
3
Descriptive Epidemiology of the Perinatal Transmission of HIV
In 1997, at least 432 cases of perinatally transmitted AIDS were reported in the United States (CDC, 1997c). This number, however, represents only a small fraction of the number of individuals affected by this problem. First, these AIDS cases represent children born with HIV infection in 1997 and earlier years. Most of the AIDS cases resulting from children born with HIV infection in 1997 have not yet been diagnosed or reported. Second, although only a fraction of childbearing women with HIV pass the infection on to their children, each of the 6,000 to 7,000 HIV-infected women who gives birth each year requires treatment to prevent transmission as well as for her own infection. Finally, each of the millions of women who become pregnant each year must confront the possibility that she might be infected and could pass the virus on to her child.
To evaluate the progress that has already been made in implementing the Public Health Service (PHS) counseling and testing guidelines for pregnant women (CDC, 1995b), and to identify additional approaches to preventing perinatal transmission, it is important to understand recent trends and current characteristics of women and children with HIV infection and AIDS. To that end, this chapter describes the advantages and difficulties in current surveillance data systems, and presents descriptive information on the epidemiology of perinatal transmission.
HIV/AIDS Surveillance Data
The impact of the HIV/AIDS epidemic can be seen in a variety of ways. Where available, data on new HIV infections and individuals infected with HIV
are preferable, but data of this sort are often not available because, in many individuals, HIV is undetected or unreported. The HIV/AIDS epidemic, therefore, is often viewed through the imperfect lens of AIDS cases. AIDS is a clinically observable syndrome that is clearly defined and required to be reported in every state. Many individuals with new HIV infections have not progressed in their disease to the point that AIDS can be diagnosed, so AIDS statistics reflect HIV infections that occurred up to a decade or more in the past. Thus, five different type of epidemiological data can shed light on trends and patterns in perinatal transmission of HIV: (1) reported cases of AIDS in women, (2) reported cases of AIDS in children, (3) reported HIV infections in women (where available), (4) estimates of the prevalence of HIV in childbearing women based on the Survey of Childbearing Women (SCBW) (see below), and (5) reported HIV infections in newborn children. Data on HIV infections in children are typically available only in states with mandatory HIV reporting. These states monitor perinatally exposed children to see if they convert from HIV-positive due to maternal antibodies to HIV infection and AIDS status. Each type of data has its strengths and weaknesses, but taken together it is possible to construct a relatively complete picture of the perinatal HIV epidemic in the United States.
AIDS case reports, the source of the first two data series mentioned above, are gathered by state, territorial, and local health departments and reported to the Centers for Disease Control and Prevention (CDC) to form a national AIDS surveillance system. Standard CDC records for each case include information on age at diagnosis, sex, race and ethnicity, state of residence (and metropolitan area, if relevant), mode of exposure to HIV (including maternal risk for pediatric cases), month of AIDS diagnosis, date reported to CDC, and other information. The national data are made available in terms of biannual tabular reports (CDC, 1997c), an AIDS Public Information Data Set (APIDS) (CDC, 1997a), and other reports from CDC (see, for example, CDC, 1996a, 1997e; Wortley and Fleming, 1997). Many states also routinely produce HIV/AIDS surveillance reports.
Even though nearly all current pediatric AIDS cases are the result of perinatal transmission, information on reported AIDS in children provides only limited insight into the problem. First, many children infected with HIV perinatally do not develop AIDS until they are substantially older. There seems to be a bimodal distribution; approximately 48% of HIV-infected children develop AIDS by three years of age, and thereafter less than 3% per year develop AIDS (Pliner et al., 1998). Diagnosed AIDS cases thus reflect perinatal transmissions in births years earlier. Second, once diagnosed, AIDS data are subject to reporting delays. Overall, only 55% of cases are reported to CDC within three months of diagnosis, but 20% are reported more than one year after diagnosis (CDC, 1997a). Reporting delays are longer for pediatric cases (an average of six months) than for adult cases (which average three months). Published data are sometimes adjusted for
reporting delays (CDC, 1997a), but by their nature these adjustments cannot be precise.1
HIV data for women and children are more problematic. As of December 1997, HIV cases are reportable in only 30 states (in 3 of these states for children only). These states reported only 28% of all prenatally acquired AIDS cases through September 1997 (CDC, 1997e). Even in these states, the data count only individuals who have been tested, not all HIV-infected individuals.
Between 1988 and 1994, most states anonymously tested newborn heel-stick blood samples for HIV in a program called the Survey of Childbearing Women (SCBW) (Davis et al., 1995). Because newborn blood carries maternal HIV antibodies, data from this survey reflect the prevalence of HIV in childbearing women. As described in Chapter 2, this survey was discontinued, but some states have continued to test newborn blood in the same way and report the results (see Appendix D). In addition, Byers and colleagues (1998) have been able to project the data from this survey to more recent years, yet the lack of recent data complicates the assessment of the impact of the PHS counseling and treatment guidelines.
HIV And AIDS In Women
In 1997, women accounted for 21% of AIDS cases in adults, and the proportion of all cases that are female continues to grow. Most of these cases are attributed to injection drug use (32%) or heterosexual contact (38%). Since most of the women in the second category attribute their infection to sex with an injection drug user (29%) or sex with an HIV-infected partner with unknown risk (64%) (CDC, 1997c), at least two-thirds of AIDS cases in women can be directly or indirectly attributed to injection drug use. Although a subset of women with HIV have injected drugs or have had sex with a known injection drug user, an increasing proportion of women have become infected through sexual activity with men whose risk behaviors were unknown to them.
In 1997, 60% of AIDS cases reported in women were in African-American, non-Hispanic women, and 20% were in Hispanic women (CDC, 1997e). AIDS incidence rates are highest in African Americans (58.8 per 100,000 women) and Hispanics (21.5 per 100,000 women), compared to 3.0 per 100,000 in white, non-Hispanic women. AIDS is more prevalent in women in the Northeast (22.3 per 100,000 women in 1995) and the South (11.1 per 100,000 in 1995). While AIDS in women is also more common in large cities—74% of 1995 cases were in metropolitan areas with more than one million population—the greatest increases
in incidence between 1991 and 1995 were in women in the South and younger women, those who were 14 to 18 years old in 1988 (Wortley and Fleming, 1997).
Approximately 6,000 to 7,000 HIV-infected women give birth every year (Byers et al., 1998). According to the SCBW, overall, 17 per 10,000 women giving birth are infected with HIV (Davis et al., 1995). Trend data show a relatively steady national rate of HIV prevalence in childbearing women between 1989 and 1994, the last year for which data are available. There are, however, important regional variations. In the Northeast, where the epidemic started and peaked earliest, a 25% decline occurred in the number of HIV-infected childbearing women between 1990 and 1994. In the South, where the epidemic started later, there was a 25% increase between 1989 and 1991, and a level trend thereafter. The West and Midwest had stable and relatively low rates (Appendix D).
Estimates of the proportion of children born to HIV-infected women who are themselves infected with HIV vary, ranging from 14% to 33% in studies performed in the United States and Europe before the ACTG 076 (AIDS Clinical Trials Group protocol number 76) results became known. More recent estimates of the transmission rate, reflecting partial implementation of the ACTG 076 protocol, range from 3% to 10% (see Chapter 4).
Perinatally Transmitted Aids
Taking into account changing prevalence and transmission rates, perinatal transmission of HIV accounted for a cumulative total of 7,335 AIDS cases and an unknown number of HIV-infected children in the United States as of December 1997 (CDC, 1997c). There were 473 cases of pediatric AIDS (i.e., under age 13 at time of diagnosis) reported in 1997, and a total of 8,086 since the beginning of the epidemic (CDC, 1997c). Of the 473 cases in 1997, 432 (91%) were born to mothers with or at risk for HIV infection, as shown in Table 3.1. The breakout by mother's risk indicates that 107 (25%) of the known perinatally transmitted cases had mothers who used injection drugs, and an additional 60 (14%) of the mothers had sex with an injection drug user. Drug use is probably responsible for a substantial proportion of the cases born to the 249 (58%) mothers with HIV infection whose risk is not specified or who had sex with an HIV-infected person whose risk is not specified. Injection drug use, therefore, is associated with between 39% and 72% of perinatally acquired AIDS.
The number of reported perinatally acquired AIDS cases rose rapidly in the late 1980s and early 1990s, peaked around 1992, and subsequently declined by approximately 43% by 1996 (see Figure 3.1). In 1997, 473 cases of pediatric AIDS were reported (CDC, 1997c).2 This decline was due to a number of factors.
|
2 |
The 1997 figure is not adjusted for reporting delays, so is not comparable to the numbers in Figure 3.1. |
TABLE 3.1 Pediatric AIDS Cases by Exposure Category, Reported in 1997 and Cumulative Total through December 1997
|
Exposure Category |
1997 No. |
(%) |
Cumulative No. |
(%) |
|
Hemophilia/coagulation disorder |
1 |
(0) |
233 |
(3) |
|
Mother with/at risk for HIV infection |
432 |
(91) |
7,335 |
(91) |
|
Injecting drug use |
107 |
|
2,936 |
|
|
Sex with injecting drug user |
60 |
|
1,340 |
|
|
Sex with bisexual male |
7 |
|
159 |
|
|
Sex with person with hemophilia |
2 |
|
28 |
|
|
Sex with transfusion recipient |
— |
|
24 |
|
|
Sex with HIV-infected person, risk not specified |
102 |
|
1,033 |
|
|
Receipt of blood transfusion, blood components, or tissue |
7 |
|
154 |
|
|
Has HIV infection, risk not specified |
147 |
|
1,661 |
|
|
Receipt of blood transfusion, blood components, or tissue |
2 |
(0) |
374 |
(5) |
|
Risk not reported or identified |
38 |
(8) |
144 |
(2) |
|
Total |
473 |
(100) |
8,086 |
(100) |
|
SOURCE: CDC, 1997c. |
||||
First, CDC calculations based on the SCBW and other data show that between 1992 and 1995, there was a 17% decline in the number of births to HIV-infected women (Byers et al., 1998). Much of the rest has been attributed to increased testing and adherence to the ACTG 076 regimen and better prenatal and intrapartum care. Declines that occurred before the publication of the ACTG 076 findings have been attributed to broader use of ZDV (zidovudine) by women, regardless of pregnancy (see Appendix D).
Because good seroprevalence data are lacking for children, we must use AIDS case reports to understand changes in perinatally transmitted HIV. Reflecting the racial and ethnic composition of women with AIDS, perinatally transmitted cases were concentrated in African-American (60%) and Hispanic (24%) children in 1997.3 These proportions have remained relatively stable for a decade. The disparity appears greater, however, when the numbers of African-American, Hispanic, and other births are taken into account. In 1996, perinatal AIDS incidence rates (perinatal AIDS cases as a proportion of births) were roughly four times higher for African Americans than for the entire population
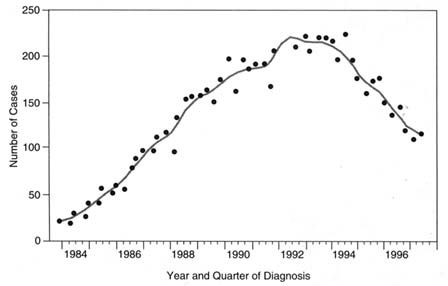
FIGURE 3.1
Number of perinatally acquired AIDS cases, by quarter year of diagnosis, 1984 through 1997. Estimates are based on cases reported through September 1997, adjusted for reporting delay and unreported risk but not for incomplete reporting of diagnosed AIDS cases. Points represent estimated quarterly incidence, and the line represents ''smoothed" incidence. SOURCE: CDC, 1997e.
(65 versus 16 per 10,000 births), and higher than average among Hispanics (19 per 10,000 births). The incidence rate for whites and others is substantially lower than average (3 per 10,000 births), leading to a 32 to 1 differential between African-American and white incidence rates (CDC, 1996b; Ventura et al., 1997).
Figure 3.2 shows trends in the number of perinatal AIDS cases, by race and ethnicity, from 1979 through 1996. The number of African-American children with AIDS grew through 1992 and fell by about 42% between 1992 and 1996. The number of cases in Hispanic children was relatively flat from 1987 through 1992 and fell by 43% between 1992 and 1996. The number of perinatal AIDS cases in white children fell by 50% between 1992 and 1996.
Trends by age at diagnosis (Table 3.2) show that the largest declines are among children diagnosed as infants, with substantial declines also among children diagnosed at ages one to five years. For older children, similar levels of decline have not been observed (CDC, 1997d). These findings are consistent with the expectation that efforts to prevent perinatal transmission would be reflected earliest in infants because older children were born before antiretroviral therapy was used widely in pregnancy (Appendix D).
Pneumocystis carinii pneumonia (PCP) is the most common AIDS-defining condition in children. Since recommendations regarding PCP prophylaxis were
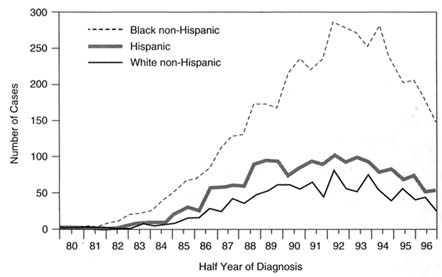
FIGURE 3.2
Number of perinatally acquired AIDS cases, by race and half year of diagnosis, 1979 through 1996. Estimates are based on cases reported through September 1997, adjusted for reporting delay and unreported risk but not for incomplete reporting of diagnosed AIDS cases. SOURCE: Lindegren et al., 1998.
evolving during the same period that dramatic declines occurred in perinatally acquired pediatric AIDS cases, it is useful to look at whether declines in pediatric AIDS reflect more than declines in PCP. CDC surveillance findings show substantial declines not only in PCP, but also in other opportunistic infections for which specific prophylaxis was not available, indicating that the decline in pediatric AIDS cases is not being driven solely by changes in PCP, but appears to reflect true declining perinatal HIV transmission rates.
Pediatric AIDS cases are concentrated in eastern states, and especially in the New York metropolitan area. In 1996, three states alone—New York, New Jersey, and Florida—reported 330 cases. This represents 49% of the diagnosed cases, even though only 15% of children are born in those states (CDC, 1996b; Ventura et al., 1998). In contrast to their concentration in the Northeast, perinatal AIDS cases are less common in most geographical areas. In 1997, 39 states had fewer than ten perinatally transmitted AIDS cases (CDC, 1997e).
Figure 3.3 displays pediatric AIDS incidence rates (perinatal AIDS cases as a proportion of births) by state for 1996 as an illustration of this great variability, ranging from 30.9 per 10,000 births in the District of Columbia to zero in 14 states. The District of Columbia. Florida (6.3 per 10,000). New York (6.1 per 10,000), New Jersey (4.3 per 10,000), Connecticut (3.8 per 10,000), and Maryland (3.0 per
TABLE 3.2 Estimated Number of Children with Perinatally Acquired AIDS, by Selected Characteristics, Year of Diagnosis, and Percentage Change from 1992 to 1996, United States, 1992–1996a
|
|
Year |
|||||
|
Characteristic |
1992 |
1993 |
1994 |
1995 |
1996 |
% Change 1992 to 1996 |
|
Race/Ethnicityb |
||||||
|
White, non-Hispanic |
133 |
126 |
92 |
95 |
67 |
-50% |
|
Black, non-Hispanic |
566 |
531 |
522 |
415 |
331 |
-42% |
|
Hispanic |
195 |
195 |
166 |
146 |
111 |
-43% |
|
Age at AIDS Diagnosis |
||||||
|
<5 years |
733 |
693 |
613 |
459 |
360 |
-51% |
|
>5 years |
168 |
169 |
179 |
202 |
156 |
-7% |
|
Regionc |
||||||
|
Northeast |
361 |
379 |
315 |
265 |
212 |
-41% |
|
South |
362 |
315 |
332 |
243 |
223 |
-38% |
|
Midwest |
60 |
74 |
54 |
67 |
30 |
-50% |
|
West |
67 |
58 |
65 |
60 |
35 |
-48% |
|
Metropolitan Statistical Area |
||||||
|
>500,000 pop. |
748 |
732 |
675 |
558 |
450 |
-40% |
|
50,000–500,000 pop. |
102 |
75 |
75 |
62 |
41 |
-60% |
|
<50,000 pop. |
51 |
53 |
42 |
39 |
22 |
-57% |
|
a Diagnosed through 1996 and reported through September 1997 adjusting for reporting delays and unreported risk. b Numbers for other racial/ethnic groups were too small for meaningful analysis. c Northeast = Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont; South = Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia; West = Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Orego, Utah, Washington, and Wyoming; and Midwest = Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin. SOURCE: CDC, 1997e. |
||||||
10,000) have the highest incidence rates. Illinois (1.4 per 10,000), California (0.9 per 10,000), and Texas (0.5 per 10,000) have incidence rates lower than the national average of 1.7 per 10,000 (CDC, 1996b; Ventura et al., 1998).
Reviewing the data by metropolitan statistical areas (MSAs) suggests that perinatal AIDS cases were even more concentrated than the state analysis suggests. In fact, two of the three MSAs with the greatest number of perinatal AIDS cases (New York City and Newark, New Jersey) are in the New York metropolitan
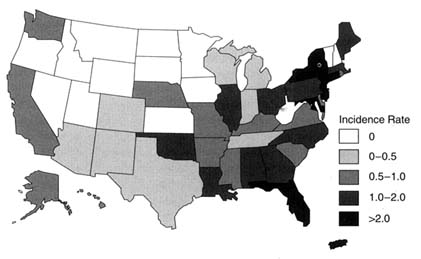
FIGURE 3.3
Annual incidence rates for perinatal AIDS. 1996, by state.
SOURCE: calculated from CDC. 1996b; Ventura et al., 1998.
area. These two MSAs alone account for 38% of all perinatal AIDS cases in the United States. Data on the distribution of AIDS cases within New York City suggest that the concentration varies substantially by neighborhood (NRC, 1993), and this patchwork pattern is likely to be found for perinatal AIDS cases as well.
Perinatal transmission cases are similarly less common in most metropolitan areas. Out of the 253 MSAs for which AIDS data are available, only 66 (26%) have had more than ten reported perinatal cases from the beginning of the epidemic through the end of 1996. Only 24 MSAs (9%), have 50 or more cumulative cases each.









