
A Century of American Narcotic Policy
David T. Courtwright
American narcotic policy has been highly variable, having passed through at least four major stages during the past 100 years. In the nineteenth and early twentieth centuries, government involvement was minimal. Drug use was largely a private matter, as was drug treatment. Addiction was understood as either a personal or a medical problem, and various treatments were provided on a fee-for-service basis. In 1909-1923, however, the federal government became progressively more involved in the field as a series of important laws, court cases, and administrative decisions effectively criminalized nonmedical narcotic use and proscribed certain treatments, notably long-term maintenance and ambulatory detoxification. The following four decades, from 1923 to 1965, might be described as the classic era of narcotic control—"classic" in the sense of simple, consistent, and rigid. Few avenues of treatment were open to addicts, and American narcotic policy was unprecedentedly strict and punitive, both in comparison with other Western countries and with what it has become in our own time. During the 1960s the police approach was challenged and gradually superseded by a hybrid approach, combining traditional law enforcement with new treatment strategies, including methadone maintenance and therapeutic communities. Since 1965 drug abuse has been regarded as a medico-criminal problem, the likely pattern of the future, although there are signs that the pendulum is beginning to swing back in the direction of strict law enforcement.
The following narrative history of these events is based on written primary and secondary sources, as well as oral history interviews with former addicts, physicians, and police personnel.1 A good deal of attention is paid to the changing epidemiology and sociology of narcotic abuse because the changes in government policy (and hence in the array of
David T. Courtwright is professor and chair of the Department of History, University of North Florida, and a member of the Committee for the Substance Abuse Coverage Study.
medical treatments available) are unintelligible without knowledge of the changing demographic and social backgrounds of the users themselves. Although this narrative focuses primarily on opiate and cocaine addiction and treatment, there is also a brief discussion of other drugs, especially alcohol. Often told separately, the histories of drug and alcohol use in America are in fact intertwined, perhaps never more so than in the last decade.
THE SOCIAL AND LEGISLATIVE ORIGINS OF NARCOTIC CONTROL
During the nineteenth century there was virtually no effective regulation of narcotics in the United States. Various preparations and derivatives of opium were freely available and widely used. Several states had statutes governing the sale of narcotics, and many municipalities forbade opium smoking, but these laws were only sporadically enforced. In practice just about anyone could secure pure drugs with little bother and at modest cost. Pharmacists even delivered drugs, dispatching messenger boys with vials of morphine to houses of high and low repute. Some customers were actually unaware of what they were purchasing: proprietors of patent medicines were notorious for slipping narcotics into their products, which before 1906 bore no list of ingredients on their labels. Doctors, too, frequently overprescribed narcotics. Opiates were among the few effective drugs they possessed, and it was tempting to alleviate the symptoms (and thus continue the patronage) of their patients, especially those who were chronically ill.
The result of all this was a narcotic problem of considerable dimensions, with perhaps as many as 300,000 opiate addicts at the turn of the century, plus an unknown number of irregular users.2 Today there are perhaps as many as 500,000 narcotic (mainly heroin) addicts in the United States, but the country's population is also much larger. On a per capita basis, narcotic abuse was certainly as bad and probably worse in the late nineteenth century.
Victorian Americans were much less worried about drugs, however, than they were about drink. An influential reform coalition, consisting mainly of native-born, white, middle-class Protestants, attacked alcohol as the principal source of social problems. Drinking was wrong because it led to drunkenness, and drunkenness led to battered wives, abandoned children, sexual incontinence, venal voting, pauperism, insanity, early death, and eternal damnation. Drinking was also objectionable because it was associated with groups whose morality was highly suspect: Catholic immigrants, machine politicians, urban blacks, demimondaines, criminals,
tramps, casual laborers, and others of the lower strata. Reformers sought to uplift and reform drunkards, but they were also frank in their desire to control their behavior and to minimize the social costs they generated. The more ardent among them fought for and achieved prohibition, first on a local and state level, and then, in January 1920, on a national basis.
Given the prevalence of narcotic use, why were Americans initially so much more agitated over the drink question? One answer lies in the comparative effects of opiates and alcohol. It was a commonplace that drink maddened whereas opium soothed. Alcoholics were notoriously obstreperous and often injured others as well as themselves. Their behavior was a public nuisance and a scandal. Addicts, by contrast, tended to be quiet and withdrawn. Although they might merit reprehension for their enslavement to a drug, theirs was a private vice, unlikely to affect anyone outside their immediate family—and in some cases even the family did not know. These distinctions were grounded in pharmacological reality, insofar as narcotics are potent tranquilizers, capable of producing a pacific and languid state. It is easier for an addict to remain inconspicuous than a drunkard.
Who the narcotic users were was as important as how they acted. There was what might be termed a "hard core" of opium smokers, mainly Chinese laborers and white criminals; they were contemptuously regarded and likely to run afoul of the law. Opium smokers, however, made up only a minority of regular users. Addicts were more often found among upper-and middle-class women, many of whom had begun using morphine to relieve the symptoms of various illnesses. Surveys taken in the late nineteenth century consistently showed that two-thirds of those addicted to medicinal opiates, such as laudanum or morphine sulfate, were female. Given that so many addicts were respectable women of ailing body and docile comportment, it is understandable that they occasioned less alarm than heavy drinkers.
Narcotic addiction was not entirely ignored by the medical profession. As the number of addicts grew in the 1870s and 1880s, some physicians began to specialize in treating addiction and to develop theories about it. They debated its etiology; whether it, along with alcoholism, was symptomatic of a more general neurological disorder; whether gradual or rapid withdrawal was to be preferred; whether withdrawal could or should be palliated with nonnarcotic drugs and, if so, which ones. A hundred years later, most of these issues are still not completely resolved.
Nineteenth-century physicians interested in addiction were handicapped by the embryonic state of medical science—they knew nothing of drug receptors or endorphins or narcotic antagonists—but they did have at least one advantage over modern researchers: almost total freedom. There were no federal regulations and no bureaucracy to deal with;
moreover, medical institutions, such as they were, largely steered clear of the problem. Doctors were thus at liberty to experiment, to prescribe purges, baths, electric therapy, dietary regimens, and various exotic concoctions for their addicted patients. Many of the leading authorities in the field operated private asylums where treatment was tailored to their particular theories of addiction.
Addicts, too, had a fair amount of choice. They could stay at one of the private asylums or attempt withdrawal as an outpatient under the supervision of a physician. Some bought ''opium habit cures,'' patent medicines that were often laced with narcotics and hence no cure at all. Or they could do nothing and simply continue to use undisguised narcotics. Few addicts were legally committed to institutional treatment. When they made an effort to quit, it was generally motivated by a sense of disgust, combined with health and financial worries and pressure from family and friends. Addicts, in short, were far less likely than alcoholics to be involuntarily confined.
A handful of late-nineteenth-century medical specialists saw addicts in a less benign light. They argued that addiction and alcoholism were in fact related, that both were a manifestation of an underlying nervous disorder called inebriety, and that "inebriates" needed institutional care, against their wills if necessary. They failed, however, to carry this last point. The public thought of addiction as neither a crime nor a fit object for mandatory treatment. Whatever resentment existed against addicts was diffuse and lacked institutional expression.
Within 25 years these attitudes had dramatically changed. Even as the country was having second thoughts about alcohol prohibition, there was virtual consensus on the need to suppress narcotic addiction. (Some extremists in the 1920s and 1930s even proposed firing squads as a permanent solution for the drug problem, on the theory that the only abstinent addict was a dead one.) This pronounced attitudinal shift was related to changing perceptions of who drug addicts were, how they acquired their habits, and how they behaved under the influence of drugs. After the turn of the century there were fewer new cases of medical addiction as physicians became more conservative in their use of narcotics and the public became more chary of self-medication, thanks to the Pure Food and Drug Act (1906) and the efforts of muckrakers like Samuel Hopkins Adams. Some existing medical addicts detoxified and remained abstinent, but the majority probably continued using morphine. Because many of them were old and ailing, however, they soon disappeared from the scene, leaving a residue of generally younger, less sympathetic users who had begun experimenting with drugs in such decidedly nonmedical establishments as brothels and saloons.
Opium smoking remained popular in the white underworld and continued to attract recruits, even though the number of Chinese living in America had begun to decline. Two powerful new drugs, cocaine and heroin, quickly spread outside medical practice and became popular euphorigenic agents. Cocaine, although not pharmacologically a narcotic, was often described as such and became associated in the public mind with crime sprees, particularly by black men. In the 1910s and early 1920s heroin use became widespread in the immigrant slums, where young men took to snorting small packets of the white powder. For some it was a passing fancy, but for others it became a lifelong preoccupation. In 1924 New York City Corrections Commissioner Frederick A. Wallis described what he took to be a typical case:
The young man, 16 to 20, leaves school because he won't study, he doesn't like discipline, and shows inclination toward truancy and dishonesty.
Out of school, his bad habits increase. He visits pool-rooms and dance halls, and chop suey restaurants and becomes one of the neighborhood rowdies or corner loafers. He goes with a gang and becomes reckless and is soon participating with the gang in neighborhood thefts. If he has a job, it becomes burdensome, and offensive to him. He then neglects his work, loses his job, and all his ambitions are in sympathy with criminal tendencies.
He is arrested first for a minor offense, spends five to ten days in prison, loses self-respect, is released and returns to society with less regard for law and constitutional authority. . . .
Having served a term in prison, he is now qualified by the gang for exploits in the underworld. . . . He soon learns. . . the easiest and most profitable way to get money with less personal hazard to himself and a lighter prison sentence, [and he] becomes a drug peddler and distributor. Before he realizes the danger he has been taught to use the drug. Soon he must have the drug at any price.
He resorts to shoplifting and indulges in other petty offenses to obtain the drug. The next step is prison again, and he returns to society again, and then is arrested for a more serious crime. The craving for drugs is growing all the time. He must have more drugs. The requirement of $2.00 a day has grown into $5.00 or $10.00 a day. In his intensified craving he becomes a bandit, a hold-up man, murder follows. A wreck, mentally, physically and morally, he is given a life sentence or the electric chair.3
What is particularly interesting about this account is its harsh, judgmental tone. It was not just that the old-fashioned medical addicts were disappearing and being replaced by a new breed, it was how people felt about it. As had been the case with alcohol, disdain for users, tinged by
ethnic and class prejudice, was an impetus for restrictive legislation. Change a very few words in Wallis's description and one finds the old stereotype of the drunkard as a menacing, irresponsible wretch.
Addiction thus went from being a pathetic condition to a stigmatized one. Like venereal disease, it came to be understood as something that was acquired through forbidden indulgence with evil associates. Also like venereal disease, it could afflict, or destroy, the lives of innocent others—the spouse, the family, the fetus, or the newborn child. Both diseases were, in a broad sense, communicable: addicts (and venereal patients) were alarming, not only because they had gotten themselves in trouble but because they might put others in the same situation. After inadvertent medical addiction ceased to be much of a factor, it was clear that the majority of new users were introduced to drugs by and often became part of a network of experienced users and dealers. A deviant subculture was in place and perpetuated itself through continuous recruiting.
Deviant groups in American history have sometimes been dealt with by informal, local means—harassment, exile, even lynching. But when such groups become large enough, or threatening enough, they often evoke a legislative response. The resultant laws serve a dual purpose. They are symbolic in that they define and reiterate majority norms; they are also instrumental to the extent that they employ the police power of the state to restrict or eliminate the objectionable behavior. There have been many instances of this, from the 1675 Massachusetts law attacking the "damnable haeresies" of the Quakers to the 1940 Smith Act, which was used to prosecute domestic communists and Nazi sympathizers. Narcotic control seems to fit neatly into this pattern. As the legal scholars Richard Bonnie and Charles Whitebread put it, "Once opiate use became identified with otherwise immoral or unliked populations, prohibition was almost automatic."4
The word "almost" must be stressed, however. The negative social and behavioral connotations surrounding nonmedical narcotic use were not, in any meaningful historical sense, a sufficient cause of the ensuing prohibition and criminalization. There was still room for the play of expert judgment and legislative discretion, and it is well known that contemporaries in other developed countries, such as Britain, arrived at less Draconian solutions. It is fair to say, however, that the sinister transmogrification of narcotic addiction was a critical precondition for the legal developments that followed. It would have made no sense—politically, culturally, morally, or in any other way—to repress addicts if they had still consisted disproportionately of sick old women. Even after the laws were changed, physicians and law enforcement officers often tacitly permitted the dwindling number of iatrogenic addicts to continue their "medication."
Being ill, these patients were sympathetic figures and, because they were isolated from the street drug subculture, posed no threat to anyone.
The transformation of American narcotic laws, like the transformation of the addict population itself, evolved over a period of time. The catalytic event was America's growing involvement in Asia, a region long notorious for its opium trade. American military governors in the recently acquired Philippines, missionaries in China, and diplomats studied the problem and sought to coordinate international efforts to eliminate or reduce the traffic. As a result of their efforts an international opium commission met at Shanghai in February 1909. The American delegation, anxious to assume a leadership role but fearful that the laissez-faire narcotic market at home left them open to charges of hypocrisy, pressed for at least token congressional legislation. This they received in the form of a hastily enacted law forbidding the importation of opium "for other than medicinal purposes," that is, opium for smoking. Banning this form of the drug cost the federal government more than $800,000 in annual revenues, but it was politically feasible because opium smoking had such low-life connotations and few American firms had a large stake in its continued importation.
Reformers were not satisfied with this one measure, however. They continued to work for a more comprehensive narcotic law, both to address the domestic problem and to bring the country into line with the provisions of an international treaty then being negotiated. Their most forceful advocate was Dr. Hamilton Wright, American delegate to the Shanghai Commission and later the Hague Opium Conference (1911-1912). Wright compiled an official report for Congress, complete with authoritative references to drug-inspired rape and miscegenation, as well as statistics that seemed to show that narcotic use was outstripping population growth. (In fact it was not; per capita consumption was down after 1900, largely owing to increased therapeutic conservatism.)
Wright also played up the prevalence of lower-class and criminal use, as may be seen from his specific addiction estimates in Table 1. The percentages reproduced here are as unfounded as they are pretentious: Wright's research was highly unsystematic and hardly merited numerical expression, let alone two-and three-decimal-point precision.5 He was, however, magnifying an epidemiological reality: by 1910 criminals and prostitutes did have much higher rates of use than the general adult population and possibly (although this is not certain) higher rates than medical personnel, who historically had a serious addiction problem. Wright was, moreover, believed. His statements and statistics were given wide circulation in the popular press, medical journals, congressional committee reports, and other official documents.
Despite his skills as a propagandist, Wright got a bill neither as soon
TABLE 1 Opiate Addiction Estimates for Various Groups in the United States Made by Hamilton Wright in 1910
|
Group |
Percentage Addicted |
|
General criminal population |
45.48 |
|
Chinese |
25.0a |
|
Prostitutes and their companions |
21.6 |
|
Prisoners in large jails and state prisonsb |
6.0 |
|
Medical profession |
2.06 |
|
Trained nurses |
1.32 |
|
Other professional classes |
0.684 |
|
General adult populationc |
0.18 |
|
College and university students |
"practically unknown" |
|
a percentage estimate includes those who smoked a pound-and-a-half or more per annum but excludes "social smokers." b As distinct from the "general criminal population," which committed lesser crimes and hence ended up in local jails rather than large or state institutions. c Exclusive of the groups enumerated above. Source: U.S. Senate, Report on the International Opium Commission and on the Opium Problems as Seen Within the United States and Its Possession (Washington, D.C.: U.S. Government Printing Office, 1910), pp. 42, 47. |
|
as nor as stringent as he wanted. He ran into opposition, especially from drug companies that did a large wholesale business in narcotics. He also encountered philosophical and constitutional difficulties, as the limits or even the existence of a federal police power were not then generally agreed upon. (Indeed, in 1918 and again in 1922 the Supreme Court would strike down something as seemingly proper and desirable as federal child labor laws.) The regulation of medical practice was a matter traditionally left to the states, and narcotics were still very much a part of medical practice.
The measure that finally passed, the Harrison Narcotic Act of 1914, was a complex compromise. It required anyone who sold or distributed narcotics—importers, manufacturers, wholesale and retail druggists, and physicians—to register with the government and to pay a small tax.6 When they sold or otherwise distributed narcotics, they had to make a detailed record of the transaction, open to government inspection. Unregistered persons caught with narcotics in their possession were presumptively guilty of violating the law, unless the drugs had been "prescribed in good faith by a physician, dentist, or veterinary surgeon registered under this Act." If convicted, they could be fined and imprisoned for up to five years. It was anticipated that such sanctions would make the narcotic traffic transparent and confine it to legitimate medical channels.
Two features of the Harrison Act are of particular interest. One is the definition of narcotics as opium-and coca-based drugs. As previously noted, opium and coca are medicinally distinct. One is a central nervous system depressant, the other a stimulant. They were combined legislatively, however, because of the assumption that both were euphorigenic, potentially habit-forming, and associated with crime. It was for similar reasons that marijuana would also later be described as a narcotic.7
The second point is the law's failure to address the question of whether an addict could receive, on an indefinite basis, a prescribed supply of narcotics. In retrospect, this was one of the most crucial lacunae in any federal statute enacted in the twentieth century. The Treasury Department officials who administered the law assumed a negative stance and initiated several prosecutions against addicts, physicians, and pharmacists for conspiracy to violate the Harrison Act. At first the Supreme Court rebuked the Treasury Department for attempting to stop physicians from prescribing for addicts; ultimately, however, it reversed itself and narrowly ruled in favor of the antimaintenance position. In two cases decided March 3, 1919, the Court sustained the constitutionality of the Harrison Act and ruled that a physician might not write prescriptions for an addict "to keep him comfortable by maintaining his customary use."
The circumstances of these cases, United States v. Doremus and Webb et al. v. United States, are revealing. Doremus was a physician who prescribed, for a price, large quantities of heroin to one Alexander Ameris,
alias Myers, who was "addicted to the use of the drug as a habit, being a person popularly known as a 'dope fiend'."8 Ameris's ethnic surname, use of heroin, and large habit were all negatives, summed up in the epithet "dope fiend." Dr. Webb was similarly accused of gross overprescription; before he was arrested he averaged more than 80 morphine prescriptions a week, at 50 cents apiece. Government attorneys decried such unprofessional behavior, likening it to a barkeeper dispensing whiskey to a drunkard.9 Five members of the Court agreed, and Webb's original conviction was upheld. Had either case involved only small amounts of narcotics prescribed by a reputable physician, it is highly likely that the decision would have gone the other way. Six years later, in Linder v. United States, the Court unanimously reversed the conviction of a respected Oregon practitioner who had prescribed one tablet of morphine and three tablets of cocaine for a stool-pigeon addict.10
The Prohibition Unit of the Treasury Department nevertheless treated Webb as the governing decision and pursued an aggressive antimaintenance policy. By threats and actual prosecutions they were able to drive a wedge of fear between the legal providers (physicians, pharmacists) and the addicts. Prosecutions of those who supplied addicts might fail, as they had with Dr. Linder—but they might also succeed, as they had with Dr. Webb and numerous others. Even if a defense were successful, the potential legal fees and loss of reputation made a physician think twice before reaching for his prescription pad. Doctors, moreover, were less and less favorably disposed toward nonmedical addicts, whom they perceived as devious, troublesome, and notoriously resistant to cure.
There were, however, some physicians who continued to write prescriptions for addicts, if only on an occasional basis. They were motivated by pity, or greed, or simply by a desire to get the users off their backs and out of town. Even at the height of its powers, the Bureau of Narcotics never completely succeeded in closing off all medical supplies to addicts. A small but significant gray market of pure drugs persisted as an alternative to the black market of adulterated heroin. Some users managed to develop extensive connections in the former and stay out of the latter altogether. Still, medical sources were chancy and could not be counted on indefinitely; doctors who wrote prescriptions too often or too openly were sure to be visited by a federal agent. That fact, as far as addicts were concerned, was the chief legacy of the Harrison Act and the 1919 Supreme Court decisions.
There was one other alternative to the black market, but it was short-lived. Following the Webb ruling, a number of cities and towns set up facilities to dispense narcotics to addicts. If private maintenance were disallowed, then organized, public maintenance might yet take its place. There were altogether 35 of these municipal "narcotic clinics," so named
because they sold morphine cheaply to their registered patients. A few also sold cocaine or heroin. What is sometimes misunderstood about these clinics is that they were not homogeneous, that their methods of operation varied. Some were geared toward indefinite maintenance, others toward detoxification through gradual withdrawal. Some were run for profit, others merely to break even. Some were models of efficient administration, others fly-by-night operations.
One thing, however, they did have in common: all were eventually closed by the federal government, most within a year of opening their doors. Treasury Department officials, determined to eliminate both licit and illicit sources of narcotics for addicts, viewed the clinics as dangerous precedents and potential obstacles to the rigorous enforcement of the Harrison Act, as recently interpreted by the Supreme Court. Consequently, they moved to abort them through a combination of critical inspections, threats, and legal pressure. February 10, 1923, when the last clinic in Shreveport, Louisiana, was finally forced to break off maintenance operations, is as appropriate a date as any to mark the beginning of the "classic" police era of narcotic control.11
The unprecedented nature of federal narcotic policy after 1923 is underscored by the fact that alcoholic beverage prohibition applied only to manufacture and sale. Neither the Eighteenth Amendment nor the law that implemented it, the Volstead Act, barred personal use and consumption by alcoholics or, for that matter, anyone else. National prohibition, moreover, was controversial from the start and lasted only 14 years. Large numbers of apparently normal people continued to drink; they resented both the prices they had to pay for bootlegged alcohol and the prohibitionists who meddled with their customary freedoms. The laws proved virtually unenforceable, as criminals manufactured or diverted alcohol and speakeasies spread across the land. The byproducts of Prohibition-gangsterism, corruption, and methanol poisoning—filled the front pages. Ardent supporters grew disenchanted. Powerful business and opinion leaders such as Pierre du Pont and William Randolph Hearst campaigned for repeal. A well-funded national organization, the Association Against the Prohibition Amendment, maintained a drumfire of criticism and propaganda. The public was told that the noble experiment had backfired and was creating a nation of drunkards. The war against narcotics, by contrast, was thought to be successful in reducing nonmedical addiction and was so portrayed by government officials.12
The onset of depression in 1929 handed the antiprohibitionists a new and decisive argument: money. "If the liquor now sold by bootleggers was legally sold, regulated, and taxed," one writer observed, "the excise income would pay the interest on the entire local and national bonded indebtedness and leave more than $200,000,000 for other urgently needed pur-
poses."13 The Democrats adopted a repeal plank in 1932, and nominee Franklin Roosevelt pledged to the convention that "the 18th Amendment is doomed."14 True to his word, he announced on December 5, 1933, that three-quarters of the states had ratified the Twenty-First Amendment, thereby ending national prohibition.
Virtually no one spoke up for the narcotic user, however; there was no Association Against the Harrison Act. On the contrary, the national champions of repeal, including Hearst and Roosevelt, persisted in seeing drug use as a criminal menace and condoned restrictive measures. One "wet" argument, dating back to the early state prohibition battles, had been that frustrated drinkers would turn to narcotic drugs, which would madden and enslave them.15 Drink was the lesser evil. Hostile toward addicts anyway, it suited the purposes of the antiprohibitionists to maintain them as a negative reference point, the dead end of their ad horrendum stories.
As for the addicts themselves, they were too few and too marginal to carry much political weight. Many of them were convicted felons and thus could not even vote. There was little that they could do about the refusal to allow maintenance, a policy that lasted more than 40 years. When the antimaintenance regime was finally challenged, it was not by the narcotic users but by an elite group of professionals—mainly lawyers, physicians, and social scientists—who had become convinced that it was unjust and unworkable. In attacking the Bureau of Narcotics, they too invoked the alleged failures of Prohibition, arguing that it was useless and counterproductive to outlaw addictive substances. It also seemed a double standard to permit pathogens like alcohol and tobacco, while proscribing "narcotics" of lesser or unproven danger, without which regular users would become violently ill. This was a fair point but, like all rational arguments, it had its limits. There was still a powerful, visceral fear of narcotic addicts and all they stood for. It was the social and moral connotations of narcotic addiction that mattered, not just the mental and physical effects of the drugs themselves.
LIFE UNDER ANSLINGER
The personification of the antinarcotic regime was Harry Jacob Anslinger, head (or, to his critics, "czar") of the Bureau of Narcotics. Anslinger was a minor diplomat who in the 1920s became involved with efforts to prevent liquor from being smuggled into the country. He was a competent and honest functionary in a field not known for either trait, and in 1929 he was made assistant commissioner of prohibition. After Levi Nutt, boss of the Prohibition Unit's Narcotic Division was tainted with scandal and demoted, Anslinger took his place. When the Bureau of
Narcotics was spun off as a distinct organization in 1930—partly to distance it from the furor over alcohol prohibition—Anslinger was named its first commissioner, a post he retained until 1962.
There was a peculiar, Jekyll-and-Hyde aspect to Anslinger's personality. The private man was humorous, cosmopolitan, fluent in several languages, musically accomplished, devoted to his wife, and loyal to his hometown friends. Anslinger also possessed a keen political intelligence. Like his contemporary Lyndon Johnson, he knew exactly whom to cultivate to advance his interests. Anslinger is remembered, however, not as a man of exceptional gifts or as a deft bureaucrat but as the ultimate tough cop. His appearance—bald, barrel-chested, square-jawed, and unsmiling, a sort of beefy Mussolini—had much to do with this. By all accounts Anslinger was intimidating. One visitor described him as "a man whose eyes seem to be cataloguing you—your features, build, clothes."
When explaining or defending his policies, Anslinger was given to curt aphorisms: "Wherever you find severe penalties, addiction disappears," or "The best cure for addiction? Never let it happen."16 He summed up his basic approach in a similarly brief manner. "We intend to get the killer-pushers and their willing customers out of selling and buying drugs," he said. ''The answer to the problem is simple—get rid of drugs, pushers and users. Period." Interdicting smuggling and jailing dealers made narcotics scarce and expensive; confining addicts made it impossible for them to spread the vice. It was, moreover, their only hope of cure. Unless addicts were confined where there was no possibility of obtaining drugs, Anslinger believed, withdrawal treatment was bound to fail. He strongly favored compulsory commitment and fretted that most states lacked statutes permitting them to pick up addicts and force them into institutions.17
Yet even this was not enough. Anslinger understood that narcotic trafficking was international in scope and required diplomatic efforts as well as strict domestic enforcement. He tirelessly attended meetings sponsored by the League of Nations, seeking agreements that would make it more difficult to smuggle drugs. In 1931, for example, he took an active role in negotiating an international pact to limit the manufacture of narcotics. Nations ratifying the treaty, of which there were 25 by 1933, were to make or import no more narcotics than necessary for estimated annual medical use, thereby reducing the surplus available for diversion into the illicit market.
Like many American diplomats of his generation, Anslinger saw the world in black and white terms. Most nations were good in that they were willing to assist others in the international campaign against the drug evil. There were also bad states, however, that not only refused to cooperate but actually used narcotics as an instrument of subversion and conquest.
At the head of Anslinger's renegade list were Imperial Japan and Communist China. ''Wherever the Japanese Army goes," he charged, "the drug traffic follows. In every territory conquered by the Japanese, a large part of the people become enslaved with drugs." In the 1950s and early 1960s he attacked the leaders of the People's Republic of China, accusing them of narcotic sales to the West to support their invasion of Korea and later of joining with Castro's Cuba to create an illicit drug network. It is not coincidental that all of the bad nations were, at the time Anslinger assailed them, military and ideological rivals of the United States. Narcotic policy dovetailed with foreign policy, a fact that enhanced Anslinger's prestige as well as his bureau's budget.18
The one eventuality that Anslinger had to guard against was the return of legal maintenance. This, he felt, would utterly defeat his plans to keep drugs out of the hands of addicts and their associates. The potential danger was great. The medical profession was enormously powerful and prestigious, having achieved what sociologist Paul Starr has called "sovereign" status by the 1930s. If physicians took seriously the idea that addiction was a disease and that, lacking a sure cure, the most favorable course of treatment was maintenance,19 then they might challenge, and ultimately defeat, the tenuous legal basis for narcotic prohibition. Fortunately for Anslinger, most practitioners were disinclined to rock the boat. Like the public at large, they tended to see drug users, especially heroin addicts and opium smokers, as vicious and declasse. Physicians were in any case oriented toward treating somatic disorders, and the dominant medical opinion of the day declared narcotic addiction to be a manifestation of psychopathology, that is, not a physical disease at all.
The psychopathy thesis was popularized by Dr. Lawrence Kolb, who was regarded as the leading addiction specialist of the mid-twentieth century. Like Anslinger, Kolb thought of addiction treatment as a process of institutionalization, detoxification, rehabilitation, and abstinence. Although Kolb occasionally complained to Anslinger of overly zealous law enforcement, the approaches of the two men were on the whole quite compatible.20
Kolb and his coworkers at the U.S. Public Health Service oversaw two federal narcotic farms at Lexington, Kentucky, and Fort Worth, Texas. With the closure of the municipal narcotic clinics in the early 1920s, there were virtually no government facilities for the treatment of addicts. They either had to remain at large or silt up the nation's prisons, which were ill designed to deal with their problems. The solution proposed by Pennsylvania Representative Stephen G. Porter (and enthusiastically backed by the Hearst newspaper chain) was to construct special facilities to quarantine and rehabilitate addicts. These "narcotic farms" were to be set in rural areas so that addicts could be removed from the tempting cities
and set to healthful work. Money was authorized in 1929. The first narcotic farm, officially known as the U.S. Public Health Service Narcotic Hospital, was completed at Lexington, Kentucky, in 1935. A second narcotic farm was opened in Fort Worth in 1938.
Of the two, Lexington was the larger and more prominent. It was to remain the single most important treatment and research facility in the country well into the 1960s. From the beginning Lexington had a mixed institutional character. Federal prison and narcotic officials saw it mainly as a penitentiary where troublesome addicts could be isolated and confined; Public Health Service physicians saw it as a hospital where mentally disturbed addicts could be treated and rehabilitated. Architecturally, Lexington reflected the official ambivalence: its beds and wards were secured with massive gates and intricate locks. As one doctor remembered it, Lexington was "more like a prison than a hospital and more like a hospital than a prison."
As a dual-purpose institution, Lexington had a dual system of admissions. Prisoner addicts could be sent there involuntarily for confinement and treatment, but voluntary patients were also permitted to check in on a space-available basis. The problem was that volunteers could leave at any time, whereas prisoners had to stay until they were paroled or completed their terms, which might be months or years after withdrawal was completed. The staff, in other words, had little or no control over the time of release.21
The addicts who went to Lexington were of two minds about the place. To some it represented a haven, a clean and well-run institution where a user could detoxify, receive medical and dental care, and obtain counseling, decent food, work, and exercise. "When I would feel bad, or get mentally disgusted," one former user recalled, "I thought to myself, 'What am I doing? I'm a drug addict. I want to quit.' So I'd go to Lexington, and I'd come out feeling like a million dollars." Altogether he went six times. Others viewed this sort of behavior with disdain. "I never went to Lexington," boasted another addict.
You want my honest opinion of the people who went down there on their own? They never should have been on heroin. They didn't have the ability to support a habit: either they couldn't make enough money working, or they weren't thieves, or they were afraid to deal. [Laughs.] We used to tell them, "What are you doing, going down to get rescued?" I doubt if I'm mistaken, but if you'll look it up, you'll find that on average better than 75 percent of the people who went to Lexington on their own repeated. Every time things got bad—boom!—they were back. See, if you go down there once, I can understand it. Even twice, even three times I can understand, if a guy makes some kind of an effort to stay away from heroin when he comes out. But a lot of users go back
to heroin immediately, and then use Lexington as a fall-back, a port in the storm.
The estimate of 75 percent is actually conservative. Several studies showed that 90 percent or more of those released from Lexington soon relapsed. These depressing figures gave rise to a controversy, muted at first but increasingly contentious by the early 1960s. Different theories of relapse were advanced, attributing it to everything from underlying personality disorders to conditioned responses to permanent metabolic changes. Some even argued that addicts returned to drug use because they missed the intense excitement of hustling and scoring drugs; once they were "in the life," everything else seemed boring by comparison.
Whatever the reason, the fact remained that large numbers of patient-inmates speedily relapsed after their release. The Lexington and Forth Worth narcotic farms survived as long as they did largely because they were compatible with official policy. Institutions that were quasi-penal and geared toward abstinence were acceptable to Anslinger, even if they did not produce large numbers of permanent cures. What was not acceptable was any form of organized maintenance, against which he fulminated at every opportunity. Anslinger blamed the rudimentary clinic system of the early 1920s for "a tremendous rise in teen-age drug addiction" and predicted that a return to such folly would increase the narcotic problem nearly 10-fold. Maintenance was also deeply repugnant: "the idea of giving a teenager heroin for the rest of his life is unthinkable. Why not set up bars for alcoholics or department stores for kleptomaniacs or brothels for homosexuals." "You know, there are so many experts in drug addiction," he complained in 1957, ''that I think if we made a survey we would find more experts than addicts."22 Anslinger appealed to the conservatism and anti-intellectualism of ordinary Americans, and also to their nativist and racial fears. He relied on the antinarcotic consensus to help him in his long, preemptive battle against maintenance; he was abetted by reporters, editorialists, political cartoonists, and filmmakers, who consistently portrayed narcotic traffickers as murderous villains. Again and again, Americans were told that the role of the government was to eliminate peddlers, not to assume their role.23
MINORITIES AND NARCOTIC USE: THE SECOND TRANSFORMATION
Anslinger may have exploited public antipathy toward narcotic dealers and users, but he did not invent it. The antinarcotic consensus had arisen from the earlier transformation of the addict population, a real demo-
graphic event helped along by imaginative statisticians and propagandists. During Anslinger's long tenure the addict population continued to evolve in a way that further strengthened his hand. The key change was the growing use of heroin by black men.
Blacks were not considered heavy drug users early in the century. They lived mainly in the rural South, were poor, and had less access to opiates than whites, who could afford doctors and patent medicines. Black workers occasionally used cocaine, as did prostitutes and petty criminals. A few field hands smoked marijuana, and some unemployed men drank excessively, but, with these exceptions, blacks had neither a disproportionate nor a very serious drug problem. On the contrary, the prevailing racial stereotype of the narcotic addict was white or Oriental.
After World War II the situation changed completely. Middle-class whites came to "imagine that ghettos [were] filled with black men mugging whites for money to pay for heroin and then injecting this evil drug so that they can spend the rest of the day nodding away in a blissful vacuum."24Figure 1 displays the statistical basis for these fears. Not only were black addicts turning up more often in federal treatment centers but they were being booked more frequently by the police, to the point that, by the 1950s, half or more of all narcotic arrests involved blacks. Something similar was happening in the Hispanic communities. In 1936 only about 1 percent of the addicts treated at Lexington were Hispanic; by 1966 more than a quarter were—13.9 percent being Puerto Rican and 12.2 percent Mexican.25
Data of this sort have been criticized as misleading because minorities are treated prejudicially and are hence more likely to end up in institutions or jails. They are particularly vulnerable during periods of racial or nativist tension, economic dislocations, or politically motivated crackdowns.26 Even in normal times it is tempting for the police to fill their quotas in the ghetto; it is easier to ticket, arrest, or prosecute those who are relatively powerless.
These biases are real but in one sense irrelevant. Statistics such as these, amplified and personalized by news stories and photographs, shape public opinion, regardless of their factual basis. Rightly or wrongly, the black junkie became a stereotype, and that made a difference. Moreover, even though these percentages may overstate the degree of involvement, there is no reason to doubt that minorities were using drugs in the 1940s and 1950s in a way they had not been before. Black narcotic arrests, for example, were increasing absolutely as well as relatively, rising from a mere 362 nationally in 1933 to 4,262 in 1950 to 11,816 in 1965. An increase of that magnitude, sustained over a long period of time, is due to something more than prejudice. Black writers and intellectuals were also sounding the alarm. Claude Brown's Manchild in the Promised Land (1965) contains
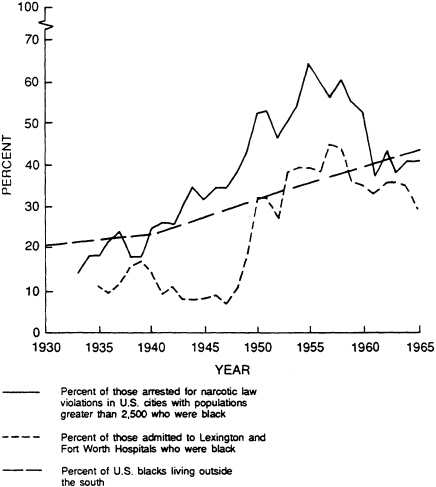
Figure 1 Indices Of Black Narcotic Use
SOURCES: P. Iiyama, S.M. Nishi, and B.D. Johnson, Drug Use and Abuse among U.S. Minorities: An Annotated Bibliography (New York: Praeger, 1976), 5; J.C. Ball and CD. Chambers, eds., The Epidemiology of Opiate Addiction in the United States (Springfield, Ill.: Charles C Thomas, 1970), 180; Bureau of the Census, Historical Statistics of the United States: Colonial Times to 1970, Part 1 (Washington, D.C.: U.S. Government Printing Office, 1975), 22.
a bitter account of the "shit plague" that befell New York City's neighborhoods in the early 1950s. Not only Harlem, "but in Brooklyn, the Bronx, and everyplace I went, uptown and downtown. It was like horse had just taken over."27
It is not hard to understand why this happened. Black narcotic use was a concomitant of urbanization. During 1915 to 1930, and again during 1940 to 1960, millions of blacks left the countryside for larger towns and cities. Jim Crow, disfranchisement, poverty, boll weevils, and agricultural mechanization made it difficult to stay, higher paying industrial jobs, especially during the war years, made it tempting to leave. Some migrants settled in southern cities; most eventually moved on to the North or West. Three major routes developed: from the south Atlantic seaboard toward the northeast urban corridor; from Mississippi toward Chicago; and from Texas and Louisiana toward California. In 1910 not a single city in the country contained 100,000 blacks. By 1960 New York City alone had more than a million. In 1910, 73 percent of the black population was rural. In 1960, 73 percent was urban.28
The blacks who fled the South were mainly young, unattached adults whose futures lay before them. They left with high hopes, singing hymns like "Jesus Take My Hand" and "I'm on the Way." What actually awaited them, the ghetto slum, has been likened to the frying pan instead of the fire. Not only did they have to face the classic dilemma of an uprooted peasantry—how to adjust to the city when what they knew was the land-but to do so under the worst possible circumstances, crowded into stinking, overpriced tenements.29 They also had to cope with the usual array of urban vice figures: pimps, prostitutes, thieves, con men, numbers runners, and all manner of drug retailers, from marijuana distributors like the legendary white hipster Milton Mezzrow to black opiate users and dealers like Malcolm Little, later Malcolm X Disoriented and demoralized, the newcomers were exposed to narcotics in a way they had never been before. So were their children, particularly those who had left school, were out of work, and spent their time on the street. The result could easily have been predicted: a growing incidence of black heroin addiction, particularly among the traditional high-risk group of single males in their late teens or early twenties.
To say that such an event was predictable is not to indulge in historical hindsight. There was ample precedent for what happened to the black urban community. It had happened before to other immigrants living in the same or similar neighborhoods. White ethnic addicts who started using narcotics in the 1920s and 1930s had substantially the same experiences as blacks who began in the 1940s and 1950s. They grew up in or moved to neighborhoods where drugs could be procured; they were on their own or unsupervised; they had friends who were users; they
yielded to curiosity or peer pressure and tried it for themselves. Thus, the ethnic slum, matrix of heroin use from about 1910 on, continued to spawn illicit narcotic use throughout the twentieth century.30 When the color of the faces in the tenement windows changed, so did the color of the addicts on the street.
Several factors, however, made the immigration-slums-narcotics tangle worse for blacks than for previous groups. First, because of their color, blacks had been and continued to be the objects of especially virulent racism. To the extent that this racism translated into educational and occupational handicaps, and to the extent that unemployment and poverty were conducive to drug and alcohol abuse, urban blacks were especially vulnerable. Living for the present made more sense for those who felt excluded from the future. Partly because of this legacy of racism, blacks had fewer political and organizational resources than other groups. There was, for example, no black counterpart to the New York Kehillah's Bureau of Social Morals, which monitored drug dealers in the Jewish immigrant community.31 Even the Mafia, the country's leading narcotic importer and wholesaler, kept the peddlers off its home turf. Ghetto blacks also had fewer familial resources. Why this was so has become a political and intellectual cause celebre; the fact remains that minority family dislocation did occur and it did contribute to addiction. The Road to H, a major study of young heroin users in New York City in the 1950s, found that 97 percent of addicts' families were characterized by "a disturbed relationship between the parents, as evidenced by separation, divorce, open hostility, or lack of warmth and mutual interest." The mother was the most important parent; about half the fathers often presented "immoral models through their own deviant activity with respect to criminality, infidelity, alcoholism, and the like."32 Keeping teenagers away from drugs in an environment in which they are plentiful requires especially active, watchful parenting. It is not likely to be done very well if parents are distracted, absent—or busy shooting up in the bathroom. Finally, there was the permanence of the black ghetto. Many of the white urban immigrants and their descendants were able to distance themselves from the tenements, moving to better quarters in safer neighborhoods and eventually to the suburbs. New York City's Jews, for example, went from Manhattan's chaotic Lower East Side, to Brooklyn and the Bronx, to Long Island, Westchester County, and New Jersey. Each step took them farther away from the primary illicit narcotic markets; indeed, to distance themselves from drugs and crime was one of the reasons suburbanites moved in the first place. Low-income blacks were not as fortunate. Even as the Civil Rights movement achieved its judicial and legislative triumphs, a collective decision was made to abandon blacks in the inner city, to leave them behind with inferior schools and inadequate services in an environment virtually assured to perpetuate poverty.
This was the result, not of a single grand conspiracy but of a thousand private, uncoordinated ones: restrictive covenants, realtors' whispered advice, bankers' lending practices. The federal government generously subsidized the fleeing whites through its tax, transportation, and mortgage policies. Urban abandonment soon developed its own momentum: as inner-city conditions progressively worsened, pressure grew on the remaining whites to escape beyond municipal lines, taking their tax dollars with them. Educated and upwardly mobile blacks were able to follow them to the suburbs, but those who were unemployed or underemployed had to stay behind. The decaying neighborhoods in which they lived were areas of heavy drug trafficking and use. Heroin became a staple in the ghetto economy, and black children grew up around older users who were both role models and potential initiators. Continued exposure, persistent discrimination, and progressive familial breakdown assured that subsequent generations of urban blacks would also suffer high rates of addiction. What began as an epidemic among black youth in the late 1940s and 1950s has long since become endemic to the urban underclass.
The growing involvement of blacks and Hispanics with narcotics and the consequent racial transformation of the addict population did not go unnoticed in high places. Anslinger himself emphasized this development. "Fifteen years ago, the Lexington and Fort Worth Hospitals had mostly white patients," he pointed out in 1957. "Today, they are filled with Negro addicts. What happened to the white addicts? You don't see them." Asked about the postwar rise in youthful addiction, Anslinger responded, "The increase is practically 100% among Negro people in police precincts with the lowest economic and social standards. . . . There is no drug addiction if the child comes from a good family, with the church, the home, and the school all integrated."33
There was truth in what Anslinger said, however bluntly he expressed it. Historically, children who were not poor, who were raised in intact families and socialized by middle-class institutions, were impervious to heroin. He did not, however, advance to the conclusion implied by his analysis: doing something about black addiction meant doing something about black economic and social conditions. Instead, Anslinger fell back on what he knew best, enforcement. During the 1950s he pushed for ever tougher sanctions against traffickers, believing that the ultimate solution lay in choking off the illicit supply. Congress, alarmed by stories of teenage users, the darkening racial cast of institutionalized addicts, the postwar renaissance of the Mafia, and the alleged trafficking of nonwhite communist countries like China, was in a mood to agree. In 1951 it passed the Boggs Act and in 1956 the Narcotic Control Act, providing progressively stiffer, mandatory sentences for possession and sale. The inflexible provisions of these laws sometimes resulted in blatant mis-
carriages of justice. In one instance a Chicano epileptic with an I.Q. of 69 was given two life terms for selling heroin to a 17-year-old provocateur; in another a black veteran with no previous record was sentenced to 50 years without parole for selling marijuana. Many states, nevertheless, followed suit, passing "Little Boggs Laws" that pegged minimum prison terms at or beyond the federal levels. A 1956 Louisiana statute provided mandatory sentences ranging from 5 to 99 years for persons who sold, possessed, or administered narcotics. In Texas possession of marijuana was punishable by 2 years to life. These were not isolated events; across the country nonfederal narcotic prosecutions were up sharply during the 1950s.34
THE END OF THE CLASSIC PERIOD, 1960-1965
Historians who have studied American narcotic policy are agreed that the 1950s marked the zenith of the punitive approach. The "new spasm of concern" felt during this decade translated into "increased regulation in familiar patterns," comments H. Wayne Morgan. "On the surface, the consensus against drug use and for enforcement seemed stronger than ever."35 Yet by 1965 the consensus had eroded and the old order, especially the categorical denial of maintenance, had been successfully challenged. Why did this happen?
The question must be answered on several levels. In the broadest terms, the Bureau of Narcotics and allied organizations were unable to bring about a lasting solution, as urban narcotic addiction remained a serious, widely publicized problem in the early 1960s. A Vietnam-like disillusionment began to set in: despite decades of escalating sanctions, narcotics were still finding their way onto the streets of America's cities. It was not for want of trying that the Bureau of Narcotics failed to stop the traffic permanently; under Anslinger it was one of the country's more efficient police organizations and the one most feared by organized crime. The problem lay in the nature of the case. Narcotics are highly compact, easily hidden substances. Two kilos in a false-bottomed suitcase are worth a small fortune. They are also reasonably easy to acquire because opium is a major cash crop and only a fraction of the world's harvest is sufficient to supply American addicts' needs.36 From the smugglers' vantage the United States is ideal: it is an open society with excellent transportation facilities, 88,633 miles of tidal shoreline, and two long boundaries with Mexico and Canada. Traffickers would forego these geographical advantages if deterred by threat of punishment, but here the bureau encountered a paradox. Successful prosecutions take suppliers out of circulation and heighten the level of risk. Given what economists call an inflexible demand curve (addicts are generally steady customers), restrictions on
supply and increased risk quickly translate into higher prices. The profits to be made from selling adulterated heroin to addicts tempt other criminals to jump into the market—criminals who are generally more ruthless and better organized than those previously arrested or deterred.37 Narcotics enforcement is like antibiotics: it wipes out disease-producing organisms, but over time it also produces more resistant strains.
Anslinger realized that the way out of this paradox was to simultaneously reduce demand by isolating and then curing addicts. Fewer customers would mean smaller profits for dealers, and at some point the illicit trade would cease to be worth the risk. The catch was that Lexington-style institutions failed to effect many permanent cures: as previously noted, addicts often went through several times, relapsing after every treatment. Narcotic wards were not without value: detoxification brought respite from the street grind and helped addicts keep their habits within manageable bounds. But the generally high relapse rates provoked skepticism and lent credence to the cliche, ''once a junkie, always a junkie."
Dissatisfaction with the big, revolving-door institutions eventually led to a search for other programs that might help addicts. One possible alternative was Synanon, a therapeutic community that evolved in Ocean Park, California, in the late 1950s under the direction of Charles Dederich, an ex-alcoholic. Dederich made no bones about the authoritarian nature of Synanon; he consciously recreated an autocratic family environment to keep people in line. He also relied heavily on group encounters led by a "Synanist," or experienced former addict. These encounters were intended to make the participants come to terms with their feelings, to assume responsibility for their own lives, and to learn to deal with their problems without recourse to drugs or alcohol. Once they could do that, they could theoretically return to the world and lead "straight" lives.38
Synanon was a relatively small-scale operation. Its real significance was that it inspired several physicians, clergymen, and social workers to establish "second-generation" therapeutic communities throughout the country. These were patterned after Synanon but incorporated significant individual variations. Several of the most important of these programs, such as Daytop Village, Odyssey House, and Phoenix House, had their inception in the middle 1960s. They did not expand rapidly, however, until the later 1960s and early 1970s, when the Lexington approach was officially discredited, the country was in the midst of a youthful drug epidemic, and private and public funding for community drug treatment programs of all sorts was readily available.
It is important to point out that, although the leaders of the therapeutic community movement criticized the impersonality and ineffectiveness of existing addiction treatment programs, they shared the traditional assumptions that abstinence was the ultimate goal and that the
police should suppress the illicit narcotic traffic. Some critics, however, began to question the very moral and political bases of American narcotic policies. Increasingly in the 1960s, liberal commentators asked why the country had a narcotic problem. Were drugs evil because they were physical and social pathogens? Or were they pathogens because illegal, hence adulterated and exorbitantly priced? Would addicts behave differently if the maintenance taboo were broken and they could receive cheap, pure medication? Specifically, would maintenance reduce the number of crimes addicts committed? Would it provide a way out of a destructive subculture and back into the productive world of family and work?
These were not new questions; they had been pointedly asked by the pioneers of organized maintenance, physicians like Charles Terry and Willis Butler. But now, after 40 years of apparently self-defeating police solutions, they were being raised again by such critics as the sociologist Alfred Lindesmith. Like most twentieth-century liberals, Lindesmith was a negative utilitarian. He believed that if a law produced many costs and few benefits, it was irrational and should be modified or abolished. This belief was the premise of his influential 1965 study, The Addict and the Law, in which he argued that American addicts were both more numerous and more "impoverished, degraded, and demoralized" than elsewhere in the Western world. He cited police estimates that up to 50 percent of big-city crime was due to addicts hustling to support their habits.39 By contrast, the British system of medical maintenance had resulted in neither serious crime nor an inordinate amount of addiction. Lindesmith and others essentially charged the Narcotics Bureau with benighted prohibitionism, resulting in huge costs to both users and society. "The American narcotics problem," summed up Marie Nyswander in 1965, "is an artificial tragedy with real victims."40
If the crime issue was one fault line along which the narcotic consensus fractured, then marijuana was another. Marijuana had come under the Bureau of Narcotics' jurisdiction as a result of the 1937 Marijuana Tax Act, passed by Congress at Anslinger's urging. Like cocaine, marijuana was identified with an internal minority (Mexicans) and alleged to produce insanity and violent, unpredictable behavior. Later, its prohibition was rationalized by what came to be known as the stepping-stone hypothesis: marijuana was not in itself habit forming, but its use led to drugs that were—like heroin. "The danger is this," testified Anslinger in 1951, "over 50 percent of those young addicts started on marijuana smoking. They started there and graduated to heroin; they took to the needle when the thrill of marijuana was gone."41
Again, Anslinger had appropriated a partial truth. Minority addicts treated at the federal narcotic hospitals typically smoked marijuana a year or two before using heroin. It did not follow, however, that marijuana led
ineluctably to heroin. Many adolescents from the same milieu, including delinquents and gang members, smoked marijuana but refrained from trying opiates.42 Nor was there any scientific evidence to substantiate the horror stories Anslinger was fond of circulating. Growing numbers of college-age marijuana smokers discovered this for themselves in the 1960s. Marijuana might not be good for their lungs, or their memories, or their waistlines, but neither did it lead to rape, madness, or axe murder. Moreover, if the authorities had misrepresented the dangers posed by marijuana, what of the other drugs they controlled? Just what was wrong with "narcotics?"43
What, in fact, was wrong with all the great American taboos? The ultimate basis for the suppression of nonmedical drug use lay in the realm of moral assumptions. Americans of the classic period were, to a degree unknown today, governed by a popular moral code, postulated on the self-evident correctness of patriotism, self-discipline, hard work, self-reliance, family stability, personal honesty, and self-restraint.44 However dishonored in practice, these virtues were consistently affirmed by religious and civil institutions and served to justify the proscription of drugs, just as they had earlier served to rationalize the prohibition of drink. During the 1960s, however, these traditional values—Harry Anslinger's values—were increasingly questioned. The principal challenges came from the mass media, the youthful counterculture, and skeptical "new class" intellectuals who were disenchanted by the status quo and optimistic that they could replace it with something better. Whatever the merits of their critique, American society did change, becoming noticeably more permissive and secular. Although this social revolution did not peak until the 1970s, it was well under way by the mid-1960s, and it did not augur well for strict narcotic control.45 Recall Anslinger's remark that maintaining addicts with drugs was like pandering to homosexuals. That analogy would be effective with a traditionalist, one who was instinctively homophobic. But for someone beginning to doubt the received wisdom, wondering if the suppression of homosexuality might not itself be unfair and counterproductive, the argument would not carry much weight. It might even backfire, lending credence to the belief that America (or Amerika, as it was soon to be called) was blindly opposed to all forms of social and political liberation, of which drug use was but one instance. 46
As for narcotic officials, they had more on their minds than the unfavorable turn of the zeitgeist. A more immediate problem, which Anslinger concealed but never resolved, was their shaky legal foundation. The denial of maintenance was predicated on distant and narrowly decided Supreme Court cases; there were also contrary precedents, like the Linder ruling. These weaknesses were not apparent to the general public, but they were known and discussed within the legal and medical communities,
together with the more general question of the propriety of maintenance. The eventual outcome of this discussion was Narcotic Drugs: Interim Report of the Joint Committee of the American Bar Association and the American Medical Association on Narcotic Drugs (1958). Authored by a panel of physicians, lawyers, and judges, and based on three years of research in the United States and Britain, the Interim Report was a temperate critique of the police approach with suggestions for further research and trial programs. Doubting ''whether drug addicts can be deterred from using drugs by threats of jail or prison sentences," it recommended the establishment of an experimental outpatient clinic that might, under certain circumstances, supply addicts so they would not have to patronize illicit dealers.47
Anslinger, who saw this guarded proposal as the hole that would sunder the dike, immediately plugged it with his fist. Denouncing the committee's plan as "so simple that only a simpleton could think it up," he launched a campaign of vilification against his opponents. The piece de resistance was Comments on Narcotic Drugs (1958), a rebuttal by the "Advisory Committee to the Federal Bureau of Narcotics" that Anslinger quickly assembled. Clinics were portrayed as proven failures, liable to spread addiction and to provide comfort to the nation's communist enemies. The solution was not less punishment but more: "Only under the impact of heavy prison sentences can we hope to rout the scum of the criminal world." And routing they deserved, because what they were really peddling was "murder on the installment plan." Experts who disputed this approach were feckless dreamers, or worse. As far as Anslinger was concerned, they ought to join the addicts in jail. His bureau spokesmen openly accused the critics of Hitlerian "Big Lie'' tactics and of endangering the health and morals of the nation.48
It did not work. Anslinger not only failed to discredit or suppress the report—it was published in. 1961 as Drug Addiction: Crime or Disease? and went through seven printings by 1969—but his tactics backfired and brought unfavorable publicity to the bureau. "The whole tenor of the [rebuttal] document," wrote Stanley Meisler in The Nation, "indicates Anslinger does not want to win the discussion as much as he wants to eliminate it.49 Historian David Musto has commented, "the bureau's vituperative attack . . . can be seen as a desperate response to the belief that, regardless of congressional support and official bureau statements, its control of narcotic enforcement in America was beginning to slip."50
The year 1962 brought further slippage. On June 25 the Supreme Court decided, in Robinson v. California, to strike down a California statute making addiction to the use of narcotics a misdemeanor, punishable by 90 days to a year in the county jail. The Court, recalling the language of Linder that addicts "are diseased and proper subjects for [medical]
treatment," condemned prison as a cruel and unusual punishment for the sick. "It is unlikely that any State at this moment in history," Justice Potter Stewart wrote, "would attempt to make it a criminal offense for a person to be mentally ill, or a leper, or to be afflicted with a venereal disease.''51 The decision did not do the appellant, Lawrence Robinson, much good—he had died in 1961—but it did scotch Anslinger's longstanding ambition to take addicts out of circulation simply because they were addicts.
The addiction-as-disease theme was being sounded elsewhere as well. In 1962 Lawrence Kolb published Drug Addiction, a collection of articles and essays pointedly subtitled A Medical Problem. Kolb, once Anslinger's wary collaborator, had grown increasingly disenchanted with punitive tactics. He now called openly for Americans to rid themselves "of the fury that propagandists have injected into our laws, administrative practices, and attitudes concerning addiction."52 Even as Kolb was airing his doubts, the chief perpetrator of the narcotic fury was being quietly eased from power. In 1962 Anslinger was forced to retire, having reached the age of 70. He was succeeded by the Narcotics Bureau's deputy commissioner, Henry L. Giordano. Anslinger did not disappear from the scene altogether; he put in an appearance at a large White House Conference on Narcotic Drug Abuse in September 1962 but seemed uncharacteristically subdued.53 This same conference recommended the establishment of a presidential commission, which met and issued its report the following year. Among its recommendations were more flexible sentencing, wider latitude in medical treatment, and more emphasis on rehabilitation and research.54
Heresies were spreading about the land now, and these even bore the imprimatur of a presidential commission. The time was ripe for someone to heed the many calls for research and actually put together an experimental maintenance program. That task was accomplished in 1963-1964 by Marie Nyswander, a psychiatrically trained clinician who had experience treating addicts, and Vincent Dole, a metabolic disease specialist who had no such experience but who brought a fresh approach to the problem. Dole began what he was later to call "humdrum observational research" with several basic pharmacological and physiological questions: What effects do opiates actually have? Why are they bad for people? What is wrong with narcotic maintenance? The answer to the latter, he discovered, was that it was extremely difficult to stabilize the amount and frequency of the dose. Subjects to whom he gave morphine constantly badgered him for more. He was prepared to concede the wisdom of the antimaintenance philosophy when he made a chance discovery. The patients to whom he gave methadone, a long-acting, synthetic opiate, did not behave in an objectionable way. They were not preoccupied with drugs and began to
turn their attention to conventional pursuits like sports or work or school. Although thoroughly addicted, their behavior appeared quite normal.
Ultimately, Dole and Nyswander hypothesized that addicts had undergone a permanent metabolic change, that they needed narcotics in a visceral way, the way a diabetic needs insulin. This explained relapse and why abstinence was not a realistic goal. But methadone maintenance could satisfy the underlying craving and enable the addict to lead a normal and productive life. Methadone could be taken orally once a day, so addicts would not have to constantly inject themselves with possibly contaminated needles. At a sufficiently high dose, methadone blocked the euphoric effects of a shot of heroin, so that addicts would not be tempted to continue using illegal narcotics. Nor would they need to because methadone, itself a narcotic, prevented withdrawal sickness. Finally, methadone was cheap and legal. Addicts could escape the grind of hustling and scoring, thereby improving their lives and reducing the amount of crime.
There was, inevitably, a reaction as both the premises and results of methadone maintenance were called into question. Critics said that the hypothesized metabolic change was mere speculation; that methadone was just a quick chemical fix, substituting one drug for another; and that it failed to significantly reduce criminal or antisocial behavior because it ignored the underlying problems of addicts—inferior or abnormal personalities, broken families, anomie, inebriety, ghetto squalor, deviant peers, structural unemployment, and so on down the list. Others charged that methadone did too much, that it was an insidious form of social control aimed at turning restive inner-city minorities into harmless zombies; or that it was dangerous—because large amounts of methadone were diverted into the black market and consumed by those who might not otherwise have used drugs. Probably the fairest and most accurate thing to say about these criticisms (and this is just a partial list) is that they arose from mixed motives. There were real and unresolved problems with methadone maintenance, but there were also vested interests to be defended, especially by those whose funding and prestige were tied to competing addiction theories and treatments. Medical controversies are seldom fought on purely scientific grounds, and methadone is a classic case.
The whole controversy might never have arisen if the Bureau of Narcotics had managed to block Dole's experimental research. This it failed to do. Dole defied the agents sent to harass him, at one point suggesting that they take him to court "so we can have a determination on this point." The bureau demurred. It might well have prevailed against an unscrupulous doctor writing prescriptions for cash, but its chance of winning against a distinguished scientist, backed by a major research institution, with a liberal majority on the Supreme Court and in a climate increasingly hostile to the police approach, was effectively nil. The bureau
also failed to prevent the program from expanding. In 1965 a ward in the Manhattan General Hospital was given over to methadone maintenance, as Dole and Nyswander came under the sponsorship of the New York City health department. Although minuscule in comparison to what it would become in the early 1970s, methadone maintenance was by 1965 officially and permanently established. It was also beginning to attract widespread and favorable attention, both in medical journals and in popular periodicals such as Look, Time, Newsweek, and Science Digest. Marie Nyswander was even accorded a profile in The New Yorker. The antimaintenance regime was over.
DRUG POLICY AND DRUG USE SINCE 1965
American narcotic policy from the early 1920s until the middle 1960s had two key objectives: the quashing of legal maintenance and the suppression of illicit narcotic transactions through vigorous police enforcement. What has happened since then has been a qualified abandonment of the first goal, but not of the second. Substances like heroin are still outlawed.55 This result was intentional: the liberal supporters of maintenance never espoused, nor could they have achieved, a libertarian resolution of the problem. The government was not about to get out of drug enforcement and proclaim caveat emptor. Most liberals were perfectly willing to see addicts, whom they regarded as victims, treated in clinics, and traffickers, whom they regarded as criminals, sent to jail. This arrangement is at best paradoxical; some critics have described it as confused and contradictory.56 What about the addict who is also a dealer? Or the addict who is a predacious criminal, before, during, and after treatment? Or the addict who diverts methadone into the black market? Methadone programs have reduced the frequency with which their clients violate the law, but they certainly have not eliminated all of their legal or behavioral problems.57
These difficulties are not unique to narcotic policy. In virtually every area in which liberals successfully challenged restrictive policies in the 1960s and 1970s, similar quandaries have arisen. Gambling is a good example. State-run lottery games and other forms of legal gambling are now freely available and widely advertised. But illegal gambling has not disappeared, as some liberals hoped or assumed; the police still have plenty of sports bookies and bolita operators with whom to contend. The public, meanwhile, gets a decidedly mixed message: some forms of gambling are acceptable, but others are not. The same is true of drug use. Classic-era narcotic policy, despite its faults, was at least consistent. Its message was unambiguous: drugs are bad for you. This was one reason why propo-
nents of therapeutic communities remained deeply suspicious of methadone maintenance. It contradicted, both symbolically and actually, the traditional goal of abstinence. "It's just another political expediency," charged Dr. Judianne Densen-Gerber, founder of the Odyssey House therapeutic community. "There's no reason to change a heroin user to methadone, just as there's no reason to change a scotch drinker to cheap wine. . . . People should not have a dependency disease. They should be able to make decisions without being controlled by their need for a substance."58
It was ironic, then, that Richard Nixon, who styled himself a hardliner and a moral conservative, should have been the president to preside over the rapid expansion of methadone maintenance. On June 17, 1971, he delivered a special message to Congress on drug abuse prevention and control. Until the recent past, Nixon observed, narcotic addiction had been viewed as a "class" (i.e., minority) problem, but now it affected many groups, including soldiers in Vietnam. Heroin addiction was growing rapidly and was responsible for a costly wave of urban crime. He proposed to meet this national emergency with additional, federally financed efforts to reduce narcotic supply and demand. To ensure that the task of demand reduction was carried out in a coordinated manner, Nixon announced the creation of the Special Action Office of Drug Abuse Prevention (SAODAP, pronounced say-oh-dap), to be located within the Executive Office and answerable directly to the President. SAODAP was given a remarkably broad charge: overall responsibility for drug treatment and rehabilitation, as well as prevention, education, training, and research programs. Only law enforcement and diplomatic efforts were outside its control.59
SAODAP's first director was Dr. Jerome H. Jaffe. His selection was not coincidental. During 1970 and 1971 several White House staff members, including Jeffrey Donfeld, Egil Krogh, and John Ehrlichman, had become convinced that methadone maintenance offered the best prospect for reducing narcotic-related crime and that any such reduction would pay substantial political dividends in the upcoming election. It would also eliminate a political liability, insofar as Nixon, who had made domestic lawlessness the centerpiece of his 1968 campaign, was under some pressure to show a tangible reduction in urban crime. Jaffe was known as a methadone advocate. "The White House staff was quite aware of my view that the use of methadone could no longer be viewed as 'a little experiment,' but needed to be incorporated into an overall approach to reducing the social cost of heroin addiction," Jaffe recalled. "It may be that I was selected to articulate and give academic credibility to the conclusion the White House staffers had already reached."60 What Jaffe did in practice was to expand both maintenance and nonmaintenance programs, with the hope that narcotic addicts would avail themselves of one or the other
approach. The result was that, while therapeutic communities and other nonhospital, abstinence-oriented programs were growing rapidly in the early 1970s, so too were their philosophically and clinically opposite numbers, the methadone maintenance programs. Between June 1971 and March 1973 the number of federally funded methadone patients doubled.61 Counting both federal and nonfederal programs, there were 80,000 persons enrolled in methadone maintenance by October 1973.62
Despite SAODAP's imprimatur and increased funding, there was still a great deal of suspicion and hostility toward methadone within the federal bureaucracy. This attitude was manifest in a barrage of detailed regulations governing dosage, duration of treatment, and security. (Item: vaults containing the methadone supply shall have locks "resistive . . . to radiological attack for twenty manhours."63) Frustrated methadone proponents argued that such micromanagement reduced the impact and effectiveness of the maintenance programs. The late Marie Nyswander, when interviewed in 1981, was amused to find herself "sounding like a Republican" on the issue of federal controls. "I don't think there's any question about it," she said. ''If we had decent treatment, in all the ways people could be treated—clinics, hospitals, doctors—then we'd probably take in the majority of addicts. But right now methadone is operating at only 30 to 50 percent of its potential.''64 Why not, she urged, permit stable, long-term patients to simply receive several months' supply from a private physician? For Nyswander, contemporary narcotic policy was insufficiently reactionary. That is to say, the clock should have been turned all the way back to 1914, when doctors still had wide latitude in maintaining addicts, rather than to 1919-1923, when a handful of municipal programs struggled to treat patients in a hostile regulatory environment. Indeed, the 1970s and 1980s might be aptly described as the New Clinic Era, with methadone maintenance understood as the vehicle of a long-delayed but ultimately limited counterrevolution.
Not all of methadone's limitations were due to bureaucratic meddling, however. Dr. Robert Newman, who presided over the expansion of methadone maintenance in New York City from 1970 to 1974, also emphasized the strength of community opposition. The first twenty clinics breezed through, he recalled, but "the next twenty were pretty darn tough. . . . Finally, it became an insurmountable problem when the neighborhoods were given almost veto power. Since 1975 I think there's been one clinic opened in the City of New York, and that over tremendous opposition." Newman was chagrined to discover that methadone was a political lightning rod:
I remember trying to open one clinic up in the Bronx, and speaking at a community meeting. I talked for forty-five minutes about methadone
and I thought I did an absolutely great job. I was sure I had everybody convinced. When I asked for questions, the first one was from some lady in the back who said, "Why don't you pick up our garbage?" I said, "What do you mean, pick up garbage?" I thought that the woman was crazy, or that I was in the wrong meeting. I said, "This isn't the Sanitation Department; we're talking about opening up a methadone clinic." She said, "You know what I mean. You're the City of New York, and you haven't picked up my garbage in two weeks.'' I said, Lady, that's another department." She said, ''Yeah, I know, you're always passing the buck; whoever we talk to, it's never their department, it's somebody else's. Well, by God, you haven't picked up my garbage and I'm not going to allow you to do what you want to do up here with this methadone clinic."
Then there was the hatred and the concern regarding addicts and addiction. It's a lot of things: it's race and class; it's fear, the realization that addicts have to commit crimes to support their habit; and it's a resentment that people are feeling that good three, four, five times a day. It's hard to express this hostility, because there's nothing to focus against. But a methadone clinic brought all these problems together. It was a building, in front of which you could picket, or wheel your baby carriages, or go to the press about. I think people really wanted to express their hostility against a problem that was so evanescent that they couldn't do it any other way.65
Finally, there were the addicts themselves, many of whom balked at entering treatment programs. There were garbled fears about methadone, complaints that it would "get into the bones" or render patients dependent for life. "It's very, very hard to quit methadone," remarked one older patient. "When a guy gets to be my age, getting off methadone pret' near kills you. I think methadone's got me hooked until I die." He conceded, however, that methadone had its good points: "Like, I used to live in Harlem. I knew a whole lot of people that used to be tramps. They wouldn't clean up, or wouldn't try to do nothing for themselves, sleeping out there on the street. Since this methadone came out you see them nice and clean, with a tie on and shoes shined, and working every day."
This amounts to a summary of the original thinking behind methadone. The drug may be a powerful narcotic and treatment may be indefinite, but what does it matter if the patients turn their lives around? The problem, however, was that not all addicts wanted to turn their lives around, nor were they necessarily enamored of shiny shoes and daily work. They regarded methadone, or for that matter any other treatment program, as a form of surrender. An addict who sought treatment had to admit to himself and his peers that he no longer had enough spunk to stay on the street and support a habit. Ethnographic studies of untreated addicts have shown that their self-image is often that of an accomplished hustler, street-wise and disciplined enough to keep themselves in money and drugs.
The "righteous dope fiends" consider addicts in methadone programs ("methadonians," "zombies," "blimps,'' "meth-heads'' or "murdocks") to be losers, while those who enter therapeutic communities are totally infra dig. One long-time user started to have foot trouble as he approached his middle fifties. His hustling suffered, and in desperation he sought help at Synanon. He quickly left. "Synanon wasn't for me," he exclaimed. "I wouldn't stand being thrown down the shit bowl [degraded] by those foul garbage junkies, snitches, winos, and sissies." 66 These attitudes have persisted and help to explain why more users do not take advantage of treatment opportunities. They also explain why, once in treatment, many patients leave or fail: they are constantly reminded of and tempted by their old self-image, the smooth operator leading a free and exciting life. There is more to becoming an ex-addict than detoxification.
For all of these reasons the treatment revolution of the late 1960s and early 1970s has proved to be something of a disappointment. According to one 1987 estimate, only 7 percent of the approximately 2.5 million Americans who had a serious drug problem were in treatment. Many of those who remain untreated were "undergoing progressive and chronic physical deterioration, as well as committing crimes and being involved in accidents that lead to injuries to themselves and others." There was an economic cost associated with this, as well as a human one. It is far less expensive for an addict to be in a treatment program than in and out of hospitals and jails.67
It is less expensive, that is, if the untreated addict survives at all. One particularly frightening development has been the spread of AIDS, a uniformly fatal disease. Caused by the human immunodeficiency virus (HIV, formerly known as LAV or HTLV-III), the virus is spread among intravenous drug users through the sharing of syringes and needles.68 There is no evidence that the virus can be spread through casual contact or the use of noninjected drugs; however, it can be spread through both homosexual and heterosexual contact and to the fetus in utero.69 The number of persons infected with HIV who will ultimately develop AIDS is not yet known with certainty, but it is at least 3 in 10—possibly as many as 10 in 10.
The period between initial exposure to HIV and development of full AIDS averages seven or eight years.70 This long latency period has permitted the rapid, unknowing spread of the virus within groups of intravenous drug users. The situation is especially bad in New York City, where there are both large numbers of cases of AIDS and high seroprevalence rates (a high percentage already infected) among intravenous drug users. By mid-1987 a third of the city's 10,000 AIDS cases were drug addicts; in nearby New Jersey and Connecticut, more than half of all diagnosed AIDS cases were addicts, their sex partners, or children.
Nationwide, nearly a quarter million intravenous drug users may already be infected.71
It is difficult to say what the long-term effect of AIDS on narcotic addiction will be because developments in AIDS are occurring very rapidly, both in the spread of the epidemic and in research on ways of potentially controlling or treating it Nevertheless, several studies on the reactions of intravenous drug users to AIDS show that the epidemic has had an effect and hint at the possibility of reducing the practice of illicit drug injection, or at least of making it more circumspect. Death has always been common among intravenous drug users, but AIDS forces a radically different psychology of death in the group. Involving a protracted and painful death, often with stigmatization and social isolation, AIDS conjures up none of the escapist fantasies associated with overdose deaths. The virus may also develop long after a person has ceased injecting drugs; one cannot be certain that stopping drugs will prevent the development of AIDS. Finally, there is the possibility of infecting friends and family, through sexual or in utero transmissions of the virus. These considerations have apparently prompted changes in the behavior of intravenous drug users in the New York area, where addicts have increased their use of sterile needles and reduced the number of persons with whom they will share drug injection equipment.72 It is possible that "safer" needle use will become the norm for intravenous narcotic addiction in the future. Fear and natural selection are both operating in that direction.
Another potential for change in narcotic addiction may be in the recruitment of new intravenous drug users. Novices usually learn to mainline through contact with experienced users whom they admire and depend on for the equipment for their first injection.73 Over time, the fear of AIDS is likely to reduce both the admiration felt for experienced intravenous users and the willingness to borrow or experiment with their needles and syringes. No one wants to borrow death, especially death by AIDS.
The threat of AIDS could reduce illicit drug injection to the point where not enough new persons are recruited to replace those intravenous users who die or quit. This would not necessarily eliminate narcotic addiction, however. It would still be possible to become addicted by sniffing or (more rarely) smoking heroin, or by the regular use of a synthetic opiate. Thus, even if AIDS should virtually eliminate intravenous drug addiction, there is no guarantee that other forms of addiction will disappear. They may even expand, as has happened with cocaine smoking.
One last point about AIDS: although there is some evidence that intravenous drug users are motivated by fear of the disease to seek treatment,74 most addicts remain at large, as noted earlier. The danger they pose to themselves and to others underscores the fact that a large
percentage of users remain outside of treatment programs. Any modality, whether geared toward maintenance, short-term detoxification, or long-term abstinence, is safer than street trafficking and use—especially if the patients do not "cheat" on the program.
Of course, patients could not cheat if street drugs were unavailable. That was a point Anslinger made repeatedly: get the addicts clean through institutional treatment and then keep them from temptation by drying up the illicit supply. Unfortunately, the strategy did not work particularly well for him, nor did it work at all well during the 1980s. Retail (street-level) drug transactions have exceeded $100 billion, up from an estimated $79 billion in 1980. Heroin imports, which generated $8 billion in 1980, grew 50 percent by 1986, from four to six metric tons per annum. Heroin purity levels were low in the early 1980s, in the 3 to 5 percent range, but they have sharply increased, owing to an influx of "China White," Mexican "black tar," and other highly potent varieties. Much of the Mexican heroin is smuggled by illegal aliens, whose chances of being caught crossing the border are as low as one in five.75
Nor is Mexico the only source of the problem. Large amounts of heroin are also shipped from Southeast Asia, a region that became a major source of supply during the Vietnam era. A third source of supply, Southwest Asian heroin, emerged in the late 1970s and expanded rapidly during the early 1980s, in the wake of political and military turmoil in the region. The one signal law enforcement accomplishment, the disruption of the famous "French connection" in the early 1970s, proved to be a transitory victory. Turkish opium processed into heroin at Marseilles, the single most important illicit source for most of the classic era, became very scarce in the U.S. after 1973; this was of little strategic significance, however, because the combined Mexican, Southeast Asian, and Southwest Asian supplies have more than made up for the deficit.76
The failure to stop the heroin traffic was by no means the only or even the worst setback for law enforcement since 1965. Officials have also had to contend with the emergence of several new street drugs, such as LSD and PCP; the diversion and abuse of licit drugs, such as Methedrine and methaqualone; and the increased popularity of illicit nonopiate drugs, such as marijuana and cocaine. Simply stated, more people from more different backgrounds have begun using more drugs.
This became apparent during the 1960s and early 1970s, as marijuana smoking spread rapidly among those whom sociologist Eric Goode described as "the growing edge of American social life." These were the baby boomers, then entering their late teens and early twenties, the prime drug-experimenting years.77 "Probably the most affluent, confident, indulged crop in human history," Timothy Leary called them, "[this] generation of young Americans threw caution to the winds and recklessly
rejected the fear-imposed systems that have kept human society surviving-the work ethic, male domination, life-style conformity, inhibition of sensuality and self-indulgence, reliance on authority."78 Leary's generalization was only half-correct: most of the pot-smoking students graduated, trimmed their hair, and went to work for hierarchical enterprises, motivated by "fear" of an empty checking account. Despite their economic assimilation, however, they retained many of the hedonic, antiauthoritarian values of their youth, including tolerance of marijuana and other drugs.
The speed with which marijuana use and trafficking expanded was remarkable. In one state, California, marijuana arrests rose from 7,560 in 1964 to 50,327 in 1968. Nationwide, federal seizures of marijuana increased more than 10-fold between 1969 and 1973, hashish seizures more than 20-fold. By 1979 an estimated 50 million Americans had tried marijuana at least once, including two-thirds of all young adults. Marijuana use has declined somewhat during the 1980s, but it remains a popular illicit drug and a source of huge profits for both international traffickers and, increasingly, domestic cultivators.79
Equally remarkable was marijuana's popularity among high school and junior high school students. Peter Santangelo, a former undercover narcotic agent who worked in southern Connecticut in the early 1970s, was struck by the youth of those who bought and sold marijuana and other drugs. "Teens, early teens, seventeen, eighteen; dungarees; long hair, never brushed, dirty, parents well-to-do," was the way he characterized his quarry.80 Nationwide, the number of 12- to 17-year-olds who had ever tried marijuana rose from virtually zero in 1960 to three out of ten in 1979.81
This was a portentous development, not only because the young marijuana smokers might "burn out" with daily use but because they were also more likely to experiment with other illicit substances. Marijuana, like tobacco and alcohol, was a gateway drug. A pattern emerged: first beer or wine, then tobacco or hard liquor, then marijuana, then another illegal drug, like LSD or cocaine.82 Some progressed all the way to the opiates, thereby contributing to the heroin epidemic of the early 1970s, but they were exceptional. Most marijuana smokers, if they went on to other drugs, chose pills, hallucinogens, or stimulants. 83 It was in the ghetto that the ultimate graduation to heroin was still most likely to occur. Epidemiological studies continued to show that minorities, especially black and Hispanic males, were heavily overrepresented among narcotic users.84 What happened after 1965, in short, was the superimposition of a new pattern of largely recreational, largely youthful, largely white, and largely nonopiate drug use on the existing pattern of inner-city narcotic use and addiction.
A partial exception to this generalization is cocaine, a crossover drug that has experienced a renaissance among both white and minority users. Popular around the turn of the century, cocaine fell into disuse during the classic era. "Cocaine addiction has disappeared," Anslinger flatly declared.85 The drug still had a few devotees, mainly individuals who were privileged, or socially marginal, or both. Among them were jazz musicians, stage and screen stars, pimps, prostitutes, and bohemians. But if federal seizures were any indication, cocaine was a remote second to heroin and other opiates. As late as 1970 only 478 pounds of the drug were confiscated nationwide.86
Today cocaine seizures are measured by the ton. Virtually all indicators of use—admissions to treatment programs, overdose deaths, student surveys, and chemical analyses of urine samples—have shown a marked increase in its consumption. By 1985 an estimated 40 percent of graduating high school seniors had tried the drug at least once. Illicit sales are so vast that the transportation and processing of money have become as difficult for cocaine traffickers as smuggling the drug itself. One dealer went to the point of removing the play money from several Monopoly games, replacing it with real money, sealing the boxes back up, and then shipping them to Colombia. A portion of such fabulous profits is naturally plowed back into production. Between 1982 and 1986 the world's supply of cocaine was roughly doubled by the planting of new coca bushes in South America, and it has continued to expand since then.87
One of the many groups to become involved in the cocaine revival of the 1970s was, ironically, methadone patients. At a sufficiently high dosage, methadone blocked the euphoric effects of heroin; that was one of its selling points. Methadone did not, however, necessarily blot out the desire to get high, and many patients soon discovered that nonopiate drugs, including cocaine, would do the trick. "Methadone . . . takes care of my heroin problem," explained one 42-year-old addict. "But I still need something, so I'm using coke. I'm shooting it." He financed his purchases with his welfare check and, when that was insufficient, by breaking into cars.88 Others raised money by selling part of their methadone on the street. Proponents of methadone maintenance were caught in a political bind. Not only was methadone pharmacologically irrelevant to the growing number of nonopiate users, it appeared (erroneously) that the programs were responsible for financing their indulgence. "The television stations in particular never tired of arranging an arrest with a local police department,'' Robert Newman complained. ''An undercover agent would go up to one of the patients in front of a clinic, offer usually twice the going rate for illicit methadone, get as many people as they wanted to sell, while all this was filmed by a clandestine TV camera."89
In reality, methadone patients made up only a fraction of the new cocaine users. Several other forces were also at work. One of them was the waning popularity and availability of amphetamines. "Contra speedamos ex cathedra," pronounced Allen Ginsberg, a warning seconded by various counterculture notables. Speed killed. It also incarcerated, with the advent of stricter production regulations. Fear and short supplies of amphetamines made cocaine attractive as a "safe" alternative stimulant—at least until 1986, when the death of college basketball star Len Bias made it abundantly clear that cocaine could also kill. 90
The highly publicized troubles that black athletes and celebrities had with cocaine were, in one sense, misleading. Because the Willie Wilsons and Richard Pryors of the world had huge amounts of disposable income and worked in high-pressure occupations, their cocaine consumption fit into what might be thought of as the traditional show-business pattern. What was different about the 1970s and 1980s was the spread of cocaine beyond these rarefied circles to the middle and professional classes, notably among baby boomers who had gone to college, flirted with the counterculture, smoked marijuana, and learned to discount official warnings about drug abuse. They also had the money and the disposition to become users, albeit on a lesser scale than the superstars. After 1982, when a glut of South American cocaine dropped wholesale prices by a third or more, those of modest means could partake.91 With vials of "crack" (potent, smokable cocaine) retailing for as low as $5, no one was priced out of the market. By the late 1980s, crack had supplanted heroin as the drug of choice in the nation's ghettos.
Crack caught on because it was easy to smoke, requiring no complicated preparations with dangerous chemicals, as had been the case with "free basing." Crack delivered the rush of intravenous injection without the risk of AIDS and other infections. A few users have experimented with smoking crack and heroin, a combination likened to "firing both barrels at the brain's pleasure centers."92 Two barrels or one, this method is likely to produce dependence because the powerful doses soon disrupt the brain's chemistry, creating a depressed, anhedonic state that can only be overcome by more and more cocaine. Some users have also been drawn into a secondary dependency on tranquilizers and depressants, such as diazepam and barbiturates, which they take to combat the hyperstimulation and nervousness resulting from the cocaine.93 Awareness of its addictive potential, together with concern over its relation to street crime, has hardened public attitudes toward the drug and altered the tone of press coverage.94 Since 1965, cocaine has gone from complete obscurity to Public Enemy Number One.
Like many historical changes, the altered pattern of use has left linguistic traces. Prior to the 1960s government officials, when describing
their task, spoke unselfconsciously of combating the narcotic traffic. This was technically inaccurate-cocaine and marijuana were not narcotics—but it made practical sense because most of their arrests and the bulk of their seizures involved opiates. Since then, however, the word "narcotic" has been replaced by the more general term "drug," as in drug problem, or the still more capacious adjective "substance," as in substance abuse. This change was forced by the growing prominence of marijuana and cocaine, as well as the development of novel practices like glue sniffing or eating hallucinogenic plants and mushrooms. It made no sense, pharmacologically or otherwise, to lump these things together as ''narcotic use,'' let alone "narcotic addiction." Some researchers sought to expand the concept of addiction itself when they saw that dependence could develop with nonopiate drugs. "We should define addiction in terms of the compulsion to take the drug rather than whether it causes withdrawal," Dr. Michael Bozarth explains. "In this sense, cocaine is at least as addictive as heroin."95
Or, one might say, as addictive as alcohol. Even as new patterns of nonopiate dependence were emerging, there was distressing evidence that the nation's oldest psychoactive nemesis was strengthening its grip on the population. Per capita consumption of alcohol rose steadily, from 2.1 gallons per capita in the early 1960s to 2.8 gallons in the late 1970s. One 1977 poll revealed that seven out of ten Americans drank, and that nearly one in five considered liquor the cause of trouble within their families. Although health concerns and adverse publicity have reduced alcohol consumption somewhat during the 1980s, it is still higher than at any time during 1920-1965.96
The pattern of American drinking has changed as well. In the 1940s and 1950s, the most numerous imbibers by far were the straight drinkers, people who regarded any substance other than alcohol (or tobacco) as beyond the pale. "Our national drug is alcohol," wrote William Burroughs in 1956. "We tend to regard the use of any other drug with special horror."97 Ambivalence or outright hostility toward drug users persisted among straight drinkers after 1965. The reverse did not apply, however. Those who took drugs had no strong feelings against alcohol, tobacco, or other licit substances. On the contrary, they used them frequently. Some psychedelic enthusiasts of the 1960s preached that alcohol was a downer and that the faithful should renounce it, but they were disappointed by the response to their exhortations. The baby boomers were, so to speak, polypharmaceutically perverse. They cheerfully experimented with a range of illicit drugs while they drank alcohol and puffed cigarettes with their conventional elders. Linkages began to develop between their dependencies. Among recovering cocaine addicts, for example, drinking is one of the most common causes of relapse. Alcohol loosens their inhibitions;
it also reminds them of their previous cocaine use, which often took place in a bar or other surroundings in which drink was present. The memory triggers a sudden overwhelming longing, and they resume use of the drug.98
If the complex and shifting pattern of multiple drug use forced government officials to change the language they used to describe the problem, the same was true of treatment providers. The 1980s were marked by the emergence of "chemical dependency" treatment centers, many of them associated with private hospitals. These programs did not sharply differentiate between drug and alcohol abusers, as had been the rule in the past. Rather, they treated conventional alcoholics, drug abusers, and patients who manifested symptoms of both disorders. (Cocaine and alcohol were the most important combination.) Most patients treated in chemical dependency units were middle-class workers or their spouses and children who could finance their stays with employer-provided insurance benefits. Unemployed or self-employed workers of modest means, by contrast, had access only to publicly financed programs, which were becoming progressively more overcrowded and understaffed as the decade wore on.
The simultaneous, sustained increases in several types of drug abuse and the consequent growth in the number of addicted persons requiring treatment raise some important questions, particularly about law enforcement strategies. Why were the police and customs agents collectively unable to contain the importation and use of illicit drugs after 1965? Why did substances once comparatively rare become increasingly common? Why, despite larger budgets, expanded personnel, and more arrests, did the responsible agencies utterly fail to stop the influx of drugs?
The short answer is money. There was, in the first place, a great deal of money to be made from American users. It was not just that there were large numbers of adolescents in the 1960s and 1970s who were willing to experiment with drugs; it was that they had the wherewithal to do so. "I mean, these kids would say, 'Dad, I need fifty dollars so I can buy a tire,' or something," Agent Santangelo observed. "And Dad would give them fifty dollars."99 Not all of the money went to the B.F. Goodrich Company. When these same youth graduated and became financially independent, they had more discretionary dollars at their disposal and could afford more expensive drugs in larger quantities. Gradually, a new stereotype, the white-collar professional squandering his salary on cocaine, emerged and joined that of the street addict who stole to support his habit. The traffickers were indifferent to whether American customers financed their use through work or theft; what mattered was that the money, or the fence-able merchandise, was there. The United States and, secondarily, Western Europe were the most logical targets for drug
wholesalers because they were affluent, consumer societies, long on currency and short on moral strictures.100 They were the perfect markets, and drugs were the perfect products because they could create and sustain their own demand.
The huge profits to be made in the United States not only provided incentives to drug wholesalers but also bought protection for the traffickers through the familiar expedient of bribery. The extent of the corruption became clear in the early 1970s, when Detective Frank Serpico started talking to reporter David Durk of the New York Times. Durk's articles led to the formation of an investigative commission headed by Whitman Knapp. The Knapp Commission's 1973 Report on Police Corruption, which highlighted problems with narcotic enforcement, made headlines for months. Its revelations, however, seem minor in comparison to what was subsequently learned about graft at the other end of the drug pipeline. Theoretically, it is much easier to choke off the commerce at its point of origin, before the drugs are concealed, shipped, and dispersed. Yet it is in those countries where drugs are grown and processed that corruption is most deeply entrenched. The bribes are actually calibrated: $10 a kilo for marijuana smuggled across the border at Tijuana, for example, with the local police commander earning upwards of $150,000 a week. Not only do Mexican authorities look the other way, they provide armed escort service for major shipments. They have also been known to torture, possibly to kill, interloping American narcotic agents. Some trafficking organizations, like the Shan United Army, which operates along the Burma-Thailand border, are so large and well armed that they do not need to infiltrate governments; they are themselves autonomous political entities. Worldwide, the illicit narcotic industry has revenues estimated by some at a half-trillion dollars a year; it is easy and expedient to divert a fraction of the cash flow to protecting exports. Anyone who can stock Monopoly games with real money can afford a few strategically placed government officials. It is simply a matter of rationalizing risk.101
The problems of enforcement in the drug-producing countries are compounded by the global economic and political situation. Many of these nations are poor and, like Mexico, burdened by international debts. Drugs are a vital source of revenue, not only for their governments, but for the peasants who can earn more by cultivating poppies, coca, or marijuana than by producing licit commodities. In Bolivia, for example, lawful exports now produce only a fraction of the revenue brought in by cocaine, which is responsible for half of the country's gross national product.102
Despite their growing dependence on drug trafficking, Bolivia and other Latin American countries were widely supposed by U.S. officials to be targets of Communist subversion during the 1980s. This created a conflict of interest: the State Department and the CIA sometimes wished
to protect, for their own geopolitical reasons, the same governments that the Drug Enforcement Administration suspected of complicity in smuggling. The 1989 ouster of Panama's General Manuel Antonio Noriega is the exception that proves the rule. Information implicating Noriega in drug trafficking has been available since 1972. For years this information was simply ignored. The CIA has gone so far as to treat major traffickers as national security "assets," using their organizations for gun-running and counterinsurgency operations.103 Foreign policy and antinarcotic efforts were occasionally at cross-purposes during Anslinger's era,104 but on the whole he was successful at keeping the two in alignment. This is no longer the case. Domestic demand, unreal profits, systematic corruption, economic dependency, inconsistent diplomacy—for all of these reasons the interdiction strategy has had difficulty stanching the flow of drugs into the country.
The sense that illicit drug trafficking and use were out of control led to the present war on drugs. The formal declaration came on August 4, 1986. President Ronald Reagan delivered a major speech "not to announce another short-term government offensive but to call instead for a national crusade against drugs-a sustained, relentless effort to rid America of this scourge—by mobilizing every segment of society against drug abuse." He called for the elimination of all drugs from workplaces and schools; voluntary (or, for key government personnel, mandatory) drug testing; improved treatment and rehabilitation programs; greater public intolerance of drug abuse; and stepped-up enforcement against domestic and international traffickers. In remarks to Republican congressmen before the address, Reagan set as his overall goal a 50 percent reduction in drug use and promised that his escalating war would mean "Pearl Harbor for the drug traffickers."
A little more than a month later, on September 14, 1986, the President made a nationally televised address, accompanied by First Lady Nancy Reagan. Again Reagan relied on martial metaphors, drawn from World War II. Americans would have to swing into action, he explained, the way they did in the 1940s, when men and women rolled up their sleeves, built tanks and planes, and planted victory gardens. "We're in another war for our freedom, and it's time for all of us to pull together again," he said. The First Lady was equally adamant. This was a total war, a war in which there could be no middle ground. Do not use drugs, and do not tolerate those who do. Firm, private refusals would create an "outspoken intolerance for drug use" and would influence by example young people who might otherwise experiment with drugs.105
There is some truth in this insight. Peer disapproval is more powerful than remote, impersonal laws; the host or hostess who says no is more effective than the prosecutor downtown. The difficulty lies in engineering
such a massive change of attitudes and behavior, particularly among young adults accustomed to and tolerant of drug use. Many legislators, although willing to fund educational programs toward that end, have also resurrected the Anslingerian tactic of stiffer penalties for dealers, up to and including execution. The death penalty was, in fact, the most widely discussed aspect of the 1986 omnibus antidrug bill. Although capital punishment for major traffickers convicted of murder (a transparently political provision favored by House members up for reelection) was blocked by the Senate, the bill that did pass nevertheless specified longer prison sentences for those who recruited juveniles to sell drugs or those who sold drugs near schools. The law also authorized $1.7 billion in additional expenditures, with most of the money to go for law enforcement and drug education.106 Two years later, just before the 1988 general election, Congress passed a second omnibus bill. This time a capital punishment provision was included, as well as substantial new civil penalties for personal use and possession. The get-tough tone has continued into the Bush administration: the White House's 1989 National Drug Control Strategy was unapologetically martial in tone and stressed the need to win back the streets from users and dealers. The pendulum seems to be swinging back to the 1950s; we may be entering a "neoclassic" era of drug control.
Is this a wise departure? Or, to put it another way, was the medicalization of the narcotic problem, the legitimatization of a hybrid approach in the 1960s and 1970s, a bad idea? Would the country have been better off if Anslinger had not retired, if he and his successors had been permitted to maintain an unwavering hard line?
The answer is almost certainly no. Although it may be true that superimposing a clinical treatment model on a criminal justice base signaled official ambivalence to the public, it is doubtful that this produced many new users. There is one school that argues just the opposite, that criminalization inevitably glamorizes a drug.107 The use of LSD, for example, peaked five years after it was made illegal; a few thousand users in 1966 swelled to an estimated 5 million by 1971.108 This does not prove that criminalization caused increased use—that would be post hoc, ergo propter hoc reasoning—but it does suggest that the laws made little concrete difference.
The point can be generalized. Drug policy is best understood as a congeries of a society's history, values, and prejudices. It is not, in and of itself, the key variable governing the extent of drug use at a given point in time. Prevalence is more likely to be determined by outside events. These include wars, epidemics, population shifts, new technologies and pharmaceutical discoveries, physician behavior, economic conditions, media coverage, and changes in moral attitudes and religious beliefs. It should be remembered that Anslinger was head of the Bureau of Narcotics at a
time when Americans were firmly opposed to narcotic use, when the press acted as his claque, smugglers lacked high-powered racing boats and Lear jets, and LSD, DMT, PCP, and other acronymic drugs were as yet unfamiliar to the public. These were far greater advantages than the Boggs Act. When circumstances changed, when the antinarcotic consensus eroded, the underclass grew and festered, new drugs became fashionable on campus, and hundreds of thousands of American troops were sent to fight in opium-rich Southeast Asia, then the scope of the problem was bound to widen. One factor alone, the coming of age of the nearly 80 million Americans born between 1946 and 1965, ensured an upsurge in drug use; in epidemiological terms, there was an unusually large number of susceptibles in the population immediately after the classic era.
Although government policy does not solely determine the prevalence of drug use, it does affect the health and behavior of the users themselves. The most important impact of punitive drug laws is on consumers, especially those who are addicts. Their hustling activities, patterns of association, routes of administration, risks of illness, and prison histories have all been shaped by the prohibition policy and its corollary, the black market. Mainlining, for example, was unknown before 1915, when addicts did not have to purchase adulterated narcotics. It is true that the preaddiction characteristics of users took a turn for the worse during the early twentieth century and that numerous addicts would have led difficult, unhealthful, and crime-filled lives with or without the assistance of the Bureau of Narcotics. The point is that their troubles, and those of the people they victimized, were exacerbated by legal strictures. Policy analyst Mark Kleiman has called this exacerbating tendency the paradox of vice control:
We make something illegal because it's a vice—bad for its devotees and bad for people around them. But for those who indulge anyway, prohibition and enforcement make the vice more dangerous; they also make these people more dangerous to the rest of us. Think of wood alcohol during Prohibition, the violence and disease associated with prostitution, the gambling debts collected by muscle rather than collection agencies.
That this paradox exists does not mean we should legalize everything—it seems to me that society is better off with 400,000 very dangerous heroin addicts obtaining the drug illegally than with 5 million addicts obtaining the drug from their doctors, even though each of them would be a little better off and a little less dangerous. It does mean that we don't get a free shot at drug dealing.109
Anslinger understood that his shot (or, more accurately, cannonade) at all types of drug dealing ultimately had to be based on some sort of least-misery-for-the-least-number rationale. That was why he continued to
rail at the narcotic clinics and "dope doctors" long after they had been suppressed; they were the floodgates that must remain closed lest the country become awash with narcotics. For three decades he managed to convince the government and the public of the correctness of his utilitarian calculation, thereby maintaining "a policy of narcotics control unlike that of almost every nation in the world."110 It was, nevertheless, a case built on bluff and intimidation. There is no objective evidence to support the idea that disallowal of maintenance saved the country from a series of mid-century narcotic epidemics.111 If the narcotic clinics had not been closed back in 1919-1920, if medical discretion and supervision had been permitted within the context of detoxification-or-maintenance programs, and if this approach had been widely emulated, then incalculable suffering, crime, and death could have been averted. Those who contemplate a purely preventative strategy for the future, who trust only in education and legal pressure, would do well to contemplate the implications of this. The combined medical-police approach, with all its contradictions and weaknesses, is by default the best policy available. The tragedy is that the country did not recognize this 40 years sooner.
Notes
|
|
of the Committee on the Judiciary (Washington, D.C.: U.S. Government Printing Office, 1974), 7-8; Institute of Medicine, Marijuana and Health (Washington, D.C.: National Academy Press, 1982), 36; Glenn Collins, "U.S. Social Tolerance of Drugs Found on Rise," New York Times, March 21, 1983, Al, B5; James Mills, The Underground Empire: Where Crime and Governments Embrace (New York: Doubleday, 1986), passim; Christine Russell, "One-Third of College Students Try Cocaine... Use of Marijuana and Other Drugs Appears to Have Declined," Washington Post, July 8, 1986, A3. |
|
80 |
Interview with Peter Santangelo, August 23, 1982. |
|
81 |
Institute of Medicine, Marijuana and Health, 37. |
|
82 |
Denise Kandel, "Stages in Adolescent Involvement in Drug Use," Science 190 (1975), 912-914, and Bruce D. Johnson et al., Taking Care of Business: The Economics of Crime by Heroin Abusers (Lexington, Mass.: Lexington Books, 1985), 182, 226-229. |
|
83 |
Table 1 in Kandel, above; 1982 National Household Survey on Drug Abuse data reproduced in Collins, "U.S. Social Tolerance," B5. It is also of interest that, among those who did progress to heroin, many apparently took precautions to avoid full-blown dependence. Heroin's reputation as an addicting drug preceded it. See Norman E. Zinberg, "Nonaddictive Opiate Use," in Criminal Justice and Drugs, especially 15. |
|
84 |
Carl D. Chambers and Leon G. Hunt, "Epidemiology of Drug Abuse," in Pradhan and Dutta, eds., Drug Abuse, Table 2-2, 13; Irving Faber Lukoff, "Consequences of Use: Heroin and Other Narcotics," in Joan Dunne Rittenhouse, ed., Report of the Task Force on the Epidemiology of Heroin and Other Narcotics (1976), 124-126; Leon Gibson Hunt, "Prevalence of Active Heroin Use in the United States,'' and S.B. Sells, ''Reflections on the Epidemiology of Heroin and Narcotic Addiction from the Perspective of Treatment Data," both in Joan Dunne Rittenhouse, The Epidemiology of Heroin and Other Narcotics, NIDA Research Monograph 16 (Rockville, Md.: Alcohol, Drug Abuse, and Mental Health Administration, National Institute on Drug Abuse, Division of Research, 1977), 63-78 and 161-163, respectively; John C. Ball et al., "Characteristics of 633 Patients in Methadone Maintenance Treatment in Three United States Cities: 45 Preliminary Tables" (Report of the Methadone Research Project, 1986), Table 602. Sells remarks, "[a] polarity can be observed between low socioeconomic level street heroin users, at one extreme, and the youthful, middle class, maladjusted, nonopioid users, at the other" (163; italics in the |
|
|
Dark Paradise. There was a long-term decline in the total number of narcotic addicts between 1910 and 1940, but this was due primarily to a decline in medical addiction. Very few new medical addicts were being created and many old ones, left over from the nineteenth century, were dying off. The Bureau's efforts were targeted at nonmedical addicts, and their numbers did not appreciably diminish, except during World War II. |






























































