
3
Engaging Large and Diverse Populations for Analysis
One potential source of data for genomic medicine implementation research is cohorts that have been assembled for discovery purposes.1 This chapter examines a genomics biobank operated by a large regional
___________________
1For more information and background reading on large genetic cohort studies, see Appendix F.
health care system, a genomics research network in Québec, and an innovative program designed to boost racial and ethnic minority participation in genomics research.
A GENOMICS-FOCUSED BIOBANK
The Geisinger Health System, based in central Pennsylvania and southern New Jersey, is an integrated health services organization that has made a commitment to genomics and personalized health care, said Andrew Faucett, the system’s director of policy and education. Geisinger is working to make the system a learning health laboratory characterized by a continuous cycle of integrated innovation, implementation, assessment, and reengineering in all aspects of its clinical and research mission. To do so, Geisinger is engaging and partnering with its patients and others in the community.
The Geisinger Health System serves a geographic area with a large, stable population of more than 2.5 million people and has more than 700,000 active patients, including many families of three or more generations, Faucett said. Geisinger has a strong and trusting relationship with its patients, he added. Having used the same electronic health record (EHR) system since 1995, the system has compiled comprehensive clinical data.
Geisinger is currently discussing options for storing genomic data within the EHRs. Genomic data in EHRs could be useful in generating automatic notifications of family members, Faucett said, and the EHRs could be provided to children and grandchildren. From a care perspective, Faucett said, it would be much easier if a patient could say something such as “I know my uncle has a Lynch Syndrome mutation” and the clinician could then simply identify the mutation and offer the patient testing instead of asking the patient’s uncle to return a signed release. “The more we can automate it with permission, the easier it will be,” he said.
The Geisinger patient population does not have much racial or ethnic diversity, Faucett said, but it does have a great deal of socioeconomic diversity. Central Pennsylvania has one of the highest poverty rates in the United States, and access issues often arise because many people live in rural communities. For that reason, he said, care close to home is part of the Geisinger model. Roughly half of Geisinger patients do not have dependable Internet access in their homes, he said, and they depend much
more on smartphone access. Those patients involved in genomics studies need quick access to information, he said, because they can very quickly become extremely concerned once they learn of their test results. “You have to have folks in place who can quickly intervene” and talk through the results with them, Faucett remarked.
Outreach
A major component of the Geisinger research vision, Faucett said, has been an online genomics data system and biobank known as MyCode®.2 One of the goals of the MyCode biobank is to help researchers gain a better understanding of the impact of genes on human health and disease states. Additionally, Geisinger hopes that information from this resource will assist in the development of tailored therapeutics, bringing its clinicians and patients one step closer to precision medicine. Community engagement has been an essential element of developing and operating the MyCode system, Faucett said. In 2006, prior to launching MyCode, Geisinger organized focus groups from the general patient population to explore the idea of a genomics database. Focus group discussions were centered on pharmacogenomics, recessive carrier status, increased risks for both preventable and treatable conditions as well as conditions that are not preventable and treatable, and genetic changes that are not currently understood. The Geisinger system provides additional outreach to the community through regular updates in the form of newsletters, and it encourages employees to participate in MyCode.
Geisinger is very interested in engaging families in preventive genomic medicine, Faucett said, in part because many of its patients come from large families. Moving forward, the system is considering bringing on more genetic counselors, reaching out to large families at reunions, and using online venues to “get the word out in a large volume without having to see each person individually.”
Return of Results
Geisinger also convened an additional six focus groups in 2012 prior to implementing procedures regarding the return of research results. One major outcome from the 2012 focus groups was the realization that par-
___________________
2For more information on MyCode, a biobank program within the Geisinger Health System, see http://www.geisinger.org/for-researchers/partnering-with-patients/pages/mycodehealth-initiative.html (accessed February 22, 2016).
ticipants wanted all results returned to them, Faucett said. “They were not comfortable with [results] going just to the health care provider, which is often what we want to do as a medical practitioner,” he said. The participants were fine if the results went to the health care provider first, but they wanted to have access to their own results, he explained. As the system is currently set up, providers receive the results about 5 days before system participants.
Participants receive information on genetic variants that have been identified as “actionable” by the American College of Medical Genetics and Genomics (ACMG), plus a few others that are not included on the list (Green et al., 2013). Geisinger does not currently examine pharmacogenomics variants because it is not equipped to return the results of these findings. Clinicians are willing to use pharmacogenomics if the data are already in the record, Faucett said, but they are not currently willing to order a test and wait to make a decision. “Our long-term goal is that this type of information will be available on every patient,” he said.
Faucett characterized the system’s work in genomics as a fusion between an academic and a business approach. Geisinger was interested in performing exome sequencing as a way of understanding the genome, but as a health care institution it also felt that it was unethical to have that information and not give something back to the patients. “That’s why [Geisinger] took the ACMG list and said, ‘Let’s return this, and let’s study it as we return it,’” Faucett said. There are economists involved with this work, but it is not currently classified as a formal implementation study. “We need more people and more money to do it that formally, but we’re trying to look at all of those issues.”
The return of results to patients is being modified based on real-time feedback. The overall intent, Faucett said, is to start with national recommendations and tailor those recommendations from within the system’s population. “It needs to be tweaked for each [Geisinger] location,” he remarked, reiterating one of the goals of implementation science which is to adapt and refine practice change strategies based on the characteristics of a particular setting.
Participants in the 2012 focus groups also requested educational materials on genomics for clinicians and for patients. Focus group participants had a lot of respect for their clinicians; however, Faucett said, they requested educational materials and an expert support system for providers and patients. Patients were comfortable with results being put in their EHR and liked the idea that their records are available throughout the system.
Engaging the Community
There is an ethics advisory committee in place for the MyCode program which includes four nationally recognized ethics experts and four local patients. The committee has worked diligently on the consent form which provides guidelines for recontacting patients, collecting longitudinal samples, returning results, placing results in the EHR, and online consent. The consent has been repeatedly revised, Faucett said. “It’s a process between the researchers, the institution, and the institutional review board. Clearly, back in 2006 everyone was terrified of genetic results; no one wanted them in the electronic medical record. . . . Now our philosophy is that returning results should be the standard practice.” Progress has been gradual but steady, Faucett said, and they are becoming more comfortable with the precision medicine movement.
Engaging the providers is also important, Faucett continued. Geisinger has taken a multifaceted approach to engaging providers, including
- An oversight committee that handles the return of results
- Frequent presentations to clinical and administrative leaders across the system
- A genetic counselor who networks with physicians and administrators
- Regular symposia that provide information on specific genomic test results
- Short courses for each of the conditions for which results are being returned
- Fact sheets and other educational materials for providers
The consent rate for MyCode is currently at 85 percent, with 98,000 individuals currently in the biobank and 88,000 of those allowing the return of results, Faucett said. Through a new partnership with Regeneron Pharmaceuticals, Inc., Geisinger is working to perform whole-exome sequencing. Thus far, whole-exome sequencing has been performed on 52,000 participants, with 44,000 of those agreeing to the return of results. The enrollment goal for the whole exome sequencing study was recently increased to 250,000 patients.
GENOMIC RESEARCH IN QUÉBEC
With a population of about 8 million, Québec spent about $45 billion on health care in 2012, representing approximately half of the province’s budget, according to Marc LePage, president and chief operating officer of Génome Québec. Per capita health care expenditures in Québec are the lowest of any province, so Québec has been successful at cost containment, LePage said, but the province has not been particularly adept at launching new innovations. To remedy this deficiency, Génome Québec was launched in 2000 and is one of six regional genomics centers that are part of a national program called Genome Canada. The mission of Genome Canada is to develop and apply genomics-based technologies that provide social and economic benefits for the Canadian population. Génome Québec has faced several challenges in its quest for accelerating the discovery of new genomic applications, which LePage described, together with solutions to overcome these barriers.
Establishing a Biobank to Foster Research and Innovation
In partnership with McGill University in Montreal, the Génome Québec program has an innovation center which includes a sequencing platform, a clinical genomics facility, and several broadly distributed population cohorts. One arm of the program, known as the CARTaGENE Biobank, is one of five regional population health projects that are part of the Canadian Partnership for Tomorrow Project (CPTP). CARTaGENE serves as a long-term bioresource that is collecting biological samples and data that are representative of the genomic diversity of Québec’s population. CARTaGENE was established with the goal of collecting more complete information about genes, environment, and lifestyle across the population and subsequently making that information easily accessible to researchers. During its first recruitment phase, CARTaGENE enlisted 20,000 participants. Participants range in age from 40 to 69 years old, and samples are collected at 12 clinical sites in four urban centers, LePage said. The data available for this cohort include answers to health questionnaires, biological samples, (including blood, saliva, urine, and cell samples), physical and clinical measures, genealogies, and nutrition and environment surveys. A second and ongoing recruitment phase has a goal of enlisting another 20,000 participants of the same ages. CPTP has been quite successful, LePage said, and it now has samples from close to 300,000 participants (Borugian et al., 2010).
To encourage innovative discoveries within the realm of genomic medicine, Génome Québec organized a Genomics and Personalized Health Competition. The request for applications was specifically designed to include a requirement for outlining implementation strategies, LePage said. For example, researchers who applied for the competition were asked to provide an implementation roadmap as part of their proposals. Competition winners received funding to complete their projects. The winning projects, now underway, cover a wide array of fields including genomics drug discovery, breast cancer detection strategies, prenatal testing, and the development of tools to advance diagnosis and treatment. With a solid foundation in basic research, Génome Québec has also become involved in technology-focused genomics and clinical applications, LePage said.
Garnering Support from Clinical Leadership and Other Challenges
Part of Génome Québec’s mission is to maximize the socioeconomic impact of genomics innovations.3 Initially Génome Québec experienced difficulty in gaining support from government leaders such as the Minister of Health and Social Services, LePage said. However, after observing the program’s success, Québec’s Ministry of Health has undergone a change of perspective, he said, and now seeks to shape rather than resist genomic initiatives. This positive change also occurred in the regulatory sphere where internal expertise at Génome Québec was initially lacking but has now been bolstered so that regulators can do an informed review on genomics applications, LePage said.
One major change that has taken place is that projects funded by Génome Québec are now often being led by clinicians rather than fundamental scientists, LePage reported. Health economists, ethicists, and regulatory personnel are working in parallel rather than in sequence to speed up implementation. The focus of the projects has been on deliverables and outcomes rather than on processes and methods, LePage said. “We’re starting with the clinical problem and working back.”
The chief executive officers of health care systems would really benefit from hearing this dialogue, observed Geoffrey Ginsburg, the roundtable’s co-director and the director at the Duke Center for Applied Genomics & Precision Medicine. Ginsburg went on to stress the importance of engaging experts in implementation science together with
___________________
3For more information on the mission and activities of Génome Québec, see http://www.genomequebec.com/en/who-we-are.html (accessed February 23, 2016).
leaders of health care systems to leverage the principles of implementation science.
Génome Québec is finding it challenging to align its databases and clinical infrastructure, LePage said. Génome Québec is trying to unite those entities now, in part through data harmonization and coordination of best practices across the portfolio. “We haven’t got it solved, but we are working on it,” he said. For now, genomic sequencing is only offered as part of research projects and not universally across the board, and program leaders are still trying to decide if universal sequencing is advisable. A current challenge is to decide whether sequencing a subgroup might yield information of clinical value, LePage said.
Effective communication with the public about genomics research and implementation has been a challenge for Génome Québec, LePage said. However, many people in Canada are eager to participate in biobanks, he said, because the Canadian public health care system is there when you have a problem, and as an individual you want to give something back. However, he also said that Canada is the only major country in the Organisation for Economic Co-operation and Development without a genetic privacy law, which means that confidence in the system could be damaged if privacy became a concern. In addition, genomics centers in Canada have been able to reach populations in urban centers and rural areas, but they have had trouble reaching out to people in aboriginal communities. These communities, LePage said, “are up in the north; they’re isolated; they have substandard care; plus they’re in a different health care system.” An Institute of Aboriginal Studies exists in Canada and is working through some of the issues related to those populations, he added.
INCLUSION OF RACIAL AND ETHNIC MINORITIES
The inclusion of racial and ethnic minorities in research requires specialized expertise and extra effort, yet most researchers know very little about effectively engaging stakeholders in the research process, said Consuelo Wilkins, executive director of the Meharry-Vanderbilt Alliance and an associate professor of medicine at the Vanderbilt University Medical Center. There is very little emphasis on methods for engaging individuals in the research process during graduate-level training programs, she noted.
Vanderbilt University has developed a program called the Community Engagement Studio which is designed to enhance the planning, design, implementation, translation, and dissemination of clinical research.4 Researchers can arrange for an advising session at the studio at any stage in the process from pre-implementation to recruitment, implementation, and dissemination. Staff members at the studio are trained to identify and recruit community members who can serve as patient stakeholders for a particular research project. Those community members learn about the research project and then provide input to the researchers, essentially acting as consultants.
Members of the Community Engagement Studio were able to advise a researcher who had been unable to recruit any African American women for a study, Wilkins said. Studio members offered guidance on how to redesign the recruiting material, on where to promote the study, and on language sensitivities involving obesity and the risk for diabetes. With this help, the researcher met the accrual goals ahead of time and had 100 percent retention in a randomized, placebo-controlled trial of a drug.
Communication involves not just recruiting members of a specific population to participate in a study but also helping them to understand and act on genetic test results, Wilkins said. According to an unpublished Vanderbilt survey cited by Wilkins, genomic literacy varies by population group, with terms such as “pharmacogenomics,” “genetic testing,” and “precision medicine” being more or less familiar to members of different groups. “Of Caucasians who responded, 76 percent were extremely or moderately familiar with genetic testing, but only 54 percent of African Americans were,” Wilkins said.
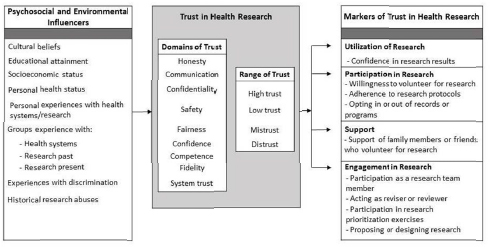
Another critical issue in engaging minority communities in research is trust, Wilkins said. “Trust is one of the most commonly cited barriers to African Americans and other racial and ethnic minorities participating in research, but it is rarely measured.” Wilkins and her colleagues have developed a conceptual framework for measuring trust in research (see Figure 3-1). When members of more affluent or dominant groups think about trust, Wilkins said, they focus on such issues as competency, honesty, and fidelity. By contrast, members of marginalized groups tend to be more concerned about whether they will be treated fairly or exposed to adverse risk. “We need to understand that and think about how we will make sure that [minority groups] are comfortable participating in the
___________________
4For more information on the Community Engagement Studio, see https://medschool.vanderbilt.edu/meharry-vanderbilt/files/meharry-vanderbilt/public_files/CES-Toolkit-web. pdf (accessed February 22, 2016).
work, and how will we understand what their concerns are and address them, not ignore them or pretend that they don’t exist,” Wilkins said.
Specific barriers to establishing trust in genomic medicine among minority groups include the eugenics movement, discrimination against people with sickle-cell trait, the potential loss of benefits or income if a genetic result is linked to a health condition, the use of DNA in the criminal justice system, and findings linked to genetics that may contradict cultural or ancestral beliefs, Wilkins said. It is important to be careful about how research findings are presented in order to ensure that the findings are seen as inclusive and not insensitive to particular populations, she added.
Strategies for recruiting and retaining minorities in research include: performing accurate feasibility assessments, staffing the program adequately with personnel experienced in engaging minorities, and devoting additional effort to retention, Wilkins said. For example, engaging populations of interest requires carefully tailored recruitment materials, appropriate language in consent forms, seeking advice on recruitment strategies, demonstrating respect and value, and offering appropriate compensation.
SOURCE: Consuelo Wilkins, National Academies of Sciences, Engineering, and Medicine workshop presentation, November 19, 2015.
“Most researchers underestimate the amount of time and resources that are required to engage minorities in research,” Wilkins concluded. “I often get called to help researchers when they’re stuck and not able to reach their recruitment goals. Even when I come up with a plan . . . it often requires 30 to 50 percent more time and research staff to actually recruit minorities into research.” And even if a particular strategy works in one group, it will not automatically translate to another group, she said.
Considering Evidence and Coverage Issues
Implementation science aims to develop generalizable knowledge, but the question is, “Generalizable to whom?” said Alexandra Shields, an associate professor at Harvard Medical School and Massachusetts General Hospital. Poor and minority communities are often missing from the evidence base, Shields said. Much of the evidence currently available is built on discovery databases drawn almost entirely from people of European ancestry (Knerr et al., 2011). “This is an issue that we need to take seriously, given the diversity that we know exists,” she said. Researchers have a responsibility to investigate the source populations upon which evidence was developed, she added, and if the evidence is not based upon a diverse set of populations or patient samples, then additional studies may need to be conducted.
Shields also recommended that implementation research should be applied not just to the genetic test itself, but to the clinical care that follows after the test results are received. This includes the follow-up that ensures that the patient gets the care indicated by the test results. In that respect, implementation research could be applied to a bundled set of health care services, Shields observed. She went on to emphasize the importance of Medicaid and the Affordable Care Act coverage as being critical to the health care that patients receive. If Medicaid does not cover genomic services in a particular state, the poor may not have access to these treatments, Shields noted. A systematic analysis of the coverage of genomic services may provide valuable information about the extent to which people can access these services, she said.
Paying careful attention to the characteristics of an organization is important for designing effective implementation strategies, Shields said. For example, safety net hospitals and community health centers that serve disadvantaged patient populations may not see genomic medicine as important relative to the health needs of their populations, such as substance abuse, hepatitis C infection, and HIV infection. “We need to
strategically engage those provider groups . . . in how they conceive of genomics relative to these other health conditions,” Shields said.
Timing the Thinking About Implementation
When is the most appropriate time to introduce implementation science into the translation of results into clinical applications? Patient advocates involved in the grant review process have become increasingly concerned about the impact of research, said Jane Perlmutter, president and founder of the Gemini Group and a patient advocate and cancer survivor. Involving patients and advocacy groups during the early stages of research design “has helped make sure that [researchers] at least think about the path from what they’re doing to how it will impact patients,” she said.
It is possible for researchers to think about implementation too early in the process, particularly if they try to push a finding into the clinic prematurely, said Brian Mittman of Kaiser Permanente Research. “Those of us who are conducting research and developing innovative practices always feel very strongly that what we’ve developed needs to be implemented and spread about, when in fact we should be waiting until we have a good solid body of evidence.” Nevertheless, planning for implementation and implementation research does need to start very early, he added. For instance, with the development and implementation of clinical practice guidelines, the implementation team should be “involved in the process from day one, helping to develop the guidelines, helping to understand the evidence and the controversies, helping to identify ways of wording the recommendations, and providing the supporting justification,” Mittman said. If this were to happen “the implementation process would be much simpler,” he concluded.












