
7
Implementing Quarantine to Reduce or Stop the Spread of a Contagious Disease
Implementation of quarantine by state, local, tribal, and territorial public health agencies is recommended to reduce disease transmission and associated morbidity and mortality during an outbreak only after consideration of the best available science regarding the characteristics of the disease, the expected balance of benefits and harms, and the feasibility of implementation.
Finding Statements and Certainty of the Evidence
| •••• High ••• Moderate •• Low • Very Low | ||
| Finding Statement | Certainty | |
| Quarantine can be effective at reducing overall disease transmission in the community in certain circumstances | •••• | |
| Quarantine can reduce the time from symptom onset to diagnosis in quarantined individuals | •• | |
| Congregate quarantine for influenza and agents with similar transmissibility can increase risk of infection among those in the shared setting | •••• | |
| Quarantine can result in psychological harms among quarantined individuals, including posttraumatic stress disorder, anxiety, and anger, the risk of which increases with the duration of quarantine | ••• | |
| Quarantine can be associated with individual financial hardship for quarantined individuals | •••• | |
| Emphasis on health by those leading the outbreak response (i.e., health-promoting leadership) can reduce depression and anxiety symptoms in quarantined individuals | • | |
| While adherence to quarantine measures can vary by culture, disease, and socioeconomic status, use of various strategies, including risk communication and messaging and access to employment leave can improve adherence | ••• | |
Implementation Guidance
Considerations for when to implement quarantine
![]() Early on in the outbreak, especially when there is a shortage or absence of available medical countermeasures
Early on in the outbreak, especially when there is a shortage or absence of available medical countermeasures
![]() Only after weighing the resources required for quarantine against the expected benefits
Only after weighing the resources required for quarantine against the expected benefits
![]() When the basic reproductive number (R0) of a given pathogen is in a range in which quarantine can be expected to reduce transmission importantly. Quarantine may be more effective for a pathogen with moderate R0, or for a pathogen with a higher R0 that has previously produced durable immunity in a population
When the basic reproductive number (R0) of a given pathogen is in a range in which quarantine can be expected to reduce transmission importantly. Quarantine may be more effective for a pathogen with moderate R0, or for a pathogen with a higher R0 that has previously produced durable immunity in a population
![]() When quarantine can reliably separate identified individuals from the general population for durations commensurate with the expected duration of asymptomatic infectiousness
When quarantine can reliably separate identified individuals from the general population for durations commensurate with the expected duration of asymptomatic infectiousness
![]() When the asymptomatic infectious period is short or there is no asymptomatic infectious period
When the asymptomatic infectious period is short or there is no asymptomatic infectious period
![]() When exposed individuals can be identified reliably and quickly
When exposed individuals can be identified reliably and quickly
![]() When isolation of individuals once they become symptomatic is slow or unreliable without quarantine
When isolation of individuals once they become symptomatic is slow or unreliable without quarantine
Considerations for how to implement quarantine
![]() Consider voluntary before legally enforced quarantine
Consider voluntary before legally enforced quarantine
![]() Avoid congregate quarantine whenever possible to reduce the risk of disease transmission among those in the shared setting
Avoid congregate quarantine whenever possible to reduce the risk of disease transmission among those in the shared setting
![]() Implement quarantine at a smaller scale before considering implementation at a large scale
Implement quarantine at a smaller scale before considering implementation at a large scale
![]() Understand the population on which quarantine will be imposed. At-risk populations will require greater consideration because of the potential for greater harms
Understand the population on which quarantine will be imposed. At-risk populations will require greater consideration because of the potential for greater harms
![]() Allow reasonable modifications of policies to suit the needs of the situation and the people placed under quarantine
Allow reasonable modifications of policies to suit the needs of the situation and the people placed under quarantine
![]() Ensure that a legal framework is in place and develop options for different levels of quarantine that are matched to the pathogen and risk of exposure
Ensure that a legal framework is in place and develop options for different levels of quarantine that are matched to the pathogen and risk of exposure
Considerations for during and after the implementation of quarantine
![]() Use culturally informed approaches to quarantine, and use an orientation of care approach rather than enforcement
Use culturally informed approaches to quarantine, and use an orientation of care approach rather than enforcement
![]() Ensure transparent risk communications. Provide clear messaging on the rationale for quarantine
Ensure transparent risk communications. Provide clear messaging on the rationale for quarantine
![]() Provide financial, food, and social and psychological support to quarantined individuals
Provide financial, food, and social and psychological support to quarantined individuals
![]() Plan for what will happen as and after quarantine measures are lifted
Plan for what will happen as and after quarantine measures are lifted
DESCRIPTION OF THE PRACTICE
Defining the Practice
The committee examined the evidence for the circumstances in which implementing quarantine is effective at reducing or stopping the spread of a contagious disease. It also examined potential undesirable effects or harms associated with quarantine and factors that may mediate its effectiveness (e.g., resources, setting, enforcement). Quarantine is one type of non-pharmaceutical intervention (NPI), and falls primarily under Capability 11: Non-Pharmaceutical Interventions (NPI Capability) in the Centers for Disease Control and Prevention’s (CDC’s) Public Health Emergency Preparedness and Response Capabilities: National Standards for State, Local, Tribal, and Territorial Public Health (CDC PHEPR Capabilities) (CDC, 2018).
At the time of this writing, the nation and the world were responding to a pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (the causative agent of coronavirus disease 2019 [COVID-19]). The committee selected quarantine as one of its four review topics using the specific process described in Chapter 3 and Appendix A. This careful topic selection process and the committee’s evidence review were conducted well in advance of the COVID-19 pandemic; therefore, the evidence review did not include studies examining applications of quarantine, social distancing strategies, or other NPIs implemented specifically in response to COVID-19. However, the committee reflects on its review in the context of COVID-19 at the end of this chapter.
Quarantine is the physical separation and restriction of movement of individuals who may have been exposed to a contagious disease, who may or may not be infected but are not ill, and who may become infectious to others (CDC, 2017). Thus, individuals who are quarantined are asymptomatic and may or may not be infected or pose any danger to others. This is in contrast to isolation, which is the sequestration of individuals known to be infected with a contagious disease, who often are symptomatic.
Quarantine is an NPI that falls under the general designation of social distancing (i.e., measures intended to reduce direct physical contact between individuals to reduce the transmission of contagious diseases). The NPI Capability, and specifically quarantine, is closely linked to other CDC PHEPR Capabilities (see Box 7-1).
The types and intensity of quarantine measures can differ. The decision to implement quarantine includes the following components:
- Who—determination of which asymptomatic individuals might have been exposed to the infectious agent and whether the likelihood of exposure and the consequences of transmission are great enough to warrant separation from the community.
- Where—decisions about whether the physical separation should occur at home, in a health care facility, or in some other designated facility.
- How—decisions about whether quarantine should be voluntary or mandatory, and if the latter, how to enforce it.
- Duration—determination as to the length of quarantine, which is generally based on the incubation period (if known) of the infectious agent to which the person has potentially been exposed.
In sum, quarantine is always implemented in a target population for which infection status is unknown but in which there is some increased probability of infection due to possible or known exposure.
Scope of the Problem Addressed by the Practice
NPIs are often used in efforts to reduce disease transmission. For novel infections or those without effective and available treatments or vaccines, NPIs are the only means available to curb the spread of the disease (Aiello et al., 2010; Aledort et al., 2007; Love et al., 2007). NPIs have played important roles in notable contagious disease emergencies, most notably in the 1918 pandemic influenza and the 2003 severe acute respiratory syndrome (SARS) coronavirus outbreak (Markel et al., 2006, 2007; Svoboda et al., 2004). Quarantining
suspected asymptomatic carriers of an illness has been public health practice for centuries (Barbisch et al., 2015; Gensini et al., 2004); the term itself stems from the practice of keeping ships at harbor for 40 days (“una quarantina”) during the great plagues of Europe in an effort to prevent the spread of disease between cities. In the 21st century, quarantine has been part of the response for multiple global infectious disease outbreaks:
- The novel coronavirus COVID-19 pandemic in 2019 (ongoing at the time of this writing). In January 2020, China attempted to institute city-level quarantine in Wuhan on a historically unprecedented level, prohibiting intercity movement and severely limiting intracity transportation (Lai et al., 2020). As the virus spread globally, countries, including the United States, and localities implemented quarantine and various social distancing measures as well (CDC, 2020; Nussbaumer-Streit et al., 2020).
- The Middle East respiratory syndrome (MERS) coronavirus in 2015 in Korea and the Middle East. Quarantine was implemented along with other NPI measures, as well as use of antiviral regimens (Oh et al., 2018).
- The Ebola virus in 2014. The outbreak resulted in the quarantine of individuals and communities in West Africa and of some travelers returning from West Africa to the United States (Sell et al., 2019).
- H1N1 in Australia and China, among other countries in 2009 (Binns et al., 2010; Chin et al., 2012). Quarantine was used along with school closures in the United States (Copeland et al., 2012).
- SARS in eastern Asia and Canada in 2003. Quarantine was employed along with mass screening of travelers and other control measures (Svoboda et al., 2004; Zhang et al., 2011).
- Smaller-scale outbreaks in which quarantine was used for control, such as localized measles epidemics (CDC, 2004; Collier et al., 2013; Gahr et al., 2014; Gastanaduy et al., 2016; Sugerman et al., 2010).
- Historical outbreaks during which quarantine was implemented (e.g., 1918–1919 influenza pandemic), with available data being applied to understand the effects of quarantine and other NPIs (MacDougall, 2007; Markel et al., 2006, 2007; Sattenspiel and Herring, 2003).
Questions raised by public health emergency preparedness and response (PHEPR) practitioners as critical to the use of quarantine surround its implementation, such as deciding when to implement it, whom to quarantine, and what operational supports to institute so that the quarantine is more likely to be successful (note that “success” in this context is usually measured by determining people’s adherence to the quarantine’s restrictions, not by documenting reduced transmission of disease). There can be significant political pressure to implement quarantine, as was seen with the 2014 Ebola epidemic and travelers returning from West Africa to the United States (Asgary et al., 2015; Miles, 2015), and there is a potential hypothetical social value associated with the practice as a means of calming public fears during an epidemic. On the other hand, there can be pressure not to quarantine, and implementing quarantine may also contribute to public fears during an epidemic.
CDC issued the Final Rule for Control of Communicable Diseases: Interstate and Foreign1 in 2017, which enhanced the ability to prevent the introduction, transmission, and spread of communicable diseases in the United States. Each state also has its own legal authorities over
___________________
1 See https://www.federalregister.gov/documents/2017/01/19/2017-00615/control-of-communicable-diseases (accessed June 25, 2020).
quarantine. In January 2020, in response to the ongoing COVID-19 outbreak, CDC issued federal quarantine orders for the first time in more than 50 years (CDC, 2020). In 2017, CDC published community mitigation guidelines for pandemic influenza and concluded, based on the available evidence, that voluntary home quarantine of exposed household members might be recommended (CDC, 2017). More recently, the World Health Organization (WHO) reviewed the evidence and provided guidance on the use of quarantine, among other NPI measures, for mitigating the risk and impact of pandemic influenza (quarantine was not recommended) (WHO, 2019).
The committee considered the implementation of different types of quarantine (not just household quarantine) as a strategy for reducing the spread of any contagious disease. Some of the findings discussed in the CDC guidelines and the WHO guidelines for pandemic influenza reflect issues similar to those considered by the committee and discussed in this chapter (e.g., the effectiveness of quarantine in reducing the burden of disease, the location of quarantine, its scale). Having clear guidelines as to when quarantine should improve outcomes and how best to implement it may help public health practitioners implement this practice so as to maximize its benefits and minimize its harms.
OVERVIEW OF THE KEY REVIEW QUESTIONS AND ANALYTIC FRAMEWORK
Defining the Key Review Questions
Theoretically, the benefit of quarantine is effective curbing of the spread of contagious diseases by preventing person-to-person transmission. Therefore, the primary question posed by the committee in this review is: “In what circumstances (e.g., based on biologic factors, risks, resource availability, legal authorities, social context) is quarantine effective at reducing or stopping the spread of a contagious disease?” To answer this primary question, the committee sought evidence on several sub-questions related to evidence on the pros and cons of specific adherence strategies, the documented benefits and harms of implementing quarantine, and the factors that create barriers to and facilitators of its implementation (see Box 7-2).
The evidence review focused on those aspects of quarantine that fall primarily under the jurisdiction of public health. In evaluating the effectiveness of quarantine, however, the committee considered studies from occupational health and hospital settings. The committee did
not include studies in which the effect of NPIs bundled together was examined (Markel et al., 2007), and instead focused its review on trying to tease out the impact of quarantine alone. The committee did not broaden its evidence search to include practices of self-quarantine intended to avoid potential exposures beyond a contagious disease scenario, such as people who choose to shelter in place following an environmental, chemical, or radiological event to limit exposure to potential toxins or radiation. Furthermore, the committee did not include evidence examining cordon sanitaire and shelter-in-place and stay-at-home orders, such as those that have been implemented among various localities, states, and countries in response to the COVID-19 pandemic. While the latter encompass types of quarantine under a broad definition of the term, these strategies had not been used until recently in modern public health responses to infectious disease outbreaks. Furthermore, such actions and others, such as travel bans, are intended to restrict the movement of all people in a geographic region, regardless of individual level of exposure risk. This makes these interventions qualitatively different from traditional quarantine, which is based on an assessment of likely individual exposure.
Analytic Framework
For the purposes of this review, the committee developed an analytic framework to present the causal pathway and interactions between quarantine and its components, populations, and outcomes of interest (see Figure 7-1). The mechanism by which quarantine can ultimately reduce or stop the spread of a contagious disease is well established and noncontroversial: there is a period of time (the incubation period) between when a person is exposed to a contagious illness and when that person, if infected, becomes contagious to others; if individuals who are exposed and become infected are not in contact with anyone else at the time they become contagious, they cannot spread the infection (Drews, 2013). As a practical matter, implementing quarantine entails determining which people are at higher risk of having been infected because of exposure but are not yet showing signs or symptoms of illness and are therefore presumed not yet to be contagious, and then physically segregating these people from others for a defined period of time, usually intended to exceed the incubation period of the illness (WHO, 2019). If any of these people become ill during their time under quarantine, they will have been prevented from being in contact with those not infected and spreading the infection more widely.
Quarantine relies on a number of important assumptions regarding the biology of the contagious disease at hand (e.g., How readily transmissible is the agent? Is it transmissible during the incubation period or only after symptoms arise?). Of particular note is that the value of quarantine in preventing the spread of contagion will vary based on when during the course of infection individuals become contagious. For example, if an infected person does not become contagious until some time after symptoms of the illness emerge, the theoretical value of quarantining asymptomatic people may be reduced (because the same benefit could be achieved by monitoring for early symptoms and isolating those who became ill). By contrast, if infected people become contagious while they are still asymptomatic, the value of quarantine is potentially much greater. But such biological factors are not the only factors that can alter the effectiveness of quarantine as a strategy for reducing or halting the spread of a contagious illness; the effectiveness of quarantine is also dependent on a number of social factors, including the extent to which exposed individuals can be contacted and their subsequent willingness and ability to adhere to quarantine. The outcomes of quarantine may hinge as well on its interaction with other NPIs.
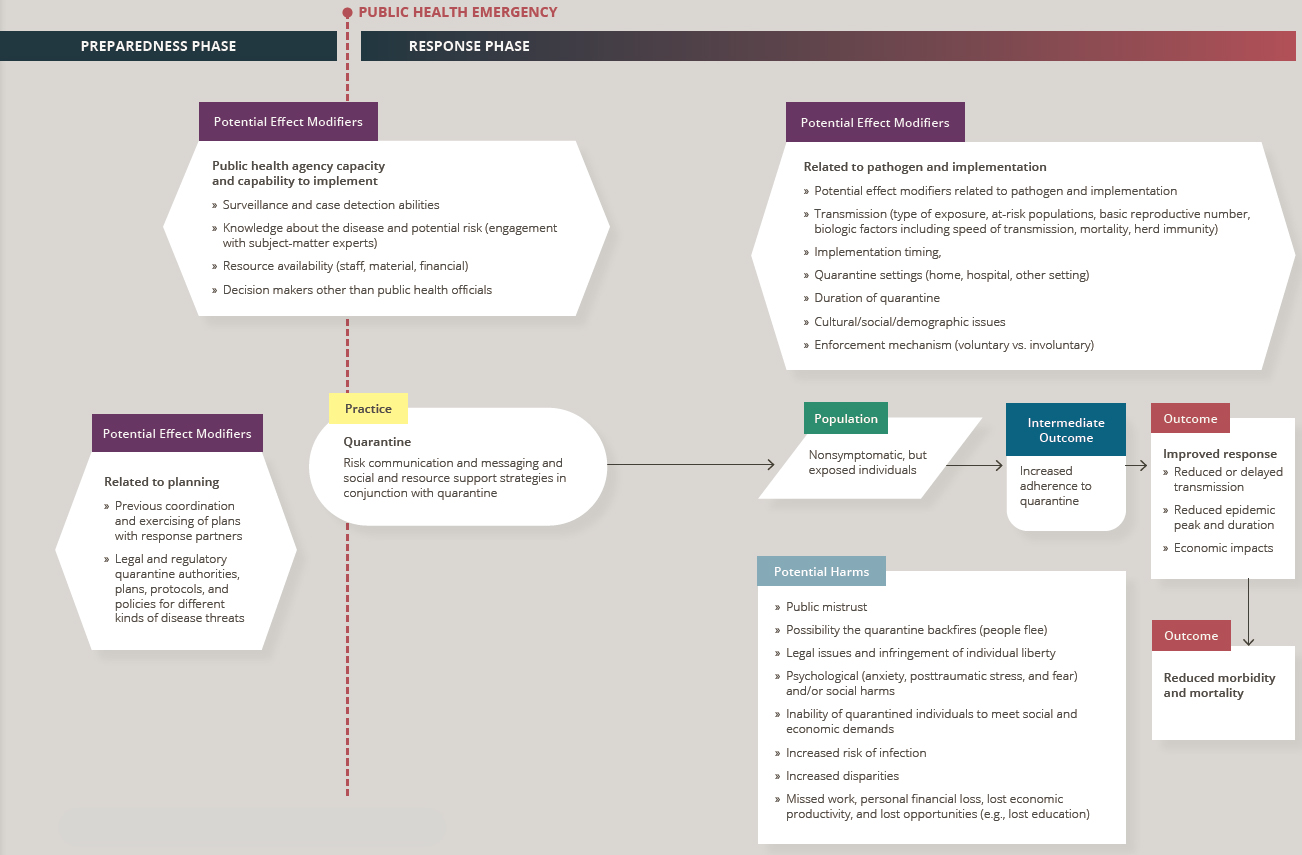
NOTE: Arrows in the framework indicate hypothesized causal pathways between interventions and outcomes.
OVERVIEW OF THE EVIDENCE SUPPORTING THE PRACTICE RECOMMENDATION2
This section summarizes the evidence from the mixed-method review examining the implementation of quarantine to reduce or stop the spread of a contagious disease. Following the summary of the evidence of effectiveness, summaries are presented for each element of the Evidence to Decision (EtD) framework (encompassing balance of benefits and harms, acceptability and preferences, feasibility and PHEPR system considerations, resource and economic considerations, equity, and ethical considerations), which the committee considered in formulating its practice recommendation. Full details on the review strategy and findings can be found in the appendixes: Appendix A provides a detailed description of the study eligibility criteria, search strategy, data extraction process, and individual study quality assessment criteria; Appendix B4 provides a full description of the evidence, including the literature search results, evidence profile tables, and EtD framework for implementing quarantine; and Appendix C links to all the commissioned analyses that informed this review. Table 7-1 shows the types of evidence included in this review.
Effectiveness
Three quantitative comparative studies address the overarching key question regarding in what circumstances quarantine is effective at reducing or stopping disease transmission in the community. These three studies examine whether quarantine reduced disease transmission in response to three different contagious diseases: H1N1 pandemic influenza, SARS, and measles. Another six quantitative comparative studies and four quantitative noncomparative studies examine other potential benefits and harms of quarantine, as well as strategies that may be effective at improving adherence to quarantine. (Refer to Section 1, “Determining Evidence of Effect,” in Appendix B4 for additional detail.)
Consistent with the methods described in Chapter 3, in making its final judgment on the evidence of effectiveness for quarantine, the committee considered other types of evidence that could inform a determination of what works for whom and in which contexts, ultimately reaching consensus on the certainty of the evidence (COE) for each outcome. Including other forms of evidence beyond quantitative comparative studies is particularly important when assessing evidence in settings where controlled studies are challenging to conduct and/or other forms of quantitative comparative data are difficult to obtain. Descriptive evidence from real-world implementation of practices offers the potential to corroborate research findings or explain differences in outcomes in practice settings, even if it has less value for causal inference. Moreover, qualitative studies can complement quantitative studies by providing additional useful evidence to guide real-world decision making, because well-conducted qualitative studies produce deep and rich understandings of how interventions are implemented, delivered, and experienced. Other forms of evidence considered for evaluation of effectiveness included mechanistic evidence, evidence from modeling studies, evidence from qualitative studies, and quantitative data reported in case reports that involved a real disaster or public health emergency.
The evidence suggests that quarantine can be effective at reducing overall disease transmission in the community in certain circumstances (high COE based on three quantitative studies, mechanistic evidence, modeling evidence, and case report evidence) and reducing
___________________
2 To enhance readability for an end user audience, this section does not include references. Citations supporting the findings in this section appear in Appendix B4.
TABLE 7-1 Evidence Types Included in the Mixed-Method Review of Implementing Quarantine
| Evidence Typea | Number of Studies (as applicable)b |
|---|---|
| Quantitative comparative | 9 |
| Quantitative noncomparative (postintervention measure only) | 4 |
| Qualitative | 16 |
| Modeling | 12c |
| Descriptive surveys | 13 |
| Case reports | 28 |
| After action reports | N/A |
| Mechanisticd | Yes |
| Parallel (systematic reviews) | N/A |
a Evidence types are defined in Chapter 3.
b Note that sibling articles (different results from the same study published in separate articles) are counted as one study in this table. Mixed-method studies may be counted in more than one category.
c The committee chose a sample of 12 studies out of 47 modeling studies for detailed review based on an assessment of their methodologic approach, data sources, relevance to the key questions for this practice, potential implications for public health practice, and disease condition studied. Given the time and resources available, the committee had to exclude a number of well-conducted modeling studies. Studies were excluded from detailed review if they reported major limitations to their model conclusions due to such factors as excessive uncertainty about modeling parameter values.
d For the purposes of this report, the committee defined mechanistic evidence as evidence that denotes relationships for which causality has been established—generally within other scientific fields, such as chemistry, biology, economics, and physics (e.g., the accelerating effect of the gravitational attraction of Earth and the slowing effect of air resistance)—and that can reasonably be applied to the PHEPR context through mechanistic reasoning. Mechanistic evidence is discussed further in Chapter 3.
the time from symptom onset to diagnosis in quarantined individuals (low COE based on one quantitative study, mechanistic evidence, modeling evidence, and case report evidence). However, quarantine can result in harms for those individuals on whom it is imposed, including increased risk of infection among those placed together in congregate quarantine settings3 (high COE based on two quantitative studies and mechanistic evidence); psychological harms, the risk of which increases with the longer duration of quarantine (moderate COE based on six quantitative studies, qualitative evidence, and case report evidence); and individual financial hardship (high COE based on two quantitative studies, mechanistic evidence, and qualitative evidence). There is very low COE (based on one quantitative study and case report evidence) that an emphasis on health by those leading the outbreak response (i.e., health-promoting leadership) can reduce depression in quarantined individuals. The effectiveness of quarantine is also dependent on a number of social factors, some of which might be addressed through various implementation strategies. There is moderate COE that while adherence to quarantine measures can vary by culture, disease, and socioeconomic status, use of various strategies, including risk communication and messaging and access to employment leave, can improve adherence.
___________________
3 A congregate quarantine setting is the sharing of the same room or facilities with an infected case. This is mainly applicable to individuals quarantined at home who fall ill and thereby increase the likelihood of another household member acquiring the illness.
Findings from a Synthesis of Modeling Studies: Quarantine Is More Effective Under Certain Circumstances
Across the 12 modeling studies considered, quarantine was found to be more or less likely to be effective depending on systematic and consistent factors related both to characteristics of the pathogen and to the population and setting (see Table 7-2). Understanding of these systematic relationships is aided specifically by one of the modeling studies included in this review (Peak et al., 2017), which contains analyses for a range of diseases and attempts to provide answers to this question within a common modeling framework.4 (Refer to Section 2, “Findings from a Synthesis of Modeling Studies: Quarantine Is More Effective Under Certain Circumstances,” in Appendix B4 for additional detail.)
Consistent with the findings of Peak and colleagues (2017), as well as the other modeling studies and the drivers of effectiveness they identify or imply, quarantine was more likely to be effective at reducing or stopping the spread of a contagious disease in the following circumstances:
- Moderate basic reproductive number (R0)—when the R0 of a given pathogen is in a range in which quarantine can be expected to reduce transmission importantly. Quarantine may be more effective for a pathogen with a moderate R0, or for a pathogen with a higher R0 that has previously produced durable immunity in a population (i.e., the population in question has been exposed previously) such that the effective reproductive number (Re)5 in the population even without intervention is relatively lower. If a pathogen has a high R0, more transmission may occur before quarantine can be implemented, reducing quarantine’s effectiveness at limiting the final size of the outbreak. As a practical matter, for pathogens with a very low R0 (i.e., <1), disease transmission will not be sustained, making quarantine theoretically effective but perhaps practically unnecessary.
- Shorter incubation period—when quarantine can reliably separate identified individuals from the general population for durations commensurate with the expected duration of asymptomatic infectiousness. Quarantine may become infeasible or less effective as the result of reduced adherence if its duration must be very long because of a prolonged incubation period (the period between exposure and when infection becomes detectable).
- Relatively short asymptomatic infectiousness period—when the asymptomatic infectious period is short or there is no asymptomatic infectious period. When there is a long period of asymptomatic infectiousness, quarantine of recently infected people must be extremely rapid and comprehensive to prevent transmission by asymptomatic individuals, which may be so logistically challenging as to be practically infeasible. In addition, if the asymptomatic infectious period is long in absolute terms, quarantine may become infeasible or less effective because of reduced adherence (see the previous bullet).
- Rapid identification—when exposed individuals can be identified reliably and quickly.
___________________
4Peak et al. (2017) was selected as the scaffold for the synthesis of modeling studies because it considers factors for a range of diseases, whereas the other included modeling studies look at only one disease.
5 Note that the pathogen’s R0 changes over time as the result of interventions and as the infection establishes immunity. The Re (in this case in the presence of quarantine) is related conceptually to the ability of an infection to have persistent or growing prevalence in a population (when Re is above 1, the disease will have growing prevalence; below 1, it will decline).
TABLE 7-2 Summary of Findings on the Effectiveness of Quarantine from 12 Modeling Studies
| Disease | Quarantine Likely Effective? | Notes |
|---|---|---|
| Ebola | Yes | Two studies find quarantine can drive Re <1a (D’Silva and Eisenberg, 2017; Peak et al., 2017). |
| Hepatitis A | Yes based on 1 study | One study finds quarantine can drive Re <1 (Peak et al., 2017). |
| Influenza A/H1N1 | Maybe | Two studies. One study finds quarantine can drive Re <1 (Peak et al., 2017). Another study focuses on delaying the epidemic peak and suggests that quarantine can possibly be effective depending on the specific features of the pathogen in the population and the level of intervention (An der Heiden et al., 2009). |
| Middle East respiratory syndrome (MERS) | Yes | Two studies find quarantine can drive Re <1 (Ahn et al., 2018; Peak et al., 2017). |
| Pertussis | No based on 1 study | One study finds quarantine is unlikely to drive Re <1 (Peak et al., 2017). |
| Severe acute respiratory syndrome (SARS) | Maybe | Seven studies. Three studies identify situations in which quarantine may not be effective in driving Re <1, with effectiveness depending on the pathogen’s basic reproductive number (R0) in a given population (less likely with higher R0), the likely effectiveness of isolation of symptomatic individuals as an alternative strategy, the likelihood of there being individuals who are asymptomatic but contagious and the fraction of those individuals, and the ability to quickly identify a large fraction of exposed individuals for quarantine (Day et al., 2006; Hsieh et al., 2007; Peak et al., 2017). Four studies find (or in essence assume [based on models of past limited outbreaks]) that sufficiently effective, properly scaled and targeted, or potentially dynamic quarantine policies can drive Re <1 (Feng et al., 2009; Gupta et al., 2005; Mubayi et al., 2010; Podder et al., 2007). |
| Smallpox | Maybe | Two studies. One study finds quarantine is unlikely to drive Re <1. Another study finds that early initiation of quarantine that removes a large fraction of exposed cases can likely avoid an epidemic resulting from a smallpox bioterrorism attack (Meltzer et al., 2001; Peak et al., 2017). |
| Measles | Yes/maybe based on 1 study | One study finds that despite measles having a high R0, if there is a sufficient level of background immunity, it may be possible to use quarantine to end an outbreak quickly. However, with lower levels of background immunity, quarantine is unlikely to drive Re <1 or to do so quickly (Enanoria et al., 2016). |
a Re = effective reproductive number (in this case in the presence of quarantine), which conceptually is related to the ability of an infection to have persistent or growing prevalence in a population (when Re is above 1, the disease will have growing prevalence; when it is below 1, prevalence will decline).
- To aid isolation—when isolation of individuals once they become symptomatic is slow or unreliable without quarantine, quarantine may reduce transmission through its effects on facilitating more rapid isolation of ill and contagious individuals.
Balance of Benefits and Harms
Quarantine can be effective at reducing the transmission of contagious disease and has the possible additional benefit of reducing the time to diagnosis for infected patients who are being monitored while under quarantine. However, it also can result in a number of harms. In particular, quarantine has the potential to result in the abridging of individual or community rights of freedom, movement, and association. In addition, as noted above, there
may be an increased risk of infection among those placed together in congregate quarantine settings. Quarantine can also create financial instability, social stigma, and compromised psychological well-being for quarantined individuals. Given these undesirable effects of quarantine, which can be both short and long term, the balance of benefits and harms is open to debate and should be assessed on a case-by-case basis. (Evidence source: synthesis of evidence of effect and qualitative evidence synthesis. Refer to Section 3, “Balance of Benefits and Harms,” in Appendix B4 for additional detail.)
Acceptability and Preferences
Overall, the public understands and accepts the general concept of quarantine, but this understanding and acceptance is not uniform across all societies, and the acceptability of quarantine can vary depending on levels of social trust in the authorities implementing it. Moreover, fear of harms may make quarantine unacceptable in some communities. The acceptability of and preference for quarantine may differ as well across the multiple individuals and agencies that often must work together to implement quarantine, with some advocating for an emphasis on voluntary adherence and others seeking mandatory enforcement, which may include a militaristic response. In general, the evidence suggests that voluntary quarantine is more acceptable, and therefore can be more effective, than mandatory quarantine. (Evidence source: qualitative evidence synthesis, case report evidence synthesis, and descriptive survey study evidence. Refer to Section 4, “Acceptability and Preferences,” in Appendix B4 for additional detail.)
Feasibility and PHEPR System Considerations
Quarantine is more effective at reducing or stopping the transmission of a contagious disease when exposed individuals can be identified reliably and quickly. To initiate quarantine in a timely manner requires accurate, up-to-date, and specific pre- and intra-outbreak surveillance, as well as preexisting organizational frameworks and linkages to rapid decision making, including an in-place legal framework. Feasibility is also related to the scale of quarantine; if quarantine is uncoordinated and implemented at an intense level in multiple geographic areas, there is greater potential for redundancy and excess effort and resource expenditures, as well as for flight of individuals beyond designated boundaries. In addition, quarantine may become infeasible or less effective because of reduced adherence when the proposed duration of quarantine is longer. Although staffing and operational capacities to implement quarantine currently exist in many agencies, operational limitations may arise when quarantine is implemented on a large scale. Home quarantine may be more feasible than providing designated facilities for quarantined individuals, but is not without concerns over such harms as increased risk of infection among those housed together and challenges with adherence. (Evidence source: synthesis of modeling studies, qualitative evidence synthesis, and case report evidence synthesis. Refer to Section 5, “Feasibility and PHEPR System Considerations,” in Appendix B4 for additional detail.)
Resource and Economic Considerations
Implementing quarantine is highly resource intensive (e.g., the potential need to provide financial compensation, food, and social support). Therefore, factors that need to be considered when deciding whether to implement quarantine include resource availability, such as
the ability to mobilize public health personnel to conduct contact tracing (to identify those who might warrant being placed in quarantine) and regular symptom monitoring of those in quarantine (to detect those who are becoming ill and require isolation and medical care). Resources related to the medical care of quarantined individuals include environmental decontamination, waste management, safe transportation, and availability of sufficient stocks of such supplies as masks and thermometers. Quarantine may be costly not only for response agencies but also for the individuals placed in quarantine, and has the potential to result in broad social and economic disruption. Quarantined individuals may incur both direct and indirect costs, including child care expenses and lost wages due to a lack of employer or government compensation. Thus, public health agencies need to consider the resources required for quarantine against its expected benefits. (Evidence source: qualitative evidence synthesis, case report evidence synthesis, and descriptive survey study evidence. Refer to Section 6, “Resource and Economic Considerations,” in Appendix B4 for additional detail.)
Equity
People in quarantine may be publicly labeled as potential carriers of a contagious disease, which can lead others to develop toward them feelings of avoidance, suspicion, mistrust, and fear, and thus stigma. When people from already marginalized communities are quarantined, this stigmatization can exacerbate marginalization and discrimination, which can last well beyond the quarantine period.
When considering whether or how to impose quarantine on members of at-risk populations, public health leaders and agencies need to acknowledge that greater harms are likely to result for marginalized populations, creating a stronger obligation to protect them. At-risk populations can have additional needs affecting their ability to adhere to quarantine, and agencies need to consider the impact on various sub-populations based on demographics, socioeconomic considerations, and baseline access to resources. For example, potential challenges to quarantine arise when it involves transient populations such as people that are homeless, as they may be difficult to locate and monitor. Additionally, being forced to miss work can potentially exacerbate preexisting socioeconomic inequalities. The inequitable impacts of quarantine tend to be compounded over time such that the longer a quarantine lasts, the more sacrifice it requires of those being quarantined, and the more likely it is to exacerbate underlying societal, economic, and health care inequities. Finally, health care workers on whom quarantine is imposed may experience financial, social, and psychological harms, similar to those that occur to the general public; however, these harms may be amplified for health care workers for a number of reasons because of their responsibilities. (Evidence source: synthesis of evidence of effect, qualitative evidence synthesis, case report evidence synthesis, and descriptive survey study evidence. Refer to Section 7, “Equity,” in Appendix B4 for additional detail.)
Ethical Considerations
When implemented correctly and in the proper setting, quarantine is ethically justified by the expectation that it will protect unexposed people from the harm of being exposed to and contracting a contagious disease—a notion that has been called the harm principle. Given this ethical justification (i.e., that quarantine prevents harm), one could say that any quarantine action that does not in fact reduce or stop the spread of a contagious disease is unethical. Of course, the problem with saying this is that one may not know whether a quar-
antine will be effective until it is tried. In reality, then, the core ethical obligation involved in considering whether to implement quarantine is to do the very best to determine in advance whether the quarantine will work, and to implement it in ways that will maximize its effectiveness while minimizing the extent to which it infringes on individual or group liberties and rights (principle of proportionality).
Another ethical consideration for quarantine is the need to recognize that people in quarantine are giving up their personal freedoms (whether voluntarily or not) in an effort to protect their community, and thus deserve gratitude and respect (principle of respect for persons and communities). Indeed, this consideration represents one justification for efforts to ensure that people in quarantine are well cared for, and that they do not suffer stigma later on. The other justification for such efforts is utilitarian (principle of harm reduction/benefit promotion): people who fear being placed in quarantine may flee the area, potentially spreading the contagion even farther than it might have spread without a threatened quarantine. This is not an entirely hypothetical concern; there are several real-world examples of quarantines that failed or even backfired when people threatened with quarantine fled the area. With regard to legal justifications, essentially all governments have laws and regulations that allow for the implementation of quarantine in some circumstances. In the United States, these laws are primarily at the state rather than the federal level, which means that it is important for public health professionals to be familiar with the specific legal requirements in their locality. (Evidence source: committee discussion drawing on key ethics and policy texts. Refer to Section 8, “Ethical Considerations,” in Appendix B4 for additional detail.)
CONSIDERATIONS FOR IMPLEMENTATION
The following considerations for implementation were drawn from the syntheses of quantitative comparative studies, modeling studies, qualitative research studies, and case reports, as well as descriptive surveys, the findings of which are presented in Appendix B4. Note that this is not an exhaustive list of considerations; additional implementation resources should be consulted before the practice recommendation is implemented.
Facilitating Adherence to and Minimizing Harms from Quarantine Measures
Ensure Transparent and Strategic Risk Communication Using Clear Definitions
Communication strategies can increase adherence to quarantine, and frequent and transparent communication with the public is likely to ease fear and anxiety. Communication needs to take place over the full course of the event; strive to be bidirectional; and involve multiple channels, such as mass media and education campaigns via billboards and bus advertisements, and multiple sources. Effective communication will provide information about the contagious disease and the need and instructions for the quarantine measures. It is important in these communications not to arouse fear and anxiety, not to be stigmatizing, not to use terms with confusing meanings, and to include clear and consistent information about infection control and coping strategies. Anecdotal evidence shows that basic knowledge of the pathogen at hand is associated with willingness to adhere to quarantine measures and suggests that the higher the perception of risk, the more likely people are to do what they
say they are going to do with respect to quarantine. Public health agencies need to consider these issues when developing communication strategies. (Evidence source: synthesis of evidence of effect, qualitative evidence synthesis, case report evidence synthesis, and descriptive survey study evidence. Refer to Section 9, “Facilitating Adherence to and Minimizing Harms from Quarantine Measures,” in Appendix B4 for additional detail.)
Adapt Policy: Voluntary Versus Legally Enforced Quarantine
Some modeling studies indicate that adherence may be more likely with less strict quarantine procedures, leading to greater effectiveness. In other words, quarantine may be more effective when the people on whom it is imposed adhere voluntarily to the quarantine restrictions rather than adhering under the threat of legal enforcement, perhaps because people adhere out of an altruistic choice (of which they are proud) rather than an enforced obligation (of which they are resentful or ashamed). Another factor that may make quarantine restrictions more acceptable is allowing reasonable modifications of rules and procedures to suit the needs of the situation and those being placed under quarantine. These factors may be particularly relevant in societies that place greater value on individual liberties. In sum, while some legally enforceable quarantine strategies may be relevant in the U.S. context, more intrusive or aggressive measures may provoke greater resistance and make quarantine less effective. If quarantine is legally enforced, public health agencies need to ensure that a legal framework and a clear process for carrying out proposed enforcement measures are in place. (Evidence source: synthesis of modeling studies, qualitative evidence synthesis, and case report evidence synthesis. Refer to Section 9, “Facilitating Adherence to and Minimizing Harms from Quarantine Measures,” in Appendix B4 for additional detail.)
Provide Financial Compensation, Food, and Social and Psychological Support
Factors that may make quarantine measures more acceptable include the provision of financial compensation for lost work or access to employment leave, provision of food and other basic necessities, and provision of social and psychological support by governmental or other agencies. This compensation may include partial or full income replacement for the duration of the quarantine; assurance of job security after the quarantine ends; and payment for child care, rent, water, electricity, and other utilities. The government and other agencies can deliver food and basic necessities directly to people in quarantine, or agencies can assist neighbors, friends, and volunteers with the purchase and delivery of such items. An important consideration is matching food support to the dietary needs and preferences of the people under quarantine. Social and psychological support can take many forms, including dedicated or preexisting general confidential telephone hotlines that provide professional counseling, in-person mental health services, provision of social services by local health or civic affairs departments, daycare, and community committees mobilizing for such gestures as comforting letters and prayer services. Engaging a wide range of community partners such as businesses, schools, charitable organizations, community and faith-based organizations, and mental health resources can help in preparing resources to meet potential needs in the event of a quarantine. (Evidence source: synthesis of evidence of effect, qualitative evidence synthesis, case report evidence synthesis, and descriptive survey study evidence. Refer to Section 9, “Facilitating Adherence to and Minimizing Harms from Quarantine Measures,” in Appendix B4 for additional detail.)
Use Culturally and Contextually Relevant Approaches: A Community and Care Orientation
Agencies need to keep in mind that the impact of quarantine at the community level may be more important to the members of the community on which quarantine is imposed as opposed to the level of the individual or the abstract “common good.” When quarantine is imposed on some individuals in a community, especially one with tight social bonds, the life of the whole community may be affected. Thus, to ensure that individuals on whom quarantine is imposed adhere to proposed restrictions, agencies need to understand the life circumstances, economic status, political history, level of trust in agencies and government, and cultural and religious customs of the community to which those individuals belong and work in cooperation with its existing power and leadership social structures. The approach adopted by agencies in their interactions with people under quarantine needs to embody care, showing concern for their needs and extending empathetic support. Such an approach stands in contrast to one that emphasizes control and enforcement. Trusted local leaders can help facilitate trust and act as liaisons between the community and district health authorities, and integrating them into response planning and allowing them to provide feedback before decisions related to public health interventions are made may promote adherence to quarantine measures. (Evidence source: qualitative evidence synthesis, case report evidence synthesis, and descriptive survey study evidence. Refer to Section 9, “Facilitating Adherence to and Minimizing Harms from Quarantine Measures,” in Appendix B4 for additional detail.)
Other Implementation Considerations
The following conceptual findings inform the perspectives and approaches public health agencies could consider when implementing quarantine.
Define the Effectiveness of Quarantine More Broadly
Agencies and researchers often judge the effectiveness of quarantine from one of two perspectives: it is deemed effective (or not) either (1) if it reduces or stops the spread of a contagious disease, or (2) if people in quarantine adhere to its rules. Yet, because quarantine represents a significant restriction on individual liberty and is essentially always imposed on people who would rather not be subjected to it, at least two additional effectiveness criteria need to be considered when evaluating a quarantine action: the extent to which the quarantine measures succeed in (1) protecting the civil rights of quarantined individuals, including due process; and (2) protecting quarantined individuals from experiencing avoidable harms, including social, financial, psychological, and medical harms. (Evidence source: qualitative evidence synthesis and case report evidence synthesis. Refer to Section 10, “Other Implementation Considerations,” in Appendix B4 for additional detail.)
Develop Options for Different Levels of Quarantine and Plans for Integration with Other NPIs
Agencies can enhance the effectiveness of quarantine by developing screening and monitoring criteria that allow for graded options for quarantine that are matched to the characteristics of the contagious disease at hand, its spread, and the risk of exposure. Modeling studies that explore quarantine efforts in various localities or focus differential quarantine efforts on locally exposed individuals and travelers entering an area suggest that the relative
value of these efforts depends on the fraction of an epidemic or outbreak driven by local transmission versus imported cases. Local quarantine efforts can have direct and indirect spillover effects. If quarantine is used to help control an outbreak in one area, nearby areas may face fewer imported cases; hence, the need for implementing quarantine in these surrounding areas may be reduced (an example of direct spillover). Moreover, chains of such spillovers to areas not directly connected to the original area can occur, which may alter the need for or required level and speed of quarantine in these areas as well (indirect spillover). As a result, if quarantines are implemented in an uncoordinated manner in multiple areas, redundancy and excess effort and resource expenditure may occur. Additionally, modeling studies that compare quarantine with other, less invasive or intensive NPIs note that it may be possible to achieve similar levels of control using these alternatives without the potential social stigma of quarantine, its potential to cause social and economic disruption, and its potential large-scale use of resources. This may be especially true for less transmissible infections or those that have a very short or no asymptomatic infectious period. (Evidence source: synthesis of modeling studies and qualitative evidence synthesis. Refer to Section 10, “Other Implementation Considerations,” in Appendix B4 for additional detail.)
Consider Implementing Quarantine Early, Especially When There Is a Shortage or Absence of Available Medical Countermeasures
At the start of a contagious disease outbreak, there may be a shortage or absence of countermeasures such as drugs and vaccines. Similarly, there may be regions in the country where the stockpile of drugs and vaccines is limited or the delivery of such supplies will take time because of remoteness. In these circumstances, NPIs, including quarantine, may be the only measures available to combat the outbreak. Modeling studies suggest that quarantine is more effective when implemented earlier in an outbreak, and even a relatively ineffective quarantine may help blunt or slow the epidemic curve, allowing more time for resources to arrive in the area. (Evidence source: synthesis of modeling studies, qualitative evidence synthesis, and case report evidence synthesis. Refer to Section 10, “Other Implementation Considerations,” in Appendix B4 for additional detail.)
Integrate and Coordinate Response at the Systems Level
Multiple and often competing interests are involved in deciding whether, when, and how to implement quarantine. Agencies need to keep in mind that the planning and implementation of quarantine require interagency and multisectoral cooperation, encompassing both the legal and political systems. Planning also needs to consider the scalability of operations, as the number of people placed in quarantine may rise during the course of a contagious disease event. Robust preexisting organizational frameworks can enable efficient redirection of the resources necessary to implement quarantine. Collaborative agreements and coordinated incident command are essential for incidents involving multiple jurisdictions (e.g., civilian, military, federal, tribal). A strong sense of political will and a shared sense of urgency also facilitate the rapid establishment of command structures aimed at steering action and mobilizing relevant sectors and resources. The need for flexibility is important as well, as existing plans and predetermined control measures may need to be modified as the event evolves. Public health agencies also need to coordinate on and plan for when and how to lift quarantine measures and what will happen as and after quarantine measures are lifted. (Evidence source: qualitative evidence synthesis and case report evidence synthesis. Refer to Section 10, “Other Implementation Considerations,” in Appendix B4 for additional detail.)
EVIDENCE GAPS AND FUTURE RESEARCH PRIORITIES
The committee noted several design limitations in the studies included in this review that could be addressed in future research. There have been few quantitative comparative studies of when quarantine is effective at reducing the spread of contagious disease, and of these, some relied on inadequate outcome measures; for example, the use of rapid diagnostic testing and clinical diagnosis rather than laboratory-confirmed disease may have resulted in greatly underestimated numbers of infections. Several of the quantitative studies of quarantine evaluated effectiveness only with regard to adherence (an intermediate outcome, measuring the effectiveness of implementation) and not with regard to the effects of quarantine on the course of the outbreak. Whenever possible, it is important for studies to include measures of the impact of quarantine on the outbreak. Additionally, the authors of some studies of effectiveness do not report whether any of the quarantined individuals ended up infected. This is an essential outcome to report since a quarantine that sequesters only healthy people is, by definition, ineffective at reducing disease transmission. Because it is difficult to evaluate quarantine using randomized controlled trials, researchers need to ensure that robust data are used in any future experimental studies.
During a pandemic, CDC has advised public health agencies (including the agency itself) to carry out monitoring and evaluation (M&E) of NPIs and collect data on
- the degree of transmission and the severity of the pandemic;
- the type and extent of NPI implementation;
- the level of adherence to NPI measures, the emergence of intervention fatigue, and the effectiveness of NPIs in mitigating a pandemic’s impact (e.g., effects on virus transmission, hospitalizations, and deaths); and
- secondary negative effects of NPIs and the effectiveness of strategies for mitigating those effects (Qualls et al., 2017).
To capture these data, M&E systems, capacities, and capabilities need to be established before a pandemic occurs. Quasi-experimental designs could make use of these data to evaluate the effectiveness of quarantine.
In addition to measuring the impact of quarantine on the spread of illness and studying metrics related to the effectiveness of implementation (adherence), quarantine needs to be recognized as reflecting an infringement of basic human rights of freedom of movement and association. Accordingly, it is important to incorporate at least two additional outcomes into evaluations of quarantine actions: the extent to which the quarantine procedures succeed in (1) protecting the civil rights of quarantined individuals, including due process; and (2) protecting quarantined individuals from experiencing avoidable harms (including social, financial, mental health, and medical harms). Finally, because quarantine tends to affect many people in a community, not just those who are quarantined, the impact of implementing a quarantine on a community, and even states or the country as a whole, needs to be examined. In its review, the committee considered outcomes related to both psychological and financial harms. Many of the quantitative studies that addressed these outcomes were of poor methodological quality—they used a cross-sectional survey design, had sample size limitations, were conducted months after the implementation of quarantine (i.e., postintervention), and used scales that may not have been validated. Future research on the secondary effects of quarantine, including harms, will need to apply more rigorous methods.
Future studies also will need to clearly define the quarantine protocol used and its components (e.g., type of quarantine, type of support provided, types of resources required). One challenge with reviewing evidence on quarantine is that NPIs are often implemented in bundles. Studies examining quarantine in real circumstances or in models often include effects from screening and isolation; vaccination programs (if possible); and social distancing or other behavioral changes, such as avoiding public transit, wearing masks, and increasing handwashing. The multifaceted nature of NPI use in real-world implementation makes it difficult to discern the specific impact of quarantine. Research on quarantine could benefit from advances in the study of complex interventions in the fields of health care and humanitarian aid (see Chapter 8 for additional detail regarding methodological improvements).
Much of the evidence on the effectiveness of quarantine is reliant on mathematical and statistical modeling and simulation studies. The committee found modeling studies using empirical data from actual outbreaks to be particularly useful. Real-time, rapid modeling during an outbreak or epidemic has proven valuable in guiding decision making during response (Rivers et al., 2019), and further efforts to expand the capability for and coordination and use of such real-time modeling would be helpful. Additional modeling research focused on identifying the impact on the effectiveness of quarantine of the pathogen involved, the host (if an animal vector), and population differences would also be beneficial.
As previously noted, many questions regarding quarantine relate to its implementation. The qualitative literature is useful in examining the barriers to and facilitators of the implementation of quarantine, but additional qualitative research is warranted to describe specific aspects of quarantine from the perspectives of both the agencies that implement it and the people on whom it is imposed. As multiple, and often competing, interests (e.g., political, the public) are involved in quarantine decision making, analysis and synthesis of findings from individual media reports could be informative. Indeed, a recent WHO guideline on emergency risk communications reflects the incorporation of a synthesis of media reports into the review on which the guideline is based (WHO, 2017). In addition, no studies included in the committee’s review examined quarantine (simulated or real) implemented by tribal or territorial public health agencies or imposed upon those populations, which the committee believes is a significant gap in understanding the effectiveness of quarantine in these con-
texts. It will be important for future qualitative research to make a point of seeking out best practices in these areas. Moreover, there is a need for greater investment in implementation science methods and approaches for evaluating aspects of quarantine implementation.
Quarantine and the COVID-19 Pandemic
In response to COVID-19, states and localities have been implementing combinations of various NPIs, such as social distancing, cancellation of mass gatherings, school and business closures, isolation and quarantine, and shelter-in-place and stay-at-home orders, among others, at different intensities and speeds. At the time of this writing, WHO and CDC were recommending 14 days of quarantine for individuals having had close contact with a confirmed COVID-19 case (Jernigan, 2020; WHO, 2020). This duration was based on the virus’s estimated incubation period. The committee concluded that many of the findings from its mixed-method review are transferrable to COVID-19, as the evidence was drawn from a number of different quarantine episodes, including similar severe coronavirus outbreaks (SARS and MERS).
Since the onset of the COVID-19 pandemic, several rapid reviews of the evidence have examined the effectiveness of quarantine alone or in combination with other public health measures, adherence to quarantine, and the psychological impact of quarantine (Brooks et al., 2020; Nussbaumer-Streit et al., 2020; Webster et al., 2020). Findings from these rapid reviews are consistent with those of the committee’s review. Findings from a Cochrane review examining the effectiveness of quarantine during severe coronavirus outbreaks (which included 10 modeling studies on COVID-19) indicate that quarantine is important in reducing disease incidence and mortality and that early implementation of quarantine is important to ensuring its effectiveness (Nussbaumer-Streit et al., 2020). Webster and colleagues (2020) examined the published literature on reasons for and factors associated with adherence to quarantine and found that the main factors associated with adherence were the knowledge people had about the disease and quarantine procedures, social norms, perceived benefits and risks, and such practical issues as running out of supplies or financial consequences. A rapid review of the evidence on the psychological impacts of quarantine found that quarantine results in posttraumatic stress symptoms, confusion, and anger and that to reduce the psychological impacts, officials should quarantine individuals for no longer than required, provide a clear rationale for quarantine and information about protocols, and ensure the provision of sufficient supplies (Brooks et al., 2020). Brooks and colleagues also note that quarantine may have long-lasting psychological effects.
Given the rapid and evolving nature of the COVID-19 pandemic and the speed with which new studies are being published on non-peer-reviewed, preprint servers, the committee was unable to update its evidence review at the time of this writing to incorporate studies examining the implementation of quarantine as applied to COVID-19. Additionally, given that China was the first country to observe the novel coronavirus, relevant published data are more widely available from China, which implemented sweeping control measures, such as cordon sanitaire, that were beyond the scope of this review. However, it will be important to expand and update this review of quarantine once the field has rigorously collected, analyzed, and published such data.
The COVID-19 pandemic, like past epidemics, has illustrated gaps and themes related to designing and rapidly executing scientific research specifically on quarantine during the response phase. Chapter 8 addresses the importance of having in place in nonemergency times the infrastructure needed to be able to identify research priorities and support the deployment of rapid response teams with applied research expertise during a public health
emergency. Perhaps not surprisingly, mathematical and statistical modeling, epidemiological models, and simulation studies have dominated the research on quarantine, further emphasizing the importance of continuing to improve review methodologies to evaluate and incorporate these types of studies into reviews of the evidence. As different geographic areas have been implementing quarantine and other NPIs in various combinations and at different intensities and speeds, comparing the effectiveness of these strategies (e.g., by using a matched comparison group design; see Chapter 8 for additional detail) will help inform preparedness and response efforts for future pandemics. Additionally, as a complement to effectiveness research, qualitative research is vital for understanding and capturing the social responses to and implications of quarantine and this pandemic.
Many of the issues discussed in the committee’s review, including the timing of quarantine implementation; voluntary versus mandatory enforcement of quarantine; harms of quarantine; communication strategies; and financial, food, social, and psychological support for quarantined individuals, will require further examination in the context of the COVID-19 pandemic. A critical research gap highlighted by the pandemic is evidence on when and how to lift quarantine measures. During and following the COVID-19 pandemic, it will be crucial to coordinate research efforts to ensure that the priority questions related to quarantine are answered with appropriate and rigorous methods.
REFERENCES
References marked with an asterisk (*) are formally included in the mixed-method review. The full reference list of articles included in the mixed-method review can be found in Appendix B4.
*Ahn, I., S. Heo, S. Ji, K. H. Kim, T. Kim, E. J. Lee, J. Park, and K. Sung. 2018. Investigation of nonlinear epidemiological models for analyzing and controlling the MERS outbreak in Korea. Journal of Theoretical Biology 437:17–28.
Aiello, A. E., R. M. Coulborn, T. J. Aragon, M. G. Baker, B. B. Burrus, B. J. Cowling, A. Duncan, W. Enanoria, M. P. Fabian, Y. H. Ferng, E. L. Larson, G. M. Leung, H. Markel, D. K. Milton, A. S. Monto, S. S. Morse, J. A. Navarro, S. Y. Park, P. Priest, S. Stebbins, A. M. Stern, M. Uddin, S. F. Wetterhall, and C. J. Vukotich, Jr. 2010. Research findings from nonpharmaceutical intervention studies for pandemic influenza and current gaps in the research. American Journal of Infection Control 38(4):251–258.
Aledort, J. E., N. Lurie, J. Wasserman, and S. A. Bozzette. 2007. Non-pharmaceutical public health interventions for pandemic influenza: An evaluation of the evidence base. BMC Public Health 7:208.
*An der Heiden, M., U. Buchholz, G. Krause, G. Kirchner, H. Claus, and W. H. Haas. 2009. Breaking the waves: Modelling the potential impact of public health measures to defer the epidemic peak of novel influenza A/H1N1. PLOS ONE 4(12):e8356.
Asgary, R., J. A. Pavlin, J. A. Ripp, R. Reithinger, and C. S. Polyak. 2015. Ebola policies that hinder epidemic response by limiting scientific discourse. American Journal of Tropical Medicine & Hygiene 92(2):240–241.
*Barbisch, D., K. L. Koenig, and F. Y. Shih. 2015. Is there a case for quarantine? Perspectives from SARS to Ebola. Disaster Medicine and Public Health Preparedness 9(5):547–553.
*Binns, P. L., V. Sheppeard, and M. P. Staff. 2010. Isolation and quarantine during pandemic (H1N1) 2009 influenza in NSW: The operational experience of public health units. New South Wales Public Health Bulletin 21(1–2):10–15.
Brooks, S. K., R. K. Webster, L. E. Smith, L. Woodland, S. Wessely, N. Greenberg, and G. J. Rubin. 2020. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet 395(10227):912–920.
*CDC (Centers for Disease Control and Prevention). 2004. Postexposure prophylaxis, isolation, and quarantine to control an import-associated measles outbreak—Iowa, 2004. Morbidity and Mortality Weekly Report 53(41):969–971.
CDC. 2017. Quarantine and isolation. https://www.cdc.gov/quarantine/index.html (accessed January 21, 2020).
CDC. 2018. Public health emergency preparedness and response capabilities: National standards for state, local, tribal, and territorial public health. Atlanta, GA: Centers for Disease Control and Prevention. https://www.cdc.gov/cpr/readiness/00_docs/CDC_PreparednesResponseCapabilities_OctOcto2018_Final_508.pdf (accessed March 19, 2020).
CDC. 2020. CDC issues federal quarantine order to repatriated U.S. citizens at March Air Reserve Base. https://www.cdc.gov/media/releases/2020/s0131-federal-quarantine-march-air-reserve-base.html (accessed May 21, 2020).
Chin, B. S., Y. T. Chae, H. K. Choi, J. H. Baek, S. J. Jin, S. Y. Shin, S. H. Han, J. Y. Choi, C. O. Kim, Y. G. Song, S. H. Jeong, and J. M. Kim. 2012. Viral shedding of 2009 pandemic H1N1 and evaluation of quarantine recommendations. Japanese Journal of Infectious Diseases 65(2):105–110.
*Collier, M. G., A. Cierzniewski, T. Duszynski, C. Munson, M. Wenger, B. Beard, R. Gentry, J. Duwve, P. K. Kutty, and P. Pontones. 2013. Measles outbreak associated with international travel, Indiana, 2011. Journal of the Pediatric Infectious Diseases Society 2(2):110–118.
Copeland, D. L., R. Basurto-Davila, W. Chung, A. Kurian, D. B. Fishbein, P. Szymanowski, J. Zipprich, H. Lipman, M. S. Cetron, M. I. Meltzer, and F. Averhoff. 2012. Effectiveness of a school district closure for pandemic influenza A (H1N1) on acute respiratory illnesses in the community: A natural experiment. Clinical Infectious Diseases 56(4):509–516.
*Day, T., A. Park, N. Madras, A. Gumel, and J. Wu. 2006. When is quarantine a useful control strategy for emerging infectious diseases? American Journal of Epidemiology 163(5):479–485.
*Drews, K. 2013. A brief history of quarantine. The Virginia Tech Undergraduate Historical Review 2. http://doi.org/10.21061/vtuhr.v2i0.16.
*D’Silva, J. P., and M. C. Eisenberg. 2017. Modeling spatial invasion of Ebola in West Africa. Journal of Theoretical Biology 428:65–75.
*Enanoria, W. T., F. Liu, J. Zipprich, K. Harriman, S. Ackley, S. Blumberg, L. Worden, and T. C. Porco. 2016. The effect of contact investigations and public health interventions in the control and prevention of measles transmission: A simulation study. PLOS ONE 11(12):e0167160.
*Feng, Z., Y. Yang, D. Xu, P. Zhang, M. M. McCauley, and J. W. Glasser. 2009. Timely identification of optimal control strategies for emerging infectious diseases. Journal of Theoretical Biology 259(1):165–171.
*Gahr, P., A. S. DeVries, G. Wallace, C. Miller, C. Kenyon, K. Sweet, K. Martin, K. White, E. Bagstad, C. Hooker, G. Krawczynski, D. Boxrud, G. Liu, P. Stinchfield, J. LeBlanc, C. Hickman, L. Bahta, A. Barskey, and R. Lynfield. 2014. An outbreak of measles in an undervaccinated community. Pediatrics 134(1):e220–e228.
*Gastanaduy, P. A., J. Budd, N. Fisher, S. B. Redd, J. Fletcher, J. Miller, D. J. McFadden, 3rd, J. Rota, P. A. Rota, C. Hickman, B. Fowler, L. Tatham, G. S. Wallace, S. de Fijter, A. Parker Fiebelkorn, and M. DiOrio. 2016. A measles outbreak in an underimmunized Amish community in Ohio. New England Journal of Medicine 375(14):1343–1354.
Gensini, G. F., M. H. Yacoub, and A. A. Conti. 2004. The concept of quarantine in history: From plague to SARS. Journal of Infection 49(4):257–261.
*Gupta, A. G., C. A. Moyer, and D. T. Stern. 2005. The economic impact of quarantine: SARS in Toronto as a case study. Journal of Infection 50(5):386–393.
*Hsieh, Y. H., C. C. King, C. W. Chen, M. S. Ho, S. B. Hsu, and Y. C. Wu. 2007. Impact of quarantine on the 2003 SARS outbreak: A retrospective modeling study. Journal of Theoretical Biology 244(4):729–736.
Jernigan, D. B. 2020. Update: Public health response to the coronavirus disease 2019 outbreak—United States. Morbidity and Mortality Weekly Report 69(8):216–219.
Lai, S., N. W. Ruktanonchai, L. Zhou, O. Prosper, W. Luo, J. R. Floyd, A. Wesolowski, M. Santillana, C. Zhang, X. Du, H. Yu, and A. J. Tatem. 2020. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature. https://doi.org/10.1038/s41586-020-2293-x.
Love, E. G., K. N. Reed-Hirsch, and L. J. Kilborn. 2007. The role of nonpharmaceutical interventions during a pandemic. Texas Medicine 103(10):42–44.
MacDougall, H. 2007. Toronto’s health department in action: Influenza in 1918 and SARS in 2003. Journal of the History of Medicine & Allied Sciences 62(1):56–89.
Markel, H., A. M. Stern, J. A. Navarro, J. R. Michalsen, A. S. Monto, and C. DiGiovanni. 2006. Nonpharmaceutical influenza mitigation strategies, U.S. communities, 1918–1920 pandemic. Emerging Infectious Diseases 12(12):1961–1964.
Markel, H., H. B. Lipman, J. A. Navarro, A. Sloan, J. R. Michalsen, A. M. Stern, and M. S. Cetron. 2007. Nonpharmaceutical interventions implemented by US cities during the 1918–1919 influenza pandemic. Journal of the American Medical Association 298(6):644–654.
*Meltzer, M. I., I. Damon, J. W. LeDuc, and J. D. Millar. 2001. Modeling potential responses to smallpox as a bioterrorist weapon. Emerging Infectious Diseases 7(6):959–969.
Miles, S. H. 2015. Kaci Hickox: Public health and the politics of fear. American Journal of Bioethics 15(4):17–19.
*Mubayi, A., C. K. Zaleta, M. Martcheva, and C. Castillo-Chavez. 2010. A cost-based comparison of quarantine strategies for new emerging diseases. Mathematical Biosciences & Engineering 7(3):687–717.
Nussbaumer-Streit, B., V. Mayr, A. I. Dobrescu, A. Chapman, E. Persad, I. Klerings, G. Wagner, U. Siebert, C. Christof, C. Zachariah, and G. Gartlehner. 2020. Quarantine alone or in combination with other public health measures to control COVID 19: A rapid review. Cochrane Database of Systematic Reviews 4(CD013574). doi: 10.1002/14651858.CD013574.
Oh, M.-D., W. B. Park, S.-W. Park, P. G. Choe, J. H. Bang, K.-H. Song, E. S. Kim, H. B. Kim, and N. J. Kim. 2018. Middle East Respiratory Syndrome: What we learned from the 2015 outbreak in the Republic of Korea. The Korean Journal of Internal Medicine 33(2):233–246.
*Peak, C. M., L. M. Childs, Y. H. Grad, and C. O. Buckee. 2017. Comparing nonpharmaceutical interventions for containing emerging epidemics. Proceedings of the National Academy of Sciences of the United States of America 114(15):4023–4028.
*Podder, C. N., A. B. Gumel, C. S. Bowman, and R. G. McLeod. 2007. Mathematical study of the impact of quarantine, isolation and vaccination in curtailing an epidemic. Journal of Biological Systems 15(02):185–202.
Qualls, N., A. Levitt, N. Kanade, N. Wright-Jegede, S. Dopson, M. Biggerstaff, C. Reed, and A. Uzicanin. 2017. Community mitigation guidelines to prevent pandemic influenza—United States, 2017. Morbidity and Mortality Weekly Report 66:1–34. http://dx.doi.org/10.15585/mmwr.rr6601a1externalicon.
Rivers, C., J.-P. Chretien, S. Riley, J. A. Pavlin, A. Woodward, D. Brett-Major, I. Maljkovic Berry, L. Morton, R. G. Jarman, M. Biggerstaff, M. A. Johansson, N. G. Reich, D. Meyer, M. R. Snyder, and S. Pollett. 2019. Using “outbreak science” to strengthen the use of models during epidemics. Nature Communications 10(1):3102.
Sattenspiel, L., and D. A. Herring. 2003. Simulating the effect of quarantine on the spread of the 1918–19 flu in central Canada. Bulletin of Mathematical Biology 65(1):1–26.
Sell, T. K., M. P. Shearer, D. Meyer, M. Leinhos, E. G. Carbone, and E. Thomas. 2019. Influencing factors in the development of state-level movement restriction and monitoring policies in response to Ebola, United States, 2014–15. Health Security 17(5):364–371.
Sugerman, D. E., A. E. Barskey, M. G. Delea, I. R. Ortega-Sanchez, D. Bi, K. J. Ralston, P. A. Rota, K. Waters-Montijo, and C. W. Lebaron. 2010. Measles outbreak in a highly vaccinated population, San Diego, 2008: Role of the intentionally undervaccinated. Pediatrics 125(4):747–755.
Svoboda, T., B. Henry, L. Shulman, E. Kennedy, E. Rea, W. Ng, T. Wallington, B. Yaffe, E. Gournis, E. Vicencio, S. Basrur, and R. H. Glazier. 2004. Public health measures to control the spread of the severe acute respiratory syndrome during the outbreak in Toronto. New England Journal of Medicine 350(23):2352–2361.
Webster, R. K., S. K. Brooks, L. E. Smith, L. Woodland, S. Wessely, and G. J. Rubin. 2020. How to improve adherence with quarantine: Rapid review of the evidence. Public Health 182:163–169.
WHO (World Health Organization). 2017. Communicating risk in public health emergencies. Geneva, Switzerland: World Health Organization. https://apps.who.int/iris/bitstream/handle/10665/259807/9789241550208-eng.pdf;jsessionid=E5F98FC8DA6FB72F155C32FD528A7955?sequence=2 (accessed March 19, 2020).
WHO. 2019. Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza. Geneva, Switzerland: World Health Organization. https://apps.who.int/iris/bitstream/handle/10665/329438/9789241516839-eng.pdf?ua=1 (accessed March 19, 2020).
WHO. 2020. Considerations for quarantine of individuals in the context of containment for coronavirus disease (COVID-19). Geneva, Switzerland: World Health Organization. www.who.int/internal-publications-detail/considerations-for-quarantineof-individuals-in-the-context-of-containment-for-coronavirusdisease-(covid-19) (accessed May 7, 2020).
Zhang, Y., P. Yang, S. Liyanage, H. Seale, Y. Deng, X. Pang, L. Tian, B. Liu, L. Zhang, and Q. Wang. 2011. The characteristics of imported cases and the effectiveness of outbreak control strategies of pandemic influenza A (H1N1) in China. Asia Pacific Journal of Public Health 24(6):932–939.

























