
7
Promoting Health Equity Through Early Care and Education
INTRODUCTION
Several important threads are evident throughout this report: the importance of intervening early, preferably before adversity occurs, but if not, soon after; the inextricable interplay between genes and the child’s environment in producing health; the need to support caregivers of children—those who spend significant time with children and therefore have an important impact on children’s growth and development; and the need to create healthy, supportive environments. Knowing that most young children participate in some type of nonparental care on a regular basis (formal or informal arrangements), the early care and education (ECE) platform is a significant opportunity for health promotion and advancing health equity (see the committee’s conceptual model, Figure 1-9, in Chapter 1). ECE is defined here as nonparental care that occurs outside the child’s home. ECE services may be delivered in center-based settings, school-based settings, or home-based settings (i.e., a setting other than a child’s home) (NASEM, 2018); however, this chapter also discusses programs that support parents, such as home visiting. Education itself is incredibly important when it comes to health (García, 2015). Because educational attainment positively correlates with health outcomes, investments in ECE are critical to decreasing disparities to set the stage for future success (Barnett, 2013; NASEM, 2017a). In this chapter, the committee discusses how to apply the important learnings from early development to the ECE system, including the importance of a properly supported and trained ECE workforce, access to quality ECE, and
resources to support these needs. At the end of the chapter, the committee provides recommendations detailing the specific actions needed to ensure that ECE meets its potential to promote child health and well-being. See Box 7-1 for an overview of the chapter.
While ECE has primarily focused on whether it improves children’s cognitive and social-emotional development, as well as academic readiness, there is some indication that ECE may influence child (and even adult) health outcomes, including physical, emotional, and mental health (Campbell et al., 2014; D’Onise et al., 2010; Muennig et al., 2011). What is also of critical importance is how ECE is related to children’s cognitive development, social-emotional development, academic readiness and achievement, and health and well-being, as well as how it can lead to health equity. Hahn and colleagues (2016) postulate that ECE advances health equity through several interrelated systems (see Figure 7-1).
ECE programs increase children’s cognitive, social, and health outcomes through enhancing children’s motivation for school and readiness
to learn and identifying problems that impede learning. This, in turn, helps children improve their cognitive ability and social and emotional competence while increasing their use of preventive health care. There is also evidence that participation in a high-quality early learning program is associated with children’s self-regulation; approaches to learning, such as their motivation and persistence; and executive function (EF) skills, which are domain-general skills that transfer to many areas of development, including learning to read, making friends, and dealing with new challenges (Holliday et al., 2014; Pianta et al., 2009; Yoshikawa et al., 2013). These short-term outcomes of ECE are then expected to lead to lower risk of dropping out of school, greater school engagement, and subsequently better educational attainment, which results in increased income and health care, decreased social and health risk, and improved health equity. Traditionally, ECE is thought of as being confined to a specific age range. For this report, the committee discusses ECE in the context of birth through 8–10 years of age. Another National Academies report,
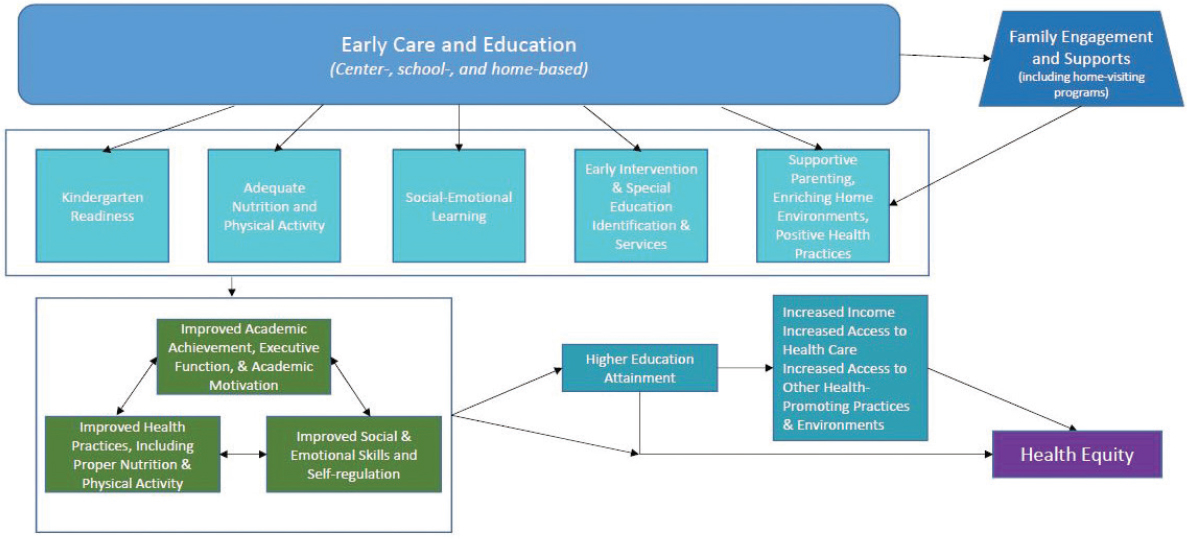
SOURCE: Informed by Hahn et al., 2016.
The Promise of Adolescence: Realizing Opportunity for All Youth, picks up from here, discussing health and development from the onset of puberty into adolescence and early adulthood (NASEM, 2019).
DIRECT LINKS BETWEEN ECE AND HEALTH EQUITY
Health, social-emotional, and other health-related behavioral outcomes are some of the most commonly reported from evaluations of ECE programs, aside from the often-cited cognitive outcomes (Cannon et al., 2017; Carney et al., 2015; Fisher et al., 2014; Rossin-Slater, 2015). ECE programs have been shown to reduce externalizing and internalizing behaviors (Carney et al., 2015), improve social-emotional skills (D’Onise et al., 2010; Hahn et al., 2016), reduce substance use (Cannon et al., 2017; Jones et al., 2015), and improve physical health or well-being (D’Onise et al., 2010; Rossin-Slater, 2015; Sabol and Hoyt, 2017). ECE can produce this range of results through different pathways. It can provide services to children and/or their parents directly that impact their health outcomes and related skills and behaviors; implement evidence-based curricula or interventions to improve children’s social-emotional skills, which are associated with both short- and long-term health and cognitive effects; and support the training and well-being of early childhood educators.
While reviews of the research literature suggest that ECE programs can be a promising lever for improving health outcomes and equity, they also show instances where ECE programs have weak, nonexistent, or even negative impact on children’s behavior and health (Cannon et al., 2017; D’Onise et al., 2010; Hahn et al., 2016; Herbst and Tekin, 2011; Rossin-Slater, 2015). These mixed and negative findings could reflect factors such as lack of program quality, poor fidelity to the program model, and limited program duration. The following section takes a deeper dive into specific ECE programs or interventions that have produced significant results on health and discusses their characteristics.
Links Between ECE and Health Outcomes
A number of studies and reviews of the literature have found positive relationships between participation in ECE programs and physical health indicators and outcomes (Hahn et al., 2016; Kay and Pennucci, 2014). Most of the associated benefits tend to be related to obesity, access to health care, and early screenings and detection. For example, low-income preschoolers enrolled in a center-based program are less likely to experience food insecurity than if they were cared for by parents exclusively or by an unrelated adult in a home setting (Gundersen and Ziliak, 2014). Using a quasi-experimental methodology on data from the Eunice Kennedy
Shriver National Institute of Child Health and Human Development’s Study of Early Child Care and Youth Development (NICHD SECCYD), Sabol and Hoyt (2017) found that 4-year-olds who attended center-based ECE programs had lower blood pressure when they were 15 years old than those who were in a home-based environment, whether that was with a parent, a relative, or a nonrelative.
Hahn et al. (2016) sought to examine the impact of ECE on fostering the health equity outcomes of low-income and racial and ethnic minority children through a meta-analysis. They focused on state and district programs, the federal Head Start program, and foundational model programs, such as the HighScope Perry Preschool Project (PPP) and Carolina Abecedarian (ABC) program. They included studies that were for children aged 3 or 4 years; primarily focused on low-income or racial and ethnic minority populations; were not conducted only in the summer; were based on behavioral interventions; included assessment of effects on children’s health and health-related or academic outcomes; and had a control or comparison population and provided enough data for analysts to calculate effect size and adjust for confounding. Findings were included for the following outcomes: standardized achievement (effect found across program types); high school graduation (effect found only for Head Start); grade retention (effect found across program types); assignment to special education (Head Start was not evaluated on this measure; effect found for all other programs); and crime (effect found across all program types) (see Table 7-1 for more information). Additional analyses examining the persistence of effect of programs on academic achievement and cognitive ability showed a rapid decrease of effects after the program ended, then a gradual decline over time. Higher program quality based on observational data and having teachers with a bachelor’s degree or higher had greater effects on student standardized achievement. There were insufficient data to examine impact of class size, hours, duration, or benefits of additional components, such as family engagement or health access. In sum, there was consistent evidence that center-based ECE programs improved educational and health-related outcomes for low-income and ethnic minority preschool-age children, with some indication of long-term outcomes. Hahn et al. (2016) further note that the fade-out of center-based ECE effects for cognitive and achievement outcomes could likely be because many low-income and ethnic minority children are likely to attend low-resourced (i.e., lower-quality) elementary schools and have teachers with fewer credentials. Others, such as Duncan and Magnuson, have postulated that “preschool programs may affect something other than basic achievement and cognitive test scores, and perhaps these other program impacts, unlike achievement and cognitive impacts, persist over time” (Duncan and Magnuson, 2013, p. 120). That
TABLE 7-1 Effects of Center-Based Early Childhood Education Programs on Education, Social, and Health-Related Outcomes (data for all program types combined)
| Outcome (number of studies; program types included) | Mean Age at Follow-Up, y | Standardized Mean Difference (95% CI) | Effect Meaningful? | Consistent Across Body of Evidence? |
|---|---|---|---|---|
| Test scores (27 studies; all types) | 3.7 | 0.29 (0.23−0.34) | Yes | Yes |
| High school graduation (7 studies; all types) | 20.0 | 0.20 (0.07−0.33) | Yes | Yes |
| Grade retention (12 studies; all types) | 17.0 | −0.23 (−0.43 to −0.02) | Yes | Yes |
| Assignment to special education (6 studies; state and district and model programs) | 15.5 | −0.28 (−0.49 to −0.08) | Yes | Yes |
| Crime (5 studies; all types) | 25.0 | −0.23 (−0.45 to 0.05) | Yes | No |
| Teen birth (3 studies; Head Start and model programs) | 18.0 | −0.46 (−0.92 to 0.0) | Yes | No |
| Self-regulation (5 studies; state and district and Head Start programs) | 18.0 | 0.21 (0.14−0.28) | Yes | Yes |
| Emotional development (7 studies; state and district and Head Start programs) | 4.0 | 0.04 (−0.05 to 0.12) | No | No |
SOURCE: Hahn et al., 2016.
is, looking at discrete and constrained skills, such as letter naming, may not be good predictors, whereas focusing on unconstrained skills, such as self-regulation and expressive language, would be more appropriate. Thus, there is more to understand about the fade-out effect, or arguably the catch-up effect, especially in the changing landscape where more children are in out-of-home settings.
The research is equivocal, however, especially for health, social, and emotional outcomes. Herbst and Tekin (2011) found that 4-year-old children of single mothers who were enrolled in nonparental care
through a child care subsidy were more likely to be obese or overweight when they were kindergartners than those who stayed home. As with a study by Hawkinson and colleagues (2013), this study also found an association between subsidy use and poor cognitive outcomes. A review of 37 studies found “generally null effects of preschool interventions across a range of health outcomes” (D’Onise et al., 2010, p. 1432), leading the authors to caution against relying on a “flimsy evidence base” to inform policy (D’Onise et al., 2010, p. 1432). However, the study did find “a general trend toward beneficial effects, with particularly beneficial effects for overweight and obesity, mental health, social competency, and crime prevention” (D’Onise et al., 2010, p. 1432). They also found that across the studies, half of the comparisons related to immunization and general health yielded positive impacts (and none produced adverse effects).
Foundational Research in ECE
The foundational studies of the HighScope PPP and Carolina ABC project provide the most robust findings regarding the link between ECE and health equity throughout the life course. As described below, these two programs—which occurred in two different states and were conducted by two different teams in two different decades—have similar short- and long-term outcomes. They also shared some common characteristics: they focused on children with the greatest needs and employed an educated and responsive teacher, low child–teacher ratio, active and language-rich learning opportunities, child assessment, and home visiting and family support activities.
Some caution, however, should be taken in generalizing these findings due to the limitations of these studies. They occurred more than 50 years ago, when most children in poverty did not have access to early education services and programs. The samples, primarily African American children, are not representative of the general population. They were also small and continued to decrease over time. Finally, these controlled programs have not been adequately replicated at a large scale. It is also critical to note that not all children in the treatment groups performed at the highest level and in the end, did not surpass their more economically advantaged peers. For example, in the PPP study almost one-third of children from the treatment groups were arrested five or more times by age 40, almost one-third did not graduate high school, and almost two-thirds of children from the treatment group required public assistance as adults (Gomby et al., 1995). Thus, these programs did not equalize the outcomes for children from low-income households in comparison to their higher-income peers.
While PPP and ABC provide a blueprint to build from to support children’s school readiness, achievement, and health equity throughout the life course, policy makers and practitioners alike need to base their decisions on lessons beyond those from these studies, such as more contemporary ECE programs and interventions discussed in this chapter, to ensure that all children, especially children with the greatest needs, have the same opportunity to thrive and lead healthy lives.
HighScope Perry Preschool Project (PPP)
The HighScope PPP started in 1962 with a focus on serving 3- and 4-year-olds (it was 1–2 years long) with a home visiting component. The program aims to promote social and cognitive development in children who are at risk due to poverty. Schweinhart and Weikart (1997) showed that students enrolled in the program in 1986 had more positive behavior and attitudes than students in the control group (Schweinhart and Weikart, 1997). In addition, experimental evaluations of study participants in their teens and 20s showed that even years later, when study participants were in their teens and 20s, students formerly enrolled in the program “had higher academic grades and earnings, higher rates of high school graduation, fewer arrests and out-of-wedlock births, and lower levels of welfare receipt than their peers who were not in a preschool program” (Child Trends, 2012). Furthermore, children in the intervention group had higher rates of safety-belt use and engaged in fewer risky health behaviors, such as smoking and illicit substance use, in adulthood compared to those in the control group. At age 27, former PPP students were more likely to be employed and had higher earnings than students in the control group (Child Trends, 2012; Schweinhart et al., 2005). This continued into age 40, with former PPP students having higher earnings, committing fewer crimes, and being more likely to hold a job and to have graduated from high school than adults who did not participate in PPP. In 2019, Heckman and Karapakula presented findings from the HighScope PPP Age 55 Study (Heckman and Karapakula, 2019a). They indicated that the program kept parent engagement active longer, which resulted in more warmth and less authoritarian parenting. They also found that at age 55, the female participants in the early childhood intervention group had lower cortisol (39.01 versus 89.29 picograms per milligram) compared to the control group, and the male participants were less likely to have high cholesterol levels (mean differences in high cholesterol1 were 0.71 in the treatment group versus 0.94 in the control group). Female participants
___________________
1 High total cholesterol indicates whether total cholesterol concentration in milligrams per deciliter is 220 or higher.
in the intervention group were also less likely to be uninsured for a prolonged period compared to the control group (Heckman and Karapakula, 2019b). In addition, they reported intergenerational effects for children of intervention participants: completion of high school, good health status, stable employment, and a history of never having been suspended and arrested (Heckman and Karapakula, 2019a).
Carolina Abecedarian (ABC) Study
The Carolina ABC Study is a center-based intervention that enrolled families between 1972 and 1977 based on a high-risk index. During recruitment, 111 infants were matched on high-risk scores and then assigned to preschool treatment or control status. Fifty-seven infants were assigned to the experimental group and 54 to the control group (Campbell et al., 2012). The families in the study were mostly African American with young mothers, less than a high school education, unmarried, living in multigenerational homes, and reporting no earned income (Campbell et al., 2012). The service delivery model for the experimental group was a 5-year, full-day, year-round, center-based program with a comprehensive curriculum (LearningGames®) (Sparling and Lewis, 1979) focused on educational games addressing children’s cognition, language, and adaptive behavior. The program also emphasized health care and family support programs. Activities were individualized for the child’s needs, with more conceptual and group-oriented activities as children got older. Families in both the experimental and control groups received supportive social services. Findings showed that children in the 0–5 intervention group had better cognitive, academic, and emotional outcomes (Ramey and Ramey, 2004). This also had persistent effects when children were in their 20s, with children in the treatment group having better intellectual test performance and reading and mathematics test scores, more years of education, and a greater likelihood of being enrolled in college (Campbell et al., 2012; Frank Porter Graham Child Development Institute, 2012). By age 30, the treatment group was more likely to have completed a bachelor’s degree, have consistent employment, not use public assistance, and have delayed parenthood. Regarding health outcomes, Campbell et al. (2014) found through biomedical data that children in the intervention group at age 35 had significantly lower risk factors for cardiovascular and metabolic disease, especially for male participants (i.e., mean systolic blood pressure for the control group was 143 versus 126 for boys in the intervention group). “One in four males in the control group was affected by metabolic syndrome, while none in the treatment group were” (Ramey, 2018, p. 539).
Looking across the body of research, Head Start appears to be particularly effective at promoting young children’s physical health (see
Box 7-2 for more information on Head Start). The Head Start Impact Study showed that children enrolled in the program had better access to dental care while they were in the program and to health insurance when they were in kindergarten (Puma et al., 2012). Broader reviews of research on Head Start show positive impacts on obesity, immunization, screening for hearing and vision problems, and even child mortality (Belfield and Kelly, 2013; Rossin-Slater, 2015; Yoshikawa et al., 2013). In addition, in their review of Early Child Longitudinal Study-Birth Cohort (ECLS-B) data, Belfield and Kelly (2013) found that Head Start provided its participants “protective effects against . . . asthma, respiratory ailments, allergies, and being on medication” (Belfield and Kelly, 2013, p. 322). Lee et al. (2013) used data from ECLS-B to analyze low-income children’s nutrition, weight, and health care receipt at kindergarten entry. They compared (a) Head Start participants and all nonparticipants, and (b) Head Start participants and children in pre-kindergarten (pre-K), other center-based care, other nonparental care, or only parental care using propensity score–weighted regressions. They found Head Start effects were larger compared to informal child care settings rather than center-based settings. Specifically, Head Start children had lower body mass index (BMI) scores and probability of being overweight compared to children in home-based settings; had better healthy eating habits than children in center- and home-based settings; and were also more likely to have dental care checkups compared to children in any other type of setting, including pre-K and center-based settings. Furthermore, dosage appears to matter. Frisvold and Lumeng (2011) analyzed administrative data from more than 1,500 children from Head Start programs in Michigan from 2001 to 2006 and found that children who participated in full-day Head Start were 25 percent less likely to be obese at the end of an academic year than those who enrolled in half-day programs. The effect seems to be more pronounced for boys and African American children.
One reason that Head Start stands out among ECE programs with respect to impact on physical health outcomes may be that the program design includes a robust health component (such as requiring programs to provide diverse nutrition and health services, helping families receive physical examinations by scheduling screening appointments or offering screenings directly onsite, assisting families in applying for age-appropriate health care services, providing health promotion activities directly onsite, and tracking each child’s health progress) (Lee et al., 2013). In their review of the literature, Yoshikawa et al. (2013) concluded that “in contrast to the literature on Head Start and health outcomes, there are almost no studies of the effects of public prekindergarten on children’s health” (Yoshikawa et al., 2013, p. 5) because pre-K programs typically do not provide health-related services.
However, pre-K programs can incorporate such services and potentially achieve similar outcomes. A recent evaluation of the Universal Pre-K (UPK) program in New York City found that the expansion of the program “led to increases in rates of diagnosis of asthma and vision problems, to increased rates of screening for immunization or infectious disease, and to increased rates of treatment of hearing and vision problems” among Medicaid recipients who were eligible for UPK (Hong et al., 2017, p. 3). The researchers attribute some of these findings to UPK’s program requirements, which include immunizations and developmental screenings for all enrolled students. In other words, by incorporating direct services2 into their program design, Head Start and New York City’s UPK initiative have become opportunities to effect broad improvements in young children’s health outcomes.
Head Start and the UPK program in New York City are just two examples of large-scale, publicly funded ECE programs that have demonstrated generally positive results for preschool children. Others include state-funded pre-K programs in Georgia, New Jersey, North Carolina, and Oklahoma and district-run programs, like that of Boston. In a review of the body of research behind these and other large, publicly funded programs, Phillips et al. (2017) concluded that there is robust evidence of short-term benefits, especially in cognitive and academic skills. However, “the available evidence about the long-term effects of state pre-k programs offers some promising potential but is not yet sufficient to support confident overall and general conclusions about long-term effects” (Phillips et al., 2017, p. 10). For example, Lipsey et al. (2018) found that although children who participated in the Tennessee pre-K program demonstrated better cognitive skills than the control group, this advantage was lost or even reversed by 2nd or 3rd grade.
Still, the promising results from large-scale, publicly funded pre-K programs, in light of the impacts that Head Start and New York City’s UPK program have on young children’s health outcomes, suggest that ECE programs that serve significant proportions of young children can be a platform for interventions that promote health equity.
Home-Based Child Care Programs
Home-based child care is regulated family child care and family, friend, and neighbor care (Porter et al., 2010b). As mentioned earlier, it is a common arrangement for many young children in the United States,
___________________
2 For example, immunization and a valid and reliable developmental screening tool to identify students with potential developmental delays and English Language Acquisition support needs.
particularly those from low-income families and families of color (Porter et al., 2010b). As Porter et al. note, “parents use these arrangements for a variety of reasons, including convenience, flexibility, trust, shared language and culture, and individual attention from the caregiver” (Porter et al., 2010a, p. 1). Home-based child care also serves as a primary nonparental care arrangement for infants and toddlers (Corcoran et al., 2019). (See Chapter 3 for statistics by race, ethnicity, and income.)
While most young children who are not yet enrolled in kindergarten participate in some kind of weekly center- or school-based early childhood program, 41 percent of them receive care weekly from a relative, and 22 percent participate in nonrelative care in a home environment (Corcoran et al., 2019). (Twelve percent of young children receive care in more than one of these settings on a weekly basis.) The number of children in center-based care increases as children get older. Furthermore, about 3.6 million of the approximately 3.7 million home-based providers are “unlisted”: they are not registered with, licensed by, or regulated by a public agency. Together, these home-based providers serve more than 7 million young children (National Survey of Early Care and Education Project Team, 2016). Children of color are more likely to receive care from a relative, while white children are more likely to participate in nonrelative home-based care. Infants and toddlers are more likely to be cared for in a home setting—whether with a relative or nonrelative—while preschool-aged children are more likely to be enrolled in a center- or school-based program. Families with a household income of $75,000 or less are also more likely to put their young children in relative care (Corcoran et al., 2019). Thus, to the extent that regulations and policies related to safety and quality promote better care and child development, the youngest children, low-income children, and children of color could disproportionately lack access to ECE opportunities that are more equipped to support their cognitive, social-emotional, and healthy development.
The majority of evidence linking ECE to children’s health, education, and well-being is primarily from center- and school-based programs. Some studies have shown a link between home-based programs and children’s academic skills and social-emotional development. For example, Iruka and Forry (2018) found that children in home-based programs that were high quality and engaged frequently in enriching literacy and numeracy activities (e.g., learning names of letters, learning the conventions of print, using manipulatives, using a measuring instrument, learning about shapes and patterns) were likely to have stronger reading and math skills compared to children in home-based programs that were low quality and engaged in fewer enriching activities. This is consistent with prior work by Forry et al. (2013) using data from a multistate study of a professional development intervention showing that the quality
of home-based programs, their child-centered beliefs (e.g., progressive beliefs that children should have autonomy and be allowed to express their ideas), and their perceptions of job demands were related to children’s school readiness, emotional health (e.g., initiative, self-control, and attachment), and internalizing and externalizing problem behaviors.
However, mostly correlational data indicate that children in centers compared to family child care homes had higher cognitive, language, and school readiness scores but increased likelihood of contracting communicable illnesses and otitis media (ear infection), which is likely due to the large group size (Bradley and Vandell, 2007). While the data are mixed, there is indication that children in home-based programs have stronger social-emotional competence compared to children who attended center-based programs (Belsky et al., 2007). In their analyses examining multiple child care arrangement and children’s academic and behavioral outcomes, Gordon et al. (2013) found that preschool children, on average, scored higher on reading and math assessments when they attended centers alone or centers in combination with home-based programs than home-based programs only or parental care. There were no differences in children’s social-emotional development between families who used or did not use multiple care arrangements. The stronger benefits for children’s cognitive and school readiness skills for center-based compared to home-based programs have also been seen for Latino children (Ansari and Winsler, 2012).
These better academic outcomes for center- versus home-based programs are likely due to higher teacher education and more training opportunities (Bradley and Vandell, 2007). However, the larger group size in center-based programs may preclude sensitive individual care and attending to children’s social-emotional needs, which could exacerbate problem behaviors (Gordon et al., 2013). There is still a need for more rigorous examination of the differential impact based on program type and accounting for differences in teacher education and training, sociodemographics of children and families, and more robust health-related outcomes.
Quality Rating and Improvement Systems (QRISs)
Motivated in part by ECE research, states and localities have implemented QRISs to promote and enhance ECE program quality across various sectors and settings, including schools, community-based organizations (center- and home-based), and Head Start. State and local policy makers have used research linking high-quality early childhood education and children’s outcomes in developing QRISs to ensure that children, especially disadvantaged children, are attending high-quality education
programs during the early years. QRISs could serve as a unifying framework for defining quality across ECE programs and a defined pathway for achieving it. Moreover, without a strategy such as a QRIS, ECE programs could have inequitable resources for improvement, exacerbating the variance of quality among programs and leading to inequitable outcomes for children, families, and communities. When funded adequately and supported as a unifying strategy for ECE, QRISs can raise the overall quality of the ECE system and create more equity across communities.
Almost all QRISs measure staff training and education and assess the classroom or learning environment (Burchinal et al., 2015). Factors such as parent-involvement activities, business practices, child–staff ratios, and national accreditation status vary by state (Burchinal et al., 2015; Zellman and Perlman, 2008). QRISs serve multiple purposes, including providing a standardized method to rate program quality—based on a set of criteria—and to make the program rating information available to parents, as is done with restaurant ratings. The rating system is built on the primary assumption that parents often lack good information about program quality and that such information would inform their decisions on program selection (Burchinal et al., 2015). Consequently, providers who work with lower-quality programs would be incentivized to enhance the quality of their program or leave the market (Burchinal et al., 2015; Zellman and Perlman, 2008). In addition, QRISs represent a systematic approach to providing a range of technical assistance, resources, and incentives for programs to improve their quality (Burchinal et al., 2015). This could entail consultation on quality improvement, increased investments for professional development scholarships, microgrants for other targeted efforts, and increased subsidy payments for more highly rated programs (Burchinal et al., 2015). It has been noted that regarding QRIS,
the goal of these efforts is to foster and support providers’ efforts to improve the quality of care they provide. Thus, [QRISs] attempt to improve quality by affecting both the demand for high-quality care and the supply of such care. Of course, the success of such efforts rests on the ability of rating systems to accurately identify and measure key aspects of quality and the willingness of providers to participate in a rating system. (Burchinal et al., 2015, p. 255; see also Zellman and Perlman, 2008)
Validation of QRISs has yielded mixed findings. The Race to the Top—Early Learning Challenge Grant resulted in a proliferation of QRIS validation studies. Prior to this, most research on QRISs was descriptive and focused on issues of implementation. A recent synthesis of the validation studies by Tout et al. (2017) from 10 states found that while these ECE rating systems were valid (i.e., independent observations indicated meaningful differences across levels), most programs were, on
average, providing a moderate level of quality and inconsistently associated with child outcomes, mostly for social-emotional development and EF outcomes.
There has been a limited focus on children’s physical health. In their synthesis of states’ QRIS validation studies, Tout et al. (2017) found that only two states focused on physical development, which included BMI and fine and gross motor skills. One state found a link between its QRIS and children’s fine motor development, indicating that higher-rated programs were associated with improved fine motor development. Several states have included nutrition, physical activity, and screen time as part of their QRIS standards (Gabor and Mantinan, 2012). In their report to examine state efforts to address obesity prevention in QRISs, Gabor and Mantinan (2012) found specific standards, including a focus on nutrition (including standards), physical activity and screen time limits, professional development for staff and teachers, and sharing information about nutrition and physical activity with families.
The differences in system designs across states make it difficult to draw general conclusions from these validation studies about their links to various domains of children’s development, especially health. The voluntary nature of QRISs in most states and the varying standards also make it difficult to establish a causal link between them and child outcomes. Even with these limitations, the QRIS is one potential, and perhaps underused, platform that could increase the use of evidence-based, health-promoting practices and standards in a mixed-delivery system by unifying leadership and governance, standards, financing, stakeholder engagement, improvement supports, accountability, and continuous quality improvement. As QRISs expand, mature, and become better funded, they could serve as the one point of entry that promotes high-quality programming across various settings (e.g., home, school, centers) and provides more children, especially children with the greatest needs, with access to beneficial ECE experiences that meet their comprehensive needs regardless of program funding.
Early Intervention for Children with Developmental Disabilities
Early Intervention3 services support the early development of children with developmental delays or specific health conditions that could lead to delay (e.g., genetic disorder, birth defect, hearing loss). These services and programs intend to help children catch up and increase their chances for school and life success, though most of this work falls
___________________
3 Early intervention refers to services for children ages 0–3. Early childhood special education refers to services for children ages 3–5.
to parents and families. Early intervention services are provided under the Individuals with Disabilities Education Act (IDEA). Eligible children are able to receive services free of charge (or at a reduced rate) through federal grants to states. Each state has its own definition of developmental delay and its own process for determining eligibility and identifying eligible children. Families with children under age 3 who qualify for early intervention receive an Individualized Family Service Plan that defines goals and the types of services that will support the family and child. Children older than age 3 who are eligible for special education services under IDEA meet with school professionals to develop an Individualized Education Program to support their educational goals.
Some of the specialists who work with children include speech-language pathologists, who help with communication speech and language delays; physical therapists, who strengthen children’s movement, gross motor skills, and physical development; occupational therapists, who improve fine motor, cognitive, sensory processing, and communication skills; nurses, who support children’s health status and address feeding and growth concerns; social workers, who assess and support children’s social and emotional development; and developmental therapists, who design learning activities to promote children’s learning and social interaction skills.
Early Intervention (Children Under 3 Years Old)
A substantial body of research supports the effectiveness of early intervention for children’s functioning (Bruder, 2010; Guralnick, 2005). However, these studies suffer from methodological limitations, such as sample heterogeneity, lack of control groups, narrowly defined outcomes, and inappropriateness of standardized measures of intelligence (Bruder, 2010). Nevertheless, there is a body of research indicating that children who receive early intervention services (Part B or Part C) are less likely to see a decline in their functioning over time, with effect sizes of 0.5 to 0.75 of the standard deviation (Guralnick, 1998). This is supported by a foundational meta-analysis of 31 studies examining the effect of early intervention, which found that early intervention was “effective in promoting developmental progress in infants and toddlers with biologically based disabilities” (Shonkoff and Hauser-Cram, 1987, p. 650). The mean effects of early intervention services ranged from 0.43 for motor development to 1.17 for language development. In particular, they found that “programs that served a heterogeneous group of children, provided a structured curriculum, and targeted . . . parents and children together appeared to be the most effective” (Shonkoff and Hauser-Cram, 1987, p. 650).
In their study of community-based early intervention services for children who were in neonatal intensive care units (NICUs), Litt et al. (2018) analyzed retrospective data from the U.S. Department of Education’s National Early Intervention Longitudinal Study and found that longer and more intensive services were associated with higher kindergarten skills ratings and the importance of following up after children left the NICU. These findings are consistent with those from McManus et al. (2012) in their longitudinal study of mother–infant dyads from three NICUs in southeastern Wisconsin. They matched pairs of dyads using propensity-score matching to reduce selection bias and estimate the effect of early intervention services on cognitive function trajectories. They found that service receipt was positively associated with children’s cognitive functioning and trajectory and more maternal supports (e.g., mothers’ report of emotional, informational, child care, financial, respite, and other support) was associated with better outcomes for families over time. Unfortunately, national data indicate that children who qualify for early intervention services are not likely to receive them, with this issue especially pronounced for black children (Boyd et al., 2018).
Most of the recent evidence about early intervention has primarily focused on children with autism spectrum disorder (ASD), which “is characterized by severe and sustained impairment in communication and social interaction and restricted patterns of ritualistic and stereotyped behaviors manifested [before] 3 years old” (APA, 2013). Children with ASD often qualify for early intervention services, usually because they are not developing in social, play, language, and cognitive domains at the expected pace (Landa, 2018). In her review of the efficacy of early interventions for young children with or at risk for ASD, Landa (2018) found that greater intervention intensity (hours and duration in months) and fidelity of implementation were associated with greater child gains. One of the applied behavior analysis approaches for children with ASD is called Early Intensive Behavioral Intervention (EIBI), which focuses on remediation of deficient language, imitation, pre-academics, self-help, and social interaction skills (Peters-Scheffer et al., 2011). In a meta-analysis examining the effectiveness of EIBI, Peters-Scheffer and colleagues (2011) found that the experimental groups outperformed the control groups on IQ, nonverbal IQ, expressive and receptive language, and adaptive behavior, with differences of 4.96–15.21 points on standardized tests. Reichow (2011) offered a similar conclusion in his overview of five meta-analyses of EIBI for young children with ASD, but he also stressed the importance of more information about child characteristics, additional knowledge on the characteristics of EIBI programs used in real-world settings, and guidelines focused on the intensity, duration, level of treatment fidelity, and therapist experience and/or training necessary to achieve optimal outcomes.
There are disparities in service access for economically disadvantaged and racial and ethnic minority families who have children with ASD (Boyd et al., 2018), and these children are also “at risk for poorer outcomes in comparison to their white and higher-income counterparts, including a more severe symptom presentation (e.g., more severe language and cognitive delays)” (Boyd et al., 2018, p. 20; CDC, 2014; Cuccaro et al., 2007; Fountain et al., 2012). One posited rationale for these poorer outcomes is lower-quality or fewer services (Boyd et al., 2018) and lower likelihood of being referred for services (Delgado and Scott, 2006).
Early Intervention/Special Education (Children 3 Years Old and Older)
Special education provides children with disabilities with specialized services designed to “prepare them for further education, employment, and independent living.”4 “Practitioners are responsible for providing specific services, instructional strategies or routines, and resources that mitigate the impact of the disability on a child’s learning or behavior” (Morgan et al., 2010, p. 236). “Helping the child to benefit from the school’s curriculum should in turn increase subsequent educational and societal opportunities” (ED, 2018; Morgan et al., 2010, p. 236).
The majority of students with disabilities performed in the “below basic” achievement level in all four areas of measurement (mathematics and reading, in 4th and 8th grade) in 2017. The gaps between students with disabilities and those without disabilities are substantial (Advocacy Institute, 2019). Youth with disabilities are also more likely to drop out of school, be delinquent, be unemployed, earn less, and be unsatisfied with their adult lives (Blackorby and Wagner, 1996; Horowitz et al., 2017; Thurlow et al., 2002). There is some evidence that at the end of the school year, youth placed in special education classrooms sometimes score lower on measures of reading, writing, and mathematics skills than they did at the start of the school year (Lane et al., 2005; Morgan et al., 2010).
Establishing rigorous evidence for special education services through randomized controlled trials (RCTs) is not possible because of the legal entitlement to these services for children meeting eligibility criteria, the small sample sizes, and the distinct categories and severities of disabilities (Hocutt, 1996). Thus, different quasi-experimental approaches (e.g., propensity matching) are used to gauge the impact of special education services on children’s outcomes. In one study using propensity-score matching with data from the Early Childhood Longitudinal Study-Kindergarten Class (ECLS-K), 1998–1999, which is a large-scale, nationally representative sample of U.S. schoolchildren, Morgan et al. (2010) examined whether
___________________
4 Individuals with Disabilities Education Improvement Act. P.L. 108-446.
children receiving special education services displayed (1) greater reading or mathematics skills, (2) positive learning-related behaviors, or (3) less frequent externalizing or internalizing problem behaviors than closely matched peers not receiving such services. The results indicated that special education services had either a negative or statistically non-significant impact on children’s learning or behavior but a small positive effect on children’s learning-related behaviors, such as their attention on task. Part of these findings may be due to the settings in which children are receiving services. For example, a review conducted by Ruijs and Peetsma (2009) examining the effects of inclusion on students with and without special education showed neutral to positive effects of inclusive education. Specifically, they found that students with special educational needs performed academically better in inclusive than noninclusive settings, possibly because they could learn from more able students or be more motivated to succeed because of the academic focus. Mixed results were found for social-emotional development, with some positive outcomes on social and emotional ratings and negative outcomes based on peer perceptions.
Other Issues in Special Education
Disproportionality in identification Skiba et al.’s (2005) analyses of cross-sectional state-level data indicated that black and Hispanic children were overrepresented in special education. They found this for multiple disability conditions, including intellectual disability, emotional disturbance, speech-language impairment, and learning disability. This supported prior work conducted by Oswald et al. (1999) using cross-sectional, nationally representative, and district-level data showing that minorities were overrepresented in special education, specifically in the mild mental retardation and serious emotional disturbance categories. Oswald et al. (1999) defined disproportionality as “the extent to which membership in a given ethnic group affects the probability of being placed in a specific special education disability category” (Oswald et al., 1999, p. 198), such as mild mental retardation. Morgan et al. (2015), using ECLS-K 1998 data, found minority students were underrepresented, which contradicts previous findings. Analyses of ECLS-K data of multiyear longitudinal observations and extensive covariate adjustment for potential child-, family-, and state-level confounds showed that minority children were consistently less likely than similar white, English-speaking children to be identified as having a disability and so to receive special education services. From kindergarten entry to the end of middle school, racial and ethnic minority children were less likely to be identified as having learning disabilities, speech or language impairments, intellectual disabilities, health impairments, or emotional disturbances. Language-minority children were less
likely to be identified as having learning disabilities or speech or language impairment (Morgan et al., 2015). Many reasons likely account for the mixed findings, including cross-sectional versus longitudinal data, national compared to state or local data, child- versus school-level data, special education category, and trying to equate white and ethnic minority children when the latter are more likely to experience larger risk factors for developmental delay (e.g., poverty).
Nutrition Support Programs
For young students in elementary grades, schools are critical settings to support their health, such as in the area of nutrition. The National School Lunch Program (NSLP) was established under the National School Lunch Act, signed by President Harry Truman in 1946, to “safeguard the health and well-being of the Nation’s children and to encourage the domestic consumption of nutritious agricultural commodities and other foods” (USDA, 2017). The largest of the five school- and center-based programs, NSLP fed about 30 million children each school day in 2014 and cost $12.7 billion (CBO, 2015). In 2014, 52 percent of school-aged children (ages 5–18) participated in NSLP, and 23 percent participated in the School Breakfast Program (SBP) (CBO, 2015). Almost half of all lunches served are provided free to students, with an additional 10 percent at reduced prices. Ethnic minority students participate in NSLP at slightly higher levels than white students, and students from low-income households participate at higher rates than those from higher-income households (Ralston et al., 2008). Ninety-four percent of schools, both public and private, choose to participate in the program (though they are not required to offer NSLP meals). NSLP accounts for 17 percent of the total federal expenditures for all food and nutrition assistance programs (Ralston et al., 2008). School meals are required to meet nutritional targets for calories, protein, calcium, iron, and vitamins. Recent changes in standards have made these meals healthier by reducing salt and saturated fat and increasing servings of fruits and vegetables. While such policies should theoretically lead to improvements in health and nutrition, there is emerging evidence that children may be less likely to consume healthier meals. Some schools have also stopped participating in NSLP because of the increased costs. To be sure, these findings are from only a few studies, and more research on the overall impact on higher nutrition standards is needed (Gundersen, 2015).
Under separate legislation, this program provides free, reduced-price, and full-price breakfasts to students. Other related programs include the Summer Food Service Program (also known as the Summer Meals Program), which extends the availability of free breakfasts and lunches into the summer months in low-income areas; the Special Milk Program,
which provides subsidized milk to schools; and the After-School Snack Program, which “reimburses schools for healthy snacks given to students in educational after-school programs” (Ralston et al., 2008, p. 5). Food insecurity increases during the summer months, when children do not have access to NSLP, and the Summer Food Service Program could alleviate this problem. As of 2012, the Summer Food Service Program has a budget of under $400 million and serves a fraction of the children that NSLP serves (Gundersen, 2015). Alternatively, Supplemental Nutrition Assistance Program (SNAP) benefits can be increased during the summer months. Based on one demonstration project, it is estimated that an increase of about $2 billion in SNAP could minimize the spike in food insecurity during the summer (Gundersen and Ziliak, 2014).
Based on the report from Ralston et al. (2008), there is mixed evidence on the impact of NSLP on obesity and nutrition. For example, some studies show that children who participate in NSLP have higher intake of key nutrients and lower intake of sweets compared to nonparticipants. Other studies find high intakes of fat and sodium, which may be due to school programs not following the guidelines about fat and sodium levels. This mixed finding may be due to selection effect. For example, in their examination of NSLP on children’s behavior, health, and academic outcomes, Dunifon and Kowaleski-Jones (2003) found that NSLP was associated with an increase in children’s externalizing behavior and health limitation (i.e., limitation in being able to participate in regular activities) and a decrease in their math scores. However, once family-level factors associated with the selection of children’s NSLP participation were adjusted, the effects attenuated. Even after addressing selection effects, there are still mixed findings about the impact of NSLP, with some studies finding participants likely to be overweight (e.g., Schanzenbach, 2009) and others (Gundersen, 2015; Hofferth and Curtin, 2005) finding no effect on obesity. Recent studies to address missing counterfactuals and systematic underreporting of program participation (Gundersen et al., 2012) through causal analytical approaches found some indication of a positive link between NSLP and health outcomes. For example, Gunderson et al. (2012), using data from the 2001–2004 National Health and Nutrition Examination Survey study conducted by the National Center for Health Statistics and the Centers for Disease Control and Prevention, found that NSLP reduced the prevalence of food insecurity by at least 3.8 percent, the rate of poor health by at least 29 percent, and the rate of obesity by at least 17 percent.
While questions remain about the impact of NSLP on child outcomes, there is consistent evidence about the SBP. Whereas almost all schools participate in NSLP, about 75 percent are part of the SBP, serving 13.2 million children in 2013 (Gundersen and Ziliak, 2014). Frisvold (2015) used the National Assessment of Educational Progress (NAEP) and ECLS-K to
determine the impact of SBP on school achievement. Using the NAEP data, he found that availability of SBP increases math by 9 percent of a standard deviation and reading achievement by 5–12 percent of a standard deviation. ECLS-K data show that SBP increases math achievement by 2.7 percent of a standard deviation, reading achievement by 2.0 percent of a standard deviation, and science achievement by 0.9 percent of a standard deviation each school year. Gleason and Dodd (2009) also found a positive effect of SBP but not NSLP on children’s health. Specifically, they found that participation in the SBP is associated with lower BMI but saw no evidence for participation in NSLP and BMI. This association is strongest among white children and not significant for Hispanic children. The mechanism of the effect between SBP and learning is likely through improvement in nutrition, such as increased milk and fruit consumption and decreased soda consumption (Frisvold, 2015).
Beyond NSLP and SBP, there is a need to conduct in-depth examination of other food and nutrition programs. The Child and Adult Care Food Program (CACFP) reimburses child care programs (both centers and homes) and after-school programs for meals and snacks. Funded at about $3 billion and serving 3.3 million children in 2013, it is much smaller than NSLP and SBP. One study using the ECLS-B dataset found that participating in CACFP was not associated with any changes in the experience of food insecurity (Gundersen and Ziliak, 2014).
Summary
The PPP and ABC studies were seminal because they inspired research on why the early years are so important to cognitive and health outcomes. They also inspired the design and implementation of large-scale, publicly funded ECE programs that the field continues to evaluate, improve, and refine over time—many of which are discussed in this chapter. The evidence linking health equity to ECE programs and services, including Head Start, pre-K, early intervention, special education, and nutrition programs, is mixed. However, the totality of the research demonstrates effects that are generally positive, albeit with small effect sizes and non-findings in some instances. This indicates that ECE can play an important role in improving health outcomes that could lead to health equity and there is value in continuing to ensure that children have high-quality early learning experiences from birth, though programs may differ in standards, practices, auspices, workforce, dosage, and timing. In order to maximize the impact of ECE, the field will have to better understand how the lessons of PPP and ABC apply (or not) in the current context, with a different counterfactual (i.e., more children with access to some ECE) and more diverse children and programs that operate under different funding
systems and auspices. The field will also have to learn from contemporary large-scale, publicly funded programs and identify essential ingredients that lead to robust health outcomes and health equity. Only then can ECE be meaningfully part of a health promotion strategy that ensures children with the greatest needs are being served, that their needs are met early and consistently (e.g., through early intervention and nutrition), and in a diversity of settings (e.g., home- or center-based care) through a unifying system that provides high-quality access for all children.
LINKAGES BETWEEN ECE AND HEALTH EQUITY THROUGH SOCIAL-EMOTIONAL DEVELOPMENT
Social-Emotional/Behavioral Development
Social-emotional skills, including emotional processes, social/interpersonal skills, and cognitive regulation (Jones and Bouffard, 2012), in young children have been shown to predict later health outcomes and behaviors, such as substance use or abuse, mental health problems (e.g., depression), and teen pregnancy (Conti et al., 2010; Jones et al., 2015; Moffitt et al., 2011).5 Conversely, externalizing behaviors are associated with later behavioral and academic problems, such as grade retention, school dropout, and lower school engagement (Schindler et al., 2015). Social-emotional skills are especially critical for children and families who experience trauma because of the ways in which such adverse events can impact brain development and affect children’s cognitive and healthy development (see Chapter 2 for more details). For these children and families, those adults, professionals, and programs in both early childhood settings and public schools that provide nurturing and safe environments and bolster self-regulation and social-emotional skills can help mitigate the effects of and build resilience in the face of traumatic experiences (Bartlett et al., 2017). (See Box 7-3 for definitions of key terms.)
How effective are ECE programs in providing such environments? Some reviews of ECE programs have found adverse effects on children’s social behaviors, especially externalizing behaviors (D’Onise et al., 2010). Analyses of data from the ECLS (Loeb et al., 2007; Magnuson et al., 2007) and the NICHD SECCYD (Belsky et al., 2007) found that participation in
___________________
5 Jones and Bouffard define these core skills further: “Emotional processes include emotional knowledge and expression, emotional and behavioral regulation, and empathy and perspective-taking. Social/interpersonal skills include understanding social cues, interpreting others’ behaviors, navigating social situations, interacting positively with peers and adults, and other prosocial behavior. Cognitive regulation includes attention control, inhibiting inappropriate responses, working memory, and cognitive flexibility or set shifting” (Jones and Bouffard, 2012, p. 4).
ECE was associated with more reports of behavior problems, including increased externalizing behaviors and lower self-regulation, but also better cognitive outcomes, such as vocabulary and early reading and math skills. More time in ECE appears to be correlated with more pronounced behavioral issues, and the relationship sometimes persisted beyond kindergarten. See Figure 7-2 for an organizing framework for promoting social-emotional outcomes.
However, studies that examined different kinds of ECE or specific interventions in these programs reveal that ECE and public education can be vehicles for cultivating social-emotional skills and reducing bullying behaviors for older children through effective professional development, coaching, and use of evidence-based curricula. For example, an evaluation of the Chicago School Readiness Program shows that the combination of training in classroom management and job-embedded coaching helped Head Start teachers create more “emotionally and behaviorally supportive classroom environments” and reduced children’s emotional and behavioral challenges and improved their EF skills (Raver, 2012, p. 683). Based on the broader body of research, the evaluators further suggested that results like these may lead to “biobehavioral benefits with health impact,” such as lower cortisol in reaction to stress and lower risk of obesity (Raver, 2012, p. 684).
Another teacher training program implemented in Head Start programs, Incredible Years, produced “small but statistically significant improvements in children’s knowledge of emotions, social problem-solving
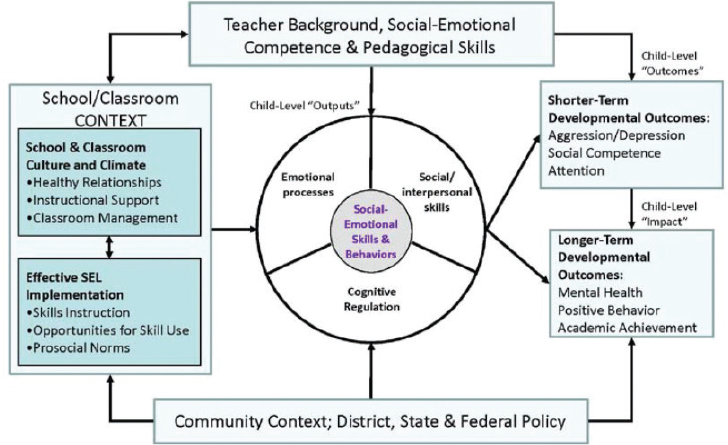
NOTE: Adapted from collaborative work conducted with Celene Domitrovich as part of the Preschool to Elementary School SEL Assessment Workgroup, Collaborative for Academic, Social and Emotional Learning.
SOURCE: Jones and Bouffard, 2012.
skills, and social behaviors” but no impact on children’s problem behaviors or EFs (inhibition, working memory, cognitive flexibility), except among those who were exhibiting the most challenging behaviors at the beginning of the school year (Morris et al., 2014, p. 9 of the executive summary). The Good Behavior Game is a behavior management program for elementary schools, and evaluations show that children who participated in it were less likely to behave disruptively. As young adults, they were also less likely to receive diagnoses of conduct or personality disorders or use mental health services than a control group (NASEM, 2016b).
Other trainings for educators offer more direct support inside the classroom. The Early Childhood Consultation Partnership provides mental health consultation to ECE programs that serve children from birth through age 5 in Connecticut. Consultants work with early childhood educators for 8 weeks, at 4–6 hours per week, to improve the social-emotional environment of the classroom, behavior management strategies, and interactions and support for specific children with social-behavioral challenges. An evaluation using randomized assignment showed that preschoolers whose teachers participated in the intervention were rated as exhibiting less externalizing behaviors, such as hyperactivity, restlessness, and impulsivity (Gilliam et al., 2016a).
Research on curricula designed to improve young children’s social-emotional skills yields generally positive but sometimes mixed findings. For instance, a study of Head Start programs that were randomly assigned to implement Preschool PATHS showed that it had “small to moderate positive impacts on . . . children’s knowledge of emotions, social problem-solving skills, and social behaviors” but no impact on their problem behaviors or EF (Morris et al., 2014, p. 13 of the executive summary). Another RCT of the PATHS curriculum led to high levels of social competence, reduced aggression, and improved print knowledge but only for children who started the year with low levels of EF (Bierman et al., 2008). The researchers followed these children for 1 more year, examining 13 child outcomes at the end of kindergarten. In general, they found a sustained, small to moderate impact on social-emotional skills (as opposed to language and literacy), including enhanced learning engagement, improved social competence, and reduced aggression. The effects were especially strong among children who entered low-achieving schools (Bierman et al., 2014).
Another curriculum, Tools of the Mind, was designed to increase EF in young children—especially preschoolers and kindergarteners. The curriculum relies heavily on play-based learning, and teachers who use it with fidelity spend about 80 percent of each day promoting EF. In a study using randomized assignment, children who experienced the curriculum consistently outperformed those who did not on a variety of EF tasks (Diamond et al., 2007). Other studies showed that the curriculum has greater impact on children who may need more support, such as those who attend high-poverty schools (Blair and Raver, 2014) or have issues with hyperactivity or inattention (Solomon et al., 2017). However, Farran et al. (2015) found that children who participated in the Tools curriculum generally performed no better than those in the control group in EF tasks, and in some cases, the control group children performed better. Importantly, the researchers found that the teachers in the treatment group spent less than half of their class time on activities from the curriculum. In addition, while these teachers generally implemented the activities, how they interacted with children (e.g., time spent on content areas, listening versus talking, positive behavioral reinforcement, scaffolding) was not significantly different than their counterparts in the control group. These findings led the researchers to wonder whether a “reliance on a curriculum to affect child outcomes may be less important than changing interaction patterns in the classroom” (Farran et al., 2015, p. 83).
Looking at older, school-aged children, a meta-analysis of 213 school-based social-emotional learning (SEL) programs showed that “students demonstrated enhanced SEL skills, attitudes, and positive social behaviors following intervention, and also demonstrated fewer conduct problems and
had lower levels of emotional distress” (Durlak et al., 2011, pp. 412–413). For example, Second Step is a violence prevention curriculum aimed at a wider range of children from ages 4 to 14. Through short (20–50-minute) lessons, classroom management support, and parent training, the program has been found to reduce aggressive behaviors (NASEM, 2016b, p. 198).
Across the above interventions, one key ingredient for success appears to be curricula that are intentionally designed to promote targeted skills and strong training and professional development (McClelland et al., 2017; Morris et al., 2014). In addition, when they are effective, they appear to have compensatory effects for those children who live or learn in more challenging or adverse environments. As described earlier, SEL can encompass a range of skills. Effective curricula or interventions are explicit about which specific skills are targeted and have intentionally designed activities or program components that target those skills. In their meta-analysis of 31 studies that focused on externalizing behaviors, Schindler et al. (2015) found that ECE programs that implemented “enhancements” or interventions that target specific social-emotional competencies were more effective at improving children’s behaviors than those that relied on a “global” curriculum that addressed children’s learning and developmental domains comprehensively. Durlak et al. (2011) suggest that effective programs use curricula that are “SAFE”: sequenced (activities that are designed to connect and build on each other to strengthen social-emotional skills), active (instruction based on active learning strategies), focused (curricula designed to support SEL), and explicit (targeting specific social-emotional skills rather than general development in this domain).
Beyond the design of the intervention or curriculum, the support provided to early childhood educators who implement SEL programs also appears to matter. In their study of Head Start programs, Morris et al. (2014) attribute successful interventions to high-quality training followed by opportunities to practice new strategies in the classroom and ongoing support from coaches who provide feedback. Raver (2012) and Gilliam et al. (2016a) also emphasize this level of support for educators. However, Schindler et al. (2015) found that interventions that focused more on improving children’s social-emotional skills directly (e.g., through specific activities or lessons in a curriculum) are more effective than training teachers to use more effective behavioral management strategies: while “the addition of a caregiver behavior management training program enhancement was not associated with significant reductions in externalizing behavior problems” (Schindler et al., 2015, p. 253), the “addition of a child social skills training enhancement . . . resulted in half of a standard deviation reduction in externalizing behavior problems . . . which is nearly twice as large as the effect found in a previous
study for high-quality social and emotional learning programs implemented in primary and secondary schools” (Schindler et al., 2015, p. 257).
That said, as described above, research on early childhood mental health consultation programs may point to a promising way to improve teachers’ performance in the classroom. In a qualitative analysis of six statewide or local early childhood mental health consultation programs, Duran et al. (2009) found that effective programs share three core components:
- A robust infrastructure for implementation, including strong leadership, clear program design, clear organizational structure, effective hiring, training, support and supervision of staff, strong partnerships, evaluation, and funding;
- Highly qualified consultants, defined as having a master’s degree in a mental health field, demonstrating core knowledge and skills, and able to develop strong relationships with colleagues, providers, and families; and
- High-quality and comprehensive services that are child centered and targeted to both classrooms and homes, including referral to services that providers and families may need beyond consultation.
In addition, interventions at the classroom or teacher level are more likely to be effective if they are supported by the leadership and broader culture of the school or ECE program. Effective educators are more able to demonstrate their competencies if they work under supportive leadership and policies (IOM and NRC, 2015). Similarly, in its review of the research on antibullying efforts, which focuses mostly on school-aged children, the National Academies’ Committee on the Biological and Psychosocial Effects of Peer Victimization: Lessons for Bullying Prevention emphasized the importance of implementing interventions across all school contexts (not just the classroom) and involving all school staff (NASEM, 2016b). For example, the playground or the lunch room can be a “hotspot” for aggressive behaviors as well as an opportunity to promote prosocial interactions. (See Box 3-4 in Chapter 3 for this committee’s findings on the effects of bullying in early childhood.)
Finally, it is unclear how critical it is for SEL interventions—whether through a curriculum or consultation—to include a parent education or engagement component. Many programs do so to ensure that the strategies implemented in the classroom are reinforced at home (Duran et al., 2009; McClelland et al., 2017). For example, Fast Track is an intervention for students in grades 1 through 10 that is designed to improve children’s social, cognitive, and problem-solving skills by addressing the “interactions of influences” across the school, the home, and the individual
(NASEM, 2016b, p. 201). Longitudinal RCTs of the program found that participants showed lower incidence of diagnoses of psychiatric or behavioral disorders through high school and “reduced adult psychopathology at age 25 among high-risk early-starting conduct-problem children” (NASEM, 2016b, p. 201). Unfortunately, the evaluation was not able to disaggregate the impact of the parent engagement component.
Other research had ambiguous findings. In one small, quasi-experimental study of the Incredible Years program, Williford and Shelton (2008) found that parents in the intervention group were more likely to report the use of effective parenting skills, but they did not observe a significantly lower or different level of disruptive behavior when compared with those in the control group. The two groups also did not differ in their experience of stress. The researchers posited that more robust and targeted interventions may be needed for families, as opposed to relying on a supplement to a classroom-based or teacher-focused intervention. In their qualitative review, Duran et al. (2009) also found that “engaging parents/caregivers can be difficult because they believe the services are unwarranted, unfamiliar, or stigmatizing, or because various factors impede their ability to actively participate in consultation activities (e.g., transportation, time constraints)” (p. 8 of the executive summary).
Perhaps a better approach to strengthening social-emotional development through ECE is to consider the comprehensive array of cross-sector strategies that meet the needs of children and families. The evidence described above suggests that early childhood educators are more effective at promoting social-emotional development when they have access to effective training and consultation and evidence-based curricula. But even with those supports, ECE programs and educators may lack the capacity to fully provide what children and families need, especially recipients who have experienced trauma, chronic stress, or adverse experiences. ECE programs and teachers may need to partner with other community agencies that provide services, such as screening, referrals, and enrollment in programs outside the ECE sector (e.g., mental health, legal, child welfare) (Caringi et al., 2015). Such an approach would be aligned with the way the National Child Traumatic Stress Network conceives of a “trauma-informed child- and family-services system” (Bartlett et al., 2017, p. 8) (see Box 7-8 in this chapter for more).
An example of such a cross-sector strategy to support the multiple domains of children’s development, especially the environments of school-aged children, is through implementation of full-service schools (Zigler and Finn-Stevenson, 2007). Full-service community schools (FSCSs) focus on “integrat[ing] academic, health, and social supports with youth and community development strategies,” (Biag and Castrechini, 2016, pp. 157–158), which is especially critical for children and families
experiencing multiple challenges. “The goal is to more efficiently use resources to bolster students’ learning, strengthen families, and promote healthy communities” (Biag and Castrechini, 2016, pp. 157–158; Blank et al., 2003). By coordinating services at school (by colocating or other mechanisms), community schools try to address service fragmentation and encourage more communication and collaboration among providers and educators (Biag and Castrechini, 2016). There is mixed evidence relating FSCSs with student outcomes. Using longitudinal data from six high-poverty majority-Latino community schools, Biag and Castrechini (2016) examined how participation in a FSCS influenced students’ educational outcomes. The results indicated that participating in a FSCS that included family engagement opportunities and extended learning programs was associated with modest gains in students’ attendance and achievement in math. In another example of FSCS, Whitehurst and Croft (2010) found that the Harlem Children’s Zone did not produce higher academic gains than some other charter schools not identified as FSCSs. These mixed findings are likely due to the variation in FSCSs and their communities (Sanders, 2016), thus indicating a need for more effectiveness studies. Unfortunately, many of the evaluations on FSCSs to date have focused on academic outcomes, which calls for an intentional focus on health and social-emotional outcomes. See Box 7-4 for an example of a promising model that was designed to close the achievement gap by providing wraparound services for families.
Other school and education reform efforts found to have an effect on children’s learning and behavior are the Comer School Development Program (SDP) and the 21st Century Community Learning Centers (21st CCLC). The Comer SDP was developed by James Comer and the Child Study Center at Yale University in 1968 to improve the educational experiences of low-income ethnic minority children. This model includes three mechanisms (School Planning and Management Team, Student and Staff Support Team, and Parent/Family Team); three operations (Comprehensive School Plan, Staff Development Plan, and monitoring and assessment); and three guiding principles (collaboration, consensus decision making, and no-fault problem solving) (Lunenburg, 2011). SDP is implemented in 1,150 schools across the world. Studies of SDP schools show significant student gains in achievement, attendance, behavior, and overall adjustment (Lunenburg, 2011). It is theorized that the SDP model effect manifests through improvement in school climate, indicated by improved relationships among staff and students, collaboration among staff, and central focus on students (Lunenburg, 2011). Quasi-experimental design studies have shown that students in SDP schools in comparison to students in matched non-SDP schools showed significant gains in achievement, behavior, and overall school adjustment (Haynes
and Comer, 1990a,b). Studies have emphasized the importance of implementation of key components of the SDP to find evidence of effectiveness (Cook et al., 1999; Haynes et al., 1998).
The 21st CCLC program provides students in high-poverty communities across the nation with the opportunity to participate in academic enrichment and youth development programs designed to enhance their well-being (ED, 2010). Programs provide the following activities: academic enrichment learning programs; tutoring; supplemental educational services; homework help; mentoring; recreational activities; career or job training for youth; drug and violence prevention, counseling, and character education programs; expanded library service hours; community service or service-learning programs; and activities that promote youth leadership (ED, 2010). Studies of 21st CLCC have been mixed, with limited significant findings associated with gains in achievement scores and some gains in parental involvement in school and student commitment to work (Durlak and Weissberg, 2013). In their review of after-school programs beyond the 21st CLCC, Durlak and Weissberg (2013) found four evidence-based practices that formed the acronym SAFE: (S) step-by-step training approach, (A) emphasis on active forms of learning through practicing new skills, (F) focused specific time and attention on skill development, and (E) explicitness in defining the skills being promoted. Students who participated in SAFE programs had more positive social behaviors (effect size of 0.29 versus 0.06 for other programs), reduction in problem behaviors (effect size of 0.30 versus 0.08 for other programs), school grades (effect size of 0.22 versus 0.05 for other programs), self-perception (effect size of 0.37 versus 0.13 for other programs), and academic achievement (effect size of 0.20 versus 0.02 for other programs). Thus, there is a need to examine and incorporate these evidence-based approaches in all aspects of learning during the school day or extended day.
Social-Emotional Learning, Trauma-Informed Care, and Suspensions and Expulsions
Suspensions and expulsions in ECE or K–12 settings are often used as a deterrent for misbehavior, which could be due to many factors, including learning disabilities and social-emotional needs in response to trauma, chronic stress, and adverse experiences. “Suspension” is either out-of-school or in-school suspension, which often lasts from 1 to 10 days but varies across states and localities. “Expulsion” is the permanent removal of students from an ECE or school setting. The U.S. Department of Education’s Office for Civil Rights (ED OCR, 2016) found that students with disabilities served by the IDEA (11 percent) are more than twice as likely to receive one or more out-of-school suspensions compared to
students without disabilities (5 percent). More than 1 out of 5 American Indian or Alaska Native (22 percent), Native Hawaiian or other Pacific Islander (23 percent), black (23 percent), and multiracial (25 percent) boys with disabilities served by the IDEA received one or more out-of-school suspensions, compared to 1 out of 10 white (10 percent) boys with disabilities served by the IDEA. Black students are 2.3 times as likely to receive a referral to law enforcement or be subject to a school-related arrest as white students (ED OCR, 2016), emphasizing the need for trauma-informed approaches in schools.
Turning to children in general education, more than 250 preschoolers are suspended or expelled daily (Malik, 2017). Estimates show that as many as 8,710 3- and 4-year-old children may be expelled from or pushed out of their state-funded preschool or pre-K classrooms annually—a rate nearly three times that of students in kindergarten through 12th grade. In child care centers, expulsion rates are 13 times what they are in kindergarten through 12th grade. These rates are particularly pernicious for black children, who are suspended and expelled at much higher rates than their peers. Black preschoolers are 3.6 times more likely to receive one or more suspensions than white preschoolers (Meek and Gilliam, 2016). Black children represent only 19 percent of preschool enrollment but are 47 percent of children receiving one or more out-of-school suspensions; in comparison, white children are 41 percent of preschool enrollment but 28 percent of children receiving one or more out-of-school suspensions (Boyd et al., 2018; Meek and Gilliam, 2016).
Various scholars, and more recently, Gilliam et al. (2016b), suggested that teachers’ implicit bias may be the underlying cause for this “push-out” of black children, especially boys, from these early learning settings as teachers view black children as older and more culpable (Goff et al., 2014). These biased views and attitudes about black children are likely to contribute to children’s disengagement in school. In a meta-analytic study using 53 studies examining the link between suspension and student outcomes, Noltemeyer et al. (2015) found an inverse relationship between suspension and achievement and a positive relationship between suspension and school dropout. Effect sizes ranged from 0.10 for in-school suspension and 0.24 for out-of-school suspension to 0.32 for the effect of suspension on achievement tests. There was an effect size of 0.28 for the effect of suspension on school dropout. Noltemeyer et al. (2015) also found that the percentage of male ethnic minority students and family socioeconomic status (SES) moderated the relationship between suspension and achievement; this was also the case for school dropout. This indicates that the exclusionary practices are not beneficial for students’ achievement and learning process and may heighten risk for children from ethnic and low-SES households. These practices are
especially harmful when they contribute to pushing students of color into the school-to-prison pipeline (see Box 7-5 for more information).
In response to suspension and expulsion, there have been two general approaches for training professionals—trauma-informed care (TIC) and implicit bias training (see the section on supports for the ECE professional for an overview of both approaches to help address suspension and expulsion issues).
Social-Emotional Learning and Dual-Language Learners
Research suggests that children who are bilingual tend to have better self-regulation skills than their monolingual peers (Castro et al., 2013). They have enhanced ability to control their attention and greater EF skills, such as planning, working memory, and cognitive flexibility. Researchers
attribute this advantage to bilingual children’s experiences at paying attention to their environment and other contextual cues to understand when to use one language over another (Castro et al., 2013). A 2017 National Academies report concluded that dual-language learners (DLLs) “who have a strong base in their [home language] and acquire high levels of English proficiency will realize the cognitive, linguistic, social, and cultural benefits of becoming bilingual” (NASEM, 2017b, p. 175). Conversely, DLLs’ loss of proficiency in their home language may also compromise their social-emotional development. For instance, “children who do not develop and maintain proficiency in their home language may lose their ability to communicate with parents and family members and risk becoming estranged from their cultural and linguistic heritage” (NASEM, 2017b, p. 175).
Thus, to strengthen DLLs’ social-emotional health and self-regulation, it is important for ECE and elementary schools to foster their home language skills. Research also shows that when educators implement evidence-based practices that support bilingual development, DLLs’ maintenance of their home language does not come at the cost of their proficiency in English (NASEM, 2017b).
LINKAGES BETWEEN ECE AND HEALTH EQUITY THROUGH PARENTING AND THE HOME ENVIRONMENT
Another crucial pathway through which ECE leads to health equity is the family and home environment (see Chapter 4 for the importance of family cohesion and support). As indicated in the pathway by Hahn et al. (2016), ECE programs support a positive, enriching, and stable home environment through parents’ participation in educational, social, health, and job training opportunities. This pathway can lead to improvement in children’s and families’ cognitive, social, and health outcomes, which then impacts children’s outcomes that lead to higher education attainment and health equity. This pathway is particularly supported by the National Academies report Parenting Matters: Supporting Parents of Children Ages 0–8 (NASEM, 2016a), which emphasized the evidence about strengthening parental knowledge, attitudes, and practices to improve children’s cognitive and social-emotional well-being. Specifically, it found that parental knowledge of child development is positively associated with parent behaviors. Parents with knowledge of evidence-based parenting practices, especially those related to promoting children’s physical health and safety, such as vaccination and use of seat belts, are more likely to engage in those practices.
Ample evidence exists that parental knowledge of how to meet their children’s basic physical (e.g., hunger) and emotional (e.g., wanting to
be held or soothed) needs, as well as of how to read infants’ cues and signals, ensures proper child growth and development (Bowlby, 2008; Chung-Park, 2012; Regalado and Halfon, 2001; Zarnowiecki et al., 2011). Parents’ attitudes about specific practices, such as breastfeeding and engagement in children’s education, were related to parents’ behaviors and use of services. They found strong evidence that the following parenting practices are important to children’s physical health and safety and emotional and behavioral, social, and cognitive competence: (a) contingent responsiveness (“serve and return”)—adult behavior that occurs immediately after a child’s behavior and is related to the child’s focus of attention, such as a parent smiling back at a child; (b) warmth and sensitivity; (c) routines and reduced household chaos; (d) shared book reading and talking to children; (e) practices that promote children’s health and safety—in particular, prenatal care, breastfeeding, vaccination, ensuring adequate nutrition and physical activity, monitoring, and household and vehicle safety; and (e) use of appropriate (less harsh) discipline (McClelland et al., 2017).
The pathway linking ECE to health equity through supporting responsive parenting and a quality home environment is generally supported by many programs, including the three foundational early childhood programs, each of which included a significant family engagement component—the HighScope PPP, focused on 3- and 4-year olds, the Carolina ABC Study, focused on children birth to age 3, and the Chicago Child-Parent Centers (CPCs) (see Box 7-6). While these studies are quite old, focused on particular populations (i.e., African Americans), and specific to local areas, in addition to being unable to disentangle the impact of teacher practices compared to family engagement practices, they provide long-term and intergenerational evidence of the importance of engaging with families while also providing high-quality learning experiences in classrooms. Other early childhood programs, including home visiting programs that serve mothers prenatally and last until the children are 3 years old and family engagement programs for preschool- and school-age children, provide additional support for the links between ECE and healthy equity through parenting.
Family Engagement Programs
The focus on family engagement has been bolstered by the recent federal funds for parent and family community engagement centers (U.S. Department of Education [ED] Statewide Family Engagement Center Program through the Consolidated Appropriations Act of 2018). As reviewed in the Parenting Matters report, some ECE programs “provide full- or part-time classroom-based services (center or family child care) for children
from birth to age five” that “often include parenting education and other services for families (sometimes starting prenatally)” (NASEM, 2016a, p. 159). To address the overall conditions of families, these programs are designed to improve parenting knowledge, attitudes, and practices with the goal of supporting children’s cognitive and social-emotional development and success in school (Brooks-Gunn et al., 2000; Chase-Lansdale and Brooks-Gunn, 2014; Fantuzzo et al., 2013). These parent-focused programs have several different structures. For example, some include parent supports (and parent self-sufficiency support) as well as intensive classroom-based services for children that are multipronged. Others offer services that are primarily classroom-based with either some parenting education services or some parent self-sufficiency services (NASEM, 2016a).
In their examination of the impact of Head Start on child outcomes through parenting, Puma et al. (2012) did not find significant differences on parenting-related measures, included disciplinary practices, educational supports, parenting styles, parent participation in and communication with the school, and parent and child time together (NASEM, 2016a). With respect to Early Head Start, there was some evidence that programs that were mixed delivery (center and home) had favorable and consistent impact on parenting outcomes, including sensitive parenting and language-rich environments.
Other school-based parent engagement programs have been found to be effective for children’s outcomes. For example, the Companion Curriculum uses Head Start teachers to encourage parents’ participation in the classroom and provides workshops and activity spaces in the classroom that focus on training parents to engage in parent–child learning activities (Mendez, 2010; NASEM, 2016a). There were no benefits for parents, but there was significant improvement in children’s vocabulary in a quasi-experimental study (Mendez, 2010). Another example is documented in the Parenting Matters report (NASEM, 2016a, p. 163):
The Kids in Transition to School (KITS) Program is a short-term, targeted, evidence-based intervention aimed at increasing early literacy, social skills, and self-regulatory skills among children who are at high risk for school difficulties. This program provides a 24-session readiness group for children that promotes social-emotional skills and early literacy as well as a 12-session parent workshop focused on promoting parent involvement in early literacy and the use of positive parenting practices. In a pilot efficacy trial with 39 families, Pears and colleagues found that children in families who received the KITS intervention demonstrated early literacy and social skill improvements as compared with their peers who did not receive the intervention (Pears et al., 2014). In randomized controlled studies, foster children who received the intervention exhibited improvements in social competence, self-regulation skills, and early literacy skills. (Pears et al., 2007, 2012, 2013)
Two-generational model programs, such as Head Start, Project Redirection, New Chance demonstration, Ohio’s Learning and Earning Program, Teen Parent Demonstration, and the Comprehensive Child Development Program from the 1980s and 1990s, offered mothers a wide range of services, including parenting classes, job training, mandatory schooling, and child care (Granger and Cytron, 1999; NASEM, 2016a; Polit, 1989). Many of these programs have not resulted in significant positive outcomes, at least based on older versions of the models (NASEM, 2016a). The new iterations of two-generation models focus
on the education benefits to children of high-quality ECE programs and higher parental levels of education and labor force motivation. Parenting knowledge, attitudes, and practices may be improved, but the improvement comes indirectly through higher parental job skills and education and reduced household stress rather than explicit programming directed at parenting skills. (NASEM, 2016a, p. 166)
Examples of these new iterations that have evaluations planned or under way are the CareerAdvance Community Action Project of Tulsa, Oklahoma; The Annie E. Casey Foundation Atlanta Partnership; and the Housing Opportunity and Services Together project (NASEM, 2016a; see Chase-Lansdale and Brooks-Gunn, 2014, for others).
There are also other family-focused interventions for school-age children. In one example, the ParentCorps program, parent groups (see Box 7-7; also documented in NASEM, 2016a)—“co-facilitated by teachers and mental health professionals with expertise in behavior management—are used to help parents establish structure and routines for children, teach positive parenting practices (e.g., positive reinforcement and consistent consequences), and provide opportunities for facilitator-observed parent–child interactions” (NASEM, 2016a, p. 171). In addition to reduced behavior problems among children in the treatment group, parents displayed more effective parenting practices than in the control group. Parents in the treatment group reported using more effective disciplinary practices and receiving higher scores on tests of knowledge of effective behavior management strategies; in addition, higher-quality parenting was observed for parent–child interactions by the research team (Brotman et al., 2011).
As documented in the Parenting Matters report (NASEM, 2016a), Getting Ready is an evidence-supported intervention that targets parents’ decision-making role at school (Sheridan et al., 2010). The program includes parent–teacher conferences, monthly family socialization, and teacher home visits with parents using structured interactions. The goal is to actively engage parents in learning and behavior goal setting and decision making. “Together, teachers and parents identify learning opportunities at home and school and plan how educators and parents can complement each other’s efforts to promote learning and track children’s growth. Priorities include affirming parents’ competence, increasing their access to information on child development, and reinforcing positive parenting practices” (Knoche et al., 2012; NASEM, 2016a, pp. 171–172). Knoche et al. (2012) identified treatment effects for parental warmth and sensitivity, learning support, and autonomy support. Sheridan et al. (2014) found that, relative to children in the control group, children in the Getting Ready intervention had a significantly greater decline in disruptive behaviors such as difficulty standing still and tendency to run around; however, no differences were seen for other learning-related behaviors. Children’s language and literacy were also improved, and one study found some evidence that the program’s effects on achievement were greatest for children at highest risk for underachievement (that is, those children whose parents have less than a high school education and those who did not speak English prior to treatment) (Sheridan et al., 2011). Thus, there is some evidence that schools’ partnership and engagement with parents through specific and structured approaches are related to improved parenting and child academic and behavioral outcomes; unexpectedly, these outcomes seem stronger in older age groups. However, caution is warranted because these are not national studies and, in many instances, are localized and researcher controlled, unlike the Head Start and Early Head Start studies.
Home Visiting Programs
One particular early childhood program focused on supporting parents and enhancing positive parenting and reducing/preventing child abuse and maltreatment is home visiting (see Chapter 4 for additional background on home visiting, including health impacts and a committee recommendation). Home visiting (which targets families with pregnant women and children from birth through age 5—though most attend until children are 3 years old) has been found to increase parental knowledge and practices and reduce parental stress and depression while also supporting child health and reducing maltreatment. The general short-term outcomes of home visiting programs include (1) decreasing parent stress, depression, and isolation; (2) increasing family self-sufficiency; (3) enhancing parenting knowledge of child development; (4) increasing self-efficacy in the parenting role; (5) healthier parent–child relationships and interactions; (6) increasing positive guidance and decreasing harsh punishment; and (7) supporting children’s learning. The long-term outcome is to enhance children’s well-being, social competence, and school readiness.
Based on strict criteria for what counted as evidence and a systematic review of that evidence (adapted in part from ED’s What Works Clearinghouse),6 the U.S. Department of Health and Human Services’ (HHS’s) Home Visiting Evidence of Effectiveness identified many effective models that impact various outcomes, including positive parenting practices, family economic self-sufficiency, child health, child development and school readiness, and reductions in child maltreatment. Regarding positive parent practices, the review shows that
while many individual evaluations of home visiting programs have shown impacts on parenting practices tied to positive developmental outcomes, the average impacts of home visiting on parenting practices are not large. Nor is there a strong pattern of effects on parenting practices across evaluation studies and home visiting models. (NASEM, 2016a, p. 151)
None of the home visiting models were linked to reductions in juvenile delinquency, family violence, and crime. Healthy Families America, however, had one or more favorable impacts in each of the eight domains, and Nurse-Family Partnership had favorable impacts in seven domains, followed by Early Head Start—Home Visiting with favorable impacts in five domains. See the Parenting Matters report for synthesis of home visiting and various models, and the Home Visiting Evidence for Effectiveness website by HHS’s Administration for Children and Families for
___________________
6 For more information, see Institute of Education Sciences. n.d. What Works Clearinghouse. Find What Works. https://ies.ed.gov/ncee/wwc/FWW (accessed July 15, 2019).
a recent examination of all home visiting models.7 These findings are consistent with the 2019 results from the Mother and Infant Home Visiting Program Evaluation (MIHOPE) and MIHOPE–Strong Start Studies of Evidence-Based Home Visiting, namely, that MIHOPE found positive effects on some family outcomes (e.g., home environment) but MIHOPE–Strong Start found little effect on birth outcomes and prenatal behaviors (Michalopoulos et al., 2019).
In summary, there is some evidence linking family engagement, including home visiting and support, to children’s health and well-being. While it is challenging to disentangle family engagement and support from ECE classroom practices, there is indication that supporting family functioning and processes and providing resources and strategies will likely lead to better outcomes for parents themselves and their children, resulting in health equity. Current evidence indicates the importance of tailoring services and programs to meet the needs of individual families and ensuring that families and children with the greatest needs are engaged throughout the duration of the program/services. With new approaches to family engagement and support, such as the Two Gen 2.0 models, more actionable evidence is emerging about how best to support children and their families in the early years.
LINKAGES BETWEEN ECE AND HEALTH EQUITY THROUGH SUPPORTS FOR THE ECE PROFESSIONAL
The salutary effects that ECE can have on the physical, mental, and social-emotional health of children—whether through the inclusion of comprehensive services, evidence-based curriculum, high-quality professional development and supports, or effective family engagement—can be disrupted if the ECE professionals themselves are not trained or supported to implement best practices or navigate systems of services for children and families outside the ECE sector. Since the release of the National Academies report Transforming the Workforce for Children Birth Through Age 8: A Unifying Foundation (IOM and NRC, 2015), there has been increased interest from funders, policy makers, and advocates in overhauling the professional preparation and ongoing supports for early childhood educators so that these experiences—and the policies and funding that shape them—better reflect the science of early development.8 For example, states
___________________
7 For more information, see U.S. Department of Health and Human Services. n.d. Home Visiting Evidence of Effectiveness. See https://homvee.acf.hhs.gov (accessed June 14, 2019).
8 See initiatives from national organizations, such as Power to the Profession, National Governors Association, and Council of Chief State School Officers, and state-led initiatives, such as in Colorado, Minnesota, and Nebraska.
and national organizations have developed statements of core professional competencies that inform the training of these educators. The report found that, in most cases, these statements need to be updated to follow recent developments in science and research. Some of these areas are especially relevant to promoting young children’s health and well-being, such as knowledge and skills related to working effectively with children who have experienced chronic stress, trauma, and adversity; collaboration with professionals in ECE or the education sector; promotion of self-regulation and related EFs; and support for DLLs. Incorporating these issues into efforts to improve policies, systems, and programs that prepare and support early childhood educators is critical to maximizing the potential of ECE programs to improve health outcomes and equity. For example, teachers, especially those who work with students who experience trauma, can be more effective if they receive more training and education on mental health issues and skills to access relevant services from that sector (Hydon et al., 2015).
Training and supports for early childhood educators are needed to help them adjust their practice to acknowledge their own biases and their understanding that children’s behavioral challenges and learning difficulties are often due to the toxic stress response and undiagnosed and untreated trauma (Matthews et al., 2018; Ramirez et al., 2012). It is important to note that these trainings are critical for supporting children’s learning and healthy development beyond addressing suspension and expulsion. Whether or not children are suspended or expelled, many are exposed to traumatic experiences, including abuse and neglect, family and media violence, community or school violence, loss of a parent, parents dealing with substance abuse, and mental or other health challenges. In turn, children who experience trauma can exhibit behaviors in ECE programs and schools that may indicate social-emotional challenges. Box 7-8 describes a trauma-informed service system for children and families.
Trauma-Informed Care or Practices
TIC is defined as a “recognition of the pervasiveness of trauma and a commitment to identify and address it early . . . [and it] involves seeking to understand the connection between presenting symptoms and behaviors and the individual’s past trauma history” (Hodas, 2006, p. 5) (see Box 7-9 for more information). TIC can be provided in multiple settings by trained, committed professionals who understand the principles of a TIC system, including
- trauma and how it may impact children’s identity, how they will view the world, and coping mechanisms;
- children and their contexts, including their family and community contexts, and supporting children to be active in their healing process;
- services that are strengths based and promote children’s self-control and coping skills; and
- the service relationship, which is based on relationships and trust that is earned over time.
There is emerging evidence about the impact of TIC and trauma-informed practices (TIPs) for children’s outcomes and well-being. For example, Zakszeski et al. (2017) conducted a review to describe the implementation and evaluation of trauma-focused school practices. They found that most approaches used Cognitive Behavioral Intervention for Trauma in Schools, followed by drama instruction, eye movement desensitization and reprocessing training, coping/social skill instruction, and comprehensive, multitiered systems. Zakszeski et al. (2017) found that most of the studies reported positive treatment outcomes, especially reduction in symptoms of trauma and internalizing problems, but effect sizes were not included to determine magnitude. The limitation of the studies in this review was that most occurred with subpopulations of children rather than across the student population. There has been a call for more rigorous study and review of TIC and TIP beyond their implementation (Bryson et al., 2017). See Box 7-10 for an example of a promising model that employs a cognitive behavioral intervention to address trauma in schools.
Implicit Bias Training
Implicit biases are unconscious and involuntary attitudes that can influence one’s affect, behavior, and cognitive processes (Boysen, 2010). It has been suggested that implicit bias is one reason for the disproportionality of suspension and expulsion rates for black children and children with special needs. That is, educators may see the normative behaviors of black children in particular as dangerous and aggressive, even when there is no evidence of misbehavior (Gilliam et al., 2016b). Implicit bias training may be a potential strategy to counter these unconscious biases. Evidence is emerging on the impact of implicit bias training, mostly from the public health and nursing sectors. One core feature of implicit bias training is cultural competence, which “is the process and ability of an individual or organization to function effectively within different cultural situations” (Betancourt et al., 2003; Cross et al., 1989; Gallagher and Polanin, 2015, p. 333); it “combines a set of congruent behaviors with attitudes and knowledge that facilitate an individual or a system to work successfully in various cultural contexts other than their own culture” (Gallagher and Polanin, 2015, p. 333). See Box 7-11 for more information on the importance of cultural competence and sensitivity in ECE.
Scholars caution about the focus on cultural competence without antiracist training. A literature review by Allen (2010) indicates that cultural competence training could be strengthened by antiracist training to adequately ensure that professionals are able to
challenge discrimination experienced by minority cultural groups, such as ethnocentrism, cultural biases, and overt and covert discrimination
due to racial difference . . . [and cultural competence training may limit] culture to a static entity and reduces understanding of peoples’ behavior to prescribed cultural norms. This promotes cultural stereotyping with the risk of discrimination and it fails to account for individual and family differences within cultural groups. (Allen, 2010, p. 315)
However, there is an absence of a validated antiracist training and intervention.
Other options to address unconscious bias are mindfulness training and prejudice habit breaking. It is theorized that mindfulness training could reduce implicit bias by (1) deactivating the “prejudice network,” which involves the activation of the amygdala (or threat responses) and reduces the ventromedial prefrontal cortex (or the empathy and “humanizing” pathway) (Burgess et al., 2017); (2) meditating to increase one’s ability to become aware of implicit biases, once they are activated, and to engage in self-regulatory processes to behave in less discriminatory and prejudicial ways; (3) reducing stress and internal sources of cognitive load that contribute to the activation and application of implicit biases; (4) activating empathy and compassion, which reduce the activation and application of implicit bias and promote willingness to engage with members of stigmatized groups; and (5) improving one’s ability to communicate and focus on the other person’s individual characteristics rather than their group membership. While Burgess et al. (2017) provide a strong rationale for mindfulness as a strategy to address implicit bias, there is a need for systematic implementation and examination in this area. It should also be noted that in order to maximize mindfulness, it is imperative for individuals to recognize their own implicit bias, any privilege that comes with their social status, and unintentional microaggressions (i.e., “brief and commonplace daily verbal, behavioral, or environmental indignities, whether intentional or unintentional, that communicate negative slights and insults”) (Godsil et al., 2014; Sue et al., 2007).
Devine’s prejudice habit-breaking framework argues that implicit biases are deeply entrenched habits developed through socialization experiences (Devine et al., 2012). “Breaking the habit” of implicit bias therefore requires learning about the contexts that activate the bias and how to replace the biased responses with responses that reflect one’s nonprejudiced goals. Thus, when people who are opposed to prejudice believe they have acted with bias, they will seek out information to help them break this habit of prejudice or bias. That training includes (1) stereotype replacement (recognizing stereotypic responses within oneself and society), (2) counter-stereotypic imaging (imagining examples of outgroup members who counter popularly held stereotypes), (3) individuating (viewing others according to their personal rather than stereotypic characteristics), (4) perspective taking (adopting the perspective of a member of the stigmatized group), and (5) contact (increasing exposure to outgroup members). In an RCT, Devine et al. (2012) showed that participants in an 8-week habit-breaking training showed significant decrease in their explicit bias but also became more acutely aware of discrimination in society. This study was conducted with introductory graduate students
who were likely biased in their willingness to participate. There is a need for more rigorous examination of this training approach with educational professionals and those caring for and teaching young children.
Supporting ECE Workforce Well-Being
In addition, even the most competent early childhood educators will not be effective if they are not physically, mentally, and social-emotionally healthy. Educators who have strong social-emotional awareness and skills are more likely to develop close, constructive relationships with children, implement SEL programs effectively, and be more able to create a positive classroom climate. Conversely, educators who are stressed, depressed, or have low social-emotional skills are more likely to be less sensitive and warm toward children and have more conflictual relationships with them. Since children who live in high-stress communities or with adverse conditions benefit the most from warm, enriching interactions with adults, it is critically important for them to be in ECE programs in which the educators are social-emotionally healthy and strong (Becker et al., 2017; IOM and NRC, 2015; Jones and Bouffard, 2012; Roberts et al., 2019; Whitaker et al., 2015). Indeed, McClelland et al. (2017) found that effective social-emotional interventions often include building teachers’ own social-emotional skills, as well as children’s.
Unfortunately, it has been well documented that compared to other fields, the ECE workforce experiences a high level of stress and depression; one reason is the stress of low compensation and benefits (see IOM and NRC, 2015). Most of them (53 percent) participate in at least one of four public support or health care programs for low-income individuals, compared to 21 percent of the U.S. workforce in general (Whitebook et al., 2018). On average, child care teachers earn less than $11 per hour, or about $22,000 per year—barely over the federal poverty guidelines for a family of three. There is also emerging evidence (Borntrager et al., 2012; Hydon et al., 2015) that when educators work with children who experience trauma and significant adverse experiences, whether in ECE programs or public schools, they can experience “secondary traumatic stress” (STS), or “the natural consequent behaviors and emotions resulting from knowing about a traumatizing event experienced by a significant other—the stress resulting from helping or wanting to help a traumatized or suffering person” (Hydon et al., 2015, p. 320).
Which supports or interventions can help educators manage or mitigate their general social-emotional health and their experience of stress, depression, or STS? For early childhood educators, an analysis of the National Survey of Early Care and Education found that “informal workforce supports” that help teachers feel that they are a part of a team and
respected as professionals were related to lower stress. Studies of public school teachers by Borntrager et al. (2012) and Caringi et al. (2015) similarly found that working in schools that provided or encouraged peer support was associated with lower STS. In addition, stable classroom assignments were related to lower stress, as was (unsurprisingly) higher pay. Teachers with higher household incomes (more than $45,000 per year) experienced less stress than those earning less (Madill et al., 2018). In another analysis, Roberts et al. (2019) found that early childhood educators who had no health insurance, received high professional demands with few work-related resources, and had multiple jobs were more likely to have depressive symptoms. Interestingly, Madill et al. (2018) found that more formal professional supports, such as small group size and access to professional development or coaching, were not related to early childhood educators’ experience of stress.
There is emerging evidence that professional support that is targeted to improve the mental and social-emotional well-being of educators could be helpful. In their small, qualitative study, Caringi et al. (2015) reported that teachers’ practice of “self-care” techniques helped them manage their stress. In her small study of educators and caregivers in a residential program for AIDS-affected children and youth, Lucas (2007) found that training on “reframing” and realistic goal setting with children and parents led to a decrease in emotional exhaustion. (Reframing has teachers identify children’s and families’ strengths and assets rather than their faults, which helps teachers approach problems and obstacles collaboratively with those they serve rather than treating these as issues they need to “fix” on their own.)
Another promising type of intervention is to improve “dispositional mindfulness” (Becker et al., 2017; Hydon et al., 2015). Mindfulness is related to the ability to regulate one’s emotions, thoughts, and attention. People who are mindful are more aware of their thoughts, feelings, and reactions to their surroundings and better able to refrain from judgment, which enables them to react more calmly to a given situation and to better understand others’ perspectives and behaviors before responding. In one study based on a survey of 1,001 Head Start teachers, those who were more mindful had closer relationships with children and less conflict with them, partly because mindfulness is also associated with fewer depressive symptoms.
A mindful disposition may help teachers view challenging interactions with more equanimity. Alternatively, mindful teachers may have fewer challenging interactions. Their attention and focus may help them to be proactive in their guidance of young children, structuring the classroom for successful interactions and diffusing potentially difficult situations before they begin. . . . Teachers who are more mindful may be better able
to disengage from depressive or ruminative thoughts, and experience fewer difficult exchanges with children. Additionally, a mindful disposition may help teachers appraise stressors differently, such that children’s difficult behavior may not be perceived as a threat. Mindful teachers may be aware of situations that may elicit challenging behavior, and take action to engage in reappraisal to regulate their emotional response. (Becker et al., 2017, p. 48)
One program, called Cultivating Awareness and Resilience in Education (CARE), has demonstrated impact on teachers’ mindfulness. CARE provides 30 hours of training in group-based settings and individual sessions with trainers. The program includes “emotion skills instruction, mindfulness practices, and compassion-building activities” (Becker et al., 2017, p. 49). RCTs with elementary teachers showed improvements in their mindfulness and emotional regulation. In one of those studies, researchers also observed improvements in teachers’ emotional support for students (Becker et al., 2017).
This study also indicated that for programs of this nature to be viable and sustainable, school leaders’ buy-in is necessary. Strong leadership is influential in early childhood educators’ professional support systems (IOM and NRC, 2015). While local program administrators and leaders may not be able to improve educators’ professional preparation programs, compensation levels, or benefit packages on their own, they are critical to establishing an organization and environment that supports their staff’s mental health and minimizes stress—whether through opportunities for them to collaborate or appreciate each other’s work, training on topics such as TIC, or self-care interventions, like mindfulness training.
ECE CONCLUSIONS AND RECOMMENDATIONS
Below, the committee provides conclusions and recommendations, based on the information reviewed in this chapter, to ensure adequate resources for ECE programs and educators, support and improve competencies for the ECE workforce, and improve access to ECE for eligible children. The goal of these recommendations is to advance the ECE system to promote health equity during the early childhood period to set the course for good health and well-being into adulthood.
Allocation of Adequate Resources to Support Health-Promoting ECE Programs and Educators
ECE programs, including systems that support and ensure standards for high quality (e.g., QRISs), can be comprehensive platforms for ensuring all children are healthy and prepared for school and life. That can
only occur if these programs and systems adopt specific practices and processes that have been shown to have such impacts and set a threshold that ensures all participating programs are sufficiently high quality, as opposed to more general benchmarks related to quality (e.g., teacher education levels, class size, professional development). Furthermore, current funding levels for child care, pre-K, and Head Start generally are not based on systematic estimates of the cost of quality, including those elements that promote better health outcomes. It is also critical to consider the cost of funding programs to ensure that they reach all eligible children. Until that has been remedied, our nation will not maximize the potential of ECE programs to promote the health and school readiness of young children, especially those who tend to fall on the wrong side of the health equity equation (e.g., low-income children and children of color).
For ECE to be part of a system that ensures children are healthy and ready for school and life, these programs need
- Adequate resources to support the “whole child,” including cognitive, emotional, social, and physical development, regardless of setting (e.g., home, center, or school). This includes adequately supporting programs’ implementation of standards and content that are health promoting (e.g., high-quality nutrition and physical activity) for child, family, and staff outcomes, ensuring children’s access to effective early intervention and special education services, and tailoring specific resources and supports for various settings and providers (e.g., home-based providers);
- The ability to implement the recommendation from the National Academies reports Transforming the Workforce for Children Birth Through Age 8: A Unifying Foundation (IOM and NRC, 2015) and Transforming the Financing of Early Care and Education (NASEM, 2018) addressing the level of compensation and access to basic benefits (such as health care and housing); ensuring work environments and conditions that respect the demands of the ECE profession, including adequate resources and opportunities for teamwork (e.g., planning time, substitutes); offering ongoing training to maintain educators’ own emotional well-being; and developing school and program leaders’ knowledge and competencies in creating an organizational culture that supports the social-emotional health and well-being of children, families, and educators;
- The capacity (funding, staffing, skill sets) to provide or make referrals (and follow-up) to various agencies or integrated
- partnerships with professionals from various sectors or organizations (e.g., home visitors, social workers, health services) that meet the various needs of children and their families;
- An SEL component that has the following characteristics:
- Strong training and support (e.g., job-embedded coaching, early childhood mental health consultants) for educators on specific SEL skills;
- Curricula intentionally designed to build specific SEL skills through sequenced and active learning experiences;
- Promotion of a supportive organizational culture and climate by engaging the involvement of the leaders, paraprofessionals, and other staff of the school or ECE program; and
- Supports for the social-emotional health of parents and early childhood professionals and staff, including leaders.
- Educators who are well trained and well supported to develop critical professional competencies and support children’s social, emotional, and physical health. Educators need to develop specialized skills that ensure children are healthy and prepared for school. In order for them to use these skills effectively, their own physical, emotional, and mental health needs to be supported; and
- Adequate resources and support to systematically identify factors that support or hinder integration at the federal, state, and local levels, as well as the impact of this effort for children, families, and communities.
- public–private partnerships) that have decision-making power over ECE programs should establish program standards and accountability systems, such as a quality rating and improvement system, linked with better school readiness and health outcomes and provide adequate funding and resources to implement and sustain these standards effectively.
- The Office of Child Care and the Office of Head Start at the federal level, along with state, local, tribal, and territorial early care and other education agencies, should assess the full cost of implementing standards that promote health outcomes and equity as described above, including supporting educators’ own health and well-being, and work with Congress to align funding levels of the major federal ECE programs—child care subsidy and Head Start—accordingly.
- Health and human service entities, the federal Early Learning Interagency Policy Board, state Early Childhood Advisory Councils, and federal, state, local, tribal, and territorial agencies that oversee home visiting and ECE programs should ensure greater programmatic coordination and policy alignment to ensure effective allocation of resources.
- The Office of Planning, Research & Evaluation in the Administration for Children and Families, along with the U.S. Department of Education, should examine the feasibility and seek resources to conduct (a) an implementation study to examine the design and implementation of this comprehensive ECE approach that incorporates health standards and (b) an outcomes study that examines the impact on children’s school readiness and achievement, and health outcomes, with particular attention to eliminating disparities and gaps prior to school entry.
Health-Focused Competencies of the Workforce
The ECE workforce and other professionals are critical in implementing evidence-based practices in ECE settings that support children’s wellbeing, leading to health equity. However, there is a need for systems and supports to strengthen their competencies and skills, as well as stability, in supporting health-promoting and health equity practices.
Specific areas include
- Strengthening professionals’ understanding of and capacity to collaborate with professionals from other sectors, such as health and social work (interprofessional learnings);
- Implementing practices and policies based on the understanding of the link between biology and children’s learning and development and impact on children’s readiness for school and school success;
- Educating professionals about unconscious biases and practices that undermine the learning and social-emotional health of diverse children and their families;
- Training and coaching on effective antibias and culturally responsive practices that strengthen professionals’ effectiveness in supporting the learning, social-emotional health, and well-being of diverse children and families (including DLLs); and
- Effectively implementing practices and policies informed by understanding of trauma, adverse childhood experiences, toxic stress, and racism.
Access and Affordability
Children who experience comprehensive high-quality ECE early in life and for multiple years are likely to show stronger cognitive, academic, and social-emotional outcomes over time. Unfortunately, many children who could benefit the most from ECE are less likely, for various reasons, to
access these high-quality ECE environments early and for longer periods. To ensure health promotion and health equity in the early years, there is a need to ensure that these programs are available to and affordable for families as early as possible and as long as possible.
The strategic plan should be modeled after and build on the relevant performance standards of Early Head Start and Head Start, which emphasize mixed settings, the whole child, family and community engagement, transition between home and school, and continuous quality improvement. It should also strengthen the program components discussed in
this chapter that lead to stronger school readiness and health outcomes, including mitigating the impact of adverse experiences and toxic stress for children, families, teachers, and staff. Critical components include a comprehensive social-emotional strategy that encompasses both the classroom (curriculum, teacher training, and support) and program or school (leadership, culture, and climate) levels and educators who have the competencies described in Recommendation 7-2. The plan should identify strategies to bolster capacity and resources of new and existing programs to implement these more ambitious standards, including by incentivizing collaboration among Head Start, pre-K, and child care programs. Implementation of this plan will likely require funding from Congress.
A national evaluation led by the Office of Head Start, Office of Child Care, Office of the Assistant Secretary for Planning and Evaluation, and Office of Planning, Research & Evaluation in the Administration for Children and Families is needed to examine and inform the design, implementation, and effect of this expanded access and strengthening of Early Head Start and Head Start to enhance children’s school readiness and achievement and health outcomes.
Heeding the findings from the Head Start Impact Study that program implementation and workforce challenges vary widely from site to site, which leads to variable outcomes (Phillips et al., 2017), the improvement and scale-up strategy described in this recommendation should include mechanisms that help new providers incorporate program features and conditions that are associated with stronger outcomes. For example, an evaluation can provide rapid-cycle feedback (see Chapter 8 for more) to ensure faithful implementation of the “upgraded” program model and fidelity and to inform ongoing midcourse corrections as needed to reach targeted health outcomes. This study will help to identify factors that supported or hindered expansion and access at the federal, state, and local levels, as well as the impact of this effort for children, families, and communities.
State policy makers (e.g., governors, legislators, agency leaders, pre-K administrators) should also consider how pre-K funding and policies can support the program and workforce characteristics discussed in this chapter that are associated with health outcomes. State pre-K programs are highly variable, and some will be better positioned to serve as a platform for promoting health equity than others. In the final analysis, the committee believes that among the major publicly funded ECE programs, Head Start’s history, program design, quality standards, targeted populations, and evidence base make a useful platform from which to build expanded access to comprehensive high-quality ECE programs. Health promotion (including social-emotional health) and family engagement are already important goals of the program that can be strengthened based on evidence from this report. The program’s historical focus on children furthest
from opportunity can help address inequities among different racial and income groups. With an intentional effort to bolster its health-promoting strategies, provide adequate resources for educators and leaders to implement them effectively, and expand access to all eligible children, Head Start can be a critical element of our nation’s cross-sector approach to improving child health and reducing inequities.
CONCLUSION
The ECE system is a critical setting to provide young children with a strong foundation for skill building and positive learning, as well as shaping social-emotional, cognitive, and physical health. This chapter delves into the evidence on ECE programs and childhood outcomes with respect to the many different service settings (e.g., home-, school-, and center-based care). In addition, the committee highlights salient issues and populations related to health equity throughout the chapter, such as early intervention for children with developmental disabilities, DLLs, and implicit bias training for educators. Based on its review of the evidence and committee expertise, the committee applies the evidence to provide recommendations in the areas of allocating adequate resources to support ECE programs and educators, supporting and training the workforce, and improving access to quality ECE for eligible children. By targeting these key areas that are instrumental to an effective and equitable system, the committee identifies a comprehensive approach to leveraging and enhancing the current ECE system to promote health equity. The following chapter integrates the crosscutting themes from the report and applies them to inform a systems approach to promote equitable prenatal and childhood development.
REFERENCES
Advocacy Institute. 2019. National Assessment of Educational Progress (NAEP). http://www.advocacyinstitute.org/NAEP/NationPerformance2013-15-17.shtml (accessed April 2, 2019).
Allen, J. 2010. Improving cross-cultural care and antiracism in nursing education: A literature review. Nurse Education Today 30(4):314–320.
Ansari, A., and A. Winsler. 2012. School readiness among low-income, Latino children attending family childcare versus centre-based care. Early Child Development and Care 182(11):1465–1485.
APA (American Psychiatric Association). 2013. Diagnostic and statistical manual, 5th ed. Washington, DC: American Psychiatric Association.
Barnett, W. S. 2013. Getting the facts right on pre-K and the president’s pre-K proposal. New Brunswick, NJ: National Institute for Early Education Research.
Barnett, W. S., and A. H. Friedman-Krauss. 2016. State(s) of Head Start. New Brunswick, NJ: National Institute for Early Education Research.
Bartlett, J. D., S. Smith, and E. Bringewatt. 2017. Helping young children who have experienced trauma: Policies and strategies for early care and education. Publication #2017-19. Bethesda, MD: Child Trends.
Becker, B. D., K. C. Gallagher, and R. C. Whitaker. 2017. Teachers’ dispositional mindfulness and the quality of their relationships with children in Head Start classrooms. Journal of School Psychology 65:40–53.
Belfield, C. R., and I. R. Kelly. 2013. Early education and health outcomes of a 2001 U.S. birth cohort. Economics & Human Biology 11(3):310–325.
Belsky, J., D. L. Vandell, M. Burchinal, K. A. Clarke-Stewart, K. McCartney, and M. T. Owen. 2007. Are there long-term effects of early child care? Child Development 78(2):681–701.
Betancourt, J. R., A. R. Green, J. E. Carrillo, and O. Ananeh-Firempong, 2nd. 2003. Defining cultural competence: A practical framework for addressing racial/ethnic disparities in health and health care. Public Health Reports 118(4):293–302.
Biag, M., and S. Castrechini. 2016. Coordinated strategies to help the whole child: Examining the contributions of full-service community schools. Journal of Education for Students Placed at Risk 21(3):157–173.
Bierman, K. L., R. L. Nix, M. T. Greenberg, C. Blair, and C. E. Domitrovich. 2008. Executive functions and school readiness intervention: Impact, moderation, and mediation in the Head Start REDI program. Development and Psychopathology 20(3):821–843.
Bierman, K. L., R. L. Nix, B. S. Heinrichs, C. E. Domitrovich, S. D. Gest, J. A. Welsh, and S. Gill. 2014. Effects of Head Start REDI on children’s outcomes 1 year later in different kindergarten contexts. Child Development 85(1):140–159.
Blackorby, J., and M. Wagner. 1996. Longitudinal postschool outcomes of youth with disabilities: Findings from the National Longitudinal Transition Study. Exceptional Children 62(5):399–413.
Blair, C., and C. C. Raver. 2014. Closing the achievement gap through modification of neurocognitive and neuroendocrine function: Results from a cluster randomized controlled trial of an innovative approach to the education of children in kindergarten. PLoS ONE 9(11):e112393.
Blank, M. J., A. Melaville, and B. P. Shah. 2003. Making the difference: Research and practice in community schools. Washington, DC: The Coalition for Community Schools.
Borntrager, C., J. C. Caringi, R. van den Pol, L. Crosby, K. O’Connell, A. Trautman, and M. McDonald. 2012. Secondary traumatic stress in school personnel. Advances in School Mental Health Promotion 5(1):38–50.
Bowlby, J. 2008. A secure base: Parent-child attachment and healthy human development. New York: Basic Books.
Boyd, B. A., I. U. Iruka, and N. P. Pierce. 2018. Strengthening service access for children of color with autism spectrum disorders: A proposed conceptual framework. International Review of Research in Developmental Disabilities 54:1–33.
Boysen, G. A. 2010. Integrating implicit bias into counselor education. Counselor Education and Supervision 49(4):210–227.
Bradley, R. H., and D. L. Vandell. 2007. Child care and the well-being of children. Archives of Pediatrics and Adolescent Medicine 161(7):669–676.
Brooks-Gunn, J., L. J. Berlin, and A. S. Fuligni. 2000. Early childhood intervention programs: What about the family? In Handbook of early childhood intervention, 2nd ed., edited by J. P. Shonkoff and S. J. Meisels. New York: Cambridge University Press. Pp. 549–588.
Brotman, L. M., E. Calzada, K. Y. Huang, S. Kingston, S. Dawson-McClure, D. Kamboukos, A. Rosenfelt, A. Schwab, and E. Petkova. 2011. Promoting effective parenting practices and preventing child behavior problems in school among ethnically diverse families from underserved, urban communities. Child Development 82(1):258–276.
Brotman, L. M., S. Dawson-McClure, K. Y. Huang, R. Theise, D. Kamboukos, J. Wang, E. Petkova, and G. Ogedegbe. 2012. Early childhood family intervention and long-term obesity prevention among high-risk minority youth. Pediatrics 129(3):e621–e628.
Brotman, L. M., S. Dawson-McClure, E. J. Calzada, K. Y. Huang, D. Kamboukos, J. J. Palamar, and E. Petkova. 2013. Cluster (school) RCT of ParentCorps: Impact on kindergarten academic achievement. Pediatrics 131(5):e1521–e1529.
Brotman, L. M., S. Dawson-McClure, D. Kamboukos, K. Y. Huang, E. J. Calzada, K. Goldfeld, and E. Petkova. 2016. Effects of ParentCorps in prekindergarten on child mental health and academic performance: Follow-up of a randomized clinical trial through 8 years of age. JAMA Pediatrics 170(12):1149–1155.
Bruder, M. B. 2010. Early childhood intervention. Exceptional Children 76(3):339–355.
Bryson, S. A., E. Gauvin, A. Jamieson, M. Rathgeber, L. Faulkner-Gibson, S. Bell, J. Davidson, J. Russel, and S. Burke. 2017. What are effective strategies for implementing trauma-informed care in youth inpatient psychiatric and residential treatment settings? A realist systematic review. International Journal of Mental Health Systems 11:36.
Burchinal, M., K. Magnuson, D. Powell, and S. S. Hong. 2015. Early childcare and education. In Handbook of child psychology and developmental science: Ecological settings and processes, Vol. 4, edited by M. H. Bornstein, T. Leventhal, and R. M. Lerner. Hoboken, NJ: John Wiley & Sons. Pp. 223–267.
Burgess, D. J., M. C. Beach, and S. Saha. 2017. Mindfulness practice: A promising approach to reducing the effects of clinician implicit bias on patients. Patient Education and Counseling 100(2):372–376.
Campbell, F. A., E. P. Pungello, M. Burchinal, K. Kainz, Y. Pan, B. H. Wasik, O. A. Barbarin, J. J. Sparling, and C. T. Ramey. 2012. Adult outcomes as a function of an early childhood educational program: An Abecedarian Project follow-up. Developmental Psychology 48(4):1033–1043.
Campbell, F., G. Conti, J. J. Heckman, S. H. Moon, R. Pinto, E. Pungello, and Y. Pan. 2014. Early childhood investments substantially boost adult health. Science 343(6178):1478–1485.
Cannon, J. S., M. R. Kilburn, L. A. Karoly, T. Mattox, A. N. Muchow, and M. Buenaventura. 2017. Investing early: Taking stock of outcomes and economic returns from early childhood programs. Santa Monica, CA: RAND Corporation.
Caringi, J. C., C. Stanick, A. Trautman, L. Crosby, M. Devlin, and S. Adams. 2015. Secondary traumatic stress in public school teachers: contributing and mitigating factors. Advances in School Mental Health Promotion 8(4):244–256.
Carney, R., B. Stratford, K. A. Moore, A. Rojas, and P. Daneri. 2015. What works for reducing problem behaviors in early childhood: Lessons from experimental evaluations. Bethesda, MD: Child Trends.
CASEL (Collaborative for Academic, Social, and Emotional Learning). n.d. What is SEL? https://casel.org/what-is-sel (accessed April 2, 2019).
Castro, D. C., E. E. García, and A. M. Markos. 2013. Dual language learners: Research informing policy. Chapel Hill, NC: The University of North Carolina, Frank Porter Graham Child Development Institute, Center for Early Care and Education—Dual Language Learners.
CBITS (Cognitive Behavioral Intervention for Trauma in Schools). n.d.-a. Home. http://cbitsprogram.org (accessed July 15, 2019).
CBITS. n.d.-b. Cognitive behavioral intervention for trauma in schools: Success stories. http://cbitsprogram.org/success-stories (accessed June 11, 2019).
CBO (Congressional Budget Office). 2015. Child nutrition programs: Spending and policy options. Washington, DC: Congressional Budget Office.
CDC (Centers for Disease Control and Prevention). 2014. Prevalence of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2010. Morbidity and Mortality Weekly Report Surveillance Summaries 63(2):1–21.
Center on the Developing Child at Harvard University. n.d. Executive function & self-regulation. https://developingchild.harvard.edu/science/key-concepts/executive-function (accessed April 2, 2019).
Chase-Lansdale, P. L., and J. Brooks-Gunn. 2014. Two-generation programs in the twenty-first century. The Future of Children 24(1):13–39.
Child Trends. 2012. HighScope Perry Preschool. https://highscope.org/perry-preschool-project (accessed July 9, 2019).
Child Welfare Committee, National Child Traumatic Stress Network. 2013. Child welfare trauma training toolkit: Comprehensive guide, 3rd ed. Los Angeles, CA, and Durham, NC: National Center for Child Traumatic Stress.
Chung-Park, M. S. 2012. Knowledge, opinions, and practices of infant sleep position among parents. Military Medicine 177(2):235–239.
Conti, G., J. Heckman, and S. Urzua. 2010. The education-health gradient. American Economic Review 100(2):234–238.
Cook, T. D., F.-N. Habib, M. Phillips, R. A. Settersten, S. C. Shagle, and S. M. Degirmencioglu. 1999. Comer’s School Development Program in Prince George’s County, Maryland: A theory-based evaluation. American Educational Research Journal 36(3):543–597.
Corcoran, L., K. Steinley, and S. Grady. 2019. Early childhood program participation, results from the National Household Education Surveys Program of 2016. Washington, DC: U.S. Department of Education, National Center for Education Statistics, Institute of Education Sciences.
Cross, T., B. Bazron, K. Dennis, and M. Isaacs. 1989. Towards a culturally competent system of care: A monograph on effective services for minority children who are severely emotionally disturbed. Washington, DC: Georgetown University Child Development Center.
Cuccaro, M. L., J. Brinkley, R. K. Abramson, A. Hall, H. H. Wright, J. P. Hussman, J. R. Gilbert, and M. A. Pericak-Vance. 2007. Autism in African American families: Clinical-phenotypic findings. American Journal of Medical Genetics, Part B: Neuropsychiatric Genetics 144b(8):1022–1026.
Dawson-McClure, S., E. Calzada, K. Y. Huang, D. Kamboukos, D. Rhule, B. Kolawole, E. Petkova, and L. M. Brotman. 2015. A population-level approach to promoting health child development and school success in low-income, urban neighborhoods: Impact on parenting and child conduct problems. Prevention Science 16(2):279–290.
Delgado, C. E. F., and K. G. Scott. 2006. Comparison of referral rates for preschool children at risk for disabilities using information obtained from birth certificate records. The Journal of Special Education 40(1):28–35.
Devine, P. G., P. S. Forscher, A. J. Austin, and W. T. Cox. 2012. Long-term reduction in implicit race bias: A prejudice habit-breaking intervention. Journal of Experimental Social Psychology 48(6):1267–1278.
Diamond, A., W. S. Barnett, J. Thomas, and S. Munro. 2007. Preschool program improves cognitive control. Science 318(5855):1387–1388.
D’Onise, K., J. W. Lynch, M. G. Sawyer, and R. A. McDermott. 2010. Can preschool improve child health outcomes? A systematic review. Social Science & Medicine 70(9):1423–1440.
Duncan, G. J., and K. Magnuson. 2013. Investing in preschool programs. Journal of Economic Perspectives 27(2):109–132.
Dunifon, R., and L. Kowaleski-Jones. 2003. The influences of participation in the National School Lunch Program and food insecurity on child well-being. Social Service Review 77(1):72–92.
Duran, F., K. Hepburn, M. Irvine, R. Kaufmann, B. Anthony, N. Horen, and D. Perry. 2009. What works?: A study of effective early childhood mental health consultation programs. Washington, DC: Georgetown University Center for Child and Human Development.
Durlak, J. A., and R. P. Weissberg. 2013. Afterschool programs that follow evidence-based practices to promote social and emotional development are effective. In Expanding minds and opportunities: Leveraging the power of afterschool and summer learning for student success, section 3: Recent evidence of impact, edited by T. K. Peterson. Washington, DC: Collaborative Communications Group. Pp. 24–28.
Durlak, J. A., R. P. Weissberg, A. B. Dymnicki, R. D. Taylor, and K. B. Schellinger. 2011. The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Development 82(1):405–432.
ED (U.S. Department of Education). 2010. 21st Century Community Learning Centers (21st CCLC) analytic support for evaluation and program monitoring: An overview of the 21st CCLC performance data: 2008–09 (sixth report). Washington, DC: U.S. Department of Education.
ED. 2018. 40th annual report to Congress on the implementation of the Individuals with Disabilities Education Act, 2018. Washington, DC: U.S. Department of Education, Office of Special Education and Rehabilitative Services, Office of Special Education Programs.
ED OCR (Office for Civil Rights). 2016. 2013-2014 Civil Rights Data Collection: A first look. Key data highlights on equity and opportunity gaps in our nation’s public schools. Washington, DC: U.S. Department of Education, Office for Civil Rights.
Fantuzzo, J., V. Gadsden, F. Li, F. Sproul, P. McDermott, D. Hightower, and A. Minney. 2013. Multiple dimensions of family engagement in early childhood education: Evidence for a short form of the Family Involvement Questionnaire. Early Childhood Research Quarterly 28(4):734–742.
Farran, D. C., S. J. Wilson, D. Meador, J. Norvell, and K. Nesbitt. 2015. Experimental evaluation of the Tools of the Mind pre-K curriculum: Technical report. (Working paper). Nashville, TN: Peabody Research Institute, Vanderbilt University.
Fisher, B., A. Hanson, and T. Raden. 2014. Start early to build a healthy future: The research linking early learning and health. Chicago, IL: Ounce of Prevention Fund.
Forry, N., I. U. Iruka, K. Tout, J. Torquati, A. Susman-Stillman, D. Bryant, and M. P. Daneri. 2013. Predictors of quality and child outcomes in family child care settings. Early Childhood Research Quarterly 28(4):893–904.
Fountain, C., A. S. Winter, and P. S. Bearman. 2012. Six developmental trajectories characterize children with autism. Pediatrics 129(5):e1112–e1120.
Frank Porter Graham Child Development Institute. 2012. The Abecedarian Project: High-quality early child care has long-lasting effects. FPG Snapshot #66. https://fpg.unc.edu/sites/fpg.unc.edu/files/resources/snapshots/FPG_Snapshot66_2012.pdf (accessed July 9, 2019).
Frisvold, D. E. 2015. Nutrition and cognitive achievement: An evaluation of the School Breakfast Program. Journal of Public Economics 124:91–104.
Frisvold, D. E., and J. C. Lumeng. 2011. Expanding exposure: Can increasing the daily duration of Head Start reduce childhood obesity? Journal of Human Resources 46(2):373–402.
Gabor, V., and K. Mantinan. 2012. State efforts to address obesity prevention in child care quality rating and improvement systems. Ann Arbor, MI: Altarum Institute.
Galindo, C., S. Sonnenschein, and A. Montoya-Ávila. 2019. Latina mothers’ engagement in children’s math learning in the early school years: Conceptions of math and socialization practices. Early Childhood Research Quarterly 47:271–283.
Gallagher, R. W., and J. R. Polanin. 2015. A meta-analysis of educational interventions designed to enhance cultural competence in professional nurses and nursing students. Nurse Education Today 35(2):333–340.
GAO (U.S. Government Accountability Office). 2018. K–12 education: Discipline disparities for black students, boys, and students with disabilities. Washington, DC: U.S. Government Accountability Office.
García, E. 2015. Inequalities at the starting gate: Cognitive and noncognitive skills gaps between 2010–2011 kindergarten classmates. Washington, DC: Economic Policy Institute.
Gilliam, W. S., A. N. Maupin, and C. R. Reyes. 2016a. Early childhood mental health consultation: Results of a statewide random-controlled evaluation. Journal of the American Academy of Child and Adolescent Psychiatry 55(9):754–761.
Gilliam, W. S., A. N. Maupin, C. R. Reyes, M. Accavitti, and F. Shic. 2016b. Do early educators’ implicit biases regarding sex and race relate to behavior expectations and recommendations of preschool expulsions and suspensions? A research study brief. New Haven, CT: Yale University Child Study Center.
Gleason, P. M., and A. H. Dodd. 2009. School breakfast program but not school lunch program participation is associated with lower body mass index. Journal of the American Dietetic Association 109(Suppl 2):S118–S128.
Godsil, R. D., L. R. Tropp, P. A. Goff, and J. A. Powell. 2014. Addressing implicit bias, racial anxiety, and stereotype threat in education and health care. Perception Institute.
Goff, P. A., M. C. Jackson, B. A. Di Leone, C. M. Culotta, and N. A. DiTomasso. 2014. The essence of innocence: Consequences of dehumanizing black children. Journal of Personality and Social Psychology 106(4):526–545.
Gomby, D. S., M. B. Larner, C. S. Stevenson, E. M. Lewit, and R. E. Behrman. 1995. Long-term outcomes of early childhood programs: Analysis and recommendations. The Future of Children 5(3):6–24.
Gordon, R. A., A. Colaner, M. L. Usdansky, and C. Melgar. 2013. Beyond an “either-or” approach to home- and center-based child care: Comparing children and families who combine care types with those who just use one. Early Childhood Research Quarterly 28(4):918–935.
Granger, R. C., and R. Cytron. 1999. Teenage parent programs a synthesis of the long-term effects of the new chance demonstration, Ohio’s learning, earning, and parenting program, and the teenage parent demonstration. Evaluation Review 23(2):107–145.
Gundersen, C. 2015. Food assistance programs and child health. The Future of Children 25(1):91–109.
Gundersen, C., and J. P. Ziliak. 2014. Childhood food insecurity in the U.S.: Trends, causes, and policy options. Princeton, NJ: The Future of Children.
Gundersen, C., B. Kreider, and J. Pepper. 2012. The impact of the National School Lunch Program on child health: A nonparametric bounds analysis. Journal of Econometrics 166(1):79–91.
Guralnick, M. J. 1998. Effectiveness of early intervention for vulnerable children: A developmental perspective. American Journal on Mental Retardation 102(4):319–345.
Guralnick, M. J. 2005. Early intervention for children with intellectual disabilities: Current knowledge and future prospects. Journal of Applied Research in Intellectual Disabilities 18:313–324.
Hahn, R. A., W. S. Barnett, J. A. Knopf, B. I. Truman, R. L. Johnson, J. E. Fielding, C. Muntaner, C. P. Jones, M. T. Fullilove, and P. C. Hunt. 2016. Early childhood education to promote health equity: A community guide systematic review. Journal of Public Health Management and Practice 22(5):e1–e8.
Hajizadeh, N., E. R. Stevens, M. Applegate, K. Y. Huang, D. Kamboukos, R. S. Braithwaite, and L. M. Brotman. 2017. Potential return on investment of a family-centered early childhood intervention: A cost-effectiveness analysis. BMC Public Health 17(1):796.
Hawkinson, L. E., A. S. Griffen, N. Dong, and R. A. Maynard. 2013. The relationship between child care subsidies and children’s cognitive development. Early Childhood Research Quarterly 28(2):388–404.
Haynes, N. M., and J. P. Comer. 1990a. Helping black children succeed: The significance of some social factors. In Going to school: The African American experience, edited by K. Lomotey. Albany, NY: State University of New York Press.
Haynes, N. M., and J. P. Comer. 1990b. The effects of a school development program on self-concept. The Yale Journal of Biology and Medicine 63(4):275–283.
Haynes, N. M., C. L. Emmons, and D. W. Woodruff. 1998. School Development Program effects: Linking implementation to outcomes. Journal of Education for Students Placed at Risk 3(1):71–85.
Heckman, J. J., and G. Karapakula. 2019a. Intergenerational and intragenerational externalities of the Perry Preschool Project. Working Paper 2019-033. Chicago, IL: Human Capital and Economic Opportunity Global Working Group, University of Chicago.
Heckman, J. J., and G. Karapakula. 2019b. The Perry Preschoolers at late midlife: A study in design-specific inference. NBER Working paper no. 25888. Cambridge, MA: National Bureau of Economic Research.
Herbst, C. M., and E. Tekin. 2011. Child care subsidies and childhood obesity. Review of Economics of the Household 9(3):349–378.
HHS (U.S. Department of Health and Human Services). 2017. Head Start program facts: Fiscal year 2017. https://eclkc.ohs.acf.hhs.gov/about-us/article/head-start-program-facts-fiscal-year-2017 (accessed April 18, 2019).
HHS. 2018. Family well-being: Strategies to support family safety, health, and financial stability. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families, Office of Head Start, Office of Child Care; National Center on Parent, Family and Community Engagement.
Hocutt, A. M. 1996. Effectiveness of special education: Is placement the critical factor? The Future of Children 6(1):77–102.
Hodas, G. R. 2006. Responding to childhood trauma: The promise and practice of trauma informed care. Pennsylvania Office of Mental Health and Substance Abuse Services. http://www.childrescuebill.org/VictimsOfAbuse/RespondingHodas.pdf (accessed July 11, 2019).
Hofferth, S. L., and S. Curtin. 2005. Poverty, food programs, and childhood obesity. Journal of Policy Analysis and Management 24(4):703–726.
Holliday, M. R., A. Cimetta, C. Cutshaw, D. Yaden, and R. Marx. 2014. Protective factors for school readiness among children in poverty. Journal of Education for Students Placed at Risk 19:125–147.
Hong, K., K. Dragan, and S. Glied. 2017. Seeing and hearing: The impacts of New York City’s universal prekindergarten program on the health of low-income children. Working Paper 23297. Cambridge, MA: National Bureau of Economic Research.
Horowitz, S. H., J. Rawe, and M. C. Whittaker. 2017. The state of learning disabilities: Understanding the 1 in 5. New York: National Center for Learning Disabilities.
Hydon, S., M. Wong, A. K. Langley, B. D. Stein, and S. H. Kataoka. 2015. Preventing secondary traumatic stress in educators. Child and Adolescent Psychiatric Clinics of North America 24(2):319–333.
IOM and NRC (Institute of Medicine and National Research Council). 2015. Transforming the workforce for children birth through age 8: A unifying approach. Washington, DC: The National Academies Press.
Iruka, I., and N. D. Forry. 2018. Links between patterns of quality in diverse settings and children’s early outcomes. Journal of Education 198(1):95–112.
Jones, D. E., M. Greenberg, and M. Crowley. 2015. Early social-emotional functioning and public health: The relationship between kindergarten social competence and future wellness. American Journal of Public Health 105(11):2283–2290.
Jones, S. M., and S. M. Bouffard. 2012. Social and emotional learning in schools: From programs to strategies. Social Policy Report 26(4):1–33.
Kay, N., and A. Pennucci. 2014. Early childhood education for low-income students: A review of the evidence and benefit-cost analysis. Doc. No. 14-01-2201. Olympia, WA: Washington State Institute for Public Policy.
Knoche, L. L., S. M. Sheridan, B. L. Clarke, C. P. Edwards, C. A. Marvin, K. D. Cline, and K. A. Kupzyk. 2012. Getting Ready: Results of a randomized trial of a relationship-focused intervention on the parent–infant relationship in rural Early Head Start. Infant Mental Health Journal 33(5):439–458.
Landa, R. J. 2018. Efficacy of early interventions for infants and young children with, and at risk for, autism spectrum disorders. International Review of Psychiatry 30(1):25–39.
Lane, K. L., J. H. Wehby, M. A. Little, and C. Cooley. 2005. Students educated in self-contained classrooms and self-contained schools: Part II—how do they progress over time? Behavioral Disorders 30(4):363–374.
Lee, R., F. Zhai, W. Han, J. Brooks-Gunn, and J. Waldfogel. 2013. Head Start and children’s nutrition, weight, and health care receipt. Early Child Development and Care 28(4):723–733.
Leininger, M., and M. McFarland. 2002. Transcultural Nursing Concepts, Theories, Research and Practice, 3rd ed. New York: McGraw-Hill.
Lipsey, M. W., D. C. Farran, and K. Durkin. 2018. Effects of the Tennessee Prekindergarten Program on children’s achievement and behavior through third grade. Early Childhood Research Quarterly 45:155–176.
Litt, J. S., M. M. Glymour, P. Hauser-Cram, T. Hehir, and M. C. McCormick. 2018. Early intervention services improve school-age functional outcome among neonatal intensive care unit graduates. Academic Pediatrics 18(4):468–474.
Loeb, S., M. Bridges, D. Bassok, B. Fuller, and R. W. Rumberger. 2007. How much is too much? The influence of preschool centers on children’s social and cognitive development. Economics of Education Review 26(1):52–66.
Lucas, L. 2007. The pain of attachment—“You have to put a little wedge in there”: How vicarious trauma affects child/teacher attachment. Childhood Education 84(2):85–91.
Lunenburg, F. C. 2011. The Comer School Development Program: Improving education for low-income students. National Forum of Multicultural Issues Journal 8(1):1–14.
Madill, R., T. Halle, T. Gebhart, and E. Shuey. 2018. Supporting the psychological well-being of the early care and education workforce: Findings from the National Survey of Early Care and Education. OPRE Report 2018-49. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families, Office of Planning, Research & Evaluation.
Magnuson, K. A., C. Ruhm, and J. Waldfogel. 2007. Does prekindergarten improve school preparation and performance? Economics of Education Review 26(1):33–51.
Maina, I. W., T. D. Belton, S. Ginzberg, A. Singh, and T. J. Johnson. 2018. A decade of studying implicit racial/ethnic bias in healthcare providers using the implicit association test. Social Science & Medicine 199:219–229.
Malik, R. 2017. New data reveals 250 preschoolers are suspended or expelled every day. Center for American Progress. https://www.americanprogress.org/issues/early-childhood/news/2017/11/06/442280/new-data-reveal-250-preschoolers-suspendedexpelled-every-day (accessed June 14, 2019).
Matthews, H., R. Ullrich, and W. Cervantes. 2018. Immigration policy’s harmful impacts on early care and education. Washington, DC: Center for Law and Social Policy.
McClelland, M. M., S. L. Tominey, S. A. Schmitt, and R. Duncan. 2017. SEL interventions in early childhood. The Future of Children 21(1):33–47.
McManus, B. M., A. C. Carle, and J. Poehlmann. 2012. Effectiveness of Part C early intervention physical, occupational, and speech therapy services for preterm or low birth weight infants in Wisconsin, United States. Academic Pediatrics 12(2):96–103.
Meek, S. E., and W. S. Gilliam. 2016. Expulsion and suspension in early education as matters of social justice and health equity. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. doi: 10.31478/201610e.
Mendez, J. L. 2010. How can parents get involved in preschool? Barriers and engagement in education by ethnic minority parents of children attending Head Start. Cultural Diversity and Ethnic Minority Psychology 16(1):26–36.
Michalopoulos, C., S. S. Crowne, X. A. Portilla, H. Lee, J. H. Filene, A. Duggan, and V. Knox. 2019. A summary of the results from the MIHOPE and MIHOPE—Strong Start studies of evidence-based home visiting. OPRE Report 2019-09. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families, Office of Planning, Research & Evaluation.
Moffitt, T. E., L. Arseneault, D. Belsky, N. Dickson, R. J. Hancox, H. Harrington, R. Houts, R. Poulton, B. W. Roberts, S. Ross, M. R. Sears, W. M. Thomson, and A. Caspi. 2011. A gradient of childhood self-control predicts health, wealth, and public safety. Proceedings of the National Academy of Sciences of the United States of America 108(7):2693–2698.
Morgan, P. L., M. Frisco, G. Farkas, and J. Hibel. 2010. A propensity score matching analysis of the effects of special education services. The Journal of Special Education 43(4):236–254.
Morgan, P. L., G. Farkas, M. M. Hillemeier, R. Mattison, S. Maczuga, H. Li, and M. Cook. 2015. Minorities are disproportionately underrepresented in special education: Longitudinal evidence across five disability conditions. Educational Research 44(5):278–292.
Morris, P., S. K. Mattera, N. Castells, M. Bangser, K. Bierman, and C. Raver. 2014. Impact findings from the Head Start CARES demonstration: National evaluation of three approaches to improving preschoolers’ social and emotional competence. OPRE Report 2014-44. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families, Office of Planning, Research & Evaluation.
Muennig, P., D. Robertson, G. Johnson, F. Campbell, E. P. Pungello, and M. Neidell. 2011. The effect of an early education program on adult health: The Carolina Abecedarian Project randomized controlled trial. American Journal of Public Health 101(3):512–516.
NASEM. 2016a. Parenting matters: Supporting parents of children ages 0–8. Washington, DC: The National Academies Press.
NASEM. 2016b. Preventing bullying through science, policy, and practice. Washington, DC: The National Academies Press.
NASEM. 2017a. Communities in action: Pathways to health equity. Washington, DC: The National Academies Press.
NASEM. 2017b. Promoting the educational success of children and youth learning English: Promising futures. Washington, DC: The National Academies Press.
NASEM. 2018. Transforming the financing of early care and education. Washington, DC: The National Academies Press.
NASEM. 2019. The promise of adolescence: Realizing opportunity for all youth. Washington, DC: The National Academies Press.
National Education Association. n.d. Discipline and the school-to-prison pipeline (2016). https://ra.nea.org/business-item/2016-pol-e01-2 (accessed June 14, 2019).
National Survey of Early Care and Education Project Team. 2016. Characteristics of home-based early care and education providers: Initial findings from the National Survey of Early Care and Education. OPRE Report 2016-13. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families, Office of Planning, Research & Evaluation.
New, R. S., and M. Cochran. 2007. Early childhood education (four volumes): An international encyclopedia, Vol. 1–4. Westport, CT: Praeger Publishers. http://www.encyclopedias.biz/dw/Encyclopedia%20of%20Early%20Childhood%20Education.pdf (accessed July 10, 2019).
Noltemeyer, A. L., R. M. Ward, and C. McLoughlin. 2015. Relationship between school suspension and student outcomes: A meta-analysis. School Psychology Review 44(2):224–240.
Northside Achievement Zone. 2019. NAZ results summary: An innovative approach that is working. Minneapolis, MN: Northside Achievement Zone.
Northside Achievement Zone. n.d. What is NAZ? https://northsideachievement.org/who-we-are (accessed April 2, 2019).
NYU (New York University) School of Medicine. 2019. ParentCorps Langone Health. https://med.nyu.edu/departments-institutes/population-health/divisions-sections-centers/health-behavior/center-early-childhood-health-development/parentcorps (accessed July 11, 2019).
Oswald, D. P., M. J. Goutinho, A. M. Best, and N. Singh. 1999. Ethnic representation in special education: The influence of school-related economic and demographic variables. The Journal of Special Education 32(4):194–206.
Pears, K. C., P. A. Fisher, and K. D. Bronz. 2007. An intervention to promote social emotional school readiness in foster children: Preliminary outcomes from a pilot study. School Psychology Review 36(4):665–673.
Pears, K. C., H. K. Kim, and P. A. Fisher. 2012. Effects of a school readiness intervention for children in foster care on oppositional and aggressive behaviors in kindergarten. Children and Youth Services Review 34(12):2361–2366.
Pears, K. C., P. A. Fisher, H. K. Kim, J. Bruce, C. V. Healey, and K. Yoerger. 2013. Immediate effects of a school readiness intervention for children in foster care. Early Education and Development 24(6):771–791.
Pears, K. C., C. V. Healey, P. A. Fisher, D. Braun, C. Gill, H. M. Conte, J. Newman, and S. Ticer. 2014. Immediate effects of a program to promote school readiness in low-income children: Results of a pilot study. Education and Treatment of Children 37(3):431–460.
Peters-Scheffer, N., R. Didden, H. Korzilius, and P. Sturmey. 2011. A meta-analytic study on the effectiveness of comprehensive ABA-based early intervention programs for children with autism spectrum disorders. Research in Autism Spectrum Disorders 5(1):60–69.
Phillips, D. A., M. W. Lipsey, K. A. Dodge, R. Haskins, D. Bassok, M. R. Burchinal, G. J. Duncan, M. Dynarski, K. A. Magnuson, and C. Weiland. 2017. Puzzling it out: The current state of scientific knowledge on pre-kindergarten effects. A consensus statement. Washington, DC: The Brookings Institution.
Pianta, R. C., W. S. Barnett, M. Burchinal, and K. R. Thornburg. 2009. The effects of preschool education: What we know, how public policy is or is not aligned with the evidence base, and what we need to know. Psychological Science in the Public Interest 10(2):49–88.
Polit, D. F. 1989. Effects of a comprehensive program for teenage parents: Five years after project redirection. Family Planning Perspectives 21(4):164–187.
Porter, T., T. Nichols, P. Del Grosso, C. Begnoche, R. Hass, L. Vuong, and D. Paulsell. 2010a. A compilation of initiatives to support home-based child care. Washington, DC, and Princeton, NJ: Office of Planning, Research & Evaluation, Administration for Children and Families, and Mathematica Policy Research.
Porter, T., D. Paulsell, P. Del Grosso, S. Avellar, R. Hass, and L. Vuong. 2010b. A review of the literature on home-based child care: Implications for future directions. Washington, DC: Administration for Children and Families, Office of Planning, Research & Evaluation.
Puma, M., S. Bell, R. Cook, C. Heid, P. Broene, F. Jenkins, A. Mashburn, and J. Downer. 2012. Third-grade follow-up to the Head Start Impact Study: Final report. OPRE Report 2012-45. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families, Office of Planning, Research & Evaluation.
Ralston, K., C. Newman, A. Clauson, J. Guthrie, and J. Buzby. 2008. The National School Lunch Program: Background, trends, and issues. Economic Research Report Number 61. Washington, DC: U.S. Department of Agriculture.
Ramey, C. T. 2018. The Abecedarian approach to social, educational, and health disparities. Clinical Child and Family Psychology Review 21(4):527–544.
Ramey, C. T., and S. L. Ramey. 2004. Early learning and school readiness: Can early intervention make a difference. Merrill-Palmer Quarterly 50(4):471–491.
Ramirez, M., Y. Wu, S. Kataoka, M. Wong, J. Yang, C. Peek-Asa, and B. Stein. 2012. Youth violence across multiple dimensions: A study of violence, absenteeism, and suspensions among middle school children. The Journal of Pediatrics 161(3):542–546.
Raver, C. C. 2012. Low-income children’s self-regulation in the classroom: Scientific inquiry for social change. American Psychologist 67(8):681–689.
Regalado, M., and N. Halfon. 2001. Primary care services promoting optimal child development from birth to age 3 years: Review of the literature. Archives of Pediatrics and Adolescent Medicine 155(12):1311–1322.
Reichow, B. 2011. Overview of meta-analyses on early intensive behavioral intervention for young children with autism spectrum disorders. Journal of Autism and Developmental Disorders 42(4):512–520.
Roberts, A. M., K. C. Gallagher, A. M. Daro, I. U. Iruka, and S. L. Sarver. 2019. Workforce well-being: Personal and workplace contributions to early educators’ depression across settings. Journal of Applied Developmental Psychology 61:4–12.
Rose, E. 2010. The promise of preschool: From Head Start to universal pre-kindergarten. New York: Oxford University Press.
Rossin-Slater, M. 2015. Promoting health in early childhood. The Future of Children 25(1):35–64.
Ruijs, N. M., and T. T. D. Peetsma. 2009. Effects of inclusion on students with and without special educational needs reviewed. Educational Research Review 4(2):67–79.
Sabol, T. J., and L. T. Hoyt. 2017. The long arm of childhood: Preschool associations with adolescent health. Developmental Psychology 53(4):752–763.
Sanders, M. 2016. Leadership, partnerships, and organizational development: Exploring components of effectiveness in three full-service community schools. School Effectiveness and School Improvement 27(2):157–177.
Schanzenbach, D. W. 2009. Do school lunches contribute to childhood obesity? The Journal of Human Resources 44(3):684–709.
Schindler, H. S., J. Kholoptseva, S. S. Oh, H. Yoshikawa, G. J. Duncan, K. A. Magnuson, and J. P. Shonkoff. 2015. Maximizing the potential of early childhood education to prevent externalizing behavior problems: A meta-analysis. Journal of School Psychology 53(3):243–263.
Schneidman, L., and A. L. Woodward. 2016. Are child-directed interactions the cradle of social learning? Psychological Bulletin 142(1):1–17.
Schweinhart, L. J., and D. P. Weikart. 1997. The High/Scope Preschool Curriculum Comparison Study through age 23. Early Childhood Research Quarterly 12(2):117–143.
Schweinhart, L. J., J. Montie, Z. Xiang, W. S. Barnett, C. R. Belfield, and M. Nores. 2005. Lifetime effects: The High/Scope Perry Preschool study through age 40. Ypsilanti, MI: High Scope Press.
Sheridan, S. M., L. L. Knoche, C. P. Edwards, J. A. Bovaird, and K. A. Kupzyk. 2010. Parent engagement and school readiness: Effects of the Getting Ready intervention on preschool children’s social-emotional competencies. Early Education and Development 21(1):125–156.
Sheridan, S. M., L. L. Knoche, K. A. Kupzyk, C. P. Edwards, and C. A. Marvin. 2011. A randomized trial examining the effects of parent engagement on early language and literacy: The Getting Ready intervention. Journal of School Psychology 49(3):361–383.
Sheridan, S. M., L. L. Knoche, C. P. Edwards, K. A. Kupzyk, B. L. Clarke, and E. M. Kim. 2014. Efficacy of the Getting Ready intervention and the role of parental depression. Early Education and Development 25(5):746–769.
Shonkoff, J. P., and P. Hauser-Cram. 1987. Early intervention for disabled infants and their families: A quantitative analysis. Pediatrics 80(5):650–658.
Silva, K. G., P. M. Shimpi, and B. Rogoff. 2015. Young children’s attention to what’s going on: Cultural differences. Advances in Child Development and Behavior 49:207–227.
Skiba, R. J., L. Poloni-Staudinger, A. B. Simmons, and L. R. C. Feggins-Azziz. 2005. Unproven links: Can poverty explain ethnic disproportionality in special education? The Journal of Special Education 39(3):130–144.
Smith, T. B., M. G. Constantine, T. W. Dunn, J. M. Dinehart, and J. A. Montoya. 2006. Multicultural education in the mental health professions: A meta-analytic review. Journal of Counseling Psychology 53(1):132–145.
Solomon, T., A. Plamondon, A. O’Hara, H. Finch, G. Goco, P. Chaban, L. Huggins, B. Ferguson, and R. Tannock. 2017. A cluster randomized-controlled trial of the impact of the Tools of the Mind curriculum on self-regulation in Canadian preschoolers. Frontiers in Psychology 8:2366.
Sparling, J., and I. Lewis. 1979. Learningames for the first three years: A guide to parent-child play. New York: Walker and Company.
Sperry, D. E., L. L. Sperry, and P. J. Miller. 2018. Reexamining the verbal environments of children from different socioeconomic backgrounds. Child Development 90(4):1303–1318.
Stein, B. D., L. H. Jaycox, S. H. Kataoka, M. Wong, A. K. Langley, J. L. Avila, A. Bonilla, P. Castillo-Campos, J. B. Cohen, K. L. Dean, J. L. DuClos, M. N. Elliott, P. Escudero, A. Fink, S. Fuentes, K. L. Gegenheimer, K. Halsey, A. P. Mannarino, E. Nadeem, V. K. Ngo, V. P. O’Donoghue, M. Schonlau, M. M. Scott, P. Sharma, W. Wenli Tu, D. Walker, and C. Zaragoza. 2011. Helping children cope with violence and trauma: A school-based program that works. Santa Monica, CA: RAND Corporation.
Sue, D. W., C. M. Capodilupo, G. C. Torino, J. M. Bucceri, A. M. B. Holder, K. L. Nadal, and M. Esquilin. 2007. Racial microaggressions in everyday life: Implications for clinical practice. American Psychologist 62(4):271–286.
Temple, J. A., and A. J. Reynolds. 2007. Benefits and costs of investments in preschool education: Evidence from the Child–Parent Centers and related programs. Economics of Education Review 26(1):126–144.
The National Child Traumatic Stress Network. n.d. Creating trauma-informed systems. https://www.nctsn.org/trauma-informed-care/creating-trauma-informed-systems (accessed June 10, 2019).
The Urban Child Institute. 2019. Social and emotional development in early childhood? The first years last a lifetime. http://www.urbanchildinstitute.org/resources/publications/goodstart/social-and-emotional-development (accessed June 14, 2019).
Thurlow, M., M. Sinclair, and D. Johnson. 2002. Students with Disabilities who drop out of School—Implications for policy and practice. National Center on Secondary Education and Transition Issue Brief 1(2). http://www.ncset.org/publications/viewdesc.asp?id=425 (accessed April 18, 2019).
Tout, K., K. Magnuson, S. Lipscomb, L. Karoly, R. Starr, H. Quick, and J. Wenner. 2017. Validation of quality ratings used in quality rating and improvement systems (QRIS): A synthesis of state studies. OPRE Report 2017-92. U.S. Department of Health and Human Services. https://www.acf.hhs.gov/opre/resource/validation-quality-ratings-used-quality-rating-improvement-systems-qris-a-synthesis-of-state-studies (accessed June 28, 2019).
USDA (U.S. Department of Agriculture). 2017. PART 210—National School Lunch Program. https://www.fns.usda.gov/part-210%E2%80%94national-school-lunch-program (accessed July 10, 2019).
Whitaker, R. C., T. Dearth-Wesley, and R. A. Gooze. 2015. Workplace stress and the quality of teacher–children relationships in Head Start. Early Childhood Research Quarterly 30:57–69.
Whitebook, M., C. McLean, L. J. E. Austin, and B. Edwards. 2018. The Early Childhood Workforce Index—2018. Berkeley, CA: Center for the Study of Child Care Employment, University of California, Berkeley.
Whitehurst, G. J., and M. Croft. 2010. The Harlem Children’s Zone, Promise Neighborhoods, and the broader, bolder approach to education. Washington, DC: Brown Center on Education Policy at Brookings.
Williford, A. P., and T. L. Shelton. 2008. Using mental health consultation to decrease disruptive behaviors in preschoolers: Adapting an empirically-supported intervention. Journal of Child Psychology and Psychiatry 49(2):191–200.
Yoshikawa, H., C. Weiland, J. Brooks-Gunn, M. R. Burchinal, L. M. Espinosa, W. T. Gormley, J. Ludwig, K. A. Magnuson, D. Phillips, and M. J. Zaslow. 2013. Investing in our future: The evidence base on preschool education. Washington, DC, and New York: Society for Research in Development and Foundation for Child Development.
Zakszeski, B. N., N. E. Ventresco, and A. R. Jaffe. 2017. Promoting resilience through trauma-focused practices: A critical review of school-based implementation. School Mental Health 9(4):310–321.
Zarnowiecki, D., N. Sinn, J. Petkov, and J. Dollman. 2011. Parental nutrition knowledge and attitudes as predictors of 5–6-year-old children’s healthy food knowledge. Public Health Nutrition 15(7):1284–1290.
Zellman, G. L., and M. Perlman. 2008. Child-care quality rating and improvement systems in five pioneer states: Implementation issues and lessons learned. Santa Monica, CA: RAND Corporation.
Zigler, E., and M. Finn-Stevenson. 2007. From research to policy practice: The school of the 21st century. American Journal of Orthopsychiatry 77(2):175–181.







































































