
1
Introduction
Human exposure to lead can cause adverse effects in the nervous, cardiovascular, renal, hematologic, immunologic, and reproductive systems. Lead exposure is also known to induce adverse developmental effects in utero.
The primary route of lead exposure in the workplace is through the inhalation of airborne particles containing lead. Worker exposure can be measured by sampling the air concentration of lead within the workers’ breathing zone. In order to determine if workers inhale too much lead, industrial or occupational hygienists compare the measured worker exposures to an occupational exposure limit (OEL). The OEL is a general term for a maximum contaminant level in the workplace that is intended to limit exposure concentrations and protect worker health. (See Box 1-1.)
The Occupational Safety and Health Administration (OSHA) sets and enforces national standards for safety and health in the workplace. In carrying out its mission, OSHA sets 8-hour time-weighted-average (TWA) permissible exposure limits (PELs) as the highest concentration of a chemical to which a worker may be exposed (29 CFR 1910.1000).
In 1978, OSHA set the current PEL for airborne lead at 50 µg/m3 (29 CFR 1910.1025) based on an assessment of studies that reported adverse health effects at different blood lead levels (BLLs). OSHA considers an average BLL of 40 µg/dL to be the upper acceptable limit to protect workers from adverse health effects.
PREVIOUS NATIONAL ACADEMIES REPORT ON POTENTIAL HEALTH RISKS TO U.S. DEPARTMENT OF DEFENSE FIRING-RANGE PERSONNEL FROM RECURRENT LEAD EXPOSURE
During the decades since the OSHA PEL was set, reviews of the scientific literature reported substantial evidence of a diversity of health effects associated with BLLs at less than 40 μg/dL (e.g., EPA [2006] and NTP [2012]). In light of the relationships between lead exposure and adverse health effects, the U.S. Department of Defense (DoD) asked the National Academies to evaluate potential health risks to firing-range personnel from recurrent lead exposure and determine whether the current OSHA exposure standard for lead adequately protects DoD firing-range workers. The committee established by the National Academies in response to DoD’s request concluded that a BLL of less than 40 µg/dL (which is implicit in the OSHA standard) is not sufficiently protective of personnel who have repeated lead exposures on firing ranges (NRC 2013). That committee recommended that DoD review its guidelines and practices for protecting workers from lead exposure on firing ranges. That committee also recommended that DoD consider lowering the acceptable BLLs to more stringent levels that reduce the risk of adverse health effects in workers.
DOD’S INITIATIVE TO DEVELOP AIRBORNE LEAD OCCUPATIONAL EXPOSURE LIMITS
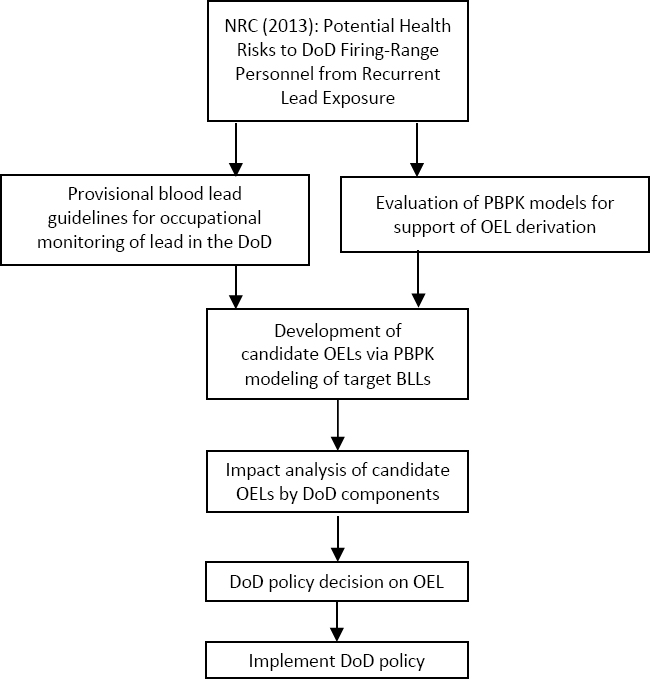
In response to that National Academies report, DoD pursued the development of lower allowable BLLs and lower OELs that would apply to all occupational exposures within DoD, not just firing ranges (Seibert 2019). DoD used a phased approach for developing an OEL for airborne lead (see Figure 1-1).
As described in Sweeney (2019), the approach comprised revising the risk management options for measured BLLs in DoD occupational settings, developing airborne exposure levels that would be predictive of BLLs of concern, analyzing impacts on DoD’s mission and costs associated with lowered BLLs, and selecting and implementing the OEL.
Based on its review of the literature on health effects at BLLs less than 40 µg/dL, a team assembled by the U.S. Army Public Health Command recommended replacing the OSHA BLL guidelines for worker removal and return to work with more stringent guidelines. The team also provided multiple management recommendations for various BLLs in the range of < 5 to > 80 μg/dl (USAPHC 2017).
As indicated in Figure 1-1, DoD’s approach for developing an OEL for airborne lead involved deriving airborne lead concentrations for BLLs of interest to DoD management. The airborne concentrations were estimated by using a biokinetic model (also referred to as a physiologically-based pharmacokinetic model).1 Biokinetic modeling provides a mathematical technique for estimating absorption, distribution, metabolism, and excretion of a chemical in humans. Such models can be used to relate the amount of lead exposure to the amount of lead found in the blood and other tissue at different points in time. The O’Flaherty biokinetic model was recommended for use in OEL development by DoD (Sweeney 2015). Sweeney (2019) describes, in general, how the O’Flaherty model was modified and presents the results of applying the DoDO’Flaherty model in support of developing a lead OEL for DoD workers.
COMMITTEE’S STATEMENT OF TASK FOR THE REVIEW OF THE DOD-O’FLAHERTY MODEL
DoD requested that a National Academies committee be established to evaluate whether the DoDO’Flaherty model used to derive airborne lead concentrations from BLLs, as described in Sweeney (2019), was appropriate (see Appendix A for the committee’s Statement of Task). The committee also was asked to consider whether an appropriate model was chosen, whether modifications to the model were appropriately justified, and whether the assumptions in and inputs to the model were reasonable. The committee was asked not to recommend specific OEL values.
As part of carrying out its task, the committee was asked to provide an overall summary conclusion on DoD’s selected approach and the application of the approach for derivation of lead OEL values. It also was asked to address the following specific topics:
- Were the DoD-O’Flaherty model selection, parameterization, and validation appropriate, given the intended purpose—to develop OELs for DoD civilian and military workers?
___________________
1 In this report, the terms physiologically-based pharmacokinetic model and biokinetic model are interchangeable.
- Were the inhalation rates used within the DoD-O’Flaherty model appropriate to represent DoD workers (military and civilian) who are occupationally exposed to lead?
- Were background levels of lead in air appropriately accounted for within the DoD-O’Flaherty model and representative of DoD workers who are occupationally exposed to lead?
- Is particle size variation appropriately accounted for within the DoD-O’Flaherty model and representative of lead absorption within the DoD workers (military and civilian) who are occupationally exposed to lead?
ORGANIZATION OF THE REPORT
In Chapter 2, the committee discusses the approach it used to address the elements of its task, as well as other relevant aspects. In doing so, the committee presents considerations for determining the appropriateness of DoD’s selected approach and the application of that approach for derivation of airborne concentrations from BLLs. Chapter 3 presents the committee’s evaluation of the specific items listed in its Statement of Task and other relevant aspects. The chapter also provides conclusions and recommendations stemming from the committee’s evaluations.



