
CURRENT WORKFORCE DATA
In order to move ahead with new care and delivery models, said Erin Fraher, associate professor in the department of family medicine at the University of North Carolina at Chapel Hill, it is critical to begin with a data-based understanding of the current state of the health workforce. Some of this data was presented by Fraher, who focused her presentation on four needs-based arguments:
- New care delivery and payment models require a broader definition of who is in the health workforce.
- Health care services and the health workforce are shifting into ambulatory and home settings; therefore, training needs to reflect this shift.
- Efforts to reform training need to focus not just on the workforce pipeline but also on retooling the existing workforce.
- Higher quality data are needed to measure shifts in employment, training, and clinical placements.
Current Health Care Workforce
Fraher began with an overview of the people who make up the health workforce. She noted that, while the workforce is often thought of in terms of “traditional” professions such as physicians and nurses, there are a wide variety and a huge number of other professions within health care. Professionals such as nursing assistants, social workers, and mental health workers are growing in number and are “increasingly at the forefront” of health care, said Fraher. Tables 2-1 to 2-3 provide a snapshot of the range and distribution of the health care workforce in 2017.
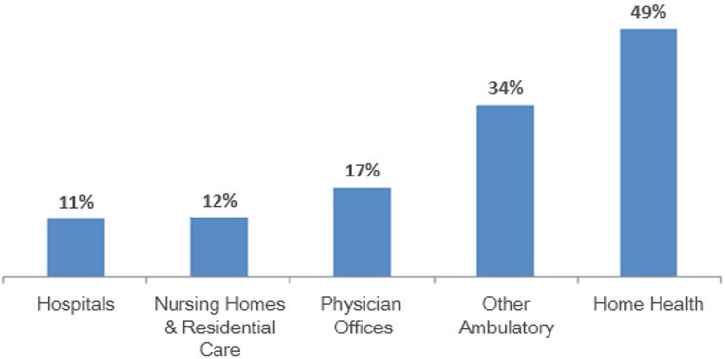
Shift Away from Hospitals
Most of the people working in health care, said Fraher, are not employed in hospitals. Among professionals classified as health practitioners and technical/support staff, 39 percent work in hospitals. Yet, 42 percent work in ambulatory settings, 15 percent in nursing and residential care facilities, and 5 percent in social assistance settings (note in Fraher, 2018: Sums to 101 percent due to rounding). Job growth is also heavily weighted toward non-hospital settings (see Figure 2-1). In 2018 alone, said Fraher, the ambulatory sector added 21,100 jobs—representing more than 60 percent of all new health care hires—compared with 8,200 new hospital hires.
Several changes in the health care system are contributing to the move away from hospital employment, added Fraher, including an increasing
TABLE 2-1 Health Care’s “Traditional” Jobs in a Sampling from 2017
| Who is in the health workforce? The usual professions you think of… | |||
| Sample Health Care Jobs in the United States, 2017 | |||
| Physicians and Surgeons | 877,616 | Pharmacists | 309,330 |
| Nurse Practitioners | 234,000a | Optometrists | 37,240 |
| Physician Assistants | 122,555 | Chiropractors | 33,630 |
| Registered Nurses | 2,906,840 | Occupational Therapists | 126,050 |
| Licensed Practical and Licensed Vocational Nurses | 702,700 | Physical Therapists | 225,420 |
| Dentists | 198,517 | Speech Therapists | 142,360 |
| Dental Hygienists | 211,600 | Respiratory Therapists | 128,250 |
| Total (sample professions): | 6,256,108 | ||
aThis number has been revised since prepublication release.
SOURCE: Presented by Fraher, November 13, 2018.
TABLE 2-2 Support Occupations in a Sampling from 2017
| Who work with many others | |||
| Sample Support Occupations in the United States, 2017 | |||
| Nursing Assistants | 1,453,670 | Psychiatric Technicians and Aides | 65,770 |
| Home Health Aides | 820,960 | Phlebotomists | 122,550 |
| Medical Assistants | 646,320 | Surgical Technologists | 100,270 |
| Pharmacy Technicians and Aides | 453,680 | Opticians Dispensing | 75,450 |
| Dental Assistants | 337,160 | Ophthalmic Medical Technicians | 48,060 |
| Therapy Assistants and Aides | 194,850 | Orderlies | 52,630 |
| Health Information Technicians | 204,220 | EMTs | 251,860 |
| Total (sample professions): | 4,827,450a | ||
aThis number has been revised since prepublication release.
NOTE: EMT = emergency medical technician.
SOURCE: Presented by Fraher, November 13, 2018.
TABLE 2-3 Mental Health and Social Service Workforce in a Sampling from 2017
| And increasingly with mental health and social service workers | |||
| Sample Mental Health and Social Service Occupations in the United States, 2017 | |||
| Health Care Social Workers | 167,730 | Substance Abuse, Behavioral Health and Mental Health Counselors | 241,930 |
| Mental Health and SUD Social Workers | 112,040 | Community Health Workers | 54,760 |
| Social and Human Service Assistants | 384,080 | Marriage and Family Therapists | 42,880 |
| Rehabilitation Counselors | 103,840 | Clinical, Counseling, and School Psychologists | 108,060a |
| Total (sample professions): | 1,215,320 | ||
aThis number has been revised since prepublication release.
NOTE: SUD = substance use disorder.
SOURCE: Presented by Fraher, November 13, 2018.
SOURCES: Presented by Fraher, November 13, 2018. Authors’ analysis of Bureau of Labor Statistics Current Employment Statistics data. Ani Turner, Charles Roehrig, Katherine Hempstead, What’s Behind 2.5 Million New Health Jobs?, Health Affairs Blog, March 17, 2017, https://www.healthaffairs.org/do/10.1377/hblog20170317.059235/full (accessed July 26, 2019). Copyright © 2017 Health Affairs by Project HOPE–The People-to-People Health Foundation, Inc.; Turner et al., 2017.
focus on social determinants of health, new fee-for-service models, and payers referring more patients for home health services. However, this shift away from hospital employment is not reflected in the training of health professionals. Most health professionals are still trained in acute care settings, said Fraher, and there is “an unwritten supposition” that health professionals need to start in inpatient settings to gain the necessary skills (Bodenheimer and Mason, 2016). This idea is now being questioned and there have been calls in fields such as nursing and pharmacy, Fraher said, to expand workforce training into the variety of settings in which professionals will actually work. For example, the American Society of Health-System Pharmacists Research and Education Foundation released a report in 2015 that predicted a major shift from inpatient to outpatient care and included a call for pharmacy staff development programs to “ensure that there are adequate opportunities for education and training in management of ambulatory care pharmacy practice, transitions of care, and medication management of chronic illnesses” (Beans, 2016). Inge Corless, the forum representative from the American Academy of Nursing, remarked that significant challenges exist to finding appropriate placements and supervisors for training nurses outside of the acute care setting. Fraher agreed and said that in addition to the challenges in finding settings and supervisors, there are stringent regulatory requirements about who can oversee nursing education, which could complicate efforts to have nurses trained in community-based settings. Fraher added that such challenges are not unique to nursing, and that as patient support moves away from acute care, every health profession will have to grapple with how to train workers in home and community-based settings.
These data (shown in Figure 2-1) along with shifts in care, said Fraher, require a broader definition of the health care workforce. Workforce planning efforts need to engage workers, in home- and community-based settings, including such health care professionals as patient navigators, community health workers, paramedics, and dietitians. Workforce training needs to acknowledge and support integrated care delivery models that utilize health professionals in new ways and require interprofessional collaboration, added Fraher. For example, social workers—who were traditionally not included in health workforce data—can serve as behavioral health specialists, can manage and coordinate care among health care teams, and can refer patients to community resources (Fraser et al., 2018).
Perhaps most importantly, remarked Fraher, is the broadening definition of the health care workforce that includes the patient, family, and community as essential parts of the team. Health care team models that engage the patient, Fraher said, can promote shared decision making; encourage providers to do more asking, listening, and educating; emphasize a focus
on health literacy, coaching, and goal setting; and honor and validate the work of caregivers and families.
Fraher shared an example of a patient-centered, interprofessional model of community-based health care: Community Aging in Place—Advancing Better Living for Elders (Johns Hopkins School of Nursing, 2019). This program allows a senior to age in his or her own home with the help of a team that includes an occupational therapist, a registered nurse, and a handyman. The team works together to make home modifications and provide assistive devices that help the patient navigate his or her home more safely. Participation in the program, which is currently active in 12 cities, has been shown to alleviate symptoms of depression and improve the individual’s ability to perform activities of daily living. This program, said Fraher, is a great example of how non-traditional health care workers—such as handymen—can serve as essential members of a patient’s interprofessional care team.
Retooling the Current Workforce
Discussions about training for the future of health care largely focus on redesigning the curricula used to prepare students to enter the work environment. However, said Fraher, new entrants comprise a very small percentage of the overall workforce (see Table 2-4). The health care system will not be transformed by new entrants, she said, but by the workforce that is already employed in the system: To facilitate such a transformation, training would need to be “embedded in collaborative practice environments that benefit patients, learners, and the health care system.” Fraher commented that one of the biggest challenges in retooling the current workforce is that “time spent training is not time spent billing.” Health systems are reluctant to take providers away from patient care for training, no matter how valuable it may be in the long run. Another challenge, she said, is that providers do not have the curricula or systems in place to educate the existing workforce. One way to address this, she suggested, might be to develop modular courses around specific topics, such as care coordination or patient engagement.
Fraher said that the focus is often on the “shiny new graduates” but that, in order to make real change, the existing workforce must be addressed. Joanne Spetz at the University of California, San Francisco, added that another strategy is to help create motivation for the existing workforce to retool. Spetz told participants about a Health Resources and Services Administration–funded project in Los Angeles County and its focus on a “mission of transformation” in order to motivate the workforce to redevelop their skills. The project brought nurses together to talk about professionalism and the nursing role, and to train in specific skills. It also brought
TABLE 2-4 Number of Health Professionals in the Workforce Versus New Entrants to the Workforce as Identified Within Select Professions for the Year 2012
| Profession | Total Workforce | New Entrants | New Entrants as a Percentage of Total Workforce |
| Physicians | 835,723 | 21,294a | 2.5% |
| Physician Assistants | 106,419 | 6,207 | 5.8% |
| Registered Nurses | 2,682,262 | 146,572 | 5.5% |
| Licensed Practical Nurses and Licensed Vocational Nurses | 630,395 | 60,519 | 9.6% |
| Dentists | 157,395 | 5,084 | 3.2% |
| Chiropractors | 54,444 | 2,496 | 4.6% |
| Optometrists | 33,202 | 1,404 | 4.2% |
| Social Workers | 724,618 | 41,769 | 5.8% |
| Physical Therapists | 198,400 | 10,102 | 5.1% |
| Occupational Therapists | 90,483 | 6,227 | 6.9% |
aThe number of physician graduates includes those completing medical and osteopathic schools in the United States; it does not include graduates of foreign medical schools who enter the pipeline at the graduate medical education level, also known as residency training.
SOURCE: Presented by Fraher, November 13, 2018.
in students from a local university. The engagement and interaction between nurses and students energized everyone to get involved in creating a better system. Fraher said that, ultimately, retooling will only be successful if the existing workforce becomes comfortable with taking on new roles and letting go of their traditional tasks; in her view, this can be one of the harder barriers to overcome. Reamer Bushardt, a pharmacist, physician assistant, and senior associate dean at The George Washington University, added that transforming the system will require “humility by all involved” and resisting the tendency to protect one’s own profession.
Better Data
Finally, said Fraher, better data are needed to monitor workforce trends in employment and education. The data that are currently available are not always an accurate reflection of reality. For example, if a nurse works in an ambulatory practice that is owned by a hospital, the data may inaccurately count the nurse as a hospital employee. Another data gap, said Fraher, is
in capturing the health care workers—such as social workers—who act as bridges between ambulatory and inpatient care. In order to fully understand the current workforce and the trends occurring in health care, concluded Fraher, it is critical that the data collected are accurate and complete.
THE FUTURE WORKFORCE
The U.S. population, like that of the rest of the world, is aging, said Joanne Spetz, an economist at the University of California, San Francisco. Projections show disproportionate growth in the number of people older than 65: that growth is particularly pronounced among those older than 85 (see Figure 2-2). These are the ages, said Spetz, at which there are increasingly complex, serious diseases and both cognitive and functional losses taking place. Alzheimer’s disease is a particular concern in this age group. Projections suggest that the number of older people with Alzheimer’s will increase from 4.7 million in 2010 to more than 13 million by 2050 (see Figure 2-3).
Spetz asked the pressing question: Who is going to take care of this aging population and their complex health issues? A 2008 Institute of Medicine report projected that there will be a need for 3.5 million additional
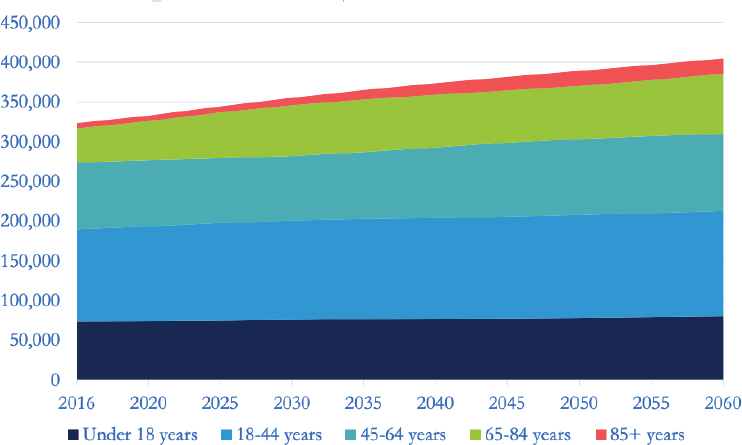
SOURCES: Presented by Spetz, November 13, 2018. Projected Age Groups and Sex Composition of the Population: Main Projections Series for the United States, 2017–2060. U.S. Census Bureau, Population Division: Washington, DC.
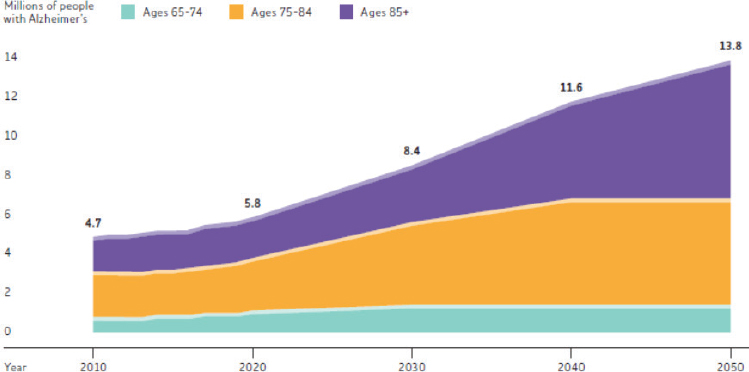
SOURCES: Presented by Spetz, November 13, 2018; Alzheimer’s Association, 2018; U.S. Census Bureau, 2017.
health care workers in order to meet the continued needs of the population by 2030. This type of long-term care (LTC) primarily takes place in home- and community-based settings, said Spetz, with only 25 percent of LTC occurring in institutions such as nursing homes and assisted living facilities. Because of the variety of settings for LTC, that workforce is also varied: Institutions are primarily staffed by certified nursing assistants and licensed practical nurses who are supervised by registered nurses (RNs), while patients in home- and community-based settings are cared for by a combination of people: family members, friends, clergy, community members, direct-care workers, nurses, therapists, counselors, pharmacists, and physicians (see Figure 2-4).
Spetz remarked that, while the health care workforce is often thought of in terms of physicians, physicians actually make up only a small percentage of the caregivers in LTC. However, physicians do play an important role in providing and coordinating related forms of care. The number of physicians specializing in areas relevant to this population is low. Spetz further noted that many training program slots in geriatrics go unfilled. Of those which are filled, she said, up to 80 percent are supported by international students—an indicator that the United States is not producing a sufficient supply of geriatricians to fill the nation’s requirements. Retention is also an issue. With half of all U.S. geriatricians failing to recertify, there is now a projected shortfall of 13,000 geriatricians by 2030 (Kottek et al., 2017). A similar shortfall is projected within palliative care. Despite the obvious overlap between these two specialties, there are few opportunities for dual
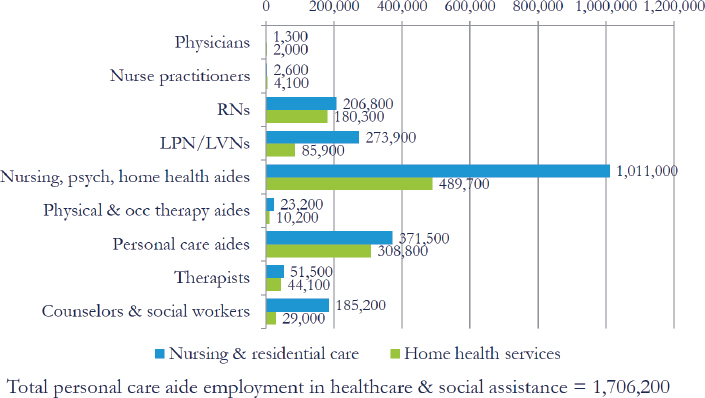
NOTE: LPN/LVN = licensed practical nurse/licensed vocational nurse; occ = occupational; psych = psychiatric; RN = registered nurse.
SOURCE: Presented by Spetz, November 13, 2018.
specialization or cooperation between fields, Spetz pointed out. Pamela Jeffries, dean of nursing at The George Washington University, commented on the accreditation system for palliative care nursing, which she said recently changed. Nurses can now sit for certification without having special academic training in the area and this has reduced the number of people enrolled in associated specialty programs.
Spetz said the majority of the LTC workforce is made up of nurses, home health aides, and personal care aides (privately employed workers who assist with daily care activities). Nurse practitioners employed in nursing and residential care facilities are a rapidly growing part of the LTC labor market, she added, particularly in comparison with physicians and physician assistants. Home health and personal care aides also make up a large percentage of the LTC workforce, although the job titles, education, and requirements for these workers vary widely. In California, home health aides are employed by home health agencies, certified by the Department of Public Health, and must have 120 hours of education and training. Unregistered home care aides, in contrast, are employed directly by consumers. They are not required to be certified or registered or to undertake any education or training. There are a number of other categories of home workers, said Joanne Spetz at the University of California, San Francisco, each with their own training and certification requirements (or lack thereof),
including affiliated or independent registered home care aides and in-home support services providers.
Spetz underscored the importance of adequate training. If these workers even receive training, she said, it is almost never in collaboration with other members of the health care team, such as nurses or physicians. Unfortunately, this means that various workers who are taking care of patients have not learned to work together or to communicate effectively. Spetz noted that team communication is particularly important if the patient has dementia or Alzheimer’s. Susan Scrimshaw, the recent past president of The Sage Colleges and former co-chair of the forum, observed that home health care workers are doing a “tremendous amount of very valuable work.” Proper training, she said, would enable them to identify risks and to reach out to the rest of the team when a patient needs additional attention. Spetz responded by saying that Washington State has been working to develop a training and professionalization program for home workers, one that creates a career ladder along which additional specialization and knowledge may lead to better pay. Spetz further remarked that Washington expects the program to lead to “lower emergency department visits, fewer hospitalizations, and fewer institutionalizations.” There are some other “glimmers of hope” in interprofessional training for home and community-based care, she said: a Centers for Medicare & Medicaid Services (CMS) (2019) test project called Independence at Home Demonstration trains and analyzes outcomes of home care–based teams led by physicians and nurse practitioners; Veterans Health Administration programs train patient-aligned care teams; and other small pilot projects that train home care aides to be collaborative care team members.
PROVIDER PERSPECTIVE ON TRAINING
Chris MacDonell, a managing director at the Commission on Accreditation of Rehabilitation Facilities (CARF) International, said that its accreditation system works with providers of rehabilitation services in 27 different countries. MacDonell sent a survey to 1,000 CARF-affiliated providers in the United States to learn more about workforce development and management. The 78 survey responses were compiled and presented at the workshop. Results showed that 72 percent of providers offered clinical internships and 53 percent offered pre-clinical experiences. Those experiences included both inpatient and outpatient rehabilitation, which is in contrast to other professions, wherein more student opportunities are in the outpatient arena. MacDonell captured the general opinion of the respondents who work with students, quoting one of them as saying: “Working with students is an excellent way to keep our employees current [and] develop their mentoring/leadership skills. [It] has been one of the
most successful recruitment strategies for new grads. Definitely worth the time invested!”
In the survey, MacDonell asked providers about challenges they faced working with students in rehab settings. The main challenge—cited by more than 25 percent of survey respondents—was a lack of available staff to precept students. Other challenges included interference with productivity requirements, insufficient communication with the university or college, and students being inadequately prepared for work in clinical settings. MacDonell noted that concerns with productivity expectations and staff shortages were also commonly reported, as was the view that “seeing patients” ultimately takes priority over training students.
The survey included questions about what educators should consider when developing or revising their student experiences. According to MacDonell, providers gave a lot of feedback in this area, which included the following considerations:
- Students should have realistic expectations about working in the real world. For example, a student in a placement may only have 20 minutes to do an assessment rather than several hours.
- Students should understand the restrictions and requirements of billing guidelines, particularly Medicare rules.
- Education systems should consider the financial burden on the clinic sites. One respondent expressed a fear that “placing the burden on the clinic sites will substantially impact the number of clinical sites in the future.”
- Students are often unprepared for the demands of the work environment: the productivity expectations, the ability to streamline priorities, the ability to interact with relevant populations, etc. MacDonell noted that a particular concern was with the students’ ability to understand the diversity and cultural issues of populations served.
- Preceptors need to understand the students’ base of knowledge.
- Educational institutions should invite providers to lecture on the realities of health care, including current and projected trends, and how these realities should impact the expectations of new graduates. MacDonell said that, as accreditors, CARF believes that redesigning education and training will require a focus on input from all key parties, feedback, and communication.
- Clinical supervisors could benefit from guidance about how to be good supervisors (e.g., how to provide constructive feedback).
- Students who score well in academics do not always do well in clinical settings; they tend to lack the necessary communication and social skills. MacDonell said that, as the health care system
-
moves toward person-centered care, students need the skills to understand the patient’s perspective and to communicate effectively with families.
- Educational institutions and clinical sites must improve their two-way communication.
In closing, MacDonell cited an often quoted maxim that says, “If you want to travel fast, you travel alone. If you want to go far, travel with others.” The others in this case, said MacDonell, are the clinical placements. If educational institutions want to give students meaningful clinical learning opportunities, they need to engage with the clinical settings and listen to both their concerns and their perspectives.
DISCUSSION
The presentations by Fraher, Spetz, and MacDonell triggered numerous ideas, thoughts, and concerns in the minds of the workshop attendees that were shared during the large group discussions. The comments touched on three critical areas for the health professions that included the cost of education and training; the role of technology; and the ties that are or could more closely unite educators across the education to practice continuum.
Cost of Education and Training
Spetz talked about the potential for “huge cost savings” from programs like Independence at Home that use a home care–based team approach. She also brought up work being done in Washington State, mentioned previously in this chapter, that creates a career ladder for personal care aides through a joint arrangement between the workers union and the state government. Those in state government believe there will be a cost savings in the end by ensuring adequate training and a better wage so nursing aides can earn more money while attaining additional specialization and knowledge. The government also expects lower utilization rates of expensive urgent care facilities. This example triggered a response from Pamela Jeffries who commented that hospitals are now starting to charge education programs to precept their students. Programs that receive support from CMS can better manage the added expense, she said, but this is not the situation in nursing. In those cases, the additional costs are shifted to the student.
Guardia Banister, executive director of the Institute for Patient Care at Massachusetts General Hospital (MGH), and her partner Mary Knab at the MGH Institute of Health Professions, spoke about their shared resource model that is detailed in Chapter 4. “The hospital provides instructors,
the institute funds CFC [clinical faculty coordinator] time, and we come together and find multiple ways in which we can figure out together what’s going to work with our shared resources in a way that’s cost-effective and works for all stakeholders involved,” Knab remarked. Charnetia Young from CVS Health also talked about cost but from an industry training perspective. “We want costs reduced, quality increased, and access expanded,” while acknowledging that “ultimately, businesses have to be profitable, just like hospital systems.”
It was Barbara Barney-Knox and Jane Robinson, both with California Correctional Health Care Services, who brought up the conversation about a return on investment (ROI) for their nurse training program housed at a correctional facility. “We want to develop our RN workforce from our existing employees and we want to reduce turnover rate, vacancy rate, reduce the recruiting costs and really become an employer of choice,” they said. Fraher offered numerous suggestions on how they might quantify the cost to benefit ratio. In support of Fraher’s ideas, Barney-Knox reported that turnover rates can cost upward of $58,000. This could be used as part of the ROI argument for continuing the program, Fraher suggested, along with documentation of a happier and more committed prison workforce, and statistics showing a diminished need for emergency care and fewer hospitalizations.
The Role of Technology
Several participants discussed the role of technology in training students and retraining the existing workforce. Fraher said that one issue that needs to be considered is the degree to which technology will “substitute versus supplement versus enhance.” For example, technology could substitute for a provider with a service such as in-home blood pressure monitoring. It could supplement communication between the home and the provider, and it could enhance by providing more detailed or new types of information. Spetz added that tech developers often do not think about the health workforce, and sometimes not even about the end user (e.g., the patient or community). She said there is a lack of consideration about who is going to use the technology, how will it affect practice, and how it will affect the education that is needed. She joked that some developers have “never talked to an old person but think it’s going to be so cool to put monitors on all of them.” Fraher added that while the perspective of the health care provider is important, technology should be patient-centered and developed in a way that meets the patients’ needs, rather than trying to retrofit the existing workforce with new technologies.
Strengthening Ties Across the Education to Practice Continuum
During the question and answer period, several workshop participants commented on the importance of engagement and communication with the faculty who act as preceptors for students in clinical placements. MacDonell said that faculty should be invited into the classroom regularly to discuss the realities of health care. Lemmietta McNeilly, chief staff officer representing the American Speech-Language-Hearing Association, added that, while academic institutions and communities vary across the country, there should be a minimum number of times students actually observe or hear from real-life health professionals who are currently practicing. Frank Ascione, director of the Center for Interprofessional Education and Professor of Pharmacy at the University of Michigan, described the “very successful” model of partnership his college had with preceptors.
The first element of the model includes site preceptors as part of the school’s clinical faculty, which means they receive continuous professional development and that the expectations and responsibilities of all parties are clear. Second, the preceptors are “guaranteed” that students will be on their “best behavior,” Ascione said, with efforts made to align the expectations of students and preceptors. Finally, the model seeks to demonstrate the value students add to the clinical setting. For example, he said, students were involved in published medication reconciliation projects—cataloging a patient’s full list of medications—which were a clear demonstration of how sites can benefit from student involvement. MacDonell responded by saying the CARF survey showed that many providers do not see the value in having students in clinical placements and instead view students as a further demand on their already limited time and resources. She said that if the model and results Ascione described were replicated in other sites, this could help providers and organizations see the value in serving as clinical placements.
Susan Skochelak of the American Medical Association concurred with MacDonell that students and faculty need to better understand the realities of the health care system. While the educational system is “great” at teaching basic and clinical science, said Skochelak, it is missing health system sciences. For example, students need to learn about social determinants of health, working in teams, the structure of the health care system, patient safety, and value-based care. MacDonell agreed, saying that if students lack a “reality-based course” about what a clinical setting will be like, “it really creates havoc within the clinical setting.”
Bushardt shared his experience as a department chair and clinical operations executive at an academic health center. The health center used a system to identify how many months it took for a new recruit to be fully prepared for practice. He said that students from schools where educators
were the “most engaged and curious about the transition of new graduates into practice” and who had spent time in the health system to try to understand provider and administrator concerns were better prepared to enter practice than their colleagues who had not gone to such schools. Skochelak shared a model where students learn about the system not from provider preceptors but from patient navigators who truly understand “what is working and isn’t working for a patient and their family.” McNeilly further commented on the challenges in teaching students about the reality of today’s health care system while also keeping faculty at educational institutions up to date on current health, educational, and community systems. She asked, “How do we enhance the knowledge and skills of the faculty who have not actively engaged in clinical practice for several years?”
Pamela Jeffries, dean of nursing at The George Washington University, listed several concerns with shifting training from acute care to other settings. First, in her experience, she said, it is not feasible or sustainable to train one or two students in a community setting given the financial and time burdens placed on the site and the supervisor. Second, nursing education is largely geared toward preparing students for the National Council Licensure Examination (NCLEX), a standardized exam nurses must pass in order to practice. NCLEX is weighted toward acute care nursing, so even nurses who plan to work in community settings must learn acute care in order to pass. Launette Woolforde, who represents the National League for Nursing, agreed with Jeffries saying that, if there is to be a shift in the testing standards to more closely meet the realities of the workplace, educational institutions need to work with licensing agencies. In addition, said Woolforde, there is resistance from traditional practice leaders who believe nurses must be trained in acute care before working in other settings. This resistance would have to be addressed for there to be change, she said. Mary Dickow with the Organization for Associate Degree Nursing added to the discussion. She cited a pilot project in California that is trying to shift the clinical rotation experiences for students away from acute care settings. The project is based on a program at Thomas Jefferson University in which clinical placements are completely community-based and 98.5 percent of students pass the NCLEX. McNeilly shared another challenge that exists within community-based training, which is finding competent clinical educators who are willing to supervise students in placements; this is particularly challenging in fields such as speech-language pathology. For example, she said, the current requirement that only speech-language pathologists can supervise graduate students in speech-language pathology limits the ability to train students in a variety of settings with varied patient populations.
Malcolm Cox, formerly with the U.S. Department of Veterans Affairs, asked the presenters what it would take to move beyond the accretion of
data toward making real changes. He noted that, while related data are more powerful now than 30 years ago, the issues and the trends have not changed significantly. Spetz responded to Cox by describing a challenge posed by the current financial incentive structure. These incentives are aimed at training in acute care, she said, so a change in training toward greater community-based settings would require a shift in dollars: Some community settings may view training students as a financial burden for which they need to be compensated, and universities may not have the money to do so. Cox acknowledged that financial incentives are a significant problem and noted that policy changes will be necessary to make a difference. Fraher stated that data alone are insufficient for change; however, data can be used to “challenge the prevailing narrative” and to frame issues in a way that encourages policy discussions. Fraher called herself a “data agitator” and said that producing data is incredibly important, but that using data to “make people uncomfortable” is how changes get made.
Anthony Breitbach, representing the Association of Schools of Allied Health Professions, built on Fraher’s remarks by saying that transforming the health care system must be an iterative process: It starts with students and existing workers getting engaged and agitated enough to want to create a more dynamic health care system that, in turn, will attract “even better and brighter students.” He argued, “We lose good [students] because they see the same old thing. If they see [a] bigger and wider [line of] thinking that’s really addressing societal needs, I think students who initially wouldn’t even go into health care” would be attracted to join the health workforce. These energized students would energize the care providers, he said, which would then help transform the system.
REFERENCES
Alzheimer’s Association. 2018. 2018 Alzheimer’s disease facts and figures. Alzheimer’s & Dementia 14(3):367–429.
Beans, B. E. 2016. Experts foresee a major shift from inpatient to ambulatory care. P&T: A Peer-Reviewed Journal for Managed Care and Formulary Management Decision Makers 41(4):231–237.
Bodenheimer, T., and D. Mason. 2016. Registered nurses: Partners in transforming primary care. Paper read at Registered Nurses: Partners in Transforming Primary Care conference in Atlanta, GA.
CMS (Centers for Medicare & Medicaid Services). 2019. Independence at home demonstration. https://innovation.cms.gov/initiatives/independence-at-home (accessed February 21, 2019).
Fraher, E. 2018. The health workforce in the US: Trends and challenges facing efforts to strengthen links between education and practice. PowerPoint presented at the Global Forum on Innovation in Health Professional Education’s Joint Workshop on Strengthening the Connection Between Health Professions Education and Practice, Washington, DC.
Fraser, M. W., B. M. Lombardi, S. Wu, L. de Saxe Zerden, E. L. Richman, and E. P. Fraher. 2018. Integrated primary care and social work: A systematic review. Journal of Social Work and Research 9(2):175–215.
IOM (Institute of Medicine). 2008. Retooling for an aging America: Building the health care workforce. Washington, DC: The National Academies Press.
Johns Hopkins School of Nursing. 2019. Community aging in place—advancing better living for elders (CAPABLE). https://nursing.jhu.edu/faculty_research/research/projects/capable/index.html (accessed March 14, 2019).
Kottek, A., T. Bates, and J. Spetz. 2017. The roles and value of geriatricians in healthcare teams: A landscape analysis. San Francisco, CA: University of California, San Francisco, Health Workforce Research Center on Long-Term Care.
Turner, A., C. Roehrig, and K. Hempstead. 2017. What’s behind 2.5 million new health jobs? In Health Affairs Blog: Health Affairs. https://www.healthaffairs.org/do/10.1377/hblog20170317.059235/full (accessed March 18, 2019).
U.S. Census Bureau. 2017. Projected age and sex composition of the population: Main projections series for the United States 2017–2060. Washington, DC: U.S. Census Bureau, Population Division.


















