
The workshop’s second session examined why the concepts and principles of health equities and inequities are important to society as a whole. Four speakers discussed the contextual perspectives of history, culture, law, immigration status, and socioeconomic status. The session was co-moderated by Vanessa Northington Gamble, university professor of medical humanities and professor of health policy and American studies at The George Washington University, and Shavon Arline-Bradley, founding principal of R.E.A.C.H. Beyond Solutions, LLC, and co-founder of the Health Equity Cypher Group.
CIVIL RIGHTS LAWS AND POLICIES
Angela McGowan, project director in the Office of Disease Prevention and Health Promotion, Office of the Assistant Secretary of Health, U.S. Department of Health and Human Services (HHS), offered a legal perspective on the role of civil rights laws and policies in improving health equity. She began with an overview of Healthy People, the nation’s HHS-led prevention agenda for improving health and achieving health equity by identifying science-based, measurable objectives with targets to be achieved by the end of the decade. Healthy People is in its fourth decade, she noted, and its success requires tracking of data-driven outcomes every decade to monitor progress and guide action.
McGowan shared the Healthy People vision: “a society in which all people live long, healthy lives.” She explained that its mission includes
increasing public awareness and understanding of the determinants of health, disease, and disability, as well as opportunities for progress, and engaging multiple sectors to strengthen policies and improve practices. One of Healthy People’s overarching goals, she continued, is to achieve health equity, eliminate disparities, and improve the health of all groups, and one of the frameworks used to pursue that goal is based on the social determinants of health (CDC, 2019a; ODPHP, 2019). She cited this framework’s five domains: economic stability, education, health and health care, neighborhood and built environment, and social and community context.
McGowan next addressed the role of law in achieving health equity and addressing legal barriers. Law can be helpful as a lever to protect and promote health, she observed, by creating standards and enforcement mechanisms that can influence individual behavior and societal norms and by authorizing governments to act on community needs. She stressed the critical importance of implementation, enforcement, and evaluation once a law has been enacted, to monitor its impact and any unintended consequences. McGowan reminded the workshop participants that there are different types of laws at the federal, state, local, and tribal levels—constitutions, statutes, ordinances, regulations, and case law, for example—that are important to health equity. She highlighted that because tribes are recognized as nations, tribal laws include treaties, and the U.S. Constitution gives the federal government the authority to regulate commerce with Indian tribes. Therefore, she said, tribes are part of the United States but have a separate, parallel court system.
McGowan next shared highlights from the Healthy People 2030 advisory committee’s issue brief about law and legal policy as critical determinants of health (Wright, 2019). First, she said, law and policy, such as bans on tobacco smoking or seatbelt laws, are helpful as direct responses to health-harming social conditions and deficiencies. Second, laws can help perpetuate social conditions that can be harmful to physical, social, or emotional health and well-being, which McGowan stressed is to be avoided. Third, selective application of laws can be driven by biases that affect distributions of health and well-being. Fourth, McGowan reiterated that laws are hollow in the absence of implementing regulations, funding, and effective enforcement. Lastly, she observed that laws and policies can affect health and well-being based on the ways in which they are interpreted by the courts.
McGowan then quoted the definition of civil rights in Black’s Law Dictionary: They “belong to every citizen of the state or country or, in a wider sense, to all of its inhabitants, and are not connected with the organization or administration of government. They include the rights of property, marriage, protection by laws, freedom of contract, trial by jury, etc.” (Garner and Black, 2004). McGowan explained that although the Declaration of
Independence proclaimed as a core American value life, liberty, and the pursuit of happiness for all, various groups have been challenged to ensure that these principles apply to all people and to protect individuals from discrimination based on race, gender, age, nationality, and disability.
McGowan next turned to a series of civil rights laws. She began by noting that the first civil rights laws emerged after the Civil War, mentioning the 13th, 14th, 15th, and 19th Amendments; the Civil Rights Act of 1866; and the Indian Citizenship Act as laws that expanded the definition of who held certain civil rights. She also cited two Supreme Court cases important to desegregation: Brown v. Board of Education and Simkins v. Moses H. Cone Memorial Hospital. The 1960s brought many civil rights laws, she continued, pointing to the Civil Rights Act; Social Security Act amendments; and the Voting Rights Act, which she said was notable for addressing literacy and limited English proficiency as barriers to access to the right to vote. She explained that opportunities for addressing equal employment opportunities and education followed, such as the Title IX amendment that prohibited discrimination in education due to sex. McGowan also mentioned two laws prohibiting discrimination against people with disabilities—Section 504 of the Rehabilitation Act and the Americans with Disabilities Act—calling the latter a seminal law as it required reasonable accommodations for employees and accessibility of public accommodations. Finally, she touched on the Patient Protection and Affordable Care Act of 2010 and its increased health care coverage options, as well as Obergefell v. Hodges (2015), which held that the fundamental right to marry applied to same-sex couples.
Turning back to Healthy People’s social determinants of health framework, McGowan referenced Kumanyika’s presentation (see Chapter 2) as she explained that each of the framework’s five domains reflects several underlying factors, all of which have relevance to law and policy. She delved into two of the framework’s domains—health and health care, and education—by elaborating on examples of relevant civil rights laws and protections.
Civil rights laws have been integral to improving access to health care services and facilities, McGowan explained, such as through desegregation of these facilities and prohibition of discrimination, conditions that became stipulations for receiving federal funding in the mid-1960s. The Civil Rights Act of 1964 (Title VI) and Medicare (1966) prohibited discrimination and tied federal funds to nondiscrimination and segregation, she observed, remarking that “the power of the purse can be very helpful.” She added that research conducted after these laws were passed indicated health benefits from desegregation, including improvements in infant mortality and childbearing outcomes of adult daughters born after the Civil Rights Act became law.
Civil rights laws also addressed other barriers to health care access, McGowan continued, prohibiting discrimination based on race, color, national origin, sex, age, or disability. She pointed out that national origin includes language, which she said has paved the way for limited English proficiency and language barriers to be addressed through provisions that require interpreters and translations, for example. She noted that obesity is covered by the Americans with Disabilities Act only if it is seen as a physical impairment limiting activity and affecting one or more body systems.
McGowan went on to discuss education, underscoring its important impact on health. She explained that federal funding supports public education and includes equal access for students, noting that integration orders had improved educational outcomes and increased funding for schools in majority African American districts. McGowan observed that many inequities exist among school jurisdictions, and suggested that stakeholders in the field would benefit from demonstrating that these inequities can impact such long-term outcomes as incarceration and unsafe environments.
In closing, McGowan observed that though federal and in some cases state or local agencies are responsible for implementing, monitoring, and enforcing civil rights laws, civil rights approaches can be used broadly and applied on a community level. She acknowledged that civil rights laws can help achieve equality as they prohibit discrimination and help direct federal funding, but they do not necessarily get to equity. She encouraged working with communities, relying on sound data, and emphasizing voluntary compliance to help move beyond equality to achieve equity (see Figure 4-1).
AN AFRICAN AMERICAN PERSPECTIVE
Shavon L. Arline-Bradley, founding principal of R.E.A.C.H. Beyond Solutions, LLC, and co-founder of the Health Equity Cypher Group, discussed health inequities that impact African Americans. She began by emphasizing a definition of health inequities that focuses on differences in health status or in the distribution of health resources (NASEM, 2017). She identified as differences in health status for African Americans (compared with whites) higher rates of diabetes, stroke, infant mortality, maternal mortality, breast cancer mortality, and HIV/AIDS and death from coronary artery disease. African Americans are more likely than whites to die at early ages from all causes, she added, and they experience disparities in resources that affect the ability to be a healthy African American in the United States (CDC, 2017a). These resources, she elaborated, include the cost and accessibility of health care; a built environment with safe spaces to play, work, and commute; and opportunities for education, employment, public safety, and transportation (NASEM, 2017).
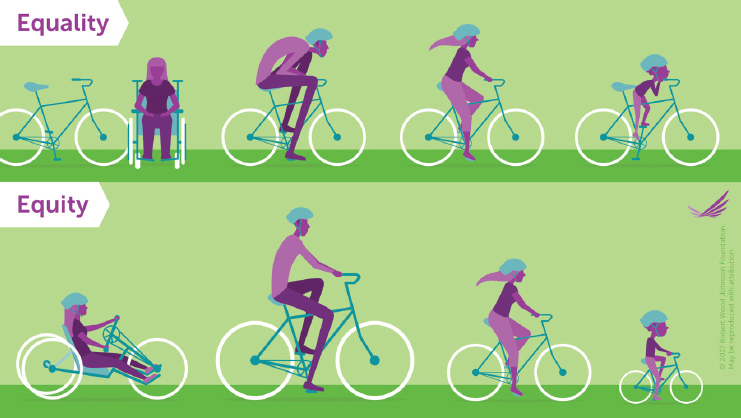
SOURCES: Presented by Angela McGowan, April 1, 2019. Used with permission from the Robert Wood Johnson Foundation (2017).
Arline-Bradley maintained that these experiences of resource disparities for the black community are driven by historical and present-day racism, classism, sexism, discrimination, injustice, segregation, and social isolation. These “isms” and other determinants have hidden behind such terms as “inequity” and “disparities,” she asserted, adding that these determinants have a “massive impact” on the experiences of African American communities.
Focusing on race and the experience of racism as a harmful determinant of health, Arline-Bradley advocated for understanding the institutional (e.g., housing, health care, education) and individual practices, whether intentional or not, that create and reinforce oppressive systems that disadvantage certain groups. She argued that the “lived experience” of race—how people are treated, the resources and jobs available to them, the location where they are likely to live, how they perceive the world, the environmental exposures they face, and the opportunities they have to reach their full potential—either promotes or constrains people’s opportunity to be healthy (Smedley et al., 2008).
Arline-Bradley suggested that such “upstream” determinants of health as housing and education have been shaped by a history of racism. Chattel slavery provides a historical context for the social determinants of health, she elaborated, asserting that the remnants of this practice still infiltrate the United States today. She compared slavery’s stripping of African Americans’
basic human rights and social and legal protections, known as “social death,” with their past and present-day experiences with education, health care access, and voting rights. If African Americans are oppressed with respect to these rights they are supposed to have, she asked, how can they sustain their health in this country?
To illustrate how such contexts as race and class can affect health status, Arline-Bradley recounted a personal story of two of her relatives, born in the early 1900s, who could not access white hospitals because they were African American. Both died at young ages, she said, because this barrier prevented them from getting timely medical care.
Arline-Bradley highlighted that racism operates independently of class, which she suggested helps explain why racial health inequities persist even after controlling for socioeconomic status. Segregation and social isolation persist across income levels, she noted, and everyday discrimination impacts chronic stress (Smedley et al., 2008). She shared a quote from W. E. B. DuBois in 1899 that she said is still true today. In The Philadelphia Negro: A Social Study, DuBois wrote “One thing of course we must expect to find, and that is a much higher death rate at present among Negroes than among Whites: this is one measure of the difference in their social advancement” (DuBois, 1899, p. 148).
According to Arline-Bradley, best practices for addressing health inequities include amplifying and investing in cross-sector partnerships to advance both institutional and public policies that improve opportunities to make healthier choices. She also proposed raising awareness and becoming more politically vocal about structural issues that impact communities of color, and enforcing antidiscrimination laws and policies (Metzl and Roberts, 2014). She called for more research to inform community efforts, to understand how policy changes affect health outcomes, and to discern how cognitive and affective processes influence implicit bias and what interventions can disrupt those processes. She argued that evidence-based programs that feature cross-sector collaboration and create sustainable research opportunities can advance research and the public health care workforce (NASEM, 2017).
Finally, Arline-Bradley urged researchers to integrate community-based models as a standard part of their research portfolios; to develop interventions that consider every social determinant of health for the target community; and to use their data to empower and build the people, “not just publish about the people” (Bor et al., 1995). In closing, she urged the connection of research, programs, and policy, and encouraged the perspective of civil rights advocacy and efforts as a catalyst to improve health behaviors and dismantle oppressive systems.
A HISPANIC/LATINO PERSPECTIVE
Ruth Enid Zambrana, professor in the Department of Women’s Studies and director of the Consortium on Race, Gender, and Ethnicity, University of Maryland, College Park, discussed health equity in Hispanic/Latino populations. She began by sharing an anecdote about a recent trip to the grocery store to purchase fruit and milk, noting that the high cost for a few items could likely have purchased a fast-food meal for a family of four. She urged those discussing obesity in low-income populations to acknowledge an unregulated food industry in the United States whereby the options for low-income families and children often include easily available, inexpensive foods that are nutrient poor and highly caloric.
Zambrana outlined four points that she would discuss in her presentation: the impact of social determinants and risk factors on everyday life for Latinos; equity discourse as action rather than research; an equity focus on structural racism and the policies that perpetuate it; and her belief that structural racism, not culture, is a predictor of inequality. She appealed for dispelling the myth that the United States is a country of immigrants, arguing that misinformation needs to be corrected for Americans to address historically underrepresented groups (African Americans with a history of slavery in the United States, Mexican Americans, Puerto Ricans, and Native Americans).
Latinos come from many countries throughout the world, Zambrana pointed out, and may be white, black, mestizo, or indigenous, clarifying that the term “Hispanic” simply captures Spain’s influence in a country’s history. In the 1980s, she reported, Mexican and Puerto Rican groups resisted the “Hispanic” label because it denied their mixed ancestry, and at the same time there was a call to make Americans and especially government agencies aware of the historical and contemporary inequities in social and economic opportunities, such as higher education. For instance, Zambrana continued, Mexican Americans were denied education in California and Texas until the 1960s. This example of institutional racism helps explain why this group’s level of education remains relatively low, she explained, adding that low education has a ripple effect across such domains as access to home ownership, employment opportunities, and the wealth gap.
Turning to the origins of the Latino population in the United States, Zambrana reported that Mexican Americans have consistently represented 60 to 70 percent of the Latino population, and Puerto Ricans close to 10 percent. The next most populous groups are Salvadoran, Cuban, Dominican, and Guatemalan, followed by those from various Latin American countries that Zambrana said have emigrated since the 2000s because of civil unrest and disruption in their home countries. Overall, she said for context, Latinos represent 18 percent of the U.S. population (Radford and Noe-Bustamante, 2019).
Zambrana next reviewed sociodemographic data for the six most populous groups of Latin origin as she described differences in country of birth, educational attainment, income, health insurance status, English proficiency, and likelihood of citizenship (see Table 4-1). Mexicans are the least likely to be foreign born, she highlighted, noting that many people think of Mexicans as immigrants even though they have been in the United States for many generations. Mexicans have the youngest median age, she added, and for those aged 25 or older, only 9 percent have a bachelor’s degree and 26 percent have a high school diploma. Along with Puerto Ricans, Dominicans, and Guatemalans, she reported, Mexicans are most likely to live in poverty (27 percent) and lack health insurance (34 percent). These patterns have remained relatively stable for the past 40 years, Zambrana underscored, suggesting the importance of studying the persistent effect of those longstanding patterns. She noted further that Mexicans and Puerto Ricans
| Variable | Mexicans | Puerto Ricans | Cubans | Salvadorans | Dominicans | Guatemalans |
|---|---|---|---|---|---|---|
| Foreign-Born | 36% | 1%* | 59% | 62% | 57% | 67% |
| Median Age | 25 | 27 | 40 | 29 | 29 | 27 |
| HS Diploma Only >25 Years | 26% | 30% | 29% | 24% | 26% | 22% |
| Bachelor’s Degree or More >25 Years | 9% | 16% | 24% | 7% | 15% | 8% |
| Median Personal Earnings | $38,700 | $36,000 | $40,000 | $43,000 | $34,000 | $39,000 |
| Live in Poverty | 27% | 27% | 18% | 20% | 26% | 26% |
| No Health Insurance | 34% | 15% | 25% | 41% | 22% | 48% |
| Proficient in English >5 Years | 64% | 82% | 58% | 46% | 55% | 41% |
| Share of Citizens | 73% | 99% | 74% | 55% | 70% | 49% |
*Foreign-born includes those not born in the continental United States (not including Puerto Rico) and whose parents are not U.S. citizens.
SOURCES: Presented by Ruth Enid Zambrana, April 1, 2019 (data from Motel and Patten, 2012; Pew Research Center, 2012). Reprinted with permission.
are most likely to be proficient in English, despite what she said was a myth that among groups of Latin origin, they are least likely to be. Mexicans, Puerto Ricans, and Cubans are most likely to be citizens, she added. Finally, she noted that Cubans, who continue to have refugee status, are the most likely to hold a bachelor’s degree (Radford and Noe-Bustamante, 2019).
Zambrana next presented data illustrating the poverty status of Latino groups. Despite their similarity to whites and Asians with respect to the prevalence of having a full-time worker in the family, she observed, Latinos are the racial/ethnic group most likely to have family income below the federal poverty level (Artiga et al., 2016). She stressed that poverty is a barrier to a host of life-course resources, such as education. Low education, she explained, in turn decreases opportunities for employment that provides access to quality health care benefits and other critical economic resources. As an example, she pointed out that many Mexican Americans and Central Americans tend to work for low pay with no health benefits as seasonal or migrant workers, unskilled workers, and day laborers. In addition, she stated that inadequate to no access to health care services, combined with limited education, is linked to low health literacy and fewer opportunities to communicate with health care providers. Poverty also impedes access to nutritious foods, she added, and to built environments that support safe recreational spaces and physical activity.
Zambrana displayed a chart listing the number of search results and review articles for research conducted on Latino health topics from 2001 to 2016. She pointed out that much research in this area exists, highlighting 464 articles on obesity, 624 on diabetes, and 278 on physical activity. Furthermore, she argued, 40 years of consistent research demonstrates the impact of social and economic determinants of health, such as the physical environment, housing quality, and zip code of residence, on such conditions as obesity and metabolic syndrome. Institutional discrimination is less likely to be studied as a determinant of social and economic disadvantage, she suggested, but new work is addressing this topic.
Zambrana urged caution around the utility of the acculturation construct across all Latino subgroups, which in her view homogenizes all immigrants and Latinos into a single category (even though certain populations tend to be from upper classes). This construct, she emphasized, disallows a focus on history, class, and race and drives differences among Latinos and varying social determinants by subgroup. To illustrate, she pointed out that many South Americans and Cubans tend to possess higher levels of education relative to other Latino groups and are racialized as white, which she argued makes their life course trajectory and economic and social integration into U.S. society different.
Zambrana next showed data on the low rates of adult health insurance coverage among Latinos compared with other racial/ethnic groups, as well
as the Latino population’s relatively high prevalence of delaying health care for cost-related or non-cost-related reasons (Artiga et al., 2016). Family wealth is important, she observed, and it is difficult for families to break out of the intergenerational cycle of poverty. She cited data on the racial gaps in median household income between Latinos and blacks ($43,300) and whites and Asians ($71,300 and $77,900, respectively) (Pew Research Center, 2016). She commented further that the 2008 recession had decreased Latinos’ wealth by 85 percent. In short, Zambrana asserted, the assessment of Latino obesity and its impact on other health conditions requires a social determinants framework that accounts for the intersecting linkages among class or socioeconomic status, racialization, health insurance, place/community resources, economic and discriminatory stressors, and lack of time and recreational spaces, observing that lower socioeconomic status is correlated with higher levels of overweight and obesity. Thus, she stressed that the major factors driving obesity are structural, not individual.
Zambrana then shifted to data on health risk behaviors among foreign- and U.S.-born Latino groups, noting that such disaggregated data are relatively rare. She compared the prevalence of smoking, physical inactivity, obesity, and overweight among Latino groups, flagging the relatively high prevalence of overweight and obesity among U.S.-born Mexicans, physical inactivity and overweight among Mexican immigrants, and overweight and obesity among both U.S.-born and immigrant Puerto Ricans. She added that Central Americans, whether U.S. born or immigrants, had the lowest prevalence of overweight and among the lowest prevalence of obesity (Singh et al., 2013). Sharing another source of disseminated data on Latino population groups, Zambrana reported that the prevalence of obesity was highest among Dominicans and Puerto Ricans (for both men and women) (Daviglus et al., 2012). These data can help identify priority populations for efforts to combat obesity, she suggested, proposing that Mexicans, Dominicans, and Puerto Ricans are the populations of highest priority. They have some of the highest levels of obesity among Latinos, she elaborated, and are more affected than other Latinos by social determinants including poverty, psychosocial stressors, and lack of benefits.
Zambrana closed by urging studies focused not on culture but on social determinants and inequalities in Latinos, such as inequalities in access to health care resources, material conditions, and neighborhood effects. She claimed that the focus on culture has derailed knowledge production and contributed to increasing disparities and inequity (Zambrana, 2011). She proposed an emphasis on translating what is known, “as opposed to continuing to study the same material conditions and expecting to find a different answer, because we won’t.”
AN AMERICAN INDIAN/ALASKA NATIVE PERSPECTIVE
Valarie Blue Bird Jernigan, professor of rural health and director of the Center for Indigenous Health Research and Policy, Oklahoma State University, spoke about how inequities in the social determinants of health relate to obesity prevention and control for American Indian/Alaska Native (AI/AN) populations. For context, she explained that this group numbers 5.2 million and includes 566 sovereign tribal nations concentrated mainly in the western United States, representing about 2 percent of the total U.S. population (U.S. Census Bureau, 2011). She added that the U.S. federal government recognizes native people as citizens of sovereign tribal nations, and this government-to-government relationship affords tribes the ability to deal directly with the federal government.
Jernigan explained that the health disparities experienced by native people arise from general socioeconomic factors in combination with specific cultural and historical factors that are related to their past experiences. She outlined key time periods in the history of tribal nations and American governments since the United States was colonized (see Figure 4-2), noting that this era is generally considered “a very dark time” for native people, one from which they are slowly emerging and seeking healing. The historical experiences of Native Americans include epidemic disease, removal and restriction to reservations, and forced assimilation and urbanization, she recounted, sharing a personal perspective as she described the experiences of her Native American family members. She recalled that her relatives were relocated to urban cities during the Termination Period, a strategy she said was intended to move native people off the land so they would avail themselves of local services in the cities, and the government could then take back their land. Given increased understanding of the role of these historical traumas in Native Americans’ everyday lives, she argued, the study of obesity, diabetes, and other health conditions in these populations must consider the influence of those experiences.
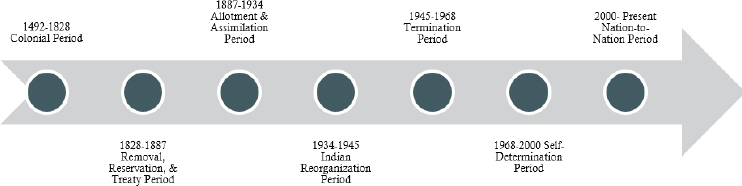
SOURCE: Presented by Valarie Blue Bird Jernigan, April 1, 2019. Reprinted with permission.
Inequities in the social determinants of health affect AI/AN populations more than other racial/ethnic groups in some cases, Jernigan suggested, highlighting that native people have the highest prevalence of poverty among such groups. They also have lower median household income levels and are more likely to lack health insurance coverage relative to the United States as a whole, she added, and are twice as likely to drop out of school than whites (11 percent versus 5 percent, respectively) (U.S. Census Bureau, 2017).
Jernigan focused on the food environment in native communities, highlighting a lack of access to healthy foods and widespread food insecurity (Jernigan et al., 2012, 2017b). In Oklahoma, she elaborated, the prevalence of food insecurity (62 percent) is four times higher than in the general U.S. population and is associated with obesity, diabetes, and hypertension (Jernigan et al., 2017b). She characterized as “shocking” how difficult it is to find healthy foods in native communities, adding that healthy foods are more expensive in native communities than in neighboring non-native communities, and that many native people rely on convenience stores that sell foods high in fat, sugar, and sodium (Jernigan et al., 2012, 2017b).
Jernigan explained that historically, native people’s removal and restriction to reservations resulted in their reliance on the U.S. Department of Agriculture’s Food Distribution Program on Indian Reservations (FDPIR), a monthly program that provides canned and packaged surplus foods. Although intended to augment native people’s household food income, she observed, these food commodities are the only source of food for many native families. Moreover, she continued, most of these foods are high in sugar and fat, and in the past, there was a lack of fresh fruits and vegetables. Despite improvements to the foods offered in the FDPIR, it has been associated with the prevalence of diabetes, hypertension, and obesity among American Indians (Dillinger et al., 1999). Jernigan noted that the literature on food preferences and eating behaviors has evolved to recognize the role of childhood experiences with food, and suggested that native people’s lack of exposure to fruits and vegetables makes it difficult to introduce these foods later in life.
Jernigan then drew attention to a lack of indigenous models of holistic health and wellness for use in designing culturally appropriate, sustainable interventions (Jernigan et al., 2018). The concept of wellness among many indigenous peoples is community-centered, she explained, and emphasizes the perspective that people belong to one another and that the land and its animals are an inherent part of one’s self (Donatuto et al., 2011). In many native communities, she continued, the historical loss of land has led to a loss of culture, knowledge, traditional foods, and ultimately purpose and meaning for native people (King et al., 2009). Jernigan proposed that disconnection from the land has made it difficult to address related
health disparities, suggesting that obesity is “the tip of the iceberg.” She emphasized the importance of culturally centered interventions driven by indigenous concepts of wellness, referencing studies indicating that mental and physical health improves when native people eat traditional foods, engage in traditional activities (e.g., stickball, hula), and “spend time on the land” (Kaholokula et al., 2017; Kirmayer et al., 2009).
In her summary of key implications, Jernigan highlighted that U.S. federal and state obesity policies may not reach tribal citizens because of the sovereign status of tribes, and that the generalizability of “evidence-based” obesity programs and policies is unclear in the context of diverse tribal settings and infrastructures. She called for funding of culturally centered, rigorously designed studies with strong evaluation components. She stressed that tribal nations and communities must have the capacity and infrastructure to implement policies, and it would therefore benefit public health advocates to be familiar with tribal policy-making processes. In closing, she emphasized that tribal leadership benefits from data on health impact and cost-effectiveness as it strives to make informed decisions because tribes are sovereign nations, and the economic impact of programs and policies is key.
DISCUSSION
To kick off the discussion period, session co-moderator Vanessa Northington Gamble commented on themes from the four presentations summarized above. With regard to law, she noted that 1924 was an important year for civil rights in state and federal laws. To illustrate, she referenced the Virginia Racial Integrity Act of 1924, which she said banned marriage between a black and a white person and also defined who could be called Native American. The 1924 Immigration Act, she continued, defined who could be a citizen and excluded Japanese people from naturalization. These legal acts may not appear to be relevant for health care, Gamble suggested, but she expressed her belief that this historical context is important to consider. She highlighted as another theme from the presentations the strength of the human spirit and the resilience of communities in rising above challenges and using their social capital to pursue solutions from within. She also reiterated the importance of examining the lived experiences of people, as well as a group’s historical experiences, to address its social determinants of health effectively.
Following Gamble’s remarks, the session speakers responded to questions from participants about pursuing health equity through structural changes and reparations, community-engaged research, and the Fair Housing Act.
Structural Changes and Reparations
A participant observed that achieving structural transformation by changing laws and policies appears to be necessary in the pursuit of health equity, noting that the speakers had presented a framework in which health equity is a function of historical inequities and challenges. Now that recognition of the importance of historical experiences has emerged, this participant wondered whether there is an opportunity to influence the conversation around reparations, framing it from a health equity standpoint as an opportunity to effect structural change.
Arline-Bradley confirmed that reparations are one part of the solution, but asserted that they will not come close to fully remediating the effect of the African American experience in the United States. Reparations have fiscal as well as political implications, she suggested, clarifying that she is a proponent of reparations as a partial measure, but not as the answer to comprehensive changes in equity. Zambrana cautioned against being distracted by the issue of reparations and proposed that stakeholders influence the “knowledge producers,” such as the National Academies, that can begin to promote a reversal of structural racism. She advocated for universal health care and education, financed by taxes, which she called “two great places to start on health equity.” She added that educating the U.S. population, including university students and professionals with political power, about inequality and inequity is imperative. Jernigan applauded the idea of taking a health perspective on reparations, referencing the Close the Gap Initiative in Australia as an example of an effort to help heal historical injustices. She appealed for health leaders to take responsibility for discussing historical factors as determinants of contemporary disparities and to push for truth and reconciliation.
Community-Engaged Research
Another participant alluded to an apparent bias or “white-centeredness” in the existing research on disparities, and asked whether a change in research frameworks is necessary based on the increasingly recognized importance of allowing affected populations to have a voice in research priorities. Arline-Bradley advocated for community-led approaches in which community members are empowered to help create research agendas, noting that funding priorities do not always align with a community’s values. In the past, she said, researchers have informed communities about research priorities but failed to recognize when the communities had different values and priorities with respect to what research should address. McGowan mentioned that the National Academies’ consensus study Communities in Action emphasized early and continuing community involvement, including
the importance of using data to inform a community about local health inequities and how to address them through a collaborative process (NASEM, 2017). Zambrana wondered whether community-engaged research is a form of deception if researchers tell communities their voices are desired but then cannot act on their contributions.
Another participant asked what innovative methods could be used to inform and engage communities. McGowan suggested that social media and geographic information systems mapping tools could be applied locally to tell the story. Zambrana noted that the populations experiencing health inequities may feel as though a request for participation is an additional burden in their strapped lives, and added that such requests are also a stretch because most of the community organizing for these populations is done by upper-middle-class people. Arline-Bradley argued that the communities deemed overburdened are also perceptive about what is happening. She appealed for a balance between avoiding overburdening people and creating space and opportunities for those who want to be involved. Jernigan urged participation as an organic response to researchers entering a community to give something, not take something. People will share the responsibility, she suggested, if they are working together on something meaningful that they deeply accept as true.
Policies with Disparate Impact and Discriminatory Effect: The Fair Housing Act
McGowan was asked to comment on the Fair Housing Act and whether there is any movement to analyze current initiatives in light of the act’s history in an attempt to repair its consequences with respect to inequities. She replied that civil rights laws apply to intentional discrimination, but an emerging trend is to apply them to disparate impact and discriminatory effect as well. She described the Fair Housing Act as an example of where a historical analysis would show the disparate racial impact of redlining and mortgage and financing practices, noting that, according to a 2015 Supreme Court opinion, the act provided an opportunity to examine disparate impact.
















