
2
Risk Assessment and Nutrition: Sharing Perspectives
Communication among members of different but related fields can be useful in addressing complex topics—in this case, nutritional risk assessment. This chapter addresses relationships between risk assessment and nutrition from the perspective of a risk assessor, a nutritional epidemiologist, a nutritionist in the food industry, and a physician working in prevention for the federal government. In particular, it addresses classical risk assessment processes and how they might be related to nutritional risk assessment, the questions and the challenges that nutrition poses for risk assessors, and selected applications of risk assessment in the food industry and the federal government.
A RISK ASSESSOR’S PERSPECTIVE: WHAT QUESTIONS CAN RISK ASSESSMENT ANSWER?
Presenter: Joseph Rodricks
Risk assessment is an activity that provides a crucial link between regulatory and public health policy decision making. It offers a highly systematic framework within which information can be organized and evaluated to serve the practical needs of decision makers. It provides information on what can and cannot be learned from the available research about threats to human health. Joseph Rodricks identified the focus of risk assessment, briefly described the risk assessment process, outlined
risk assessment questions related to the types of data, mentioned the application of risk assessment to nutritional risk, and identified topics for future efforts.
The Focus of Risk Assessment
According to Rodricks, two major questions are the focus of risk assessment:
-
What is the probability (preferably expressed quantitatively) that adverse health effects will occur in individuals exposed to an agent (whether it is a chemical, biological, or physical agent) or activity?
-
Under what conditions of exposure to an agent or activity are individuals unlikely to incur adverse health effects?
The use of risk management activities for risk assessment is inappropriate. Risk management activities include the identification of when risks become excessive or intolerable, the factors that should be considered in making decisions to reduce risks, and the means that should be used to reduce or manage risks.
The Risk Assessment Process
The process of risk assessment, which underwent its first major review by the National Research Council in 1983 (NRC, 1983), is a process that is still evolving. Figure 2-1 depicts the risk assessment process and features the key role of the decision-making context in designing a risk assessment.
Many years of experience have demonstrated that preservation of the integrity of the process requires the following:
-
delineation of the problem to be addressed (the decision to be made),
-
mechanisms to ensure interactive dialogues among all parties involved in risk assessment,
-
clear identification of the questions to be addressed by risk assessment,
-
the availability of the technical resources needed for risk assessment,
-
protection of the integrity of the risk assessment process by ensuring that decision makers (the risk managers) and others cannot exert influence on the risk assessors,
-
careful descriptions of the uncertainties involved in the risk assessment,
-
complete coverage of the risk questions,
-
adequate scientific peer review, and
-
the clear presentation of results so that they may be understood by decision makers and other parties.
Although these points may seem obvious, they are often overlooked. In addition, with regard to the presentation of results, those who provide results from risk assessments need to recognize that many people do not understand probabilities.
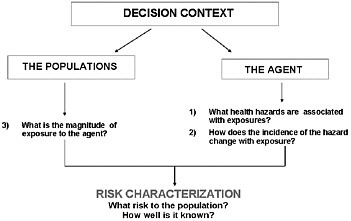
FIGURE 2-1 Steps in the risk assessment process. Note that hazard is an inherent property of the agent; it is not equivalent to risk.
Questions and Default Options Related to Types of Data
In risk assessment, the nature of the data leads to different types of questions. These questions are listed in Box 2-1.
The publication Risk Assessment in the Federal Government (NRC, 1983) notes that several default options may be available for addressing variability within populations, variability across species, and other factors that affect the findings of studies. Default options are policy judgments on how to accommodate uncertainties. That is, default options are used to make inferences in the absence of convincing evidence that indicates which of several competing methods or models is correct. An example of a default option is the scaling factor that is to be used to convert test responses in rodents to estimated responses in humans.
|
BOX 2-1 Risk Assessment Questions Related to Types of Data Hazard and dose—response data Derived from human studies
Derived from animal studies
From several studies that report different findings
Exposure (dose) data
|
Although the selection of default options introduces controversy, it ensures consistency and minimizes the possibility of the inappropriate manipulation of the findings from risk assessments. Default options tend to be cautious, potentially erring on the side of safety. In individual cases, a departure from the default may be allowed if it is well supported by the evidence (NRC, 1983).
Applying Risk Assessment Methods to Nutritional Risk Assessment
Although risk assessment cannot compensate for a lack of data and knowledge, it can guide research. There is a need for experimental models that can be used to study excessive nutrient intakes. Current thinking predicts a threshold for inadequate intakes, a threshold for excessive intakes, and a region between the two that is a condition of homeostasis. The extent to which the tails of the distribution of intakes for a nutrient fall outside the range of homeostasis provides a description of the nutrient intakes that may result in health risks.
Concluding Remarks
Rodricks identified five important topics for future efforts:
-
development of consensus guidelines for the extrapolation of the findings and data from previous studies and other default options for future risk assessments;
-
determination of the certainty of evidence supporting homeostasis;
-
examination of how the range of homeostasis varies among individuals, including the consideration of people who differ by life stage (growth, development, reproductive state, aging), nutritional status, and, perhaps, health status;
-
useful ways to describe individual and population risks given the variabilities mentioned above; and
-
improved methods for describing scientific uncertainties to decision makers and others.
A NUTRITIONAL EPIDEMIOLOGIST’S PERSPECTIVE: RELEVANT ISSUES IN NUTRITIONAL RISK ASSESSMENT
Presenter: Shiriki Kumanyika
Given that food is a human need and a universal exposure, dietary intakes can be evaluated as positive, negative, or neutral for health. Shiriki Kumanyika addressed the kinds of questions that are pertinent to nutritional risk assessment and the methods used to quantify nutritional risk. She then identified challenges to the assessment of nutritional risk.
Framing the Questions
In the United States, many different groups pose questions about nutritional risk. These groups include the Institute of Medicine’s Food and Nutrition Board; various agencies of the federal government that address health, food safety, and food regulation; the Dietary Guidelines Advisory Committee; disease-focused organizations, such as the American Heart Association and the American Cancer Society; life-stage interest groups, such as the American Academy of Pediatrics and the March of Dimes; the food industry; and consumers. The nature of the questions reflects the group’s interest or responsibility. Consumers’ perceptions of risk, however, often do not match the risks identified by other groups.
Types of Risk
In nutrition, risk may take a number of forms, including
-
the adequacy–toxicity continuum as it relates to the direct effects of essential nutrients;
-
food-borne illnesses, including allergies; and
-
the broad areas of the effects of diet on health as they relate to the prevention and management of chronic diseases.
Population Considerations
Risks vary within populations. Population considerations that are important in assessments of nutritional risk include life stage, genetics, environmental stressors, behaviors (such as smoking) that influence nutrient requirements and metabolic vulnerability, and health status. Ethnic differences may need to be considered for some nutrients, such as sodium, potassium, and calcium.
Food and Nutrition Variables
A wide range of dietary substances may pose risks. These substances include proteins, fats, carbohydrates, fiber, vitamins, and minerals that occur naturally in foods or that are added to foods or taken as supplements; other naturally occurring food constituents; contaminants; toxins; mutagens; botanicals; other nonnutrient dietary supplements; and alcohol. The category “other naturally occurring food constituents” includes an array of substances ranging from anthocyanins to sulfides (allium) (Van Duyn and Pivonka, 2000). In addition to individual food components and supplements, other food and nutrition variables may affect risk either positively or negatively. These variables include specific foods; food processing and preparation methods; and entire dietary patterns, which entail interactions within the mix of nutrients and foods consumed. The complexity that is integral to the food supply and dietary patterns adds to the complexity of risk assessment.
Outcomes
Physiological indicators of the effects of diet on health include changes related to growth; adipose tissue; musculoskeletal tissue; metabolism; cognitive function; and the gastrointestinal, cardiovascular, reproductive, immunological, and neurological systems (Task Force on Community Preventive Services, 2005). Health outcomes of major public health importance for assessing the effects of diet include cardiovascular diseases, different types of cancers, type 2 diabetes mellitus, obesity, dental caries, and osteoporosis (WHO, 2003). Each of these diseases has subcategories. Many reversible intermediates (e.g., hypertension and elevated low-density lipoprotein cholesterol concentrations) occur be-
tween dietary intakes and possible morbidity and mortality outcomes. Multiple pathways and multiple targets also add to the complexity of risk assessment.
The effects of a single nutrient substance may involve many different pathways (Blumberg, 1997). For example, many nutrients and food variables could affect the risk of the same disease, but in different ways. For example, increased intakes of soluble fiber and vitamin B6 could help prevent cardiovascular disease, whereas increased intakes of saturated fat and sodium could increase the risk (Blumberg, 1997; Esrey, et al., 1996). Another element of the complexity is that many of the cellular and biochemical mechanisms that play a role in the pathogenesis of major chronic diseases appear to be interrelated (Deckelbaum et al., 1999).
Quantification of Nutritional Risks
The quantification of nutritional risks informs guidance to the public about diet and supplement intake. Two major groups have worked to quantify nutritional risks in the United States: (1) the Food and Nutrition Board of the Institute of Medicine, which developed the Dietary Reference Intakes (DRIs), and (2) the Dietary Guidelines Advisory Committee (advising the U.S. Department of Health and Human Services and the U.S. Department of Agriculture, which jointly publish the Dietary Guidelines for Americans).
Published DRIs include values for Estimated Average Requirements (EARs), Adequate Intakes, Recommended Dietary Allowances (RDAs), and Tolerable Upper Intake Levels (ULs) for 45 nutrients or nutrient categories (IOM, 2006). In some cases, EARs and ULs were not set because of a lack of data. The 2005 Dietary Guidelines for Americans (DHHS/USDA, 2005) provide nine focus areas, ranging from adequate nutrients within calorie needs to food safety. Themes in the 2005 Dietary Guidelines for Americans include calories needed to achieve desirable weight; limits on total and saturated fat and cholesterol intakes; the consumption of a variety of foods, with an emphasis on plant sources; moderate sugar and salt intakes; and alcohol consumption in moderation, if used. The advisory committee that encouraged these themes considered adequacy, the avoidance of excess or toxic amounts of nutrients, and the prevention of chronic illness (DGAC, 2005).
Concluding Remarks
Kumanyika identified the need to address the following challenging topics:
-
inconclusive or absent data;
-
adverse effects (e.g., on chronic diseases, within the range of nutrient intakes that falls between the extremes of adequacy and toxicity);
-
the various effects (i.e., sometimes beneficial and sometimes harmful) of a given nutrient or diet pattern, depending on the level consumed or, perhaps, on the interactions between nutrients or food constituents;
-
the safety risks of recommended foods, such as fish; and
-
paradigms that are appropriate for the examination of evidence related to chronic disease outcomes and to risks that the consumption of single foods or dietary patterns may pose, as such paradigms may differ from those used to address other types of outcomes or exposures (IOM, 2002).
A number of the research needs identified by the 2005 Dietary Guidelines Advisory Committee (DGAC, 2005) are also relevant to the area of nutritional risk assessment. A major challenge rests with addressing the complexity of assessing nutritional risk in an acceptable manner. Current risk assessment approaches address questions relating to the direct effects of single or relatively specific and selective exposures. However, there are many types of nutritional risk, many variables, many endpoints, and many interactions. The result is a set of very complex questions, and the applicability of current methods to addressing complex exposures and multiple possible endpoints is unclear.
AN INDUSTRY PERSPECTIVE: HOW THE FOOD INDUSTRY USES RESULTS FROM RISK ASSESSMENT
Presenter: Kathryn Wiemer
The food industry actively applies risk management principles in a variety of areas, including food safety and nutrition. Kathryn Wiemer provided a brief overview of food fortification and illustrated how Gen-
eral Mills applies risk management principles to discretionary food fortification decisions. The application of risk management principles involves, in part, the use of findings from nutritional risk assessments.
Milestones in Fortification History
The food industry informs consumers about food fortification by means of the nutrition label. Figure 2-2 depicts milestones in food fortification history beginning in 1973, when the FDA established U.S. Recommended Daily Allowances (U.S. RDAs) for labeling foods, and projected to about 2012. The U.S. RDAs differ from the Recommended Dietary Allowances (RDAs) mentioned earlier in this chapter. In particular, the U.S. RDAs were based on the 1968 Recommended Dietary Allowances set by the National Research Council. Beginning in 1993, the FDA called for Daily Values (DVs) to replace the U.S. RDAs on nutrition labels, but, despite revisions of the Recommended Dietary Allowances after 1968, the DVs were also based on the 1968 values.
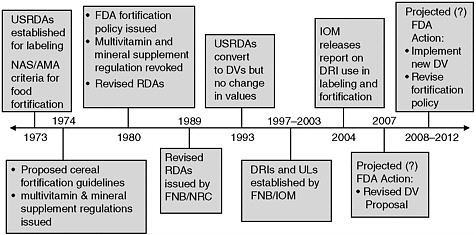
FIGURE 2-2 Milestones in food fortification history.
NOTE: AMA = American Medical Association; DRI = Dietary Reference Intake; DV = Daily Value; FDA = Food and Drug Administration: FNB = Food and Nutrition Board; NAS = National Academy of Sciences: RDA = Recommended Dietary Allowance; UL = Tolerable Upper Intake Level; US RDA = U.S. Recommended Daily Allowance.
Discretionary Fortification
Discretionary fortification refers to the addition of nutrients to food, excluding cases in which the food product is formulated to meet a standard of identity promulgated by the FDA, such as for enriched flour.
Principles
The FDA’s fortification policy (FDA, 1980) outlines principles for the addition of nutrients to foods. Although this policy is not a regulation, it provides guidance to the food industry. More recently, the report Dietary Reference Intakes: Guiding Principles for Nutrition Labeling and Fortification (IOM, 2003) presented guiding principles related to the discretionary fortification of foods (Figure 2-3). The guiding principles address topics related to risk assessment, such as the distribution of usual intakes in the population, how the discretionary fortification would alter the dietary intake of the nutrient in question, and, if applicable, the severity of the adverse effect on which the UL for the nutrient is based. Although these guidelines and recommendations were designed to assist regulatory agencies that oversee fortification, the food industry considers them as well; and they pose a number of challenges. In particular, when
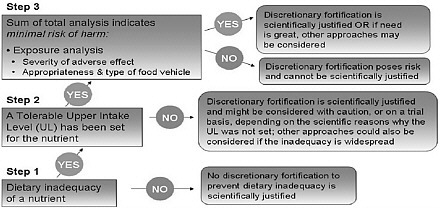
FIGURE 2-3 Decision tree for the discretionary fortification of foods.
SOURCE: IOM (2003).
making discretionary fortification decisions, the food industry must consider FDA’s fortification policy, ULs for nutrients, the findings in the report Dietary Reference Intakes: Applications in Dietary Assessment (IOM, 2001a), public policy on health, including Dietary Guidelines, and evolving scientific nutrient research.
General Mills’s Approach
General Mills’s approach to discretionary fortification uses FDA’s fortification policy (FDA, 1980) as the framework and DRI reports as the core. The approach includes the steps shown in Box 2-2.
|
BOX 2-2 General Mills’s Approach to Discretionary Fortification
|
One current issue involves the overlap among DVs, Recommended Dietary Allowances (RDAs), and ULs, especially since the DVs do not change for different age groups whereas RDAs and ULs do. The DV for several nutrients is higher than the UL for certain age groups. Wiemer directed attention to zinc: the DV is 15 milligrams (mg), but the UL for children ages 1 to 3 years (7 mg) is much lower than the DV, and the UL for children ages 4 to 8 years (12 mg) is somewhat lower than the DV. Meat, fish, and poultry; ready-to-eat cereals; other grain products; and milk are the main sources of zinc in the U.S. diet and account for well over 67 percent of the total average zinc intake.
Further analysis of dietary intake data shows that, compared with the percentage of people whose zinc intakes are greater than the UL, a higher percentage of people are not meeting the EAR for zinc. Estimates indicate that reducing the amount of zinc in cereal would decrease but not eliminate the occurrence of intakes by children that exceed the UL for zinc.
Wiemer took the position that industry can and should play a role in addressing nutrient intake shortfalls, pointing out several shortfalls identified in the Dietary Guidelines for Americans (DHHS/USDA, 2005): calcium, magnesium, and vitamin D for bone health; whole grains and fiber for heart and digestive health; and healthy fats (omega-3 fatty acids) and potassium for heart health.
Concluding Remarks
In summary, Wiemer posed several challenging questions:
-
What is the best approach for interpreting and applying the DRI values to discretionary fortification?
-
Should all UL values have equal weight? (Consider vitamin A and zinc.)
-
What approach is appropriate when UL values for children are lower than the current DV or the RDA or EAR for adults?
-
-
How can the benefit of fortification for one subpopulation be balanced against the potential risk of adverse effects for another subpopulation?
-
What approach will be used to develop ULs for nutrients that are being added to foods but for which no UL has been set (for example, omega-3 fatty acids)?
A PUBLIC POLICY PERSPECTIVE: LIMITATIONS OF CURRENT RISK ASSESSMENT METHODS FOR DECISION MAKING
Presenter: William Dietz1
The presentation addressed the limitations of current methods for assessing the risk of obesity, the consideration of specific foods and food behaviors (rather than nutrients) as risk factors for obesity, and the risk of high folic acid intakes to certain subpopulations. William Dietz’s perspective is that of a person who is involved in prevention and, therefore, in helping make decisions based on the available data.
Limitations of Current Methods for Assessing the Risk of Obesity
Uncertainties exist about the use of body mass index (BMI) as a predictor of risk. Moreover, two of the proximal determinants of BMI—energy expenditure and energy intake—have limitations. Because these two factors are interrelated and can not be examined independently of one another, there may not be a threshold effect for either of them in terms of the risk for obesity.
Energy Expenditure Measurements
Cross-sectional data indicate that obese individuals are less active than those who are not overweight. An important meta-analysis (Fogelholm and Kukkonen-Harjula, 2000), however, concluded that the findings are very mixed from prospective studies of the impact of baseline physical activity on changes in body fat levels. Using doubly labeled water, Bandini and colleagues (1990) found that the total energy expen-
diture of obese adolescents exceeds that of nonobese youth. As a group, the nonresting energy expenditure among preadolescent girls did not predict changes in body fat levels over about a 5-year period. Moreover, the physical activity level, which is the ratio of total energy expenditure to the resting metabolic rate, is similar between obese and nonobese individuals (Bandini et al., 1990). The type of energy expenditure that is most promising as a predictor of weight gain is based on the amount of nonexercise type of energy expenditure, such as fidgeting, that an individual engages in. However, good measurement techniques are not yet available for determining this type of energy expenditure (Dietz et al., 1994).
Energy Intake Measurements
Bandini and colleagues (1990) found that self-reported metabolizable energy intake was substantially lower than measured total energy expenditure in adolescents, and the degree of underreporting tended to increase with increases in BMI. This limitation of self-reported intake data (obtained by using diet records or diet recalls) has been confirmed in many other studies. Moreover, Subar and colleagues (2003) demonstrated that estimates of energy and protein intakes from food frequency questionnaires have very low correlations with the estimates obtained by multiple 24-hour recalls. Thus, estimates of energy intake are not good determinants of the risk of becoming obese.
Foods and Behaviors as Risk Factors for Obesity
Because neither measures of energy expenditure nor energy intake serve as good determinants of the risk of developing obesity, some investigators are examining data on foods and food behaviors as risk factors for obesity. The consumption of sugar-sweetened beverages is one example of a potential risk factor for obesity. Observational studies have found a positive relationship between the consumption of sugar-sweetened beverages and weight change (Berkey et al., 2004; Ludwig et al., 2001; Phillips et al., 2004; Striegel-Moore et al., 2006; Welsh et al., 2005). The evidence has been consistent, with some studies showing that there is a dose–response relationship and that sugar-sweetened beverage intake relates temporally to changes in body weight.
Fructose—the major source of which is sugar-sweetened beverages—may be a potential contributor to obesity. There is no insulin response to this monosaccharide (in contrast to the insulin response obtained when fructose is delivered in the form of the disaccharide sucrose). Studies also implicate fructose consumption as a risk factor for hypertriglyceridemia, hepatic and adipose insulin resistance, a small increase in plasma glucose concentration, and mild gastrointestinal distress or irritable bowel syndrome. One problem in examining the relationship between fructose intake and the development of obesity is a lack of data that can be used to examine changes in fructose intake over time. Dietz underscored the need for intervention studies, especially ones involving sugar-sweetened beverages, to learn more about the potential contribution of suspect foods or nutrients to various disease outcomes.
Other dietary variables potentially related to the development of obesity include the energy density of food, portion sizes, meal patterns, binge eating, restrained eating, nighttime eating syndrome, the glycemic index of food, and macronutrient ratios.
The Risk of High Folic Acid Intakes to Certain Groups
In the United States, the fortification of enriched cereal grains with folic acid has resulted in a marked decline in the incidence of pregnancies affected by neural tube defects. Nonetheless, it appears that subsets of the population with the TT gene sequence variant of the methylene tetrahydrofolate reductase enzyme may be at increased risk of low plasma folate concentrations (R. J. Berry, National Center for Birth Defects and Developmental Disabilities, personal communication, February 14, 2007). This raises concern that a folate intake high enough to achieve the desired plasma folate concentrations in this subgroup may approach the UL. In part because an estimated 38 percent of people of Chinese descent and 20 to 25 percent of the Hispanic population have this gene variant, this topic merits consideration. The potential adverse effects of high folic acid intake include interactions with other B vitamins, effects such as hypermethylation, seizure thresholds, and an incomplete conversion of folic acid to its active form. At present, there is a limited capacity to measure the outcomes. Moreover, Rosenberg (2005) pointed out that there is no clear assignment of the responsibility to monitor the population for adverse effects of folic acid fortification.
Concluding Remarks
The three examples given—energy balance and obesity, foods and food-related behaviors and obesity, and folic acid and its potential adverse effects—illustrate selected limitations of current methods of risk assessment and point out challenges for the future.
OPEN DISCUSSION
During the open discussion, the workshop participants raised a number of points relating to discretionary fortification. Among the topics addressed were the following:
-
the influence of nutrient bioavailability on discretionary fortification decisions,
-
the influence of labeling requirements for portion size on the nutrient profile that appears on the label of fortified cereal,
-
the extent to which food companies consider information about the fortification of other companies’ food products as a part of their discretionary fortification decisions,
-
concern about iodization policies in the face of both the increased consumption of prepared foods made with noniodized salt and the decreased use of iodized table salt, and
-
ways to handle the effects of increased folic acid consumption on vitamin B12 status and its health effects.
Other topics that were discussed during the open discussion have been incorporated into Chapter 6, Perspectives on Challenges and Solutions: Summary Remarks and Suggested Next Steps.


















