
APPENDIX A
The Study Approach
This appendix describes important definitions and the process by which disorders examined in this report were selected, analyzed, and evaluated to develop the report:
-
definition of brain disorders and selection of specific disorders;
-
definition of developing country;
-
early history of the study;
-
charge to the committee;
-
commissioned papers and technical input to the study;
-
workshop and committee meetings; and
-
other IOM reports on global health.
BRAIN DISORDERS AND SELECTION OF SPECIFIC DISORDERS FOR SECTION II
For the purposes of this report, neurological, psychiatric, and developmental disorders in the aggregate are referred to as brain disorders. These disorders include the following conditions from the classification system of the Global Burden of Disease study: neuropsychiatric conditions (unipolar depression, bipolar disorder, schizophrenia, epilepsy, alcohol use, dementia and other degenerative and hereditary CNS disorders, Parkinson's disease, multiple sclerosis, drug use, posttraumatic stress disorder, obsessive-compulsive disorders, and panic disorder); self-inflicted injuries (included in the wider category of inten-
tional injuries); cerebrovascular disease (included under cardiovascular disease); and the developmental disabilities given in Table 6-1 of this report, but not included in the global burden of disease classification.
Part I of the report discusses the challenges posed by brain disorders: the global burden they impose, the stigma and lost productivity associated with these conditions, the role of poverty and gender, the capacity of local health systems to care for these conditions, and the priorities for services, training, and research to lessen the burden of these disorders in the early years of the 21st century. Estimation of the global burden caused by the broad range of disorders is complicated by their not all being included in estimates of the global burden of disease, and for those that are included, their not having been classified, analyzed, and reported in a way that allows the individual disorders to be assembled simply and accurately. Rather they are drawn from the group of neuropsychiatric disorders, with the additions of self-inflicted illness, cerebrovascular disease or stroke, and additional estimations for developmental disabilities (not included in the Global Burden of Disease Study) based on prevalence data from developing countries.
Part II of the report focuses on six classes of disorders—developmental disabilities, epilepsy, schizophrenia, bipolar disorder, unipolar depression, and stroke—in order to consider specific opportunities for cost-effective interventions and priorities for research. In selecting these categories of disorders, sponsors of the report considered the following criteria:
-
the magnitude and severity of the disorder, as measured by prevalence and disability;
-
inclusion of disorders that affect different age groups from infancy to senescence; and
-
the likelihood of identifying cost-effective interventions for a disorder.
The framework for studying each category of disorder includes an overview of the epidemiology, a review of knowledge supporting existing and potential interventions, and projections of the feasibility, cost, and expected impact of those interventions.
DEVELOPING COUNTRIES
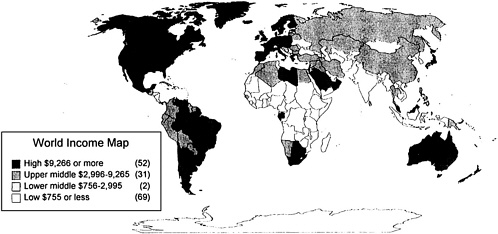
This report uses the term developing countries to describe those countries with economies classified as middle-and low-income in the 1999/2000 World Development Report (World Bank, 1999). They have per capita incomes that average less than $9,361 (see Figure A-1). These are subdivided into low-income countries with average per capita incomes of $760 or less, lower middle-income countries with average per capita incomes of $761 to $3,030, and upper middle-income countries with average per capita incomes of $3,031 to $9,361. The different countries in these groupings are developing at their own rates and
have different capacities and challenges in providing health care services to their populations. They tend to share a number of the following characteristics:
-
Low GDP per capita: In most developing countries, a serious disparity exists between increasing population size and low industrial and agricultural productivity. This situation is often aggravated by heavy external indebtedness, restricted access to global markets, and insecure prices of exportable raw commodities.
-
Young populations: The pyramidal age structure in most developing countries has a very broad base, due to the relative and absolute predominance of young people, and a narrow tip.
-
High infant mortality and low life expectancy: Although both indicators have moderated over the last decade, the vital statistics of a majority of the developing countries still lag behind the so-called developed world. The HIV/AIDS epidemic in Sub-Saharan Africa and the breakdown of health infrastructures throughout Central and Eastern Europe are creating worsening rates in these regions.
-
Epidemiological transition: While communicable diseases and malnutrition remain prime causes of morbidity in developing countries, the incidence of noncommunicable diseases such as heart disease, stroke, cancer, and diabetes is increasing, creating a double burden of disease.
-
Weak health care infrastructure: A shortage of skilled health care workers plagues most developing countries, where the relatively few medical professionals tend to be concentrated in urban areas. Health expenditure per capita in developing countries is typically a fraction of that in the developed world.
-
Social unrest and violent conflict: The subsequent disruption to and loss of infrastructure reduces the availability of health services. Additionally, the attention and funds for social services and healthcare are diverted to military and defense efforts.
-
Other features: Many, but not all, developing countries also suffer the following disadvantages: low literacy rates, especially among women; predominantly traditional, rural forms of social organization; extreme climates; frequent natural catastrophes such as drought, floods, and famine; large-scale population displacement; and epidemic rates of HIV/AIDS.
EARLY HISTORY OF THE STUDY
In 1998 the Global Forum for Health Research* agreed to Dr. Donald Silberberg's request for support to develop a report on neurological and psychiatric disorders in low- and middle-income countries. Dr. Silberberg recommended that the study be undertaken by the Institute of Medicine's (IOM) Board on Global Health. It would provide an independent assessment of the magnitude of the health burden in developing countries due to these disorders, the risks for disorders, the health care currently provided, and gaps in that care. The study would then review for some specific disorders, such as developmental disabilities, epilepsy, schizophrenia, stroke and unipolar depression, affordable diagnostic assessment procedures, treatments, and rehabilitation for low-income populations. IOM's Board on Global Health discussed the study with the directors of four institutes of the National Institutes of Health (National Institute of Mental Health, National Institute of Neurological Disorders and Stroke, National Institute of Child Health and Human Development, and Fogarty International Center) and staff of the Centers for Disease Control and Prevention (CDC). The NIH and CDC directors proposed that the scope of the study be broadened to include bipolar disorder, and provided support for the expanded study. The Board on Global Health shaped the proposed study to be responsive to the needs and opportunities presented in its 1997 report, America's Vital Interest in Global Health.
CHARGE TO THE COMMITTEE
The committee will prepare a consensus report that defines the increasing burden caused by neurological, psychiatric, and developmental disorders, and identifies opportunities to effectively reduce that burden with cost-effective strategies for prevention, diagnosis, and treatment of several major conditions. It will also identify the areas for research, development, and capacity strengthening that would contribute most significantly to reducing the burden of these disorders.
The study will review the overall burden of disease caused by a range of disorders. It will then focus on the following disorders to identify strategies for prevention, low-cost treatment, priorities for research and development, and for capacity building to meet the needs of developing countries:
|
* |
The Global Forum for Health Research is a Swiss foundation, created in 1997 by the World Health Organization, the World Bank, bilateral cooperation agencies, international and national foundations, national and international nongovernmental organizations, and private sector companies to promote research to improve the health of poor people. |
-
developmental disabilities;
-
unipolar depression;
-
bipolar disorder;
-
schizophrenia;
-
epilepsy; and
-
stroke.
COMMISSIONED PAPERS AND TECHNICAL INPUT TO THE STUDY
The study covers diverse topics and diverse settings so the committee commissioned several papers on the broad range of topics to be covered in the report. These papers were as follows:
-
“Health Services Research” by Vikram Patel;
-
“Poverty, Gender, and Nervous System Disorders” by Vikram Patel;
-
“The Role of Primary Care Providers and the Community” by Oyewusi Gureje;
-
“Congenital Anomalies in Developing Countries” by Eduardo Castilla;
-
“Disability in Sub-Saharan Africa: An Overview” by Gregory Powell;
-
“Disability in Jamaica” by Marigold (Molly) Thorburn;
-
“Disability in Bangladesh” by Nalia Khan; and
-
“Bipolar Disorder in Developing Countries” by Kwame Julius McKenzie.
In addition, several experts were appointed as technical reviewers for specific chapters. They provided written reviews that were considered by the committee for the final drafting of the chapters.
-
Chapter 2: Drs. Norman Satorius, Alex Cohen, and Joop de Jong;
-
Chapter 3: Drs. Gretchen Birbeck, Joop de Jong, Matthew Menken, Vikram Patel, and Ellis D'Arrigo Busnello;
-
Chapter 5: Drs. Robert Edgerton, Rune Simeonsson, and Molly Thorburn;
-
Chapter 6: Drs. Gretchen Birbeck, Michel Dumas, Jerome Engel, Pierre-Marie Preux, Leonid Prilipko, J.W.A.S. Sander, and Robert Scott;
-
Chapter 7: Dr. Oyewusi Gureje;
-
Chapter 8: Dr. Kwame McKenzie;
-
Chapter 9: Drs. Oyewusi Gureje and Jessie Mbwambo; and
-
Chapter 10: Drs Jose Biller, William Harlan, Niphon Poungvarin, and Ralph Sacco.
WORKSHOP AND COMMITTEE MEETINGS
The committee held a workshop in Washington, D.C., on November 8–9, 1999, to hear the perspective of sponsors and presentations from other experts on the major areas of the study, and to identify or clarify issues that would be important for the study charge. This was a valuable opportunity to explore the thinking of additional experts and to identify with them sources of information on the range of topics and issues. The agenda for the workshop is given in Appendix C. The individuals and their presentation topics are listed below:
-
Dr. Alex Cohen, “Mental Health of Indigenous People”;
-
Dr. Beugre Kouassi, “Epidemiology and Prevention of Epilepsy in Africa” and “Epidemiology and Prevention of Stroke in Africa”;
-
Dr. Thomas Langfitt, “Risk Factors and Outcomes for Children and Youth”;
-
Dr. Jessie Mbwambo, “Depression in Developing Countries”;
-
Dr. Vikram Patel, “Epidemiology of Common Mental Disorders in Developing Countries, with a Special Focus on Poverty and Female Gender as Risk Factors, ” and a “Health Systems Model of Approaching Mental Health Research and Program Implementation and the Overall Policy Implications of Cultural and Health System Diversity in Mental Health Care”;
-
Dr. Norman Sartorius, “The Global Burden of Disease”;
-
Dr. Peter Schantz, “Cysticercosis in Developing Countries”; and
-
Dr. Harvey Whiteford, “Mental Health Economics.”
Following the 2-day workshop, the committee met for deliberations twice in Washington D.C.: November 10, 1999, and May 9–10, 2000. Representatives of the committee's writing groups also met on March 29–30, 2000. Additionally, committee members along with IOM staff and consultants deliberated upon, contributed to, and reviewed the development of the report by e-mail, telephone, and mail between November 1999 and July 2000, then in September 2000 and January 2001 after revisions in response to external review.
OTHER IOM REPORTS ON GLOBAL HEALTH
This report on neurological and psychiatric disorders is one of a series of reports that address issues of global health and health policy:
-
Assessment of Future Scientific Needs for Live Variola Virus, 1999;
-
Control of Cardiovascular Diseases in Developing Countries: Research, Development, and Institutional Strengthening, 1998;
-
Prevention of Micronutrient Deficiencies: Tools for Policymakers and Public Health Workers, 1998;
-
America's Vital Interest in Global Health, 1997;
-
In Her Lifetime: Female Morbidity and Mortality in Sub-Saharan Africa , 1996;








