
“The U.S. immigration system is not ruled by logic,” said Walter Ewing, senior researcher at the American Immigration Council. “It has been created from a long series of political compromises among U.S. lawmakers driven by all sorts of contradictory motivations, some of which have little if anything to do with immigration,” he said.
In the first two sessions of the workshop, Ewing and two other presenters—Antonia Villarruel, Margaret Bond Simon Dean of Nursing at the University of Pennsylvania School of Nursing, and Karthick Ramakrishnan, associate dean of the University of California, Riverside, School of Public Policy, and professor of public policy and political science—provided a historical overview and a current snapshot of immigration policy in the United States. Debates over integration are not new, said Villarruel, adding that “they are part of a continual story of us as Americans.” They emerge from “a juxtaposition of two diverging ideologies: nationalism and inclusion,” she said.
ADVENT AND DECLINE OF THE QUOTA SYSTEM
The naturalization acts passed in the years shortly after the creation of the United States, which restricted citizenship to “free white persons,” governed naturalization policy for much of the 19th century, Villarruel began. A series of Chinese exclusion acts in 1882, 1892, and 1902, borne partly out of economic concerns in the western United States, banned Chinese laborers from immigrating and barred Chinese immigrants who already resided in the United States from naturalizing.
The Emergency Quota Act of 1921 and the Immigration Act of 1924 established immigration quotas based on the existing population of the United States, Villarruel continued. Following passage of these acts, most of the immigrants coming to the United States were from Europe, with immigration from Asian countries still barred. These immigration acts generally did not deal with the Western Hemisphere, though a set of agreements around World War II were designed to bring primarily Mexican immigrants to the United States to meet labor shortages. As Ewing described the period after 1924, “Northern and western Europeans were in, and everybody else was effectively out—except for Mexicans and other inhabitants of the Western Hemisphere, who were left outside of the quota system due to their usefulness as easily exploited agricultural laborers.”
The position of nativists gradually eroded after the 1920s for a number of reasons, Ewing said. The eugenic concept of white racial superiority on which the quota system was based was thoroughly discredited in scientific circles by the 1950s. “In addition,” Ewing pointed out, “at the height of the Cold War, it seemed hypocritical of the U.S. government to decry communism but to not offer refuge to people who had fled communist regimes.” The Civil Rights Movement was growing in the 1950s and 1960s,
highlighting the racism that made African Americans second-class citizens even as race served as the foundation of the immigration system. “Finally,” noted Ewing, “over the course of the 4 decades during which the quota system was in force, generations of immigrants had successfully integrated into U.S. society and given birth to very Americanized children.” (Box 2-1 provides differing definitions of the term immigrant.)
1965 IMMIGRATION AND NATIONALITY ACT
The year 1965 was a major turning point in U.S. immigration policy. One year after the Civil Rights Act passed, the Immigration and Nationality Act of 1965 dismantled the national origins quota system. The new system allotted 170,000 visas to immigrants from the Eastern Hemisphere (with a 20,000 per-country limit) and 120,000 to the Western Hemisphere (with no per-country limit, although one was added in later years). Within these broad numerical caps, visas would go to the family members of legal immigrants (family members of U.S. citizens were—and still are—exempt from the caps), workers needed by U.S. employers, and refugees. “The authors of the bill did not expect it to have much of an effect on immigration overall, arguing that the benefits of the new system would flow primarily to Europeans with family members in the United States—not to Asians or Africans,” Ewing said, adding that “in hindsight, the authors of the bill were obviously very wrong.”
Growing economic inequality between the developed and less developed world made the developed world an attractive destination for people who wanted a chance for a better life. The forces of globalization rendered the nations of the world increasingly interconnected in terms of trade, transportation, and communication. “The end result was that, over the course of the decades following the 1965 immigration law, millions of people from Latin
America, the Caribbean, and Asia journeyed to the United States—some legally, some not,” said Ewing. As a result of these trends, noted Villarruel, Mexicans became the nation’s largest immigrant group, and by 2013 they were the largest immigrant group in 33 states.
As immigration in general, and undocumented immigration in particular, increased during the 1970s and 1980s, policy debates broke out over whether immigration was a net benefit to the United States or a threat. On one side of this debate, said Ewing, were organizations devoted to the advancement of rights for immigrants, refugees, Latinos, and Asians, which argued that immigrants were an economic and cultural asset to the nation. On the other side was a new generation of nativists who couched their anti-immigrant arguments in terms of immigration’s contribution to the “overpopulation” of the United States, resulting in increased competition for jobs, housing, schools, and other public services. Ewing said:
While these new nativists didn’t use the terminology of eugenics and “racial betterment” that the prior generation of nativists had, the imagery provoked by their rhetoric was clear: the dark-skinned hordes of the developing world would overrun the light-skinned peoples of the developed world unless drastic action was taken.
IMMIGRATION REFORM AND CONTROL ACT AND SUBSEQUENT LEGISLATION
In the face of large-scale undocumented immigration—and in an attempt to balance the demands of employers, immigrant rights groups, and nativists—Congress passed the Immigration Reform and Control Act (IRCA) in 1986. The act granted legal status to many of the undocumented immigrants already living in the country, opened the doors to hundreds of thousands of new agricultural guest workers from Mexico, and increased border enforcement. In addition, it created criminal penalties for employers who knowingly hired undocumented workers.
However, “the law ran aground for a couple of reasons,” observed Ewing. First, it did not create flexible avenues for future immigration to the United States. As the economic integration of the Western Hemisphere increased—a process culminating in the North American Free Trade Agreement (NAFTA) of 1994—the movement of workers was not liberalized in the same way as the movement of commodities. “Ironically, NAFTA’s supporters had predicted that it would decrease undocumented migration by creating more jobs in Mexico,” said Ewing, adding:
That didn’t happen as planned. In fact, competition from U.S. multinational corporations drove many Mexican workers out of their jobs or off their farmland. And newly unemployed Mexicans knew that the best place to go in search of a new job was the United States.
A second reason for IRCA’s long-term failure was the poor design and implementation of sanctions for employers who knowingly hired undocumented workers. “Proving whether someone knowingly or unknowingly hires an undocumented immigrant is not an easy task,” Ewing observed. Criminal penalties against employers were rarely enforced, nor were labor laws, which might have diminished the exploitation of workers in general, regardless of where they were born. In addition, many of the numerous documents deemed acceptable as proof of legal residence in the United States were easily forged.
As the law proved ineffective, hundreds of thousands of immigrants and refugees from every corner of the globe came to the United States each year. “In the process, they created new neighborhoods or breathed life into old, decaying ones,” Ewing pointed out. But, as a result, the cultural landscape of many regions in the United States shifted dramatically. “For instance, in some cities, Spanish-language media outlets now have more viewers than their English-language competitors,” he said.
This transformation of U.S. society has provoked a nativist backlash, Ewing pointed out. Some native-born Americans are irate that their tax dollars might pay for the education of children whose parents are undocumented. Others are incensed that they have to “press one for English, two for Spanish” when they call their bank, he continued. This anger contributed to the passage of Proposition 187 in California in 1994, which would have denied virtually every public service (including education) to undocumented immigrants and their children. It also would have required every public employee, from teachers to doctors, to report undocumented immigrants to federal authorities. “Proposition 187 was struck down as unconstitutional in federal court and never took effect,” said Ewing, adding:
However, it did propel Republican Pete Wilson into the governor’s mansion in 1994, thanks to his support for the initiative and a campaign based on nativist fears of an undocumented Mexican invasion of the state. Much to the chagrin of nativists, Wilson and Proposition 187 motivated tens of thousands of immigrants who were eligible to naturalize to actually do so and then register to vote—as Democrats.
During the early 1990s, the federal government began fortifying the U.S.–Mexico border against undocumented immigration with more Border Patrol agents, new technologies to detect unauthorized crossings, and hundreds of miles of fencing. “Yet, the end result wasn’t fewer undocumented immigrants in the United States, but more,” said Ewing, He added:
True, more died while crossing the border in remote locations in an attempt to evade the Border Patrol. But, once they got here, they were more likely to stay. Whereas in the past they might have worked here for a few years and then gone home, perhaps later to return for a few more years of
work, now they stayed permanently because crossing the border was so difficult. And they had their relatives join them in the United States rather than be forever separated from them.
The undocumented population grew from 3.5 million in 1990 to a high of 12.2 million in 2007 before dropping to about 11.3 million in 2016.
In 1996, Republicans in Congress authored the Illegal Immigration Reform and Immigrant Responsibility Act, the Antiterrorism and Effective Death Penalty Act, and the Personal Responsibility and Work Opportunity Reconciliation Act. These bills made sweeping changes to immigration law, making it easier to deport or deny federal welfare benefits even to lawfully present immigrants. “In the end, the goal of the immigration provisions of these laws was to make life as difficult as possible not only for undocumented immigrants but for green card holders as well,” Ewing said.
IMMIGRATION TODAY
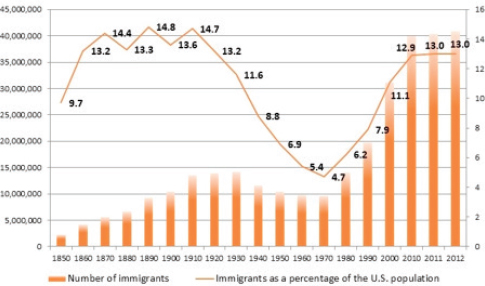
The United States today has a large number of immigrants in terms of absolute numbers, but it has not reached the previous high water marks of immigrants as a percentage of the U.S. population (see Figure 2-1). As of 2016, the United States had about 43.7 million immigrants, representing 13.5 percent of the population. Adding the first and second generation together, about one-quarter of the U.S. population is either an immigrant or a second-generation immigrant.
Before 2009, Latinos made up the largest share of U.S. migration; since then, it has been Asians (see Figure 2-2). In 2015, 36 percent of immigrants entering the country were from Asian countries and 31 percent were from Latino countries, and the number of Asian immigrants is likely to increase, said Ramakrishnan. In addition, the undocumented immigrant population has plateaued for a variety of reasons, including U.S. enforcement policy and demographic changes in Mexico. In recent years, more Mexican nationals have been going back to Mexico rather than arriving in the United States. “If there is a wall, it might keep people from returning to Mexico,” Ramakrishnan pointed out, emphasizing a point made by Ewing. Greater border enforcement after 1996 had the same effect, Ramakrishnan pointed out, in that it “reduced the number of cross-border trips and, in many ways, kept unauthorized immigrants here.”
As pointed out earlier, immigration since the 1965 Immigration Act has caused significant demographic changes in the United States. As one example, the United States does not currently have many second-generation Asian immigrants over the age of 50, because Asians only started immigrating to the United States around 1970. As another example, immigration
SOURCES: Ramakrishnan presentation, November 28, 2017. From NASEM, 2015.
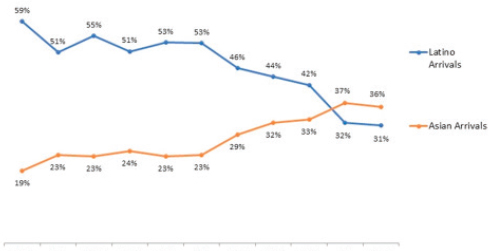
SOURCES: Ramakrishnan presentation, November 28, 2017. From NASEM, 2015.
has brought a significantly higher proportion of Hindus and Muslims to the U.S. population.
HEALTH AND WELL-BEING OF IMMIGRANTS
Legal status shapes many kinds of outcomes for immigrants, Ramakrishnan pointed out. In 2012, naturalized citizens made up 41.8 percent of immigrants, legal permanent residents accounted for 27.4 percent, undocumented immigrants made up 26.3 percent, and temporary and discretionary legal residents made up the remaining 4.5 percent. The number of deportations, which was below 50,000 before 1996, rose to almost 440,000 in 2012, before declining to about 240,000 in 2016 (though this number has been rising again since then), he explained. Immigration detention increased about 40 percent in the first year of the Trump administration, but the removal figures did not increase by similar amounts. “What that has meant is long detentions of immigrants in various facilities, public as well as private, and there are all sorts of public health and family health implications that flow out of that,” Ramakrishnan said.
Undocumented status does not fully impede integration, but it does have intergenerational effects on the children of undocumented immigrants, he noted.1 For example, 5.2 million children in the United States live in mixed-status families, and 4.5 million of these children were born in the United States. They are now living under “a regime of increased deportation, or at least increased fear of deportation,” said Ramakrishnan, and these fears can contribute to negative health outcomes. Children of undocumented parents have lower levels of cognitive development in early and middle childhood, greater mental health issues in adolescence, and lasting negative effects on adult educational attainment and income, he explained.
Naturalization has major consequences for health and access to care. However, the United States lags behind other Organisation for Economic Co-operation and Development countries in the citizenship rates of working-age immigrants who have lived more than 10 years in a country—50 percent versus 61 percent, Ramakrishnan stated. Low levels of naturalization create barriers to political integration as well as other types of social integration. Based on the available survey data, most immigrants want to naturalize but do not do so because it is too complicated or expensive, he said.
In terms of political participation, first-generation immigrants are less likely to vote than are the second or third generations, Ramakrishnan explained. However, lack of experience with the U.S. political system and low
___________________
1 For more information on the integration of immigrants into U.S. society, see NASEM, 2015.
levels of outreach and mobilization by political parties combine to produce lower participation. While many activities do not require citizenship, such as contacting officials, boycotting products, or expressing political views online, he noted that noncitizens are less likely to participate in these activities than citizens. This is true even for volunteers, which “should be a major concern,” Ramakrishnan observed, “to the extent that volunteerism affects community dynamics and the ability of localities to be resilient in the face of budget cuts and economic shocks.”
Ramakrishnan explained that the majority—85 percent—of first-generation immigrants speak another language, but half report speaking English well or very well. Children of immigrants and later generations are acquiring English and losing their ancestors’ language at roughly the same rates as past immigrant waves, with the transition to speaking solely English usually occurring within three generations, he explained. Spanish is the one language that persists into the third generation, but the great majority of that generation is English dominant if not monolingual.
Immigrants have better health outcomes on average than native-born Americans even though they have less access to health care and insurance, Ewing said, adding that they have lower rates of adult and infant mortality and give birth to fewer underweight babies than natives, despite higher poverty rates and greater barriers to health care. They are less likely to die from cardiovascular disease and all cancers combined and have less obesity, depression, and alcohol and drug abuse. Over time these advantages decline and their health status converges with the native born. “Their health status—and that of their children—worsens the longer they live in the United States,” Ewing pointed out, adding “As they adopt an ‘American’ diet high in fats, sugars, and processed foods, they experience sharp increases in obesity, diabetes, and high blood pressure.” A decline in health status also occurs between the first and second generations.
Like their predecessors, modern nativists inaccurately stereotype immigrants as being prone to criminality and resistant to assimilation—both of which are demonstrably false, said Ewing. In addition, nativists have long blamed immigrants for spreading diseases into the United States from elsewhere, such as HIV, H1N1, Ebola, and Zika. “But viruses don’t respect borders or care about nationality,” observed Ewing. “International travelers to a country are just as capable of spreading a disease as the indigenous population. For that reason, border controls are not particularly effective at stemming the spread of epidemics,” he said.
Finally, immigrants are overrepresented both at the bottom and at the top of the education scale. In addition, a racial dynamic is involved; for example, Asian immigrants tend to be overrepresented among those with bachelor’s degrees or higher, and Latino immigrants tend to be overrepresented among those with less than a high school education. However, these
are very broad generalizations, Ramakrishnan observed, and all racial and ethnic groups contain people with a wide range of incomes and education. For example, refugee populations primarily from Southeast Asia, such as the Burmese, Cambodians, Hmong, and Vietnamese, tend to have levels of bachelor’s degree attainment that are lower than those of Latino and African American populations in the United States, he explained.
CONTINUING INTEGRATION OF IMMIGRANTS INTO U.S. SOCIETY
Ramakrishnan was a member of the panel that produced the report The Integration of Immigrants into American Society. That report pointed out that integration occurs across multiple dimensions, including socioeconomic, political, sociocultural, spatial, familial, and health dimensions. In addition, the report observed that immigrant families are making strong intergenerational progress in educational attainment, including among Latino and black immigrants. Poverty rates among Asian Americans are lower than the overall U.S. rates, although Asian American senior poverty is higher than the average senior poverty rate. In addition, as immigrants are making their way to new destinations in states controlled by Republicans, this has led to new anti-immigrant laws.
The aging of the native-born population in the United States is rendering immigration a demographic necessity, Ewing stated. The retirement of the baby boomers will create a demand for new workers to take the place of those who retire from the labor force. The Social Security and Medicare programs also will be called upon to serve a rapidly growing number of older Americans, with immigration a potential way to reduce pressure on these programs.
In addition, demand will grow for both highly skilled and less-skilled health care workers to look after the growing ranks of elderly Americans, Ewing observed. Already, as of 2015, 28 percent of physicians and surgeons were immigrants, as were 24 percent of nursing, psychiatric, and home health aides.
ASIAN AMERICANS AND PACIFIC ISLANDERS
Finally, Ramakrishnan presented some of the data he and his colleagues have been collecting on Asian Americans and Pacific Islanders. Asian Americans have been the fastest growing racial group since 2000, with much of that growth fueled by immigration. In fact, Asian Americans are the only major racial group in the United States of which a majority are immigrants, Ramakrishnan pointed out, despite the misconceptions that most immigrants are Latinos and that Latinos are mostly immigrants. By
about 2050, according to projections from the Pew Research Center, the foreign-born population will include more Asian Americans than Latinos. Already, the share of registered voters who are foreign born is higher for Asian Americans than Latinos in California—44 percent compared with 33 percent—and it is approaching parity (30 versus 33 percent) for the United States as a whole.
The Asian American community is both one group and many groups, said Ramakrishnan. Asian is a single racial category in the United States built over many years of exclusion from citizenship. But the Asian American community also has tremendous diversity in terms of socioeconomic status, language, health, geographic ancestry, political activity, and other measures. As just one indication of this diversity, Ramakrishnan mentioned the political activity of recent Chinese immigrants using WeChat to exchange information, political messages, and rumors.
Another feature of the Asian American population that is often overlooked is the extent of undocumented immigration. Today, about 1.6 million Asian Americans are undocumented, representing about one in seven Asian immigrants. In addition, about as many Asian Americans as Latinos in the United States have limited English proficiency, Ramakrishnan observed. Large Asian groups such as the Chinese, Korean, and Vietnamese have significant language needs.
“Data like these can help make our conversation about immigration more complex,” said Ramakrishnan. He said:
When immigrant equals Latino and Latino equals immigrant, while that may be empowering for certain communities, what we saw in the last election is that there is a lot of harm that can also be done in terms of how these issues get visualized, especially with a majority white population.
Even within the Asian American community, the impression is widespread that Asian Americans are in the United States predominantly on employer-based visas. In fact, most Asian Americans are in the United States based on family sponsorships, and “any attempt to cut back on the family visa provision will affect Asian Americans and, importantly, will increase the undocumented population,” said Ramakrishnan. He further explained:
This notion that people just need to wait in line, well, tell that to the Filipino relative waiting over 20 years to reunite with their family members. Most people won’t wait that long—for good reason—so we need to think about what these policy changes will mean not only for the Asian American community but for American society in general.
STATE-LEVEL POLICIES
A prominent topic in this session of the workshop and in other sessions was the role of state governments in immigration policy. With the federal government deadlocked on immigration reform since 1996, state and local governments have stepped in to fill the void. Some have voted to prevent police from inquiring about someone’s immigration status. Others have joined the federal 287(g) program, which trains local police officers to act as immigration agents. Oakland, California, requires all municipal departments to have bilingual employees on staff. Prince William County, Virginia, denied all county services of any kind to undocumented immigrants, and Hazleton, Pennsylvania, passed an ordinance making it a crime to rent an apartment to an undocumented immigrant. The result has been “a complete mess,” Ewing observed, “a patchwork of conflicting rules and regulations on topics that should have been decided at the federal level.”
As did Ewing, Ramakrishnan pointed to wide variation in the states in enforcing federal immigration laws while also citing differences in areas such as adult education and workforce training, in-state tuition, financial aid, driver’s licenses, professional licenses, and child health insurance. Ramakrishnan and other Californians have been writing and talking about state citizenship, a status that would not “threaten federal citizenship but that works in parallel and in many ways exceeds the standards set at the federal level.” Though more research is needed on the policy effects of state laws, “Funders not just at the state level but at the national level can pay attention to the policy changes that are happening at the local and state level and look at their possible effects,” he said.
Though opinions vary about the advantages and disadvantages of state-level policies on immigration, Ramakrishnan pointed out that experiments at the state level have often been the source of important innovations. Furthermore, the federal government remains so deadlocked on immigration that progress may only be available at the state level. Other states besides California, including Connecticut, Illinois, and New York, have been working on the issue, Ramakrishnan observed. Ewing, however, pointed out that “There are states in which the political reality may never allow enfranchisement of immigration populations.… It presents real operational challenges on the ground.” Ramakrishnan agreed: “There are limits to state citizenship, especially in terms of providing health benefits at the state level—it’s very expensive to do.”
Nevertheless, Ramakrishnan pointed to the advantages of state-level innovations above a floor of federal immigration policies. The analogy would be the minimum wage in which the federal floor does not hold back states like California. “We cannot count on Congress or the presidency
to come through, and we’ve known this now for more than 15 years,” he said, adding that “instead of waiting for funding, let’s get on with it and do the work.” Philanthropies in California have coordinated their efforts to work on specific issues, which has been effective, he said. “Any hope for federal reform will depend on building up the political case for it at the state level,” he concluded.
DATA SECURITY AND THE NEED FOR DISAGGREGATED DATA
Another prominent topic in this and other sessions was whether any data provided to federal agencies by immigrants could be used against them. For example, both Ewing and Ramakrishnan acknowledged that immigrants may be reluctant to provide information to the census. “Census 2020 is going to be the perfect storm,” Ramakrishnan predicted, citing his fear of what an undercount of the immigration population could mean to immigrants. “In many ways the nativists will have won, because representation [and] resources in all those districts will go down dramatically,” he said. Similar issues arise when data are collected from immigrants in community health departments, college financial aid forms, or driver’s license offices.
The 2015 National Academies report recommended continuing the practice of collecting the nativity of not only the respondent but also the father and the mother, as has been done in the past. “When you are trying to understand immigrant integration, we need to look across generations, and you can’t do that if you don’t have the nativity,” he explained. Ramakrishnan also expressed the belief that such data will be held securely, “because otherwise you will never see anyone sign up for something like DACA [Deferred Action for Childhood Arrivals] again.” Ewing, however, expressed his opinion that people in power today “are perfectly capable of misusing this information.”
Ramakrishnan also pointed to the continued need to collect disaggregated data in the census and other surveys. As an example of the need for fine-grained data, Ramakrishnan pointed to the difference between Asian American and Latino populations in accepting DACA:
There is a “coming out” dynamic within Latino communities, where it’s not a stigma but in fact could be empowering for people to speak up and be visible, [whereas the] completely opposite dynamic is happening within the Asian undocumented communities. We wouldn’t know the magnitude of that unless we have the data to show how low the participation of some of these Asian DACA-eligible populations are.
Another example involves rates of uninsured people among Asian Americans, which dropped substantially after enactment of the Patient Protection and Affordable Care Act. However, the numbers differ by ethnic group, again demonstrating “why data disaggregation is so critical,” Ramakrishnan said.














