
4
Systemic Influences on Outcomes in Pregnancy and Childbirth
The individual-level risks discussed in the previous chapter are just one source of risk during pregnancy and childbirth. As shown in the committee’s conceptual model (refer to Figure 1-7 in Chapter 1), systems-level factors can contribute to existing risk factors or create new ones, shaping quality, access, choice, and outcomes in birth settings. These factors include structural inequalities and biases, the social determinants of health, and financing and policy decisions in the health system. In this chapter, we explore these systems-level influences that confer risk during pregnancy and childbirth. First, we discuss the current landscape of inequity in maternal and neonatal outcomes and consider a birthing justice framework for understanding and ameliorating these disparities. Next, we explore the outermost circle of the model, the structural inequities and biases that contribute to disparities in outcomes along racial/ethnic, socioeconomic, and linguistic lines. We then move inward on the model to a discussion of the social determinants of health, which provides a framework for understanding the impact of upstream factors on individual health and risk. Finally, we consider the innermost circle and the role of policy and financing in the health system in patterning women’s access to care and risk in pregnancy and childbirth. Our analyses lead to a series of conclusions, which are presented in the final section of the chapter.
INEQUITIES IN MATERNAL AND NEWBORN OUTCOMES
The United States has considerable and persistent racial/ethnic inequities in maternal and newborn outcomes (see Table 4-1; see also, e.g.,
Howell, 2018; Martin et al., 2018a). Across a number of risk and protective factors (e.g., maternal education, early initiation of prenatal care), Black, Hispanic, and American Indian/Alaska Native (AIAN) women fare worse than their non-Hispanic White and Asian counterparts (see Table 4-1). For example, 77.3 percent of White women and 81.1 percent of Asian women entered prenatal care in the first trimester, compared with 72.3 percent of Hispanic women, 66.6 percent of Black women, and 63.4 percent of AIAN women. Asian and White women are also more likely to have private insurance to cover their birth than are Black, Hispanic, and AIAN women. These disparities in protective factors are reflected in disparities in outcomes. Rates of preterm birth and low birthweight are higher among Black, AIAN, and Hispanic women than White women.1 In the case of low birthweight, Black women are more than twice as likely to have a low-birthweight infant as White women (refer to Table 4-1). Most strikingly, rates of pregnancy-related mortality and infant mortality are substantially higher among Black women compared with White women. The disparity in the White–Black infant mortality rate has persisted for decades (David and Collins, 1997; Collins et al., 2002).
Breaking down these broad racial/ethnic categories into ethnic subgroups reveals further disparities. Among Hispanic women, Puerto Rican, Mexican, Central and South American, and Cuban women all have different levels of risk and protective factors. For example, 82.2 percent of Cuban women initiated prenatal care in the first trimester—a greater proportion than White and Asian women—while only 67.7 percent of Central and South American women did so. Similarly, the infant mortality rate among births to Cuban women is 4.0 in 1,000, compared with 6.5 in 1,000 for Puerto Rican women.
There are many factors that may contribute to these racial/ethnic disparities in maternal and infant health outcomes. One factor that we consider here is the concept of “weathering.” Researchers have proposed that exposure to experiences of discrimination across the lifespan has the effect of “weathering” women of color, increasing their allostatic load,2 and, ultimately, physiologically compromising their health and pregnancies (Geronimus et al., 2006; Holzman et al., 2009; Lu and Halfon, 2003). In light of these realities, a thoughtful discussion of risk and birth settings must be placed in the context of historical and present-day inequities that may contribute to risk and impede equitable access to birth settings for
___________________
1 Asian women have higher rates of low birthweight but lower rates of preterm birth compared with White women.
2 Allostatic load refers to the “dysregulation of the stress response process; it is the ‘wear and tear’ on the body that arises from chronic, prolonged or persistent activation of allostatic effectors and a breakdown of the regulatory feedback mechanisms” (Wallace and Harville, 2013, p. 1025).
women across lines of race, ethnicity, social class, education, country of origin, language, ability, and region.
The concept of reproductive justice provides a useful framework to shape the discussion of ethnicity, racism, and birth settings. The reproductive justice framework and movement were started by a group of 12 Black women to address major gaps in reproductive health and rights frameworks that failed to recognize and address the circumstances of women of color and other groups that have often been marginalized and oppressed (Ross, 2017). The reproductive justice framework describes reproductive rights as human rights (Ross and Solinger, 2017). The framework further defines reproductive rights as (1) the right to have children under the circumstances of one’s choosing, (2) the right to not have children using the methods of one’s choosing, and (3) the right to raise one’s children in safe and healthy environments (Ross, 2017). In this way, it centers on access rather than individual choice (Sister Song, n.d.; Ross and Solinger, 2017).
The concept of birthing justice emerged to extend the reproductive justice framework to childbearing. Similar to reproductive justice overall, birthing justice starts from the position that the movement for birthing rights and care options has failed to recognize and address the circumstances of traditionally marginalized and underserved groups, which compound the childbearing challenges faced by more advantaged families (Oparah et al., 2018). Thus, birthing justice is predicated on the idea that while individual choice is necessary, it is not sufficient for just and equitable access and opportunity (Sister Song, n.d.). Research shows, for example, that home birth is on the rise among well-educated, wealthy, and White women (Boucher et al., 2009; MacDorman and Declercq, 2019). However, out-of-pocket costs or locale may put certain birth settings out of reach for socially or financially disadvantaged populations. In such an environment, a reproductive justice framework poses the question, “Do all women really have ‘choice’ of birth setting?” Accordingly, reproductive and birth justice platforms not only advocate for traditional reproductive and birth rights, but also provide a framework that focuses attention on the social, political, and economic inequalities among different communities that contribute to infringements of these rights and constrain choice (Oparah and Bonaparte, 2015).
The birthing justice framework and movement recognize that many disadvantaged women receive substandard maternal care. In particular, they note that the history and current reality of Black women’s receipt of facility-based care in the United States includes lack of access, segregated wards, denial or delays in receiving needed care, biased treatment, and substandard care (Oparah and Bonaparte, 2015). Further, many women of color, women with disabilities, immigrant women, people of varied gender identities and sexual orientations, and other groups lack access to birth options, to quality
TABLE 4-1 Pregnancy and Birth Outcomes by Race, Ethnicity, and Hispanic Origin, 2017
| Race and Hispanic Origin | All | Non-Hispanic White | African American/Black | Alaskan Indian/American Native | Asian |
|---|---|---|---|---|---|
| Demographic | |||||
| Age (years) of mother at first birth | 26.8 | 27.6 | 24.9 | 23.3 | 30.3 |
| Births to unmarried mothers (%) | 39.8 | 28.5 | 69.5 | 69.1 | 11.8 |
| Mother born in the 50 states or District of Columbia (%) | 76.9 | 93.2 | 83.1 | 98.9 | 17.8 |
| Maternal education (%) | |||||
| High school diploma or higher | 86.7 | 92.8 | 86.1 | 78.0 | 93.2 |
| Bachelor’s degree or higher | 32.3 | 41.8 | 17.3 | 8.4 | 64.2 |
| Initiation of prenatal care (%) | |||||
| First trimester | 77.3 | 82.4 | 66.6 | 63.4 | 81.1 |
| Late or no prenatal care | 6.3 | 4.5 | 10.2 | 12.6 | 5.1 |
| Health insurance for delivery (%) | |||||
| Medicaid | 43.0 | 30.5 | 65.9 | 67.3 | 25.0 |
| Private insurance | 49.1 | 63.1 | 27.7 | 19.5 | 65.2 |
| Self-pay | 4.1 | 3.0 | 3.0 | 1.8 | 6.8 |
| Other | 3.8 | 3.4 | 3.4 | 11.4 | 2.9 |
| Infant birth outcomes (%) | |||||
| Preterm gestational age (<37 weeks) | 9.9 | 9.1 | 13.9 | 11.9 | 8.5 |
| Low/very low birthweight | 9.7 | 8.1 | 16.8 | 9.7 | 9.7 |
| Interventions | |||||
| Cesarean birth | 32.0 | 30.9 | 36.0 | 28.5 | 33.2 |
| Low-riska | 26.0 | 24.9 | 30.4 | 22.8 | 27.8 |
| Induction of labor | 25.7 | 28.9 | 23.9 | 26.7 | 20.5 |
| Pregnancy-related mortality per 10,000 births | — | 13.0 | 42.8 | 32.5 | 14.2 |
| Infant mortality rate per 1,000 live births | 5.8 | 4.7 | 11.0 | 9.2 | 3.8 |
aLow-risk cesarean birth rate is the number of singleton, term (37 weeks or more of gestation based on the obstetric estimate), cephalic cesarean deliveries to women having a first birth per 100 women with singleton, term, cephalic deliveries.
SOURCES: Martin et al. (2018b); Centers for Disease Control and Prevention (2019a); Ely and Driscoll (2019).
| Native Hawaiian or Other Pacific Islander | All Hispanic | Hispanic Origin | ||||
|---|---|---|---|---|---|---|
| Mexican | Puerto Rican | Cuban | Central/South American | Other/Unknown Hispanic | ||
| 24.9 | 24.8 | 24.2 | 24.7 | 27.4 | 26.5 | 24.8 |
| 48.7 | 52.2 | 50.2 | 64.2 | 52.5 | 50.5 | 52.9 |
| 36.7 | 52.0 | 55.1 | 71.5 | 43.7 | 16.9 | 68.0 |
| 77.3 | 72.1 | 70.6 | 82.9 | 91.4 | 61.6 | 79.5 |
| 9.7 | 13.5 | 10.5 | 15.8 | 28.1 | 18.4 | 15.7 |
| 52.5 | 72.3 | 72.0 | 76.0 | 82.2 | 67.7 | 74.6 |
| 19.6 | 7.7 | 7.9 | 6.1 | 4.2 | 9.3 | 7.0 |
| 56.2 | 60.2 | 61.7 | 60.1 | 52.7 | 54.7 | 61.6 |
| 28.6 | 28.5 | 27.1 | 34.1 | 43.1 | 26.9 | 29.8 |
| 6.3 | 6.7 | 6.7 | 1.4 | 1.6 | 12.9 | 3.5 |
| 8.9 | 4.7 | 4.5 | 4.4 | 2.7 | 5.5 | 5.1 |
| 10.5 | 9.6 | 9.4 | 11.2 | 9.1 | 9.1 | 10.2 |
| 8.9 | 8.7 | 8.2 | 11.4 | 8.6 | 8.1 | 9.7 |
| 31.0 | 31.8 | 30.4 | 33.9 | 45.8 | 31.3 | 33.9 |
| 26.8 | 25.6 | 24.0 | 27.5 | 39.2 | 26.0 | 26.6 |
| 17.5 | 21.6 | 21.1 | 24.2 | 22.6 | 20.5 | 22.8 |
| — | 11.4 | — | — | — | — | — |
| 7.6 | 5.1 | 5.1 | 6.5 | 4.0 | 4.5 | — |
care, and to care well suited to their needs (Oparah and Bonaparte, 2015, p. 6; Howell et al., 2016; Prather et al., 2018).
In the following section, we consider the birthing justice framework of access with the reality of medical and obstetric risk factors, patterned by the social determinants of health.
STRUCTURAL INEQUITIES AND BIASES
In its conceptual model, the committee recognizes that structural inequities and biases are historically rooted and deeply embedded in policies, laws, governance, and culture, such that power and resources are distributed differentially across characteristics of identity (race, ethnicity, gender, class, sexual orientation, and others), all of which influence health outcomes. Thus, any discussion of risk assessment, choice, and equity in birth settings and birth outcomes must encompass the historical problem of disparate outcomes influenced by structural racism. Disparities and inequities in U.S. health care are well documented across a myriad of chronic medical conditions and mental health disorders (see, e.g., Braveman et al., 2005; Institute of Medicine, 2003). Racism and discrimination—both in the health care system and in everyday life—have a well-documented impact on the health of marginalized communities. The adverse impacts of racism can be manifested in lower-quality health care; residential segregation and lack of affordable housing; acts of state-inflicted violence, punitive policing, and mass incarceration; or the accumulation of daily stressors resulting from micro- and macro-level aggressions, unconscious and conscious bias, and discrimination. They can thereby influence the health outcomes of pregnant people and their infants, causing considerable racial/ethnic disparities in pregnancy-related outcomes (Dominguez et al., 2008).
Moreover, these disparities persist regardless of socioeconomic status (Collins and Hammond, 1996). For example, Black women in the United States had the greatest risk of pregnancy-related mortality from 2011 to 2015, with a mortality ratio of 42.8 per 100,000 live births, followed by AIAN women at 32.5 (Centers for Disease Control and Prevention, 2019a), while the ratio for non-Hispanic White women was 13.0. As discussed earlier in this chapter, non-Hispanic Black women have higher rates of preterm labor (13.9%), low/very low fetal birthweights (16.8%), and infant mortality (11 per 1,000 live births) compared with non-Hispanic White women (refer to Table 4-1). Neither material conditions nor adverse maternal and child outcomes by race and ethnicity have changed significantly over the past four decades (Zambrana et al., 1999). These disparities in outcomes likely arise through a number of mechanisms. Below, we detail inequitable treatment in the health care system, the health effects of racism and discrimination, inequitable allocation of resources, and racism as risk.
Inequitable Treatment in the Health Care System
In the health care system, racism frequently manifests in differences in care. Individuals from racial/ethnic minority groups and of lower socioeconomic status tend to receive lower-quality health care than their White and high-status counterparts, even when issues of access are addressed (Agency for Health Research and Quality, 2018; Howell and Zeitlin, 2017; Fiscella and Sanders, 2016; Institute of Medicine, 2003; Anderson et al., 2003). This discrepancy has been documented throughout the health care system (Anderson et al., 2003), including in maternity care (McLemore et al., 2018; Braveman et al., 2010).
Over the past two decades, researchers have documented forms of disrespect and abuse in maternity care (Abuya et al., 2015; Okafor et al., 2015; Sando et al., 2016; Ishola et al., 2017). The term “obstetric violence” was introduced into the discourse on maternal experiences of birth in Latin America in the early 1990s, and was used to help shape discussions of disrespect and abuse within the larger frameworks of structural and gendered violence (Sadler et al., 2016). The term is intended to convey the assertion that the acts it denotes are inadequately captured by other terms such as “maternal dissatisfaction” or “negative birth experiences.”
Until relatively recently, mistreatment during labor and birth was assumed to be a problem unique to the global south and/or low-resource systems. Today, however, it is better understood that various forms of disrespect and abuse can also occur in high-resource countries, including the United States, and that rates and types of mistreatment vary by birth setting and by maternal race/ethnicity (Childbirth Connection, 2013; see also Chapter 3). The Listening to Mothers III survey found, for example, that approximately one in five Black and Hispanic women experience mistreatment from hospital-based care providers due to their race, ethnicity, cultural background, and/or language. Compared with 8 percent of White mothers, 19 percent of Hispanic mothers and 21 percent of Black mothers reported poor treatment while hospitalized to give birth (Childbirth Connection, 2013, p. 5). In an article published in 2018, anthropologist Dana-Ain Davis analyzes the birth stories of Black women in the United States. Participants’ narratives describe multiple forms of racism encountered over the course of care, leading Davis to argue that the term “obstetric racism” (as opposed to obstetric violence) better captures the particularities of Black women’s experiences of prenatal, intrapartum, and postpartum care. Black women see obstetric racism as a threat to positive birth outcomes. In response, some attempt to mitigate their risk of obstetric racism by utilizing midwives and doulas and avoiding the hospital when home and birth center birth services are available (Davis, 2018).
In the hospital setting, racial/ethnic minority patients are reported to experience the most palpable discrimination and lack of clinical attention, and often face the worst clinical outcomes (Sperlich et al., 2017). Women of color have contributed their own stories of mistreatment, bias, and discrimination in the maternity care system. For example, in a recent survey of 2,700 women from a nonrepresentative sample, one-third of women of color who had given birth in a hospital setting reported being mistreated by staff, compared with fewer than one-sixth of White women (Vedam et al., 2019). Mistreatment ranged from violations of physical privacy to being threatened or refused treatment by birth attendants.
In addition to these types of blatant and intentional acts of discrimination, racism may impact the quality of care through implicit bias or poor cross-cultural communication, which itself is a form of bias and discrimination. The way providers perceive their patients’ ability to manage pain is influenced by the patient’s perceived race and ethnicity and gender, and physicians and other members of the care team may better understand and pick up on implicit cues from patients who share their racial and gender identities (Institute of Medicine, 2003). This could help explain the disparities in epidural use in the United States: White women have the highest rate of epidural use (68.6%), followed by Black women (62.1%), Asian women (61.8%), Native Hawaiian and Other Pacific Islander women (52.8%), Hispanic women (47.7%), and AIAN women (42.1%). Although medical researchers have interpreted differences in epidural use by ethnicity and perceived race as an issue of access, limited research has been performed on the tertiary factors that may contribute to these discrepancies, including patient–provider communication, perceived pain tolerance among members of minority groups, and increased pressure from physician recommendations around whether pain medication is needed (Morris and Schulman, 2014). Patient–provider trust may also play a role. The relationship between patients and providers is often mediated by provider attitudes regarding socioeconomic status, race, and ethnicity. Low-income women are less likely to develop patient–provider trust and communication, increasing the risk for adverse birth outcomes (Sheppard et al., 2004). Provider concordance may play a role as well. There is evidence to suggest that patients in racially concordant relationships are more satisfied with their care and communication (Cooper et al., 2003). However, because of the relative dearth of obstetricians and midwives of color, there is not a robust literature examining the impact of racial concordance on pregnancy care. This raises the critical need to diversify the maternity care workforce, which is discussed at greater length in Chapter 7.
Health Effects of Racism and Discrimination
Racism has also been hypothesized to impact pregnancy and birth outcomes through greater exposure to chronic stress (Giscombé and Lobel, 2005; Nuru-Jeter et al., 2008). Although chronic stress can cause health problems in people of all racial/ethnic backgrounds, racial/ethnic minority individuals may experience unique stressors, such as racial discrimination, or common stressors, such as economic adversity and trauma, at higher rates. For example, in addition to stress related to racial discrimination, low-income women of color may experience stress related to limited economic security, limited childcare availability, the cost of health services, inadequate family and social support, the need to continue working during pregnancy to support the family financially, and other psychological stressors, all of which contribute to negative health outcomes (Dominguez et al., 2008; Lobel et al., 1992; Hogue and Bremner, 2005). Further, the communal impact of mass incarceration, state-imposed violence, policing, and detainment on pregnancy outcomes remains unclear and warrants further research.
Such chronic stress can lead to greater wear and tear, or weathering, on the body and brain as environmental factors “get under the skin,” a concept known as allostatic load (Geronimus, 2002; Seeman et al., 1997; McEwen and Seeman, 1999). As these daily stressors build up and allostatic load increases, cellular aging speeds up, heightening vulnerability to stress-related health conditions, such as diabetes (Alhusen et al., 2016; Rubin, 2016). The higher allostatic load caused by racism is hypothesized to degrade the reproductive health of people of color, making it more difficult for individuals to enter pregnancy healthy. In effect, chronically high levels of interpersonal and systemic discrimination and prejudice can adversely impact pregnancy morbidity, health behaviors, and childbirth outcomes of these target groups (Giurgescu and Misra, 2018; Provenzi et al., 2018; Lima et al., 2018). Evidence suggests that this reflects the embodiment of stress resulting from structural inequity and the physiologic response to systemic racism (see, e.g., Geronimus, 1992; Lobel et al., 1992; Domingez et al., 2008).
Inequitable Allocation of Resources
In addition to the daily stressors due to experiencing racism, the inequitable distribution of societal resources and attention may negatively impact a woman’s chances of entering pregnancy and childbirth healthy. This inequitable distribution is the result of a long history of legal (and other) mistreatment of members of relevant social groups. Many women of color and with low incomes have limited education; lower health literacy
and knowledge of birth options, including less access to shared decision making; and less access to quality resources such as housing, a living wage, employment, and social services. Thus these women experience the cumulative impact of multiple and chronic stressors. Racial discrimination can be one mechanism by which access to material resources and services that promote health, such as prenatal care, is reduced (National Academies of Sciences, Engineering, and Medicine, 2019). For example, AIAN, Native Hawaiian, and non-Hispanic Black women are least likely to receive prenatal care in the first trimester and most likely to receive late or no care compared with non-Hispanic White women. They are also most likely to rely on Medicaid as their principal source of payment for birth services, followed by Latina women (refer to Table 4-1).
Racism as Risk
As a result of inequitable treatment; chronic stressors, weathering, and intergenerational trauma; and inequitable distribution of resources, women of color enter into their reproductive lives, and ultimately their pregnancies, at risk for adverse pregnancy outcomes. The label “Black,” for example, although a social construct and not a marker of genetic difference, has served as a risk factor for almost all poor obstetric outcomes, when in fact, it is racism, not race, that increases Black women’s risk. While compounding social disadvantages with financial disadvantage means that low-income women of color face health challenges, it is critically important that membership in a specific perceived racial/ethnic group not be used to overdetermine a given patient’s risk assessment such that it alone constrains the birth setting or maternity care provider options made available. Thus while properly assessing medical risk and monitoring for medical and/or obstetric complications among women of color is critical, ethnicity or perception of race alone should not determine level of risk. In fact, there is evidence to suggest that socially and financially disadvantaged women may thrive in midwifery models of care across all birth settings (Raisler and Kennedy, 2005; Huynh, 2014; Hill et al., 2018; Hardeman et al., 2019). The woman-centered philosophy of care that characterizes these models affirms agency among women of color, and group prenatal care models offer needed social support. Thus these models likely mitigate the harmful impact of medical models that have historically failed to trust the competence and capabilities of women, particularly Black women, including the experiences of disregard and disrespect described by many Black women in traditional care (Huynh, 2014; Vedam et al., 2019; Yoder and Hardy, 2018; Davis, 2018).
The available evidence is inadequate to determine health outcomes among women of color associated with home and birth center births or with hospital births that follow the midwifery model of care. Until more
data are available to guide policy, there may be important opportunities to integrate midwifery models of care and doulas (dedicated support persons for laboring women) for labor support into hospital-based delivery settings. Doing so would enable women of color, particularly those with elevated medical, social, or obstetric risk factors, to still garner the benefits of woman-centered midwifery models of care and labor support.
In summary, racism and racial discrimination, whether manifested in the health care system, through chronic stress, or in reduced access to services, has tangible impacts on the lives of women of color and their families, impacts that are seen in racial/ethnic disparities in adverse birth outcomes.
SOCIAL DETERMINANTS OF HEALTH
The medical and obstetrical risk factors discussed in Chapter 3 must be understood in the context of the social determinants of health, the “upstream factors that shape behavior and influence health” (National Academies of Sciences, Engineering, and Medicine, 2019, p. 81). The word “determinants” in this context should be interpreted as mutable influencing factors, factors that can be changed through social and economic actions. These upstream factors are related to social identity and structural inequity. A previous National Academies report, Communities in Action: Pathways to Health Equity, states:
The dimensions of social identity and location that organize or “structure” differential access to opportunities for health include race and ethnicity, gender, employment and socioeconomic status, disability and immigration status, geography, and more. Structural inequities are the personal, interpersonal, institutional, and systemic drivers—such as, racism, sexism, classism, able-ism, xenophobia, and homophobia—that make those identities salient to the fair distribution of health opportunities and outcomes. Policies that foster inequities at all levels (from organization to community to county, state, and nation) are critical drivers of structural inequities. The social, environmental, economic, and cultural determinants of health are the terrain on which structural inequities produce health inequities. These multiple determinants are the conditions in which people live, including access to good food, water, and housing; the quality of schools, workplaces, and neighborhoods; and the composition of social networks and nature of social relations (National Academies of Sciences, Engineering, and Medicine, 2017, pp. 100–101).
When discussing the social determinants of health, it is important to consider a life-course perspective. The relationship between social factors and health is not one of a series of discrete steps, but rather an integrated continuum of exposures, experiences, and interactions over a lifetime
(Mullings and Wali, 2001; Fine and Kotelchuck, 2010; Braveman et al., 2005). In addition, using an intersectional community-driven lens helps explain the individual, community, environmental, and policy spheres influencing adverse health outcomes across populations and over time.
While there is a growing body of literature on the social, economic, and environmental determinants of health and their impacts on health outcomes, establishing causality is challenging because the evidence is often in the form of cross-sectional analyses, and the pathways to health outcomes are not always clearly delineated. This may be due, in part, to the complexity of the mechanisms involved and the long time periods required to observe outcomes (Braveman and Gottlieb, 2014; Braveman et al., 2011; Marmot et al., 2010; National Academies of Sciences, Engineering, and Medicine, 2017). That said, new methods and frameworks are emerging in the literature to better understand causality amidst complex exposures.
In pregnancy and childbirth, the social determinants of health may be reflected in a woman’s knowledge of prenatal care (individual); the amount of support she receives from her family, friends, and community (social); experiences with racism and other social and environmental stressors (social); the way she is treated by her care provider (institutional); and the policies and practices of her insurer (systemic). The committee’s approach to understanding the social determinants of health in maternity care is illustrated in its conceptual framework (Figure 1-7 in Chapter 1). The figure shows the social determinants—such as housing, transportation, and education—that influence experiences in the maternity care system for women and infants. It also illustrates how structural inequities and biases, such as institutional racism, underlie the social determinants of health for women from marginalized populations. Although the committee’s conceptual framework focuses primarily on the prenatal and intrapartum periods, it is important to note that the social determinants of health affect women’s well-being throughout their lives, not just during pregnancy and childbirth.
Of course, each level of influence may occur simultaneously and interact with other levels (National Research Council, 2006). The disadvantages that members of historically marginalized social groups confront in the contemporary United States are not isolated; rather, they tend to cluster and are intergenerational, impacting life-course social and economic opportunities and health outcomes. In other words, people who are at a disadvantage in terms of, for example, socioeconomic status are also at a disadvantage in terms of educational attainment, where they live, where they work, and where they play—all of which impact health outcomes. Furthermore, these disadvantages are not ahistorical; rather, they are part of a long history of legal (and other) mistreatment of members of the relevant social groups.
A vast literature documents a host of social determinants of health associated with poor pregnancy outcomes (Chisholm et al., 2017; Blumenshine
et al., 2010; Lu and Halfon, 2003; Lobel et al., 1992; Collins et al., 1993). These social determinants impact a woman’s health and the health and well-being of her child, possibly for years to come. We detail the specific influences of interpersonal relationships and social support, transportation, employment status, and housing below.
Interpersonal Relationships and Social Support
Intimate Partner Violence
Nationwide, an estimated 2 percent of U.S. women experience violence in a given year, and one in four women experience violence in their lifetime (Tjaden and Thoennes, 2000). Black women, low-income women, and young women (ages 20–34) are at the greatest risk of abuse from intimate partners (Aizer, 2011). Some studies suggest that violence may start or escalate during pregnancy or the postpartum period, with prevalence rates of intimate partner violence during pregnancy estimated to range from 3.9 to 8.3 percent (Brownridge et al., 2011).
Intimate partner violence both before and during pregnancy is associated with a host of negative maternal and infant outcomes, including maternal and fetal injury, elevated maternal stress, inadequate gestational weight gain and nutrition, substance use, and elevated risk of low-birthweight and preterm birth, among others (American College of Obstetricians and Gynecologists, 2012; Alhusen et al., 2015). The health effects of violence on pregnant women can be direct and immediate (such as injuries associated with blunt trauma to the maternal abdomen) and indirect and downstream (such as exacerbation of chronic illnesses and delayed initiation of prenatal care) (Alhusen et al., 2015). Assaults serious enough to require hospitalization during pregnancy are associated with an average decrease in birthweight of 163 grams (Aizer, 2011).
Women experiencing intimate partner violence during pregnancy need additional support from their health care providers and referrals to community resources (American College of Obstetricians and Gynecologists, 2012). Moreover, having a trusting relationship with care providers during pregnancy may mitigate the adverse effects of violence for both the woman and her infant (Alhusen et al., 2015). Accordingly, women who experience intimate partner violence may be better served in birth settings that allow for greater relationship building between providers and the women they serve.
Moreover, the experience of violence or trauma earlier in life can impact the health of women during pregnancy. Posttraumatic stress disorder, a manifestation of previous traumatic stress, has been associated with increased odds of low birthweight, preterm birth, and pregnancy complica-
tions (Seng et al., 2001, 2011; Sperlich et al., 2017). Women with trauma histories and their partners may benefit from trauma-informed approaches to maternity care (Sperlich et al., 2017).
Social Support
The support of family, partners, friends, and systems during pregnancy and childbirth is associated with a host of positive maternal and infant health outcomes. Providing social support during pregnancy to women who need it may reduce the risk of such adverse birth outcomes as preterm birth, low birthweight, and postpartum depression (Collins et al., 1993). A recent Cochrane review found that programs offering additional social support to women at risk of having a low-birthweight infant reduced the risk of hospitalization during pregnancy and cesarean birth. Such programs also slightly reduced the risk of low birthweight and preterm birth among at-risk women (East et al., 2019).
One of the most typical sources of social support during pregnancy is partners, friends, and family members. Among family members, female relatives such as mothers, grandmothers, and sisters can provide needed material and emotional support. However, for some, these sources of support may be disrupted by larger societal trends, such as the rise of mass incarceration. Over the past 50 years, incarceration in the United States has increased on a large scale, and the effects have been felt most acutely in low-income Black and Latino communities (National Research Council, 2014). Women from communities with high rates of incarceration may lose access to important sources of social and material support during pregnancy if they or their loved ones are incarcerated. In an analysis of data from the Pregnancy Risk Assessment Monitoring System (PRAMS), Wildeman (2012) found that having an incarcerated father substantially increased the odds of infant mortality for his offspring, although this relationship was modified by whether the parent was abusive (see the above section on intimate partner violence for a more detailed discussion of the effect of violence on pregnancy outcomes). Another analysis of PRAMS data, conducted by Dumont and colleagues (2014), found that women who had an incarcerated partner or were incarcerated themselves in the year prior to birth were less likely to begin prenatal care in the first trimester or receive at least nine prenatal visits and were more likely to experience stressful events (e.g., homelessness or job loss). In short, women who experience incarceration are at greater social risk, which can translate to greater clinical risk for themselves and their infants.
For women with greater social risk, providing sources of support, whether through a doula, a community health worker, friends, family members, or a group prenatal care model, may be an effective interven-
tion, regardless of setting. Providing low-income women with doulas has been shown to contribute to positive health outcomes, improved patient–provider relationships, improved adherence to medical advice, and increased satisfaction (Wint et al., 2019; Hardeman and Kozhimannil, 2016). One program in New York City pairs low-income Black and Latina women with a certified doula (Thomas et al., 2017). In addition to providing direct labor support during the intrapartum period, the doulas provide case management services (e.g., screening for depression, food insecurity, and intimate partner violence and making referrals to services when necessary) and prenatal education over the course of seven home visits (three prenatal and four postpartum). Women who received these enhanced doula services had lower rates of preterm birth and low birthweight compared with women in the same neighborhood who did not receive those services (Thomas et al., 2017). (See Chapter 5 for additional discussion of outcomes and doula services.)
Community health workers can also serve as a source of social support as well as outreach, education, and informal counseling for pregnant people (American Public Health Association, 2019). In the Safe Start program in Philadelphia, for example, community health workers engaged pregnant women with high clinical risk factors in care navigation. Women in the program had substantially lower odds of inadequate prenatal care, inpatient admission, and emergency room visits, and higher odds of attending their postpartum visit and using contraception postpartum (Srinivas et al., 2019). In addition, group prenatal care models, such as CenteringPregnancy, have been shown to reduce stress and psychosocial risk factors among women with the highest levels of self-rated stress (Ickovics et al., 2011).
Transportation
For decades, transportation has been identified as a potential barrier to accessing prenatal care, especially for low-income and rural women (Institute of Medicine, 1985, 1988). When transportation is limited, unavailable, unaffordable, or difficult to use, women have greater difficulty accessing prenatal care (Heaman et al., 2015). For women in rural areas, the time and distance needed to travel to prenatal care visits may be challenging, particularly if women need to access specialty care in urban areas far from home (Leighton et al., 2019). In urban areas, transportation challenges such as traffic congestion, accessibility of public transit, and ease of using public transit while pregnant or with small children may also create barriers to accessing prenatal care (Heaman et al., 2015; Institute of Medicine, 1988). Disruptions to public transit service may create accessibility challenges as well. For example, in spring 1992, the drivers of the public transit system serving Allegheny County, Pennsylvania, engaged in a 4-week labor strike,
causing severe service disruptions (Evans and Lien, 2005). During this time, researchers documented a decrease in the number of prenatal care visits among pregnant women in the area. Women who relied most heavily on public transportation—city residents and Black women—had the greatest reduction in prenatal visits. Among these women, researchers identified lower average birthweights, shorter gestations, and higher rates of smoking during pregnancy (Evans and Lien, 2005).
However, transportation, like the other social determinants of health, is modifiable. Programs that aim to provide available, reliable, and affordable transportation to pregnant people show some promise in increasing use of prenatal care. In a novel pilot program in Columbus, Ohio, pregnant women and new mothers can request on-demand transportation to health clinics, grocery stores, and other important locations using a mobile application similar to popular ridesharing services (The City of Columbus, 2019).
Employment Status
Among social determinants, the workplace and related social policies play a major role in maternal well-being and ability to care for infants (National Partnership for Women & Families, 2018a), as well as reproductive health at a population level. During adolescence, for example, having access to positive educational, social, and employment opportunities can promote healthy growth and development (National Academies of Sciences, Engineering, and Medicine, 2019). These opportunities can also help prevent pregnancy and childbearing during the teenage years (Romero et al., 2016). Although teen pregnancy rates have decreased substantially since the 1990s, rates remain high for youth of color, who are more likely to live in communities with limited educational and employment opportunities, a key social determinant of teenage pregnancy (Romero et al., 2016; National Academies of Sciences, Engineering, and Medicine, 2019).
Specific to pregnancy and childbirth, access to paid parental leave and paid sick days promotes maternal and infant health during pregnancy and through early life. While such access is slowly expanding in the United States (National Partnership for Women & Families, 2018b), it is not available to a large segment of the workforce (Bureau of Labor Statistics, 2019).
In addition, access to workplace protections and exposure to harmful occupational situations is unevenly distributed in the United States, with low-wage, part-time, shift, and self-employed workers, among whom Black women are disproportionately represented, being much less likely to have workplace protections and benefits compared with their more advantaged counterparts (National Partnership for Women & Families, 2018c; Office of the Assistant Secretary for Planning and Evaluation, 2014; Presser,
2003). Indeed, rotating shift work, night shift work, and long work hours themselves pose pregnancy risks (Cai et al., 2019). Moreover, economic security is an important contributor to health and well-being, especially during pregnancy, and women in general experience lower pay relative to their male counterparts, with women of color shouldering greater burdens than White women (National Partnership for Women & Families, 2019a).
Housing
Housing, which includes “the availability or lack of availability of high-quality, safe, and affordable housing for residents of varying income levels,” as well as the environments that surround it, has been widely recognized as a social determinant of health (National Academies of Sciences, Engineering, and Medicine, 2017, p. 140). Stable, affordable housing is hypothesized to affect health through several possible mechanisms, including freeing up family resources to afford health expenditures or nutritious food, reducing the stress associated with unstable housing, and improving the safety and quality of the indoor environment, among others (Maqbool et al., 2015). In the United States, access to stable, affordable, and safe housing has historically been limited for African Americans and other racial/ethnic minority groups by discriminatory practices. Housing instability has no one definition but is thought to encompass having difficulty paying housing costs, spending greater than 50 percent of household income on housing, frequent moves, overcrowding, or living temporarily with relatives or friends (Kushel et al., 2006). One estimate places the prevalence of homelessness among pregnant women at 4 percent nationwide, based on data from the PRAMS (Richards et al., 2011).
In studies of reproductive-age women, homelessness and housing instability have been associated with adverse neonatal outcomes. In one study of 613 low-income pregnant women and teenage girls receiving prenatal care in New York City, housing instability was independently associated with low birthweight, even after controlling for clinical, behavioral, and demographic factors (Carrion, 2015).
Other studies of pregnant women who experienced homelessness show a relationship between maternal homelessness and maternal and infant health outcomes. Richards and colleagues (2011), using data from the PRAMS, found that women experiencing homelessness, as compared with women with stable housing, were significantly less likely to receive prenatal care in the first trimester or receive a well-baby checkup. Moreover, the infants of women experiencing homelessness had significantly longer hospital stays and lower birthweights compared with those women with stable housing. A study of nearly 4,000 women experiencing homelessness in Toronto, Canada, found that women who experienced homelessness had an almost
three times greater risk of preterm birth and an almost seven times greater risk of low birthweight (Little et al., 2005). The authors note that these increased risks occurred within a setting where health care is universally available (Little et al., 2005).
Housing may affect the health of pregnant women and their offspring through several mechanisms. Pregnant women experiencing homelessness face substantial barriers to prenatal care (Bloom et al., 2004) and adequate nutrition (Little et al., 2005), both of which may contribute to adverse birth outcomes. In addition, the stress associated with homelessness and housing instability has been associated with a greater risk of low birthweight and preterm birth (Dunkel-Schetter and Tanner, 2012). The external environment or neighborhood surrounding housing can also impact pregnant people’s health (National Academies of Sciences, Engineering, and Medicine, 2017). For example, the neighborhood food environment, which refers to “the availability of food venues such as supermarkets, grocery stores, corner stores, and farmer’s markets, including food quality and affordability,” can support a person’s ability to afford and maintain a healthy diet (National Academies of Sciences, Engineering, and Medicine, 2017, p. 145). Given the importance of nutrition during pregnancy for both maternal and child health, programs and interventions to support women’s access to nutritious food, such as the Special Supplemental Nutrition Program for Women, Infants, and Children, can positively impact birth outcomes (National Academies of Sciences, Engineering, and Medicine, 2019).
HEALTH SYSTEM: POLICY AND FINANCING
Operating within the context of structural inequities and biases and social determinants of health is the health system. In this section, we explore the innermost circle of our conceptual model, the health system, and its role in the patterns of women’s risk in pregnancy and childbirth. The health system, writ large, includes the geographic distribution of the health care workforce; the certification, licensure, and scope of practice of that workforce; the financing of maternity care services; and the resultant access to services for the population. In maternity care, these features of the health system can contribute to a woman’s risk profile in pregnancy and birth. We discuss these features of the health care system in detail below.
Geography and Workforce Distribution
Notable disparities in maternal health by geography persist in the United States. For example, women living in rural communities have greater risks of such poor outcomes as preterm birth and maternal and infant mortality, likely because of lack of access to maternity and prenatal care in
their local areas (Grzybowski et al., 2011). These statistics are especially troubling considering that 15 percent of U.S. births are to women living in rural communities (Kozhimannil, 2014).
One driver of the disparities in maternal and neonatal health by geography in the United States is likely the uneven distribution of maternity care facilities and providers throughout the country, which leaves many women without access to prenatal and postpartum care, and without birthing options near home. Many rural—and even some urban—areas lack maternity care providers and hospitals with maternity units. A “maternity care desert,” as defined by the March of Dimes, is a county in which maternity care services are limited or absent because of either a lack of services or barriers to a woman’s ability to access those services (March of Dimes, 2018a). Women living in these counties have limited access to appropriate preventive, prenatal, and postpartum care. All told, as many as 5 million women live in these maternity care deserts. Figure 4-1 shows the number of hospitals with maternity units by U.S. county.
Closures of hospitals in rural and underserved urban areas may also contribute to disparities in outcomes by geography. These closures are the result of a confluence of factors, including the complex fixed and variable
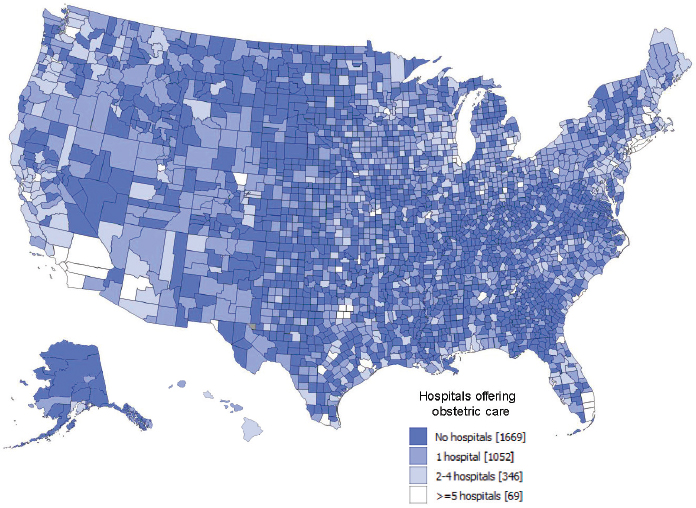
SOURCE: March of Dimes (2018a).
costs associated with labor and delivery units, compounded by low patient volumes and low Medicaid reimbursement levels (Hung et al., 2016).
Rural areas have been losing hospitals steadily, with 179 hospitals in rural counties closing between 2004 and 2014. When rural counties are not adjacent to urban areas, the consequences of these closures are clear: an increase in unattended out-of-hospital births, preterm births, and births in hospitals without maternity units (Kozhimannil et al., 2018a). From 2004 to 2014, the total percentage of rural counties in the United States with hospital-based maternity care services declined from 55 percent to 46 percent (Kozhimannil et al., 2018a). All counties experiencing closures of hospital-based maternity units saw significant increases in the number of births occurring in hospitals without a maternity unit. In addition, closures of hospital maternity care units in urban underserved communities often result from high costs and economic pressures. In 2017, for example, the only two maternity care units on the east side of Washington, DC, closed their doors, leaving the predominantly Black and largely low-income population, with limited public transportation services, to find care elsewhere (Itkowitz, 2017). Moreover, hospital closures appear to be associated with decreased use of outpatient prenatal care services, suggesting that when hospitals leave, local prenatal care services follow (Kozhimannil et al., 2018a; Shah, 2018). The lack of access to prenatal care services may be one reason why initiation of prenatal care tends to be later among rural than urban women (American College of Obstetricians and Gynecologists, 2014). Delayed prenatal care has been associated with greater risk of preterm birth, which is of particular concern in rural areas, where the nearest hospital with a neonatal intensive care unit may be hours away (Shah, 2018).
In addition to the lack of available birthing facilities in certain regions of the country, both rural and urban areas are affected by the maldistribution of maternity care providers (see Figure 4-2). In 2016, almost one-half of all counties in the United States were without an obstetrician, and 40 percent had neither an obstetrician nor a certified nurse midwife, largely because they lacked hospitals with maternity services (March of Dimes, 2018a).
Of greatest concern is the relationship between inadequate access to care and the observed increased rates of prematurity following service closures in the more geographically isolated counties. Even after adjusting for maternal age, race/ethnicity, education, and common clinical conditions at the county level, a significant association with increased prematurity remains, with a 0.67 percentage point (95% confidence interval [CI], 0.02–1.33) increase in the year after closure (Kozhimannil et al., 2018a). Particularly concerning is the reduced access to prenatal care among birthing families in the period following service closure. Studies of workforce density have shown that rural counties without hospital obstetric services
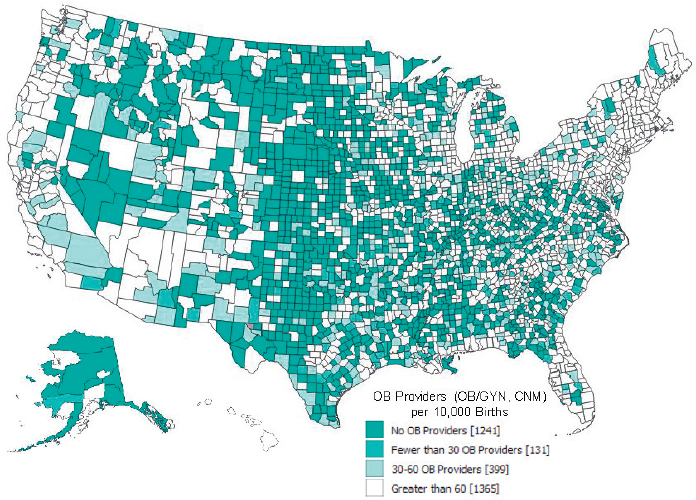
SOURCE: March of Dimes (2018a).
are also likely to lack an obstetric workforce, including obstetricians, midwives, and family practice physicians (American College of Obstetricians and Gynecologists, 2014).
Some programs have attempted to address the challenge of providing prenatal care services in rural areas by adapting existing models to suit rural settings. For example, providers of the CenteringPregnancy group prenatal care model in South Carolina found that the program had difficulty engaging and retaining women from rural parts of the state (Centers for Medicare & Medicaid Services, 2019). In response, the program implementers adjusted the CenteringPregnancy model to increase its sustainability among rural programs, which see a lower volume of pregnant women. Program implementers also sought grant funding to support free technical assistance for programs in rural areas. Participants in the program, including rural women, have reduced rates of preterm birth, low birthweight, cesarean sections, and gestational diabetes (Centers for Medicare & Medicaid Services, 2019).
Other systems attempt to address geographic challenges by bringing women to maternity care services. Alaska, for example, has the highest proportion of out-of-hospital births in the country (out-of-hospital births make up 7.9% of all births, compared with 1.6% of births nationwide). Of these births, 5.6 percent occur in birth centers, while 1.9 percent occur
in homes. Although the vast majority of births in Alaska are to women living in urban areas, such as Anchorage and Fairbanks, about one-fifth of births are to women who reside outside of these population centers (Alaska Department of Health and Social Services, 2019). If these women have complicated pregnancies or live in remote areas that lack any birthing facilities, they must travel—often long distances—to reach hospitals and specialists equipped to care for them and their newborns (Association of State and Territorial Health Officials, 2015).
Alaska’s perinatal regionalization system attempts to address the state’s geographic challenge by transporting women to settings with appropriate care. In remote areas, healthy women leave their home communities between 34 and 36 weeks of pregnancy to deliver safely at a regional medical center. Women with more urgent needs for care may travel by ambulance, helicopter, or fixed-wing aircraft to reach appropriate care, and are accompanied by a perinatal transport team that consists of a neonatal nurse practitioner and a registered nurse (Association of State and Territorial Health Officials, 2015). Women who require ongoing treatment from perinatal and neonatal specialists may be transferred by air ambulance to Anchorage, or may move there early in their pregnancy to receive care (Association of State and Territorial Health Officials, 2015). Although this system is successful in bringing women to needed care, it can impose psychosocial and cultural costs on women. For example, Indigenous women may highly value giving birth on their ancestral lands and dislike having to leave their home communities to give birth (Kornelsen et al., 2010; see also the Chapter 3 discussion of preferences in birth setting).
Solutions for addressing the challenges of the women’s health care workforce have been proposed. Increasing the number of advanced practice providers working in maternity care is a common recommendation across multiple sources. For example, the American College of Obstetricians and Gynecologists (ACOG) estimates that having nurse practitioners, certified nurse midwives, and physician assistants join OB/GYN practices would meet the demands of women in the future (Rayburn, 2017). Moreover, it may be beneficial to create models that expand family physicians’ participation in maternity care and provision of laborist care within hospital and micro-hospital settings, as well as provide midwifery care for low-risk women in home and birth center settings (Avery et al., 2018).
Another potential solution is to increase the number of midwives and freestanding birth centers in rural areas, thereby lowering costs while providing quality care (Centers for Medicare & Medicaid Services, 2019). Rural areas that have experienced the closure of hospital maternity units have had increased out-of-hospital births and births in hospitals without maternity care units (Kozhimannil et al., 2018a). Collaboration between rural home/birth center providers and local hospitals is critical so that
coordinated and seamless transfers can occur when necessary. In addition, family physicians play an important role in providing health care in rural areas (Goldstein et al., 2018), including providing the majority of hospital-based maternity care services in those areas (Young, 2017). Despite their importance to rural communities, however, family physicians may face challenges in obtaining hospital privileges to perform cesarean births and building collaborative relationships with other maternity care providers (Eden and Peterson, 2018). Moreover, rural hospital closures may limit their ability to provide full-scope maternity care services.
There is also concern over the lack of diversity in the maternity care workforce. ACOG found in 2017 that 58.7 percent of obstetricians were female, and the majority of them were White, while Black and Hispanic obstetricians currently in the workforce were underrepresented relative to the general population (Rayburn, 2017). This finding reflects the lack of diversity within the maternity care workforce as a whole. For example, 61 percent of all nurse practitioners are non-Hispanic White, as are more than 80 percent of certified nurse midwives in California (Spetz et al., 2018). Limited data on the demographic distribution of licensed doulas are available, but it is widely acknowledged that this profession is disproportionately represented by White women (Lantz et al., 2005). The lack of physicians, nurses, and allied health professionals of color is a longstanding workforce issue in maternity care and health care generally (Xue and Brewer, 2014).
Workforce Certification, Licensure, and Scope of Practice
In addition to the workforce distribution issues discussed above, recent analyses have identified concerns about the supply of maternity care providers—specifically obstetricians—available to meet demand in the United States. Although obstetricians are just one type of provider of maternity care in the United States, they are the focus of the majority of data collected on maternity care providers. Accordingly, the gap in the obstetrician workforce is the most available means of estimating the projected gaps in maternity care providers as a whole. A 2016 report from the National Center for Health Workforce Analysis highlights the future of providers of women’s health services, noting that the numbers of both obstetricians and family physicians in the United States are declining. Factors contributing to this decline include early retirement from obstetrics, changing practice patterns (e.g., part-time practices), growing subspecialization, and the increasing value placed on work–life balance (Rayburn, 2017). According to the Health Resources and Services Administration’s (HRSA’s) Health Workforce Simulation Model (2016), the number of obstetricians is expected to decrease by about 4 percent (from 41,720 to 40,230 full-
time equivalents [FTEs]), while total demand is expected to increase by 8 percent (from 41,720 to 45,160 FTEs), based on the assumption that the current rates of retirement and workforce participation will hold over the next decade. Notably, ACOG similarly anticipates large numbers of retirements given that in 2009, on average, male OB/GYNs retired from the obstetrics portion of their practice at age 52 and female OB/GYNs at age 44. Retirements may also be prompted by financial and work–life balance concerns within the workforce (Rayburn, 2017). Additionally, the number of family physicians providing maternity care has declined. The proportion of U.S. family physicians reporting providing maternity care declined from 23.3 percent in 2000 to 9.7 percent in 2010, and those who reported providing such care spent an average (aggregated over 2000 to 2010) of 10 percent of their time doing so (Tong et al., 2012).
Given these trends, the United States will increasingly need to rely on other advanced practice providers for maternal health services, including certified nurse midwives, certified midwives, certified professional midwives, physician assistants, and women’s health nurse practitioners. Although evidence on certified midwives and certified professional midwives is more limited, their skills are needed to close the workforce shortages that the United States faces. However, an important barrier exists to increasing the supply of those providers with respect to their ability to be credentialed in some jurisdictions and have practice privileges in some facilities. As noted in Chapter 2, states are responsible for licensing health care professionals and for dictating where they can practice, what services they can provide, and whether they are required to be supervised. The wide variation in regulation, certification, and licensing for nonphysician providers across the United States impedes access to high-quality maternal care for all women, as these providers could prove invaluable in addressing workforce shortages and the maldistribution of other providers if the health care system facilitated their growth and practice. For example, if certified nurse midwives and nurse practitioners were permitted to practice to the full extent of their education and training in all jurisdictions, they could greatly alleviate the shortage of maternity care providers, and could improve access to care for women across the country (see, e.g., Institute of Medicine, 2011; Buerhaus, 2018).
Further limiting access is that not all states license birth centers. Currently, this is the case in nine states (see Figure 4-3). Licensing statutes in those states that have them are generally written with great specificity, designed to ensure that planned births in birth centers are limited, to the extent feasible, to healthy, low-risk women, and that midwives provide care that keeps their clients healthy and continually assess and identify problems early so they can be properly and promptly addressed (American Public Health Association, 1982).
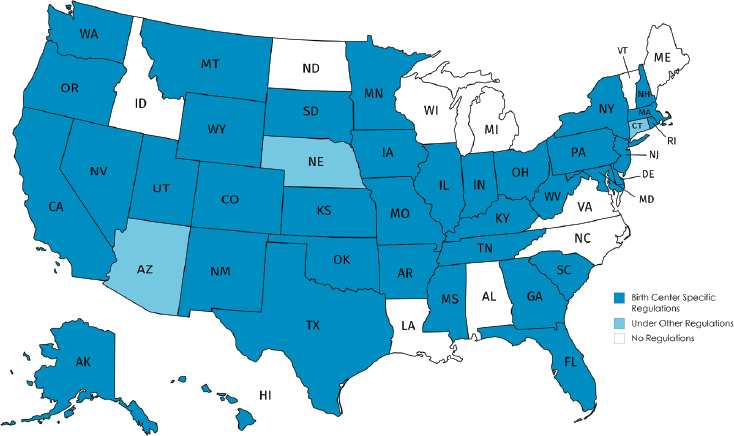
SOURCE: American Association of Birth Centers (2019). Used with permission of the American Association of Birth Centers. Created with Mapchart.net.
Maternity Care Financing
As discussed in Chapter 2, sources of financing for maternity care may include commercial insurance (with some out-of-pocket costs), Medicaid, and self-payment, among others. The type of financing strongly influences a woman’s choice of care provider and her access to various types of care. Women covered by Medicaid, a program designed to support low-income individuals, are particularly constrained by financing, as they are unlikely to have the resources to pay for care unless it is covered under the Medicaid program. While women with private insurance may, in theory, have additional options, many are often constrained by the types of providers and settings that are reimbursed under their plans and similarly may be unable to pay for services that are not covered.
Thus a woman’s choice of and access to providers and facilities are largely dependent on whether and how her care is financed and the type of coverage she has. Most women with private insurance choose providers and facilities that are covered by their plans, and women with Medicaid use providers who accept Medicaid (Holgash and Heberlein, 2019). In both Medicaid and private insurance, there is variation in what maternity care services are covered and to what extent (Kaiser Family Foundation, 2017, 2007). Timing of entry into prenatal care is also influenced by financing. Medicaid eligibility is dependent on whether a state has ex-
panded Medicaid and whether it has “presumptive” Medicaid. If a state has expanded Medicaid, women with low incomes may already have coverage before pregnancy and may continue to have coverage afterward. If a woman relies on pregnancy-related Medicaid, she cannot receive coverage until after she is pregnant, may experience a delay in access to services if her state does not have presumptive eligibility, and may lose her coverage 2 months after giving birth. If a woman is uninsured and applies for Medicaid or if the state lacks a presumptive eligibility policy, it may take 45 days for Medicaid to go into full effect, which can delay entry into prenatal care. Among policy proposals to strengthen childbearing women’s access to health care are legislative provisions to expand access to Medicaid to a full year after birth and to make pregnancy a special enrollment period when a woman can buy into marketplace insurance coverage outside of the annual enrollment period.
Payment is also an issue with respect to incentives for more intervention. For example, Medicaid and other payers generally reimburse hospitals at a higher level for cesareans, although some states (e.g., Minnesota) have leveled vaginal and cesarean provider payment. In addition, payment, especially by Medicaid, may not cover the facility fee for birth, so that home and birth center settings, unable to cover their marginal costs, are unable to accept a large proportion of Medicaid patients. This is the case despite documented cost savings and reduction in preterm birth, among other benefits for Medicaid beneficiaries in birth centers, in comparison with similar women receiving maternity care in typical Medicaid care settings (Hill et al., 2018) and for home versus hospital birth overall (Wax et al., 2010). Moreover, the lowest-reimbursed providers are often those outside of a hospital—in birth centers and home birth settings attended by midwives, whose model of care is among the most labor-intensive (see Chapter 2).
Access to Prenatal and Birth Care
Timely and appropriate prenatal care is important for supporting the health of women and their offspring during pregnancy and at birth. By engaging women early in pregnancy, providers are able to conduct screenings; assess risks; and provide psychosocial, cultural, and educational support to women and their families, with the objective of improving health for women and their babies. While a causal relationship has not been established (Gadson et al., 2017), delayed entry into prenatal care and/or underutilization of these services has been associated with several adverse maternal and neonatal outcomes, including maternal mortality, preterm birth, and low birthweight (Moaddab et al., 2018). Thus, access to affordable, culturally appropriate prenatal care is an important component of the
maternity care system. In addition, the cultural competence of care needs to be considered. A recent report from the National Academies, Vibrant and Healthy Kids, calls for providing prenatal care and education services that are culturally and linguistically appropriate to promote uptake (National Academies of Sciences, Engineering, and Medicine, 2019).
For some women, access to prenatal care is limited. Black women, AIAN women, women of low socioeconomic status, rural women, and immigrant women all face systemic barriers to accessing early and adequate prenatal care (see Table 4-1 presented earlier; see Box 4-1 for discussion of the challenges to accessing materity care among immigrant women). These barriers include lack of available services, lack of insurance coverage or funds to cover prenatal care visits, and experiences of racism in the health care system, among others (Slaughter-Acey et al., 2019; Swartz et al., 2017; Gadson et al., 2017; Mazul et al., 2017). As discussed earlier in this chapter, other social determinants of health, such as transportation and lack of social support, can also create barriers to accessing prenatal care (Mazul et al., 2017; Heaman et al., 2015).
Enhanced prenatal care services, such as those tested in the Strong Start for Mothers and Newborns initiative, may be one method for increasing access to prenatal care and reducing disparities in birth outcomes. Box 4-2 provides a detailed description of the Strong Start initiative and recent outcomes.
Summary
The structure, policies, and financing of the health care system all influence the health outcomes of pregnant people and newborns. These features of the health system can contribute to a woman’s risk profile in pregnancy and birth, her ability to access and choose birth settings, and the quality of care she receives in those settings. In the presence of systemic barriers—whether financial, social, or regulatory—the choice made is often constrained and made in the absence of available alternatives.
Finding 4-1: Birthing facilities and maternity care providers are unevenly distributed across the United States, leaving many women without access to prenatal, birthing, and postpartum care and choices among options near home.
Finding 4-2: Women living in rural communities and underserved urban areas have greater risks of poor outcomes, such as preterm birth and maternal and infant mortality, in part because of lack of access to maternity and prenatal care in their local areas.
Finding 4-3: Access to midwifery care is limited in some settings because some types of midwives are not licensed in some states and do not have admitting privileges in some medical facilities, but this varies across the country. The wide variation in regulation, certification, and licensing of maternity care professionals across the United States is an impediment to access to all birth settings.
Finding 4-4: Access to all types of birth settings and providers is limited because of the lack of universal coverage for all women, for all types of providers, and at levels that cover the cost of care.
CONCLUSION
This chapter has reviewed the many systems-level social and environmental factors that can influence a woman’s health status, readiness for pregnancy, access to and use of prenatal and intrapartum care, and access to choices surrounding that care. Risk during pregnancy and childbirth is not simply the result of medical and obstetrical risk factors. Rather, these individual-level risk factors are often the result of a series of systems-level factors, such as structural inequalities and biases (in both the health system and society at large), policy and financing features of the health system, and the social determinants of health. These upstream factors, the conditions and context within which an individual lives, shape a woman’s health and the health and well-being of her child. These negative or positive social influences can change a woman’s risk profile in pregnancy and in childbirth.
Moreover, these systems-level factors can confer their own risk on pregnant women. As an example, inequities in maternal and newborn outcomes, in particular for Black and AIAN women, can be traced to structural inequities and biases including racism, which both increases stress during pregnancy and influences how a woman is treated. Delayed prenatal care in the face of provider shortages, for example, can increase a woman’s risk for a host of adverse pregnancy outcomes, without changing her individual medical and obstetrical risk. This in turn influences her willingness to seek maternity care and other aspects of access to care. Understanding the role that nonclinical factors play in determining clinical risk is essential for developing risk-appropriate models of care.
CONCLUSION 4-1: Systems-level factors and social determinants of health such as structural racism, lack of financial resources, availability of transportation, housing instability, lack of social support, stress, limited availability of healthy and nutritious foods, lower level of education, and lack of access to health care (including mental health
care) are correlated with higher risk for poor pregnancy outcomes and inequity in care and outcomes.
These systemic risk factors are felt at the individual and population levels. For individual women, systemic risk factors hamper access and contribute to medical, obstetrical, and social risks. At the population level, these systemic factors translate into disparities in maternal and neonatal outcomes along lines of race, class, and geography. Other social determinants of health also influence both access and outcomes, including housing, employment status, health literacy and education, transportation, location of services, and location of maternity care professionals. Policy regarding access and financing can strongly impact women’s ability to get adequate maternity care.
As a result, women’s options will be limited by the availability of different types of birth settings and maternity care providers within or near their community, including hospital resources and within-hospital options. Availability is particularly challenging in rural areas and in some inner cities. A woman’s choices are further limited by health insurance and Medicaid restrictions; economic circumstances; access to transportation; and cultural and linguistic factors, such as language barriers with providers and her perception of how she will be received and treated.
Understanding and differentiating the risk stratification conferred by individual- and systems-level risk as well as access to choices of birth settings for pregnant people in the United States is one key aspect of analyzing health outcomes by birth setting. In the next chapter, we turn to this consideration, as well as other data and methodological considerations for understanding birth settings research.
































