
6
Bioavailability of Compounded Bioidentical Hormone Therapy Preparations
There is little published information on the bioavailability and pharmacokinetics of compounded bioidentical hormone therapy (cBHT) preparations.1,2 The lack of data results largely from the fact that compounding pharmacies making cBHT preparations are not required to conduct clinical studies to determine the bioavailability of a finished preparation (FDA, 2016, 2017). Moreover, the sheer diversity and heterogeneity of cBHT preparations and pharmacy practices makes any comparative bioavailability studies difficult to conduct.3 While it is true that compounding provides alternate methods of drug delivery to fit patients’ unique health needs (U.S. Senate Special Committee on Aging, 2007), it is also important that when a cBHT preparation is delivered using a route of administration that differs from that of a U.S. Food and Drug Administration (FDA)-approved product with the same active pharmaceutical ingredient (API)—often the case with compounded preparations—its bioavailability, and ultimately its safety and efficacy, would be unknown.
In the absence of bioavailability data, there are important variables to consider, including, but not limited to, the particle size of the API, degree of mixing and type of mixing equipment used to make a given preparation, route of drug administration, and presence of other excipients (nonactive
___________________
1Bioavailability refers to the amount of administered drug or substance within the body that is free to have an active effect on biological targets.
2Pharmacokinetics is the study of the kinetics of drug absorption, distribution, metabolism, and elimination.
3 See Chapter 5 for a review of the various cBHT preparations.
ingredients in the preparation). These variables can each decrease or increase bioavailability of the API (Allen and Ansel, 2013; Khadka et al., 2014; Kuhl, 2005; Remington and Beringer, 2006).4 For example, while the APIs used in two cBHT preparations prepared at two different compounding pharmacies may be identical, the excipients in the two preparations can have differing physicochemical properties that can potentially affect the bioavailability of APIs in the two compounded preparations dispensed to patients (Allen and Ansel, 2013; Khadka et al., 2014; Remington and Beringer, 2006).
Conceivably, the results of one-off studies would not be that useful given the potentially small number of individuals who would receive any of the large number of different cBHT preparations. However, in the absence of bioavailability data, the specific effect of these variables on the safety and efficacy of the cBHT preparations is unknown. While the committee appreciates the potential of personalized medicine and what it can offer to patients, the balance of safety and effectiveness with personalized medicine is a balance that needs to be further explored.
MEASURING CONCENTRATIONS OF STEROID HORMONES
Current clinical guidance suggests there is insufficient evidence to support claims that multiple blood, serum, or saliva tests can be used to precisely individualize hormone therapy (e.g., ACOG, 2018; Endocrine
___________________
4 This report does not specifically address the role of protein binding and its effect on bioavailability of compounded preparations owing to lack of data. Also, the potential effect of body mass index (BMI) affecting steroidal hormone levels in postmenopausal women receiving compounded preparation is not addressed owing to lack of data.
Society, 2019; NAMS, 2020; Santoro et al., 2016).5 Because no studies have demonstrated that using hormone concentrations to guide treatment is effective or useful, the American College of Obstetricians and Gynecologists recommends using clinical symptoms to guide treatment (ACOG, 2018). Nonetheless, some prescribers of cBHT use hormone imbalance as a rationale and guide for treating the symptoms of menopause (NASEM, 2019a,b).6
Characterizing hormone imbalance typically involves measuring hormone concentration levels in saliva, plasma, serum, or urine, and patients interested in this approach can find websites offering hormone balance test kits. Patients collect samples of saliva and/or blood and mail them to a designated laboratory. These labs often use bioanalytical methodology that lacks the rigors of the validated bioanalytical methods required to analyze pharmacokinetic samples collected in FDA-approved clinical studies (Herold and Fitzgerald, 2003; Kane et al., 2007). In addition, differences in steroid hormone levels can depend on the matrix used to measure the hormone concentration. One study, for example, examined the distribution of progesterone in venous whole blood, venous serum, fingertip capillary blood, and saliva after topical application of either cream or gel formulations compounded at a local pharmacy (Du et al., 2013). After topical administration of progesterone, saliva and capillary blood levels were 10-fold and 100-fold greater, respectively, than those seen in serum or whole blood. The investigators who conducted this study concluded that relying on serum levels of progesterone for monitoring topical administration of progesterone could lead to underestimation of tissue levels and consequent overdose.
Furthermore, in 2007, the Centers for Disease Control and Prevention (CDC) launched a project focused on standardizing hormone measurement (Vesper et al., 2008). In the project communication materials, CDC states
Despite physician’s wide spread use of hormone test results, the laboratory measurement of steroid hormones is subject to extreme variability especially when hormones are present in low concentrations, as is usually the case for testosterone in women and children, and for estradiol in men, children, and postmenopausal women. (CDC, 2008)
___________________
5 As an example, the North American Menopause Society states that hormone concentrations are not required to determine whether a woman has the “right amount” of hormones, since the optimal hormone concentrations in postmenopausal women have not, in fact, been established (NAMS, 2020).
6 More information is available at https://www.ucihealth.org/blog/2019/03/bioidentical-hormone-therapy (accessed October 23, 2019).
Measuring Hormone Concentrations: Salivary Testing
Salivary testing is often promoted by online analytical laboratories as a convenient, noninvasive method for hormone sampling. At the same time, several professional medical societies have issued public statements that saliva testing is unnecessary and has not been proven to be accurate nor reliable, mainly because the variation in the day-to-day or within-a-day hormone concentrations in an individual is large enough to make any one measurement uninformative (ACOG, 2018; Endocrine Society, 2019; Goodman et al., 2011; NAMS, 2017). In one study, for example, researchers compared salivary versus serum testosterone concentrations in postmenopausal women receiving transdermal testosterone supplementation (Flyckt et al., 2009). The data suggested there was no correlation between salivary testosterone and any of the serum testosterone measurements (see Figure 6-1), leading the researchers to conclude that the results

SOURCE: Flyckt et al., 2009.
did not support the routine use of salivary testosterone concentrations in postmenopausal women.
While the bioanalytical method used in the comparative analysis in Figure 6-1 is a validated radioimmunoassay (Flyckt et al., 2009),7 there have been specific concerns over the accuracy and reliability of immunoassays to assess testosterone measurements (Cao et al., 2007; Davis et al., 2019). A recent consensus position statement from several medical associations on the use of testosterone therapy in women stated that direct assays for the measurement of total and free testosterone are highly unreliable (Davis et al., 2019). Concerns regarding immunoassay assessments of steroid hormones are the result, in part, of a lack of immunospecificity caused by cross-reactivity with other steroids having a similar structure; poorly optimized quantification; and improper validation against standards (Clifton et al., 2016; Holst et al., 2004; Keevil et al., 2014). Recently, several authors have demonstrated that liquid chromatography–tandem mass spectrometry (LC-MS/MS) methodology can reliably and accurately measure testosterone levels in both male and female saliva samples (Clifton et al., 2016; Keevil et al., 2014), highlighting potential benefits in its use in cBHT research. (See the section “Bioanalytical Methods to Measure the Bioavailability of Steroid Hormones” in this chapter for an additional discussion on this topic.)
Measuring Hormone Concentrations: Urine Testing
Physicians who prescribe cBHT may also advocate for the use of urine testing to measure hormone levels. At the committee’s open session in May 2019, invited speakers Lyn Hogrefe, M.S., and David Rosensweet, M.D., noted that they prefer urine hormone testing because it is easier for patients and less expensive than other forms of testing (NASEM, 2019a,b). Advocates for this approach also claim that urine testing allows them to evaluate safety through measuring hormone metabolites, and that urine sampling provides a measure of free, “bioavailable” hormones. Importantly, while hormone level testing at clinical labs, for the purpose of checking normal values, may serve a clinical purpose, this type of testing stands as a distinct issue from that of testing for the bioavailability of a compounded preparation, which is lacking.
___________________
7 Reports that include serum concentrations of steroid hormone in cBHT preparations often use radioimmunoassays/immunochemiluminometric assay methods to measure steroid hormone concentrations (Glaser et al., 2013; Miller et al., 2000; Wren et al., 2003b).
Measuring Hormone Concentrations: FDA Requirements for FDA-Approved Hormone Products
As a comparison to the various protocols described above, FDA requires the measurement of steroid hormones in plasma or serum in bioequivalence studies with pharmacokinetic endpoints (FDA, 2019a). For example, FDA guidance on measuring estradiol in bioequivalence studies of estradiol vaginal tablets, gels, or creams identifies “estradiol in plasma” as the appropriate biological fluid to measure estradiol (FDA, 2011a, 2014, 2019a). Similar FDA guidance specifies plasma or serum as the appropriate biological fluid for measuring the levels of other steroid hormones, such as progesterone and testosterone, in clinical studies with pharmacokinetic endpoints (FDA, 2011b, 2019b).
BIOANALYTICAL METHODS TO MEASURE THE BIOAVAILABILITY OF STEROID HORMONES
LC-MS/MS is the gold standard methodology used today to support clinical studies with pharmacokinetic endpoints (FDA, 2018). LC-MS/MS is typically used because of the selectivity and specificity of the detection methodology, a requirement of validated bioanalytical methods. Examples of commercially available validated LC-MS/MS bioanalytical assays exist for many of the bioidentical hormones on the market today (see Table 6-1).
Recently, investigators evaluated urinary estrogen and progesterone metabolites using dried filter paper samples and gas chromatography with tandem mass spectrometry (Newman et al., 2019). This prospective observational study compared the results of urine and serum analyses. A secondary aim of the study compared results from dried urine samples collected at four times over a 10- to 14-hour time period (the 4-spot method) and the 24-hour collection method, which collects liquid urine samples over a full 24-hour period. Researchers obtained similar results from the 4-spot dried urine and the 24-hour liquid urine collection methods. Furthermore, based on the results of a comparison between dried urine and serum assays, the authors concluded that the dried urine assay may be a good surrogate for serum testing in clinical assessments of hormone disorders.
| Study | Analyte | Bioanalytical Method | Lower Limit of Quantitation |
|---|---|---|---|
| Pickar et al., 2015 | Unconjugated estradiol | HPLC–tandem mass spectrometry | 25.3 pg/mL |
| Unconjugated estrone | HPLC–tandem mass spectrometry | 5 pg/mL | |
| Total estrone | HPLC–tandem mass spectrometry | 0.1 ng/mL | |
| Progesterone | HPLC–tandem mass spectrometry | 0.4 ng/mL | |
| Singh et al., 2006 | Total testosterone | HPLC–tandem mass spectrometry | 0.5 ng/dL |
| Sood et al., 2013 | Estradiol | High-performance liquid chromatography (HPLC)–tandem mass spectrometry | 2.5 pg/mL |
| Estrone | HPLC–tandem mass spectrometry | 2.5 pg/mL | |
| Estriol | Competitive binding immunoenzymatic assay | 0.07 ng/mL | |
| Progesterone | Competitive binding immunoenzymatic assay | 0.08 ng/mL |
SOURCES: Pickar et al., 2015; Singh et al., 2006; Sood et al., 2013.
BIOAVAILABILITY OF COMPOUNDED BIOIDENTICAL HORMONE THERAPY PREPARATIONS
From the limited bioavailability data on cBHT preparations that exist in the literature, the following four studies on compounded estrogen cream, testosterone pellets, progesterone cream, and a lozenge containing estradiol, progesterone, testosterone, and dehydroepiandrosterone (DHEA) serve as examples of how such studies are conducted.
Example Study 1: Compounded Estrogen Cream
Study Design and Results
One group of investigators (Sood et al., 2013) conducted a pharmacokinetic evaluation of cBHT preparations as part of a randomized, blinded, four-arm, 16-day clinical trial of 40 postmenopausal women. The study arms assigned women to receive a compounded cream containing a commonly used 80:20 ratio of estriol and estradiol (Bi-est) and 100 mg of compounded oral progesterone or a conventional estradiol patch (Vivelle-Dot 0.05 mg) and oral progesterone capsule (Prometrium 100 mg). The Bi-est creams were compounded to include a dosage of 2.0 mg (1.6 mg estriol/0.4 mg estradiol),
2.5 mg (2 mg estriol/0.5 mg estradiol), or 3.0 mg (2.4 mg estriol/0.6 mg estradiol).
The investigators measured serum concentrations of estradiol, estrone, estriol, and progesterone, and generated a 24-hour pharmacokinetic profile after the first and last application of the cream or patch. The resulting analysis showed that estradiol exposure at steady-state—as determined after the last application—for all strengths of the compounded cream was less than that from the patch, though hormone levels for test subjects who received 3.0 mg of the compounded Bi-est preparation were not statistically different from those who received the patch (see Figure 6-2). The American Medical Association commented on this study, concluding that given the unpredictable pharmacokinetics of compounded formulations, the use of cBHT cannot be supported in comparison to well-tested FDA-approved hormone therapy options (AMA, 2016).
Study Limitations
In this study, participants who received one of the compounded estrogen preparations using the Bi-est ratio had wide fluctuations in their estradiol concentrations both after the initial administration as well as at steady-state. In contrast, estradiol absorption with the patch was more consistent across subjects. Participants receiving one of the three compounded dosage formulations based on the Bi-est 80:20 ratio had lower estrone concentrations than those from the patch. There were certain limitations with
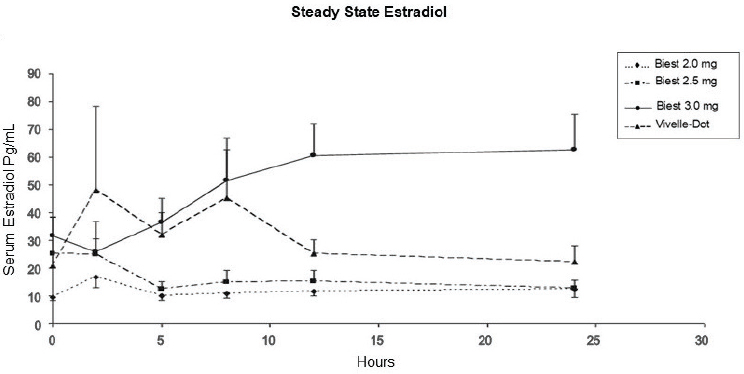
NOTE: Serum estradiol (pg/mL) as a function of time in hours (measured on days 15 and 16).
SOURCE: Sood et al., 2013.
the assay for measuring estriol, and as a result most subjects had estriol concentrations that were below the lower limit of detection. Progesterone concentrations were relatively similar after administration of the compounded and conventional bioidentical progesterone dosage forms in all four groups, suggesting that micronized progesterone is similarly absorbed across compounded and conventional dosage forms (Sood et al., 2013). However, the most informative bioavailability comparisons are those conducted between identical dosage forms, so a more appropriate reference in the study would have been an FDA-approved hormone product such as estradiol cream, estradiol gel, or estradiol spray products.
Another limitation of the study was the small number of subjects—between 7 and 10—in comparative arms of the study. Furthermore, given that Vanicream was used as the base for all three compounded estrogen formulations, the study results are not generalizable to all possible dosage formulations using the 80:20 Bi-est ratio. Variations in the content uniformity of estradiol and progesterone in compounded combined forms of oral capsule and transdermal cream preparations sourced from different compounding pharmacies is a concern among some professional medical associations (Davis et al., 2014; Stanczyk et al., 2019).
Regardless of the limitations of the study, the low and variable concentrations of serum estradiol obtained with the 2.0 and 2.5 mg Bi-est preparations in this study are concerning and cast doubts on the ability of compounded creams to provide relief of vasomotor symptoms and protect against bone loss. One case, for example, found that a patient treated for vasomotor symptoms with a dosage formulation using the Tri-est ratio (80 percent estriol, 10 percent estrone, and 10 percent estradiol) for several months experienced an initial relief of symptoms that returned even after increasing the dose (Davis et al., 2014). The patient’s symptoms later improved after the prescribing physician switched the patient to an FDA-approved estradiol transdermal delivery system.
Example Study 2: Compounded Testosterone Subcutaneous Pellet
Study Design and Results
Investigators (Glaser et al., 2013) conducted a pharmacokinetic study in 12 previously untreated postmenopausal women who each received 100 mg testosterone as a subcutaneous implant compounded by a local pharmacy in Cincinnati, Ohio. The research team measured serum total testosterone at baseline, 4 weeks, and 16 weeks following the testosterone pellet implantation. Total testosterone was measured by an immunoassay (Bayer Advia Centaur), and for comparison a duplicate specimen was sent to a second lab for measurement by liquid chromatography. There were significant
interindividual variability in testosterone concentrations at week 4, mean serum level was 190.8 ± 80 ng/dL (range 83–368 ng/dL, CV 41.9 percent) (see Figure 6-3) and week 16 (CV 41.6 percent). These levels exceed the serum total testosterone reference range of 8–60 ng/dL in women (Mayo Clinic Laboratories, 2020).
The authors stated that the concept of using a single serum testosterone concentration measurement to guide therapy is inherently unreliable, extremely variable, and ignores the complexity of the physiologic events that controls hormone production and release. Instead, the authors concluded, safety, tolerability, and clinical response should guide therapy (Glaser et al., 2013).
Considerations Related to the Use of Compounded Testosterone
In contrast to the conclusions reached by Glaser et al. (2013), a 2019 global consensus position statement, endorsed by multiple professional medical societies, recommended against the use of compounded testosterone in women (Davis et al., 2019). The report states that “blood total testosterone level should not be used to diagnose hypoactive sexual desire disorder/dysfunction.” The report recommended that treatment should be with formulations that achieve blood concentration of testosterone that approximate premenopausal physiological concentrations (Davis et al., 2019).
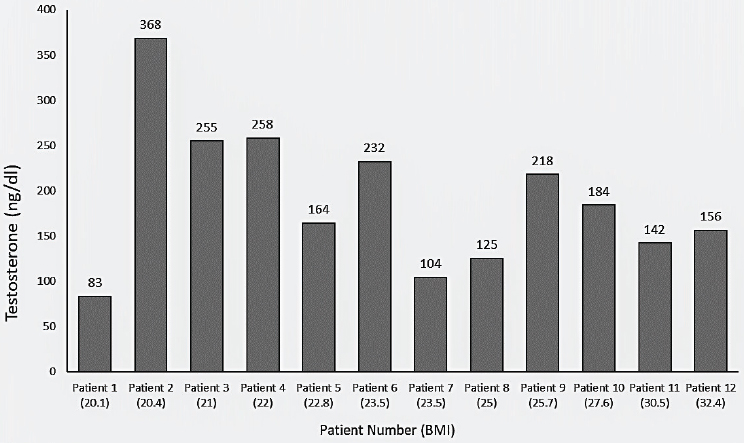
SOURCE: Glaser et al., 2013.
The potential differences in the use of testosterone in therapeutic treatment plans for women versus men is another consideration regarding compounded testosterone. In women, measurement of serum total testosterone is used only to exclude high baseline or supraphysiological concentrations (Davis et al., 2019). In men with hypogonadism, however, measuring total testosterone during hormone therapy in conjunction with symptoms relief is part of the treatment plan (Bhasin et al., 2018).
Researchers have also expressed concerns regarding the quality control of compounded testosterone preparations, in terms of a lack of uniformity in testosterone content and its potential to compromise the safety and efficacy of treatment (Grober et al., 2015). One study tested 7 gel testosterone preparations and 3 cream testosterone preparations from 10 compounding pharmacies within the Toronto, Canada, area. Results showed significant variability both within and between pharmacies in terms of the measured concentrations of testosterone in the finished compounded preparations (Grober et al., 2015).
Finally, to serve as a potential reference point, transdermal testosterone cream is available as a traditionally manufactured product in Australia, 1 percent Androfeme (Lawley Pharmaceuticals, 2016), and has publicly available bioavailability data to consider. The steady-state pharmacokinetics of Androfeme was investigated after daily application for 21 days in healthy postmenopausal women (Fooladi et al., 2015). Serum total testosterone, free testosterone, sex hormone binding globulin, and metabolic concentrations were measured using LC-MS/MS. On day 22, 5 mg testosterone cream restored both total and free testosterone levels to levels above and within the reference range, respectively, for premenopausal women.
Example Study 3: Compounded Progesterone Cream
Study Design and Results
A randomized, crossover clinical trial was conducted in 10 postmenopausal women to investigate the bioavailability of 80 mg of progesterone from compounded cream or gel applied daily to the inner thigh for 14 days (Du et al., 2013). Metered doses of compounded progesterone cream or gel were prepared by a compounding pharmacy, and on day 14 of the study, the investigators collected serial venous blood, fingertip capillary blood drawn just prior to drug application, and saliva samples up to 24 hours after the final application. The analysis was conducted using chromatographic purification followed by radioimmunoassay. Bioavailability data (see Table 6-2) showed that topical application of progesterone produced saliva and capillary blood concentrations that were approximately 10-fold and 100-fold greater, respectively, than those seen in serum or
| Cream | Gel | Cream/Gel Paired Differencea | ||||||
|---|---|---|---|---|---|---|---|---|
| Median | 25% Percentile | 75% Percentile | Median | 25% Percentile | 75% Percentile | Median | P | |
| Serum (n = 8) | ||||||||
| Cmax, ng/mL | 0.71 | 0.53 | 1.42 | 0.59 | 0.42 | 0.93 | 0.331 | 0.0781 |
| Tmax, ng/mL | 9.00 | 5.00 | 14.00 | 8.00 | 3.50 | 10.00 | 1.00 | 0.6250 |
| AUC0–24 h, ng h mL–1 | 12.39 | 10.31 | 19.68 | 8.32 | 6.92 | 12.98 | 5.00 | 0.0391 |
| Whole blood (n = 8) | ||||||||
| Cmax, ng/mL | 0.57 | 0.38 | 0.96 | 0.29 | 0.22 | 0.52 | 0.306 | 0.0391 |
| Tmax, ng/mL | 8.00 | 5.00 | 16.00 | 7.00 | 3.00 | 10.00 | 1.50 | 0.2969 |
| AUC0–24 h, ng h mL–1 | 7.51 | 6.40 | 13.07 | 4.41 | 3.66 | 7.19 | 3.88 | 0.0156 |
| Saliva (n = 7) | ||||||||
| Cmax, ng/mL | 8.71 | 4.13 | 12.07 | 7.36 | 2.42 | 8.14 | 2.63 | 0.4688 |
| Tmax, ng/mL | 1.00 | 1.00 | 2.00 | 6.00 | 3.00 | 8.00 | –4.00 | 0.0938 |
| AUC0–24 h, ng h mL–1 | 39.02 | 23.64 | 51.78 | 58.37 | 14.66 | 73.86 | –11.97 | 0.6875 |
| Capillary (n = 7) | ||||||||
| Cmax, ng/mL | 65.10 | 61.60 | 95.60 | 58.70 | 28.70 | 84.40 | 11.20 | 0.8125 |
| Tmax, ng/mL | 8.00 | 1.00 | 24.00 | 8.00 | 4.00 | 12.00 | 2.00 | 0.4688 |
| AUC0–24 h, ng h mL–1 | 1,056 | 585 | 1,260 | 999 | 219 | 1,250 | 260 | 0.6875 |
a Values in bold show significant difference.
SOURCE: Du et al., 2013.
whole blood. It is unclear why there were large differences between whole blood and capillary blood progesterone concentrations. The high capillary blood and saliva concentrations may suggest optimal absorption and transport of progesterone to tissues from both compounded topical preparations (Du et al., 2013).
Considerations
Other researchers have commented on the disparity between progesterone concentrations in saliva and capillary blood, as compared to serum or whole blood. Based on current evidence, the therapeutic significance of higher progesterone concentrations in saliva and capillary blood is unclear (Ruan and Mueck, 2014). The effectiveness of percutaneous progesterone delivery in protecting the endometrium from unopposed estrogen is in question, mostly because of the very low serum progesterone concentrations achieved via that route of administration (Du et al., 2013; Ruan and Mueck, 2014; Stanczyk, 2014; Whelan et al., 2013; Wren et al., 2005). In a review article (Fugh-Berman and Bythrow, 2007), the authors compared the serum and plasma progesterone levels from topical progesterone creams from several studies (Burry et al., 1999; Carey et al., 2000; Cooper et al., 1998; Lewis et al., 2002; O’Leary et al., 2000) and found it was less than 5 ng/mL, the minimum level believed to induce secretory endometrium. Based on these findings and others, researchers suggest that serum or plasma progesterone concentrations should not be used as an index of tissue exposure of progesterone following topical progesterone cream therapy (Stanczyk, 2014).
Example Study 4: Compounded Estradiol, Progesterone, Testosterone, and DHEA Lozenge
Study Design and Results
Investigators have evaluated the pharmacokinetics of compounded estradiol, progesterone, testosterone, and DHEA in an open-label study in six postmenopausal women following dosing with a lozenge using the transbuccal route of administration (Wren et al., 2003b). Each lozenge, formulated by a compounding pharmacy (Bondi Junction, Australia) as a single batch, contained 17β estradiol (0.5 mg), progesterone (200 mg), testosterone (2.0 mg), and DHEA (10 mg), along with several excipients. Subjects administered one-half of a lozenge twice daily for 2 weeks, and the researchers measured hormone plasma and saliva concentrations over a 12-hour interval. Plasma and saliva concentrations of hormones were measured using validated radioimmunoassays. Substantial intersubject
variability in all hormone plasma concentrations were observed. In addition, concentrations in saliva were highly variable, especially following the first single dose, with ratios of saliva/plasma concentration of estradiol of more than 1,000. Data showed that the hormones were rapidly absorbed via the buccal mucous membrane, and peak plasma concentration of estradiol and progesterone were similar to the concentrations typically found in menstruating women.
Considerations
While the transbuccal route is a novel approach for administering steroid hormones to postmenopausal women, Wren et al. (2003b) noted the need for safety and efficacy studies to support the use of that particular route of administration. An earlier report (Miller et al., 2000) showed that sublingual administration of micronized estradiol and progesterone, with and without micronized testosterone, favorably decreases serum and urine markers of bone metabolism and prevents bone loss. Of note, the study medication was prepared at a local pharmacy from a single batch to avoid variability in hormonal content and composition of the sublingual tablets.
BIOAVAILABILITY OF TRADITIONALLY MANUFACTURED BIOIDENTICAL HORMONE THERAPY PRODUCTS
As discussed in Chapter 8 of this report, patients may not be aware of or understand that FDA-approved bioidentical hormone therapy (BHT) products exist and are readily available. As more FDA-approved forms of BHT products become available, some patient concerns about conventional hormone therapy may be allayed, and other therapy options (e.g., nonhormonal or conventional BHT) may have greater appeal (L’Hermite, 2017; Thompson et al., 2017). To serve as a reference point for the example studies discussed above, the following sections provide examples of bioavailability studies for traditionally manufactured bioidentical hormone products.
Reference Study on the Bioavailability of Traditionally Manufactured Bioidentical Progesterone Cream
Researchers at the Royal Hospital for Women in Randwick, Australia (Wren et al., 2003a), conducted a parallel, double-blind, randomized, placebo-controlled trial comparing the efficacy of percutaneous progesterone cream with a placebo cream. Seventy-two postmenopausal women completed the evaluation for vasomotor symptoms, blood lipid levels, bone metabolite markers, and quality of life. Subjects received 32 mg of progesterone in a cream (ProFeme, manufactured by Lawley Pharmaceuticals, Perth,
Australia)8 or the same amount of cream containing no active ingredient. The cream was applied for a total of 12 weeks. While there was a significant increase in circulating serum progesterone by a median of 0.20 ng/mL, there was no detectable change in vasomotor symptoms, mood characteristics, sexual feelings, blood lipid levels, or bone metabolite markers.
Reference Study on the Bioavailability of FDA-Approved Bioidentical Estradiol and Progesterone Combination Product
On October 29, 2018, FDA-approved Bijuva (estradiol and progesterone) capsules, the first FDA-approved BHT combination of estradiol and progesterone in a single, oral capsule for the treatment of moderate to severe vasomotor symptoms associated with menopause in women with a uterus.9 As part of the approval process, the pharmacokinetics and oral bioavailability of a capsule combining 17β estradiol and progesterone was compared to those of widely used and approved separate formulations of estradiol and progesterone coadministered to healthy postmenopausal women (Pickar el al., 2015). Serial blood samples were collected, and the resulting plasma was used to measure unconjugated estradiol, total estrone, unconjugated estrone, and progesterone. Bioequivalence data supported the conclusion that the combination 17β estradiol and progesterone product demonstrated bioavailability similar to those of the respective reference products of estradiol and progesterone (Pickar et al., 2015).
CONCLUDING STATEMENTS
In summary, optimal bioavailability of an active ingredient in a compounded preparation is essential for exerting its intended pharmacological action. The paucity of bioavailability data from cBHT preparations is problematic and casts doubts on both safety and efficacy of these preparations. Even the small number of available clinical trials that attempted to evaluate bioavailability of cBHT lack the rigor of those conducted for FDA-approved BHT products.10 Most of the existing studies do not have an active control and thus lack meaningful comparative data. In addition, most existing studies relied on the use of radioimmunoassays or methods used at clinical labs that are not as selective and specific as LC-MS/MS bioanalytical methods.
___________________
8 Product information available at https://www.lawleybasecamp.com/media/pdf/pi-au/profeme-10-pi.pdf (accessed May 7, 2020).
9 Product information available at https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/210132s000lbl.pdf (accessed May 7, 2020).
10 As a resource for general considerations for bioavailability studies, see https://www.fda.gov/media/121311/download (accessed May 7, 2020).
REFERENCES
ACOG (American College of Obstetricians and Gynecologists). 2018. Committee opinion: Compounded bioidentical menopausal hormone therapy. Washington, DC: American College of Obstetricians and Gynecologists.
Allen, L. V., and H. C. Ansel. 2013. Ansel’s pharmaceutical dosage forms and drug delivery systems. 10th ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins.
AMA (American Medical Association). 2016. Hormone therapies: Off-label uses and unapproved formulations (resolution 512-a-15). Chicago, IL: American Medical Association.
Bhasin, S., J. P. Brito, G. R. Cunningham, F. J. Hayes, H. N. Hodis, A. M. Matsumoto, P. J. Snyder, R. S. Swerdloff, F. C. Wu, and M. A. Yialamas. 2018. Testosterone therapy in men with hypogonadism: An endocrine society clinical practice guide. Journal of Clinical Endocrinology & Metabolism 103(5):1715–1744.
Burry, K. A., P. E. Patton, and K. Hermsmeyer. 1999. Percutaneous absorption of progesterone in postmenopausal women treated with transdermal estrogen. American Journal of Obstetrics and Gynecology 180(6 Pt 1):1504–1511.
Cao, M., L. Shu, J. Li, J. Su, W. Zhang, Q. Wang, T. Guo, and Y. Ding. 2007. The expression of estrogen receptors and the effects of estrogen on human periodontal ligament cells. Methods and Findings in Experimental and Clinical Pharmacology 29(5):329–335.
Carey, B. J., A. H. Carey, S. Patel, G. Carter, and J. W. Studd. 2000. A study to evaluate serum and urinary hormone levels following short and long term administration of two regimens of progesterone cream in postmenopausal women. BJOG: An International Journal of Obstetrics and Gynaecology 107(6):722–726.
CDC (Centers for Disease Control and Prevention). 2008. Standardizing hormone measurements. Atlanta, GA: Centers for Disease Control and Prevention.
Clifton, S., W. Macdowall, A. J. Copas, C. Tanton, B. G. Keevil, D. M. Lee, K. R. Mitchell, N. Field, P. Sonnenberg, J. Bancroft, C. H. Mercer, A. M. Wallace, A. M. Johnson, K. Wellings, and F. C. W. Wu. 2016. Salivary testosterone levels and health status in men and women in the British general population: Findings from the Third National Survey of Sexual Attitudes and Lifestyles (NATSAL-3). The Journal of Clinical Endocrinology & Metabolism 101(11):3939–3951.
Cooper, A., C. Spencer, M. I. Whitehead, D. Ross, G. J. Barnard, and W. P. Collins. 1998. Systemic absorption of progesterone from Progest cream in postmenopausal women. Lancet (London, England) 351(9111):1255–1256.
Davis, R., P. Batur, and H. L. Thacker. 2014. Risks and effectiveness of compounded bioidentical hormone therapy: A case series. Journal of Women’s Health 23(8):642–648.
Davis, S. R., R. Baber, N. Panay, J. Bitzer, S. C. Perez, R. M. Islam, A. M. Kaunitz, S. A. Kingsberg, I. Lambrinoudaki, J. Liu, S. J. Parish, J. Pinkerton, J. Rymer, J. A. Simon, L. Vignozzi, and M. E. Wierman. 2019. Global consensus position statement on the use of testosterone therapy for women. The Journal of Clinical Endocrinology & Metabolism 104(10):4660–4666.
Du, J. Y., P. Sanchez, L. Kim, C. G. Azen, D. T. Zava, and F. Z. Stanczyk. 2013. Percutaneous progesterone delivery via cream or gel application in postmenopausal women: A randomized cross-over study of progesterone levels in serum, whole blood, saliva, and capillary blood. Menopause 20(11):1169–1175.
Endocrine Society. 2019. Position statement: Compounded bioidentical hormone therapy. Washington, DC: Endocrine Society.
FDA (U.S. Food and Drug Administration). 2011a. Draft guidance on estradiol: Vaginal tablet. Silver Spring, MD: U.S. Food and Drug Administration.
FDA. 2011b. Draft guidance on progesterone: Oral capsule. Silver Spring, MD: U.S. Food and Drug Administration.
FDA. 2014. Draft guidance on estradiol: Vaginal cream. Silver Spring, MD: U.S. Food and Drug Administration.
FDA. 2016. Pharmacy compounding of human drug products under Section 503A of the federal Food, Drug, and Cosmetic Act guidance. https://www.fda.gov/media/94393/download (accessed May 31, 2020).
FDA. 2017. FDA’s human drug compounding progress report: Three years after enactment of the Drug Quality and Security Act. https://www.fda.gov/drugs/human-drug-compounding/fdas-human-drug-compounding-progress-report-three-years-after-enactment-drug-quality-and-security (accessed June 9, 2020).
FDA. 2018. Bioanalytical method validation: Guidance for industry. Silver Spring, MD: U.S. Department of Health and Human Services.
FDA. 2019a. Draft guidance on estradiol: Transdermal gel. Silver Spring, MD: U.S. Food and Drug Administration.
FDA. 2019b. Draft guidance on testosterone: Transdermal extended release film. Silver Spring, MD: U.S. Food and Drug Administration.
Flyckt, R. L., J. Liu, H. Frasure, K. Wekselman, A. Buch, and S. A. Kingsberg. 2009. Comparison of salivary versus serum testosterone levels in postmenopausal women receiving transdermal testosterone supplementation versus placebo. Menopause 16(4):680–688.
Fooladi, E., S. E. Reuter, R. J. Bell, P. J. Robinson, and S. R. Davis. 2015. Pharmacokinetics of a transdermal testosterone cream in healthy postmenopausal women. Menopause 22(1):44–49.
Fugh-Berman, A., and J. Bythrow. 2007. Bioidentical hormones for menopausal hormone therapy: Variation on a theme. Journal of General Internal Medicine 22(7):1030–1034.
Glaser, R., S. Kalantaridou, and C. Dimitrakakis. 2013. Testosterone implants in women: Pharmacological dosing for physiologic effect. Maturitas 74(2013):179–184.
Goodman, N. F., R. H. Cobin, S. B. Ginzburg, I. A. Katz, and D. E. Woode. 2011. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the diagnosis and treatment of menopause. Endocrine Practice 17(Suppl 6):1–25.
Grober, E. D., A. Garbens, A. Bozovic, V. Kulasingam, M. Fanipour, and E. P. Diamandis. 2015. Accuracy of testosterone concentrations in compounded testosterone products. Journal of Sex Medicine 12:1381–1388.
Herold, D. A., and R. L. Fitzgerald. 2003. Immunoassays for testosterone in women: Better than a guess? Clinical Chemistry 49(8):1250–1251.
Holst, J. P., O. P. Soldin, T. Guo, and S. J. Soldin. 2004. Steroid hormones: Relevance and measurement in the clinical laboratory. Clinics in Laboratory Medicine 24(1):105–118.
Kane, J., J. Middle, and M. Cawood. 2007. Measurement of serum testosterone in women: What should we do? Annals of Clinical Biochemistry 44(Pt 1):5–15.
Keevil, B. G., P. MacDonald, W. Macdowall, D. M. Lee, F. C. W. Wu, and N. Team. 2014. Salivary testosterone measurement by liquid chromatography tandem mass spectrometry in adult males and females. Annals of Clinical Biochemistry 51(Pt 3):368–378.
Khadka, P., J. Ro, H. Kim, I. Kim, J. T. Kim, H. Kim, J. M. Cho, G. Yun, and J. Lee. 2014. Pharmaceutical particle technologies: An approach to improve drug solubility, dissolution and bioavailability. Asian Journal of Pharmaceutical Sciences 9(6):304–316.
Kuhl, H. 2005. Pharmacology of estrogens and progestogens: Influence of different routes of administration. Climacteric 8(Suppl 1):3–63.
Lawley Pharmaceuticals. 2016. Product label: Androfeme 1% cream. Western Australia: Lawley Pharmaceuticals.
Lewis, J. G., H. McGill, V. M. Patton, and P. A. Elder. 2002. Caution on the use of saliva measurements to monitor absorption of progesterone from transdermal creams in postmenopausal women. Maturitas 41(1):1–6.
L’Hermite, M. 2017. Bioidentical menopausal hormone therapy: Registered hormones (non-oral estradiol ± progesterone) are optimal. Climacteric 20(4):331–338.
Mayo Clinic Laboratories. 2020. Testosterone, total, bioavailable, and free, serum. Reference values. https://www.mayocliniclabs.com/test-catalog/Clinical+and+Interpretive/83686 (accessed May 7, 2020).
Miller, B. E., M. J. De Souza, K. Slade, and A. A. Luciano. 2000. Sublingual administration of micronized estradiol and progesterone, with and without micronized testosterone: Effect on biochemical markers of bone metabolism and bone mineral density. Menopause 7(5):318–326.
NAMS (North American Menopause Society). 2017. The 2017 hormone therapy position statement of the North American Menopause Society. Menopause 24(7):728–753.
NAMS. 2020. What is hormone testing? http://www.menopause.org/publications/clinical-practice-materials/bioidentical-hormone-therapy/what-is-hormone-testing (accessed March 10, 2020).
NASEM (National Academies of Sciences, Engineering, and Medicine). 2019a. Dr. Daved Rosensweet presentation to the Committee during the open session of Meeting Two. May 6, 2019 (available through the National Academies Public Access File).
NASEM. 2019b. Ms. Lyn Hogrefe presentation to the Committee during the open session of Meeting Two. May 6, 2019 (available through the National Academies Public Access File).
Newman, M., S. M. Pratt, D. A. Curran, and F. Z. Stanczyk. 2019. Evaluating urinary estrogen and progesterone metabolites using dried filter paper samples and gas chromatography with tandem mass spectrometry (GC-MS/MS). BMC Chemistry 13(1):20.
O’Leary, P., P. Feddema, K. Chan, M. Taranto, M. Smith, and S. Evans. 2000. Salivary, but not serum or urinary levels of progesterone are elevated after topical application of progesterone cream to pre- and postmenopausal women. Clinical Endocrinology 53(5):615–620.
Pickar, J. H., C. Bon, J. M. Amadio, S. Mirkin, and B. Bernick. 2015. Pharmacokinetics of the first combination 17β-estradiol/progesterone capsule in clinical development for menopausal hormone therapy. Menopause (New York) 22(12):1308–1316.
Remington, J. P., and P. Beringer. 2006. Remington: The science and practice of pharmacy. Philadelphia, PA: Lippincott Williams & Wilkins.
Ruan, X., and A. O. Mueck. 2014. Systemic progesterone therapy—oral, vaginal, injections and even transdermal? Maturitas 79(3):248–255.
Santoro, N., G. D. Braunstein, C. L. Butts, K. A. Martin, M. McDermott, and J. V. Pinkerton. 2016. Compounded bioidentical hormones in endocrinology practice: An Endocrine Society scientific statement. The Journal of Clinical Endocrinology & Metabolism 101(4):1318–1343.
Singh, A. B., M. L. Lee, I. Sinha-Hikim, M. Kushnir, W. Meikle, A. Rockwood, S. Afework, and S. Bhasin. 2006. Pharmacokinetics of a testosterone gel in healthy postmenopausal women. The Journal of Clinical Endocrinology & Metabolism 91(1):136–144.
Sood, R., R. A. Warndahl, D. R. Schroeder, R. J. Singh, D. J. Rhodes, D. Wahner-Roedler, R. S. Bahn, and L. T. Shuster. 2013. Bioidentical compounded hormones: A pharmacokinetic evaluation in a randomized clinical trial. Maturitas 74(4):375–382.
Stanczyk, F. Z. 2014. Treatment of postmenopausal women with topical progesterone creams and gels: Are they effective? Climacteric 17(Suppl 2):8–11.
Stanczyk, F. Z., C. Niu, C. Azen, S. Mirkin, and J. M. Amadio. 2019. Determination of estradiol and progesterone content in capsules and creams from compounding pharmacies. Menopause (New York) 26(9):966–971.
Thompson, J. J., C. Ritenbaugh, and M. Nichter. 2017. Why women choose compounded bioidentical hormone therapy: Lessons from a qualitative study of menopausal decision-making. BMC Women’s Health 17(1):97.
U.S. Senate Special Committee on Aging. 2007. Bioidentical hormones: Sound science or bad medicine. 110th Congress, 1st Session. April 19, 2007.
Vesper, H. W., J. C. Botelho, C. Shacklady, A. Smith, and G. L. Myers. 2008. CDC project on standardizing steroid hormone measurements. Steroids 73(13):1286–1292.
Whelan, A. M., T. M. Jurgens, and M. Trinacty. 2013. Bioidentical progesterone cream for menopause-related vasomotor symptoms: Is it effective? Annals of Pharmacotherapy 47(1):112–116.
Wren, B. G. 2005. Transdermal progesterone creams for postmenopausal women: More hype than hope? Medical Journal of Australia 182(5):237–239.
Wren, B. G., S. M. Champion, K. Willetts, R. Z. Manga, and J. A. Eden. 2003a. Transdermal progesterone and its effect on vasomotor symptoms, blood lipid levels, bone metabolic markers, moods, and quality of life for postmenopausal women. Menopause 10(1):13–18.
Wren, B. G., R. O. Day, A. J. McLachlan, and K. M. Williams. 2003b. Pharmacokinetics of estradiol, progesterone, testosterone and dehydroepiandrosterone after transbuccal administration to postmenopausal women. Climacteric 6(2):104–111.
This page intentionally left blank.




















