
B4
Mixed-Method Review of Implementing Quarantine to Reduce or Stop the Spread of a Contagious Disease
This appendix provides a detailed description of the methods for and the evidence from the mixed-method review examining the implementation of quarantine to reduce the spread of a contagious disease, which is summarized in Chapter 7.1
KEY REVIEW QUESTIONS AND ANALYTIC FRAMEWORK
Theoretically, the perceived benefit of quarantine is effective curbing of the spread of contagious diseases by not allowing person-to-person transmission. Therefore, the primary question posed by the committee in this review is: “In what circumstances (e.g., based on biologic factors, risks, resource availability, legal authorities, social context) is quarantine effective in reducing or stopping the spread of a contagious disease?” To answer this primary question, the committee sought evidence on several sub-questions related to evidence on the pros and cons of specific adherence strategies, the documented benefits and harms of implementing quarantine, and the factors that create barriers to and facilitators of its implementation (see Box B4-1).
For the purposes of this review, the committee developed an analytic framework to present the causal pathway and interactions between quarantine and its components, populations, and outcomes of interest (see Figure B4-1). The mechanism by which quarantine can ultimately reduce or stop the spread of contagious disease is well established and noncontroversial: there is a period of time (the incubation period) between when a person is exposed to a contagious illness and when that person, if infected, becomes contagious to others; and if individuals who are exposed and become infected are not in contact with anyone else at the time they become contagious, they cannot spread the infection (Drews, 2013).
___________________
1 This appendix draws heavily on four reports commissioned by the committee: “Data Extraction and Quality Assessment: Methodology and Evidence Tables” by the Brown University Center for Evidence Synthesis in Health; “Quarantine as a Non-Pharmaceutical Intervention: Qualitative Research Evidence Synthesis” by Pradeep Sopory and Julie Novak; “Use of Quarantine as a Non-Pharmaceutical Intervention for Public Health Emergencies: Findings from Case Reports” by Sneha Patel; and “In What Situations Do Modeling Studies Suggest Quarantine is More Versus Less Effective to Control Infectious Disease Outbreaks?” by Jeremy Goldhaber-Fiebert (see Appendix C).
EVIDENCE SUPPORTING THE PRACTICE RECOMMENDATION
This section summarizes the evidence from the mixed-method review examining implementing quarantine to reduce or stop the spread of a contagious disease. It begins with a description of the results of the literature search and then summarizes the evidence of effectiveness. In formulating its practice recommendation, the committee considered evidence beyond effectiveness, which was compiled using an Evidence to Decision (EtD) framework encompassing balance of benefits and harms, acceptability and preferences, feasibility and public health emergency preparedness and response (PHEPR) system considerations, resource and economic considerations, equity, and ethical considerations. The evidence from each methodological stream applicable to each of the EtD criteria is discussed; a synthesis is provided in Table B4-10 later in this appendix and in Chapter 7. Graded finding statements from evidence syntheses are italicized in the narrative below.
Full details about the study eligibility criteria, search strategy, and processes for data extraction and individual study quality assessment are available in Appendix A. Appendix C links to all the commissioned analyses informing this review.
Results of the Literature Search
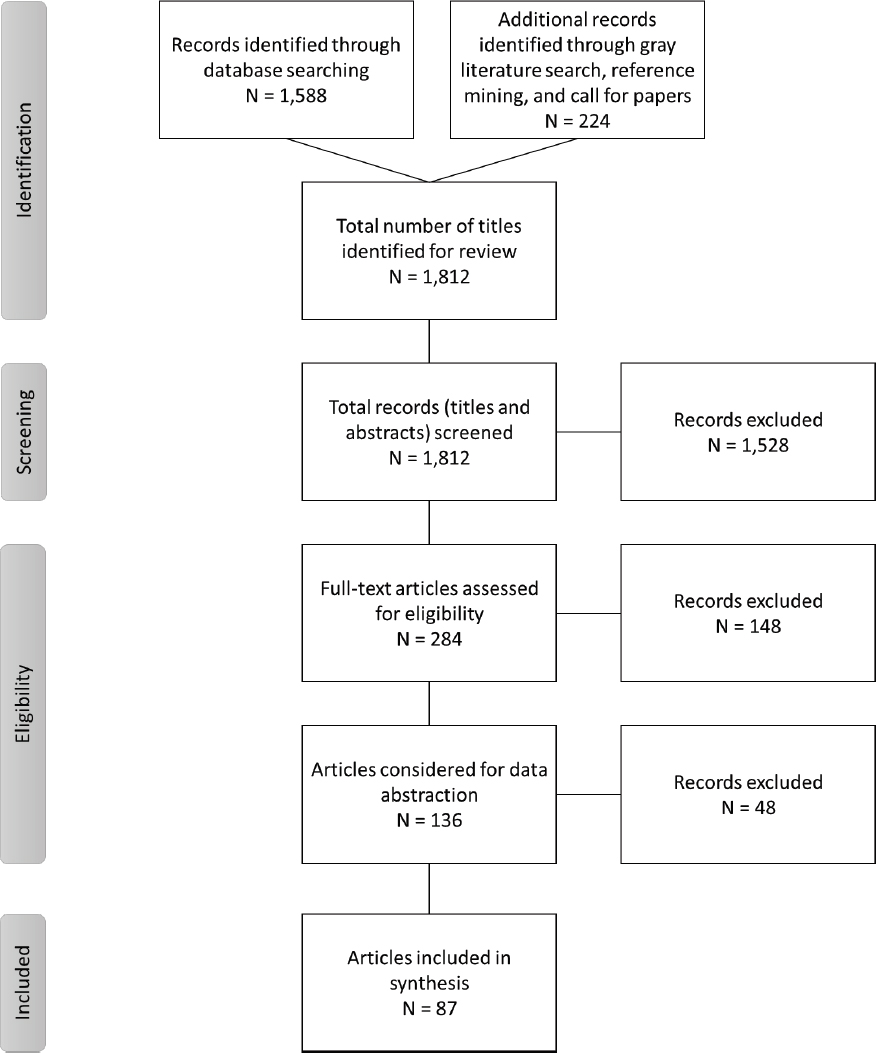
The searches of bibliographic databases identified a total of 1,588 potentially relevant citations (deduplicated) for the mixed-method review of implementing quarantine to reduce or stop the spread of a contagious disease. A search of the gray literature, reference mining, and a call for reports contributed an additional 224 articles. All 1,812 citations were imported into EndNote and were included in title and abstract screening. During screening, 1,528 articles were excluded because their abstracts did not appear to answer any of the key questions or they indicated that the articles were commentaries, editorials, or opinion pieces. After the abstracts had been reviewed, 284 full-text articles were reviewed and assessed for eligibility for inclusion in the mixed-method review. The committee considered 136 articles for data extraction and ultimately included 88 articles in the mixed-method review. Figure B4-2 depicts the literature flow, indicating the number of articles included and excluded at each screening stage. Table B4-1 indicates the types of evidence included in this review.
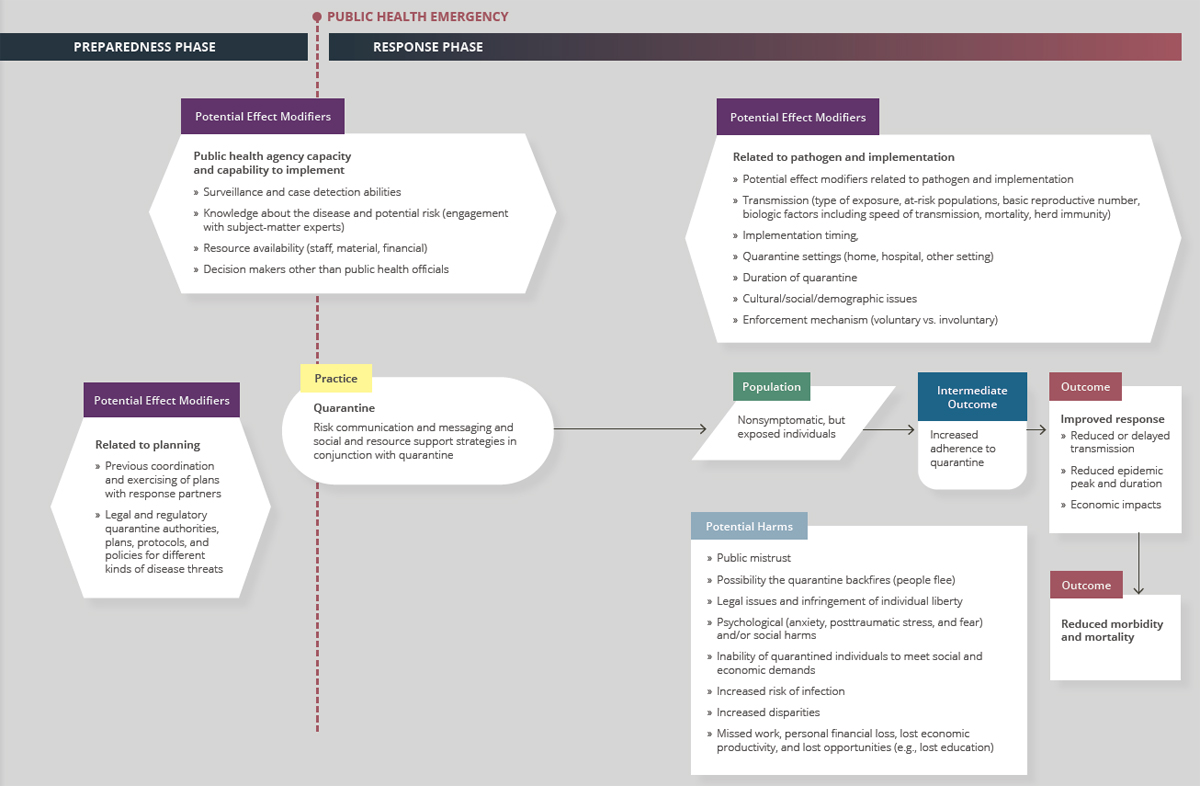
NOTE: Arrows in the framework indicate hypothesized causal pathways between interventions and outcomes.
| Evidence Typea | Number of Studies (as applicable)b | |
|---|---|---|
| Quantitative comparative | 9 | |
| Quantitative noncomparative (postintervention measure only) | 4 | |
| Qualitative | 16 | |
| Modeling | 12c | |
| Descriptive surveys | 13 | |
| Case reports | 28 | |
| After action reports | N/A | |
| Mechanisticd | Yes | |
| Parallel (systematic reviews) | N/A | |
a Evidence types are defined in Chapter 3.
b Note that sibling articles (different results from the same study published in separate articles) are counted as one study in this table. Mixed-method studies may be counted in more than one category.
c The committee chose a sample of 12 studies out of 47 modeling studies for detailed review based on an assessment of their methodologic approach, data sources, relevance to the key questions for this practice, potential implications for public health practice, and disease condition studied. Given the time and resources available, the committee had to exclude a number of well-conducted modeling studies. Studies were excluded from detailed review if they reported major limitations to their model conclusions due to such factors as excessive uncertainty about modeling parameter values.
d For the purposes of this report, the committee defined mechanistic evidence as relationships for which causality has been established—generally from other scientific fields, such as chemistry, biology, economics, and physics (e.g., the accelerating effect of the gravitational attraction of Earth and the slowing effect of air resistance)—which can reasonably be applied to the PHEPR context through mechanistic reasoning. Mechanistic evidence is further discussed in Chapter 3.
1. Determining Evidence of Effect
Three quantitative comparative studies addressed the overarching key question regarding in what circumstances quarantine is effective at reducing or stopping the spread of a contagious disease in the community. These three studies examined whether quarantine reduced disease transmission in response to three different contagious diseases: H1N1 pandemic influenza, severe acute respiratory syndrome (SARS), and measles. Another six quantitative comparative studies and four quantitative noncomparative studies examined other potential benefits and harms of quarantine, as well as strategies that may be effective at improving adherence to quarantine.
A meta-analysis of the evidence for the effectiveness of quarantine was not feasible, so the committee conducted a synthesis without meta-analysis (as described in Chapter 3). Consistent with the methods described in Chapter 3, in making its final judgment on the evidence of effectiveness for quarantine, the committee considered other types of evidence that could inform a determination of what works for whom and in which contexts, ultimately reaching consensus on the certainty of the evidence (COE) for each outcome. Including forms of evidence beyond quantitative comparative studies is particularly important when assessing evidence in settings where controlled studies and/or other forms of quantitative comparative data are difficult to obtain, as is the case with studying quarantine. As discussed in Chapter 3, descriptive evidence from real-world implementation of practices offers the potential to corroborate research findings or explain differences in outcomes in practice settings, even
if it has lesser value for causal inference. Moreover, qualitative studies can complement quantitative studies by providing additional useful evidence to guide real-world decision making, because well-conducted qualitative studies produce deep and rich understandings of how interventions are implemented, delivered, and experienced. Other forms of evidence considered for effectiveness included mechanistic evidence, evidence from modeling studies, and quantitative data reported in case reports of real disasters or public health emergencies.
Benefit: Reduced Overall Disease Transmission in the Community
Evidence from quantitative research studies
Three quantitative comparative studies examined whether the use of quarantine can reduce disease transmission in the community. First, a “quasi-cluster randomized” controlled trial conducted by Miyaki and colleagues (2011) evaluated quarantine as an intervention in Japanese workplaces during the H1N1 influenza pandemic in 2009–2010. Employees of one of two randomly selected automobile factories were assigned to follow a home quarantine protocol, while employees at the other automobile factory were assigned to follow their company’s standard operating procedures. At the factory implementing quarantine (N = 6,634), employees who developed influenza-like illness were ordered to stay home with pay (i.e., they were placed in non-state-enforced home quarantine), and employees whose cohabiting family members developed influenza-like illness were asked to stay home under quarantine. The factory’s health management department managed implementation of the quarantine protocol. In the control factory (N = 8,500), employees reported to work or stayed home when ill per their normal practice. The researchers found a statistically significant 20 percent lower odds of employees testing positive for H1N1 influenza in the factory implementing quarantine compared with the control factory (hazard ratio 0.799; 95% confidence interval [CI] 0.658–0.970; p = 0.023). No one died of H1N1 influenza. The study was limited because outcome measurement was inadequate (use of a rapid test and clinical diagnosis may have greatly underestimated influenza infections), the study did not adjust for baseline differences between groups, and the study was underpowered for death. The study was deemed to be of moderate methodological quality for the analysis of overall H1N1 infection rates.
Second, Bondy and colleagues (2009) conducted a retrospective nonrandomized comparative study on quarantine using data from the 2003 SARS outbreak in Toronto, Canada. The authors made quantitative estimates of the reduction in secondary cases attributable to quarantine, based on information from 8,498 people who were quarantined. They estimated that the “secondary case count difference” (the average transmissions per case, similar to a risk difference) was −0.133 (95% CI −0.213, −0.053) transmitted cases for quarantined versus nonquarantined cases, which translated to a “number needed to quarantine” of 7.51 (95% CI 4.68, 18.9). That is, for every 7.51 people quarantined after exposure to SARS, one additional case of SARS was prevented. The adjusted secondary case count ratio (similar to the incident rate ratio) was 0.352 (95% CI 0.127, 0.981). The authors note that their study was underpowered, and to estimate statistical significance, they used multiple analyses that did not all agree. The article addresses measurement errors, but it is unclear whether this was a major concern with respect to the conclusions drawn. Overall, the study (and each outcome) was deemed to be of moderate methodological quality.
Finally, a retrospective nonrandomized comparative study conducted by Delaporte and colleagues (2013) evaluated 73 people exposed to measles who were quarantined and 173 people who were exposed to measles but not quarantined during a measles epidemic in Geneva, Switzerland, in 2011. The quarantined group represented all of those who met quarantine criteria and were quarantined; the nonquarantined group represented an undescribed
sample of those who met quarantine criteria but were not quarantined. Those who were quarantined were half as likely to transmit measles within their household compared with those who were not quarantined and did not transmit any cases outside the household. Overall, quarantine reduced the risk of measles transmission by nearly 75 percent (p = 0.002). In this study, every case of transmission outside the household was connected to a nonquarantined person. The authors of this study defined their analyzed samples poorly, and the characteristics of the two samples were not compared or adjusted for. Overall, the study (and each outcome) was deemed to be of poor methodological quality.
Other evidence that may inform effectiveness
The committee considered mechanistic evidence, modeling evidence, and quantitative data from case reports for the primary outcome of interest—reducing or stopping disease transmission. Relevant mechanistic evidence was identified from published historical reviews, and as noted earlier, there is little dispute that properly applied quarantine can reduce disease transmission rates (Drews, 2013; Tognotti, 2013). Indeed, the practice of quarantine was an effective response to disease outbreaks before the underlying causes of contagious diseases were understood. For centuries, quarantine has been the cornerstone of a coordinated outbreak-control strategy, which also has included isolation, sanitary cordons, bills of health issued to ships, fumigation, disinfection, and regulation of persons believed to be responsible for spreading illness. The advent of the germ theory of disease in the 1800s brought a new and powerful scientific underpinning to support modern quarantine. The idea that microscopic “germs” could lead to disease and that these germs could be passed from one person to another led to notions of exposure, infection, latent infection, incubation periods, and more (Drews, 2013). Thus, the mechanistic evidence behind quarantine as a means of reducing disease transmission, given the right circumstances, is very solid: quarantine aims to interrupt the chain of contagious disease transmission by separating individuals at risk of becoming contagious from susceptible populations.
The committee identified relevant modeling evidence from a detailed synthesis of 12 selected modeling studies. Across these 12 modeling studies, quarantine was found to be more effective for pathogens with certain specific characteristics (see the section on findings from modeling studies later in this appendix, and specifically Table B4-9). In addition, quarantine was more likely to be effective in several specific types of populations and settings. In summary, quarantine was found to drive the effective reproductive number (Re)2 <1 for Ebola; hepatitis A; Middle East respiratory syndrome (MERS); and possibly pandemic influenza, SARS, smallpox, and measles. It was not found to drive Re <1 for pertussis. Given that a number of assumptions in these studies tend to lead to overestimation of the potential effectiveness of quarantine, it is likely prudent to assume that quarantine’s effectiveness is somewhat lower than what is estimated and predicted by the modeling studies.
Across the remaining 35 modeling studies (those that were not examined in detail), 24 models considered the effectiveness of quarantine per se, and all 24 models found it to be effective in at least some circumstances. However, in nine of these studies, quarantine was inextricably linked with co-strategies such as safe burial practices (as are typical of real-world practice).
Finally, the committee identified relevant evidence on this question from case reports that also include some epidemiological quantitative data. Specifically, the committee exam-
___________________
2 Effective reproductive number (Re): Note that the pathogen’s basic reproductive number (R0) changes over time as the result of interventions and as the infection establishes immunity. The Re (in this case in the presence of quarantine) is conceptually related to the ability of an infection to have persistent or growing prevalence in a population (when the Re is above 1, the disease will have growing prevalence; below 1, prevalence will decline).
ined case reports that report on the number of individuals who eventually developed confirmed or probable illness during the time they were under quarantine. The rationale for examining such data is that a quarantine protocol that ended up placing only healthy people into quarantine was, by definition, ineffective at reducing the spread of a disease since those healthy people never posed a risk to the larger population. By contrast, a quarantine protocol that placed people in quarantine who eventually did end up being infected has a definable probability of having prevented one or more subsequent infections (as suggested by the three quantitative studies summarized above). The committee found 12 case reports that provide information on whether any individuals in quarantine developed illness. In five of these studies, none of those quarantined had confirmed or probable illness (CDC, 2004; Collier et al., 2013; Ehlkes et al., 2017; Grigg et al., 2015; Plipat et al., 2017); in the other seven, at least one quarantined person developed confirmed or probable illness during the quarantine period (CDC, 2003a,b; Chen et al., 2005; Pang et al., 2003; Reaves et al., 2014; Svoboda et al., 2004; Ward et al., 2010).
Summary of the evidence
The committee concluded that there is high COE that quarantine can be effective at reducing overall disease transmission in the community in certain circumstances. Three quantitative comparative studies (Bondy et al., 2009; Delaporte et al., 2013; Miyaki et al., 2011) provide low COE regarding the effect of quarantine on reduced overall disease transmission (see Table B4-2). As for other forms of evidence,3 taken together, the weight of the evidence is sufficient to upgrade the COE to high. Mechanistic data support the practice, as do modeling data, although effectiveness varies with characteristics of the pathogen. In addition, seven case reports may be seen as supportive, as there were illnesses in the quarantine groups that could have been transmitted; an additional five case reports with no illnesses in the quarantine groups have an equivocal impact on the COE. There are no discordant studies.
___________________
3 As described in Chapter 3, the committee reviewed other evidence that informed the COE (e.g., mechanistic evidence, experiential evidence from case reports and after action reports, qualitative evidence) for coherence with the findings from the quantitative research studies and classified that evidence as very supportive, supportive, inconclusive (no conclusion can be drawn on coherence, either because results are mixed or the data are insufficient), or unsupportive (discordant with the findings from the quantitative research studies). The distinction between supportive and very supportive is based on the magnitude of the reported effect and the directness of the evidence to the question of interest.
| Quality Assessment | Number of Studies | 3 |
| Study Infomation | Miyaki et al., 2011 Quasi-cluster randomized controlled trial, moderate methodological quality (▲) Bondy et al., 2009 Retrospective nonrandomized comparative study (NRCS), moderate methodological quality (▲) Delaporte et al., 2013 Retrospective NRCS, poor methodological quality (▲) |
|
| Risk of Bias | Serious | |
| Inconsistency | Not serious | |
| Indirectness | Serious (Miyaki et al., 2011, study was conducted in an occupational health setting) | |
| Imprecision | Not serious | |
| Publication Bias | Unlikely | |
| Upgrade for Large Effect, Dose Response, Plausible Confounding | No | |
| Summary of Findings | Initial Certainty of the Evidence (COE) | Low |
| Other Evidence | Supportive mechanistic evidence, supportive modeling evidence, supportive case report evidence, and no discordant studies | |
| COE | High (reduces overall disease transmission) | |
NOTE: Effect direction: upward arrow (▲) = improvement/beneficial effect; downward arrow (▼) = harm/negative effect; sideways arrows (◄►) = no effect; up and down arrows (▲▼) = mixed effect/conflicting findings.
Benefit: Reduced Time from Symptom Onset to Diagnosis
Evidence from quantitative research studies
A single retrospective nonrandomized comparative study conducted by Hsieh and colleagues (2005) during the SARS outbreak in Taiwan in 2003 compared quarantined (N = 24) and nonquarantined people (N = 452) with respect to the time from onset of symptoms to diagnosis for those who became ill. Those who were not quarantined had a longer time (2.89 days) from onset of symptoms to clinical diagnosis (and hospital admission) relative to quarantined people (1.20 days) (p = 0.0061), but there was no difference in time from clinical diagnosis to final classification (i.e., confirmation of diagnosis of SARS) (7.54 days for nonquarantined people and 7.76 days for quarantined people; p = 0.7864). The authors did not adjust for differences between groups, and there was high loss to follow-up for time to classification. Overall, the study (and each outcome) was deemed to be of poor methodological quality.
Other evidence that may inform effectiveness
The committee considered mechanistic evidence, modeling evidence, and quantitative data from case reports for the outcome of reduced time from symptom onset to diagnosis. Mechanistically, people in quarantine—-
especially hospital quarantine—might also receive very close follow-up care, which could lead to a shorter time from symptom onset to diagnosis. Some modeling studies also assume that quarantine can help accelerate isolation in some circumstances, and may be a more effective option when the process of closely monitoring and then isolating individuals once they become symptomatic is slow or unreliable. One case report also addresses the importance of the difference in time from onset of illness to diagnosis with respect to the diffusion velocity of an epidemic in the early stages of pandemic influenza (Zhang et al., 2012). This case report shows that quarantine of close contacts allowed these high-risk subjects to be monitored closely over a longer period of time, which had important implications in reducing the risk of disease transmission by enabling timely detection of disease in those who had onset of illness.
Summary of the evidence
The committee concluded that there is low COE that quarantine can reduce the time from symptom onset to diagnosis in quarantined individuals. One quantitative comparative study (Hsieh et al., 2005) provides very low COE regarding the effect of quarantine on this outcome (see Table B4-3). The weight of other forms of evidence, taken together, is sufficient to upgrade the COE to low. There are no discordant studies.
| Quality Assessment | Number of Studies | 1 |
| Study Infomation | Hsieh et al., 2005 Retrospective nonrandomized comparative study (NRCS), poor methodological quality (▲) |
|
| Risk of Bias | Very serious | |
| Inconsistency | Not applicable | |
| Indirectness | Not serious | |
| Imprecision | Serious | |
| Publication Bias | Unlikely | |
| Upgrade for Large Effect, Dose Response, Plausible Confounding | No | |
| Summary of Findings | Initial Certainty of the Evidence (COE) | Very low |
| Other Evidence | Supportive mechanistic evidence, supportive modeling evidence supportive evidence from one case report, and no discordant studies | |
| COE | Low (reduces time from symptom onset to diagnosis) | |
NOTE: Effect direction: upward arrow (▲) = improvement/beneficial effect; downward arrow (▼) = harm/negative effect; sideways arrows (◄►) = no effect; up and down arrows (▲▼) = mixed effect/conflicting findings.
Harm: Increased Risk of Infection in Congregate Quarantine Settings
Evidence from quantitative research studies
Two quantitative comparative studies examined risk of infection in congregate quarantine settings,4 both finding an increased risk. The “quasi-cluster randomized” controlled trial conducted by Miyaki and colleagues (2011) was discussed previously. In addition to the findings from this study noted earlier, the researchers found that factory employees with ill family members who were told to quarantine at home (with their ill family members) were twice as likely to develop H1N1 influenza compared with workers with ill family members from the control factory, who were not required to stay home (relative risk 2.17; p <0.001). The second study, a retrospective nonrandomized comparative study conducted by Chu and colleagues (2010) during the pandemic H1N1 influenza season in China in 2009, assigned asymptomatic students who had been exposed to influenza during a train ride (N = 152) to different quarantine dormitory rooming situations for 12 days upon their return to a university. Quarantined students either shared both a room and a toilet with other quarantined students or shared a toilet but had a single room. Students were also categorized based on whether they had (by the end of quarantine) shared either a toilet or a room with another student who became ill. Students were not assigned randomly, but rooming situations were dictated by available rooms without regard for rooming preferences. Among those who shared rooms or toilets, those who shared with virus-positive contacts were more than three times more likely to develop a fever or influenza-like illness (p = 0.02, although H1N1 positivity was not generally tested). The rooming situation of those not exposed to virus-positive students during quarantine was not associated with the likelihood of developing a fever or illness. This study had serious methodological limitations related to the way in which students were assigned to rooming situations, inadequate outcome assessment, and lack of adjustment, among other concerns, nor did it directly analyze the effect of the different rooming situations (for all quarantined students). Overall, the study (and each outcome) was deemed to be of poor methodological quality.
Other evidence that may inform effectiveness
The committee considered mechanistic evidence for the outcome of increased risk of infection in congregate quarantine settings. The mechanism by which quarantine results in an increased risk of infection in congregate settings is underpinned by the germ theory of disease. Quarantine may increase the contact between symptomatically ill individuals and people who are not ill or infected (i.e., only suspected of being exposed) with whom they come in contact within the quarantine area (mechanistic evidence for quarantine was discussed in prior sections).
Summary of the evidence
The committee concluded that there is high COE that congregate quarantine for influenza and agents with similar transmissibility can increase the risk of infection among those in the shared setting. Two quantitative comparative studies (Chu et al., 2010; Miyaki et al., 2011) provide moderate COE regarding the effect of congregate quarantine on increased risk of infection among those quarantined together (see Table B4-4). In considering other evidence, the weight of the mechanistic evidence is sufficient to upgrade the COE to high.
___________________
4 A congregate quarantine setting is the sharing of the same room or facilities with an infected case. This is applicable mainly to individuals quarantined at home who fall ill and thereby increase the likelihood that another household member will acquire the illness.
| Quality Assessment | Number of Studies | 2 |
| Study Infomation | Miyaki et al., 2011 Quasi-cluster randomized controlled trial, moderate methodological quality (▼) Chu et al., 2010 Retrospective nonrandomized comparative study (NRCS), poor methodological quality (▼) |
|
| Risk of Bias | Serious | |
| Inconsistency | Not serious | |
| Indirectness | Not serious | |
| Imprecision | Not serious | |
| Publication Bias | Unlikely | |
| Upgrade for Large Effect, Dose Response, Plausible Confounding | No | |
| Summary of Findings | Initial Certainty of the Evidence (COE) | Moderate |
| Other Evidence | Very supportive mechanistic evidence (no counterfactual) | |
| COE | High (increases risk of infection among those in the shared setting) | |
NOTE: Effect direction: upward arrow (▲) = improvement/beneficial effect; downward arrow (▼) = harm/negative effect; sideways arrows (◄►) = no effect; up and down arrows (▲▼) = mixed effect/conflicting findings.
Harm: Psychological
Evidence from quantitative research studies
Three quantitative comparative studies and three noncomparative quantitative studies examined the potential for psychological harms in quarantined individuals. They are briefly summarized below in the order in which they were published, which also corresponds to specific epidemics (SARS and MERS).
A cross-sectional (postintervention) survey conducted by Hawryluck and colleagues (2004) in 2003 examined the experiences of 129 people quarantined during the 2003 Toronto SARS outbreak, “after participants ended their quarantine period.” The study found no statistically significant difference in adherence to recommended infection control measures during quarantine (e.g., remaining in residences, wearing masks, temperature monitoring) by health care workers compared with non–health care workers. Symptoms of posttraumatic stress disorder (PTSD) (as measured with the Impact of Event Scale-Revised [IES-R], a measure of levels of psychological distress) and depression (as measured with the Center for Epidemiologic Studies-Depression Scale [CES-D]) were similar among those who underwent home- versus work-based quarantine. Those who experienced ≥10 days of quarantine had statistically significantly worse PTSD symptoms (p = 0.005) and had nonsignificantly worse depression symptoms (p = 0.07) compared with those who underwent <10 days of quarantine. Those who wore a mask at all times during quarantine (against recommendations, which allowed for masks to be taken off under some circumstances) had statistically significantly
higher PTSD and depression symptoms relative to those who followed the recommendations and those who never wore a mask (p = 0.003). Worse PTSD and depression symptoms during quarantine were also associated with lower income. According to the study authors, the survey may have preferentially selected those with greater distress. The survey also captured a very small sample of those quarantined (<1 percent). Overall, the study (and each outcome) was deemed to be of poor methodological quality.
Reynolds and colleagues (2008) conducted a similar but much larger cross-sectional (postintervention) survey in 2003, 6 weeks after the Toronto SARS outbreak, among 1,057 quarantined people. Compared with non–health care workers, they found that health care workers had a greater likelihood of severe PTSD symptoms (by IES-R score ≥20; p <0.001) and reported more PTSD symptoms; more avoidance symptoms, intrusion symptoms, and hyperarousal symptoms; and greater loss of income related to being quarantined (p = 0.001). The survey underrepresented younger people, and the authors note a high risk of recall bias. Overall, the study (and each outcome) was deemed to be of poor methodological quality.
In a retrospective, nonrandomized comparative study, Marjanovic and colleagues (2007) evaluated the experiences of 333 nurses quarantined during the 2003 Toronto SARS epidemic. In adjusted analyses, quarantine (or longer quarantine time) was associated with higher scores on a then-unvalidated measure of avoidance behavior (p <0.001) and state anger (by the State-Trait Anger Expression Inventory [STAXI] anger subscale) (p = 0.008), but not greater emotional exhaustion (as measured by the Maslach Burnout Inventory-General Survey emotional exhaustion subscale) (p = 0.113). Overall, the study (and each outcome) was deemed to be of poor methodological quality largely because of a lack of clarity about the comparison that was made.
Wu and colleagues (2008, 2009) and Liu and colleagues (2012) report on a retrospective nonrandomized comparative study of employees at a major Beijing hospital (N = 549) 3 years after that city’s SARS outbreak in 2003. Compared with nonquarantined employees, those who were quarantined were found to have been more likely to have had alcohol-related symptoms (questions adapted from the National Household Survey on Drug Abuse), PTSD symptoms (by IES-R) (p <0.001), and depression symptoms (by CES-D) (p <0.0001) during the 3 years after the SARS epidemic. The study authors do not provide a clear definition of quarantine, and it is possible that some of those considered quarantined were actually in isolation and experienced illness with SARS. For PTSD and depression symptoms, the study was deemed to be of moderate methodological quality, and for alcohol-related symptoms, the study was deemed to be of poor methodological quality because of the use of an unvalidated tool.
A cross-sectional (postintervention) survey conducted by Jeong and colleagues (2016) 4 to 6 months after a MERS outbreak in South Korea in 2015 compared psychological and other outcomes between people quarantined for 2 weeks who ended up having MERS (N = 36) and those quarantined who did not (N = 1,656). The study also compared quarantined individuals based on their degree of exposure to individuals with MERS before being placed in quarantine. Quarantined people who developed MERS reported having more medical expenses (p <0.001) and less sufficient food and water, ability to bathe, or access to self-care products (p <0.001) during quarantine compared with quarantined people who did not develop MERS. Individuals with greater prior exposure to people with MERS reported greater anxiety and anger symptoms 4 to 6 months after quarantine. Of note, the study did not compare people quarantined with similarly exposed people who were not quarantined. The study authors report that the anxiety and anger scales used (Generalized Anxiety Disorder Scale and STAXI, respectively) may not be valid in this population, and notably, many angry people refused to participate in the survey. Overall, the study (and each outcome) was deemed to be of poor methodological quality.
Lee and colleagues (2018) conducted a retrospective nonrandomized comparative study (a longitudinal series of surveys) during and following the MERS outbreak of 2015 in South Korea, comparing quarantined and nonquarantined health care personnel at a MERS-affected hospital. In a first survey during the MERS epidemic quarantine period, quarantined and nonquarantined health care personnel (N = 359 total respondents) had similar scores on the IES-R scale. Six weeks later, the authors conducted a follow-up survey (N = 77 total respondents) of just those personnel who had high distress scores on the first survey (scoring in a range that made them “PTSD eligible”). Overall, at 6 weeks, IES-R scores were similar among quarantined and nonquarantined employees. In the follow-up survey of more distressed health care personnel, however, those who had been quarantined were statistically significantly more likely (p = 0.03) to have “sleep and numbness” symptoms on the IES-R. For both surveys, the respondents were substantially different from the nonrespondents with respect to their health care roles; response rates varied widely by job description. Non-response rates, in particular on the follow-up survey, were high. The authors do not define quarantine. The “sleep and numbness” outcome is inadequately reported and appears to be an ad hoc measure. Outcome results are not fully reported. Overall, the study (and each outcome) was deemed to be of poor methodological quality.
Other evidence that may inform effectiveness
The committee considered findings from a qualitative evidence synthesis and quantitative data from case reports for the outcome of psychological harm. Overall, eight qualitative studies examined the psychological harms of quarantine, including social isolation and social stigma (Cava et al., 2005a; Desclaux et al., 2017; DiGiovanni et al., 2004; Lin et al., 2010; Maunder et al., 2003; Pellecchia et al., 2015; Robertson et al., 2004; Schemm Dwyer et al., 2017).
People on whom quarantine is imposed may experience the harm of social isolation (high confidence in the evidence).5 This harm is documented in four quarantine studies among members of the general public, as well as health care workers placed under quarantine (Cava et al., 2005a; DiGiovanni et al., 2004; Lin et al., 2010; Robertson et al., 2004). Quarantine typically required restriction of physical contact with close others, including spouses, children, and siblings; wearing a mask, which is further distancing; and even home quarantine, all of which resulted in feelings of physical and psychological isolation.
People on whom quarantine is imposed may experience the harm of social stigma (high confidence in the evidence). Unless the quarantine is kept secret, people on whom it is imposed may be publicly labeled as potential carriers of a contagious disease, which may in turn lead others to develop feelings of avoidance, suspicion, mistrust, and fear, and thus stigma, toward the quarantined people. The seven qualitative studies found that when people from already-marginalized communities were quarantined, this stigmatization could exacerbate discrimination and marginalization, a situation that could last well beyond the quarantine period (Cava et al., 2005a; Desclaux et al., 2017; DiGiovanni et al., 2004; Lin et al., 2010; Pellecchia et al., 2015; Robertson et al., 2004; Schemm Dwyer et al., 2017).
People on whom quarantine is imposed may also experience the harm of negative psychological states, including anxiety, fear, worry, stress, and loneliness (high confidence in the evidence). Six qualitative studies found that the sources for these psychological harms
___________________
5 This italicized statement with an associated confidence level is a qualitative evidence finding statement from the commissioned report “Quarantine as a Non-Pharmaceutical Intervention: Qualitative Research Evidence Synthesis” by Pradeep Sopory and Julie Novak (see Appendix C). The Grading of Recommendations Assessment, Development and Evaluation Confidence in the Evidence from Reviews of Qualitative Research (GRADE-CERQual) was used to assess the confidence in synthesized qualitative findings (analytic and some descriptive themes). Additional details on GRADE-CERQual can be found in Chapter 3.
could be the social isolation and stigmatization noted above, as well as the financial stress that can accompany quarantine and worry about the possibility of inflicting harm on others (Cava et al., 2005a; DiGiovanni et al., 2004; Lin et al., 2010; Maunder et al., 2003; Pellecchia et al., 2015; Robertson et al., 2004).
Health care workers on whom quarantine is imposed may experience additional harms (high confidence in the evidence). Three qualitative studies found amplified harms for health care workers (Desclaux et al., 2017; Maunder et al., 2003; Robertson et al., 2004). For example, they experienced stronger negative psychological states such as anxiety, and additional stress from fear, guilt, or shame that they could have infected patients before being quarantined. Health care workers under quarantine also worried about leaving their colleagues understaffed and overworked. In cases of “work quarantine,” where essential health care workers must continue to come to work, having contact with patients known to be infected could lead to even greater anxiety. This situation could also lead to resentment and conflict with nonessential coworkers placed in home instead of work quarantine. One case report includes data on the frequency of mental disorders among 6,231 people placed in quarantine for exposure to MERS in South Korea; 1,221 (19.3 percent) showed emotional disturbances such as depression (Yoon et al., 2016).
Summary of the evidence
The committee concluded that there is moderate COE that quarantine can result in psychological harm among quarantined individuals, including PTSD, anxiety, and anger, the risk of which increases with the duration of quarantine. Three quantitative comparative studies (Lee et al., 2018; Liu et al., 2012; Marjanovic et al., 2007; Wu et al., 2008, 2009) and three quantitative noncomparative studies (Hawryluck et al., 2004; Jeong et al., 2016; Reynolds et al., 2008) provide low COE regarding the effect of quarantine on psychological harms among quarantined individuals (see Table B4-5). The weight of other forms of evidence, taken together, is sufficient to upgrade the COE to moderate. There is very supportive evidence with high certainty from a synthesis of eight qualitative studies and a supportive case report. There are no discordant studies.
TABLE B4-5 Effect of Quarantine on Psychological Harms in Quarantined Individuals
| Quality Assessment | Number of Studies | 6 |
| Study Infomation | Lee et al., 2018 Retrospective nonrandomized comparative study (NRCS), poor methodological quality (▼) Liu et al., 2012; Wu et al., 2008, 2009 Retrospective NRCS, moderate methodological quality (▼) Marjanovic et al., 2007 Retrospective NRCS, poor methodological quality (▼) Hawryluck et al., 2004 Cross-sectional (postintervention), poor methodological quality (▼) Jeong et al., 2016 Cross-sectional (postintervention), poor methodological quality (▼) Reynolds et al., 2008 Cross-sectional (postintervention), poor methodological quality (▼) |
|
| Risk of Bias | Serious | |
| Inconsistency | Not serious | |
| Indirectness | Not serious | |
| Imprecision | Not serious | |
| Publication Bias | Unlikely | |
| Upgrade for Large Effect, Dose Response, Plausible Confounding | Large effect | |
| Summary of Findings | Initial Certainty of the Evidence (COE) | Low |
| Other Evidence | Very supportive qualitative evidence, supportive evidence from one case report, and no discordant studies | |
| COE | Moderate (increases psychological harm) | |
NOTE: Effect direction: upward arrow (▲) = improvement/beneficial effect; downward arrow (▼) = harm/negative effect; sideways arrows (◄►) = no effect; up and down arrows (▲▼) = mixed effect/conflicting findings.
Harm: Individual Financial Hardship
Evidence from quantitative research studies
Two quantitative noncomparative studies—by Reynolds and colleagues (2008), discussed above, and Kavanagh and colleagues (2012), discussed in a following section—examined whether being placed in quarantine led to financial losses for quarantined individuals. Both found that it did. Kavanagh and colleagues (2012) found that 38 percent of surveyed households lost pay to care for a child in home quarantine, which in 42 percent of cases led to financial difficulties (e.g., unable to pay a bill). Lost pay occurred more frequently in households without access to leave (p <0.001). Reynolds and colleagues (2008) found that health care workers were more likely than non–health care workers to experience a decline in household income during the 2003 SARS outbreak in Toronto (p <0.05).
Other evidence that may inform effectiveness
The committee considered mechanistic evidence and findings from a qualitative evidence synthesis for the outcome of individual financial hardship. Mechanistic evidence applies to understanding the process by which quarantine can be associated with financial loss: people who are quarantined are unable to work, which may result in a loss of income.
People on whom quarantine is imposed may experience the harm of financial instability (high confidence in the evidence). Five qualitative studies examined financial losses among quarantined individuals (Baum et al., 2009; Braunack-Mayer et al., 2010; Cava et al., 2005a; Desclaux et al., 2017; DiGiovanni et al., 2004). People were often placed in quarantine with little advance notice, which affected their employment status and resulted in the loss of regular wages and other income without compensation. This situation could be exacerbated for people whose income comes from part-time work, casual work, or self-employment.
Summary of the evidence
The committee concluded that there is high COE that quarantine can be associated with individual financial hardship for people who are quarantined. Two nonquantitative comparative studies (Kavanagh et al., 2012; Reynolds et al., 2008) provide low COE regarding the effect of quarantine on financial hardship among quarantined individuals (see Table B4-6). The weight of other forms of evidence, taken together, is sufficient to upgrade the COE to high. There is very supportive mechanistic evidence, as well as very supportive evidence with high certainty from a synthesis of five qualitative studies. There are no discordant studies.
TABLE B4-6 Effect of Quarantine on Financial Hardship in Quarantined Individuals
| Quality Assessment | Number of Studies | 2 |
| Study Infomation | Kavanagh et al., 2012 Cross-sectional (postintervention), moderate methodological quality (▼) Reynolds et al., 2008 Cross-sectional (postintervention), poor methodological quality (▼) |
|
| Risk of Bias | Serious | |
| Inconsistency | Not serious | |
| Indirectness | Not serious | |
| Imprecision | Not serious | |
| Publication Bias | Unlikely | |
| Upgrade for Large Effect, Dose Response, Plausible Confounding | Large effect | |
| Summary of Findings | Initial Certainty of the Evidence (COE) | Low |
| Other Evidence | Very supportive mechanistic evidence, very supportive qualitative evidence, and no discordant studies | |
| COE | High (increases financial hardship) | |
NOTE: Effect direction: upward arrow (▲) = improvement/beneficial effect; downward arrow (▼) = harm/negative effect; sideways arrows (◄►) = no effect; up and down arrows (▲▼) = mixed effect/conflicting findings.
Strategies for Reducing Harms
Evidence from quantitative research studies
A single quantitative noncomparative study examined depression in quarantined individuals and the provision of family support and the promotion and emphasis of health by those leading the outbreak response (i.e., “health-promoting leadership”). Adler and colleagues (2018) published a cross-sectional (postintervention) survey of 501 soldiers on a U.S. military base who had returned from West Africa with possible exposure to Ebola in 2014. The study evaluated the association of family support and health-promoting leadership behaviors by local senior leaders with the soldiers’ mental health and attitudes toward the quarantine. Using a regression model, the authors found that health-promoting leadership behaviors were independently associated with fewer depression (p = 0.04) and anxiety (p = 0.008) symptoms, less functional impairment (p = 0.03), and more positive attitudes toward quarantine (p <0.001) and preventive medicine (p <0.001). No statistically significant associations were found with PTSD symptoms or insomnia. Perception of family support was not associated with PTSD, depression, or anxiety symptoms but was associated with fewer insomnia symptoms (p <0.001), less functional impairment (p = 0.04), and more positive attitudes toward the quarantine (p <0.001) and the preventive medicine practices enacted during the quarantine (p <0.001). The survey methods and outcomes are not described and were not validated. The predictor “health-promoting leadership behaviors” was based on soldiers’ answers to the survey about their leaders; however, it is unclear how this variable (or variables) was entered into the model. Overall, the study (and each outcome) was deemed to be of poor methodological quality.
Summary of the evidence
The committee concluded that there is very low COE that an emphasis on health by those leading the outbreak response (i.e., health-promoting leadership) can reduce depression and anxiety symptoms in quarantined individuals. One nonquantitative comparative study (Adler et al., 2018) provides very low COE regarding the effect of health-promoting leadership on depression in quarantined individuals (see Table B4-7).
| Quality Assessment | Number of Studies | 1 |
| Study Infomation | Adler et al., 2018 Cross-sectional (postintervention), poor methodological quality (▲) |
|
| Risk of Bias | Very serious | |
| Inconsistency | Not applicable | |
| Indirectness | Not serious | |
| Imprecision | Serious | |
| Publication Bias | Unlikely | |
| Upgrade for Large Effect, Dose Response, Plausible Confounding | No | |
| Summary of Findings | Initial Certainty of the Evidence (COE) | Very low |
| Other Evidence | Not applicable | |
| COE | Very low (reduces depression and anxiety symptoms) | |
NOTE: Effect direction: upward arrow (▲) = improvement/beneficial effect; downward arrow (▼) = harm/negative effect; sideways arrows (◄►) = no effect; up and down arrows (▲▼) = mixed effect/conflicting findings.
Strategies for Improving Adherence to Quarantine Measures
Evidence from quantitative research studies
A single quantitative noncomparative study examined the implementation of risk communication and messaging and social and resource support strategies as ways of improving adherence to quarantine. Kavanagh and colleagues (2011, 2012) and McVernon and colleagues (2011) conducted this cross-sectional (postintervention) survey about 6 months after a pandemic of H1N1 influenza in Australia in 2009 among 297 households affected by the quarantine of children thought to have been exposed at school. Households that reported understanding what they were meant to do during quarantine were more than twice as likely to comply fully with quarantine recommendations compared with those that did not (odds ratio [OR] 2.27; 95% CI 1.35–3.80) (Kavanagh et al., 2011). Among families in which all resident parents were employed, those with available sick leave were twice as likely to stay home throughout quarantine (OR 2.07; 95% CI 0.82–5.23) (Kavanagh et al., 2012). Those who took time off were more than twice as likely to stay home throughout quarantine (OR 2.47; 95% CI 1.17–5.22; p = 0.02), although whether parents took time off from work was not associated with full compliance (OR 1.27; 95% CI 0.61–2.67). Households without access to paid leave were about three times more likely to have lost pay to care for their quarantined child (p <0.001). Households in which the child was not ill were much more likely to have another child visit the household compared with those with ill children (p <0.001) (McVernon et al., 2011). Similarly, households in which no family members were ill were more likely to have another adult visit during quarantine (p = 0.04). The authors note a high risk of recall bias, and the response rate may have been low. Overall, the study (and each outcome) was deemed to be of moderate methodological quality.
Other evidence that may inform effectiveness
The committee considered findings from a qualitative evidence synthesis for the outcome of improved adherence. Eight qualitative studies examined the importance of risk communication for adherence to quarantine measures (Cava et al., 2005b; DiGiovanni et al., 2004; Lin et al., 2010; Pellecchia et al., 2015; Robertson et al., 2004; Schemm Dwyer et al., 2017; Sell et al., 2018; Smith et al., 2012). This evidence suggests that agencies can use communication strategically to increase adherence to quarantine during a contagious disease event. This communication is equally important for both the public and the health care staff on whom quarantine has been imposed (high confidence in the evidence). The findings of these qualitative studies indicate that communication should emphasize persuasion over threat and aim to be bidirectional. They suggest further that communication should take place over the full course of the event and should involve multiple channels, including mass media and interpersonal channels, and multiple sources, including public health and health care staff. The communication should, in particular, provide information about the disease, as well as the need for and instructions for the quarantine; not arouse fear and anxiety; not be stigmatizing; not use terms with confusing meanings; and include clear and consistent information about infection control and coping strategies.
Summary of the evidence
The committee concluded that there is moderate COE that while adherence to quarantine measures can vary by culture, disease, and socioeconomic status, use of various strategies, including risk communication and messaging and access to employment leave, can improve adherence. One quantitative noncomparative study (Kavanagh et al., 2011, 2012; McVernon et al., 2011) provides low COE regarding the effect of risk communication and messaging and access to employment leave on improved adherence to quarantine measures (see Table B4-8). The weight of other forms of evidence, taken together, is sufficient to upgrade the COE to moderate. There is very supportive evidence with high certainty from a synthesis of eight qualitative studies. There are no discordant studies.
| Quality Assessment | Number of Studies | 1 |
| Study Infomation | Kavanagh et al., 2011, 2012; McVernon et al., 2011 Cross-sectional, moderate methodological quality (▲) |
|
| Risk of Bias | Serious | |
| Inconsistency | Not applicable | |
| Indirectness | Not serious | |
| Imprecision | Serious | |
| Publication Bias | Unlikely | |
| Upgrade for Large Effect, Dose Response, Plausible Confounding | Large effect | |
| Summary of Findings | Initial Certainty of the Evidence (COE) | Low |
| Other Evidence | Very supportive qualitative evidence and no discordant studies | |
| COE | Moderate (improves adherence) | |
NOTE: Effect direction: upward arrow (▲) = improvement/beneficial effect; downward arrow (▼) = harm/negative effect; sideways arrows (◄►) = no effect; up and down arrows (▲▼) = mixed effect/conflicting findings.
2. Findings from a Synthesis of Modeling Studies: Quarantine Is More Effective Under Certain Circumstances
As previously discussed, across the 12 modeling studies considered, quarantine was found to be more or less likely to be effective depending on systematic and consistent factors related both to characteristics of the pathogen and to the population and setting (see Table B4-9).6 Understanding of these systematic relationships is aided specifically by one of the modeling studies included in this review (Peak et al., 2017), whose authors provide analyses for a range of diseases and attempt to provide answers to this question within a common modeling framework.7
Consistent with the findings of Peak and colleagues (2017), as well as the other modeling studies and the drivers of effectiveness their authors identify or imply, quarantine was more likely to be effective at reducing or stopping the spread of a contagious disease in the following circumstances:
___________________________
6 An expert in modeling methodology assessed the selected group of quarantine modeling studies in detail, including the specific model structures and equations and how the interventions were instantiated within these structures and equations. This assessment was intended to determine whether assumptions encoded in such structures and equations could plausibly have had a strong impact on the results found in the studies. Likewise, a careful reading of the methods section of each paper was focused on extracting explicitly documented assumptions, as well as other, implicit assumptions based on methodological decisions (e.g., no change in mixing rates as the epidemic grows because of such processes as social distancing, perfect versus imperfect identification/case finding to be eligible for quarantine, asymptomatic transmission).
7 Peak et al. (2017) was selected as the scaffold for the synthesis of modeling studies because that study considered factors for a range of diseases, whereas the other included modeling studies that looked only at one disease.
- Moderate basic reproductive number (R0)—when the R0 of a given pathogen is in a range in which quarantine can be expected to reduce transmission importantly. Quarantine may be more effective for a pathogen with a moderate R0 or for a pathogen with a higher R0 that has previously produced durable immunity in a population (i.e., the population in question has been exposed previously) such that the effective reproductive number (Re) in the population even without intervention is relatively lower. If a pathogen has a high R0, more transmission may occur before quarantine can be implemented, reducing quarantine’s effectiveness at limiting the final extent
- of the outbreak. As a practical matter, for pathogens with a very low R0 (i.e., <1) disease transmission will not be sustained, making quarantine theoretically effective but perhaps practically unnecessary (see also footnote 2 earlier in this appendix).
- Shorter incubation period—when quarantine can reliably separate identified individuals from the general population for durations commensurate with the expected duration of asymptomatic infectiousness. Quarantine may become infeasible or less effective as the result of reduced adherence if its duration must be very long because of a prolonged incubation period (the period between exposure and when infection becomes detectable).
- Relatively short asymptomatic infectious period—when the asymptomatic infectious period is short or there is no asymptomatic infectious period. When there is a long period of asymptomatic infectiousness, quarantine of recently infected people must be extremely rapid and comprehensive to prevent transmission by asymptomatic individuals, which may be so logistically challenging as to be practically infeasible. In addition, if the asymptomatic infectious period is long in absolute terms, quarantine may become infeasible or less effective because of reduced adherence (see the previous bullet).
- Rapid identification—when exposed individuals can be identified reliably and quickly.
- Use of quarantine to aid isolation—when isolation of individuals once they become symptomatic is slow or unreliable without quarantine. In these circumstances, quarantine may reduce transmission through its effects on facilitating more rapid isolation of ill and contagious individuals.
TABLE B4-9 Summary of Findings on the Effectiveness of Quarantine from 12 Modeling Studies
| Disease | Quarantine Likely Effective? | Notes |
|---|---|---|
| Ebola | Yes | Two studies found that quarantine can drive Re <1a (D’Silva and Eisenberg, 2017; Peak et al., 2017). |
| Hepatitis A | Yes based on 1 study | One study found that quarantine can drive Re <1 (Peak et al., 2017). |
| Influenza A/H1N1 | Maybe | Two studies. One study found that quarantine can drive Re <1 (Peak et al., 2017). Another study focused on delaying the epidemic peak and indicated that quarantine can possibly be effective depending on the specific features of the pathogen in the population and the level of intervention (An der Heiden et al., 2009). |
| Middle East respiratory syndrome (MERS) | Yes | Two studies found that quarantine can drive Re <1 (Ahn et al., 2018; Peak et al., 2017). |
| Pertussis | No based on 1 study | One study found that quarantine is unlikely to drive Re <1 (Peak et al., 2017). |
| Severe acute respiratory syndrome (SARS) | Maybe | Seven studies. Three studies identified situations in which quarantine may not be effective in driving Re <1, with effectiveness depending on the pathogen’s basic reproductive number in a given population (less likely with higher R0b), the likely effectiveness of isolation of symptomatic individuals as an alternative strategy, the likelihood of there being individuals who are asymptomatic but contagious and the fraction of those individuals, and the ability to quickly identify a large fraction of exposed individuals for quarantine (Day et al., 2006; Hsieh et al., 2007; Peak et al., 2017). Four studies found (or in essence their authors assumed [based on models of past limited outbreaks]) that sufficiently effective, properly scaled and targeted, or potentially dynamic quarantine policies can drive Re <1 (Feng et al., 2009; Gupta et al., 2005; Mubayi et al., 2010; Podder et al., 2007). |
| Smallpox | Maybe | Two studies. One study found that quarantine is unlikely to drive Re <1. Another study found that early initiation of quarantine for a large fraction of exposed cases can likely avoid an epidemic resulting from a smallpox bioterrorism attack (Meltzer et al., 2001; Peak et al., 2017). |
| Measles | Yes/maybe based on 1 study | One study found that despite measles having a high R0, if there is a sufficient level of background immunity, it may be possible to use quarantine to end an outbreak quickly. However, with lower levels of background immunity, quarantine is unlikely to drive Re <1 or to do so quickly (Enanoria et al., 2016). |
a Re = effective reproductive number (in this case in the presence of quarantine), which conceptually is related to the ability of an infection to have persistent or growing prevalence in a population (when Re is above 1, the disease will have growing prevalence; when it is below 1, prevalence will decline).
b R0 = basic reproductive number.
3. Balance of Benefits and Harms
Synthesis of Evidence of Effect
The synthesis of evidence of effect (described above) shows that quarantine can be effective at reducing overall disease transmission in the community in certain circumstances (high COE) and reducing time from symptom onset to diagnosis in quarantined individuals (low COE). The modeling studies reviewed also support these benefits. However, quarantine can result in harms for those quarantined, including increased risk of infection among those quarantined together in congregate quarantine settings (high COE), psychological harm (moderate COE), and individual financial hardship (high COE).
Qualitative Evidence Synthesis
Indirectly, the qualitative studies included in this review found that quarantine is an important response to contagious disease outbreaks that is likely to be effective in lowering morbidity and mortality in the larger population. The 16 qualitative studies in this corpus, however, were focused much more on the process of quarantine than on disease-related outcomes, in particular on understanding the experience of the people on whom quarantine is imposed. The study findings indicate that quarantine has the potential to result in the removal of civil rights protections and, as discussed in the above section on determining evidence of effect, the occurrence of such undesirable impacts as financial instability, social stigma, and compromised psychological well-being. Given these undesirable impacts of quarantine, which can be both short and long term, the balance of benefits and harms is open to debate.
Case Report Evidence Synthesis
As with the qualitative studies, most of the case reports reviewed do not directly address the benefits of quarantine. Those that do so mention potential benefits of reduced risk of transmission and increased public confidence based on experience with SARS in China, Singapore, and Taiwan (CDC, 2003a,b; Ooi et al., 2005). Although acknowledging challenges with careful application of quarantine measures, the Centers for Disease Control and Prevention’s (CDC’s) Morbidity and Mortality Weekly Report indicates that quarantine effectively eliminated the risk for transmission of SARS from quarantined people to community members (CDC, 2003a). Ooi and colleagues (2005) describe how quarantine gave the public in Singapore confidence to continue with their daily activities, given their knowledge of public health safeguards against SARS (Ooi et al., 2005). They conjecture that the public would otherwise have taken actions to avoid public places, resulting in a situation in which the unaffected majority instead of the affected minority would stay at home. Most of the case reports reviewed note the unintended consequences or harms related to quarantine, including the potential for increased transmission and mortality due to its inappropriate application, its impact on emergency and routine services, restrictions on civil liberties, psychological impacts and stigmatization, and lost wages and school absence.
4. Acceptability and Preferences
Qualitative Evidence Synthesis
Nine qualitative studies examined the acceptability of quarantine (Baum et al., 2009; Bell and WHO, 2004; Cava et al., 2005b; Desclaux et al., 2017; DiGiovanni et al., 2004; Leung et al., 2008; Lin et al., 2010; Pellecchia et al., 2015; Robertson et al., 2004). These studies found that the public understood and accepted the general concept of quarantine as one of the mechanisms for slowing the transmission of a contagious disease through a population. Even vulnerable groups, such as the homeless, were not opposed to the idea in general. People had several reasons for this view, including a sense of duty, ethical concerns, and civic-mindedness. Thus, agencies can facilitate adherence to quarantine by acknowledging that the public in general accepts, and does not resist, the general idea of quarantine as a response to an infectious disease event (high confidence in the evidence). These qualitative studies also found that the acceptability of and preference for quarantine differed across the various agencies working together to implement quarantine, with some advocating an emphasis on voluntary adherence and others seeking mandatory enforcement, which may include a militaristic response. If community groups are added as stakeholders, which in
many instances they should be, the divergence of views on the acceptability of quarantine as a public health intervention may become even wider. Open-ended deliberations among stakeholders could address this divergence and achieve common ground. Furthermore, the implementation of quarantine is unique to contagious disease outbreaks and perhaps to other emergencies in which the health hazard may be communicable through contact. Therefore, capacity building, such as through training, may require a dedicated one-hazard focus, which may not be feasible for an agency to implement on a regular basis.
Case Report Evidence Synthesis
Quarantine may not be acceptable to all communities, given case reports of psychological distress; anxiety; and fear of income loss, stigma, and social isolation. Furthermore, as noted above and as evidenced by findings from a tabletop exercise in San Diego, authorities and public health agencies may have differing preferences with regard to the implementation of quarantine (DiGiovanni et al., 2005).
It is possible that the provision of food, wage compensation, and other financial or in-kind supports can enhance the acceptability of quarantine. Making quarantine voluntary instead of mandatory also could increase its acceptability (CDC, 2003b; Chen et al., 2005; Chung et al., 2015; Ehlkes et al., 2017; Pang et al., 2003; Reaves et al., 2014; Yoon et al., 2016; Zhang et al., 2012). Lessons learned from case reports in Liberia and Ohio indicate that engaging local leaders and involving community members during the planning and implementation phases helped support safe and effective quarantine (Gastañaduy et al., 2016; Nyenswah et al., 2015). Additionally, efforts made to minimize stigmatization of Ebola survivors through education, social mobilization, and reintegration programs may have led to greater adherence to voluntary quarantine because community members did not fear being stigmatized (Reaves et al., 2014). By contrast, a case report of MERS from South Korea indicates that many quarantined individuals were unwilling to provide personal information because of anticipated sigma or negative local perception of MERS (Yoon et al., 2016).
Descriptive Survey Study Evidence
Tracy and colleagues (2009) conducted a survey of the public perceptions of quarantine following a contagious disease outbreak in Canada. Responses revealed a high rate of public acceptance of quarantine as a means of controlling the spread of a contagious disease. The vast majority of respondents expressed strong support for the use of quarantine in a contagious disease outbreak, for legal penalties against absconders, for social supports for those affected, and for public safeguards against potential inappropriate use. A survey conducted by Teh and colleagues (2012) collected information on attitudes toward and understanding of quarantine measures in quarantined households in Australia during the H1N1 outbreak in that country. Most respondents said that they considered quarantine useful and that the quarantine measures imposed were justified; the proportion of respondents who expressed the latter view increased when the survey asked about a scenario of more serious pandemic influenza. A survey examining the public’s reaction to the use of quarantine in Hong Kong, Singapore, Taiwan, and the United States found strong majorities favor quarantining in each country (Blendon et al., 2006). In general, Americans were less supportive of more restrictive monitoring methods (e.g., use of electronic bracelets or guards) than were people living in other regions and strongly preferred home quarantine. Kelly and colleagues (2015) assessed perceptions and beliefs about possible Ebola-related policies, such as mandatory quarantine, in the United States. A majority of respondents said that all individuals who have been exposed to an Ebola patient should be quarantined for 21 days whether or not they show
symptoms. Among respondents to a survey examining trust in government and public attitudes toward mandatory quarantine in the case of a smallpox outbreak in the United States, statistically significant predictors of opposition to mandatory quarantine policy were believing government would abuse power and personal liberties would be violated (Taylor-Clark et al., 2005). Conversely, having children and fears about personally contracting smallpox were significant predictors of support for mandatory quarantine. Overall, more people were opposed to mandatory vaccination than to mandatory quarantine.
5. Feasibility and PHEPR System Considerations
Synthesis of Modeling Studies
Findings from the synthesis of 12 modeling studies indicate the importance of preoutbreak surveillance. Initiating quarantine in a timely manner requires accurate and granular pre- and intra-outbreak surveillance, as well as linkages to rapid decision making and implementation efforts. Modeling studies that explored the use of quarantine in various localities or focused effects of differential quarantine on locally exposed individuals and travelers entering an area found that the relative value of these efforts depends on the fraction of an epidemic or outbreak that is driven by local transmission versus imported cases. A further finding of modeling studies is that if quarantine is implemented in an uncoordinated manner in multiple areas, the result can be redundancy and the expenditure of excess effort and resources.
Qualitative Evidence Synthesis
The corpus of qualitative studies makes clear that all of the staffing and operational capacities necessary to implement quarantine, such as the ability to initiate a legal order and ensure its enforcement, conduct contact tracing, and monitor adherence to quarantine, currently exist in many agencies and need not be newly created. Some study authors point out that if quarantine will need to be scaled up from a small number of people, to a very large population, shortages of staffing and supplies may occur, but these shortages can be planned for in advance (Sell et al., 2018). However, for implementation of quarantine to be effective in a broader sense and avert restrictions on civil liberties and other harms requires that agencies clearly articulate their overall strategic vision and a corresponding plan for conducting quarantine operations. As noted in the above section on acceptability and preferences, moreover, the unique applicability of quarantine to emergencies in which a health hazard may be communicable through contact may necessitate a dedicated one-hazard focus for capacity building, whose regular implementation may be problematic.
Case Report Evidence Synthesis
Few case reports address the feasibility of quarantine; however, those that do so describe issues related to resources and scale (Grigg et al., 2015; Pang et al., 2003; Reaves et al., 2014). To achieve effective quarantine at a large scale, jurisdictions must have adequate capabilities and resources (Grigg et al., 2015; Reaves et al., 2014). Preexisting organizational frameworks also are necessary to support effective quarantine (Reaves et al., 2014). Pang and colleagues (2003) cite several factors to be considered in deciding who should be quarantined, such as resource availability, the ability to mobilize public health personnel, and social acceptability (Pang et al., 2003). Weighing these factors together is important in developing a feasible plan for quarantine or alternative measures that may be more effective in a given set of circumstances.
6. Resource and Economic Considerations
Qualitative Evidence Synthesis
As noted earlier, the provision of financial compensation, food, and professional social support to people on whom quarantine is imposed can facilitate adherence. The qualitative evidence base does not address the economic considerations associated with providing these resources; however, one can surmise that providing financial compensation for people in quarantine will require a large commitment of financial resources. Some authors (Cava et al., 2005b; DiGiovanni et al., 2004) suggest that the government or employers could assume this responsibility. Assistance with food will also require substantial economic resources, and some authors (Cava et al., 2005b; Desclaux et al., 2017; Pellecchia et al., 2015; Schemm Dwyer et al., 2017) suggest that funding for this purpose could be provided by the government or its agencies. Support may be required in particular for certain populations under quarantine, such as university students (Beaton et al., 2007) or homeless people (Leung et al., 2008). Economic resources will be required as well for the provision of professional support and the creation of organizational mechanisms for interagency deliberations and training. Resources related to the medical care of quarantined individuals include those needed for environmental decontamination, waste management, safe transportation, and availability of sufficient stocks of such supplies as masks and thermometers (Schemm Dwyer et al., 2017; Sell et al., 2018). Whether funding for all of these resources is to be provided by the government or the agencies themselves can be discussed among the agencies.
Case Report Evidence
Some case reports address the need to carefully consider the resources needed for quarantine against the expected benefits (CDC, 2003b; Chung et al., 2015; Collier et al., 2013; Gastañaduy et al., 2016; Nyenswah et al., 2015; Yasuoka, 2009; Zhang et al., 2012). For instance, during a 2011 measles outbreak in Indiana, the state health department incurred costs in the tens of thousands of dollars for public health measures. Although it is unclear how much of this expenditure was allocated to quarantine, findings suggest a greater need to weigh the burden of time and resources associated with quarantine against the desired outcomes (Collier et al., 2013). A further consideration is the provision of food and accommodations for health care workers quarantined in hospitals, as well as wage compensation for those placed on administrative leave (Chung et al., 2015). Still another is payment for quarantined people who are self-employed to compensate for some of their lost income, as well as compensation for small businesses employing 50 or fewer people that were ordered to close temporarily, costs that one case report indicates were funded by the government (Ooi et al., 2005). In another example, the city of Dallas made provisions for food and water for a pet in a household that had potentially been exposed to Ebola, and also requested state assistance to support quarantine-related costs (Spengler et al., 2015). In addition, the ability of agencies to quickly mobilize resource and surge capacity to cope with workloads imposed by quarantine (Binns et al., 2010; Tay et al., 2010; Tsang and Lam, 2003) requires substantial investment in public health personnel and infrastructure, including training and exercises for health care workers and leadership (Nathawad et al., 2013). Finally, as previously mentioned, the implementation of quarantine may be costly not only for public health agencies, hospitals, and local authorities but also for the public. Members of the public may incur both direct and indirect costs, including child care expenses, lost wages due to a lack of employer or government compensation, psychological harm, social stigma, and curtailment of civil liberties.
Descriptive Survey Study Evidence
Porten and colleagues (2006) assessed the amount of extra resources necessary for local public health agencies to implement quarantine and other control measures during the SARS outbreak in Germany. They found that local public health agencies with at least one SARS case under investigation had invested nearly double the working hours of those without a case under investigation. Many local public health agencies may have been hesitant to impose home quarantine on professionally active contacts for extended periods of time because they wished to avoid the need to provide financial compensation. Katz and colleagues (2019) sought to identify key features of preparedness, such as facilities, budget, and legal authority, that affected state and local public health officials’ decision to implement social distancing (isolation or quarantine) measures. A majority of public health agencies reported that despite having legal authority to make social distancing decisions, they lacked facilities and a line item in their budget for isolation or quarantine measures.
7. Equity
Synthesis of Evidence of Effect
The committee’s synthesis of evidence of effect showed that harms can result for those individuals placed in quarantine, including psychological harm (moderate COE) and individual financial hardship (high COE). As discussed earlier in the section on evidence of effect, quarantined households without access to paid leave from work are more likely to lose pay, and many experience further financial consequences. For low-income households in particular, being forced to take leave from work can exacerbate existing socioeconomic inequalities. Moreover, when people from already-marginalized communities are quarantined, the resulting stigmatization can result in an exacerbation of discrimination and marginalization that can last well beyond the quarantine period (Cava et al., 2005a; Desclaux et al., 2017; DiGiovanni et al., 2004; Lin et al., 2010; Pellecchia et al., 2015; Robertson et al., 2004; Schemm Dwyer et al., 2017). Unless the quarantine is kept confidential, those on whom it is imposed may be publicly labeled as potential carriers of a contagious disease, which may lead others to develop feelings of avoidance, suspicion, mistrust, and fear, and thus stigma, toward them. Thus, people on whom quarantine is imposed may experience the harm of social stigma (high confidence in the evidence). Furthermore, health care workers on whom quarantine is imposed may experience several harms—financial, social, and psychological, among others—similar to those experienced by the general public, but sometimes amplified (Desclaux et al., 2017; Maunder et al., 2003; Robertson et al., 2004). Three qualitative studies found that health care workers on whom quarantine is imposed may experience additional harms beyond those experienced by the general public (high confidence in the evidence).
Qualitative Evidence Synthesis
Five qualitative studies examined considerations with respect to at-risk populations when implementing quarantine (Baum et al., 2009; Charania and Tsuji, 2013; Desclaux et al., 2017; Leung et al., 2008; Pellecchia et al., 2015). These populations have unique needs that require modified quarantine policies to meet their life needs. In addition, as noted above, the harms of quarantine, such as financial, social, and psychological harms, may be especially pronounced for these groups. Thus, quarantine needs to be applied to at-risk groups with caution and a strong orientation of care. When imposing quarantine on at-risk populations
relative to the general population, agencies should accept a greater need for modifications to standard policies and assume that greater harms will result from the quarantine (high confidence in the evidence).
Synthesis of Case Report Evidence Synthesis
Case reports note the importance of considering the impact of quarantine on various sub-populations based on demographics, socioeconomic considerations, and access to resources. They observe that potential challenges to quarantine arise when it involves transient populations, such as homeless people, as they may be difficult to locate and monitor (Smith et al., 2015). Residents of homeless shelters who have challenges with continuity of care due to a lack of documentation in health records may pose additional challenges, as was the case with a measles outbreak in Minnesota when the disease was confirmed in a 9-month-old, U.S.-born infant who resided in a homeless shelter and had recently returned from abroad (Gahr et al., 2014). Extra effort is also necessary to support those quarantined in homeless shelters, who may face unique challenges and have access to fewer resources compared with people who self-quarantine in their own homes (CDC, 2003b; Gahr et al., 2014). Insufficient support may lead to ineffective quarantine and increase the risk of transmission in this population. Additionally, members of communities that are hesitant to engage with the public health system may require strategic, culturally tailored outreach to ease their fear and anxiety (Gastañaduy et al., 2016; Smith et al., 2015). As discussed earlier, unintended consequences of quarantine orders may include stigmatization of certain groups if adequate attention is not paid to cultural and social considerations (CDC, 2004; Smith et al., 2015). The Ebola case report from Dallas, for example, describes concerted efforts to minimize stigma by working with organizations and leaders from the local Liberian community (Smith et al., 2015). In addition, schoolchildren were provided with laptops, textbooks, and lesson plans to encourage adherence to quarantine measures. Financial assistance may help ease an otherwise inequitable burden among lower-income communities (Chung et al., 2015; DiGiovanni et al., 2005; Smith et al., 2015).
Descriptive Survey Study Evidence
Seale and colleagues (2009) conducted a survey to determine the community’s attitude toward pandemic influenza in Australia, and found that respondents who were self-employed or in casual employment were statistically significantly more likely to view being unable to work during home quarantine as problematic. Blake and colleagues (2010) found that some employment characteristics (inability to work from home, lack of paid sick leave) were statistically significantly associated with working adults’ perceived likelihood of financial problems and thus their ability to comply with quarantine recommendations. Respondents who would not be paid if unable to work were almost five times more likely than those who would be paid to say that they would likely lose their job or business as a result of having to stay home from work for 7 to 10 days. Wray and colleagues (2012) assessed individual and community factors likely to facilitate or hinder adherence to public health directives. They found that community demographics (e.g., measures of ethnic homogeneity and poverty) were likely to have the greatest influence on public health directives that last long and require high levels of sacrifice.
8. Ethical Considerations8
Because being placed in quarantine represents an infringement of an individual’s or group’s core liberty rights, it must be justified by an appeal to some equally or more important rights of others that it protects. Specifically, quarantine is almost always justified by the notion that it will protect unexposed people from the harm of being exposed to and contracting a contagious disease, or what is referred to as the harm principle. Given this ethical justification, one could say that any quarantine action that does not in fact reduce or stop the spread of a contagious disease is, by definition, unethical. Of course, the problem with saying this is that one might not know whether quarantine will be effective until it has been tried. In reality, then, the core ethical obligation of those considering whether to implement quarantine is to do the very best they can to determine in advance whether the quarantine will work, and to implement it in ways that will maximize its effectiveness while minimizing the extent to which it infringes on individual or group liberty rights. This latter idea—that if one is required to take actions that will restrict people’s liberties, one should do so in the least restrictive way possible that achieves the desired effect—is called the proportionality principle. This principle is widely discussed in public health ethics, as well as written into laws that allow public health authorities to implement quarantine and other measures that restrict people’s liberties.
Another ethical consideration is the need to recognize that people in quarantine are giving up their personal freedoms (whether voluntarily or not) in an effort to protect their community, and therefore are deserving of gratitude and respect. This is one justification for ensuring that people in quarantine are well cared for and that they do not suffer stigma later on. The other reason to be as kind as possible to those in quarantine is utilitarian: people who are deathly afraid of being placed in quarantine may flee the area, potentially spreading the contagion farther than it might have spread without a threatened quarantine. This is not an entirely hypothetical concern; there are several real-world examples of quarantines that failed or even backfired when people threatened with quarantine fled the area. With regard to legal justifications, essentially all governments have laws and regulations that allow for the implementation of quarantine in some circumstances. In the United States, these laws are primarily at the state rather than the federal level, which means it is important for public health professionals to be familiar with the specific legal requirements in their locality.
___________________
8 Ethical considerations included in this section were generated through committee discussions, drawing on the ethical principles laid out in Box 3-4 in Chapter 3 and key ethics and policy texts, including the 2009 Institute of Medicine letter report on crisis standards of care (IOM, 2009), the 2008 CDC white paper “Ethical Guidance for Public Health Emergency Preparedness and Response: Highlighting Ethics and Values in a Vital Public Health Service” (Jennings and Arras, 2008), Emergency Ethics: Public Health Preparedness and Response (Jennings et al., 2016), and The Oxford Handbook of Public Health Ethics (Mastroianni et al., 2019).
TABLE B4-10 Evidence to Decision Summary Table for Implementing Quarantine
| In what circumstances (e.g., based on biologic factors, risks, resource availability, legal authorities, social context) is quarantine effective? | |
|---|---|
| Balance of Benefits and Harms Quarantine can be effective at reducing the transmission of contagious disease and has the possible additional benefit of reducing the time to diagnosis for infected patients who are being monitored while under quarantine. However, it also can result in a number of harms. In particular, quarantine has the potential to result in abridging individual or community rights of freedom, movement, and association. In addition, there may be an increased risk of infection among those placed together in congregate quarantine settings. Quarantine can also create financial instability, social stigma, and compromised psychological well-being for quarantined individuals. Given these undesirable effects of quarantine, which can be both short and long term, the balance of benefits and harms is open to debate and should be assessed on a case-by-case basis. |
Sources of Evidence
|
| Acceptability and Preferences Overall, the public understands and accepts the general concept of quarantine, but this understanding and acceptance is not uniform across all societies, and the acceptability of quarantine can vary depending on levels of social trust in the authorities implementing it. Moreover, fear of harms may make quarantine unacceptable in some communities. The acceptability of and preference for quarantine may differ as well across the multiple individuals and agencies that often must work together to implement quarantine, with some advocating an emphasis on voluntary adherence and others seeking mandatory enforcement, which may include a militaristic response. In general, the evidence suggests that voluntary quarantine is more acceptable, and therefore can be more effective, than mandatory quarantine. |
Sources of Evidence
|
| Feasibility and Public Health Emergency Preparedness and Response System Considerations Quarantine is more effective at reducing or stopping the transmission of a contagious disease when exposed individuals can be identified reliably and quickly. To initiate quarantine in a timely manner requires accurate, up-to-date, and specific pre- and intra-outbreak surveillance, as well as preexisting organizational frameworks and linkages to rapid decision making, including an in-place legal framework. Feasibility is also related to the scale of quarantine; if quarantine is uncoordinated and implemented at an intense level in multiple geographic areas, there is greater potential for redundancy and excess effort and resource expenditures, as well as for flight of individuals beyond designated boundaries. In addition, quarantine may become infeasible or less effective because of reduced adherence when the proposed duration of quarantine is longer. Although staffing and operational capacities to implement quarantine currently exist in many agencies, operational limitations may arise when quarantine is implemented on a large scale. Home quarantine may be more feasible than providing designated facilities for quarantined individuals, but is not without concerns over such harms as increased risk of infection among those housed together and challenges with adherence. |
Sources of Evidence
|
| Resource and Economic Considerations Implementing quarantine is highly resource intensive (e.g., the potential need to provide financial compensation, food, and social support). Therefore, factors that need to be considered when deciding whether to implement quarantine include resource availability, such as the ability to mobilize public health personnel to conduct contact tracing (to identify those who might warrant being placed in quarantine) and regular symptom monitoring of those in quarantine (to detect those who are becoming ill and require isolation and medical care). Resources related to the medical care of quarantined individuals include those needed for environmental decontamination, waste management, safe transportation, and availability of sufficient stocks of such supplies as masks and thermometers. Quarantine may be costly not only for response agencies but also for the individuals placed in quarantine, and has the potential to result in broad social and economic disruption. Quarantined individuals may incur both direct and indirect costs, including child care expenses and lost wages due to a lack of employer or government compensation. Thus, public health agencies need to consider the resources required for quarantine against its expected benefits. |
Sources of Evidence
|
| Equity When considering whether or how to impose quarantine on members of at-risk populations, public health leaders and agencies need to acknowledge that greater harms are likely to result for marginalized populations, creating a stronger obligation to protect them. At-risk populations can have additional needs affecting their ability to adhere to quarantine, and agencies need to consider the impact on various subpopulations based on demographics, socioeconomic considerations, and baseline access to resources. For example, potential challenges to quarantine arise when it involves transient populations such as people that are homeless, as they may be difficult to locate and monitor. Additionally, being forced to miss work can potentially exacerbate preexisting socioeconomic inequalities. The inequitable impacts of quarantine tend to be compounded over time such that the longer a quarantine lasts, the more sacrifice it requires of those being quarantined, and the more likely it is to exacerbate underlying societal, economic, and health care inequities. Finally, health care workers on whom quarantine is imposed may experience financial, social, and psychological harms, similar to those that occur to the general public; however, these harms may be amplified for health care workers for a number of reasons because of their responsibilities. |
Sources of Evidence
|
|
| Ethical Considerations When implemented correctly and in the proper setting, quarantine is ethically justified by the expectation that it will protect unexposed people from the harm of being exposed to and contracting a contagious disease—a notion that has been called the harm principle. Given this ethical justification (i.e., that quarantine prevents harm), one could say that any quarantine action that does not in fact reduce or stop the spread of a contagious disease is unethical. Of course, the problem with saying this is that one may not know whether a quarantine will be effective until it is tried. In reality, then, the core ethical obligation involved in considering whether to implement quarantine is to do the very best to determine in advance whether the quarantine will work, and to implement it in ways that will maximize its effectiveness while minimizing the extent to which it infringes on individual or group liberties and rights (principle of proportionality). Another ethical consideration for quarantine is the need to recognize that people in quarantine are giving up their personal freedoms (whether voluntarily or not) in an effort to protect their community, and thus deserve gratitude and respect (principle of respect for persons and communities). Indeed, this consideration represents one justification for efforts to ensure that people in quarantine are well cared for and that they do not suffer stigma later on. The other justification for such efforts is utilitarian (principle of harm reduction and benefit promotion): people who fear being placed in quarantine may flee the area, potentially spreading the contagion even farther than it might have spread without a threatened quarantine. This is not an entirely hypothetical concern; there are several real-world examples of quarantines that failed or even backfired when people threatened with quarantine fled the area. With regard to legal justifications, essentially all governments have laws and regulations that allow for the implementation of quarantine in some circumstances. In the United States, these laws are primarily at the state rather than the federal level, which means it is important for public health professionals to be familiar with the specific legal requirements in their locality. |
Source of Evidence
|
|
CONSIDERATIONS FOR IMPLEMENTATION
The following considerations for implementation were drawn from the syntheses of quantitative comparative studies, modeling studies, qualitative research studies, and case reports, as well as descriptive surveys.
9. Facilitating Adherence to and Minimizing Harms from Quarantine Measures
Ensure Transparent and Strategic Risk Communication Using Clear Definitions
Synthesis of evidence of effect
The committee’s synthesis of evidence of effect showed that while adherence to quarantine measures can vary by culture, disease, and socioeconomic status, use of various strategies, including risk communication and messaging and access to leave, can improve adherence (moderate COE).
Case report evidence synthesis
Lessons learned from case reports also stress the importance of open, frequent, and transparent communication with the public to ease fear and anxiety (Ehlkes et al., 2017; Tay et al., 2010; Tsang and Lam, 2003; Ward et al., 2010). Useful channels for public communication include daily press briefings, television and radio announcements, Internet bulletins, health talks, and a hotline for public enquiry. During the SARS outbreak in Beijing, the city’s Ministry of Health and municipal government also ran education campaigns via billboards, bus advertisements, and traditional banners (Pang et al., 2003). In the U.S. context, during the 2011 measles outbreak in Indiana, the state issued local media releases and used the Indiana Health Alert Network to inform community members and providers about potential exposure to the disease (Collier et al., 2013).
Strategic timing of communication can be an important facilitator of effective quarantine. During the H1N1 pandemic of 2009 in Singapore, a gradual strategic shift from containment to mitigation as part of the risk communication strategy enabled the public to adapt to new measures (Tay et al., 2010). Home visits to provide health education for those quarantined at home may also promote adherence (Ooi et al., 2005). In addition, the public and health care workers need to have a clear understanding of the term “quarantine,” which is often misunderstood despite having backing by legal authority (Barbisch et al., 2015), and differences in interpretation may lead to inconsistent application of quarantine laws across jurisdictional boundaries.
Descriptive survey study evidence
Eastwood and colleagues (2009, 2010) found that having a basic knowledge of pandemic influenza was statistically associated with willingness to adhere to quarantine measures. Their findings suggest further that discordance between what people state they will do and what they actually do relates to how they perceive risk. Bauerle Bass and colleagues (2010) investigated factors and specific sociodemographic characteristics that may influence an individual’s decision to adhere to quarantine measures. Their findings indicate that overall knowledge regarding avian influenza, beliefs about its severity, and the perceived likelihood that the respondent and/or his or her significant other(s) might contract it were predictive of willingness to adhere.
Adapt Policy: Voluntary Versus Legally Enforced Quarantine
Synthesis of modeling studies
Some modeling studies found that adherence may be greater with less strict quarantine procedures, making those procedures more effective despite them being less strict.
Qualitative evidence synthesis
Seven qualitative studies found a flexible quarantine implementation policy to be important (Bell and WHO, 2004; Cava et al., 2005b; Charania and
Tsuji, 2013; Desclaux et al., 2017; DiGiovanni et al., 2004; Leung et al., 2008; Sell et al., 2018). Findings from these studies suggest that people on whom quarantine is imposed may find the restrictions acceptable if agencies adapt quarantine policies to suit populations and situations (moderate confidence in the evidence). Quarantine restrictions may be more acceptable if reasonable modifications of rules and procedures are made to suit the needs of the situation and the people being placed under quarantine. These modifications might include changes to policies related to using tobacco and alcohol in group facilities, leaving quarantine sites to obtain supplies or go to work, and using public transportation to get to work. In this regard, quarantine can be seen as a nuanced measure that is dependent on the situation.
Case report evidence synthesis
Several case reports address the use of both voluntary and compulsory quarantine; however, they do not examine whether one of these strategies leads to greater adherence than the other (CDC, 2004; Chen et al., 2005; Chung et al., 2015; Collier et al., 2013; Ehlkes et al., 2017; Ooi et al., 2005; Plipat et al., 2017; Reaves et al., 2014; Tay et al., 2010). Voluntary self-quarantine of health care workers in Dallas during the 2014 cluster of Ebola had high adherence; more than 30 health care workers adhered to the quarantine in the absence of a public health order, as did all but a small subset of additional contacts (Chung et al., 2015). Similarly, during the SARS outbreak in Toronto, only 0.1 percent of contacts requiring quarantine had to be issued an enforceable quarantine order because of initial noncompliance. At the same time, while voluntary quarantine may motivate people to adhere because of a sense of choice, fear of prosecution and hefty fines may encourage even greater adherence. Some case reports cite use of police, sheriffs, and security agencies to enforce quarantine policies, some guarding doors and buildings and others conducting random checks on quarantined individuals (Barbisch et al., 2015; CDC, 2003b; Collier et al., 2013; Ooi et al., 2005; Pang et al., 2003). Yet, while some legally enforceable strategies may be relevant in the U.S. context, more invasive or aggressive measures may face resistance. Therefore, cultural context needs to be carefully considered when strategies are developed. This was the case during a tabletop exercise in San Diego focused on quarantine, when civilian law enforcement officials frequently expressed concerns about carrying out enforcement measures requested by civilian public health authorities (DiGiovanni et al., 2005), instead urging an emphasis on public education to minimize the need for enforcement.
Provide Financial Compensation, Food, and Social and Psychological Support
Synthesis of evidence of effect
The committee’s synthesis of the evidence of effect showed that an emphasis on health by those leading the outbreak response (i.e., health-promoting leadership, discussed earlier) can reduce depression and anxiety symptoms among quarantined individuals (very low COE). The evidence of effect also indicates that while adherence to quarantine measures can vary by culture, disease, and socioeconomic status, it can be improved through the use of various strategies, including risk communication and messaging and access to employment leave (moderate COE).
Qualitative evidence synthesis
Four qualitative studies found providing financial compensation for people subject to quarantine to be important (Baum et al., 2009; Braunack-Mayer et al., 2010; Cava et al., 2005a; Desclaux et al., 2017). This compensation included partial or full income replacement for the duration of the quarantine; assurance of job security and
economic recovery following the end of quarantine; and payment for rent, water, electricity, and other utilities. Findings from these studies suggest that people on whom quarantine is imposed may find the restrictions acceptable depending on the provision of financial compensation by government or other agencies (high confidence in the evidence).
Six qualitative studies found that providing food for quarantined people is important (Braunack-Mayer et al., 2010; Cava et al., 2005a; Desclaux et al., 2017; DiGiovanni et al., 2004; Leung et al., 2008; Pellecchia et al., 2015). Findings from these studies suggest that government and other agencies can deliver food directly or assist neighbors, friends, and volunteers with its purchase and delivery. Agencies need to keep in mind that any food support provided should match the dietary needs and wishes of the people under quarantine. People on whom quarantine is imposed may find the restrictions acceptable depending on the provision of food and other basic necessities by government and other agencies (high confidence in the evidence).
Six qualitative studies found that providing professional social support to quarantined people is important (Braunack-Mayer et al., 2010; Cava et al., 2005a; Desclaux et al., 2017; Lin et al., 2010; Maunder et al., 2003; Schemm Dwyer et al., 2017). Authors of these studies cite the provision of such support in the form of a dedicated new or preexisting general confidential telephone hotline that offers professional counseling and the provision of cell phones to those who do not possess one so they can stay connected to support networks. People on whom quarantine is imposed may find the quarantine restrictions acceptable depending on the provision of professional social support by government and other agencies (high confidence in the evidence).
Case report evidence synthesis
Several case reports describe provision of food, accommodations, social and psychological support, medical leave, and wage compensation to quarantined people (CDC, 2003b; Chen et al., 2005; Chung et al., 2015; Ehlkes et al., 2017; Pang et al., 2003; Reaves et al., 2014; Yoon et al., 2016; Zhang et al., 2012). During the 2014 Ebola cluster in Dallas, for instance, the hospital where health care workers were quarantined provided food, accommodations, and wage compensation (Chung et al., 2015). Based on Dallas’s experience, Smith and colleagues (2015) suggest that public health emergency preparedness for an Ebola outbreak could be enhanced by engaging a wide range of community partners, such as businesses, schools, charitable foundations, community and faith-based organizations, and mental health providers and organizations in readying support resources to meet potential needs of quarantined individuals (Smith et al., 2015). They also cite the importance of providing laptops, textbooks, and school supplies and developing lesson plans that can be completed at home. Although the effectiveness of these measures is not specifically assessed, case reports from Beijing, Liberia, South Korea, and Taiwan also mention the role of social and psychological supports—for example, having community committees mobilize to make such gestures as giving flowers and comforting letters, conducting prayer services, providing social services through local health or civic affairs departments, offering day care, and providing mental health services (CDC, 2003b; Nyenswah et al., 2015; Pang et al., 2003; Yoon et al., 2016). During the 2009 H1N1 outbreak in China, people quarantined in hotels were provided room service, and the government budget supported living expenses (Zhang et al., 2012).
Descriptive survey study evidence
Wray and colleagues (2012) assessed individual and community factors that are likely to facilitate or hinder adherence to public health quarantine directives. They found less likelihood of adherence to a 6-day quarantine among individuals anticipating a need for supplies and those finding it difficult to stay home.
Use Culturally and Contextually Relevant Approaches: A Community and Care Orientation
Qualitative evidence synthesis
The authors of eight qualitative studies emphasize the importance of considering the community perspective rather than the individual perspective when developing a quarantine strategy (Baum et al., 2009; Braunack-Mayer et al., 2010; Cava et al., 2005b; Charania and Tsuji, 2013; Desclaux et al., 2017; Leung et al., 2008; Pellecchia et al., 2015; Smith et al., 2012). Findings from these studies suggest that agencies need to understand that the members of a community on whom quarantine is imposed often regard its impact at the community rather than the individual or abstract “common good” level to be more important. Therefore, agencies need to consider the life circumstances of and work cooperatively with the community to increase adherence to quarantine (high confidence in the evidence). Quarantine is generally conceptualized as restriction of the rights of individuals for the benefit of the abstract “common good,” which may be thought of as the larger society. Between these two levels of the individual and the larger society, however, exists the level of the community, which may be understood as a group of individuals with strong social bonds (Smith et al., 2012). When quarantine is imposed on some members of a community, those tight social bonds mean that the life of the whole community is affected as well. Thus, to ensure that individuals on whom quarantine is imposed adhere to its restrictions, agencies need to understand the community’s life circumstances, such as economic status, political history, trust of agencies and government, and cultural and religious customs, and work in cooperation with its existing power and leadership social structures.
Two qualitative studies highlight the importance of considering the care rather than the enforcement perspective with respect to those placed in quarantine (Desclaux et al., 2017; Maunder et al., 2003). Findings from these studies suggest that agencies can have an orientation of care, as opposed to an orientation of enforcement, toward the people on whom quarantine is imposed to increase adherence (low confidence in the evidence). Such an orientation means interacting with quarantined people in a way that resembles care, showing concern for their needs, and extending empathetic support rather than emphasizing control and enforcement.
Case report evidence synthesis
Given the cultural diversity of the United States, culturally informed strategies may enable more effective quarantine. For instance, during measles outbreaks in a Somali community in Minnesota and an Amish community in Ohio, efforts were made to engage community, religious, and spiritual leaders as advisors because of their strong influence on social networks (Gahr et al., 2014; Gastañaduy et al., 2016). Lessons learned from the Ebola outbreak in Dallas include that “recognizing unique cultural, linguistic, and socioeconomic differences helped ensure contacts’ compliance with monitoring, particularly among the community contacts” (Smith et al., 2015). Contact tracers found that because the first Ebola patient was Liberian, many of his contacts were part of the local Liberian community. Therefore, they engaged aid organizations to provide familiar food and clothing in a culturally sensitive manner.
Trust is mentioned as an important factor in facilitating effective quarantine in case reports from Germany, Liberia, and Singapore (Ehlkes et al., 2017; Nyenswah et al., 2015; Tay et al., 2010). During the 2014 Ebola outbreak in Liberia, community trust and confidence in response efforts were found to be challenging at times, as some community members might not have been willing to accept proposed quarantine without first witnessing the devastating effect of the disease on their village (Nyenswah et al., 2015). Trusted local leaders helped facilitate trust and acted as liaisons between community leaders and district health
authorities, suggesting that integrating trusted local leaders into response planning and giving them an opportunity to provide feedback before decisions related to public health interventions are made may promote effective quarantine. A case report of the 2009 H1N1 outbreak in Singapore also mentions the importance of building trust in advance of a public health crisis (Tay et al., 2010). Public perception of the quality and credibility of decisions related to control measures and policies reportedly enabled buy-in from health care stakeholders during the response to that outbreak, particularly for policies that were burdensome to implement. The authors recommend regular engagement among stakeholders during “peacetime” as a way of fostering stronger coordination of public health control measures during a crisis. In their case report of the 2016 outbreak of Lassa fever in Germany, Ehlkes and colleagues (2017) describe how contact-tracing interviews can be used as an opportunity to build trust between investigators and interviewees to enhance adherence to quarantine (Ehlkes et al., 2017). Although these findings are based on case reports from abroad, they may be applicable in the United States as well, given that the level of trust between the public and key stakeholders is likely to influence the effectiveness of quarantine, particularly in communities that may have a historical distrust of the U.S. government.
Descriptive survey study evidence
Bauerle Bass and colleagues (2010) investigated factors and specific sociodemographic characteristics that may influence an individual’s decision to adhere to quarantine measures. The findings of this survey align with the qualitative and case report evidence regarding the importance of understanding the life circumstances of and working in cooperation with the community to increase adherence. Differences were observed among demographic groups in the willingness to comply with quarantine orders, with women and individuals who were not employed being more willing to remain at or to go to a government-designated facility if ordered to do so.
10. Other Implementation Considerations
The following conceptual findings inform the perspectives and approaches public health agencies could consider when implementing quarantine.
Define the Effectiveness of Quarantine More Broadly
Qualitative evidence synthesis
Fourteen qualitative studies highlight the potential need for a broader definition of effectiveness for quarantine (Baum et al., 2009; Beaton et al., 2007; Bell and WHO, 2004; Braunack-Mayer et al., 2010; Cava et al., 2005b; Desclaux et al., 2017; DiGiovanni et al., 2004; Lin et al., 2010; Maunder et al., 2003; Pellecchia et al., 2015; Robertson et al., 2004; Schemm Dwyer et al., 2017; Sell et al., 2018; Smith et al., 2012). The results of these studies suggest that agencies may want to judge the effectiveness of quarantine not only using the metric of medical outcomes but also in terms of the degree of protection of the civil rights of the public on whom quarantine is imposed. Along the same lines, agencies may also want to judge the effectiveness of quarantine in terms of the extent to which the public on whom quarantine is being imposed is protected from harms that result from the quarantine restrictions (moderate confidence in the evidence). Agencies typically judge the effectiveness of quarantine only from a single utilitarian criterion of reduction of morbidity and mortality in the general population. However, because quarantine almost always is imposed on a group of people without their consent, it may also be important to include two additional criteria—protection of civil rights and protection from harms—when judging the effectiveness of quarantine.
Case report evidence synthesis
Barbisch and colleagues (2015) are the only authors who explicitly mention difficulty with determining the effectiveness and equitable application of quarantine policies, particularly given the issues of personal liberties. The authors assert that the restrictive nature of quarantine means it should be evaluated for efficacy. For instance,
Is the action supported by evidence of improved outcomes?; can it be effectively implemented given the need for balanced [Stuff, Staff, and Structure] surge?; will it lead to unintended negative outcomes?; are other less restrictive public health measures such as monitoring and social distancing equally effective?; and finally, given the impact on civil liberties, is it reasonable, and is it enforceable? (Barbisch et al., 2015)
Develop Options for Different Levels of Quarantine and Plan for Integration with Other Non-Pharmaceutical Interventions
Synthesis of modeling studies
The modeling studies reviewed provide a number of other important points regarding the invasiveness of quarantine. Findings from modeling studies that compared quarantine with other, less invasive or intensive interventions, such as symptom monitoring or voluntary reporting, suggest that these alternatives may make it possible to achieve similar levels of effectiveness and control for less transmissible infections that lack asymptomatic infectious periods without incurring the potential harms of social stigma, social and economic disruption, and large-scale use of resources. Results of modeling studies that explored quarantine efforts carried out in various localities or focused differential quarantine efforts on locally exposed individuals and travelers entering an area suggest that the relative value of these control efforts depended on the fraction of an epidemic or outbreak driven by local transmission versus imported cases.
Local quarantine efforts may have both direct and indirect spillover effects, reducing transmission in areas not implementing quarantine. If quarantine is used to help control an outbreak in one area, nearby areas may face fewer imported cases; hence, the need to implement quarantine in these surrounding areas may be reduced (an example of direct spillover). Moreover, chains of such spillovers to areas not directly connected to the original area can occur, which may alter the need for or required level and speed of quarantine in these areas as well (indirect spillovers). As a result, if quarantines are implemented in an uncoordinated manner in multiple areas, redundancy and excess expenditure of effort and resources may result.
Qualitative evidence synthesis
Four qualitative studies addressed different levels of quarantine (Bell and WHO, 2004; Charania and Tsuji, 2013; Desclaux et al., 2017; Smith et al., 2012). Findings from these studies suggest that agencies can enhance the effectiveness of quarantine by developing screening and monitoring criteria that allow for graded quarantine options matched to the characteristics of the infectious disease and its spread (moderate confidence in the evidence). Different levels of quarantine appropriately depend on the severity and magnitude of the contagious disease situation. Similarly, criteria for placing people in quarantine can differ based on risk of exposure; contacts, such as people exposed to ill family members in close quarters, are at highest risk (aside from health care workers with certain unprotected patient care exposures).
Consider Implementing Quarantine Early, Especially When There Is a Lack of Available Medical Countermeasures
Synthesis of modeling studies
Results of modeling studies that explored the timing of initiating quarantine tend to emphasize that it is more effective if implemented closer to when the first case occurs or is equivalently effective but involves quarantining substantially fewer exposed individuals.
Qualitative evidence synthesis
Three qualitative studies examined the implementation of quarantine in situations in which medical response infrastructure is lacking (Bell and WHO, 2004; Braunack-Mayer et al., 2010; Charania and Tsuji, 2013). Findings from these studies suggest that agencies need to recognize that for regions lacking robust medical response infrastructures, non-pharmaceutical interventions such as quarantine may be especially effective (moderate confidence in the evidence). The international experience shows that at the start of a contagious disease outbreak, countries may lack targeted countermeasures, such as drugs and vaccines. Similarly, there may be regions in a country where the stockpile of drugs and vaccines is limited or where the delivery of such supplies may take time because of remoteness or other logistical obstacles. In these circumstances, non-pharmaceutical interventions have often been the only measures available to combat epidemics, especially at the beginning of an outbreak (Bell and WHO, 2004; Braunack-Mayer, 2010; Charania and Tsuji, 2013).
Case report evidence synthesis
A SARS case report from Singapore describes how the decision to undertake quarantine measures was not necessarily based on scientific evidence of the merits of quarantine but on the need to protect the public from a serious new disease with a high case fatality rate (14 percent) (Ooi et al., 2005). The absence of effective vaccination and antiviral treatment strengthened the argument for quarantine management to stop the spread of the disease, given its potentially catastrophic consequences.
Integrate and Coordinate Response at the Systems Level
Qualitative evidence synthesis
Four qualitative studies examined the importance of understanding that quarantine requires interagency coordination (Desclaux et al., 2017; DiGiovanni et al., 2004; Schemm Dwyer et al., 2017; Sell et al., 2018). Findings from these studies suggest that agencies can facilitate adherence to quarantine by understanding that to implement quarantine, multiple agencies and multiple jurisdictions are required to work in concert (moderate confidence in the evidence). Planning and implementation of quarantine require interagency coordination that includes the legal system. This interagency coordination needs to include plans for the scalability of operations in terms of the number of people placed in quarantine during the course of a contagious disease outbreak.
Case report evidence synthesis
Findings from case reports indicate that effective control measures do not work in isolation and require coordination among key stakeholders (Tsang and Lam, 2003). The majority of case reports describe quarantine as one of multiple measures implemented during a response. Integrated responses at the systems level have been found to be essential for a coherent response in fostering a better-coordinated system (Tay et al., 2010). Reliance on preexisting organizational frameworks can also enable efficient redirection of resources (Reaves et al., 2014). In addition, collaborative agreements and coordinated incident command are highlighted as essential for areas with multiple jurisdic-
tions (e.g., civilian, military, federal, tribal) (DiGiovanni et al., 2005). Case reports mention as well the general need for public health surge capacity in light of the threats of emerging diseases and large-scale outbreaks (Binns et al., 2010; Svoboda et al., 2004; Tsang and Lam, 2003). A strong sense of political will and urgency is viewed as facilitating the rapid establishment of command structures aimed at steering action and mobilizing relevant sectors and resources (Tsang and Lam, 2003). Furthermore, the need for flexibility is stressed, as existing plans and predetermined control measures may need to be modified as a public health emergency evolves (Chung et al., 2015; Tay et al., 2010).
REFERENCES FOR ARTICLES INCLUDED IN THE MIXED-METHOD REVIEW
Quantitative Comparative Studies
Adler, A. B., P. Y. Kim, S. J. Thomas, and M. L. Sipos. 2018. Quarantine and the U.S. military response to the Ebola crisis: Soldier health and attitudes. Public Health 155:95–98.
Bondy, S. J., M. L. Russell, J. M. Lafleche, and E. Rea. 2009. Quantifying the impact of community quarantine on sars transmission in Ontario: Estimation of secondary case count difference and number needed to quarantine. BMC Public Health 9:488.
Chu, C. Y., C. Y. Li, H. Zhang, Y. Wang, D. H. Huo, L. Wen, Z. T. Yin, F. Li, and H. B. Song. 2010. Quarantine methods and prevention of secondary outbreak of pandemic (H1N1) 2009. Emerging Infectious Diseases 16(8):1300–1302.
Delaporte, E., C. A. Wyler Lazarevic, A. Iten, and P. Sudre. 2013. Large measles outbreak in Geneva, Switzerland, January to August 2011: Descriptive epidemiology and demonstration of quarantine effectiveness. European Communicable Disease Bulletin 18(6):7.
Hawryluck, L., W. L. Gold, S. Robinson, S. Pogorski, S. Galea, and R. Styra. 2004. SARS control and psychological effects of quarantine, Toronto, Canada. Emerging Infectious Diseases 10(7):1206–1212.
Hsieh, Y. H., C. C. King, C. W. Chen, M. S. Ho, J. Y. Lee, F. C. Liu, Y. C. Wu, and J. S. JulianWu. 2005. Quarantine for SARS, Taiwan. Emerging Infectious Diseases 11(2):278–282.
Jeong, H., H. W. Yim, Y. J. Song, M. Ki, J. A. Min, J. Cho, and J. H. Chae. 2016. Mental health status of people isolated due to Middle East Respiratory Syndrome. Epidemiology and Health 38:e2016048.
Kavanagh, A. M., R. J. Bentley, K. E. Mason, J. McVernon, S. Petrony, J. Fielding, A. D. LaMontagne, and D. M. Studdert. 2011. Sources, perceived usefulness and understanding of information disseminated to families who entered home quarantine during the H1N1 pandemic in Victoria, Australia: A cross-sectional study. BMC Infectious Diseases 11:2.
Kavanagh, A. M., K. E. Mason, R. J. Bentley, D. M. Studdert, J. McVernon, J. E. Fielding, S. Petrony, L. Gurrin, and A. D. LaMontagne. 2012. Leave entitlements, time off work and the household financial impacts of quarantine compliance during an H1N1 outbreak. BMC Infectious Diseases 12:311.
Lee, S. M., W. S. Kang, A. R. Cho, T. Kim, and J. K. Park. 2018. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Comprehensive Psychiatry 87:123–127.
Liu, X., M. Kakade, C. J. Fuller, B. Fan, Y. Fang, J. Kong, Z. Guan, and P. Wu. 2012. Depression after exposure to stressful events: Lessons learned from the severe acute respiratory syndrome epidemic. Comprehensive Psychiatry 53(1):15–23.
Marjanovic, Z., E. R. Greenglass, and S. Coffey. 2007. The relevance of psychosocial variables and working conditions in predicting nurses’ coping strategies during the SARS crisis: An online questionnaire survey. International Journal of Nursing Studies 44(6):991–998.
McVernon, J., K. Mason, S. Petrony, P. Nathan, A. D. LaMontagne, R. Bentley, J. Fielding, D. M. Studdert, and A. Kavanagh. 2011. Recommendations for and compliance with social restrictions during implementation of school closures in the early phase of the influenza a (H1N1) 2009 outbreak in Melbourne, Australia. BMC Infectious Diseases 11:257.
Miyaki, K., H. Sakurazawa, H. Mikurube, M. Nishizaka, H. Ando, Y. Song, and T. Shimbo. 2011. An effective quarantine measure reduced the total incidence of influenza A H1N1 in the workplace: Another way to control the H1N1 flu pandemic. Journal of Occupational Health 53(4):287–292.
Reynolds, D. L., J. R. Garay, S. L. Deamond, M. K. Moran, W. Gold, and R. Styra. 2008. Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiology and Infection 136(7):997–1007.
Wu, P., X. Liu, Y. Fang, B. Fan, C. J. Fuller, Z. Guan, Z. Yao, J. Kong, J. Lu, and I. J. Litvak. 2008. Alcohol abuse/dependence symptoms among hospital employees exposed to a SARS outbreak. Alcohol and Alcoholism 43(6):706–712.
Wu, P., Y. Fang, Z. Guan, B. Fan, J. Kong, Z. Yao, X. Liu, C. J. Fuller, E. Susser, J. Lu, and C. W. Hoven. 2009. The psychological impact of the SARS epidemic on hospital employees in China: Exposure, risk perception, and altruistic acceptance of risk. Canadian Journal of Psychiatry 54(5):302–311.
Modeling Studies
Included in Detailed Analysis
Ahn, I., S. Heo, S. Ji, K. H. Kim, T. Kim, E. J. Lee, J. Park, and K. Sung. 2018. Investigation of nonlinear epidemiological models for analyzing and controlling the MERS outbreak in Korea. Journal of Theoretical Biology 437:17–28.
An der Heiden, M., U. Buchholz, G. Krause, G. Kirchner, H. Claus, and W. H. Haas. 2009. Breaking the waves: Modeling the potential impact of public health measures to defer the epidemic peak of novel influenza A/H1N1. PLOS ONE [Electronic Resource] 4(12):e8356.
Day, T., A. Park, N. Madras, A. Gumel, and J. Wu. 2006. When is quarantine a useful control strategy for emerging infectious diseases? American Journal of Epidemiology 163(5):479–485.
D’Silva, J. P., and M. C. Eisenberg. 2017. Modeling spatial invasion of Ebola in West Africa. Journal of Theoretical Biology 428:65–75.
Enanoria, W. T., F. Liu, J. Zipprich, K. Harriman, S. Ackley, S. Blumberg, L. Worden, and T. C. Porco. 2016. The effect of contact investigations and public health interventions in the control and prevention of measles transmission: A simulation study. PLOS ONE [Electronic Resource] 11(12):e0167160.
Feng, Z., Y. Yang, D. Xu, P. Zhang, M. M. McCauley, and J. W. Glasser. 2009. Timely identification of optimal control strategies for emerging infectious diseases. Journal of Theoretical Biology 259(1):165–171.
Gupta, A. G., C. A. Moyer, and D. T. Stern. 2005. The economic impact of quarantine: SARS in Toronto as a case study. Journal of Infection 50(5):386–393.
Hsieh, Y. H., C. C. King, C. W. Chen, M. S. Ho, S. B. Hsu, and Y. C. Wu. 2007. Impact of quarantine on the 2003 SARS outbreak: A retrospective modeling study. Journal of Theoretical Biology 244(4):729–736.
Meltzer, M. I., I. Damon, J. W. LeDuc, and J. D. Millar. 2001. Modeling potential responses to smallpox as a bioterrorist weapon. Emerging Infectious Diseases 7(6):959–969.
Mubayi, A., C. K. Zaleta, M. Martcheva, and C. Castillo-Chavez. 2010. A cost-based comparison of quarantine strategies for new emerging diseases. Mathematical Biosciences & Engineering 7(3):687–717.
Peak, C. M., L. M. Childs, Y. H. Grad, and C. O. Buckee. 2017. Comparing nonpharmaceutical interventions for containing emerging epidemics. Proceedings of the National Academy of Sciences of the United States of America 114(15):4023–4028.
Podder, C. N., A. B. Gumel, C. S. Bowman, and R. G. McLeod. 2007. Mathematical study of the impact of quarantine, isolation and vaccination in curtailing an epidemic. Journal of Biological Systems 15(2):185–202.
Not Included in Detailed Analysis
Adams, B. 2016. Household demographic determinants of Ebola epidemic risk. Journal of Theoretical Biology 392:99–106.
Ahmad, M. D., M. Usman, A. Khan, and M. Imran. 2016. Optimal control analysis of Ebola disease with control strategies of quarantine and vaccination. Infectious Diseases of Poverty 5(1):72.
Aldis, G. K., and M. G. Roberts. 2005. An integral equation model for the control of a smallpox outbreak. Mathematical Biosciences 195(1):1–22.
Bachinsky, A. G., and L. P. Nizolenko. 2013. A universal model for predicting dynamics of the epidemics caused by special pathogens. BioMed Research International 2013:467078.
Barrett, C. L., S. G. Eubank, and J. P. Smith. 2005. If smallpox strikes Portland. Scientific American 292(3):42–49.
Blackwood, J. C., and L. M. Childs. 2016. The role of interconnectivity in control of an Ebola epidemic. Scientific Reports 6:29262.
Carrat, F., J. Luong, H. Lao, A. V. Salle, C. Lajaunie, and H. Wackernagel. 2006. A “small-world-like” model for comparing interventions aimed at preventing and controlling influenza pandemics. BMC Medicine 4:26.
Chau, P. H., and P. S. Yip. 2003. Monitoring the severe acute respiratory syndrome epidemic and assessing effectiveness of interventions in Hong Kong special administrative region. Journal of Epidemiology and Community Health 57(10):766–769.
Davey, V. J., R. J. Glass, H. J. Min, W. E. Beyeler, and L. M. Glass. 2008. Effective, robust design of community mitigation for pandemic influenza: A systematic examination of proposed us guidance. PLOS ONE [Electronic Resource] 3(7):e2606.
Del Valle, S., H. Hethcote, J. M. Hyman, and C. Castillo-Chavez. 2005. Effects of behavioral changes in a smallpox attack model. Mathematical Biosciences 195(2):228–251.
Dénes, A., and A. B. Gumel. 2019. Modeling the impact of quarantine during an outbreak of Ebola virus disease. Infectious Disease Modelling 4:12–27.
Ferguson, N. M., D. A. Cummings, S. Cauchemez, C. Fraser, S. Riley, A. Meeyai, S. Iamsirithaworn, and D. S. Burke. 2005. Strategies for containing an emerging influenza pandemic in Southeast Asia. Nature 437(7056):209–214.
Gumel, A. B., S. Ruan, T. Day, J. Watmough, F. Brauer, P. van den Driessche, D. Gabrielson, C. Bowman, M. E. Alexander, S. Ardal, J. Wu, and B. M. Sahai. 2004. Modeling strategies for controlling SARS outbreaks. Proceedings of the Royal Society of London—Series B: Biological Sciences 271(1554):2223–2232.
Halloran, M. E., N. M. Ferguson, S. Eubank, I. M. Longini, Jr., D. A. Cummings, B. Lewis, S. Xu, C. Fraser, A. Vullikanti, T. C. Germann, D. Wagener, R. Beckman, K. Kadau, C. Barrett, C. A. Macken, D. S. Burke, and P. Cooley. 2008. Modeling targeted layered containment of an influenza pandemic in the United States. Proceedings of the National Academy of Sciences of the United States of America 105(12):4639–4644.
Huo, X. 2015. Modeling of contact tracing in epidemic populations structured by disease age. Discrete and Continuous Dynamical Systems—Series B 20(6):1685–1713.
Iwami, S., Y. Takeuchi, and X. Liu. 2009. Avian flu pandemic: Can we prevent it? Journal of Theoretical Biology 257(1):181–190.
Jung, E., S. Iwami, Y. Takeuchi, and T. C. Jo. 2009. Optimal control strategy for prevention of avian influenza pandemic. Journal of Theoretical Biology 260(2):220–229.
Kato, F., K. Tainaka, S. Sone, S. Morita, H. Iida, and J. Yoshimura. 2011. Combined effects of prevention and quarantine on a breakout in SIR model. Scientific Reports 1:10.
Lagorio, C., M. Dickison, F. Vazquez, L. A. Braunstein, P. A. Macri, M. V. Migueles, S. Havlin, and H. E. Stanley. 2011. Quarantine-generated phase transition in epidemic spreading. Physical Review E: Statistical, Nonlinear, & Soft Matter Physics 83(2 Pt 2):026102.
Li, X., W. Geng, H. Tian, and D. Lai. 2013. Was mandatory quarantine necessary in China for controlling the 2009 H1N1 pandemic? International Journal of Environmental Research and Public Health [Electronic Resource] 10(10):4690–4700.
Lipsitch, M., T. Cohen, B. Cooper, J. M. Robins, S. Ma, L. James, G. Gopalakrishna, S. K. Chew, C. C. Tan, M. H. Samore, D. Fisman, and M. Murray. 2003. Transmission dynamics and control of severe acute respiratory syndrome. Science 300(5627):1966–1970.
Lloyd-Smith, J. O., A. P. Galvani, and W. M. Getz. 2003. Curtailing transmission of severe acute respiratory syndrome within a community and its hospital. Proceedings of the Royal Society of London—Series B: Biological Sciences 270(1528):1979–1989.
Longini, I. M., Jr., A. Nizam, S. Xu, K. Ungchusak, W. Hanshaoworakul, D. A. Cummings, and M. E. Halloran. 2005. Containing pandemic influenza at the source. Science 309(5737):1083–1087.
Mesnard, A., and P. Seabright. 2009. Escaping epidemics through migration? Quarantine measures under incomplete information about infection risk. Journal of Public Economics 93(7):931–938.
Ngwa, G. A., and M. I. Teboh-Ewungkem. 2016. A mathematical model with quarantine states for the dynamics of Ebola virus disease in human populations. Computational and Mathematical Methods in Medicine 2016:9352725.
Nishiura, H., K. Patanarapelert, M. Sriprom, W. Sarakorn, S. Sriyab, and I. Ming Tang. 2004. Modeling potential responses to severe acute respiratory syndrome in Japan: The role of initial attack size, precaution, and quarantine. Journal of Epidemiology and Community Health 58(3):186–191.
Pandey, A., K. E. Atkins, J. Medlock, N. Wenzel, J. P. Townsend, J. E. Childs, T. G. Nyenswah, M. L. Ndeffo-Mbah, and A. P. Galvani. 2014. Strategies for containing Ebola in West Africa. Science 346(6212):991–995.
Perlroth, D. J., R. J. Glass, V. J. Davey, D. Cannon, A. M. Garber, and D. K. Owens. 2010. Health outcomes and costs of community mitigation strategies for an influenza pandemic in the United States. Clinical Infectious Diseases 50(2):165–174.
Roberts, M. G., M. Baker, L. C. Jennings, G. Sertsou, and N. Wilson. 2007. A model for the spread and control of pandemic influenza in an isolated geographical region. Journal of the Royal Society Interface 4(13):325–330.
Sang, Z., Z. Qiu, X. Yan, and Y. Zou. 2012. Assessing the effect of non-pharmaceutical interventions on containing an emerging disease. Mathematical Biosciences and Engineering 9(1):147–164.
Uribe-Sánchez, A., A. Savachkin, A. Santana, D. Prieto-Santa, and T. K. Das. 2011. A predictive decision-aid methodology for dynamic mitigation of influenza pandemics. Operations Research Spectrum 33(3):751–786.
Wu, J. T., S. Riley, C. Fraser, and G. M. Leung. 2006. Reducing the impact of the next influenza pandemic using household-based public health interventions. PLOS Medicine 3(9):e361.
Yan, X., Y. Zou, and J. Li. 2007. Optimal quarantine and isolation strategies in epidemics control. World Journal of Modelling and Simulation 3(3):202–211.
Yang, Y., P. M. Atkinson, and D. Ettema. 2011. Analysis of CDC social control measures using an agent-based simulation of an influenza epidemic in a city. BMC Infectious Diseases 11:199.
Zhang, Q., and D. Wang. 2015. Assessing the role of voluntary self-isolation in the control of pandemic influenza using a household epidemic model. International Journal of Environmental Research and Public Health [Electronic Resource] 12(8):9750–9767.
Qualitative Studies
Baum, N. M., P. D. Jacobson, and S. D. Goold. 2009. “Listen to the people”: Public deliberation about social distancing measures in a pandemic. American Journal of Bioethics 9(11):4–14.
Beaton, R., A. Stergachis, J. Thompson, C. Osaki, C. Johnson, S. J. Charvat, and N. Marsden-Haug. 2007. Pandemic policy and planning considerations for universities: Findings from a tabletop exercise. Biosecurity and Bioterrorism 5(4):327–334.
Bell, D. M., and WHO (World Health Organization Working Group on Prevention of International and Community Transmission of SARS). 2004. Public health interventions and SARS spread, 2003. Emerging Infectious Diseases 10(11):1900–1906.
Braunack-Mayer, A. J., J. M. Street, W. A. Rogers, R. Givney, J. R. Moss, J. E. Hiller, and Flu Views Team. 2010. Including the public in pandemic planning: A deliberative approach. BMC Public Health 10:501.
Cava, M. A., K. E. Fay, H. J. Beanlands, E. A. McCay, and R. Wignall. 2005a. The experience of quarantine for individuals affected by SARS in Toronto. Public Health Nursing 22(5):398–406.
Cava, M. A., K. E. Fay, H. J. Beanlands, E. A. McCay, and R. Wignall. 2005b. Risk perception and compliance with quarantine during the SARS outbreak. Journal of Nursing Scholarship 37(4):343–347.
Charania, N. A., and L. J. Tsuji. 2013. Assessing the effectiveness and feasibility of implementing mitigation measures for an influenza pandemic in remote and isolated first nations communities: A qualitative community-based participatory research approach. Rural and Remote Health 13(4):2566.
Desclaux, A., D. Badji, A. G. Ndione, and K. Sow. 2017. Accepted monitoring or endured quarantine? Ebola contacts’ perceptions in Senegal. Social Science and Medicine 178:38–45.
DiGiovanni, C., J. Conley, D. Chiu, and J. Zaborski. 2004. Factors influencing compliance with quarantine in Toronto during the 2003 SARS outbreak. Biosecurity and Bioterrorism 2(4):265–272.
Leung, C. S., M. M. Ho, A. Kiss, A. V. Gundlapalli, and S. W. Hwang. 2008. Homelessness and the response to emerging infectious disease outbreaks: Lessons from SARS. Journal of Urban Health 85(3):402–410.
Lin, E. C., Y. C. Peng, and J. C. Tsai. 2010. Lessons learned from the anti-SARS quarantine experience in a hospital-based fever screening station in Taiwan. American Journal of Infection Control 38(4):302–307.
Maunder, R., J. Hunter, L. Vincent, J. Bennett, N. Peladeau, M. Leszcz, J. Sadavoy, L. M. Verhaeghe, R. Steinberg, and T. Mazzulli. 2003. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. Canadian Medical Association Journal 168(10):1245–1251.
Pellecchia, U., R. Crestani, T. Decroo, R. Van den Bergh, and Y. Al-Kourdi. 2015. Social consequences of Ebola containment measures in Liberia. PLOS ONE 10(12):e0143036.
Robertson, E., K. Hershenfield, S. L. Grace, and D. E. Stewart. 2004. The psychosocial effects of being quarantined following exposure to SARS: A qualitative study of Toronto health care workers. Canadian Journal of Psychiatry 49(6):403–407.
Schemm Dwyer, K., H. Misner, S. Chang, and N. Fajardo. 2017. An interim examination of the U.S. public health response to Ebola. Health Security 15(5):527–538.
Sell, T. K., M. P. Shearer, D. Meyer, H. Chandler, M. Schoch-Spana, E. Thomas, D. A. Rose, E. G. Carbone, and E. Toner. 2018. Public health resilience checklist for high-consequence infectious diseases—Informed by the domestic Ebola response in the United States. Journal of Public Health Management and Practice 24(6):510–518.
Smith, M. J., C. M. Bensimon, D. F. Perez, S. S. Sahni, and R. E. G. Upshur. 2012. Restrictive measures in an influenza pandemic: A qualitative study of public perspectives. Canadian Journal of Public Health 103(5):348–352.
Descriptive Survey Studies
Bauerle Bass, S., S. Burt Ruzek, L. Ward, T. F. Gordon, A. Hanlon, A. J. Hausman, and M. Hagen. 2010. If you ask them, will they come? Predictors of quarantine compliance during a hypothetical avian influenza pandemic: Results from a statewide survey. Disaster Medicine and Public Health Preparedness 4(2):135–144.
Blake, K. D., R. J. Blendon, and K. Viswanath. 2010. Employment and compliance with pandemic influenza mitigation recommendations. Emerging Infectious Diseases 16(2):212–218.
Blendon, R. J., C. M. DesRoches, M. S. Cetron, J. M. Benson, T. Meinhardt, and W. Pollard. 2006. Attitudes toward the use of quarantine in a public health emergency in four countries. Health Affairs 25(2):w15–w25.
Eastwood, K., D. Durrheim, J. L. Francis, E. T. d’Espaignet, S. Duncan, F. Islam, and R. Speare. 2009. Knowledge about pandemic influenza and compliance with containment measures among Australians. Bulletin of the World Health Organization 87(8):588–594.
Eastwood, K., D. N. Durrheim, M. Butler, and A. Jon. 2010. Responses to pandemic (H1N1) 2009, Australia. Emerging Infectious Diseases 16(8):1211–1216.
Katz, R., A. Vaught, and S. J. Simmens. 2019. Local decision making for implementing social distancing in response to outbreaks. Public Health Reports 134(2):150–154.
Kelly, B., L. Squiers, C. Bann, A. Stine, H. Hansen, and M. Lynch. 2015. Perceptions and plans for prevention of Ebola: Results from a national survey. BMC Public Health 15:1136.
Porten, K., D. Faensen, and G. Krause. 2006. SARS outbreak in Germany 2003: Workload of local health departments and their compliance in quarantine measures—Implications for outbreak modeling and surge capacity? Journal of Public Health Management and Practice 12(3):242–247.
Seale, H., M. L. McLaws, A. E. Heywood, K. F. Ward, C. P. Lowbridge, D. Van, J. Gralton, and C. R. MacIntyre. 2009. The community’s attitude towards swine flu and pandemic influenza. Medical Journal of Australia 191(5):267–269.
Taylor-Clark, K., R. J. Blendon, A. Zaslavsky, and J. Benson. 2005. Confidence in crisis? Understanding trust in government and public attitudes toward mandatory state health powers. Biosecurity and Bioterrorism 3(2):138–147.
Teh, B., K. Olsen, J. Black, A. C. Cheng, C. Aboltins, K. Bull, P. D. Johnson, M. L. Grayson, and J. Torresi. 2012. Impact of swine influenza and quarantine measures on patients and households during the H1N1/09 pandemic. Scandinavian Journal of Infectious Diseases 44(4):289–296.
Tracy, C. S., E. Rea, and R. E. Upshur. 2009. Public perceptions of quarantine: Community-based telephone survey following an infectious disease outbreak. BMC Public Health 9:470.
Wray, R. J., J. K. Harris, K. Jupka, S. Vijaykumar, E. W. Mitchell, W. Pollard, E. Zielinski-Gutierrez, D. Reissman, and K. Lubell. 2012. Individual and community influences on adherence to directives in the ecommmunvent of a plague attack: Survey results. Disaster Medicine and Public Health Preparedness 6(3):253–262.
Case Reports
Barbisch, D., K. L. Koenig, and F. Y. Shih. 2015. Is there a case for quarantine? Perspectives from SARS to Ebola. Disaster Medicine and Public Health Preparedness 9(5):547–553.
Binns, P. L., V. Sheppeard, and M. P. Staff. 2010. Isolation and quarantine during pandemic (H1N1) 2009 influenza in NSW: The operational experience of public health units. New South Wales Public Health Bulletin 21(1–2):10–15.
CDC (Centers for Disease Control and Prevention). 2003a. Efficiency of quarantine during an epidemic of severe acute respiratory syndrome—Beijing, China, 2003. Morbidity and Mortality Weekly Report 52(43):1037–1040.
CDC. 2003b. Use of quarantine to prevent transmission of severe acute respiratory syndrome—Taiwan, 2003. Morbidity and Mortality Weekly Report 52(29):680–683.
CDC. 2004. Postexposure prophylaxis, isolation, and quarantine to control an import-associated measles outbreak—Iowa, 2004. Morbidity and Mortality Weekly Report 53(41):969–971.
Chen, K. T., S. J. Twu, H. L. Chang, Y. C. Wu, C. T. Chen, T. H. Lin, S. J. Olsen, S. F. Dowell, I. J. Su, and S. R. T. Taiwan. 2005. SARS in Taiwan: An overview and lessons learned. International Journal of Infectious Diseases 9(2):77–85.
Chung, W. M., J. C. Smith, L. M. Weil, S. M. Hughes, S. N. Joyner, E. M. Hall, J. Ritch, D. Srinath, E. Goodman, M. S. Chevalier, L. Epstein, J. C. Hunter, A. J. Kallen, M. P. Karwowski, D. T. Kuhar, C. Smith, L. R. Petersen, B. E. Mahon, D. L. Lakey, and S. J. Schrag. 2015. Active tracing and monitoring of contacts associated with the first cluster of Ebola in the United States. Annals of Internal Medicine 163(3):164–173.
Collier, M. G., A. Cierzniewski, T. Duszynski, C. Munson, M. Wenger, B. Beard, R. Gentry, J. Duwve, P. K. Kutty, and P. Pontones. 2013. Measles outbreak associated with international travel, Indiana, 2011. Journal of the Pediatric Infectious Diseases Society 2(2):110–118.
DiGiovanni, C., N. Bowen, M. Ginsberg, and G. Giles. 2005. Quarantine stressing voluntary compliance. Emerging Infectious Diseases 11(11):1778–1779.
Ehlkes, L., M. George, G. Samosny, F. Burckhardt, M. Vogt, S. Bent, K. Jahn, and P. Zanger. 2017. Management of a Lassa fever outbreak, Rhineland-Palatinate, Germany, 2016. European Communicable Disease Bulletin 22(39).
Gahr, P., A. S. DeVries, G. Wallace, C. Miller, C. Kenyon, K. Sweet, K. Martin, K. White, E. Bagstad, C. Hooker, G. Krawczynski, D. Boxrud, G. Liu, P. Stinchfield, J. LeBlanc, C. Hickman, L. Bahta, A. Barskey, and R. Lynfield. 2014. An outbreak of measles in an undervaccinated community. Pediatrics 134(1):e220–e228.
Gastañaduy, P. A., J. Budd, N. Fisher, S. B. Redd, J. Fletcher, J. Miller, D. J. McFadden, 3rd, J. Rota, P. A. Rota, C. Hickman, B. Fowler, L. Tatham, G. S. Wallace, S. de Fijter, A. Parker Fiebelkorn, and M. DiOrio. 2016. A measles outbreak in an underimmunized Amish community in Ohio. New England Journal of Medicine 375(14):1343–1354.
Grigg, C., N. E. Waziri, A. T. Olayinka, J. F. Vertefeuille, and Centers for Disease Control and Prevention. 2015. Use of group quarantine in Ebola control—Nigeria, 2014. Morbidity and Mortality Weekly Report 64(5):124.
Nathawad, R., P. M. Roblin, D. Pruitt, and B. Arquilla. 2013. Addressing the gaps in preparation for quarantine. Prehospital and Disaster Medicine 28(2):132–138.
Nyenswah, T., D. J. Blackley, T. Freeman, K. A. Lindblade, S. K. Arzoaquoi, J. A. Mott, J. N. Williams, C. N. Halldin, F. Kollie, and A. S. Laney. 2015. Community quarantine to interrupt Ebola virus transmission—Mawah Village, Bong County, Liberia, August–October, 2014. Morbidity and Mortality Weekly Report 64(7):179–182.
Ooi, P. L., S. Lim, and S. K. Chew. 2005. Use of quarantine in the control of SARS in Singapore. American Journal of Infection Control 33(5):252–257.
Pang, X., Z. Zhu, F. Xu, J. Guo, X. Gong, D. Liu, Z. Liu, D. P. Chin, and D. R. Feikin. 2003. Evaluation of control measures implemented in the severe acute respiratory syndrome outbreak in Beijing, 2003. JAMA 290(24):3215–3221.
Plipat, T., R. Buathong, S. Wacharapluesadee, P. Siriarayapon, C. Pittayawonganon, C. Sangsajja, T. Kaewpom, S. Petcharat, T. Ponpinit, J. Jumpasri, Y. Joyjinda, A. Rodpan, S. Ghai, A. Jittmittraphap, S. Khongwichit, D. R. Smith, V. M. Corman, C. Drosten, and T. Hemachudha. 2017. Imported case of Middle East respiratory syndrome coronavirus (MERS-CoV) infection from Oman to Thailand, June 2015. European Communicable Disease Bulletin 22(33):17.
Reaves, E. J., L. G. Mabande, D. A. Thoroughman, M. A. Arwady, and J. M. Montgomery. 2014. Control of Ebola virus disease—Firestone District, Liberia, 2014. Morbidity and Mortality Weekly Report 63(42):959–965.
Smith, C. L., S. M. Hughes, M. P. Karwowski, M. S. Chevalier, E. Hall, S. N. Joyner, J. Ritch, J. C. Smith, L. M. Weil, W. M. Chung, S. Schrag, S. Santibanez, and Centers for Disease Control and Prevention. 2015. Addressing needs of contacts of Ebola patients during an investigation of an Ebola cluster in the United States—Dallas, Texas, 2014. Morbidity and Mortality Weekly Report 64(5):121–123.
Spengler, J. R., S. Stonecipher, C. McManus, H. Hughes-Garza, M. Dow, D. L. Zoran, W. Bissett, T. Beckham, D. A. Alves, M. Wolcott, S. Tostenson, B. Dorman, J. Jones, T. J. Sidwa, B. Knust, and C. B. Behravesh. 2015. Management of a pet dog after exposure to a human patient with Ebola virus disease. Journal of the American Veterinary Medical Association 247(5):531–538.
Svoboda, T., B. Henry, L. Shulman, E. Kennedy, E. Rea, W. Ng, T. Wallington, B. Yaffe, E. Gournis, E. Vicencio, S. Basrur, and R. H. Glazier. 2004. Public health measures to control the spread of the severe acute respiratory syndrome during the outbreak in Toronto. New England Journal of Medicine 350(23):2352–2361.
Tay, J., Y. F. Ng, J. Cutter, and L. James. 2010. Influenza A (H1N1-2009) pandemic in Singapore—Public health control measures implemented and lessons learnt. Annals of the Academy of Medicine Singapore 39(4):313–324.
Tsang, T., and T. H. Lam. 2003. SARS: Public health measures in Hong Kong. Respirology 8(Suppl):S46–S48.
Ward, K. A., P. Armstrong, J. M. McAnulty, J. M. Iwasenko, and D. E. Dwyer. 2010. Outbreaks of pandemic (H1N1) 2009 and seasonal influenza A (H3N2) on cruise ship. Emerging Infectious Diseases 16(11):1731–1737.
Yasuoka, A. 2009. Infection control of the H1N1 influenza in hospitals and local region. Respirology 3:A120.
Yoon, M. K., S. Y. Kim, H. S. Ko, and M. S. Lee. 2016. System effectiveness of detection, brief intervention and refer to treatment for the people with post-traumatic emotional distress by MERS: A case report of community-based proactive intervention in South Korea. International Journal of Mental Health Systems 10(1):51.
Zhang, Y., P. Yang, S. Liyanage, H. Seale, Y. Deng, X. Pang, L. Tian, B. Liu, L. Zhang, and Q. Wang. 2012. The characteristics of imported cases and the effectiveness of outbreak control strategies of pandemic influenza A (H1N1) in China. Asia-Pacific Journal of Public Health 24(6):932–939.
Mechanistic Evidence
Drews, K. 2013. A brief history of quarantine. The Virginia Tech Undergraduate Historical Review 2. http://doi.org/10.21061/vtuhr.v2i0.16.
Tognotti, E. 2013. Lessons from the history of quarantine, from plague to influenza A. Emerging Infectious Diseases 19(2):254–259. https://dx.doi.org/10.3201/eid1902.120312.
Ethics and Policy Text
IOM (Institute of Medicine). 2009. Guidance for establishing crisis standards of care for use in disaster situations: A letter report. Washington, DC: The National Academies Press
Jennings, B., and J. Arras. 2008. Ethical guidance for public health emergency preparedness and response: Highlighting ethics and values in a vital public health service. https://www.cdc.gov/od/science/integrity/phethics/docs/white_paper_final_for_website_2012_4_6_12_final_for_web_508_compliant.pdf (accessed February 23, 2020).
Jennings, B., J. D. Arras, D. H. Barrett, and B. A. Ellis. 2016. Emergency ethics: Public health preparedness and response. New York: Oxford University Press.
Mastroianni, A. C., J. P. Kahn, and N. E. Kass, eds. 2019. The Oxford handbook of public health ethics. New York: Oxford University Press. https://www.oxfordhandbooks.com/view/10.1093/oxfordhb/9780190245191.001.0001/oxfordhb-9780190245191 (accessed June 3, 2020).














































