
1
Introduction
As the leading cause of death worldwide, cardiovascular disease (CVD) has a major impact on both developed and developing nations. Although the spotlight is more often on the global burden of mortality associated with malaria, tuberculosis, and HIV/AIDS, CVD causes more than three times the annual deaths of these three diseases combined. Indeed, nearly 30 percent of all deaths in low and middle income countries are attributable to CVD, and more than 80 percent of CVD-related deaths worldwide now occur in low and middle income countries (WHO, 2008b). This health burden is accompanied by a deleterious economic impact. However, despite the significant and growing health and economic burden in low and middle income countries, CVD and related chronic diseases are not included by most stakeholders in their investments and commitments to improving the health of the world’s people.
CVD and related chronic diseases were once considered to be diseases of industrialized nations. However, in recent years an increasingly robust body of epidemiological evidence has highlighted the proliferation of CVD risk factors worldwide, including obesity, hypertension, and diabetes. The worsening of cardiovascular health around the world—and most notably in developing countries—reflects significant global changes in behavior and lifestyle. The “westernization” of dietary habits, decreased levels of physical activity, increased childhood obesity, and increased tobacco consumption—accelerated by industrialization, urbanization, and globalization—now threaten once-low-risk regions. In addition, the decline in infectious diseases and improved childhood nutrition have contributed to the aging of populations in many low and middle income countries, resulting in an increasing
number of individuals who survive to the age at which risk factors they accrued throughout childhood and early adulthood manifest as chronic diseases. This has resulted in an epidemic that is “old” in its similarity to the rise in CVD that occurred in the developed world in previous decades, yet brings with it new characteristics that are a result of contemporary global circumstances.
STUDY CHARGE, APPROACH, AND SCOPE
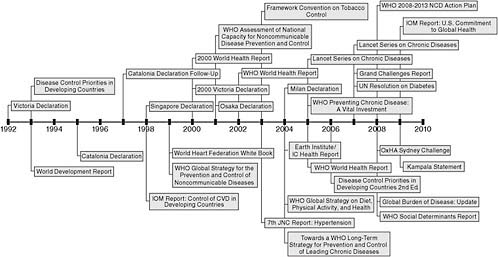
Over the past several decades, a considerable amount has been learned about the determinants of CVD as well as how to reduce CVD incidence and mortality. Building on this knowledge and the emerging evidence of the growing burden of CVD in developing countries, there has been a steady escalation of international reports, declarations, and resolutions calling attention to the growing threat of the global CVD epidemic. These are summarized in Figure 1.1 and Box 1.1 later in this chapter, where they are discussed in more detail to set the historical context for this report.
These declarations, reports, and resolutions have resulted in a growing recognition that CVD, and chronic noncommunicable diseases more broadly, are a worldwide problem whose burden is increasingly felt by low and middle income countries. In the past several years, this recognition has begun to translate into guidance for action. However, despite examples from the developed world that demonstrate promise and hope for the reduction of disease burden on a national level, the burden of CVD has continued to grow and concrete steps toward scaling up CVD treatment and prevention efforts in developing countries have been slow to materialize. Recognizing a need to help catalyze progress from guidance and strategies to actions, the National Heart, Lung, and Blood Institute (NHLBI) sponsored this study by the Institute of Medicine (IOM), and an ad hoc committee was convened to study the evolving global epidemic of CVD and offer conclusions and recommendations pertinent to its control.
Study Charge
The full Statement of Task for the Committee on Preventing the Global Epidemic of Cardiovascular Disease: Meeting the Challenges in Developing Countries can be found in Appendix A. In summary, the committee was charged with synthesizing and expanding relevant evidence and knowledge based on research findings, with an emphasis on developing concepts of global partnership and collaborations, and on recommending actions targeted at global governmental organizations, nongovernmental organizations (NGOs), policy and decision makers, funding agencies, academic and research institutions, and the general public.
In response to its charge, the committee undertook an analysis of the current state of efforts to reduce the global epidemic of CVD based on a review of the available literature and of information gathered from various stakeholders in CVD and global health. In this analysis, the committee evaluated why there has not been more action to address CVD; assessed the available evidence on intervention approaches to prevent and manage CVD, including knowledge and strategies pertinent to their implementation in low and middle income countries; and drew conclusions about the necessary next steps to move forward.
Prior reports have identified general priorities and recommended a wide range of possible actions for a multitude of stakeholders; indeed, the findings and conclusions of this report reinforce many of those messages and priorities. In this report’s recommendations, however, the committee has emphasized advancing the field beyond messages about broad conceptual solutions and has identified a limited set of specific actions targeted to specific stakeholders. These actions are intended to encourage a sufficient shift in the global health and development agenda to facilitate critical next steps that will build toward the eventual goal of widespread dissemination and implementation of evidence-based programs, policies, and other tools to address CVD and related chronic diseases in developing countries.
Study Approach
The committee met four times to deliberate in person, and conducted additional deliberations by teleconference and electronic communications. Public information-gathering sessions were held in conjunction with the second and third meetings; the complete agendas for these sessions can be found in Appendix C. The committee also commissioned several papers that informed the study; these are referenced within the report.
The committee reviewed literature and information from a range of disciplines and sources. A comprehensive systematic review of all primary literature relevant to the study’s broad charge was not within the scope of the study. Instead, this report represents a summative description of the key evidence, with illustrative research examples discussed in more detail. In order to limit the length of this document and to avoid replication of existing work, the committee sought existing relevant, high-quality systematic and narrative reviews. In content areas where these were available, the report includes summaries of key findings, but otherwise refers the reader to the available resources for more detailed information.
For intervention approaches to reduce the burden of disease, the committee reviewed the literature to identify relevant examples of interventions, programs, or policies that target CVD and related CVD-risk factors, as well as to identify areas in which relatively little applicable intervention research has been conducted. The committee’s approach to the analysis
of intervention evidence is described in full in Chapter 5. In summary, the committee emphasized effectiveness, contextual generalizability, feasibility, and relevance for real-world implementation. Therefore, the focus was on identifying intervention approaches for CVD with evidence in developing countries. Where this evidence was limited, examples were sought that offer generalizable lessons from interventions with evidence from both CVD-specific approaches in developed countries and developing country evidence for non-CVD health outcomes.
Using this approach, the report strives to move the field beyond a discussion of general intervention approaches and policy priorities in the broad terms of prior reports, such as “reduce salt consumption,” “improve diets,” “reduce tobacco use,” “increase physical activity,” and “screen and treat biological risk factors and disease.” The report achieves this by offering a pragmatic review of the available evidence in the context of potential for implementation of interventions and strategies, while recognizing the complexities of heterogeneity and variability in capacity among different low and middle income countries. Indeed, the committee’s goal was to go beyond the relatively few well-known intervention examples that appear in many preceding reports to instead gather information of sufficient depth, breadth, and specificity on actual intervention implementation in order to realistically inform resource prioritization in real-world, country-specific decision making.
Applying this approach revealed significant gaps in the evidence base and led to greater specificity and clarity in defining the needs to transition from knowledge to action, which has resulted in a research agenda focusing on implementation research and additional economic analysis. However, the committee does not intend that the findings highlighting ongoing research priorities be taken as a suggestion of inaction. A principle throughout the report is one of being action oriented based on available findings.
Study Scope and Audiences
This committee was tasked by the sponsor to focus on cardiovascular disease, which is the largest contributor to the global burden of chronic disease (WHO, 2008b). This focus was clearly mandated by the Statement of Task, but with the understanding that the report should consider CVD in the context of other related chronic diseases that share common risk factors and intervention approaches, especially diabetes, cancer, and chronic respiratory disease (Nabel, 2009). The term cardiovascular disease can encompass a wide range of diseases, such as coronary heart disease, congestive heart failure, vascular diseases of the brain and kidney, peripheral vascular disease, congenital heart defects, and infectious cardiac disease. As evidenced in Chapter 2, the committee focused its attention primarily on the major contributors to global CVD mortality, coronary heart disease
and stroke, and on the major modifiable risk factors for cardiovascular diseases, especially tobacco use, unhealthy diet, physical inactivity, obesity, hypertension, dyslipidemia, and elevated blood glucose as well as broader determinants associated with risk for CVD. In addition, although not the major emphasis of the report, in some regions there continues to be a high burden of infectious cardiac disease, particularly rheumatic heart disease and Chagas disease (Muna, 1993; WHO, 2003b; WHO Study Group and WHO, 2004). Therefore, these are also reviewed briefly in Chapter 2 of the report, along with pericarditis and cardiomyopathies caused by tuberculosis (TB) and HIV.
In order to identify steps to prevent and mitigate the growing burden of cardiovascular disease, the committee was charged by the sponsor to study CVD “prevention and management.” In the course of its deliberations among experts from a range of disciplines that have a role in addressing cardiovascular disease, such as public health, health communications, and cardiology, the committee found that different fields often use different terms and definitions to categorize similar intervention approaches and that many intervention approaches do not fall into clearly delineated categories. The committee felt that it was not in its mandate nor was it feasible within the study scope and timeline to come to consensus definitions of terms and their subcategories. Therefore, to prevent confusion and to avoid detracting from key messages with discussions of nomenclature, the committee refers broadly to health promotion, prevention, treatment, and disease management, but whenever possible the committee refers to specific intervention approaches descriptively rather than categorically and makes no attempt to assign them to further subcategories.
Furthermore, the committee views health promotion, prevention, treatment, and disease management as part of a continuous spectrum. The committee interpreted its charge to be inclusive of this spectrum of approaches rather than as a mandate to recommend choices among them, and the committee found that the entire range warrants attention in order to truly address CVD and related chronic diseases. Indeed, the totality of the available intervention and economic evidence supports a balanced approach in which promotion and prevention is emphasized, but which also recognizes the need for effective, appropriate, quality delivery of medical interventions for risk reduction and treatment. The appropriate balance of investment in different intervention approaches across this spectrum is a challenge for evidenced-base policy decisions that is discussed in Chapter 7.
The sponsor’s charge to the committee clearly anticipated that the very nature of the problem necessitates concerted action by a wide range of stakeholders. As articulated in the committee’s Framework for Action (Chapter 8), the committee also recognizes the need to be broad in the approach to the problem, and thus the report has messages and recommenda-
tions aimed at multilateral and bilateral development and health agencies, national and subnational governments in low and middle income countries, nongovernmental organizations, professional societies, research and training institutions, and the private sector (see Figure 8.2 in Chapter 8).
However, unlike many of the preceding documents in the field of global chronic diseases, this report was initiated by a specific stakeholder with the will and resources to act upon its recommendations. Therefore, the committee viewed this study as first and foremost an opportunity to provide independent, external guidance to NHLBI to inform and support its emerging investments in global CVD and to help set goals and priorities that will ensure the success of current and future endeavors to incorporate global health into its activities, including its strategic partnerships with other relevant stakeholders within the United States and internationally. The committee also viewed the report as an opportunity to identify ways in which the U.S. global health agenda, along with the international global health agenda, can evolve to be more inclusive of chronic diseases, providing elaboration on a mandate that was issued in the 2009 IOM report The U.S. Commitment to Global Health (IOM, 2009).
As a result, the committee focused many of its recommendations on the fundamental goal of identifying actions that could be taken or supported by the study sponsor, NHLBI, and its potential partners within the U.S. government. As the ultimate recommendation language indicates, many of these actions would also be appropriate for other stakeholders, and many are recommended in the context of collaborative strategies. This relative emphasis on the U.S. government as a key target for the report’s messages does not reflect a judgment on the part of the committee that the needed worldwide actions should be centered in the United States, but simply reflects an emphasis on the logical primary and receptive audience for a report sponsored by a U.S. government agency and conducted by the U.S. Institute of Medicine. This capacity to convey credible messages to the U.S. government gives this report the potential to have an unprecedented influence compared to prior reports on this topic. This is especially the case given its timely publication during a process of reflection and evolution of U.S. global health priorities, evidenced by the current administration’s emerging Global Health Initiative (U.S. Department of State, 2010).
HISTORICAL CONTEXT
A Growing Focus on Global Health
The past decade has seen increased recognition that the international community must take action to improve the health of all people worldwide. In 1997, the IOM released its report America’s Vital Interest in Global
Health, which emphasized that the United States has a vital and direct stake in the health of people around the globe and that it should increase investments in foreign aid to improve health (IOM, 1997). Since then, the U.S. government has significantly increased its development spending on health. U.S. Agency for International Development (USAID) and U.S. State Department global health program funding grew by 350 percent between 2001 and 2008, and by 2006 health aid made up 23 percent of total U.S. allocable aid (IOM, 2009; OECD, 2008). This pattern of increased funding for global health by the United States can be expected to continue for the next 6 years as President Obama requested that Congress allocate $63 billion to global health between 2009 and 2014 for his new Global Health Initiative (U.S. Department of State, 2010). At the international level, the establishment of the Global Fund to Fight AIDS, Tuberculosis and Malaria; the Global Alliance for Vaccines and Immunizations; and the Millennium Development Goals were examples of important steps in bringing global health issues to the forefront. Finally, the establishment of major private funders such as the Bill & Melinda Gates Foundation and the William J. Clinton Foundation infused significant new capital into the fight against the causes of disease and suffering.
While these new investments and commitments to improving the health of the world’s people were unprecedented and have undoubtedly saved millions of lives, the majority of these efforts have largely ignored CVD and other chronic noncommunicable diseases. This extends to the Millennium Development Goals, in which chronic diseases are not explicitly mentioned and are instead relegated to Millennium Development Goal 6, grouped into the catchall category of “other diseases.”
International Realization of CVD Burden
Although not emphasized in most major global health efforts, the increasing burden of CVD in developing countries was first recognized on the international stage at least as long ago as the first international declaration on CVD in 1956, when India proposed a resolution on CVD and hypertension at the Ninth World Health Assembly (WHO, 1956). The growing burden of chronic diseases was further highlighted by the World Bank’s 1984 report China: Health Sector, which noted the increasing burden of CVD among China’s health challenges (World Bank, 1984). However, evidence of the growing chronic disease burden more broadly in low and middle income countries did not begin to gain significant notice until the early 1990s. At this time, advances in epidemiological methods and metrics as well as more accurate data allowed for novel analyses of worldwide disease burden (Jamison et al., 1993). These analyses shed light on the truly global impact of CVD and other chronic diseases and helped
instigate a number of international reports, declarations, and resolutions calling attention to the growing threat of the global CVD epidemic. These efforts from the past two decades are described briefly here and summarized in Figure 1.1 and Box 1.1.
Documentation of the Disease Burden
One of the first such publications to highlight the global burden of CVD and chronic diseases was the 1993 World Development Report by the World Bank. This report focused on the critical role that investments in health play in international development, also emphasizing the rising burden of chronic diseases in low and middle income countries. The report also introduced the Global Burden of Disease study, which definitively established that chronic diseases are responsible for more deaths worldwide than any other cause (Murray and Lopez, 1996; WHO, 2003b).
As the realization of the true global burden of CVD began to grow among the international public health community, several major reports examined national capacities to implement CVD prevention and treatment programs. These reports, most notably the 1999 World Heart Federation White Book on the Impending Global Pandemic of Cardiovascular Diseases (Achutti et al., 1999) and the 2001 World Health Organization (WHO) Assessment of National Capacity for Noncommunicable Disease Prevention and Control (Alwan et al., 2001), found that the majority of countries did not have chronic disease control policies, programs, funding, or the will to take action. As a result, there was little prevention or control under way.
A series of reports from multilateral organizations further examined the growing burden of CVD and other chronic diseases in developing countries. These included the 2000, 2002, and 2005 World Health Reports and the Global Burden of Disease Reports from 1996, 2006, and 2008 (Lopez and Disease Control Priorities Project, 2006; Murray and Lopez, 1996; WHO, 2000, 2002, 2008b, 2008c). In addition, the 2004 Earth Institute/IC Health Report, which examined the social and macroeconomic impact of the growing CVD epidemic, concluded that the burden of cardiovascular mortality and disability was likely to drastically affect working-age adults in developing countries, leading to substantial reductions in productivity and ensuing economic losses (Leeder et al., 2004).
Taken together, these reports established that CVD is the number one cause of death worldwide, that about 80 percent of these deaths occur in low and middle income countries, that the disease burden will only increase in the coming decades, that it will likely have detrimental economic impacts on low and middle income countries, and that control efforts are not sufficient to address the disease burden. These data and projections forced the realization that the global health agenda must expand beyond infectious
diseases and maternal and child health to include CVD and other chronic diseases. These reports also recognized that global CVD is a complex problem, influenced by interdependent factors that involve many sectors and stakeholders extending far beyond the realm of health and public health systems.
Calls for Action
As the new disease burden data were making the true worldwide toll of CVD increasingly clear, calls for action were issued from a number of sources. In 1998 the IOM released a report titled Control of Cardiovascular Diseases in Developing Countries: Research, Development, and Institutional Strengthening. It offered recommendations to better document the magnitude of cardiovascular disease burden, use case-control studies to develop prevention strategies, address risk factors such as hypertension and tobacco use, evaluate low-cost drug regimens, improve the affordability of care for CVD, build research and development capacity, and develop institutional mechanisms to facilitate CVD prevention and control (IOM, 1998).
In a series of declarations from the International Heart Health Conferences, the cardiovascular community called on multinational organizations, governments, civil society, and communities to take immediate action on CVD prevention and control. The first of these was the Victoria Declaration in 1992, which was subsequently followed by the Catalonia Declaration (released in 1995 with a follow-up in report in 1997), the Singapore Declaration in 1998, the second Victoria Declaration in 2000, the Osaka Declaration in 2001, and most recently the Milan Declaration in 2004 (Advisory Board of the Fifth International Heart Health Conference, 2004; Advisory Board of the First International Conference on Women, Heart Diseases, and Stroke, 2000; Advisory Board of the Fourth International Heart Health Conference, 2001; Advisory Board of the International Heart Health Conference, 1992; Advisory Board of the Second International Heart Health Conference, 1995; Grabowsky et al., 1997; Pearson et al., 1998).
In addition to the declarations of the International Heart Health Conferences, a number of other reports and resolutions highlighted the growing worldwide epidemic of CVD and related chronic diseases and issued additional calls to action for its prevention and control. These included the United Nations (UN) Resolution on Diabetes announced in 2007, the 2008 Sydney Resolution and Sydney Challenge from the Oxford Health Alliance Summit, and the 2009 Kampala Statement (Chronic Disease Summit, 2009; The Sydney Resolution, 2008; United Nations General Assembly, 2006). In
2009, the IOM report The U.S. Commitment to Global Health also recognized the need to apply resources to chronic diseases in the developing world as part of the global health agenda (IOM, 2009).
Taken together, these publications shone a brighter spotlight on the burden of CVD, placed increasing pressure on national governments and the international community, and offered recommendations to tackle the issue of CVD. However, despite these calls for action, implementation of CVD prevention and control programs in developing countries has been slow to materialize.
New Strategies, Policies, and Partnerships
To try to initiate implementation of these calls for action, the international community has begun to take steps to develop strategies and plans for action. While serving as director general of WHO, Gro Harlem Brundtland elevated the treatment and control of chronic diseases to the same level of urgency as infectious diseases. In 1999, Brundtland presented the WHO Executive Board with a draft Global Strategy for the Prevention and Control of Noncommunicable Diseases, which emphasized improving chronic disease surveillance, addressing common risk factors, and improving primary care services worldwide (Brundtland, 1999). This Global Strategy was later discussed at the Fifty-Third World Health Assembly, where the Assembly called on the Director General to continue prioritizing chronic diseases and urged Member States to redouble their noncommunicable disease surveillance, prevention, and control efforts (WHA, 2000).
In 2003, after 5 years of unprecedented negotiation, the Member States of WHO unanimously adopted the Framework Convention on Tobacco Control, the first and only legally binding treaty ever adopted by WHO. This treaty called for the implementation of tobacco reduction strategies and new regulatory policies, and a formal reporting mechanism on progress is being implemented (WHO, 2003a). This was followed by the 2004 WHO Global Strategy on Diet, Physical Activity, and Health as well as the 2007 Grand Challenges in Global Health report in Nature (Daar et al., 2007; WHO, 2004), which outlined research and policy priorities for chronic diseases. The 2008 release of the WHO 2008-2013 Action Plan for the Global Strategy for the Prevention and Control of Noncommunicable Diseases (WHO, 2008a) established a policy framework for action, with specific recommendations for WHO, Member States, and civil society. However, this action plan does not specify who will act on specific recommendations, what resources they need, and to whom governments would be accountable for inaction.
THE CHALLENGES OF TAKING ACTION
As part of its charge, the committee assessed why there has not been more concrete action to address global CVD despite the considerable progress in delineating strategies and policies. One of the challenges is the lack of awareness and understanding of the growing burden of CVD in the developing world. Indeed, the formerly pervasive perspective, expressed by the World Bank in 1999, was that CVD is a problem that afflicts only the affluent, that addressing CVD does not need to be on the health agenda for nonindustrialized nations, and that resources dedicated to CVD would potentially serve to increase the gap between the rich and poor (Gwatkin and Guillot, 1999). However, because of the intense efforts described above to more accurately document and draw attention to the economic and health burden of CVD, this misperception has been recognized and is beginning to be reversed. Indeed, the past declarations and recent global strategies provide a welcome sign that the international community is more aware of the importance of CVD and chronic diseases. This was demonstrated by the very different perspective articulated more recently by the World Bank (2007), which recognized the very real effects of chronic diseases on the poor and in developing countries and acknowledged chronic noncommunicable diseases as a development priority. As a result of the significant progress in raising awareness among major global health stakeholders, this report has the advantage of being released in a climate of greater receptivity to its messages than previous documents. Nevertheless, there remains a gap between the burden of disease and the level of awareness, and this report offers an additional tool to further equip those working in this field to continue their laudable efforts to increase attention to the problem.
In addition, even with an increasing recognition by the global health community of the health and economic burden of CVD in the developing world, there remain significant barriers to effective action. These barriers include the perception of CVD as a competitor to other health needs, causing it to remain a low priority and resulting in a lack of financial, individual, and institutional resources; insufficient capacity to meet CVD needs, including health workforce and infrastructure capacity as well as implementation and enforcement capacity for policies and regulatory approaches; insufficient knowledge of the effectiveness and feasibility of programs and policies in contexts similar to those in which they need to be implemented; a high degree of fragmentation of efforts by various players; and a lack of clear leadership and collaboration focused on defined goals and outcomes.
Although the prevailing attitudes about the importance of CVD are changing, both global health funders and national governments of low and middle income countries have yet to elevate action to address CVD as a pri-
ority. This is in part because of very important and legitimate high-priority development needs, as outlined in the Millennium Development Goals. Global health and development stakeholders and national governments in the developing world face very real and critical challenges that remain far from adequately addressed in the areas of poverty and hunger reduction, basic development priorities, and a range of health issues in areas such as infectious disease and maternal and child health.
This report is timely in its publication during a period of serious discussions among most stakeholders revisiting the priorities of the global health agenda. However, the realities of competing priorities persist. Therefore, the committee felt that the current climate of both transition and greater receptivity to chronic disease needs can best be converted into action by identifying opportunities to invest in the components of solutions for global CVD that are best aligned with the existing primary missions and developing strategic approaches of global health stakeholders. With this in mind, the report advances the issue of the global epidemic of cardiovascular disease by focusing less on an independent call for action to address CVD, but rather on identifying entry points for CVD to be a part of the current and future global health agenda as it continues to evolve.
Thus, rather than competing against existing priorities, leaders in the CVD community need to better communicate the importance of integrating attention to CVD within these priorities to policy and decision makers. Better alignment among these priorities has the potential to synergistically improve economic and health status. Furthermore, this can help ensure that current and future health and development efforts do not inadvertently worsen the growing epidemic of chronic diseases. Without a new approach that includes chronic diseases, the health dividend gained from progress in other areas of global health could be squandered as one set of problems is tackled while a new set is allowed to grow.
Recognizing the importance of including CVD in the development and global health agendas of international stakeholders and national governments in low and middle income countries is a crucial factor in increasing the allocation of resources that can be applied to chronic noncommunicable diseases. However, more resources alone will not solve the problem of the growing epidemic of CVD. There is a need for progress and increased capacity at the policy, institutional, and research levels so that CVD prevention and control can be implemented in developing countries.
There is also a gap in knowledge about how to transfer the considerable body of knowledge on etiology and modifiable risk factors into feasible large-scale efforts within the context-specific needs of developing countries. The epidemiological evidence is strong, but evidence for specific interventions implemented in low and middle income countries showing the benefits of improving CVD outcomes, or even in changing risk factors, is largely
unavailable. This gap within the field of global CVD presents an additional barrier to action and is a critical area to tackle in order to have the capacity to act as the previously described barriers of political will and lack of resources are overcome.
Therefore, to fill this knowledge gap and thus to effectively prevent and control CVD in the developing world, there is a need for an increased focus on policy research, health systems research, and implementation research to provide the necessary knowledge to solve the challenges associated with intervention programs, workforce capacity, and other needs. This research will further help ensure that health and public health systems can deliver interventions at clinical, community, and population levels. It is imperative that the results of research be transformed into effective disease control programs, and that best practices from communities that have had a head start on tackling the CVD epidemic be more effectively evaluated and adapted for implementation. Lessons learned in controlling infectious diseases also need to be applied for the purpose of bringing down rates of CVD. The current emphasis in the global health community on developing health systems capacity also provides a window of opportunity to improve capacity for delivery of preventive and therapeutic care for chronic diseases. In addition, policies in nonhealth sectors of government and the private sector need to be developed synergistically to reduce, or at least not adversely affect, risk for CVD.
Finally, the stakeholders and global partnerships that are emerging to tackle CVD need to be more effectively marshaled and coordinated to support the implementation of actions to address the problem. Many players share the responsibility to address CVD. They include international, regional, national, and local players. While different stakeholders will have different relative strengths and different appropriate contributions to a worldwide effort to address the rising disease burden, each player that commits to taking action has in common the need to plan strategically as current efforts are continued and expanded or new ones are adopted. The process of translating goals into action is a complex, difficult, and long-term effort that succeeds when groups work together as part of their strategic planning and implementation of efforts. It would not be practical, efficient, or effective for a single mechanism of coordination to govern all actions to reduce the global burden of disease. However, sustainable progress on CVD and related chronic diseases can be enhanced if there is greater communication among stakeholders to avoid unnecessary duplication of efforts and if players with complementary functions and goals define shared messages and coordinate better to take decisive action together. Many emerging mechanisms for coordination at global, regional, and national levels can be strengthened to serve this purpose, while new alliances and partnerships can also be sought. Such partnerships have proven highly effective at mobilizing
commitments toward the prevention and treatment of infectious diseases such as AIDS, tuberculosis, malaria, measles, and polio, especially when built on the principles of establishing trust, agreeing on priorities and outcomes, and implementing transparent reporting and monitoring.
A FRAMEWORK FOR ACTION
The ultimate goal in meeting the challenges of CVD in the developing world is to first create environments that promote health and help prevent the acquisition and augmentation of risk. Second is to build systems and implement programs to effectively detect and reduce risk and to manage CVD. The committee has identified several “essential functions” that are required to meet these goals. These include advocacy and leadership at global and national levels, developing policy, program implementation, capacity building, research focusing on evaluating approaches in developing countries that are context specific and culturally relevant, ongoing monitoring and evaluation, and funding. Successfully carrying out these functions will require resources—financial, technical, and human—and the combined efforts of many players over long periods of time.
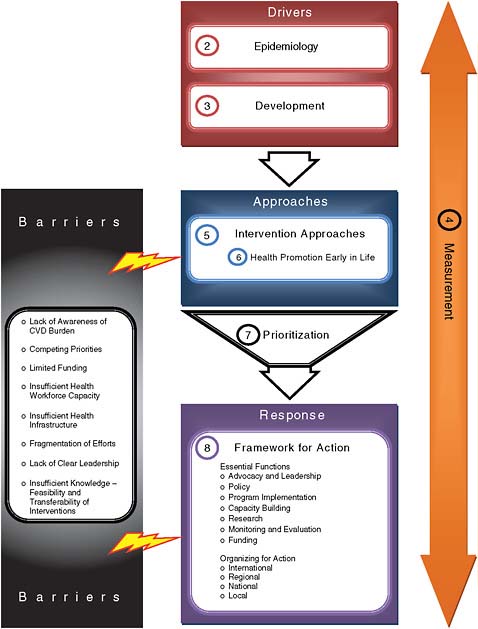
Thus, in response to its charge to offer conclusions and recommendations pertinent to the control of the evolving epidemic of CVD in developing countries, in this report the committee articulates a framework for action to reduce the economic and health burden of CVD and related chronic diseases. As outlined in Figure 1.2, the chapters that follow present the committee’s analysis in support of this framework.
Chapters 2 and 3 describe the determinants of global CVD and its increasing impact, along with related chronic diseases, on the health, welfare, and economies of low and middle income countries, thus providing a clear mandate for action. Chapter 4 describes measurement and evaluation as a fundamental element for the framework and as a means to develop, implement, and sustain effective approaches to reduce the burden of disease. Chapter 5 discusses intervention approaches to reduce the burden of disease, and Chapter 6 more specifically relates the importance of targeting mothers, children, youth, and young adults for prevention interventions in order to achieve long-term success in promoting cardiovascular health and reducing the burden of CVD. Chapter 7 describes the economic analyses that help inform policy decisions about prioritization of investments. Finally, Chapter 8 brings together all the preceding components to describe the essential functions that are needed to address global CVD and how the major stakeholders in CVD, in related chronic diseases, and in global health and development can be organized at global, national, and local levels to create a framework for implementing the necessary actions to control the global epidemic of CVD.
|
|
|
|
|
|
|
|
|
REFERENCES
Abegunde, D. O., C. D. Mathers, T. Adam, M. Ortegon, and K. Strong. 2007. The burden and costs of chronic diseases in low-income and middle-income countries. Lancet 370(9603):1929-1938.
Achutti, A., I. Balaguer-Vintro, A. B. d. Luna, J. Chalmers, A. Chockalingam, E. Farinaro, R. Lauzon, I. Martin, J. G. Papp, A. Postiglione, and K. S. Reddy. 1999. The world heart federation’s white book: Impending global pandemic of cardiovascular diseases: Challenges and opportunities for the prevention and control of cardiovascular diseases in developing countries and economies in transition. Edited by A. Chockalingam and I. Balaguer-Vintro. Spain: Prous Science.
Advisory Board of the Fifth International Heart Health Conference. 2004. The Milan Declaration: Positioning technology to serve global heart health. http://www.internationalhearthealth.org/Publications/milan_declaration.pdf (accessed February 5, 2009).
Advisory Board of the First International Conference on Women, Heart Diseases, and Stroke. 2000. The 2000 Victoria Declaration—women, heart disease and stroke: Science and policy in action. http://www.internationalhearthealth.org/Publications/victoria_eng_2000.pdf (accessed February 5, 2009).
Advisory Board of the Fourth International Heart Health Conference. 2001. The Osaka Declaration: Health, economics and political action: Stemming the global tide of cardiovascular disease. http://www.internationalhearthealth.org/Publications/Osaka2001.pdf (accessed February 5, 2009).
Advisory Board of the International Heart Health Conference. 1992. The Victoria Declaration on Heart Health. http://www.internationalhearthealth.org/Publications/victoria_eng_1992.pdf (accessed February 5, 2009).
Advisory Board of the Second International Heart Health Conference. 1995. The Catalonia Declaration: Investing in heart health. http://www.internationalhearthealth.org/Publications/catalonia1995.pdf (accessed February 5, 2009).
Alwan, A. D., David Maclean, and Ahmed Mandil. 2001. Assessment of national capacity for noncommunicable disease prevention and control: The report of a global survey. Geneva: World Health Organization.
Asaria, P., D. Chisholm, C. Mathers, M. Ezzati, and R. Beaglehole. 2007. Chronic disease prevention: Health effects and financial costs of strategies to reduce salt intake and control tobacco use. Lancet 370(9604):2044-2053.
Beaglehole, R., S. Ebrahim, S. Reddy, J. Voute, and S. Leeder. 2007. Prevention of chronic diseases: A call to action. Lancet 370(9605):2152-2157.
Brundtland, G. H. 1999. Global strategy for the prevention and control of noncommunicable diseases: Report by the director-general. Geneva: World Health Organization.
Chronic Diseases Summit. 2009. Kampala statement: Preparing communities: Chronic diseases in Africa and Asia. Kampala, Uganda.
CSDH (WHO Commission on Social Determinants of Health). 2008. Closing the gap in a generation: Health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. Geneva: World Health Organization.
Daar, A. S., P. A. Singer, D. L. Persad, S. K. Pramming, D. R. Matthews, R. Beaglehole, A. Bernstein, L. K. Borysiewicz, S. Colagiuri, N. Ganguly, R. I. Glass, D. T. Finegood, J. Koplan, E. G. Nabel, G. Sarna, N. Sarrafzadegan, R. Smith, D. Yach, and J. Bell. 2007. Grand challenges in chronic non-communicable diseases. Nature 450(7169):494-496.
Epping-Jordan, J. E., G. Galea, C. Tukuitonga, and R. Beaglehole. 2005. Preventing chronic diseases: Taking stepwise action. Lancet 366(9497):1667-1671.
Fuster, V., and J. Voûte. 2005. MDGs: Chronic diseases are not on the agenda. Lancet 366(9496):1512-1514.
Gaziano, T. A., G. Galea, and K. S. Reddy. 2007. Scaling up interventions for chronic disease prevention: The evidence. Lancet 370(9603):1939-1946.
Grabowsky, T. A., J. W. Farquhar, K. R. Sunnarborg, V. S. Bales, and Stanford University School of Medicine. 1997. Worldwide efforts to improve heart health: A follow-up to the Catalonia Declaration—selected program descriptions. http://www.international hearthealth.org/Publications/catalonia.pdf (accessed February 5, 2009).
Gwatkin, D. R., and M. Guillot. 1999. The burden of disease among the global poor: Current situation, future trends, and implications for strategy. Washington, DC: World Bank.
Horton, R. 2005. The neglected epidemic of chronic disease. Lancet 366(9496):1514.
Horton, R. 2007. Chronic diseases: The case for urgent global action. Lancet 370(9603): 1881-1882.
IOM (Institute of Medicine). 1997. America’s vital interest in global health: Protecting our people, enhancing our economy, and advancing our international interests. Washington, DC: National Academy Press.
IOM. 1998. Control of cardiovascular diseases in developing countries. Washington, DC: National Academy Press.
IOM. 2009. The U.S. commitment to global health: Recommendations for the new administration. Washington, DC: The National Academies Press.
Jamison, D. T., H. W. Mosley, A. R. Measham, and J. L. Bobadilla, eds. 1993. Disease control priorities in developing countries. 1st ed. New York: Oxford University Press.
Jamison, D. T., J. G. Breman, A. R. Measham, G. Alleyne, M. Claeson, D. B. Evans, P. Jha, A. Mills, and P. Musgrove, eds. 2006. Disease control priorities in developing countries. 2nd ed. New York: Oxford University Press.
Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. 2003. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Bethesda, MD: National Heart, Lung, and Blood Institute, NIH, HHS.
Leeder, S., S. Raymond, and H. Greenberg. 2004. A race against time: The challenge of cardiovascular disease in developing economies. Edited by The Earth Institute. New York: Trustees of Columbia University.
Lim, S. S., T. A. Gaziano, E. Gakidou, K. S. Reddy, F. Farzadfar, R. Lozano, and A. Rodgers. 2007. Prevention of cardiovascular disease in high-risk individuals in low-income and middle-income countries: Health effects and costs. Lancet 370(9604):2054-2062.
Lopez, A. D., and Disease Control Priorities Project. 2006. Global burden of disease and risk factors. Oxford University Press; Washington, DC: World Bank.
Muna, W. F. T. 1993. Cardiovascular disorders in Africa. World Health Statistics Quarterly 46(2):125-133.
Murray, C. J. L., and A. D. Lopez, ed. 1996. The global burden of disease. Cambridge, MA: Harvard University Press.
Murray, C. J. L., A. D. Lopez, World Health Organization, World Bank, and Harvard School of Public Health. 1996. The global burden of disease: A comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020, Summary. Geneva: World Health Organization.
Nabel, E. G. 2009. Sponsor perspective on institute of medicine committee on preventing the global epidemic of cardiovascular disease. Presentation at the Public Information Gathering Session for the Institute of Medicine Committee on Preventing the Global Epidemic of Cardiovascular Disease, Washington, DC.
OECD (Organisation for Economic Co-operation and Development). 2008. Measuring aid to health. Paris, France: OECD.
Pearson, T. A., V. S. Bales, L. Blair, S. C. Emmanuel, J. W. Farquhar, L. P. Low, L. J. MacGregor, D. R. MacLean, B. O’Connor, H. Pardell, and A. Petrasovits. 1998. The Singapore Declaration: Forging the will for heart health in the next millennium. CVD Prevention 1(3):182-199.
Reddy, K. S., B. Shah, C. Varghese, and A. Ramadoss. 2005. Responding to the threat of chronic diseases in India. Lancet 366(9498):1744-1749.
Strong, K., C. Mathers, S. Leeder, and R. Beaglehole. 2005. Preventing chronic diseases: How many lives can we save? Lancet 366(9496):1578-1582.
The Sydney Resolution. 2008. Paper read at Oxford Health Alliance 2008 Summit, Syndey Australia.
United Nations General Assembly. 2006. Resolution adopted by the General Assembly: World Diabetes Day. Sixty-first session.
U.S. Department of State. 2010. Implementation of the global health initiative: Consultation document. Washington, DC: U.S. Department of State.
Wang, L., L. Kong, F. Wu, Y. Bai, and R. Burton. 2005. Preventing chronic diseases in China. Lancet 366(9499):1821-1824.
WHA (World Health Assembly). 2000. Prevention and control of noncommunicable diseases. Geneva: World Health Organization.
WHO (World Health Organization). 1956. Cardiovascular diseases and hypertension. In Program of the ninth World Health Assembly. Geneva: World Health Organization.
WHO. 2000. The world health report 2000—health systems: Improving performance. Geneva: World Health Organization.
WHO. 2002. The world health report 2002—reducing risks, promoting healthy life. Geneva: World Health Organization.
WHO. 2003a. WHO framework convention on tobacco control. Geneva: World Health Organization.
WHO. 2003b. The world health report: 2003: Shaping the future. Geneva: World Health Organization.
WHO. 2004. Global strategy on diet, physical activity and health. Geneva: World Health Organization.
WHO. 2005a. Preventing chronic diseases: A vital investment. http://www.who.int/chp/chronic_disease_report/full_report.pdf (accessed April 23, 2009).
WHO. 2005b. The world health report 2005—make every mother and child count. Geneva: World Health Organization.
WHO. 2008a. 2008-2013 action plan for the global strategy for the prevention and control of noncommunicable diseases. Geneva: World Health Organization.
WHO. 2008b. The global burden of disease: 2004 update. Geneva: World Health Organization.
WHO. 2008c. The world health report 2008—primary health care: now more than ever. Geneva: World Health Organization.
WHO. 2010. WHO framework convention on tobacco control. http://www.who.int/fctc/en/ (accessed May 26, 2010).
WHO Study Group on Rheumatic Fever and Rheumatic Heart Disease, and WHO. 2004. Rheumatic fever and rheumatic heart disease: Report of a WHO expert consultation, Geneva, 20 October-1 November 2001, World Health Organization technical report series. Geneva: World Health Organization.
World Bank. 1984. China: The health sector. Washington, DC: World Bank.
World Bank. 1993. World development report 1993: Investing in health. New York: Oxford University Press.
World Bank. 2006. Disease control priorities project. http://www.dcp2.org/main/Home.html (accessed May 26, 2010).
World Bank. 2007. World development report 2007. Washington, DC: World Bank.
Yach, D., and C. Hawkes. 2004 (unpublished). Towards a WHO long-term strategy for prevention and control of leading chronic diseases. Geneva: World Health Organization.






























