were recruited in the 2-month period after their 70th birthday. This potentially imparts a survival bias, meaning that persons from the catchment area with very high levels of POPs may have been disproportionately excluded from the study sample. In addition, results are limited by the relative non-specificity of the POPs examined, although the battery of congeners did include octachlorodibenzo-p-dioxin, which is relevant to Vietnam veterans.
VAO committees have reviewed several studies from the PIVUS data or subsets of it. The subjects of these studies have included sex differences in the concentrations of 17 of 21 POPs (Salihovic et al., 2012a); a new method for extracting POPs from human blood (Salihovic et al., 2012b); and associations between POPs and type 2 diabetes (D. H. Lee et al., 2011), fat mass and abdominal obesity (D. H. Lee et al., 2012a; Rönn et al. 2011), stroke (D. H. Lee et al., 2012b), and carotid atherosclerosis (Lind et al., 2012). Many other studies from the PIVUS cohort have examined relationships between POPs and surrogate health outcomes, including CVD measures and risk factors; examples include left ventricular systolic and diastolic dysfunction (Sjöberg Lind et al., 2013b), left ventricular hypertrophy (Sjöberg Lind et al., 2013a), and carotid atherosclerosis (Lind et al., 2012). In addition to these health outcomes, changes in weight (Lind et al., 2013), inflammatory markers, complement system, and oxidative stress (Kumar et al., 2014a,b,c) have also been studied. These studies augment previous publications from PIVUS that examined a range of indicators related to CVD and cardiovascular health. The topics of new publications from the PIVUS cohort reviewed in this volume include outcomes of hypertension (Lind et al., 2016), circulating lipid levels (Penell et al., 2014), and cognitive impairment (D. H. Lee et al., 2014).
Other studies of Swedish cohorts have also been included in the VAO series when the exposures have been relevant.
Taiwanese Environmental Studies
Two populations with environmental exposures in Taiwan have been examined by VAO committees: residents of contaminated areas and mother–child studies. The first type of studies primarily examined people who resided near a closed factory in the An-nan District of Tainan City in southwestern Taiwan that had manufactured PCP, which left the area highly contaminated with dioxin. Na-PCP, a widely used pesticide, had been used in the production process at the abandoned factory, and after the factory shut down, a large quantity was improperly stored and later released into the environment. A cross-sectional study was conducted in 2005–2007 using subjects recruited from a health center near the
factory, and the final sample consisted of about 80% of the invited residents of the community. A series of publications using these data have been reviewed by prior VAO committees, an overview of which is provided here. The general limitations for all those studies include an unknown age at first exposure to PCDDs and PCDFs; an unknown duration of exposure; the cross-sectional design; an adjustment for obesity as one element of metabolic syndrome, rather than BMI; and some arbitrary choices inherent in factor analysis. J. W. Chang et al. (2010) used these data to report on the relationship between exposure to PCDDs and PCDFs and hypertension in metabolic syndrome in 1,490 non-diabetic people residing in this area. In addition, an analysis of the association between each congener and the prevalence of metabolic syndrome was conducted. J. W. Chang et al. (2011a) then reported on the same cross-sectional study, restricted to 1,449 non-diabetic residents, to investigate the joint effects of exposure to dioxins (from the factory) and mercury (from eating contaminated seafood from the reservoir near the factory) on pancreatic endocrine function; the committee noted several limitations with the study’s analysis and methods for assessing insulin-resistance. Using the same cross-sectional study with enrollment extended to December 2009, J. W. Chang et al. (2011b) investigated the association between PCDD and PCDF exposure and continuous measures of CVD within 10 years as measured by the Framingham Risk Score, a formula for combining established risk factors into a single number, using a sample of 914 residents who did not have CVD and who were 30–45 years old. One limitation is the use of the Framingham score; other factors are associated with risk but were not included in the score, such as socioeconomic position, genetics, and imaging biomarkers. A fourth publication using this cross-sectionally collected data involved 1,167 residents who were more than 50 years old and had fasting blood samples available to investigate the biochemical profiles of those exposed to PCDDs and PCDFs (J. W. Chang et al., 2012). For this analysis, there were three exposure groups of retired Na-PCP workers: those who still lived locally, those who lived locally but did not knowingly eat polluted fish, and those who had moved away. Three control groups did not include any Na-PCP workers and consisted of local residents who had eaten polluted fish, local residents who had not eaten polluted fish, and “background participants” in Taiwan’s general population. The first two of the control groups made up the 1,167 in the study population. The limitations of the study include the unknown PCDD and PCDF concentrations in retired workers who moved away and knowledge about when the exposure ceased. There may also be important unmeasured confounders related to which workers moved away and which ones did not.
Three new studies among the residential population near this factory were identified and reviewed in the current volume. The outcomes examined are type 2 diabetes (C. Y. Huang et al., 2015), chronic kidney disease (C. Y. Huang et al., 2016), and hyperuricemia (J. W. Chang et al., 2013).
The second type of relevant environmental exposure studies conducted in the Taiwanese population are mother-and-child studies, which have been reviewed
in Chapter 8. These have included findings from a prospective study of healthy Taiwanese mothers and their children recruited during the mothers’ pregnancy to study the associations between exposures to PCDDs, PCDFs, and PCBs and health outcomes (Chao et al., 2004, 2007; P. H. Su et al., 2010, 2012; S. L. Wang et al., 2004, 2005). The study enrolled pregnant women who had no clinical complications, were 25–35 years old, and delivered in the period December 1, 2000, to November 30, 2001, in a medical center in central Taiwan, the location of a solid-waste incinerator. Participants completed a questionnaire concerning maternal age, occupation, disease history, cigarette smoking, alcohol consumption, dietary habits, and the baby’s stature. Biologic samples (including placenta, umbilical cord blood, mother’s venous blood, and breast milk) were collected for analysis of PCDDs, PCDFs, and PCBs. A total of 610 women were enrolled (80% of those invited). The placenta was collected from and the questionnaire completed by 430 participants. Of those, 250 provided sufficient venous blood for the chemical analyses. Of the 250, 175 provided adequate breast-milk samples. S. L. Wang et al. (2004) reported on PCDDs, PCDFs, and PCBs in the biologic samples and on correlations among specimens. Chao et al. (2004) reported on PCDDs, PCDFs, and PCBs in breast milk and the cumulative dose derived for infants exclusively breastfed versus those formula-fed. In a follow-up analysis, S. L. Wang et al. (2005) examined the association between high and low in utero exposures to PCDDs, PCDFs, and PCBs and the thyroid and growth hormones in the newborns overall and by sex. S. L. Wang et al. (2006) examined the association between PCDDs, PCDFs, and PCBs measured in the placenta and estrogens and metabolites measured in mothers’ blood. P. H. Su et al. (2010) reported on the 2-year and 5-year follow-ups of the mother–child pairs of S. L. Wang et al. (2005). Children’s anthropomorphic measures were obtained, including height, weight, BMI, head circumference, chest girth, bone age, and the ratio between bone age and chronologic age. Thyroid, sex-hormone, and growth-factor concentrations were measured in venous blood samples obtained from those children whose mothers’ serum PCDD and PCDF TEQs were available. The anthropomorphic measures and the thyroid, sex-hormone, and growth-factor concentrations were compared in children with high (≥15 pg-TEQ/g of lipid) versus low (< 15 pg-TEQ/g of lipid) in utero PCDD and PCDF concentrations. Comparisons were made by sex and by pooling all children. P. H. Su et al. (2012) reported on the 8-year follow-up of the same cohort in a subset of 23 boys and 33 girls. In addition to anthropomorphic measures used in previous waves, reproductive development (breast, genital, and armpit stages) was assessed. P. H. Su et al. (2015) conducted a study of 56 children from the cohort stratified into high- and low-exposure groups based on maternal PCB and PCDD/F concentrations to examine hormone levels and other measures of blood chemistry.
Other studies of health effects in offspring prenatally exposed to the COIs in Taiwan have been reviewed, but they have been from different population samples.
Vietnamese Environmental Studies
Various epidemiologic studies have been conducted in subsets of the Vietnamese population who were exposed to the herbicide spraying that occurred during the Vietnam War. In a review paper, Constable and Hatch (1985) summarized the unpublished results of studies conducted by researchers in Vietnam. They also examined nine reports that focused primarily on reproductive outcomes (Can et al., 1983a,b; Huong and Phuong, 1983; Khoa, 1983; Lang et al., 1983a,b; Nguyen, 1983; Phuong and Huong, 1983; Trung and Chien, 1983). Vietnamese researchers later published the results of four additional studies: two on reproductive abnormalities (Phuong et al., 1989a,b), one on mortality (Dai et al., 1990), and one on hepatocellular carcinoma (Cordier et al., 1993). Ngo et al. (2006) published a meta-analysis that addressed an association between exposure to herbicides in Vietnam and birth defects and that covered some reports reviewed previously by Constable and Hatch (1985), some new Vietnam studies, and studies on U.S. and Australian veterans who served in Vietnam.
In general, three types of environmental studies have been conducted in Vietnam and reviewed by VAO committees: those that have measured environmental concentrations of contaminants in soil or animals (food) in “hot spot” areas such as Bien Hoa City (Schecter et al., 2003), studies of mother–child pairs and concentrations of dioxins in breast milk, and surrogate measures of health outcomes in adults in contaminated areas. In total, 10 new studies of outcomes in the Vietnamese population were identified and reviewed for the current volume.
C. H. Nguyen et al. (2017) examined serum TCDD levels and the expression of AHR and a variety of pro-inflammatory cytokines in people living in areas that were sprayed with herbicides and in areas that were not. Two studies (S. Hansen et al., 2009; Nhu et al., 2009) examined maternal concentrations of organochlorine chemicals and dioxins in communities known to have been sprayed with herbicides during the war compared with communities that were not sprayed. However, no results were reported on associations between the concentrations of these chemicals in mothers and health status in mothers or infants. Two new studies of mothers and their children in different herbicide-contaminated and non-contaminated areas in Vietnam were reviewed in the current volume (Anh et al., 2017; Van Tung et al., 2016).
Several studies have examined mother–infant pairs who were living near the Da Nang airbase, the site of a former U.S. airbase, which is an area of documented high exposures to TCDD and other PCDD/Fs. The Da Nang Birth Cohort consists of 216 mother–infant pairs recruited in 2008–2009. The recruitment and residence area includes two districts in a surrounding area of 10 kilometers from the former air base. This is because the residents outside the immediate area of the airbase have also been shown to have high dioxin levels suspected to have been caused by the ingestion of contaminated food and water originating from the airbase. Breast-milk samples were collected from each nursing mother 1 month after
she gave birth in order to quantify the levels of 17 different 2,3,7,8-substituted PCDD and PCDF congeners, and TEQs were calculated.
Tai et al. (2013) examined 216 mother–infant pairs and relationships between the dioxin levels in breast milk and infant neurodevelopment parameters (based on the Bayley Scales of Infant and Toddler Development) at 4 months of age. Tai et al. (2016) followed the birth cohort longitudinally for neurodevelopment and physical growth during the first 3 years of life. In Pham et al. (2015), the Bayley Scales of Infant Development, 3rd edition, was administered at age 12 months to examine differences in overall cognition, language composite, receptive language and expressive language, and motor skills. Nishijo et al. (2014) examined 153 mother–infant pairs in the Da Nang birth cohort to evaluate potential associations between perinatal dioxin exposure and autism spectrum disorders in the children. Nishijo et al. (2015) focused on urinary metabolite levels in 26 children who were part of the study cohort and examined associations with dioxin-exposure-induced neurodevelopmental deficits. Using this same birth cohort, Tran et al. (2016) investigated effects of early life exposure to dioxins in 176 children. Dioxins were measured at birth and 5 years of age and compared with outcomes of the Movement Assessment Battery for Children-2 test and other tests of pattern reasoning, planning ability, and neurodevelopmental skills.
Although they are not a primary health outcome of interest per se, X. Sun et al. (2013) compared prostate-specific antigen levels (which may be indicative of a risk for prostate cancer, but is not a surrogate of prostate cancer) in a cross-sectional study of men over the age of 50 years residing in the Phu Cat district (a presumed contamination hot spot, n = 101) with those residing in the Kim Bang district (presumed non-sprayed, n = 97). Analyses were adjusted for age and included stratification by occupation, including farmers and other non-farm occupations. Results of this study are limited by its cross-sectional design and, in particular, the relatively crude measurement of exposure assessment many years after the time when herbicide spraying would have occurred. In a second study by X. L. Sun et al. (2014) that used similar methodology and surrogate indicators of health (and thus has similar limitations), serum dioxin and steroid hormone levels were compared between 48 men in the presumed hot spot area (Phu Cat district) and 36 men in the non-sprayed area (Kim Bang district). Five dioxin congeners expressed as TEQs were calculated along with the levels of nine serum steroid hormones, including testosterone, cortisol, estradiol, and others. Multiple linear-regression analyses were conducted with statistical adjustments made for age, BMI, employment status, and tobacco use.
Using the same study population as in prior studies (X. L. Sun et al., 2013, 2014), two new publications compared steroid hormone levels and other blood chemistry between men residing in the presumed hot spot area and men residing in the non-sprayed area (X. L. Sun et al., 2016, 2017). However, these studies are somewhat limited in that these measures do not serve as indicators or even surrogates of health conditions or diseases of primary concern to Vietnam veterans.
CASE-CONTROL STUDIES
Numerous case-control studies have been reviewed in previous updates, some of which have produced multiple publications on the same population or dataset. For example, several case-control studies of specific cancers, such as STS, HL, and NHL, in Sweden were carried out to investigate exposure to phenoxyacetic acids and other relevant COIs (Eriksson et al., 1979, 1981, 1990; Hardell, 1977, 1979, 1981; Hardell and Bengtsson, 1983; Hardell and Eriksson, 1988, 1999; Hardell and Sandström, 1979; Hardell et al., 1980, 1981, 2002; Olsson and Brandt, 1988; Persson et al., 1989, 1993; Wingren et al., 1990). Similarly, overlapping case-control studies have been conducted among New Zealanders exposed to phenoxy herbicide and chlorophenols examining incidence and mortality from specific cancers (Pearce et al., 1985, 1986a,b, 1987; Smith and Pearce, 1986; A. H. Smith et al., 1983, 1984). Other case-control studies conducted internationally have addressed the connection between the COIs and various cancers in England (Balarajan and Acheson, 1984; Magnani et al., 1987), France (Aras et al., 2014; Orsi et al., 2009), Italy (Amadori et al., 1995; Donna et al., 1984; LaVecchia et al., 1989; Musicco et al., 1988; Nanni et al., 1996; Vineis et al., 1986), Canada (McDuffie et al., 1990; Ng et al., 2010; Spinelli et al., 2007), Australia (Smith and Christophers, 1992), and Denmark (Mellemgaard et al., 1994).
Case-control studies have been conducted in various U.S. populations looking for associations of herbicides with cancers. Studies have included leukemia mortality among white farmers in Nebraska (Blair and Thomas, 1979; Blair and White, 1985), Iowa (Burmeister, 1981; Burmeister et al., 1982), and in Iowa and Minnesota (L. M. Brown et al., 1990). Another study investigated associations of leukemia and NHL with 2,4-D in eastern Nebraska (Zahm et al., 1990). Other lymphohematopoietic cancer outcomes investigated as case-control studies in U.S. populations include NHL (Cantor, 1982; Cantor et al., 1992; Czarnota et al., 2015; Hartge et al., 2005; Tatham et al., 1997; Zahm et al., 1993), multiple myeloma (Boffetta et al., 1989; L. M. Brown et al., 1993; Morris et al., 1986), and NHL and HL (Dubrow et al., 1988). Other studies have assessed, generally using occupation or residence as surrogates for exposure, multiple cancer outcomes, such as gastric cancer, prostate cancer, NHL, and multiple myeloma (Burmeister et al., 1983); STS, HL, and NHL (Hoar et al., 1986); and STS and NHL (Woods and Polissar, 1989; Woods et al., 1987). In a subset of participants in the Hartge et al. (2005) study, De Roos et al. (2005a) studied associations between the overall TEQs of PCBs, furans, and dioxins but not TCDD alone.
Non-cancer health outcomes have also been investigated in case-control studies: birth defects and congenital anomalies (Blatter et al., 1997; García et al., 1998; Nurminen et al., 1994), spontaneous abortion (Carmelli et al., 1981), mortality from neurodegenerative diseases associated with occupational risk factors (R. M. Park et al., 2005; Schulte et al., 1996), and Parkinson disease (Firestone et al., 2005, 2010; Liou et al., 1997; Seidler et al., 1996; Semchuk et al., 1993).
Again, as this chapter is not intended to be a compendium of every study ever reviewed in the VAO series, only those cohorts and groups that have contributed more than one study for review by VAO committees and for which new information is available are considered here. A full account of every study ever reviewed in the VAO series that has provided evidentiary weight for an association between exposure to the COIs and a health outcome can be found in the supplementary tables (available at www.nap.edu/catalog/25137), and details of the studies can be found in the corresponding report for which they were first identified and reviewed by a VAO committee. Some additional information may be found in the subsections of “Conclusions from VAO and Previous Updates” for an outcome throughout the chapters.
National Birth Defects Prevention Study
The National Birth Defects Prevention Study (NBDPS) is a population-based case-control study conducted cooperatively by CDC and eight monitoring centers throughout the United States (in Arkansas, California, Georgia, Iowa, Massachusetts, New Jersey, New York, and Texas) using a standardized study methodology (Yoon et al., 2001). Starting in October 1, 1997, the individual centers began monitoring births in their respective areas for the occurrence of more than 30 types of birth defects (excluding cases attributable to single-gene conditions or chromosomal abnormalities) for comparison with randomly selected sets of live-born babies without malformations. Information about demographics and possible exposures is abstracted from an extensive telephone interview that the mothers complete within 24 months of delivery. On the basis of the work histories, job classifications are assigned by an industrial hygienist and processed using a job-exposure matrix and expert opinion used to derive occupational exposures. Buccal epithelial samples are gathered for DNA testing from the infant and its parents. Major limitations of the study are the lack of exposure specificity (e.g., using general categories of insecticides, herbicides, and fungicides), crude exposure histories (ever/never), lack of exposure concentrations or durations, and the use of self-report, which may introduce recall bias especially among mothers whose child has been diagnosed with a birth defect. Despite those limitations and the fact that the results are only potentially relevant to child-bearing female Vietnam veterans, several publications using data from all of the NBDPS or just subsets of the NBDPS have been reviewed by VAO committees.
Rocheleau et al. (2011) reported on the association between maternal occupational pesticide exposure and the risk of hypospadias in the NBDPS using a sample of 647 cases of hypospadias and 1,496 controls with estimated delivery dates of October 1997–December 2002. Most exposure was to insecticides only or to three types of pesticides (insecticides, herbicides, and fungicides), but there was generally a low level of occupational pesticide exposure in the study population. The lack of exposure specificity made it difficult to make an association
between the birth defects and any pesticide exposure or an individual pesticide exposure, and other exposures of the population could have contributed to the outcome in question. In a separate analysis of NBDPS data, Kielb et al. (2014) analyzed the occurrence of isolated craniosynostosis, gastroschisis, diaphragmatic hernia, or transverse limb deficiencies in children born to employed women with due dates between October 1, 1997, and December 31, 2002. Cases included 871 live-born, stillborn, or electively terminated fetuses, which were compared to 2,857 live-born control infants. The odds of the appearance of these musculoskeletal malformations were examined in relation to periconceptional maternal occupational exposure to insecticides, herbicides, or fungicides (classified as yes/no) for each job held during the period of 1 month pre-conception through 3 months post-conception.
Several papers from the California Center (in the San Joaquin Valley) of the NBDPS have been published, although many of the same limitations apply as for analyses with the full NBDPS. The center has monitored deliveries from 1997 to 2006 and has invested considerable effort toward developing time-specific estimates of exposure to individual pesticides by women residing in the area at the time of delivery. Carmichael et al. (2014) evaluated 569 medically confirmed congenital heart defect cases (8 different types) and 785 non-malformed controls born during 1997–2006. Maternal pesticide exposure was crudely classified as “any” versus “no exposure” based on the commercial application of pesticides within a 500-meter radius of the mother’s address during a 3-month periconception window (determined by data obtained from the California Pesticide Use Report record system). Exposure to individual pesticides was examined, including the dimethylamine salt of 2,4-D. Analogous investigations were conducted on neural tube defects and orofacial clefts (W. Yang et al., 2014) and on gastroschisis (Shaw et al., 2014).
Several new publications from the NBDPS were identified for the current update. Makelarski et al. (2014) and Pettigrew et al. (2016) both examined associations of spina bifida with parental non-specific herbicide exposure. Rocheleau et al. (2015) examined the association between maternal occupational exposure to fungicides, insecticides, and herbicides and the risk of congenital heart defects among offspring. Specific publications from the California Center of the NBDPS included studies of gastroschisis (Shaw et al., 2014) and anotia/microtia, anorectal atresia/stenosis, transverse limb deficiency, craniosynostosis, and diaphragmatic hernia (Carmichael et al., 2016).
Upper Midwest Health Study
The Upper Midwest Health Study (UMHS) was initiated by NIOSH as a population-based case-control study of cancer risk in a non-metropolitan Midwestern U.S. population. Several reports from the study were reviewed in previous updates. Chiu et al. (2004) and W. J. Lee et al. (2004a) conducted pooled
analyses of two earlier case-control studies of NHL carried out by the UMHS in Iowa and Minnesota (Cantor et al., 1992) and in Nebraska (Zahm et al., 1990). Chiu et al. (2004) examined the association of NHL with agricultural pesticide use and familial cancers, and W. J. Lee et al. (2004a, 2006) looked at NHL in asthmatic people who reported pesticide exposure. Data from Nebraska (B. C. Chiu et al., 2006, based on Zahm et al., 1990, 1993) were used to determine if the risk of NHL was driven by any specific subtypes. Tissue samples were analyzed from 172 of 385 cases for the presence of a specific chromosomal translocation (t(14;18)(q32;q21)). Two studies focused on pesticide use and the risk of adenocarcinomas of the stomach and esophagus (W. J. Lee et al., 2004b) and the risk of gliomas (W. J. Lee et al., 2005) in white Nebraska residents over 21 years old who were identified from the Nebraska Cancer Registry and matched to controls drawn from an earlier study by Zahm et al. (1990). Other publications evaluated farm pesticide exposure in men (Ruder et al., 2004) and women (Carreon et al., 2005) in Iowa, Michigan, Minnesota, and Wisconsin in relation to gliomas as part of the UMHS. Ruder et al. (2006) reported a follow-up of Ruder et al. (2004) that evaluated gliomas in UMHS participants, but the new analyses provided no evidence of a greater use of pesticides in cases than in controls, and agents were not specified. Ruder et al. (2009) reported another follow-up in the same group, which had similar findings and, again, provided no specificity of agents. Finally, Yiin et al. (2012) has reported findings from new analyses of the UMHS sample that incorporated more detailed exposure information that was not used in previous analyses, including years of use and estimated cumulative exposures to categories of pesticides, including phenoxy herbicides, and the use of specific agents, including 2,4-D and dicamba.
Cross-Canada Study of Pesticides and Health (Rare Tumors Study)
The Cross-Canada Study of Pesticides and Health (Rare Tumors Study) was designed as a full population-based case-control study of men in six Canadian provinces to address the relation of four relatively uncommon malignancies—HL, NHL, multiple myeloma, and STS—with occupational and domestic exposure to pesticides (McDuffie et al., 2001). A target number of cases of each cancer type was preset for each province. Researchers gathered incident cases that were diagnosed starting on September 1, 1991, from the provincial cancer registries (or hospital records) in Québec until the end of 1994 or until the target number was reached. People who had Kaposi sarcoma or who were HIV positive were excluded. Physician consent was obtained, and diagnoses were confirmed with pathology reports and a review of preserved tissues. Consent forms and questionnaires were sent to the cases. The controls were men at least 19 years old identified in the health-insurance records of Alberta, Manitoba, Saskatchewan, and Québec; from telephone listings for Ontario; and from voter lists in British Columbia. The controls were selected randomly to obtain a stratified age distribution matching
that of the cases, and they were sent consent forms and questionnaires. All 1,506 controls who responded were used in comparisons for each of four cancer groups: 316 HL cases, 517 NHL cases, 342 multiple myeloma cases, and 357 STS cases.
The postal questionnaire gathered standard demographic information, personal and family medical histories, employment history, smoking behavior, and basic data on pesticide exposure. The pilot study tested the reliability of self-reported pesticide use by comparison with purchase records. Any subject who reported at least 10 hours of pesticide exposure per year was asked to complete a telephone questionnaire on the details of the pesticide exposure; in addition, 15% of the remaining subjects were randomly selected to answer the telephone survey. A conditional logistic regression stratified on age and province and adjusted for all covariates found to be associated with the outcome at the 0.05 level of significance was used to estimate odds ratios for specific active ingredients, including dicamba and the phenoxy herbicides 2,4-D, Mecoprop, MCPA, and diclofop-methyl. Dose–response relationships were investigated for the cumulative time spent in mixing or applying particular products.
A series of publications have addressed the relationship between each of the cancers and various risk factors. Those pertaining to herbicides overall or to the particular ones of interest are as follows:
- HL: Karunanayake et al. (2012); P. Pahwa et al. (2003)
- NHL: Hohenadel et al. (2011); McDuffie et al. (2001)
- Multiple myeloma: P. Pahwa et al., (2003, 2012)
- STS: P. Pahwa et al., (2003, 2011)
A number of other publications arising from that dataset have addressed topics somewhat more tangential to the interests of the VAO reports. For instance, McDuffie et al. (2005) and P. Pahwa et al. (2006) considered the possible role of exposure to insect repellents, particularly DEET and phenoxy herbicides, in the genesis of the malignancies in question. McDuffie et al. (2009) examined family histories of cancers in first-degree relatives of the study participants to assess the interaction between family history and pesticide exposure. Hohenadel et al. (2011) investigated how various combinations of pesticide exposures influenced the occurrence of NHL. Ghosh et al. (2011) investigated the association of occupational exposures other than pesticides with the occurrence of multiple myeloma. M. Pahwa et al. (2012) examined the interactions between self-reported pesticide exposures and self-reported measures of immune suppression (asthma, allergies, hay fever) and the risk of NHL, but this analysis is limited by the use of self-reported measurements of immunologic conditions and the non-specific and crude self-report classification of pesticide use, which did not characterize exposure use by duration, intensity, or frequency. Similarly, Navaranjan et al. (2013) examined HL relative to the number of pesticides to which an individual reported exposure and to estimates of work-related exposure and home-related
exposure, grouped by class (herbicides, insecticides, and fungicides). This study is also limited by the relatively nonspecific and crude self-report classification of pesticide use, which significantly limits direct inference to the effects of herbicide exposure during military service in Vietnam.
This page intentionally left blank.