
1
Migration, Mobility, and Health
OVERVIEW
Opening presentations by Mark Miller of the University of Delaware and Brian Gushulak of the Canadian Immigration Department Health Branch set the context for this workshop by exploring the history and ongoing political and public health significance of human migration and mobility. Their contributions to this chapter establish a firm foundation for those that follow, providing both a wealth of detail and an overarching view of the changing picture of human migration through the ages, and particularly during the recent decades.
Miller’s essay reviews human migratory history, focusing on the contemporary “Age of Migration” that began around 1970. This era “has witnessed major developments in human mobility affecting all areas of the world,” Miller writes. “Understanding this still evolving global migratory context bears importantly upon comprehension of contemporary microbial threats.” Conversely, he notes the importance of health issues to the study of migration and security, particularly in recent years.
Miller examines the geopolitical origins of the present Age of Migration and examines its defining features. These he characterizes as the globalization, acceleration, differentiation, politicization, feminization, and proliferation of migration in the traditional sense (the one-way movement of people from one homeland to another); the advent of formal mechanisms supporting “circular” migrations such as guestworker programs; and the growth of international tourism. Reflecting on the future of migration and development, and recognizing that “the chief threats to U.S. security since the 1970s arose from failed states and the abysmal living conditions of average people in much of the world,” Miller advocates a
stronger commitment on the part of the United States to development in Africa, the Middle East, and other developing countries, including increased admissions of permanent residents from these regions.
In his subsequent contribution, Gushulak, along with his colleague Douglas MacPherson, of McMaster University and Migration Health Consultants, Inc., presents a comprehensive history of migration-associated disease and disease control policies. The authors characterize “modern migration”—the mechanism that drives Miller’s “Age of Migration”—in terms of its departure from traditional migratory patterns, and explore the challenges it presents for global health, and particularly for the control of infectious diseases.
In order to “shift the paradigm” of disease control away from policies focused on geopolitical borders and individual infectious diseases, Gushulak and MacPherson introduce the concept of “population mobility” to replace traditional considerations of migration. “Considering mobility as a global health determinant provides a model upon which we can integrate disease management policies, processes for prevention, knowledge of disparate prevalence environments, and a rigorous health threat to risk assessment ability,” the authors write, and they suggest several approaches to the control of mobility-related disease to support this model.
INTERNATIONAL MIGRATION PAST, PRESENT, AND FUTURE1
Mark J. Miller, Ph.D.2
University of Delaware
Public health has been importantly influenced by human mobility patterns since time immemorial. A rich, but frequently overlooked, tradition of scholarship attests to the significance of understanding human mobility for comprehension of events involving plagues and spatial diffusion of illnesses (Diamond, 1997; McNeill, 1977). Many students of world politics and international relations have distinguished themselves by their neglect of health questions in explanations of wars and conquests (Koslowski, 2000). Nevertheless, no effort will be made here to reprise that literature. Rather, the focus will be upon sketching what Stephen Castles3 and I call The Age of Migration, the contemporary migratory epoch that
began circa 1970 which has witnessed major developments in human mobility affecting all areas of the world. Understanding this still evolving global migratory context bears importantly upon comprehension of contemporary microbial threats. Health issues comprise a not insignificant dimension of the still emerging field of study of migration and security, a scholarly focus of considerable historical pedigree that reemerged after the Cold War and especially after 9/11 (Castles and Miller, 2009).
Migrations Past: International Migration in the Modern Age
To paraphrase Kemal Karpat,4 rarely does migration not figure importantly in the history of humankind. Recent anthropological evidence concerning the late Iron Age in Europe suggests that distinctive societies were much more interconnected and fluid than once thought (Wells, 2001). The prosperity and goods of ancient Greece and Rome fostered trade and myriad other interactions just as the military might of Greece and Rome posed a perceived grave threat to tribes and peoples on the periphery, forcing them to adapt, change, and define their identities. The extensive Viking migrations of the eighth to eleventh centuries gave rise to plunder and violence. But those migrations also involved trade and commerce. Medieval migration of Jews in Europe often was linked to rulers’ efforts to spur economic development and to generate greater tax revenues. Much the same could be said about medieval German migrations eastward (Miller, 2008).
The term international migration, which the United Nations (UN) defines as occurring when a citizen or national of one state moves to another state for a period of at least one year, presupposes the existence of an international system of states. Many students of international relations trace the emergence of the contemporary international or Westphalian system to seventeenth-century Europe and the end of the Thirty Years War5 brought about by the treaties of Westphalia. This embryonic nation-state system then diffused to the rest of the world through processes of colonization and imperialism followed by decolonization and the embrace of the sovereign national state system born of Europe after World War II.
Voyages of discovery, conquest, and trade by Europeans marked the advent of the Modern Age. European domination of the New World ensued as many indigenous people succumbed to European-borne diseases, although European populations also were adversely affected by diseases contracted in non-European areas for which Europeans possessed insufficient or little immunity. In general, with the major exception of the 400-year-long African slave trade, which involved over 15 million Africans, population transfers initially were
quite limited (Curtin, 1997). The cost of maritime travel was prohibitive except for the wealthy and, in an age of Mercantilism, European rulers viewed their subjects as valued possessions, especially for military conscription. The anti-migration norm began to erode only after 1800.
A number of developments set the stage for the first era of mass migration, which mainly involved Europeans. The French Revolution gave birth to a new norm, a human right to emigrate. Technological innovations and other factors began to make transatlantic travel economically possible for larger segments of the European population. Many of the former colonies comprising the newly founded American Republic welcomed and encouraged settlement by Europeans. Population growth, particularly in Great Britain and Ireland, which can partially be attributed to improvements in public health, particularly in cities, also constituted a factor.
The growth of the Irish population figured centrally. Ireland had been incorporated into Great Britain in 1801, resulting in growing migration of Irish to England in particular. The poverty of many of the Irish migrants and their Roman Catholicism caused alarm. Soon local governments discovered it was less expensive to help transfer the Irish to Canada and the United States than to provide for them in situ. By the 1820s, the mercantilist anti-emigration norm had eroded (Zolberg, 2006).
Between 1820 and 1939, roughly 60 million Europeans immigrated to the New World, which included Argentina and other areas in Latin America, Australia, and New Zealand as well as the United States and Canada (Hatton and Williamson, 1998, 2005). However, the composition of the migration flows changed over time, especially after abolishment of serfdom in the Czarist Empire. By the late-nineteenth century, many areas in western and northern Europe had become zones of immigration, particularly France which, in the interwar period, had become the world’s premier land of immigration.
In the United States by the 1880s and 1890s, concerns over the effects of immigration had increased. The first federal commission to study immigration, thereby inaugurating migration studies in the United States, suggested reductions in immigration, recommendations that began to be translated into law by 1917. The Quota Acts of 1921 and 19246 severely curtailed European migration to the United States. Other New World immigration lands emulated the United States, thereby bringing the first period of mass migration to a virtual end.
After the Great Depression and the long night of World War II, a number of areas reemerged as significant lands of immigration or emigration. The United States admitted several groups of “displaced persons” and continued to admit Mexican temporary workers, which had resumed under a 1942 bilateral accord
with Mexico.7 A major reform of U.S. immigration law in 19528 somewhat reopened the “Golden Door” which had largely been closed in the 1920s. The resumption of immigration policy was accentuated by the 1965 amendments to the 1952 law, which came into effect in 1968 (Daniels, 2004).
Hatton and Williamson (2005) have identified five developments that precipitated the Age of Migration by 1970. Latin America changed from being a net importer of international migrants to a net exporter. The bulk of Latin American emigrants went to the United States as Latin American economic growth lagged behind that of the United States. Later, and especially after the Cold War, significant flows of Latin Americans would also go to Europe, especially to the Iberian Peninsula and Italy. Western Europe itself also became a major zone of immigration, especially after a large faction of post-World War II guestworkers settled, contrary to expectations, and were joined by family members. The oil-producing areas of the Middle East and North Africa also became major zones of immigration. Unlike during the era of mass European emigration to the New World, areas of Asia and Africa also became significant zones of emigration to other areas of the world, but especially to Western Europe and parts of the New World. Finally, somewhat later, the areas of Eastern Europe, long frozen by Soviet domination, itself an echo of the mercantilist antimigration norm, began to thaw. Ostpolitik9 and détente10 began to open the door to emigration. The collapse of Communist governments led to large-scale emigration followed by migration transition; that is, Central and European states simultaneously became lands of emigration and immigration especially after the European Union (EU) enlargements of 2004 and 2007, which brought 12 additional states into the European regional integration framework.
The Age of Migration
Stephen Castles and I maintain that the current era is defined by six general tendencies:
-
The globalization of migration: the tendency for more and more countries to be crucially affected by migratory movements at the same time (Miller, 2008).
-
The acceleration of migration: international migration is increasing in all the world’s regions. While the percentage of international migrants in the world’s population remains roughly constant at between 2 and 3 percent, the world’s population continues to grow and will do so for several decades into the future, before peaking at about nine billion persons. Most future growth will occur in Africa and Asia. Nevertheless, growth of international migration is not inexorable. Repatriations, for instance, have significantly reduced some refugee populations (Miller, 2008).
-
The differentiation of migration: most countries, states, and governments around the world face increasingly complex challenges in regulating international migration as they encounter, and sometimes precipitate, diverse inflows of migrants (Miller, 2008). Immigration countries tend to receive migrants from a larger number of source countries, so that most immigration lands have entrants from a broad spectrum of social, economic, and cultural backgrounds.
-
The politicization of migration: international migration-related issues are becoming increasingly salient in domestic politics, bilateral and regional relations, and at the global level as witnessed by the creation of the Global Commission on International Migration (GCIM) and the convening of a high-level conference on migration and development at the UN in 2006. After consultation with then UN Secretary-General Kofi Anan in 2003, a number of UN member states funded the GCIM to conduct research, promote dialogue, and make recommendations about policies concerning international migration.11 It mainly stressed the potential benefits of international migration for development. In 2003, the UN General Assembly also decided to hold a high-level dialogue on international migration and development in 2006. The Secretary-General’s report on this meeting recommended a forum for UN member states to discuss migration and development issues further. However, the forum was to be purely advisory and was not intended to facilitate negotiations. The first Global Forum on Migration and Development was hosted by the Belgian government in July 2007, with a second in Manila in October 2008.
-
The feminization of migration: women have become more salient participants in international migration. Many international flows are comprised mainly of women, such as domestic workers in the Middle East. And women are disproportionally victims of human trafficking (Miller, 2008).
-
The proliferation of migration transition: more and more states have experienced migration transition; that is, traditional lands of emigration
|
11 |
The 2005 report of the Geneva-based commission can be accessed at www.gcim.org. |
-
have become lands of immigration. States as diverse as Thailand, Turkey, Morocco, Greece, Italy, Spain, the Republic of South Korea, and Mexico have experienced transition during the Age of Migration (Miller, 2008).
Table 1-1 summarizes the evolution of global migration between 1960 and 2005. There is mounting evidence that the worldwide financial and economic crisis of 2008-2009 has disproportionately adversely affected international migrants as has been the pattern in earlier economic crises such as in the mid-1970s.12
Other measures of human mobility likewise attest to the growing significance of international migration. Table 1-2 lists the top 10 countries with the highest numbers of international migrants in 1990 and 2005. Spain viewed itself as a land of emigration and as a transit zone as late as 1990. Virtually all of its nearly five million migrants in 2005 had arrived illegally, were legalized, or arrived through family reunification measures.
Table 1-3 indicates that international tourism is surging despite the War on Terrorism. Refugee and asylum-seeker flows, widespread human trafficking and smuggling, short-term highly skilled labor flows, student study abroad, and other forms of international mobility suggest that few human beings today are unaffected by international migration. In 2009, the Organisation for Economic Cooperation and Development (OECD) estimated that approximately five million people cross international borders each year to take up residency in a developed country.
Thoughts About the Future of Migration and Development13
Usually understanding the past serves as the best guide to understanding the future. International migration played a central role in the shaping of the modern, Westphalian world in which we still live. It is likely to continue forging and reforging states and societies in the future.
International migration can foster development in both receiving and sending areas, as attested to by the U.S.-Swedish migratory relationship before 1914.14 High hopes were attached to the promise of international migration generating sustained socioeconomic and political development in the Asian and African hinterlands of West Europe in the 1960s and 1970s, but those hopes largely proved misplaced.
Nevertheless, a new optimism has arisen over prospects for migration and development through well-managed bilateral and regional policies. This optimism
|
12 |
Postings on the effects of the ongoing crisis for international migrants can be found at www.age-of-migration.com. |
|
13 |
The following text comes from Miller (2008). |
|
14 |
Hatton and Williamson (2005) observe that Sweden largely closed its development gap with Great Britain and other more advanced European states between 1860 and 1914 when about one-fifth of all Swedes emigrated to the New World and principally to the upper midwest of the United States. |
TABLE 1-1 Number of International Migrants by Region, 1960-2005 (in millions)
TABLE 1-2 The 10 Countries with the Highest Number of International Migrants (in millions)
|
Rank |
1990 |
|
2005 |
|
|
1 |
United States of America |
23.3 |
United States of America |
38.4 |
|
2 |
Russian Federation |
11.5 |
Russian Federation |
12.1 |
|
3 |
India |
7.4 |
India |
10.1 |
|
4 |
Ukraine |
7.1 |
Ukraine |
6.8 |
|
5 |
Pakistan |
6.6 |
France |
6.5 |
|
6 |
Germany |
5.9 |
Saudi Arabia |
6.4 |
|
7 |
France |
5.9 |
Canada |
6.1 |
|
8 |
Saudi Arabia |
4.7 |
India |
5.7 |
|
9 |
Canada |
4.3 |
United Kingdom |
5.4 |
|
10 |
Australia |
4.0 |
Spain |
4.8 |
|
SOURCE: Based on data in UNDESA (2006) and reprinted from Koslowski (2008) with permission from the Center for Migration Studies. |
||||
is linked to more precise understanding of the vast volume of migrant remittances to homelands.
A number of scholars and policy makers have advocated temporary foreign worker admissions policies in OECD democracies as part of a circular migration strategy to promote mutually beneficial development in sending and receiving states. A certain skepticism about such advocacy appears in order.
The historical track record of temporary foreign worker admissions policies in democratic settings can be termed checkered at best. Guestworker, seasonal
TABLE 1-3 International Tourist Arrivals (in millions, ordered in 2006 ranking)
|
Rank |
|
1995 |
2000 |
2002 |
2003 |
2004 |
2005 |
2006 |
|
|
World |
535.0 |
682.0 |
702.0 |
691.0 |
761.0 |
803.0 |
846.0 |
|
1 |
France |
60.0 |
77.2 |
n/a |
75.0 |
75.1 |
75.9 |
79.1 |
|
2 |
Spain |
34.9 |
47.9 |
n/a |
50.8 |
52.4 |
55.9 |
58.5 |
|
3 |
US |
43.5 |
51.2 |
43.6 |
41.2 |
46.1 |
49.2 |
51.1 |
|
4 |
China |
20.0 |
31.2 |
36.8 |
33.0 |
41.8 |
46.8 |
49.6 |
|
5 |
Italy |
31.1 |
41.2 |
n/a |
39.6 |
37.1 |
36.5 |
41.1 |
|
6 |
UK |
23.5 |
25.2 |
n/a |
24.7 |
27.7 |
28.0 |
30.7 |
|
7 |
Germany |
14.8 |
19.0 |
n/a |
18.4 |
20.1 |
21.5 |
23.6 |
|
8 |
Mexico |
20.2 |
20.6 |
19.7 |
18.7 |
20.6 |
21.9 |
21.4 |
|
9 |
Austria |
17.2 |
18.0 |
n/a |
19.1 |
19.4 |
20.0 |
20.3 |
|
10 |
Russia |
n/a |
n/a |
n/a |
20.4 |
19.9 |
19.9 |
20.2 |
|
11 |
Turkey |
7.1 |
9.6 |
n/a |
13.3 |
16.8 |
20.3 |
n/a |
|
SOURCE: Based on data in UNWTO (2005, 2006, 2007) and reprinted from Koslowski (2008) with permission from the Center for Migration Studies. |
||||||||
worker, and bracero-style policies15 had problems and unintended consequences for quite well understood reasons. The Swiss reformed their seasonal worker policy in 1964 to allow those workers who worked five consecutive seasons to adjust to resident status under diplomatic pressure from Italy. The volume of seasonal foreign worker admissions also became controversial, leading to the divisive anti-Ueberfremdung16 campaigns of the 1970s which gave way to similarly unsuccessful referenda campaigns to abolish seasonal foreign worker policies as incompatible with human dignity in the 1990s. Swiss seasonal worker policy was not mismanaged. And as late as the 1973 to 1975 period, many seasonal worker permits were not renewed due to the recession, thereby enabling Switzerland to shift some of the costs of the recession to Italy.
Similarly, German guestworker policies generally were well administered. But there was considerable political sympathy for legally admitted foreign
workers by the 1970s. German courts blocked conservative efforts to enforce rotation after 1973 as incompatible with the Federal Republic’s legal engagements and responsibilities. This constituted an enormous victory for German postwar democracy that is too little appreciated.
Bracero-policy history between Mexico and the United States does not appear to have yielded much evidence of fostering sustainable development in Mexico. U.S. recruitment of temporary Mexican foreign workers dates back to before World War I. Such recruitment helped set in motion large-scale unauthorized migration to the United States. Significantly more unauthorized Mexican workers were returned to Mexico than legally recruited during the 1942 to 1964 period. The United States unilaterally terminated the policy in a period of growing consciousness and concern about civil rights and the effects temporary foreign worker admissions had upon American farm workers.
The evolution of French seasonal foreign worker admissions after World War II somewhat resembled events in Switzerland. Admissions of seasonal workers mainly for agricultural employment crested at about 250,000 per year in 1968 but were steadily phased out afterward. Significant numbers of seasonal workers became so-called faux saissoniers (or false seasonal workers) and overstayed their visas. Many applied for the recurrent legalizations between 1972 and the 1980s. Seasonal foreign worker admissions continue today but in very small numbers.
Since 1990, a new generation of temporary foreign worker admission policies have emerged in Europe, especially in Southern Europe. The new policies are more narrow-gauged than policies during the guestworker era. The key issue is: Will their outcomes resemble those of the guestworker era? Advocates of circular migration policies take an optimistic view.
Spain’s recent bilateral initiatives toward Black African states in Western Africa perhaps best exemplify the optimistic perspective. In return for cooperation with Spain and the EU on management of international migration, including prevention of illegal migration and human trafficking, as well as readmission of citizens illegally entering the European space, Spain will provide for job training and then admit trained and prepared foreign workers for time-bound employment in sectors lacking adequate labor supply such as agriculture.
At first glance, such policies may appear constructive, even progressive. But almost by definition, the legal status of temporary foreign workers is contingent. Usually the foreign workers are tied, as it were, to a particular employer or industry. Of course, there is no incontrovertible way to measure need for additional foreign workers in a given industry, but especially in agriculture. Perceptions of need represent outcomes of political and legal battles usually pitting employers against unions. Usually, employers have their way even with governments of the left, which has been the case in Spain since 2004.
It is important to point out that there are viable policy alternatives to the circular migration model. Spain could also admit more persons from West Africa with permanent alien resident status. Those Africans admitted would be free to
work throughout Spain. Nothing would constrain these workers to become EU citizens but it would be a possibility. Such legally admitted permanent resident aliens would be free to travel back and forth to their homelands. But many certainly would opt for naturalization.
Herein lies the major advantage of increased admission of permanent resident aliens. Spain and Spaniards would have to accept the likely reality of settlement, giving Spanish society and government a strong incentive to foster immigrant integration. Historically, supposedly temporary foreign worker policies have resulted in significant settlement. But states and societies were unprepared for such unexpected outcomes leading to integration deficits and long-term integration issues.
Preliminary analysis of Spain’s temporary foreign worker admissions, the so-called contingents, suggests that the historic pattern of unexpected policy outcomes will continue. Several contingents served as ways to legalize aliens in irregular status rather than to recruit foreign workers from abroad. Perceived unfairness in the administration of the contingents has roiled Spain’s relations with Morocco and several other homelands whose governments feel that more of their citizens should be legally admitted under bilateral agreements. Spanish unions and employers often disagree on how large the authorized contingent should be, reminiscent of the annual “headaches” that Swiss cantonal and federal officials spoke of in the 1970s and 1980s.
Further enlargement or deepening of the EU and of other regional integration frameworks worldwide also merits consideration. Canada, the United States, and Mexico could emulate the history of regional integration in Europe. The key problem lies in the dissimilarity between the North American Free Trade Agreement (NAFTA) and the EU. NAFTA does not have a political project, unlike the European Community (EC) and now the EU. The Security and Prosperity Partnership (SPP)17 agreement announced by the three NAFTA heads of state in 2005 may suggest a move in that direction.
However, within each region and globally one can readily discern a need for greater cooperation between more developed and lesser developed states to promote greater socioeconomic development. The history of European structural funds designed to promote a more even playing ground within the European space deserves careful scrutiny by the NAFTA partners.
Unfortunately, most OECD member states have ducked negotiations over international migration and development issues. The pattern was set at the 1986 OECD-sponsored conference on the future of international migration. The U.S. delegation was instructed to avoid anything resembling North/South dialogue at
that conference. The Reagan Administration adamantly opposed Willy Brandt-style North/South Dialogue.18
The U.S. position appears to have evolved little ever since. It would take inspired American leadership for the decades-long migration and development stalemate to change. American leaders of either party simply continue to endorse the benefits of globalization and free trade as evidence mounts that it increases socioeconomic disparities, both within and between states and societies. The circular migration advocacy risks generating false hopes that bilateral and regional cooperation on international migration will result.
A new approach to migration and development would serve U.S. interests. The chief threats to U.S. security since the 1970s arose from failed states and the abysmal living conditions of average people in much of the world (Cooper, 2003). After 9/11, a window of opportunity opened but it has been largely squandered. Nevertheless, successful prosecution of the War on Terrorism requires progress on sustainable development in Africa, the Middle East, and elsewhere within what Thomas Barnett (2004) calls the “non-integrated gap area.” The important question revolves around the credibility of options proposed to bring about development. The track records of structural funds in contexts of regional integration and of increased admissions of permanent resident aliens appear preferable to the circular migration model.
PEOPLE, BORDERS, AND DISEASE—HEALTH DISPARITIES IN A MOBILE WORLD19
Brian D. Gushulak, M.D.20
Migration Health Consultants, Inc.
Douglas W. MacPherson, M.D., M.Sc. (CTM), F.R.C.P.C.21
Migration Health Consultants, Inc.
Introduction
The relationships between migration and introduced diseases of epidemic proportions are a recurrent story in human history (Morens et al., 2008). Epi-
demic events and other scourges of mankind have always traveled along the lines of human population mobility. In this paper, the term population mobility will be used when human “migration” extends beyond traditional patterns of the regulated processes of immigration and emigration.22 This is based on the concept that modern aspects of population mobility between disparate health environments can be more important in the context of health and globalization than the administrative or legal status of the person moving or the geopolitical boundaries that may be crossed.
Disease has frequently followed those pulled to new destinations by opportunity, better conditions, or simple inquisitiveness; or pushed from their homes by events, calamity, or chaos. The ebbs and flows of populations have often involved a connection between different environmental, socioeconomic, genetic, biological, or behavioral conditions that existed between the migrant and host populations (Ampel, 1991). The dynamic interaction of the populations and the determinants of health influenced and changed those who were migrating as well as the populations hosting the migrants.
Experiences involving disease and migration have been woven into human-kind’s social, cultural, and medical history. Remotely, epidemics of plague, cholera, leprosy, and syphilis, and more recently, HIV/AIDS, viral hemorrhagic fevers, severe acute respiratory syndrome (SARS), and swine influenza H1N1 have defined policy responses to protecting regional interests in economics, trade, security, and health (IOM, 1992). Detailed historical and scientific discourses regarding the origin of disease and its introduction into previously unaffected parts of the world have continued for centuries (Harper et al., 2008). Several of the public health and infectious disease challenges facing today’s increasingly integrated and globalizing world have similarities in context to situations involving migration, illness, and disease that have occurred in the past.
Traditionally, the implications and consequences of the relationships between disease, migration, and population mobility are described in terms of individual diseases, time periods, or events. This paper will approach migration and disease control frameworks through a process-related lens that includes several parameters associated with population mobility. Those parameters include population dynamics, differentials in disease or health indicator prevalence, the phases of migration (pre-departure, transit, post-arrival including return travel), and perceived and real risks to the health of the migrant and host populations.
Local, regional, and more recently international disease control strategies have been developed over time in response to the long-felt, but perhaps underappreciated, relationships between human mobility and disease (MacPherson and Gushulak, 2001; Welshman and Bashford, 2006). Frequently, existing immigration health control and mitigation practices reflect integral components from the
history of public health. In doing so, they often mirror the perceived nature of the health risk and science of the era in which they were developed. In terms of migration and imported infections, those approaches were commonly based on diseases of topical interest at the time and the sociological, legal, or administrative characteristics (seafarers, crusaders, military personal, humanitarian workers, immigrants, refugees, asylum seekers, migrant workers, smuggled and trafficked persons) of new arrivals.
Examining the evolution of programs to mitigate international disease importation reveals a pattern of reactive public health policies intended to mitigate risks. Over time, changes in transportation technology, migration patterns, and advances in medical science have also changed the nature and perception of risk. Changing perceptions of threat and risk have themselves been associated with corresponding changes in the disease control endeavors (Gill et al., 2001).
Older methods of disease control and mitigation were progressively superseded by approaches designed on the basis of improved capacity or better understanding of the nature of the risks themselves. For example, the nineteenth-century international consultations that were convened in Paris to deal with controlling the spread of cholera (Goodman, 1952), and which began a process that continues to this day through the revision of the International Health Regulations,23 preceded the germ theory of disease and subsequently evolved with the science of microbiology. This global evolutionary process of change, challenge, and response continues. The interfaces of migration, human mobility, and disease control remain an important aspect of national, regional, and global public health activity.
By its very nature, reactive policy development and implementation will always be tested by new or unanticipated events and processes. When those events occur against a background of low-speed travel and a limited degree of global integration there is often adequate time for policy development to meet a specific disease event. This pattern of specific or situational threat or risk and the response is the traditional model that underlies most migration-associated disease control strategies. The dynamic changes present in situations of high-volume, rapid, and increasingly diverse migration significantly challenge the traditional, situational, or disease-specific event and response paradigm. In this context of decreasing cycle times and prerequisite need for anticipatory planning, policies and practices often need to be more generic and broadly applicable to reflect the evolutionary changes in risk.24
To be effective, programs, practices, and policies must reflect the nature and dynamics of current challenges. Several of the factors that influence and affect migration, disease, and health have recently undergone significant change. In many circumstances those changes have not yet generated corresponding responses in migration health policy or program design. Given the importance and prominence of global infectious disease control in the context of human development, security, economics, and social integration, it is an appropriate and necessary time to consider the health implications of modern migration and population mobility (MacPherson et al., 2007). Examining the international spread of diseases of public health importance as a component of the process of human migration and population mobility can perhaps offer new elements in the approach to global health and disease control.
This paper reviews the history of migration and disease control policies in contrast with the modern health implications of human population mobility. It will also describe the impact that mobility has, and will continue to exert, in a rapidly globalizing world where trade, economics, security, and the environment all are interacting factors with health consequences. The focus of this discussion will be transmissible infectious diseases of global public health significance. The principles presented can equally be applied to any illness or condition associated with inter-regional differentials in prevalence that can be linked by mobile populations (Gushulak and MacPherson, 2006).
History of Migration and Disease Control Policies
There is an intimate relationship between human mobility, the introduction and spread of infectious diseases, and consequential attempts at control and mitigation of adverse health outcomes (Cunha, 2004; Gellert, 1993). Observations that plagues and epidemic diseases followed the arrival of traders, commercial ventures, travelers, pilgrims, colonists, soldiers, and other migrants have been noted for centuries (Cartwright, 1972; Curtin, 1989). For an equally long period of time, religious orders, cities, states, and nations have implemented disease control policies and practices in what would be recognized today as public health interventions triggered by population mobility and disease events.
Extensive and coordinated attempts were made to mitigate the impact of leprosy in medieval Europe (Miller and Smith-Savage, 2006). The disease is believed by some to have afflicted returning pilgrims and crusading soldiers from the Middle East, although there are suggestions that it was present in Europe before the Crusades (Browne, 1975). Whatever its origin, it was a major health concern of the time (Edmond, 2006). Leprosy control efforts were associated with the development of policies of inspection and isolation enforced by religious and municipal authorities. Facilities and institutions were constructed to house and deal with those believed to have the disease. Once in place, these facilities and practices could be easily applied to other similar situations.
By the fourteenth century, commerce and trade from the rapidly expanding renaissance city-states and nations had reached intercontinental levels not seen since the height of the Roman Empire. Those extensions to the east reached the Caspian Sea and western Asian areas at the same time as that region was experiencing an epidemic of plague (Herlihy, 1997). The outbreaks of plague in close association with the arrival of vessels carrying individuals who were ill or who became ill shortly after arrival were responsible for the development of organized health responses that became shared between many nations. Civic, municipal, and national policies and instructions were implemented to require vessels, goods, cargo, as well as passengers and crew to be denied port landing in an attempt to prevent disease introduction. Periods of detention sufficient to allow incubating disease to present with clinical illnesses were introduced and the process of quarantine was born. At the same time, municipal and civic health officers and staff were employed to deal with imported disease events.
Quarantine practices accompanied the Europeans during their subsequent colonization activities and were introduced in the Americas and other regions. While originally focused on specific infections of epidemic potential such as plague, cholera, and yellow fever, quarantine became the cornerstone of organized, coordinated attempts to deal with globalization and disease control.
The impacts on commerce associated with the global pandemic of cholera in the nineteenth century precipitated regional responses to regulate the movement of vessels, goods, and individuals in an attempt to reduce imported disease risk (Baldwin, 1999). It is historically notable that at this time international and intercontinental maritime traffic included a large human component of migrants destined from Europe to the opportunities of the “New World” as well as populations banished or transported for criminal or legal reasons, and trafficking in human slaves.
The principles of inspection, isolation, and denial of admission were applied to new arrivals at quarantine stations and ports of entry (Parascandola, 1998). The health policies and practices of traditional border inspection services were created to prevent the introduction of diseases arriving with immigrant populations. Initially organized around the seaports where most immigrants arrived, several immigration-receiving nations later moved the medical assessment of immigrants to the place of departure, further with the intended outcome of reducing the risk of arrival of unwanted diseases.
As major immigration nations began to regulate the process through legislation at the end of the nineteenth century, the medical inspection of newly arriving immigrants became required in nations such as the United States and Canada. The requirement for systematic medical inspection to detect both noninfectious and some infectious diseases resulted in the expansion of port-of-entry medical activities. Extensive inspection station facilities were constructed at large ports such as Ellis Island in New York (Yew, 1980), Angel Island in California (Lucaccini,
1996), and Grosse Ille in Canada25 (Montizambert, 1893). Medical inspection at these facilities provided opportunities to identify those with clinical illness. Depending on the situation and disease, individuals could be hospitalized, quarantined, or returned to their place of origin. Similar to modern border-associated processes, the true effectiveness of these activities was influenced by availability of accurate screening processes (Imperato and Imperato, 2008), the failure of inspection to detect those arriving with latent or subclinical illness, the logistical challenges of providing services at multiple ports of entry (Stern and Markel, 1999) and the application of screening based on the status, class of transport (i.e., steerage), or nationality of the arrival (Fairchild, 2004).
An example is provided by the approach to trachoma, a disease that could result in deportation if detected during immigration inspection in the early part of the twentieth century (Dwork, 1999). The denial of admission to those with disease detected on a brief clinical examination may have reduced the burden of disease in North America at the time. However, the ultimate control of trachoma required the development of antibiotic therapy and social and economic improvements that prevented its acquisition (Cook, 2008).
Approaches to infections of public health concern were also influenced by the sociological conditions present during the origin of immigration health policies and practices. Initial port health medical assessment and screening, for example, was often based on the class in which the passenger traveled, and was only required for steerage and third-class passengers. Weaknesses in those screening policies have been appreciated for some time, as noted in 1922:
The quarantine officers allow first cabin passengers and usually the second cabin passengers coming from abroad to enter with very little or no medical inspection, as if the possession of money to buy better accommodations were a guarantee against various infections. (Copeland, 1922)
The organized screening and health assessment of arriving immigrants and refugees thus undertaken by several nations continues in this basic form to this day (Australian Department of Immigration and Citizenship, 2008; CDC, 2008a; Citizenship and Immigration Canada, 2003; Immigration New Zealand, 2005). The general approach to immigration health remains focused on the screening of certain groups for certain diseases, predominantly transmissible infections. Diseases of great interest in the early twentieth century, such as trachoma and smallpox, are no longer public health issues of concern. Current listings and types of disease to which immigration screening is organized tend to reflect illnesses of public health importance of the mid- to late-twentieth century, such as tuberculosis, sexually transmitted diseases, and some tropical infections. While
no longer based on the class of passage, foreign nationals may remain subject to health requirements that are not applied to other travelers on the basis of visa or immigration status rather than travel heath-related risk.
The Demography and Nature of Modern Migration
Discussions regarding the demography of migration relevant to health are hampered by the lack of standard definitions concerning the populations of interest (Lemaitre, 2005). These definitional gaps challenge the development of appropriate and effective strategies to deal with the health consequences of migration.
Traditional administrative classifications of immigrants and emigrants in current use frequently do not adequately account for the diversity in the determinants of health and health outcomes of modern international migrants. At the level of individual countries, the issue is frequently complicated by differing approaches to the definition and use of nationality, citizenship, and residence. Depending on location, the same or different terms may be applied to several functionally different populations. For example, the terms immigrant, refugee, and migrant may variously be applied to new legal residents from foreign countries, as well as refugee claimants, asylum seekers, temporary foreign workers, illegal and irregular migrants, and international students. Traditional definitions based on administrative criteria may not include or consider other subpopulations of migrants whose health status is a direct result of their migration experience (The Hague Process on Migration and Refugees and UNESCO, 2008). Examples in this category include those who are trafficked or smuggled, children born to newly arrived migrants, those with dual or multiple citizenship, stateless individuals, and long-staying international visitors.
International attempts to standardize terminology related to migration frequently consider the intent of the individual to change their place of residence or the duration of their stay. Migrants, unlike visitors or travelers, can be considered people changing their usual place of residence to live, work, or study in another nation, either permanently or on a temporary basis. Some international definitions further refine this classification on the basis of time, using a 12-month period to separate migrants from other travelers or international visitors (UN, 1998).
Using those international definitions, it is estimated that there are approximately 200 million international migrants (International Organization for Migration, 2008) living outside of their normal country of residence. About 60 percent of these international migrants reside in the economically advanced regions of the world and 40 percent are found in developing regions. Much of the growth in international migration has taken place within the past decade. If these foreign-born persons were considered a separate national population, international migrants would represent the fifth largest nation in the world (Table 1-4). The magnitude of this migrant population reveals the current global demographic
TABLE 1-4 Population by Nation, 2008
|
Country |
Population (millions) |
|
China |
1,325 |
|
India |
1,149 |
|
United States of America |
305 |
|
Indonesia |
240 |
|
International Migrants |
200 |
|
Brazil |
195 |
|
Pakistan |
173 |
|
Nigeria |
148 |
|
Bangladesh |
147 |
|
Russia |
142 |
|
Japan |
128 |
|
SOURCE: Adapted with permission from Population Reference Bureau (2008a). |
|
significance of migration. The proportional contribution of the health and disease outcomes of this large mobile population cohort in terms of global health and disease management is also significant.
In addition to its magnitude-derived importance, modern migration is functionally a much different process than the historical patterns of immigration when most immigration-related disease control activities were developed. Recent demographic, social, and geopolitical forces have made the dynamics of international migration subject to a new series of influences. Together those influences have produced major changes in the processes and patterns of modern migration.
Migration is both an integral component and a consequence associated with globalization. International migration is affected and influenced by global population pressures. In spite of slowing rates of growth, total human population is predicted to continue to increase until it exceeds 10 billion individuals (Figure 1-1). These current global population dynamics will influence international population mobility in two ways (Hillebrand, 2007). First, the increasing size of the global population will continue to sustain present volumes and provide a growing pool of current and future migrants. Concurrently, the differential population demographics present between several economically advanced and developing nations related to aging populations and evolving birth rates will affect the need and demand for immigration in low-population-growth nations.
Changes in regional population density and growth rates affect and will continue to influence migration and population mobility (Table 1-5). Patterns of immigration and population flows reflect diverse and emerging demographic, economic, and social pressures, many of which differ from historical immigration trends (World Bank, 2008). The health and disease challenges associated with
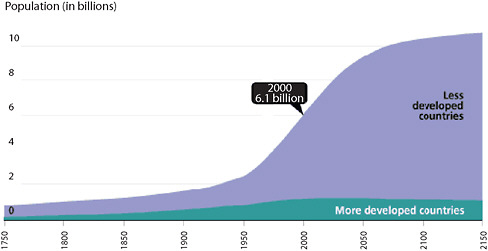
FIGURE 1-1 World population growth, 1750-2150.
SOURCE: Reprinted with permission from Population Reference Bureau (2008b).
TABLE 1-5 Country and Region Population with Rate of Growth
|
Current Top 10 Countries by Population Size |
1950 Population, in thousands |
2002 Population, in thousands (percent growth per year) |
2025 Projected Population, in thousands (percent growth per year) |
||
|
China |
554,760 |
1,294,377 |
(2.56) |
1,470,787 |
(0.59) |
|
India |
357,561 |
1,041,144 |
(3.68) |
1,351,801 |
(1.3) |
|
United States of America |
157,813 |
288,530 |
(1.59) |
346,822 |
(0.88) |
|
Russia |
102,702 |
143,752 |
(0.77) |
125,687 |
(–0.55) |
|
Japan |
83,625 |
127,538 |
(1.01) |
123,798 |
(–0.13) |
|
Indonesia |
79,538 |
217,534 |
(3.34) |
272,911 |
(1.1) |
|
Brazil |
53,975 |
174,706 |
(4.3) |
218,980 |
(1.1) |
|
Bangladesh |
41,783 |
143,364 |
(4.68) |
210,823 |
(2.05) |
|
Pakistan |
39,659 |
148,721 |
(5.3) |
250,981 |
(2.99) |
|
Nigeria |
29,790 |
120,047 |
(5.8) |
202,957 |
(3) |
|
Selected Regions |
|||||
|
Asia (excl. Middle East) |
1,331,636 |
3,493,424 |
(3.12) |
4,345,549 |
(1.06) |
|
Europe |
548,206 |
725,124 |
(0.62) |
683,532 |
(–0.25) |
|
Sub-Saharan Africa |
176,775 |
683,782 |
(5.52) |
1,157,847 |
(3.01) |
|
North America |
171,365 |
319,925 |
(1.67) |
383,678 |
(0.87) |
|
South America |
112,995 |
355,695 |
(4.13) |
460,770 |
(1.28) |
|
Oceania |
12,607 |
31,281 |
(2.85) |
40,020 |
(1.21) |
|
World |
2,519,495 |
6,211,082 |
(2.82) |
7,936,741 |
(1.21) |
|
SOURCE: Based on data from World Resources Institute (2009). |
|||||
these modern movements are reflective of several elements that have developed since traditional immigration health policies were conceived.
In addition to the forces of global population growth, the past five to six decades have been associated with a series of important new factors that have made the current process of migration markedly different than the traditional immigration/emigration pattern that marked most of the previous 200 years (Table 1-6).
At the global level, one of the major political influences affecting historical migration flows has been the process of decolonialization. At the end of World War II, most of Africa, a considerable part of South and Southeast Asia, and much of the Caribbean were colonial components of other nations, primarily in Europe. In 1955, the United Nations had 76 member states; by 1965 that number had risen to 117, and by 1990 there were 159 member states (UN, 2009a). Currently, there are 192 member states (UN, 2009b). Residents of previous colonies could access or avail themselves of residence in the previous colonizing power depending on location, history, and factors related to independence, and post-colonial relations (Gibney and Hansen, 2005). Several resulting post-colonial population flows established connections that changed the nature of immigration, the influences of which continue to be observed (Reynolds, 2001).
Geopolitical influences on migration continued toward the end of the twentieth century, when the dissolution of the former Soviet Union and end of the Cold War produced major changes in migration. Population redistributions that followed the end of the USSR were extensive and extended beyond Europe (Bade, 2003). The rising of the “Iron Curtain” opened new migration and travel pathways that have allowed new routes of access for migrant flows through previously restricted areas.
Another significant factor influencing modern migration that has implications for the mitigation and management of health and disease risk has been the evolution of refugee and displaced persons movements. During the Cold War, many refugee movements had significant political overtones and intercontinental
TABLE 1-6 Major Influences in Migration Dynamics Since the 1950s
|
Influences on Modern Migration |
|
Differential regional population growth |
|
Decolonialization |
|
Availability, accessibility, and affordability of air travel |
|
Speed of travel |
|
Magnitude of international mobility |
|
Refugee and internally displaced persons producing situations—civil, political, and environmental |
|
End of the Soviet Union |
|
Evolution of international labor market demands |
|
SOURCE: Based on data in Gushulak and MacPherson (2006). |
refugee resettlement frequently involved European populations. The geopolitical differences that marked that period of history often made these movements permanent. That dynamic began to evolve in response to the conflicts in Southeast Asia and Central Asia in the 1970s. International activities to deal with the human consequences of conflict and disaster became more internationally coordinated and more often involved the temporary resettlement of large numbers of refugees (Suhrke and Klink, 1987). These movements and resettlement programs often involve the movement of populations between locations of disparate disease epidemiology compared to that of the settlement country. In some cases, for example with the humanitarian evacuation from Kosovo in 1999, the speed of the movement exceeds the capacity of traditional screening programs, necessitating the return to “on arrival holding” and medical screening (CDC, 1999).
Modern migration patterns for refugees are also being affected by geopolitical factors. The political and ideological limits on immigration associated with the “East-West” entente26 often prevented the return travel of refugees to their place of origin and hindered family reunification. Many of those restrictions are no longer relevant and travel is common by previous refugees and subsequent generations of offspring to their country of ancestral origins.
International labor migration has also changed considerably during the past four decades. Globalization and the concept of human capital as a component of an international workforce have produced extensive effects on migration dynamics (ILO, 2009). The rapid growth and contraction of economic sectors produces large flows of migrant labor and populations of temporary workers. Many of these events have occurred in locations that until recently have not been nations of immigration, such as the Middle East or East Asia. Economic opportunity also acts as a “pull” factor for disadvantaged persons seeking employment or improved living conditions. Often these are unregulated or unofficial migrant populations that can be large enough to affect national demographic indicators as seen with population flows into the United States from Mexico and Central America and into Southern Europe from Africa and Asia. Some of the greatest growth in labor demand now occurs in economically emerging nations in Asia (Zlotnik, 2003). Gender aspects of labor migration have also changed in the recent past. Modern labor migration frequently involves migrant women moving internationally or within nations from rural to urban settings.
Finally, another factor in modern migration relevant to disease control activities has been the evolution of international travel. Until the 1950s, intercontinental migration was accomplished primarily by ship. The introduction of commercial jet aircraft in 1958 triggered an abrupt shift in mode of travel (IATA, 2009). Journeys that previously required days of ocean travel could now be made in a few hours (New York Times, 1960). At the same time,
increased aircraft size and efficiency reduced costs and increased access for air travel. Current international and intercontinental movement statistics describe unprecedented levels of human travel. International transportation authorities estimate that 831 million passengers flew internationally and 1.249 billion flew within their own country of residence in 2007 (IATA, 2007). The World Tourism Organization estimated 924 million international tourist arrivals (UNWTO, 2009) in 2008. This explosive growth in air travel over the past five decades and the reduced travel time associated with this growth in volume have greatly compromised the ability of existing policies and practices based on screening and quarantine to control the international spread of infectious diseases (Bitar et al., 2009).
How Modern Migration Will Functionally Impact on Global Health in the Future
Activities to mitigate the risks of infectious diseases of public health significance resulting from international migration reflect the characteristics of the migratory process at the time they were developed. Basic components of historical migratory population flows were structured on a traditional linear and primarily unidirectional format based on the great migration patterns of the nineteenth and early twentieth centuries (Figure 1-2).
The characteristics of this historical immigration/emigration pattern of migration included limited or restricted migrant source regions. Most of the current immigration medical activities were developed at the time when population flows originated in Europe and some parts of Asia and ended in Europe, European colonies, or the Americas. The travel undertaken by immigrants was long and often arduous but it tended to be as direct as possible. New migrants were greeted
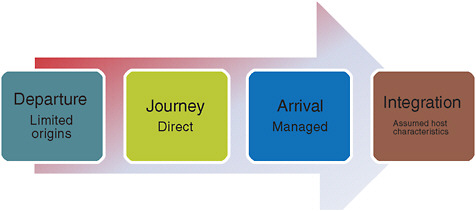
FIGURE 1-2 Traditional pattern of migration.
SOURCE: Based on data in Gushulak and MacPherson (2004).
on arrival by an organized system of registration, evaluation, and an assessment that frequently included a medical evaluation. While social and cultural differences present on arrival reflected the migrants’ origin, it was often assumed or anticipated that the new arrivals would integrate into the host population and over time would come to reflect the characteristics and determinants of their new home. Return travel to the migrant’s place of origin was uncommon either because the cost of such journeys was frequently beyond the economic capacity of the new immigrants, or because political and legal consequences for those who left as refugees prevented it.
In this immigration/emigration paradigm of population mobility, legal and administrative processes and border frontiers played an integral role in the approach to disease control. Following the long-standing approach to quarantine and sea travel, interventions were instigated on the basis of reports of illness or death during travel or the detection of illness or disease on arrival. The duration of the migrants’ journey and the time required to unload the vessels and process immigrants was considered to be sufficient to allow for the presentation of significant infectious diseases, which de facto represented a differential prevalence risk to public health of the recipient population, to a degree where they could be detected through clinical screening.
Additional carryovers from traditional port-of-entry quarantine included directing inspection and control activities to specific populations based on social or administrative classifications of the migrant. Returning residents, citizens, or passengers traveling in upper-class situations were often exempt from medical evaluation, even if they embarked on the same conveyance and at the same location as the prospective immigrants.
Modern migration, and in particular migration patterns that have developed during the past 50 years, displays a different pattern than that of the historical precedents (Figure 1-3).
Migration in today’s globalizing world can be conceptualized as a continuum of related and linked components of pre-departure, transit, and arrival phases including repeated return or onward travel. Each one of these mobility phases is associated with factors that have consequences for health and disease in both migrant and host populations through which the migrant has lived or transited. Traditional disease control processes and policies based on the historical patterns of migration are not robust enough to address the harm or benefit of the modern aspects of continuous and circular migration. The historical bases for these processes are being invalidated by modern circumstances of repetitive, rapid, and high-volume travel between origin and destination locations; varying disparities in the determinants of health between source, transit, and host destinations; and the greater international mobility of migration populations in general. This increased mobility can be observed through the migration continuum and makes the travel patterns and histories of many modern populations of migrants different than those of earlier immigrants and refugees.
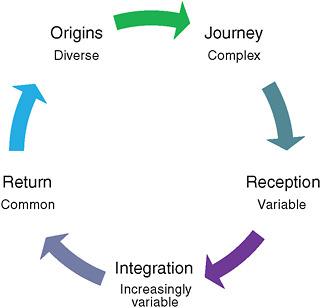
FIGURE 1-3 Modern patterns of migration.
SOURCE: Based on data in Gushulak and MacPherson (2004).
Different subpopulations of migrants, each with different determinants of health characteristics, are represented as special populations in the numerator of the total migrant populations in the denominator. Examples of special populations include asylum seekers, illegal or irregular migrants, and those with dual or multiple citizenships. The majority of these population-based characteristics were not considered when historical immigration health practices were implemented. Health interventions and disease control practices often remained based in concept and practice on administrative or traditional definitions of immigrants and emigrants and historical linear patterns of movement.
How Modern Migration Processes Challenge Border Disease Control Policies
The evolution and characteristics of modern migration dynamics present three sets of challenges in the context of modern border disease control activities. The first set of challenges results from the growth in the volume of migration from increasingly diverse migrant populations, origins, and destinations. This growth has occurred against the background of sustained and in some cases increasing disparity in the health indicators, and disease incidence and prevalence levels between source and recipient regions.
In recent decades, developments in international trade and travel have been implicated in the rapid redistribution of arthropod-borne vectors or the diseases
they transmit. Examples include extension of the yellow fever vectors in the eighteenth and nineteenth centuries; Anopheline mosquito malaria vectors in the 1930s (Soper and Wilson, 1943); Aedes albopictus and dengue (Halstead, 2007); the extension of West Nile virus infection into North America (Hayes and Gubler, 2006); and the spread of chikungunya infections in Europe (Simon et al., 2008).
The distribution of known and as yet unrecognized diseases of public health importance remains markedly variable between geographical locations, communities, and populations (Waldvogel, 2004). Some of the epidemiological gradients result from a small number of easily predicable and appreciated factors such as the distribution of vector-borne infections transmitted by geographically defined vectors. Many of the epidemiological disparities observed in other disease distributions are the product of complex relationships of many factors. The major determinants of health (socioeconomic status, genetics and biology, behavioral issues, and the environment) variably affect individual and population-based health status within and between regions and locations. These influences are themselves subject to other global events such as climate change and economic ups and downturns. International migration, by providing a population-based link that bridges those differential zones of health and disease prevalence, affects both inter-regional disease epidemiology and policies (Mackenbach, 2009). Existing policies and programs that owe their basis to the historical premises that migrants or refugees represent homogeneous cohorts will be unable to adequately mitigate the impacts of modern diverse risk profiles.
As an illustration, consider the example of two refugees, one a university lecturer from a metropolitan area, the other a displaced agricultural worker residing in a rural refugee camp, who are both admitted to the same resettlement country. Administratively, both are refugees and present situations where traditional immigration health interventions for “refugees” would be applied in a similar manner. If considered in the context of mobile population health risk assessment, the response and interventions might be different. Policies and programs designed during a time of much simpler immigration formalities may no longer be appropriate for current or future global health needs. Triggers for health interventions or evaluations based on administrative classifications of migrants and other mobile populations will not provide sufficiently robust response mechanisms to deal with the modern diversity and disparity of those populations.
The second challenge to traditional immigration health activities is a product of the technical and social evolution of the transportation industry. The epidemiological and infectious disease consequences of changes in transportation commerce are not limited to human migration but include goods and conveyances as means of moving infectious agents, diseases, and vectors (Tatem et al., 2006). The introduction of commercial jet aircraft saw the speed and volume of international travel increase as access to and affordability of air travel expanded. By the early 1960s, travel by jet aircraft rapidly became the major mode of long-
distance travel, allowing individuals both a reduction in travel times and easier access to previously isolated locations. Although the public health implications of this revolution in travel were appreciated at the time, the full consequences of the impact of shorter travel times on the procedures and protocols in place to manage the international spread of communicable diseases did not receive great attention until the 1990s. Then, during the initial phases of the revisions to the International Health Regulations in light of the expanding knowledge about emerging and reemerging infectious diseases, the role of the border and frontier in disease control began to be reconsidered. The technical and operational challenges posed by the arrival of international travelers who could now undertake an intercontinental journey within the incubation period of infections posing international public health significance became topics of interest at the international health policy table.
The evolution of air travel also greatly expanded the number of points of international access and ports of entry for migrants and other international travelers. In 1960, for example, nearly half of all air passengers subject to U.S. quarantine inspection arrived at a single airport, Idlewild (now known as JFK Airport) in New York (McKinnon and Remund Smith, 1962). Currently there are more than 100 airports in the United States through which international arrivals can enter the country (DHS, 2003). In 2007, 831 million passengers flew internationally (IATA, 2007) and JFK Airport alone dealt with 21.5 million international passengers (Airports Council International, 2009). Individually assessing the health status of international arrivals without significantly compromising transportation, given the volumes and scope of modern international travel, are functionally and logistically huge challenges.
In the past, a relatively small number of international entry points in any region serviced the majority of new arrivals. These were usually seaports or controlled land crossings. Traditional immigration health practices were concentrated at these limited numbers of ports of entry. Extensive experience in managing the health issues of migrants was acquired by people engaged in those activities. Frequently, ancillary expertise and scientific and diagnostic capacities also became located near major seaports, as reflected in the distribution of institutes of tropical medicine, many of which developed from mariners’ hospitals or care institutions.
Quarantine and immigration health practices that were based on the individual examination of new arrivals were developed to deal with the great waves of immigration in the last century. They also included facilities for the routine holding and isolation of those suspected to pose an adverse public health risk, allowing for evaluation over time. Modern patterns of migration and travel have made many of these processes and practices impractical. As the time required to complete international air travel has decreased, it is now possible to embark, complete an international journey, and clear immigration or customs formalities within the incubation period of most infections of public health importance. The
risks of spreading previously isolated infections through air travel were anticipated and predicted as air transportation technology evolved. Disease control programs to deal with the new threats continued to be focused on international airports as isolated ports of entry. This perpetuated the premise of the national frontier as a structure to prevent disease entry (Findlay, 1946).
When immigration involves travel by ship, the time for presentation and identification of imported disease acquired during the journey has been progressively reduced as the time required to complete travel has decreased. This effect has been elegantly described in studies of measles imported to Fiji (Cliff and Haggett, 2004). The introduction of more rapid steam-driven ocean travel reduced the exposure and infection of susceptible passengers. Disease that historically had run its course prior to arrival became a post-arrival risk (Figure 1-4). This inverse relationship between the incubation period for infections and the time required to complete international travel has a direct impact on the relevance of the border as a limiting factor in disease importation. Further implications were recognized soon after the introduction of intercontinental commercial air travel. For example, this comment on irregular migration in 1949 noted the relationship between high-speed travel and incubation periods: “In view of the fact that the farthest point in the world is now within the incubation period of the major infectious diseases, illegal entry into this country by air creates a grave risk to the public health” (Gartside, 1949).
The relationships between transit time, incubation periods, and disease occurrence described in Figure 1-4 also highlight principles of international disease control. While the speed of travel allows for journeys to be completed within the incubation period of many infections, it also acts to reduce the likelihood of infection acquired during travel. Depending on factors such as transmissibility, virulence, and inoculum size, when passengers do travel while in the communicable period of an infection, the speed of modern air transportation reduces exposure time and the chance of disease acquisition by other travelers during the journey. Together these factors diminish the likelihood that new arrivals will present with clinical disease that was either acquired or developed during the journey.
The challenges posed by travel, migration, and population mobility in the context of global infectious diseases of public health significance are regularly being recognized. Several operational difficulties involved in border health interventions were apparent during the SARS-related events of 2003 (Svoboda et al., 2004). Other operational challenges are noted in contingency planning in the event of a pandemic influenza event or similar disease emergency of enhanced global public health interest (Brahmbhatt, 2005; Epstein et al., 2007; UK Department of Health, 2007; WHO, 2006). As during plague and cholera in the remote past, the Spanish flu in 1918-1920, and SARS in 2003, the implications and consequences of modern population mobility and the limitations of border containment and mitigation strategies to prevent disease importation were again both apparent and noted during the international responses to a novel influenza H1N1
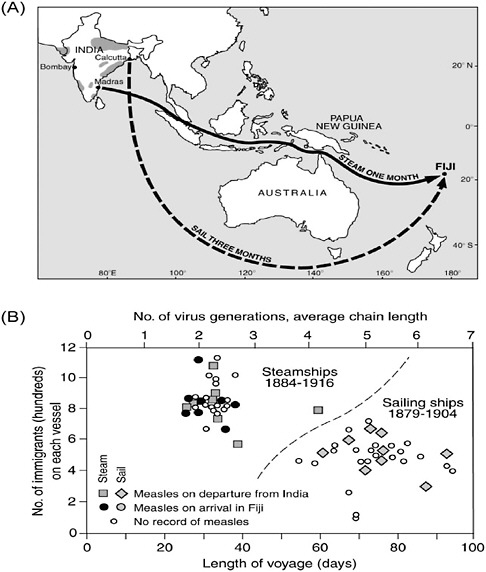
FIGURE 1-4 Measles outbreaks associated with two modes of international travel.
SOURCE: Reprinted from Cliff and Haggett (2004) with permission from Oxford University Press.
infection detected in North America in March to April of 2009 (Barry, 2009; Khan et al., 2009; WHO, 2009a).
Border-associated technological solutions designed to reduce the introduction of important infections during urgent public health situations have been considered. Some border screening solutions were introduced as components of
the international SARS control response but analysis of these solutions has not been favorable (Samaan et al., 2004; St. John et al., 2005). In spite of recommendations to the contrary by the World Health Organization (WHO, 2009b), border containment strategies were applied by some nations during the initial phases of the 2009 influenza H1N1 pandemic (SOS International, 2009). At the time of this publication, the cost, impact, and potential effectiveness, or lack thereof, related to these interventions have not been evaluated.
The third aspect of modern migration that exceeds the intent and capacity of traditional immigration and border health policies results from changes in migration patterns themselves. The evolution of migration from a linear, unidirectional pattern to a more continuous and circular pattern of modern population mobility has not been accompanied by policy or programmatic design to accommodate these and future changes. Current social and economic factors facilitate and support the increasingly frequent and recurrent travel by resettled migrants between their new home and other locations, including their place of reference. Their place of reference may be their country of birth, political or faith-based affiliation, education, ancestral migration, spousal or offspring association, or future opportunity. This modern type of travel involves the migrants themselves and other members of their families, including children born to new immigrants after their arrival. The latter movements are known as travel to visit friends or relatives (“VFR travel”); although originally used as an economic measure of travel, trade, and the foreign-born diaspora, it is an area of increasing interest in the travel medicine and global public health sectors (Angell and Cetron, 2005; Leder et al., 2006). The importance of VFR travelers and similar risk-profiled travelers in the context of disease control and mitigation policies and practices for all migrants are the gaps between defining the intent of travel and evaluation of the risk assessment and outcome profiles (Behrens et al., 2007). The completion of administrative and legal immigration formalities brings to an end most immigration health requirements. Some individuals who change their status after arrival or who were noted on immigration screening to have medical concerns may be required to undergo further medical follow-up, but the majority of these cases cease to be subjected to immigration health attention.
Under usual circumstances of post-landing, arriving populations become part of the host population in terms of public health consideration. There is increasing concern that the travel and mobility characteristics of some migrant cohorts differ from those of other components of the domestic population. Interventions and risk mitigation efforts directed at reducing some travel-associated disease risks may be more important in “VFR-like” and other migrant travel situations, but national public health program and policy aspects may not reflect these needs. As populations of recent migrant origin travel more frequently, they may represent mobile populations at differential risks of disease.
Other aspects of the circular and recurrent patterns of migration extend beyond the traditional aspects of migration health. The globalization of com-
merce, communication, and the immediacy of interconnectiveness that is supported and enhanced by current technology and transportation facilitate the social and cultural continuation of practices, beliefs, and activities. Many of these bridge disparities in health-related events between migrant origin and destination locations. Most of the health implications of these linkages are related to epidemiological differences and disparities between the locations. Relevant disparities in this context go beyond the personal determinants of health and include the control and regulation of food, nutritional, pharmaceutical, and medical products, practices, and activities, in addition to other broader societal, environmental, and behavioral factors.
Modern technology and transportation allow many migrants access to goods and services available outside of their new place of residence. Increasing ease of access provides linkages between divergent systems of international regulation, surveillance, and control standards that vary between locations. Some migrant communities represent markets for the continued importation of traditional foods, pharmaceutical products, and traditional medical practices. Some of these can be associated with the international introduction of infectious diseases or other risks. The international trade in noninspected or nonregulated foodstuffs and traditional therapies is extensive. The acquisition and preparation of bushmeat, for example, may be associated with the exposure to and potential emergence of zoonotic infections (Wolfe et al., 2005). While consumption of the product represents less risk, the importation of bushmeat may also be associated with the importation of human and animal infections. It is estimated that as much as 15,000 pounds of bushmeat may be imported into the United States monthly (Barry, 2007).
Migrants, their families, and other mobile populations may also return to familiar locations to receive medical care and treatment. When those services are provided in locations where infection control, pharmaceutical standards (Primo-Carpenter and McGinnis, 2009), inspections, antibiotic management, and medical and surgical treatment practices may not be regulated or under stringent standards (Yankus, 2006), the risk of acquisition of unusual or resistant infections and subsequent introduction into their new place of residence is present.
Modern Migration and Global Infectious Disease Surveillance and Control
Attempts to mitigate the impact of migration on the international epidemiology of infectious diseases can be considered in the classic relationships between the host, organism, and environment. Each can pose specific challenges for source, transit, and recipient countries when health outcome determinants have components that arise beyond the national borders where direct control might be exerted.
Pre-departure medical examination and assessment of some classes of immigrants, refugees, or certain cohorts of visitors from designated countries is practiced by nations with long-standing immigration programs, such as
Australia, Canada, New Zealand, the United Kingdom, and the United States. Other nations may require the routine examination of some migrant or refugee groups after arrival. Depending on the nation and situation, the medical evaluation of migrants may be voluntary. The health assessment approach for non-traditional migrants such as asylum seekers, long-staying visitors, temporary workers, international students, and illegal or irregular migrants is even less well defined or practiced. The result is an international collection of diverse processes, many of which are rooted in old paradigms and protocols of traditional immigration health.
The historical focus of international regulations and disease control has been on a list of specific conditions or microorganisms. This belies the complexity of the nature of transmissible infectious diseases that must include consideration of multiple microbial organism factors, such as incubation period, patency, latency, chronic infection and infectious states, transmissibility, virulence, and infectious and noninfectious sequelae. The characteristics of microbial contagiousness and virulence for human beings, and the availability of effective diagnostic, therapeutic, and specific preventative interventions, such as antibiotics or vaccines, have been more recent considerations in the international disease control approach. System characteristics, such as clinical and public health services for surveillance, detection, confirmation, notification, and the requirement for timely and effective international response further complicate shifting the paradigm from its origin in simple screening of disease for the purpose of preventing the admission of disease.
Medical screening for disease exclusion, supported by national legislation and regulations, on the basis of danger to public health (Gushulak and MacPherson, 2000) is being supplanted in importance and investments by global infectious disease surveillance and emergency preparedness. Interest in infectious disease threats and risks due to potential events such as avian influenza adapting to human hosts, or a globally significant pandemic influenza, have been augmented by concerns regarding new threats. Modern preparedness strategies now include considerations related to novel virulent pathogens occurring in nature or organisms that are malfeasant in design and unleashed on a susceptible population. Most of this interest originates in low prevalence, but threat and risk intolerant countries.
Against a background of endemic outbreaks of largely enteric or respiratory transmitted diseases in economically advanced countries is the risk of imported diseases. Outbreaks of enteric diseases presenting with acute illness, such as salmonellosis or botulism, largely occur due to contaminated food or food products (CDC, 2009a; Sheth et al., 2008; Wachtel et al., 2003). Hepatitis A outbreaks in low-prevalence regions brought in by nonimmune migrants with secondary spread have also been described (Heywood et al., 2007).
Short-incubation respiratory infections that manifest with typical clinical symptoms have grasped international public health attention in the post-SARS and avian-to-human influenza period of the last decade. Equally, the fear of a
pandemic influenza event has generated global surveillance and emergency preparedness investments of an unprecedented magnitude (Gottschalk et al., 2009). Beginning in April 2009, pandemic influenza preparedness planning was tested in response to what had become, by June, the 2009 H1N1 influenza pandemic (WHO, 2009c). Systems and procedures developed to deal with pandemic influenza were employed and utilized during the recognition phase of the disease and subsequent international surveillance activities as the infection spread locally across the planet (Trifonov et al., 2009). Modern diagnostic and information technologies were extensively utilized as part of or in parallel to these surveillance undertakings allowing for an almost “real-time” monitoring of a developing global infection (Brownstein et al., 2009). Information response resulted in pandemic contingency conceived and developed for more virulent infections and serious disease undergoing evolutionary modification (Miller et al., 2009). At the same time, in spite of the same information base, national responses and interventions at frontiers and borders continued to vary depending on national plans, requirements, and mitigation strategies. “Real-time” pressures within the existing regulatory frameworks precluded deliberate risk assessment discussions within health and between health and other international sectors.
Against this background, “normal” diseases of public health importance, such as vaccine-preventable respiratory viral infections like influenza, mumps (CDC, 2006), and measles (CDC, 2008b), are also regularly reported as imported events with secondary transmission in local populations.
Chronic infections, infections with prolonged latent periods, and infectious with noninfectious consequences are emerging as important phenomena related to migration and may offer unique opportunities for effective mitigation and control. In nations where long-standing public health activities and programs have been effectively implemented and supported, several infectious diseases of previous historical importance are now present in low or very low prevalence levels. Migrants and mobile populations arriving from less-advantaged locations where the prevalence of these infections remain elevated may represent population cohorts posing increased personal and public health risk of disease compared with elements of the domestic or host population (Barnett and Walker, 2008; Falzon and Aït-Belghiti, 2007; Palumbo et al., 2008; Stauffer et al., 2008).
In situations where domestic prevalence disease rates are very low, the sustained arrival of migrant populations from endemic regions will affect the epidemiology of the infection at the destination. Chronic enteric infections, including Taenia solium (Schantz et al., 1992), Strongyloides stercoralis (Boulware et al., 2007; Robson et al., 2009), and others may take decades to present clinically or only present through detection of secondary transmission (Hotez, 2008; Moore et al., 1995). The changing incidence and disease nature of tuberculosis infections in immigrant-receiving nations is another example of delayed presentations of diseases of public health significance due to chronic states and latency (CDC, 2009b). Similar observations have been made for several other chronic infec-
tions; hepatitis B (CDC, 2008d), Chagas disease (Milei et al., 2009), malaria (D’Ortenzio et al., 2008), and schistosomiasis (Salvana and King, 2008).
Existing immigration health-related disease control policies with the historical focus on specific infections of acute epidemic potential or acute transmission do not accommodate chronic diseases or the consequences of infectious diseases. In spite of the importance of all of these infections in terms of national and international public health, an accurate measure of the impact of chronic infectious diseases and their consequences can be hard to obtain. Examples include H. pylori-related gastric carcinoma (Ohno et al., 2009) and hepatoma resulting from chronic hepatitis infections (Gupta and Altice, 2009; Kim et al., 2008; Umemura et al., 2009) arriving with migrants. The nature of latent or chronic infections is such that the presentation frequently occurs long after the period of travel that brought the infected migrant to the new destination. As a result, the majority of those presenting with clinical disease are individuals who have completed citizenship formalities and, unless diseases are tracked by the patient’s place of birth, the relationship to travel and migration may be lost.
For all of these factors, disease surveillance and global public health intelligence alone (WHO, 2009d,e) have been and will continue to be inadequate to control the threat and risk of importation of diseases of public health importance. As advocated by international public health experts, greater inter-regional openness and collaboration are essential to achieve the goals of global emerging infectious disease prevention and control (NIC, 2008). These ideals require shared technical expertise, commonality in definitions, visionary policy approaches that encompass and embrace disparate environments, and an explicit recognition that diverse populations on the move are utilizing multiple processes during relocation that do not follow traditional concepts.
Shifting the Paradigm: Population Mobility Globalizes Health Disparity
The nature and context of modern migration is currently at the interface of several related determinants of health (socioeconomic, behavioral, genetic and biological, and environmental) and globalization (trade, technology, telecommunications, and travel). Our understanding of the inter-relatedness and dependency of these factors continues to develop since the policies and programs designed to mitigate disease risks in migrants were designed. The majority of those traditional, policy-driven practices have become compromised or operate at the limits of validity.
The Border Is Irrelevant as a Barrier to Disease
The speed of travel and the volume of human mobility have combined to render political frontiers of marginal use in the context of international disease control. Globalization has seen the trade and commercial sectors work toward
seamless borders and the greater facilitation of movement and the exchange of goods and services. However, many public health control policies remain nationally focused and sustain principles based on the political or administrative frontier as a disease-limiting tool (Kicman-Gawłowska, 2008).
The demise of the border as a filter for the admission of infectious diseases has in parallel led to a situation where mitigating the risks of imported infections has become shared across the health sector. The fact that imported or travel-associated disease events are now more likely to present away from the border generates new demands on national health services at the very local level. Clinical awareness, diagnostic capacity, treatment, and management capabilities to deal with imported infections are now needed universally. This has implications and consequences for health educators, providers, certification, and regulatory bodies involved in health services. This explicitly requires engagement of policy makers and contingency planners.
As national borders have become less effective limits to the international spread of infectious diseases, an effective public health response assumes greater international importance. Solutions and strategies to prevent and respond to the threats and risks of the spread of diseases between disparate environments must expand beyond national perspectives. Globalization of risks needs to be met with coordinated international responses and preparedness. Increasingly integrated, multipartnered programs and activities have been created to more efficiently deal with global infectious disease risks. Similar approaches are needed to address the current and future pressures of migration and international disease control. The challenge will require a paradigm-shifting reconsideration of the policies and programs based on the historical perception of the role of the political border as a barrier to disease. Critical and comprehensive analysis and evaluation of national and international responses to the 2009 H1N1 influenza pandemic will be essential if important shifts in approaches are to be achieved related to global health considerations and international population mobility.
Public Health Challenges Increasingly Arise Beyond the Jurisdiction of Local Control Authorities
Traditionally public health control activities responded to situations by addressing the current event while acting in a coordinated manner to prevent its recurrence or eliminating its source. Commonly, municipal, civic, and provincial or state programs evolved as part of broader national policies designed to ensure and maintain health standards and reduce levels of risk across the country. Since the mid-eighteenth century, international regulations for disease control were limited in scope to a defined list of specific infectious agents or diseases. The management and control was left to individual nations with the consequence that control activities would vary related to national levels of development, resources and capacities, and perception of risk.
Disparities in public health capacities are often indirectly proportional to corresponding disease prevalence patterns. The domestic transmission of several historically significant infections has been eliminated in many economically advanced nations. These infections remain at higher prevalence in other locations. Against this growing pattern of disparity in prevalence, globalization and population mobility are actually increasing the risk of international disease transmission (Elefsiniotis et al., 2009; Enserink, 2007; Hinman et al., 2004; Payne and Coulombier, 2009; Stark et al., 2008).
The result often requires that public health agencies invest more resources in the control of local events that are arising beyond the jurisdiction of domestic control authorities. The solution is an integrated response to the globalization of disease risk as standard components of domestic prevention, mitigation, and control strategies. The prudent investment in public health interventions at the source of the event for primary prevention, mitigation, or control may be more effective in terms of both resources and outcomes than secondary control attempts in other locations (Schwartzman et al., 2005). Cost-effective methods that exist for meeting these challenges will require a greater international policy commitment and diversion of program resources away from nationally focused activities toward integrated globally applied interventions.
Health Aspects of the Evolution of the Immigration/Emigration Paradigm
In order to more effectively address the modern nature and scope of global migration, historically based policies and program approaches based on traditional patterns of immigration need to be revised. The dynamics of the flow of individuals and populations across disparities in the determinants of health and outcome measurements are the source of all adverse public health outcomes related to the international spread of infections. Policies, processes, and programs intended to manage these events need to encompass an approach to risk that is wider than the current specific disease or administrative class of migrant models currently in use.
Considering mobility as a determinant of global health provides a model upon which integrated disease management policies, processes for prevention, knowledge of disparate prevalence environments, and a rigorous health threat to risk assessment ability can be designed and implemented. Policies and programs intended to mitigate the risks of disease importation through migration would be more logically based on current factors or future modeling more directly related to risk and undesired health outcomes rather than specific diseases or historical patterns of immigration. The need to increase the flexibility of traditional disease list-based control methodologies to more effectively meet modern approaches to threat-risk assessment is reflected in the 2005 revision of the International Health Regulations that created a greater expectation on national surveillance and international reporting. This approach to public health, of course, is not enough
without integrating within health and between other sectors of global society including health systems and services, occupational and labor health, security, economics and trade, agriculture and food management, and the environment.
A process of creating more effective tools with the capacity to meet as yet undefined or emerging threats has become a cornerstone of international public health preparedness and response. Extending the process into the sphere of migration health is strongly supported by empirical evidence, recurrent international experience, and projections of the importance of population growth and mobility for the future of global health.
New Approaches for Migration and Disease Control
It is apparent that human migration will continue to be an important component of global infectious disease distribution. Population migration, disparate health system environments, and gaps in disease prevalence will both continue and probably grow as components of international disease spread over the near and medium term. As migration expands, the need to plan and prepare to deal with the associated infectious and noninfectious disease consequences of population mobility will become interests of more nations and health authorities. Reflecting that growing interest, the health of migrants was the subject of recent EU discussions in Portugal and a resolution at the WHO World Health Assembly in 2008 (WHO, 2008). The convergence of the increasing need to address the issues and the expanding awareness of the importance of health related to global migration provide an opportunity to modernize and revise policies and programs that are no longer effective.
Those revisions will require and benefit from the following undertakings:
-
An integrated approach to migration health threat to risk assessment, analysis, and interpretation. Global health policies will need to reflect the dynamics, diversity, and disparities that are associated with the demography of modern migration and population mobility. Threat to risk assessment practices need to be more complex and inclusive of outcome determinants rather than being based on administrative migrant class or disease lists. This risk management approach to meeting the disease challenges of migration will better direct resources where benefit can be expected and have the potential to reduce unnecessary practices in low-risk situations. This meets the intent of the International Health Regulations while adhering to standard population and public health principles.
The United States has recently begun moves in this direction. Centers for Disease Control and Prevention (CDC) guidelines for the immigration medical examinations of foreign nationals have been amended to incorporate more flexible, risk-based approaches based on epidemiological and
-
other factors (CDC, 2008c). These changes provide increased capacity to immigration medical screening to be aligned with situations constituting a public health emergency of international concern that require notification to WHO according to the International Health Regulations.
-
Functional approach to borders and boundaries. The potential for international spread of infectious diseases in association with migration remains a component of a world that contains health disparities and is ever more linked through mobile populations. Political boundaries are increasingly less effective components of control programs and policies. Any new or modern approaches to migration health and infectious disease control will need to address that reality.
Migration and population mobility globalize risks that have in the past frequently remained isolated. As high-speed travel provides the opportunity for larger numbers of people to move between health disparities, the concept of the global village increasingly extends to the health care sector. While serious acute events of international public health significance are rare, sustained high levels of migration do affect the epidemiology of several infections in those nations transiting or receiving migrants. This has effects on the clinical awareness of health service providers and the need to consider rarely encountered diseases. It also expands the demands for diagnostic and management capacities that historically have been limited in distribution or location.
The globalization of risk resulting from the fading role of the national boundary will mean that the education and training of health care providers will need to focus more attention on the global aspects of migration health (Boulware et al., 2007). Health services and public health systems must support investigative capacities extending further into the health care delivery sector to support clinical services and international public health.
-
Modeling migration health on other coordinated international actions. Individual national programs, particularly when they are directed toward threats and risks that originate beyond their areas of jurisdiction, may have some role in dealing with the secondary effects of those risks. In terms of primary prevention, these approaches will be predictably ineffective. Coordinated international efforts are now essential in any attempt to control diseases of global public health significance. Local and national activities must continue but as components of integrated multilateral mitigation strategy. Migration health control activities could easily follow that pattern. National immigration and citizenship legislative and regulatory requirements make it unlikely that nations that require immigration health
-
interventions will reduce or eliminate those requirements. Those policies and programs could be easily integrated into global strategies supporting improved migration-associated disease control (Cattacin and Chimienti, 2007).
-
Immigration health screening, for example, when it is undertaken by those nations who require it for national legislative purposes, could be integrated into other global health activities. Currently, in excess of two million individuals undergo routine immigration medical evaluation annually for resettlement. While limited to specific infections and certain migrants, the information is presently used only for national immigration requirements. Supporting global tuberculosis activities is an obvious example; the majority of nations who utilize immigration health screening have elements of tuberculosis screening in their programs. The aggregate use of this and similar data could be used in conjunction with other global public health activities. Other potential activities include international collaborative longitudinal studies of migrant health outcomes. Such studies using standardized methodology and definitions could significantly improve knowledge regarding the outcome of chronic or latent infections in migrants.
Conclusions
Designed to prevent the introduction of a limited list of diseases of historical public health significance that arose beyond national boundaries, most immigration health activities play at best a minimal role in international disease control activities in the modern context. While required by some immigrant-receiving countries’ national legislation, they are often based on the historical quarantine-derived strategies of exclusion and isolation, principles that for the most part only represent population-based public health approaches in very limited circumstances. The world public health community remains challenged by a variety of disease threats, several of which are intimately associated with population mobility.
Recent awareness of the implications of local disease events for global health has prompted the revision and reconsideration of some of the basic historical principles behind organized disease control (Cetron and Simone, 2004). Some of the migration-related aspects of that revised regulatory methodology originate from the same historical approaches to disease control and are subject to many of the same weaknesses that prompted the revision of the International Health Regulations in 2005. Migration in its modern mobility-derived context plays an increasingly important role in the global epidemiology of infectious diseases and that role will continue as long as disease disparities exist and populations link high-prevalence to low-prevalence regions through mobility.
Considering population mobility as a determinant of global health has implications for the systems required for prevention, mitigation, and control of serious events of global public health significance. Addressing the health implications of population mobility will also assist global public health activities through the reduction of population-based health disparities in prevalence. Reducing those primary prevalence differences decreases the likelihood that movement of people between those environments will link the differences.
MILLER REFERENCES
Barnett, T. P. 2004. The Pentagon’s new map: war and peace in the twenty-first century. New York: G. P. Putnam’s Sons.
Castles, S., and M. J. Miller. 2009. The age of migration, 4th edition. New York: Guilford.
Cooper, R. 2003. The breaking of nations. New York: Grove Press.
Curtin, P. 1997. Africa and global patterns of migration. In Global history and migrations, edited by W. Gangwu. Boulder, CO: Westview.
Daniels, R. 2004. Guarding the golden door. New York: Hill and Wang.
Diamond, J. 1997. Guns, germs and steel, the fates of human societies. New York: W. W. Norton.
Hatton, T. J., and J. G. Williamson. 1998. The age of mass migration: causes and economic effects. Oxford and New York: Oxford University Press.
———. 2005. Global migration and the world economy. Boston: MIT Press.
Independent Commission on International Development Issues. 1983. Common crisis north-south cooperation for world recovery. Cambridge, MA: MIT Press.
Koslowski, R. 2000. Migrants and citizens. Ithaca, NY: Cornell University Press.
———. 2008. Global mobility and the quest for a global migration regime. In International migration and development: continuing the dialogue: legal and policy perspectives, edited by J. Chamie and L. Dall’Oglio. Geneva, Switzerland: International Organization for Migration.
McNeill, W. H. 1977. Plagues and people. Garden City, NY: Anchor Books.
Miller, M. J. 2008. Migration and development: past, present, and future. Prepared for International Organization for Migration/Center for Migration Studies, Conference on International Migration and Development: Continuing the Dialogue—Legal and Policy Perspectives, Millennium UN Plaza Hotel, New York City, January 17-18, http://www.udel.edu/poscir/faculty/MMiller/MigrationDevelopmentPastPresentFuture.htm (accessed October 19, 2009).
UNDESA (United Nations Department of Economic and Social Affairs). 2006. Trends in total migrant stock: the 2005 revision. New York: United Nations Department of Economic and Social Affairs.
UNWTO (United Nations World Tourism Organization). 2005. Tourism market trends. UNWTO.
———. 2006. Tourism market trends. UNWTO.
———. 2007. Tourism market trends. UNWTO.
Wells, P. S. 2001. Beyond Celts, Germans, and Scythians. London: Duckworth.
Zolberg, A. 2006. A nation by design: immigration policy in the fashioning of America. Cambridge, MA and New York: Harvard University Press and Russell Sage Foundation.
GUSHULAK AND MACPHERSON REFERENCES
Airports Council International. 2009. Statistics: top 30 world airports [by international passengers]. ACI Information Brief July 2008, http://www.aci.aero (accessed January 23, 2009).
Ampel, N. M. 1991. Plagues—what’s past is present: thoughts on the origin and history of new infectious diseases. Reviews of Infectious Diseases 13(4):658-665.
Angell, S. Y., and M. S. Cetron. 2005. Health disparities among travelers visiting friends and relatives abroad. Annals of Internal Medicine 142(1):67-72.
Australian Department of Immigration and Citizenship. 2008. Health Requirement for Permanent Entry to Australia, Form 1071i. Design date 01/08, http://www.immi.gov.au/allforms/pdf/1071i.pdf (accessed March 13, 2009).
Bade, K. J. 2003. Europe: a continent of immigration at the end of the twentieth century. In Migration in European history. Malden, MA: Wiley-Blackwell.
Baldwin, P. 1999. Contagion and the state in Europe, 1830-1930. Cambridge, UK: Cambridge University Press.
Barnett, E. D., and P. F. Walker. 2008. Role of immigrants and migrants in emerging infectious diseases. Medical Clinics of North America 92(6):1447-1458.
Barry, E. 2007 (November 17). A taste of baboon and monkey meat, and maybe of prison, too. New York Times.
Barry, J. M. 2009 (June 23). Pandemic reality check. What can be done—and what can’t be done to protect against H1N1. The Washington Post.
Behrens, R. H., C. H. Hatz, B. D. Gushulak, and D. W. MacPherson. 2007. Illness in travelers visiting friends and relatives: what can be concluded? Clinical Infectious Diseases 44(5):761-762.
Bitar, D., A. Goubar, and J. C. Desenclos. 2009. International travels and fever screening during epidemics: a literature review on the effectiveness and potential use of non-contact infrared thermometers. Eurosurveillance 14(6), http://www.eurosurveillance.org/images/dynamic/EE/V14N06/art19115.pdf (accessed February 15, 2009).
Boulware, D. R., W. M. Stauffer, B. R. Hendel-Paterson, J. L. Rocha, R. C. Seet, A. P. Summer, L. S. Nield, K. Supparatpinyo, R. Chaiwarith, and P. F. Walker. 2007. Maltreatment of Strongyloides infection: case series and worldwide physicians-in-training survey. American Journal of Medicine 120(6):545-551.
Brahmbhatt, M. 2005. Avian and human pandemic influenza—economic and social impacts. Speech at WHO Headquarters, Geneva, Switzerland, November 7-9.
Browne, S. G. 1975. Some aspects of the history of leprosy: the leprosie of yesterday. Proceedings of the Royal Society of Medicine 68(8):485-493.
Brownstein, J. S., C. C. Freifeld, and L. C. Madoff. 2009. Digital disease detection—harnessing the web for public health surveillance. New England Journal of Medicine 360(21):2153-2155, 2157.
Cartwright, F. F. 1972. Disease and history: the influence of disease in shaping the great events of history. New York: Thomas Y. Crowell.
Cattacin, S., and M. Chimienti. 2007. From control policies to health policies as a tool for inclusion. International Journal of Public Health 52(2):73-74.
CDC (Centers for Disease Control and Prevention). 1999. Health status of and intervention for U.S.-bound Kosovar refugees—Fort Dix, New Jersey, May-July 1999. Morbidity and Mortality Weekly Report 48(33):729-732.
———. 2006. Mumps outbreak at a summer camp—New York, 2005. Morbidity and Mortality Weekly Report 55(7):175-177.
———. 2008a. Technical instructions for panel physicians, http://www.cdc.gov/ncidod/dq/panel.htm (accessed February 20, 2009).
———. 2008b. Update: measles—United States, January-July 2008. Morbidity and Mortality Weekly Report 57(33):893-896.
———. 2008c. Addendum to the technical instructions for medical examination of aliens: updated screening for communicable diseases of public health significance, http://www.cdc.gov/ncidod/dq/pdf/ifr_100608/ti_addendum.pdf (accessed March 5, 2009).
———. 2008d. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. Morbidity and Mortality Weekly Report Recommendations and Reports 57(RR-8):1-20.
———. 2009a. Multistate outbreak of Salmonella infections associated with peanut butter and peanut butter-containing products—United States, 2008-2009. Morbidity and Mortality Weekly Report 58(4):85-90.
———. 2009b. Plan to combat extensively drug-resistant tuberculosis: recommendations of the Federal Tuberculosis Task Force. Morbidity and Mortality Weekly Report Recommendations and Reports 58(RR-3):1-43.
Cetron, M., and P. Simone. 2004. Battling 21st-century scourges with a 14th-century toolbox. Emerging Infectious Diseases 10(11):2053-2054.
Citizenship and Immigration Canada. 2003. Designated medical practitioners handbook, http://www.cic.gc.ca/english/pdf/pub/dmp-handbook.pdf (accessed January 14, 2009).
Cliff, A., and P. Haggett. 2004. Time, travel and infection. British Medical Bulletin 69:87-99.
Cook, J. A. 2008. Eliminating blinding trachoma. New England Journal of Medicine 358:1777-1779.
Copeland, R. S. 1922. Import diseases as they affect the work of the New York City Health Department. American Journal of Public Health 12(3):202-204.
Cunha, B. A. 2004. Historical aspects of infectious diseases, part I. Infectious Disease Clinics of North America 18(1):XI-XV.
Curtin, P. D. 1989. Death by migration: Europe’s encounter with the tropical world in the 19th century. Cambridge, UK: Cambridge University Press.
DHS (U.S. Department of Homeland Security). 2003. U.S.-visit implementation at air ports of entry, http://www.dhs.gov/xlibrary/assets/usvisit/US-VISIT_EA-Air-1003.pdf (accessed January 12, 2009).
D’Ortenzio, E., N. Godineau, A. Fontanet, S. Houze, O. Bouchaud, S. Matheron, and J. Le Bras. 2008. Prolonged Plasmodium falciparum infection in immigrants, Paris. Emerging Infectious Diseases 14(2):323-326.
Dwork, D. 1999. Health conditions of immigrant Jews on the lower east side of New York: 1880-1914. Medical History 25(1):1-40.
Edmond, R. 2006. Leprosy and empire: a medical and cultural history. Cambridge, UK: Cambridge University Press.
Elefsiniotis, I. S., I. Glynou, I. Zorou, I. Magaziotou, H. Brokalaki, E. Apostolopoulou, E. Vezali, H. Kada, and G. Saroglou. 2009. Surveillance for hepatitis B virus infection in pregnant women in Greece shows high rates of chronic infection among immigrants and low vaccination-induced protection rates: preliminary results of a single center study. Eurosurveillance 14(9), http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19132 (accessed March 13, 2009).
Enserink, M. 2007. Infectious diseases. Chikungunya: no longer a third world disease. Science 318(5858):1860-1861.
Epstein, J. M., D. M. Goedecke, F. Yu, R. J. Morris, D. K. Wagener, and G. B. Bobashev. 2007. Controlling pandemic flu: the value of international air travel restrictions. PLoS ONE 2(5):e401.
Fairchild, A. L. 2004. Policies of inclusion: immigrants, disease, dependency, and American immigration policy at the dawn and dusk of the 20th century. American Journal of Public Health 94(4):528–539.
Falzon, D., and F. Aït-Belghiti. 2007. What is tuberculosis surveillance in the European Union telling us? Clinical Infectious Diseases 44(10):1261-1267.
Findlay, G. M. 1946. The internal combustion engine and the spread of disease. British Medical Journal 2(4486):979-982.
Gartside, V. O. B. 1949. A danger to public health. British Medical Journal 1(4611):911.
Gellert, G. A. 1993. International migration and control of communicable diseases. Social Science and Medicine 37(12):1489-1499.
Gibney, M. J., and R. Hansen. 2005. Immigration and asylum: from 1900 to the present. Santa Barbara, CA: ABC-CLIO, Ltd.
Gill, G., S. Burrell, and J. Brown. 2001. Fear and frustration—the Liverpool cholera riots of 1832. Lancet 358(9277):233-237.
Goodman, N. M. 1952. International health organizations and their work. Philadelphia, PA: The Blakiston Company.
Gottschalk, R., J. Dreesman, K. Leitmeyer, and G. Krause. 2009. Infectious disease emergencies: responsibility of municipal, state and federal health protection authorities with reference to the international health regulations. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 52(2):183-192.
Gupta, S., and F. L. Altice. 2009. Hepatitis B virus infection in U.S. correctional facilities: a review of diagnosis, management, and public health implications. Journal of Urban Health 86(2):263-279.
Gushulak, B. D., and D. W. MacPherson. 2000. Population mobility and infectious diseases: the diminishing impact of classical infectious diseases and new approaches for the 21st century. Clinical Infectious Diseases 31(3):776-780.
———. 2004. Population mobility and health: an overview of the relationships between movement and population health. Journal of Travel Medicine 11(3):171–178.
———. 2006. Migration medicine and health: principles and practice. Hamilton, Canada: BC Decker.
The Hague Process on Migration and Refugees and UNESCO. 2008. People on the move: handbook of selected terms and concepts, version 1.0, http://www.thehagueprocess.org/upload/pdf/PDFHandbookWEBSITE.pdf (accessed March 10, 2009).
Halstead, S. B. 2007. Dengue. Lancet 370(9599):1644-1652.
Harper, K. N., P. S. Ocampo, B. M. Steiner, R. W. George, M. S. Silverman, S. Bolotin, A. Pillay, N. J. Saunders, and G. J. Armelagos. 2008. On the origin of the treponematoses: a phylogenetic approach. PLoS Neglected Tropical Diseases 2(1):e148.
Hayes, E. B., and D. J. Gubler. 2006. West Nile virus: epidemiology and clinical features of an emerging epidemic in the United States. Annual Review of Medicine 57:181-194.
Herlihy, D. 1997. The Black Death and the transformation of the west. Cambridge, MA: Harvard University Press.
Heywood, P., J. Cutler, K. Burrows, C. Komorowski, B. Marshall, and H. L. Wang. 2007. A community outbreak of travel-acquired hepatitis A transmitted by an infected food handler. Canadian Communicable Disease Report 33(11):16-22.
Hillebrand, E. 2007. Too many or too few? Demographic growth and international migration. Compass 2020. Berlin: Friedrich-Ebert-Stiftung.
Hinman, A. R., W. A. Orenstein, and M. J. Papania. 2004. Evolution of measles elimination strategies in the United States. Journal of Infectious Diseases 189(Suppl 1):S17-S22.
Hotez, P. J. 2008. Neglected infections of poverty in the United States of America. PLoS Neglected Tropical Diseases 2(6):e256.
Howard-Jones, N. 1975. The scientific background of the International Sanitary Conferences 1851-1938. Geneva: WHO, http://whqlibdoc.who.int/publications/1975/14549_eng.pdf (accessed July 1, 2009).
IATA (International Air Transport Association). 2007. Total passenger traffic results, http://www.iata.org/ps/publications/2007-results.htm (accessed January 22, 2009).
———. 2009. History–part 3, http://www.iata.org/about/history_3.htm (accessed January 22, 2009).
ILO (International Labour Office). 2009. International labour migration and development: the ILO perspective, http://www.ilo.org/public/english/protection/migrant/download/mig_brief_development.pdf (accessed March 3, 2009).
Immigration New Zealand. 2005. Medical and chest x-ray certificate, form 1007, http://www.immigration.govt.nz/NR/rdonlyres/DE431E92-0ADE-4B5F-81F9-18DF08E5B2EA/0/1007.pdf (accessed March 1, 2009).
Imperato, P. J., and G. H. Imperato. 2008. The medical exclusion of an immigrant to the United States of America in the early twentieth century. The case of Cristina Imparato. Journal of Community Health 33(4):225-240.
International Organization for Migration. 2008. The world migration report 2008. Geneva, Switzerland.
IOM (Institute of Medicine). 1992. Emerging infections: microbial threats to health in the United States. Washington, DC: National Academy Press.
Khan, K., J. Arino, W. Hu, P. Raposo, J. Sears, F. Calderon, C. Heidebrecht, M. Macdonald, J. Liauw, A. Chan, and M. Gardham. 2009. Spread of a novel influenza A (H1N1) vrus via global airline transportation. New England Journal of Medicine 361(2):212-214.
Kicman-Gawłowska, A. 2008. The prophylaxis of communicable diseases in points of entry under the International Health Regulations (2005). Przeglad Epidemiologiczy 62(4):751-758.
Kim, S. R., M. Kudo, O. Hino, K. H. Han, Y. H. Chung, H. S. Lee, and the Organizing Committee of Japan-Korea Liver Symposium. 2008. Epidemiology of hepatocellular carcinoma in Japan and Korea: a review. Oncology 75(Suppl 1):13-16.
Leder, K., S. Tong, L. Weld, K. C. Kain, A. Wilder-Smith, F. von Sonnenburg, J. Black, G. V. Brown, and J. Torresi. 2006. Illness in travelers visiting friends and relatives: a review of the GeoSentinel Surveillance Network. Clinical Infectious Diseases 43(9):1185-1193.
Lemaitre, G. 2005. The comparability of international migration statistics problems and prospects. OECD Statistics Brief Vol. 9, http://www.oecd.org/dataoecd/60/44/36064929.pdf (accessed July 29, 2008).
Lucaccini, L. F. 1996. The public health service on Angel Island. Public Health Reports 111(1): 92–94.
Mackenbach, J. P. 2009. Politics is nothing but medicine at a larger scale: reflections on public health’s biggest idea. Journal of Epidemiology and Community Health 63(3):181-184.
MacPherson, D. W., and B. D. Gushulak. 2001. Human mobility and population health. New approaches in a globalizing world. Perspectives in Biology and Medicine 44(3):390-401.
MacPherson, D. W., B. D. Gushulak, and L. Macdonald. 2007. Health and foreign policy: influences of migration and population mobility. Bulletin of the World Health Organization 85(3):200-206.
McKinnon, M. L., and L. C. Remund Smith. 1962. Quarantine inspection of international air travelers. Public Health Reports 77(1):65-69.
Milei, J., R. A. Guerri-Guttenberg, D. R. Grana, and R. Storino. 2009. Prognostic impact of Chagas disease in the United States. American Heart Journal 157(1):22-29.
Miller, M. A., C. Viboud, M. Balinska, and L. Simonsen. 2009. The signature features of influenza pandemics—implications for policy. New England Journal of Medicine 360(25):2595-2598.
Miller, T. S., and R. Smith-Savage. 2006. Medieval leprosy reconsidered. International Social Science Review 81(1-2):16-28.
Montizambert, F. 1893. The Canadian quarantine system. Public Health Papers and Reports 19:92-103.
Moore, A. C., L. I. Lutwick, P. M. Schantz, J. B. Pilcher, M. Wilson, A. W. Hightower, E. K. Chapnick, E. I. Abter, J. R. Grossman, J. A. Fried, D. A. Ware, X. Haichou, S. S. Hyon, R. L. Barbour, R. Antar, and A. Hakim. 1995. Seroprevalence of cysticercosis in an Orthodox Jewish community. America Journal of Tropical Medicine and Hygiene 53(5):439-442.
Morens, D. M., G. K. Folkers, and A. S. Fauci. 2008. Emerging infections: a perpetual challenge. Lancet Infectious Diseases 8(11):710-719.
New York Times. 1960. Air travel gains over sea voyages: twice as many fly between U.S. and Europe as go by ship in first half of ’60. August 28. P. S16.
NIC (U.S. National Intelligence Council). 2008. Strategic implications of global health. Document ICA 2008-10D, http://www.odni.gov/nic/PDF_GIF_otherprod/ICA_Global_Health_2008.pdf (accessed March 3, 2009).
Ohno, T., M. Sugimoto, A. Nagashima, H. Ogiwara, R. K. Vilaichone, V. Mahachai, D. Y. Graham, and Y. Yamaoka. 2009. Relationship between Helicobacter pylori hopQ genotype and clinical outcome in Asian and Western populations. Journal of Gastroenterology and Hepatology 24(3):462-468.
Palumbo, E., G. Scotto, D. C. Cibelli, G. Faleo, A. Saracin, and G. Angarano. 2008. Immigration and hepatitis B virus: epidemiological, clinical and therapeutic aspects. Eastern Mediterranean Health Journal 14(4):784-790.
Parascandola, J. 1998. Doctors at the gate: PHS at Ellis Island. Public Health Reports 113:83-86.
Payne, L., and D. Coulombier. 2009. Hepatitis A in the European Union: responding to challenges related to new epidemiological patterns. Eurosurveillance 14(3), http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19101 (accessed March 3, 2009).
Population Reference Bureau. 2008a. 2008 World population data sheet, http://www.prb.org/pdf08/08WPDS_Eng.pdf (accessed January 19, 2009).
———. 2008b. Population growth, http://www.prb.org/Educators/TeachersGuides/HumanPopulation/PopulationGrowth.aspx (accessed January 21, 2009).
Primo-Carpenter, J., and M. McGinnis. 2009. Matrix of drug quality reports in USAID-assisted countries. Rockville, MD: U.S. Pharmacopeia Drug Quality and Information Program, http://www.usp.org/pdf/EN/dqi/ghcDrugQualityMatrix.pdf (accessed June 8, 2009).
Reynolds, D. 2001. One world divisible: a global history since 1945. New York: W. W. Norton.
Robson, D., N. J. Beeching, and G. V. Gill. 2009. Strongyloides hyperinfection syndrome in British veterans. Annals of Tropical Medicine and Parasitology 103(2):145-148.
Salvana, E. M., and C. H. King. 2008. Schistosomiasis in travelers and immigrants. Current Infectious Disease Reports 10(1):42-49.
Samaan, G., M. Patel, J. Spencer, and L. Roberts. 2004. Border screening for SARS in Australia: what has been learnt? Medical Journal of Australia 180(5):220-223.
Schantz, P. M., A. C. Moore, J. L. Muñoz, B. J. Hartman, J. A. Schaefer, A. M. Aron, D. Persaud, E. Sarti, M. Wilson, and A. Flisser. 1992. Neurocysticercosis in an Orthodox Jewish community in New York City. New England Journal of Medicine 327(10):692-695.
Schwartzman, K., O. Oxlade, R. G. Barr, F. Grimard, I. Acosta, J. Baez, E. Ferreira, R. E. Melgen, W. Morose, A. C. Salgado, V. Jacquet, S. Maloney, K. Laserson, A. P. Mendez, and D. Menzies. 2005. Domestic returns from investment in the control of tuberculosis in other countries. New England Journal of Medicine 353(10):1008-1020.
Sheth, A. N., P. Wiersma, D. Atrubin, V. Dubey, D. Zink, G. Skinner, F. Doerr, P. Juliao, G. Gonzalez, C. Burnett, C. Drenzek, C. Shuler, J. Austin, A. Ellis, S. Maslanka, and J. Sobel. 2008. International outbreak of severe botulism with prolonged toxemia caused by commercial carrot juice. Clinical Infectious Diseases 47(10):1245-1251.
Simon, F., H. Savini, and P. Parola. 2008. Chikungunya: a paradigm of emergence and globalization of vector-borne diseases. Medical Clinics of North America. 92(6):1323-1343.
Soper, F. L., and D. B. Wilson. 1943. Anopheles gambiae in Brazil: 1930 to 1940. New York: Rockefeller Foundation.
SOS International. 2009. Pandemic preparedness—airport screening, http://www.internationalsos.com/PandemicPreparedness/SubCatLevel.aspx?li=5&languageID=ENG&subCatID=87 (accessed July 1, 2009).
St. John, R. K., A. King, D. de Jong, M. Bodie-Collins, S. G. Squires, and T. W. Tam. 2005. Border screening for SARS. Emerging Infectious Diseases 11(1):6-10.
Stark, D., S. van Hal, R. Lee, D. Marriott, and J. Harkness. 2008. Leishmaniasis, an emerging imported infection: report of 20 cases from Australia. Journal of Travel Medicine 15(5):351-354.
Stauffer, W. M., M. Weinberg, R. D. Newman, L. M. Causer, M. J. Hamel, L. Slutsker, and M. S. Cetron. 2008. Pre-departure and post-arrival management of P. falciparum malaria in refugees relocating from sub-Saharan Africa to the United States. American Journal of Tropical Medicine and Hygiene 79(2):141-146.
Stern, A. M., and H. Markel. 1999. All quiet on the third coast: medical inspections of immigrants in Michigan. Public Health Reports 114(2):178-182.
Suhrke, A., and F. Klink. 1987. Contrasting patterns of Asian refugee movements: the Vietnamese and Afghan syndromes. In Pacific bridges: the new immigration from Asia and the Pacific Islands, edited by J. T. Fawcett and B. V. Carino. Staten Island, NY: Center for Migration Studies. Pp. 85-102.
Svoboda, T., B. Henry, L. Shulman, E. Kennedy, E. Rea, W. Ng, T. Wallington, B. Yaffe, E. Gournis, E. Vicencio, S. Basrur, and R. H. Glazier. 2004. Public health measures to control the spread of the severe acute respiratory syndrome during the outbreak in Toronto. New England Journal of Medicine 350(23):2352-2361.
Tatem, A. J., D. J. Rogers, and S. I. Hay. 2006. Global transport networks and infectious disease spread. Advances in Parasitology 62:297-347.
Trifonov, V., H. Khiabanian, and R. Rabadan. 2009. Geographic dependence, surveillance, and origins of the 2009 influenza A (H1N1) virus. New England Journal of Medicine 361(2):115-119.
UK Department of Health. 2007. Pandemic flu: a national framework for responding to an influenza pandemic. The Department, London, http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_080734 (accessed March 3, 2009).
Umemura, T., T. Ichijo, K. Yoshizawa, E. Tanaka, and K. Kiyosawa. 2009. Epidemiology of hepatocellular carcinoma in Japan. Journal of Gastroenterology 44(Suppl 19):102-107.
UN (United Nations). 1998. Department of Economic and Social Affairs Statistics Division. Recommendations on statistics of international migration. Revision 1. Statistical Papers Series M, No. 58, Rev. 1. New York: The Organization, http://unstats.un.org/unsd/publication/SeriesM/SeriesM_58rev1E.pdf (accessed, November 10, 2008).
———. 2009a. Growth in United Nations membership, 1945-present, http://www.un.org/members/growth.shtml (accessed January 14, 2009).
———. 2009b. List of member states, http://www.un.org/members/list.shtml (accessed March 8, 2009).
UNWTO (United Nations World Tourism Organization). 2009. International tourism challenged by deteriorating global economy. World Tourism Barometer 7(1), http://unwto.org/facts/eng/pdf/barometer/UNWTO_Barom09_1_en_excerpt.pdf (accessed February 15, 2009).
Wachtel, M. R., J. L. McEvoy, Y. Luo, A. M. Williams-Campbell, and M. B. Solomon. 2003. Cross-contamination of lettuce (Lactuca sativa L.) with Escherichia coli O157:H7 via contaminated ground beef. Journal of Food Protection 66(7):1176-1183.
Waldvogel, F. A. 2004. Infectious diseases in the 21st century: old challenges and new opportunities. International Journal of Infectious Diseases 8(1):5-12.
Welshman, J., and A. Bashford. 2006. Tuberculosis, migration, and medical examination: lessons from history. Journal of Epidemiology and Community Health 60:282-284.
WHO (World Health Organization). 2006. WHO pandemic influenza draft protocol for rapid response and containment. Updated draft May 30, 2006, http://www.who.int/csr/disease/avian_influenza/guidelines/protocolfinal30_05_06a.pdf (accessed March 4, 2009).
———. 2008. Health of migrants, 61st WHA, WHA61.17. Geneva, Switzerland: WHO, http://www.who.int/gb/ebwha/pdf_files/A61/A61_R17-en.pdf (accessed November 2, 2008).
———. 2009a. Is it safe to travel?, http://www.who.int/csr/disease/swineflu/frequently_asked_questions/travel/en/index.html (accessed July 1, 2009).
———. 2009b. Influenza A(H1N1)—update 7, http://www.who.int/csr/don/2009_05_01/en/index.html (accessed July 1, 2009)
———. 2009c. World now at the start of 2009 influenza pandemic, http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/index.html (accessed July 1, 2009).
———. 2009d. Epidemic and pandemic alert and response, http://www.who.int/csr/en/ (accessed February 20, 2009).
———. 2009e. Epidemic and pandemic alert and response. Global Outbreak and Response Network, http://www.who.int/csr/outbreaknetwork/en/ (accessed February 20, 2009).
Wolfe, N. D., P. Daszak, A. M. Kilpatrick, and D. S. Burke. 2005. Bushmeat hunting, deforestation, and prediction of zoonotic disease emergence. Emerging Infectious Diseases 11(12):1822-1827.
World Bank. 2008. Chapter 5. Factor mobility and migration. In World development report 2009 “reshaping economic geography.” Washington, DC: World Bank, http://siteresources.worldbank.org/INTWDR2009/Resources/4231006-1225840759068/WDR09_11_Ch05web.pdf (accessed March 1, 2009).
World Resources Institute. 2009. Earth trends—the environmental information portal. Population, Health, and Human Well-being. Country Profiles, http://earthtrends.wri.org/country_profiles/index.php?theme=4 (accessed February 16, 2009).
Yankus, W. 2006. Counterfeit drugs: coming to a pharmacy near you. American Council on Science and Health, http://www.acsh.org/publications/pubID.1384/pub_detail.asp (accessed June 8, 2009).
Yew, E. 1980. Medical inspection of immigrants at Ellis Island, 1891-1924. Bulletin of the New York Academy of Medicine 56(5):488-510.
Zlotnik, H. 2003. The global dimensions of female migration. Migration Policy Institute, http://www.migrationinformation.org/feature/display.cfm?ID=109 (accessed March 2, 2009).















































