
Executive Summary
Approximately 200,000 women currently serve on active duty in the U.S. Armed Forces (with an additional 150,000 serving in the Reserves), representing approximately 15 percent of the total active-duty personnel. The lifting of the combat exclusion rule in 1993 has resulted in the opening of large numbers of military positions that were previously closed to women and has increased the opportunities for women to advance in their careers. Thus, in spite of the current effort to decrease the size of the active-duty force, the percentage of women serving on active duty is increasing, as is the age and ethnic diversity of this population. As a result of the downsizing of the military, the opening of more positions to women, and the increasing frequency of sudden deployment, women in the military must be ''ready," that is, prepared to perform a variety of tasks under conditions that can be extremely adverse. Military readiness encompasses optimum health, fitness, and performance. All military personnel are required to adhere to standards of body composition, physical fitness, and appearance1 that are believed to promote readiness.
While the requirement that personnel adhere to such standards is mandated by the Department of Defense (DoDD 1308.1, 1981, 1995), each branch of service is permitted to set its own standards and to test compliance with these standards in a way that is compatible with the mission of that branch.
The use of body composition, physical fitness, and task performance standards to evaluate personnel, as well as the assessment methods used, are issues of utmost interest to the scientific community and constitute active areas of investigation. At the same time, many questions have been raised by military personnel, researchers, and advisory groups such as the Defense Advisory Committee on Women in the Services (DACOWITS) regarding the particular standards and assessment methods used by the Armed Forces, the differences among the branches of service, and the implications for personnel readiness. The purpose of this report, prepared under a grant from the Defense Women's Health Research Program, is to examine whether current standards for body composition, physical fitness, and appearance, and the methods used to assess compliance with those standards, support military readiness by ensuring optimal health and job performance of active-duty servicewomen.
The Committee's Task
In 1992, the Committee on Military Nutrition Research (CMNR) of the Institute of Medicine (IOM) was asked by the U.S. Army to evaluate the body composition and fitness standards for personnel accession (recruitment) into and retention in all branches of active service, with regard to the impact of these standards on recruitment, physical fitness, and task performance in the Armed Forces. After conducting a workshop to investigate these issues, the CMNR released a report concluding that the standards of body composition that appeared to be required for women to achieve the desired appearance goal (low fat-free mass [FFM] and percent body fat) seemed to conflict with those necessary for performance of many types of military tasks (higher FFM often accompanied by increased body fat) (IOM, 1992). The committee recommended that body composition standards be based primarily on considerations of task performance and health and that they be validated with regard to the ethnic diversity of the military population. In addition, the committee recommended the development of task-specific performance tests; development of objective appearance standards, if these could be deemed necessary; and continuation of research on the relationships among body composition, health, and physical
|
|
smart," one of the two goals of weight control. The regulation goes on to qualify the standard by emphasizing that enlarged waistlines, "potbellies," detract from good military appearance. No objective criteria (rating scales) have been associated with the appearance standard as it is enforced. (This is discussed further in Chapters 2 and 3). Only a small number of studies have examined how the appearance standard as enforced is linked to body composition. Although appearance is slightly associated with body fat, it is associated more significantly with abdominal circumference (AR 600-9, 1986; Hodgdon et al., 1990; Vogel and Friedl, 1992). Although Army, Navy, and Marine Corps personnel must supply recent photos of themselves to their selection (promotion) boards (this practice has been eliminated by the Air Force and de-emphasized by the Navy), appearance judgments can be rendered at any time. When these involve a suspicion of overweight (as opposed to untidy uniforms or other details of appearance), the individual must be weighed and may be required to have a body fat determination, and if necessary, to enter the weight management program (with attendant career consequences). |
performance of military personnel. Also recommended was evaluation of the long-term outcome of individuals referred to military weight management programs for failure to adhere to standards.
At the autumn 1994 conference of DACOWITS, one of the concerns identified by the group was the need to address the body composition and physical fitness standards of the military and the impact of these standards on the health of women, particularly with regard to the potential influence of the standards on food intake and nutritional status. A report released by the IOM in 1995 to provide recommendations for research on the health of military women identified a number of gaps in research pertaining to the health and performance of military women. These included research on optimal physical fitness for military women, injury prevention, and ways to achieve and assess physical fitness, as well as fitness standards, including those for fitness during pregnancy and the postpartum period.
In 1995, in light of efforts to consider creation of DoD-wide fitness and body composition standards, calls to ensure that all personnel are physically able to perform their assigned tasks, and evidence suggesting that attempts to adhere to body composition and appearance standards may place active-duty women at special risk for inadequate nutrient intake, the CMNR was asked to appoint a subcommittee to examine issues of body composition, fitness, and appearance standards and their impact on the health, nutritional status, and performance of active-duty military women. Specifically, they were asked by the Army to address the following questions:
- What body composition standards best serve military women's health and fitness, with respect to minimum lean body mass, maximum body fat, and site specificity of fat deposition? Are the appearance goals of the military in conflict with military readiness?
- Should any part of the Military Recommended Dietary Allowances (MRDAs) be further adjusted for women? Should there be any intervention for active-duty women with respect to food provided, dietary supplementation, or education?
- What special guidance should be offered with respect to return-to-duty standards and nutrition for women who are pregnant or breastfeeding?
In April 1996, the CMNR convened a subcommittee comprising experts in the areas of body composition, exercise physiology, obesity, women's nutrition, epidemiology and survey design, cognitive psychology, and pregnancy and lactation. Several members of the parent committee were included to provide continuity. The subcommittee was designated the Committee on Body Composition, Nutrition, and Health of Military Women (BCNH committee).
Methods
In considering the questions posed by the military, the subcommittee consulted with a liaison panel composed of military researchers and health care personnel. A workshop was convened in September 1996 to bring together additional military personnel in the areas of physical fitness assessment, training, medicine, and nutrition, as well as civilian researchers and practitioners in the areas of physical fitness and performance, pregnancy, eating disorder assessment, and
nutrition. The proceedings of this workshop, summarized in Appendix A, helped to focus the questions and identify sources of information. A search of civilian and military literature citation indices was conducted for the years 1991 to 1996, inclusive, to capture all military and civilian research that was relevant to the main issues and not captured by earlier IOM reports. Additional information was provided by those reports (IOM 1992, 1995), by searches of the General Accounting Office database and the World Wide Web, by the military liaison panel members, by individuals contacted at a number of military and civilian agencies, as well as by contacting representatives of municipal law enforcement and firefighting services nationwide. The BCNH committee drew upon these materials and its collective expertise to respond to the Army's questions and prepare their recommendations.
Background
At the present time, the evaluation of body composition by each branch of the military is performed periodically by a two-step procedure (see Table S-1). The first step consists of a weight determination and comparison with a service-specific table of maximum allowable weights for height (along with an appearance determination). Personnel who exceed the weight-for-height limits for their gender (in the case of the Army and Air Force, also for age group) or who are judged to present a nonmilitary appearance are subjected to further assessment. This second step consists of body fat estimation using service-specific, circumference-based equations (Table S-2) standardized by underwater weighing. Each branch of service utilizes a different set of weight-for-height standards, body fat standards, and anthropometric equations. As a result, personnel who exceed the body fat standards for one branch of service may be in compliance with the standards of another branch. Personnel who fail to comply with the body fat standards of their own branch are referred to a weight management program (at the discretion of the commander). While administration of military weight management programs is left to each service individually, these programs generally require a single visit to a health professional, followed by regular weigh-ins until the weight and body fat goals are reached. Individuals are required to demonstrate continuing progress toward these goals by losing a prescribed number of pounds per month. Failure to show continued progress in weight loss, or continued failure to comply with body fat standards without a medical waiver, can result in separation from service.
Fitness is assessed by the military at the same time that body composition is determined. Each branch of service uses different test procedures (Table S-1). While aerobic fitness (endurance) is assessed by each service, the Army, Navy, and Marine Corps fitness tests incorporate additional tests of basic strength and flexibility (such as timed push-ups and sit-ups). Fitness test performance is rated on a gender-and age-specific scale. Unacceptable performance on the fitness test results in referral to a remedial program. Regular fitness training is mandated by the DoD, although duty time is not allowed for such training except in the Army and Marine Corps.
Testing of strength and task performance (as one of the qualifications for placement in military operational specialties [MOSs]), such as that currently used by most municipal firefighting services and many law enforcement agencies, is limited to the Air Force at the present time and to a very small number of MOSs in other branches of service.
TABLE S-1 U.S. Military Practices and Policies Pertaining to Body Composition, Fitness, and Pregnancy
|
Practice or Policy |
DoD Directive/ Instruction |
Army |
Navy |
Air Force |
Marine Corps |
Coast Guard |
|||
|
Frequency of Weight/Height, BF, and Fitness Assessment |
Formally evaluated and tested at least annually |
Semiannual |
Semiannual PRT optional for members > 50 years (NAVOP 064/90, 1990) |
Annual |
Semiannual |
At least annual and upon random urinalysis testing |
|||
|
Assessment Procedures* |
Circumference measure technique |
Circumference measure if maximum allowable weight for height exceeded |
Circumference measure if maximum allowable weight for height exceeded |
Circumference measure if maximum allowable weight for height exceeded |
Circumference measure if maximum allowable weight for height exceeded |
Frame size determined by wrist measure (see COMDTINST M1020.8C, 1994) |
|||
|
|
|
|
|
|
|
|
|
Circumference measure if maximum allowable weight for height exceeded |
|
|
Men's BF Standard |
Range: 18–26% |
Age |
Max %BF |
22% |
Age |
%BF |
18% |
Maximum allowable weight by frame size or if exceeded |
|
|
|
|
17–20 |
20 |
|
> 29 |
20 |
|
Age |
%BF |
|
|
|
21–27 |
22 |
|
30+ |
24 |
|
< 30 |
23 |
|
|
|
28–39 |
24 |
|
|
|
|
31–39 |
25 |
|
|
|
40+ |
26 |
|
|
|
|
40+ |
27 |
|
|
|
(AR 600-9, 1986) |
|
|
|
|
|
|
|
|
Women's BF Standard |
Range: 26–36% |
Age |
Max %BF |
30% (NAVADMIN 071/93, 1993) |
Age |
%BF |
26% |
Maximum allowable weight by frame size or if exceeded |
|
|
|
|
17–20 |
30 |
|
> 29 |
28 |
|
Age |
%BF |
|
|
|
21–27 |
32 |
|
30+ |
32 |
|
< 30 |
33 |
|
|
|
28–39 |
34 |
|
|
|
|
31–39 |
35 |
|
|
|
40+ |
36 |
|
|
|
|
40+ |
37 |
|
|
|
(AR 600-9, 1986) |
|
|
|
|
|
|
|
|
Fitness Test |
Annual |
Adjusted for age and gender (AR 350-41, 1993) |
Sit-reach; |
Submaximal cycle ergometer test, percent of standard |
Men: 3-mi run |
None |
|||
|
|
Adjusted for age and gender |
|
|
Curl-ups × 2 min |
|
|
Curl-ups |
|
|
|
|
|
|
|
Push-ups × 2 min |
|
|
Push-ups |
|
|
|
Practice or Policy |
DoD Directive/Instruction |
Army |
Navy |
Air Force |
Marine Corps |
Coast Guard |
|
Fitness Test |
Cardiovascular and muscular endurance |
2-mi run; Sit-ups × 2 min†; Push-ups × 2 min |
1.5-mi run/walk or 500-yd swim (age and gender adjusted) |
based on VO2max, age and gender specific (AFI 40-501, 1996) |
Pull-ups × 2 min |
|
|
|
(DoDI 1308.3, 1995) |
|
+ BF standards (OPNAVINST 6110.1D, 1990) |
|
Women: 1.5-mi run; Curl-ups; Push-ups; Bent-arm hang × 2 min |
|
|
Duty Time for Physical Fitness |
May authorize 1 1/2 hrs 3×/wk |
Authorize duty time |
Commanding officer's discretion |
Commanding officer's discretion |
Part of weekly training day |
Commanding officer's discretion |
|
Pregnancy |
|
• Exempt from body composition, fitness testing (AR 40-501, 1995) |
• Exempt from body composition, fitness testing |
• Exempt from body composition, fitness testing |
• Full-duty status and deployable until medical officer certifies that full duty is medically inadvisable |
• Exempt from body composition testing |
|
|
|
• Nondeployable |
• 20-wk Rule (no shipboard duty after 20th week of gestation) |
• Restrictions based on work environment |
• May not participate in contingency operations or be deployed for operations aboard Navy vessels |
• >28 weeks, 40-h work week; no overseas duty |
|
|
|
• At 20 weeks, standing at parade rest/attention < 15 minutes |
• 6-h Rule (medical evacuation for ER must be within 6 hours) (OPNAVINST 6000.1A, 1989) |
• Pregnant members assigned to areas without obstetrical care will have assignment curtailed by 24th week (AFI 44-102, 1996) |
• Flight personnel are grounded unless cleared by medical waiver |
• Other duty restrictions based on work environment; no rescue swimmer duties |
|
|
|
• At 28 weeks, 40-h week/8-h day |
• 40-h work week |
|
• Excused from duties (physical training or standing in formation) that in the opinion of the medical officer are hazardous to her health or to her unborn child |
• Not deployable during 20th week through 6 months postpartum |
|
|
|
|
• Standing at parade rest/attention no more than 20 min |
|
|
• Time to medical evacuation for emergencies < 3 hours |
|
|
|
|
|
|
|
• No flight duties after 2nd trimester |
|
|
|
|
|
|
|
• Prenatal sick leave not to exceed 30 days |
|
|
|
|
|
|
• Remains available for worldwide assignment |
|
|
|
|
|
|
|
• Pregnant Marines stationed in Hawaii will not be detached after their 6th month; if overseas, they may be detached at their normal rotation tour date; if assigned to shipboard duty, the Marine will be reassigned at first opportunity and no later than the 20th week of pregnancy |
|
|
Postpartum |
|
• Return to duty at 6 weeks |
• Return to duty at 6 weeks |
• Return to duty at 6 weeks |
• Return to duty at 6 weeks (or as soon after delivery as medical officer certifies) |
For nursing mothers, the 6-mo weight standards exemption following delivery will begin at the conclusion of the nursing period, but no later than 12 months postdelivery |
|
|
|
• Exempt from weigh-in until 6 months |
• Exempt from weigh-in until 6 months |
• Exempt from weigh-in until 6 months |
• Exempt from weigh-in until 6 months |
• Postdelivery maternity leave up to 6 weeks |
|
|
|
• Physical training at own pace for 45 days |
• Exempt from fitness testing for 6 months |
• Deferment from deployment until 4 months postpartum |
• Exempt from fitness testing for 6 months |
• Not deployable until 6 months postpartum |
|
|
|
• Exempt from fitness testing for 135 days (FM 21–20, 1992) |
• Deferment from deployment until 4 months postpartum |
• Exempt from fitness testing for 6 months (AFI 40-502, 1994) |
• Deferment from deployment until 4 months postpartum |
|
|
|
|
• Deferment from deployment until 4 months postpartum |
• No policy regarding breastfeeding |
• Commander may approve up to 18 months deferral |
• (MCO 5000.12D, 1995) |
|
|
Practice or Policy |
DoD Directive/Instruction |
Army |
Navy |
Air Force |
Marine Corps |
Coast Guard |
|
Postpartum |
|
• No policy regarding breastfeeding |
|
• No policy regarding breastfeeding |
• No policy regarding breastfeeding |
• Exempt from weight standards for up to 6 months |
|
NOTE: DoD, Department of Defense; BF, body fat; PRT, physical readiness test; NAVOP, Naval Operational Message; COMDTINST, Commandant Instruction; AR, Army Regulation; NAVADMIN, Naval Administrative Message; DoDI, Department of Defense Instruction; OPNAVINST, Naval Operations Instruction; VO2max, maximal oxygen consumption; AFI, Air Force Instruction; FM, Field Manual; MCO, Marine Corps Order. * See Table S-2 for equations. † Number of sit-ups performed in 2 minutes. |
||||||
TABLE S-2 U.S. Military Body Composition Equations
|
Army (Vogel et al., 1988) |
|
Men |
|
Percent fat = 76.5 × Log10(abdomen II* - neck) - 68.7 × Log10(height) + 46.9 R = 0.82, SEE = 4.02 |
|
Women |
|
Percent fat = 105.3 × Log10(weight) - 0.200 × wrist - 0.533 × neck - 1.574 × forearm + 0.173 × hip - 0.515 × height - 35.6 R = 0.82, See = 3.60 |
|
Navy (Hodgdon and Beckett, 1984a, b) and Air Force |
|
Men |
|
Density = -0.191 × Log10(abdomen II - neck) + 0.155 × Log10(height) + 1.032 Percent fat = 100 × [(4.95/density) - 4.5] R = 0.90, SEE = 3.52 |
|
Women |
|
Density = -0.350 × Log10(abdomen I† + hip + neck) + 0.221 × Log10 (height) + 1.296 Percent fat = 100 × [(4.95/density) - 4.5] R = 0.85, SEE = 3.72 |
|
Marine Corps (Wright et al., 1980, 1981) |
|
Men |
|
Percent fat = 0.740 × abdomen II - 1.249 × neck + 40.985 R = 0.81, SEE = 3.67 |
|
Women |
|
Percent fat = 1.051 × biceps - 1.522 × forearm - 0.879 × neck + 0.326 × abdomen II + 0.597 × thigh + 0.707 R = 0.73, SEE = 4.11 |
|
NOTE: Circumference measurements and height are in centimeters. SEE, standard error of the estimate. * Abdomen II is the circumference, measured in transverse plane, at the level of the umbilicus. † Abdomen I is the "natural waist" and is defined as the smallest circumference, measured in the transverse plane, obtained between the lower margin of the xiphoid process and the umbilicus. SOURCE: Adapted from Hodgdon (1992). |
Throughout the military, women who become pregnant while on active duty are exempt from compliance with body composition standards until 6 months postpartum. Compliance with fitness standards must be achieved by 135 days (Army) to 180 days (Navy and Air Force), although medical waivers are permitted. Active-duty women are permitted 6 weeks maternity (convalescent) leave and are deployable at 4 months unless a medical waiver is granted.
Findings
Although the current weight-for-height tables used by each branch of the military are derived from actuarial tables of mortality and morbidity risk, other estimates of body composition, such as the body mass index (BMI, weight in kilograms divided by the square of height in meters), have been shown to predict health risk with greater validity and equal ease; the BMI shows good correlation with total body fat in women of military age. The preponderance of evidence suggests that a BMI range of 19 to 25 is associated with minimal risk of morbidity and mortality. Table S-3 shows the BMIs corresponding to current Army weight-for-height limits, and Table S-4 shows the weight ranges that would correspond to a BMI range of 19 to 25 for representative heights.
The equations used by the military to predict body fat have been validated only against the method of underwater weighing and on a population of individuals who no longer reflect the age, ethnic, or gender profile of the current population of military personnel. (Approximately 40% of active-duty military women are members of a minority group, although the percentages differ by branch of service. The majority of active-duty women are under the age of 262; the percentage above age 40 is very small.) Because of the test population used, technical problems with the reference method, and proposed variations in body fat distribution among ethnic groups, it has been hypothesized that the equations may not be valid and may underpredict or overpredict body fat for some groups, particularly when applied to women. However, thus far, systematic ethnic variations in body fat distribution remain controversial, there has been no evidence that the military equations have systematically overpredicted body fat in any ethnic group, and there are no data on how body fat assessments provided by these equations compare with estimations provided by four-compartment methods of body fat determination for women in various ethnic groups. The equations tend to underpredict body fat at levels close to the upper limits and above.
Data obtained from the Army Health Risk Appraisal database for 1995 on approximately 17,000 female soldiers revealed a mean BMI of 22.7 ± 3.29 (SD), with 13.9 ± 0.1 percent at a BMI of 27.3 or greater (the Healthy People 2000 [DHHS, 1991] definition of obesity). It was not possible to obtain a breakdown of the percentage of women at each BMI, nor were comparable data available from the other branches of service. Estimates of overweight personnel were obtained from a self-report survey (Survey of Health-Related Behaviors among Military Personnel, Bray et al., 1995). According to this survey, approximately 10 percent of active-duty women
TABLE S-3 Current Maximum U.S. Army Weight-for-Height Limits for Women (Screening Table Weight) with Corresponding Body Mass Index (BMI)* by Age Group
TABLE S-4 Expected Weight Ranges by Height for Women with Body Mass Index* Range of 19 to 25
under age 20 and over age 25 were overweight by the standards of Healthy People 2000 (DHHS, 1991), while 6 percent of women aged 20 to 25 were overweight. However, these figures underestimate the percentages of women who are out of compliance with military weight standards. According to the same survey (Personal communication, R. M. Bray, Research Triangle Park, N.C., 1996), the prevalence of underweight (defined by the survey as a BMI < 19.8) is 14.5 percent for women under age 20, 11 percent for women ages 20 to 25, 10 percent for women ages 26 to 34, and 5 percent for women age 35 and older. The prevalence of BMI less than 19 ranges from 3.6 percent for all Navy women to 6.8 percent for Marine Corps women. Data on numbers of individuals separated from service for failure to comply with the weight standards were obtained (from Defense Manpower Data Center, Rosslyn, Va.) but do not provide an accurate picture of the percentage of personnel out of compliance because administrative separation is an action that is at the discretion of the commander.
Studies have shown that a significant percentage of female Army personnel, particularly those in the youngest age groups, fail the Army physical fitness test (for example, the failure rate of women in the 18–21 age group is 36%). Comparable data were not available for the other
branches of the military. Self report data show that approximately 60 percent of active-duty women exercise regularly. Anecdotal evidence shows that compliance with provision of duty time for fitness training is command dependent.
The performance of personnel on military fitness tests does not correlate well with their performance on task-specific performance tests or tests of the strength required for MOSs that demand heavy and moderately heavy lifting and carrying capabilities. Military researchers have recommended the adoption of task-specific performance tests, such as those used in the civilian sector; general and task-specific strength training; and where possible, task redesign.
Performance by military women on strength tests is correlated with higher body weight and associated FFM.3 Because of higher FFM, women who exceed the weight-for-height standard during basic combat training may perform better on tests of strength than their thinner counterparts; however, women who exceed weight-for-height standards achieve slower run times (a measure of endurance capacity) than women who are in compliance with the weight standards. The maintenance of an appearance standard that promotes lower weight for height thus presents a dilemma for promotion of optimum physical readiness, especially for the more physically demanding (strength-requiring) MOSs.
It was not possible to obtain outcome data on any of the military weight management programs or information on how a representative sample of military sites administers their programs. Comparison of the programs as described in the regulations with current recommendations for civilian weight loss and management programs suggests that greater contact with nutrition professionals and nutrition education, increased emphasis on incorporating fitness and other lifestyle changes, and establishment of long-term maintenance programs may be necessary to ensure success of the programs.
Assessments of the nutritional status and food intake of active-duty women have been limited to small studies of women in temporary training and field settings. Results of these studies suggest that because the nutrient density of operational (field) rations and military dining hall menus is based on an average daily energy intake of 3,600 kcal, reliance on operational rations or dining hall offerings may make it difficult for women to obtain the recommended levels of calcium, iron, and folic acid while balancing energy intake with expenditure; moreover, the MRDAs have not been modified since 1985 and are based on the 1980 Recommended Dietary Allowances (RDAs). A large-scale nutritional survey of active-duty women in garrison and deployed throughout the world has recently been completed, and a study of energy expenditure in active-duty women is in progress.
Evidence also suggests that chronic dieting or frequent crash dieting to comply with weight standards may compromise women's nutritional status and fitness level. It is difficult at this time to ascertain the prevalence of disordered eating (as characterized by behaviors ranging from repeated crash dieting and/or chronic restrained eating to chronic starvation and/or cycles of bingeing and purging) among active-duty women. Survey data suggest that the percentage of active-duty women who perceive themselves to be overweight is high and exceeds the percent who actually are overweight. Evidence suggests that self-perception of overweight is linked to chronic dieting. Several small surveys have attempted to assess the percentage of active-duty personnel
who are engaging in disordered eating behaviors or other unhealthy weight management behaviors (such as use of diet pills and laxatives, purging, and excessive physical activity), and have reported incidences both similar to and significantly higher than those among comparable civilian populations. However these results must be called into question because of small sample sizes and low response rates, possibly reflective of the fact that until recently, diagnosis of an eating disorder has been considered grounds for discharge from the military, and the perception that this policy is still enforced has not disappeared.
Whether the incidence of disordered eating among active-duty women is comparable to or greater than among civilian women may be less important an issue, however, than the impact that chronic dieting and other disordered eating behaviors have been shown to have on operational performance. Research has demonstrated that chronic dieting by energy restriction results in significant decrements in performance on several tests of cognitive function; other studies have suggested that dieting increases the risk for amenorrhea and stress fracture injuries.
While a minority of active-duty women under the age of 26 are married (35% of enlisted and 30% of commissioned officers), the majority over the age of 26 are married (61% of enlisted and 60% of commissioned officers). The percentage of women who are parents varies considerably by service and status, ranging from 16 percent of Marine Corps officers to 42 percent of Army enlisted personnel. Very few data are available on pregnancy weight gain, nutrition, and exercise; postpartum weight loss; pregnancy outcome; and lactation among active-duty military women. Available data from civilian women suggest that it would be difficult for a woman whose gestational weight gain was within the range recommended by the IOM (1990) to return to her postpartum weight within the 6 months currently allowed. The body composition equations currently in use have not been validated on a postpartum population of women. No data were available regarding postpartum return to fitness for a military population.
Recommendations
The major recommendations are presented below in response to the questions posed by the Army.
What body composition standards best serve military women's health and fitness, with respect to minimum lean body mass, maximum body fat, and site specificity of fat deposition? Are the appearance goals of the military in conflict with military readiness?
- The BCNH committee recommends the revision of the two-tiered body composition and fitness screen.
As illustrated in Figure S-1, the first tier should consist of semiannual assessment of BMI and fitness (including strength and endurance). The acceptable range of BMIs, based on considerations
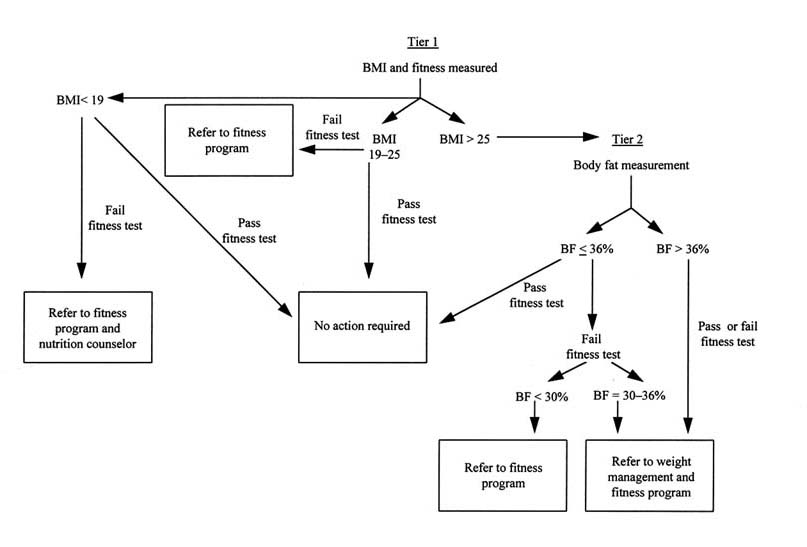
- of health, is recommended to be 19 to 25,4 independent of age. Individuals whose BMI falls within the desirable range and who pass the fitness test need no further screening. Individuals with a BMI greater than 25 should be subjected to a second tier of screening, based on body fat assessment. The committee believes that women with BMIs less than 19 can be fit to perform. However, as BMI decreases below 19, women may be at risk for malnutrition and should be considered for medical evaluation.
Individuals whose body fat is assessed at 36 percent or less and who pass the fitness test will be considered within standard. Individuals whose body fat exceeds 30 percent and who fail the fitness test will be referred to weight management and fitness programs. Individuals whose body fat exceeds 36 percent will be referred to a weight management program, regardless of fitness score.
- The BCNH committee also recommends development of a single service-wide equation derived from circumference measurements for assessment of women's body fat, to be validated against a four-compartment model using a population of active-duty women or a population that is identical in ethnic and age diversity to that of military women. Development and validation of this equation may result in reconsideration of the recommended BMI cut-offs, in part as a result of establishing the measurement error.
- The BCNH committee recommends an increasing emphasis on general fitness for health and readiness by enforcing uniformly across all services and MOSs regular and monitored participation in a fitness program consisting of a minimum of 3 d/wk of endurance exercise at 60 to 80 percent of maximum capacity for 20 to 60 minutes and 2 d/wk of resistance exercise using all major muscle groups at 85 percent of one repetition maximum (ACSM, 1990). Such a program, in addition to promoting fitness, assists in maintenance of weight and FFM and may result in lower body fat. Periodic fitness and body composition testing adjusted appropriately for gender should be conducted to determine both endurance and strength and should be similar across all services. More frequent testing would promote continuous adherence to weight and physical fitness programs and decrease injurious behaviors that result from efforts to pass performance and body composition tests.
- The committee further recommends development of task-specific, gender-neutral strength and endurance tests and standards for use in the determination of placement in MOSs that require moderate and heavy lifting. Additional fitness programs should be created and enforced to develop and maintain the strength, endurance, and flexibility required by these MOSs.
- The BCNH committee recommends that, in view of the association between FFM (as an indirect indicator of skeletal muscle mass) and strength, the military consider developing an appropriate minimum recommended BMI for accession of women.
- The current appearance standard does not appear to be linked to performance, fitness, nutrition, or health. The BCNH committee recommends that if the military deems appearance standards to be necessary, objective criteria (that do not discriminate on the basis of ethnicity) should be developed and utilized.
Should any part of the MRDAs be further adjusted for women? Should there be any intervention for active-duty women with respect to food provided, dietary supplementation, or education?
- In view of current ongoing efforts by the Food and Nutrition Board to revise the RDAs upon which the MRDAs (AR 40-25, 1985) are based, the BCNH committee advises that revision of the MRDAs be deferred to a later time and has chosen to concentrate on several nutritional issues of importance to active-duty women.
- The BCNH committee reinforces the requirement for adequate energy and nutrient intakes to reflect the needs of the body at a moderate activity level (2,000–2,800 kcal/d). To ensure adequate nutrient intakes, female personnel must be educated on how to meet both energy and nutrient needs whether they are deployed and subsisting on operational rations or whether they are in garrison. This education is required to enable women to choose foods of higher nutrient density and to maintain a fitness program that will allow greater energy intake. The committee reinforces the recent efforts of the Army to begin providing complete nutritional labeling of all ration components and to include information to enable identification of nutrient-dense components that would help women meet the MRDAs at their usual energy intake. The committee also supports efforts to create ration supplements that would satisfy requirements that may not be readily met through the usual intake of rations. The committee recommends nutritional labeling of all dining hall menu items and provision of food selection guidelines to women in garrison.
- The BCNH committee recommends that all military women maintain or achieve healthy weight through a continuous exercise and fitness program. If weight loss is a goal, nutrition education and ongoing counseling should be provided for guidance in achieving a healthy, but reduced energy, diet. Emphasis must be placed on preventing overweight and maintaining long-term weight management through lifestyle changes, rather than on crash dieting to lose weight for a scheduled weigh-in. Adequate energy intake should be encouraged to reduce risks of injury and amenorrhea.
What special guidance should be offered with respect to return-to-duty standards and nutrition for women who are pregnant or breastfeeding?
- The BCNH committee recommends that all women be encouraged to eat an adequate diet during pregnancy and lactation as recommended by the IOM (1990, 1991). The committee further recommends an intake of 400 µ/d dietary folate during childbearing years, 600 µg/d dietary folate during pregnancy and 500 µg/d during lactation as recommended by the IOM (1998). A daily supplement of 30 mg of ferrous iron (IOM, 1990) is recommended during the second and third trimesters of pregnancy. During pregnancy and lactation, women should abstain from smoking. Although alcohol should be avoided during pregnancy, a very moderate intake may be permitted during lactation (IOM, 1990).
- The BCNH committee recommends that pregnant women without obstetrical or medical complications engage in moderate levels of physical activity to maintain cardiovascular and muscular fitness throughout the pregnancy and the postpartum period. The American College of Obstetricians and Gynecologists (ACOG, 1994) has published guidelines that should be used to
- advise pregnant active-duty women to modify their physical fitness program. Programs should be individualized and made available to healthy women who can and wish to exercise. These programs may also incorporate strength training, although the extent of the benefits of such training during pregnancy remains to be determined.
- The BCNH committee recommends the endorsement of the IOM guidelines for gestational weight gain as outlined in the text. Women should be encouraged to gain within the IOM recommendations during pregnancy and to lose weight postpartum through appropriate nutritional counseling and exercise programs. The BCNH committee recommends that the proposed time allowance for compliance to weight and body fat standards postpartum be consistent with IOM recommendations for gestational weight gain. When satisfactory progress is being made toward compliance, an allowance of up to 1 year postpartum should be given for attainment of body weight standards.
- Resumption of exercise postpartum will depend on the type of delivery and postpartum state of the woman and should be left to the discretion of the woman's obstetrician. Once clearance is given to resume exercise, a time allowance of 180 days should be sufficient for the woman to meet physical fitness standards.
- The Healthy People 2000 (DHHS, 1991) goal for breastfeeding specifies that at least 75 percent of women should breastfeed their babies in the early postnatal period and 50 percent of women should continue to breastfeed until their babies are 5 to 6 months old. As the military has provided no indication as to why they should not strive to comply with this goal, the committee recommends that efforts be made to promote and support breastfeeding among all servicewomen, where appropriate. Promotion of breastfeeding can be incorporated into prenatal classes, family support classes, hospital policies, and training of health care providers.
- The BCNH committee calls attention to the persistent anemia and musculoskeletal and cardiovascular changes that may continue in some women postpartum. These changes may present potential health problems for the mother and compromise her fitness status. Women with low iron stores before pregnancy or excessive blood losses at delivery may require an extended period (5–10 months) to replete and normalize stores.
- An increase in the length of exemption from deployment from 4 to 6 months postpartum is recommended to support maternal postpartum recovery, breastfeeding, and enhanced infant health and development.
- The BCNH committee acknowledges that childbearing is compatible with a military career when planning and education on effective birth control and counseling on the importance of timing pregnancy in one's military career are provided to all servicemembers. The committee therefore recommends training and education for all supervisory personnel regarding pregnancy policy, as well as a prenatal counseling program for pregnant active-duty women. These policies should be implemented to reduce attrition and enhance military readiness.
Recommendations For Future Research
Currently, there are no systematically collected data describing what military women do to meet weight and fitness standards (both before and after childbirth), how effective their behaviors
are at maintaining weight and fitness standards, and the long-term health consequences of these behaviors. A DoD-wide evaluation system is recommended.
Survey Design and Administration
Relevant Data from Previous Surveys of Military Personnel and in Existing DoD Databases
Several research projects have been conducted by the services on the health-related behaviors of servicemembers. In addition to the wide variety of demographic and personnel data maintained in the Defense Manpower Data Center database, health outcome data are maintained in several medical cost accounting databases.
Effective Use of Existing Data
A combination of the survey instruments that have been used in the past would be suitable for collecting most of the information needed (including longitudinal data). The personnel and medical databases are capable of producing much of the remaining information needed. However, the committee finds that there are two problems with this method of data collection. First, some of the survey data were collected anonymously (with no identification numbers of any type), precluding any attempt to examine the data longitudinally or merge the databases with existing personnel and medical databases that contain the demographic and health outcome data needed for a comprehensive analysis of the data. Second, the personnel and medical databases were not designed to be linked to each other or to survey databases. Thus, although much potentially worthwhile information is collected, little meaningful analysis can be performed.
Recommendations for New Methods
The committee recommends that the military survey a representative sample of active-duty personnel individually and review the individuals' personnel and medical records during the course of the interview. This method would enable the investigator to obtain all the data needed in a single effort, ensure quality control of the data, build a database that would preserve the anonymity of the individual, and obviate the need to merge automated information systems with highly sensitive data. However, the need to create a system that will obtain information from several large and representative samples of the entire DoD over the course of several years may make this choice cost-prohibitive.
An alternative recommendation is to expand the triennial Survey of Health-Related Behaviors among Military Personnel to include the demographic, medical, nutrition, fitness, and pregnancy data needed. Changing the questionnaire to include social security number, as was done with the Navy's Perceptions of Wellness and Readiness Assessment survey and the Army's Health Risk Appraisal survey, would permit a longitudinal and potentially integrated database to be developed. The practice of using questions from federal surveys of health and fitness-related
behaviors in the general U.S. population should be continued so that comparisons between military and civilian populations can be made.
Additional Data Needed
As recommended by an earlier IOM report (1992), longitudinal studies of people admitted to military weight management or remedial fitness programs should be conducted to determine the outcome of these programs as recommended changes in program procedures are implemented.
Career, active-duty, military women constitute a unique population of individuals who are required to maintain their weight and body fat and fitness at prescribed levels. Longitudinal studies of health risk factors (cardiovascular, musculoskeletal, metabolic) and outcomes are recommended for these women.
The DoD is encouraged to monitor pregnancy outcome (birth weight, preterm delivery, low birth weight and small-for-date infants, and congenital anomalies) as well as pregnancy wastage (miscarriage) according to service, rank, and MOS to identify potential problems associated with certain military jobs, physical training, or hazardous environments. Longitudinal studies are recommended on body weight and fitness of women who have given birth. It is recommended that health surveys be expanded to collect information on the pregnancy history of active-duty women. Suggested questions are those used by Evans and Rosen (1996).
Additional Research Recommendations
- Additional research is needed to refine and standardize anthropometric equations for body fat prediction and to validate them against current four-compartment models. This research must include a population that is representative of active-duty military women in ethnic and age profile.
- In view of the relationship between skeletal muscle/FFM and strength, and recent developments in the ability to assess these parameters, research is recommended to develop an expedient method for the prediction of FFM using anthropometric measurements.
- The use of standard military equations in postpartum women for estimating body fat at return-to-duty testing has not been validated. Therefore, the BCNH committee recommends that validation studies be conducted in these women, controlling for ethnicity, age, and parity.
- Task assessment and redesign are recommended, where appropriate, to ensure genderneutral accession and retention standards in individual MOSs.
- Further research is recommended on the incidence and risk factors for stress fracture and other musculoskeletal injuries in active-duty women.
- Additional research is needed on the effects of environmental stressors on the nutritional status and needs of active-duty women. It is recommended that the military coordinate its research efforts in this area with those of the civilian sector.
References
ACOG (American College of Obstetricians and Gynecologists). 1994. Exercise during pregnancy and the postpartum period. ACOG Technical Bulletin 189. February. Washington, D.C.: ACOG.
ACSM (American College of Sports Medicine). 1990. ACSM position stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness in healthy adults. Med. Sci. Sports Exerc. 22:265–274.
AFI (Air Force Instruction) 40-502. 1994. See U.S. Department of the Air Force, 1994.
AFI (Air Force Instruction) 40-501. 1996. See U.S. Department of the Air Force, 1996.
AFI (Air Force Instruction) 44-102. 1996. See U.S. Department of the Air Force, 1996.
AR (Army Regulation) 40-25. 1985. See U.S. Departments of the Army, the Navy, and the Air Force, 1985.
AR (Army Regulation) 600-9. 1986. See U.S. Department of the Army, 1986.
AR (Army Regulation) 350-41. 1993. See U.S. Department of the Army, 1993.
AR (Army Regulation) 40-501. 1995. See U.S. Department of the Army, 1995.
Bray, R.M., L.A. Kroutil, S.C. Wheeless, M.E. Marsden, S.L. Bailey, J.A. Fairbank, and T.C. Harford. 1995. Health behavior and health promotion. Department of Defense Survey of Health-Related Behaviors among Military Personnel. Report No. RTI/6019/06-FR. Research Triangle Park, N.C.: Research Triangle Institute.
COMDTINST (Commandant Instruction) M1020.8C. 1994. See U.S. Department of the Navy, U.S. Coast Guard Headquarters, 1994.
DHHS (U.S. Department of Health and Human Services). 1991. Healthy People 2000: National Health Promotion and Disease Prevention Objectives. DHHS (PHS) Publ. No. 91-50212. Public Health Service, U.S. Department of Health and Human Services. Washington, D.C.: U.S. Government Printing Office.
DoDD (Department of Defense Directive) 1308.1. 1981. See U.S. Department of Defense, 1981.
DoDD (Department of Defense Directive) 1308.1. 1995. See U.S. Department of Defense, 1995.
DoDI (Department of Defense Instruction) 1308.3. 1995. See U.S. Department of Defense, 1995.
Evans, M.A., and L. Rosen. 1996. Women in the military: Pregnancy, command climate, organizational behavior, and outcomes. Technical Report No. HR 96-001, Part I, Defense Women's Health Research Program. Fort Sam Houston, Tx.: U.S. Army Medical Department Center and School.
FM (Field Manual) 21-20. 1992. See U.S. Department of the Army, 1992.
Hodgdon, J.A. 1992. Body composition in the military services: Standards and methods. Pp. 57–70 in Body Composition and Physical Performance, Applications for the Military Services, B.M. Marriott and J. Grumstrup-Scott, eds. Committee on Military Nutrition Research, Food and Nutrition Board, Institute of Medicine. Washington, D.C.: National Academy Press.
Hodgdon, J.A., and M.B. Beckett. 1984a. Prediction of percent body fat for U.S. Navy men from body circumferences and height. Report no. 84-11. San Diego, Calif.: Naval Health Research Center.
Hodgdon, J.A., and M.B. Beckett. 1984b. Prediction of percent body fat for U.S. Navy women from body circumferences and height. Report no. 84-29. San Diego, Calif.: Naval Health Research Center.
Hodgdon, J.A., P.I. Fitzgerald, and J.A. Vogel. 1990. Relationships between body fat and appearance ratings of U.S. soldiers. Report No. 90-01. San Diego, Calif.: Naval Health Research Center.
IOM (Institute of Medicine). 1990. Nutrition during Pregnancy: Part I, Weight Gain; Part II, Nutrient Supplements. Subcommittee on Nutritional Status and Weight Gain during Pregnancy, Subcommittee on Dietary Intake and Nutrient Supplements during Pregnancy, Committee on Nutritional Status during Pregnancy and Lactation, Food and Nutrition Board. Washington, D.C.: National Academy Press.
IOM (Institute of Medicine). 1991. Nutrition during Lactation. Subcommittee on Lactation, Committee on Nutritional Status during Pregnancy and Lactation, Food and Nutrition Board. Washington, D.C.: National Academy Press.
IOM (Institute of Medicine) 1992. Body Composition and Physical Performance, Applications for the Military Services , B.M. Marriott and J. Grumstrup-Scott, eds. Committee on Military Nutrition Research, Food and Nutrition Board. Washington, D.C.: National Academy Press.
IOM (Institute of Medicine). 1995. Recommendations for Research on the Health of Military Women. Committee on Defense Women's Health Research, Food and Nutrition Board. Washington, D.C.: National Academy Press.
IOM (Institute of Medicine). 1998. Dietary Reference Intakes: Folate, Other B Vitamins, and Choline. Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Food and Nutrition Board. Washington, D.C.: National Academy Press.
MCO (Marine Corps Order) 5000.12D. 1995. See U.S. Department of the Navy, U.S. Marine Corps Headquarters, 1995.
NAVADMIN (Naval Administrative Message) 071/93. 1993. See U.S. Department of the Navy, 1993.
NAVOP (Naval Operational Message) 064/90. 1990. See U.S. Department of the Navy, 1990.
OPNAVINST (Naval Operations Instruction) 6000.1A. 1989. See U.S. Department of the Navy, Office of the Chief of Naval Operations, 1989.
OPNAVINST (Naval Operations Instruction) 6110.1D. 1990. See U.S. Department of the Navy, Office of the Chief of Naval Operations, 1990.
U.S. Department of Defense. 1981. Department of Defense Directive 1308.1. ''Physical Fitness and Weight Control Programs." June 29. Washington, D.C.
U.S. Department of Defense. 1995. Department of Defense Directive 1308.1. "Physical Fitness and Body Fat Programs." July 20. Washington, D.C.
U.S. Department of Defense. 1995. Department of Defense Instruction 1308.3. "Physical Fitness and Body Fat Programs Procedures." August 30. Washington, D.C.
U.S. Department of the Air Force. 1994. Air Force Instruction 40-502. "The Weight Management Program." November 7. Washington, D.C.
U.S. Department of the Air Force. 1996. Air Force Instruction 40-501. "The Air Force Fitness Program." February 1. Washington, D.C.
U.S. Department of the Air Force. 1996. Air Force Instruction 44-102. "Patient Care and Management of Clinical Services." February 1. Washington, D.C.
U.S. Department of the Army. 1986. Army Regulation 600-9. "The Army Weight Control Program." September 1. Washington, D.C.
U.S. Department of the Army. 1992. Field Manual 21-20. "Physical Fitness Training." September 30. Washington, D.C.
U.S. Department of the Army. 1993. Army Regulation 350-41. "Training in Units." March 19. Washington, D.C.
U.S. Department of the Army. 1995. Army Regulation 40-501. "Standards of Medical Fitness." August 30. Washington, D.C.
U.S. Department of the Navy. 1990. Naval Operational Message 064/90. "Physical Readiness Program." June 22. Washington, D.C.
U.S. Department of the Navy. 1993. Naval Administrative Message 071/93. "Physical Readiness Program Changes." April 29. Washington, D.C.
U.S. Department of the Navy, Office of the Chief of Naval Operations. 1989. Naval Operations Instruction 6000.1A. "Management of Pregnant Women." February 21. Washington, D.C.
U.S. Department of the Navy, Office of the Chief of Naval Operations. 1990. Naval Operations Instruction 6110.1D. "Physical Readiness Program." January 18. Washington, D.C. .
U.S. Department of the Navy, U.S. Coast Guard Headquarters. 1994. Commandant Instruction M1020.8C. "Allowable Weight Standards for the Health and Well-Being of Coast Guard Military Personnel." Washington, D.C.
U.S. Department of the Navy, U.S. Marine Corps Headquarters. 1995. Marine Corps Order 5000.12D. "Marine Corps Policy on Pregnancy and Parenthood." October 4. Washington, D.C.
U.S. Departments of the Army, the Navy, and the Air Force. 1985. Army Regulation 40-25/Navy Command Medical Instruction 10110.1/Air Force Regulation 160-95. "Nutritional Allowances, Standards, and Education." May 15. Washington, D.C.
Vogel, J.A., and K.E. Friedl. 1992. Army data: Body composition and physical capacity. Pp. 89–103 in Body Composition and Physical Performance, Applications for the Military Services, B.M. Marriott and J. Grumstrup-Scott, eds. Committee on Military Nutrition Research, Food and Nutrition Board, Institute of Medicine. Washington, D.C.: National Academy Press.
Vogel, J.A., J.W. Kirkpatrick, P.I. Fitzgerald, J.A. Hodgdon, and E.A. Harman. 1988. Derivation of anthropometry based body fat equations for the Army's weight control program. Technical Report No. T17-88. Natick, Mass.: U.S. Army Research Institute of Environmental Medicine.
Wright, H.F, C.O. Dotson, and P.O. Davis. 1980. An investigation of assessment techniques for body composition of women Marines. U.S. Navy Med. 71:15–26.
Wright, H.F., C.O. Dotson, and P.O. Davis. 1981. Simple techniques for measurement of percent body fat in man. U.S. Navy Med. 72:23–27.
























