
6
Accelerating the Rate of Learning Through Population-Based Research Strategies
Hendricks Brown and Uma Kotagal co-moderated a session on accelerating the rate of learning how best to promote health equity through population-based research strategies. The goal of this session was to explore alternative research methodologies to increase participation and engagement, with the aim of narrowing the gap on health disparities. Presentations from Regina James, National Institute on Minority Health and Health Disparities (NIMHD), and Peter Margolis, Cincinnati Children’s Hospital Medical Center, included examples of research methodologies that may be translated to promote behavioral health equity for children and families, as well as methodologies that embed research into practice.
LEVERAGING RESEARCH TO CLOSE THE GAP
Regina James presented on how to leverage research to close the gap in health disparities for children and families. She first focused on research strategies to address health equity, and then moved to methods of accelerating the rate of learning about health disparities.
Four Research Strategies to Address Health Equity
James first summarized four population-based strategies that can be, or are currently being, utilized to address health equity: Community-Based Participatory Research (CBPR), Multi-Level Interventions, Pragmatic Study Design, and Quality Improvement Framework.
CommunityBased Participatory Research
James described several key components of CBPR, beginning with partnership development, intervention development, and dissemination and implementation. NIMHD is currently conducting the Reducing Racial Disparities in Access to Kidney Transplantation (RaDIANT) study with the Southeastern Kidney Transplantation Coalition at Emory University. The study is trying to address the low rates of transplantation in the southeastern United States, as data show that more people stay on dialysis than are able to have transplants. The goal of this study is to reduce disparity in referral for transplant evaluation, with the long-term goal of leading more people to receive organ transplants.
James explained that the RaDIANT study included a number of partners, including transplant patients, staff at dialysis facilities and transplant centers, quality improvement organizations, and patient advocacy organizations. The intervention involved monthly webinars with staff at the dialysis facilities so they can lead discussions on how to address barriers to referrals. Partnerships between transplant and dialysis patients were also made available. The initial results found the facilities that received the intervention increased their referrals by 75 percent, yet the longer-term question has yet to be answered: Does this intervention lead to more people receiving transplants? James suggested that participants consider the value of CBPR in addressing health disparities, specifically related to behavioral health and well-being of children and families, and possibly reproduce and scale effective interventions on a larger platform.
Multilevel Intervention
According to James, the multilevel intervention involves, at a minimum, three levels: patient, provider, and health care system. It is able to target multiple determinants of health simultaneously within complex systems. The intervention provides the potential to reach larger numbers of participants at the population level, rather than at the individual level, leading to broader health impact on disparate populations (see Figure 6-1 for the potential targets of multilevel interventions).
The Transdisciplinary Collaborative Centers for Health Disparities Research on Chronic Disease Prevention is the NIMHD initiative on multilevel interventions. James said the initiative’s goals are to initiate and implement multilevel interventions to promote health equity; build strong collaborations among researchers, providers, communities, and other stakeholders; and develop cross-system solutions to eliminate health disparities and address the social determinants of health.

SOURCE: James (2017).
James discussed two ongoing NIMHD-supported research studies: Native-Controlling Hypertension and Risk through Technology and Flint Center for Health Equity Solutions. The goal of the first study is to improve blood pressure control and associated cardiovascular disease and stroke risk in American Indians, Alaska Natives, Native Hawaiians, and Pacific Islanders at the individual, family, community, provider, and policy levels. The second study aims to improve substance abuse recovery, physical activity, and diet in African Americans in Flint, Michigan, at the individual, family, and community levels.
Pragmatic Study Design
James said the Pragmatic Study Design evaluates the effectiveness of interventions in the health care setting where individuals receive routine medical care. NIMHD does not have a current solicitation in this area, but the National Institute on Diabetes and Digestive and Kidney Diseases does have a current solicitation focused on pragmatic research in health care settings to improve diabetes and obesity prevention care, two areas that significantly impact minority populations.
In addition, James also explained that the Patient-Centered Outcomes Research Institute is supporting the Chicago Trial, a three-arm multicenter randomized trial with African American and Latino children that present to the emergency room (ER) with uncontrolled asthma. There are three levels of intervention: ER education, in which a member of the research team reviews an informational guide on how to better control asthma with children and families; ER education and home visits, in which a community health worker visits the child’s home in addition to the aforementioned ER education; and enhanced regular care, in which children receive usual care along with education about how to use an inhaler. According to James, this is an ongoing pragmatic trial, but it may be useful when thinking about how to design studies to address issues of health equity for children and families.
Quality Improvement Framework
The fourth research strategy James discussed is the Quality Improvement (QI) Framework, which allows for the identification of areas of improvement. Once a strategy is implemented and data are collected, implementers monitor progress and adjust strategies as needed. The QI approach may be used with health disparities research, although it is important to note the benefits and challenges, James stated. A benefit is that this framework offers a platform to address modifiable aspects of health care disparities and gives proactive attention to the social determinants of health. However, according to James, some health care organizations do not routinely collect race and ethnicity data, so they would be unable to address racial and ethnic disparities with this framework. Further challenges with the QI Framework may include the potential to undermine care for the underserved, particularly in the case of incentivizing providers to avoid caring for high-risk children and families.
James also addressed the potential effects of the QI Framework on health disparities. She referred to a study conducted by Lion and Raphael (2015) that showed that QI interventions could potentially reduce disparities, help them remain constant, or increase disparities depending on who the QI intervention benefits.
Two Methods to Accelerate Learning About Health Disparities
Next, James summarized two methods that can be used to accelerate learning about the causes and implications of health disparities: the use of big data in research and rapid health care learning systems.
The Use of Big Data in Research
James explained that the government has adopted the use of big data to accelerate the process of addressing health disparities. The National Institutes of Health has the Big Data to Knowledge initiative (BD2K),1 in which NIMHD participates through training individuals to utilize big data as they conduct their research. She cited work by Zhang, Pérez-Stable, and colleagues (2017), who published Big Data Science: Opportunities and Challenges to Address Minority Health and Health Disparities in the 21st Century. Zhang and colleagues stated that researchers need to incorporate standardized collection of race, ethnicity, socioeconomic status, and other social determinants of health measures in all systems that collect health data. They also recommended enhancing public health surveillance by incorporating geographic variables and social determinants of health for geographically defined populations, and ensuring that active efforts are made to address disparity reduction during both the planning and implementation stages of new big data approaches.
Rapid Health Care Learning Systems
James referenced a 2006 workshop on the learning health care system (Institute of Medicine, 2007). She highlighted the use of electronic health record (EHR) databases in research, especially with the use of technology that allows for larger datasets to address issues around health, health care, and health disparities. At the same time, James said, the move toward using big data and EHRs provides the opportunity to track social determinants of health. EHR databases offer a standardized platform for collecting social determinants of health data in clinical settings to address health disparities, she said. They also allow health care providers to capture and begin to address upstream factors in patient care. James provided the example of the Oregon Community Health Information Networks research team, which has developed a set of EHR-based tools to help community health centers collect and manage patients’ social determinants of health. Domains currently being captured in EHRs that can address the impact of social determinants of health include race and ethnicity, alcohol, tobacco, and residential address. She said eight additional domains should be captured: educational attainment, financial resources strain, stress, depression, physical activity, social isolation, intimate partner violence, and neighborhood median household income.
James concluded by restating the population-based research strategies that can be used to address health equity for children and environments, as
___________________
well as the important role that the social and physical environment in which a child is born, grows, and develops plays in his or her health status, with the family context being a key determinant of health.
ENGAGING CONTRIBUTIONS OF PATIENTS, CLINICIANS, AND RESEARCHERS TO CO-PRODUCE HEALTH
Peter Margolis presented on accelerating learning through systems that engage the contributions of patients, clinicians, and researchers to produce health. Expanding on James’ description, the learning health care system aims to achieve improved outcomes through new knowledge and technologies, big data, and the increasingly dynamic and complex health care environment.
The learning health care system, Margolis stated, is a single system for producing better health. Rather than separating research from clinical care, it uses data generated at the point of care, aggregates data to become knowledge, and rapidly applies new knowledge to clinical care. Information flows through the learning health care system starting with the interaction between patients and clinicians, which may be virtual via telehealth models, and produces data through clinical health care records. Data are entered into databases and registries, and applications are then run to summarize the results and feed reports back into the health care delivery system. This type of quality improvement approach, stated Margolis, helps to standardize care and reduce unwanted variability, and as a result, more is learned about patient outcomes as well as gaps in current performance.
Addressing Challenges
Margolis explored the possibility of creating a chronic care system through collective motivation and intelligence of patients and clinics, through which all stakeholders could collaborate, problem solve, and use collective creativity and expertise in active ways to improve health. He addressed three main challenges: (1) how to develop an organizational structure that could simultaneously apply and learn, (2) how to engender cooperation, and (3) how to communicate.
Margolis stated he turned to networks to overcome the challenge of developing an organizational structure that could apply and learn. Margolis defined a network as an actor-oriented organizational structure with three parts: (1) actors (people, clinics, machines, databases), who engage with a shared purpose and have the capabilities for self-organization; (2) renewable and expandable commons where actors share their resources; and (3) protocols, processes, and infrastructure that enable peer-to-peer collaboration.
Margolis said that in order to build a system in which everyone participated, his team needed to build on a mechanism to engender cooperation. He cited Martin Nowak (2006), professor of biology and mathematics at Harvard University, who developed five rules for engendering cooperation: (1) kin selection (people tend to cooperate with their genetic relatives), (2) direct reciprocity (“if I help you, you help me”), (3) indirect reciprocity (calling attention to the generous and heroic acts of others), (4) network selection (neighbors helping neighbors), and (5) group selection (groups of cooperators outcompete other groups).
Margolis noted that taking advantage of networks requires new ways to lead and practice, which requires communication. Leaders direct and listen to others, yet Margolis highlighted a third and more important way to lead: enabling people to connect and cooperate. This leadership style, he stated, enables and empowers interaction and involves sharing, generosity, trust, connectivity, and cooperation.
Principles and Examples of Learning Health Care System Networks
Margolis and colleagues learned four guiding principles for the design of a learning health care system network: (1) focusing on outcomes; (2) building community; (3) effectively using technology; and (4) producing a learning system that uses a variety of methods across learning, social sciences, clinical research, quality improvement, and system science to produce more rapid learning.
The pilot learning health care system network is ImproveCareNow.2 It began in 2007 when a group of pediatric gastroenterologists came together to improve outcomes for children with inflammatory bowel disease. According to Margolis, the group soon realized the need to involve additional stakeholders, including deep involvement of families and patients. Beginning with 9 care centers and 60 percent of children in remission, the number of care centers grew to 106 with 28,000 patients in 2017, with the rate of remission at 80 percent, thanks to information and knowledge sharing, collaboration, and cooperation.
Margolis shared that the learning health care system has been replicated in other clinical networks, including the Solutions for Patient Safety Network, The Ohio Perinatal Collaborative, and the National Pediatric Quality Improvement Collaborative. A nonclinical example, the All Children Thrive Network, showed improvement in reading scores in schools that participated in the quality improvement network.3
___________________
2 For more information, see http://www.improvecarenow.org.
3 For more information, see http://allchildrenthrive.org.
These networks require technology, an information-sharing exchange, and community building, Margolis explained. The technology will capture data with EHRs to use in both clinical care and research. A team of volunteers developed an information-sharing exchange platform for the ImproveCareNow Network, Margolis said, using a platform similar to Pinterest, in which patients and care centers can upload observations, diagrams, information on particular problems, forms, and other resources and knowledge that can help drive change and improve outcomes.
Margolis noted that the community needs to be engaged and invested early on in the process in order for a network to develop a deep understanding of the lives and goals of those affected by and living with a particular condition. He said health care centers use family-centered design principles to understand the communities with whom they engage: trust, empathy, and empowerment. In addition, Margolis stated that community organizations use public narrative, or storytelling, to engage participants in their network through online videos. Community networks, he said, can enable people to become more engaged and start to contribute. But in all networks, he added, about 1 to 10 percent of people produce most of the content used. Social networks and social network production rely on the fact that this 1 to 10 percent are willing to make a contribution.
As an example, Margolis shared an idea that emerged from a patient, a statistician, a clinical epidemiologist, and a gastroenterologist. The group wondered if tracking tools could be used to help patients document and learn about their disease, thereby customizing their treatment. One example Margolis cited was a 19-year-old with Crohn’s disease who began tracking her sleep patterns and nocturnal stools. Through her efforts, she and her clinician determined which treatment was most effective. One such tracking tool is the Eureka N-of-1 mobile app, which allows patients to set reminders for symptoms they want to track. Patients can document their symptoms and view data on an online dashboard.
Margolis also emphasized that rather than a top-down approach, learning health care system networks use a bottom-up approach through which exponential growth is documented (see Figure 6-2). The model engages people who want to participate because the system is meeting their needs. The challenging part, according to Margolis, is not immediately identifying who will step forward and contribute. “In this model, we are waiting for somebody who is excited or interested to show up . . . the idea is to enable and empower people, and encourage them to attract others,” he said.
In closing, Margolis called for creating a system that facilitates fewer inequities. He stressed the need for transparency, the ability for individuals to control the use of resources, and the power to act. His team is starting to see the network model overcome artificial barriers between clinical care and research by producing a platform through which it is possible to learn
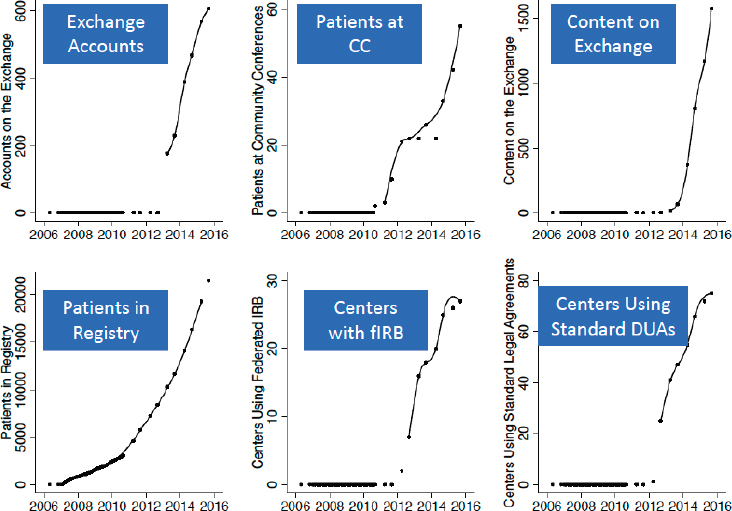
NOTE: IRB = Institutional Review Board, DUAs = Data Use Agreements.
SOURCE: Margolis (2017).
and apply. It also allows for contributions from a large community of people who self-organize around problems they find are important to them and co-produce solutions.
This page intentionally left blank.










