
2
Exploring Challenges to Developing Treatments for Pain and Opioid Use Disorders
Given the complexity of chronic pain and opioid use disorders, many workshop participants discussed challenges to advancing the discovery and development of new treatments, including the complex experience of pain, a lack of resources to treat pain, insufficient understanding of pain mechanisms, and limitations in conducting clinical trials.
THE COMPLEX EXPERIENCE OF PAIN
Christin Veasley reminded workshop participants that everyone who lives with chronic pain experiences it differently. Moreover, she said, although a survey by Research!America Analytics found that about two-thirds of respondents said they know someone who experiences “pain so severe that they sought prescription medications to treat it,” only 18 percent described pain as a major public health problem (Research!America, 2013). She also said there is a disconnect between how the public views and defines pain and chronic pain compared to the perspectives of researchers and clinicians.
The experience of chronic pain is very complex, said Veasley. Many people with chronic pain have multiple diagnoses that contribute to their experience of pain, yet these classifications and diagnoses may lack meaningfulness to patients who simply say they have chronic pain. In addition, people experience pain differently from a biopsychosocial perspective, she said. So, for instance, while one person with fibromyalgia may have fatigue and impaired psychosocial function, another may have a sleep disorder, depression, and dyscognition. These co-occurring symptoms combine to create a unique experience for each individual, said Veasley. Nora
Volkow added that pain is variable over time, with some syndromes having exacerbation of pain later in the day. This could be explained by social processes such as less activity and distraction at the end of the day, that is, without the distractors patients are more aware of the pain sensation, but this also could reflect circadian variability, she said.
Stigma and personal biases also influence how the public views people with pain, said Veasley. Due to recent awareness efforts, families, friends, and workplaces find it acceptable for someone to have a diagnosed chronic pain disorder; however, due to the continued stigmatization surrounding pain, many still consider it a “weakness” if the person allows the pain condition to impact his/her productivity and ability to function in various professional and social roles. Also related to stigmatization is the criminalization of pain, when people suffering from chronic pain are perceived as criminals or encounter increased scrutiny because of their pain management treatments (Terplan, 2017). Having chronic pain does not mean that you are an opioid user, and being an opioid user does not mean you are an opioid abuser who would engage in illegal activities to access the drug, said Veasley. Even those who have an opioid use disorder deserve the best, most humane, and empathic medical care, she said.
INSUFFICIENT RESOURCES TO TREAT PAIN
From a clinical perspective, Veasley noted a shortage of pain specialists; insufficient training on pain for primary care providers; a lack of team-based, multimodal, coordinated treatment; and a meager evidence base on which to assess benefits and risks of any treatment approach. Sharon Walsh added that there are barriers to using drugs currently available. For example, prior authorization may be needed before buprenorphine can be given at discharge from the emergency department. She also cited the need for higher affinity and efficacy therapies for both overdose and maintenance, particularly in light of the availability of fentanyl and fentanyl analogues, as well as a need for better data about who is at risk of repeat overdose. Scott Powers, professor of pediatrics at the University of Cincinnati College of Medicine, noted that the discovery and development of novel treatment approaches will also require a better understanding of reasons for adherence and non-adherence, and strategies to maximize adherence. William Maixner, director of the Center for Translational Pain
Medicine at Duke University, added that reimbursement is poor for multidisciplinary services, biopsychosocial approaches, and non-opioid-based approaches to treat pain.
Volkow suggested that combinations of medications may be needed to make a meaningful difference in the lives of people with chronic pain, opioid use disorders, and complex co-morbidities, yet the regulatory approval process for combinations of drugs can be particularly daunting.
INSUFFICIENT UNDERSTANDING OF PAIN MECHANISMS
To achieve the Federal Pain Research Strategy priority of identifying new, non-addictive pain therapies and treatments for opioid use disorders, Porter noted that a deeper understanding of pain mechanisms will be needed. Pain is a highly heterogeneous, multisystem illness that involves the neurological, endocrine, and immune systems, yet few animal or human models account for this complexity and heterogeneity, said Veasley. In complex diseases such as pain, thousands of genetic modifiers influence risk, noted Clifford Woolf, professor of neurology and neurobiology at Harvard Medical School and director of the F.M. Kirby Neurobiology Center at Children’s Hospital Boston. Genes may also modulate the transition from acute to chronic pain, said Volkow. Other neural mechanisms that underlie the acute-to-chronic pain transition are also not well understood, said Maixner. Woolf added that most preclinical models are built around evoked pain rather than spontaneous pain, although the latter is the most common complaint of patients. Tony Yaksh, professor of anesthesiology and pharmacology at the University of California, San Diego, and John Kehne, program director in the Division of Translational Research at the National Institute of Neurological Disorders and Stroke, both said that preclinical research in pain, as in many other disease areas, has been plagued by a lack of reproducibility.
UNDERSTANDING CHALLENGES IN CONDUCTING CLINICAL TRIALS
Elevated placebo responses in pain trials have made it difficult to demonstrate efficacy in clinical trials, said Tor Wager, director of the Cognitive and Affective Neuroscience Laboratory at the University of Colorado Boulder. He commented that the biological, genetic, and
neurocircuitry mechanisms underlying the placebo response are complex, poorly understood, and entangled with many emotional, experiential, cultural, and cognitive factors. Andrew Ahn, chief scientific officer for pain and headache at Eli Lilly and Company, added that placebo responses may also be affected by the natural history of the disorder (e.g., the frequency of pain attacks) and expectations about the treatment. Wager stated that statistical artifacts further compromise understanding of placebo responses.
Clinical trials have also been hampered by inadequate measures of pain that incorporate sleep, mood, fatigue, and function, said Veasley. Seena Ajit, assistant professor of pharmacology and physiology at Drexel University, added that the role of circadian variability in pain responses has not been studied from the perspective of different biomarkers of pain, including neuroimaging and miRNA markers.
Conducting efficient clinical trials has also been limited by implementation barriers. Ahn noted that pain is generally treated by primary care physicians, whose practices are not set up to allow comprehensive assessment of the problem or to deliver much-needed multidisciplinary care. Walsh added that few providers and Federally Qualified Health Centers offer treatment for opioid use disorders.
Yaksh and Walter Koroshetz said that progress in clinical trials has also been slowed by inadequate sharing of data and knowledge about preclinical and clinical pain therapy development, and the science of addiction. Furthermore, Jessica Hulsey Nickel noted that because there is inadequate reimbursement for drugs that treat addiction or reverse overdose, pharmaceutical companies lack incentives to develop these treatments.
THE PENDULUM SWING OF CARE: UNDERSTANDING PATIENT NEEDS
Veasley said there has been a pendulum swing in the medical scientific world when it comes to managing pain (see Figure 2-1). On one extreme of the pendulum, no one is prescribed opioids, there is a basic science research focus, biological measures with little to no self-report are used, and patients are not involved in the research process. On the other extreme of the pendulum, opioids are used more frequently, and translational and clinical science research has increased, with a focus on objective biological measures as well as patient-reported outcomes. Placebo-controlled trials
are being supplemented with pragmatic real-world trials, and patients have become an integral component of the research enterprise. The challenge is finding a balance between the two extremes and what is best for the patient, Veasley said.
Potential opportunities presented by individual workshop participants to address these challenges are highlighted in succeeding chapters.
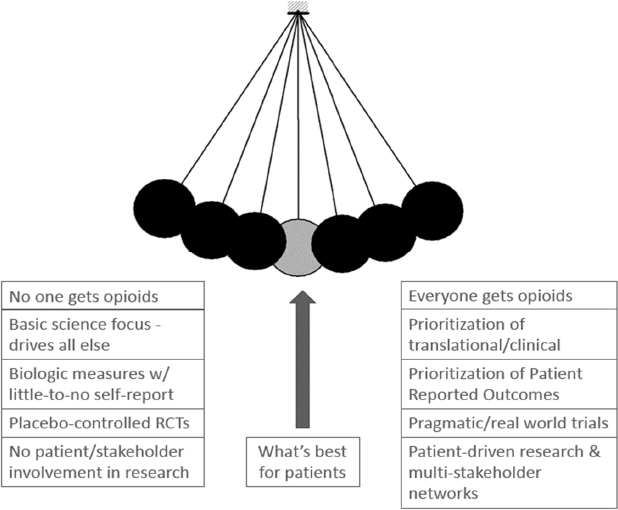
NOTE: RCT = randomized controlled trial.
SOURCE: Presented by Christin Veasley, October 11, 2017.
This page intentionally left blank.






