
The opening session of the workshop, moderated by Blumenstock, served as an unclassified briefing on U.S. planning for nuclear incidents. It also provided an overview of the evolution of preparedness for a nuclear event over the past 10–15 years, a period of major change in the field; speakers were asked to consider the implications of these changes in the current nuclear threat environment. This chapter summarizes the four speaker presentations and the discussion that followed.
SETTING THE STAGE: NUCLEAR DETONATION RESPONSE PLANNING
The panel opened with John MacKinney, senior policy adviser, Countering Weapons of Mass Destruction Office, U.S. Department of Homeland Security (DHS), providing a brief history of federal nuclear attack response planning, the changing threat environment, and needs moving forward.
A Brief History of Federal Terrorist Nuclear Attack Response Planning
“The concern that somebody would sneak a nuclear weapon into the United States goes back to post-World War II, 1946,” MacKinney began. After seeing the destruction in Hiroshima and Nagasaki, the federal government was very concerned that someone might be able to sneak a bomb into the United States, either by sea or land, because at the time bombs were small enough to go unnoticed. Even today, while the technology, techniques, and intelligence have improved, there are still significant limitations to actually detecting and discovering a weapon. A famous Senate testimony from Robert Oppenheimer during the post-World War II era raised alarms, and many reports and studies were conducted. But the warnings came and went
until the 1970s, when a host of nuclear hoaxes raised alarms again and led to the establishment of the Nuclear Emergency Support Team (NEST) in the U.S. Department of Energy (DoE), which sent highly specialized teams into the field to look for, discover, and then render safe nuclear weapons. NEST still exists today, updated for the current threat environment.
Not until after 9/11 did the threat of a nuclear incident enter the forefront of national conversation again, when both improvised nuclear device (IND) and radiological dispersal device (RDD) terrorism became critical concerns for the federal government. By 2003, an interagency group had been formed to directly work on response planning for INDs and RDDs. The initial focus was largely on radiological impacts, but in the process of the interagency working group meetings, MacKinney recalled, it was fairly easily determined that a nuclear bomb was much more than a radiological incident—additional consequences would include a massive blast effect in addition to the initial pulse of radiation and fallout and potentially electromagnetic pulse effects. The damage to infrastructure, response organizations, and communications would be extensive, MacKinney said. Because of these other potential impacts and the greater scope of damage, a case was made to the relevant White House policy committee that a special planning effort was needed. The White House agreed unanimously, according to MacKinney.
By 2008, DHS was aggressively pursuing nuclear response planning. This led to the publication of Planning Guidance for a Response to a Nuclear Detonation, with a second edition issued in 2010 (FEMA/DHS, 2010). After release of the guidance, response planning was essentially turned over to the Federal Emergency Management Agency (FEMA). MacKinney described this guidance as “the bible” for how to approach nuclear attack planning.
DHS Roles and Responsibilities
According to MacKinney, Michael Chertoff, secretary of DHS from 2005 to 2009, once said, “The role of DHS is to keep bad people and bad things out of the country.” Most DHS components, including Customs and Border Protection, the Transportation Security Administration, and the U.S. Coast Guard, are involved with the prevention of terrorists and transnational criminals, as well as weapons materials, from entering the country. Several offices, including the Office of Intelligence and Analysis, help determine threats, and Homeland Security Investigations, part of Immigration and Customs Enforcement, conducts counterproliferation investigations to track down people who are trying to export U.S. technologies for the development of nuclear weapons and other weapons of mass destruction (WMDs) capabilities. Finally, MacKinney’s office, Countering Weapons of
Mass Destruction, coordinates counter-WMD planning and provides technical advice and support to operators in the field, MacKinney said. All of this work is conducted in concert with the Federal Bureau of Investigation, the U.S. Department of Defense (DoD), DoE, and others. “We really seem to be a deterrent, in the end analysis,” MacKinney said. “It’s extremely difficult to keep things out of the country, but we want to make sure that the adversary understands that the risk is high to them. So we seek to deter.”
Operating through the National Response Framework (NRF) (DHS, 2013), FEMA has a unique role within DHS—the agency manages post-incident logistics. It leads and coordinates federal support and federal response to the state and local entities that are in charge on the ground and plans for every major kind of disaster, MacKinney said. In 2008, the DHS Office of Strategy, Policy, and Plans established a FEMA program that integrated CBRN (chemical, biological, radiological, and nuclear) into its WMD response capabilities. The NRF annex, Nuclear/Radiological Incident Annex to the Response and Recovery Federal Interagency Operational Plans (DHS, 2016b), describes the capabilities that federal departments bring to bear in a radiological or nuclear incident through task orders or mission assignments by FEMA (this will be addressed further in Chapter 7).
Changing Threats Since Preparedness Planning Was First Done
Threat levels have changed since nuclear preparedness planning first began in earnest around 2005–2006, MacKinney continued. At that time, the primary organizational threat was al-Qaida. Thus, the focus was on al-Qaida and similar organizations with the resources and ability to recruit scientists and technicians and the danger of their potential acquisition of a critical mass of plutonium or enriched uranium to construct a bomb, MacKinney said. If terrorists could construct a bomb, would they achieve nuclear yield, and how much? The nuclear response community zoomed in on a range of 1–10 kilotons (kt) of TNT (trinitrotoluene) and thus began planning for a 10 kt IND (meaning, MacKinney noted, not the same as a state weapon, although an IND could be a state weapon that has been partially dismantled and modified). Subsequently, there were murmurings that 10 kt was too low and that perhaps the response community ought to start considering weapons with 50 kt or greater yields. Nonetheless, even exercises conducted today assume a 10 kt range, MacKinney said.
“North Korea has changed this calculus substantially,” MacKinney said, and has forced the issue around whether the nuclear preparedness community should consider larger bombs. There is no longer any question that they should be, he said. At the time of the workshop, North Korea had completed a total of six tests; one test, conducted in September 2017, achieved a yield estimated (by DoD), using seismic data, to be between 70
and 280 kt. Other estimates were in the 200–250 kt range. The possibility of a 1–10 kt device being snuck into the country and set off in a city without warning is still a threat, MacKinney clarified, but it has been amplified by this new additional threat of weapons with yields in the hundreds of kilotons.
In addition to the greater yield of this new threat, the method of delivery has also changed, MacKinney said. North Korea is primarily focused on missile development technologies, either an intercontinental ballistic missile (ICBM), with about a 20-minute warning time, or a short- or medium-range missile launched from a ship, with about a 5-minute warning time. MacKinney underscored the difference in warning time between a terrorist weapon and a missile launch. In a terror scenario, the experts’ assumption is that the terrorists would notify the media that they were about to explode a bomb but would give no further warning. North Korea, in contrast, would likely offer a warning prior to a missile launch—unless North Korea were to smuggle a weapon into the United States and use it for distortion, in which case it is unknown whether there would be warning, MacKinney said.
Addressing the size of the larger yield weapons, MacKinney said that miniaturizing a bomb and moving it onto the tip of a warhead is quite a challenge, and it is unknown how far the North Koreans have progressed in that direction. Reentry is also a challenge, especially for an ICBM, as the reentry vehicle has to survive very high heat and energy. Targeting is difficult as well. Yet, MacKinney cautioned, it would be naive to dismiss North Korea’s ability to solve such issues. In his opinion, because it has achieved substantial yield, there is a good likelihood that North Korea can also miniaturize and deliver the warhead.
Exploring Nuclear Preparedness Needs Going Forward
MacKinney identified several needs moving forward. The first is to continually refine the question. He emphasized that nuclear threats are constantly changing and that approaches to preparedness should continue to evolve as the threats evolve.
Second, he called for solutions that transcend the threat and serve broader objectives. Evacuation sheltering, improved methods of communication, fixing disrupted communications, medical response, and mutual aid all need to be designed to meet needs during and after any major disaster, not just a nuclear disaster. In fact, this is fundamentally how FEMA operates, MacKinney stated. While obviously there are complications unique to the nuclear arena, response plans cannot be so specific to a nuclear attack that they take away from preparedness for other, higher probability disasters, he said.
Next, he called for resilience: public resilience, technological resilience, rapid medical triage, rapid clearing of debris, rapid restoration of communications and global positioning system technology, and rapid repair of critical infrastructure. All of these, he said, will help the country rebuild after a disaster. But most importantly, in his opinion, is resilience of the American psyche. He stressed the role that government plays, including prior to a disaster, by preparing the population for the reality that major disasters occur. When a disaster does happen, in his opinion, it is critical that the president address it publicly to reassure those affected.
Finally, disaster exercises typically involve only federal resources and state and local planners, not the public. In MacKinney’s opinion, given the importance of resilience and risk communication during a disaster, these exercises should also include the public.
UPDATED MODELING: NUCLEAR BLASTS AND FALLOUT IN AN URBAN ENVIRONMENT
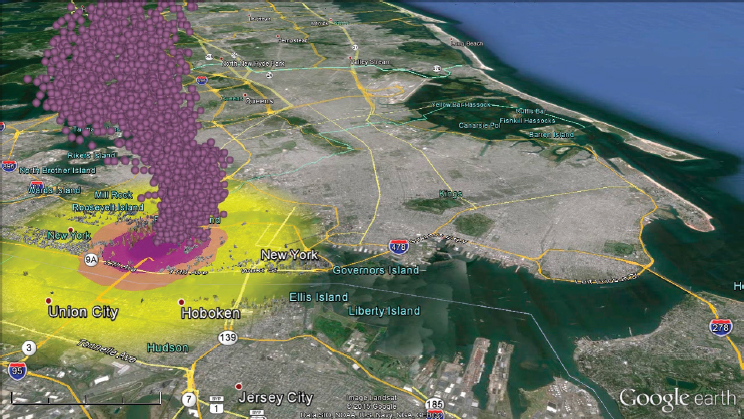
As nuclear preparedness has changed since the early 2000s, so too has the modeling of nuclear blasts. Brooke Buddemeier, principal investigator, Global Security Directorate, Lawrence Livermore National Laboratory, explained how the early models, in 2005–2008, predicted a circular range of blast effects and a cigar-shaped fallout (IOM, 2009) (see Figure 2-1). However, an inherently problematic assumption of these early models was that everyone affected was standing outside in a “desert” (i.e., with no buildings or other forms of cover in the area). Today’s models, in contrast, have more sophisticated capabilities because of the kinds of data that are available on urban environments, including the types of buildings and both daytime and nighttime populations for each city block. Unlike the simplified models of the mid-2000s, current models demonstrate a dynamic fallout pattern that moves in different directions and with significant variation in radiation levels across geography (see Figure 2-2), Buddemeier said.
Moreover, current models are able to account for distinct thermal effects of detonation at different altitudes. When compared to a near-ground detonation, a detonation at a height of 300 meters would result in reduced impact of thermal injuries and other line-of-sight effects due to the protection provided by the urban environment (Marrs et al., 2007). For prompt radiation compared to an open area, detonation in a high-rise area would result in a much curtailed range of effects from injurious levels of radiation exposure.
Buddemeier remarked that this updated modeling has helped to inform not only the federal Planning Guidance for a Response to a Nuclear Detonation (FEMA/DHS, 2010), as mentioned by MacKinney, but also a variety of additional guidance documents that followed (DHS, 2016a,c;
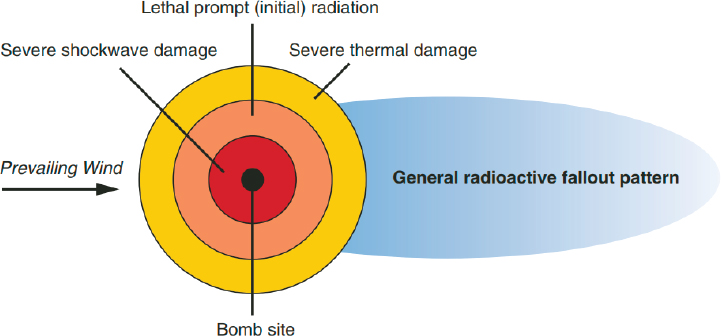
NOTE: An illustration with circular prompt (initial) effects and a cigar-shaped fallout pattern.
SOURCES: Buddemeier presentation, August 22, 2018, and NAE and DHS, 2005.

NOTES: The dynamic fallout pattern of a 10 kt nuclear detonation in Washington, DC, based on a block-by-block assessment of prompt effects, overpressure, thermal effects, prompt radiation, and fallout dose and dose rate. The height of each block represents the radiation levels on that block.
SOURCE: Buddemeier presentation, August 22, 2018.
FEMA, 2013; NCRP, 2011), including Nuclear/Radiological Incident Annex to the Response and Recovery Federal Interagency Operational Plans (DHS, 2016b).
An Example: A 10 kt Detonation in New York City’s Times Square
In order to contextualize the terminology and response zones defined in the guidance documents cited above, Buddemeier described an example of a 10 kt ground detonation in Times Square (New York City [NYC]) to demonstrate how the updated models predict varying effects across five key response zones: three blast zones (severe damage, moderate damage, light damage) and two fallout zones (dangerous fallout zone, hot zone). He described a 10 kt detonation as a bright flash of light that is the equivalent of 1,000 suns seen a mile away. In terms of yield, it is the equivalent of about 5,000 Oklahoma City bombs. This particular example was based on a real weekday population and real weather (from noon on August 14, 2009).
Blast Zones
The severe damage blast zone from a 10 kt detonation would extend approximately 0.5 miles from the blast site, and there would not be many survivors in this area, Buddemeier said. There would be some very severe building damage, and many buildings close to the detonation site would collapse. The moderate damage blast zone would extend from about 0.5 miles to about 1 mile, Buddemeier said. This zone would include significant structural damage, with blown-out building interiors, collapsed buildings, and fires, but survival would be much higher than in the severe damage blast zone. Buddemeier noted that because of the number of people in this zone who would survive but have significant injuries, the moderate damage zone is a priority in many response plans. Finally, the light damage blast zone would extend from approximately 1 mile to 3 miles, Buddemeier explained. Although most people in this zone would not be injured, it is still a zone of concern as there would still be significant damage as well as broken and flying glass. In addition, there would be minor crush injuries from structures collapsing or falling from the shock wave.
Fallout Zones
Buddemeier explained that fallout occurs when the explosive fireball, which is so hot that it actually shoots up like a bubble at more than 100 miles per hour, drawing in thousands of tons of dirt and debris, which then mix with the fission products (i.e., created in the explosion), creates a mushroom cloud. The cloud then rises several miles into the atmosphere,
about 5 miles for a 10 kt bomb, where any winds in the upper atmosphere can move the cloud in different directions. When the particles fall back to earth, Buddemeier said, they emit dangerous radiation that can injure people and contaminate surfaces. Dangerous levels of fallout create visible dust and debris, he noted. In the 10 kt NYC example, during the first 2 hours of the event, the cloud would move to the south, over Queens (see Figure 2-3).
Survivors and Casualties
Before describing the specific results of the model with regard to survivors and casualties, Buddemeier reiterated that the model accounted for all of the buildings in the area. In addition, a starting assumption, which he hoped would not be the case in a real event but one that was useful for the purposes of modeling, was that some people were outside for the entire first 2 hours following detonation while others were indoors.
Most would not survive in the severe damage zone (see the red circle in Figure 2-4). However, in the moderate damage zone (see the orange ring in Figure 2-4), with a total population of 740,000 in the example, most people would survive, but there would be significant injuries—an estimated 250,000 “at-risk” injuries or exposures, which Buddemeier defined as injuries or
NOTES: Activity of the mushroom cloud during the first 2 hours of a modeled 10 kt nuclear detonation in NYC. The purple balls represent the cloud.
SOURCE: Buddemeier presentation, August 22, 2018.
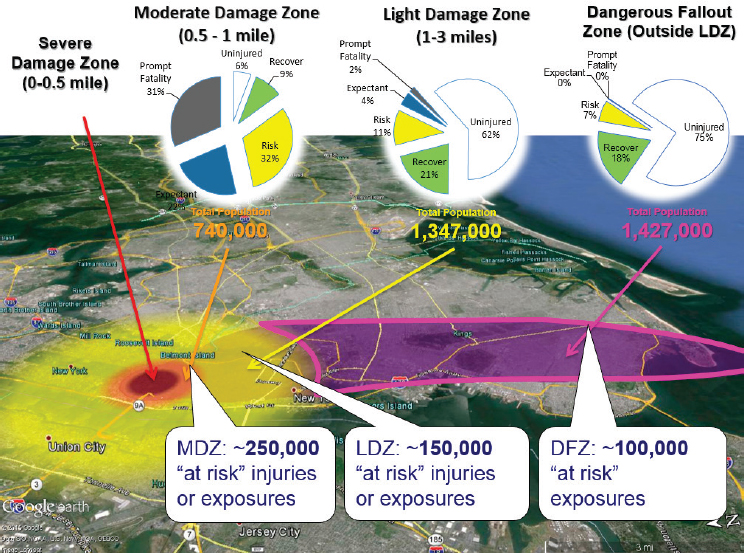
NOTES: Fallout after 2 hours. Colored contours on the ground represent the different blast zones (red, orange, yellow) and the dangerous fallout zone (purple).
SOURCE: Buddemeier presentation, August 22, 2018.
exposures that would benefit from medical care. In the light damage zone (see the yellow ring in Figure 2-4), with a total population of 1,347,000, most people would be uninjured, but there would still be an estimated 150,000 at-risk injuries or exposures. Finally, in the dangerous fallout zone outside of the prompt effect (see the purple section in Figure 2-4), with a total population of 1,427,000, most people would be uninjured, but there would be an estimated 100,000 people with at-risk exposure.
In sum, Buddemeier said there would be approximately 500,000 people in the at-risk category. Four hundred thousand people would also be classified as “low exposure,” meaning that they may have been exposed to enough radiation to become sick but have a good chance at recovery without medical assistance. Buddemeier said that radiation takes time to manifest, with acute radiation syndrome often progressing over weeks, allowing for extended opportunities for medical intervention. He predicted that with medical care, more than 100,000 at-risk fatalities could be avoided.
Buddemeier emphasized the dynamic nature of nuclear incidents. In the NYC example, at 3 hours, then 4 hours, and so on, the cloud continued to move downwind, depositing radioactive material on the ground beneath it. Moreover, radiation levels change with time—they grow, then shrink back as fallout decays, Buddemeier noted. Initially, decay is rapid. In this example, the maximum extent of the dangerous fallout zone is only about the length of Queens (see Figure 2-4), reaching that maximum at about 2.5 hours after detonation. However, the hot zone—the second fallout zone—stretches down most of New Jersey, reaching its maximum extent at about 18 hours before shrinking back (see Figure 2-5).
Of note, the contours determined by this type of model and illustrated here in Figures 2-3, 2-4, and 2-5 are defined as areas where actionable
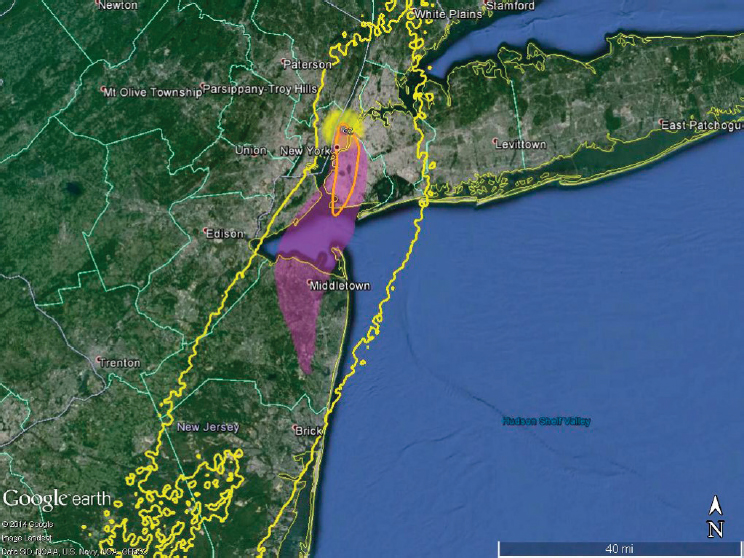
NOTES: Orange contour represents the maximum extent of the dangerous fallout zone 2.5 hours following detonation (this same area is represented by the purple shaded area in Figure 2-4); yellow contour represents maximum extent of the hot zone (18 hours after detonation); and purple shaded area represents the hot zone at 1 week.
SOURCE: Buddemeier presentation, August 22, 2018.
protections are necessary. There would still be detectable contamination outside of the hot zone. In this example, Buddemeier said, the entire eastern seaboard would have low levels of detectable radiation. After an event of this magnitude, there may be no “clean” area.
Key Fallout Considerations: Implications for Sheltering
Not only is fallout decay rapid, Buddemeier noted—with more than half of the energy being released in the first hour and 80 percent in the first day—but it is not a significant inhalation hazard either. The primary hazard from fallout is through exposure to the penetrating gamma radiation from the particles. Moreover, it is readily visible as it falls, as thousands of tons of dirt and debris are lofted into the air. Most importantly, it takes approximately 15 minutes for that fallout to arrive. “So you have time to take action to protect yourself,” Buddemeier said.
“Where you are in a building makes a big difference.” Being in a building away from the roof and ground outside confers better protection. “If you’re in a basement,” he said, “even better.” Even being in a half basement of a single-story wood-frame house can be 10 times more protective than being outside (see Figure 2-6).
Sheltering in Place
Sheltering not only can save many people, Buddemeier stated, but it is also something that does not necessarily need to be done before a detonation. In the Times Square example, assuming that everyone stands outside for 12 hours after detonation—which Buddemeier noted is not recommended but is a helpful baseline assumption for modeling purposes—almost 1.5 million people outside the severe and moderate damage zone would have significant radiation exposure. However, if everyone were to run into even a low-quality shelter, nearly 1 million of those people would be saved from significant exposure. Buddemeier explained that if everyone ran into what is considered adequate shelter, such as a shallow basement in a wood-frame house or a two- or three-story brick structure, more than 1 million individuals would be saved from significant exposure. In cities like NYC or Washington, DC, where brick and cement buildings are ubiquitous, exposures could be reduced to a level at which nobody would be lethally exposed, Buddemeier predicted.
Get Inside, Stay Inside, Stay Tuned
Buddemeier explained that the concept that sheltering even after a detonation could save so many thousands of people from significant ex-
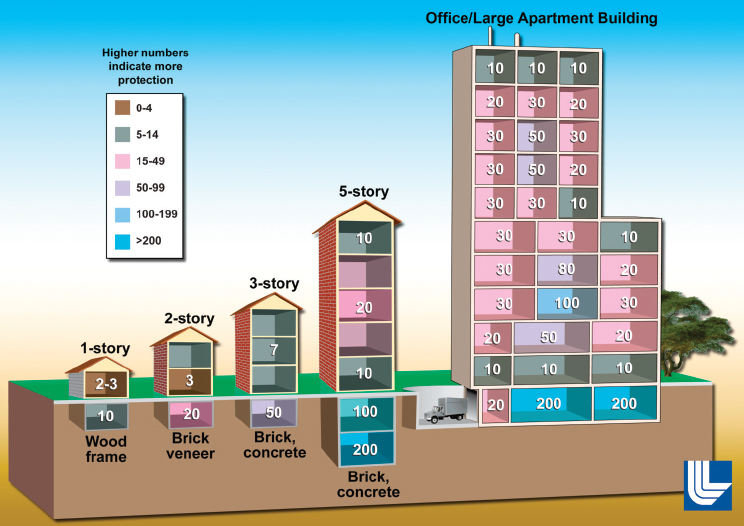
NOTE: Different degrees of protection from fallout while in a building, compared to being outside; the bigger the number, the better the protection.
SOURCES: Buddemeier presentation, August 22, 2018, and Buddemeier and Dillon, 2009.
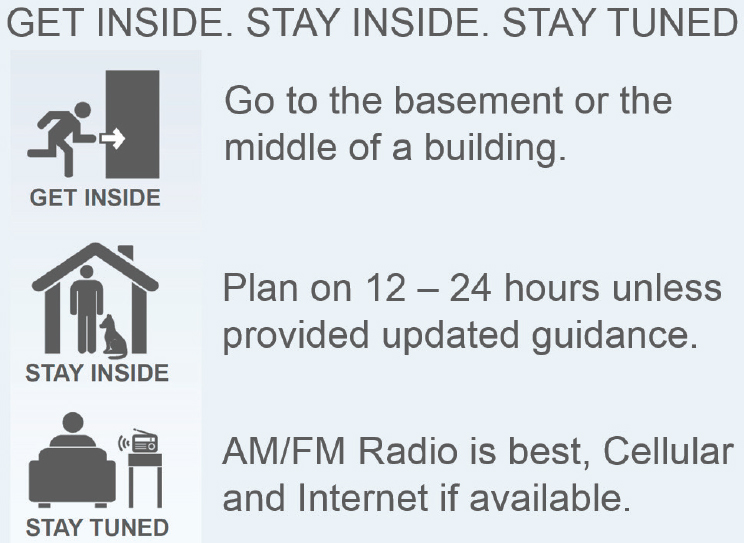
posure helped generate the “Get inside, stay inside, stay tuned” campaign. The campaign advises people to get inside to the basement or middle of a building, plan on remaining there for 12–24 hours to avoid the highest levels of fallout radiation outside, and stay tuned by radio or, if available, cellular internet services (see Figure 2-7).
Higher Yields and Height of Burst
The relationship between yield and blast effect is not linear, Buddemeier pointed out. For a 100 kt yield, for example, the blast effect is only about double what it is for a 10 kt bomb.
Regarding height of burst, Hiroshima and Nagasaki were both detonated at between 1,500 and 2,000 feet off the ground. While both had the expected cap and stem mushroom cloud, both also had an air gap, and it was because of that air gap that there was no significant fallout (see Figure 2-8). Buddemeier explained that the radioactive material produced
SOURCE: Buddemeier presentation, August 22, 2018.
in the explosion was so fine that it actually drifted into the atmosphere. It is only when a fireball falls to earth and the fission products mix with the dirt and debris that the heavier particles that fall back down are created, Buddemeier said. Although there is global fallout when a bomb is detonated that far off the ground, it is not the severe local fallout that causes the kind of issues he described in the NYC Times Square example.
Addressing Today’s Expanded Threat Base
In the event of an imminent nuclear threat, as MacKinney had mentioned, people would likely have 10–20 minutes to find a good shelter, Buddemeier said. He pointed out that the same shelter that protects against fallout can also protect against prompt effects.
In a no-notice detonation, however, “duck and cover” still works as protection against prompt effects, he said. For example, if someone sees a bright flash, because it would take several seconds for the blast wave to reach this person, ducking and covering can protect against the initial
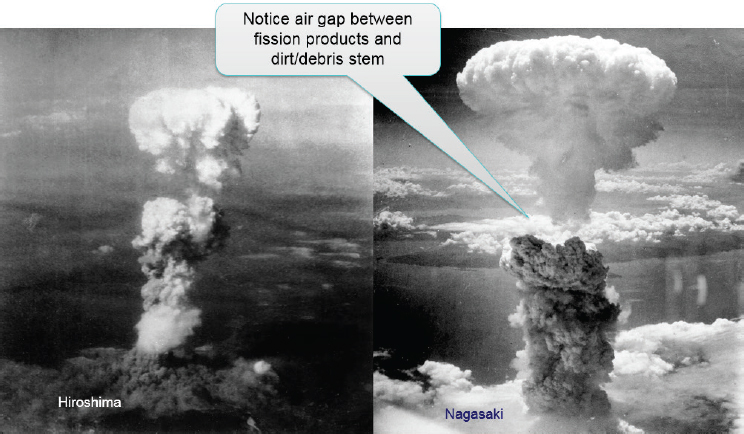
NOTE: The Hiroshima and Nagasaki cap and stem mushroom clouds with air gaps between the fission products (in the cap) and the heavier dirt and debris (in the stem).
SOURCE: Buddemeier presentation, August 22, 2018.
effect. However, to protect against fallout (i.e., if the fireball is close enough to the earth to generate fallout concern), given that it takes 15 minutes or more for fallout to reach the ground, then, following the initial effect, there is some time to find shelter and get into a basement or central room, Buddemeier said.
Regardless of warning time for those sheltering, Buddemeier said there should be a way to communicate with them about time spent sheltering, instructions for next steps, and potential hazards (e.g., fire) after sheltering.
“The bottom line,” Buddemeier said, “is that ‘Get inside, stay inside, stay tuned’ works for both a threat of attack as well as if an attack does occur.”
Saving Lives After a Nuclear Detonation
Buddemeier said that for those who are unable to get into adequate shelters and for people who are injured by the prompt effects, a rapid response could save hundreds of thousands of lives. In closing, he called for more analysis to better understand what the expanded threat means in terms of higher yields and heights of bursts and how to plan a response for those types of situations.
EXPLORING MEDICAL AND PUBLIC HEALTH PREPAREDNESS FOR A NUCLEAR INCIDENT: FROM THE PERSPECTIVE OF THE OFFICE OF THE ASSISTANT SECRETARY FOR PREPAREDNESS AND RESPONSE
Kevin Yeskey, principal deputy assistant secretary for preparedness and response, Office of the Assistant Secretary for Preparedness and Response (ASPR), U.S. Department of Health and Human Services (HHS), described the office’s role in all-hazards preparedness and its work specific to nuclear threats.
ASPR’s All-Hazards Charge
Because of its all-hazards charge, ASPR responds to a range of disasters and public health emergencies, Yeskey said. More specifically, under FEMA’s Emergency Support Function #8, ASPR has 17 responsibilities, including water safety, food safety, environmental health, worker safety, and the provision of medical care. In all of its activities, Yeskey said, ASPR supports preparedness at state, local, territorial, and tribal levels. “The better prepared they are,” he said, “the less we have to do, the less we have to engage, and the more resilient they become by doing that.”
Yeskey recalled that when Robert Kadlec, current assistant secretary for preparedness and response, assumed his position, he spoke of 21st-century threats—such as emerging infectious diseases, nuclear threats, and other CBRN threats—and the need for contemporary solutions to those threats. Yeskey reiterated the all-hazards charge to ASPR and, like MacKinney, cautioned against specifically planning for any one event at the expense of others. As an example, he mentioned the New Madrid earthquake scenario,1 where it has been predicted that a magnitude 7.7 earthquake would impact more than 150 counties across 8 states (Alabama, Arkansas, Illinois, Indiana, Kentucky, Mississippi, Missouri, and Tennessee), displacing 2 million people and causing 86,000 casualties.
Challenges in Nuclear Incident Preparedness and Response
Yeskey listed several preparedness challenges in an all-hazards approach but also noted that the list specifically applied to a nuclear scenario because of the extent of patient movement and the need for specialty care. He predicted that in the event of a nuclear incident, many providers would offer support, but a methodical approach would be critical to a successful
___________________
1 For more information on the scenario, see https://communities.geoplatform.gov/geoconops (accessed December 10, 2018).
medical response. “With competent people providing care—not just anyone who has a license and feels they need to be there,” Yeskey said.
Lack of Medical Capacity
The National Disaster Medical System (NDMS), with its 94 teams, including 57 medical teams and 2 critical care surgical teams, still lacks the capabilities and capacity to respond to all of these new 21st-century scenarios, including a nuclear scenario, Yeskey said. While most teams are very skilled at providing initial stabilization and treatment, given that most team members are emergency or flight nurses, doctors, or paramedics, these scenarios would likely require specialty care in orthopedics, burns, trauma, and pediatrics, as well as rehabilitation when the initial response passed into a recovery phase. Yeskey emphasized the need to engage the private sector to help provide this specialty care. However, engaging hospitals and private health care systems in emergency preparedness is difficult, Yeskey said, because they are often concerned with day-to-day activities.
Jurisdictional Issues
Nuclear incident preparedness and response is also challenged by a range of jurisdictional issues. In the NYC detonation example described by Buddemeier, Yeskey pointed out that there were four states involved in that scenario. Within each of those states, each county and each city has its own procedures, protocols, emergency medical services (EMS) systems, and public health department, all of which operate separately. They may even have distinct communication systems and may not be aware of procedures in neighboring counties. In addition, jurisdictional boundaries may limit licensed professionals from crossing borders to practice their specialties, which is of particular concern in a nuclear scenario given that resources—including members of the workforce—will need to be divided strategically. Finally, jurisdictional issues unique to islands or remote places pose a specific challenge. It is hard to move equipment, people, and supplies to places that are several hundred miles away from the continental United States.
Workforce Training and Situational Awareness
Yeskey commented on CBRN training for medical practitioners: “If you talk to providers about what they are trained in and what they feel comfortable in . . . the general providers in the country don’t know a whole lot about CBRN and the medical management of those cases.” Yeskey also referred to the “fog of war,” meaning that it is very difficult after an event to secure basic information from impacted jurisdictions about the operat-
ing status of their health care system, such as whether their emergency departments or operating rooms are open, whether they are on the power grid or how long their generators will last, and whether patients have been transferred, and if so, where.
Recovery
Yeskey mentioned that recovery after Hurricane Harvey (August 2017) in Texas only finished around June 2018 and that recovery from the 2017 hurricanes in the U.S. Virgin Islands and in Puerto Rico was still ongoing. Those were devastating events that impacted infrastructure, health care, and the migration of people to elsewhere, he said. “We are still recovering, trying to restore those areas to maybe a little bit better than normal—but at least to prehurricane levels,” he added. He compared those recovery efforts to the nuclear scenario and the need to think not just about the immediate response to an event but also about the long-term recovery, including plans for displaced populations.
ASPR Operational Guidance
ASPR has been active in nuclear preparedness and response for more than 10 years and during that time has issued several operational guidance documents to help state, local, tribal, and territorial partners with preparedness planning in their specific jurisdictions, Yeskey said. He highlighted A Decision Makers Guide: Medical Planning and Response for a Nuclear Detonation (HHS/ASPR, 2017) and noted that ASPR has also assisted its federal partners in writing some of their guidance documents, playbooks, and manuals. In addition, ASPR works with subject matter experts, particularly in the health care field, to help identify needs and move forward with respect to these needs. ASPR has also engaged private industry on hospital preparedness for a nuclear event.
Allocation and Use of Scarce Resources: Triage and Trauma
Yeskey cautioned that despite the availability of operational guidance and other documents, an important factor to consider as the field moves forward is the allocation and use of scarce resources. Early on during a nuclear disaster, the need for medical countermeasures and other medical resources will outstrip regional supply. An important piece of addressing this will be figuring out how to triage patients to make sure they receive the care they need and that trauma is addressed.
Adding to the challenge will be combined injuries, Yeskey said, including individuals who suffer from physical injuries and radiation sickness. “It
won’t be conventional triage categories that are used,” he said. In Yeskey’s opinion, there should be further discussion around the allocation of scarce resources and convincing practitioners to incorporate different procedures, policies, and treatment guidelines for successful management of the overall scenario as well as individual patients.
Additional ASPR Responsibilities: Clinical Guidance, Stockpiling Medical Countermeasures, Medical Care, and Interagency Activities
Clinical Guidance
In addition to its operational guidance documents, ASPR has also issued clinical guidance. In Yeskey’s opinion, a valuable reference—and one that has been very well received by the medical community—is the Radiation Emergency Medical Management website, www.remm.nlm.gov. A combined initiative by ASPR, the HHS Office of Planning and Emergency Operations, the National Library of Medicine, and other federal partners, it contains practical knowledge about the management of patients who have been exposed to radiation. Yeskey noted that after the Fukushima incident,2 the website experienced an uptick in traffic, presumably because of efforts to prepare for incoming patients.
Medical Countermeasures in the Strategic National Stockpile
ASPR’s Biomedical Advanced Research and Development Authority (BARDA) is responsible for the procurement and development of medical countermeasures for CBRN threats, and many of them are procured for the Centers for Disease Control and Prevention’s (CDC’s) Strategic National Stockpile (SNS) to be used in specific scenarios, including medical countermeasures for acute radiation syndrome. In collaboration with the American Burn Association, burn experts, and radiation experts, efforts are under way to develop countermeasures for burns as well, Yeskey said (burn countermeasures are not yet in the stockpile). Another late-stage development supported by BARDA is the development of biodosimetry for measuring the level of radiation exposure relatively quickly. Finally, BARDA is also examining innovative treatment pathways based on a better, different understanding of how injuries occur at the cellular level, with the goal being to intervene and stop the cellular cascade. (Yeskey referred
___________________
2 On March 11, 2011, an earthquake caused a nuclear incident at three nuclear reactors at Fukushima Daiichi. For more information on the incident, see http://www.world-nuclear.org/information-library/safety-and-security/safety-of-plants/fukushima-accident.aspx (accessed December 10, 2018).
workshop participants to Steve Adams’s presentation on the second day of the workshop for a more complete discussion of medical countermeasures in the SNS; see Chapter 7.)
Medical Care
ASPR’s NDMS has 6,000 volunteers that it can deploy during a disaster to help with medical care, Yeskey said. In July 2018, a large NDMS training was conducted to bring volunteers up to speed on CBRN issues, including management of the SNS and use of its materiel. Yeskey identified two medical care issues of particular importance for a nuclear incident scenario: displaced people and pediatrics.
Yeskey invited participants to imagine a scenario in which there are 2 million displaced people, 40 percent of whom have at least one chronic medical condition and 50 percent have at least one prescribed medication; these people are located in shelters in areas where pharmacies will be closed. “So how are we going to make sure that those folks who need their daily medications are getting those so they don’t turn into acute medical problems that have to be seen in emergency departments?” Yeskey asked. Compounding the challenge, he said, people would likely arrive at hospitals and clinics to request tests for radiation exposure. He reminded participants what had happened after the 2001 anthrax attacks and mentioned the large number of people who had arrived at emergency departments in Florida to request nasal swab testing for exposure.
Regarding pediatrics, he emphasized that, regardless of the type of care being provided—whether burn care, trauma care, or care for radiation exposure—the necessary equipment and supplies need to be in place to ensure that children are cared for properly.
Interagency Activities
ASPR’s interagency work with CDC and the Food and Drug Administration (FDA) involves issuing emergency use authorizations, managing the stockpile extension programs to extend the life of components in the stockpile, ensuring food safety during a disaster, and examining critical infrastructure that could be damaged after an event like this that could impact not only the rest of the health care system but also the manufacturing process for saline and other medical countermeasures.
Development of a Regional Disaster Health Response System
While still in a pilot phase, Yeskey said, ASPR has been developing a tiered Regional Disaster Health Response System (RDHRS) aimed at
overcoming the challenges he previously described (see Figure 2-9). Yeskey stressed that the focus of this regional system is readiness and that it does not replace normal patient referral patterns or the day-to-day activity of hospitals. Rather, he said, when those patterns and hospitals become overwhelmed or damaged, the regional system will provide an alternate way to ensure that patients receive the care they need when they need it.
With respect to how the regional system will operate, Yeskey explained that the intention is to capitalize on ASPR’s investments in hospital coalitions and build on its Hospital Preparedness Program (HPP). The goal is to establish regional treatment centers (“regional referral centers” in Figure 2-9) across the country that are capable of caring for patients with complicated needs and are also able to enable smaller community hospitals to provide similar care through telemedicine, mobile teams, and trainings so that those smaller hospitals can keep patients alive until they arrive at a regional facility. Thus, there would be a baseline of trauma systems and health care coalitions that feed into regional centers. The system would be similar, he said, to ASPR’s regional treatment network for Ebola.3 In fact, he said, it is an expansion of that network. In addition, there would be medical operations centers (“regional disaster coordinating center” in Figure 2-9) to provide situational awareness, break down jurisdictional regulations and laws that prevent licensed practitioners from crossing state boundaries, and further leverage the Emergency Management Assistance Compact across states.
“The important piece of this,” Yeskey said, “is exercises.” Rather than conventional self-evaluated exercises, ASPR hopes to conduct exercises based on training and readiness standards. At the time of the workshop, the first pilot project was scheduled to begin on October 1, 2018.4 Following the pilot projects, Yeskey said, ASPR hopes to identify best practices and expand to additional states and partners nationwide.
RESOURCES AND CAPABILITIES AVAILABLE AT THE FEDERAL LEVEL
This workshop was not the first time that the National Academies has evaluated medical preparedness to respond to a terrorist nuclear event, John Crapo, deputy program manager, National Nuclear Security Administration, DoE, began. He referred participants to the 2008 National Academies workshop Assessing Medical Preparedness to Respond to a Terrorist Nuclear Event (IOM, 2009). That workshop concluded with a wrap-up by
___________________
3 For more information on this network, see https://www.phe.gov/Preparedness/planning/hpp/reports/Documents/RETN-Ebola-Report-508.pdf (accessed December 10, 2018).
4 Two pilot projects are under currently under way: one at Nebraska Medicine in Omaha and another at Massachusetts General Hospital in Boston.
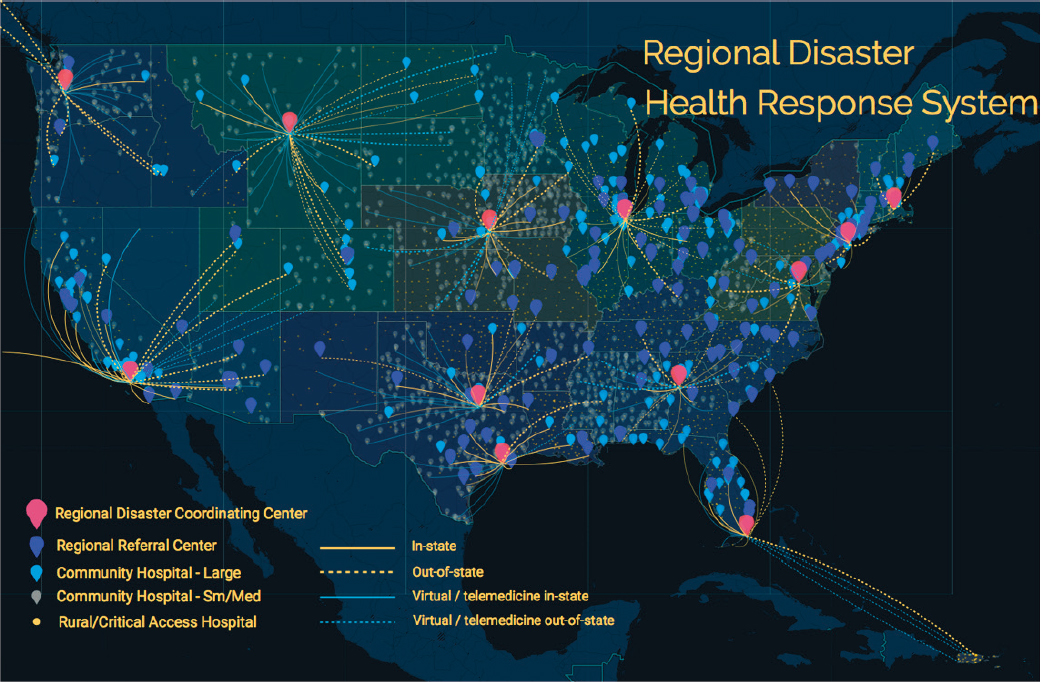
SOURCE: Yeskey presentation, August 22, 2018.
Georges Benjamin, executive director, American Public Health Association, during which he summarized nine main points reflecting the presentations and discussions, and Crapo revisited these in his remarks.
One of the main takeaways from the 2009 workshop was that local areas were only just beginning to consider planning for response to an IND or a radiological exposure detonation within their jurisdictions. There was also a lack of awareness at the local level of what assets might be available at the state and federal levels and how to procure those assets locally. In addition, Crapo said, there was an assumption that it would be weeks to months before federal resources could be fully mobilized to assist states and locals in response to certain events. Finally, there was a lack of clarity around the meaning of medical and public health preparedness for a nuclear incident.
The first “report card” on preparedness planning for a nuclear incident was released by FEMA in a report to Congress in 2010, in which it stated that more than 80 percent of urban areas were prepared to meet the challenges of a large-scale or catastrophic incident, but less than 50 percent had specific IND and RDD response plan annexes to their all-hazards plans (FEMA, 2010).
A second report card came out in 2013 in the form of a Government Accountability Office report on nuclear terrorism response plans (GAO, 2013), Crapo said. Of 27 major urban areas surveyed, 63 percent had RDD-specific response plans either completed or in development, and 60 percent had IND-specific response plans either completed or in development. “So we’re moving in the right direction,” Crapo said, “but we need to continue to move the needle to the right.”
To that end, Crapo continued, the federal government decided to set an example for regional, state, and local entities for planning for nuclear and radiological incidents, beginning with Presidential Policy Directive 8, in 2011, which designated that the federal government would develop integrated national planning frameworks across five mission areas: prevention, protection, mitigation, response, and recovery. Echoing Yeskey, Crapo highlighted that within the response mission area, the defined planning architecture was based on the all-hazards paradigm (see Figure 2-10). Based on a Federal Interagency Operational Plan, each federal region was to develop its own regional operation plan, and states and local jurisdictions would be encouraged to develop their own all-hazards plans with guidance from FEMA, Crapo said. At all levels, nuclear/radiological annexes are encouraged to help plan for that specific threat.
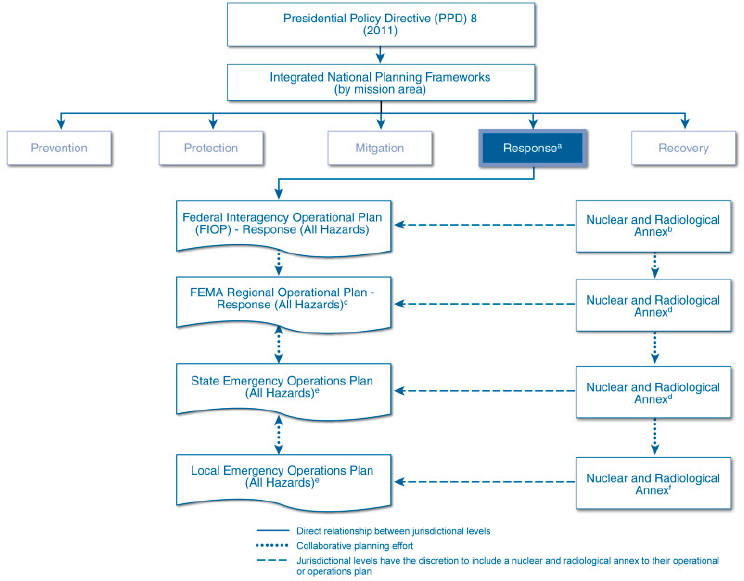
aDHS issued its first National Response Framework in 2008 that included emergency support functions, incident annexes, and the partner guides. A new response framework is under development.
bFEMA is considering the need to revise the existing nuclear and radiological incident annex to the National Response Framework as an annex to a forthcoming FIOPs for the response and recovery mission areas.
cThis plan is based on FEMA’s Regional Planning Guide, which outlines the means to implement the planning process consistent with FEMA’s Comprehensive Preparedness Guide (CPG) 101.
dState governments have the option to develop specific plans that are annexed to their emergency operations plans based on their assessment of the hazard risk, such as a nuclear and radiological annex. As of 2012, all regional offices, states, and Urban Areas Security Initiative locations must use the Threat and Hazard Identification and Risk Assessment process.
eThis plan is based on FEMA’s Comprehensive Preparedness Guide (CPG) 101.
fLocal governments have the option to develop specific plans that are annexed to their emergency operations plans based on their assessment of the hazard risk, such as a nuclear and radiological annex. Local governments often use the Hazard Identification and Vulnerability Assessment process to develop their Hazard Mitigation Plans.
SOURCES: Crapo presentation, August 22, 2018, and GAO, 2013.
The Nuclear/Radiological Incident Annex
Adding to MacKinney’s description of the Nuclear/Radiological Incident Annex to the Response and Recovery Federal Interagency Operational Plans (DHS, 2016b) earlier in the session, Crapo said that the annex is the document that guides federal response and planning efforts involving nuclear/radiological incidents. It identifies overarching coordinating responsibilities of the Federal Radiological Preparedness Coordinating Committee, which provides direction for some 20 federal agencies, departments, and offices responsible for ensuring efforts of the federal government in preparing and planning for response, and of the Radiological Emergency Preparedness Program, which is specific to nuclear power plant response.
Essentially, Crapo said, the annex lays out a concept of operations for a response to a nuclear or radiological incident by identifying the primary authorities (e.g., if an incident occurs at a DoD facility, then DoD is in charge); reinforcing the need to coordinate all planning efforts with regional, state, and local jurisdictions to ensure a coordinated and collaborative response; identifying additional federal agency capabilities to respond; and defining support and coordination elements. Crapo went on to discuss two of these components in more detail: federal agency capabilities and the support and coordination elements.
Key Federal Agency Capabilities
Department of Energy
Crapo said that within the federal response mission space, DoE has bifurcated its capabilities into two areas: (1) crisis response and (2) consequence management. As part of crisis response, DoE is responsible for searching for materials that may be used for nefarious purposes. To do this, it relies on its capabilities to conduct surveillance, identify materials outside of regulatory control, and train regional partners to stabilize devices containing materials outside of regulatory control until a Render Safe team can respond. With respect to DoE’s consequence management capabilities, personnel are trained and equipped to provide timely, actionable, and scientifically defensible decision support to local decision makers for the protection of public responders and the environment. As part of its consequence management capabilities, DoE maintains monitoring and assessment, medical support, and modeling.
Consequence Management
In the area of modeling, Crapo explained that DoE’s National Atmospheric Release Advisory Center (NARAC) at the Lawrence Livermore National Laboratory has a sophisticated 3-D modeling capability that can predict atmospheric dispersion of a release of radiological material from an explosive device. NARAC is connected to multiple meteorological centers and has atmospheric and assessment scientists who can produce a model of situational awareness based on the meteorological data. This is an important capability, Crapo said, because the fidelity of early information can be very sparse. However, they can provide an initial footprint to help inform planning efforts and protective action recommendations. Then, as additional information comes in, the models can be refined to reflect the “ground truth.”
Although initial measurements are conducted at the state and local levels, they can be supplemented by DoE’s regional Radiological Assistance Program (RAP), Crapo noted. DoE maintains nine RAP regions, each prepared to send teams to conduct monitoring activities in the event of a release of radiological material into the environment from any source but particularly an RDD or IND explosion. Each region is tethered to a national laboratory, with a core element of full-time staff that support the program.
In addition to RAP, DoE also maintains an Aerial Monitoring System (AMS) for rapid characterization of the magnitude and extent of a release from either a facility or an RDD or IND, Crapo noted. It does this through the use of radiation detection equipment and scientists on board both fixed and rotary wing aircraft. “Flying low and slow is the way to do that,” Crapo said. Optimally, a helicopter would fly with the radiation detection equipment outside the aircraft to provide the level of fidelity needed to make critical protective action decisions. Unfortunately, he said, fixed wing aircrafts are better suited for the initial response, and therefore initial answers will be “coarse.” Further details are pursued later through rotor wing capability. AMS capabilities come from the Nellis Air Force Base Remote Sensing Laboratory (RSL) in North Las Vegas and the Andrews Air Force Base RSL outside of Washington, DC.
Also responding out of RSL Nellis is a Consequence Management Response Team (CMRT) to conduct an initial assessment. With its monitoring/sampling and geographic information system (GIS) capabilities, it produces situational awareness, supports planning efforts, and informs protective action decisions. It also comes with a fairly light laboratory analysis capability, Crapo noted.
“Once we have done our sampling, once we have done our analysis,” Crapo said, “it is important that we translate that scientific information into actionable and comprehensive information for key leaders and decision
makers.” That is the role of DoE’s Consequence Management Home Team. It is empaneled mostly out of RSL Andrews, although it reaches out to other national laboratories, including Sandia National Laboratories, Los Alamos National Laboratory, and Lawrence Livermore National Laboratory.
DoE also provides for medical management. Crapo’s office sponsors the Radiation Emergency Assistance Center/Training Site (REAC/TS), a center of excellence for treatment of radiation injury located in Oakridge, Tennessee. The center provides advice and assistance in the management of radiation injury for victims of INDs or RDDs, either through virtual and in-person consultation or by deploying a team to a site. REAC/TS also maintains a Cytogenetic Biodosimetry Laboratory, where a dicentric chromosome assay is used to conduct retrospective dose assessments from blood samples. The assay results are provided to health care providers to drive treatment decisions. In addition, REAC/TS has a robust training capability to help the medical community become better prepared to respond to a mass casualty situation involving radiation exposure, Crapo said.
Other Federal Agencies Involved in the Response
In addition to DoE’s capabilities, DoD offers a range of CBRN response capabilities as well, Crapo said. These include 22-person civil support teams that can respond immediately to an incident, much like DoE’s RAP teams, and larger teams (1,500 people) of trained, organized, and equipped personnel that can be deployed within a certain period of time to assist with emergency medicine, decontamination, and other issues. “Lots of folks, lots of equipment, lots of help,” Crapo commented.
Elsewhere in the federal government, the U.S. Department of Veteran Affairs (VA) maintains a Medical Emergency Radiological Response Team (MERRT), under Executive Order 12657 (1988), to assemble and deploy a health care professional team to the scene of an incident, where it can provide medical advice and assistance in treatment of radiation injury. Ultimately, Crapo said, VA would like to have 33 full teams, with each team having at least one physicist and one physician. Currently, MERRT has 17 health physicists, 8 physicians, and 3 emergency managers.
Crapo noted that these efforts and agencies were only a small sampling of capabilities available at the federal level and that other speakers would be discussing other capabilities, including within HHS, DHA and its component agencies, and the U.S. armed forces.
Support and Coordination of Federal Response
As defined in the Nuclear/Radiological Incident Annex to the Response and Recovery Federal Interagency Operational Plans (DHS, 2016b), the sup-
port and coordinating elements of the federal response include the Federal Radiological Monitoring and Assessment Center (FRMAC). Crapo said that at the scene of a radiological or nuclear incident, all federal radiological monitoring and assessment activities are coordinated by FRMAC (i.e., after the initial CMRT assessment). Another key support and coordinating element is the Interagency Modeling and Atmospheric Assessment Center, maintained by FEMA, which serves as a single point for the federal government for the coordination and dissemination of products related to the modeling of hazardous atmospheric releases. Yet another key coordinating element is the Advisory Team for Environment, Food and Health (A-Team). A collaboration among the Environmental Protection Agency, U.S. Department of Agriculture, FDA, and CDC, A-Team provides advice and assistance on decision making for protective actions for the public and responders. It responds both virtually and on the scene. Finally, Crapo mentioned the Nuclear/Radiological Incident Task Force, which was discussed further by Luis Garcia (see Chapter 7 for more information).
Asset Response Time Line
Figure 2-11 provides a snapshot of what to expect from the various federal agencies in support of state and local jurisdictions in response to a nuclear or radiological incident. Within the first few hours, state and local responders will be on the scene, as well as RAP and a Command Support Team. As time progresses, more and more people will show up. In Crapo’s opinion, while the response may reach a robust capability within 48 hours, 72 hours is probably more realistic.
DISCUSSION
Speakers from the panel on federal roles and responsibilities participated in an open discussion with the audience, summarized below.
The Range of Potential Attacks: How Is the Federal Government Planning for Different Scenarios?
A participant who identified himself as a retired naval intelligence officer and a research ethicist commented on the mentality, or intention, of a perpetrator and remarked that there are many types of potential nuclear incidents that do not involve a bomb in a major city. He asked to what extent military intelligence is helping to define in an expansive way the nature of potential nuclear threats so that the agencies developing response plans can at least become aware of the broader range of actors and modalities that might be used in an attack.
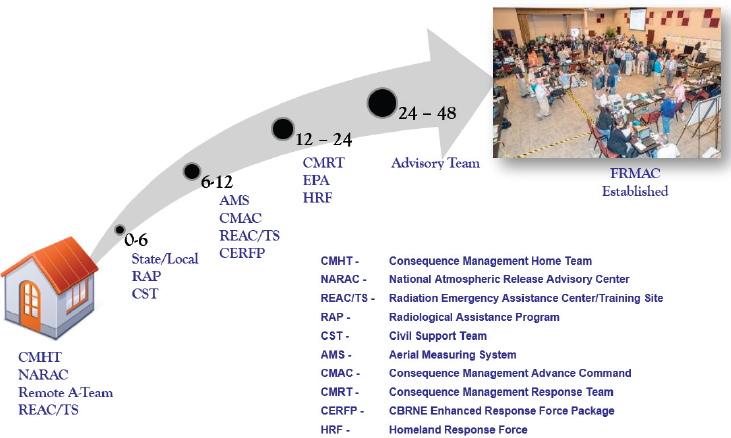
SOURCE: Crapo presentation, August 22, 2018.
Disclaiming that he does not work for DoD or represent the intelligence community and is unable to divulge sensitive information, MacKinney responded that every potential threat is evaluated on an ongoing basis. In the past, the primary nuclear threat was terrorism. With respect to nuclear and radiological terrorism, the focus has been on RDDs and INDs. Although a nuclear bomb is extremely difficult for terrorists to achieve, nevertheless that possibility is monitored closely. The emerging threat from North Korea is one that MacKinney described as being in a “fuzzy zone” between terrorism and war. It would be an act of war if North Korea were to attack the United States, but the attack would be treated like a terrorist attack in terms of an internal U.S. government response. According to MacKinney, the same plans that were developed for a response to al-Qaida are being used when considering a North Korean attack.
ASPR’s Regional Disaster Health Response System
Jody Wireman, environmental health adviser, Defense Health Agency, asked for additional information on the rollout of RDHRS. Yeskey clarified that ASPR is not building more facilities. “We’re not here to build brick-and-mortar hospitals, burn centers, or anything like that,” he said. Rather, ASPR hopes to use existing infrastructure to better facilitate the delivery of care to patients who need it and to access the capabilities of
existing facilities in a way that is meaningful. He mentioned that HPP evolved from a program that initially provided money to hospitals for purchasing and stockpiling items into a system that builds competencies. The regional system is currently at a point in its evolution where it is forming coalitions among EMS, public health, and hospitals (at least two hospitals per coalition) that work cooperatively, not competitively, to ensure that a region has the capabilities to take care of patients and provide care. Thus, not necessarily every hospital will maintain all capabilities, but the broader coalition will. In addition, Yeskey said, ASPR is investigating options to build state-to-state agreements so that resources can be exchanged without federal involvement, which is only time consuming and often ineffective for small-scale events.
Risk Communication: Accessing Initial Models
Ed McDonough, public information officer, Maryland Emergency Management Agency, asked Crapo what the time line would be for accessing the first DoE models that become available following a nuclear incident and whether state and local health agencies know how to access the models. Crapo replied that initial models should be available within 15–30 minutes of notification but would only be as mature as the information that was provided as part of the modeling request, although they would also take into consideration available meteorological conditions to indicate how particles would disperse in the atmosphere. Crapo said states should know how to access the models either directly through NARAC or through FEMA’s FRMAC.
Electromagnetic Pulse Effect
David Winks, managing director, AcquSight, commented that in both air burst and surface burst scenarios, there is also an electromagnetic pulse (EMP) effect that could impact generator controls, medical equipment in the facilities, and the ability of vehicles to respond in the area. He asked Buddemeier if it would be possible to model EMP effects that might be outside the initial blast zone. Buddemeier agreed that EMP is a significant concern, particularly for high-yield, high-altitude detonations, during which there is a “lensing effect” through the atmosphere. For that type of situation, Buddemeier said that EMP effects need more evaluation. In contrast, with near ground-level detonations, although there is some EMP effect, it is much more constrained to the blast damage zones. While some local disruptions would be expected, transmission towers from AM/FM radio towers, for example, would still be working and could still reach into the areas of concern.






























