
PART IV
Making a Difference: Controlling the Epidemic Through Social Intervention
The transmission of HIV infection occurs most often during sexual and drug-related activities, that involve interactions among two or more individuals. Several types of social relationships interact with one another and with HIV-related behaviors. These range from couples to social networks, from the community to the larger society and the media. Basic social-science research in each of these areas has already contributed both to a better understanding of the AIDS epidemic and to better design of HIV interventions. However, additional basic research questions should be central in the development of new interventions to reduce those high-risk behaviors that remain —and are spreading HIV—even after all that has been done.
SOCIAL NETWORKS
Social networks are sets of social linkages or interactions among individuals. These linkages are usually defined in terms of particular social relationships, such as kinship ties, friendships, or commercial transactions. Figure 1 presents a schematic of social networks, that are smaller and simpler than those actually found among research subjects. If two or more subjects are “linked,” this means that they are members of each other's social networks. Social networks can be thought of as being either “egocentric” (the set of persons with whom an index person has relationships) or as “sociometric” (the set of linkages and persons in a given community or other social unit of
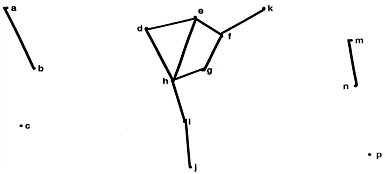
FIGURE 1. Social Network Structures.
Social networks can be between two individuals (dyadic), illustrated by connections between a and b, or m and n, in the diagram. More complex networks, the middle diagram, involve more individuals and relationships. Networks can overlap and new networks can form as well, which could be reflected if connections were made between any previously unconnected individuals (b and h, or g and p and j and p, for example).
interest). Figure 2 presents the concept of the “egocentric” or personal network, which is the set of persons who are directly linked to a given subject. In risk networks, two or more members are linked if they engage in a particular risk behavior together, such as unprotected sex or drug injection.
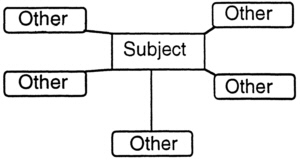
FIGURE 2. Egocentric Social Network.
Analysis of a social network centered around an individual can also be useful. Such analysis could be applied, for example, to analyzing the transmission of HIV from the soldier described in the story of Acéphie in Part II of this summary.
Research on social networks contributes to a better understanding of the course of the epidemic and can inform and improve HIV intervention research. Social network analysis is an important tool for understanding HIV transmission because transmission occurs between individuals who make up a network. Some persons may form bridges between what would otherwise be unconnected networks. Such persons play key roles in viral transmission within a large network (see Laumann et al., 1994, Chapters 6 and 7 on sexual networks and the relevance of networks to epidemiology). Other networks may be diffuse and loosely tied together. There is evidence that HIV may spread rapidly in a particular city when the virus penetrates the core of a large sociometric network of drug injectors. Other research has shown that many male injection drug users are involved in primary relationships with women who do not use drugs, thus, involving these women in the drug injectors ' network. Interestingly, however, the risk to these women may not be simple to assess because at
least one study suggests that infected drug injectors were much more likely to use condoms consistently in their sexual relations with noninjectors (Friedman et al., 1994).
Research is needed on how and why networks change over time; on the effects of both sociometric and egocentric networks (and changes in these networks) on social norms, risk behavior, and HIV transmission; and on the use of networks as a strategy of intervention.
LARGE-SCALE SOCIAL CONTEXTUAL INFLUENCES ON THE SPREAD OF HIV
The HIV epidemic is shaped by sociohistorical and sociocultural factors. These include geographical location, local social structure, cultural beliefs and activities, racial and gender stratification, laws, policies, and programs, as well as the process of community disruption described earlier in the case examples from New York City, Haiti, and Thailand. All of these factors are important for understanding and influencing HIV-risk behavior. Research has also demonstrated that the relationship of some high-risk behaviors to HIV infection varies by race, ethnicity, socioeconomic status, geographic location, and culture. Sociological and anthropological research can contribute to a better understanding of the role of the sociohistorical and sociocultural factors, and basic research on ethnic, cultural, and geographic differences can influence the design of targeted interventions. For example, premarital sex, the use of condoms, anal intercourse, and the use of injection drugs are known to have very different meanings for people coming from different cultural heritages and ethnic backgrounds, which in turn support different practices. For example, some Hispanic/Latino men, who engage in penetrative anal sex with other men, regard this behavior as reflecting machismo. In contrast, they may regard only men engaging in receptive anal sex as homosexual. Examples of interventions based on basic research into the culture and organization of populations at risk are the outreach programs among injection drug users in San Francisco and Chicago; these programs were based on years of ethnographic study of their communities.
Much of the early research on AIDS was conducted in the United States or Western Europe, and some of this research was applied to other countries without regard for cultural context. Interventions designed for Western nations, however, were not always effective in changing behaviors among people in African and Asian countries.
Gender Differences: An Example of Contextual Influences
Research has indicated that gender differences influence HIV-risk behaviors, impose barriers to behavior change, and facilitate infection processes (Pivnick et al., 1994; Thompson Fullilove et al., 1993; Schoepf, 1992; Thompson Fullilove et al., 1990). For example, gender roles and cultural norms influence the behaviors of men and women and the nature of their relationships, which in turn influence the nature of their sexual and drug-using behaviors. Women often do not have the same bargaining power as men in negotiating sexual or drug-using behavior. Research has demonstrated that women's involvement with drug use and drug-related crime is greatly influenced by their male partners; whereas men's involvement with drugs is influenced by other men. Recent research has also shown that in some but not all cities women drug injectors get infected with HIV earlier in their injection careers than do men; and that in New York City, this higher level of infection is confined to women with high-risk egocentric injecting risk networks (Friedman et al., 1995). This suggests that additional research is needed to explore power relations between women and men, how these affect the negotiation of safer sex and safer drug use, and how both these power relations and their effects can be changed. Research is also needed to investigate the relation of physical and sexual abuse to HIV-risk behaviors and to initiation into drug use. Research is needed also to explore gender-specific approaches to HIV prevention; specifically, research is needed that targets women who have recently started using drugs, women at risk for using drugs, and women with male partners who use drugs.
MODELS UNDERLYING PREVENTIVE INTERVENTION
There is a growing body of research on HIV preventive interventions employing basic social science concepts such as those identified in the previous section. In addition, there is greater recognition for the need to expand HIV prevention efforts beyond the individual to incorporate social theories of subcultural change. A number of social models discussed at the workshop can be used as a basis for changing subculture: diffusion theory, leadership-focused models, social network theory, social movement/community mobilization theory, models of changing the social environment, and public communication models. HIV prevention strategies based on these social models, which are described below, can effect change at a number of levels, including individual behavior, network structures and norms, and broader social structures. They represent the first step in an expanded HIV prevention
research agenda that encompasses not only the individual but also small groups, subcultures, communities, and the larger society.
Diffusion Theory
Diffusion is the process by which an innovation (including an idea, practice, or object) is communicated to the members of a social system through particular channels (Rogers, 1983). The theory of cultural diffusion is a basic component of anthropological and sociological models of cultural change, and it considers characteristics of both the cultures and the innovations that make it more or less likely for a given innovation to be adopted by a given subculture. Diffusion operates through a chain of influence, from one person to the next. An outreach program in San Francisco designed to help drug injectors provides an example of how the process of diffusion can be utilized to control HIV infection. The intervention started as a word-of-mouth educational program promoting the use of bleach to decontaminate syringes, but it grew to include the distribution of bleach by outreach workers who facilitated the dissemination and acceptance of the innovation. Seroprevalence had been rising prior to the introduction of this innovation, but it subsequently leveled off.
Leadership-Focused Models
Leadership-focused models combine elements of diffusion theory and community organizing theory to encourage naturally occurring group “leaders” to exhibit and communicate an innovation to their peers. Since the innovation may depart from the group's established social norms, these models often rely on making risk-reduction strategies socially normative within the target populations. Successful HIV interventions based on this model have included recruiting former injection drug users to communicate with social networks of injection drug users about the risks of sharing needles; recruiting popular opinion leaders in gay bars to exhibit and communicate AIDS risk reduction messages to their peers; and recruiting sex workers, clients, brothel owners, and brothel managers as peer educators to target behavior changes, including consistent condom use. However, to the extent that influence patterns change rapidly, or that social networks are short-lived, or that there is serious resistance to change among influential segments of a subculture, leadership-focused approaches might be less effective.
Social Network Theory
Recent research suggests that interventions that are based on network concepts or that target the network as the unit of intervention may be effective in reducing risky behaviors and infection levels. In Baltimore, injection drug users were asked to recruit network members to attend a multisession workshop on HIV prevention. Those who attended reduced their risk behaviors more than the randomized controls did (Latkin et al., in press). Interventions that measure and attempt to change larger-scale network structures have not yet been tested. Future research is needed to improve the methodology of social network research and to assess its potential role in intervention. The following methodological issues need to be studied: 1) how to combine formal quantitative techniques, ethnography, and historical perspectives into more effective methods for studying networks; 2) how to gather valid data about social linkages in high-risk populations; 3) how to study social settings such as shooting galleries in network terms; 4) how to conduct sampling in network studies; 5) how to use statistical inference techniques in network studies; and 6) how high-risk individuals such as drug injectors perceive and use their sociometric networks.
Additional research is also needed to incorporate existing knowledge of large-scale social networks of subpopulations and egocentric personal social networks into HIV preventive intervention research. Finally, research is needed on what social conditions and social policies, if changed, might lead to lower-risk social network patterns.
Social Movement/Community Mobilization Theory
Social movement theory describes how social movements initiated by members of the culture change that culture's representations, institutions, or experiences (see Box 2). Although social movements usually develop from the efforts of existing or emergent local leaders, they are sometimes stimulated by outside interventions. Changes that occur may be intended or unintended.
The social movement approach is an important strategy when local popular involvement is needed to implement changes necessary for improving the health of the community. One of the best examples of social movements that have promoted risk reduction is the mobilization that occurred among gay men in response to AIDS. During the 1980s, the gay and lesbian communities of several U.S. cities developed explicit and ongoing AIDS risk-reduction messages and offered a range of outreach programs, including condom availability. The period also witnessed the formation of numerous groups to
advocate for increased resources for AIDS research and of extensive support groups for people with AIDS. These groups had a culture-changing impact.
Friedman and Wypijewska (1995) have suggested that research is needed on 1) the conditions that encourage and discourage mobilization of communities at risk for AIDS; 2) whether efforts to alter the social contexts and conditions of such communities can facilitate effective community mobilization; 3) whether and how efforts by outside agencies to stimulate community mobilization can be successful; 4) the circumstances under which, and procedures by which, community mobilization efforts can change in risk behaviors, risk networks, or other variables in ways that lead to reduced HIV transmission; 5) the best strategies and tactics for such mobilization; and 6) issues regarding how social movements are institutionalized and how to measure the effects of such institutionalization.
|
BOX 2 Drug Users' Organizations: Lives and Responsible Actions Media images of drug injectors portray them as selfish, violent, and hopelessly dependent on their drugs. Both media and academic researchers suggest that it is underlying personality disorders and/or incompetence that lead them to drug use in the first place. Engaging in ethnographic research on drug users' organizations, and talking to users about their lives as part of this research, produces a very different picture of drug users and leads to the possibility of using organizations formed by drug users to spread the HIV prevention message. Street Voice is a drug users' organization in Baltimore that is comprised primarily of African Americans. For a number of years, it has published a street newsletter that carries news about HIV-related issues and changes in local treatment programs or welfare rules, and articles in which users talk about their lives. The organization's members are very friendly to each other and to researchers. Their conversation is by no means confined to issues of getting and using drugs; they also talk with each other about a wide variety of topics, including general political issues, problems that arise in a shelter they are involved in operating for homeless persons, and the structure of the local labor market. |
|
Baltimore's Street Voice is by no means the only drug users' organization. There are dozens of drug users' organizations in Europe, about a dozen in Australia, about ten in the United States, and at least two in Canada. Many of the European and Australian groups receive government funding for their AIDS activities. In Australia, the Netherlands, and Germany, the groups are major actors in formulating AIDS policy and in conducting HIV intervention programs among drug injectors. Drug users' organizations are less common in developing countries; indeed, an organization in Brazil appears to be the only one of its kind. Drug users' organizations and researchers in Australia are currently trying to form such organizations in a number of Asian countries. In addition to local drug users' organizations, there are national and international coordinating bodies, such as the Dutch Federation of Junky Unions, the North American Users Network, the International Drug Users' Network, the Australian IV League, and the European Interest Group of Drug Users. The latter two are particularly active and effective. Researchers have reported that meetings of these organizations are friendly and well-run, even though the presiders and other participants may be active drug users. Drug users' organizations and their members usually have a very active street presence, and they provide assistance and friendship to users and others in their communities. In many areas, they provide the most effective syringe-exchange services. They also work with other users to decide what norms and procedures will be effective in reducing syringe-sharing, unprotected sex, and other risk behaviors, and then help to promulgate and win support for these new norms. |
Models of Changing the Social Environment
Social environments may predispose people to behave in certain ways and may also influence whether or not individuals are able to change their
behaviors. Attempts to change social environments may include changing public policies or social structure. Such efforts are important public health strategies when the existing policies or social structure influence people to behave in unsafe or unhealthy ways. Social policy issues that affect HIV-related behavior include laws and policies on the distribution and possession of syringes, laws on same-sex sex, distribution of condoms in schools, and the content of AIDS education in schools. Examples of social structural issues include policies related to racial and gender stratification, institutionalized homophobia, and urban economic development processes and structures that may disrupt neighborhoods. Friedman and Wypijewska (1995) have suggested that research is needed on the benefits and drawbacks of different social policies and structural effects and on the conditions that influence the success of efforts to change such policies or structures. An example of efforts to change policies that has met with some success is the movement in some cities to establish syringe exchanges (National Research Council and Institute of Medicine, 1995).
We need to learn more about the extent to which changes in action-outcome contingencies are maintained over time within the various social contexts. Social systems, especially interpersonal relationships, are dynamic. Is the maintenance of change within dyads and partnerships dependent on the maintenance of change within communities? Can changes within communities be maintained if they are not accompanied by policy changes?
Public Communication (Media) Models
Long-term HIV prevention research is likely to include planned communication efforts to shape individuals' inclination to high-risk behaviors, groups' social norms regarding safe behavior, and communities' support for HIV prevention education and services. Currently the scope of activity is not this broad. The history and present experience of mass media campaigns are dominated by theories about how individuals process information and respond to a well-articulated and largely agreed upon set of potential individual-level communication objectives, and by conceptualization of the audience as a sizable group of individual, independent targets for the message. Mass media health campaigns with true group-level or community-level communication objectives are the exception rather than the rule.
Group-level outcomes involve people's relationships—specifically, the structural and interactional aspects of social networks (Monge, 1987). How people are linked together in a network of ties will influence the flow of information among them. Examples of structural variables of interest in HIV prevention campaigns are the presence of opinion leaders (members of the
social system who have the ability to influence their peers consistently) and change agencies (people from outside the social system who are perceived as credible sources of information) in the social network. Interactional aspects of social networks have to do with the qualities of relationships and the interpersonal communication within them. Interactional variables of special relevance to HIV communication campaigns direct attention to the degree to which interpersonal communication supports appropriate preventive behaviors. Group-level campaigns try to affect people's relationships in ways that in turn promote HIV prevention.
Community-level campaigns are those that try to increase participation of citizens and gatekeepers of formal organizations, such as government agencies, businesses, schools, hospitals, voluntary organizations, and religious groups, in HIV prevention activities, program funding, and policy issues. Research on planned communication programs as well as on unplanned media coverage targeted to communities should increasingly test theories, such as those related to agenda setting, and systematically address outcomes related to community agenda, participation norms, and efficacy.
The Classification of Preventive Interventions
The above discussion of six models of preventive intervention is certainly not an exhaustive listing of theories underlying social-science based intervention, nor do these models, when put into practice, necessarily constitute distinct forms of intervention. For example, diffusion theory and social network theory are general perspectives that can be used, alone or together, to analyze or plan community interventions. Leadership-focused, social movement, and public communications models describe ways of accessing and working with or on the target population—through leaders, through collective self-motivation, or through the media. Accessing target populations is not limited, however, to these three approaches. Access might be through outreach workers, peers working with peers; meetings, newsletters or other instruments of self-organization of the target group; or institutions such as prisons, emergency rooms and methadone clinics.
Differentiation or classification of interventions according to whether they are based on theory, goals, target populations, or the manner in which they access and work with their target populations can be a subject of controversy and could benefit from further research or synthesis of existing research. For example, any single intervention can be analyzed from a number of theoretical perspectives, even though it might have been based on a single theoretical perspective. In addition, categorizing interventions based on their goals or results may not always be appropriate, because these often overlap. An
argument has been made in some fields that differentiation should be based on target populations or on the manner in which the intervention programs access and work with the target population (IOM 1994b, 1995).
The State of the Art of Preventive Intervention
HIV/AIDS preventive interventions have been functioning since the mid-1980s in dozens of U.S. cities. Many of these programs have been the subjects of detailed evaluation studies. As a result, there is now a second-generation of interventions operating in some communities. For example, some of these interventions are intended to enlist high-risk persons as participants in helping access and educate their peers. (See Box 3.)
Some of the theoretical models presented in this section have provided the foundations for current intervention programs. Other models need to be developed into detailed plans for implementing new prevention programs. Research for both second-generation and new preventive interventions must evaluate the efficiency and effectiveness of novel approaches.
|
BOX 3 Preventive Interventions Many AIDS-prevention interventions are based on the hierarchy inherent in the provider/client relationship. An alternative approach is for providers to attempt to empower people at risk of HIV infection to provide services for their peers. This approach increases the interdependence of these at-risk persons and helps to create and strengthen self-help networks within the community. A program in Eastern Connecticut targets out-of-treatment injection drug users (IDUs) to recruit other users to use the facilities at a storefront base of operation—HIV testing and counseling, risk-reduction education, and prevention materials. Recruitment is done via a coupon system; for each IDU recruited, the user who recruited him or her receives a modest monetary reward. These recruits, in turn, are also given a limited number of coupons to recruit still other IDUs within their network. The IDUs are also given incentives to educate their peers in the community. The extent to which IDUs pass on information to those they recruit can be measured through questions added to standard interview schedules, and the reward to the recruiter depends on the recruit's knowledge. (See Heckathorn's response to the commissioned paper by Craig Ewart for more details regarding this promising intervention.) |












