
1
Pathophysiology and Epidemiology of Stress Fractures in Military Women
ESSENTIAL CONCEPTS
A stress fracture is an overuse injury to bone that results from the accumulation of strain damage from repetitive load cycles much lower than the stress required to fracture the bone in a single-load cycle (Brukner and Bennell, 1997). Stress fractures are commonly associated with vigorous exercise, especially that involving repetitive, weight-bearing loads, like running or marching (Jones et al., 1989).
Although the term stress fracture implies a break in bone continuity, many injuries labeled as stress fractures are not associated with a fracture line on plain radiography (Jones et al., 1989). The normal reaction of bone to stress is a localized acceleration of bone remodeling that alters the micro-architectural configuration to better withstand the altered loading environment. Ordinarily this remodeling does not result in pathology, but repeated application of unaccustomed stress may increase the number of activated bone remodeling units. Because the resorption precedes the formation by several weeks in the remodeling process, a short-term loss of bone may result, which ranges from mild levels that do not significantly weaken the bone to levels that are sufficiently high to lead to complete bone failure or fracture (Jones et al., 1989). Because this process exists along a continuum, the clinical features also exist along a continuum from mild to severe.
The biologic adaptability of bone to repetitive strain is mediated by cells surrounded by a mineralized connective tissue matrix of collagen fibers and ground substance. Bone cells arise from different cell lines and carry out various functions including matrix formation, mineralization,
and resorption. Osteoblasts are derived from local bone marrow mesenchymal cells and are located on all bone surfaces where active bone formation is taking place (Cowin et al., 1991; Marks and Popoff, 1988). Their main function is to synthesize and secrete the organic matrix of bone. Once osteoblasts stop forming bone, they may either decrease their synthetic activity and remain on the surface of the bone where they are known as bone-lining cells, or they may surround themselves with matrix and become osteocytes. Bone-lining cells are elongated and contain fewer organelles than osteoblasts. The main role of these cells is to contract and secrete enzymes that remove the thin layer of osteoid covering the mineralized matrix. This allows osteoclasts to attach to bone and begin resorption (Buckwalter et al., 1996). Osteocytes comprise more than 90 percent of the bone cells in the mature human skeleton. They are connected to adjacent osteocytes, active osteoblasts, and bone lining cells by numerous cytoplasmic projections that travel in channels (canaliculi) through mineralized matrix (Boivin et al., 1990). These interconnections may allow the cells to sense deformation of bone by mechanical loads and to coordinate the remodeling process.
Osteoclasts are derived from extraskeletal, hematopoietic stem cells (Girasole et al., 1992). They are large, motile, multinucleated cells found on bone surfaces that are undergoing resorption. To resorb the bone matrix, osteoclasts bind to the bone surface and create an acidic environment by secreting proteins and enzymes (Peck and Woods, 1988).
The extracellular matrix of bone is comprised of both inorganic and organic components. The inorganic component contributes approximately 65 percent of the wet weight of bone and consists mainly of calcium and phosphate in crystals of hydroxyapatite (Boivin et al., 1990). Other ions within the bone matrix include carbonate, citrate, fluoride, and magnesium and chloride in much smaller quantities. The inorganic matrix of bone performs two essential functions: it serves as an ion reservoir, and it gives bone most of its strength and stiffness (Buckwalter et al., 1995). The organic components, comprising 20 percent of the wet weight of bone, are collagen fibrils and an interfibrillar ground substance composed of as many as 200 noncollagenous proteins including osteocalcin, osteonectin, osteopontin, and various glycoproteins. These organic constituents give bone its flexibility and resilience (Martin, 1991), and the matrix macromolecules appear to contribute to the structure and functional qualities of bone (Meghji, 1992). The majority of the organic matrix is produced by osteoblasts, the most abundant protein being type 1 collagen (Boivin et al., 1990). Collagen molecules are secreted as procollagen into the extracellular space. They are then assembled into fibrils that are arranged such that spaces exist between molecules to accommodate the calcium and phosphate crystals.
HORMONAL REGULATION OF BONE METABOLISM AND REMODELING
The dynamic processes involved in bone metabolism relate to the events associated with bone formation and bone resorption. The extent to which these two processes are in balance determines whether bone mass will be gained (in youth), conserved (in young adults), or lost (in middle-aged and older adults). As noted earlier, the cells involved in bone formation and bone resorption are the osteoblast and the osteoclast, respectively. Bone markers refer to biochemical moieties that result from the secretory products of these cells or from the formation or breakdown of type 1 collagen, the organic substrate upon which mineralization occurs.
A large number of modulators, including hormones, growth factors, and cytokines,1 interact at the level of the osteoblast, osteoclast, and other cells to regulate bone remodeling (Margolis et al., 1996). Systemic hormones that either regulate calcium balance or affect bone remodeling include parathyroid hormone, calcitonin, vitamin D, estrogen, progesterone, growth hormone (GH), thyroid hormone, glucocorticoids, and androgens.
Paracrine and autocrine factors involved in bone remodeling include IGF and cytokines such as tumor necrosis factor (TNF)-a, transforming growth factor (TGF)-b, and interleukins (IL). The sequence of molecular events in biochemical coupling of bone resorption to bone formation is not well understood but appears to involve the generation of classical messenger molecules, such as cyclic nucleotides and prostaglandins by load-sensing cells (Marcus, 1996).
In general, systemic endocrine modulators activate both resorption and formation of bone, while paracrine/autocrine factors have more specific effects (Rosen, 1997). Some growth factors are bound to the extracellular matrix in latent form prior to release and activation by other elements in the remodeling cascade. Binding proteins (particularly the IGF-binding proteins) and hormone receptors play critical roles in modulating the activity of hormones and growth factors. Thus, "hormonal and paracrine factors orchestrate a remodeling sequence that also requires a skeletal matrix loaded with inactive growth factors" (Rosen, 1997, p. 1194).
|
HORMONES THAT REGULATE CALCIUM BALANCE Parathyroid Hormone Parathyroid hormone (PTH) is an important hormone regulating bone mineral content (Margolis et al., 1996). PTH stimulates the reabsorption of calcium from the glomerular filtrate, enhances calcium resorption from bone, and increases absorption of calcium from the gastrointestinal tract, secondarily through its effect on renal formation of active vitamin D metabolites. Calcium concentration in the extracellular fluid is the major regulator of PTH secretion (stimulation at low calcium concentrations and inhibition at high calcium concentrations). PTH mobilizes calcium from areas of bone in rapid equilibration with the extracellular matrix and also increases the synthesis of bone enzymes that promote bone resorption and remodeling. Calcitonin Calcitonin is a hormone, produced by the parafollicular or C-cells of the thyroid gland, whose principal action is the lowering of serum calcium concentration (Aurbach et al., 1992). Its mechanism of action is through inhibition of bone resorption mediated by cyclic adenosine monophosphate (cAMP). |
|
Vitamin D Vitamin D (1,25 dihydroxyvitamin D3) is a key hormone in the regulation of intestinal calcium absorption; it increases the fractional absorption of calcium and, to a lesser extent, increases the absorption of phosphate and magnesium. Vitamin D also has a direct anabolic effect on bone cells (Aurbach et al., 1992). |
|
HORMONES THAT REGULATE BONE REMODELING Estrogen Estrogen appears to be the critical initiator of the pubertal growth spurt in boys and girls. Estrogen acts primarily, but not exclusively, as an antiresorptive agent on bone. Estrogens suppress osteoblast release of cytokines, which recruit osteoclasts for bone resorption. The cytokine IL-6 is upregulated in estrogen deficiency in most, but not all, studies, and may be responsible for enhanced bone resorption (Margolis et al., 1996). Estrogen deficiency is also accompanied by suppression of osteoblast production of fibronectin, a key element of the extracellular matrix that is important in the recruitment, differentiation, and subsequent function of preosteoblasts. Estrogen has pronounced antiresorptive effects and stimulates bone formation. Progesterone Considerably less is known regarding the action of progesterone on human bone. Progesterone appears to modulate bone resorption and protect against bone loss (Graham and Clarke, 1997). It has been postulated that progesterone antagonizes glucocorticoid-mediated bone loss through its ability to act as a ligand for the glucocorticoid receptor (Conover, 1996). Progesterone's effects on estrogen receptors are highly tissue specific, and more work is required to understand the interaction between estrogen and progesterone in human bone. Growth Hormone The growth-related effects of growth hormone are primarily mediated by insulin-like growth factor (IGF)-1, a member of the insulin-like gene family. Recent studies have shown that growth hormone and IGF-1 have synergistic effects on bone formation. The effects of IGF-1 are described further in the section on paracrine and autocrine factors. Thyroid Hormone Thyroid hormones interact with both nuclear and cell membrane receptors in bone and influence responses of bone cells (Stern, 1996). Thyroid hormone stimulates osteoblast activity, but also promotes resorption through activation of cytokine pathways that lead to osteoclast differentiation. Anabolic effects are more apparent in younger animals and children. Catabolic effects become more prominent at increasing doses. Exogenously administered thyroid hormones are known to increase the risk for bone loss. Estrogens and bisphosphonates can diminish thyroid hormone-stimulated bone loss. |
|
Glucocorticoids Direct effects of glucocorticoids on bone are apparent (Lukert and Kream, 1996). Glucocorticoid receptors have been identified on osteoblasts. At high concentrations, glucocorticoids decrease protein, RNA, and DNA synthesis in bone cells and inhibit COL1A1 gene expression, leading to reduced amounts of type I collagen for bone matrix formation. Glucocorticoids induce osteoporosis; with each remodeling cycle, less bone is replaced, resulting in defective bone formation. Glucocorticoids also exert multiple, indirect effects on bone (Lukert and Kream, 1996). They inhibit pituitary secretion of growth hormone (GH) and cause alterations in insulin-like growth factor (IGF)-binding proteins, leading to a fall in the biologic activity of growth factors with a loss of their anabolic effect on bone. Glucocorticoids also inhibit the secretion of gonadotropin, follicle-stimulating hormone/luteinizing hormone, adrenocorticotrophic hormone, estrogen, testosterone, dehydroepiandrosterone, and androstenedione. Glucocorticoids decrease the transport of calcium and phosphorus and increase the secretion and sensitivity to parathyroid hormone. Cortisol secreted by the adrenal gland in physiologic amounts is essential for differentiation and function of osteoblasts and osteoclasts (Lukert and Kream, 1996). However, supraphysiologic doses of cortisol inhibit bone formation, thus leading to net bone loss. Androgens Administration of androgens (testosterone and 5- |
|
PARACRINE AND AUTOCRINE FACTORS INVOLVED IN BONE REMODELING Insulin-Like Growth Factors Insulin-like growth factors (IGFs) play a key role in bone remodeling by facilitating recruitment of osteoblasts and osteoclasts. IGF-1 is produced in the liver in response to growth hormone (GH) and circulates in combination with IGF-2 and IGF-binding proteins. IGFs are also produced by the osteoblast and stored in latent form in the extracellular matrix. In fact, IGF-2 is the most abundant growth factor stored in human extracellular matrix (Conover, 1996). Other growth factors include transforming growth factor (TGF)-b, basic fibroblast growth factor, and platelet-derived growth factor, all of which can influence production of IGFs by osteoblast cells. While IGFs have some mitogenic effects, their primary action appears to be promotion of osteoblast activity. IGF-1 also stimulates osteoclast recruitment and inhibits collagenase activity (Rosen, 1997). Both IGF-1 and TGF-b are increased with mechanical loading. Most studies have demonstrated that subcutaneous administration of IGF-1 to animals stimulates linear growth and new bone formation (Rosen, 1997). Short-term treatment of postmenopausal women with IGF-1 results in increased bone turnover. Low-dose IGF-1 (15 mg/kg twice daily) has been shown to increase circulating levels of the markers of bone synthesis, without increasing the markers of bone resorption (Ghiron et al., 1995). No clinical trials with IGF-1 have been conducted in which bone density, fractures, or long-term safety with respect to apoptosis or neoplasms were the primary study outcomes. Further research is needed to establish the role of IGF-1 in treatment of low bone mass or fractures. |
|
The presence of estrogen stimulates GH secretion and potentiates the anabolic effect of GH by upregulating GH-receptors on the osteoblast (Slootweg et al., 1997). IGF-1 production is stimulated by estrogen in bone cell cultures and changes the IGF-binding proteins to increase the effective concentration of IGF-1 (Schmidt et al., 1996; Slootweg et al., 1997). Estrogen has also been reported to stimulate TGF-b, another anabolic agent in bone, and may increase extracellular matrix-bound growth factors (Margolis et al., 1996). Prostaglandins Cytokines, growth factors, and hormones, as well as mechanical loading, increase prostaglandin production in bone (Pilbeam et al., 1996). A recently identified enzyme, prostaglandin G/H synthase (PGHS-2), apparently mediates much of the prostaglandin production induced with bone remodeling. PGHS-2 is usually expressed at low levels but can be rapidly and transiently induced to very high levels by a number of factors including mechanical loading, interleukin (IL)-1, tumor necrosis factor (TNF)-a, and TGF-b. Prostaglandin production is also increased in bone by endothelial growth factor, platelet-derived growth factor, parathyroid hormone (PTH), and PTH-related protein, and to a lesser extent by vitamin D and thyroid hormone. Nonsteroidal anti-inflammatory drugs (NSAIDs), which inhibit prostaglandin synthesis, suppress new bone formation normally induced by mechanical loading (Pilbeam et al., 1996). Paradoxically, bone resorption induced by immobilization is also blunted by indomethacin or other NSAIDs. |
PATHOPHYSIOLOGY OF STRESS FRACTURES
Bone Loading
During physical activity, forces from ground impact and muscle contraction result in bone stress, defined as the load or force per unit area that develops on a plane surface, and bone strain, defined as the deformation or change in bone dimension. In clinical terms, stress is a measure of the load applied, and strain is a measure of the degree of lengthening or deformation that results. Repetitive strains are essential for the maintenance of normal bone mass. This fact is evident during situations of disuse, immobilization, and weightlessness where dramatic bone loss occurs. Physical activity can lead to increased bone mass as bone adapts to the additional loads placed upon it. However, bone can also lose strength as a result of repetitive loads imposed during normal daily activity if they are applied at too-frequent intervals (Martin and Burr, 1989). This loss of strength is attributed to the formation and propagation of microscopic cracks within bone. If the load is continually applied, these "microcracks" can spread and coalesce into "macrocracks." If repair does not occur, a stress fracture may eventually result.
During physical activity, contact with the ground generates forces within the body. With running, vertical ground reaction force has been shown to vary from 2 to 5 times body weight (Bates et al., 1983; Cavanagh and Lafortune, 1980), and during jumping and landing activities, ground reaction forces can reach 12 times body weight (Deporte and Van Gheluwe, 1989; McNitt-Gray, 1991; Ramey et al., 1985). Transient impulse forces associated with ground reaction forces are propagated upward from the foot, undergoing attenuation as they pass toward the head (Light et al., 1980; Wosk and Voloshin, 1981). A number of factors influence the magnitude, propagation, and attenuation of the impact forces. These include running speed (Frederick and Hagy, 1986; Frederick et
al., 1981; Hamill et al., 1983; Nigg et al., 1987), muscular fatigue (Dickinson et al., 1985), type of foot strike (Cavanagh and Lafortune, 1980; Oakley and Pratt, 1988), foot and ankle morphology, body weight (Frederick and Hagy, 1986; Hamill et al., 1983), training surface and terrain (Hamill et al., 1984, Nigg and Segesser, 1988), footwear and lower extremity alignment (Dufek and Bates, 1991).
Accelerated Remodeling
Cyclic loading creates bone stress through intermittent and repetitive skeletal muscle contraction and loading forces. Normal remodeling—the bone's response to cyclic loading due to ground reaction forces—is a sequential process of osteoclastic resorption and osteoblastic new bone formation. This process takes place continuously on both periosteal and endosteal surfaces within cortical bone and on the surface of trabeculae (Parfitt, 1984). The main functions of remodeling are to adapt bone to mechanical loading, to prevent the accumulation of microfractures or fatigue damage (Marcus, 1991; Parfitt, 1988), and to maintain blood calcium levels.
Repetitive loads to bone applied below the load required for single cycle failure (the load that would break bone with a single application) produce cumulative microdamage and initiate the process of accelerated remodeling. Microscopically, the first sign of accelerated remodeling is vascular congestion, thrombosis, and osteoclastic resorption. With continued loading, these signs progress to coalescence of resorbed cavities and then to microfractures with extension to the cortex. For this reason, the clinical response of bone to load can be seen along a continuum from accelerated remodeling to a complete fracture (Figure 1-1). Training influences bone loading and is itself affected by four factors. The volume of training is a function of the total number of strain cycles received by the bone, and the intensity of training (load per unit time, pace, speed) is a function of the frequency of strain cycles applied to bone. The magnitude of each strain and duration of each strain cycle are functions of body weight, muscular shock absorption capability, and lower extremity biomechanical alignment. Impact attenuation is both intrinsic (muscular factors) and extrinsic (equipment and training surfaces). Eccentric muscular strength is important, but even more important is the muscle's ability to resist fatigue; to continue to contract effectively for a sustained period of time. This important factor is a function of metabolic adaptations that occur with training. Foot type and lower extremity biomechanical alignment may affect gait mechanics but altered gait may also occur from fatigue, disease, and injury. Finally, bone health is a major factor that determines the response of bone to loading and is affected by diet and nutrition, genetics, endocrine and hormonal status, the amount of regular exercise, and the presence of bone disease.
Symptamology, physical examination findings, and the results of radiographic imaging studies will be a function of the degree of progression of the injury along the continuum. Initially, accelerated remodeling does not produce symptoms, and plain radiographs will be normal, although magnetic resonance imaging (MRI) may show marrow edema and the nuclear bone scan will show focal uptake of technetium in proportion to the rate of osteoclastic activity. As accelerated remodeling progresses, mild pain will occur some time after the onset of exercise and, with further progression, occur earlier in the exercise bout. Without cessation of loading, pain intensity will increase and will be present even after the exercise bout and with normal activities of daily living. At this point, a technetium bone scan will be positive in all three phases, MRI will show marrow
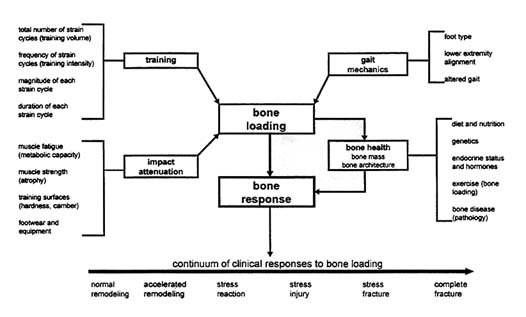
FIGURE 1-1 Determinants of stress fractures. Causal relationships of some of the factors that influence bone health and bone response to loading.
edema, but plain radiographs that specifically detect new bone formation or complete fractures, will still be negative. By the time plain radiographs are positive, a full-blown stress fracture is present. It is important to recognize that this process is on a continuum both physiologically and clinically, and that early intervention is associated with more rapid healing.
Microdamage
Whether microdamage precedes or follows bone remodeling is unclear. Mori and Burr (1993) demonstrated a significant increase in new remodeling events after bone microdamage was induced. Remodeling occurred preferentially in fatigue-damaged regions. However, there were still three times more resorption spaces than microcracks, which suggests that factors other than microdamage also initiate remodeling. Conversely, some human studies suggest that microdamage occurs at pre-existing sites of accelerated remodeling where osteoclastic resorption weakens an area of bone and subjects it to higher strains prior to the addition of new bone by osteoblasts (Burrows, 1956; Engh et al., 1970; Johnell et al., 1982; Johnson et al., 1963; Jones et al., 1989; Michael and Holder, 1985; Roberts and Vogt, 1939; Straus, 1932; Sweet and Allman, 1971). In a temporal series of stress fracture biopsies mainly from the upper tibial cortex in humans, initial histology revealed accelerated cortical resorption (Jones et al., 1989; Johnson et al., 1963). Although no microfracture was seen at this stage, a thin crack was evident in many of the specimens a week later, followed by osteoblastic activity and new bone formation. The study by Li et al. (1985)
employed an exercising rabbit model to assess sequential pathologic changes in the internal structure of the tibia caused by controlled excessive physical activity during a 10-wk period. It was not until the second week that small cracks appeared in the haversian system (the basic unit of structure of compact bone). At this stage, there was obvious osteoclastic resorption and a large number of cavity formations together with increasing subperiosteal osteoblast activity and periosteal proliferation. Most tibiae adapted successfully to changes in bone strain from repetitive loading through internal remodeling, and fractures only appeared if excessive stress continued in a tibia weakened by osteoclastic resorption.
DIAGNOSIS
The diagnosis of stress fracture is based on two factors: (1) local bone pain exacerbated by physical activity and associated with a history of new or recently increased level of physical activity, and (2) plain radiographic abnormalities or focal uptake of technetium on isotopic bone scans at the site of the pain (Matheson et al., 1987a). Computerized tomography and magnetic resonance imaging have also been used to help resolve uncertain cases (Brukner and Bennell, 1997). These techniques vary in their ability to detect the different types of bone pathology associated with a stress reaction. For example, there is often no detectable abnormality on plain x-rays for at least 2 to 3 weeks after symptoms have appeared, and in some cases, abnormalities will never be apparent (Brukner and Bennell, 1997; Matheson et al., 1987b). X-rays have high specificity but poor sensitivity in detecting stress fractures. In contrast, bone scans can detect a developing stress fracture at the stage of increased remodeling, within hours of the injury. Although a bone scan is very sensitive, it will also detect other types of bone lesions, and thus it lacks specificity for the identification of stress fractures. In addition, the bone scan may detect increased bone remodeling that is not associated with any symptoms or immediate danger of bone failure (Matheson et al., 1987a). It is important, then, to correlate results from bone imaging with clinical symptoms when diagnosing stress fractures (Brukner and Bennell, 1997). Different grading systems have been proposed to integrate findings on bone scans and x-rays with clinical symptoms in an effort to promote uniform diagnoses (Jones et al., 1989), but no single system has been adopted. In general, the U.S. military studies reviewed in this report defined stress fractures either through a combination of clinical symptoms and bone image evidence, or a definitive diagnosis noted on the medical record. (Jones et al., 1989).
EPIDEMIOLOGY
Stress fractures were first described in the military as the ''march fracture," and in the 1950s stress fractures were identified in the civilian athletic population. In Army recruits undergoing basic training, five injury types are repeatedly cited as accounting for the majority of all training injuries: stress fractures, overuse injuries of the knee, plantar fascitis, achilles tendonitis, and ankle sprains (Jones et al., 1983; Kowal, 1980; Reinker and Ozburne, 1979). Similarly, these same types of injuries are cited as accounting for the majority of all injuries in civilian running and jogging
programs (Clement et al., 1981; James et al., 1978; Pagliano, 1980) as well as in training programs for endurance athletes (Fredericson, 1996; Marti, 1988; O'Toole, 1992).
Table 1-1 summarizes the estimated cumulative incidence of stress fractures in U.S. military trainees in several studies conducted over the past 20 years. These estimates vary from 1 to 21 percent in women and from less than 1 to 9 percent in men. The variation in these estimates likely reflects both true and methodological influences. For example, some variation in stress fracture occurrence is to be expected due to differences in training program length and intensity among different military services. However, methodological differences and sampling bias between the studies probably also has an influence. For example, rates reported by Reinker and Ozburne (1979) were based only on subjects who were referred to a specialty clinic. Those reported by Kowal (1980) were based on self-report, and Brudvig and colleagues (1983) used a heterogeneous population (i.e., men and women in both basic and advanced training during a 1-y period) as the denominator when calculating incidence rates in their study. Another factor to consider is the method used to diagnose a stress fracture. For example, focal uptake of technetium on bone scan overestimates the incidence while plain radiography underestimates it. However, the higher occurrence in women than in men appears to be a common finding in military studies, as is a higher occurrence in Caucasians than in non-Caucasians. Stress fracture rates in military servicewomen shown in Table 1-1 are approximately 1.2 to 11 times higher than in men. This gender pattern was also observed in a recent study of Army-wide hospitalizations for spontaneous femur fractures, with female soldiers on active duty having a tenfold higher hospitalization rate than males (MSMR, 1997). Data from Marine recruits suggest that differential symptom reporting may play a role in the observed gender differences in stress fracture, as female recruits are more likely to report overall injury symptoms than males (Shaffer, 1997). Additional data from other services would be useful to support this possibility. The small amount of data by race in Table 1-1 suggest that the fracture rate in Caucasians is 3 to 8 times higher than in African Americans. Hospitalization rates for femur stress fractures were almost twice as high in Caucasian, non-Hispanic soldiers as in African Americans, and almost 30 percent higher than in Hispanics (MSMR, 1997). More data would be useful to confirm the actual magnitude of the African American/Caucasian difference in stress fracture rates.
Most studies on stress fracture occurrence in the military have focused on the basic training period. The small amount of data available suggest that, although injury rates decline after basic training, they are still a problem. For example, nearly 40 percent of the hospitalizations for spontaneous femur fractures in active-duty Army personnel occurred during the third or fourth month of training, which corresponds to the period of advanced individual training (AIT) for most soldiers (MSMR, 1997). Overall injury rates among female Army trainees were lower in advanced training (30%) than in basic combat training (BCT, 52%), and no longer differed from that seen among male trainees (24% during AIT and 27% during BCT) (Knapik and Henderson, 1997). Interestingly, the injury rate during AIT was 43 percent among women who were allowed to attend civilian schooling between BCT and AIT. The study authors speculated that this higher injury rate might be due to loss of physical conditioning in the extended period between basic and advanced training.
Data on stress fracture occurrence among civilians are limited to studies of athletes, and, with few exceptions, these are predominantly case reports or cross-sectional studies that cannot
TABLE 1-1 Estimated Cumulative Incidence of Stress Fractures (%) among U.S. Military Trainees
provide an estimate of true incidence (Brukner, 1997). Estimates of stress fracture incidence in civilian female track and field athletes or runners from two prospective studies were roughly 20 percent (Bennell et al., 1996; Zernicke et al., 1993), while a third prospective study that focused on athletes from various sports reported a 7 percent incidence (Johnson et al., 1994). This variation in rates may reflect both true and methodological differences in these studies. In
contrast to findings among military trainees, stress fracture rates among civilian female athletes are more similar (i.e., 1–3.5 times) to those in male civilian athletes (Brukner and Bennell, 1997). However, data for civilian athletes may not be directly comparable with those for military recruits due to differences in training, footwear, and initial fitness level (Bennell et al., 1996; Montgomery et al., 1989).
The skeletal site of the stress fracture may vary between men and women in the military (Table 1-2). The data in Table 1-2, although based on small sample sizes, suggest that female trainees are more likely to develop stress fractures in the upper leg and pelvis, while male trainees are more likely to have lower extremity stress fractures. Pelvic and femur fractures require more time for rehabilitation and may result in more disability and operational costs than stress fractures that occur below the knee. For example, hospitalizations for spontaneous femur fractures in active-duty Army soldiers between 1993 and 1996 resulted in more than a month of lost duty days on average, and more than a total of 7 lost duty years (MSMR, 1997). More than half of the hospitalized cases required surgery for internal fixation of the fracture. Factors causing this variation in site distribution of stress fractures in military women may include alterations in stride length (women are encouraged to march and keep the same stride as men, which is longer than what they are accustomed to) and the form in which they prepare to perform push-ups (women drop to their knees, men to their hands) (Shaffer, 1997). If an altered site distribution is confirmed, these findings further underscore a different pattern of stress fractures in military women, since, besides being more common, they tend to occur in skeletal sites with varying degrees of risk.
Military Training Programs
Military basic training programs vary from a duration of 6 weeks for basic military training (BMT) in the Air Force, to 11 to 13 weeks for Marine Corps recruit depot (MCRD), 9 weeks for Navy recruit training command (RTC), and 8 weeks for Army BCT. Table 1-3 summarizes the key features of each of these service programs.
Army
Most recruits prepare to enter the service and basic training through participation in the Delayed Entry Program (DEP) that exists in most recruiting centers. Between 70 and 80 percent of all recruits across the services spend at least 30 days in this program. Attendance and adoption of physical training recommendations (a minimum of once a month and no more than 90 minutes/exercise session) have been poor (Report of the Federal Advisory Committee on Gender-Integrated Training and Related Issues, to the Secretary of Defense, December 1997). Male DEP participants are required to correctly perform 13 push-ups and females must perform 1 push-up prior to enlistment. Physical training (PT) programs may consist of non-contact team sports (i.e. softball, touch or flag football, volleyball, basketball). Physical conditioning exercises may also be used instead of, or in combination with, those mentioned above. DEP training programs are not designed to replicate basic training conditions and environment, or to push members to meet the
TABLE 1-2 Anatomical Site of Stress Fracture among U.S. Military Trainees
|
|
|
|
Percent of All Stress Fractures |
|||
|
|
|
|
Women |
Men |
||
|
Study |
Sample |
Anatomical Site |
n |
% |
n |
% |
|
Protzman and Griffis, 1977 |
West Point cadets |
Foot |
4 |
40 |
5 |
42 |
|
|
|
Tibia/fibula |
3 |
30 |
7 |
58 |
|
|
|
Femur, incl. neck |
3 |
30 |
0 |
0 |
|
Brudvig et al., 1983 |
Army trainees |
Foot |
65 |
43 |
94 |
65 |
|
|
|
Tibia/fibula |
54 |
36 |
34 |
24 |
|
|
|
Femur, incl. neck |
17 |
11 |
12 |
8 |
|
|
|
Pelvis |
15 |
10 |
4 |
3 |
|
Iannacchione et al., 1995 |
Air Force trainees |
Ankle/foot |
18 |
58 |
6 |
75 |
|
|
|
Shin/lower leg |
10 |
32 |
2 |
25 |
|
|
|
Upper leg |
3 |
10 |
0 |
0 |
|
Shaffer, 1997 |
Marine recruits |
Foot |
* |
26 |
* |
46 |
|
|
|
Tibia |
* |
26 |
* |
50 |
|
|
|
Femur |
* |
23 |
* |
2 |
|
|
|
Pelvis |
* |
25 |
* |
2 |
|
* Data are not available. |
||||||
Army physical fitness standards applicable to active duty servicemembers, (USAREC Reg 601-95). Prior to departure for basic training, recruits to a Military Entrance Processing Site (MEPS) where a history and physical exam is performed and a form SF 88-93 is completed. Medical officers evaluate each recruit's physical capabilities based on a thorough medical history and examination. Recruits can be referred for orthopedic consultation if indicated by history or by observation of completion of a set of floor exercises designed to screen for musculoskeletal abnormalities (Sgt. Waters, Baltimore, MD MEPS, Personal communication, 1998).
Within the first couple of days of arrival at Army BCT, recruits will undergo a prediagnostic qualifying test. A female recruit must be able to do at least one push-up, and a male recruit must be able to do at least 13 push-ups. If these criteria are not met, the recruit is then referred to the Fitness Training Unit (FTU), which is designed to take the extremely poor performers and work with them through a specially designed training program to assure they can pass the entry criteria for push-ups, sit-ups, and a 2-mi run. Approximately 5 to 8 percent of a recruiting class are referred to the FTU. While assigned to the FTU, the soldier is provided fitness instruction as well as time to work on fitness activities. These fitness activities include aerobic and anaerobic exercises, but push-up performance remains the standard by which a soldier is assessed for advancement to BCT. A trainee has up to 21 days to achieve successfully the push-up standards of the fitness company. As soon as the female recruit can do 6 push-ups and the male recruit 20 push-ups, they re-enter BCT. If recruits are unable to achieve these standards, they are separated from the Army on grounds of not meeting medical fitness standards (Department of the Army, AR 350-15, AR 350-41).
TABLE 1-3 Summary of U.S. Military Training Programs
|
|
Army |
Navy |
Marine Corps |
Air Force |
|
Course duration (includes fitness + academic training) |
BCT: 8 wks AIT: varies greatly OSUT*: 13 wks |
RTC: 9 wks |
MCRD Men: 11 wks Women: 13 wks |
BMT: 6 wks |
|
Gender Integrated |
Yes: at some sites |
Yes |
No |
Yes |
|
Stratify by fitness level on entry |
Yes: if fails pre-diagnostic; assigned to FTU |
No |
PCP assignment available (pending initial strength test results) |
Yes: 5 levels for women, 4 levels for men |
|
Fitness training emphasis |
CR endurance (running, marching); Muscular endurance (push-ups, sit-ups) |
CR endurance (running, marching); Muscular endurance (push-ups, sit-ups) |
CR endurance (running, modified interval training); Muscular endurance (circuit resistance training) |
CR endurance (running for time instead of distance); Muscular endurance (circuit resistance training) |
|
Physical fitness testing requirements for graduation |
BCT for age group 17-21 by event score† 2-mi run time (min) Men: 16:54 Women: 19:54; Sit-ups (2 min) Men: 42 Women: 40; Push-ups (2 min) Men: 32 Women: 13 |
RTC for age group 17-19# 1.5-mi (run/walk) Men: 12:45 Women: 15:00; Curl-ups (2 min) Men: 45 Women: 40; Push-ups (2 min) Men: 38 Women: 18 |
MCRD for age group 17–26; Sit-ups⊕ (2 min) 45 (min); Dead hang pull-ups (men) 3 (no time limit); Flexed arm hang (women) 15 s; 3-mi run time (min) Men: 28 Women: 31 |
BMT for age group under 30; 2-mi run time (min) Men: 18 Women: 21; Sit-ups (within 2 min) Men: 45 Women: 38; Push-ups (within 2 min) Men: 30 Women: 14 |
|
|
AIT and OSUT; 2-mi run time (min); Men: 15:54 Women: 18:54; Sit-ups (2 min) Men: 52 Women: 50; Push-ups (2 min) Men: 42 Women: 18 |
|
|
|
|
Recruits trained yearly (n) |
Men: 55,496; Women: 13,329 |
Men: 45,000; Women: 9,000 |
Men: 45,000; Women: 2,500 |
34,500 |
|
Dropout rate (includes all causes) |
12–15% (3% due to physical fitness) |
|
Men: 10–12% Women: 15–18%‡ |
9.13%§ |
|
NOTE: BCT, basic combat training; AIT, advanced individual training; OSUT, one-station unit training; RTC: recruit training command; MCRD, Marine Corps recruit depot; BMT, basic military training; FTU, fitness training unit; PCP, Physical Conditioning Platoon; CR, cardiorespiratory. |
||||
|
* OSUT is a combination of BCT and AIT for some military occupational specialties. † For BCT, must score > 150 event pts (>50 pts each category); for AIT, must score > 160 event pts (> 60 pts each category). Event points stratified by age groups. ‡ Approximately 50% due to medical problems. § Reasons for discharge: total 1,375 recruits discharged during study period (Recruit Fitness Study, 9/95); 731 for new or pre-existing medical reasons; men, 55.6% injury related; women, 46.8% injury related. # Satisfactory score constitutes passing. ⊕ Effective 1 Jul 98, crunch sit-up will replace standard sit-up: 50 (2 min). |
||||
|
SOURCE: Army, L. Tomasi (personal communication, U.S. Army Physical Fitness School, Ft. Benning, Ga., 1998); Navy and Marine Corps, CDR R. A. Shaffer (personal communication, Naval Health Research Center, San Diego, Calif., 1998) Lt. Col. L. Pappa (personal communication, Training and Education Division, Marine Corps Combat Development Command, Quantico, Va., 1998); Air Force, MSGT L. Caramante (personal communication, 939th Training Squadron, Lackland AFB, San Antonio, Tx., 1998.) |
||||
At the end of the first week of BCT, a diagnostic training test is performed (1- or 2-mi run, sit-ups, and push-ups) as a screening and introductory testing measure. Over the next 6 to 7 weeks, the physical training continues in a regimental fashion. Certain factors are considered in the design of all military fitness training programs. These factors, Frequency, Intensity, Time and Type or "FITT," are the rationale for the Army's fitness program (Table 1-4). At approximately 7 weeks, the recruits take a repeat physical fitness test.2 They must score a minimum of 50 points in each event and a minimum total of 150 points to graduate from BCT and proceed to the AIT course.
When recruits fail, their cases are reviewed to determine reason(s) for failure. Approximately 3 percent leave BCT for physical fitness reasons and approximately another 12 percent leave for medical reasons (for example, cellulitis, stress fractures, pre-existing conditions).
All Army recruits who enter advanced training must have achieved a minimum fitness test score of 150 points. Depending on the training course (infantry, artillery, armor, military police), the duration of time in advanced training may vary. For infantry AIT, the course is 13 weeks. To graduate from advanced training, a recruit must achieve 60 points in each event and a total of 180 points.
Guidance on the planning and development of physical fitness training is outlined in the Army's Physical Fitness Training manual (FM 21-20, 1992). The manual provides guidelines for developing programs that will improve and maintain physical fitness levels for all Army personnel and includes specific chapters devoted to physical training during initial entry training and to injuries.
Navy and Marine Corps
In response to concerns about the incidence of musculoskeletal injuries among Marine Corps recruits, the Marine Corps convened several panels of Marine Corps and Navy researchers and sports physicians in 1995. These panels reviewed the Marine Corps Recruitment Depot (MCRD) physical training programs and issued a report that resulted in program revisions and the creation of a user's manual, A Physical Training Program to Reduce Musculoskeletal Injuries in U.S. Marine Corps Recruits (Almeida et al., 1997). The revised program was tested in 1995,
TABLE 1-4 FITT Factors Applied to Physical Conditioning Program
further modifications were made, and the new program was implemented in 1996 (personal communications, LTC Leon Pappa, Quantico VA, 1998; J. Hodgdon, NHRC San Diego, 1998). The modified training program targeted the average U.S.Marine Corps recruit, who is in poor to fair physical condition on arrival at MCRD. The new program contained a number of features:
-
a more progressive ramp-up of the running component in terms of distance, frequency, and intensity;
-
fewer formation runs and more individual runs;
-
addition of conditioning runs during Second Phase,
-
decreased total running mileage and increased total muscle strength and endurance training for a more balanced conditioning program;
-
modification of the Daily 7 calisthenics and the circuit course exercises to (a) target all major muscle groups, (b) enhance the strength training stimulus, and (c) reduce injury risk;
-
implementation of a comprehensive flexibility training program;
-
addition of exercise warm-up and cool-down routines;
-
a more progressive ramp-up of load-bearing conditioning hikes; and
-
modification of the scheduling of different physical training events to maximize training benefit and minimize the risks of overtraining and overuse injuries.
Through the implementation of the modified physical training program, stress fractures in male Marine Corps recruits have been reduced by 50 percent with no decrease in fitness level at graduation.
Based on the original panel recommendations and the experiences of the Marine Corps with the modified physical training program, the Navy has implemented a similar curriculum modification for female recruits, resulting in a 49 percent decrease in lower extremity overuse injuries.
Air Force
In the spring of 1994, the 737th Training Group at Lackland Air Force Base, the group responsible for BMT, was required to increase the fitness levels of its trainees. The Air Force Office of Prevention and Health Services Assessment (OPHSA) provided the consulting expertise for the design of a new physical conditioning (PC) program. The program included five key features:
-
an initial recruit fitness assessment,
-
separation into ability groups,
-
running for time instead of distance,
-
circuit resistance training with sandbags as weights, and
-
intertrainee encouragement.
In addition, OPHSA developed student academic material and collaborated on lesson plans for a new 4 h block of class instruction time that focused on exercise physiology and fitness principles. Recommended modifications to the PC program were field tested, and dramatic
improvements in the 2-mile run times were noted, as well as larger gains for push-ups and pull-ups in male trainees. Injury rates were not proportionally increased in males, and only a small increase was noted in the proportion of women reporting injuries. However, hip/leg injuries for women and ankle/foot injuries for men remained constant throughout basic training. Results from the field study validated the prototype PC program and demonstrated significant improvements over the existing PC program. Based on these findings, OPSHA recommended adoption of the new program in February 1995.
Fitness Levels of Recruits
Initial fitness levels have been found to be strongly related to subsequent development of stress fractures during basic training (Canham et al., 1996; Deuster and Jones, 1997; Shaffer, 1997). Some investigators have reported that differences in injury incidence no longer exist between genders when men and women of the same aerobic fitness levels are compared (Canham et al., 1996). Also, because women are smaller in body size, their average muscular strength may be less than that of men, but when expressed per pound of body weight, men's and women's strength may be similar (IOM, 1998). Table 1-5 summarizes data on initial fitness levels by gender in Army and Air Force recruits, respectively. Women had lower initial fitness scores than men, except for flexibility (Bell et al., in press; Canham et al., 1996). Data from Canham and colleagues (1996) suggest that fitness levels of all Army recruits have declined slightly over time between the mid-to late-1980s and the mid-1990s. One anecdotal report indicated that 75 percent of the incoming Army recruits who do not meet initial fitness standards are female (Bell, 1988). From experiences in Operation Desert Shield/Storm, it was apparent that many Air Force service personnel were ill-prepared for the rigors of the desert. This was attributed to the lack of preparation achieved in basic training. In female Air Force recruits, run test failures at baseline were reported to be 53 percent compared with 33 percent in male recruits (Jaeger et al., 1996).
The Navy reports that greater than 30 percent of Marine Corps recruits were in poor to very poor condition (i.e., 30 percent of incoming recruits cannot run 1.5 mile in less than 12 minutes) (Shaffer et al., 1994).
By the completion of the 8-wk Army BCT, women still performed fewer push-ups and ran more slowly than men, but women showed greater improvement over initial levels (i.e., improvements in sit-ups, push-ups, and run times were 98, 156, and 23 percent for women compared with 44, 54, and 16 percent for men) (Stoneman, 1997). Thus, it would appear that women are capable of achieving significant improvements in cardiovascular fitness and muscular endurance but may require a longer period to achieve levels comparable to men.
TABLE 1-5 Physical Fitness Levels of Military Recruits Entering Basic Training
|
Study |
Characteristic |
Women |
Men |
|
U.S. Army training programs |
|
|
|
|
Bell et al., in press |
|
|
|
|
Pre-BCT fitness 1988 |
Maximum handgrip strength (kg) |
67.3 |
117.2 |
|
|
Flexibility (cm) |
32.6 |
34.8 |
|
|
Initial 1-mi run time (min) |
10.1 |
7.6 |
|
|
Initial sit-ups (n) |
30.9 |
43.7 |
|
|
Initial push-ups (n) |
10.9 |
32.4 |
|
Canham et al., 1996, BCT |
|
|
|
|
Ft. Jackson 1984 |
2-mi run time* (min) |
20.2 |
15.6 |
|
|
Sit-ups (n) |
40 |
55 |
|
|
Push-ups (n) |
12 |
31 |
|
Ft. Jackson 1988 |
2-mi run time* (min) |
20.3 |
16.4 |
|
|
Sit-ups (n) |
34 |
44 |
|
|
Push-ups (n) |
10 |
31 |
|
Ft. Leonard Wood 1995 |
2-mi run time* (min) |
22.5 |
17.7 |
|
|
Sit-ups (n) |
33 |
41 |
|
|
Push-ups (n) |
11 |
31 |
|
Bell et al., in press |
|
|
|
|
Post-BCT fitness 1988 |
End 2-mi run time (min) |
17.4 |
14.0 |
|
|
End sit-ups (n) |
61.3 |
63.0 |
|
|
End push-ups (n) |
27.9 |
49.8 |
|
U.S. Air Force training programs** |
|
|
|
|
Wilborn, 1997 |
|
323 |
423 |
|
Baseline |
2-mi run time (min) |
21:42 |
17:21 |
|
|
sit-ups (n)/2 min |
31 |
42 |
|
|
push-ups (n) |
15 |
39 |
|
Final |
2-mi run time* (min) |
18:09 |
14:56 |
|
|
sit-ups (n)/2 min |
49 |
57 |
|
|
push-ups (n) |
27 |
50 |
|
NOTE: Basic combat training (BCT) = 8 weeks. * Predicted from 1-mi run time to allow comparison with physical fitness training scores. ** Random sample data from Basic Military Training Physical Conditioning program trainees at Lackland Air Force Base. |
|||
SUMMARY
A stress fracture occurs when changes in physical activity produce a site-specific mechanical ''load." This load results in an acute imbalance between the rate of osteoclastic resorption and the rate of osteoblastic new bone formation. Bone metabolism and remodeling are regulated by a large number of modulators including hormones, growth factors, and cytokines that interact at the level of the osteoblast, osteoclast, and other cells to regulate bone remodeling. Systemic hormones that affect bone remodeling include parathyroid hormone, calcitonin, vitamin D, estrogen, progesterone, growthhormone, thyroid hormone, glucocorticoids, and androgens. Stress fractures are diagnosed using a combination of clinical symptoms and results from bone imaging studies.
Estimates of stress fracture rates in military women during basic training range from 1 to 20 percent, while rates in military men range from less than 1 to 9 percent. This variation likely reflects both true variation in rates and methodological differences between the studies. Rates in civilian female athletes show less variation and do not substantiate the theory that a true difference exists. Stress fractures are more common in military women than in men, with estimates in women being 1.2 to 11 times higher than in men in the various studies performed to date. The difference in findings between military trainees and civilian athletes may reflect differences in training, footwear, and initial fitness levels between these two groups. Female military trainees appear to be more likely to suffer stress fractures in the upper leg and pelvis than are males. These fractures are more costly in terms of rehabilitation and potential disability than those that occur in the lower leg. Female military trainees also appear to be more likely to enter training with low fitness levels, which increases their risk of incurring a stress fracture, presumably due to premature muscle fatigue.




















